cns stimulant by yogesh sangle
TRANSCRIPT
CNS STIMULANTS
1
PRESENTED BY- YOGESH PARMESHWAR SANGLEFINAL YEAR B.PHARM
GUIDED BY-MR.B.A.BAVISKARGOVT. COLLEGE OF PHARMACY, AMRAVATI
CNS consist of Brain and Spinal cord, and serves to coordinate and direct all body functions.
Homeostasis is control by CNS. Compounds that increase an initial low level of
physiological activity are generally classified as CNS stimulant.
Many drugs are used as CNS stimulant. Some of the important drugs are classified here.
Introduction
Classification1. Psychomotor stimulantscause: Excitement, Euphoria, Decrease feeling offatigue and Increase motor activity
I. nicotine, II. cocaine, III. amphetamine,IV. methylphenidate.
2. Hallucinogens (psychotomimetic)Affect thought, perception, and mood
I. Lysergic acid diethylamide (LSD)II. Tetrahydrocannibinol (THC)
2
Therapeutic Indications andContraindications for CNS Stimulants
Obesity (anorectic agents).Attention Deficit Hyperactivity Disorder (ADHD); lackthe ability to be involved in any one activity for longerthan a few minutes.Narcolepsy: It is a relatively rare sleep disorder, that ischaracterized by uncontrollable bouts of sleepinessduring the day. It is sometimes accompanied bycatalepsy, a loss in muscle control, or even paralysisbrought on by strong emotion, such as laughter.Contraindications:patients with anorexia, insomnia, asthenia, psychopathic
3
A. Nicotine:
� Nicotine is the active ingredient in tobacco.� Used in smoking cessation therapy,� Nicotine remains important, because:
it is 2nd only to caffeine as the most widely used CNSstimulant
and 2nd only to alcohol as the most abused drug.Actions of Nicotine:Low dose: ganglionic depolarizationHigh dose: ganglionic blockade
8
Actions of NicotineI. CNS:1.
2.
Low dose: euphoria, arousal, relaxation, improvesattention, learning, problem solving and reaction time.High dose: CNS paralysis, severe hypotension(medullary paralysis)
II. Peripheral effects:� Stimulation of sympathetic ganglia and adrenal
medulla→↑ BP and HR (harmful in HTN patients)� Stimulation of parasympathetic ganglia→↑ motor
activity of the bowel� At higher doses, BP falls & activating ceases in both
GIT and bladder
9
Adverse effects:� CNS; irritability and tremors� Intestinal cramps, diarrhea� ↑HR & BP
Withdrawal syndrome:nicotine is addictive substance� physical dependence on nicotindevelops rapidly and can be
severe.� Bupropion: can reduce thecraving for cigarettes� Transdermal patch and chewinggum containing nicotine
11
B. Cocaine (highly addictive drug)Mechanism of action:blockade of reuptake of themonoamines (NE, serotoninand dopamine).Thus, potentiates andprolongs the CNS andperipheral actions of thesemonoamines.Only clinical use as localanesthetics.
13
Action:� Initially produces the intenseeuphoria by prolongation of
dopaminergic effects in thebrain’s pleasure system (limbicsystem) producing the “Rush”.
� This follows by dysphoria in fewminutes as it is degraded byplasma estrases
Chronic intake of cocaine depletes dopamine.This depletion triggers the vicious cycle of craving forcocaine.
14
Pharmacological effects:a. CNS-behavioral effects result from powerful
stimulation of cortex and brain stem.� Cocaine acutely increases mental awareness and
produces a feeling of wellbeing and euphoria similar tothat produced by amphetamine.
� Like amphetamine, cocaine can produce hallucinationsand delusions of paranoia or grandiosity.
� Cocaine increases motor activity, and at high doses, itcauses tremors and convulsions, followed by
respiratory and vasomotor depression.15

Pharmacological effects :b. Sympathetic NS: peripherally potentiate the actionof NE→ fight or flightc. Hyperthermia:� impair sweating & cutaneous vasodilation� ↓Perception of thermal discomfortd. local anesthetic action: blockade of voltage-activated Na+ channel.� Cocaine is the only LA that causes vasoconstriction,chronic inhalation of cocaine powder → necrosis and
perforation of the nasal septum� Cocaine is often self-administered by chewing,
intranasal snorting, smoking, or intravenous (IV)16injection.
Adverse effects:� Anxiety reaction that includes: hypertension,tachycardia, sweating, and paranoia.Because of the irritability, many users take cocaine with alcohol.A product of cocaine metabolites and ethanol is cocaethylene,which is also psychoactive and cause cardiotoxicity.� Depression: Like all stimulant drugs, cocaine stimulation of the
CNS is followed by a period of mental depression.� Addicts withdrawing from cocaine exhibit physical and
emotional depression as well as agitation.The latter symptom can be treated with benzodiazepines or
phenothiazines.� Toxic effects:� Seizures treated by I.V diazepam� Fatal cardiac arrhythmias treated by propranolol 17
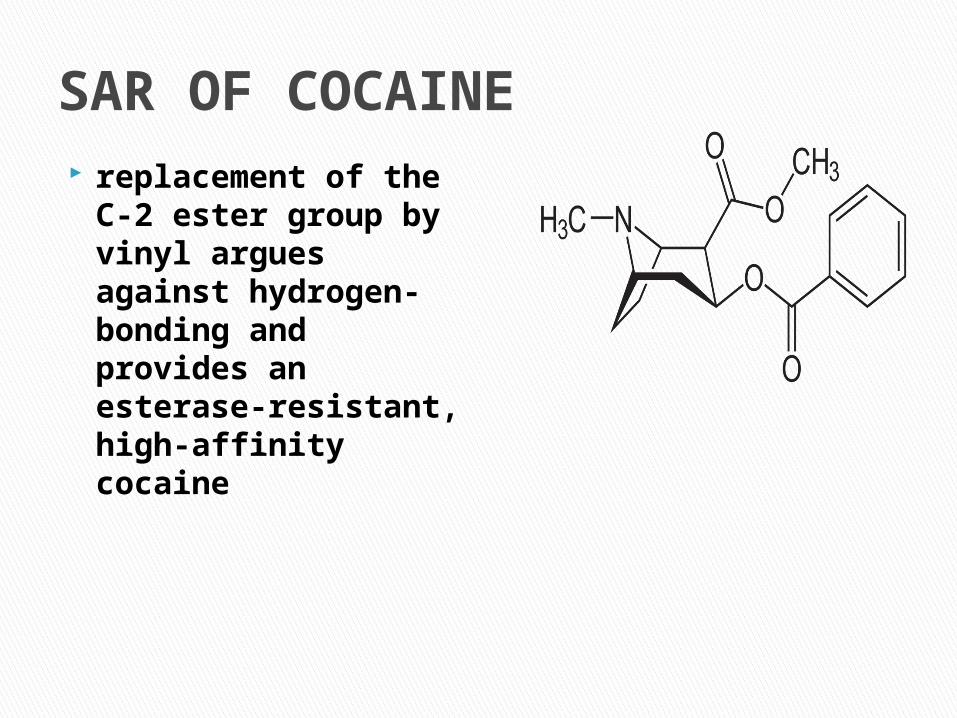
SAR OF COCAINE replacement of the
C-2 ester group by vinyl argues against hydrogen-bonding and provides an esterase-resistant, high-affinity cocaine
C. Amphetamine� Is a non catecholamine, (shows neurologic and clinicaleffects quite similar to those of cocaine).
�Dextroamphetamine is the majormember of this class compoundsmethamphetamine (speed) is a derivative of amphetamine that can be smoked and it is preferred by many abusers.
�
�
18
Mechanism of action:Amphetamine, act by
releasing intracellularstores of catecholamines.
also inhibits MAO, highlevel catecholamines arereadily released into
synaptic spaces.
19
Actions:a. CNS: the major behavioral effects of amphetamineresult from a combination of its dopamine and NE
release enhancing properties.� Amphetamine stimulates the entire cerebrospinalaxis, brainstem, and medulla.� This leads to increase alertness, decrease fatigue,depressed appetite, and insomnia.
b. Sympathetic Nervous System: indirectly stimulatingthe receptors through NE release.
20
Adverse effects:The anorectic effect of amphetamine is due to its actionin the lateral hypothalamic feeding center.CVS: palpitations, cardiac arrhythmia, HTN, anginalpain, and circulatory collapse. Headache, chills, and
excess sweating may also occur. GIT: anorexia, nausea, vomiting, abdominal cramps,and diarrhea.Overdoses are treated with chlorpromazine or
haloperidol, with urine acidification to enhanceexcretion.
22
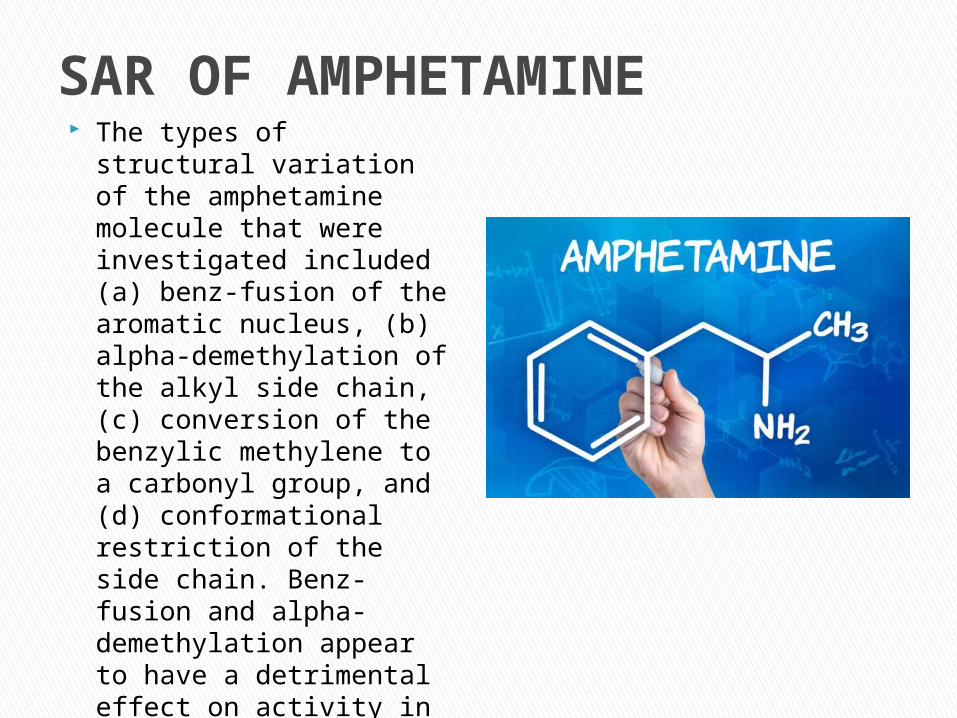
SAR OF AMPHETAMINE The types of structural
variation of the amphetamine molecule that were investigated included (a) benz-fusion of the aromatic nucleus, (b) alpha-demethylation of the alkyl side chain, (c) conversion of the benzylic methylene to a carbonyl group, and (d) conformational restriction of the side chain. Benz-fusion and alpha-demethylation appear to have a detrimental effect on activity in that none of these analogs produced amphetamine-appropriate responding.
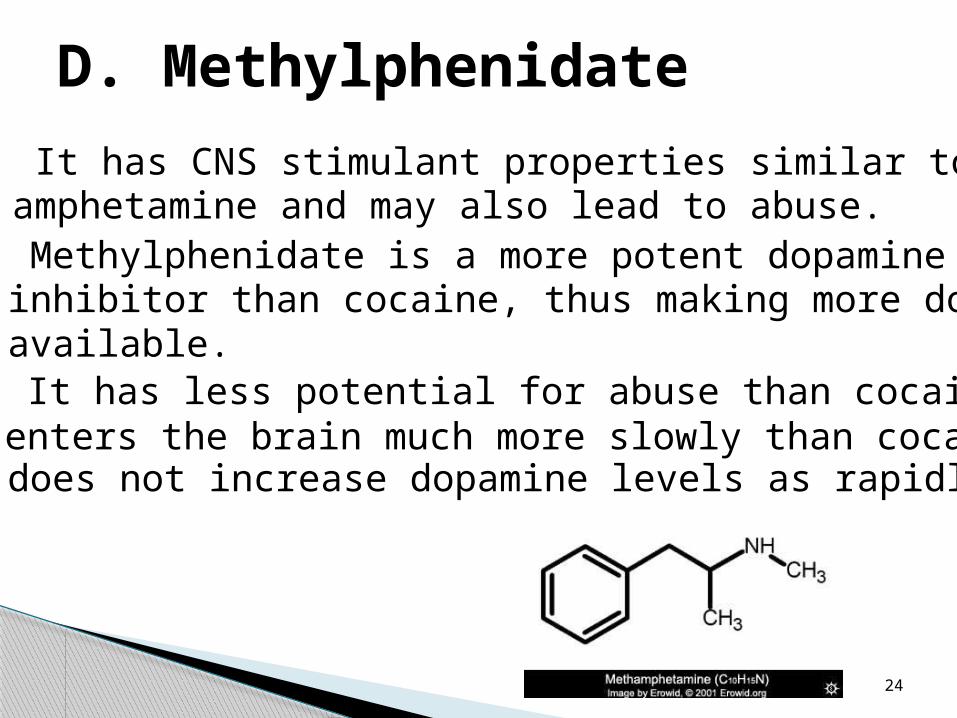
D. Methylphenidate� It has CNS stimulant properties similar to those ofamphetamine and may also lead to abuse.� Methylphenidate is a more potent dopamine transportinhibitor than cocaine, thus making more dopamineavailable.� It has less potential for abuse than cocaine, because itenters the brain much more slowly than cocaine and,does not increase dopamine levels as rapidly.
24
Therapeutic uses:� Methylphenidate and its active isomer,
(Dexmethylphenidate), have been used for severaldecades in the treatment of ADHD in children aged 6to 16.
� It is also effective in the treatment of narcolepsy.
25
Adverse reactions:� GIT effects are the most common; abdominal painand nausea.
� Other reactions include anorexia, insomnia,nervousness, and fever.
� In seizure patients, methylphenidate seems toincrease the seizure frequency, especially if the
patient is taking antidepressants.
� Methylphenidate is contraindicated in patients withglaucoma.
26
Threo methylphenidate derivatives with halo- substituents on the aromatic ring had the increased binding potency, while electron donating substituents caused little change, or a small loss of binding potency. N-substituents generally caused a marked loss of potency, except for benzyl which slightly increased potency. For the unsubstitued amine, reduction of the methyl ester to hydroxyl sharply reduced potency; conversion of the hydroxyl to methyl ether restored affinity. For N-benzyl (tertiary amine) derivatives, these same transformations both increased affinity.
SAR OF METHYLPHENIDATE
Narcolepsy: (day time sleepiness)� Amphetamine, methylphenidate.
� Recently, a new drug, modafinil (wakefulness-promoting agent) and its R-enantiomer derivative,armodafinil, have become available to treatnarcolepsy.
� Modafinil produces fewer psychoactive andeuphoric effects as well as, alterations in mood,perception, thinking, and feelings typical of otherCNS stimulants.
27
II. Hallucinogens (psychotomimetic)
� A few drugs have the ability to induce alteredperceptual states reminiscent of dreams, are
accompanied by bright, colourful changes in theenvironment and by a plasticity of constantlychanging shapes and colour.
� The individual under the influence of these drugs isincapable of normal decision making, because the
drug interferes with rational thought.
29
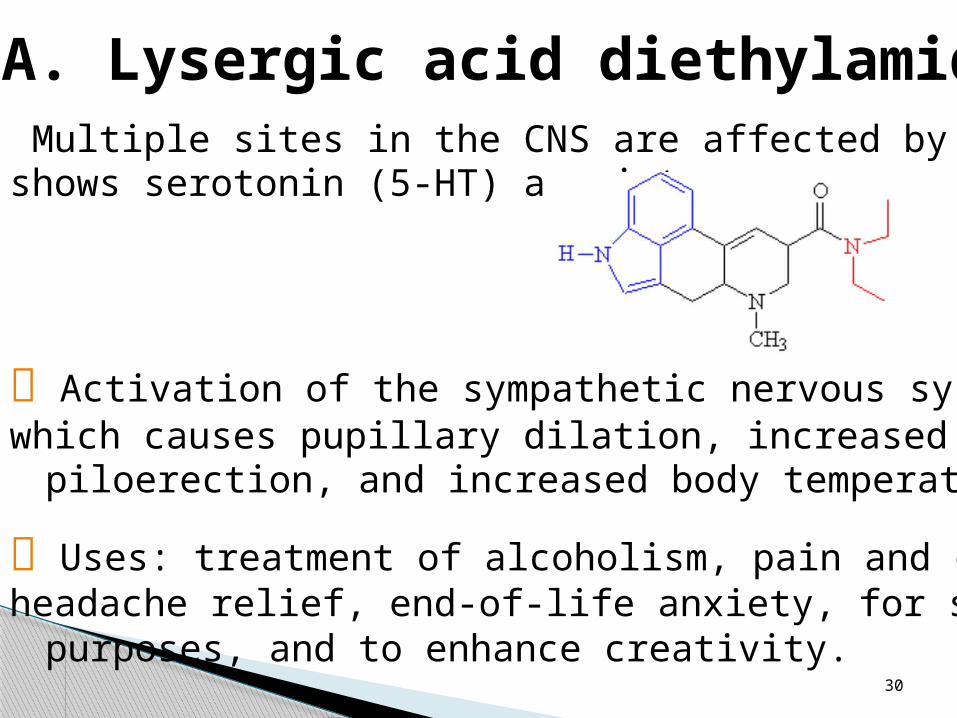
A. Lysergic acid diethylamide (LSD)� Multiple sites in the CNS are affected by (LSD) andshows serotonin (5-HT) agonist.
Activation of the sympathetic nervous system occurs,which causes pupillary dilation, increased BP,
piloerection, and increased body temperature.
Uses: treatment of alcoholism, pain and clusterheadache relief, end-of-life anxiety, for spiritual
purposes, and to enhance creativity.30
Adverse effects:� Include hyperreflexia, nausea, and muscular weakness.
� High doses may produce long-lasting psychoticchanges in susceptible individuals.
� Temporarily impair the ability to make sensiblejudgments and understand common dangers,
temporary confusion, difficulty with abstract thinking, orsigns of impaired memory and attention span, thusmaking the user more susceptible to accidents andpersonal injury.
31
B. Tetrahydrocannabinol (THC)� The main psychoactive alkaloid contained in marijuana is
tetrahydrocannabinol (THC), which is available asdronabinol.
� THC can produce euphoria, followed by drowsiness andrelaxation.
� SE: appetite stimulation, xerostomia, visual hallucinations,delusions, and enhancement of sensory activity. 32
Mechanism of action:� THC receptors, designated CB1 receptors, have been
found on inhibitory presynaptic nerve terminals.CB1 is coupled to a G protein.
� Interestingly, endocannabinoids have been identified inthe CNS.
� These compounds, which bind to the CB1 receptors, aremembrane-derived and are synthesized on demand, and
they may act as local neuromodulators.
� The action of THC is believed to be mediated through theCB1 receptors but is still under investigation.
33
ADHD drugs. Ampakines. Eugeroics. Amphetamines (class) Dopamine precursors. Amphetamine. Caffeine. Ephedrine
RECENT DRUG USE:-
a)Medicinal Chemistry by Dr S.S Kadam Dr K.R. Mahadik, Dr K.G. Bhotra By Nirali Prakashan Revised edition Page NO 8.1
b)Essential of Medical Pharmacology by K.D Tripathi 7th edition Page No 374-486
Reference

THANK YOU !!