clinical quality measures, meaningful use, and...
TRANSCRIPT
Welcome to the Data Analytics Toolkit PowerPoint presentation on clinical
quality measures, meaningful use, and data analytics.
According to the Centers for Medicare and Medicaid
Services, Clinical Quality Measures (or CQMs) are
tools that help us measure and track the quality of
healthcare services provided by eligible
professionals (EPs), eligible hospitals (EHs) and
critical access hospitals within our health care
system. These measures use a wide variety of data
that are associated with a provider’s ability to deliver
high-quality care or relate to long term goals for
health care quality. CQMs measure many aspects of
patient care including: health outcomes, clinical
processes, patient safety, efficient use of healthcare
resources, care coordination, patient engagements,
population and public health, and clinical guidelines.

In order to effectively capture, calculate and report
clinical quality measures electronically,
organizations must use data analytics.
HIMSS, the Health Information Management
Systems Society, defines healthcare analytics as
“the systematic use of data and related clinical and
business (C&B) insights developed through applied
analytical disciplines such as statistical, contextual,
quantitative, predictive, and cognitive spectrums to
drive fact-based decision making for planning,
management, measurement and learning.” (HIMSS,
2013)
Thus, the CQMs included in the EHR incentive
program are considered health data analytics. The
purpose of the CQMs are to collect data on specific
populations to improve decision-making and overall

population health.

Clinical quality measures are required to be
reported for multiple state and federal programs.
This table illustrates how the same measure may be
reported to multiple programs. For example, NQF#
0031 measures breast cancer screening and it can
be reported for the CMS EHR Incentive Program,
the Physician Quality Reporting System, the
Accountable Care Organization shared savings
program, and the Medicare Advantage Program.

The EHR Incentive Program is broken into three
different Stages. Stage 1 is focused on data capture
and reporting; Stage 2 is focused on advanced
clinical processes; and Stage 3 is focused on
improved outcomes. The measures and objectives
of the program are known as “meaningful use” of
certified EHR technology.
Within Stage 1 meaningful use, Clinical Quality
Measures are a required core objective for eligible
professionals and eligible hospitals. Through 2013,
eligible professionals must submit 3 core measures
and 3 menu measures (core measures are required
for all professionals and menu refer to those

measures that are most relevant for the
professional’s specific practice).
Eligible hospitals are required to submit 15 clinical
quality measures, regardless of hospital size, type
or location.
The timeline of the EHR Incentive Program includes
a major upgrade based upon updated EHR
certification standards. Beginning in 2014, Eligible
Professionals and Eligible Hospitals are required to
report CQMs based upon the 2014 specification,
regardless of the professionals’ or hospitals’
particular stage of meaningful use. The 2014
specifications for CQM reporting include that:
-Eligible Professionals must report 9 of 64 approved
CQMs (the total number of approved CQMS has
been increased from 38)
-Eligible Hospitals must report 16 of 29 approved

CQMs—there were 15 eligible CQMs for hospitals
previously.
-The CQMs must be reported using data captured
directly within the certified EHR technology and
reported directly to CMS using the certified
technology.
-Measures selected by both Eligible Hospitals and
Eligible Professionals must cover at least three of
the National Quality Strategy domains.

The purpose of the National Quality Strategy is to
align national quality measure and quality
improvement actions. The Strategy is focused on
better care, healthy people and communities, and
affordable care. The Strategy has six priority areas.
1. Improving patient safety;
2. Engaging patients;
3. Promoting care coordination;
4. Promoting prevention;
5. Promoting best practices within communities;
6. Reducing costs.

The EHR Incentive Program and its clinical quality
measure requirement provide a great example of
data analytics, which involves the analysis of high
quality data. To successfully attest to meaningful
use and receive incentive payments, eligible
professionals and hospitals are required to use
certified EHR technology to collect, calculate, and
report clinical quality measures to the Center for
Medicare and Medicaid Services.

To further illustrate the point of how clinical quality
measures are related to data analytics, let’s turn to
the structure of the CQMs themselves. For each
clinical quality measure, specific data elements are
required to determine if a patient will be included or
excluded in the measure. In order to accurately
include or exclude patients from a measure, the
certified EHR technology must have the defined
data elements constructed properly and the
measures defined accurately to reflect care
provision within the ambulatory or acute care
setting. Just as a point of reference, there are an
average of 27 data elements required to calculate
each EH CQM and 16 for each EP CQM. This point

reflects the complexity of clinical quality measure
specifications and calculations.

To demonstrate the relationship between clinical
quality measures and data analytics, take for
example this image. It is the interface used by EHR
vendors when testing their software for EHR
Certification, which is also required for meaningful
use. The EHR software must be able to calculate
the number of patients included in the population,
the denominator and whether there were any
exclusions, the numerator and any exclusions, and
finally exceptions for each measure. Exceptions
refer to such things as the measure falling outside of
the provider’s scope of practice.

The complexity of calculating clinical quality
measures underscores the importance of data
quality itself. The old adage of “garbage in, garbage
out” is relevant here. If the data collected within the
EHR lacks integrity, the validity of the CQM is
questionable. This is the reason why data analytics
is on a continuum from data collection to knowledge
utilization. Without high quality data to analyze, the
findings of the analysis are irrelevant. For example,
it is important that the measures are constructed in
a way that pulls data from the correct fields and that
there are not duplicate fields for data entry.

Let’s turn to an example of how key clinical activities
are essential for capturing high quality data that can
be used for calculating and reporting clinical quality
measures. NQF measure 0001 is related to
completing asthma assessments for patients with
specific symptoms.
The measure is defined as the “Percentage of
patients aged 5 through 40 years with a diagnosis of
asthma and who have been seen for at least 2 office
visits, who were evaluated during at least one office
visit within 12 months for the frequency (numeric) of
daytime and nocturnal asthma symptoms.”

This measure is presently a menu set measure for
meaningful use.
The rationale for the clinical quality measure is
outlined in the clinical guidelines, which drive clinical
documentation to support the provision of care. The
clinical guideline for this measure include monitoring
of signs and symptoms, pulmonary function, quality
of life/functional status, pharmacotherapy, and
patient-provider communication.
http://www.qualitymeasures.ahrq.gov/content.aspx?i
d=28054&search=asthma+assessment

In order to measure asthma assessments, numerous types of data are
required to be captured within the electronic health record, including different
types of data for calculating the numerator and denominators. For example, in
order to accurately calculate and report this measure, six different structured
data points are used, including both SNOMED and ICD-9/ICD-10 (both of
which are also required for EHR certification).
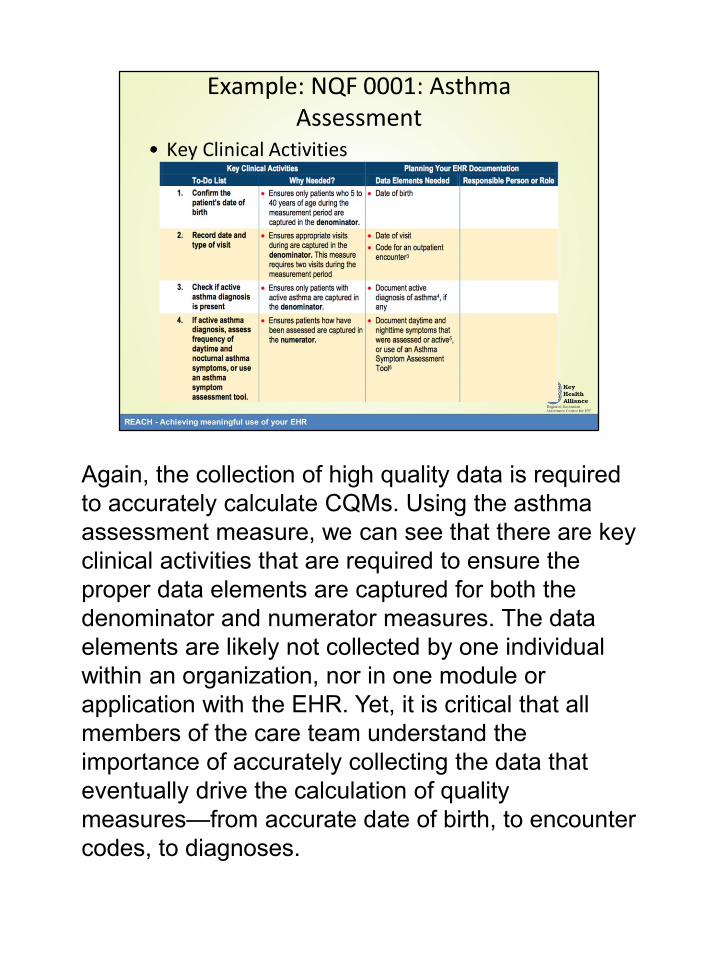
Again, the collection of high quality data is required
to accurately calculate CQMs. Using the asthma
assessment measure, we can see that there are key
clinical activities that are required to ensure the
proper data elements are captured for both the
denominator and numerator measures. The data
elements are likely not collected by one individual
within an organization, nor in one module or
application with the EHR. Yet, it is critical that all
members of the care team understand the
importance of accurately collecting the data that
eventually drive the calculation of quality
measures—from accurate date of birth, to encounter
codes, to diagnoses.

To drill further into the calculation of this measure,
the measure is limited to only those patients aged 5-
40 with an active diagnosis of asthma who have had
at least two encounters within the past twelve
months where one of the visits included the
evaluation of asthma symptoms. To calculate
encounters, CPT codes are required.

To complicate matters, there are multiple asthma
diagnoses that must be included in the analysis to
define the measure population. There are a total of
13 ICD-9 diagnosis codes for asthma—they are all
shown here.
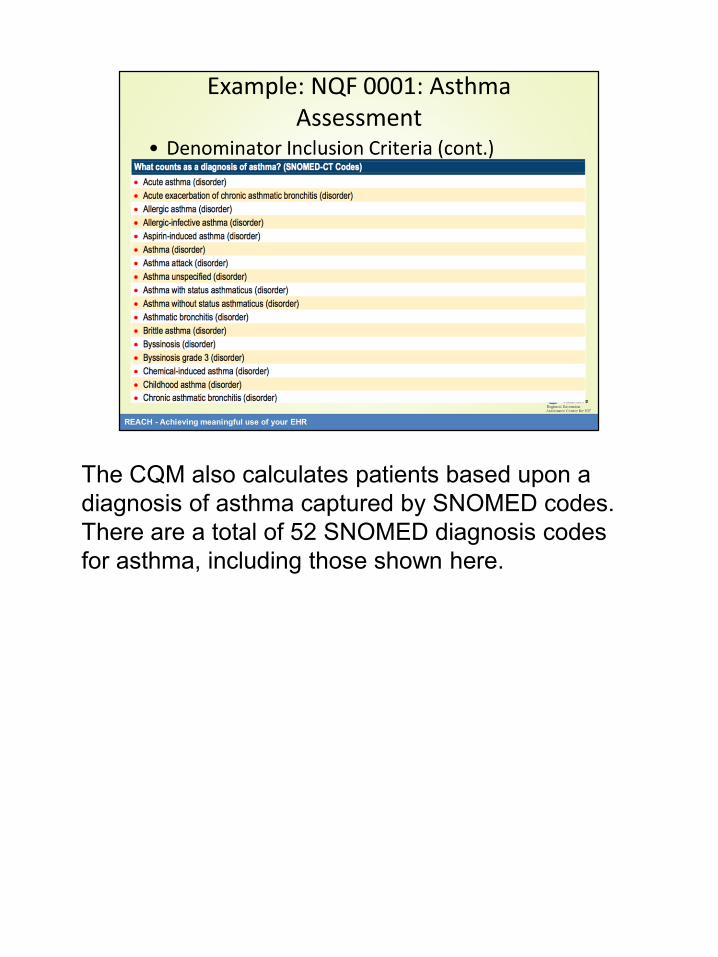
The CQM also calculates patients based upon a
diagnosis of asthma captured by SNOMED codes.
There are a total of 52 SNOMED diagnosis codes
for asthma, including those shown here.
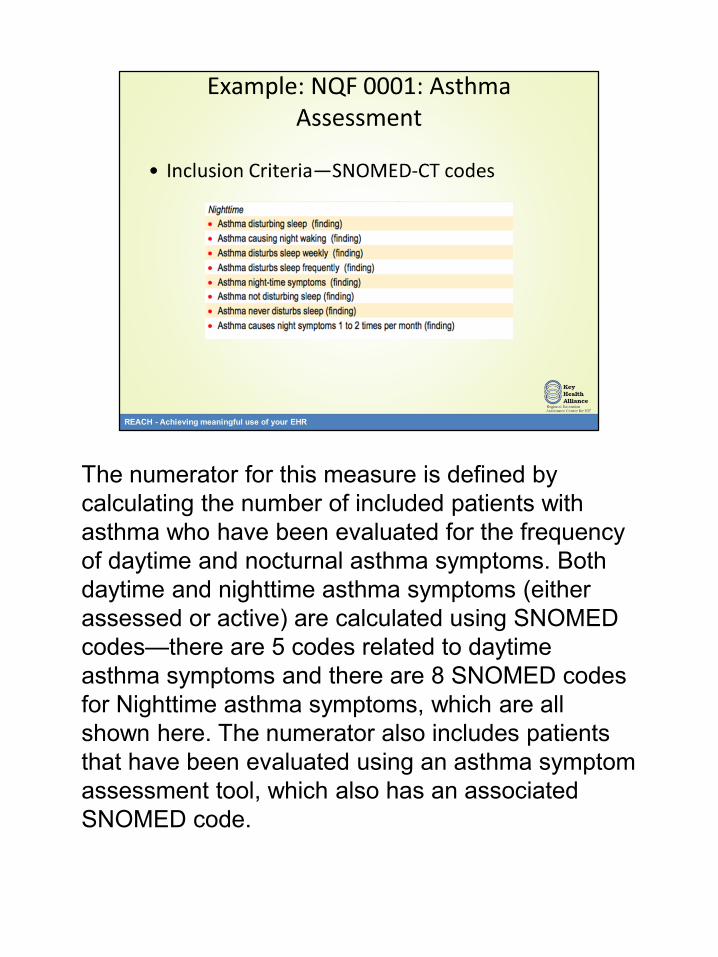
The numerator for this measure is defined by
calculating the number of included patients with
asthma who have been evaluated for the frequency
of daytime and nocturnal asthma symptoms. Both
daytime and nighttime asthma symptoms (either
assessed or active) are calculated using SNOMED
codes—there are 5 codes related to daytime
asthma symptoms and there are 8 SNOMED codes
for Nighttime asthma symptoms, which are all
shown here. The numerator also includes patients
that have been evaluated using an asthma symptom
assessment tool, which also has an associated
SNOMED code.
For the purpose of meeting meaningful use, the certified EHR technology must
be able to electronically collect, calculate and report clinical quality measures.
In order to accurately calculate the measures, the data must be queried from
databases, including specific calculations for the numerators, denominators,
and any exclusions for each measure. To provide an example of the
complexity of calculating these measures, please review this white paper
produced by the Computer Sciences Corporation. It shows that one
meaningful use hospital measure requires 27 data elements to be analyzed
from six different EHR source systems, including the admission system,
CPOE, provider documentation, the electronic medication administration
record, the problem list and nursing documentation. (CSC, 2010)
While the topic of clinical quality measures and data analytics is complicated,
there are many resources available to assist with the work of proper data
collection and analysis. The National Learning Consortium has developed
reference guides to detail the data elements required for calculating each
measure. These tools are a great place to get started with your work.
Additionally, CMS has developed documentation to guide the technical
development of clinical quality measures for meaningful use. It has published
specifications for data standards and sample database programming to
calculate each meaningful use measure. This is a great guide for those
individuals and organizations looking to understand the structure of measures
and how to develop queries to extract measures from databases.