clinical overview and discussion of in the - … · clinical overview and discussion of laboratory...
TRANSCRIPT

5/27/2015
1
Clinical Overview and DiscussionOf Laboratory Medicine inThe Oncology Practice
Cancer & Hematology Centers of
Western Michigan
• 8 Cancer Centers located in Western Michigan -privately owned but working collaboratively with area hospitals
• 3 Centers include on-site, physician owned laboratories
• 19 Oncologists/16 are also Hematologists• Treatment of all types of solid tumor cancers, blood
related cancers along with coagulation disorders and hematological disease
• Dedicated to bringing state of the art cancer care treatment to the community
5/27/2015
2
Grand Rapids Furniture City

5/27/2015
3
Johnson Cancer Center
Lab Staff of Today
5/27/2015
4
Main Laboratory Instrumentation
Laboratory Equipment:
• Sysmex XN 1000• Roche Cobas 6000• Siemens PFA 100
In-House Test Menu = 75 tests on these 3 instruments
Sysmex XN‐1000
Roche Cobas 6000
5/27/2015
5
Clinic Laboratory Instrumentation
and Test Menu
Laboratory Equipment:
• Roche C111• Sysmex KX-21N
In-House Test Menu on these 2 instruments = 20
Sysmex KX 21N Roche C111
Role of the Laboratory
• The lab plays a huge part in overall flow of the patient through the centero Lab results drive treatment options
• Speedy on-site testing allows for real time decision making by the provider
• Laboratory Information System interfaced to patient’s Electronic Medical Record for easy and fast access to laboratory results
5/27/2015
6
Help, Healing and Hope for our Patients
Role of the Laboratory
• Test menu developed to support both cancer care needs and general lab testing
• Annual in-house test volumes =150,000 panels (over 1,000,000 tests per year)
• Patients are drawn for all needed tests whether done on site or sent out to a reference laboratory
Capital Acquisitions
• Factors to consider when purchasing equipment• Space limitations• Extensive test menu • Reliability – relatively no down time• Back-up equipment not an option
for us• Increases overall cost of test• No room for extra equipment

5/27/2015
7
Important Features for Capital Acquisitions
• Quick turn around time - stat option essential
o Many chemotherapy treatments cannot be given until lab results are available and within range
o Several insurance companies require lab values to be submitted with the treatment billing invoices or coverage will be denied
• High level training program for testing personnel in order to be knowledgeable and efficient in the use of the new equipment and to be able to train others
Down Stream of Down Time
• Instrumentation down time halts care in a cancer care environment
o Phone Support - Need reliable and knowledgeable support to get instrument up and running as quickly as possible
o Field Service - Need engineers to respond in a timely fashion when issues are more severe
o Down Time - Results in sent out lost revenue and increase wait times for patients
When there is down timePatient satisfaction is greatly decreased !
Revenue Benefit of the Lab
• Test menu developed for practicality & revenue. • Tests to be brought in-house are determined by the
test cost and insurance allowable reimbursement.• Important to maximize equipment capabilities to
lower cost of individual test.• Decrease in turn around time of lab tests yields
increased number of patients that can be treated in a given time.
• This equates to increased revenue from chemotherapy treatment.
5/27/2015
8
Why have a P.O.L.?
• Provide physicians with consistent, in-house testing so they can compare apples to apples.
• Quick turn around times, with results populating the patient’s EMR, allow the physician to make changes in the patient’s treatment regimen.
• The physicians get spoiled with this level of service and it becomes their expectation.
• Be proactive in introducing new tests that would play a beneficial role in their practice of medicine.
Why Sysmex Works at CHC
• CHC has been a Sysmex customer for over 20 years• Equipment needs expanded as the physician practice grew
from 4 to 19 doctors o K 1000→ K 4500→ XT 2000i→ XN 1000
• The XN-1000 is a perfect fito Meets our space limitationso Very little down timeo Additional parameters that provide useful information to the physicians.o Quick turn around times.o Allows us to be a reference lab for our off site clinicso Interfaced with our LIS and EMR to provide real time results that populate in the
patient’s electronic chart• Account Managers - honest and knowledgeable with strong,
trusting, working relationships.• Customer Service Representatives - easy to work with, go
above and beyond to exceed our expectations.• Field Service Engineers - friendly and quick to respond.
XN‐1000
• Cancer and Hematology Center Laboratory at LHCP is enjoying the benefit of the new Sysmex XN-1000.
• 5 new reportable parameters:• Immature Granulocytes (IG)
• Nucleated RBC (NRBC)
• Immature Retic Fraction (IRF)
• Reticulocyte Hemoglobin Equivalent (RET-He)
• Immature Platelet Fraction (IPF)
5/27/2015
9
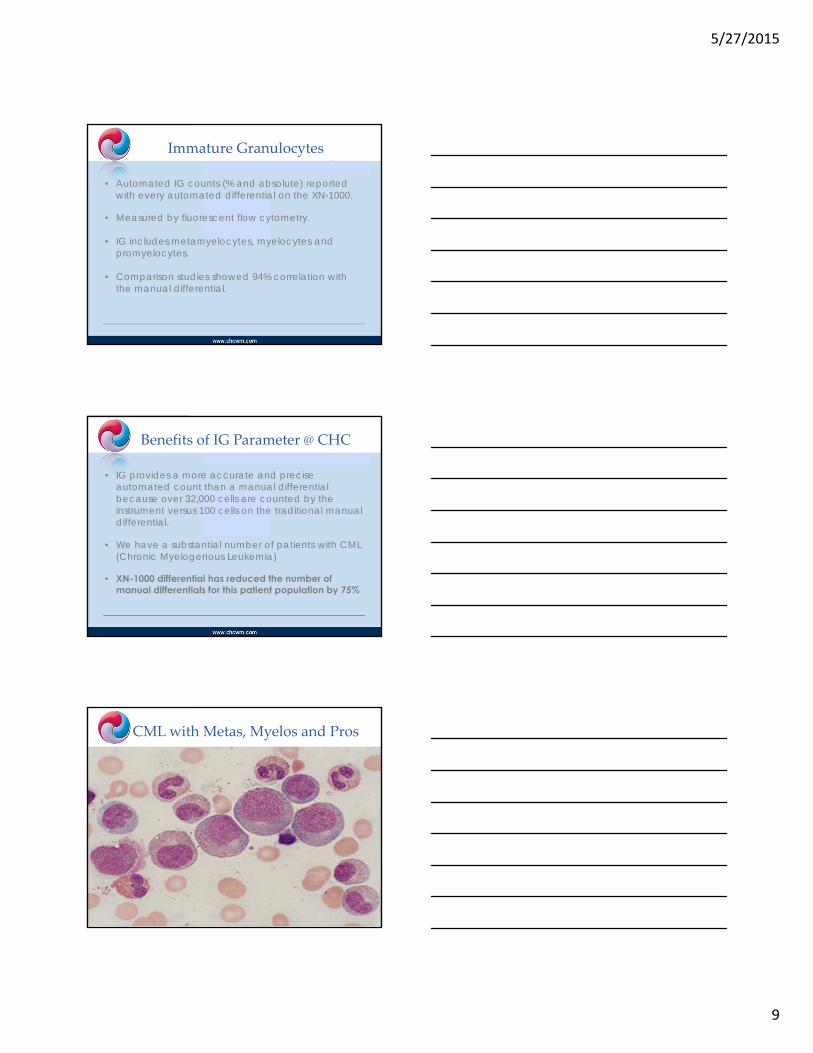
Immature Granulocytes
• Automated IG counts (% and absolute) reported with every automated differential on the XN-1000.
• Measured by fluorescent flow cytometry.
• IG includes metamyelocytes, myelocytes and promyelocytes.
• Comparison studies showed 94% correlation with the manual differential.
Benefits of IG Parameter @ CHC
• IG provides a more accurate and precise automated count than a manual differential because over 32,000 cells are counted by the instrument versus 100 cells on the traditional manual differential.
• We have a substantial number of patients with CML (Chronic Myelogenous Leukemia)
• XN-1000 differential has reduced the number of manual differentials for this patient population by 75%
CML with Metas, Myelos and Pros

5/27/2015
10
XN 1000 Automatic Differential on
CML patient
IG = 28.9%
(Metas, Myelos and Pros)
Manual Differentialon CML patient.
Metas, Myelocytesand Promyelocytes
IG = 27% 27 %
Benefits of IG Parameter @ CHC
• IG is particularly beneficial for patients receiving WBC production stimulation drugs (Neupogen and Neulasta).
• Purpose of chemotherapy drugs is to kill cancer cells -Side effects is destruction of other cells, including WBCs.
• Patients with WBC less than1000 are very susceptible toinfection.
• Drugs such as Neupogen and Neulasta stimulate WBCproduction in the bone marrow.

5/27/2015
11
Benefits of IG Parameter @ CHC
• Because the circulating WBC count is at such a low level, stimulated WBC’s are released from the marrow sooner – without the chance to fully mature.
• Immature forms are mainly Metas and Myelos with an occasional Pro or Blast.
• The IG parameter is useful when increased WBC is easily explained by the drug stimulation and the IG’s are expected.
Patient Receiving Neulasta
IG = 11.9%
Neulastainjection
Metas in Patient Receiving Neulasta
5/27/2015
12
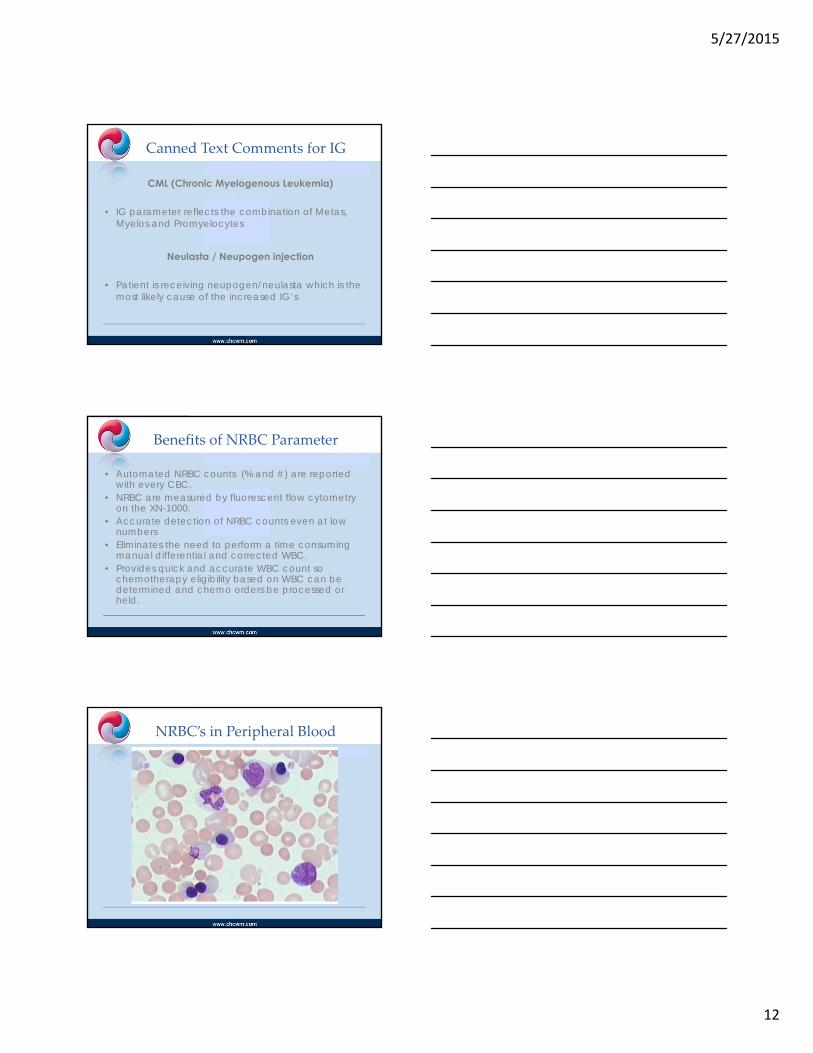
Canned Text Comments for IG
CML (Chronic Myelogenous Leukemia)
• IG parameter reflects the combination of Metas, Myelos and Promyelocytes
Neulasta / Neupogen injection
• Patient is receiving neupogen/neulasta which is the most likely cause of the increased IG’s
Benefits of NRBC Parameter
• Automated NRBC counts (% and #) are reported with every CBC.
• NRBC are measured by fluorescent flow cytometry on the XN-1000.
• Accurate detection of NRBC counts even at low numbers
• Eliminates the need to perform a time consuming manual differential and corrected WBC.
• Provides quick and accurate WBC count so chemotherapy eligibility based on WBC can be determined and chemo orders be processed or held.
NRBC’s in Peripheral Blood

5/27/2015
13
Benefits of Accurate WBC
• ANC (absolute neutrophil count) is followed and used to determine whether chemo will be given.
• When the ANC is 1000 or less it raises the question of whether chemo will be given:o Depends on where the patient is in the their cycleo Possible dose reduction verses holding
• ANC <500 – chemo not given
Patient with
Normal WBC = 10.25
High NRBC = 19.4
Normal WBC with High RBC
Patient with
LowWBC = 1.14
High NRBC = 11.4
ANC = 530
ANC= 530
Low WBC High NRBC

5/27/2015
14
Patient with
Low WBC = 0.68
High NRBC = 30.9
ANC = 280
ANC = 280
Low WBCHigh NRBC
Canned Text Comments for NRBC’s
Hold Ups and Holding Chemo
• Hold ups in the lab delay the entire flow of through the infusion center o Example: Performing a manual diff to get an accurate WBC.
• Chairs are scheduled for each patient for a particular block of time based on their treatment.
• Lab result delays cause pharmacy orders to be delayed…cause chair time to get off schedule.
• Nurses & support staff end up working O.T. – very costly. Average of one hour of nurse O.T. = $50/hour
• Increases cost of providing health care and impacts bottom line and profitability of the practice.

5/27/2015
15
Effects of Holding Chemotherapy
• Holding chemo is necessary for the health and safety of the patient but causes problems of its own.
• Chemo drugs need to be authorized for payment.• Included in the authorization day of treatment,
dose and time frame.• Any changes require a need for reauthorization.• Example:
o Patient authorized to get chemo for 6 months. o Chemo is held for a week due to low platelet count. o This extends patient’s treatment out to 6 months and 1 week. o Insurance stops paying at 6 months unless reauthorization
obtained.
Holding Chemotherapy
• Anemiao Chemo rarely held for anemia - easy to correct with PRBC
transfusion.
• Low ANCo Usually chemo dose is reduced and supported with Neulasta.
• Plateletso Many times chemo is held because of low platelets.o Transfused platelets are quickly killed off by the chemotherapy
drugs. o Best to wait for patient’s marrow to recover and begin platelet
production on its own rather than to transfuse platelets for very little benefit.
Immature Platelet Fraction (IPF)
• IPF is a measure of immature platelets in the circulating blood
• An increased IPF with thrombocytopenia may indicate:o Peripheral destruction or consumption of platelets such as:
• Idiopathic thrombocytopenia (ITP) • Thrombotic thrombocytopenic purpura (TTP) • Disseminated intravascular coagulation (DIC)
5/27/2015
16
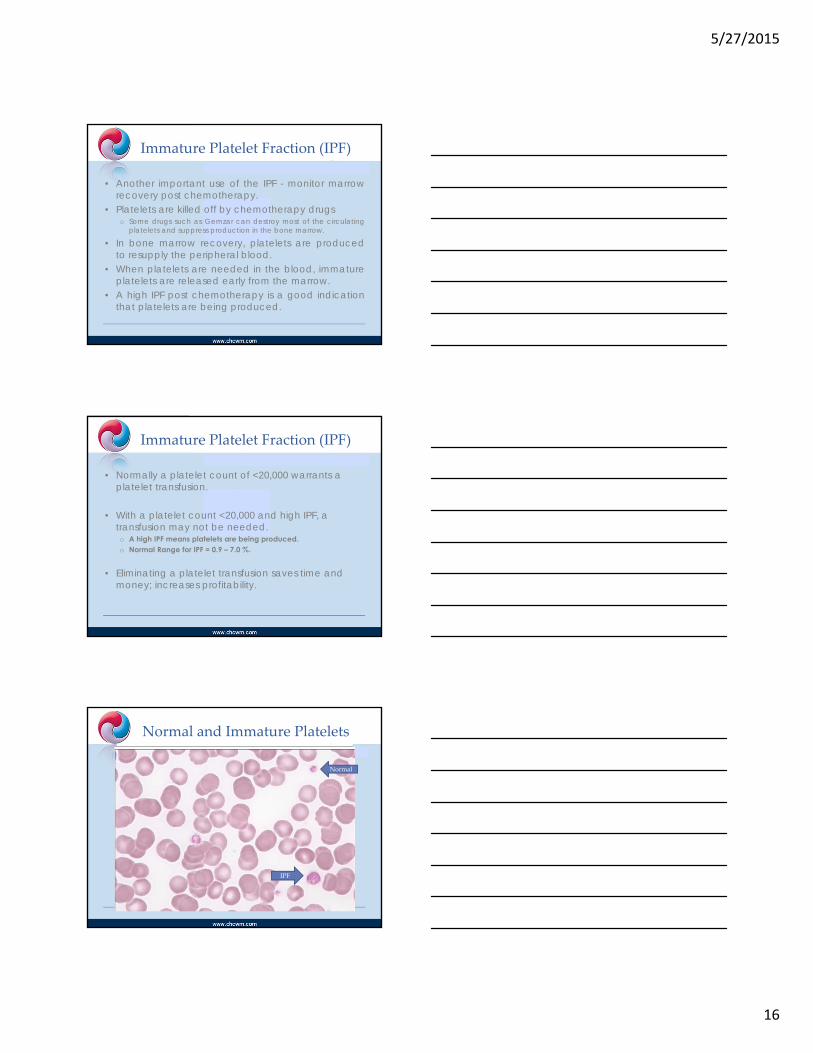
Immature Platelet Fraction (IPF)
• Another important use of the IPF - monitor marrowrecovery post chemotherapy.
• Platelets are killed off by chemotherapy drugso Some drugs such as Gemzar can destroy most of the circulating
platelets and suppress production in the bone marrow.
• In bone marrow recovery, platelets are producedto resupply the peripheral blood.
• When platelets are needed in the blood, immatureplatelets are released early from the marrow.
• A high IPF post chemotherapy is a good indicationthat platelets are being produced.
Immature Platelet Fraction (IPF)
• Normally a platelet count of <20,000 warrants a platelet transfusion.
• With a platelet count <20,000 and high IPF, a transfusion may not be needed.o A high IPF means platelets are being produced. o Normal Range for IPF = 0.9 – 7.0 %.
• Eliminating a platelet transfusion saves time and money; increases profitability.
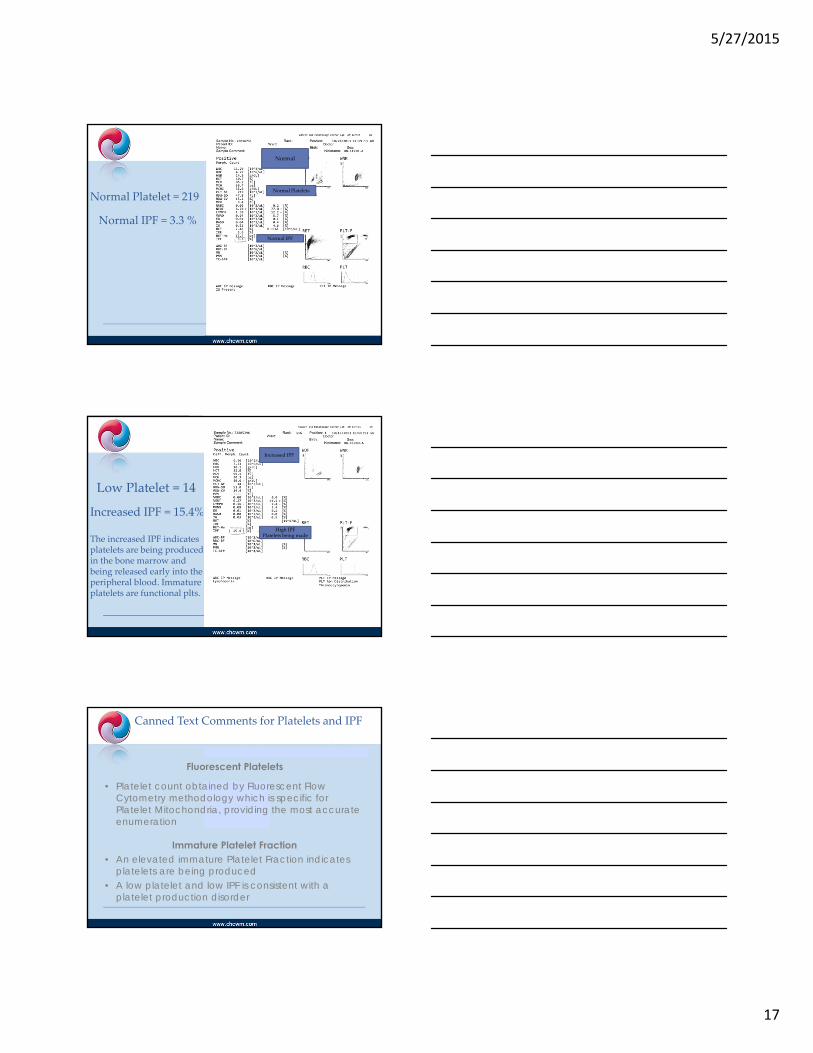
Normal and Immature Platelets
IPF
Normal
5/27/2015
17
Normal Platelet = 219
Normal IPF = 3.3 %
Normal
Normal Platelets
Normal IPF
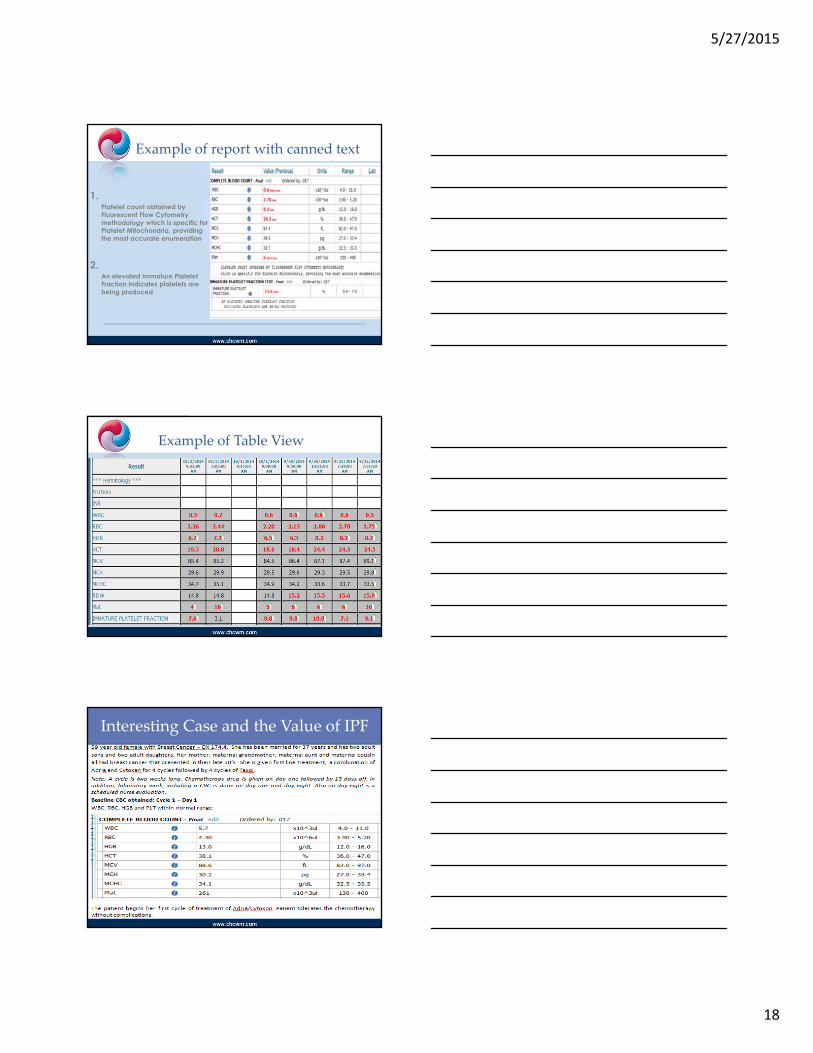
Low Platelet = 14
Increased IPF = 15.4%
The increased IPF indicatesplatelets are being producedin the bone marrow and being released early into the peripheral blood. Immature platelets are functional plts.
Increased IPF
High IPFPlatelets being made
Canned Text Comments for Platelets and IPF
Fluorescent Platelets
• Platelet count obtained by Fluorescent Flow Cytometry methodology which is specific for Platelet Mitochondria, providing the most accurate enumeration
Immature Platelet Fraction• An elevated immature Platelet Fraction indicates
platelets are being produced• A low platelet and low IPF is consistent with a
platelet production disorder
5/27/2015
18
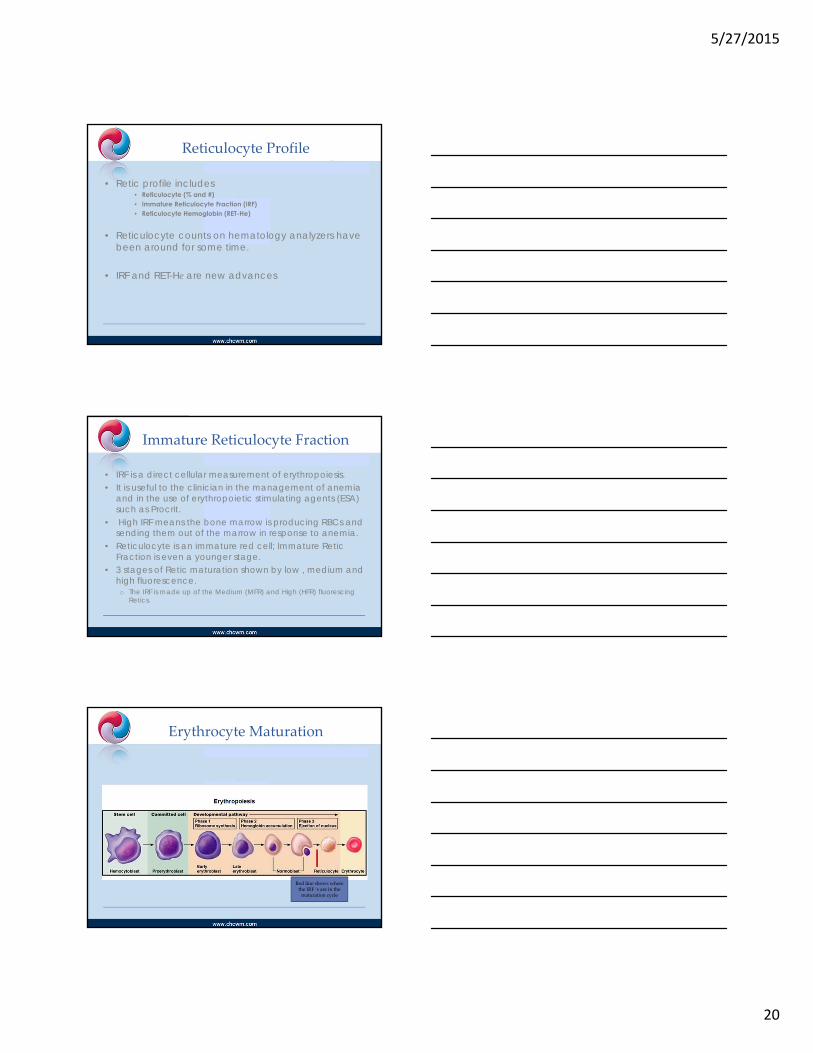
Example of report with canned text
1.Platelet count obtained by Fluorescent Flow Cytometry methodology which is specific for Platelet Mitochondria, providing the most accurate enumeration
2.An elevated immature Platelet Fraction indicates platelets are being produced
Example of Table View
Interesting Case and the Value of IPF

5/27/2015
19
Low Platelets with High IPF
The patient’s platelet count has dropped from 137,000 on day one ofthe 3rd cycle down to 17,000 on day eight. However, the IPF issignificantly high at 50%. This means the bone marrow is responding byproducing and releasing platelets from the bone marrow at a rapid ratein order to compensate for the shortage in the peripheral blood. Thepatient does not receive any blood products at this time because of herown body’s ability to respond to her platelet need.
Summary
Before having the ability to run and report the immature plateletfraction parameter, this patient would have been given a platelettransfusion on day eight of her third cycle. The IPF test gave a good lookat what was going on in the patient’s bone marrow and how her ownbody was responding. The IPF is a valuable tool in bone marrow plateletassessment and production rates. The IPF in this case saved the patienta platelet transfusion resulting in reduced medical costs and increasedpatient satisfaction
5/27/2015
20
Reticulocyte Profile
• Retic profile includes • Reticulocyte (% and #) • Immature Reticulocyte Fraction (IRF) • Reticulocyte Hemoglobin (RET-He)
• Reticulocyte counts on hematology analyzers have been around for some time.
• IRF and RET-He are new advances
Immature Reticulocyte Fraction
• IRF is a direct cellular measurement of erythropoiesis. • It is useful to the clinician in the management of anemia
and in the use of erythropoietic stimulating agents (ESA) such as Procrit.
• High IRF means the bone marrow is producing RBCs and sending them out of the marrow in response to anemia.
• Reticulocyte is an immature red cell; Immature Retic Fraction is even a younger stage.
• 3 stages of Retic maturation shown by low , medium and high fluorescence. o The IRF is made up of the Medium (MFR) and High (HFR) fluorescing
Retics.
Erythrocyte Maturation
Red line shows where the IRF ‘s are in the maturation cycle
5/27/2015
21
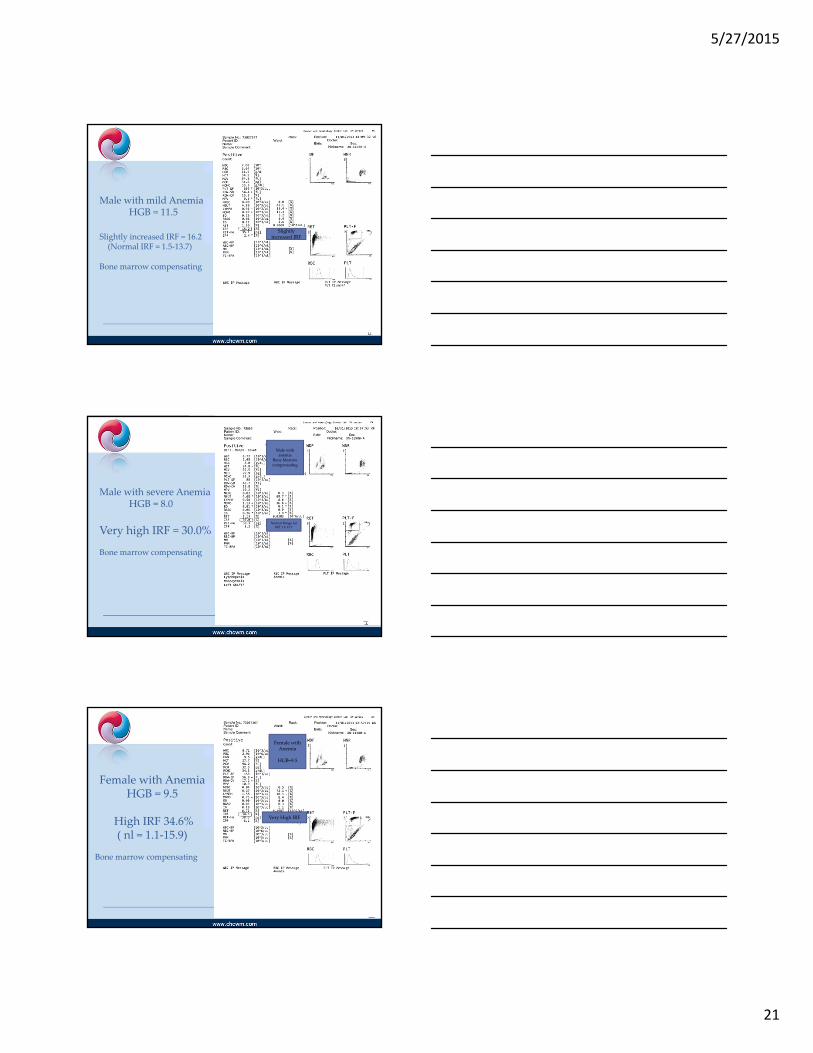
Male with mild AnemiaHGB = 11.5
Slightly increased IRF = 16.2(Normal IRF = 1.5‐13.7)
Bone marrow compensating
Slightly increased IRF
Male with severe AnemiaHGB = 8.0
Very high IRF = 30.0%
Bone marrow compensating
Male with anemia
Bone Marrow compensating
Normal Range for IRF 1.5‐13.7
Female with AnemiaHGB = 9.5
High IRF 34.6%( nl = 1.1‐15.9)
Bone marrow compensating
Female with Anemia
HGB=9.5
Very High IRF

5/27/2015
22
Erythropoiesis
Male with AnemiaHGB = 9.4
IRF= 0.0 %
Bone marrow not compensating
Patient will most likely need transfusion in the near future
Male with anemia but bone marrow not compensating
IRF = 0.0 %
RBC Breakdown
5/27/2015
23
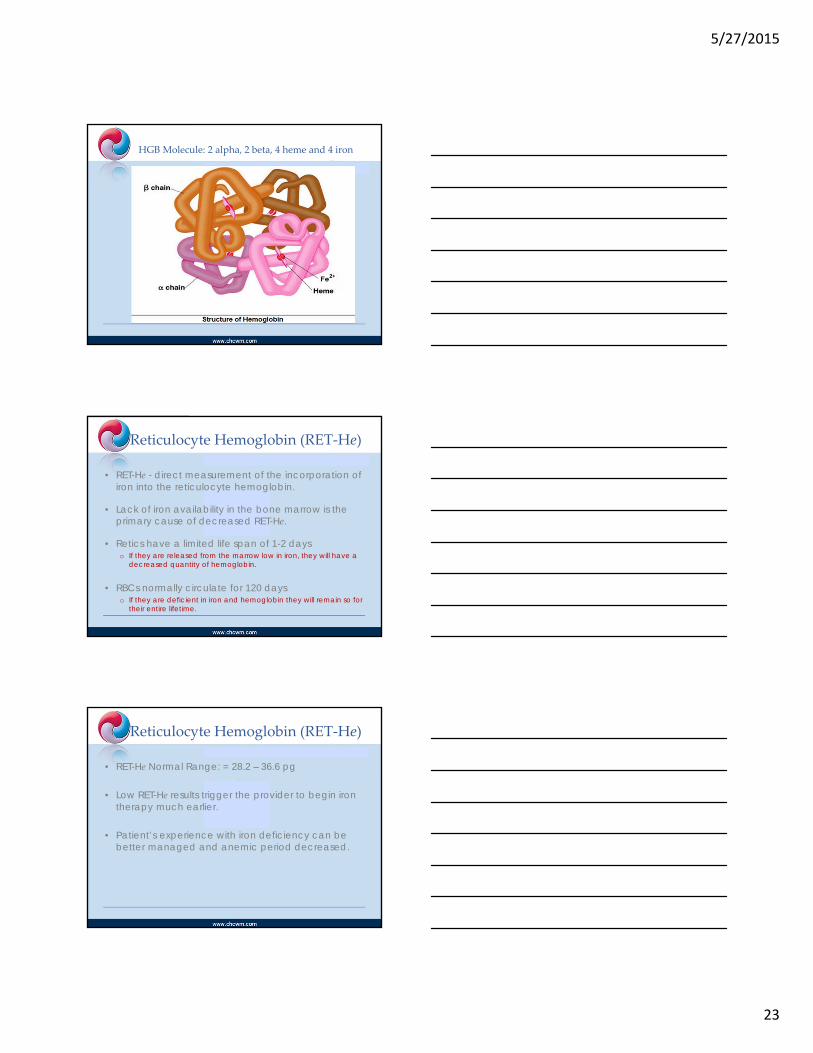
HGB Molecule: 2 alpha, 2 beta, 4 heme and 4 iron
Reticulocyte Hemoglobin (RET‐He)
• RET-He - direct measurement of the incorporation of iron into the reticulocyte hemoglobin.
• Lack of iron availability in the bone marrow is the primary cause of decreased RET-He.
• Retics have a limited life span of 1-2 days o If they are released from the marrow low in iron, they will have a
decreased quantity of hemoglobin.
• RBCs normally circulate for 120 days o If they are deficient in iron and hemoglobin they will remain so for
their entire lifetime.
Reticulocyte Hemoglobin (RET‐He)
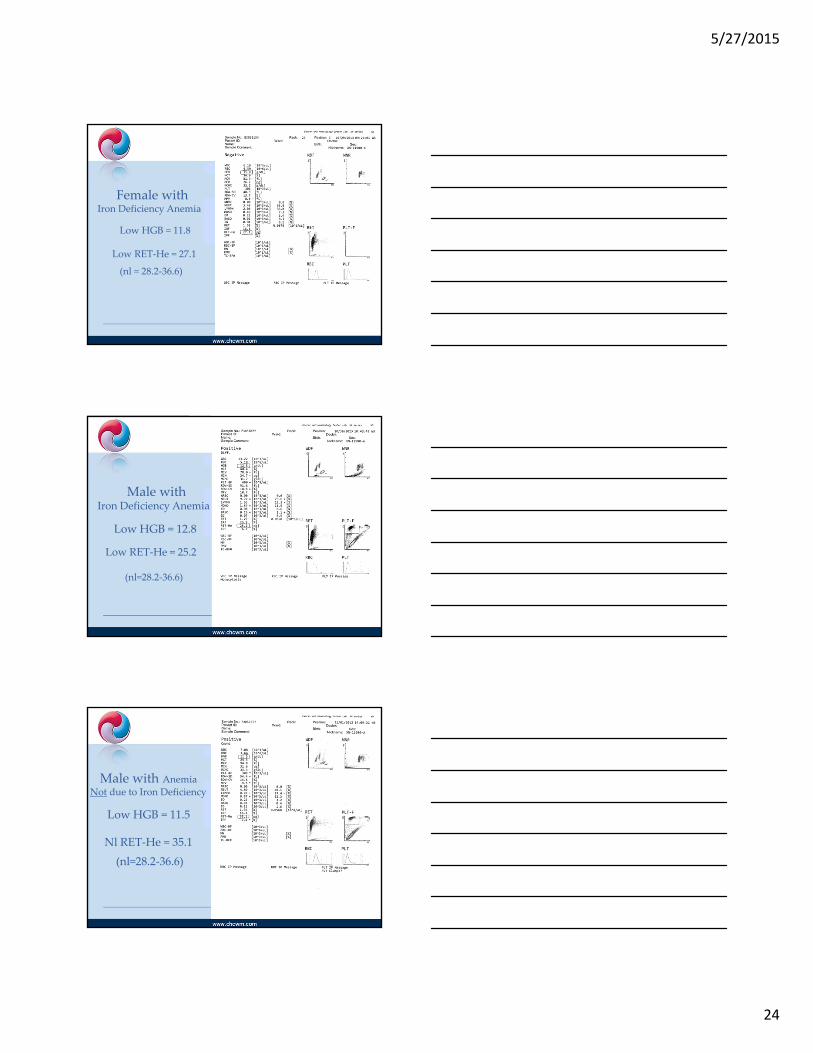
• RET-He Normal Range: = 28.2 – 36.6 pg
• Low RET-He results trigger the provider to begin iron therapy much earlier.
• Patient’s experience with iron deficiency can be better managed and anemic period decreased.
5/27/2015
24
Female withIron Deficiency Anemia
Low HGB = 11.8
Low RET‐He = 27.1
(nl = 28.2‐36.6)
Male withIron Deficiency Anemia
Low HGB = 12.8
Low RET‐He = 25.2
(nl=28.2‐36.6)
Male with Anemia
Not due to Iron Deficiency
Low HGB = 11.5
Nl RET‐He = 35.1
(nl=28.2‐36.6)
5/27/2015
25
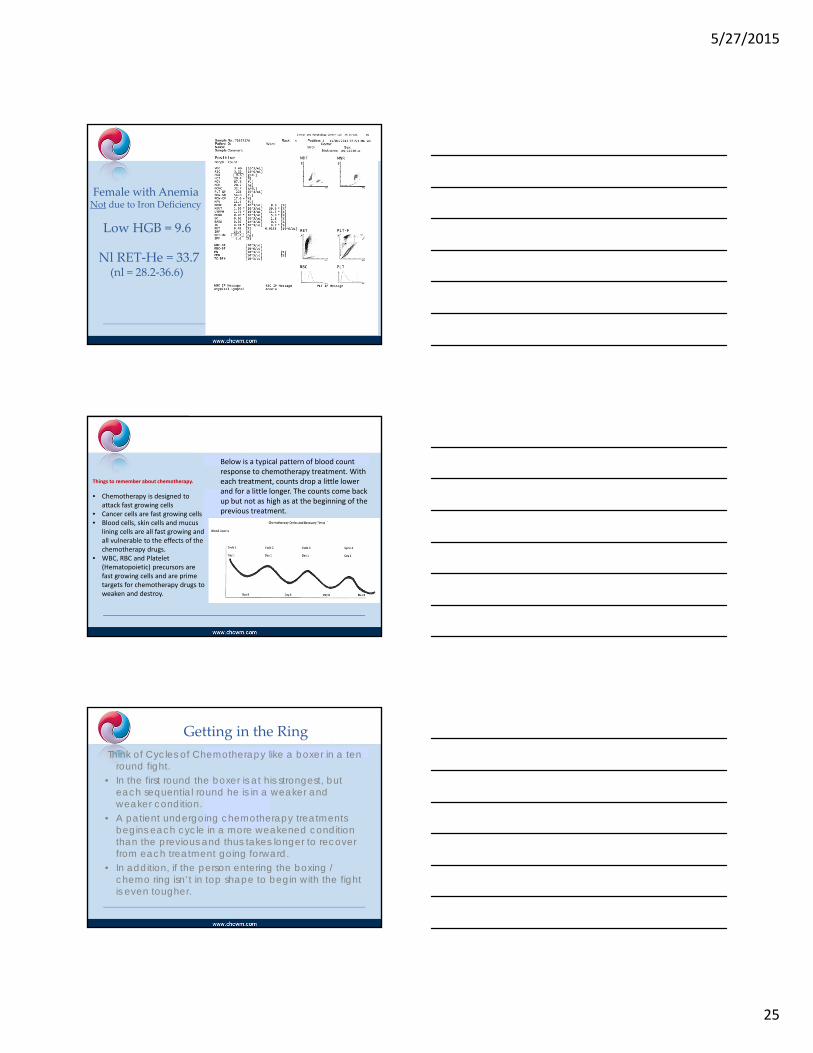
Female with Anemia Not due to Iron Deficiency
Low HGB = 9.6
Nl RET‐He = 33.7(nl = 28.2‐36.6)
Below is a typical pattern of blood count response to chemotherapy treatment. With each treatment, counts drop a little lower and for a little longer. The counts come back up but not as high as at the beginning of the previous treatment.
Things to remember about chemotherapy.
• Chemotherapy is designed to attack fast growing cells
• Cancer cells are fast growing cells• Blood cells, skin cells and mucus
lining cells are all fast growing and all vulnerable to the effects of the chemotherapy drugs.
• WBC, RBC and Platelet (Hematopoietic) precursors are fast growing cells and are prime targets for chemotherapy drugs to weaken and destroy.
Getting in the Ring
Think of Cycles of Chemotherapy like a boxer in a ten round fight.
• In the first round the boxer is at his strongest, but each sequential round he is in a weaker and weaker condition.
• A patient undergoing chemotherapy treatments begins each cycle in a more weakened condition than the previous and thus takes longer to recover from each treatment going forward.
• In addition, if the person entering the boxing / chemo ring isn’t in top shape to begin with the fight is even tougher.

5/27/2015
26
Summing It Up
Sysmex XN – 1000 – Our Healthcare Partner
• Easy to use
• Ready state – no wait to start
• Fast processing of results
• Customized “rules” to fit our needs
• Reflex testing
XN 1000 Maintenance
• Sysmex XN 1000
• No routine maintenance
• No start up maintenance Run controls and ready to go
• Simple step by step reagent replacement
• Walk away shut down – load cell clean and go

5/27/2015
27
Overall Results
• Accurate and rapid laboratory results greatly improve efficiency throughout the entire cancer center.
• Improves patient satisfaction by decreasing wait time and providing valuable information for treatment plan.
• New parameters on the Sysmex XN-1000 expand the patient’s hematology picture.
• Allows physicians to make quick and important changes in the care and treatment of their patients to improve outcomes.
Lab Staff of Tomorrow