comment je traite un patient infecté par le vih aux ... · primo-infection symptomatique...
TRANSCRIPT

Comment je traite un patient infecté par le
VIH aux différents stades de la maladie ?
Tristan FERRY
Service de Maladies Infectieuses et Tropicales Hôpital de la Croix-Rousse,
Université Claude Bernard Lyon1, Lyon
Unité INSERM U851, Pathogénie Bactérienne et Immunité Innée, Centre National de Référence des Staphylocoques,
Faculté de Médecine Laennec, Lyon

Qu
an
tité
Activation immune
Virémie
Lymphocytes CD4+ circulants
Lymphocytes CD4+ muqueux
4–8
semaines
Aiguë
5-15 ans
Chronique 2-3 ans
SIDA
Les différents stades

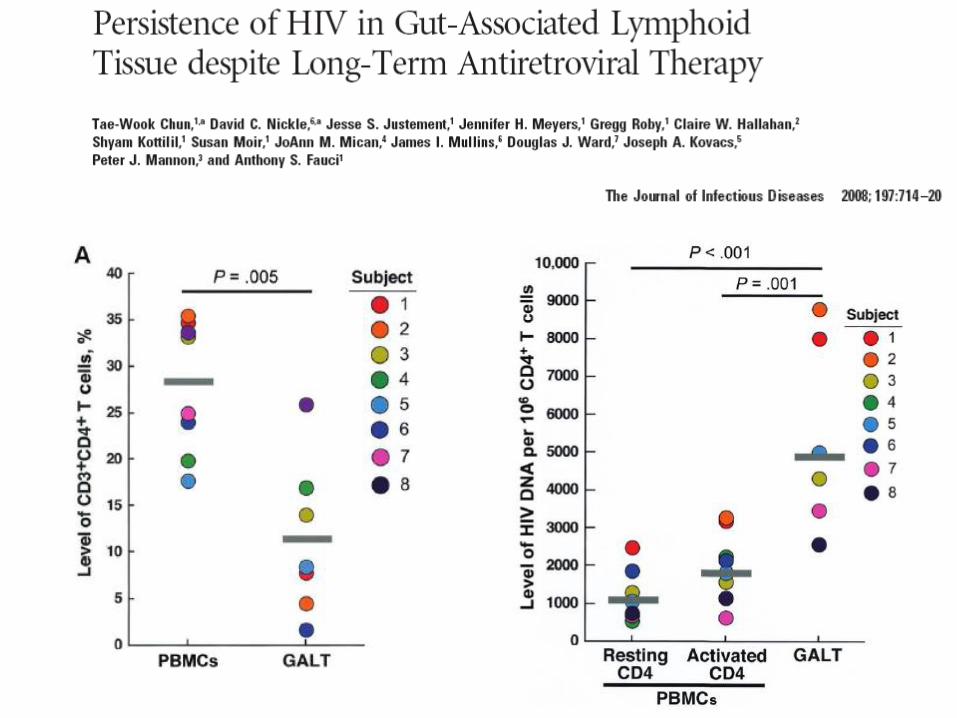
Primoinfection et réservoir

Primoinfection et réservoir
• Le réservoir s’établie pendant la phase de primoinfection
• Présence du génome viral dans les tissus – Tube digestif
– Tissu lymphoïde (plaque de payer)
– Tissu cérébral
Thérapeutique aux différents stades
• Initiations de traitement « usuelles » – Stade SIDA
• Traitement de l’infection opportuniste
• Traitement antirétroviral
– Stade d’infection chronique
• Switch pour multirésistance
• Simplification thérapeutiques ou « allègement »
• Intensification thérapeutique pour espérer réduire le réservoir – Dès la primoinfection
– Au cours de l’infection chronique chez le patient indétectable
Sont exclus de la présentation :
- co-infection VIH/hépatites
- femmes enceintes

Thérapeutique aux différents stades
• Initiations de traitement « usuelles » – Stade SIDA
• Traitement de l’infection opportuniste
• Traitement antirétroviral
– Stade d’infection chronique
• Switch pour multirésistance
• Simplification thérapeutiques ou « allègement »
• Intensification thérapeutique pour espérer réduire le réservoir – Dès la primoinfection
– Au cours de l’infection chronique chez le patient indétectable
Sont exclus de la présentation :
- co-infection VIH/hépatites
- femmes enceintes

PIs
NNRTIs
NRTIs
Fusion Inhibitors (FIs)
Inhibiteur du CCR5
Inhibiteur d’intégrase

Les ARV depuis 1987…
AZT ddI
ddC d4T
SQV
3TC
RTV
IDV
NVP
NFV
DLV
EFV
ABC APV
LPV/
RTV TDF
TPV DRV
ATV
FPV
ENF
FTC
0
5
10
15
20
25
1987 2010
MRV
RTG
Efficacité partielle
Résistance
1996 HAART
HIGHLY ACTIVE ART
RPV

Molécules disponibles en 2012
NNRTIs
Efavirenz (EFV)
Nevirapine (NVP)
Etravirine (ETV)
Rilpivirine (RPV)
PIs
Ritonavir (RTV)
Fosamprenavir (FPV)
Indinavir (IDV)
Saquinavir (SQV hgc)
Tipranavir (TPV)
Lopinavir/ritonavir (LPV/RTV)
Atazanavir (ATV)
Darunavir (DRV)
Didanosine (ddI) Stavudine (D4T) Zidovudine (AZT)
Abacavir (ABC) Lamivudine (3TC) Emtricitabine (FTC) Tenofovir (TDF)
3TC/ABC/AZT 3TC/ABC 3TC/AZT FTC/TDF
NRTIs
Fusion Inhibitors (FIs)
Enfuvirtide (ENF)
Inhibiteur d’intégrase
Raltegravir (RTG)*
Inhibiteur du CCR5
Maraviroc (MRV)*

La trithérapie ou HAART basée sur un
“backbone” : association de 2 NRTI
N R
T
I
N R
T
I
N R
T
I
N R
T
I
N N R T I I P boosté
HAART Backbone
=
2 NRTI

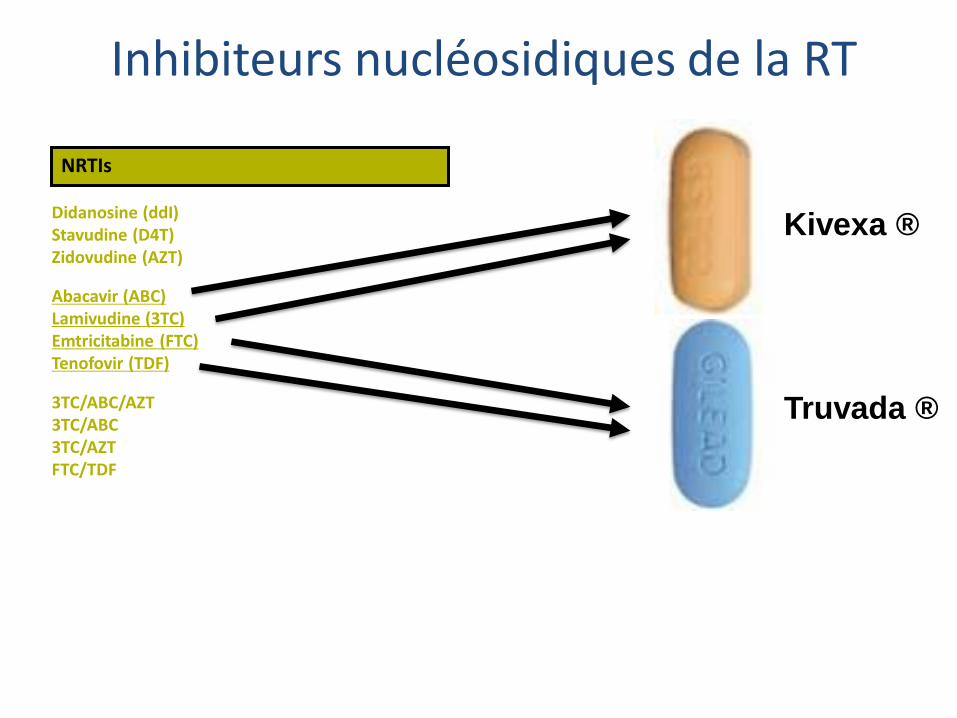
Inhibiteurs nucléosidiques de la RT
Didanosine (ddI) Stavudine (D4T) Zidovudine (AZT)
Abacavir (ABC) Lamivudine (3TC) Emtricitabine (FTC) Tenofovir (TDF)
3TC/ABC/AZT 3TC/ABC 3TC/AZT FTC/TDF
NRTIs
Activité antirétrovirale
Inhibe la transcriptase inverse du VIH
Arrêt de l’élongation de l’ADN
Avantages
Peu d’interaction médicamenteuses
Peu de prise par jour
Formes combinées
Mais…
Toxicité « familiale » par inhibition de l’ADN pol mitochondriale Toxicité spécifique de chacune des molécules
Didanosine (ddI) Stavudine (D4T) Zidovudine (AZT)
Abacavir (ABC) Lamivudine (3TC) Emtricitabine (FTC) Tenofovir (TDF)
3TC/ABC/AZT 3TC/ABC 3TC/AZT FTC/TDF
NRTIs
Kivexa ®
Truvada ®
Inhibiteurs nucléosidiques de la RT

NNRTIs
Efavirenz (EFV)
Nevirapine (NVP)
Etravirine (ETV)
Rilpivirine (RPV)
Activité antirétrovirale Inhibe la transcriptase inverse du VIH
Altère sa capacité à synthétiser l’ADN
Avantages ½ longue (EFV)
Peu de toxicité au long terme
Mais… Toxicité immédiate « familiale » Hypersensibilité Rash
Toxicité immédiate spécifique (EFV) Inducteur enzymatique Faible barrière génétique 1 seule mutation suffit à conférer une résistance « à toute la famille »
Vertiges Cauchemars Sd dépressif
Inhibiteurs NON nucléosidiques de la RT

Molécules disponibles en 2012
NNRTIs
Efavirenz (EFV)
Nevirapine (NVP)
Etravirine (ETV)*
Didanosine (ddI) Stavudine (D4T) Zidovudine (AZT)
Abacavir (ABC) Lamivudine (3TC) Emtricitabine (FTC) Tenofovir (TDF)
3TC/ABC/AZT 3TC/ABC 3TC/ZDV FTC/TDF
NRTIs
Kivexa ®
Truvada ®
Atripla ®
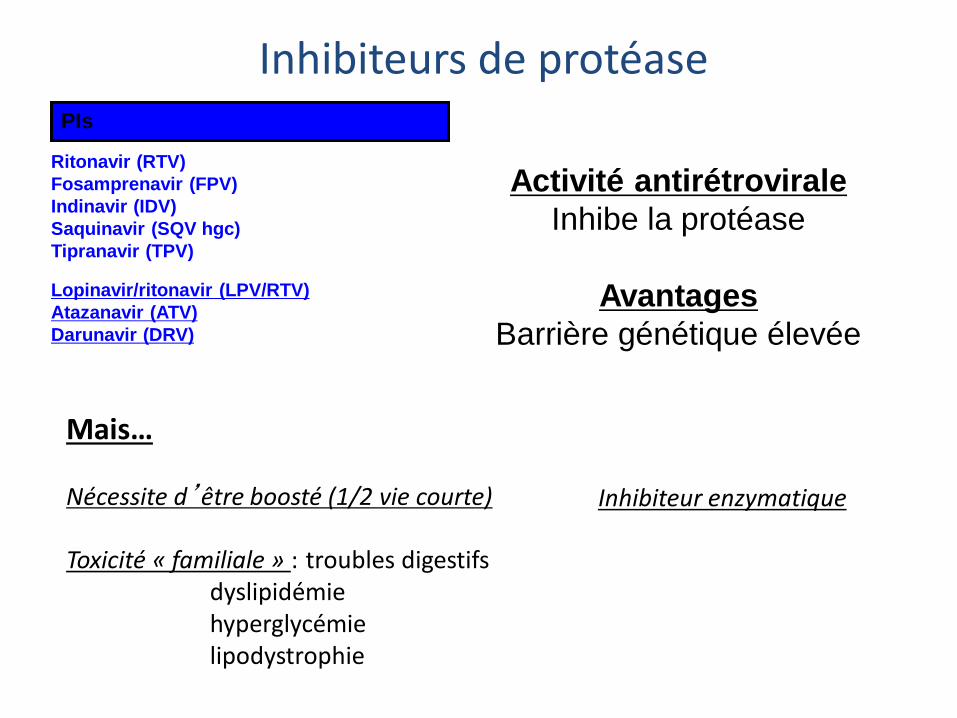
Inhibiteurs de protéase PIs
Ritonavir (RTV)
Fosamprenavir (FPV)
Indinavir (IDV)
Saquinavir (SQV hgc)
Tipranavir (TPV)
Lopinavir/ritonavir (LPV/RTV)
Atazanavir (ATV)
Darunavir (DRV)
Activité antirétrovirale
Inhibe la protéase
Avantages
Barrière génétique élevée
Mais… Nécessite d’être boosté (1/2 vie courte) Toxicité « familiale » : troubles digestifs dyslipidémie hyperglycémie lipodystrophie
Inhibiteur enzymatique

Utilisation du ritonavir comme booster • Le ritonavir est le plus puissant inhibiteur du CYP3A4
• Augmente la concentration des autres IP lorsqu’il est utilisé à petites doses (100 mg/prise) en diminuant leur métabolisme par le CYP3A

• Le boost réduit la survenue de résistance aux IP
• Le boost réduit également la survenue de résistance aux INRT
Kempf DJ, et al. J Infect Dis 2004;189:51-60.
Incidence de la résistance après traitement initial par HAART avec IP boosté ou non

NNRTI IP boosté
M184V 35,3% 21%
K65R 5,3% 0%
≥ 1 TAM 1,5% 0,6%
Résistance
IP ou NNRTI
53% 0,9%
p< 0,001
P= 0,01
p< 0,001
P= 0,62
R. GUPTA et al ; CID 2008 , 47, 712-22
IP boostés versus INNRTI

PIs
Ritonavir (RTV)
Fosamprenavir (FPV)
Indinavir (IDV)
Saquinavir (SQV hgc)
Tipranavir (TPV)
Lopinavir/ritonavir (LPV/RTV)
Atazanavir (ATV)
Darunavir (DRV)
Inhibiteurs de protéase

PIs
Ritonavir (RTV)
Fosamprenavir (FPV)
Indinavir (IDV)
Saquinavir (SQV hgc)
Tipranavir (TPV)
Lopinavir/ritonavir (LPV/RTV)
Atazanavir (ATV)
Darunavir (DRV)
Inhibiteurs de protéase
PIs
Ritonavir (RTV)
Fosamprenavir (FPV)
Indinavir (IDV)
Saquinavir (SQV hgc)
Tipranavir (TPV)
Lopinavir/ritonavir (LPV/RTV)
Atazanavir (ATV)
Darunavir (DRV)
Inhibiteurs de protéase

Les objectifs du traitement ARV
Charge virale indétectable (<50 copies/mL):
◦ Maximalise la restauration immunitaire,
◦ Minimise le risque de transmission,
◦ Minimise la pression de sélection.
CD4+ > 500/mm3 :
◦ Pendant plus de 3 ans, mortalité identique à
celles des personnes VIH séronégatives.
Amélioration de la tolérance du traitement et
de la qualité de vie

Mortality in HIV+ Pts Similar to General Population When CD4 > 500 for 5-7 Yrs
• Overall mortality in HIV-infected patients 7-fold higher than general population
• After 6th year of follow-up, mortality among patients with CD4+ cell counts ≥ 500 cells/mm3 comparable to that of the general population
Lewden C, et al. J Acquir Immune Defic Syndr. 2007;46:72-77.
Truncation for Duration of Follow-up, Yrs
Median Time Spent With CD4+ Cell Count ≥ 500 cells/mm3 After Truncated
Duration of Follow-up, Yrs (IQR)
Deaths, n SMR (95% CI)
0 (n = 1208) 4.5 (2.1-7.0) 37 2.5 (1.8-3.5)
1 (n = 1156) 4.2 (2.1-6.4) 29 2.1 (1.4-3.1)
2 (n = 1083) 4.0 (2.1-5.6) 26 2.2 (1.4-3.2)
3 (n = 1031) 3.5 (1.8-4.8) 22 2.1 (1.3-3.2)
4 (n = 967) 3.0 (1.5-3.8) 18 2.1 (1.3-3.4)
5 (n = 864) 2.4 (1.4-3.0) 12 1.9 (1.0-3.2)
6 (n = 763) 1.6 (1.0-2.2) 2 0.5 (0.1-1.6)
7 (n = 610) 0.9 (0.5-1.3) 1 0.5 (0.0-2.6)

Les objectifs du traitement ARV
Test de génotypage pour guider le choix des ARV (7-10 j)
M1 : charge virale doit diminuer d’au moins 2 log10,
M3 : charge virale doit être < 400 copies/mL,
M6 : charge virale doit être indétectable (<50 copies/mL)

Quand débuter le traitement ARV en 2013
Stade C, après le traitement de l’IO
Stade B (candidose oropharyngé, zona, etc.),
Stade A (asymptomatique):
◦ < 350 CD4+/mm3 (ou 15%),
◦ < 500 CD4+/mm3, nouveauté 2010
◦ > 500 CD4+/mm3, non recommandé
- Sauf si :
Primo-infection symptomatique (neurologique : méningite ou paralysie faciale)
Femme enceinte
- Possible si :
◦Age de plus de 50 ans, FRCV,
◦Charge virales > 5 log10, Co-infection VHB ou VHC,
◦Baisse rapide des CD4, HIV-associated nephropathy (HIVAN)

1ère intention EFV+TDF+FTC Si pas de R et si pas Psy, observance et rein OK
ABC+3TC Si HLA B5701-
TDF+FTC Si rein OK
+
NNRTI
RTV/ATV
RTV/DRV
RTV/LPV
IP

Preferred/Recommended
Regimens: DHHS and IAS-USA
*IAS-USA: based on extensive clinical experience. †DHHS: should not be used in first trimester of pregnancy or in women trying to conceive or not using
effective and consistent contraception. ǂDHHS: should not be used in patients who require > 20 mg omeprazole equivalent per day. §IAS-USA: based on data that indicate that this agent is comparable to key third agents but more limited
experience in naive patients.
EFV*† ATV/RTV*ǂ
DRV/RTV§ RAL§
TDF/FTC +
DHHS Guidelines. October 2011. Thompson MA, et al. JAMA. 2010;304;321-333.

ECHO/THRIVE: Rilpivirine vs Efavirenz in
Treatment-Naive Patients
• D/C due to AE more common with EFV vs RPV: 8.5% vs 4.1%
• More virologic failures with RPV vs EFV: 14% vs 7.6%
– Difference due to more VF between Wks 0-48 at HIV-1 RNA > 100,000; VF similar Wks 48-96
– NRTI mutations more common with VF on RPV vs EFV
– Cross-resistance to ETR more common with RPV failure (E138K mutation)
100
80
60
40
20
0
HIV
-1 R
NA
< 5
0 c/
mL
(%)
78%
78%
RPV 25 mg QD (n = 686) EFV 600 mg QD (n = 682)
Wks
0 4 8 12 16 24 32 40 48 60 72 84 96 2
84%
82%
Cohen C, et al. AIDS 2010. Abstract THLBB206. Cohen C, et al. Lancet. 2011;378:229-237.
Molina JM, et al. Lancet. 2011;378:238-246. Cohen C, et al. CROI 2012. Abstract 626.

ECHO, THRIVE: Response to RPV vs EFV
in Patients With High VL, Low CD4
• Reduced response to RPV vs EFV at VL > 100,000 copies/mL and
CD4+ cell counts < 200 cells/mm³
-3.6 (-9.8 to +2.5)
> 100,000 copies/mL
125/ 165
121/ 153
246/ 318
149/ 181
136/ 171
285/ 352
77 81 79 80
76 82
Pat
ien
ts (
%)
40
0
100
20
80
60
Pooled THRIVE ECHO
HIV-1 RNA < 50 copies/mL at Wk 48 by Baseline VL
6.6 (1.6-11.5)
≤ 100,000 copies/mL
162/ 181
170/ 187
332/ 368
136/ 163
140/ 167
276/ 330
90 83
91 84
90 84
Pat
ien
ts (
%)
40
0
100
20
80
60
ECHO THRIVE Pooled
EFV Rilpivirine
Cohen C, et al. AIDS 2010. Abstract THLBB206. Cohen C, et al. Lancet. 2011;378:229-237.
Molina JM, et al. Lancet. 2011;378:238-246. Cohen C, et al. CROI 2012. Abstract 626.


Elvitegravir/Cobicistat/TDF/FTC vs
EFV/TDF/FTC in Treatment-Naive Patients
• Multicenter, randomized, double-blinded, active-
controlled phase III study
Sax P, et al. Lancet. 2012 Jun 30;379:2439-48.
HIV-infected treatment-naive patients with HIV-1 RNA ≥ 5000 copies/mL,
any CD4+ cell count, CrCl ≥ 70 mL/min
(N = 700)
Wk 48
primary analysis
Elvitegravir/Cobicistat/TDF/FTC QD
+ EFV/TDF/FTC placebo QD
(n = 348)
EFV/TDF/FTC QD + Elvitegravir/Cobicistat/TDF/FTC placebo QD
(n = 352)
Planned follow-up
to Wk 192 Stratified by
baseline HIV-1 RNA
> or ≤ 100,000 copies/mL

Elvitegravir/Cobicistat Regimen Noninferior
to EFV Regimen at Wk 48
• Greater CD4+ count increase with EVG/COBI vs EFV: 239 vs 206 cells/mm3 (P = .009)
• Among pts with confirmed virologic failure or rebound, resistance detected in 8/14 pts in
EVG/COBI arm vs 8/17 pts in EFV arm
– Primary integrase mutations and primary NNRTI mutations observed in 7 and 8 pts in EVG/COBI and
EFV arms, respectively
– All 8 pts in EVG/COBI arm had M184V/I mutation vs 2 pts in EFV arm; 3 and 2 had K65R, respectively
84 82
HIV-1 RNA > 100,000 c/mL
90 85
0
20
40
60
80
100
HIV
-1 R
NA
< 5
0 c
/mL
at
Wk
48
(%
)
88
Overall HIV-1 RNA ≤ 100,000 c/mL
84 EVG/COBI/FTC/TDF (n = 348)
EFV/FTC/TDF (n = 352)
Sax P, et al. Lancet. 2012 Jun 30;379:2439-48.

Safety of Elvitegravir/Cobicistat
Regimen vs EFV Regimen • Significantly greater incidence of nausea with EVG/COBI regimen
• Significantly greater incidence of sleep disturbance, dizziness, rash
with EFV regimen
• 1.4% of patients discontinued EVG/COBI regimen due to renal
abnormalities vs no patients on EFV regimen
– Significantly greater increase in median serum creatinine from
baseline to Wk 48 in EVG/COBI group: 0.14 vs 0.01 mg/dL (P <
.001)
– Majority of increase in serum creatinine clearance occurred
within
2 wks of starting treatment and progressed minimally over time
• Significantly greater increases in total, LDL, and HDL cholesterol
from baseline to Wk 48 in EFV vs EVG/COBI groups (all P ≤ .001)
Sax P, et al. Lancet. 2012 Jun 30;379:2439-48.

Elvitegravir/Cobicistat/TDF/FTC vs ATV/RTV
+ TDF/FTC in Naive Patients
• Multicenter, randomized, double-blinded, active-controlled
phase III study
DeJesus E, et al. Lancet. 2012 Jun 30;379:2429-38
HIV-infected treatment-naive patients,
HIV-1 RNA ≥ 5000 copies/mL, any CD4+ cell count,
CrCl ≥ 70 mL/min
(N = 708)
Wk 48
primary analysis
Elvitegravir/Cobicistat/TDF/FTC QD
+ ATV/RTV + FTC/TDF placebo QD
(n = 353)
ATV/RTV + TDF/FTC QD + Elvitegravir/Cobicistat/TDF/FTC placebo QD
(n = 355)
Planned follow-up
to Wk 192 Stratified by
baseline HIV-1 RNA
> or ≤ 100,000 copies/mL

85 82
93 90 90
87
HIV-1 RNA > 100,000 c/mL
0
20
40
60
80
100
HIV
-1 R
NA
< 5
0 c
/mL
at
Wk
48
(%
)
Overall HIV-1 RNA ≤ 100,000 c/mL
EVG/COBI/|TDF/FTC (n = 353)
ATV/RTV + TDF/FTC (n = 355)
Elvitegravir/Cobicistat Regimen Noninferior
to ATV/RTV Regimen at Wk 48
• Similar CD4+ cell count increases in both study arms at Wk 48
• Among pts with confirmed virologic failure or rebound, resistance detected in
5/12 pts in EVG/COBI arm vs 0/8 pts in ATV/RTV arm
– 4/5 pts in EVG/COBI arm had M184V/I mutation; 4 had primary integrase mutations
DeJesus E, et al. Lancet. 2012 Jun 30;379:2429-38

Safety of Elvitegravir/Cobicistat
Regimen vs ATV/RTV Regimen • Similar rates of grade 3/4 adverse events between arms: 13% in
EVG/COBI and 14% in ATV/RTV arm
– Most common adverse events: diarrhea, nausea
• Grade 3/4 hyperbilirubinemia more common in ATV/RTV group:
58% vs 1%
• Significantly greater increase in median serum creatinine from
baseline to Wk 48 in EVG/COBI group: 0.12 vs 0.08 mg/dL (P <
.001)
– Majority of increase in serum creatinine clearance occurred within 2 wks
of starting treatment and progressed minimally over time
• Significantly greater increase in median triglycerides from baseline
to Wk 48 in ATV/RTV group: 23 vs 8 mg/dL (P = .006); otherwise no
difference in lipid values
DeJesus E, et al. Lancet. 2012 Jun 30;379:2429-38

Les thérapeutiques “de départ” en 2013
Regimen Advantages Disadvantages
EFV based Simplicity
(1 pill once daily) CNS effects may thwart adherence (if concerns about
follow-up)
PI based Once-daily dosing If irregular adherence, least
concern about resistance at VF
No single-tablet regimen or coformulations with NRTIs
Possibility of visible adverse effects that would disclose status
RAL based Minimal adverse effects Few drug-drug interactions
Twice-daily dosing No single-tablet regimen or coformulations with
NRTIs
RPV based Simplicity
(1 pill once daily) Minimal adverse effects
Food requirements Less effective at high HIV-1 RNA count
EVG/COBI based
Simplicity (1 pill once daily)
Minimal adverse effects
Only short-term data available More 2-class resistance in VF than EFV Effect on creatine clearance but no effect on GFR Drug-drug interactions similar to RTV

Thérapeutique aux différents stades
• Initiations de traitement « usuelles » – Stade SIDA
• Traitement de l’infection opportuniste
• Traitement antirétroviral
– Stade d’infection chronique
• Switch pour multirésistance
• Simplification thérapeutiques ou « allègement »
• Intensification thérapeutique pour espérer réduire le réservoir – Dès la primoinfection
– Au cours de l’infection chronique chez le patient indétectable
Sont exclus de la présentation :
- co-infection VIH/hépatites
- femmes enceintes

• Essai ANRS139, multicentrique
non comparatif
• 103 patients, médiane CD4 à J0 :
255/mm3, médiane CV à J0 : 4
log10 c/ml (IQR : 3,6 - 4,6)
• 83 % des patients reçoivent
également des INTI, 12 % ENF
• 14 % reçoivent uniquement la
trithérapie RAL + ETR + DRV/r
(sans autre ARV)
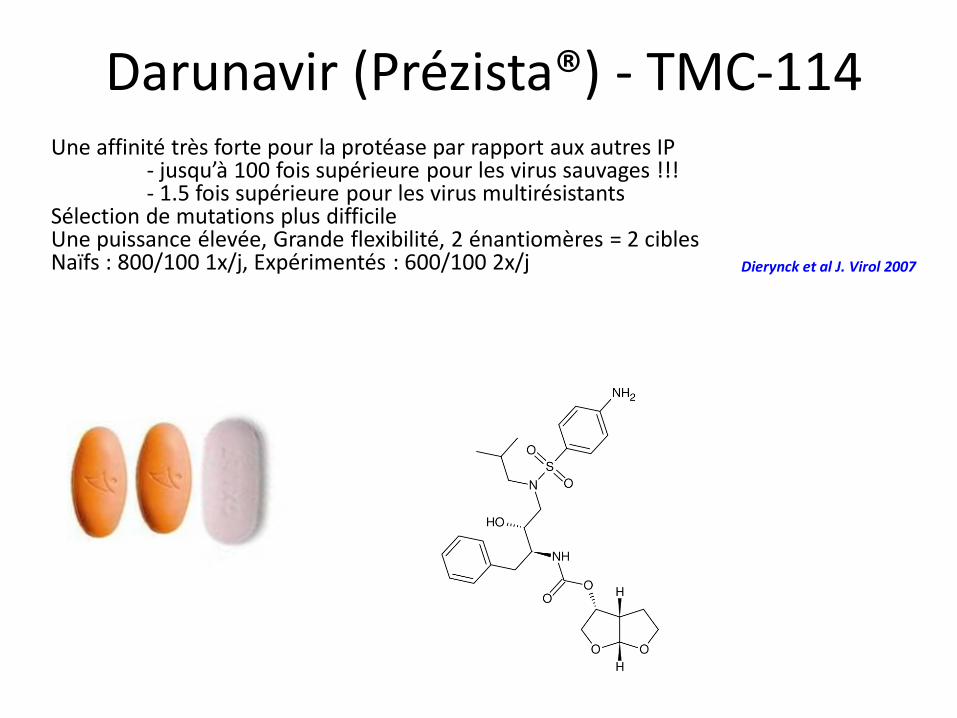
Darunavir (Prézista®) - TMC-114 Une affinité très forte pour la protéase par rapport aux autres IP - jusqu’à 100 fois supérieure pour les virus sauvages !!! - 1.5 fois supérieure pour les virus multirésistants Sélection de mutations plus difficile Une puissance élevée, Grande flexibilité, 2 énantiomères = 2 cibles Naïfs : 800/100 1x/j, Expérimentés : 600/100 2x/j Dierynck et al J. Virol 2007



D’après A.Y. Kovalevsky et al ; J. Mol. Biol. ; 2006 ; 363(1) ; 161-73
LES DEUX ENANTIOMERES DU DARUNAVIR SE FIXENT A DES SITES DIFFERENTS DE LA PROTEASE

Thérapeutique aux différents stades
• Initiations de traitement « usuelles » – Stade SIDA
• Traitement de l’infection opportuniste
• Traitement antirétroviral
– Stade d’infection chronique
• Switch pour multirésistance
• Simplification thérapeutiques ou « allègement »
• Intensification thérapeutique pour espérer réduire le réservoir – Dès la primoinfection
– Au cours de l’infection chronique chez le patient indétectable
Sont exclus de la présentation :
- co-infection VIH/hépatites
- femmes enceintes

Reasons to Consider
Treatment Simplification
• Improve adherence, convenience, and quality of life – Reduce number of doses
– Reduce number of pills
– Reduce number of drugs
– Reduce costs
• Many physicians fear simplification out of perceived risk of tolerability issues and loss of virologic suppression
• However, if simplification is not effective, reverting back to the previous regimen is an option if carefully managed

Claxton AJ, et al. Clin Ther. 2001;23:1296-1310.
Adherence Inversely Related to
Number of Doses per Day
Studies of Electronic Monitoring of Adherence
Mean
Do
se-T
akin
g
Ad
he
ren
ce (
%)
71
0
20
40
80
100
Overall
79
QD
69
BID
65
TID
51
QID
60
P = .008
P < .001
P = .001

Stone VE, et al. J Acquir Immune Defic Syndr. 2004;36:808-816.
HIV-positive patients on ART including ≥ 3 antiretrovirals (N = 299) 6 US cities Self-report questionnaire with aid of facilitator
Not Helpful at All Pills/Day Dosing
Frequency Food Rules Biggest Pill
Extremely Helpful
0
20
40
60
80
100
Mean Relative Impact of Regimen
Features on Adherence

ARV Agents Approved for Once-Daily
Dosing and Fixed-Dose Combinations
Agents Approved for Once-Daily Dosing
Class US EU
NRTIs
ABC 3TC ddI FTC TDF
ABC 3TC ddI FTC TDF
NNRTIs EFV
NVP-XR EFV
NVP-XR
PIs
ATV/RTV FPV/RTV (for tx-naive patients only)
DRV/RTV (for tx-naive patients or tx-exp patients without DRV resistance mutations) LPV/RTV (for tx-naive patients only)
ATV/RTV DRV/RTV (for tx-naive patients or tx-exp patients
without DRV resistance mutations) LPV/RTV (if necessary)
Approved Once-Daily Fixed-Dose Combinations
Class US EU
NRTIs TDF/FTC ABC/3TC
TDF/FTC ABC/3TC
PIs LPV/RTV LPV/RTV
Two drug classes EFV/TDF/FTC RPV/TDF/FTC
EFV/TDF/FTC RPV/TDF/FTC

DHHS Guidelines, October 2011.
• Patients without a history of treatment
failure or drug-resistant virus
• Patients receiving complex regimens
– However, for some forms of treatment
simplification (eg, boosted PI monotherapy),
good adherence is a prerequisite
Optimal Candidates for Treatment
Simplification

• In patients with controlled viremia, simplifying treatment to improve quality of life should be considered[1-4]
• When switching treatment, for whatever reason, maintenance of virologic suppression remains the main concern
• Efficacy and likely adherence to the new regimen should be considered
• Numerous clinical trials have studied the efficacy, safety, and tolerability of a switch in patients with stable virologic suppression
1. DHHS Guidelines, October 2011. 2. GeSIDA Guidelines, January 2012. 3. EACS Guidelines, 2011.
4. Thompson MA, et al. JAMA. 2010;304;321-333.
Summary and Additional
Considerations

Within-Class Simplifications
• Preserves unused drug classes for potential future use
• Types of simplifications
– PI substitutions
• Simplification from twice-daily PI to once-daily PI
• Simplification from boosted PI to unboosted PI
– NNRTI substitutions
• Simplification to agents with reduced dosing frequency or
coformulated agents
– NRTI substitutions
• Simplification to agents with reduced dosing frequency or
coformulated agents

Rubio R, et al. HIV Med. 2010;11:545-553.
SIMPATAZ: Simplification From PI-
Based Therapy to ATV/RTV
• 183 virologically suppressed patients enrolled in multicenter, prospective,
noninterventional study
– Physician recommended treatment simplification
• At Mo 12, 95% of patients on treatment maintained undetectable HIV-1 RNA
• Overall AE rate low
– 3.8% of patients experienced moderate to severe AEs, judged related to ATV/RTV
– Only 1 discontinuation judged related to ATV/RTV AE
• Total cholesterol, triglycerides, and LDL cholesterol all improved significantly
• Proportion of patients classifying themselves as highly satisfied with
their antiretroviral therapy regimen increased significantly from baseline
to Month 12 after switch (47% vs 91%; P < .001)

Squires K, et al. HIV Clin trials 2012;13:233-44
ARIES: Switch From a RTV-
Boosted PI to Unboosted ATV
P = .390
0
20
40
60
80
100
ATV
HIV
-1 R
NA
< 5
0 c
/mL
at
Wk
14
4 (
%)
77 73
ATV/RTV
515 virologically suppressed treatment-naive patients with no evidence of virologic failure during 36-wk induction phase of ATV/RTV + ABC/3TC randomized to switch to unboosted ATV or no change for 48 wks
Tx-Related Grade 2-4 AEs, %
ATV (n = 189)
ATV/RTV ( n = 180)
BL to Wk 36 26 30
Hyperbilirubinemia 13 13
Diarrhea 4 3
Nausea 3 2
Wk 36 to Wk 144 13 23
Hyperbilirubinemia* 6 14
*P = .0232
Changes in median lipid levels from randomization to Wk 144 more favorable with ATV vs ATV/RTV therapy


Out-of-Class Simplifications
• Can be useful option for patients with
tolerability issues
• Strategies
– Simplification from PI-based regimen to RAL
– Simplification from PI-based regimen to
NNRTI-based regimen
• NVP-based regimens
• EFV/FTC/TDF
• RPV/FTC/TDF

Lipoatrophie - lipodystrophie
Lipo-atrophie: NRTI (d4T > ddI > AZT, 3TC,
abacavir), pas d’anomalies métaboliques.
Toxicité mitochondriale
Lipodystrophie:
antiprotéases (IP) et
anomalies métaboliques
Courtesy Bernard Hirschel et Alexandra Calmy, HCUGE

AZT/3TC/NELFI AZT/DDI/NELFI AZT/DDI/EFZ AZT/DDI/LOPIr
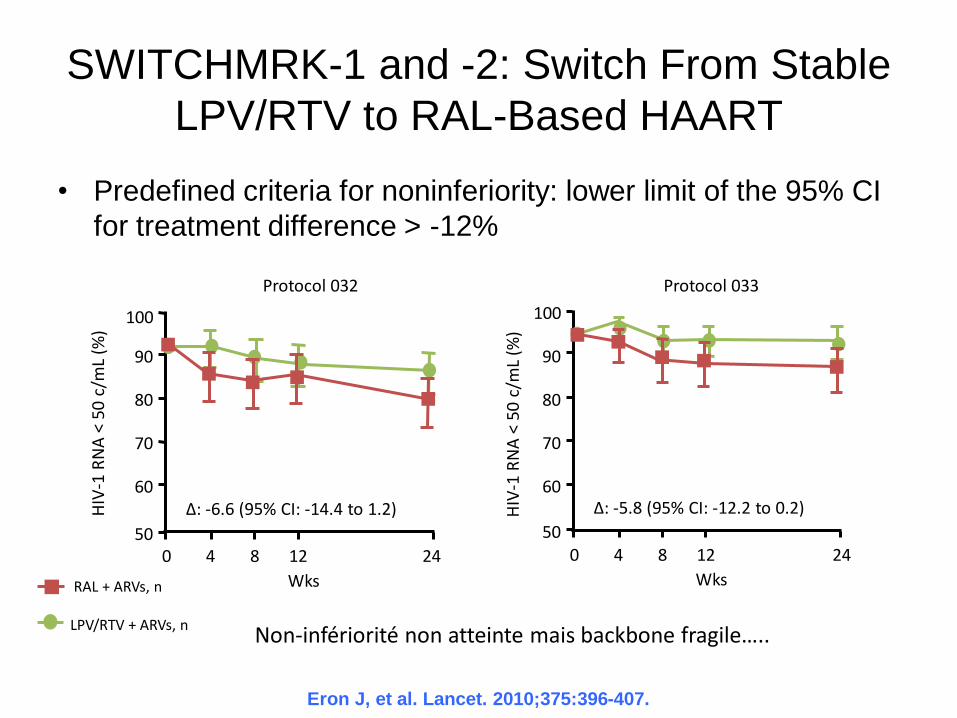
Eron J, et al. Lancet. 2010;375:396-407.
SWITCHMRK-1 and -2: Switch From Stable
LPV/RTV to RAL-Based HAART
• Predefined criteria for noninferiority: lower limit of the 95% CI
for treatment difference > -12%
RAL + ARVs, n LPV/RTV + ARVs, n
50
60
70
80
90
100
0 4
Wks
HIV
-1 R
NA
< 5
0 c
/mL
(%)
8 12 24
87%
81%
∆: -6.6 (95% CI: -14.4 to 1.2)
Protocol 032 Protocol 033
50
60
70
80
90
100
0 4
Wks
8 12 24
∆: -5.8 (95% CI: -12.2 to 0.2)
94%
88%
HIV
-1 R
NA
< 5
0 c/
mL
(%)
Non-infériorité non atteinte mais backbone fragile…..

Eron J, et al. Lancet. 2010;375:396-407.
SWITCHMRK -1 and -2: Significant
Decrease in Lipids With Switch to RAL
Mean
Ch
an
ge F
rom
Baselin
e
at
Wk 1
2 (
%)
-50
-40
-30
-20
-10
0
10
20 RAL + ARVs
LPV/RTV + ARVs Protocol 032 Protocol 033
*
NS nps -12.8
0.7
-15.2
2.3
-41.5
3.6
-2.4
2.1
-0.9
0.8
NS nps -12.4
1.3 2.9
8.2 4.0
0.6
-0.6 -2.5
-14.8
-42.8
Fasting
Cholesterol Fasting
Non-
HDL-C
Fasting
TG†
Fasting LDL-C
Fasting
HDL-C
Fasting
Cholesterol Fasting
Non-
HDL-C
Fasting
TG† Fasting
LDL-C
Fasting
HDL-C
*P < .0001; †median change from BL at Wk 12, %.
*
*
* *
*


Switches That Reduce the Number
of Active Drugs in a Regimen
• Reduces drug exposure and may improve tolerability of regimen
• Strategies – Boosted PI monotherapy
• Avoids NRTI toxicities; reduces costs
– Ongoing clinical trials of switches to boosted PI + 3TC only
• Simplification from 2 NRTIs plus a third agent to ATV/RTV + 3TC as maintenance therapy (SALT)[1]
• Simplification from LPV/RTV plus 2 NRTIs to LPV/RTV + 3TC[2]
1. ClinicalTrials.gov. NCT01307488. 2. ClinicalTrials.gov. NCT01471821.
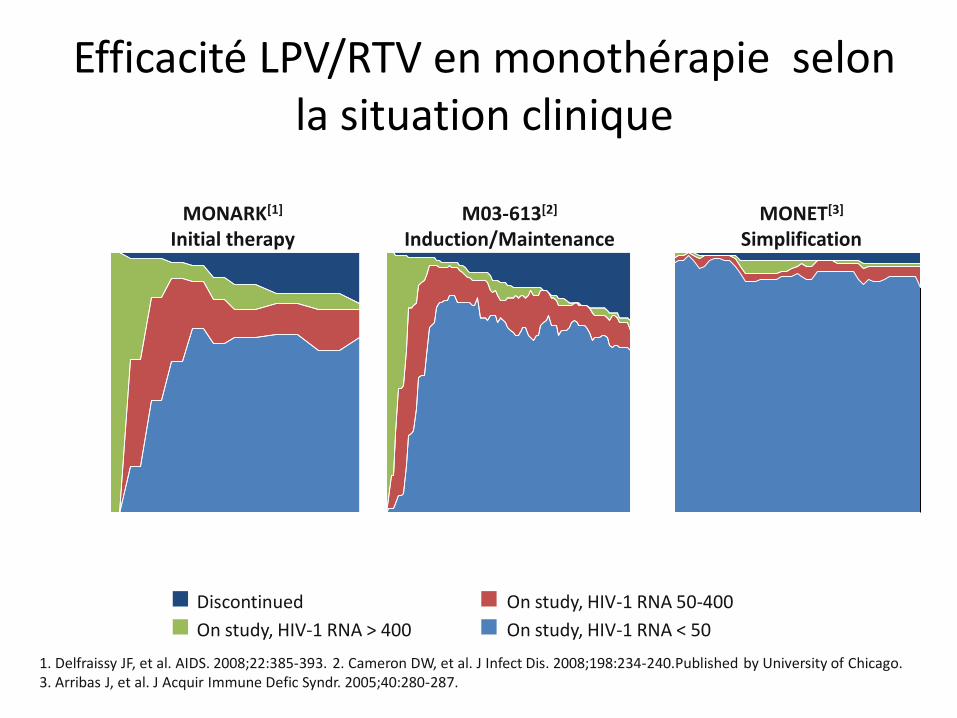
Efficacité LPV/RTV en monothérapie selon la situation clinique
MONARK[1]
Initial therapy M03-613[2]
Induction/Maintenance
0
20
40
60
80
100
0 16 32 Wk
48 0 16 32 48 64 80 96 Wk Wk
36 48 12
MONET[3]
Simplification
Discontinued
On study, HIV-1 RNA > 400
On study, HIV-1 RNA 50-400
On study, HIV-1 RNA < 50
1. Delfraissy JF, et al. AIDS. 2008;22:385-393. 2. Cameron DW, et al. J Infect Dis. 2008;198:234-240.Published by University of Chicago. 3. Arribas J, et al. J Acquir Immune Defic Syndr. 2005;40:280-287.
0 24
Pat
ien
ts (
%)


Studies of ATV/RTV Monotherapy
Study ATARITMO[1] ACTG 5201[2] Karlström[3] OREY[4]
Results 2 pts (7%) with VF at Wk 24 (1 d/c, 1 protocol violation)
5 pts with virologic “blips”
34 simplified to ATV/RTV monotherapy
88% (30) did not experience VF at Wk 48 after simplification
1 pt with VL = 508 at final visit
Stopped at 15 pts
5 VFs
No pts completing 72 wks on monotherapy without VF
9/14 (64%) with virologic success after median 36 wks
21% with tx failure
12% with virologic rebound
Resistance Not tested in plasma samples
5 pts genotyped
No major PI RAMs
No low frequency ATV resistance variants detected
3 pts genotyped
No PI resistance mutations
7 pts genotyped 1 pt with ATV
resistance mutation N88S at Wk 48
1 additional pt with N88S + M46L after Wk 48
1. Vernazza P, et al. AIDS. 2007;21:1309-1315. 2. Wilkin T, et al. J Infect Dis. 2009;199:866-871. 3. Karlström O, et al. J Acquir Immune Defic Syndr. 2007;44:417-422. 4. Pulido F, et al. EACS 2009. Abstract PS4/6.

EACS 2011[1] IAS-USA 2010[2] DHHS 2011[3]
PI/RTV monotherapy
with BID LPV/RTV or
QD DRV/RTV might
represent an option in
patients with intolerance
to NRTI or for treatment
simplification
Therefore, PI/RTV
monotherapy is not
recommended except in
exceptional
circumstances when
other drugs cannot be
considered for reasons of
toxicity/tolerability
In aggregate, boosted PI
monotherapy as initial or
as simplification treatment
has been somewhat less
effective in achieving
complete virologic
suppression and avoiding
resistance. Therefore, this
strategy cannot be
recommended outside of
a clinical trial
1. EACS Guidelines version 6, 2011. 2. Thompson MA, et al. JAMA. 2010;304;321-333.
3. DHHS Guidelines, 2011.
Guidelines Differ Regarding PI
Monotherapy

Reasons to Consider Treatment
Simplification • Improve adherence, convenience, and quality of life: active
simplification
– Reduce number of doses
– Reduce number of pills
– Reduce number of drugs
– Reduce costs
• In patients with controlled viremia and no tolerability issues,
simplifying treatment to improve quality of life should be considered
• Many physicians fear simplification out of perceived risk of
tolerability issues and loss of virologic suppression
• However, if simplification is not effective, reverting back to the
previous regimen is an option if carefully managed

Potential Benefits of Treatment
Simplification • Several highly convenient regimens available, including newer
agents and reformulations/coformulations of older drugs with
less frequent dosing and less toxicity
– Regimens with lower pill burdens and less frequent daily dosing
are associated with better adherence
• When switching treatment, for whatever reason, maintenance
of virologic suppression remains the main concern
– Studies have identified simplification strategies that usually
maintain virologic suppression and often reduce adverse events
• Previous use of suboptimal therapy may reduce likelihood of
effective treatment response

Thérapeutique aux différents stades
• Initiations de traitement « usuelles » – Stade SIDA
• Traitement de l’infection opportuniste
• Traitement antirétroviral
– Stade d’infection chronique
• Switch pour multirésistance
• Simplification thérapeutiques ou « allègement »
• Intensification thérapeutique pour espérer réduire le réservoir – Dès la primoinfection
– Au cours de l’infection chronique chez le patient indétectable
Sont exclus de la présentation :
- co-infection VIH/hépatites
- femmes enceintes



69 patients sous HAART
avec CV < 50 c/ml
depuis plus d’un an
HAART + RAL (intensification)
HAART poursuivi (témoin)
n = 45
n = 24
Randomisation 2 : 1 S24
- Augmentation transitoire
de l’ADN épisomale non
intégré après 2 et 4 chez
29% des patients
intensifiés
- Activation CD8 plus
importante

Le plus dur reste à faire…. Cibler le réservoir !

Conclusion
• Les acquis :
– Simplicité des traitement de première ligne
– Possibilité de simplification thérapeutiques
• A venir (espoir d’éradication) :
– Intensification lors de la primoinfection
– Intensification lors de l’infection chronique


J Acquir Immune Defic Syndr. 2012 Dec 15;61:557-564