clinical practice guidelines for pelvic girdle pain in the
TRANSCRIPT

1
Clinical Practice Guidelines for Pelvic Girdle Pain in the Postpartum Population
Adrienne H. Simonds, PT, PhD; Karen Abraham, PT, PhD; Theresa Spitznagle, PT, DPT, WCS
Department of Rehabilitation and Movement Sciences (Dr Simonds), Rutgers, The State University of New Jersey, Newark, New Jersey; School of Health Professions (Dr Abraham), Shenandoah University, Winchester, Virginia; Division of Physical Therapy (Dr Spitznagle), Program in Physical Therapy Washington University School of Medicine, Saint Louis, Missouri
Correspondence: The Guideline team welcomes comments on the guideline. Reviewer feedback should be provided via the Google form. This document should not be distributed.
Grant Support: This Guideline was supported by grants from the APTA and the Academy of Pelvic Health Physical Therapy (formerly the Section on Women’s Health). The authors are members of the APTA and Academy of Pelvic Health Physical Therapy, both of which provided funds for travel to meetings and clerical services in support of the guideline. Funding sources did not influence the content or process of development of the guideline.
Acknowledgements: The Guideline team would like to thank the APTA and Academy of Pelvic Health Physical Therapy for their support.
INTRODUCTION
Aim of the Guidelines
The Academy of Pelvic Health Physical Therapy (APHPT) of the American Physical Therapy Association (APTA) is committed to creating evidence-based practice guidelines for women’s health physical therapy management of patients with musculoskeletal impairments. The purposes of this clinical guideline are to describe evidence-based physical therapy practice including screening, diagnosis, prognosis, intervention, and assessment of outcome for women with postpartum pelvic girdle pain (PP-PGP). Specific aims include:
• Define common terminology related to PP-PGP, • Identify appropriate outcome measures to assess changes resulting from
physical therapy interventions, • Identify interventions supported by current best evidence to address impairments
of body function and structure, activity limitations, and participation restrictions associated with common musculoskeletal conditions,

2
• Provide information to inform stakeholders regarding the care of women with PP-PGP, and
• Create a reference publication for clinicians, academic instructors, clinical instructors, students, interns, residents, and fellows regarding the best current practice regarding PP-PGP.
Statement of Intent
This guideline is not intended to be construed or to serve as a standard of clinical care. Standards of care are determined on the basis of all clinical data available for an individual patient and are subject to change as scientific knowledge and technology advance and patterns of care evolve. These parameters of practice should be considered guidelines only. Adherence to them will not ensure a successful outcome in every patient, nor should they be construed as including all proper methods of care or excluding other acceptable methods of care aimed at the same results. The ultimate judgment regarding a particular clinical procedure or treatment plan must be made in light of the clinical data presented by the patient, the diagnostic and treatment options available, and the patient’s values, expectations, and preferences. However, we suggest that the rationale for significant departures from accepted guidelines be documented in the patient’s medical records at the time the relevant clinical decision is made.
Pelvic Girdle Pain
Pelvic girdle pain (PGP) is defined as “pain experienced between the posterior iliac crest and the gluteal fold, particularly in the vicinity of the sacroiliac joint (SIJ). The pain can radiate into the posterior thigh and can occur in conjunction with pain in the symphysis”.1 This operational definition of PGP was utilized in the construction of the search strategy and creation of these recommendations. Based on this definition of PGP, pubic PS (PS) pain was included in the guideline, as some clients with PGP will report both anterior and posterior pelvic pain.
Pelvic girdle pain is a condition that may result from pregnancy or other factors. The etiology and pathogenesis of PP-PGP is not well-understood. Pelvic girdle pain may develop during pregnancy and continue into the postpartum period. It may also develop after delivery and its clinical course appears independent of pain in pregnancy. These differences in onset time of PGP are important, as little is known about which individuals in pregnancy will develop pain and which individuals postpartum will develop pain.
This is not a guideline on delivery-related trauma to the pelvis. Delivery-related trauma to the pelvis has not been correlated to PP-PGP specifically, but has been linked to PS rupture/diastasis and pain, coccydynia and pelvic fractures (which are covered in medical screening and differential diagnosis sections of this guideline). Coccyx pain, or coccydynia, is a condition where the location and mechanism of pain differs from PP-PGP,2 and therefore was not included in this guideline. Clients with coccyx pain would need to be examined and treated differently than those with PP-PGP. Additionally,

3
unique interventions such as intrarectal mobilization and soft tissue work are specific to the condition of coccydynia and not to the condition of PP-PGP. For these reasons, coccydynia was excluded in this guideline.
Defining the Postpartum Period
The postpartum period is often defined as the time from delivery through the first 6 to 8 weeks. However, because not all physical changes return to pre-pregnancy states during that time, sources identify women as postpartum for up to 12 months after delivery.3,4 The authors completed the search strategy based on both the 6 to 8-week and 12-month operational definitions of postpartum, but too few results were identified in these searches. As a result, the authors revised the operational definition of postpartum for this guideline to refer to the time period from delivery through the second postpartum year.
Medical care postpartum, including screening and knowledge of PP-PGP, is variable both internationally and domestically. The World Health Organization recommends at least 3 additional postnatal contacts for mother and newborn should occur on day 3, between 7 and 14 days, and at 6 weeks, including home visits within the first week and a screening for back pain.5 The American College of Obstetricians and Gynecologists (ACOG) has redefined the postpartum period to include a fourth trimester and recommends contact with a maternal care provider within the first 3 weeks and a comprehensive visit including physical, social and psychological health within 12 weeks.4 The role of lactation is important, as studies show that hormonal levels in nursing women continue to be elevated similar to that of pregnancy. Women should therefore be followed by medical providers until cessation of lactation. Most women who continue to breastfeed or pump beyond the first postpartum year conclude around the second postpartum year. We propose that all women who continue to breastfeed or pump be considered within the fourth trimester.
Currently there is no recommendation for screening for PP-PGP or the potential physical disability associated with this condition in the postpartum period. As a result, no recommendations for physical therapy referrals are listed for this condition in published maternal care guidelines. Access to physical therapists for PP-PGP evaluation is also variable.6
Associated Physical Changes That Occur Postpartum
Physical changes associated with the effects of pregnancy, trauma during labor and delivery and physiological recovery processes in the postpartum period impact the clinical presentation, examination and interventions provided to women with PP-PGP after delivery. The primary focus of this guideline is on the specific condition of PGP in the postpartum population. Recommendations made are based on current evidence and best practice. When literature on PGP in postpartum women existed, recommendations were made regarding secondary postpartum physical health impairments, such as abdominal and pelvic floor muscle weakness. However, when literature was not specific to PGP in the postpartum population, the authors did not make a recommendation for practice. Readers are encouraged to seek alternative sources for references on the

4
assessment and rehabilitation of physical changes in the postpartum client associated with the effects of pregnancy, trauma during labor and delivery, and/or the normal physiological recovery processes that are independent of PP-PGP.
METHODOLOGY
Search Strategy
A comprehensive literature search was performed from May 2015 through December 2020 in the following databases: PubMed (National Center for Biotechnology Information), CINAHL (EBSCO), Cochrane Library (Wiley), Web of Science (Thomson Reuters) and PEDro (Centre for Evidence-Based Physiotherapy). A combination of keywords and subject headings were used. The primary search terms used were: pelvic girdle pain, low back pain, lumbosacral region, lumbopelvic, postpartum period, physical therapy modalities and exercise therapy. Articles were included if they were written in English and related to risk factors, diagnosis, medical screening, examination, outcome measures, prognosis, intervention or models of care for PGP in the postpartum population. Research designs included Randomized Controlled Trials (RCTs), cohort, case series and case reports. Articles were excluded if they discussed cancer-related pelvic pain or perineal pain, were not specific to postpartum women with PGP, or were poster or conference abstracts. Articles on pregnancy-related PGP were included only if a postpartum data was provided. A reference librarian verified the search.
Clinical Questions Searched
The authors designed the guideline search strategy to investigate the following clinical questions:
• What risk factors are most associated with PP-PGP? • What medical screening procedures should be performed with PP- PGP? • What physical therapy examination, outcome measures and diagnoses are
most valid, reliable and clinically useful for PP- PGP? • What do we know about the prognosis for recovery from PP-PGP? • What theoretical models of care are available to best guide interventions for
PP-PGP? • What physical therapy interventions are most effective and clinically useful for
PP-PGP?
Evidence Appraisal, Level of Evidence Recommendations, and Grade Assignments
Once the search strategy was complete, the authors independently screened titles and abstracts based on inclusion and exclusion criteria described above. Titles and abstracts were screened by 2 authors independently for inclusion. Additionally, 2 authors independently appraised included articles. The level of evidence definitions and recommendation grading system outlined in the APTA Clinical Practice Guidelines Manual7 was utilized (Table 1). A third author was consulted to resolve any

5
discrepancies. Extracted critical elements were entered into an Excel data file. In the presence of 2 or more articles that were well-done and provided consistent evidence, a strong recommendation was made. In the presence of either 1 well-done article OR weaker articles that provided consistent evidence, a moderate recommendation was made. In the presence of conflicting evidence or lower quality studies, a weak recommendation was made. In the absence of evidence, expert opinion was provided. Aggregate analysis of the literature was done to determine an overall level of evidence. Table 2 provides the definitions of the Aggregate Evidence Levels.
RECOMMENDATIONS
RISK FACTORS
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence that individuals are more likely to develop PP-PGP if there is a prior history of lumbar or PGP, including PGP during pregnancy.
There is moderate evidence that pain location in the posterior pelvis; pain with rolling in bed and with weight bearing; multiparity; Cesarean delivery; presence of depressive symptoms; higher BMI, work dissatisfaction and lactation are associated with the development of PP-PGP. There is weak evidence for the following risk factors as associated with PP-PGP: maternal age; maternal height; fetal weight; epidural anesthesia; and duration of second stage of labor.
MEDICAL SCREENING
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence that mood disorders are common postpartum. Mood disorders may begin up to 4 weeks postpartum, and there is an increased incidence at 2 to 3 years after delivery. PTs should administer a depression index to screen for mood disorders postpartum; screen for suicidal ideation; refer to psychological, gynecological or primary care providers for depressive symptoms; and refer to the emergency department in the presence of suicidal ideation.
Aggregate Evidence Level II Grade of Recommendation: B
There is moderate evidence that postpartum women (with or without c/o PP-PGP) are at risk for muscle impairments in the pelvic floor, abdominal, hip and back regions following pregnancy and delivery. PTs should screen for urinary and fecal incontinence; perform abdominal wall, back and hip strength testing; and refer to a pelvic health physical therapist should patients report urinary and/or fecal incontinence symptoms.

6
Aggregate Evidence Level III Grade of Recommendation: C
There is weak evidence that delivery may result in injury to the pudendal nerve resulting in denervation of the perineal muscles, abnormal sensation and/or sexual dysfunction. Radicular symptoms (sensory and strength impairments in a lower extremity) with a history of traumatic or prolonged labor may also be present. PTs should perform a lower quarter neurological assessment including sensory and motor assessment of the perineal region and pelvic floor and refer for medical examination of the lumbosacral plexus in the presence of distal neurologic symptoms.
Aggregate Evidence Level IV
Grade of Recommendation: C
There is weak evidence that women with PP-PGP may present with femoral neck or sacral fractures to secondary low bone mineral density (BMD). There is weak evidence that breastfeeding is associated with reduced BMD. There is weak evidence that heparin use during pregnancy is associated with transient osteoporosis. PTs should screen for activity-associated pain that improves with rest, breastfeeding status postpartum, and heparin use in pregnancy, delivery or postpartum. PTs should perform boney palpation over site(s) of pain. PTs should refer for magnetic resonance imaging (MRI) to rule out stress fracture when a patient presents within 2 weeks of delivery with any of the following complaints: severe pain; decreased or inability to weight bear; antalgic gait or limp; sudden onset of pain located at SIJ, buttocks, low back, or PS; or pain relieved with lying down.
EXAMINATION
Aggregate Evidence I Grade of Recommendation: A
There is strong evidence for a consistent clinical presentation of PP-PGP that involves: pain location in the posterior pelvis in the region of the SIJ and/or anterior pain at the PS, pain with rolling in bed, and pain with lower extremity (LE) weight bearing. PTs should inquire about location of pain, pain with rolling, and pain with LE weight bearing.
Aggregate Evidence Level III Grade of Recommendation: C
There is moderate evidence validating the use of the Oswestry Low Back Pain Disability Questionnaire, and the Pelvic Girdle Questionnaire, and weak evidence validating the use of the Quebec Back Pain Disability Scale to measure disability associated with PP-PGP. These measures are appropriate for use as part of examination of women with PP-PGP.
Aggregate Evidence Level V

7
Grade of Recommendation: P
Alignment testing of pelvic girdle bony landmarks is common in physical therapy practice, but has inconsistent evidence for its reliability and validity, especially in PP-PGP. PTs may perform alignment testing at pelvic landmarks to determine the presence of asymmetry during the examination; however, this should not be performed in isolation.
Aggregate Evidence Level: V
Grade of Recommendation: P
There is no evidence specific to the postpartum population to support palpation of the PS to rule in the presence of anterior PP-PGP. PTs may palpate the PS as part of a comprehensive examination of the pelvic girdle, as both posterior and anterior pain symptoms may be present. Anterior pain at the PS warrants a different clinical decision-making process. Aggregate Evidence Level: V
Grade of Recommendation: P
There is limited evidence to support palpation of the long dorsal ligament (LDL) test specific to the postpartum population. The lack of agreement among the LDL, Posterior Pelvic Pain Provocation (P4) and Active Straight Leg Raise (ASLR) tests in non-severe case presentations suggest that the tests do not assess the same structures and/or function in postpartum women without severe PGP. PTs may perform the LDL test, but this test should not be performed in isolation.
Aggregate Evidence Level II-III Grade of Recommendation: A B
There is strong evidence to support the use of the Posterior Pelvic Pain Provocation (P4) Test and moderate evidence to support the use of the Flexion-Abduction-External Rotation (FABER) Test to rule in PP-PGP. PTs should perform the P4 Test. PTs may perform additional provocation tests as necessary to confirm the location of pain and irritability of the structures.
Aggregate Evidence Level V Grade of Recommendation: P
The PS experiences laxity, trauma, and/or pain associated with pregnancy and delivery. PTs should not perform Gaenslen’s test in the first 4 weeks postpartum or beyond 4 weeks postpartum in the presence of PS pain.
Aggregate Evidence Level V Grade of Recommendation: C

8
There is weak evidence to support the use of the Modified Trendelenburg Test for women with PP-PGP. Standing tests may reproduce symptoms in the presence of impaired loading response. Based on strong evidence for pain reproduction with limb loading, PTs should perform standing examination tests including: double limb support, single limb support, and transitional movements, to observe and assess the level of difficulty, presence of pain, and movement impairments during trunk and limb movements. Future research on PP-PGP should include standing single limb loading tests for determining pain and movement impairments.
Aggregate Evidence Level II Grade of Recommendation: A
There is strong evidence that the Active Straight Leg Raise (ASLR) test allows for the assessment of supine limb loading. The ASLR test assesses the ability of both bony and muscle systems to provide appropriate stabilization of the pelvic girdle to allow for pain-free movement of the lower extremities. PTs should perform the ASLR for PP-PGP.
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence that muscle function is impaired in PP-PGP. There is evidence to suggest that at a minimum the following should be assessed: force production, endurance, resting muscle tone, and muscle length. Muscle function is an important element to include in the PT examination of clients with PP-PGP.
Aggregate Evidence Level V Grade of Recommendation: C
There is weak evidence to support the examination of diastasis rectus abdominis (DRA) in women with PP-PGP. There is moderate evidence to suggest that the presence of DRA impacts the function of the abdominal wall and pelvic floor muscles. PTs may perform DRA assessment for PP-PGP. Future research should investigate a potential relationship between DRA and PP-PGP.
PROGNOSIS
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence to suggest that prognosis of recovery depends on initial pain and disability scores. There is strong evidence to suggest that women with greater disability and pain scores should be expected to recover more rapidly and return to function. There is strong evidence to suggest that women with low disability scores and low pain scores at the start of physical therapy intervention demonstrate minimal gains. PTs should assess pain level and administer a disability questionnaire to inform prognosis. Future research should investigate fear-avoidance behaviors and mental health to potentially identify women not following a “normal” course of recovery after PP-PGP.
9
There is strong evidence to suggest that women who present to PT beyond 3 months after delivery may experience minimal to no gains with intervention. PTs should advocate for initiating care in early postpartum (before 3 months postpartum) to reduce likelihood of chronic PP-PGP.
Regardless of intervention, there is strong evidence to suggest that women may continue to experience low disability and/or pain at 1 year and at 2 years postpartum. It is unclear if this is based on pre-existing or comorbid conditions or if this is related to a natural progression of recovery from pregnancy and childbirth. Future research should investigate the implication of these confounding variables on continued pain and disability at 1 and 2 years postpartum.
INTERVENTION
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence to support the inclusion of patient education on PP-PGP, normal changes postpartum and body mechanics in the intervention. PTs may educate clients on pain and physiology behind PP-PGP and normal changes postpartum. PTs may instruct clients on functional movement strategies associated with activities of daily living (ADLs) and childcare tasks. Future research should explore educational methods for PP-PGP in relation to outcome.
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence to support the use of a pelvic belt for PP-PGP in conjunction with co-interventions, such as education, functional training, and exercise. PTs should not use a pelvic belt in isolation.
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence that the use of manual therapy interventions is no better than stabilization exercises for long term > 6 months improvement in outcomes. There is strong evidence for the use of manual therapy in conjunction with co-interventions to provide short term improvements in pain and disability in PP-PGP. PTs should not apply manual therapies in isolation.
Aggregate Evidence Level V
Grade of Recommendation: P
Based on the wide use of patient education and ergonomic advice in intervention studies, PTs may consider functional training as an intervention for PP-PGP. Functional training has not specifically been studied in PP-PGP. Future research should implement

10
functional training, including gait, double-limb, single-limb, transitional movements, ADLs/IADLs, and child care tasks.
Aggregate Evidence Level I Grade of Recommendation: A
There is strong evidence to support the use of exercise to improve performance of pelvic floor, back flexors, back extensors, and hip extensors. There is strong evidence to suggest that improving performance of musculature does not consistently improve pain and disability in women with PP-PGP. PTs should prescribe exercise to address muscle performance impairments. PTs should not prescribe exercise that is painful. PTs may instead consider co-interventions, such as education, pelvic belt, an assistive device for gait, functional training, and/or manual therapy until tolerance to exercise improves.
THEORETICAL MODELS OF CARE
Aggregate Evidence Level V
Grade of Recommendation: P
There is limited evidence to support the use of a specific theoretical model for the diagnosis/classification and subsequent intervention for PP-PGP. Patho-anatomical models of care fail to direct decisions on intervention. Examination and intervention studies suggest that impaired limb loading is a primary movement impairment for PP-PGP. Future research should consider classification systems that include examination for both pain location and movement impairments in PP-PGP.
Summary
Please refer to online materials for details associated with each recommendation, as well as literature summary tables. The authors propose a hybrid diagnostic model that includes examination of both pain location and movement impairments to assess and classify PP-PGP. The aim of this hybrid model is to include examination for symptomatic joints as well as the specific patterns of movement that contribute to impaired load transfer of the pelvic girdle.8 The authors propose 3 classifications of PP-PGP: 1) sacroiliac joint load transfer impairment with or without asymmetry (unilateral joint involvement), 2) pelvic girdle load transfer impairment (2 or more joints involved),3) pubic symphysis load transfer impairment. The Clinical Decision-Making (CDM) Flowchart for PP-PGP (Figure 1) facilitates implementation of this proposed PP-PGP classification into clinical practice. The CDM Flowchart is designed to help readers select appropriate tests and measures to determine a specific diagnosis that can subsequently direct intervention strategies. Decisions are based on pain location, pain response to treatment, presence of asymmetry, and movement impairments contributing to the presenting load transfer impairments.

11
MANUSCRIPT BODY
RISK FACTORS Pain in pregnancy can be predictive of pain postpartum, therefore where applicable studies that correlate clinical presentation during pregnancy with persistent pain postpartum are represented in this summary. There is a specific subset of women that develop PP-PGP that did not experience PGP during pregnancy. It is unclear what mechanisms contribute to differences in pain onset. See Table 3 for details associated with risk factors in women experiencing PP-PGP.
There is strong evidence that the following risk factors that contribute to experiencing PP-PGP; history of prior lumbar and/or PGP,9-14 location of pain in the posterior or anterior aspect of the pelvis during pregnancy,9,10,15-18 high level of disability at day one postpartum19,20, Cesarean section delivery,14,21-23 postpartum pain with turning in bed and weight bearing,10,19 and >2 provocative tests during pregnancy.11,15,21,22 Modifiable risk factors that PTs may address include pain with activity during pregnancy, physical therapy care for women immediately post-Cesarean delivery or for women with a high level of disability or pain immediately postpartum.
MEDICAL SCREENING
Screening during the postpartum period has been organized to highlight system and tissue considerations for medical referrals and/or specific physical therapy examination tests to guide clinical decision-making. Pain in the lumbopelvic region in the postpartum population may be associated with conditions that warrant a medical referral, such as: inflammatory, infective, traumatic, neoplastic, degenerative or metabolic disorders. The physical therapist should proceed with caution and consider a medical referral for any history of trauma, unexplained weight loss, history of cancer, steroid use, substance abuse, human immunodeficiency virus or immunosuppressed state, neurological symptoms or signs, fever, and/or feelings of malaise. The PT should complete a review of systems as part of the physical therapy examination to identify signs and symptoms of medical disorders and refer as appropriate. Failure to achieve functional improvements and/or lumbopelvic pain that does not reduce with rest, and/or severe, disabling pain may also require a medical referral.
Pregnancy negatively impacts bone mineral density, which does not immediately resolve postpartum. Studies have demonstrated average BMD decreases with loss of trabecular bone of 1.8 to 3.4% in the lumbar spine, 3.2±0.5% at the hip, 4.3% in the femoral neck, 4.2±0.7% at the distal forearm and 6% at the calcaneus across trimesters in the antepartum period.24 Generally, these losses in BMD resolve within 6 months of delivery 24 but can be prolonged in women who breastfeed or those who take blood-thinners such as heparin.25-27 Low BMD may increase risk of fracture when associated
12
with unusual forces. Therefore, a complete history should include lactation status, birth history and activity profile for a complete understanding of risk of compromised bone integrity. The hip and sacrum are the most common postpartum sites of loss of bone integrity. Symptoms associated with hip and/or sacral fracture may include groin pain, pain that radiates to the hip, severe pain with weight bearing that is relieved when lying supine, and altered/antalgic gait. Clinical examination may reveal pain with provocation testing, palpation, and motion testing in multiple directions but the gold standard for diagnosis of bony compromise is the MRI.28-30
The joints of the pelvic ring are particularly susceptible to injury due to the presence of abnormal forces, the laxity induced during pregnancy, and trauma associated with delivery.31 A prospective case control study by Wurdinger et al32 compared pelvic MRI images of 19 postpartum women 2-5 days post-delivery with images from 11 healthy, nulliparous women. The images revealed a larger gap in the pelvic ring joints and signal changes in the pubic cartilage in 8/13 asymptomatic and 5/6 symptomatic postpartum women as compared to the nulliparous women. Of the 6 symptomatic women, MRI revealed SIJ lesions (2/6) and PS rupture (1/6). The patients reported symptoms including PP-PGP that radiated to the hips and waddling gait. Therefore, all postpartum women should be screened for functional impairments that indicate asymmetrical loss of the integrity of the pelvic girdle (pain with rolling, single limb stance, stairs, asymmetrical sitting). Severe pain in the anterior PS, paint to touch, difficulty weight bearing, and/or urinary symptoms may suggest PS diastasis.33 When PS diastasis is suspected, referral for imaging is warranted.
It is important to differentiate between musculoskeletal dysfunction and systemic issues that may affect the joints. Musculoskeletal dysfunctions associated with the hip can include bursitis/tendonitis, chondral damage/loose bodies, capsular laxity, femoral acetabular impingement, and labral irritations/tears. Hip pain that warrants a medical referral may include systemic issues such as infection, Paget’s disease, rheumatoid, psoriatic, and septic arthritis, and/or hematoma which have all been reported postpartum.34-36 The clinical presentation of hip pain of a systemic origin is similar to that of hip pain of musculoskeletal origin with complaints of difficulty with gait, and bilateral buttock pain within the first 2 weeks postpartum. Musculoskeletal and systemic causes can be differentiated by the presence of fever in the systemic cases.37-41 Pain complaints in the anterior abdominal wall and/or perineum in the postpartum period may also be associated with non-musculoskeletal conditions. It is important to consider the presence of uterine rupture, umbilical hernia, infection, obstetric fistula, and/or incomplete delivery of the placenta as possible causes. Once again, the symptoms in these more severe conditions may mimic musculoskeletal causes. For example, Tennfjord et al42 reported that women with obstetric fistula commonly experienced complaints of leg pain, difficulty walking, and reduced function in the ankle and knee joints post-delivery. Differentiating factors include a greater severity of the pain, presence of associated signs/symptoms (fever, severe bleeding, ballooning of the abdominal region, continuous stool or urine loss), and/or failure to improve. The presence of any of these symptoms would warrant an immediate physician referral.

13
The physical therapist should also rule out the presence of lumbar spine dysfunctions which may mimic PGP by the presence of pain below the posterior superior iliac spine (PSIS) with possible radiation into the buttocks and lower extremities. Such conditions may include spondylolisthesis, lumbar disc dysfunction, and/or other space occupying lesions around the spinal cord and/or nerve roots. If lumbar dysfunction is suspected, movement testing of the lumbar spine combined with a complete neurologic screen should be performed including screening for the presence of lower and upper motor neuron signs as well as bowel/bladder dysfunction.
The pelvic girdle musculature is at risk for impairments due to the physical changes associated with pregnancy as well as the trauma of delivery. Most impairments do not require immediate medical referral and are amenable to physical therapist management. However, inability to activate the pelvic floor musculature (PFM), loss of sensation (unilateral or bilateral perineal hypoesthesia) and/or urinary or fecal incontinence should initiate a referral to a physician. Inability to activate the PFM may indicate an injury to the pudendal nerve or another branch of the lumbosacral plexus. Risk factors for nerve injury include: delivery of multiple fetuses, prolonged labor, small or skeletally-immature pelvis, and instrument-assisted delivery.43-46 Symptoms such as pain in the lower back/buttock and lower extremities, foot drop, and gait dysfunction may also be associated with more severe nerve injury.
In addition to physical complaints, mood disorders are common during the postpartum period. Most postpartum women will experience the postpartum “blues'' associated with the re-balancing of hormone levels following delivery of the fetus and placenta.47 However, some women will experience clinical depression and in a limited number of severe cases, postpartum psychosis. Any suspicion of postpartum depression should warrant a referral to a physician and/or mental health practitioner. The Edinburgh Postnatal Depression Scale (EPDS) is considered the gold-standard for screening of postpartum depressive symptoms.48 Postpartum depression is likely to begin within 4 weeks of delivery, but may occur as early as one day post-delivery.49 It is considered clinically significant if the symptoms are present most of the day, nearly every day, for nearly 2 weeks. Symptoms are consistent with the DSM-IV criteria for major depression. A minimum of 5 of the following must be present in order to meet the criteria: depressed mood, severe anxiety, markedly diminished interest or pleasure with activity, appetite disturbance (loss with weight loss), sleep disturbance (insomnia and fragmented sleep), physical agitation, psychomotor slowing, fatigue, feelings of worthlessness or excessive guilt, decreased concentration, and/or recurrent thoughts of death or suicidal ideation.50-
52 A score of greater than or equal to 10 on the EPDS is considered to indicate the presence of depressive symptoms. However, any positive response to the suicidal ideation on item #10 (even with a score <10) should be considered a red flag and initiate an immediate referral to the emergency department. In addition, depression may result in somatization, and therefore should be considered when patients do not improve as expected.
EXAMINATION

14
This CPG provides clinicians with a core set of examination tests and measures supported by the best available evidence. The CPG will enable clinicians to:
• determine the presence of clinical findings associated with a PP-PGP diagnosis as described and
• identify changes in impairments, function, activity limitations, and participation restrictions over an episode of care in physical therapy.
Clinicians should choose the most appropriate measures based on the patient’s presentation, needs, and goals.
OUTCOME MEASURES
A variety of domains need to be specifically assessed in women with PP- PGP. Measures of pain, general health status and disability, postpartum quality of life, and mental health including psychological and emotional status should be conducted by the clinician. Outcome measures specifically validated in women with PP-PGP include the Oswestry Low Back Pain Disability Questionnaire (ODQ) and the Pelvic Girdle Questionnaire (PGQ). The PGQ is the only outcome measure designed specifically to evaluate impairments and functional limitations of PGP during pregnancy and postpartum.53 The PGQ includes questions from previously established functional outcome measures (Disability Related Index (DRI), ODQ, and Roland-Morris Disability Questionnaire (RMDQ)) and functional activity questions considered clinically relevant by clinicians and a patient focus group. Specific questions are asked related to perceived disability associated with pain intensity, personal hygiene, lifting, walking, sitting, standing, sleeping, sexual activity, social activity, and traveling.
The Quebec Back Pain Disability Scale (QBPDS) is a measure validated in the general population with nonspecific low back pain to measure the grade of disability.54 It is frequently used in studies as a comparison measure in studies investigating pregnancy-related PGP.55-60 However, the QBPDS has not been specifically validated in the postpartum population. See Table 4 for details associated with disability outcome measures utilized for PP-PGP.
PHYSICAL TESTS and MEASURES
Any abnormal findings identified during the screening examination should be followed up with a detailed examination. Specific recommendations for selection of procedures to rule in PP-PGP and inform the selection of interventions are detailed below. The order of physical measures presented is representative of a typical examination flow based on position. The PT should consider modification of positions based on patient mobility and tolerance.
The recommendations describe the current evidence regarding a combination of pathoanatomic (Table 5) and movement testing to confirm the location of pain and identify specific limitations that contribute to load transfer impairments. Testing for muscle performance (strength, timing/coordination, and endurance), ligament/joint

15
integrity, and performance during limb (upright) and trunk (supine) loading tasks will be discussed. Assessment for symmetrical responses to testing, i.e., agreement between testing on the right versus left sides should be emphasized due to the association between asymmetry and the presence of PP-PGP. A gold standard test is not available. Therefore, the validity of the clinical tests available is difficult to assess. Most of the physical tests/measures have a very high specificity, but lower sensitivity. Therefore, a combination of tests is likely necessary to rule out the presence of PP-PGP. Reliance on the results of a single test may result in a false negative result.
Palpation
Alignment Testing
Palpation of bony landmarks has been described to assist with identification of asymmetry of the pelvic joints but generally has not been studied in the postpartum population. Palpation may be performed in seated or standing positions. Landmarks most commonly palpated for alignment include: the iliac crests, anterior superior iliac spine (ASIS), posterior superior iliac spine (PSIS), and pubic tubercles. A number of studies have shown poor intra- and inter-tester reliability with alignment testing through palpation. In addition, asymmetry in position was not strongly associated with the presence of PGP.61 Therefore, the PT may choose to perform alignment testing but should not rely on those results in isolation to determine the diagnosis and/or intervention strategy.61-64
Pubic symphysis palpation
Though the available evidence is limited to expert opinion, palpation of the PS is an important element to include in examination of women with PP-PGP. To determine PS involvement in PP-PGP, assessment begins with palpation for pain in standing or in supine with the Symphysis Pain Palpation Test (SPPT). In the SPPT, the anterior portion of the PS is palpated. If the palpation causes pain that persists more than 5 s after removal of the examiner’s hand, it is recorded as pain. If the pain disappears within 5 s it is recorded as tenderness. Pubic symphysis palpation should not be done in isolation, joint involvement should be confirmed by provocation testing (FABER test) and standing assessment (Modified Trendelenburg Test) which are described below.65 Positive testing would indicate that the PS is involved in the anterior pain and impairments associated with limb loading should be assessed.
Long Dorsal Ligament (LDL) Palpation
Vleeming et al8,66-68 explains that the LDL becomes taut with specific motions at the SIJ and that tension across the LDL contributes to form closure at the pelvic girdle. Pain to touch in this region suggests ligamentous strain. There is weak evidence to support inclusion of palpation of the Long Dorsal Sacroiliac Ligament (LDL) in postpartum clients with posterior PP-PGP.68 The LDL Test involves palpation of the LDL directly under the caudal part of the posterior superior iliac spine (PSIS) in prone and assessment of symptom provocation. The examiner scores the pain as positive or negative on a 4-point scale: no pain=0; mild=1; moderate=2; unbearable=3. The scores on both sides are added so that the sum score can range from 0–6. Palpation of the LDL should not be done in isolation. The LDL Test is typically used in combination with

16
the Posterior Pelvic Pain Provocation Test (P4) test and the Active Straight Leg Raise Test (ASLR) (described below) with a patient presenting with lumbopelvic and/or SIJ pain.
Njoo et al69 reported high intertester reliability of LDL palpation; however, the study population was not specific to postpartum women and did not differentiate between those with lumbar sites of pain and PGP. Vleeming et al68 specifically evaluated the use of the LDL test in the postpartum population and demonstrated little agreement between results of LDL and ASLR or P4 testing in the absence of severe PP-PGP presentation. Specificity of the LDL test was found to be 0.98 only when severe case presentation patients were included. The lack of agreement among the LDL, P4 and ASLR tests in non-severe case presentations suggest that the tests do not assess the same structures and/or function in PP-PGP women without severe symptoms. Therefore, the clinical value of a positive LDL test, the reliability of LDL palpation across a diverse postpartum population, and the relationship between presence of pain at the LDL and function remain unclear.
Provocation Testing
Provocation testing is used to rule in the presence of pain at the SIJ and/or the PS. several provocation tests have been described in the pelvic girdle pain and SIJ literature. However, only 2 provocation tests - the Posterior Pelvic Pain Provocation Test (P4) and the Flexion Abduction External Rotation (FABER or Patrick’s Test) - have been specifically described in the postpartum population. Gaenslen’s test70 should not be performed within the first 4 weeks postpartum due to the risk of injury (see below). Further research should explore the mechanisms that potentially explain variability in positive testing among palpation, provocation, and load transfer testing in relation to pelvic girdle structure and function in the postpartum population.
Posterior Pelvic Pain Provocation (P4) Test
There is strong evidence to support inclusion of the P4 test to rule in PP-PGP.71-74 The P4 test is performed with the patient in the supine position with the hip and knee flexed to 90° on the side being tested. A light manual pressure is applied to the patient’s flexed knee along the longitudinal axis of the femur while the examiner stabilizes the contralateral pelvis through a force applied over the superior anterior iliac spine. The test is considered positive when the patient reports a familiar well-localized pain deep in the gluteal area on the ipsilateral side.73
FABER (Patrick’s) Test
There is moderate evidence to suggest inclusion of the FABER test to rule in PP- PGP. The FABER test is performed with the patient in supine. The limb on the painful side is placed so that the ankle is just above the knee of the contralateral limb. The examiner provides a gentle downward pressure on the knee of the painful side while stabilizing the ASIS of the non-painful side. The examiner assesses the presence and location of pain. Patients presenting with PP-PGP will often report pain posteriorly (at the PSIS) or anteriorly (at the PS) on the ipsilateral side during this test.
Gaenslen’s Test

17
Though the available evidence is limited to expert opinion, Gaenslen’s test 70,75 should be performed with caution in postpartum clients. The test is performed with the patient positioned in supine with the painful limb resting very near the end of the treatment table. The examiner raises the non-painful side hip to 90 degrees. A downward force to the painful side lower limb is applied while simultaneously applying a flexion-based counterforce to the flexed limb. A positive test is described as pain with the application of the torque across the pelvic joints. Because of the risk of PS trauma during pregnancy/childbirth, it is recommended that PTs not perform the Gaenslen’s test for the first 4 weeks postpartum or beyond 4 weeks postpartum in the presence of PS pain.
Assessment of Sacroiliac Joint Motion
Several researchers have investigated SIJ mobility and laxity in postpartum women using Doppler imaging.76,77 While SIJ laxity was elevated during pregnancy, Damen et al77 reported that mean SIJ laxity values decreased from 36 weeks pregnancy to 8 weeks postpartum and were within a normal range by 8 weeks postpartum. Asymmetric laxity of the SI joints rather than the degree of laxity was associated with PP-PGP.77 Asymmetric laxity of SIJ in pregnancy corresponded with a 2.8 relative risk ratio for moderate to severe PGP persisting at 8 weeks postpartum.76,77 No clinical measures were identified that were reliable and valid in the postpartum population for assessment of asymmetrical laxity of the pelvic girdle (SIJ and PS). Though the available evidence is limited to expert opinion, we recommend that functional assessment be used to determine asymmetrical responses to limb loading. PTs should use tests that assess limb loading, specifically ASLR and single limb standing assessments, from immediately to up to 1 year postpartum. Future research should consider the use of Doppler ultrasound in clinical practice to measure laxity.
Functional Limb Loading Assessment
The ability to stabilize the pelvis in order to allow movement of the lower extremities involves adequate co-contraction of lumbopelvic muscles and is important to return to full participation in functional activities postpartum. Functional limb loading can be assessed in standing, in supine, and through observation of functional task performance.
Active Straight Leg Raise:
There is strong evidence to support inclusion of the Active Straight Leg Raise (ASLR) in the examination of women with PP- PGP.55,56,58,59,71,74,77-79 This test assesses supine limb loading as a means to determine ability to stabilize the pelvic girdle and trunk in response to the movement of the lower extremity.80 To perform the ASLR, the patient is positioned in supine. The patient is asked to raise each limb approximately 6 inches while assessing for pain. If lifting the limb was painful, the examiner then stabilizes the pelvis by compressing the ASIS medially or by placing a belt around the pelvis. The patient is again asked to raise the affected limb approximately 6 inches. If this movement is no longer painful, the test is considered positive.57-59
A positive ASLR test is suggestive of impaired coordination of the lumbopelvic muscles. A positive test suggests that the individual would benefit from exercises to improve

18
muscle performance for stabilization in order to function optimally. A negative ASLR test in the presence of PP-PGP, generally indicates adequate levels of co-contraction of lumbopelvic muscles and appropriate force closure of the pelvic girdle.
Standing Assessment:
Standing tests for PP-PGP can be considered in 3 categories: 1-double limb support, 2-single limb support, and 3-transitional movements. Standing in double limb support is unlikely to elicit symptoms (pain or difficulty with the task) except in severe case presentations.81 Standing in single limb support or transitional movements, such as sit-to-stand, walking, and/or rolling in bed are more likely to reproduce anterior or posterior pain and/or result in abnormal movement patterns in women with PP-PGP.19,57,81,82 Though the available evidence is limited, based on common functional complaints, standing tests should be performed including, single leg stance, transition from sitting to standing, and walking.53 Clinicians should observe and assess the level of pain and degree of movement impairment of their clients during these 3 functional movement assessments in order to determine whether the individual is able to manage the transfer of the load of the trunk and pelvis over the limb. Examination that is performed solely in the seated and/or supine positions is less likely to evoke symptoms in milder dysfunction. If the individual is unable to be assessed in standing, the ASLR can be used to determine limb loading effects on pain and trunk motion in the supine position.
Traditionally, the Modified Trendelenburg Test71 (pain produced at the anterior or posterior region of the pelvic girdle during limb loading while the opposite hip is flexed to 90 degrees) the Gillet (March)83 or Stork test84,85 (palpation for mechanical locking of the sacrum and ilium during a standing hip flexion task) have been performed to determine load transfer impairments of the PS or SIJ. These types of standing tests are used to identify the location of pain (Modified Trendelenburg Test) or asymmetries in motion across the SI joint (Gillet/March or Stork). Unfortunately, the literature is silent regarding appropriateness of the Gillet (March) or Stork test in the postpartum population. Only the Modified Trendelenburg test has been reported in the PP-PGP population.15,21,22,86 Thus, future research is needed to investigate the appropriateness of the combined testing of palpation with single leg stance to objectively measure limb loading impairments in PP- PGP. There is also a need to identify other specific impairments/muscle performance issues that contribute to the load transfer impairment.
Muscle Function Assessment
Because of the enlargement of the uterus combined with weight gain and hormonal changes the abdominal, lumbar, and hip musculature are exposed to abnormal forces during pregnancy and childbirth. Postpartum women are at risk for; loss of fascial integrity of the abdominal and pelvic floor muscles; changes in resting length (abdominals, pelvic floor, thoracic back extensors muscles are lengthened; lumbar back extensors are shortened), changes in resting muscle tone, and also acute inflammation associated with the trauma of childbirth. These physical changes may lead to reduced or altered muscle function/performance.
The literature investigating what muscle function changes persist in the postpartum period is evolving. There is strong evidence to support that muscle performance

19
impairments are present in PP-PGP. However, there is limited evidence linking altered muscle performance to the presence of persistent PP-PGP. Given the lack of robust evidence to improve pain, we have assembled the available literature on muscle function and performance and operationalized this construct unique to PP-PGP.
There is strong evidence to suggest that the following should be prioritized in the specific assessment of a PP-PGP:
• timing of contraction (multifidi, abdominals, and PFM) • endurance (back extensors, trunk flexors) • strength/force production (hip extensors, back extensors, abdominals, and PFM) • resting tone/over activity (multifidi/abdominals/pelvic floor musculature)
The following tests have been described to assist in assessing muscle function.
Timing of contraction
Pregnancy and childbirth may result in altered timing of muscle contraction. The ASLR is one method that has been used to assess appropriate timing of contraction in the postpartum population. Sjodahl et al20 demonstrated delayed onset of contraction of the PFM and abdominals during the ASLR in women with PP-PGP as compared to those without pain. Surface electromyography (EMG) was utilized to measure abdominal and PFM activity.
Endurance testing
Back flexor endurance test: To test isometric endurance of back flexors, McQuade et al87 describe a supine test with arms crossed over the chest, hands on the opposite shoulders, hips bent, and knees and feet apart. Participants were asked to nod and continue to lift their head and shoulders until the inferior angle of the scapula was lifted from the surface, and maintain the position as long as possible.82 The number of seconds that the position was maintained for was recorded up to a maximum of 120 seconds.
Back extensor muscle endurance test: To measure the isometric endurance of the back extensors, participants lay prone with their arms crossed and the trunk horizontal off the table. The pelvis was fixed to the table by straps and the lower legs were held in place by the tester.88 The time that this position was maintained was recorded in seconds and the test up to a maximum of 120 seconds. This may be uncomfortable in the presence of PP-PGP. Therefore, use of this test should be used judiciously.
Resting tone
There is moderate evidence to suggest that there may be increased resting tone in the back extensors, abdominals, and/or pelvic floor musculature in women with PP-PGP. A variety of tests/measures can be used to assess the resting tone of the musculature. Over activation can be identified clinically with the use of palpation, electromyography (EMG) biofeedback, manometry, and diagnostic ultrasound (US). The strongest evidence suggests use of EMG biofeedback and/or manometry.
Force production

20
Trunk/Back flexor musculature: Moderate evidence exists that suggest that force production may be impaired in the trunk flexor musculature in women postpartum. Maximum voluntary isometric contraction (MVIC) of the trunk musculature has been used to measure force production capacity of the trunk flexors postpartum and found that postpartum women were weaker at all angles than nulliparous women.89 However, the relationship between impaired force production and the presence of PP-PGP has not been established.
Hip musculature: Moderate evidence exists that the hip musculature, in particular hip extensors should be assessed (See Table 6) due to the relationship between hip extensor weakness and the presence of PP-PGP.20,82,90 Gutke et al82 reported lower hip extension strength and gait speed in women reporting PP-PGP. Maximal voluntary isometric hip extension or adduction can be measured with a dynamometer and compared between sides. However,
functional assessment may also be warranted. Pelvic floor musculature: There is strong evidence to suggest that pelvic floor muscle function is impaired in the postpartum period. Muscle strength assessment of the PFM through manometry has been shown to be reliable and valid.91,92 PFM endurance has been defined as a sustained maximal contraction and was quantified during the first 10 s as the area under the curve.93 Manometry measurement has demonstrated higher reliability coefficients than digital muscle testing on maximum voluntary contraction strength, endurance and vaginal resting pressure.94 Weakness of PFM has not been specifically associated with PP-PGP. However, further investigation is warranted. The PFM has been found to automatically contract during the ASLR.78 However, manual compression during the ASLR reduced the automatic PFM contraction by 62-66%. There was no difference between those with PP-PGP vs. those without PP-PGP in the reduction in PFM force.78 These results suggest that the PFM performance is important in pelvic girdle stabilization, and therefore, should be assessed and any identified impairments addressed.
Muscle length: Due to the physical stresses and hormonal changes during pregnancy and childbirth, the pelvic girdle musculature is at risk for changes in muscle length postpartum. The back extensors and hip flexors are most likely to be shortened while the pelvic floor and abdominal muscles are most likely to be lengthened. At the time of this guideline, there was limited to no evidence describing reliable and valid measures of pelvic muscle length in this population. Future research should investigate the effect of muscle length changes in individuals with PP-PGP.
Diastasis Recti Abdominis Assessment: A common finding in postpartum women is Diastasis Recti Abdominis (DRA), in which the linea alba has been disrupted due to the lengthening of the abdominal wall during pregnancy. DRA has been associated with the presence of pelvic floor dysfunction,95 but no studies have specifically linked the presence of DRA with the presence of PP-PGP. The clinical assessment of DRA is generally performed with the patient in supine. The clinician observes and palpates the inter-recti distance during an active trunk flexion (actively lifting the head/shoulders off of the table).
There is no agreement as to the degree of separation that is considered clinically significant, however, an inter-recti distance greater than two finger widths at, above, or below the umbilicus warrants additional investigation. Because DRA can impact the

21
integrity and function of the abdominal wall,96 all postpartum women should be screened for the presence of DRA and an appropriate treatment plan be established when DRA is identified regardless of the presence or absence of PP-PGP. Future research should consider classifying abdominal muscle performance (over or under active) in the presence of DRA and/or pelvic floor disorders to understand contributions to PP-PGP. (See Table 7 for a summary of the literature associated with DRA.)
DIAGNOSIS/CLASSIFICATION
Pelvic girdle pain in the postpartum client may resemble that of pregnancy-related PGP or pelvic girdle pain syndromes in the non-pregnant population. Several theoretical classification models – biopsychosocial97,98, pathoanatomic75,99, treatment based100,101 and movement based classifications102-105 may be considered when applying this guideline to the individual client with PP-PGP. The challenge with choosing the appropriate model for PP-PGP is highlighted when one considers the scope of this condition. Consideration of several factors commonly present with PP-PGP are needed to classify the condition including; the psychological state of the women, the number of joints involved, and the underlying functional impairments associated with faulty joint kinematics. Each of this factors needs to be considered to direct care decisions.
The biopsychosocial model97 highlights the importance of the psychological state of the women and may be considered when incorporating moderators that may affect intervention outcomes. This is especially important with the postpartum client who require additional education and referrals to other medical providers because of postpartum health, independent of PP-PGP. The utility of the biopsychosocial model is limited in that it does not guide specificity for interventions beyond patient educational needs.
Considering the kinematics of the pelvic girdle is also an important factor when attempting to classify PP-PGP. The shape of the sacrum, ilium, PS, and supporting connective tissues are uniquely designed to create form closure, which allows a locking mechanism during limb loading.67,106 In addition, the surrounding musculature, when activated in a coordinated fashion, reinforces the stability of the pelvic joints providing force closure.8,107-111 Thus, using provocative testing to understand which joints are involved (SIJ and PS) is important. However, given the interaction between joint loading and muscle performance, it is important to not simply perform provocative testing in isolation. Provocative tests provide insight into the pathoanatomic location of the pain, but do not provide guidance related to the specificity of the impairments needed to be addressed during intervention.
The treatment based classification model100,101 relies heavily on alignment to determine the need to provide a manipulative technique. However, there is strong evidence to support the lack of reliability in identifying pelvic girdle alignment and accessory motion impairments in the non-pregnant population.112,113 Clinicians should not rely solely on

22
alignment testing to determine treatment options. Once involved joints have been identified and the presence of asymmetry has been determined, movement testing is needed to determine specific patterns of movement and coexisting impairments to determine an individualized care plan. Thus, based on the evidence associated with presenting symptoms and physical limitations of women with PP-PGP, the authors propose a classification system that considers key aspects of each of the reported models noted above including, alignment, provocative testing, and movement testing. The focus of this model is associated with identification of specific load transfer impairments of the pelvic girdle. The authors propose 3 categories of load transfer impairments for PP-PGP:
1) Sacroiliac joint load transfer impairment with or without asymmetry,
2) Pelvic girdle load transfer impairment (2 or more joints), and
3) Pubic symphysis load transfer impairment.
The Clinical Decision-Making (CDM) Flowchart (Figure 1) facilitates implementation of this proposed PGP classification into clinical practice. The CDM Flowchart is designed to help readers select appropriate tests and measures based on the respective theoretical models as well as develop appropriate intervention strategies for the client with PP-PGP, based on location of pain, pain response to treatment, movement related load transfer impairments, and presence of asymmetry (alignment and muscle performance). The focus of this classification system is on nociceptive aspects of PP-PGP. The authors recognize that nocioplastic PP-PGP would require additional considerations, but due to the limited amount of research in this area, this is considered beyond the scope of this CPG.
Hybrid Diagnostic Model
The components of the movement system104,114 that need to be considered in order to classify PP-PGP include consideration of state of each component of the system, bone, muscle, integument (including fascia), ligament, and neural control. Individuals with PP-PGP may have persistent pregnancy-related connective tissue laxity77,115-117 and muscle performance impairments in the supportive muscle groups of the pelvic girdle.20,42,78,79,82,96,118-124 The primary movement impairment that results is an inability to adequately control joint stability at the SIJ, PS, or both during functional movements that require limb or trunk loading. In women with PP-PGP, there is impaired muscle function in the abdominals,10,96 back flexors and extensors, hip adductors and extensors,20,79,90 and pelvic floor muscles, 78,122 combined with excessive or asymmetrical accessory motion at the SIJ and/or PS.55,76,77,97,125. These impairments cause difficulty and pain with functional tasks such as walking, moving from sit to stand, and rolling. 99,126
It is theorized that maladaptation of the ability to transfer the weight of the trunk over the limb occurs because of reduced kinematic locking mechanism of the joints, contributing to impairments in both the structural stability of the joint and the muscle performance.8,80,84,85,106,118,127-129 Because directionality of movement is unique to the individual,130-132 specific assessment of alignment and muscle performance during testing will allow individualized treatment plans to be developed. The focus of treatment

23
is to improve muscle performance of the abdominals, back and hip extensors and pelvic floor muscles to improve stabilization of the pelvic girdle during functional activities and load transfer tasks. Specific attention needs to be given to movements that impose asymmetrical stresses across the SIJ or PS.8,55 For example, excessive trunk and lumbopelvic rotation during single leg stance occurs due to reduced performance of the abdominals, hip, and back extensors to assist in stabilization of the SIJ during this task. Impaired muscle performance of specific muscles that affect the stability of the pelvic joints may be determined during movement testing of the spine and hip, and can include bending, return from bending, standing on one leg, and lifting one leg in supine. Due to reduced reliability in the non-pregnant population112,113 and the lack of specificity found in utilizing testing in the postpartum population,100 palpation should not be solely relied upon to direct treatment strategies for PP-PGP. However, in the presence of continued asymmetry of the pelvic joints combined with the presence of pain that does not reduce with increased muscle performance and/or mechanical stabilization, an attempt to correct a suspected positional impairment could be considered, followed by prescribing specific stabilization activities.100
Diagnostic Categories
A load transfer impairment will present with excessive and/or asymmetrical motion causing impaired stability of the joint during limb loading and with rolling if recumbent. Symptoms may present either unilateral (Sacroiliac Joint Load Transfer Impairment-Table 8) or bilateral (Pelvic Girdle Load Transfer Impairment-Table 9). Key tests and signs that may be present for Sacroiliac Joint Load Transfer Impairment include: positive of the LDL (in more severe cases), active straight leg raise, Modified Trendelenburg, Stork or March testing, P4 and FABER test all producing symptoms in the region of the posterior SIJ. Strength testing would reveal reduced performance of the gluteal muscles on the side of pain, and if unilateral in presentation, asymmetrical back and abdominal muscle performance impairments will be present. Impaired performance of the muscles that create force closure across the joint may be determined during movement testing. (Forward bending, single leg stance, supine hip flexion, prone hip extension). Focus of treatment is improving single leg stance mechanics during functional tasks by both mechanical (belt) and/or muscle (force) stabilization of the pelvic ring reducing the motions that impose physical stresses across the SIJ. In the presence of asymmetry that does not resolve with use of a belt, functional training and stabilization exercises, the use of joint mobilization should be considered.
A pelvic girdle load transfer impairment that includes 2 or more joints is considered part of a continuum of worsening impairment indicating increased severity of the condition. Pain and instability would occur with limb loading at 2-3 regions. Ambulation is severely limited for individuals who have this condition and a pelvic belt and assistive device may be warranted to allow protection of the supportive connective tissues of the pelvic girdle. Treatment will need to consider positions of the surrounding joints including maintaining normal lumbar lordosis to assist with locking of the SIJ posteriorly combined with reduced mechanical stress across the PS. Avoidance of excessive flexion of the lumbosacral region as well as reduction of hip range of motion for flexion

24
and abduction is needed during functional activities, sit to supine, sitting, and sit to stand.
A Pubic Symphysis Load Transfer Impairment (Table 10) will present with anterior pelvic girdle pain and potential excessive motion (superior glide or rotation) at the PS during loading of the limb. Key tests and signs include a positive palpation test for the PS, positive Modified Trendelenburg or single limb test. Pain located at the PS is triggered with end range hip flexion or abduction. Pain improves commonly with manual compression across the pelvis or belt stabilization. Focus of treatment is stabilization of the PS during limb loading (muscle activation and belt stabilization) as well as reduction of mechanical stress on the PS during functional activities that create either rotational stress across the pelvis (active hip flexion, walking, rolling in bed, in and out of a car) or gap the PS (leg abduction). Persistence of an asymmetry of the PS requires assessment for leg length discrepancy or a positional impairment. Correction of a positional impairment should be followed by stabilization exercises to reduce the physical stress across the tissues related to the PS (abdominal, pelvic floor, adductor and gluteal musculature). Impaired performance of the muscles that create force closure across the joint may be determined during movement testing.
For all of the categories of load transfer impairment specific childcare activities should be assessed including; positions for play and nursing the baby, carrying the baby, diaper changes and pushing a stroller.
PROGNOSIS
Hemingway et al133 notes that prognosis is the risk of future health-related impairments given a specific condition. Prognosis of recovery from PP-PGP appears to depend on initial pain and disability scores. Women with greater disability and higher pain scores should be expected to recover more rapidly and return to function. Conversely, women with low disability and low pain scores should be expected to recover to a lesser extent. For this latter group, clinicians should administer measures of fear-avoidance behavior and depression because of the likelihood of confounding factors and the increased likelihood of minimal gains with physical therapy intervention.
Across studies, a portion of women failed to achieve 0% disability and/or absence of pain at 6 months to 1 year17,20,134 and at 2 years postpartum.135 It is unclear if the continuation of pain and disability found in these studies is directly related to unresolved PP-PGP or indicative of confounding factors, such as pre-existing conditions, reduced hip extension and trunk flexion performance, postpartum depression, and/or the development of chronic pain and fear-avoidance behavior. The addition of fear-avoidance questionnaires and measures of mental health in future research may facilitate better identification of women with PP-PGP not following a “normal” course of recovery.
There is conflicting evidence that age is a non-modifiable risk factor for poorer prognosis. Both younger age (<30) and older age (>30) have been identified as corresponding to higher rates, intensity and/or duration of pain in PP-PGP. This finding may be attributable more to parity than maternal chronological age. Young women and

25
older women (>30 years) have higher rates/intensity/duration of pain.10,13 In a study by Gutke et. al10, each year older corresponded to a 1.2 increased risk for PGP in postpartum women at 3 months after delivery. Conversely, Wu et. al13 found that younger women were more likely to have PGP than their older counterparts. Significant relationships related to the presence of PGP at 1 year postpartum are associated with a combined presence of increased age and reduced muscle performance of the hip extensors and trunk flexors.20 Future studies should employ techniques to stratify groups based on parity, utilize age- and parity-matched controls and perform subgroup analyses to further investigate inter-relationships among parity, age, pain intensity, duration, and prevalence.
As previously noted in the risk factors for developing PP-PGP, women are more likely to develop PP-PGP if they have experienced pain during pregnancy and if they have more severe symptoms at the time of presentation.9-14 However, some women do not have PGP during pregnancy, but develop PGP during the postpartum period.136,137 Why PGP during pregnancy persists into the postpartum period is not well understood. See Table 11 for a summary of the literature that consistently reports that PP-PGP is persisting from 3 months to 12 years postpartum. Future research should investigate factors that contribute to this persistent pain syndrome.
INTERVENTION
Pregnancy-related studies were excluded from the intervention recommendations unless a PT intervention was applied specifically for PP-PGP and the PT intervention was applied within the first postpartum year. For some interventions, such as therapeutic modalities, an insufficient amount of studies were available upon which to make a recommendation for or against the use of the intervention, including therapeutic ultrasound, infrared, and electrical stimulation. Outcome measures most commonly reported were pain and disability. Co-interventions were common across intervention studies for PP-PGP.
Education
Education interventions across PP-PGP studies included the following components: pathology, etiology, and clinical presentation of PGP; load transfer impairment; rationale for belt stabilization; and strategies to minimize pain during functional activities and Instrumental Activities of Daily Living (IADLs) using both biomedical and biopsychosocial approaches.16,98,138-146
Bastiaenen et. al.98 compared the effects of a biopsychosocial-tailored intervention for PP-PGP to usual care. The biopsychosocial intervention consisted primarily of self-management and fear-avoidance concepts, with education on lumbopelvic anatomy. Reduced disability after 3 months of treatment was reported in both groups, but to a greater extent in the biopsychosocial intervention group (+2 points on Roland-Morris Disability Questionnaire (RDQ)).98 However, no significant differences were found between groups at 6 and 12 months post-intervention.142

26
Exercise
Exercise intervention studies reported significant improvements in pain and disability in all groups, regardless of the type of exercise intervention delivered.16,123,134,138-140,143,145-
153 Greater improvements have been reported in muscle performance, pain, and disability as compared to controls or usual care groups. Outcomes of exercise interventions compared to those of manual therapy interventions were consistently superior for reported long-term outcomes. Exercise interventions directed at muscle strengthening consistently report improvements in strength and disability post-intervention. The specificity of exercise does not appear to significantly impact pain or disability outcomes. Exercise intervention studies often included the use of a pelvic belt as a co-intervention to reduce pain during exercise and improve function. Exercise generally did not worsen symptoms. All groups experienced reductions in pain and disability, and the use of belts may have contributed to improved outcomes. Therefore, it is our recommendation that PTs should use pelvic belts in conjunction with education and exercise interventions.
Stabilization exercises were the most common exercises prescribed and are defined as progressive strengthening of the abdominals, back extensors, and pelvic floor musculature. Stabilization exercises emphasize activation of the transversus abdominus (trA) and pelvic floor musculature (PFM) prior to limb or trunk movements for adequate force closure of the pelvic girdle. Improvements in muscle function of the paraspinals,145 abdominals,147 hip extensors,139 hip adductors and abductors,147 and pelvic floor123,149 were reported in exercise-based intervention studies in PP-PGP. Evidence on the effectiveness of trunk stabilization exercises for the management of PP-PGP is summarized in Table 12: Stabilization Exercises.
Exercise interventions have been conducted as early as within the first postpartum week,138,151 but most frequently beginning at 6, 8, or 12 weeks postpartum. Intervention duration ranged from 4 weeks to 20 weeks. Session time, when reported, ranged from 40 to 120 minutes. Stabilization exercises were provided most commonly with co-interventions, including modalities, stretching, therapeutic exercise, pelvic floor muscle contraction (PFMC), manual therapy and soft tissue mobilization, physical activity and home exercise program, education, and functional training.
Pelvic Belt
Pelvic belts were most commonly utilized in combination with exercise intervention studies90,144,146,154 (See Table 13). The application of a pelvic belt has been demonstrated to reduce laxity and ASLR scores155 and increase hip adductor force production.90 In combination with exercise interventions, the application of the pelvic belt has been demonstrated to reduce pain.144,146
The pelvic belt may be worn at either a high (at the ASIS) or low (at the PS) position. The pelvic belt in either position has been shown to reduce laxity and improve ASLR

27
scores as compared to no belt. The pelvic belt worn in a high position decreased SIJ laxity to a significantly greater degree than the low position.155
Interestingly, all studies that investigated effects of the pelvic belt enrolled participants with a minimum Visual Analogue Scale (VAS) score of 30 mm or greater.144,155 Therefore, the value of pelvic belt use is unclear in PP-PGP women with low pain severity (<30 mm on VAS). Future research should investigate the clinical value of pelvic belt use in PP-PGP women with pain severity <30 mm on the VAS and the use of a pelvic belt during the first 4 weeks postpartum.
Manual Therapy
Manual therapy intervention studies with PP-PGP were included if two criteria were met: 1) at least one manual therapy intervention was directed to the pelvic girdle, and 2) the pain description or inclusion criteria were consistent with PP-PGP. Studies were excluded if manual therapy was applied only to the lumbar spine and/or hip and if the pain description was consistent with lumbar pain. There is strong evidence supporting the application of manual therapy interventions in conjunction with co-interventions to provide short-term improvements in pain and disability in PP-PGP.16,100,145,156 PTs should not apply manual therapies in isolation. There is strong evidence that the use of manual therapy interventions is no better than stabilization exercises for long-term improvement (>6 months) in outcomes.16,134
Al-Sayegh et al100 reported improved ODI and VAS scores in PP-PGP utilizing a high velocity thrust technique (HVTT) mobilization to the pelvis. The population studied was within one year of giving birth. As many as 19% had delivered within the previous month. No adverse effects were reported. In the presence of asymmetry, severe disability (>40%) as measured with the ODI score and/or VAS >3, PTs may consider the use of HVTT if PP-PGP is non-responsive to functional activity training and therapeutic exercise targeted to their specific load transfer impairment.100 In addition, non-success following HVTT was defined by failure to achieve a 50% reduction in ODI score post-intervention. Non-success was predicted with 75% probability when 2 of the 3 variables (age >35, VAS best >3, negative prone knee bend test) were present. Non-success was predicted with 87% probability of non-success with 3 of 3 variables present. PTs may consider using a pelvic belt in combination with exercise for women with PP-PGP who do not respond to HVTT.
Summary of Limitations in Intervention Studies
Well-described educational interventions, patient-centered language, and instructional elements are lacking. Studies utilized multiple theoretical frameworks for exercise interventions and lacked true control groups. Inconsistencies in reporting of intervention parameters, including frequency, duration, and combinations of therapeutic interventions applied, made synthesis of best practice recommendations challenging. Most exercise-based intervention studies utilized pelvic belts across groups, making it difficult to investigate the effects of exercise and pelvic belts in isolation. Additionally,
28
most intervention studies include multiple co-interventions. Co-interventions such as medication use, involvement with additional health providers or participation in other therapies, physical activity, and description of postpartum standard of care after delivery across international studies, were identified and make it difficult to both determine the impact of any one intervention. Longer follow-up (beyond completion of intervention), compliance mechanisms, and proposed explanations for worsening of pain during, or following, intervention are needed across all intervention studies.
Results of PP-PGP belt studies may not be as generalizable to less severe cases of PGP (VAS<30 mm). High-quality biomechanical studies evaluating physical and/or functional changes following belt use and large, longitudinal studies investigating belt use with functional tasks and pain complaints in the population with PP-PGP have generally not been conducted. Future research should be performed with PP-PGP to investigate the biomechanical effects of pelvic belt use, especially during ASLR testing, standing double-limb and single limb support testing, and functional tasks.
RESEARCH RECOMMENDATIONS
Based on this Clinical Practice Guideline, there are several future research recommendations that span each aspect of this review. Table 14 provides the recommendations based on each section.
Much emphasis has been placed on the use of provocation tests to rule in or out PP-PGP. While this type of testing helps to inform the clinician as to the location of the pain and the irritability of the tissues, this type of testing provides little information regarding specific impairments/functional limitations to guide the selection of appropriate interventions. Future research will need to compare the value of provocation tests to those of functional measures to streamline the diagnosis and treatment of PP-PGP.
It is common practice to measure the change in thickness of the abdominal, multifidus, and/or pelvic floor musculature as a means of assessing improvement in patients with lumbar and/or pelvic girdle pain. Currently, there is little evidence to suggest that the change in thickness of the musculature correlates with resolution of PP-PGP. Preliminary evidence suggests that the thickness of the musculature is of lesser value than appropriate activation of the musculature, including appropriate timing and coordination of muscle activation with functional tasks. Future research should examine the best measures of muscle performance to guide intervention.
Standing tests have been described in the assessment of women with PP-PGP. However, most literature on standing tests for PGP have been performed longitudinally starting with populations that develop PGP during pregnancy and with additional assessment of the PGP groups at various time points in the postpartum period.157 However, little research exists on standing tests/measures specifically for the identification of PGP in the postpartum population, regardless of the time of symptom onset. Future research should follow groups as a whole rather than following painful cohorts during pregnancy into the postpartum period.
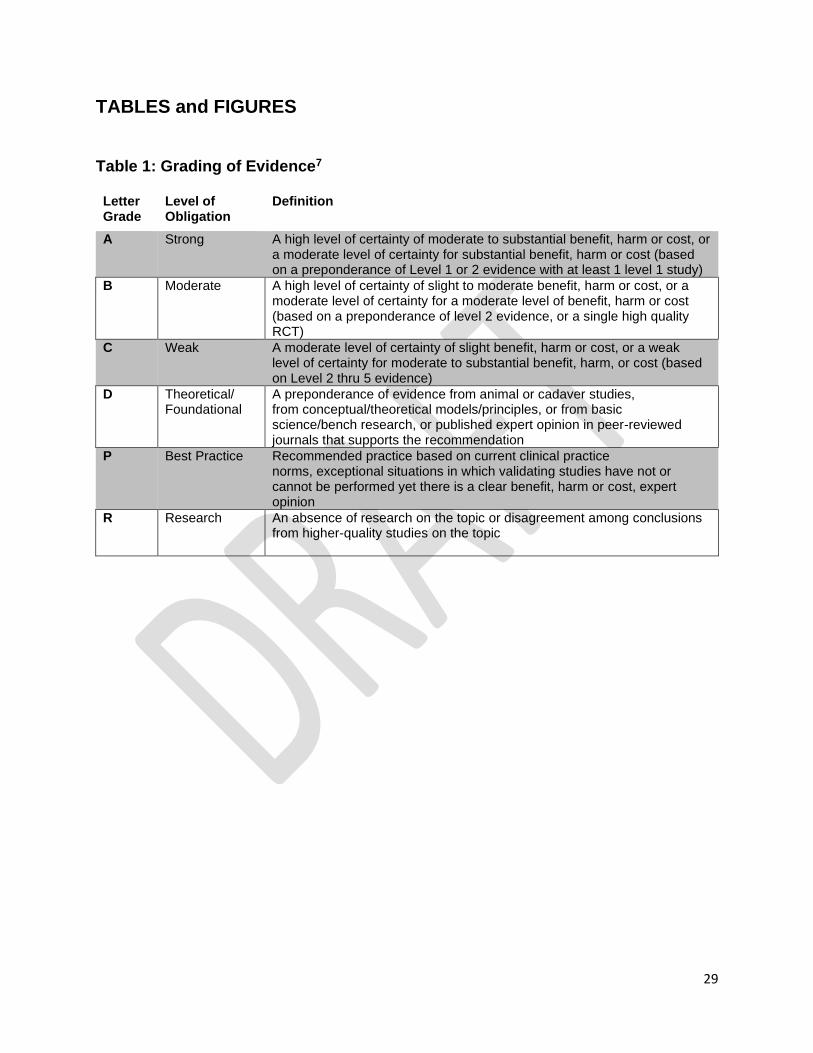
29
TABLES and FIGURES
Table 1: Grading of Evidence7
Letter Grade
Level of Obligation
Definition
A Strong A high level of certainty of moderate to substantial benefit, harm or cost, or a moderate level of certainty for substantial benefit, harm or cost (based on a preponderance of Level 1 or 2 evidence with at least 1 level 1 study)
B Moderate A high level of certainty of slight to moderate benefit, harm or cost, or a moderate level of certainty for a moderate level of benefit, harm or cost (based on a preponderance of level 2 evidence, or a single high quality RCT)
C Weak A moderate level of certainty of slight benefit, harm or cost, or a weak level of certainty for moderate to substantial benefit, harm, or cost (based on Level 2 thru 5 evidence)
D Theoretical/Foundational
A preponderance of evidence from animal or cadaver studies, from conceptual/theoretical models/principles, or from basic science/bench research, or published expert opinion in peer-reviewed journals that supports the recommendation
P Best Practice Recommended practice based on current clinical practice norms, exceptional situations in which validating studies have not or cannot be performed yet there is a clear benefit, harm or cost, expert opinion
R Research An absence of research on the topic or disagreement among conclusions from higher-quality studies on the topic

30
Table 2. Level of Evidence Definitions7
Types of Studies
Level of Evidence Intervention/ prevention
Pathoanatomic/ risk/clinical course/prognosis/differential diagnosis
Diagnosis/ diagnostic accuracy
Prevalence of condition/ disorder
Exam/ outcomes
I. Evidence obtained from high-quality systematic reviews, diagnostic studies, prospective studies, or randomized controlled trials (RCTs)
Systematic review of high-quality RCTs(a) High quality RCT (a)
Systematic review of prospective cohort studies High-quality prospective cohort study (b)
Systematic review of high-quality diagnostic studies High-quality diagnostic study with validation (c)
Systematic review of high-quality cross-sectional studies High-quality cross-sectional study (d)
Systematic review of prospective cohort studies High-quality prospective cohort study
II. Evidence obtained from lesser-quality diagnostic studies, prospective studies, or RCTs (eg, weaker diagnostic criteria and reference standards, improper randomization no blinding, less than 80% follow-up)
Systematic review of high-quality cohort studies High-quality cohort study (b) High-quality outcomes research High-quality quasi-experimental study (g) High-quality single-subject design (h) Lower-quality RCT (e)
Systematic review of retrospective cohort studies Lower-quality prospective cohort study High-quality retrospective cohort study Consecutive cohort study Outcomes study or ecological study (f)
Systematic review of exploratory diagnostic studies or consecutive cohort studies High-quality exploratory diagnostic study Consecutive retrospective cohort study
Systematic review of studies that allows relevant estimate Lower-quality cross-sectional study
Systematic review of lower-quality prospective cohort studies Lower-quality prospective cohort study
III. Case-controlled studies or retrospective studies
Systematic review of case-controlled studies High-quality case-
Lower-quality retrospective cohort study High-quality cross-sectional study Case-controlled study
Lower-quality exploratory diagnostic study Nonconsecutive retrospective cohort study
Local non-random study
High-quality cross-sectional study

31
controlled study Outcomes study or ecological study (f) Lower-quality cohort study
IV. Case series Case series Case series Case-controlled study
Lower-quality cross-sectional study
V. Expert opinion Expert opinion
Expert opinion Expert opinion Expert opinion
Expert opinion
a. High quality includes RCT>80% follow-up; blinding; appropriate randomization procedures. b. High-quality or dramatic effect cohort study includes > 80% follow-up c. High-quality diagnostic study includes consistently applied reference standard and blinding. d. High-quality prevalence study is a cross-sectional study that uses a local and current random sample or censuses. e. Weaker diagnostic criteria and reference standards, improper randomization, no blinding, < 80% follow-up may add threats to bias and validity. f. High-quality outcome or ecological studies use instrumental variable(s) or other control for confounding factors. g. High-quality comparative study without random assignment to groups. h. Must have a minimum of “a” and B” phase.

32
Table 3. Factors Associated with a Higher Risk of PP-PGP
LOE Risk Factor Relative Risk (95% CI) Author (Year)
I/II History of prior LBP and/or PGP
Pain in year prior to pregnancy
OR=2.2, p=.0001 Albert et al9
Pain in prior pregnancy
χ21=6.43, p=.03 Simonds et al14
OR=16.08 (8.47 to 30.51) Elden et al11
OR=2.28 (1.12 to 4.66), p=.0236
Gutke et al10
r=0.52, p<.0001 Wu et al13
I/II Pain location Posterior pain only OR=3.4 (−1.0 to 7.8), p=.03
Bergström et al 18
PS pain only OR=11.8 (2.3 to 21.2), p=.03
Gausel et al17
Number of pain locations
OR=8.0 (−0.03 to 16), p=.05 Vøllestad et al15
Posterior pelvis and/or deep in the gluteal region, with/without radiation into the posterior thigh but not down to the foot
OR=3.39 (1.17 to 9.81), p=.02 Gutke et al10
Combined PS and posterior pain
OR=8.4 (−0.07 to 17), p=.03 Albert et al9

33
II
High disability High ODI (postpartum day 1)
ODI in pregnancy ODI>20: OR=3.3 (1.1 to 9.7), p=.034 ODI>40: OR=5.1 (1.7 to 15.0), p=.003 (23.5 [11.03, 50.32], p<0.0001)
Gutke et al19
ODI (3 months postpartum)
B=−1.14 (−2.04 to −0.24), t=−2.56, p<.0140
Sjödahl et al20
II
Pain with activity
When turning in bed OR=1.47 (1.14 to 1.90), p=.003 Gutke et al10
74% reported pain Mens 199657
With weight bearing 90% reported pain after 30 min of standing
81% reported pain with standing on one leg
81% reported pain with walking for 30 min
Mens 199657
50% with pain after 5 mins of standing
Ronchetti et al81
II
Mode of delivery
Cesarean section higher risk of PP-PGP
Adjusted OR=2.0 (1.3 to 4.9) Mukkannavar et al21
X21=17.39; p<0.001 Munro et al23
χ21=4.89; p=.05 Simonds et al14
OR=2.3 (1.4 to 3.9)
Bjelland et al158

34
Vaginal delivery/twin delivery associated with PS diastasis
OR=12.6 (1.48 to 106.46), p=.020 (vaginal delivery)
OR=9.20 (2.52 to 33.57), p=0.001 (Twin delivery)
Yoo et al159
II Provocation testing of the pelvic girdle
High number of bilateral positive pain provocation tests
OR=1.79 (1.25 to 2.57), p=.0015
Elden et al11
l/II
ASLR (score 0-3) OR=4.4 (1.1 to 17.5), p=.035 Vøllestad et al15
Unilateral P4 Adjusted OR=1.8 (1.1 to 3) Mukkannavar et al21,
ASLR test score ≥4 Adjusted OR=2.3 (1.2 to 3.3) Mukkannavar et al21,
II/III Parity Multiparous OR=2.2, p<.001 Albert et al9
OR=1.3 (0.47 to 2.24)
OR=1.42 (0.29 to 3.76)
Gutke et al10
OR=1.2 (0.6 to 2.1), p=.01
OR=1.6 (1.1 to 2.6, p=.01
Gashaw et al160
>3 pregnancies X2 = 5.89, p=.05 Mukkannavar et al22
2 pregnancies X2 =32, p<.0001 Wu et al13
BMI Increased BMI OR=1.14 (1.04 to 1.25), p=.01 Biering et al161

35
Depressive symptoms
More depressive symptoms higher risk
OR=3.58 (1.39 to 9.22), p=.008 Gutke et al50
Work dissatisfaction
Unhappy with work more likely to have PP-PGP
OR= 10.06 (2.16 to 46.91), p=0.003 Gutke et al10
Work status No work outside the home –more likely to have PP-PGP
X2=9.81, p=.002 Mukannavar et
al21
Lactation status
Sitting while breastfeeding
Adjusted OR=1.5 (0.9 to 2.8) Mukkannavar et al21
Low endurance of trunk flexors OR=1.18 (1.01 to 1.37), p=.04
Gutke et al10
B=−1.23 (−1.83 to −0.62), t=−4.10, p<0.0002
Sjödahl et al20
II
Older Maternal age OR=1.2, (1.07 to 1.36), p=.002 Gutke et al10
B=−1.36 (−2.11 to −0.60), t=−3.63, p<0.0008
Sjödahl et al20
Abbreviations: ASLR, Active Straight Leg Raise; BMI, Body Mass Index; CS, Cesarean Section; FABER, Flexion, abduction, external rotation test; LBP, low back pain; LOE, Level of evidence; OR, odds ratio; PP-PGP, Postpartum Pelvic Girdle Pain; P4, Posterior Pelvic Pain Provocation Test; χ2, Chi square statistic
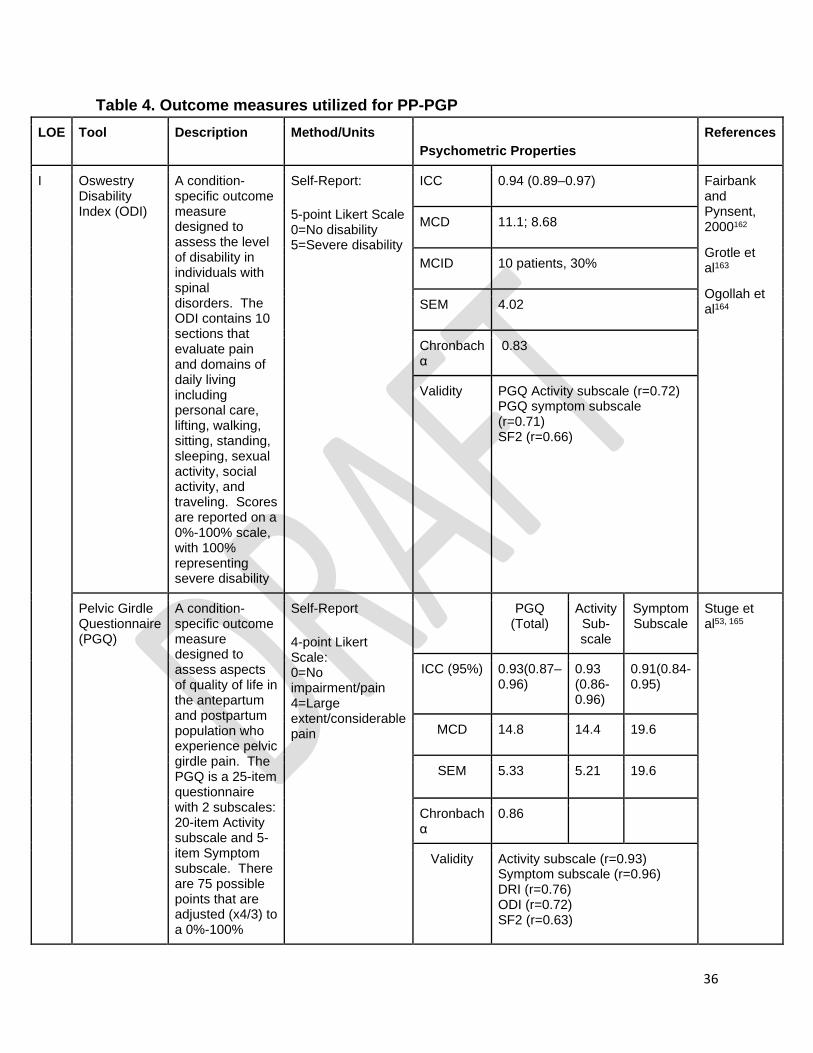
36
Table 4. Outcome measures utilized for PP-PGP
LOE Tool Description Method/Units Psychometric Properties
References
I Oswestry Disability Index (ODI)
A condition-specific outcome measure designed to assess the level of disability in individuals with spinal disorders. The ODI contains 10 sections that evaluate pain and domains of daily living including personal care, lifting, walking, sitting, standing, sleeping, sexual activity, social activity, and traveling. Scores are reported on a 0%-100% scale, with 100% representing severe disability
Self-Report: 5-point Likert Scale 0=No disability 5=Severe disability
ICC 0.94 (0.89–0.97) Fairbank and Pynsent, 2000162
Grotle et al163
Ogollah et al164
MCD 11.1; 8.68
MCID 10 patients, 30%
SEM 4.02
Chronbach α
0.83
Validity PGQ Activity subscale (r=0.72) PGQ symptom subscale (r=0.71) SF2 (r=0.66)
Pelvic Girdle Questionnaire (PGQ)
A condition-specific outcome measure designed to assess aspects of quality of life in the antepartum and postpartum population who experience pelvic girdle pain. The PGQ is a 25-item questionnaire with 2 subscales: 20-item Activity subscale and 5-item Symptom subscale. There are 75 possible points that are adjusted (x4/3) to a 0%-100%
Self-Report 4-point Likert Scale: 0=No impairment/pain 4=Large extent/considerable pain
PGQ
(Total) Activity Sub- scale
Symptom Subscale
Stuge et al53, 165
ICC (95%) 0.93(0.87–0.96)
0.93 (0.86-0.96)
0.91(0.84-0.95)
MCD 14.8 14.4 19.6
SEM 5.33 5.21 19.6
Chronbach α
0.86
Validity Activity subscale (r=0.93) Symptom subscale (r=0.96) DRI (r=0.76) ODI (r=0.72) SF2 (r=0.63)

37
Scale, with 100% representing the highest impact on quality of life.
Quebec Back Pain Disability Scale (QBPDS)
The QBPDS is a 20-item self-administered instrument designed to assess the level of functional disability in individuals with back pain. The scale is a reliable and valid measure used for monitoring the progress of individual patients participating in treatment or rehabilitation programs. The minimum score is 20 and the maximum score is 100. Higher scores correlate to greater disability. % of maximal disability = (score) – 20) / 80 * 100% Minimum detectable change (90% confidence) 15 points
Self-report 5-point Likert Scale 0= not difficult at all 5= unable to do
ICC (95%)
0.70 to 0.99 Kopec et al54
Damen et al55 Mens et al59
MCD 15
SEM 5.33
Chronbach α
0.89 to 0.96
Validity ODI (r=0.80) RMDQ (r=0.77) SF-36 (r=??)
Abbreviations: LOE, Level of evidence, DRI, disability rating index; ICC, interclass correlation coefficient, MCD, minimal clinical difference; MCID, minimal clinical; PGQ, Pelvic girdle questionnaire, QBPDS, Quebec Back Pain and Disability Scale, RMDQ, Roland-Morris Disability Questionnaire; SEM, standard error of the measure; SF2, Short Form 36: Physical functioning

38
Table 5. Special Tests for PP-PGP
LOE Test Study Population
Psychometrics Reference
Sn Sp Re NPV PPV
I PS Palpation Test
*2269 pregnant women at week 33 of gestation
0.60 0.99 k= 0.89
Albert et al166
III Long Dorsal Ligament Palpation
178 women with PGP since pregnancy or that began within 3 w postpartum receiving PT at OP clinic 0.5 to 4.8 y postpartum (median 1.7 y)
0.76
0.86
Vleeming et al68
Mixed - both pregnant and postpartum were reported. Mixed PGP/LBP group (n=61) Controls (n=63)
0.21 0.98 k= 0.76 (0.64 to 0.88)
Njoo69
I/II Posterior Pelvic Pain Provocation Test (P4)
Postpartum women who experienced PGP during pregnancy Current PGP (n=51) No current PGP (n=238)
0.569
0.164 0.90 0.42 Olsen et al71
Women with persistent pelvic girdle pain after delivery (n = 32)
0.88 0.89
0.87 0.89 Gutke et al73
Women with postpartum PGP (n = 200) Women with Lumbopelvic pain (n=50) Healthy women (n = 50)
0.69
Mens et al74

39
Pregnant and postpartum women with PGP (2 and 6 months post-delivery) (n=38) Pregnant women without PGP (n=14)
0.70 - 0.74
Hansen et al72
II FABER Test Postpartum women who experienced PGP during pregnancy Current PGP (n=51) No current PGP (n=238)
0.608 0.205
0.909 0.517
Olsen et al71
I Active Straight Leg Raise Test
Postpartum women who experienced PGP during pregnancy Current PGP (n=-51) No current PGP (n=238)
0.588 0.151
0.829 1.00 Olsen et al71
49 pairs of women at least 6 months postpartum- with PGP and without PGP
ICC 0.886 - 0.955 (R leg) 0.905 - 0.952 (L leg)
Stuge et al78
Patients with PGP and ≥3 on 0–10 pain score
0.58 0.97
Damen et al77
Women with postpartum PGP (n = 200) Women with Lumbopelvic pain (n=50) Healthy women (n = 50)
0.87 0.94 r=0.87
Mens et al74
II Modified Trendelenburg
Postpartum women who experienced
Anterior pain 0.176
0.02
0.846
0.563
Olsen et al71

40
PGP during pregnancy Current PGP (n=51) No current PGP (n=238)
Posterior pain 0.49
0.08
0.849
0.50
*No available evidence specific to reliability/validity in the postpartum population.
Abbreviations: FABER, Flexion, abduction, external rotation test; LBP, Low back pain; LOE, Level of evidence; Re, Reliability; Sn, Sensitivity; Sp, Specificity; PGP, pelvic girdle pain; P4, Posterior Pelvic Pain Provocation Test; NPV, Negative Predictive Value: proportion of patients with a positive test who are correctly diagnosed; PPV, Positive Predictive Value: proportion of patients with a negative test who are correctly diagnosed; w, weeks

41
Table 6: Muscle Function Assessment in PP-PGP
LOE Muscle Function
Test/Measures Study Population Study Findings Reference
II Timing of Contraction
ASLR Women with persistent PP-PGP (n=28) Women without PGP (n=13)
The PP-PGP group showed a delayed onset in both the PFM (p=0.01) and muscles of the lower lateral abdominal wall (p<0.01) compared with the control group).
Sjodahl et al79
II Endurance Trunk flexor endurance test
Women with persistent PP- PGP and PP-PGP in combination with lumbar pain at 3 months postpartum (n=88) and 15 months postpartum (n=58)
Age + trunk flexor endurance was predictive of disability 15 months postpartum
Sjodahl et al20
Back flexor and back extensor muscle endurance tests
Women 3 months postpartum classified into groups • no low back pain
• PP-PGP
• lumbar pain
• combined lumbar and PP-PGP
Women with PP-PGP have lower endurance of back flexors than women without pain (mean difference 17.9 sec, p=.001).
Back extensors (Mean difference 28.3 sec, p<0.001, compared to women without LBP or PP-PGP)
Gutke et al82
II Force Production
Maximal hip ADD force using hand-held dynamometry
Postpartum women 49 women with long-lasting posterior PP-PGP (n=49) Postpartum women and of the same age group without PGP (n=37)
Women with PP-PGP demonstrated significantly reduced hip ADD force during ASLR testing (without belt) than controls (107+/-51 N vs. 211+/-42 N) (p<0.00001).
Mens90
Hip extensor strength using hand-held dynamometry
Women with persistent PGP and PGP in combination with lumbar pain at 3 months postpartum
Disability + hip extensor strength was predictive of disability 15 months postpartum
Sjodahl et al20
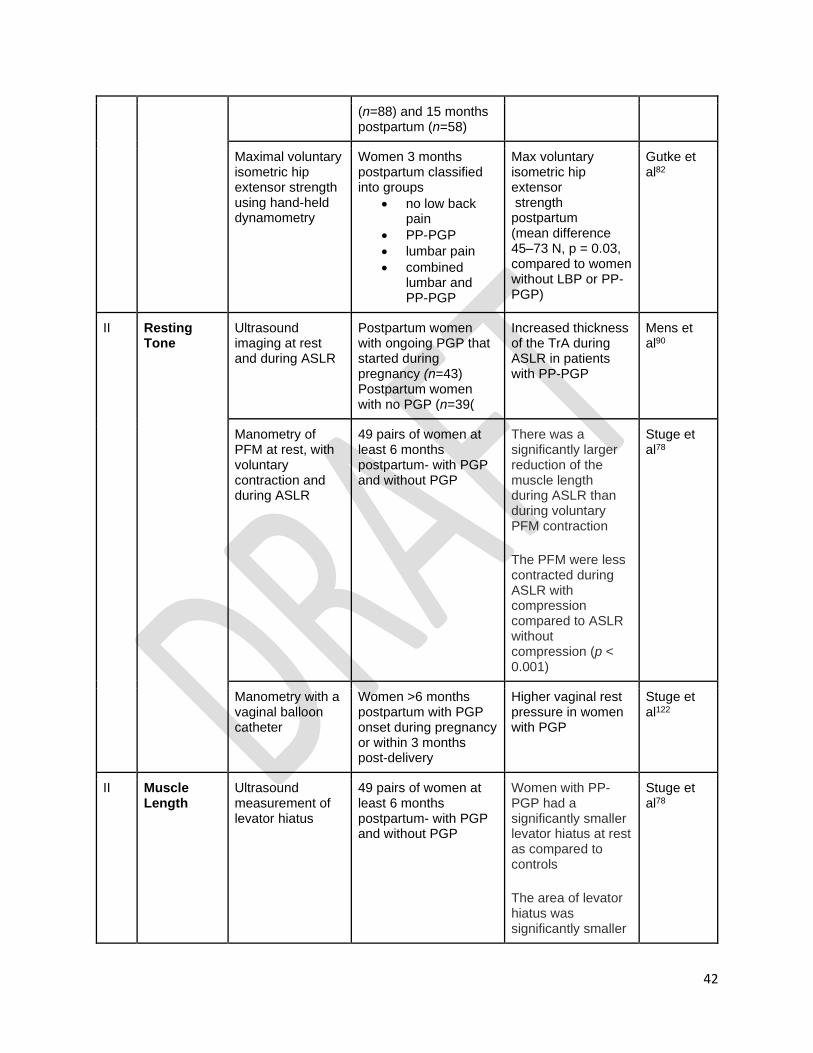
42
(n=88) and 15 months postpartum (n=58)
Maximal voluntary isometric hip extensor strength using hand-held dynamometry
Women 3 months postpartum classified into groups
• no low back pain
• PP-PGP
• lumbar pain
• combined lumbar and PP-PGP
Max voluntary isometric hip extensor strength postpartum (mean difference 45–73 N, p = 0.03, compared to women without LBP or PP-PGP)
Gutke et al82
II Resting Tone
Ultrasound imaging at rest and during ASLR
Postpartum women with ongoing PGP that started during pregnancy (n=43) Postpartum women with no PGP (n=39(
Increased thickness of the TrA during ASLR in patients with PP-PGP
Mens et al90
Manometry of PFM at rest, with voluntary contraction and during ASLR
49 pairs of women at least 6 months postpartum- with PGP and without PGP
There was a significantly larger reduction of the muscle length during ASLR than during voluntary PFM contraction The PFM were less contracted during ASLR with compression compared to ASLR without compression (p < 0.001)
Stuge et al78
Manometry with a vaginal balloon catheter
Women >6 months postpartum with PGP onset during pregnancy or within 3 months post-delivery
Higher vaginal rest pressure in women with PGP
Stuge et al122
II Muscle Length
Ultrasound measurement of levator hiatus
49 pairs of women at least 6 months postpartum- with PGP and without PGP
Women with PP-PGP had a significantly smaller levator hiatus at rest as compared to controls The area of levator hiatus was significantly smaller
Stuge et al78

43
during ASLR in women with PP-PGP compared to the control group
Ultrasound measurements of levator hiatus area
Women >6 months postpartum with PGP onset during pregnancy or within 3 months post-delivery
Smaller Levator hiatus area in PGP vs. control
Stuge et al122
Abbreviations: ADD, adductor ASLR; Active straight leg raise; c-section, cesarean section delivery; FABER, Flexion, abduction, external rotation test; LBP, Low back pain; LOE, Level of evidence; Sn, Sensitivity; Sp, Specificity; PFM, Pelvic floor muscles; PGP, pelvic girdle pain , PP-PGP, Postpartum Pelvic Girdle Pain; P4, Posterior Pelvic Pain Provocation Test

44
Table 7. Summary of Evidence Regarding DRA in Postpartum Women
LOE Study Population Findings on DRA in postpartum population Citation
II Women 12-14 months postpartum with DRA (IRD ≥ 2.2 cm; n = 18) and without DRA (IRD < 2.2 cm; n = 22)
• Women with DRA demonstrated significantly lower trunk muscle rotation torque and scored lower on the sit-up test than those without DRA.
• IRD was negatively correlated with both trunk rotation torque (rho=-0.367) and sit-up test score (rho=-0.514).
Hills et al167
Postpartum women who were running a minimum of once per week (n=507)
• Among women who had given birth to a child within the past 2 years, 32% perceived RA separation
• Compared with primiparous women, multiparous women were more likely to report a perceived RA separation (OR, 2.11; 95% CI, 1.08-4.26)
• The odds of perceived RA separation were greater among women with a Caesarean section delivery than women who never had a Caesarean section (OR, 2.20; 95% CI, 1.05-4.70)
• Postpartum SUI increased the odds of perceived RA separation more than 2-fold (OR=2.25; 95% CI, 1.02-5.08; p=0.040)
• Antenatal weight training decreased the odds of abdominal separation (OR, 0.51; 95% CI, 0.26-0.96)
Blyholder et al168
Primiparous postpartum women (n=84)
• The prevalence of DRA decreased from 100% at gestational week to 35-39% at 6 months
postpartum.
Fernandes da Mota et al169
Postpartum women (n=40) and age-matched nulliparous females (n=20) Measurements taken 4 to 8 weeks and 6 to 8 months after childbirth
• The IRD at 2.5 cm above the umbilical ring and at the upper margin of the umbilical ring decreased (p=.013 and p=.002, respectively)
• A negative correlation between IRD and abdominal muscle function at 7 weeks and 6 months postpartum was found (r=0.34 to 0.51; p<.05, except for trunk flexion strength at 6 months postpartum [p=.064]).
• IRD changes between 7 weeks and 6 months postpartum were correlated with improvement in trunk flexion strength (Spearman rho=0.38, p=.040).
• At 6 months after childbirth, postpartum women had greater mean IRDs at all 4 locations (from cranial to caudal: 1.80 ± 0.72, 2.13 ± 0.65, 1.81 ± 0.62, and 1.16 ± 0.58 cm) than those of nulliparous females (0.85 ± 0.26, 0.99 ± 0.31, 0.65 ± 0.23, and 0.43 ± 0.17 cm) (all p<.001).
Liaw et al96
Women seeking medical care for lumbar or pelvic area diagnoses who had delivered at least one child (n=39, PD) Women with a history of LAP (n=8) CON (n=53)
• Incidence of DRA was 74.4% for the PD, 50.9% in the CON, and 100% in the LAP groups
• 47% of the measurements at the umbilicus showed a DRA, while 35% below the umbilicus, and 35% above was classified as DRA.
• There was a significant difference between those with and without DRA for the VAS scores for abdominal and pelvic area pain
Parker et al124

45
Abbreviations: DRA, Diastasis Recti Abdominis; CON, Control group; IRD, Inter-rectus distance, LAP, laparoscopy; LOE, level of evidence; PD, pelvic diagnosis; RA, Rectus Abdominis; SUI, stress urinary incontinence; VAS, Visual Analog Scale

46
Table 8: Sacroiliac Joint Load Transfer Impairment with or without Asymmetry
History Key Tests & Signs Differential
Diagnosis Intervention Static Dynamic
Pain and/or clicking at the region of the SIJ Unilateral pain Pain and instability with asymmetrical loading of LE/pelvis during functional mobility activities57
History / Risk Factors Prior episodes of PGP and/or LBP; SUI; PFD
Alignment: ASIS & PSIS alignment asymmetry (in more hypermobile cases changes may occur with variations of hip positions of ABD/ADD) lumbar alignment is asymmetrical Source Tests: Standing Compression: manual compression may aggravate until manual positional correction of asymmetry with compression is performed if pain abolishes or lessens with compression indicates need for belt stabilization or taping Provocative tests: 1/5 positive tests <8 w postpartum; Avoid Gaenslen’s test within the first 4 w postpartum. 3/5 positive tests >8 w postpartum (FABER, thigh thrust (P4); Sacral Spring, ASIS distraction (supine), Sacral compression (side lying) Muscle Length impairments Unilateral length changes
1. shortened hip flexor, spine extensor on the anterior rotated side;
Muscle Strength/Performance Impairments Poor unilateral control of abdominal oblique muscles, transverse abdominis, hip extensors, lateral rotators and abductors, multifidus and pelvic floor. ASLR: observe unilateral performance impairments: pelvic rotation with complaint of difficulty and/ or SIJ pain performing ASLR. Compression or positional correction with compression abolishes pain and/or increases ease of ASLR. Movement tests: Standing: Forward bending: Lumbar flexion > hip flexion, Prone hip extension: pain along the joint line. suspect positional impairment Quadruped: increased sacral region pain with position Single leg stance: (+) for pain (+Stork84,85,127, Modified Trendelenburg test), Unilateral + SLS testing occurs with less involved cases of hypermobility; Functional mobility activities: pain with rolling, sit to stand, stair climbing, transitional positions Gait: inability to transfer load of trunk from above to LE, increased trunk shift with loading or inability to load if form closure is lost. Sits asymmetrically
Movement Impairment Dx105 Lumbar Extension-Rotation Lumbar Flexion-Rotation Femoral Adduction Femoral Adduction/Medial Rotation Hip posterior glide Hip anterior glide/medial rotation Visceral Origin: Gastrointestinal, Genito-urinary, Reproductive organ disease Metastatic disease/cancers: abdominal organs, uterus, bladder, Musculoskeletal Origin: Lumbar disc Disease Inflammatory arthritis: Ankylosing spondylitis, Psoriatic arthritis, rheumatoid arthritis, lupus, Reiter syndrome, Compression fractures Labral Tear (hip) Snapping hip syndrome (groin pain) Sacral or pubic arch stress fracture (military, high impact activities, postpartum osteoporosis) Hormone Imbalance affecting ligamentous structures
1. Bracing (belt)
or taping103,116,154,155,170-173 2. Motor recruitment of Gluteal, back, abdominal, PFM20,82,122 3. Education to minimize pain during functional activities16,98,138-146 (rolling,
sit to stand, single leg stance, walking, breast feeding/childcare) 4. Consider assistive device if functional mobility severely impaired or painful Address specific movement impairments that would cause rotational stress 5. Joint Mobilization/Manipulation: Consider if asymmetry does not resolve with belt, exercise and functional training100

47
2. shorten hamstrings, gluteal muscles on posterior rotated side
Abbreviations: ABD, abduction; ADD, adduction; ASIS, anterior superior iliac spine; ASLR, Active straight leg raise; FABER, Flexion, abduction, external rotation test; LBP, Low back pain; SLS, single leg stance; SUI, stress urinary incontinence; PFD, Pelvic Floor Dysfunction; PFM, Pelvic Floor Muscle; P4, Posterior Pelvic Pain Provocation Test; PSIS, posterior superior iliac spine; SIJ, sacroiliac joint; VAS, Visual Analog Scale; w, weeks

48
Table 9: Pelvic Girdle Load Transfer Impairment (≥2 joints)
History Key Tests & Signs Differential
Diagnosis Intervention Static Dynamic
Pain and/or clicking at the region of one SIJ Bilateral Sacral Pain, Simultaneous unilateral posterior and anterior pain, or pain in all three regions is indicative of more involved case presentation Pain and instability with loading of Lower extremity/pelvis during functional mobility activities (bilateral symptoms) History / Risk Factors Prior episodes of PGP and/or LBP; SUI; PFD
Alignment: Symmetrical pelvic landmarks, flat lumbar spine Source Tests: Standing Compression: abolish or lessen pain indicates need to belt Provocative tests: 1/5 positive tests <8 w postpartum; Avoid Gaenslen’s test within the first 4 w postpartum. 3/5 positive tests >8 w postpartum: FABER/Patrick’s, P4; Sacral Spring, ASIS distraction (supine), Sacral compression (side lying) Muscle Length impairments long abdominal muscles due to the postpartum period
Muscle Strength/Performance Impairments Poor control of abdominal oblique muscles, transverse abdominis, hip extensors, lateral rotators and abductors, multifidus and pelvic floor. bilateral presentation, ASLR: Bilateral observation of pelvic rotation with difficulty and/ or SIJ pain, Compression abolishes pain and/or increases ease of ASLR. Movement tests: Standing: Forward bending: Lumbar flexion > hip flexion, Prone hip extension: delayed onset of gluteals, will test weak Quadruped: increased sacral region pain with position Single leg stance: (+) bilaterally for pain (+Stork, Modified Trendelenburg test), Bilateral +SLS testing indicates need for assistive device Functional mobility activities: pain with rolling, sit to stand, stair climbing, transitional positions Gait: inability to transfer load of trunk from above to Lower Extremity, increased trunk shift with loading or inability to load if form closure is lost. Sits in lumbar flexion.
Movement Differential105 Lumbar Flexion Lumbar Extension Femoral Adduction Femoral Adduction/Medial rotation Hip posterior glide Hip anterior glide/Medial rotation SIJ or PS Load transfer Impairment Visceral Origin: Gastrointestinal, Genito-urinary, Reproductive organ disease Metastatic disease/cancers: abdominal organs, uterus, bladder, Musculoskeletal Origin: Lumbar disc Disease Inflammatory arthritis: Ankylosing spondylitis, Psoriatic arthritis, rheumatoid arthritis, lupus, Reiter syndrome, Compression fx; Labral Tear (hip); Snapping hip syndrome (groin pain); Sacral or pubic arch stress fx (military, high impact activities, osteoporosis) Hormone Imbalance affecting ligamentous structures
1. Bracing (belt)116,154,155,170-173 2. Appropriate Motor recruitment of Gluteal, back, abdominal, PFM including timing of contraction, avoiding rotational stressors across the pelvis 3. Education to minimize pain during
functional activities16,98,138
-146 4. Consider assistive device if functional mobility severely impaired or painful172,158
5. Joint Mobilization/Manipulation not indicated in the presence of symmetrical joints Address specific movement impairments that would cause rotational stress82,152,174

49
Abbreviations: ABD, abduction; ASLR, Active straight leg raise; ASIS, anterior superior iliac spine; FABER, Flexion, abduction, external rotation test; fx, fracture; LBP, Low back pain; SLS, single leg stance; SUI, stress urinary incontinence; PFD, Pelvic Floor Dysfunction; PFM, Pelvic Floor Muscle; PGP, Pelvic Girdle Pain; P4, Posterior Pelvic Pain Provocation Test; PSIS, posterior superior iliac spine; SIJ, sacroiliac joint; w, weeks

50
Table 10: Pubic Symphysis Load Transfer Impairment
History Key Tests & Signs Differential Diagnosis Intervention
Static Dynamic Pain at the region of the PS that may or may not radiate to the groin. Anterior pain and instability in unilateral stance; pain with walking; pain with prolonged sitting with legs crossed or in asymmetrical positions (side lying, stair climbing, inclines); pain with transitional movements (sit to stand and rolling) Uro-genital symptoms may be present 31,154,175(dyspareunia, urinary incontinence, urgency frequency, pain with urination, vulvar pain)
Activity/history History of trauma during delivery, SPD during pregnancy or excessive unilateral leg loading in postpartum (lower limb injury or History of LLD)
Alignment: Without Asymmetry: Symmetrical pubic rami With Asymmetry: pubic rami asymmetry (changes with variations of hip positions, ABD/ADD, in more mobile cases symptoms may persist unless compression occurs). Palpation: Pain to palpate at PS62,112 Source Tests: Iliac Compression Test: in standing or supine128 improves pain With Asymmetry: positional correction with compression abolishes pain or lessens pain Provocative tests: Positive FABER/Patrick’s test75
Muscle Strength /Performance Impairments: Poor performance of abdominal, adductor and gluteal muscles. Movement tests: Modified Trendlenberg71: increases pain at PS Supine Hip flexion; increases pain at PS Supine abduction lateral rotation from a hip flexed position (aka bent knee fall-out): pain with leg fall out at PS or with initiation of return Gait: Increased lateral trunk shift with single leg stance, assistive device needed in more severe cases Standing Trunk motions: negative for pain
Movement Impairment 105 Femoral Adduction Femoral Adduction/Medial Rotation Hip anterior glide/Medial rotation Lumbar Rotation-Extension Lumbar Flex/rotation Lumbar Flexion Lumbar Extension Thoracic Flexion-Rotation Visceral Origin: Gastrointestinal, Genito-urinary, Reproductive organ disease Metastatic disease/cancers: abdominal organs, uterus, bladder, Musculoskeletal Origin: Osteitis PS, bone bruise, bony edema, Arthritis, fx: Compression/stress, Osteoporosis-related, PS stress fx; Adductor or Rectus abdominis strain, Cam/ Pincer Deformity, Hip impingement Hernia: Inguinal, Abdominal Fascia Thoracic disc Disease Inflammatory arthritis: Ankylosing spondylitis, Psoriatic arthritis, rheumatoid arthritis, Reiter syndrome, lupus Hormone Imbalance affecting ligamentous structures
1. Bracing (pelvic belt)146,154,170,172,173,176,177 2. Exercises of the gluteal, hip adductor and abdominal muscles.177 3. Appropriate timing for motor recruitment of gluteal, back, abdominal, PFM.174 4. Treatment of movement impairments that cause rotational stress14,103 (walking, rolling in bed, stair climbing, car transfers, carrying, ADLs) 5. Education to minimize pain during functional activities16,98,138-146
(avoid end range hip flexion and abduction) 6. Consider assistive device if functional mobility severely impaired or painful152,158 7. Joint Mobilization: If poor tolerance to stabilization, correct any Positional Impairment.178
Abbreviations: ABD, abduction; ADD, adduction; ADLs, activities of daily living; FABER, Flexion, abduction, external rotation test; fx, fracture; LLD, leg length discrepancy; SPD, symphysis pubis dysfunction

51
Table 11: Prognosis for Persistent PP-PGP LOE Prognostic
Factor Reported
Description of Participants
Mean (SD)
Prevalence of Persistent PP-PGP
Level of Disability reported in PP-PGP
Results Citation
II PP-PGP Prevalence w/Disability
N=295 Time postpartum: 12 years Age: 43.3 (4.6)
40.3% (n=119)
Self-reported health: Fair to poor (OR: 2.62 to 7.26, p<0.0001)
Spontaneous recovery with no recurrences is unlikely for a subgroup of women with PP-PGP
Bergstrom et al18
N=284 Time postpartum: <4 w to >12 w Age: 25 (4)
41% (n=116)
Moderate to high levels of disability on ODI was reported in 100% (n=116) of PP-PGP group compared to 16.7% (n=28) of No PGP group
Pain presenting at 0 to 4 w persisted at 3 months postpartum
Mukknannavar et al21
N=215 Time postpartum: 12 w to 1 year Age: 31 (4)
30% at 12 w 31% at 1 year
Physical function at 12 w and 1 year were unchanged
No improvement noted at 1 year postpartum
Robinson et al179
N=272 Time postpartum: 3 months Age: 30 (18, 44)
33% (n=89) had some form of LPP 11% (n=46): PP-PGP 17% (n=23): LPP
40% had moderate to severe disability
One in three women had a LPP classification at 3 months postpartum
Gutke et al19
N= Time postpartum: 1 w Age: 30.8
Baseline PP-PGP persisted at 12 w in 15% of cases
All groups improved with treatment
Elden et al180
PP-PGP Predictors
N=345 Time postpartum: 11 years Age: 30 (23, 39)
10.7% (37/345)
Decreased ability to perform daily activities (p<.001), lower self-efficacy (p=.046), decreased HRQL (p<.001), higher levels of anxiety & depression (p< 001), more prone to pain catastrophizing, and worked significantly fewer h/w (p=0.032)
Number of positive pain provocation tests (OR= 1.79), history of LBP (OR=2.28), positive PS pressure test (OR=2.01), positive Faber (Patrick's) test (OR=2.22), positive modified Trendelenburg test (OR=2.20)
Elden11
N=176 Time postpartum: 14 months Age: 31.9 (3.8)
15.3% (n=27) (80.7%) reported pain 115 (65.3%)
Self-reported health: Poor or quite poor
Lower pain levels Bergstrom et al181

52
reported recurrent pain 27(15.3%) reported continuous pain
N= Time postpartum: 15 months Age: 31 (28, 33)
62%
Increased age combined with and reduced trunk flexor endurance, and reduced hip extension strength combined with level of disability
Sjodahl et al20
N=273 Time postpartum: 6 months
29% (n=79)
Higher catastrophizing and more restrictive physical function = 2x risk
Olsson et al137
N= Time postpartum: 6 months
264 no LBPP 168 recurrent LBPP 32 continuous
PP-PGP predictors: Previous LBP
Morgan et al182
N=65 Time postpartum: 2 years
85% treatment group 47% control group
PP-PGP predictors: Minimum disability
Stuge et al134
N=341 Time postpartum: 2 years
8.6%
PP-PGP predictors: Combined PS and bilateral posterior pelvic pain during pregnancy had slower recovery postpartum than among women with fewer pain locations
Albert et al166
Abbreviations: hr, hours; HRQL, Health Related Quality of Life; LOE, level of evidence; LBP, low back pain; N, number; PP-PGP, Postpartum Pelvic Girdle Pain; PGP, Pelvic Girdle Pain; w, weeks

53
Table 12: Intervention for PP-PGP: Stabilization Exercise
LOE Intervention Type
Description of Intervention
Description of Participants
Outcomes Results Citation
I Stabilization exercises vs. general exercise
3x/wk x 8 wks 2 groups: Supervised stabilization exercises vs. general exercise
N=68 Time postpartum: 2 to 4 weeks
Pain (VAS) TrA muscle thickness (ultrasound) PFMC
Significant increases in TrA muscle thickness and PFMC in stabilization exercise group compared to general exercise group. Significant decreases in pain within-groups pre-to post-intervention in both stabilization and general exercise groups. No significant differences between groups for pain reduction.
Ehsani et al147
Stabilization exercises + electrothermal modalities
3x/wk x 6 wks Individualized stabilization exercises Infrared radiation and continuous ultrasound on posterior lumbopelvic region
N=34 Time postpartum: 3 to 12 months
Pain (VAS) Disability (ODI) PPT at soft tissue 3 cm lateral to the spinous processes (L1-S5)
Significant improvements in pain, disability, and PPT in both groups. Significantly greater improvements in pain, disability, and PPT in the stabilization group compared to usual care.
Saleh et al148
Stabilization exercises + PFMC
3 sessions/wk x 12 wks Individualized stabilization exercises targeting multifidus and transversus abdominis Intervention group received PFMC training in addition to stabilization exercises
N=40 Time postpartum: At least 3 months
Pain (VAS) Disability (ODI) Trunk ROM (Schober test) PFM (Kegel perineometer)
Significant differences in pain, disability, and PFM strength in favor of stabilization exercise + PFMC group than stabilization exercises alone. Both groups significantly improved in pain, disability, trunk ROM, and PFMC over time.
El Deeb et al149

54
Individualized rehabilitation + chiropractic care (spinal manipulative therapy)
12 individualized rehab sessions (w/ w/o chiro care) over 20 weeks HEP of stabilization exercises + LE stretching and strengthening, postural exercises provided to all participants
N=11 Time postpartum: 3 to 6 months
Pain (NRS, PGQ) Disability (ODI) General health status
No significant differences between groups on pain, disability or general health status. Both groups improved in pain and disability over time. No change in general health status in either group.
Gausel et al16
Stabilization exercises + PFMC, electrotherapy modalities
45-min sessions, 3x/wk x 6 wks Individualized PT, Stabilization exercises w/PFMC w/ and w/o electrotherapy modalities
N=36 Time postpartum: 12 weeks
Pain (VAS) Disability (ODI) PFMC at rest PFMC w/ MVC
Significant differences in pain, disability and PFMC MVC in favor of intervention group (p<0.05). No difference in PFMC at rest within or between groups.
Teymuri et al123
Stabilization exercises + aerobic exercise, PFMC, stretching
60-min/wk x 12 wks Group fitness classes during pregnancy Stabilization exercises, PFMC, stretching
N=105 nulliparous Time postpartum: 6 to 8 weeks
Presence of PGP (questionnaire)
No differences in PP-PGP between women who exercised during pregnancy and controls (OR=0.38, CI=0.13–1.10, p=0.07).
Haakstad et al150
Stabilization exercises
2 sessions/day x 3 days Intervention group: Core stabilization exercises along with postural correction in different positions (i.e., supine, crook lying and half sitting position & prone position) Control group: Simple back strengthening exercises in different positions (i.e. supine, crook lying)
N=40 Time postpartum: 0-2 days
Restriction in ADLs – mobility, dressing, etc. and IADLs complex tasks Muscle power of LEs (MMT) Mobility (Dependent or Independent)
Significant differences identified in favor of the intervention group for LE muscle power (p<0.001), improved IADLs (p<0.001), and improved mobility (p<0.0001).
Chaudry et al151
I Stabilization exercises
Home-based exercise, at least 2x/daily, focused on TrA, multifidus, PF
N=88 Time postpartum: At least 8 weeks
Pain (VAS) Disability (ODI) HRQOL
No difference between groups on pain intensity, HRQOL, or ODI between groups
Gutke et al139

55
Muscle function: Hip EXT Back flexor endurance Back extensor endurance Pelvic floor Gait speed
Significant differences in pain intensity at 3-month follow-up, favoring intervention group (p=0.011) Significant differences between groups in Hip EXT strength at 3-month follow-up (p=0.047) Improvement in ODI from baseline to 6-month follow-up within groups (p<0.05)
I Stabilization exercises
Comparison of 3 treatments: Standard treatment alone Standard treatment with acupuncture Standard treatment with stabilization exercises during pregnancy
N=386 Time postpartum: 12 weeks
Pain (VAS) Presence of PP-PGP (test battery)
3/4 women were pain-free at 12 weeks postpartum 99% of women tested negative for PGP at 12 weeks postpartum No difference in pain or PGP testing between groups
Elden et al140
Group training 1 (60-min session)/wk x 12 wks during pregnancy
N=301 nulliparous Time postpartum: 12 weeks
Presence of LPP Functional status (DRI) PFM strength
Significantly reduced incidence of pain (p=0.056) and increased functional status (p=0.011) postpartum in women who participated in group exercise intervention in pregnanc.
Morkved et al143
Group training 1 (120-min session), 2x/wk x 4 wks during pregnancy
N=569 with posterior PGP or PS pain Time postpartum: 6, 12 months
Pain (VAS) Presence of PGP (P4 test)
No significant differences in pain score or presence of PGP at 6 or 12 months postpartum between groups
Haugland et al152

56
I Stabilization exercises w/manual therapy, education
PT w stabilizing exercises or PT alone Home-based w equipment in home, thoroughly described on p. 353 Included mobilization, massage, education, physical activity (Per Stuge 2006 included “Emotions/Awareness” 20 weeks of treatment (1 session q2 wks)
N=81 Time postpartum: 6 to 16 weeks
Pain (VAS) Functional status (ODI) Quality of life (SF-36) Hip strength (ADD/ABD) (HHD) Endurance of back muscles (Sorensen Test), ASLR test
Significant differences in pain, disability, physical QOL scale and physical tests in favor of the stabilization exercises group Disability reduced by 50% in the intervention group Physical testing results were significant after the Intervention only, not at the 1-year postpartum follow-up
Stuge et al153
N=65 Time postpartum: 1 year, 2 year
Pain Disability QOL
Gains maintained at 2 years postpartum in the intervention group Controls reduced disability at 2 years, without intervention
Stuge et al134
I Stabilization exercises w/belt, education
Experimental Group: Diagonal trunk exercises with educational video, ergonomics, and pelvic belt (n=16) Control Group 1: Longitudinal trunk exercises with educational video, ergonomics, and pelvic belt (n=14) Control Group 2: No exercise. Educational video, ergonomics, and pelvic belt (n=14)
N=44 Time postpartum: 6 weeks to 6 months
Pain (VAS, evening pain severity; morning pain severity) Fatigue (VAS, evening fatigue severity; morning fatigue severity); General Health (NHP); Global Improvement (1, 2, 3); Mobility of pelvic joints (x-ray, mm)
No significant differences between groups Educational video and pelvic belt yielded comparable results to video-based trunk exercise intervention
Mens et al146
III Stabilization exercises, No belt
2 sessions/week, total of 14 sessions over 8 weeks Individualized PT Manual therapy, soft tissue mobilization, therapeutic exercise, gait training, patient education.
N=1 Time postpartum: 4 days
Pain (VAS) Functional status (PSFS)
PP-PGP pain decreased from 10/10 to 0/10 on VAS
Renard & Abraham138

57
Abbreviations: ABD, Abduction; ADD, Adduction; ADLs, Activities of daily living; ASLR, Active straight leg raise; EXT, extension; HHD, Hand held dynamometer; DRA, Diastasis Recti Abdominis; IADLs, Instrumental Activities of Daily Living; IRD, Inter-rectus distance; LPP, lumbopelvic pain; LOE, Level of evidence; MMT, Manual muscle test; MVC, maximal voluntary contraction; N, number; NHP, Nottingham Health Profile; NRS, Numeric Rating Scale; ODI, Oswestry Disability Index; PPT, Pain Pressure Threshold; PFMC, pelvic floor muscle contraction, PFM, pelvic floor muscle; PGP, Pelvic Girdle Pain; PP-PGP, Postpartum Pelvic Girdle Pain; P4, Posterior Pelvic Pain Provocative Test; PGQ, Pelvic Girdle Questionnaire; QOL, quality of life; RA, Rectus Abdominis; ROM, range of motion; SF-36, Short Form 36; PSFS, Patient specific functional scale; PT, Physical Therapy; TrA, transverse abdominis; VAS, visual analog scale

58
Table 13: Intervention for PP-PGP: Pelvic Belt
LOE Description of Intervention
Participants Outcomes Results Citation
I Experimental Group: Diagonal trunk exercises with educational video, ergonomics, and pelvic belt (n=16) Control Group 1: Longitudinal trunk exercises with educational video, ergonomics, and pelvic belt (n=14) Control Group 2: No exercise. Educational video, ergonomics, and pelvic belt (n=14)
N=44 Time postpartum: 6 weeks to 6 months Mean=4.1 months (Range: 1.7 to 5.6 months)
Pain (VAS, evening pain severity; morning pain severity) Fatigue (VAS, evening fatigue severity; morning fatigue severity) General Health (NHP) Global Improvement (1, 2, 3) Mobility of pelvic joints (x-ray, mm)
No significant differences between groups. Educational video and pelvic belt yielded comparable results to video-based trunk exercise intervention.
Mens et al146
I Belt = Rehband®. No specifics on tension, wear schedule, or frequency of use. Compared effectiveness of 3 different intervention programs. Belt was provided in all 3 groups. 3 groups, all received belt: Pelvic belt + info: (n=40) Home exercise, belt + info: (n=41) In clinic exercise, belt + info: (n=37)
N=118 Women tested positive in >/= 3 pelvic pain provocation tests in late pregnancy Time postpartum: 3, 6, and 12 months.
VAS Pain localization Pain type DRI
Use of a pelvic belt with information achieved comparable outcomes to use of a pelvic belt with information and either home or in-clinic exercise. No differences in pain or activity across the 3 groups. Significant reduction in pain intensity and improvements in higher activity ability from pregnancy to 12 months postpartum (p=0.000) across all 3 groups.
Nilsson-Wikmar et al144
II 2 types of belts tested: Rafys belt© and Erasmus belt© Investigated changes in hip ADD force with the addition of a pelvic belt in PP-PGP and controls
N=86 Time postpartum: >/= 6 months PP-PGP confirmed with both ASLR, P4 testing (+); pain duration > 6 months
% increase in ADD force (HHD) in 2nd ASLR attempt after tightening belt NRPS QBPDS ASLR, P4
Women with PP-PGP demonstrated significantly increased Hip ADD force with addition of a belt (from 107+/-51 N to 129+/-59 N) (p<0.00001). Women in the control group demonstrated comparable hip ADD force with and without the belt (p=0.67).
Mens90
II A belt of non-elastic material was used (model 3221/3300, Rafys, Hengelo, The Netherlands) 5 cm wide
N=25 Time postpartum: Within 5 years
VAS QBPDS SIJ laxity
Decreased SIJ laxity and reduced ASLR scores with belt compared to without belt.
Mens et al155

59
at the anterior and 7 cm at the posterior side. Tension range: 50 to 100 Newtons High position: Just below the ASIS. Low position: At PS level Doppler imaging was used to measure propagation of vibratory waves through SIJ. Measurement was performed on the SIJ dorsally pre- and post-belt application to measure the change in laxity.
VAS >30 mm (“moderate to severe”)
ASLR test
High position decreased SIJ laxity to a significantly greater degree (1.3 TU, SD=1.7 TU) than low position (0.6 TU, SD1.0 TU) (p=0.006). Positive correlation between decrease in mean laxity value w/belt in both high position (Pearson’s correlation coefficient 0.54, p=0.005) and low position (Pearson’s correlation coefficient 0.57, p=0.003) compared with no belt.
Abbreviations: ADD, Adduction; ASLR, Active Straight Leg Raise; ASIS, Anterior superior iliac spine; cm, centimeters; DRI, Disability Rating Index; LOE, Level of Evidence; N, number; NHP, Nottingham Health Profile; NRS, Numeric Rating Scale; NPRS, Numeric Pain Rating Scale; QBPDS, PP-PGP Postpartum Pelvic Girdle Pain; Quebec Back Pain Disability Score; SIJ, Sacroiliac Joint; TU, threshold units; VAS, Visual Analog Scale

60
Table 14: Intervention for PP-PGP: Manual Therapy LOE Intervention
Type Description of Participants
Description of Intervention
Outcomes Results Citation
I Manual therapy (chiropractic spinal manipulative therapy) +individualized rehabilitation
N=11 Time postpartum: 3 to 6 months
12 sessions over 20 weeks Intervention group received 12 individualized rehab sessions w/spinal manipulative therapy. Control group received 12 individualized rehab sessions. Both groups received HEP of stabilization exercises + LE stretching and strengthening, postural exercises.
Pain (NRS, PGQ) Disability (ODI) General health status
No significant differences between groups on pain, disability or general health status. Both groups improved in pain and disability over time. No change in general health status in either group.
Gausel et al16
Manual therapy (OMT)
N=80 Time postpartum: 3 to 15 months
1x/2 wks x 6 wks Intervention group received OMT (40-60 min sessions) at baseline, 2, 4, and 6 wks Controls waitlisted Time to follow-up: 8 wks, 3 months post-intervention
Pain (VAS) Disability (ODI)
Both groups significantly improved in pain over time. Larger improvements in pain (between-group difference of means, 4.8; 95% CI, 4.1-5.4; p<.001) and disability (between-group difference of means, 10.6; 95% CI, 9.9-13.2; p<.005) found in the intervention group.
Schwerla et al156
Manual therapy w/ stabilization exercises, education, physical activity
N=81 Time postpartum: 6 to 16 weeks
PT with or without stabilizing exercises Home-based w equipment in home, Included mobilization, massage, education, physical activity 20 weeks of treatment
Pain (VAS) Disability (ODI) Quality of life (SF-36) Hip strength (ADD/ABD) (HHD) Endurance of back muscles (Sorensen Test) ASLR test
Significant differences in pain, disability, physical QOL scale, and physical tests in favor of the stabilization exercises group. Disability reduced by 50% in the intervention group. Physical testing results were significant after the
Stuge et al145

61
intervention only, not at the 1-year postpartum follow-up.
N=65 Time postpartum: 1 year, 2 year
Pain (VAS) Disability (ODI) Quality of life (SF-36)
Gains maintained at 2 years postpartum in the intervention group. Controls reduced disability at 2 years, without intervention.
Stuge et al134
Manual therapy (HVTT)
N=69 Time postpartum: Within 1 year
1 or 2 sessions of HVTT over maximum 1 week’s time HVTT (to more symptomatic innominate in supine with ipsilateral side bending and contralateral trunk rotation, Grade 5), then 10 repetitions of hand-heel rock exercise in quadruped Follow-up: 2-4 day post-HVTT. Repeated up to 1 more time if ODI<50% improved
Pain (VAS, body diagram) ODI FABQ
80% of subjects experienced significant reduction in symptoms post-HVTT. Non-response to mobilization predicted by at least 2 of 3 variables with 87% accuracy. Variables included: age>35, VAS-Best>3, negative prone knee bend test. No subject had higher pain or disability after intervention.
Al-Sayegh et al100
Manual therapy w/ stabilization exercises, education, physical activity
N=81 Time postpartum: 6 to 16 weeks
20 weeks of treatment PT with or without stabilizing exercises Home-based w equipment in home, Included mobilization, massage, education, physical activity
Pain (VAS) Disability (ODI) Quality of life (SF-36) Hip strength (ADD/ABD) (HHD) Endurance of back muscles (Sorensen Test) ASLR test
Significant differences in pain, disability, physical QOL scale, and physical tests in favor of the stabilization exercises group. Disability reduced by 50% in the intervention group. Physical testing results were significant after the intervention only, not at the 1-year
Stuge et al145

62
postpartum follow-up.
N=65 Time postpartum: 1 year, 2 year
Pain (VAS) Disability (ODI) Quality of life (SF-36)
Gains maintained at 2 years postpartum in the intervention group. Controls reduced disability at 2 years, without intervention.
Stuge et al134
Abbreviations: ABD, Abduction; ADD, Adduction; ASLR, Active Straight Leg Raise; FABQ, Fear Avoidance Behavior Questionnaire; LOE, Level of Evidence; HHD, Hand held dynamometry; HVTT, High velocity thrust technique; ODI, Oswestry Disability Index; OMT, Osteopathic Manual Therapy; PGQ, Pelvic Girdle Questionnaire; NRS, Numeric Rating Scale; SF-36, Short Form 36 Physical functioning; VAS, Visual Analog Scale

63
Table 15: Recommendations for Future Research for PP-PGP
Factors Specific to Postpartum Participants
Include a comprehensive description of participants to address confounding factors unique to the postpartum population (e.g., parity, delivery-related factors, presence of postpartum depressive symptoms, lactation status, etc.).
Prognosis for Recovery & Clinical Course
Investigate fear-avoidance behaviors and mental health to identify women not following a “normal” course of recovery after PP-PGP. Investigate factors that contribute to persistent pain syndrome. Investigate the implication of these confounding variables on continued pain and disability at 1 and 2 years postpartum. Follow groups as a whole rather than just following painful cohorts during pregnancy into the postpartum period.
Examination Include standing single limb loading tests for determining pain and movement impairments. Compare the value of provocation tests to functional measures in order to streamline the examination. Examine the best measures of muscle performance to guide intervention. Investigate the effect of muscle length changes in individuals with PP-PGP. Investigate a potential relationship between DRA and PP-PGP. Consider classifying abdominal muscle performance (over or under active) in the presence of DRA and/or pelvic floor disorders to understand contributions to PP-PGP.
Investigate the biomechanical effects of pelvic belt use, especially during ASLR testing, standing double-limb and single limb support testing, and functional tasks.
Diagnosis Consider classification systems that includes pain location, response to treatment and presenting movement impairments in PP-PGP.
Intervention Explore educational methods for PP-PGP in relation to outcome. Investigate the effects of functional training, including gait, double-limb, single-limb, transitional movements, ADLs/IADLs, and child care tasks. Include a comprehensive description of exercise interventions, patient education, specific functional activity training, and use of belt. Interventions should include frequency, duration, intensity, supervision, and compliance. Future research should investigate the biomechanical effects of pelvic belt use, especially during ASLR testing, standing double-limb and single limb support testing, and functional tasks. Future research should investigate the use of a pelvic belt within the first 4 weeks postpartum.

64
Longer follow-up after intervention to investigate relationships between increased muscle strength postpartum, pain, and disability.
Abbreviations: ADLs, Activities of daily living; IADLs, Instrumental Activities of Daily Living; ASLR, Active straight
leg raise; DRA, Diastasis Recti Abdominis; PP-PGP, Postpartum Pelvic Girdle Pain

65
Figure 1. Clinical Decision-Making Flow Chart for PP-PGP
Legend: jts, joints; PG, pelvic girdle; PP-PGP, postpartum pelvic girdle pain; PS, pubic
symphysis; SIJ, sacroiliac joint; STM, soft tissue mobilization

66
References
1. Ostgaard HC. What is Pelvic Girdle Pain. In: Vleeming A MV, Stoeckart R., ed. Movement, Stability & Lumbopelvic Pain. Edinburgh: Churchill Livingstone; 2007:354.
2. Maigne JY, Chatellier G, Faou ML, Archambeau M. The treatment of chronic coccydynia with intrarectal manipulation: A randomized controlled study. Spine. 2006;31(18):E621-627.
3. Berens P. Overview of the postpartum period: Normal physiology and routine maternal care. In: Post TW, ed. UpToDate. UpToDate; 2021. Accessed January 7, 2019. https://www.uptodate.com/contents/overview-of-the-postpartum-period-normal-physiology-and-routine-maternal-care#H1205598813
4. Oswald C, Higgins CC, Assimakopoulos D. Optimizing pain relief during pregnancy using manual therapy. Can Fam Physician. 2013;59(8):841-842.
5. WHO Recommendations on Postnatal Care of the Mother and Newborn. Geneva: World Health Organization; 2013 Oct. Available from: https://www.ncbi.nlm.nih.gov/books/NBK190086/
6. Gutke A, Boissonnault J, Brook G, Stuge B. The severity and impact of pelvic girdle pain and low back pain in pregnancy: A multinational study. J Womens Health. 2018;27(4):510-517.
7. APTA Clinical Practice Guideline Process Manual, Revised. Alexandria, VA: American Physical Therapy Association; 2020.
8. Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, Willard FH. The sacroiliac joint: An overview of its anatomy, function and potential clinical implications. J Anat. 2012;221(6):537-567.
9. Albert HB, Godskesen M, Korsholm L, Westergaard JG. Risk factors in developing pregnancy-related pelvic girdle pain. Acta Obstet Gynecol Scand. 2006;85(5):539-544.
10. Gutke A, Ostgaard HC, Oberg B. Predicting persistent pregnancy-related low back pain. Spine. 2008;33(12):E386-E393.
11. Elden H, Gutke A, Kjellby-Wendt G, Fagevik-Olsen M, Ostgaard HC. Predictors and consequences of long-term pregnancy-related pelvic girdle pain: A longitudinal follow-up study. BMC Musculoskelet Disord. 2016;17:276.
12. Bastiaanssen JM, de Bie RA, Bastiaenen CH, et al. Etiology and prognosis of pregnancy-related pelvic girdle pain: Design of a longitudinal study. BMC Public Health. 2005;5:1.
13. Wu WH, Meijer OG, Uegaki K, et al. Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. Eur Spine J. 2004;13(7):575-589.
14. Simonds A, Abraham K, Hill C, Spitznagle T, Cheng M, Parrott J. Disability, pelvic girdle pain, and depressive symptoms in the first 3 months postpartum. J Womens Health Phys Therap. 2018;42:13Y 147.
15. Vollestad NK, Stuge B. Prognostic factors for recovery from postpartum pelvic girdle pain. Eur Spine J. 2009;18(5):718-726.
16. Gausel AM, Dalen I, Kjærmann I, et al. Adding chiropractic treatment to individual rehabilitation for persistent pelvic girdle pain 3 to 6 months after delivery: A pilot randomized trial. J Manipulative Physiol Ther. 2019;42(8):601-607.

67
17. Gausel AM, Kjærmann I, Malmqvist S, Dalen I, Larsen JP, Økland I. Pelvic girdle pain 3-6 months after delivery in an unselected cohort of Norwegian women. Eur Spine J. 2016;25(6):1953-1959.
18. Bergström C, Persson M, Nergård KA, Mogren I. Prevalence and predictors of persistent pelvic girdle pain 12 years postpartum. BMC Musculoskelet Disord. 2017;18(1):399.
19. Gutke A, Lundberg M, Ostgaard HC, Oberg B. Impact of postpartum lumbopelvic pain on disability, pain intensity, health-related quality of life, activity level, kinesiophobia, and depressive symptoms. Eur Spine J. 2011;20(3):440-448.
20. Sjödahl J, Gutke A, Öberg B. Predictors for long-term disability in women with persistent postpartum pelvic girdle pain. Eur Spine J. 2013;22(7):1665-1673.
21. Mukkannavar P, Desai BR, Mohanty U, Kulkarni S, Parvatikar V, Daiwajna S. Pelvic girdle pain in Indian postpartum women: A cross-sectional study. Physiother Theory Pract. 2014;30(2):123-130.
22. Mukkannavar P, Desai BR, Mohanty U, Parvatikar V, Karwa D, Daiwajna S. Pelvic girdle pain after childbirth: the impact of mode of delivery. J Back Musculoskelet Rehabil. 2013;26(3):281-290.
23. Munro A, George RB, Chorney J, Snelgrove-Clarke E, Rosen NO. Prevalence and predictors of chronic pain in pregnancy and postpartum. J Obstet Gynaecol Can. 2017;39(9):734-741.
24. Borg-Stein J, Dugan SA. Musculoskeletal disorders of pregnancy, delivery and postpartum. Phys Med Rehabil Clin N Am. 2007;18(3):459-476, ix.
25. Pettila V, Leinonen P, Markkola A, Hiilesmaa V, Kaaja R. Postpartum bone mineral density in women treated for thromboprophylaxis with unfractionated heparin or LMW heparin. Thromb Haemost. 2002;87(2):182-186.
26. Møller UK, við Streym S, Mosekilde L, Rejnmark L. Changes in bone mineral density and body composition during pregnancy and postpartum. A controlled cohort study. Osteoporos Int. 2012;23(4):1213-1223.
27. Bjelland EK, Eskild A, Johansen R, Eberhard-Gran M. Pelvic girdle pain in pregnancy: the impact of parity. Am J Obstet Gynecol. 2010;203(2):146 e141-146.
28. Goeb V, Strotz V, Verdet M, Le Loet X, Vittecoq O. Post-partum sacral fracture associated with heparin treatment. Clin Rheumatol. 2008;27 Suppl 2:S51-53.
29. Hilal N, Nassar AH. Postpartum sacral stress fracture: A case report. BMC Pregnancy Childbirth. 2016;16:96.
30. Karatas M, Basaran C, Ozgul E, Tarhan C, Agildere AM. Postpartum sacral stress fracture: An unusual case of low-back and buttock pain. Am J Phys Med Rehabil. 2008;87(5):418-422.
31. Aslan E, Fynes M. Symphysial pelvic dysfunction. Curr Opin Obstet Gynecol. 2007;19(2):133-139.
32. Wurdinger S, Humbsch K, Reichenbach JR, Peiker G, Seewald HJ, Kaiser WA. MRI of the pelvic ring joints postpartum: Normal and pathological findings. J Magn Reson Imaging. 2002;15(3):324-329.
33. Seidman AJ, Siccardi MA. Postpartum Pubic Symphysis Diastasis. [Updated 2021 Jul 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls

68
Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537043/
34. Almoujahed MO, Khatib R, Baran J. Pregnancy-associated pyogenic sacroiliitis: Case report and review. Infect Dis Obstet Gynecol. 2003;11(1):53-57.
35. Gaughan E, Eogan M, Holohan M. Pyomyositis after vaginal delivery. BMJ Case Rep. 2011;2011.
36. Kinahan AM, Douglas MJ. Piriformis pyomyositis mimicking epidural abscess in a parturient. Can J Anaesth. 1995;42(3):240-245.
37. Ozturk M, Yavuz F, Altun D, Ulubay M, Firatligil FB. Postpartum bilateral sacroiliitis caused by Brucella infection. J Clin Diagn Res. 2015;9(11):Qd07-08.
38. Liu XQ, Li FC, Wang JW, Wang S. Postpartum septic sacroiliitis misdiagnosed as sciatic neuropathy. Am J Med Sci. 2010;339(3):292-295.
39. Haq I, Morris V. Post-partum septic sacroiliitis. Rheumatology. 2001;40(10):1191-1192.
40. Stürzenbecher A, Braun J, Paris S, Biedermann T, Hamm B, Bollow M. MR imaging of septic sacroiliitis. Skeletal Radiol. 2000;29(8):439-446.
41. Vale-Fernandes E, Rodrigues F, Monteiro C, Carvalho L. Infectious postpartum sacroiliitis: The importance and difficulty of early diagnosis. Acta Medica Portuguesa. 2016;29(7-8):484-487.
42. Tennfjord MK, Muleta M, Kiserud T. Musculoskeletal sequelae in patients with obstetric fistula - A case-control study. BMC Womens Health. 2014;14:136.
43. Snooks SJ, Swash M, Henry MM, Setchell M. Risk factors in childbirth causing damage to the pelvic floor innervation. Int J Colorectal Dis. 1986;1(1):20-24.
44. Haas DM, Meadows RS, Cottrell R, Stone WJ. Postpartum obturator neurapraxia. A case report. J Reprod Med. 2003;48(6):469-470.
45. Katirji B, Wilbourn AJ, Scarberry SL, Preston DC. Intrapartum maternal lumbosacral plexopathy. Muscle Nerve. 2002;26(3):340-347.
46. Ismael SS, Amarenco G, Bayle B, Kerdraon J. Postpartum lumbosacral plexopathy limited to autonomic and perineal manifestations: Clinical and electrophysiological study of 19 patients. J Neurol Neurosurg Psychiatry. 2000;68(6):771-773.
47. Buist AE, Austin MP, Hayes BA, et al. Postnatal mental health of women giving birth in Australia 2002-2004: Findings from the beyondblue National Postnatal Depression Program. Aust N Z J Psychiatry. 2008;42(1):66-73.
48. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry. 1987;150:782-786.
49. Dennis CL. Can we identify mothers at risk for postpartum depression in the immediate postpartum period using the Edinburgh Postnatal Depression Scale? J Affect Disord. 2004;78(2):163-169.
50. Gutke A, Josefsson A, Oberg B. Pelvic girdle pain and lumbar pain in relation to postpartum depressive symptoms. Spine. 2007;32(13):1430-1436.
51. Brown SJ, Lumley JM, McDonald EA, Krastev AH, Maternal Health Study collaborative. Maternal health study: A prospective cohort study of nulliparous women recruited in early pregnancy. BMC Pregnancy Childbirth. 2006;6:12.

69
52. Gaynes BN, Gavin N, Meltzer-Brody S, et al. Perinatal depression: Prevalence, screening accuracy, and screening outcomes. Evid Rep Technol Assess (Summ). 2005;(119):1-8.
53. Stuge B, Garratt A, Jenssen HK, Grotle M. The Pelvic Girdle Questionnaire: A condition-specific instrument for assessing activity limitations and symptoms in people with pelvic girdle pain. Phys Ther. 2011;91(7):1096-1108.
54. Kopec JA, Esdaile JM, Abrahamowicz M, et al. The Quebec Back Pain Disability Scale. Measurement properties. Spine. 1995;20(3):341-352.
55. Damen L, Buyruk HM, Güler-Uysal F, Lotgering FK, Snijders CJ, Stam HJ. Pelvic pain during pregnancy is associated with asymmetric laxity of the sacroiliac joints. Acta Obstet Gynecol Scand. 2001;80(11):1019-1024.
56. Mens JM, Vleeming A, Snijders CJ, Stam HJ, Ginai AZ. The active straight leg raising test and mobility of the pelvic joints. Eur Spine J. 1999;8(6):468-473.
57. Mens JM, Vleeming A, Stoeckart R, Stam HJ, Snijders CJ. Understanding peripartum pelvic pain. Implications of a patient survey. Spine. 1996;21(11):1363-1369; discussion 1369-1370.
58. Mens JM, Vleeming A, Snijders CJ, Koes BW, Stam HJ. Validity of the active straight leg raise test for measuring disease severity in patients with posterior pelvic pain after pregnancy. Spine. 2002;27(2):196-200.
59. Mens JM, Vleeming A, Snijders CJ, Ronchetti I, Ginai AZ, Stam HJ. Responsiveness of outcome measurements in rehabilitation of patients with posterior pelvic pain since pregnancy. Spine. 2002;27(10):1110-1115.
60. Mens JM, Vleeming A, Snijders CJ, Ronchetti I, Stam HJ. Reliability and validity of hip adduction strength to measure disease severity in posterior pelvic pain since pregnancy. Spine. 2002;27(15):1674-1679.
61. Levangie PK. Four clinical tests of sacroiliac joint dysfunction: The association of test results with innominate torsion among patients with and without low back pain. Phys Ther. 1999;79(11):1043-1057.
62. Carmichael JP. Inter- and intra-examiner reliability of palpation for sacroiliac joint dysfunction. J Manipulative Physiol Ther. 1987;10(4):164-171.
63. Riddle DL, Freburger JK. Evaluation of the presence of sacroiliac joint region dysfunction using a combination of tests: A multicenter intertester reliability study. Phys Ther. 2002;82(8):772-781.
64. Toussaint R, Gawlik CS, Rehder U, Rüther W. Sacroiliac joint diagnostics in the Hamburg Construction Workers Study. J Manipulative Physiol Ther. 1999;22(3):139-143.
65. Herren C, Sobottke R, Dadgar A, et al. Peripartum pubic symphysis separation--Current strategies in diagnosis and therapy and presentation of two cases. Injury. 2015;46(6):1074-1080.
66. Buyruk HM, Snijders CJ, Vleeming A, Laméris JS, Holland WP, Stam HJ. The measurements of sacroiliac joint stiffness with colour Doppler imaging: A study on healthy subjects. Eur J Radiol. 1995;21(2):117-121.
67. Snijders CH VA, Stoeckart R, et al. In: Vleeming A MV, Dorman T, et al., ed. Movement, Stability, and Low Back Pain: The Essential Role of the Pelvis. New York, NY: Churchill Livingstone; 1997:103-114.

70
68. Vleeming A, de Vries HJ, Mens JM, van Wingerden JP. Possible role of the long dorsal sacroiliac ligament in women with peripartum pelvic pain. Acta Obstet Gynecol Scand. 2002;81(5):430-436.
69. Njoo KH, van der Does E, Stam HJ. Interobserver agreement on iliac crest pain syndrome in general practice. J Rheumatol. 1995;22(8):1532-1535.
70. Gaenslen FJ. Sacro-iliac arthrodesis: Indications, authors technic and end-results. JAMA. 1927;89(24):2031-2035.
71. Olsén M, Körnung P, Kallin S, Elden H, Kjellby Wendt G, Gutke A. Validation of self-administered tests for screening for chronic pregnancy-related pelvic girdle pain. BMC Musculoskelet Disord. 2021;22(1):237.
72. Hansen A, Jensen DV, Larsen E, Wilken-Jensen C, Petersen LK. Relaxin is not related to symptom-giving pelvic girdle relaxation in pregnant women. Acta Obstet Gynecol Scand. 1996;75(3):245-249.
73. Gutke A, Hansson ER, Zetherström G, Ostgaard HC. Posterior pelvic pain provocation test is negative in patients with lumbar herniated discs. Eur Spine J. 2009;18(7):1008-1012.
74. Mens JM, Vleeming A, Snijders CJ, Koes BW, Stam HJ. Reliability and validity of the active straight leg raise test in posterior pelvic pain since pregnancy. Spine . 2001;26(10):1167-1171.
75. Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis of sacroiliac joint pain: validity of individual provocation tests and composites of tests. Man Ther. 2005;10(3):207-218.
76. Buyruk HM, Stam HJ, Snijders CJ, Laméris JS, Holland WP, Stijnen TH. Measurement of sacroiliac joint stiffness in peripartum pelvic pain patients with Doppler imaging of vibrations (DIV). Eur J Obstet Gynecol Reprod Biol. 1999;83(2):159-163.
77. Damen L, Buyruk HM, Guler-Uysal F, Lotgering FK, Snijders CJ, Stam HJ. The prognostic value of asymmetric laxity of the sacroiliac joints in pregnancy-related pelvic pain. Spine. 2002;27(24):2820-2824.
78. Stuge B, Saetre K, Ingeborg Hoff B. The automatic pelvic floor muscle response to the active straight leg raise in cases with pelvic girdle pain and matched controls. Man Ther. 2013;18(4):327-332.
79. Sjödahl J, Gutke A, Ghaffari G, Strömberg T, Öberg B. Response of the muscles in the pelvic floor and the lower lateral abdominal wall during the Active Straight Leg Raise in women with and without pelvic girdle pain: An experimental study. Clin Biomech. 2016;35:49-55.
80. Hu H, Meijer OG, Hodges PW, et al. Understanding the Active Straight Leg Raise (ASLR): An electromyographic study in healthy subjects. Man Ther. 2012;17(6):531-537.
81. Ronchetti I, Vleeming A, van Wingerden JP. Physical characteristics of women with severe pelvic girdle pain after pregnancy: A descriptive cohort study. Spine. 2008;33(5):E145-151.
82. Gutke A, Östgaard HC, Öberg B. Association between muscle function and low back pain in relation to pregnancy. J Rehabil Med. 2008;40(4):304-311.

71
83. Meijne W, van Neerbos K, Aufdemkampe G, van der Wurff P. Intraexaminer and interexaminer reliability of the Gillet test. J Manipulative Physiol Ther. 1999;22(1):4-9.
84. Hungerford B, Gilleard W, Lee D. Altered patterns of pelvic bone motion determined in subjects with posterior pelvic pain using skin markers. Clin Biomech. 2004;19(5):456-464.
85. Hungerford BA, Gilleard W, Moran M, Emmerson C. Evaluation of the ability of physical therapists to palpate intrapelvic motion with the Stork test on the support side. Phys Ther. 2007;87(7):879-887.
86. Treatment of pelvic girdle pain in pregnancy. ACOG Clin Rev. 2005;10(5):3-3. 87. McQuade KJ, Turner JA, Buchner DM. Physical fitness and chronic low back
pain. An analysis of the relationships among fitness, functional limitations, and depression. Clin Orthop Relat Res. 1988;(233):198-204.
88. Biering-Sørensen F. Physical measurements as risk indicators for low-back trouble over a one-year period. Spine. 1984;9(2):106-119.
89. Deering RE, Senefeld J, Pashibin T, Neumann DA, Cruz M, Hunter SK. Fatigability of the lumbopelvic stabilizing muscles in women 8 and 26 weeks postpartum. J Womens Health Phys Therap. 2018;42(3):128-138.
90. Mens JMA, Pool-Goudzwaard A. The transverse abdominal muscle is excessively active during active straight leg raising in pregnancy-related posterior pelvic girdle pain: An observational study. BMC Musculoskelet Disord. 2017;18(1):372.
91. Bø K, Kvarstein B, Hagen RR, Larsen S. Pelvic floor muscle exercise for the treatment of female stress urinary incontinence: II. Validity of vaginal pressure measurements of pelvic floor muscle strength and the necessity of supplementary methods for control of correct contraction. Neurourol Urodyn. 1990;9(5):479-487.
92. Bø K, Kvarstein B, Hagen R, Larsen S. Pelvic floor muscle exercise for the treatment of female stress urinary incontinence: I. Reliability of vaginal pressure measurements of pelvic floor muscle strength. Neurourol Urodyn. 1990;9(5):471-477.
93. Braekken IH, Majida M, Ellström Engh M, Holme IM, Bø K. Pelvic floor function is independently associated with pelvic organ prolapse. BJOG. 2009;116(13):1706-1714.
94. Frawley HC, Galea MP, Phillips BA, Sherburn M, Bø K. Reliability of pelvic floor muscle strength assessment using different test positions and tools. Neurourol Urodyn. 2006;25(3):236-242.
95. Spitznagle TM, Leong FC, Van Dillen LR. Prevalence of diastasis recti abdominis in a urogynecological patient population. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(3):321-328.
96. Liaw LJ, Hsu MJ, Liao CF, Liu MF, Hsu AT. The relationships between inter-recti distance measured by ultrasound imaging and abdominal muscle function in postpartum women: a 6-month follow-up study. J Orthop Sports Phys Ther. 2011;41(6):435-443.

72
97. O'Sullivan PB, Beales DJ. Diagnosis and classification of pelvic girdle pain disorders--Part 1: a mechanism based approach within a biopsychosocial framework. Man Ther. 2007;12(2):86-97.
98. Bastiaenen CH, Bie RA, Wolters PM, et al. Effectiveness of a tailor-made intervention for pregnancy-related pelvic girdle and/or low back pain after delivery: short-term results of a randomized clinical trial [ISRCTN08477490]. BMC Musculoskelet Disord. 2006;7:19.
99. Vleeming A, Albert HB, Ostgaard HC, Sturesson B, Stuge B. European guidelines on the diagnosis and treatment of pelvic girdle pain. Eur Spine J. 2008;17:794–819.
100. Al-Sayegh NA, George SE, Boninger ML, Rogers JC, Whitney SL, Delitto A. Spinal Mobilization of Postpartum Low Back and Pelvic Girdle Pain: An Evidence-Based Clinical Rule for Predicting Responders and Nonresponders. PM&R. 2010;2(11):995-1005.
101. Delitto A, Erhard RE, Bowling RW. A treatment-based classification approach to low back syndrome: identifying and staging patients for conservative treatment. Phys Ther. 1995;75(6):470-485; discussion 485-479.
102. Spitznagle TM, Robinson CM. Myofascial pelvic pain. Obstet Gynecol Clin North Am. 2014;41(3):409-432.
103. Spitznagle T. Musculoskeletal Chronic Pelvic Pain. In: Carrière B, Feldt CM, ed. Pelvic Floor. Vol 1. New York, NY: Thieme 2006.
104. Sahrmann S, Azevedo DC, Dillen LV. Diagnosis and treatment of movement system impairment syndromes. Braz J Phys Ther. 2017;21(6):391-399.
105. Sahrmann S. Diagnosis and Treament of Movement Impairment Syndromes. St Louis, MO: Mosby; 2001.
106. Snijders CJ, Vleeming A, Stoeckart R. Transfer of lumbosacral load to iliac bones and legs Part 1: Biomechanics of self-bracing of the sacroiliac joints and its significance for treatment and exercise. Clin Biomech. 1993;8(6):285-294.
107. Richardson CA JG, Hodges PW, et al. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain. 1st ed. London: Churchill Livingst6on; 1999.
108. Vleeming A, Stoeckart R. The role of the pelvic girdle in coupling the spine and the legs: A clinical-anatomical perspective on pelvic stability. Movement, Stability & Lumbopelvic Pain. 2007:113-137.
109. Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exercises for first-episode low back pain. Spine. 2001;26(11):E243-248.
110. Hodges PW. Is there a role for transversus abdominis in lumbo-pelvic stability? Man Ther. 1999;4(2):74-86.
111. O'Sullivan PB. Lumbar segmental 'instability': Clinical presentation and specific stabilizing exercise management. Man Ther. 2000;5(1):2-12.
112. van der Wurff P, Hagmeijer RH, Meyne W. Clinical tests of the sacroiliac joint. A systematic methodological review. Part 1: Reliability. Man Ther. 2000;5(1):30-36.
113. van der Wurff P, Buijs EJ, Groen GJ. A multitest regimen of pain provocation tests as an aid to reduce unnecessary minimally invasive sacroiliac joint procedures. Arch Phys Med Rehabil. 2006;87(1):10-14.

73
114. APTA and the Movement System. American Physical Therapy Association. September 1, 2019. Accessed August 6, 2021. https://www.apta.org/patient-care/interventions/movement-system-management/movement-system-apta
115. Bjorklund K, Nordstrom ML, Bergstrom S. Sonographic assessment of symphyseal joint distention during pregnancy and post partum with special reference to pelvic pain. Acta Obstet Gynecol Scand. 1999;78(2):125-130.
116. Damen L, Spoor CW, Snijders CJ, Stam HJ. Does a pelvic belt influence sacroiliac joint laxity? Clin Biomech. 2002;17(7):495-498.
117. Lindgren A, Kristiansson P. Finger joint laxity, number of previous pregnancies and pregnancy induced back pain in a cohort study. BMC Pregnancy Childbirth. 2014;14.
118. Beales DJ, O'Sullivan PB, Briffa NK. Motor control patterns during an active straight leg raise in chronic pelvic girdle pain subjects. Spine. 2009;34(9):861-870.
119. Dumas GA, Leger A, Plamondon A, Charpentier KM, Pinti A, McGrath M. Fatigability of back extensor muscles and low back pain during pregnancy. Clin Biomech. 2010;25(1):1-5.
120. Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: Prevalence, risk factors and report of lumbopelvic pain. Br J Sports Med. 2016;50(17):1092-1096.
121. Stuge B, Mørkved S, Dahl HH, Vøllestad N. Abdominal and pelvic floor muscle function in women with and without long lasting pelvic girdle pain. Man Ther. 2006;11(4):287-296.
122. Stuge B, Saetre K, Braekken IH. The association between pelvic floor muscle function and pelvic girdle pain: A matched case control 3D ultrasound study. Man Ther. 2012;17(2):150-156.
123. Teymuri Z, Hosseinifar M, Sirousi M. The effect of stabilization exercises on pain, disability, and pelvic floor muscle function in postpartum lumbopelvic pain: A randomized controlled trial. Am J Phys Med Rehabil. 2018;97(12):885-891.
124. Parker MA, Millar LA, Dugan SA. Diastasis rectus abdominis and lumbo-pelvic pain and dysfunction: Are they related? J Womens Health Phys Therap. 2009;33(2):15-22.
125. Mens JMA, Pool-Goudzwaard A, Stam HJ. Mobility of the pelvic joints in pregnancy-related lumbopelvic pain: A systematic review. Obstet Gynecol Surv. 2009;64(3):200-208.
126. Hu H, Meijer OG, van Dieën JH, et al. Muscle activity during the active straight leg raise (ASLR), and the effects of a pelvic belt on the ASLR and on treadmill walking. J Biomech. 2010;43(3):532-539.
127. Hungerford B, Gilleard W, Hodges P. Evidence of altered lumbopelvic muscle recruitment in the presence of sacroiliac joint pain. Spine. 2003;28(14):1593-1600.
128. Beales DJ, O'Sullivan PB, Briffa NK. The effects of manual pelvic compression on trunk motor control during an active straight leg raise in chronic pelvic girdle pain subjects. Man Ther. 2010;15(2):190-199.
129. Peterson CD, Haas M, Gregory WT. A pilot randomized controlled trial evaluating three treatments for pregnancy-related low back pain: Exercise, spinal

74
manipulation, and neuroemotional technique. J Midwifery Womens Health. 2012;57(5):537-537.
130. Franklin ME, Conner-Kerr T. An analysis of posture and back pain in the first and third trimesters of pregnancy. J Orthop Sports Phys Ther. 1998;28(3):133-138.
131. Moore K, Dumas GA, Reid JG. Postural changes associated with pregnancy and their relationship with low back pain. Clin Biomech. 1990;5(3):169-174.
132. Okanishi N, Kito N, Akiyama M, Yamamoto M. Spinal curvature and characteristics of postural change in pregnant women. Acta Obstet Gynecol Scand. 2012;91(7):856-861.
133. Hemingway H, Croft P, Perel P, et al. Prognosis research strategy (PROGRESS) 1: A framework for researching clinical outcomes. BMJ. 2013;346:e5595.
134. Stuge B, Veierod MB, Laerum E, Vollestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: A two-year follow-up of a randomized clinical trial. Spine. 2004b;29(10):E197-E203.
135. Stuge B, Mørkved S, Dahl HH, Vøllestad N. Abdominal and pelvic floor muscle function in women with and without long lasting pelvic girdle pain. Man Ther. 2006;11(4):287-296.
136. Olsson CB, Nilsson-Wikmar L, Grooten WJA. Determinants for lumbopelvic pain 6 months postpartum. Disabil Rehabil. 2012;34(5):416-422.
137. Olsson CB, Grooten WJA, Nilsson-Wikmar L, Harms-Ringdahl K, Lundberg M. Catastrophizing during and after pregnancy: Associations with lumbopelvic pain and postpartum physical ability. Phys Ther. 2012;92(1):49-57.
138. Renard J, Abraham-Justice K. Manual therapy and core stabilization exercises with postpartum pelvic girdle pain and meralgia paresthetica: A case report. Journal of Womens Health Phys Therap. 2012;36:35 43.
139. Gutke A, Sjodahl J, Oberg B. Specific muscle stabilizing as home exercises for persistent pelvic girdle pain after pregnancy: a randomized, controlled clinical trial. J Rehabil Med. 2010;42(10):929-935.
140. Elden H, Fagevik-Olsen M, Ostgaard HC, Stener-Victorin E, Hagberg H. Acupuncture as an adjunct to standard treatment for pelvic girdle pain in pregnant women: randomised double-blinded controlled trial comparing acupuncture with non-penetrating sham acupuncture. BJOG. 2008;115(13):1655-1668.
141. Elden H, Ostgaard HC, Fagevik-Olsen M, Ladfors L, Hagberg H. Treatments of pelvic girdle pain in pregnant women: Adverse effects of standard treatment, acupuncture and stabilising exercises on the pregnancy, mother, delivery and the fetus/neonate. BMC Complement Altern Med. 2008;8:34.
142. Bastiaenen CH, de Bie RA, Vlaeyen JW, et al. Long-term effectiveness and costs of a brief self-management intervention in women with pregnancy-related low back pain after delivery. BMC Pregnancy Childbirth. 2008;8:19.
143. Morkved S, Salvesen KA, Schei B, Lydersen S, Bo K. Does group training during pregnancy prevent lumbopelvic pain? A randomized clinical trial. Acta Obstet Gynecol Scand. 2007;86(3):276-282.
144. Nilsson-Wikmar L, Holm K, Oijerstedt R, Harms-Ringdahl K. Effect of three different physical therapy treatments on pain and activity in pregnant women with

75
pelvic girdle pain: A randomized clinical trial with 3, 6, and 12 months follow-up postpartum. Spine. 2005;30(8):850-856.
145. Stuge B, Laerum E, Kirkesola G, Vøllestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: A randomized controlled trial. Spine. 2004;29(4):351-359.
146. Mens JMA, Snijders CJ, Stam HJ. Diagonal trunk muscle exercises in peripartum pelvic pain: A randomized clinical trial. Phys Ther. 2000;80(12):1164-1173.
147. Ehsani F, Sahebi N, Shanbehzadeh S, Arab AM, ShahAli S. Stabilization exercise affects function of transverse abdominis and pelvic floor muscles in women with postpartum lumbo-pelvic pain: A double-blinded randomized clinical trial study. Int Urogynecol J. 2020;31(1):197-204.
148. Saleh MSM, Botla AMM, Elbehary NAM. Effect of core stability exercises on postpartum lumbopelvic pain: A randomized controlled trial. J Back Musculoskelet Rehabil. 2019;32(2):205-213.
149. ElDeeb AM, Abd-Ghafar KS, Ayad WA, Sabbour AA. Effect of segmental stabilizing exercises augmented by pelvic floor muscles training on women with postpartum pelvic girdle pain: A randomized controlled trial. J Back Musculoskelet Rehabil. 2019;32(5):693-700.
150. Haakstad LAH, Bo K. Effect of regular exercise programme on pelvic girdle and lowback pain in previously inactive pregnant women: A randominzed controlled trial. J Rehabil Med. 2015;47(3):229-234.
151. Chaudry S, Siddiqui F, Hussain Shah SI. Effectiveness of core stabilization exercises along with postural correction in postpartum back pain. Rawal Medical Journal. 2013;38:256-259.
152. Haugland KS, Rasmussen S, Daltveit AK. Group intervention for women with pelvic girdle pain in pregnancy. A randomized controlled trial. Acta Obstet Gynecol Scand. 2006;85(11):1320-1326.
153. Ferreira P. Specific stabilising exercise improves pain and function in women with pelvic girdle pain following pregnancy. Aust J Physiother. 2004;50(4):259-259.
154. Bhardwaj A, Nagandla K. Musculoskeletal symptoms and orthopaedic complications in pregnancy: Pathophysiology, diagnostic approaches and modern management. Postgrad Med J. 2014;90(1066):450-460.
155. Mens JM, Damen L, Snijders CJ, Stam HJ. The mechanical effect of a pelvic belt in patients with pregnancy-related pelvic pain. Clin Biomech. 2006;21(2):122-127.
156. Schwerla F, Rother K, Rother D, Ruetz M, Resch KL. Osteopathic manipulative therapy in women with postpartum low back pain and disability: A pragmatic randomized controlled trial. J Am Osteopath Assoc. 2015;115(7):416-425.
157. Clinton SC, Newell A, Downey PA, Ferreira K. Pelvic girdle pain in the antepartum population: Physical therapy clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health From the Section on Women's Health and the Orthopaedic Section of the American Physical Therapy Association. J Womens Health Phys Therap. 2017;41(2).

76
158. Bjelland EK, Stuge B, Vangen S, Stray-Pedersen B, Eberhard-Gran M. Mode of delivery and persistence of pelvic girdle syndrome 6 months postpartum. Am J Obstet Gynecol. 2013;208(4).
159. Yoo JJ, Ha YC, Lee YK, Hong JS, Kang BJ, Koo KH. Incidence and risk factors of symptomatic peripartum diastasis of pubic symphysis. J Korean Med Sci. 2014;29(2):281-286.
160. Gashaw M, Gedlu S, Janakiraman B. Burden of pelvic girdle pain during pregnancy among women attending ante-natal clinic, Ethiopia: A cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1):494.
161. Biering K, Nohr EA, Olsen J, Andersen AMN, Hjollund NH, Juhl M. Pregnancy-related pelvic pain is more frequent in women with increased body mass index. Acta Obstet Gynecol Scand. 2011;90(10):1132-1139.
162. Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940-2952; discussion 2952.
163. Grotle M, Garratt AM, Krogstad Jenssen H, Stuge B. Reliability and construct validity of self-report questionnaires for patients with pelvic girdle pain. Phys Ther. 2012;92(1):111-123.
164. Ogollah R, Bishop A, Lewis M, Grotle M, Foster NE. Responsiveness and minimal important change for pain and disability outcome measures in pregnancy-related low back and pelvic girdle pain. Phys Ther. 2019;99(11):1551-1561.
165. Stuge B, Jenssen HK, Grotle M. The Pelvic Girdle Questionnaire: responsiveness and minimal important change in women with pregnancy-related pelvic girdle pain, low back pain, or both. Phys Ther. 2017;97(11):1103-1113.
166. Albert H, Godskesen M, Westergaard J. Prognosis in four syndromes of pregnancy-related pelvic pain. Acta Obstet Gynecol Scand. 2001;80(6):505-510.
167. Hills NF, Graham RB, McLean L. Comparison of trunk muscle function between women with and without diastasis recti abdominis at 1 year postpartum. Phys Ther. 2018;98(10):891-901.
168. Blyholder L, Chumanov E, Carr K, Heiderscheit B. Exercise behaviors and health conditions of runners after childbirth. Sports Health. 2017;9(1):45-51.
169. Fernandes da Mota PG, Pascoal AG, Carita AI, Bø K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther. 2015;20(1):200-205.
170. Kordi R, Abolhasani M, Rostami M, Hantoushzadeh S, Mansournia MA, Vasheghani-Farahani F. Comparison between the effect of lumbopelvic belt and home based pelvic stabilizing exercise on pregnant women with pelvic girdle pain; a randomized controlled trial. J Back Musculoskelet Rehabil. 2013;26(2):133-139.
171. Morino S, Ishihara M, Umezaki F, et al. The effects of pelvic belt use on pelvic alignment during and after pregnancy: a prospective longitudinal cohort study. BMC Pregnancy Childbirth. 2019;19(1):305.
172. Pennick V, Liddle Sarah D. Interventions for preventing and treating pelvic and back pain in pregnancy. Cochrane Database Syst Rev. 2013(8).

77
173. Vleeming A, Buyruk HM, Stoeckart R, Karamursel S, Snijders CJ. An integrated therapy for peripartum pelvic instability: A study of the biomechanical effects of pelvic belts. Am J Obstet Gynecol. 1992;166(4):1243-1247.
174. Wu WH, Meijer OG, Bruijn SM, et al. Gait in pregnancy-related pelvic girdle pain: Amplitudes, timing, and coordination of horizontal trunk rotations. Eur Spine J. 2008;17(9):1160-1169.
175. Figuers C, Briggs J, Thibodeaux E, Gehm W, Turbyfill H. Physical symptoms, exercise and weight management in the postpartum period: A review of pertinent literature. Journal of the Section on Women's Health. 2003;27(2):19-27.
176. Nelson PR. Pregnancy-related pelvic girdle pain presenting as low back pain: a case report. Orthopaedic Physical Therapy Practice. 2010;22(3):153-158.
177. Depledge J, McNair PJ, Keal-Smith C, Williams M. Management of symphysis pubis dysfunction during pregnancy using exercise and pelvic support belts. Phys Ther. 2005;85(12):1290-1300.
178. Howell ER. Pregnancy-related symphysis pubis dysfunction management and postpartum rehabilitation: Two case reports. J Can Chiropr Assoc. 2012;56(2):102-111.
179. Robinson HS, Mengshoel AM. Assessments of lumbar flexion range of motion: Intertester reliability and concurrent validity of 2 commonly used clinical tests. Spine. 2014;39(4):E270-e275.
180. Elden H, Hagberg H, Olsen MF, Ladfors L, Ostgaard HC. Regression of pelvic girdle pain after delivery: Follow-up of a randomised single blind controlled trial with different treatment modalities. Acta Obstet Gynecol Scand. 2008;87(2):201-208.
181. Bergstrom C, Persson M, Mogren I. Pregnancy-related low back pain and pelvic girdle pain approximately 14 months after pregnancy - pain status, self-rated health and family situation. BMC Pregnancy Childbirth. 2014;14.
182. Morgan JF, Lacey JH, Chung E. Risk of postnatal depression, miscarriage, and preterm birth in bulimia nervosa: Retrospective controlled study. Psychosom Med. 2006;68(3):487-492.