christopher i. shaffrey, md - csrs · christopher i. shaffrey, md ... n congenital cervical canal...
TRANSCRIPT
11/13/16
1
Laminoplasty/Foraminotomy:
“Why Fuse the Spine at all?”
Christopher I. Shaffrey, MD John A. Jane Distinguished Professor Departments of Neurosurgery and
Orthopaedic Surgery University of Virginia
CSRS 21st Instructional Course Wednesday, November 30, 2016 Disclosures
n Medtronic: Consultant, Royalties, Patents n Biomet: Consultant, Royalties, Patents n Globus: Educational Consultant n Nuvasive: Consultant, Patents, Royalties n K2M: Educational Consultant n Stryker: Educational Consultant n NIH: Research Grant n Department of Defense: Research Grant n NATCN: Research Grant n AO: Research Grant n AO: Fellowship support n NREF: Fellowship support
CERVICAL FORAMINOTOMY(The other motion sparing
procedure)n ADVANTAGES?
n NO FUSION n LESS ADJACENT
SEGMENT DEGENERATION
n MINIMAL POTENTIAL FOR INSTABILITY
n CAN ADDRESS DISC AND SPUR
CERVICAL FORAMINOTOMY
n ADVANTAGES?n MULTILEVEL CAN BE
DONEn GOOD TRACK RECORD
FOR DECADES n LOW REPORTED
COMPLICATION RATE
Laminoforaminotomy
n Zeidman and Ducker reviewed 172 patients n 167 (97%) had relief of pain n Foraminotomy + discectomy for motor
weakness, 36 of 39 (93%) regained normal function
n One patient with post-op central cord syndrome
Posterior cervical laminoforaminotomy for radiculopathy: review of 172 cases. Neurosurgery. 1993 Sep;33(3):356-62.

11/13/16
2
Outpatient Foraminotomy
n Tomaras and associates reviewed 200 patients with follow-up on 183 (mean f/u 19 months)
n Non-worker’s compensation patients had 93% “good” or “excellent” outcome
n Worker’s compensation patients had 78% “good” or “excellent” outcome
Outpatient surgical treatment of cervical radiculopathy. J Neurosurg. 1997 Jul;87(1):41-3
Laminoforaminotomy for Disc Herniation and
Radiculopathy n Woertgen and associates reviewed 54
patients n At 1-year follow-up, 94% showed
improvement or complete recovery n Recommended early treatment
Prognostic factors of posterior cervical disc surgery: a prospective, consecutive study of 54 patients. Neurosurgery. 1997 40(4):724-8
Laminoforaminotomy
n UVA retrospective review of prospective database n 162 patients treated using the posterior cervical
foramintomy including partial facetectomy n Minimum 5-year clinical and radiographic follow-
up
J Neurosurg Spine 10(4):347-56, 2008
Laminoforaminotomy n Resolution of radiculopathy was experienced in
104 patients (95% of patients with radiculopathy) n Mean presenting NDI Score was 18 (Range, 2-39) n Mean post-operative NDI score was 8 (Range,
0-39) n Post-operative instability on dynamic imaging was
present in 8 patients (4.9%) n Post-operative loss of lordosis was seen following
30 patients (20%) n Vast majority asymptomatic
J Neurosurg Spine 10(4):347-56, 2008
Laminoforaminotomy n 5 patients (5.6%) required a total of 9
additional cervical spine operations n 2 cases this was due to disk degeneration at
the previously operated level (treated with ACDF)
n 2 cases required surgery at adjacent segments (treated with additional posterior surgery)
J Neurosurg Spine 10(4):347-56, 2008
Tandem Keyhole Foraminotomies
n Low patient numbers n 97% resolution of
radicular pain – Small percentage took
longer than 6 months for Sx resolution
n Longer f/u needed for effect on stability

11/13/16
3
n Muscle dissection n Often epidural bleeding n More postoperative neck spasm and
pain
Disadvantages:
CERVICAL FORAMINOTOMY MIS Surgical Technique
Microendoscopic Foraminotomy (MEF) Microendoscopic Discectomy (MED)
MIS vs. Open Foraminotomy
n Fessler et al. treated 25 patients MIS and 26 open
n Radiculopathy resolved in 54%, improved in 38% in MIS group (92% overall)
n Radiculopathy resolved in 48%, improved in 40% in open group (88% overall)
n Overall, outcomes were statistically equivalent
Minimally invasive cervical microendoscopic foraminotomy: an initial clinical experience. Neurosurgery. 2002 Nov;51(5 Suppl):S37-45
CERVICAL FORAMINOTOMY
n ISSUES?:– INSTABILITY– EFFICACY– INFECTION– CSF LEAK– ROOT/CORD
DAMAGE– INCREASED REOP
RATE
Posterior Cervical Approach: Instability
n Panjabi and colleagues n functional spine unit remains stable if:
n All anterior elements intact n One facet remains intact
n Ulrich and coworkers n flexion stability preserved when:
n Posterior ligamentous elements are intact n Despite extensive facetectomy
n Zdeblick and colleagues n In vitro study showed instability if
n >50% of facet removed
Panjabi et al J Biomech 8:327–336, 1975 Ulrich et al Spine 16 (3 Suppl):S4–S9, 1991 Zdeblick TA et al J Bone Joint Surg Am 74:22–27, 1992

11/13/16
4
Posterior Cervical Approach: UVA Series
n 973 posterior cervical hemilaminectomies between 1993-2008 n 162 patients with follow-up of 5 years or more
retrospectively analyzed n Radiculopathy resolved in 95% n No significant trend towards kyphosis in spite
of extensive facetectomy and pedicle drilling
J Neurosurg Spine 10(4):347-56, 2008
97 patients with MIS cervical foraminotomy/discectomy
Cervical Spine: Anterior vs Posterior Approach
n Adjacent level disease n More prominent in ACDF: incidence of 2.9%
per year1
n Posterolateral foraminotomy and discectomy: annual incidence 1.2%2
1. Hilibrand et al J Bone Joint Surg Am 81:519–528, 1999 2. Jagannathan et al J Neurosurg Spine 10(4):347-56, 2008
Prospective Studies: ACDF vs. Posterior Foraminotomy
n Herkowitz et al. Spine 1990 n 33 patients n Good/excellent results 94% anterior vs. 75% posterior
n Korinth et al. Spine 2006 n 292 patients total n Good/ excellent results 93.6% anterior vs. 85.1% posterior n Also overall results better for soft as compared to hard disc
for both groups
J Neurosurg: Spine / August 15, 2014 T.Y. Wang et al. / The Spine Journal - (2013) -

11/13/16
5
Why Laminoplasty? n Maintains motion of instrumented segments
– Reduces biomechanical demands on adjacent segments
– May reduce adjacent segment degeneration
n Reduces post-laminectomy instability n Reduces post-laminectomy membrane formation n Lower incidence of complications compared to
multilevel corpectomy
Why Not Laminoplasty?
n Not indicated if significant kyphosis n Does not directly address significant anterior
pathologic structures – Large disc herniation or osteophyte – Significant uncinate spurs causing radiculopathy
n ? Higher incidence of axial neck pain and shoulder pain compared with multilevel corpectomy
Complications of Laminectomy
n Post-Laminectomy Deformity n Well established in children (>80%) n More controversial in adults
n reportedly 6%-52% incidence
n Herkowitz Spine 1988 n 25% incidence in CSM
n Mikawa Spine 1987 n 0% incidence in CSM; 11% in OPLL
Post-Laminectomy Membrane
n Dorsal scarring + flexion movement = ? compression n Breig 1969 n Slucky NASS 1995 n Shinomiya CSRS 1995
n Role of posterior epidural ligament – anchors dura to ligamentum flavum
Open-Door Laminoplasty Indications
n Myelopathy or myeloradiculopathy caused by: n Congenital cervical canal stenosis n Multilevel cervical spondylosis n OPLL
n Surgical contraindications n Focal severe anterior cord compression n Kyphosis n Instability
n 103 studies, the results of which contained at least 1 of the pre-specified outcome variables, were identified comprising 8949 patients
n 4949 patients for whom a JOA score was reported there was improvement from a mean (± SD) score of 9.91 (± 1.65) to a score of 13.68 (± 1.05) after a mean follow-up of 44.18 months (± 35.1 months)

11/13/16
6
n The mean preoperative and postoperative C2–7 angles (2470 patients) remained stable from 14.17° (± 0.19°) to 13.98° (± 0.19°) of lordosis (average follow-up 39 months)
n Significantly decreased kyphosis when muscle/posterior element–sparing techniques were used (p = 0.02)
n An overall mean (2390 patients) of 47.3% loss of range of motion was reported
n Those patients with VAS recorded (986 patients), the postoperative pain level at a mean follow-up of 29 months was 2.78
n % of patients who complained of postoperative axial neck pain (1249 patients evaluated), the mean percentage was 30% at a mean follow-up of 51 months
Laminoplasy Techniques A. Hirabayashi B. Kurokawa C. Hardware-
augmented Hirabayashi
D. Hardware-augmented Kurokawa
E. Muscle sparing Hirabayashi
F. Muscle sparing Kurokawa
Laminoplasty Results Compare with Corpectomy
n Herkowitz HN. A comparision of anterior cervical fusion, cervical laminectomy and cervical laminoplasy for the surgical management of multiple level spondylotic radiculopathy. Spine 13:774-80, 1988
n Yonenobu K. Laminoplasty vs. subtotal corpectomy: A comparison study of results in multisegmental cervical spondylotic myelopathy. Spine 17:1281-4, 1992
– Equivalent functional recovery LP vs. Corp – Lower complication rates with LP
Laminoplasty Results Compare with Corpectomy
n Edwards CC. Corpectomy versus laminoplasty for multilevel cervical myelopathy. Spine 27:1168-77, 2002
n Independent matched cohort analysis n Greater neurological improvement with
laminoplasty (1.6 vs 0.9 Nurick grades) n Fewer complications with laminoplasty n Less pain medication required at final follow-
up with laminoplasty
Laminoplasty – Controveries Compared to Laminectomy with Fusion
n Heller JG. Laminoplasty versus laminectomy and fusion for multilevel cervical myelopathy. An independent matched cohort analysis. Spine 26:1330-36, 2001.
n Objective [Nurick score] and subjective improvement greater in laminoplasty group
n No complications in laminoplasty group n Complications in laminectomy + fusion group:
n Nonunion / hardware failure n Subjacent degeneration
n ? Can/should do laminectomy w/o fusion?

11/13/16
7
n Systematic review and meta-analysis of cohort studies comparing anterior CORP with posterior LAMP for the treatment of multilevel cervical myelopathy due to CSM or OPLL from 1990 to December 2012
n CORP and fusion was recommended for the treatment of multilevel cervical myelopathy when the involved <3 surgical segments
n Neurological recovery was superior in the CORP group compared with the LAMP group when the mean surgical segments were <3, but were similar between the two groups in > or equal to 3
n Surgical complications and complication-related reoperation and the higher surgical trauma associated with multilevel CORP (especially in > 3 segments)
n Neurological recovery was superior in the CORP group compared with the LAMP group when the mean surgical segments were <3, but were similar between the two groups in > or equal to 3
n Surgical complications and complication-related reoperation and the higher surgical trauma associated with multilevel CORP (especially in > 3 segments)
n Operation time in the CORP group was longer than that in the LAMP group
n Average blood loss was significantly more in the CORP group compared with the LAMP group
n There were significantly more reoperations in the CORP group
Weighted Mean Difference of Postoperative JOA
Odds Ratio of Reoperation Rates
11/13/16
8
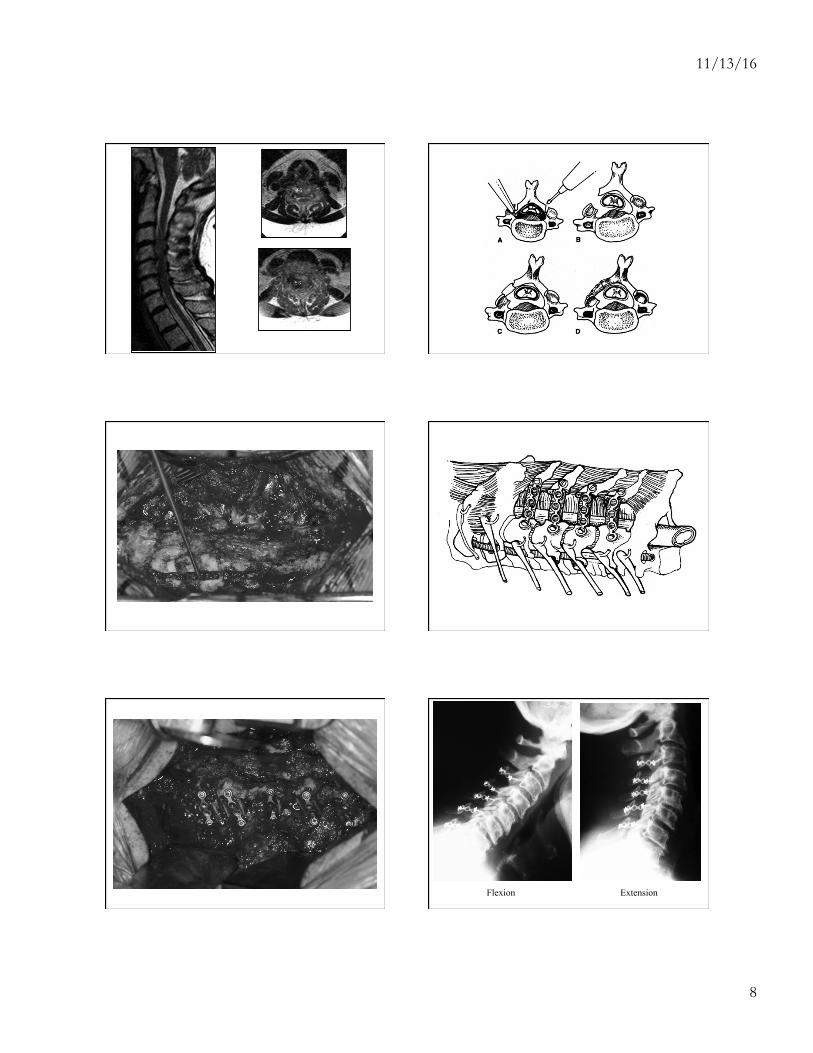
Flexion Extension

11/13/16
9
Laminoplasty - Controversies
n Increased axial pain / atrophy – ?excessive dissection / immobilization
n Fujimura Acta Orth Trauam Surg 1996 n Asano CSRS 1999 n Heller Spine 2001
n C5 nerve palsy – Reported incidence: 2% - 11% – Delayed onset – Generally transient
Indications for Fusion
n Instability n Kyphosis that fails to corrects in extension n Iatrogenic destabilization n Inflammatory disease n Severe axial pain? n Otherwise………Laminoplasty!