cll treatment algorithm and state of the art - sgh-ssh · cll treatment algorithm and state of the...
TRANSCRIPT

CLL treatment algorithm
and state of the art
Hematology
IOSI - Oncology Institute of Southern Switzerland
IOR - Institute of Oncology Research
Bellinzona - Switzerland
Davide Rossi, M.D., Ph.D.

• Newly presented pts
• First line pts
• Relapsed pts
CLL subgroups

• Newly presented pts
• First line pts
• Relapsed pts
CLL subgroups

Clinical applications of biomarkers in CLL
W&W
Asymptomatic Symptomatic
Clinical stage iwCLL criteria
Treatment
Hallek iwCLL 2017

Host Factors: Age, sex, etc
Disease Markers: Stage, lymphocyte count, LDT, etc
Ag expression: CD38, Zap70, CD49d, etc
Serology: 2M, TK, LDH, sCD23, etc
Genetics: del17p, TP53 mutation, del11q22, del13q14, trisomy 12, NOTCH1 mutation, SFRB1 mutation, etc
Biology Markers: IGVH-sequence, BCR-structure
Biomarker: variable that associates with disease outcome

CLL-IPI
Variable Adverse factor Coeff. HR
TP53 (17p) deleted and/or mutated 1.442 4.2
Grading
4
Prognostic Score 0 – 10
IGHV status Unmutated 0.941 2.6
B2M, mg/L > 3.5 0.665 2.0
Clinical stage Binet B/C or Rai I-IV 0.499 1.6
Age > 65 years 0.555 1.7
2
1
2
1
Risk group Score PatientsN (%)
5-year OS, %
HR (95% CI) p value
Very High 7 – 10 62 (5) 23.3 3.6 (2.6 - 4.8) < 0.001
High 4 – 6 326 (27) 63.6 1.9 (1.5 - 2.3) < 0.001
Intermediate 2 – 3 464 (39) 79.4 3.5 (2.5 - 4.8) < 0.001
Low 0 – 1 340 (29) 93.2
International CLL-IPI working group. Lancet Oncol 2016
Time (months)
Overa
ll surv
ival
Low
Intermediate
High
Very high
Overall survival (all patients)

• Newly presented pts
• First line pts
• Relapsed pts
CLL subgroups
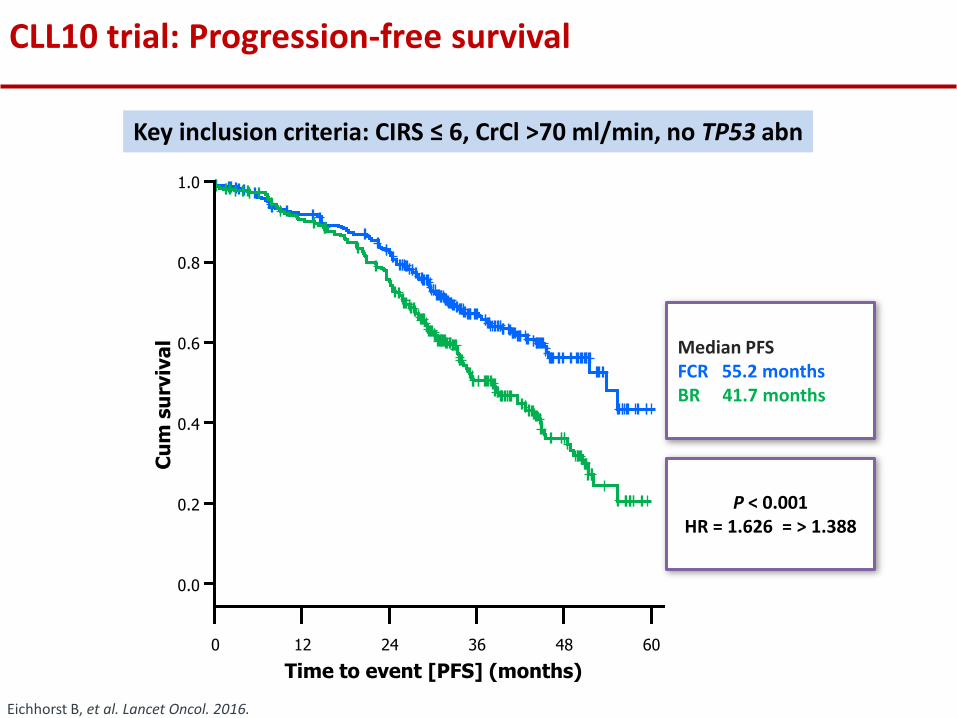
CLL10 trial: Progression-free survival
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 48 60
Cu
m s
urv
iva
l
P < 0.001 HR = 1.626 = > 1.388
Median PFS FCR 55.2 months BR 41.7 months
Time to event [PFS] (months)
Eichhorst B, et al. Lancet Oncol. 2016.
Key inclusion criteria: CIRS ≤ 6, CrCl >70 ml/min, no TP53 abn

Adverse event FCR (% of pt)
BR (% of pt)
p value
All 90.8 78.5 <0.001
Hematological AEs 90.0 66.9 <0.001
Neutropenia 81.7 56.8 <0.001
Anemia 12.9 9.7 0.28
Thrombocytopenia 21.5 14.4 0.036
Infection 39.0 25.4 0.001
TRM 3.9 2.1 0.23
FCR is more toxic than BR

Patients ≤65 years: p<0.001 Patients >65 years: p<0.170
FCR=53.6 months
BR=38.5 months
FCR=not reached
BR=48.5 months
FCR > BR in fit and untreated CLL patients (CLL10)
Eichhorst B, et al. Lancet Oncol. 2016

Goede V, et al. NEJM 2014/ Hillmen P. et al, Lancet 2015
CLL11 COMPLEMENT
G-Clb (n=336) R-Clb (n=321) O-Clb(n=217)
Age 74 (39 - 88) 73 (40 – 90) 69 (35 – 92)
ORR 78% 65% 82%
CR 21% 7% 14%
MRD neg. 20% 3% 8%
PFS med.
(mo) 29.2 15.4 22.4
Anti CD20-CLB > CLB in less fit and untreated CLL patients
CIRS score >6 and/or Cr Cl <70 mL/min

Adverse events in Clb-based chemoimmunotherapy
G-Clb (n=336) R-Clb (n=321) O-Clb(n=217)
Any AE grade ≥3 % 70 55 50
Infusion-related
reaction 20 4 10
Neutropenia 33 28 26
Anemia 4 4 5
Thrombocytopenia 10 3 5
Leukopenia 4 <1 -
Infection 12 14 9
Pneumonia 4 5 -
Goede V, et al. NEJM 2014/ Hillmen P. et al, Lancet 2015

Burger J, et al. New Engl J Med 2015
Outcome Ibrutinib (n = 136)
Chlorambucil (n = 133)
P Value
Median PFS, mos NE 18.9 < .0001
18-mo PFS rate, % 90 52
Ibrutinib is superior to chlorambucil as first line treatment in unfit CLL (RESONATE 2)
Key inclusion criteria treatment-naive CLL pts 65 yrs of age or older for pts 65-69 yrs, comorbidity that
precludes FCR no warfarin use no del(17p)

90% PFS at 5 years in TN CLL treated with ibrutinib
Median PFS 5-year PFS
TN (n=31) NR 92% R/R (n=101) 52 mo 43%
Progression-Free Survival Overall Survival
Median OS 5-year OS
TN (n=31) NR 92% R/R (n=101) NR 57%

RESONATE-2: Adverse Events
Tedeschi A, et al. ASH 2015. Abstract 495.
Parameter Ibrutinib (n = 136)
Chlorambucil (n = 133)
Selected AEs, %
Hypertension 14 0
Atrial fibrillation 6 1
Major hemorrhage 4 2
Infection 10 6

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

MDACC myelosuppression/dose reductions in patients >60 yrs1
early treatment discontinuations in patients 70 yrs2
CLL8 hematological toxicity in patients 65 yrs3
adverse events in pts with increased CIRS4
CLL10 infections in patients >65 yrs5
REACH adverse events in patients with decreased CrCl6 1Keating et al. J Clin Oncol. 2005; 2T Ferrajoli A, et al. Leuk Lymphoma. 2005: S86; 3Hallek et al. Lancet. 2010 ; 4Goede et al. Haematologica (EHA meeting abstracts). 2012; 5Eichhorst et al. Blood. 2014 (ASH meeting abstracts) ; 6Robak et al. J Clin Oncol. 2010
Biomarkers that identify unfit patients
SIOG recommendation for the identification of pts less fit for FCR:
– Older age (e.g. 65 years)
– Higher comorbidity burden (e.g. CIRS >6)
– Impaired renal function (e.g. CrCl <70 mL/min)
CrCl, creatinine clearance
CIRS, cumulative illness rating scale Stauder R et al. Ann Oncol 2017 28: 218-227

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

TP53 abnormalities in CLL
5’ 3’
1 DNA BINDING
EX4 EX9
393
Missense Nonsense Frameshift
TP53
Freq
uen
cy
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MBL Early stage CLL
CLL requiring treatment
F-refactory CLL
Richter syndrome
TP53 M
del17p13
TP53 M/del17p13
N=1/63 (1.5%)
N=30/318 (9.4%)
N=44/99 (44.4%)
N=25/38 (65.7%)
N=13/268 (4.8%)
Dohner et al, New Engl J Med 2000 ; Rasi et al, Haematologica 2012; Zainuddin et al, Leuk Res 2011; Zenz et al J Clin Oncol 2010;Rossi et al Blood 2011; Rossi et al Blood 2014
Chr17
DNA damage
P
p53P
p21
cyclin B
p53P
cyclin B
cdc2p21
BAXCaspase 9
Apoptosis
Cell cycle arrest
M P
del(17p)
p53wt
(rare)
M P
del(17p)p53mut
(>80%)
P P
LOH
p53mut
M P
p53wt/mut
(rare)
M P
normal
p arm
p53
q arm

Badoux Blood 2011; Fisher J Clin Oncol 2011; O’Brien, ASH 2014; Sharman ASH 2014; Byrd ASH 2015; Stilgenbauer, ASH 2015
Chemoimmunotherapy (CIT) vs novel agents in TP53 disrupted CLL
0%
20%
40%
60%
80%
100%
Re
spo
nse
rat
e
0%
20%
40%
60%
80%
100%
CR PR PR-L
35%
7%
83% 78% 79%
12
-mo
nth
s P
FS
18% 22%
80% 79% 72%
Response rate PFS
CIT Novel agents CIT Novel agents
Relapsed/Refractory CLL
‡

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

IGHV mutated patients gain the greatest benefit from FCR
1. Thompson PA, et al. Blood 2016; 127:303–309. 2. Fischer K, et al. Blood 2016; 127:208–215. 3. Rossi D et al. Blood 2015; 126 1921–1924, 4. Kipps T et al. ICML14 . .
2 4 6 8 10 12 14 0 16
p<0.0001 0
25
50
75
100
PFS
(%
)
Time (years)
PFS
(%
)
Time (years)
PFS
(%
)
Time (years)
0
25
50
75
100
0 10 2 4 6 8
IGHV mutated
IGHV unmutated
IGHV mutated, FCR
IGHV mutated, FC
p<0.001
MDACC Phase II study (N=300)1 CLL8 study vs. FC (N=817)2
Italian retrospective analysis (N=404)3
100
0
25
50
75
0 2 4 6 8
IGHV unmutated, FC
IGHV unmutated, FCR
IGHV mutated, Ibrutinib
IGHV unmutated, Ibrutinib
IGHV mutated, comparator
IGHV unmutated, comparator
ibrutinib vs ofatumomab
ibrutinib vs chrlorambucil
Ibrutinib-BR vs placebo-BR4

a In patients who are not eligible for any other therapies
Chl: chlorambucil; CIRS: Cumulative Illness Rating Scale; Cr: creatinine Personal communication.
FCR
Chl + anti-CD20
TP53
Chemo + anti-CD20
Age; CIRS;
Cr clearance
BR
Ibrutinib Idelalisib + Ra
IGHV Ibrutinib
Mutated and/or deleted
Wild type
Unmutated
Mutated
Can first line treatment be informed by biomarkers?

• Newly presented pts
• First line pts
• Relapsed pts
CLL subgroups

BR in relapsed CLL lacking del(17p) (HELIOS)
• Chanan-Khan A, et al. Lancet Oncol 2016;17:200–211.
Key inclusion criteria: Relapsed CLL No del(17p)
Key exclusion criteria: Resistance to bendamustine
N=289 (placebo + BR arm)
Placebo + BR
Age, years 63 (median)
del(17p) 0%
Previous lines 2 (mean)
F-refractory 26%
Placebo + BR arm: ORR: 68% Median PFS: 13.3 months
Time (months)
80
60
40
20
0
100
PFS
(%
)
0 16 24 32 8 4 12 20 28
Placebo + BR (mPFS: 13.3 mos)
Ibrutinib + BR (mPFS: NR)

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

FC, fludarabine + cyclophosphamide; FCR, FC + rituximab; MDACC, MD Anderson Cancer Center.
1. Tam CS, et al. Blood 2014; 124:3059–3064; 2. Stilgenbauer S and Zenz T. Hematology Am Soc Hematol Educ Program 2010;2010:481–488
Late relapse after first-line chemoimmunotherapy supports maintained sensitivity
Survival after first salvage after FC/FCR first-line failure: CLL8 data2
Survival after first salvage after FCR first-line failure: MDACC data1
36-month cutoff
0.0
0.2
0.4
0.6
1.0
0.8
Cu
mu
lati
ve s
urv
ival
≥6 years (n=46), 5-year OS: 71%
Time (months) 0 24 48 72 96 120 144
3–5.9 years (n=61), mOS: 54 months
1–2.9 (n=34), mOS: 27 months
<1 year (n=15), mOS: 13 months
24-month cutoff
PFS >24 months
PFS 12–24 months
PFS <12 months
Ove
rall
surv
ival
Time (months)
0.0
0.2
0.4
0.6
1.0
0.8
0 6 24 30 36 42 48 12 18

Byrd JC et al. New Engl J Med 2014 371:213-2
Salvage treatment in CLL not suitable for chemoimmunotherapy
R/R CLL Not suitable for F-based Tx • PFS <36 mo • del17p
Ofatumumab (n=195) Ibrutinib (n=196)
100
90
80
70
60
50
40
30
20
10
0 0 6 12 18
Months
Pro
gre
ssio
n-f
ree
su
rviv
al 75% PFS
ORR: 63%
R/R CLL Not suitable for cytotoxic Tx: • PFS <24 mo
Ibrutinib (RESONATE)
R/R CLL Not suitable for cytotoxic Tx: • del17p
Idelalisib-R (116)
ORR: 81%
0 2 4 6 8 1 0 1 2 1 4 1 6 1 8 2 0 2 2 2 4 2 6
0
2 0
4 0
6 0
8 0
1 0 0
T im e (m o n th s )
Pro
gre
ss
ion
-fr
ee
S
urv
iva
l (
%)
Idelalisib + R (n=110)
Placebo + R (n=110)
60% PFS
ORR: 79%
51% PFS
Venetoclax M13-982
Furman R et al. New Engl J Med 2014 370:997-1007 Stilgenbauer S et al. Lancet Oncol 2016;17:768-78

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

Ibrutinib Venetoclax
Eve
nt-
free
su
rviv
al
(pro
po
rtio
nal
)
0.0
0.2
0.4
0.6
0.8
1.0
PFS: 6.8 months2
Time (months)
del(17p) median
0 6 12 18 24 30 36 42
del(11q) del(17p)
Trisomy 12q del(13q) single Other*
Bendamustine -R
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20 22 24 26
Pro
gre
ssio
n-f
ree
surv
ival
(%
)
Time (months)
Del(17p)/TP53mut
No del(17p)/TP53mut
Idelalisib-R
P=0.94
Event-free survival in relapsed TP53 disrupted patients

1. Imbruvica® SmPC. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003791/WC500177775.pdf (accessed June 2017); 2. Zydelig® SmPC. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003843/WC500175377.pdf (accessed June 2017); 3. Venclyxto® SmPC. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/004106/WC500218800.pdf (accessed June 2017).
Idelalisib2 Ibrutinib1 Venetoclax3
Gastrointestinal disorders (consider diarrhoea/colitis risk)
Respiratory insufficiency (consider pneumonitis risk)
Mild/moderate liver impairment
Risk of bleeding-related events (incl. anticoagulant therapy)
History of atrial fibrillation/flutter, cardiac risk
factors, hypertension
Tumour lysis syndrome
Infections
• Cytopenias • Interstitial lung disease • Tumour lysis syndrome • Non-melanoma skin cancer • Drug–drug interactions • Women of childbearing
potential
• Neutropenia • Transaminase elevations • Stevens-Johnson syndrome and
toxic epidermal necrolysis • CYP3A inducers • CYP3A substrates • Hepatic impairment • Chronic hepatitis • Women of childbearing
potential
• CYP3A inducers • Women of childbearing
potential
Neutropenia
Toxicities and management for novel therapies

Lymph node
BCR
CLL CLL
Blood
chemokines
Kinase
Kinase
integrins
Kinase
Inhibitor
De Rooij, Blood 2012; Ponader, Blood 2012; Herman, abstract #185
CLL
CLL
CLL
CLL
Redistribution lymphocytosis

Lymphocytosis + Nodal Reduction with BCR Antagonists
New response criteria are required

Restoration of apoptosis through BCL2 inhibition

Response Classification MRD-negative MRD-positive Not Evaluable
CR/CRi (n=25) 20 5 0
nPR/PR (n=17) 8 8 1a
Other (n=7) 0 1b 6c
Total, n/N (%) 28/49 (57) 14/49 (29) 7/49 (16)
Venetoclax induces deep remissions
Seymour JF, et al. Lancet Oncol. 2017 Feb; 18(2): 230–240.

TLS risk assessment and prevention
Tumor burden (blood count and CT scan)
Renal function
Other co-morbidities
Assess risk factors for TLS
All LN <5 cm and ALC <25 G/L
Any LN 5 to 10 cm or ALC >25 G/L
Any LN >10 cm or ALC >25 G/L and LN >5 cm
Creatinine clearance <80 ml/min increases risk
Risk might increase with co-morbidities, splenomegaly, abnormal baseline chemistry labs, dehydratation
Establish TLS risk Low Medium High

TLS prophylaxis
Low Medium High TLS risk
HYDRATATION
Ensure adequate hydratation throughout dose-titration, particularly 2 days prior to and the days of dosing at initiation and each subsequent dose increase; IV fluids based on TLS risk who cannot mantain adequate oral hydratation
Oral (1.5-2 L) Oral (1.5-2 L) and consider additional IV if tolerated
Oral (1.5-2 L) and IV (150-200 ml/h as tolerated)
ANTI-HYPERURICEMIC AGENTS
Start anti-hyperuricemic agents 2 to 3 days prior to first dose, which may be continued through the titration phase based on the ongoing risk of TLS. Subjects allergic to allopurinol must use another uric acid reducer
Anti-hyperuricemic agents (e.g., allopurinol)
Anti-hyperuricemic agents (e.g., allopurinol)
Anti-hyperuricemic agents (consider rasburicase if
baseline uric acid is high)
BLOOD CHEMISTRY MONITORING
Correct pre-existing blood chemistry abnormalities prior to initiation of treatment. Monitor blood chemistry in real time (turn around <2h): potassium, uric acid, phosphorus, calcium, creatinine
Outpatient monitoring
• Pre-dose, 6-8, 24 h* (at 1° dose of 20 and 50 mg)
• Pre-dose at subsequent ramp-up dosease
Outpatient monitoring
• Pre-dose, 6-8, 24 h* (at 1° dose of 20 and 50 mg)
• Pre-dose at subsequent ramp-up dosease
Consider hospitalization if CrCl <80 ml/min at 1° dose of 20 and 50 mg
In hospital monitoring (1° dose of 20 and 50 mg)
• Pre-dose, 4, 8, 12, 24 h*
Outpatient monitoring (subsequent ramp-up doses)
• Pre-dose, 6-8, 24 h*
*24 h labs: do not administer the next dose until 24 h chemistry results have been evaluated.

Venetoclax in CLL After Failure of Ibrutinib or Idelalisib
100
75
50
25
0
2 4 6 8
PF
S (
%)
10 12 14
PFS
Mos Since First Dose
R/R ibrutinib
R/R idelalisib
All pts
Pts at
Risk, n
43
21
64
0
37
17
54
36
15
51
28
6
34
27
5
32
15
2
17
3
3
0%
20%
40%
60%
80%
100%
Ibrutinib Idelalisib
PR CR
Jones J, et al. ASH 2016. Abstract 637.

• 1. Schetelig J, et al. J Clin Oncol 2008; 26:5094–5100;
2. Dreger P, et al., Blood 2010; 116: 2438–2447; 3. Dreger P, et al. Blood 2013; 121:3284–3288.
Allo-SCT in high-risk CLL (CLL3X)
Eve
nt-
fre
e s
urv
ival
2
Time from SCT (months)
80
60
40
20
0
100
0 96 48 72 24
Eve
nt-
fre
e s
urv
ival
3
Time from SCT (months)
80
60
40
20
0
100
0 120 96 72 48 24
Pro
bab
ility
of
surv
ival
1
Time after HCT (years)
0.8
0.6
4.0
2.0
0.0
1.0
0 7 9 4 3 6 2 1 5 8
OS
PFS
Cu
mu
lati
ve in
cid
en
ce1
Time after HCT (years)
0.8
6.0
4.0
2.0
0.0
1.0
0 7 4 3 6 2 1 5
Relapse incidence
Non-relapse mortality
unknown (18) del(17p) (13) del(11q) (26) Other (21) del(13q) (12)
TP53 mutations (18) TP53 wt (54)
TP53 mutations vs wt: HR=0.82 (95% CI: 0.43–1.58); p=0.56
Retrospective analysis CLL3X trial
CLL3X trial: TP53 mutations

Baseline characteristics that predict outcome after alloSCT: • Remission at the time of alloSCT • Donor–patient HLA match • Donor–patient sex match
• CIR, cumulative incidence of relapse; EBMT, European Group for Blood and Marrow Transplantation; NRM, non-relapse mortality. • Van Gelder M, et al. Blood 2016; 128: Abstract 522 (oral presentation).
Outcome stratification after alloSCT in CLL (EBMT)
1.0
0.8
0.6
0.4
0.2
0.0 0 1 2
Pro
ba
bil
ity
Pro
ba
bil
ity
1.0
0.8
0.6
0.4
0.2
0.0 0 4 8 6 2
Two-year NRM, CIR, and PFS
Time since alloSCT (years)
PFS
PFS
CIR
NRM
Eight-year PFS
‘Good transplant risk’ 46-year-old reference patient with high-risk cytogenetics
Time since alloSCT (years)

• Predictive biomarkes in the 1st line setting
Pts fitness
TP53
IGHV
• Predictive biomarkes in the relapsed setting
Remission duration
TP53
Histology
Outline

Histology of progressed CLL
Ginè E, et al. Haematologica 2010; 95:1526–1533.
DLBCL-t
‘Accelerated’ CLL
‘Non-accelerated’ CLL
Survival from biopsy (months)
Pro
bab
ility
0.0
0.2
0.4
0.6
0.8
1.0
0 24 48 72 96 120 144 168
DLBCL-t, diffuse large B-cell lymphoma transformation.
Prolymphocytoid
evolution
Richter’s
syndrome
DLBCL variant

WHO 2016 Classification Richter syndrome
Clinical suspicion of transformation1,2
• Asymmetric growth of localised lymph
nodes
• Bulky disease
• B symptoms
• Sudden excessive rise in LDH level
RT
Sensitivity 91%
Specificity 80%
Positive predictive value 53%
Negative predictive value 97%
Max SUV cut-off = 5
PET/CT in RT diagnosis3
CT: computed tomography; LDH: lactate dehydrogenase; PET: positron emission tomography; SUV: standardised uptake values
1. Giné E, et al. Haematologica 2010; 95:1526–1533. 2. Rossi D, et al. Semin Oncol 2016; 43:311–319.
3. Bruzzi JF, et al. J Nucl Med 2006; 47:1267–1273.
DLBCL
Prolymphocytoid
CLL
Second cancer
Histological patterns observed in
biopsies from patients with CLL1,3

Cwynarski K, et al. J Clin Oncol 2012; 30: 2211–2217.
Ove
rall
surv
ival
(p
rop
ort
ion
)
0.8
0.6
0.4
0.2
0.0
1.0
Time (months)
0 60 48 36 24 12
0.8
0.6
0.4
0.2
0.0
1.0
Time (months)
0 60 48 36 24 12 O
vera
ll su
rviv
al
(pro
po
rtio
n)
Allo-SCT (n=25) Auto-SCT (n=34)
Prognostic Factors Chemosensitive disease; RIC
No prognostic factors identified
Post remission SCT is a potentially curative approach for Richter syndrome (EBMT)

Can treatment of R/R CLL be informed by
biomarkers?
BCR: B-cell receptor; R-chemo: rituximab chemotherapy; R-CHOP: rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone; RIC-allo-SCT: reduced-intensity conditioning allogeneic stem cell transplant; RT: Richter transformation Personal communication.
Histology: CLL
Previous Tx:
R-chemo and
BCR inhibitor
Previous Tx:
R-chemo
BR
Ibrutinib
Idelalisib + R
Venetoclax
Histology: RT
Venetoclax R-CHOP
RIC-allo-SCT RIC-allo-SCT
TP53 wt
Long
remission
duration
TP53 mutated and/or deleted
or
Short remission duration
RIC-allo-SCT