clinical safety & effectiveness session # 11 emergency center observation unit 10.15.09 date
TRANSCRIPT

Clinical Safety & Effectiveness Session # 11
Emergency Center Observation Unit
10.15.09
DATE

Project Team
• Patrick Chaftari, MDAssistant Professor , GIM, AT & EC
• Jean H Tayar, MD Assistant Professor, GIM, AT & EC
• Ashutosh GuptaClinical Business Manager, EC
• Richard A. IveyQuality Engineer, Office of Performance Improvement
• Cindy SegalClinical Quality Improvement Consultant, Office of Performance Improvement
• Cylette R. Willis, PhDAssociate Director, Quality Education and Evaluation, Office of Performance Improvement
Project Sponsor: Carmen E. Gonzalez, MDAssociate Professor, GIM, AT and ECSection Chief, EC

Improving Patient Care in the EC

EC Situation
• National benchmark ER Length of Stay (LOS) is 4 hours
• MDACC EC LOS averages 9.5 hours (up to 24 hrs )
• Current situation affects patient care and safety

Can We Improve This Picture?
• Patient safety
• Patient care
• Patient satisfaction
• Bed utilization

00-05 Hrs, N=4,734
42%
06-10 Hrs, N=3,879
34%
11-15 Hrs, N=1,328
12%
16-20 Hrs, N=642
6%
20+ Hrs, N= 675
6%
Pts Treated while in The EC (No Inpt Admission)Patients Treated While in EC (No Admission)
% of Visits by Hours in EC from Lobby Sign-In to Leave TimeApril 1, 2008 to March 31, 2009
1 year DataPrepared by: Linda DeFord OPI Clinical Informatics Data Source: EC Tracking Data

16-20 Hrs
N=642
6%
20+ Hrs
N= 675
6%
Snapshot of Patients Discharged from EC After a LOS > 16 hrs
(March 2009, 119 pts)
(14) 12%
(74) 62%
(4) 3%
(27) 23%
One year data

EC Patient Process

OBS Unit Better Care
• Opportunity to improve patient safety and patient care
• Literature review: Placement on OBS will improve quality of care and revenue Improve disposition→ clinical outcome→ decrease liability Decrease patient and caregiver frustrations Free up EC bed →Decrease some of the EC congestion →Shortens
LOS Decrease cost by efficient usage of EC and inpatient bed Avoid unnecessary admissions and decrease un-reimbursed
readmissions

Observation Unit
• Observation unit could be → a safe→ effective→ cost-saving
way of ensuring that patients who are considered to be intermediate category receives appropriate care.
10

Project

AIM Statement
The aim of this project is to increase the percentage of EC patients placed on Observation by 50% from the baseline of 1.95% to 2.93% during the pilot
period, July 1 - July 22, 2009.
• Baseline period: May 2008 - April 2009
• Process begins when provider evaluates patient in EC and ends when provider places patient on Observation
• Value to the organization – improve patient care and safety, potential financial advantage

How Will We Know That a Change is an Improvement?
Outcome measure: Percentage of EC patients placed on Observation
Data collection: Whiteboard activity report Technical charges
Specific target: 2.93%
Project Milestones
• Team created April 2009
• AIM statement created April 2009
• Weekly team meetings May - August
• Planning April - June
• Interventions implemented July 1 – 22
• Presentation August 7

Fishbone Diagram
LOW NUMBER OF PATIENTS PLACED ON
OBSERVATION
Order sets
Physicians
Lack of education
Lack criteria to place on Observation
Don’t think about it
Nurses
Technology Processes Facilities
Clerks
Do not check observation box on charge sheet
Do not notify clerks that patient placed on
Observation
Training
Data entry
Whiteboard does not visually identify current Observation patients
Unclear processes
Lack of space
Tracking LOS countdown
Identifying Observation patientsBudget to staff
space
Do not understand billing
Guidelines for disposition decision
Tracking patient progression
Appropriate forms
Confirm access to CARE system
Staffing
Paperwork
Physician hand-off
Training

PLAN: The Intervention
• Plan project • Develop presentation materials for providers• Design new EC physician order set and forms• Start general guidelines for placing patients on Observation• Gain leadership buy-in• Raise awareness of OBS availability
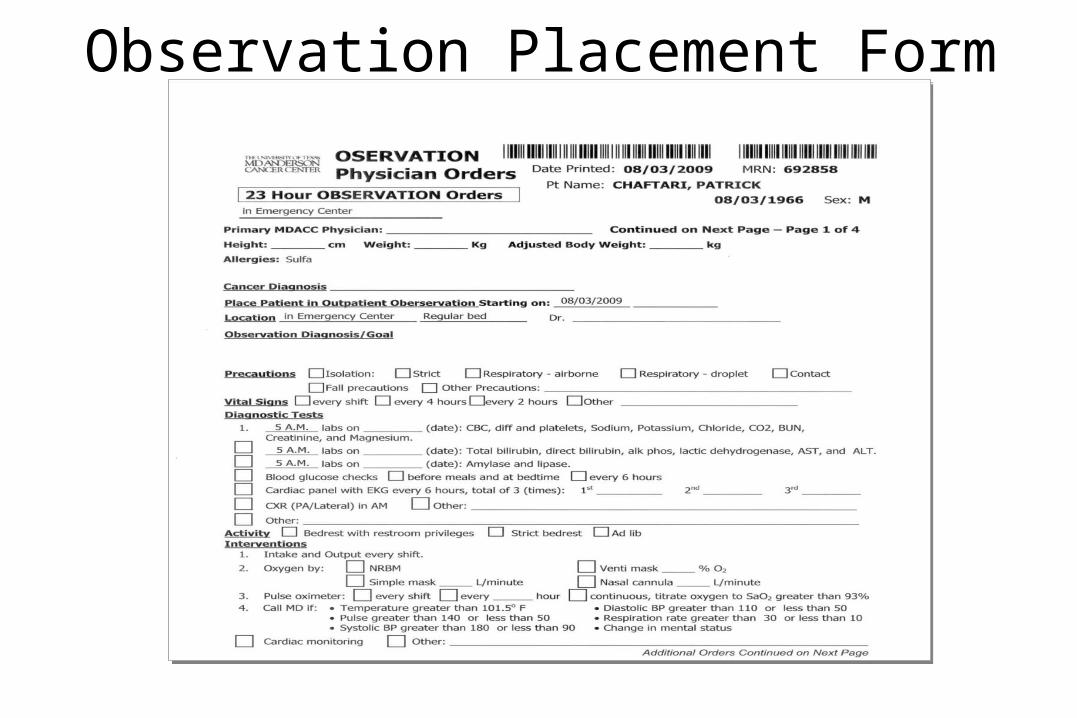
Observation Placement Form
Placeholder for Obs form and/or physician order set visual
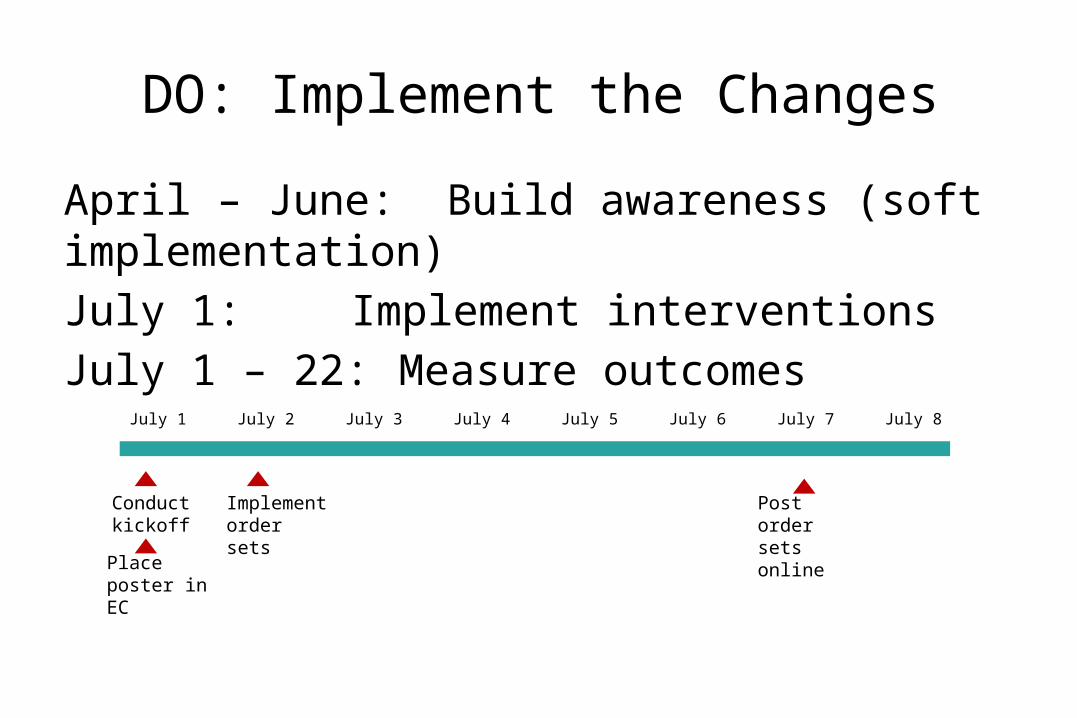
DO: Implement the Changes
April – June: Build awareness (soft implementation)July 1: Implement interventionsJuly 1 – 22: Measure outcomes
July 1 July 2 July 3 July 4 July 5 July 6 July 7 July 8
Conduct kickoff
Implement order sets
Post order sets online
Place poster in EC

EC Observation start date: July 1st,09
Consider
Observation
placement
Patient is not
ready to be
discharged home
Patient do not
meet admission
criteria
And you expect
improvement within the next
23h to the point
where the patient
could be discharged home
Upon completion of the patient’s work-up

Implementation Issues• Stakeholder identification was incomplete (Clinical Effectiveness)
→ Delay in posting physician order set •Implementation period was too short to address EC meeting schedule, introduce language and new forms
• Non-EC faculty working in the EC not familiar with the process

Results
21

Baseline(May 1, 2008 – April 30, 2009)
Project Intervention Period (July 2009)
OBS Patients1.95 % 5.20 %
391 87
Total Number of patients
20086 1674
CHECK: Results and Impact
Test of proportions p-value < 0.001

9.0%
8.0%
7.0%
6.0%
5.0%
4.0%
3.0%
2.0%
1.0%
0.0%
Month
Perc
ent of Patients
Pla
ced o
n O
bs
(%)
_X=4.6%
UCL=8.3%
LCL=0.8%
Apr-09May-08
Percent of Patients Placed on Observation of the Total EC Visits (Monthly)
Before/After Intervention Test of Means, p-value = 0.004
Source: EC WhiteboardPrepared By: Ash Gupta & Richard Ivey

0.18
0.16
0.14
0.12
0.10
0.08
0.06
0.04
0.02
0.00
Day
Perc
ent of Patient Pla
ced o
n O
bs
_P=0.0534
UCL=0.1435
LB=0
9-J un 1-J ul9-J un 1-J ul
11
Tests performed with unequal sample sizes
Percent of Patients Placed on Observation of the Total EC Visits (Daily)
Before/After Intervention Test of Means, p-value = 0.002
Source: EC WhiteboardPrepared By: Ash Gupta & Richard Ivey

Potential Financial Impact
What is the financial impact of these results on the organization?
• Decrease waste by more efficient use of EC bed and inpatients beds
• Capture of uncharged technical and professional fees
• Bed utilization and resources

0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%$0
$200,000
$400,000
$600,000
$800,000
$1,000,000
$1,200,000
$1,400,000
$1,600,000
$1,800,000
$2,000,000
Annual Technical Charges for Patients with EC Stay > 16 Hours and Discharged Home
Expected Charges Including Obs
Estimated Actual Charges
Percent of Patients Placed on Obs with EC Stay > 16 Hours
Estim
ated
Ann
ual T
echn
ical
Cha
rge
Data source: EC Whiteboard to compute LOS (May '08 - Apr '09)
Note: To estimate the actual tech-nical charges for patient with EC stay > 16 hours, an average ap-proach was used using Levels 4 and 5 charge amounts
Assuming 62% of patients with EC stay > 16 hours and discharged home were placed on obs, this represents a potential benefit of approximately $650,000
$650,000
Source: EC WhiteboardPrepared By: Ash Gupta & Richard Ivey

Assuming 62% of patients with EC stay > 16 hours and discharged home were placed on obs, this represents a potential benefit of approximately $428,000
Data source: EC Whiteboard (May '08 - Apr '09)
To estimate the charges for patients with EC stay > 16 hours, an average approach was used using Levels 4 and 5 charge amounts
‘Obs – 1 provider’ assumes that the EC provider is caring for the obs patient
‘Obs – 2 providers’ assumes that a non-EC provider is caring for the obs patient
0.10.13
0.160.19
0.220.25
0.28
0.3100000000000020.34
0.37 0.40.43
0.460.49
0.520.55
0.58
0.610000000000001
0.640000000000005
0.670000000000005
0.700000000000001
0.730000000000001
0.7600000000000040.79
0.820000000000001
0.8500000000000010.88
0.91
0.940000000000001
0.970000000000001 1$0
$200,000
$400,000
$600,000
$800,000
$1,000,000
$1,200,000
$1,400,000
$1,600,000
Estimated Annual Professional Charges for Patients with EC Stay > 16 Hours and Discharged Home
Standard Recovery
Obs - 1 provider
Obs - 2 providers
Percent of Patients Placed on Obs with EC Stay > 16 Hours
Estim
ated
Ann
ual P
rofe
ssio
nal C
harg
e
$428,000
Source: EC WhiteboardPrepared By: Ash Gupta & Richard Ivey
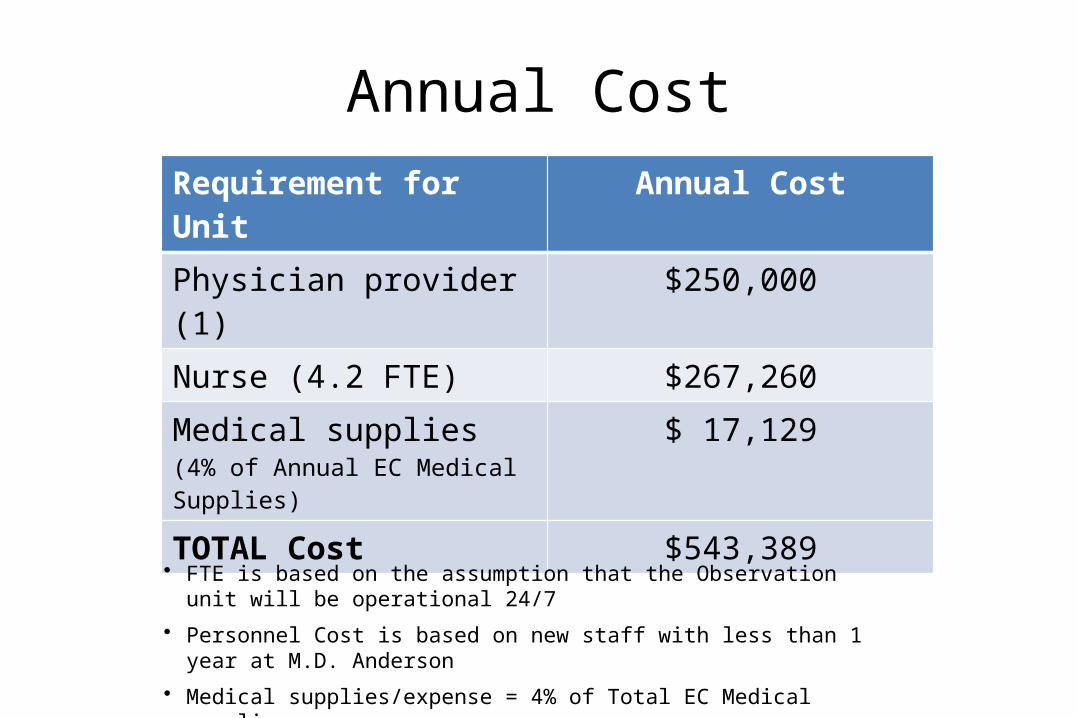
Annual CostRequirement for Unit Annual CostPhysician provider (1) $250,000Nurse (4.2 FTE) $267,260Medical supplies (4% of Annual EC Medical Supplies)
$ 17,129
TOTAL Cost $543,389
• FTE is based on the assumption that the Observation unit will be operational 24/7
• Personnel Cost is based on new staff with less than 1 year at M.D. Anderson
• Medical supplies/expense = 4% of Total EC Medical supplies
• Deduction % = 48.67
Estimated Number of Observation Beds

3 4 5 6 7 8 9 10 11 120%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Avg Utilization Rate vs Number of Observation Beds in Operation
Utilization of Obs Beds
Number of Dedicated Observation Beds
Util
izati
on R
ate The 'Utilization of Obs Beds'
is calculated as the average amount of time occupied divided by the total time available (24-7). This is done by looking at each of the dedicated beds over the entire year.
The choice of number of obs beds should be balanced with the number of patients waiting for a bed
Source: EC WhiteboardPrepared By: Richard Ivey

Next Steps
ACT: Expansion of Implementation
• Maintain and expand awareness of available OBS services in the EC
• Improve identification of OBS patients in the EC
• Review appropriate use of OBS placement
• Track progress of revenue realization

Conclusions
• OBS unit could be a viable solution to improve patient safety and quality of care in the EC
• By decreasing waste and capturing uncharged services OBS unit may provide net revenue to organization
Recommendations
• Designated OBS Unit (Closed unit)– Access limited to EC provider and/or observation
provider– “Virtual” or “Shared” OBS unit within Pod A
• Designated non-EC provider coverage– Improve safety and quality of patient care – Cost of additional provider offset by fee structure

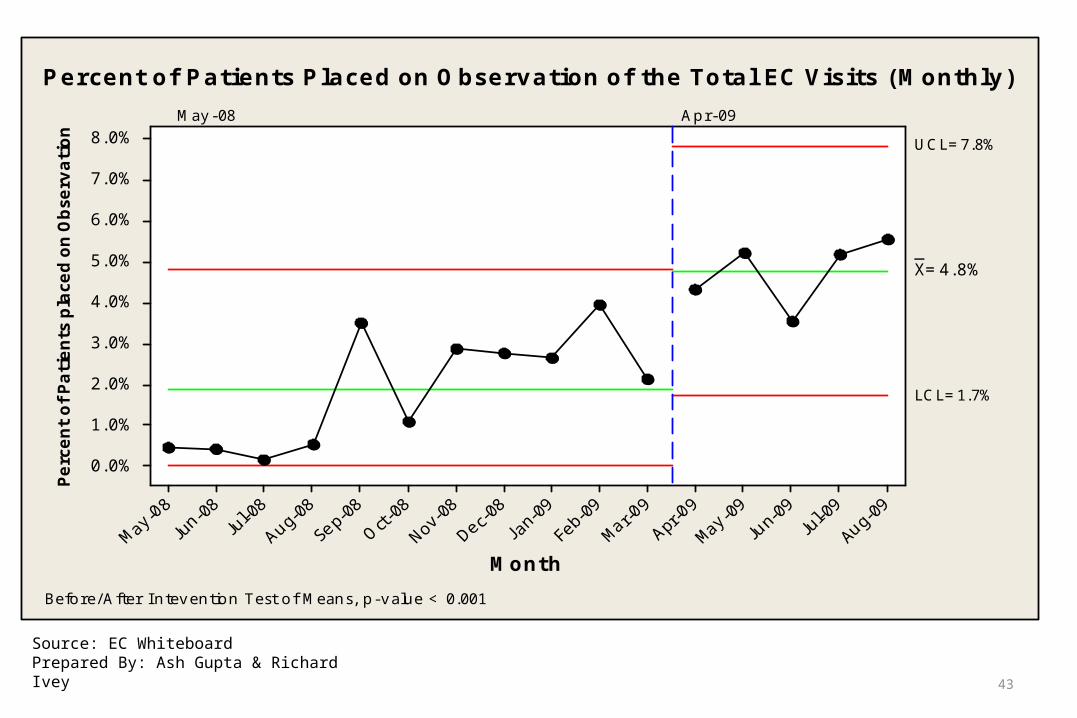
What have we accomplished so far?• Increased number of observation patients to 5.57%
• Improved patient safety Medication reconciliation Diet, activity, fluid infusion
• Improved quality of careBetter oversight by having an APN following these patients on OBS
• Increased RN satisfaction and confidence Improving communication about plan of care
42
43
8.0%
7.0%
6.0%
5.0%
4.0%
3.0%
2.0%
1.0%
0.0%
Month
Perc
ent of Patients
pla
ced o
n O
bse
rvation
_X=4.8%
UCL=7.8%
LCL=1.7%
May-08 Apr-09
Percent of Patients Placed on Observation of the Total EC Visits (Monthly)
Before/After Intevention Test of Means, p-value < 0.001
Source: EC WhiteboardPrepared By: Ash Gupta & Richard Ivey

Questions
Thank you