clinical practice guidelines for physical therapy in ... · on the basis of history-taking,...
TRANSCRIPT

1
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
IntroductionThese guidelines concern the diagnosistic and
therapyeutic processes involved in providing physical
therapy for patients with chronic obstructive
pulmonary disease (COPD). The decisions made in
arriving at Justification of the guideline
recommendations are described in detail in the
second part of these guidelines, which is entitled
“Review of evidence”.
Target group
These guidelines are intended for physical therapists
who treat patients who, as a result ofbecause of COPD,
have impaired mucus clearance, whose normal daily
life activities are limited by dyspnea, or who have
impaired exercise capacity. These physical therapists
are expected to have the relevant expertise and the
diagnostic and therapeutic skills needed to treat these
patients. Depending on the goals of treatment,
special facilities or a well-equipped exercise area may
be needed for carrying out the diagnostic and
therapeutic processes diagnosis and therapy involved
in treating these patients.
Definition of COPD
COPD includes the disorders of chronic bronchitis and
emphysema. Chronic bronchitis is defined as the
presence of continuous bronchial obstruction and of
a chronic productive cough that lasts for at least three
months in each of two successive years. In making
this diagnosis, other causes of chronic coughs should
be excluded. Emphysema is present when there is
increased lung volume accompanied by destruction
of alveolar walls, without fibrosis.
Chronic bronchial obstruction is a key factor in
patients with COPD, bringing about complaints such
as dyspnea, whether during exercise or at rest or both,
and coughing, sputum expectoration, and wheezing.
The patient’s general level of fitness deteriorates
because of the disorder and its direct and indirect
consequences, such as hypoxemia, medication use,
immobility and malnutrition. Patients may tend to
avoid exercise and this causes their general
physiological condition to deteriorate further.
Consequently, there may be problems performing
normal daily life activities and psychological
complaints may develop, which can be expressed in
the form of anxiety, depression and lowered self-
esteem. In addition, the patient may become socially
isolated.
The primary causes of COPD are cigarette smoke and
occupational exposure to high-risk substances. In
Clinical practice guidelines for physical therapy in
patients with chronic obstructive pulmonary disease
GE BekkeringI, HJM HendriksII, RVM Chadwick-StraverIII, R GosselinkIV, M JongmansV, WJ PatersonVI, CP van
der SchansVII, MCE Verhoef-de WijkVIII, M DecramerIX.
I Trudy Bekkering, physical therapist and movement scientist, Research and Development Department, Dutch Institute of Allied Health
Professions, Amersfoort, the Netherlands.
II Erik Hendriks, physical therapist and movement scientist, Research and Development Department, Dutch Institute of Allied Health
Professions, Amersfoort, the Netherlands.
III Renata Chadwick-Straver, physical therapist, Department of Physical Therapy, VU Hospital, Amsterdam, the Netherlands.
IV Rik Gosselink, physical therapist, Department of Physical Therapy and Rehabilitation, Gasthuisberg University Hospital, Leuven, Belgium.
V Machteld Jongmans, physical therapist, Department of Physical therapy, Dekkerswald University Pulmonary Center, Groesbeek,
The Netherlands.
VI Bill Paterson, physical therapist, Department of Physical therapy, Dijkzigt Academic Hospital, Rotterdam, the Netherlands.
VII Cees van der Schans, physical ttherapist, Department of Physical therapy, Academic Hospital, Groningen, the Netherlands.
VIII Mirjam Verhoef-de Wijk, physical therapist and Cesar therapist, Academic Institute for Physical Therapy, Utrecht, the Netherlands.
IX Marc Decramer, pulmonary physician, Department of Pulmonary Diseases, Gasthuisberg University Hospital, Leuven, Belgium.

addition, air pollution, genetic factors and respiratory
infections can contribute to the development of
symptoms. A poorer prognosis is associated with
persistent smoking, increased non-specific hyper
responsiveness, mucus hypersecretion, hypoxemia
and weight loss. The exercise capacity of the patient,
has a positive impact on survival.
Epidemiology
In the 1960s and 1970s, a number of cohort studies
on the prevalence of asthma or COPD were carried out
in adults aged up to 65 years in the Netherlands.
They did not differentiate between asthma and COPD.
The prevalence of COPD in the Dutch population
ranges from 13.0–16.8% in men and from 4.5–7.3%
in women. On average, 2.2 new COPD patients per
1,000 adults report to primary care physicians each
year (i.e., the incidence of COPD), while 20.4 patients
out of every 1,000 adults are diagnosed with COPD
(i.e., the prevalence of COPD). Both the incidence and
prevalence rise with age and both are higher in men
than in women. Both are related to the smoking
habit.
Position of physical therapy
In the Netherlands, patients are referred to physical
therapists by either a primary care physician or a
medical specialist. The Dutch College of General
PractitionersNederlands Huisartsen Genootschap
(NHG, Dutch College of General Practitioners) has
published guidelines on the diagnosis and treatment
of adult patients with COPD. With regard to physical
therapy, these guidelines only refer to the use of
specialized facilities. A better understanding of how
physical therapy can be used in this group of patients
– for instance, by improving communication between
physical therapist and referring physician – is
important for increasing the efficiency of care in
these individuals.
DiagnosisReferral
Patients with COPD may be referred for physical
therapy after their medication has been optimized.
Furthermore, the COPD patients must haveresult in
impaired mucus clearance, disability in performing
normal daily activities due to dyspnea, impaired
exercise capacity, or a combination of these factors.
See Table 1.
COPD is accompanied by a range of impairments,
disabilities and problems with participation. The
patient’s forced expiratory volume in one second
(FEV1), a measure of airflow obstruction, is, by itself,
not a good predictor of the degree of difficulty the
patient experiences. Optimally, the referral
documentation should contain data on the severity
and nature of the airflow obstruction, the natural
course of the disorder, and relevant medical and
psychosocial factors. If exercise training is indicated,
data from an incremental exercise test at maximum
load should be included in the referral data, if the test
was carried out. These requirements imply a need for
consultation between pulmonary specialists, physical
therapists and, if involved, other healthcare
specialists.
History-taking
In history-taking, the aim is to gain the clearest
picture possible of the patient’s health problem. The
physical therapist must determine the patient’s
general needs, expectations, degree of motivation,
need for information, and (global and local) load and
load-bearing capacity, and how the patient is coping
with the disorder and its consequences. One
component of history-taking is the quality-of-life
inventory. Questionnaires such as the Chronic
Respiratory Disease Questionnaire (CRDQ) or the St
George’s Respiratory Questionnaire (SGRQ) can be used
for this purpose. Table 2 details the main points of
history-taking. More information is given below in
the review of the evidence.
2
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Physical therapy is indicated when, because of COPD, patients:
• have problems coughing up sputum and have recurrent respiratory infections; or
• have breathlessness (dyspnea) and are, therefore, limited in their daily activities, or both.
Table 1. Main reasons for referral.
On the basis of history-taking, generally two
problems can be distinguished in these patients:
impaired mucus clearance and impaired exercise
capacity including dyspnea. In practice, these two
problems often occur in combination. Patients may
also have additional problems, such as cor pulmonale
or hypoxemia, that could influence the type of
physical therapy intervention or program selected.
Physical examination
The physical examination is defined as an
examination that covers functional impairment and
disabilities in normal daily activities. The strategy
adopted in the physical examination depends on the
health problems found. Tables 3 and 4 describe the
main points of the physical examination of patients
with impaired mucus clearance and patients with
impaired exercise capacity (including dyspnea),
respectively. They also describe how data are
obtained. More information on the physical
examination and the measuring instruments used is
given below in the review of the evidence.
Analysis
The results of history-taking and the physical
examination, supplemented by medical referral data,
provide clear evidence for deciding whether to refer a
patient for physical therapy. On the assumption that
the referring physician has correctly diagnosed COPD,
the following questions should be answered:
• Are any COPD-related health problems present?
• Which functional impairments and disabilities are
observable and what problems with participation
does the patient experience?
• Which complaints, impairments and disabilities
can be affected by physical therapy?
• Is the patient motivated to undergo physical
therapy?
On the basis of the obtained data, the physical
therapist should be able to determine whether a
referral for physical therapy is justified. If there is any
3
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
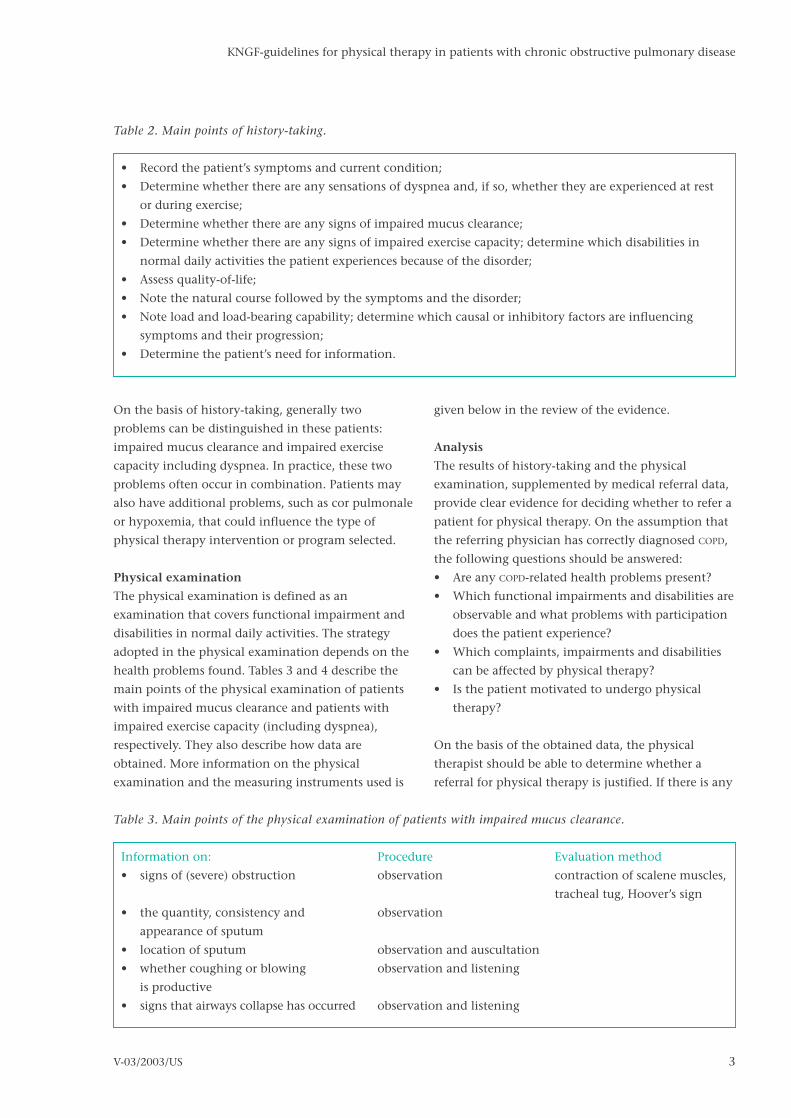
• Record the patient’s symptoms and current condition;
• Determine whether there are any sensations of dyspnea and, if so, whether they are experienced at rest
or during exercise;
• Determine whether there are any signs of impaired mucus clearance;
• Determine whether there are any signs of impaired exercise capacity; determine which disabilities in
normal daily activities the patient experiences because of the disorder;
• Assess quality-of-life;
• Note the natural course followed by the symptoms and the disorder;
• Note load and load-bearing capability; determine which causal or inhibitory factors are influencing
symptoms and their progression;
• Determine the patient’s need for information.
Table 2. Main points of history-taking.
Information on: Procedure Evaluation method
• signs of (severe) obstruction observation contraction of scalene muscles,
tracheal tug, Hoover’s sign
• the quantity, consistency and observation
appearance of sputum
• location of sputum observation and auscultation
• whether coughing or blowing observation and listening
is productive
• signs that airways collapse has occurred observation and listening
Table 3. Main points of the physical examination of patients with impaired mucus clearance.
doubt about the severity or nature of the disorder or
about any related health problems, the referring
physician should be consulted. The patient may need
to be referred back for additional diagnosis or to
adjust the treatment approach.
After it has been concluded that physical therapy is
indicated, it must be determined whether the
individual patient can be treated according to the
guidelines. Patients can be treated according to these
guidelines if:
• the referral data is adequate; and
• the patient’s medication has been optimized, as
discussed in the NHG guidelines on COPD.
Treatment plan
After the above questions have been answered,
individual treatment goals are drawn upformulated in
consultation with the patient, and a treatment plan is
formulated. In rehabilitation, the general goal of
treatment is to reduce or eliminate the patient’s
impairments, disabilities and problems with
participation, thereby improving quality of life.
Furthermore, for patients with COPD, the most
common treatment goals are:
1. to improve mucus clearance;
2. to improve exercise capacity;
3. to reduce dyspnea; and
4. to promote compliance with therapy.
In addition to those mentioned above, the patient
may experience other health problems, which in
some cases may be associated with the underlying
pulmonary disease. The therapist may deem these
problems to be such that further physical therapy is
indicated. However, these additional health problems
are not covered by these guidelines.
TherapyThe therapeutic process is geared to the treatment
plan, which, among other things, expresses the most
common treatment goals in patients with COPD.
4
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
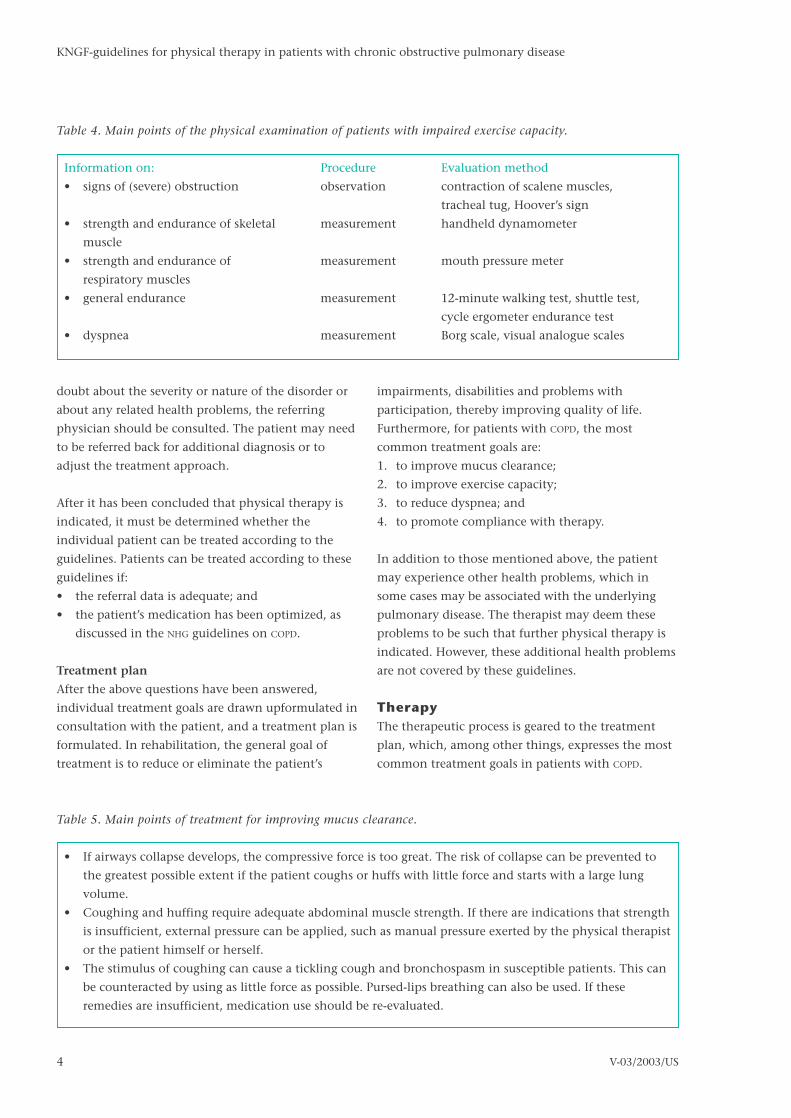
Information on: Procedure Evaluation method
• signs of (severe) obstruction observation contraction of scalene muscles,
tracheal tug, Hoover’s sign
• strength and endurance of skeletal measurement handheld dynamometer
muscle
• strength and endurance of measurement mouth pressure meter
respiratory muscles
• general endurance measurement 12-minute walking test, shuttle test,
cycle ergometer endurance test
• dyspnea measurement Borg scale, visual analogue scales
Table 4. Main points of the physical examination of patients with impaired exercise capacity.
• If airways collapse develops, the compressive force is too great. The risk of collapse can be prevented to
the greatest possible extent if the patient coughs or huffs with little force and starts with a large lung
volume.
• Coughing and huffing require adequate abdominal muscle strength. If there are indications that strength
is insufficient, external pressure can be applied, such as manual pressure exerted by the physical therapist
or the patient himself or herself.
• The stimulus of coughing can cause a tickling cough and bronchospasm in susceptible patients. This can
be counteracted by using as little force as possible. Pursed-lips breathing can also be used. If these
remedies are insufficient, medication use should be re-evaluated.
Table 5. Main points of treatment for improving mucus clearance.

Improving mucus clearance
In order to improve mucus clearance patients are
taught techniques that enable them to clear mucus
effectively by themselves. Long-term goals are, for
example, to ensure that fewer exacerbations of the
condition occur and to engender a less rapid
deterioration in pulmonary function, as indicated by
the FEV1 value.
For mucus clearance, coughing and blowing are
extremely important. The physical therapist should
first, therefore, choose to teach techniques for
effective coughing and blowing. By adjusting the
force used and matching it with the patient’s lung
volume, these techniques can be adjusted for the
individual patient.
If coughing or huffing does not result in the
expectoration of mucus, it may be possible to
promote mucus transport using forced expiration
techniques in combination with postural drainage.
Although the sole use of either postural drainage,
chest percussion or vibration, or positive expiratory
pressure has not been unequivocally substantiated by
the literature, when used in various combinations
these techniques may be effective in individual
patients. If these procedures prove not effective after
six sessions, their continued use is no longer
meaningful. Exercise can help some patients clear
mucus secretions. To encourage mucus clearance,
however, the patient must ventilate substantially .
Then, the normal conditions for exercise training
apply.
Effective procedures for mucus clearance should lead
to the expectoration of mucus, or to a reduction in
rhonchi, either during treatment or within 30
minutes after treatment. The treatment goal will have
been achieved when the patient is able clear mucus
by himself or herself.
Improving exercise capacity
The review of the evidence below describes five
reasons for reduced exercise capacity in these
patients. The different reasons for reduced exercise
tolerance can be distinguished using an incremental
exercise test at maximum load that also involves the
measurement of blood gas concentrations. In
practice, reduced exercise capacity is usually caused
by several factors. For didactic purposes, these factors
will be discussed separately here. By using the
information presented below, the physical therapist
can concentrate on certain aspects of treatment
depending on the individual patient’s needs.
Exercise capacity can be improved in two main ways:
firstly, by increasing efficiency of movement and,
secondly, by achieving a physiological training effect.
Training aimed at improving exercise capacity should
last a minimum of six weeks and a maximum of six
months. Training should be given at least three times
per week for 20–45 minutes. A physiological training
effect occurs when the body has to work against
increasing load. To achieve this, a minimum level of
intensity must be used (see the discussion on
cardiocirculatory limitations below).
1. Cardiocirculatory limitations
In training1 to increase overall exercise capacity, the
general principles for improving physical condition
5
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
• A good breathing technique is necessary for training to build exercise capacity. The breathing technique
should be adjusted for the individual patient.
• In each exercise program, attention should be paid to all the functions that are important for physical
performance, such as muscle strength, muscle endurance, speed, coordination and flexibility. Different
forms of exercise can be used, such as circuit training, sports and games, or swimming.
• Moderation is important in COPD patients. Depending on the Borg scale score or heart rate, for instance,
one patient may need to be encouraged to become more active whereas another may need to be held
back.
Table 6. Main points of treatment for improving exercise capacity.
1. The (Dutch) Classification of Procedures for Paramedical Professions (CVPB) uses the terms exercising and guidding.
6
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
can be applied. To improve exercise capacity (i.e., to
obtain a physiological training effect), one must
exercise at least three times a week for 20–45 minutes
at 60–80% of maximum heart rate. Sessions may
consist of one or more forms of exercise, such as
cycling, walking, climbing stairs and rowing. The
training effect is specific: in other words,
improvement will occur primarily in the activity
being trained. This means that the program content
must be geared to the desired activity, to the patient’s
needs, and to the patient’s main health problems. To
retain effects of the treatment after the conclusion of
therapy, exercise frequency is reduced to once or
twice a week at the same intensity.
2. Ventilatory limitations
In addition to providing a general exercise program,
inspiratory muscle training (IMT) can also be given.
These two elements are discussed separately.
General exercise program
Patients whose exercise capacity is limited by
ventilation problems can receive endurance training
unless hypoxemia (i.e., an oxygen saturation < 90%)
or severe hypercapnia (i.e., an arterial carbon dioxide
pressure > 55 mmHg) is present during exercise.
Training load is determined by the results of the
incremental exercise test, with training aiming for
60–80% of maximum load for an exercise duration of
at least 20 minutes. If hypoxemia or severe
hypercapnia is present, exercises should be carried
out using intervals . Most commonly, sequences of
two minutes of exercise followed by two minutes of
rest are repeated for a total of, at least, 20 minutes.
Even for patients who experience increased
obstruction when exercising (e.g., patients with
unstable airways), interval training is the correct way
of increasing exercise capacity. Some practical
examples are circuit training and interval walking or
cycling protocols.
Inspiratory muscle training
A prerequisite for giving inspiratory muscle training
is that the patient has diminished inspiratory muscle
strength or endurance. To determine whether this is
the case, the physical therapist should measure the
maximum inspiratory pressure at the mouth (PImax).
Reference values are given in Note 12 of the notes on
diagnosis at the end of the review of the evidence.
The appropriate equipment and expertise are required
to perform these measurements correctly. The value
of PImax determines the selection of the exercise
load. In order to train the inspiratory muscles, there
must be some inspiratory resistance. Resistance can
be either flow-dependent or flow-independent (i.e.,
threshold).
To increase the strength and endurance of the
respiratory muscles, the patient should exercise twice
daily for 15 minutes at a load level of at least 30–40%
of PImax. PImax must be measured regularly, so that
exercise intensity can be adjusted during the exercise
program, if necessary. After completion of the
exercise program, respiratory muscle strength must be
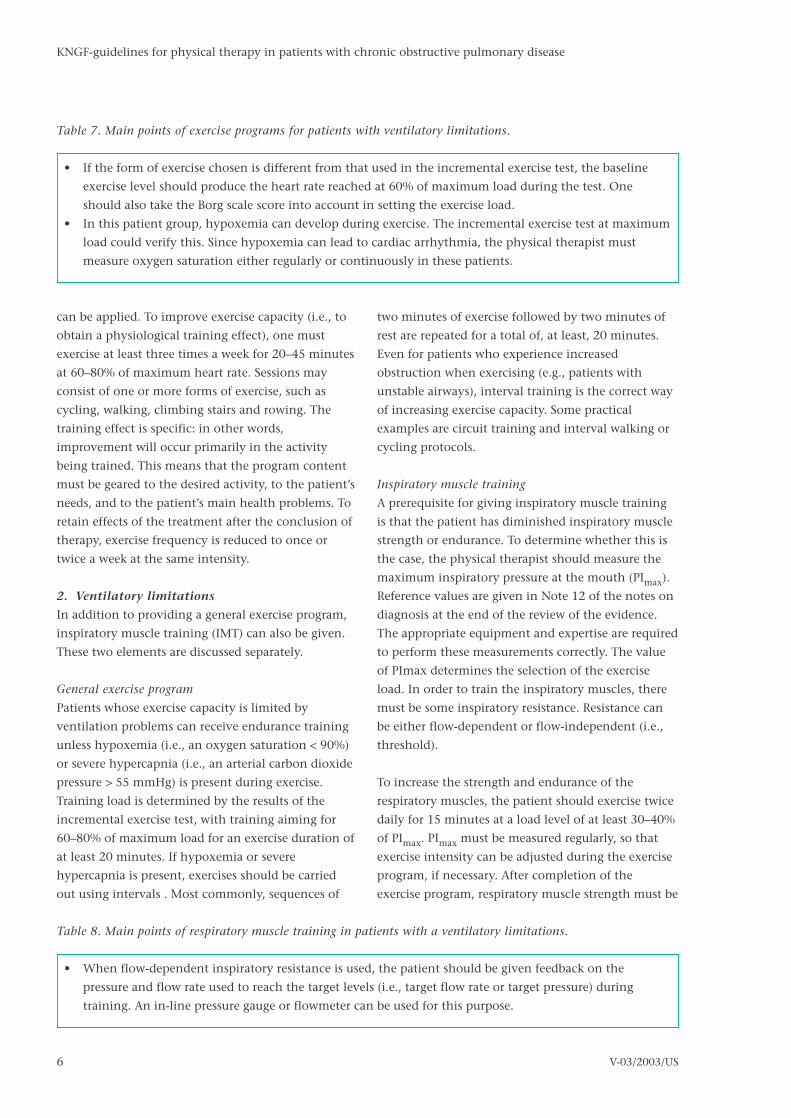
• If the form of exercise chosen is different from that used in the incremental exercise test, the baseline
exercise level should produce the heart rate reached at 60% of maximum load during the test. One
should also take the Borg scale score into account in setting the exercise load.
• In this patient group, hypoxemia can develop during exercise. The incremental exercise test at maximum
load could verify this. Since hypoxemia can lead to cardiac arrhythmia, the physical therapist must
measure oxygen saturation either regularly or continuously in these patients.
Table 7. Main points of exercise programs for patients with ventilatory limitations.
• When flow-dependent inspiratory resistance is used, the patient should be given feedback on the
pressure and flow rate used to reach the target levels (i.e., target flow rate or target pressure) during
training. An in-line pressure gauge or flowmeter can be used for this purpose.
Table 8. Main points of respiratory muscle training in patients with a ventilatory limitations.

maintained. This can be achieved by exercising at the
same intensity 2–3 times a week for two 15-minute
sessions .
3. Oxygen transport limitations
Oxygen transport limitations can result in a
desaturation during exercise. Therefore, the physical
therapist must measure oxygen saturation regularly
or continuously during training. Imminent
hypoxemia can be prevented by supplemental
oxygen therapy. The administration of oxygen is
classified in the same way as providing medication
and can only be prescribed by a pulmonary
physician, who is then responsible for treatment.
Therefore, treatment involving the administration of
oxygen should be carried out in specialized facilities.
If patients are willing, their training can take place in
a primary care facility, provided the physical therapist
has an oxymeter to monitor saturation during
treatment.
When training to increase exercise capacity in these
patients, interval training should be used unless
oxygen supplementation is prescribed. Exercise
intensity depends on the results of the incremental
exercise test. The patient should start with an exercise
load at which oxygen saturation is more than 90%,
unless otherwise indicated by the pulmonary
physician. If supplemental oxygen is given, the target
exercise load can be 60–80% of maximum load. In
addition to training exercise capacity, the physical
therapist may also teach the patient how to use his or
her physical capabilities as efficiently as possible.
Since this is more a matter of ergonomics, it would be
helpful if an occupational therapist specializing in
COPD is consulted or cooperates in treatment.
For these patients, the application of ergonomics
involves exercises aimed at improving the
performance of normal daily activities. In addition,
patients can also practice breathing exercises, such as
breathing at a slow rate with pursed lips. This may
help achieve more effective ventilation and, thereby,
a higher oxygen saturation at rest.
4. Peripheral muscle weakness
For patients with peripheral muscle weakness, an
endurance training program should be given (see the
description under cardiocirculatory limitations above)
unless hypoxemia (i.e., an oxygen saturation < 90%)
or severe hypercapnia (i.e., an arterial carbon dioxide
pressure > 55 mmHg) develops, in which case interval
training is indicated. Other functions , such as muscle
function, velocity, coordination and flexibility, also
need to be trained. Exercise load should be at least
60% of maximum load. The target exercise load
should be as high as possible for the desired duration.
In the training program, additional attention needs
to be given to improving the functioning of relevant
muscle groups.
In giving exercises to strengthen arm and leg muscles
and to improve their endurance, general training
principles apply. The patient should train three times
a week. A training regimen that emphasizes both
strength and endurance is usually employed. An
exercise load of about 60% of maximum and exercises
involving 10–30 repetitions are appropriate.
7
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Table 9. Main points of treatment for patients with oxygen transport limitations.
• If the transfer coefficient (TLco), which indicates the diffusion capacity of the lungs, is less than 50%
predicted, the risk of hypoxia occurring during exercise is very high. In these patients, it is essential to
pay extra attention to measuring oxygen saturation during exercise.
• Good nutrition is important if muscle strength is to be increased. Hypoxemia, inactivity, and, especially,
the use of oral corticosteroids all have a negative impact on muscle function. If any of these factors is
contributing to peripheral muscle weakness, it should be eliminated or its effects should be reduced.
Consultation with the relevant specialist is desirable.
Table 10. Main points of treatment for patients with peripheral muscle weakness.

5. Other factors
One other factor that influences exercise capacity is
an inadequate breathing pattern due to exercise
phobia. The patient might not have been able to
achieve his or her maximum performance during the
cycle ergometer test because of fear of bronchospasm,
dyspnea or stress. In addition, other disorders or
diseases may also have this effect.
Patients in this group can be offered an endurance
training program (see the description under
cardiocirculatory limitations above) unless
hypoxemia (i.e., an oxygen saturation < 90%) or
severe hypercapnia (i.e., an arterial carbon dioxide
pressure > 55 mmHg) develops, in which case
periodic training is indicated. Other functions, such
as muscle function, velocity, coordination and
flexibility, also need to be trained. This patient group
should begin with a very low exercise load. However,
the exercise load should be at least 60% of maximum
load and the target exercise load should be as high as
possible for the desired duration. If anxiety or stress is
contributing to the reduced exercise capacity,
relaxation exercises can be given.
Reducing dyspnea
Dyspnea has multiple causes. In treatment, therefore,
it is important to employ a range of different
approaches and to determine which is most effective
for the individual patient.
Optimizing diaphragm function
The slight contraction of the abdominal muscles
during expiration can facilitate diaphragm function.
This action positions the diaphragm optimally for the
next inspiration, resulting in a better function. In
addition, the patient can assume certain body
postures that lengthen the diaphragm, enabling it to
contract more efficiently. One example is leaning
over from a sitting position. The accessory muscles of
respiration can provide more force if the arms are
anchored in position, for example, if the patient
walks with the aid of a rollator walker or uses
handrails.
Increasing tidal volume and lowering breathing
frequency (at rest)
There are a range of different breathing exercises for
increasing the ratio of inspiration time to expiration
time. The key is to shorten inspiration relatively and
prolong expiration. This process helps patients
become aware of their breathing and gives them the
sense that they can control it and that they can even
contribute to managing their symptoms. Increasing
tidal volume and reducing the breathing rate improve
alveolar ventilation.
During pursed-lips breathing, the patient exhales
gently against slightly pursed lips. This causes the
tidal volume to increase and the frequency of
breathing to decrease. Some patients may already do
this spontaneously.
Increasing the strength and endurance of
respiratory muscles
Inspiratory muscle training can reduce dyspnea
because it increases the load-bearing capacity of the
respiratory muscles. See the discussion of ventilatory
limitations above.
Optimizing ergonomic factors
During treatment, it is important to pay attention to
ergonomic factors. This can involve giving the advice
to alternate periods of efforts with rest. The presence
of a severe obstruction can be a reason for deciding to
assess whether a patient might benefit from different
kinds of mobility aids. This could be done in
consultation with a specialized occupational
therapist, for instance. Examples of such aids are
walking aids (e.g. a rollator walker) or home
8
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Table 11. Main points of treatment for patients with dyspnea.
• In patients with COPD, the breathing pattern is usually functional. Therefore, the physical therapist
must always ensure that any change in breathing movement is an improvement for the individual
patient.
• Not all patients find pursed-lips breathing pleasant.

9
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
adjustments (e.g. the installation of a stairlift).
Desensitization
Repeated experiencing of dyspnea, for example,
during exercise in a safe environment, can reduce the
perception of dyspnea.
Improving compliance with therapy
A significant goal in ensuring therapeutic compliance
is bringing about behavioral modification. For
treatment to have lasting results, patients have to
incorporate the functions and skills learned during
treatment into their daily lives. For COPD patients, this
almost always involves complying with therapy over
the long term.
The physical therapist has a role in training the
patient in and educating the patient about the
behavioral adjustments and modifications required.
Patient education should be considered as a means of
achieving behavioral modification. Consequently,
patient education is a significant aspect of care.
A professional approach to patient education
presumes knowledge about and understanding of
how information can be presented and of the factors
that positively or negatively influence the
development of the desired behavioral modification.
Before beginning patient education, the patient’s
need for information about and training in the new
behavior must be assessed. These needs provide the
starting point for the education program. Patient
education can be subdivided into four categories:
information, instruction, education and guidance. In
practice, these four categories overlap one another. In
each category, activities require different amounts of
time, and make different demands on equipment and
on the therapist’s skills.
To achieve behavioral change, the patient must pass
through six stages:
1. being open to information about the need to
change behavior;
2. understanding and remembering the information;
3. wanting to change behavior;
4. being able to perform the modified behavior;
5. actually performing (doing) the behavior; and
6. continuing to perform the behavior over the long
term.
Analyzing the process in term of these different stages
helps in achieving an understanding of the problems
involved in therapeutic compliance. It is essential for
behavioral modification that patients have
confidence in their own capabilities (i.e., their self-
efficacy) and that the advantages of behavioral
modification outweigh the disadvantages. More
information is given in the review of the evidence.
Completion and reportingAt some point during treatment and, mandatory, at
the end of treatment, the referring physician should
be informed about the goals of treatment, the
treatment carried out and the results of treatment in
the individual patient. Communication will also have
to take place about the division of responsibilities
during rehabilitation and about any necessary
consultation with other health professionals.
After-careAfter treatment has ended, follow-up in the form of
providing after-care will be necessary. After-care is
Table 12. Main points of patient education.
• Patient education must be presented in a structured form. In other words, not too much information
should be given at once and the information should be sequenced in a way that makes sense to the
patient.
• Information given to the patient must be customized. In other words, the patient’s characteristics and
social environment must be taken into account.
• The physical therapist must continuously monitor whether the patient experiences any problems in
practicing exercises or in implementing behavioral modifications, and must provide help in working
through these issues.

provided on the condition that there are no medical
grounds for further treatment. The goal of after-care
is to ensure that the benefits of therapy are
maintained. Patients who receive after-care in a group
can derive additional benefits from contact with
peers.
In the Netherlands, the Dutch Asthma Foundation
(Nederlands Asthma Fonds) organizes athletic groups
for individuals with COPD. These involve participation
in specially adapted group sports and games. Peer
contact plays an important role in maintaining the
newly learned behavior. COPD athletic groups are
coached by physical therapists who specialize in
COPD. No suitable course of action has yet been found
for the category of patients who are not eligible to
attend COPD athletic groups (see the exclusion criteria
noted in the discussion on after-care in the review of
the evidence section).
10
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Table 13. Main points of after-care.
• Over the long term, patients find it easier to continue practicing forms of movement they enjoy. It also
appears easier to continue practicing in a group.
• Scheduling check-ups during after-care increases the patient’s motivation to maintain the behavioral
change and the state of health achieved.

11
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Introduction
The KNGF-Guidelines COPD deals with the physical
therapy treatment of patients with Chronic
Obstructive Pulmonary Disease (COPD), namely
chronic bronchitis and emphysema. The guideline
includes the diagnostic and therapeutic process in
line with the methodical therapeutic conduct.
Definition
KNGF-guidelines are defined as ‘guidelines whose
production is directed by a central body, that are
developed systematically, that are written by
experts, and dhat deal with the systematic process
of physical therapy in certain health problems
and with various (organizational) aspects of the
profession’.1,2
Objective of the KNGF-guidelines COPD
The objective of the guidelines is to describe the
‘optimal’ diagnosis and physical therapy treatment –
with regard to effectiveness, efficiency and tailored
care - for patients who have, due to COPD,
impairments in the mucus clearance or who
experience disabilities in ADL due to dyspnea or who
have exercise limitations. The recommendations are
based upon current scientific research, professional
and social insights.1-3
Besides the above mentioned goals, the KNGF-
guidelines are explicitly meant to:
• Change the care in the desired direction based on
current scientific research and improve the quality
and the uniformity of this care.
• Assure insight into tasks and responsibilities and
to stimulate cooperation.
• Support the process of decision making with
regard to the treatment or not and the use of
diagnostic and therapeutic interventions.
To make use of the guidelines it is necessary to insure
the recommendations of professional requirements.
Presenting the clinical questions
The group which has formulated these guidelines
wanted to attain an answer on the following
questions:
• Which factors can be influenced by physical
therapy?
• What is the objective of physical therapy?
• Which parts of the physiotherapeutic diagnostic
assessment are valid, reliable and useful in daily
practice?
• Which forms of treatment and prevention are
clinical significant?
Formation of the mono disciplinary working
group
In July 1996 a mono disciplinary working group of
professionals was formed to answer these clinical
questions.3 In the formation of the working group an
attempt was made to achieve a balance in
professionals with experience in the area of concern
or with an academic background. All members of the
working group have stated that they had no
conflicting interests what so ever in relation to the
development of the KNGF-guidelines. The
development of the guidelines took place from July
1996 until December 1997.
Procedure of the mono disciplinary working group
The guidelines have been developed according to the
‘Methods for the Development and Implementation
of Clinical Guidelines’.1-5 This method includes
practical instruction of the strategies used to collect
literature. In the continuation of the review of
evidence in these guidelines the specific terms used
for the search, the sources used, the period in which
the literature was published, and the inclusion or
exclusion criteria for the literature are mentioned.
For a more extensive description of the different
literature searches is referred to the background
report : The physical therapeutic interventions in
patients with chronic obstructive pulmonary
diseases.3
The members of the working group have individually
selected and graded the proceedings attaining to the
scientific evidence. Even though the scientific
evidence is prepared by individuals or by smaller
subgroups, the result is laid out and discussed within
the whole working group. The scientific evidence is
then summarized in a conclusion, including the
Review of the evidence

12
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
extent of the evidence. Besides the scientific evidence
there are other important aspects for making the
recommendations such as: reaching a general
consensus, efficiency (costs), resource availability,
necessary expertise and education, organization
aspects and the attempt for agreement with other
mono or multi disciplinary guidelines.1-3 If there was
no scientific evidence available, the
recommendations were formulated based upon
consensus within the working group or secondary
group of professionals.
The recommendations are commented on by external
professionals. Once the mono disciplinary concept
guidelines were completed they were sent to external
professionals and/or occupational organizations
(secondary working group) to attain a general
consensus within the other occupational groups or
organizations and/or with other mono and multi
disciplinary guidelines. Also the wishes and
preferences of patients are taken into account by
representation of the Dutch Asthma Foundation.
Validation by the intended users
Before publication and distribution, the guidelines
are reviewed and systematically tested by the
intended users (validation). The concept of the KNGF-
guidelines COPD was sent to a group of 64 physical
therapists working in different working environments
to judge the guidelines. The comments and remarks
from the physical therapists are documented and
discussed in the working group and if possible or
desired included in the final guidelines.
The recommendations for the practice are the result
of the available evidence, the above mentioned other
aspects and the results of testing the guideline
amongst the intended users.
Constitution, products and implementation of the
guidelines
The guidelines exist of three parts: the practical
guideline, a schematic layout of the main points of
the guideline (summary) and the review of evidence
section. All parts of the KNGF-guidelines can be read
separately. After the publication and distribution of
the guidelines amongst members of the KNGF, an
article on the most important recommendations has
been published6 and a segment promoting
professionalism has been developed and published to
stimulate the use of the guidelines in daily practice.7
The guidelines are implemented according to a
standard of implementation strategies which are
described in the method.1-5,8
Nomenclature
Orie et al.9 firstly introduced the term chronic non-
specific lung disease (CNSLD) in the 1960s. Sluiter et
al.10 continued to use this umbrella term because
they believe there is a substantial overlap between the
disorders of asthma, chronic bronchitis and
emphysema, and furthermore that these conditions
have the same pathogenesis and pathophysiology.
They hold that the distinction made between these
disorders is neither very plausible nor meaningful. In
addition to using the term CNSLD, criteria that better
delineate the patient group must also be defined.10
Outside the Netherlands, however, the term CNSLD is
rarely used.11 Moreover, in recent years, there have
been increasing indications that there is a great
difference between the disorders of asthma and COPD.
Any confirmed distinction between asthma and COPD
would have a significant impact on therapy and
prognosis.12,13
Introduction to these guidelinesTarget group
Specific and demonstrable knowledge and skills are
required for adequately treating patients with COPD.
The necessary knowledge and skills can be obtained
by having extensive experience working with these
patients or through continuing education, which
should include learning about pathology, the
mechanics of breathing, general training principles,
measuring instruments, and the interpretation of
incremental exercise test results. The special
requirements placed on the treatment environment
and equipment used should also be covered. The
treatment area must be clean and well-ventilated.
There must also be an area where patients can rest for
short periods, change their clothing and wash. A
mouth pressure meter is required for testing and
training inspiratory muscle strength. Equipment for
exercise training includes a treadmill or cycle
ergometer, exercise apparatus, an exercise mat, and a
pulse oximeter.14 When treating patients with
impaired oxygen transport, equipment for oxygen
supplementation must be available. This equipment

could belong to the patients themselves.
Defining COPD
The American Thoracic Society uses the following
definitions.15 Chronic obstructive pulmonary disease
(COPD) is characterized by airflow obstruction due to
chronic bronchitis or emphysema. The, partially
reversible, obstruction tends to be progressive and
may be associated with airway hyper reactivity.
Chronic bronchitis is defined as the presence of a
chronic productive cough that lasts for at least three
months in each of two successive years. In making
this diagnosis, other causes of chronic coughs should
be excluded. Emphysema is present when there is
abnormal permanent enlargement of the lung
accompanied by destruction of alveolar walls,
without fibrosis.15
Pulmonary function tests can be useful in making a
diagnosis and in indicating the severity of the
disorder. The European Respiratory Society states that
measuring the forced expiratory volume in one
second (FEV1). provides an indication of the severity
of the disorder.16 The American Thoracic Society has
used FEV1 to indicate the different stages of COPD,17 as
shown in Table 14.
Although FEV1 is used to indicate the severity of
pulmonary disease, this measure has not been found
to be a good predictor of quality of life nor of the
disabilities experienced by patients. Various trials
have shown that there is only a weak relationship
between pulmonary function and health-related
quality of life in COPD patients.18–21 Williams et al.22
found a weak correlation between pulmonary
function and disabilities, and a strong correlation
between dyspnea and disabilities. Okubadejo et al.20
studied the correlation between FEV1 and the results
of using the St George’s Respiratory Questionnaire
(SGRO), the Sickness Impact Profile, and the Hospital
Anxiety and Depression Scale. Only the relationship
between activity on the SGRO and FEV1 was found to be
significant. In general, levels of anxiety and
depression were found to be better predictors of
quality of life than physiological parameters.
COPD mainly affects people in middle age. Common
symptoms are dyspnea with coughing, wheezing,
sputum production, and recurrent respiratory
infection.23 Compared to persons in a normal cross-
section of the population, COPD patients have more
disabilities in their daily live. A Dutch study of 50
COPD patients found that 46% were unable or only
partly able to hold a job or keep house because of
their condition. In addition, patients were
handicapped in carrying out physical activities
involving exertion.24 Problems with mobility, vitality
and sleep, and emotional problems such as
depression and anxiety were also experienced. Social
problems took the form of difficulties in performing
housework and leisure activities, and reduced social
interaction.19
Causes
The prevalence of coughing and sputum production
is higher in smokers,25 who also exhibit a greater
annual decline in FEV1.26–28 In addition, the mortality
rate due to copd is higher in smokers.29 Increased
smoking accelerates the decline in FEV1, whereas
ceasing smoking slows the decline in FEV1.30 A study
carried out by Kauffmann et al.30 showed that
occupational exposure to certain materials was
13
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
FEV1 (% of predicted value)
European Respiratory Society mild ≥ 70%
moderately severe 50–69%
severe 35–49%
American Thoracic Society phase 1 ≥ 50%
phase 2 35–49%
phase 3 < 35%
Table 14. Two classifications of COPD severity based on measurement of forced expiratory volume in one
second (FEV1).

related to decreased FEV1. Heederik at al.31 found
relationships between occupational exposure to
certain substances, such as smoke, dust and metals,
and respiratory symptoms and pulmonary function
disorders. In addition, there are several other factors
that may be associated with copd, such as air
pollution (both indoor and outdoor), passive
smoking, socioeconomic status, genetic factors,
respiratory infection, allergy, bronchial hyper
responsiveness, age and sex.32
Prognosis
In the medical literature, a connection is usually
made between prognosis and survival. The strongest
predictors of mortality are age and FEV1. The higher
the patient’s age and the lower his or her FEV1, the
worse the prognosis.33,34 After correcting for age and
FEV1, total lung capacity, heart rate at rest, and the
degree of physical limitations and disabilities
experienced all appear to correlate positively with
mortality. Exercise capacity appears to have a
negative correlation with mortality.33
Chronic mucus hyper secretion is related to a more
rapid decline in FEV1 and is a predictor of death from
respiratory infections in COPD patients.34 Weight loss
is also associated with a poorer prognosis.35
Postma et al.36 established that deterioration in FEV1 is
determined by the degree of bronchial hyper
responsiveness, the reversibility of bronchial
obstruction, and whether the patient ceases smoking.
The more severe the hyper responsiveness, the more
rapid the deterioration. The better the reversibility,
the slower the deterioration. Smoking cessation has a
positive effect on survival and on FEV1 decline over
time.
Epidemiology
The most extensive longitudinal cohort study on the
prevalention of COPD, in which no distinction was
made between asthma and COPD, was conducted
between 1965 and 1969 in the Netherlands: the
Vlagtwedde-Vlaardingen study.37 Another study, the
Zoetermeer Epidemiological Preventive Study was
carried out between 1976–1978.38 These trials found
that the prevalence of COPD in men varies from
13.0–16.8% and, in women, from 4.5–7.3%.
In the period 1985–1988, morbidity records were
maintained by Dutch primary care physicians at the
Nijmegen University Primary Practice Institute. These
showed that the incidence and prevalence of COPD is
higher in men than women and that both measures
increase with age in both sexes. In men, the
incidence increases from 0.2 per 1,000 in the 25–34
year age group to 24.4 per 1,000 in those aged 75
years and older; in women, from 0.4 per 1,000 in the
25–34 year age group to 4.2 per 1,000 in those aged
75 years and older. In men, the prevalence increases
from 6.6 per 1,000 in the 25–34 year age group to
233.9 per 1,000 in those aged 75 years and older; in
women, from 4.0 per 1,000 in the 25–34 year age
group to 43.9 per 1,000 in those 75 years and older.38
These figures probably give underestimates because
not all COPD patients are registered with their primary
care physician as having the condition.
Combining these figures from the Nijmegen
University Primary Practice Institute with the
demographic changes expected in coming years
indicates that an increase in the number of COPD
patients can be anticipated in the future, particularly
in the 45–64 year age group.38
Work absenteeism
The average duration of sick-leave in the Netherlands
is 22 days, when calculated from all cases of illness
notified to companies. The average illness durations
for patients with chronic bronchitis and emphysema
are 77 and 167 days, respectively.39
In 1985, the total number of sick-leave days due to
obstructive pulmonary disease comprised 1.18% of all
days lost because of diagnosed sickness in the
Netherlands, which was 612,100. Of those, 167,000
sick-leave days were due to chronic bronchitis and
61,100 to emphysema.39 These data only cover cases
of sick-leave known to company organizations and to
employers who, either jointly or as a group bear the
medical insurance risk on an ongoing basis.
Position of physical therapy
In the Netherlands, patients can be referred to
physical therapists by primary care physicians or
medical specialists. The Dutch College of General
Practitioners (NHG) recently revised its primary care
14
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

guidelines for the diagnosis and treatment of COPD
patients. With regard to physical therapy, these
guidelines only refer to the use of specialized
facilities. However, recent trials on the outcome of
physical therapy have found that it deserves a role in
the treatment of patients with asthma and COPD.40-42
Only 1.7% of all physical therapy work carried out in
the primary care sector involves patients with
breathing problems.43 This is also consistent with
data on the referral policies of primary care
physicians: 89.0% of COPD patients are not referred to
other practitioners by primary care physicians, 9.0%
are referred to specialists, and only 1.8% are referred
to physical therapists.44 Possible reasons for the small
number of physical therapy referrals are that primary
care physicians may be relatively unfamiliar with the
forms of diagnosis and treatment that physical
therapists can provide for COPD patients, and that
primary care physicians may judge the severity of
obstructive pulmonary disease solely on the basis of
pulmonary function.45 This may occur despite the
fact that pulmonary function is a poor predictor of
quality of life and is a poor indicator of the quality of
life, perceives disabilities or exercise capacity,46 and of
the level of dyspnea. Having a physical therapy
consultation before referral is considered could
provide a way of clarifying the need for physical
therapy. The introduction of a consultative physical
therapy examination is one way of improving the
efficiency of care.47 The primary care physician’s
requirements from consultation can better be
satisfied by a physical therapist who has extensive
experience or who is well-trained, or both.47 In
addition, the present guidelines can also contribute
to increasing understanding of how physical therapy
can be used, thereby leading to more specific referrals
and to more knowledge of the possibilities of physical
therapy treatment .
In 1991, a study carried out at the secondary care
level in the Netherlands found that 3% of the total
number of COPD inpatients in a general hospital were
receiving treatment from physical therapists.48 No
data are available on the intervention the physical
therapists used with these patients in either primary
or secondary care, nor on the severity of the disorders
or the patients’ needs.
Pathophysiology
Bronchial obstruction is the core complaint in
patients with COPD. It can be caused by swelling of the
mucosa, the accumulation of mucus, loss of elasticity
of the lung parenchyma, or bronchospasm. These
phenomena can occur in various combinations.
Severity of bronchial obstruction
Bronchial obstruction can be quantified by measuring
dynamic pulmonary function parameters. In
particular, the maximum forced expiratory volume in
one second (FEV1) is useful. In its more severe form,
COPD may be associated with hyperinflation. In this
situation, the thorax is in a position characteristic of
inspiration when the patient is at rest. Hyperinflation
can result in a thoracic breathing pattern and an
increased load on respiratory muscles. Some clinical
observations related to the severity of obstruction are:
contraction of the scalene muscles, tracheal tug (i.e.,
downward movement of the trachea during
inspiration), and Hoover’s sign (i.e., inward
movement of the costal wall of the lower ribs during
inspiration). There are significant correlations
between these symptoms and FEV1.41 Inter-assessor
reliability is fair for observations of intercostal
retraction of the intercostal spaces, tracheal tug on
inspiration, and Hoover’s sign (Kappa minimum =
0.50, p < 0.0001 for all three symptoms).49
The typical problems affecting COPD patients that also
influence physical therapy are discussed sequentially
below.
Impaired mucus clearance
Mucus retention is very common in patients with
COPD. It can cause bronchial obstruction. In turn,
mucus retention can be caused by increased mucus
secretion or by impaired mucus transport.
Richardson and Peatfield.50 give an overview of
mechanisms that can increase mucus secretion . The
inhalation of dust or cigarette smoke increases mucus
secretion, and inhaling antigens that stimulate
inflammatory processes increases mucus production.
Impaired mucus transport may be the result of
reduced mucociliary clearance or reduced expiratory
airflow. Research carried out by Goodman et al.51
shows that smoking can result in inactive cilia.
15
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

16
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Recurrent infection can lead to a loss of ciliated
epithelium.52 The contribution airflow makes to
mucus transport depends on expiratory airflow
velocity, which is determined by the magnitude of
the airflow and bronchial tube diameter.53 Effective
mucus transport occurs at high airflow velocities. To
achieve this, airflow must be large and the total
airway cross-section must be small.
Peripheral airway obstruction restricts airflow in the
peripheral airways. In turn, reduced airflow in the
peripheral airways slows airflow in the central
respiratory tracts. This process could diminish the
efficacy of mucus transport caused by expiratory
airflow.
Mucus retention can cause pathological changes in
the lungs54, possibly because of recurrent respiratory
infection. It can even contribute to the progression of
pulmonary disease.55 The presence of hypersecretion
is a risk factor for death from COPD. Hypersecretion
leads to a greater annual decline in FEV134 and is a risk
factor for hospitalization due to COPD.56 Physical
therapy can help patients use external effort to
improve mucus transport to the greatest extent
possible and several interventions are available for
doing this (see the discussion below on therapy for
improving mucus clearance).
Reduced exercise capacity
During exercise, muscle metabolism increases
resulting in more muscle oxygen consumption and
increased carbon dioxide production. Therefore,
during exercise, additional oxygen must be
transported and additional carbon dioxide must be
removed. Folgering and van Herwaarden57 designate
four types of problems that can cause decreased
exercise capacity:
1. cardiocirculatory limitations;
2. ventilatory limitations;
3. oxygen transport limitations; and
4. psychogenic limitations.
These different types of limitation can be
distinguished with the aid of an incremental exercise
test carried out at maximum load, during which
blood gas levels are also measured.
1. Cardiocirculatory limitations
In patients with mild forms of bronchial obstruction
(i.e., FEV1 > 60% of that predicted), reduced exercise
capacity may be caused by cardiocirculatory
limitations.58 In these individuals, the circulation
cannot transport an adequate amount of oxygen to
the muscles. Because of a lack of oxygen, muscles
switch to anaerobic metabolism, which involves the
production of lactic acid.58 Cardiocirculatory
limitations are demonstrated by the age-related
reduction in maximum heart rate (i.e., 220 beats/min
minus age in years) and by a blood lactate level of
approximately 10 mmol/l.57 Endurance training can
contribute to improving exercise capacity.
2. Ventilatory limitations
In patients with moderate to severe forms of
obstruction (i.e., FEV1 < 60% of that predicted), the
respiratory pump may be overloaded by
hyperinflation, dynamic collapse, or other factors.
The presence of ventilatory limitations is indicated by
increased arterial carbon dioxide pressure (PaCO2)
during the incremental exercise test.
Ventilatory limitations can be seen as being due to an
imbalance between the load on and the load-bearing
capacity of the respiratory muscles. Respiratory
muscle load is increased by increased airways
resistance and decreased compliance of the lungs and
chest wall. At the same time, the strength (i.e., the
load-bearing capacity) of the respiratory muscles may
be impaired by hypoxemia,59 hypercapnia,60 cardiac
decompensation,(61) oral corticosteroid use,63 or
malnutrition.62,64
By measuring maximum inspiratory pressure at the
mouth (PImax), the physical therapist can obtain a
reliable indication of the strength of the inspiratory
muscles.65 The clinical signs of fatigued, or heavily
loaded, respiratory muscles are an elevated respiratory
rate and, at a later stage, abdominal paradox and
respiratory alternans.66 (Abdominal paradox is
inward movement of the abdominal wall during
inspiration and respiratory alternans is alternation
between a thoracic and abdominal breathing
pattern.) Respiratory muscle fatigue can cause
respiratory failure, resulting in the development of
hypoxemia and hypercapnia. In patients with

ventilatory limitations, the maximum voluntary
ventilation threshold can be surpassed at a certain
exercise level. However, ventilation can be increased
by increasing the tidal volume and by a relative
lengthening of the expiration time. To achieve this,
the respiratory muscles, including accessory
respiratory muscles, must work harder.
Ventilatory capacity can be increased by targeted
training of the respiratory muscles. Respiratory
muscle function can be improved by increasing the
strength or endurance, or both, of the respiratory
muscles.
3. Oxygen transport limitations
In patients with oxygen transport limitations, the
alveolar capillary membrane surface area is reduced.
This causes problems with oxygen diffusion and
contact time.67 In these patients, arterial oxygen
tension (PaO2) drops during submaximal exercise.
This can only be detected using an incremental
exercise test at the patient’s maximum exercise rate.
This group of patients must learn to use their bodies
more efficiently. Breathing exercises aimed at
lowering the respiratory rate can reduce the dead
space. Furthermore, supplemental oxygen may be
necessary to improve the patient’s exercise capacity
(68–70). Training with oxygen supplementation
improves the condition of the peripheral muscles
because the number of capillaries increases and there
are more and larger mitochondria, thereby enabling
better oxygen extraction to take place. Therefore,
better use is made of the limited amount of oxygen
present.57
4. Psychogenic limitations
If a patient stops the exercise test without having
encountered one the above limitations, it can be
assumed that the reasons for stopping are
psychogenic, for example, anxiety or exercise phobia.
In all patients with psychogenic limitations, physical
therapy can help reduce the symptoms that limit
exercise. In the clinical guidelines above, these
limitations are dealt with under the category of other
factors.
Recently, a fifth type of problem that can result in
reduced exercise capacity has been described, namely:
5. Peripheral muscle weakness
If the leg muscles become rapidly fatigued, the COPD
patient’s exercise capacity will be limited.71 Recent
research by Maltais et al.72 confirms this view. The
researchers showed that patients with COPD have
reduced aerobic capacity, with the result that lactic
acid is produced at an earlier stage during exercise.
Gosselink et al.73 concluded that pulmonary function
and peripheral muscle strength are important
determinants of exercise capacity in COPD patients.
Possible causes of general muscle weakness are cardiac
decompensation,74 corticosteroid use,63 and an
impaired nutritional stage.62,64,75
Patients with peripheral muscle weakness commonly
score very high on the Borg scale for ‘heaviness’ (i.e.,
leg fatigue). during maximum exercise. In order to
confirm that muscle weakness is the reason for
stopping exercise, additional examinations should be
performed, such as testing quadriceps muscle
strength. If the peripheral muscular strength is, at
least partly, responsible for reduced exercise capacity,
then peripheral muscle training will have to be part
of physical therapy. If hypoxemia, steroid therapy or
malnutrition contribute to reduced muscle strength,
these factors should be minimized or eliminated as
far as possible. In this regard, it should be noted that
consultation with the practitioners of other
disciplines is essential for optimal treatment.
Dyspnea
Dyspnea is the unpleasant subjective sensation of
needing to breathe, which may be due to various
mechanisms:
• Central respiratory center activity is closely
associated with sensations of dyspnea.76 The
respiratory center can be activated by changes in
blood gas concentrations, such as an increase in
arterial carbon dioxide tension (hypercapnia) or a
decrease in arterial oxygen tension (hypoxemia).
• In “length-tension inappropriateness”, patients
experience respiration as being mechanically
insufficient.77 In the body, the relationship
between the actual change in respiratory muscle
length and muscle strength is constantly being
evaluated in terms of expected changes in length.
17
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

If the length change is smaller than expected, the
person experiences dyspnea. This mechanism is
especially important when an extra demand is
placed on the respiratory apparatus.
• Psychosocial factors: emotional and situational
factors can also be associated with the sensation
of dyspnea.78
Fatigue, respiratory muscle weakness, and the fact
that the minute ventilation in COPD patients is high
all contribute to sensations of breathlessness. When
the minute ventilation is high, every increase in the
ventilation rate is a relatively large increase, which
leads to a proportionally large increase in dyspnea.79
Dyspnea seems to be affected more by repetitive
movements of the upper extremities.80 This may be
explained by the fact that these movements reduce
the ability of the upper chest muscles to contribute to
respiration. Unilateral arm movements involve less
load for the patient than bilateral movements.
Malnutrition
An underweight condition (i.e., a weight under 90%
of the ideal weight) is common in patients with
COPD.35,75,82 Its prevalence increases as the degree of
bronchial obstruction increases.35,75 The muscular
strength of respiratory and skeletal muscles is less in
patients who are underweight than in those with a
normal weight.62,83 Gray-Donald et al.64 reported
that patients who are underweight have a lower
maximum exercise capacity but that the condition
has no impact on submaximal exercise capacity or
dyspnea. In patients with COPD, fat-free body mass is a
better indicator of respiratory and skeletal muscle
strength than body weight82,84 and is a significant
determinant of exercise tolerance.75 A reduction in
fat-free body mass is associated with lower values for
respiratory and peripheral muscular strength.82 In
one group of randomly selected COPD patients (mean
FEV1, 53%), 14% were found to have reduced fat-free
body mass and reduced body weight, and 7% were
found to have only one of the two.82 Here again,
there is a need for communication between the
practitioners of different disciplines because
nutritional interventions in underweight patients can
increase respiratory and peripheral muscle
strength85,86 and improve exercise capacity.86
Diagnosis
The methodical provision of physical therapy is based
on a problem-solving approach.87 Several stages can
be distinguished in this process. The starting point is
referral by a primary care physician or medical
specialist and the patient’s reasons for seeking
medical care. The next stage is history-taking, which
is followed by an examination of the patient and
drawing conclusions, or making a physical therapy
diagnosis. In assessing the patient’s needs, the
physical therapist must determine whether physical
therapy would be helpful. If so, the therapist draws
up a treatment plan, which is periodically evaluated
during the course of treatment and after treatment
ends. The last stage is concluding treatment and
reporting back to the referring physician.88,89
Referral
The physical therapist must have all the relevant
medical and psychosocial data before the patient is
examined and, if necessary, treated. These data guide
the therapeutic approach and help the physical
therapist analyze the patient’s health problems,
interpret the examination results, and formulate
realistic and attainable treatment goals. An
understanding of the severity of the condition and its
prognosis is important for making an accurate
assessment of the results of physical therapy.
Relevant medical data includes data from pulmonary
function tests and, if the physical therapist wants to
improve the patient’s exercise capacity, an
incremental exercise test at the patient’s maximum
exercise rate. According to Cambach et al.45 certain
patients should be treated in special COPD facilities:
those whose arterial oxygen tension (PaO2) is lower
than 8.6 kPa (65 mmHg) and those whose arterial
carbon dioxide tension (PaCO2) is higher than 6.0
kPa (45 mmHg). at rest or during exercise.
History-taking
Details of the information sought and the questions
asked during history-taking are presented in Table 15.
18
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

19
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Noting the patient’s symptoms and current condition:
• reasons for referral; medical referral data (nature of obstruction: chronic bronchitis or emphysema);
• patient’s needs. How does the patient experience the consequences of COPD? What are the patient’s
expectations of treatment (physical therapy)?
• social data (family composition, occupation, family history);
• effects of the condition on emotional functioning;
• Which medications is the patient using and is he or she knowledgeable about their use?
Are there any signs of impaired mucus clearance?
• Does the patient cough? If so, is coughing productive and effective?
• Is there increased sputum secretion? If so, how much? What is the color and consistency of the sputum?
• Is there a relationship between sputum production and body posture, activity or medication use?
• Is the patient familiar with mobilization and expectoration techniques?
• Does mucus retention have any negative effects (e.g., exacerbations, recurrent infection, or fatigue)?
Are there any indications of reduced exercise capacity due to COPD?
• What is the patient’s current level of activity and has it changed as a result of the disorder?
• What is the reason for and the extent of any reduction in exercise capacity?
• Does dyspnea occur? If so, when?
Quality of life questionnaire note 1
Are there any other symptoms?
• hypoxia, hypoxemia, insomnia, morning headaches, or difficulty concentrating?
• Are there any complaints associated with respiratory movement (e.g., restricted movement, pain or
stiffness)?
• Is there any pain associated with deep breathing or coughing?
• Is there cardiac decompensation?
Recording the natural course of the symptoms and condition:
• brief summary of the onset and course of symptoms;
• notes on therapy, medication, primary care physician or specialist, hospitalization, physical therapy, and
other therapies. What were the effects of each type of therapy?
Noting the patient’s load and load-bearing capacity, the causes of symptoms, and any factors that have
influenced or are influencing symptom development:
Evaluating load-bearing capacity:
• Have any traumas occurred or operations taken place?
• Are there any other disorders (e.g., of the locomoter tract or any other tracts)?
• Has body weight decreased despite normal food consumption?
• What is the quality of the patient’s sleep (e.g., problems with falling asleep or staying asleep)?
Evaluating load:
• What demands does the patient’s environment make on him or her?
• What is the patient’s level of activity, including general activities, work and hobbies?
• Are there any aggravating factors (e.g., smoking, hyperreactivity, emotional or behavioral factors, or
factors in the work environment)?
• Which factors reduce symptoms (e.g., resting, specific environmental conditions, or medication use)?
What is the patient’s need for information? note 2
Table 15. Details of history-taking in patients with COPD. The raised figures are references to individual notes in
the appended notes on diagnosis.

Physical examination
The physical examination usually comprises
observation and palpation, since these two processes
often occur at the same time. Palpation is used to
verify the information obtained by observation. The
physical examination is divided into two parts in
order to investigate two specific problems in patients
with COPD. Table 16 describes the details of the
physical examination in patients with impaired
mucus clearance and Table 17 describes the physical
examination in those with impaired exercise capacity.
Analysis
During analysis, the patient’s health problem is
analyzed using referral data and data obtained from
the physical therapy examination. The physical
therapist should be able to determine whether
physical therapy is indicated, or whether the patient
should be referred for consultation elsewhere.
Physical therapy is indicated for patients who,
because of COPD, have impaired mucus clearance,
whose normal daily life activities are limited by
dyspnea, or who have impaired exercise capacity. The
patient should be motivated to undergo treatment
because very active participation is required to
achieve good results. After the completion of
treatment, the patient must be proactive so that the
benefits can be maintained.
Patients can be treated according to these guidelines
if their medication has previously been optimized81
and if the referral data is sufficient. If there are
indications that a patient’s medication is not optimal,
he or she should be referred back to the physician. If
a patient is suffering from disabilities due to reduced
exercise capacity, referral documentation should, if it
is complete, include data from an incremental
exercise test at the patient’s maximum exercise load.
These data are essential for determining the patient’s
exercise limitations so that the appropriate exercise
load can be used and so that the therapist can be sure
there are no contraindications. If the patient does not
satisfy the requirements for participating in exercise
training, the referring physician should be consulted.
Analysis: impaired mucus clearance
Patients with impaired mucus clearance may have
one or more impairments, such as bronchial
obstruction resulting from mucus retention or
airways collapse, or a disorder in mucus transport,
production, composition or clearance.
Systemic factors that can cause or contribute to
impaired mucus clearance include medication use,
malnutrition and other problems such as heart
ailments. These may necessitate consultation with or
treatment by another specialist.
Local factors that can cause or contribute to impaired
mucus clearance must also be taken into
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
20 51.1001.01.02
Observation:
• evaluation of coughing and huffing techniques. Can the patient cough effectively? Is there pain during
coughing? note 3
• Are there deformities of the thorax (e.g., pectus excavatum, pectus carinatum, or kyphoscoliosis)? note 4
• Is the shape of the abdominal wall abnormal (e.g., due to weakened abdominal musculature)?3
• auscultation and palpation of thoracic wall; note 5
• listening to breath sounds; note 5
• Does airways collapse occur? note 3
• assessing the quantity, consistency and appearance of mucus.
Movement testing:
• How well does the abdominal musculature function (i.e., strength and endurance)? note 3
Other measurements:
• peak expiratory flow. note 6
Table 16. Details of the physical examination in patients with impaired mucus clearance. The raised figures are
references to individual notes in the appended notes on diagnosis.
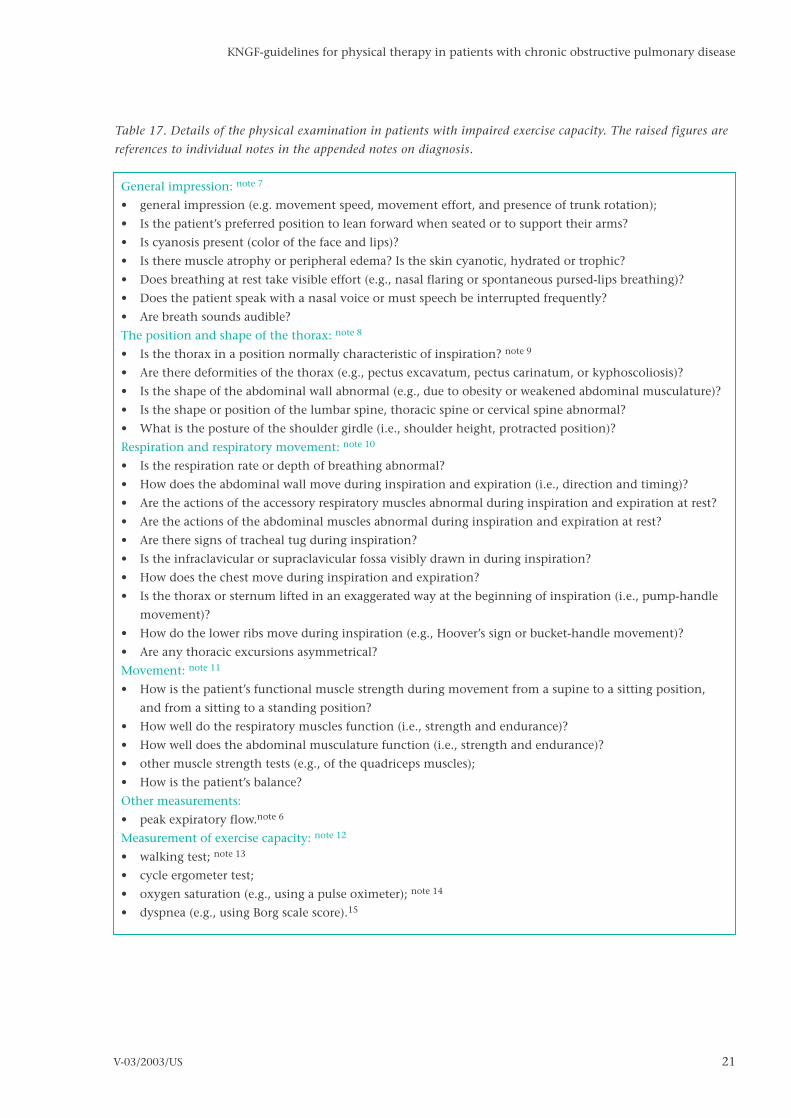
21
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
General impression: note 7
• general impression (e.g. movement speed, movement effort, and presence of trunk rotation);
• Is the patient’s preferred position to lean forward when seated or to support their arms?
• Is cyanosis present (color of the face and lips)?
• Is there muscle atrophy or peripheral edema? Is the skin cyanotic, hydrated or trophic?
• Does breathing at rest take visible effort (e.g., nasal flaring or spontaneous pursed-lips breathing)?
• Does the patient speak with a nasal voice or must speech be interrupted frequently?
• Are breath sounds audible?
The position and shape of the thorax: note 8
• Is the thorax in a position normally characteristic of inspiration? note 9
• Are there deformities of the thorax (e.g., pectus excavatum, pectus carinatum, or kyphoscoliosis)?
• Is the shape of the abdominal wall abnormal (e.g., due to obesity or weakened abdominal musculature)?
• Is the shape or position of the lumbar spine, thoracic spine or cervical spine abnormal?
• What is the posture of the shoulder girdle (i.e., shoulder height, protracted position)?
Respiration and respiratory movement: note 10
• Is the respiration rate or depth of breathing abnormal?
• How does the abdominal wall move during inspiration and expiration (i.e., direction and timing)?
• Are the actions of the accessory respiratory muscles abnormal during inspiration and expiration at rest?
• Are the actions of the abdominal muscles abnormal during inspiration and expiration at rest?
• Are there signs of tracheal tug during inspiration?
• Is the infraclavicular or supraclavicular fossa visibly drawn in during inspiration?
• How does the chest move during inspiration and expiration?
• Is the thorax or sternum lifted in an exaggerated way at the beginning of inspiration (i.e., pump-handle
movement)?
• How do the lower ribs move during inspiration (e.g., Hoover’s sign or bucket-handle movement)?
• Are any thoracic excursions asymmetrical?
Movement: note 11
• How is the patient’s functional muscle strength during movement from a supine to a sitting position,
and from a sitting to a standing position?
• How well do the respiratory muscles function (i.e., strength and endurance)?
• How well does the abdominal musculature function (i.e., strength and endurance)?
• other muscle strength tests (e.g., of the quadriceps muscles);
• How is the patient’s balance?
Other measurements:
• peak expiratory flow.note 6
Measurement of exercise capacity: note 12
• walking test; note 13
• cycle ergometer test;
• oxygen saturation (e.g., using a pulse oximeter); note 14
• dyspnea (e.g., using Borg scale score).15
Table 17. Details of the physical examination in patients with impaired exercise capacity. The raised figures are
references to individual notes in the appended notes on diagnosis.

consideration when drawing up a treatment plan and
evaluating treatment. Examples of such factors are
increased mucus viscosity, pulmonary function
limitations, bronchial obstruction, and poor
functioning of respiratory muscles, including the
abdominal muscles. For instance, patients with
purulent sputum may need to be treated more
frequently. Measuring mucus viscosity helps in
assessing how difficult it is for patients to cough up
sputum.
Analysis: impaired exercise capacity
Patients with impaired exercise capacity may be
affected by reduced general physical stamina, or by
respiratory muscle function or gas exchange
disorders, and by feelings of dyspnea. These patients
may also experience disabilities in their mobility and
on their ability to carry out personal hygiene,
housework, occupational, educational or leisure
activities, among other things.
Systemic factors that can cause or contribute to
impaired exercise capacity include medication use,
malnutrition, the presence of other complaints, and a
reduced activity level. These may necessitate
consultation with or treatment by another specialist.
Local factors that can cause or contribute to impaired
exercise capacity include pulmonary function
limitations, oxygen transport disorders, and poor
respiratory muscle function.
Treatment plan
After analysis, a treatment plan can be drawn up for
the individual patient. Treatment plans are tools for
structuring, monitoring and evaluating treatment.
The treatment plan records treatment goals, the
procedures to be used in treatment, the treatment
strategy, and the patient’s and physical therapist’s
individual responsibilities.
The treatment plan can be divided into two phases.
The aim of the first phase is to minimize or eliminate
impairments in the musculoskeletal system. For
patients with COPD, this means that the load on the
muscles controlling breathing should be reduced as
much as possible by reducing airway obstruction (i.e.,
by improving mucus clearance) and by reducing the
patient’s habitual expansion of the thorax as much as
possible from a position that is characteristic of
inspiration. Airway collapse must be prevented as far
as possible. In the second phase, the aim is to
normalize respiratory movement. For patients with
COPD, this involves adjusting respiratory movement
by optimizing the contribution of the respiratory
system’s compensatory mechanisms.
In both phases, the patient’s load-bearing capacity
can be increased. Increasing specific load-bearing
capacity partly involves improving the strength and
endurance of respiratory muscles. Increasing general
load-bearing capacity involves improving physical
stamina. The results of the physical therapy
diagnostic process determine the different emphases
in treatment.
Therapy
The therapeutic approach adopted is, in part, based
on systematic reviews of the scientific literature. The
literature considered for these reviews was collected
from the MEDLINE database and from databases of
the Dutch Institute of Allied Health Professions (NPi),
including a physical therapy index, a rehabilitation
index and an occupational therapy index. The
collected items were supplemented by scrutinizing
reference lists and by receiving additional material
from members of the steering group. Studies were
only included if they involved randomized clinical
trials on (a) the effects of physical therapy on mucus
clearance, (b) the effects of exercise training as part of
pulmonary rehabilitation in patients with COPD, or (c)
the effects of inspiratory muscle training in patients
with COPD. Each trial was evaluated on its
methodological quality by two independent reviewers
using 10 predefined criteria.90,91 These criteria were
based on generally accepted principles of scientific
research.92–94 As no more than one point was
awarded for each criterion, the highest possible score
for any trial was 10. A trial was considered to be of a
sufficiently high quality methodologically if it scored
more than five points. The conclusions drawn about
therapy are based on such high-quality trials.
Improving mucus clearance
Physical therapy employs a variety of methods for
improving mucus clearance. The following
22
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
techniques will be described sequentially: coughing
or forced expiration; postural drainage; exercise; chest
percussion and mechanical vibration; positive
expiratory pressure; the Flutter device; and autogenic
drainage. A systematic review of the efficacy of these
procedures was carried out. Inclusion criteria were:
• a randomized clinical trial was involved;
• the results concerned only one group of COPD or
cystic fibrosis patients;
• the patients underwent a physical therapy
intervention aimed at improving mucus clearance;
and
• the study outcome measures were relevant to
mucus clearance.
Coughing or forced expiration
Mechanism of action
The expiratory airflow rate is high during coughing
and forced expiration, thereby assisting mucus
transport from peripheral to central airways.53,95
Initially during coughing, high intrapulmonary
pressure is built up when the glottis is closed;
thereafter, the expiratory airflow is high when the
glottis opens. Huffing, in contrast, involves forced
expiratory airflow with an open glottis, which means
that the intrapulmonary pressure is much lower.96 If
the expiratory airflow is to be sufficient for
transporting mucus, a high flow velocity of, at least, 1
m/s (greater than 2.5 m/s is better) is needed.53
Furthermore, the thickness of the mucus layer is also
important. Coughing and huffing are more effective
when the mucus layer is thick.53
During forced expiration and coughing, dynamic
compression of the airways takes place. Dynamic
compression contributes to the development of very
high local airflow velocities in the respiratory tract.
The exact location at which the dynamic
compression caused by expiratory forces takes place
(i.e., the equal pressure point). is dependent on lung
elasticity (or lung volume), bronchial obstruction,
and bronchial stability.97
Mucus transport can be facilitated by varying the
expiratory force and equal pressure point. If there are
signs of airway collapse, however, dynamic
compression must be avoided. By using less force and
starting from a greater lung volume, compression
occurs more centrally and collapse can be, at least
partially, prevented. The advantage of forced
expiration over coughing is that the lung volume and
force can be better controlled.
Evidence supporting mucus clearance by coughing
Multiple controlled trials have shown that coughing
improves mucus transport and, thereby, mucus
clearance.98–100 The study by van der Schans et al.100
found a difference between chronic bronchitis
patients, in whom coughing was effective, and
emphysema patients, in whom the efficacy of
coughing could not be proven. It was suggested that
coughing may be less effective if lung elasticity is
compromised.
The literature also revealed that coughing is more
effective than postural drainage,98,99 but that physical
therapy (described as the combination of breathing
exercises, chest percussion, vibration, and postural
drainage) does not appear to provide any additional
benefits to coughing alone.99
Evidence supporting mucus clearance by forced
expiration (including postural drainage)
Van der Schans et al.100 report that forced expiration
techniques have positive effects in patients with
chronic bronchitis but not in those with emphysema.
The reason could be, as noted above, that forced
expiration may be less effective when the elasticity of
the lungs is compromised. When used in
combination with postural drainage, forced
expiration is effective in clearing mucus.101–103
However, it is not possible to compare the efficacy of
forced expiration techniques with that of other
procedures on the basis of evidence from the
scientific literature because the forms of the different
interventions used were highly variable as were the
types of intervention being compared.104,105
Postural drainage
Mechanism of action
In healthy individuals, the effect of gravity on mucus
clearance is negligible. This changes, however, when
there are alterations in viscoelastic properties, ciliated
epithelium function, the quantity of mucus, and the
thickness of the periciliary layer.106
23
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

Postural drainage techniques use gravity to promote
mucus transport. In practice, a particular posture is
held for a minimum of 20 minutes, with the relevant
bronchus being held vertically. It is essential that the
location of the mucus is appropriate for the posture
being held. Nine specific postures for draining the
large bronchi have been reported.107
Evidence
The efficacy of postural drainage has not been
unequivocally substantiated by literature findings.
Rossman et al.99 reported positive results in patients
with cystic fibrosis, whereas Oldenburg et al.98
showed negative results in patients with bronchitis.
The effects of postural drainage have been reported to
be inconsistent when it is used in combination with
other procedures.108,109
Exercise
Mechanism of action
Exercise increases expiratory flow velocity, the
respiratory minute volume, and sympathetic nervous
system activity. These mechanisms increase the
ciliary beat frequency, reduce mucus viscosity and,
thus, increase mucus transport.110
Evidence
The only explanatory study on the efficacy of exercise
that was of sufficiently high methodological quality
showed positive results. Exercise was found to
increase bronchial mucus transport.98 The authors of
that study also demonstrated that coughing brings
about better mucus clearance than exercise. In a
pragmatic study, no differences were found when
treatment involving exercise plus forced expiration
was compared with other interventions.108
Chest percussion and vibration
Mechanism of action
The physical vibration caused by chest percussion or
a mechanical vibrator is transferred to lung tissue and
to the respiratory tract. Mucus is loosened by the
vibration and cilia activity is stimulated. The mucus
composition may also by changed by vibration.111,112
In their reviews, Hansen et al.113 and Thomas et al.114
summarized the mechanisms of action of percussion
and vibration. The resulting motion can reduce
mucus viscosity, stimulate coughing, or, by a
resonance effect, reinforce ciliary movement.112 In
addition, Thomas et al.114 noted improvements in
ciliary function and changed mucus composition. A
percussion frequency of 25–35 Hz is optimal for
mucus transport, but is not achievable manually.115
After reviewing the literature, Thomas et al.114
concluded that the optimal frequency of vibration for
improving mucociliary clearance had not been clearly
defined but that it is under 60 Hz.
Evidence supporting mucus clearance by percussion
The evidence that percussion improves mucus
clearance is limited. The literature review did not
contain any explanatory studies of sufficiently high
methodological quality that proved percussion was
effective. Therefore, it is not possible to say whether
percussion is more effective than giving no
treatment. However, it appears that percussion given
in addition to postural drainage offers no benefits
over postural drainage alone99 nor over physical
therapy alone (defined as postural drainage plus
coughing).116
Evidence supporting mucus clearance by vibration
The only explanatory study on the efficacy of
vibration that was of sufficiently high
methodological quality gave negative results. No
difference was demonstrated between periods in
which vibration was applied and control periods.117
Positive expiratory pressure
Mechanism of action
Before mucus can be cleared from the small airways
by coughing or forced expiration, it must be moved
to a more central part of the respiratory tract. This
can be accomplished by using a positive expiratory
pressure mask or mouthpiece to give an expiratory
pressure of 10–20 cmH2O (centimeters of water).
Increasing the functional residual capacity of the
lung enables the airways to remain open during
expiration.118 Applying positive expiratory pressure
raises the pressure gradient between open and closed
alveoli, which reduces resistance in collateral and
small airways.119,120 This process encourages
collateral ventilation, enabling air to collect distally
behind the mucus. Mucus is then moved to the
central respiratory tract.
24
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

Evidence
The application of positive expiratory pressure
increases the functional residual capacity of the lung,
but this has no effect on mucus clearance. The
efficacy of positive expiratory pressure used alone
cannot be demonstrated.121 Several trials have shown
that positive expiratory pressure used in combination
with forced expiration, or coughing or huffing, does
lead to improved mucus clearance.102–104 However,
these trials do not indicate the magnitude of the
contribution of positive expiratory pressure. Because
of variability in the nature of the interventions used
and in the types of interventions being compared in
different studies, it is not possible to say how effective
positive expiratory pressure is in comparison to other
types of therapy, whether used alone or in
combination.105,108,109
Flutter device
Mechanism of action
The Flutter device uses a combination of positive
expiratory pressure and vibration or oscillation
applied through the mouth. An expiratory pressure of
5–35 cmH2O is achieved by asking the patient to hold
a small ball in the air by blowing. The movement of
the ball causes an oscillatory movement at a
frequency of 8–26 Hz.122 In this form of treatment,
respiratory tract dilatation caused by increased
expiratory pressure and airway vibration are thought
to improve mucus transport.52
Evidence
The literature review found two trials that examined
the effects of the Flutter device used in addition to or
instead of physical therapy.123,124 Both trials are of
low methodological quality and, furthermore, show
inconsistent results. The efficacy of the Flutter device
cannot, therefore, be substantiated.
Autogenic drainage
Mechanism of action
Autogenic drainage is a method in which patients
learn how to promote mucus drainage by themselves.
Controlled breathing techniques in which the
frequency and depth of breathing are varied are used
to achieve the highest possible airflow at different
levels of bronchial tree. In other words, a balance is
sought between expiratory flow, intrabronchial
pressure and bronchial wall stability. The hypothesis
is that mucus is mobilized when the patient breathes
at a low expiratory flow rate with the lung volume
lying between the functional residual capacity and
the residual volume. Thereafter, mucus is transported
to larger airways by the increase in the tidal volume.
Finally, mucus is expectorated by forced expiration,
starting with a low lung volume.125
Evidence
Miller et al.126 found no difference in mucus
expectoration between patients who used autogenic
drainage and those who used physical therapy (i.e.,
an active cycle of breathing techniques). However,
mucus clearance starts more quickly with autogenic
drainage.
Effect of physical exercise as part of pulmonary
rehabilitation
A total of 18 trials on the efficacy of physical exercise
as part of pulmonary rehabilitation in patients with
COPD were reviewed. Eleven trials were of sufficiently
high methodological quality. Physical exercise was
found to have a positive effect on stamina and
quality of life in COPD patients. The effects of exercise
on walking distance, maximum and submaximal
exercise capacity, and quality of life are described
sequentially below.
Seven trials studied the effect of exercise as part of
pulmonary rehabilitation on walking distance127–133
and on maximum exercise capacity.127–129,132,134–136
Five of the seven found a positive effect on walking
distance127–131 and four found a positive effect on
maximum exercise capacity.127,129,134,135
Exercise used as part of pulmonary rehabilitation has
also been shown to have a positive effect on
submaximal exercise capacity.130–134,137 However,
Reid and Warren136 and Busch and McClements135
failed to demonstrate any significant effect on
submaximal exercise endurance. In addition,
improvements in exercise capacity, or maximum
exercise capacity, appeared to occur in patients with
severe forms of COPD (i.e., with an FEV1 of between
35–49% of that predicted).129–131,135,136,138
In addition to improving exercise tolerance,
25
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
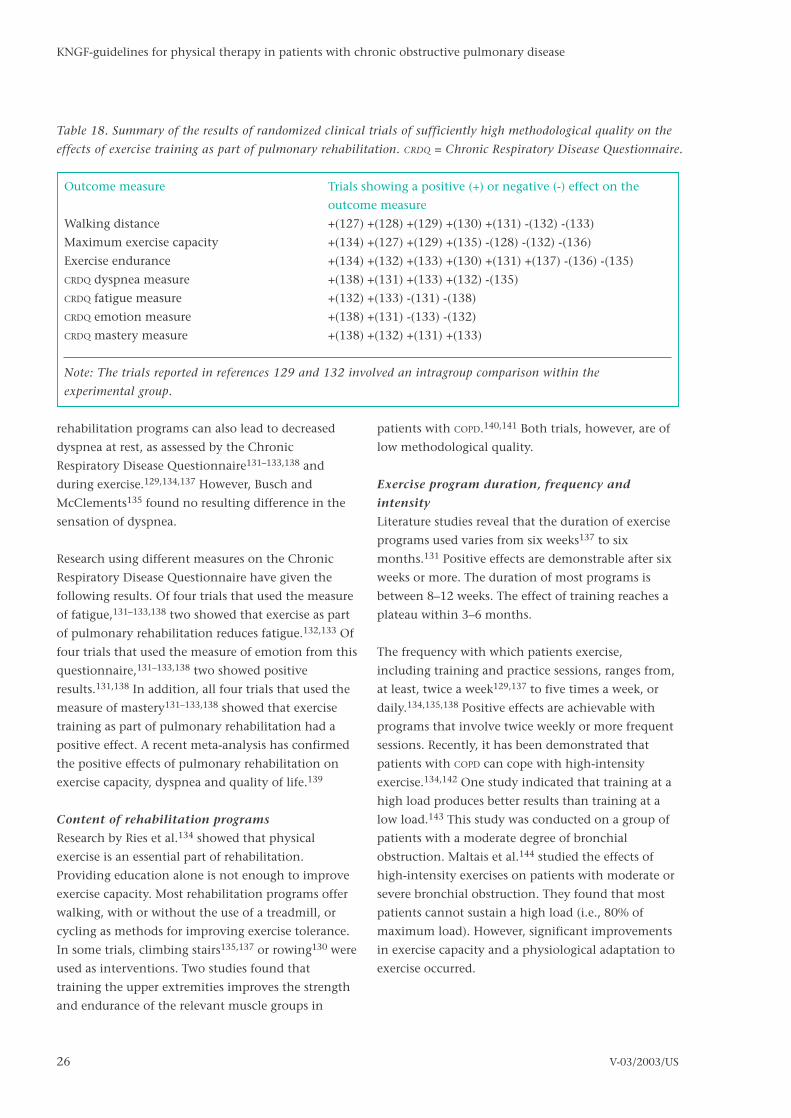
rehabilitation programs can also lead to decreased
dyspnea at rest, as assessed by the Chronic
Respiratory Disease Questionnaire131–133,138 and
during exercise.129,134,137 However, Busch and
McClements135 found no resulting difference in the
sensation of dyspnea.
Research using different measures on the Chronic
Respiratory Disease Questionnaire have given the
following results. Of four trials that used the measure
of fatigue,131–133,138 two showed that exercise as part
of pulmonary rehabilitation reduces fatigue.132,133 Of
four trials that used the measure of emotion from this
questionnaire,131–133,138 two showed positive
results.131,138 In addition, all four trials that used the
measure of mastery131–133,138 showed that exercise
training as part of pulmonary rehabilitation had a
positive effect. A recent meta-analysis has confirmed
the positive effects of pulmonary rehabilitation on
exercise capacity, dyspnea and quality of life.139
Content of rehabilitation programs
Research by Ries et al.134 showed that physical
exercise is an essential part of rehabilitation.
Providing education alone is not enough to improve
exercise capacity. Most rehabilitation programs offer
walking, with or without the use of a treadmill, or
cycling as methods for improving exercise tolerance.
In some trials, climbing stairs135,137 or rowing130 were
used as interventions. Two studies found that
training the upper extremities improves the strength
and endurance of the relevant muscle groups in
patients with COPD.140,141 Both trials, however, are of
low methodological quality.
Exercise program duration, frequency and
intensity
Literature studies reveal that the duration of exercise
programs used varies from six weeks137 to six
months.131 Positive effects are demonstrable after six
weeks or more. The duration of most programs is
between 8–12 weeks. The effect of training reaches a
plateau within 3–6 months.
The frequency with which patients exercise,
including training and practice sessions, ranges from,
at least, twice a week129,137 to five times a week, or
daily.134,135,138 Positive effects are achievable with
programs that involve twice weekly or more frequent
sessions. Recently, it has been demonstrated that
patients with COPD can cope with high-intensity
exercise.134,142 One study indicated that training at a
high load produces better results than training at a
low load.143 This study was conducted on a group of
patients with a moderate degree of bronchial
obstruction. Maltais et al.144 studied the effects of
high-intensity exercises on patients with moderate or
severe bronchial obstruction. They found that most
patients cannot sustain a high load (i.e., 80% of
maximum load). However, significant improvements
in exercise capacity and a physiological adaptation to
exercise occurred.
26
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Outcome measure Trials showing a positive (+) or negative (-) effect on the
outcome measure
Walking distance +(127) +(128) +(129) +(130) +(131) -(132) -(133)
Maximum exercise capacity +(134) +(127) +(129) +(135) -(128) -(132) -(136)
Exercise endurance +(134) +(132) +(133) +(130) +(131) +(137) -(136) -(135)
CRDQ dyspnea measure +(138) +(131) +(133) +(132) -(135)
CRDQ fatigue measure +(132) +(133) -(131) -(138)
CRDQ emotion measure +(138) +(131) -(133) -(132)
CRDQ mastery measure +(138) +(132) +(131) +(133)
Note: The trials reported in references 129 and 132 involved an intragroup comparison within the
experimental group.
Table 18. Summary of the results of randomized clinical trials of sufficiently high methodological quality on the
effects of exercise training as part of pulmonary rehabilitation. CRDQ = Chronic Respiratory Disease Questionnaire.

Follow-up
The importance of follow-up after a rehabilitation
program is clearly demonstrated by data from
Wijkstra et al.42 The researchers found that exercise
capacity tended to decrease over time, but that the
benefits could be maintained by arranging follow-
ups. Ries et al.134 followed patients after completion
of a rehabilitation program or an educational
program. Soon after the programs were completed,
there were significant differences between the two
groups, with the rehabilitation group showing more
positive results. Over the course of time, however,
these differences became less marked. In one study,
six years after rehabilitation, the survival rate in
patients who followed a rehabilitation program was
higher than in those who did not, at 67% compared
to 56%, respectively.134 The difference was not
statistically significant, however.
Effects of inspiratory muscle training (IMT)
Studies were included in the literature review if they
involved randomized clinical trials in which COPD
patients underwent respiratory muscle training to
improve the strength and endurance of respiratory
muscles. If resistance loading was involved, pressure
at the mouth had to have been measured. As the
guidelines state that training intensity should also be
defined, it was later decided to exclude trials in which
training intensity was not explicitly
described.136,145,146 Studies that involved training
with normocapnic hyperpnea were excluded147–149
because this training regimen is not practically
applicable. After applying these selection criteria, 10
trials remained for inclusion in the systematic review.
All were of sufficiently high methodological quality.
Effects of inspiratory muscle training on the
strength and endurance of inspiratory muscles
In COPD patients, genuine respiratory muscle training
leads to a significant increase in respiratory muscle
strength compared with placebo respiratory muscle
training. Increased endurance and reduced dyspnea
have also been reported.150
High-resistance respiratory muscle training produces
a greater increase in strength and endurance from
baseline than low-resistance training.151–155 In two of
the five trials considered, respiratory muscle strength
was different from that in the control group.151,153
However, Lisboa et al.,155 Harver et al.156 and Preusser
et al.152 found no difference in respiratory muscle
strength between the group that trained at a high
load and the group that trained at a low load. In
addition, Larson et al.151 and Preusser et al.152 found
no difference between the two groups in terms of
respiratory muscle endurance.
General effects of inspiratory muscle training
Two of the above five trials examined the effect of
respiratory muscle training on dyspnea.154,155 Both
found that respiratory muscle training reduces
dyspnea. Three of the five trials examined the effects
of respiratory muscle training on walking
distance.151,152,155 All three found that walking
distance had increased in the group that trained at a
high load. In addition, Preusser et al.’s study152 found
that walking distance in the group that trained at a
low load had also increased. Only Larson et al.’s
study151 found a significant difference between the
two groups.
Inspiratory muscle training combined with
exercise training
Four trials investigated the effect of adding
respiratory muscle training to exercise training by
comparing groups that received both with groups
that received exercise training alone.58,128,130,156 In all
trials, the groups that received respiratory muscle
training showed increased respiratory muscle
strength and endurance compared to baseline. This
was not seen in Berry et al.’s study128 because no
baseline values were given.
Two of these four studies showed that respiratory
muscle training provided additional gains in terms of
respiratory muscle strength and diaphragm
fatigability.58,156 Weiner et al.130 did not make any
between group comparisons, and Berry et al.128 found
no difference between the two groups.
Three of the four studies examined the additional
benefits of respiratory muscle training on walking
distance and maximum exercise capacity. Two trials
showed that respiratory muscle training gave
additional benefits,58,130 whereas another study
found that walking distance was improved by
27
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

exercise training but not by respiratory muscle
training.128
The only study that investigated the additional
effects of respiratory muscle training on dyspnea
found no difference between the two training
groups.128 Moreover, Dekhuijzen et al.58 failed to
show that respiratory muscle training offered any
additional benefit in terms of performing normal
daily activities or of emotional functioning.
The results of all these studies are summarized in
Table 19.
Exercise load, duration and frequency
Preusser et al.152 found that a training intensity of
22% PImax resulted in improved respiratory muscle
endurance and increased walking distance, but
produced no difference in respiratory muscle
strength. Larson et al.151 found no significant change
in respiratory muscle strength or endurance or in
walking distance at a training intensity of 15%
PImax. Lisboa et al.155 found an increase in strength
at a training intensity of 10% PImax. In contrast,
Heydra et al.153 found no increase in strength at a
training load of 10% PImax and Larson et al.151
found no increase in strength at a training load of
15% PImax. The literature review, therefore, found no
consistent evidence about which training intensity
results in training effects nor did it show that a
higher load leads to better results.
Literature findings on the optimum duration and
frequency of training are inconsistent. Different
studies report training periods varying from eight
weeks150,151,154,156 to six months.130 However, most
trials used a training duration in the range of 8–12
weeks.
The frequency of respiratory muscle training reported
in the selected literature varies from four 15-minute
sessions a day150 to three 15-minute sessions a
week.130 However, most trials employed a frequency
of two 15-minute sessions a day.
Since no consistent conclusions on exercise load,
duration and frequency can be derived from the
literature review, following the example of the
European Respiratory Society, it is recommended that
respiratory muscle training takes place five to seven
28
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
Outcome measure Explanatory] trials Pragmatic trials: Pragmatic trials:
high load versus low load respiratory muscle training
with or without exercise
Respiratory muscle strength* +(150) +(151) +(153) -(152) +(58) +(156) +(130) –(128)
–(154) –(155)
Respiratory muscle endurance* +(150) +(153) –(151) –(152) +(58) +(156) +(130) –(128)
Dyspnea +(150) –(128) +(154) +(155)
Walking distance +(151) –(155) –(152) +(58) +(130) –(128)
Exercise capacity** –(155) +(130) +(156)
Performance of normal daily –(58)
activities and emotional
functioning
* includes strength or diaphragm fatigability;
** (sub)maximum exercise capacity (including maximum oxygen volume consumption rate, VO2max); + =
there is a significant difference between the intervention and control groups in favor of the intervention
group; – = there is no significant difference between the two groups.
Note: The study of respiratory muscle strength and endurance carried out by Weiner et al.130 involved an
between group comparison within the experimental group.
Table 19. Summary of the results of randomized clinical trials of sufficiently high methodological quality on the
effect of respiratory muscle training, listed in terms of outcome measures.
days a week for two 15-minute sessions per day for a
minimal training duration of eight weeks. The
training load should be between 30–40% PImax157
Training method
Different training methods place different loads on
the respiratory muscles. It is possible to customize the
method for each individual on the basis of the
magnitude of pressure or flow, or a combination of
the two.158 If resistance loading is used, pressure at
the mouth will need to be monitored in order to be
certain that a specific load is being applied. A change
in breathing strategy, in particular one involving the
use of slow deep breathing, can reduce the actual load
on the respiratory muscles.159 By consensus, the
steering group recommends that the ratio of
inspiration time to expiration time should be
maintained at 3:5.
The threshold training method has been shown to be
a reliable and reproducible method of loading the
respiratory muscles in patients with COPD.160
Decreasing dyspnea
Active expiration
When respiratory demand increases in healthy
people, the abdominal muscles automatically begin
to take up some of the load.161 In patients with COPD,
the abdominal muscles contribute to breathing even
at rest. This almost exclusively involves the transverse
abdominal muscle.162 Tensing the abdominal muscles
during expiration improves the position of the
diaphragm, enabling it to deliver more force.
Reybrouck et al.163 compared the effects of active
expiration using myofeedback from the abdominal
muscles with active expiration without such
feedback. The patient group who used myofeedback
showed a significantly greater decrease in functional
residual capacity and an increase in PImax.
Reducing the respiratory rate
Breathing at a low frequency at rest results in
improved alveolar ventilation and better arterial
blood gas concentrations. However, during exercise,
low-frequency breathing does not significantly
improve gas exchange and the respiratory minute
volume is significantly reduced.164
Body posture
Adopting a particular body posture can lengthen the
diaphragm, enabling it to provide more force and to
contribute more to respiration. The study carried out
by Sharp et al.165 supports this observation. They
found that, in patients who benefit from leaning
forward, electromyographic activity in the inspiratory
accessory muscles increases significantly when they
stand up straight or sit. In contrast, therefore, leaning
forward reduces electromyographic activity in the
accessory muscles. The trials conducted by Druz and
Sharp166 and O’Neill and McCarthy167 point to the
same conclusion: that leaning forward improves the
function of the diaphragm.
Pursed-lips breathing
Pursed-lips breathing involves exhaling steadily
through slightly pursed lips. This action counteracts
dynamic compression of the respiratory tract such
that functional residual capacity decreases and
inspiratory capacity increases. In addition, pursed-lips
breathing slows the respiratory rate and increases
tidal volume.79,168,169 Not every patient benefits from
this technique. The effects of pursed-lips breathing
(i.e., decreased respiratory rate and increased tidal
volume) are more significant in patients who benefit
from pursed-lips breathing.79 Moreover, pursed-lips
breathing at rest improves blood gas
concentrations.79,168,169 These effects have not been
observed during exercise.79 Pursed-lips breathing at
rest can reduce dyspnea. The mechanism of action is
not yet clear.
Diaphragmatic breathing
Diaphragmatic breathing is wrongly thought to be an
effective way of breathing. Gosselink et al.170 found
that diaphragmatic breathing in severe COPD patients
results in poorer coordination of respiratory
movement and decreased mechanical efficiency of
the diaphragm. There is also a tendency for dyspnea
to increase.
Habituation
The mechanisms causing habituation are not yet
understood. Various trials have shown that exercise
can reduce dyspnea but physiological training does
not appear to have an effect.171,172 Rosser and Guz173
have suggested that psychological factors may
29
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

explain the reduction in dyspnea. Another study of
the importance of psychological factors showed that
dyspnea can be reduced if training occurs in a
familiar environment174 and if distracting stimuli
such as music are present during exercise.175 These
effects may occur because cognitive and contextual
factors play a role in dyspnea.
Another mechanism could be desensitization. In
desensitization, psychological or physiological factors
may lead to reduced awareness of dyspneic stimuli or
to reduced sensitivity of peripheral or central
receptors, or both.
Improving compliance with therapy
Kanters176 carried out a literature review of the
efficacy of patient education. He concluded that
patient education does result in greater compliance
with therapy in short-term disorders, but that
ensuring compliance with therapy in chronic
disorders requires continuous attention: “Patient
education cannot change the somatic basis of chronic
bronchitis or pulmonary emphysema at all. What
does occur is that the patient gains a greater grasp of
and copes more wisely with his disease”.176
Van der Burgt and Verhulst177 carried out an
overview of all the education models used in health
education and translated them into a model of
patient education for use in allied health care
practice. In so doing, they integrated the Attitude,
Social Influence and Personal Efficacy determinant
model with Hoenen et al.’s step-by-step approach to
providing information.178 The Attitude, Social
Influence and Personal Efficacy determinant model is
based upon the assumption that willingness to
change behavior is determined by a combination of
the patient’s attitude (how the individual perceives
behavioral change), social influences (how others see
behavioral change) and the patient’s perception of his
own efficacy, his self-efficacy (whether the patient
thinks it will work or not). The step-by-step approach
to providing information proposed by Hoenen et
al.178 distinguishes between the stages of openness,
understanding, willingness and doing. With allied
health care practice in mind, van der Burgt and
Verhulst added two extra phases: ability and
persistence. To do justice to the patient’s
individuality, another phase, designated ‘the person’,
was added to the model, as described below. Van der
Burgt and Verhulst177 regard patient information as a
process in which behavioral modification is the final
step. This final step cannot be taken until the
previous stages are complete. The six stages must be
completed sequentially. See Table 20.
In addition, during all stages of the educational
process, it is important to take individual
characteristics of the patient into account, such as his
or her:
• locus of control; To what extent does the patient
believe that he or she can influence the course of
his or her life?
• attribution; What factors does the patient regard
as influencing the course of his or her life?
• coping styles; How does the patient react to
significant events in his or her life?
• emotional state; Is the patient unable to accept
new information because of his or her emotional
state? The answer to this question may also
determine how the patient handles his or her
disease and its treatment.
Knibbe and Wams179)describe a system for increasing
compliance with therapy. It differentiates between
short-term and long-term compliance. To achieve
long-term therapeutic compliance, a great deal of
attention must be paid to evaluating the advantages
and disadvantages of therapy and to the individual’s
sense of their own effectiveness. The patient’s
perception of the advantages and disadvantages of
therapy can be influenced by logical argument. The
patient’s sense of individual effectiveness can be
increased by helping him or her to feel that he or she
is capable of performing the behavior, i.e., that he or
she has mastery over the situation.
Education plan
The physical therapy treatment plan must include an
education plan, in which subgoals are formulated for
each stage. The education plan can be seen as part of
a methodical approach to patient management. It
can begin during history-taking with an analysis of
the patient’s need for information: What does the
patient know about his or her disorder and about the
medications he or she will use? How efficient is the
30
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

method used for administering the medication and
does the patient know how it can be improved? What
are the patient’s and his or her partner’s expectations
of treatment? At every stage, it is important to pay
attention to any problems the patient is
experiencing. By adopting this approach, information
about the possible causes of any problems in
complying with therapy can be obtained.
Dekkers180 subdivides patient education into four
categories: information, instruction, education and
guidance. This classification is hierarchical in that
activities in the category of information require the
least intervention whereas those in the category of
guidance require the most.
• Information: providing the patient with factual
information about the disease, its treatment, and
medical care.
• Instruction: providing specific guidelines or
recommendations for patients to enable them to
assist the treatment process.
• Education: providing an explanation of the
disease and its treatment in such a way that the
patient understands the background to and
consequences of the condition and appreciates
what he or she can do to keep the disease under
control. Self-care skills should be practiced, if
necessary.
• Guidance: supporting the patient emotionally so
that he or she can cope with and come to terms
with the disease and its effects to the greatest
extent possible.
31
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
1. Openness
In patient education, the physical therapist must take into account the patient’s perceptions, expectations,
questions and concerns. Significant questions are: What is the patient most concerned about? What
preoccupations prevent the patient from being open to information about behavioral modification?
2. Understanding
Information must be presented in such a way that the patient understands it and can remember it. The
important points here are: not to present too much information at one time, to decide what information
must be presented first and what can be given later, and to repeat the message (if necessary, in another way)
and to explain it using educational aids, such as leaflets or videos. The physical therapist should check
whether the patient has actually understood the information.
3. Willingness
The physical therapist notes the factors that make the patient unwilling to act. The important questions
here are: In what way does the patient benefit from exercise? Is the patient encouraged or discouraged by
people in his or her close environment? Does the patient feel that he or she can influence the situation? The
physical therapist provides support and information on alternative courses of action. Achievable goals are
set.
4. Ability
The patient must be able to carry out the desired behavior. The essential functions and skills must be
practiced. It is important to find out what practical problems the patient expects and to explore with the
patient how these problems can be solved.
5. Doing
This stage includes implementation of the new behavior. The physical therapist makes clear, specific,
attainable agreements with the patient and sets specific goals. If possible, positive feedback is given.
6. Persistence
The patient should continue to carry out the behavior after the end of treatment. During treatment, the
physical therapist must find out from patients whether they thinks they will succeed in continuing. It is
important to find out what discourages and what encourages the patient, and what the short-term and long-
term benefits are. What helps the patient to get back on track after a relapse?
Table 20. The six stages in the process of patient education.

In practice, these four categories overlap. However, it
is important to distinguish between them so that
different goals can be targeted during patient
education. The practical consequences of the
different categories of activity are quite different, as
are the time and educational aids and skills required.
Activities under the category of education involve a
more didactic style and require more teaching aids
than disseminating information. Signs of denial or
non-acceptance indicate that the patient’s greatest
need is for emotional support. If this is the case, the
referring physician should be consulted.
The following subjects must be covered in patient
education:134,181
• medical aspects of the disorder, including the
physiology and pathophysiology of respiration;
• COPD and medication use, including oxygen
therapy;
• medication techniques and personal hygiene;
• healthy eating;
• physical therapy and breathing exercises;
• personal advice on movement; and
• ways to improve social participation.
In a study of the role of patient education in physical
therapy, Sluis182 concluded that it is a vital
component of treatment: information was provided
in 97% of therapy sessions. On the basis of this study,
Sluis made a number of observations:
• little information was given on matters of general
health, health education, and psychosocial
support, even though patients needed it. More
clarity is needed in those subjects that physical
therapists have to communicate.
• most of the information was given in the first two
sessions. The patient education plan should be
designed so that the information can be provided
evenly over the course of treatment. It is possible
for the therapist to work systematically and to pay
attention to all aspects of education without
patients having to receive too much information
at one time;
• two factors that significantly influence
compliance were the obstacles patients
experienced and a lack of positive feedback. To
help counteract these, the exercises and advice
given should be tailored to the individual patient’s
situation. The physical therapist must also
regularly pay attention to the problems
experienced by patients in performing exercises
and in implementing behavioral modification.
The physical therapist should also make greater
use of positive feedback.
In the Netherlands, the (Dutch) National Center for
Medical Information and Health Education (GVO), the
Dutch Asthma Foundation, and COPD nurses can offer
support during the educational process.
Completion of the treatment
At some point during treatment and, necessarily, at
the end of treatment, the referring physician should
be informed about the treatment carried out and its
results.183 Interdisciplinary communication is as
essential part of effective rehabilitation.
After-care
After treatment has been completed, patients must
adopt an active approach to maintain the gains they
have achieved. After-care usually involves regular
exercise. In the Netherlands, the Dutch Asthma
Foundation (Nederlands Asthma Fonds) organizes
athletic groups for individuals with COPD. These
involve participation in specially adapted group
sports and games. The patient’s health status
determines whether participation in an athletic group
is possible. The exclusion criteria are an FEV1 of less
than 1000 ml (or less than 45% of that predicted) or
arterial hypoxemia during exercise. In the
Netherlands, alternative sporting activities are
organized in several cities for patients who cannot
participate in regular COPD athletic groups.
Information about these activities can be obtained
from the Dutch Asthma Foundation.
The legal significance towards the guidelines
Guidelines are no statutory regulations, but they give
insights and recommendations, based on the results
of scientific research, which health care workers must
fulfill to attain quality care. Since the
recommendations are mainly based on the ‘average
patient’, the health care workers have to use their
professional autonomy to deviate from the guidelines
if this the patient’s situation requires this. Whenever
there is a deviation from the guidelines, this has to be
32
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

augmented and documented.1,2 The responsibility for
the interventions remains with the individual
physical therapist.
Revisions
The KNGF-guidelines are the first development in
clinical questions pertaining to diagnostics, treatment
and prevention for patients with chronic bronchitis
and emphysema. Developments that can improve the
physical therapeutic care of this group of patients,
can change the current insights written in the
guidelines. In the method for developing and
implementing guidelines is indicated that all
guidelines will be revised after three to five years
maximum after the original publication.1,2 This
means that the KNGF, together with the working
group, will decide not later than in the year 2003 if
these guidelines are still accurate. If necessary a new
working group will be installed to revise the
guidelines. The validity of the guidelines expires if
new developments give reasons to start a reversionary
process.
Before the reversionary process, also the Method for
Guideline Development and Implementation will be
updated based on new insights and cooperation
agreements made between the several guideline
developers in The Netherlands. The consensus
products of the Evidence Based Guideline Meeting
(EBRO platform), which are developed under the
auspices of the CBO, will be included in the updated
method. The uniform and transparent methods for
the determination of the amount of evidence and the
derived recommendations for practice are important
improvements.
External financing
These guidelines are subsidized by the Dutch Asthma
Foundation (NAF). The possible interests of the
subsidizer have neither influenced the content of the
guidelines nor the related recommendations.
Acknowledgement
We would like to thank all members of the second
workgroup for their part in the realization of these
KNGF-guidelines. They are: prof. dr. H. Th. M.
Folgering, mrs. prof. dr. D. S. Postma, mrs. E. M. A. L.
Rameckers, mrs. M. Telkamp, dr. J. M. Rooyackers, mr.
Thiadens and drs. Ph. J. van der Wees. Dr. ir. C. P. van
Schayck and drs. W Cambach are thanked for their
valuable contribution to the guidelines.
33
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

Notes on diagnosis1. One or more questionnaires may be used to
assess quality of life. The Chronic Respiratory
Disease Questionnaire (CRDQ), the St George’s
Respiratory Questionnaire (SGRQ) and the
Medical Psychological Questionnaire for Lung
Diseases (MPQL)186 are useful for the physical
therapist and have been tested for reliability
and validity. The MPQL) is no longer available
and will, therefore, not be discussed further
here. The CRDQ covers the effects of dyspnea on
normal daily activities, emotion, fatigue, and
symptom control.40,185,186 The SGRQ evaluates
symptoms, activities limited by dyspnea, and
the impact of COPD on other factors, such as
work, symptom control, and normal daily
activities.187,188 More information is given in
Chapter 7 of the Dutch project report.189 These
questionnaires are primarily intended to
enable the therapist to gain an impression of
the patient’s quality of life and to describe
treatment. They are not intended to determine
the effects of treatment in individual patients
because they were developed to study groups
and it is not clear how valid they are for
individuals. The SGRQ is freely available for use
(see discussion of measuring instruments in
the guidelines). Answer sheets are required to
use the CRDQ (these can be ordered through the
physical therapy departmental office at the VU
Hospital in Amsterdam, the Netherlands).
2. As far as possible, patients themselves should
determine what information they need. As a
result, the medical practitioner will be better
able to understand the patient’s life, the
patient will find the information more useful,
and he or she will be encouraged to share
responsibility for communication with the
medical practitioner.190 The treatment team
must agree on who is responsible for providing
what information to the patient.
3. Coughing or huffing may be unproductive
because there is: an inadequate expiratory
force due to muscle weakness, pain or
abdominal wall insufficiency; insufficient
inspiratory breathing volume; or
tracheobronchial collapse.14
4. This provides information on where mucus
retention can occur.
5. This provides information on where sputum is
being retained.
6. The peak expiratory flow is the maximum
airflow rate during forced expiration. The
patient can use peak flow measurements to
check airway obstruction at home. The margin
of error in these measurement is 10–20%. The
European Respiratory Society recommends
taking the highest of the first three technically
good expirations.191 This technique is not
suitable for measuring the degree of
obstruction in COPD patients.
7. Provides information about the severity of the
disorder and the patient’s disease stage.
8. Provides information about load-bearing
capacity and about the disorders that have
developed because of adaptation to pulmonary
obstruction.
9. When the thorax is in a position characteristic
of inspiration, the anteroposterior and lateral
diameters of the thorax are greater, the
epigastric angle is obtuse, the ribs and clavicle
are more horizontal, and the distance between
the cricoid and the manubrium sterni is
smaller.14
10. Provides information on the load-bearing
capacity and about the disorders that have
developed because of adaptation to pulmonary
obstruction. Respiration or respiratory
movement may adapt before changes in the
position and shape of the thorax are visible.
11. Testing movement provides information about
load-bearing capacity and muscle function
impairments in the pulmonary patient. PImax
should be measured to assess the strength of
the respiratory muscles. Normal values are
given in terms of centimeters of water
(cmH2O). by Rochester and Arora:192 for
women between the ages of 19–49 years, the
normal value is -91 cmH2O; for women
between the ages 50–69, -77 cmH2O; for
women aged 70 years and over, -66 cmH2O; for
men aged 19–49 years, -127 cmH2O; for men
aged 50–69, -112 cmH2O; and for men aged 70
years and over, -76 cmH2O. If PImax is lower
than 70% of normal, respiratory muscle
34
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

strength is reduced. A handheld dynamometer
can be used to assess the strength of other
peripheral muscles.193 For normal values and
further information, refer to Chapter 7 of the
Dutch project report.189
12. Provides information on the patient’s level of
stamina.
13. The walking test is a reliable measure of
stamina. Although the 12-minute test has
somewhat higher sensitivity, reliability and
discriminatory power,194 the 6-minute test is
recommended by the steering group because it
is quicker and, therefore, more practical. The
‘shuttle’ walking test is another option. More
information is given in the Dutch project
report.189
14. Pulse oximeters provide a non-invasive means
of estimating blood oxygen saturation. The
pulse oximeter used should be accurate during
exercise and sensitive to changes in oxygen
saturation up to a level of at least 90%. The
Hewlett-Packard and the Biox II pulse
oximeters meet these standards.195
15. The Borg scale is preferred by the steering
group because it has higher reliability and
stability and because its results correlate better
with respiration.196 The Borg scale is also
simpler to use and easier to standardize. Visual
analogue scales are good alternatives.196
35
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

Abbreviations and glossary of terms
CNSLD chronic non-specific lung disease
COPD chronic obstructive pulmonary disease
FEV1 forced expiratory volume in one second
PImax maximum inspiratory pressure at the mouth
TLco transfer coefficient, expressing the diffusion capacity of the lung per unit of lung
volume (also known as DLco and Kco)
activity execution of a task or action by an individual
disability difficulties an individual may have in executing activities. Activities can be limited
in type, duration and quality.
huffing forced exhalation with an open glottis
coughing forced exhalation with a closed glottis
disorder abnormality in a body structure, or loss of or abnormality in a physiological or
psychological function
incidence of CNSLD number of new CNSLD patients in a given period of time
incremental exercise test maximum exercise test carried out under the supervision of a pulmonary physician,
during which various parameters are measured
participation involvement in a life situation, in the context of disorders, activities, health
condition and environmental factors. Participation can be restricted in type,
duration and quality
prevalence of CNSLD number of CNSLD patients at a given point in time
36
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

1 Hendriks HJM, Reitzma E, van Ettekoven H. Centrale
richtlijnen in de fysiotherapie. Ned Tijdschr Fysiother
1996;106:2-11.
2 Hendriks HJM, van Ettekoven H, Reitzma E, Verhoeven ALJ,
van der Wees PhJ. Methode voor de centrale
richtlijnontwikkeling in implementatie in de fysiotherapie.
1998, Amersfoort, KNGF/NPi/CBO.
3 Bekkering GE, Hendriks HJM, Chadwick-Straver RVM,
Gosselink R, Jongmans M, Paterson WJ, van der Schans CP,
Verhoef-de Wijk MCE, Decramer M. Richtlijn voor het
fysiotherapeutisch handelen bij patiënten met chronisch
obstructieve longaandoeningen. Achtergronden en evaluatie
van de richtlijn COPD. 1998, Amersfoort, NPi.
4 Hendriks HJM, van Ettekoven H, van der Wees PhJ.
Eindverslag van het project Centrale richtlijnen in de
fysiotherapie (Deel 1). Achtergronden en evaluatie van het
project. 1998, Amersfoort, KNGF/NPi/CBO.
5 Hendriks HJM, Bekkering GE, van Ettekoven H Bransma JW,
van der Wees PhJ, de Bie RA. Development and
implementaion of national practice guidelines: A prospect
for continuous quality improvement in physiotherapy.
Introduction to the method of guideline development.
Physiotherapy 2000;86:535-547.
6 Bekkering GE, Hendriks HJM. Toelichting op de KNGF-
richtlijn COPD. Ned Tijdschr Fysiother 1998;108(5).
7 Deskundigheidbevorderingspakket KNGF-richtlijn COPD.
Fysiopraxis 1998.supplement
8 Hendriks HJM, van Ettekoven H, Bekkering GE, Verhoeven
ALJ. Implementatie van KNGF-richtlijnen. Fysiopraxis
2000;9:9-13.
9 Orie NGM, Sluiter HJ, de Vries K, Tammeling GJ, Witkop J.
The host factor in bronchitis. In: Orie NGM, Sluiter HJ,
editors. Bronchitis. Assen, the Netherlands: Royal van
Gorcum; 1961:43-59.
10 Sluiter HJ, Koeter GH, de Monchy JG, Postma DS, de Vries K,
Orie NG. The Dutch hypothesis (chronic non-specific lung
disease). revisited. Eur Respir J 1991;4:479-89.
11 Vermeire PA, Pride NB. A ‘splitting’ look at chronic
nonspecific lung disease (CNS-LD): common features but
diverse pathogenesis. Eur Respir J 1991;4:490-6.
12 Burrows B, Bloom JW, Traver GA, Cline MG. The course and
prognosis of different forms of chronic airways obstruction
in a sample from the general population. N Engl J Med
1987;317:1309-14.
13 Van Schayck CP. Het einde van de term CARA in zicht? [Is
the end of the term CNSLD in sight?] Ned Tijdschr
Geneeskd 1994;138:1405-8.
14 Gosselink HAAM, Cox N, Decramer M, Folgering HTM.
Fysiotherapie bij CARA. [Physical Therapy for CNSLD.] 3rd
ed. Utrecht, the Netherlands: Bunge; 1992.
15 American Thoracic Society. Standards for the diagnosis and
care of patients with chronic obstructive pulmonary disease.
ATS statement. Am J Respir Crit Care Med 1995;152:S77-
S120.
16 Siafakas NM, Vermeire P, Pride NB, Pooletti P, Gibson J,
Howard P et al. Optimal assessment and management of
chronic obstructive pulmonary disease (COPD). Eur Respir J
1995;8:1398-420.
17 American Thoracic Society. Lung function testing: selection
of reference values and interpretative strategies. Am Rev
Respir Dis 1991;144:1202.
18 Guyatt GH, Thompson PJ, Berman LB, Sullivan MJ,
Townsend M, Jones NL et al. How should we measure
function in patients with chronic heart and lung disease? J
Chronic Dis 1985;38:517-24.
19 McSweeny AJ, Grant I, Heaton RK, Adams KM, Timms RM.
Life quality of patients with chronic obstructive pulmonary
disease. Arch Intern Med 1982;142:473-8.
20 Okubadejo AA, Jones PW, Wedzicha JA. Quality of life in
patients with chronic obstructive pulmonary disease and
severe hypoxaemia. Thorax 1996;51:44-7.
21 Wijkstra PJ, ten Vergert EM, van de Mark TW, Postma DS,
van Altena R, Kraan J, Koeter GH. Relation of lung function,
maximal inspiratory pressure, dyspnoea, and quality of life
with exercise capacity in patients with chronic obstructive
pulmonary disease. Thorax 1994;49:468-72.
22 Williams SJ, Bury MR. Impairment, disability and handicap
in chronic respiratory illness. Soc Sci Med 1989;29:609-16.
23 American Thoracic Society. Standards for the diagnosis and
care of patients with chronic obstructive pulmonary disease
(COPD). and asthma. Am Rev Respir Dis 1987;136:225-44.
24 Kaptein AA, Dekker FW, Dekhuijzen PNR, Wagenaar JPM,
Janssen PJ. Patienten met chronische luchtwegobstructie.
Scores op NPV en scl-90 en hun relaties met functionele
capaciteit en belemmeringen in dagelijkse activiteiten.
[Patients with chronic airway obstruction. Scores on NPV
and scl-90 and their relationships to functional capacity and
limitations on activities of daily life.] Gezond Samenlev
1986;7:10-9.
25 Van de Lende R, Huygen C, Jansen-Koster EJ, Knijpstra S,
Peset R, Quanjer PH et al. Epidemiologisch onderzoek naar
het verband tussen luchtverontreiniging en het voorkomen
van luchtwegaandoeningen. [Epidemiological studies on the
relationship between air pollution and development of
respiratory disorders.] Ned Tijdschr Geneeskd 1975;119:577-
84.
26 Beaty TH, Menkes HA, Cohen BH, Newill CA. Risk factors
associated with longitudinal change in pulmonary function.
Am Rev Respir Dis 1984;129:660-7.
27 Knudson RJ, Knudson DE, Kaltenborn WT, Bloom JW.
Subclinical effects of cigarette smoking. A five-year follow-
up of physiologic comparisons of healthy middle-aged
smokers and nonsmokers. Chest 1989;95:512-8.
28 Tager IB, Segal MR, Speizer FE, Weiss ST. The natural history
of forced expiratory volumes. Effect of cigarette smoking
and respiratory symptoms. Am Rev Respir Dis 1988;138:837-
49.
29 Higgins MW, Keller JB. Trends in COPD morbidity and
mortality in Tecumseh, Michigan. Am Rev Respir Dis
1989;140:S42-8.
30 Kauffmann F, Drouet D, Lellouch J, Brille D. Twelve years
spirometric changes among Paris area workers. Int J
Epidemiol 1979;8:201-12.
31 Heederik D, Pouwels H, Kromhout H, Kromhout D. Chronic
non-specific lung disease and occupational exposures
estimated by means of a job exposure matrix: the Zutphen
Study. Int J Epidemiol 1989;18:382-9.
32 Buist SA. Smoking and other risk factors. In: Murray JF,
37
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
References

Nadel JA, editors. Textbook of respiratory medicine. 2nd ed.
Philadelphia: WB Saunders; 1994;1259-87.
33 Anthonisen NR, Wright EC, Hodgkin JE, IPPB Trial Group.
Prognosis in chronic obstructive pulmonary disease. Am Rev
Respir Dis 1986;133:14-20.
34 Prescott E, Lange P, Vestbo J. Chronic mucus hypersecretion
in COPD and death from pulmonary infection. Eur Respir J
1995;8:1333-8.
35 Wilson DO, Rogers RM, Wright EC, Anthonisen NR. Body
weight in chronic obstructive pulmonary disease. The
National Institutes of Health Positive-Pressure Breathing
Trial. Am Rev Respir Dis 1989;139:1435-8.
36 Postma DS, Burema J, Gimeno F, May JF, Smit JM, Steenhuis
EJ et al. Prognosis in severe chronic obstructive pulmonary
disease. Am Rev Respir Dis 1979;119:357-67.
37 Van de Lende R, Jansen-Koster EJ, Knijpstra S, Meinesz AF,
Wever AMJ, Orie NGM. Prevalentie van CARA in
Vlagtwedde en Vlaardingen (Computerdiagnose versus
artsendiagnose). [Prevalence of CNSLD in Vlagtwedde and
Vlaardingen (Computer diagnosis versus physician
diagnosis).] Ned Tijdschr Geneeskd 1975;119:1988-98.
38 Scenariocommissie Chronische Ziekten. Chronische ziekten
in het jaar 2005. Deel 2. Scenario’s over CARA 1990-2005.
[Scenario Commission on Chronic Diseases. Chronic
diseases in the year 2005. Part 2. Scenarios with CNSLD
1990-2005.] Houten/Antwerpen, the Netherlands/Belgium:
Bohn Stafleu van Loghum; 1990.
39 Van Molken MPMH, van Doorslaer EKA, Rutten FFH. CARA
in cijfers. Verslag van een pilotstudie. [CNSLD in figures.
Report on a pilot study.] 1989.
40 Gosselink HAAM, Wagenaar RC, van Keimpema A,
Chadwick-Straver RVM. Het effect van een
reactiveringsprogramma bij patiënten met CARA. [The effect
of a reactivation program among CNSLD patients.] Ned
Tijdschr Fysiother 1990;100:193-9.
41 Strijbos JH, Postma DS, van Altena R, Gimeno F, Koeter GH.
A comparison between an outpatient hospital-based
pulmonary rehabilitation program and a home-care
pulmonary rehabilitation program in patients with COPD. A
follow-up of 18 months. Chest 1996;109:366-72.
42 Wijkstra PJ, van de Mark TW, Kraan J, van Altena R, Koeter
GH, Postma DS. Long-term effects of home rehabilitation on
physical performance in chronic obstructive pulmonary
disease. Am J Respir Crit Care Med 1996;153:1234-41.
43 Van Valk RWA, Dekker J, Boschman M. Basisgegevens
extramurale fysiotherapie 1989-1992. [Basic data on
extramural physical Therapy 1989-1992.] 1995.
44 Uunk W, Dekker J, Groenewegen P. Verwijzingen van
huisartsen naar fysiotherapeuten: morbiditeits-specifieke
verwijspercentages. [Referrals by primary care physicians to
physiotherapists: morbidity-specific referral percentages.]
1991.
45 Cambach W, Chadwick-Straver RVM, Wagenaar RC, van
Keimpema A, Kemper HCG, Rijswijk H. Feasibility of a
pulmonary rehabilitation program in community-based
physiotherapy practices. J Rehab Sci 1994;7:104-12.
46 Wasserman K, Sue DY, Casaburi R, Moricca RB. Selection
criteria for exercise training in pulmonary rehabilitation. Eur
Respir J Suppl 1989;7:604s-10s.
47 Hendriks HJM, Wagner C, Dekker J, Brandsma JW. Evaluatie
van het ‘consultatief fysiotherapeutisch onderzoek’ (CFO).
in de eerstelijn. [Evaluation of the “consultative
physiotherapeutic examination” (CPE) in first-line care.]
1994.
48 Hoeksma BH, Keur M, Schreij HG. Tijdsbestedingsonderzoek
klinische fysiotherapie. [Time-allocation study of clinical
physiotherapy.] Enschede, the Netherlands: Hoeksma,
Homans and Menting; 1991.
49 Stubbing DG, Mathur PN, Roberts RS, Campbell EJ. Some
physical signs in patients with chronic airflow obstruction.
Am Rev Respir Dis 1982;125:549-52.
50 Richardson PS, Peatfield AC. The control of airway mucus
secretion. Eur J Respir Dis Suppl 1987;153:43-51.
51 Goodman RM, Yergin BM, Landa JF, Golinvaux MH, Sackner
MA. Relationship of smoking history and pulmonary
function tests to tracheal mucous velocity in non-smokers,
young smokers, ex-smokers, and patients with chronic
bronchitis. Am Rev Respir Dis 1978;117:205-14.
52 Van de Schans CP, van de Mark TW, Rubin BK, Postma DS,
Koeter GH. Chest physical therapy: mucus mobilizing
techniques. In: Bach JR, editor. Pulmonary rehabilitation.
The obstructive and paralytic conditions. Philadelphia:
Hanley and Belfus Inc; 1996;229-46.
53 Clarke SW, Jones JG, Oliver DR. Resistance to two-phase gas-
liquid flow in airways. J Appl Physiol 1970;29:464-71.
54 Mullen JB, Wright JL, Wiggs BR, Pare PD, Hogg JC. Structure
of central airways in current smokers and ex-smokers with
and without mucus hypersecretion: relationship to lung
function. Thorax 1987;42:843-8.
55 Mossberg B, Camner P, Afzelius BA. The immotile-cilia
syndrome compared to other obstructive lung diseases: a
clue to their pathogenesis. Eur J Respir Dis Suppl
1983;127:129-36.
56 Vestbo J, Prescott E, Lange P. The Copenhagen City Heart
Study Group. Association of chronic mucus hypersecretion
with FEV1 decline and chronic obstructive pulmonary
disease morbidity. Am J Respir Crit Care Med
1996;153:1530-5.
57 Folgering H, van Herwaarden C. Exercise limitations in
patients with pulmonary diseases. Int J Sports Med
1994;15:107-11.
58 Dekhuijzen PNR, Folgering HTM, van Herwaarden CLA.
Target-flow inspiratory muscle training during pulmonary
rehabilitation in patients with COPD. Chest 1991;99:128-33.
59 Bye PT, Esau SA, Levy RD et al. Ventilatory muscle function
during exercise in air and oxygen in patients with chronic
airflow limitation. Am Rev Respir Dis 1985;132:236-40.
60 Juan G, Calverley P, Talamo C, Roussos C. Effect of carbon
dioxide on diaphragmatic function in human beings. N Engl
J Med 1984;310:874-9.
61 McParland C, Krishnan B, Wang Y, Gallagher CG.
Inspiratory muscle weakness and dyspnea in chronic heart
failure. Am Rev Respir Dis 1992;146:467-72.
62 Donahoe M, Rogers RM, Wilson DO, Pennock BE. Oxygen
consumption of the respiratory muscles in normal and
malnourished patients with COPD. Am Rev Respir Dis
1989;140:385-91.
63 Decramer M, Lacquet LM, Fagard R, Rogiers P.
Corticosteroids contribute to muscle weakness in chronic
airflow obstruction. Am J Respir Crit Care Med 1994;
150:11-6.
64 Gray-Donald K, Gibbons L, Shapiro SH, Martin JG. Effect of
nutritional status on exercise performance in patients with
chronic obstructive pulmonary disease. Am Rev Respir Dis
38
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

1989;140:1544-8.
65 Morrison NJ, Richardson J, Dunn L, Pardy RL. Respiratory
muscle performance in normal and elderly subjects and
patients with COPD. Chest 1989;95:90-4.
66 Cohen C, Zagelbaum G, Gross D, Roussos C, Macklem PT.
Clinical manifestations of inspiratory muscle fatigue. Am J
Med 1982;73:308-16.
67 Jones NJ, Jones G, Edwards RHT. Exercise tolerance in
chronic airway obstruction. Am Rev Respir Dis
1971;103:477-91.
68 Davidson AC, Leach R. George RJD, Geddes DM.
Supplemental oxygen and exercise ability in chronic
obstructive airways disease. Thorax 1988;43:965.
69 Light RW, Mahutte CK, Stansbury DW, Fischer CE, Brown
SE. Relationship between improvement in exercise
performance with supplemental oxygen and hypoxic
ventilatory drive in patients with chronic airflow
obstruction. Chest 1989;95:751-6.
70 Stein DA, Bradley BL, Miller WC. Mechanisms of oxygen
effects on exercise in patients with chronic obstructive
pulmonary disease. Chest 1982;81:6-10.
71 Killian KJ, Leblanc P, Martin DH, Summers E, Jones NL,
Campbell EJM. Exercise capacity and ventilatory, circulatory,
and symptom limitation in patients with chronic airflow
limitation. Am Rev Respir Dis 1992;146:935-40.
72 Maltais F, Simard AA, Simard C, Jobin J, Desgagnés P,
Leblanc P. Oxidative capacity of the skeletal muscle and
lactic acid kinetics during exercise in normal subjects and in
patients with COPD. Am J Respir Crit Care Med
1996;153:288-93.
73 Gosselink R, Troosters T, Decramer M. Peripheral muscle
weakness contributes to exercise limitation in COPD. Am J
Respir Crit Care Med 1996;153:976-80.
74 Minotti JR, Christoph I, Oka R, Weiner MW, Wells L, Massie
BM. Impaired skeletal muscle function in patients with
congestive heart failure. Relationship to systematic exercise
performance. J Clin Invest 1991;88:2077-82.
75 Schols AMWJ. Nutritional depletion and physical
impairment in patients with chronic obstructive pulmonary
disease. Implications for therapy. 1991.
76 Guz A. Respiratory sensations in man. Br Med Bull
1977;33:175-7.
77 Campbell EJM, Howell JBL. The sensation of breathlessness.
Br Med Bull 1963;19:36-40.
78 Burns BH, Howell JBL. Disproportionately severe
breathlessness in chronic bronchitis. Quart J Med
1969;151:277-94.
79 Mueller RE, Petty TL, Filley GF. Ventilation and arterial
blood gas changes induced by pursed-lips breathing. J Appl
Physiol 1970;28:784-9.
80 Celli BR, Rassulo J, Make BJ. Dyssynchronous breathing
during arm but not leg exercise in patients with chronic
airflow obstruction. N Engl J Med 1986;314:1485-90.
81 Geijer RMM, van Schayck CP, van Weel C, Sachs APE, van de
Zwan AAC, Bottema BJAM et al. NHG-Standaard COPD:
Behandeling. [NHG Guideline COPD: Treatment.] Huisarts
Wet 1997;40:430-42.
82 Engelen MPKJ, Schols AMWJ, Baken WC, Wesseling GJ,
Wouters EFM. Nutritional depletion in relation to
respiratory and peripheral skeletal muscle function in
outpatients with COPD. Eur Respir J 1994;7:1793-7.
83 Arora NS, Rochester DF. Effect of body weight and
muscularity on human diaphragm muscle mass, thickness
and area. J Appl Physiol 1982;52:64-70.
84 Schols AMWJ, Soeters PB, Dingemans AMC, Mostert R,
Frantzen PJ, Wouters EFM. Prevalence and characteristics of
nutritional depletion in patients with stable COPD eligible
for pulmonary rehabilitation. Am Rev Respir Dis
1993;147:1151-6.
85 Wilson DO, Rogers RM, Sanders MH, Pennock BE, Reilly JJ.
Nutritional intervention in malnourished patients with
emphysema. Am Rev Respir Dis 1986;134:672-7.
86 Rogers RM, Donahoe M, Costantino J. Physiologic effects of
oral supplemental feeding in malnourished patients with
chronic obstructive pulmonary disease. A randomized
control study. Am Rev Respir Dis 1992;146:1511-7.
87 Brouwer T, Nonhof-Boiten JC, Uilreef-Tobi FC. Diagnostiek
in de fysiotherapie. Proces en denkwijze. [Diagnostics in
physical therapy. Process and approach.] Utrecht, the
Netherlands: Wetenschappelijke uitgeverij Bunge; 1995.
88 Van Ravensberg CD, Oostendorp RAB, Heerkens YF.
Diagnostiek, basis voor behandelplan en evaluatie.
[Diagnostics, a foundation for the treatment plan and
evaluation.] In: Vaes P, Aufdenkampe G, de Dekker JB, van
Ham I, Smits-Engelsman B, editors. Jaarboek fysiotherapie
kinesitherapie 1997. Houten/Diegem, the Netherlands:
Bohn Stafleu Van Loghum; 1997:302-25.
89 Oostendorp RAB, van Ravensberg CD, Wams HWA,
Heerkens YF, Hendriks HJM. Fysiotherapie; wat omvat het?
[Physical Therapy: What does it involve?] Bijblijven
1996;12:5-17, 39.
90 Kleijnen J, Knipschild P. Niacin and vitamin B6 in mental
functioning: a review of controlled trials in humans. Biol
Psychiatry 1991;29:931.
91 Kleijnen J, de Crean AJM, van Everdingen J, Krol L. Placebo
effect in double-blind clinical trials: a review of interactions
with medications. Lancet 1994;344:1347-9.
92 Pocock SJ. Clinical trials: a practical approach. Chisester, UK:
Wiley; 1983.
93 Meinert CL. Clinical trials: design, conduct and analysis.
New York: Oxford University Press; 1986.
94 Chalmers TC, Smith H, Blackburn B, Silverman B, Schroeder
B, Reitman D et al. A method for assessing the quality of a
randomized control trial. Control Clin Trials 1981;2:31-49.
95 Leith DE. Cough. Phys Ther 1968;48:439-47.
96 Langlands J. The dynamics of cough in health and in
chronic bronchitis. Thorax 1967;22:88-96.
97 Tammeling GJ, Quanjer PH. Contouren van de ademhaling
I. [Contours of breathing I.] 2nd ed. Leusden, the
Netherlands: Nederlands Astma Fonds; 1980.
98 Oldenburg FA, Dolovich MB, Montgomery JM, Newhouse
MT. Effects of postural drainage, exercise and cough on
mucus clearance in chronic bronchitis. Am Rev Respir Dis
1979;120:739-45.
99 Rossman CM, Waldes R, Sampson D, Newhouse MT. Effect
of chest physiotherapy on the removal of mucus in patients
with cystic fibrosis. Am Rev Respir Dis 1982;126:131-5.
100 Van de Schans CP, Piers DA, Beekhuis H, Koeter GH, van de
Mark TW, Postma DS. Effect of forced expirations on mucus
clearance in patients with chronic airflow obstruction; effect
of lung recoil pressure. Thorax 1990;45:623-7.
101 Van Hengstum M, Festen J, Beurskens C, Hankel M,
Beekman F, Corstens F. Effect of positive expiratory pressure
mask physiotherapy (PEP) versus forced expiration
39
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

technique (FET/PD) on regional lung clearance in chronic
bronchitis. Eur Respir J 1991;4:651-4.
102 Olséni L, Midgren B, Hornblad Y, Wollmer P. Chest
physiotherapy in chronic obstructive pulmonary disease:
forced expiratory technique combined with either postural
drainage or positive expiratory pressure breathing. Respir
Med 1994;88:435-40.
103 Mortensen J, Falk M, Groth S, Jensen C. The effects of
postural drainage and positive expiratory pressure
physiotherapy on tracheobronchial clearance in cystic
fibrosis. Chest 1991;100:1350-7.
104 Van Hengstum M, Festen J, Beurskens C, Hankel M, van de
Broek W, Buijs W et al. The effect of positive expiratory
pressure versus forced expiration technique on
tracheobronchial clearance in chronic bronchitis. Scand J
Gastroenterol Suppl 1988;143:114-8.
105 Falk M, Kelstrup M, Andersen JB, Kinoshita T, Falk P,
Stovring S et al. Improving the ketchup bottle method with
positive expiratory pressure, PEP, in cystic fibrosis. Eur J
Respir Dis 1984;65:423-32.
106 Blake J. On the movement of mucus in the lung. J Biomech
1975;8:179-90.
107 Webber BA, Pryor JA. Physiotherapy skills: techniques and
adjuncts. In: Webber BA, Pryor JA, editors. Physiotherapy for
respiratory and cardiac problems. London, UK: Churchill
Livingstone; 1993:113-71.
108 Lannefors L, Wollmer P. Mucus clearance with three chest
physiotherapy regimes in cystic fibrosis: a comparison
between postural drainage, PEP and physical exercise. Eur
Respir J 1995;5:748-53.
109 Hofmeyr JL, Webber BA, Hodson ME. Evaluation of positive
expiratory pressure as an adjunct to chest physiotherapy in
the treatment of cystic fibrosis. Thorax 1986;41:951-4.
110 Wolff RK, Dolovich MB, Obminski G, Newhouse MT. Effects
of exercise and eucapnic hyperventilation on bronchial
clearance in man. J Appl Physiol 1977;43:46-50.
111 King M, Philips DM, Gross D, Vartian V, Chang HK, Zidulka
A. Enhanced tracheal mucus clearance with high frequency
chest wall compression. Am Rev Respir Dis 1983;128:511-5.
112 Pham QT, Peslin R, Puchelle E, Salmon D, Caraux G, Benis
AM. Respiratory function and the rheological status of
bronchial secretions collected by spontaneous expectoration
and after physiotherapy. Bull Eur Physiopath Resp
1973;9:293-311.
113 Hansen LG, Warwick WJ, Hansen KL. Mucus transport
mechanisms in relation to the effect of high-frequency chest
compression (HFCC) on mucus clearance. Pediatr Pulmonol
1994;17:113-8.
114 Thomas J, DeHueck A, Kleiner M, Newton J, Crowe J, Mahler
S. To vibrate or not to vibrate: usefulness of the mechanical
vibrator for clearing bronchial secretions. Physiother Can
1995;47:120-5.
115 Radford R, Barutt J, Billingsley JG, Hill W, Lawson H, Willich
W. A rational basis for percussion-augmented mucociliary
clearance. Respir Care 1982;27:556-63.
116 Wollmer P, Ursing K, Midgren B, Eriksson L. Inefficiency of
chest percussion in the physical therapy of chronic
bronchitis. Eur J Respir Dis 1985;66:233-9.
117 Pavia D. A preliminary study of the effect of a vibrating pad
on bronchial clearance. Am Rev Respir Dis 1976;113:92-6.
118 Groth S, Stafanger G, Dirksen H, Andersen JB, Falk M,
Kelstrup M. Positive expiratory pressure (PEP-mask)
physiotherapy improves ventilation and reduces volume of
trapped gas in cystic fibrosis. Bull Eur Physiopathol Respir
1985;21:339-43.
119 Menkes HA, Traystman RJ. Collateral ventilation. Am Rev
Respir Dis 1977;116:287-309.
120 Peters RM. Pulmonary physiologic studies of the
perioperative period. Chest 1979;76:576-84.
121 Van de Schans CP, van de Mark TW, de Vries G, Piers DA,
Beekhuis H, Dankert-Roelse JE et al. Effect of positive
expiratory pressure breathing in patients with cystic fibrosis.
Thorax 1991;46:252-6.
122 Williams MT. Chest physiotherapy and cystic fibrosis. Why
is the most effective form of treatment still unclear? Chest
1994;106:1872-82.
123 Konstan MW, Stern RC, Doershuk CF. Efficacy of the Flutter
device for airway mucus clearance in patients with cystic
fibrosis. J Pediatr 1994;124:689-93.
124 Pryor JA, Webber BA, Hodson ME, Warner JO. The flutter
VRP1 as an adjunct to chest physiotherapy in cystic fibrosis.
Respir Med 1994;88:677-81.
125 Schöni MH. Autogenic drainage: a modern approach to
physiotherapy in cystic fibrosis. J R Soc Med 1989;82:32-7.
126 Miller S, Hall DO, Clayton CB, Nelson R. Chest
physiotherapy in cystic fibrosis: a comparative study of
autogenic drainage and the active cycle of breathing
techniques with postural drainage. Thorax 1995;50:165-9.
127 Wijkstra PJ, van de Mark TW, Kraan J, Altena R van, Koeter
GH, Postma DS. Effects of home rehabilitation on physical
performance in patients with chronic obstructive
pulmonary disease (COPD). Eur Respir J 1996;9:104-10.
128 Berry MJ, Adair NE, Sevensky KS, Quinby A, Lever HM.
Inspiratory muscle training and whole body reconditioning
in chronic obstructive pulmonary disease. Am J Respir Crit
Care Med 1996;153:1812-6.
129 Strijbos JH, Koeter GH, Postma DS, van Altena R.
Reactivering van patiënten met chronische
luchtwegobstructie. [Reactivation of patients with chronic
airway obstruction.] Ned Tijdschr Fysiother 1989;99:302-7.
130 Weiner P, Azgad Y, Ganam R. Inspiratory muscle training
combined with general exercise reconditioning in patients
with COPD. Chest 1992;102:1351-6.
131 Goldstein RS, Gort EH, Stubbing D, Avendado MA, Guyatt
GH. Randomised controlled trial of respiratory
rehabilitation. Lancet 1994;344:1394-7.
132 Simpson K, Killian KJ, McCartney N, Stubbing DG, Jones
NL. Randomised controlled trial of weightlifting exercise in
patients with chronic airflow limitation. Thorax 1992;
47:70-5.
133 Cambach W, Chadwick-Straver RVM, Wagenaar RC, van
Keimpema ARJ, Kemper HCG. The effects of a community-
based pulmonary rehabilitation programme on exercise
tolerance and quality of life: a randomized controlled trial.
Eur Respir J 1997;10:104-13.
134 Ries AL, Kaplan RM, Limberg TM, Prewitt LM. Effects of
pulmonary rehabilitation on physiologic and psychosocial
outcomes in patients with chronic obstructive pulmonary
disease. Ann Intern Med 1995;122:823-32.
135 Busch AJ, McClements JD. Effects of a supervised home
exercise program on patients with severe chronic obstructive
pulmonary disease. Phys Ther 1988;68:469-74.
136 Reid WD, Warren CPW. Ventilatory muscle strength and
endurance training in elderly subjects and patients with
40
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US
chronic airflow limitation. Physiother Canada 1984;
36:305-11.
137 Reardon J, Awad E, Normandin E, Vale F, Clark B, ZuWallack
RL. The effect of comprehensive outpatient pulmonary
rehabilitation on dyspnea. Chest 1994;105:1046- 52.
138 Wijkstra PJ, van Altena R, Kraan J, Otten V, Postma DS,
Koeter GH. Quality of life in patients with chronic
obstructive pulmonary disease improves after rehabilitation
at home. Eur Respir J 1994;7:269-73.
139 Lacasse Y, Wong E, Guyatt GH, King D, Cook DJ, Goldstein
RS. Meta-analysis of respiratory rehabilitation in chronic
obstructive pulmonary disease. Lancet 1996;348:1115-9.
140 Lake FR, Henderson K, Briffa T, Openshaw J, Musk AW.
Upper-limb and lower-limb exercise training in patients
with chronic airflow obstruction. Chest 1990;97:1077-82.
141 Ries AL, Ellis B, Hawkins RW. Upper extremity exercise
training in chronic obstructive pulmonary disease. Chest
1988;93:688-92.
142 Ries AL, Archibald CJ. Endurance exercise training at
maximal targets in patients with chronic obstructive
pulmonary disease. J Cardiopulm Rehabil 1987;7:594-601.
143 Casaburi R, Patessio A, Ioli F, Zanaboni S, Donner CF,
Wasserman K. Reductions in exercise lactic acidosis and
ventilation as a result of exercise training in patients with
obstructive lung disease. Am Rev Respir Dis 1991;143:9-18.
144 Maltais F, Leblanc P, Jobin J, Bérubé C, Bruneau J, Carrier L
et al. Intensity of training and physiologic adaptation in
patients with chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 1997;155:555-61.
145 Belman MJ, Shadmehr R. Targeted resistive ventilatory
muscle training in chronic pulmonary disease. J Appl
Physiol 1988;65:2726-35.
146 Goldstein R, de Rosie J, Long S, Dolmage T, Avendano MA.
Applicability of a threshold loading device for inspiratory
muscle testing and training in patients with COPD. Chest
1989;96:564-71.
147 Levine S, Weiser P, Gillen J. Evaluation of a ventilatory
muscle endurance training programme in the rehabilitation
of patients with chronic obstructive pulmonary disease. Am
Rev Respir Dis 1986;133:400-6.
148 Ries AL, Moser KM. Comparison of isocapnic
hyperventilation and walking exercise training at home in
pulmonary rehabilitation. Chest 1986;90:285-9.
149 Gigliotti F, Spinelli A, Duranti R, Gorini M, Goti P, Scano G.
Four-week negative pressure ventilation improves
respiratory function in severe hypercapnic COPD patients.
Chest 1994;105:87-94.
150 Patessio A, Rampulla C, Fracchia C, Joli F, Majani U, de
Marchi A et al. Relationship between the perception of
breathlessness and inspiratory resistive loading: report on a
clinical trial. Eur Respir J Suppl 1989;7:587s-91s.
151 Larson JL, Kim MJ, Sharp JT, Larson DA. Inspiratory muscle
training with a pressure threshold breathing device in
patients with chronic obstructive pulmonary disease. Am
Rev Respir Dis 1988;138:689-96.
152 Preusser BA, Winningham ML, Clanton TL. High- vs low-
intensity inspiratory muscle interval training in patients
with COPD. Chest 1994;106:110-7.
153 Heijdra YF, Dekhuijzen PNR, van Herwaarden CLA,
Folgering HTM. Nocturnal saturation improves with target-
flow inspiratory muscle training in patients with COPD. Am
J Respir Crit Care Med 1996;153:260-5.
154 Harver A, Mahler DA, Daubenspeck JA. Targeted inspiratory
muscle training improves respiratory muscle function and
reduces dyspnea in patients with chronic obstructive
pulmonary disease. Ann Intern Med 1989;111:117-24.
155 Lisboa C, Villafranca C, Leiva A, Cruz E, Pertuze J, Borzone
G. Inspiratory muscle training in chronic airflow limitation:
effect on exercise performance. Eur Respir J 1997;10:537-42.
156 Wanke T, Formanek D, Lahrmann H, Brath H, Wild M,
Wagner C et al. The effects of combined inspiratory muscle
and cycle ergometer training on exercise performance in
patients with COPD. Eur Respir J 1994;7:2205-11.
157 Donner CF, Howard P. Pulmonary rehabilitation in chronic
obstructive pulmonary disease (COPD) with
recommendations for its use. Eur Respir J 1992;5:266-75.
158 Belman MJ, Warren CB, Nathan SD, Chon KH. Ventilatory
load characteristics during ventilatory muscle training. Am J
Respir Crit Care Med 1994;149:925-9.
159 Belman MJ, Thomas SG, Lewis MI. Resistive breathing
training in patients with chronic obstructive pulmonary
disease. Chest 1986;90:662-9.
160 Gosselink R, Wagenaar RC, Decramer M. Reliability of a
commercially available threshold loading device in healthy
subjects and in patients with chronic obstructive pulmonary
disease. Thorax 1996;51:601-5.
161 Younes M. Determinants of thoracic excursions during
exercise. In: Whipp BJ, Wasserman K, editors. Exercise
pulmonary physiology and pathophysiology. vol 52. New
York: Marcel Dekker; 1991.
162 Ninane V, Rypens F, Yernault JC, de Troyer A. Abdominal
muscle use during breathing in patients with chronic airflow
obstruction. Am Rev Respir Dis 1992;146:16-21.
163 Reybrouck T, Wertelaers A, Bertrand P, Demedts M.
Myofeedback training of the respiratory muscles in patients
with chronic obstructive pulmonary disease. J Cardiopulm
Rehabil 1987;7:18-22.
164 Sergysels R, Willeput R, Lenders D, Vachaudez JP,
Schandevyl W, Hennebert A. Low-frequency breathing at
rest and during exercise in severe chronic obstructive
bronchitis. Thorax 1979;34:536-9.
165 Sharp JT, Druz WS, Moisan T, Foster J, Machnach W.
Postural relief of dyspnea in severe chronic obstructive
pulmonary disease. Am Rev Respir Dis 1980;122:201-11.
166 Druz WS, Sharp JT. Electrical and mechanical activity of the
diaphragm accompanying body position in severe chronic
obstructive pulmonary disease. Am Rev Respir Dis
1982;125:275-80.
167 O’Neill S, McCarthy DS. Postural relief of dyspnea in severe
chronic airflow limitation: relationship to respiratory muscle
strength. Thorax 1983;38:595-600.
168 Tiep BL, Burns M, Kao D, Madison R, Herrera J. Pursed-lips
breathing training using ear oximetry. Chest 1986;
90:218-21.
169 Thoman RL, Stoker GL, Ross JC. The efficacy of pursed-lips
breathing in patients with chronic obstructive pulmonary
disease. Am Rev Respir Dis 1966;93:100-6.
170 Gosselink RAAM, Wagenaar RC, Sargeant AJ, Rijswijk H,
Decramer MLA. Diaphragmatic breathing reduces efficiency
of breathing in chronic obstructive pulmonary disease. Am J
Respir Crit Care Med 1995;151:1136-42.
171 Sinclair DJM, Ingram CG. Controlled trial of supervised
exercise training in chronic bronchitis. BMJ 1980;1:519-21.
172 Cockcroft AE, Saunders MJ, Berry G. Randomised controlled
41
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US

trial of rehabilitation in chronic respiratory disability.
Thorax 1981;36:200-3.
173 Rosser R, Guz A. Psychological approaches to breathlessness
and its treatment. J Psychosom Res 1981;25:439-47.
174 Haas F, Salazar-Schicchi J, Axen K. Desensitization to
dyspnea in chronic obstructive pulmonary disease. In:
Casaburi R, Petti TL, editors. Principles and practice of
pulmonary rehabilitation. Philadelphia: WB Saunders; 1993.
175. Thornby MA, Haas F, Axen K. Effect of distractive auditory
stimuli on exercise tolerance in patients with COPD. Chest
1995;107:1213.
176 Kanters HW. Effectiviteit van patiëntenvoorlichting. Een
literatuuronderzoek. [Effectiveness of patient education. A
literature review.] Utrecht, the Netherlands: Landelijk
Centrum Dienstverlening; 1986.
177 Van Burgt M, Verhulst F. Doen en blijven doen.
Patiëntenvoorlichting in de paramedische praktijk. [Patient
education in paramedical practice.] Houten/Diegem, the
Netherlands: Bohn Stafleu Van Loghum; 1996.
178 Hoenen JAJH, Tielen LM, Willink AE. Patiëntenvoorlichting
stap voor stap: suggesties voor de huisarts voor de aanpak
van patiëntenvoorlichting in het consult. [Patient education
step by step: suggestions for the primary care physician in
approaching patient education during consultation.]
Uitgeverij voor gezondheidsbevordering Stichting O&O;
1988.
179 Knibbe NE, Wams HWA. Met patiëntenvoorlichting
methodisch werken aan therapietrouw. [Using patient
education to work methodically on therapeutic compliance.]
Ned Tijdschr Fysiother 1994;maart:44-51.
180 Dekkers F. Patiëntenvoorlichting: de onmacht en de pijn.
[Patient education: the powerlessness and the pain.] Baarn,
the Netherlands: Ambo; 1981.
181 Van Broek AHS. Patient education and chronic obstructive
pulmonary disease. 1995.
182 Sluijs EM. Patient education in physical therapy. 1991.
183 KNGF. Richtlijnen voor de fysiotherapeutische
verslaglegging. [Guidelines for physiotherapeutic report-
writing.] Amersfoort, the Netherlands: KNGF; 1993.
184 Cox NJM. Effects of a pulmonary rehabilitation programme
in patients with obstructive lung disease. Amsterdam, the
Netherlands: Thesis Publishers; 1990.
185 Guyatt GH, Berman LB, Townsend M, Pugsley SO, Chambers
LW. A measure of quality of life for clinical trials in chronic
lung disease. Thorax 1987;42:773-8.
186 Wijkstra PJ, ten Vergert EM, van Altena R, Otten V, Postma
DS, Kraan J et al. Reliability and validity of the chronic
respiratory questionnaire (CRQ). Thorax 1994;49:465-7.
187 Jones PW, Quirck FH, Baveystock CM. The St George’s
Respiratory Questionnaire. Respir Med 1991;85(suppl B):
25-31.
188 Jones PW, Quirck FH, Baveystock CM, Littlejohns P. A self-
complete measure of health status for chronic airflow
limitation. The St George’s Respiratory Questionnaire. Am
Rev Respir Dis 1992;145:1321-7.
189 Bekkering GE, Hendriks HJM, Chadwick-Straver RVM,
Gosselink R, Jongmans M, Paterson WJ et al. Richtlijn voor
het fysiotherapeutisch handelen bij patiënten met
chronische obstructieve longaandoeningen. Achtergronden
en evaluatie van de richtlijn COPD. [Guidelines for
physiotherapeutic management of patients with chronic
obstructive pulmonary disease. Background and evaluation
of the COPD guidelines.] Amersfoort, the Netherlands: NPi;
1998.
190 Werkgroep “Voorlichting aan CARA-patiënten”.
Voorlichting aan CARA-patiënten. Praktijk, theorie,
aanbevelingen. [Steering group “Information for CNSLD
patients.” Information for CNSLD patients. Practice, theory,
advice.] Utrecht, the Netherlands: Landelijk centrum GVO;
1988.
191 Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R,
Yernault JC. Lung volumes and forced ventilatory flows. Eur
Respir J 1993;6:5-40.
192 Rochester D, Arora NS. Respiratory muscle failure. Med Clin
North Am 1983;67:573-98.
193 Mathiowetz V. Reliability and validity of grip and pinch
strength measurements. Crit Rehab Phys Rehab Med
1991;2:201-12.
194 Garrett H, Vathenen S, Hill RA, Ebden P, Britton JR,
Tattersfield AE. A comparison of six- and twelve-minute
walk distance with 100-metre walk times in subjects with
chronic bronchitis. Thorax 1986;41:245.
195 Ries AL, Farrow JT, Clausen JL. Accuracy of two ear
oximeters at rest and during exercise in pulmonary patients.
Am Rev Respir Dis 1985;132:685-9.
196 Wilson RC, Jones PW. A comparison of the visual analogue
scale and modified Borg scale for the measurement of
dyspnoea during exercise. Clin Sci 1989;76:277-82.
42
KNGF-guidelines for physical therapy in patients with chronic obstructive pulmonary disease
V-03/2003/US