cervical duraplasty with tenting sutures via laminoplasty...
TRANSCRIPT

J Neurosurg: Spine / September 5, 2014
DOI: 10.3171/2014.7.SPINE13955
1
©AANS, 2014
CerviCal spondylotic myelopathy is a compressive myelopathy that has been attributed to spondylotic spurs, herniated discs, or hypertrophic ligaments.14
Cervical duraplasty with tenting sutures via laminoplasty for cervical flexion myelopathy in patients with Hirayama disease: successful decompression of a “tight dural canal in flexion” without spinal fusion
Clinical article
*Hirotaka ito, M.D., keisuke takai, M.D., PH.D., anD Makoto tanigucHi, M.D., PH.D.Department of Neurosurgery, Tokyo Metropolitan Neurological Hospital, Tokyo, Japan
Object. Hirayama disease, juvenile muscular atrophy of the distal upper extremity, is a rare type of cervical flex-ion segmental myelopathy and its etiology is still being debated. Two theories have been proposed: a “contact pres-sure” theory and “tight dural canal in flexion” theory. Previously reported treatments, including conservative neck collar therapy and surgical spinal fusion, used fixation of the cervical spine with the aim of avoiding contact pressure between the cord and anterior structures. On the other hand, treatment by duraplasty without spinal fusion has also been used, which aims at decompressing a tight dural canal in flexion by preventing abnormal forward displacement of the posterior dura mater without restricting cervical motion in young patients.
The authors developed a new surgical approach for treating a tight dural canal in flexion in patients with Hi-rayama disease: cervical duraplasty with tenting sutures via laminoplasty without spinal fusion. With this treatment they aimed to both decompress the spinal cord and preserve as much cervical motion as possible. The purpose of this study was to assess the clinical outcomes of patients who underwent this new surgical procedure and to investigate the etiology of Hirayama disease.
Methods. Six male patients (age range 17–23 years) with Hirayama disease underwent surgery between 2006 and 2012. The pre- and postoperative anteroposterior diameters of the dural canal in the flexed neck position, grip strength of the bilateral upper extremities, cervical alignment (C2–7), and cervical local flexion range of motion were compared. The presence or absence of surgical complications was assessed. To investigate the comparison group of Hirayama disease treated with spinal decompression, the PubMed database was searched for all relevant English-language case reports and series published between 1990 and 2013.
Results. The postoperative anteroposterior diameters of the dural canal were significantly expanded in the flexed neck position (7.2 ± 2.2 mm preoperatively vs 9.8 ± 1.7 mm postoperatively, p = 0.001). Grip strength of the upper extremities significantly improved bilaterally (20 ± 14 kg preoperatively vs 26 ± 15 kg postoperatively, p = 0.001). No significant difference was observed between pre- and postoperative cervical alignment in the neutral neck position (7.7° ± 8.1° preoperatively vs 9.0° ± 7.7° postoperatively, p = 0.74) or the cervical local flexion angle in the flexed neck position at the corresponding level of laminoplasty (16.6° ± 5.1° preoperatively vs 15.0° ± 9.4° postoperatively, p = 0.8). No surgical complications were noted, except for transient CSF leakage, which was resolved after lumbar drainage. The systematic review identified 37 cases from 7 reports: 26 with spinal fusion only, 5 with duraplasty without fusion, and 6 with combined duraplasty and fusion. In the largest series, in which 12 cases were treated with anterior fusion, cervical alignment was maintained, but local flexion motion was significantly decreased as a result of fixation. Although significant improvements in or stabilization of grip strength occurred in all 7 reported studies regardless of decompression procedures, one major delayed surgical complication was noted in a patient treated with anterior fusion. The patient developed severe kyphotic changes, which required reconstruction surgeries.
Conclusions. Cervical duraplasty with tenting sutures via laminoplasty prevented abnormal forward displace-ment of the posterior dura mater while preserving normal anterior structures and flexion motion of the cervical spine without major surgical complications. The clinical improvements achieved by the authors’ method support evidence that a tight dural canal in flexion largely contributes to segmental myelopathy in patients with Hirayama disease.(http://thejns.org/doi/abs/10.3171/2014.7.SPINE13955)
key WorDs • cervical flexion myelopathy • systematic review • forward displacement of the dura mater • spinal fusion • complication • follow-up study
Abbreviation used in this paper: ROM = range of motion.* Drs. Ito and Takai contributed equally to this work.

H. Ito, K. Takai, and M. Taniguchi
2 J Neurosurg: Spine / September 5, 2014
It is generally worsened by neck extension; however, rare groups of cervical myelopathies are caused by neck flex-ion.8
Hirayama disease, juvenile muscular atrophy of the distal upper extremity, is a rare type of cervical flexion segmental myelopathy. Major symptoms include a motor deficit and muscular atrophy of the distal upper extrem-ity with slight or no subjective or objective sensory dis-turbances.4 This muscular atrophy is unilateral in most patients and asymmetrically bilateral in others. The peak age at onset is 15–17 years, with a marked male prepon-derance, commonly slow onset and progression, and qui-escence several years after its onset.18 Because Hirayama disease differs from intrinsic motor neuron disease and spinal muscular atrophy, early diagnosis and specific treatments are important.
Two theories have been proposed as the causes of flexion myelopathy: a “contact pressure” theory and a “tight dural canal in flexion” theory. The contact pressure theory states that normal anterior structures, including intact vertebral bodies and intervertebral discs, contrib-ute to contact pressure over the spinal cord in flexion of the cervical spine.20 On the other hand, the tight dural canal in flexion theory states that abnormal forward dis-placement of the posterior dura mater contributes to spi-nal cord compression against normal anterior structures from behind.7
Treatments based on the first theory, which aim to relieve contact pressure by the fixation of normal cervi-cal vertebrae, include conservative neck collar therapy19 and anterior or posterior spinal fusion and have been frequently reported.10,11,20 However, to the best of our knowledge, treatments to decompress a tight dural canal in flexion by preventing abnormal forward displacement of the posterior dura mater without spinal fusion, such as duraplasty without spinal fusion, have been reported in only a few cases.1,3
We developed a new surgical treatment for a tight dural canal in flexion in patients with Hirayama disease: cervical duraplasty with tenting sutures via laminoplasty without spinal fusion. With this treatment we aimed to both decompress the spinal cord and preserve as much cervical motion as possible. The purpose of this study was to assess the clinical outcomes of patients who un-derwent this new surgical procedure and to investigate the etiology of Hirayama disease.
Methods
Patient Population
The study population included 6 consecutive male patients (age range 17–23 years) in whom Hirayama dis-ease was diagnosed at our institution between 2006 and 2012 (Table 1). The diagnosis of Hirayama disease was made on the basis of the following clinical signs and ex-amination results: onset between the age of 10 years and the early 20s; unilateral or asymmetrical bilateral atrophy of the intrinsic hand muscles and the flexor muscle group of the forearm, except for the brachioradialis muscle (Fig. 1); no objective sensory disturbance; no objective find-
ings in the lower extremities; a neurogenic pattern on an electromyographic examination restricted to the affected upper extremity; and neuroradiological findings that in-cluded the absence of disc herniations, spondylotic spurs, or hypertrophy of the yellow ligaments, as well as the presence of forward displacement of the posterior wall of the lower cervical dura mater in the flexed neck posi-tion, leading to spinal cord compression and spinal cord atrophy, as seen on CT myelography (Fig. 2) and/or MRI (Figs. 3 and 4). Other causes of myelopathy, such as spinal cord tumors and vascular malformations, syringomyelia, motor neuron disease, and neuropathy, were excluded.
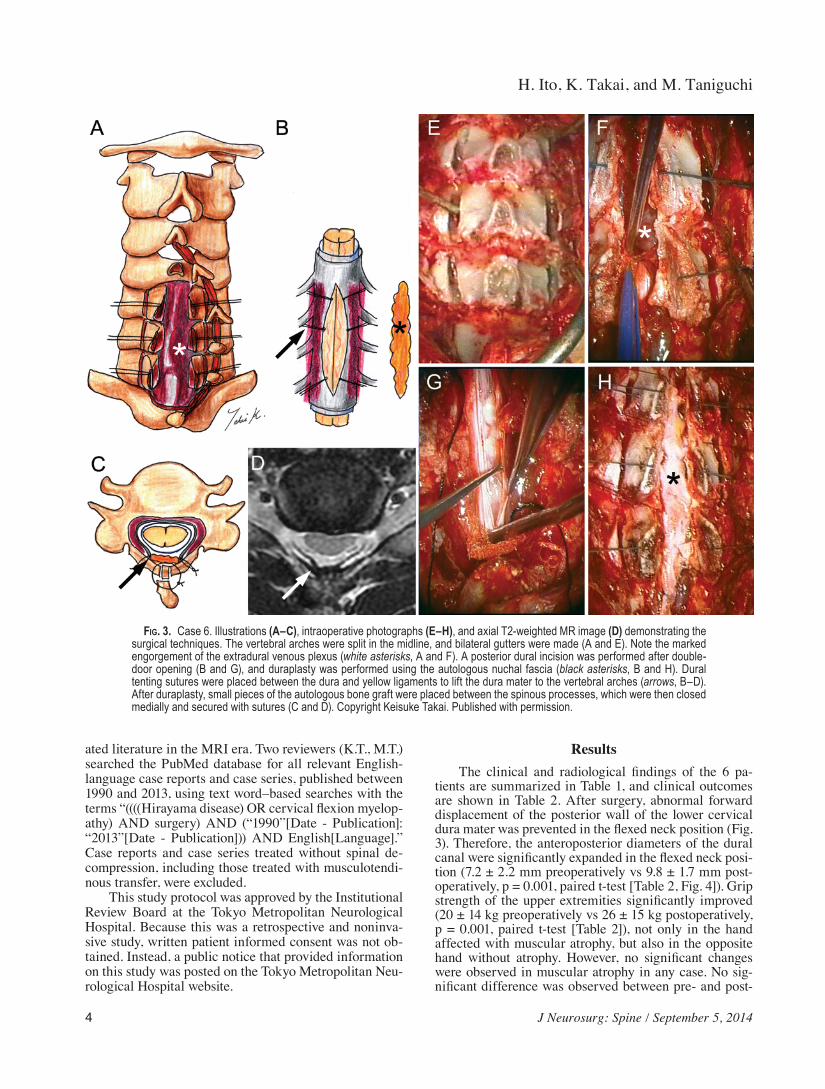
Surgical TechniquesFigure 3 shows illustrations of the surgical techniques
together with operative photographs. After a midline skin incision was made, the vertebral arches were split in the midline while preserving the spinous processes and nu-chal ligament. Bilateral hinges were made by creating bur holes through the outer cortical bone of the lamina-facet borders (Fig. 3A and E). After double-door opening of the vertebral arches, the engorged extradural venous plexus was moved outward beyond the midline (Fig. 3F) and a posterior dural incision was made under a microscope while keeping the arachnoid intact (Fig. 3B and G). Dural tenting sutures were placed between the edges of the du-ral opening and yellow ligaments to lift the dura mater to the vertebral arches and prevent forward displacement of the lower cervical dura mater in the flexed neck position (Fig. 3B and C). Duraplasty was made with the autolo-gous nuchal fascia to cover the dural opening (Fig. 3B and H). After duraplasty, small pieces of the autologous bone graft were placed between the spinous processes. The spinous processes were closed medially and secured with sutures (Fig. 3C and D). The neck was fixed postop-eratively with a cervical brace for the 1st and 2nd months, and with a soft neck collar for the 3rd month.
Data Collection and Statistical AnalysisMedical records, radiological images, and operative
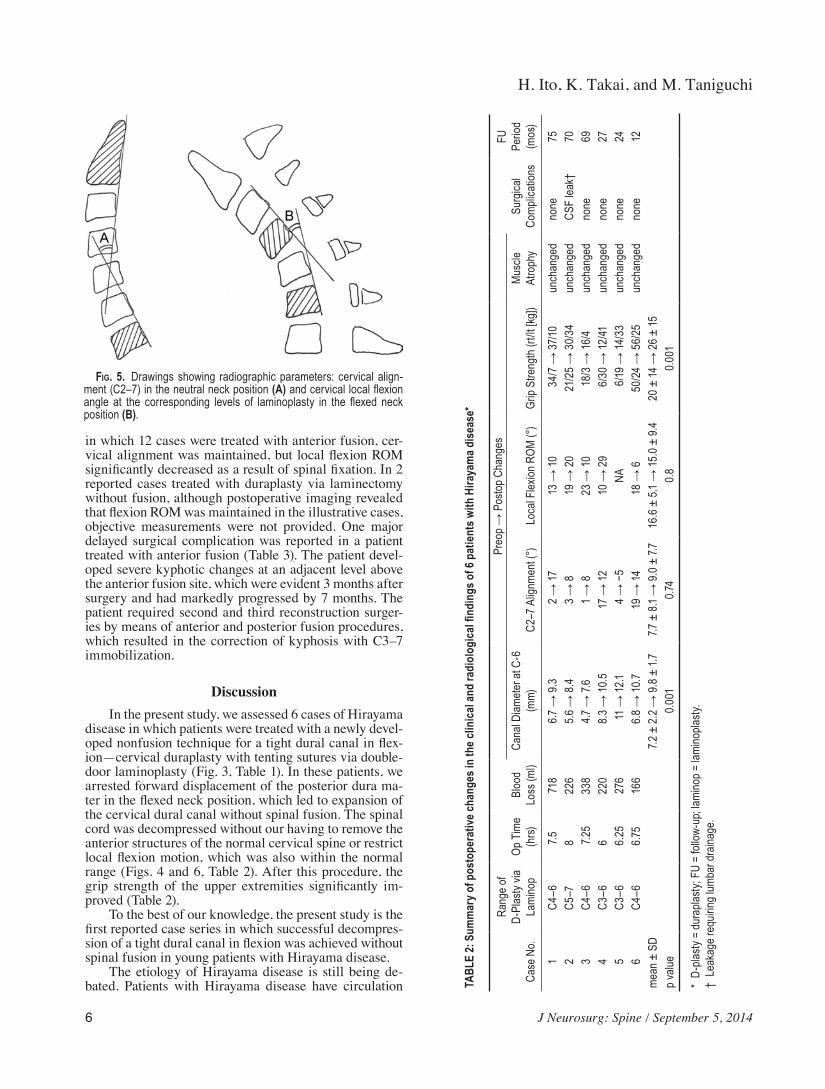
records were retrospectively reviewed to collect clinical data. The postoperative follow-up period ranged between 12 and 75 months (mean 46 months). We compared the pre- and postoperative anteroposterior diameters of the dural canal at the superior region of the C-6 vertebral body on T2-weighted MR images obtained with the pa-tient in the flexed-neck position to determine whether the cervical dural sac expanded. To confirm whether cervical alignment was maintained, we compared pre- and post-operative cervical alignment, which was measured as the angle composed of the posterior lines of the C-2 and C-7 vertebral bodies in the neutral neck position on cervical radiographs (Fig. 5). We then compared the pre- and post-operative cervical local flexion angle, which was mea-sured as the angle created by the posterior lines of the up-per and lower vertebral bodies at the corresponding levels of laminoplasty in the flexed neck position on cervical radiographs to confirm whether the cervical flexion range of motion (ROM) was maintained (Fig. 5). To assess clin-ical outcomes, we compared the pre- and postoperative

J Neurosurg: Spine / September 5, 2014
Decompression of “tight dural canal in flexion”
3
grip strengths of the bilateral upper extremities. A hand grip dynamometer was used to measure grip strengths. We also assessed the presence or absence of perioperative surgical complications such as CSF leakage, infection, new radiculopathy, new myelopathy, subdural/epidural hematoma, bone graft displacement, vertebral arch frac-tures, worsened intractable neck pain, pulmonary embo-lism, and cardiopulmonary complications.
A paired t-test was used to statistically analyze the data. SPSS II for Windows (SPSS Japan Inc.) statistical software was used for statistical analysis. A p value of < 0.05 was considered significant.
To investigate the comparison group in the reported series of Hirayama disease patients treated with spinal decompression, we systematically reviewed the associ-
TABLE 1: Summary of the preoperative clinical findings in 6 patients with Hirayama disease*
Case No.Age (yrs),
SexDuration of
Symptoms (mos) PresentationGrip Strength
(rt/lt, kg)Location of Muscle
AtrophyAbnormal EMG Findings
(neurogenic changes)
1 20, M 81 lt hand weakness 34/7 lt forearm, hand NA2 19, M 36 bilat hand weakness 21/25 bilat hands bilat Tri, FCR, FCU, FDI3 17, M 15 bilat hand weakness 18/3 bilat forearms, hands lt FDI, APB, FCR4 15, M 6 rt hand weakness 6/30 rt hand rt FCR, EDC, FDI5 18, M 37 bilat hand weakness 6/19 rt forearm, hand rt FCR, FCU, FDI, EDC, APB6 23, M 48 lt hand weakness 50/24 lt forearm, hand lt Del, Bi, Tri, FDI
* APB = abductor pollicis brevis; Bi = biceps; Del = deltoid; EDC = extensor digitorum communis; EMG = electromyography; FCR = flexor carpi radialis; FCU = flexor carpi ulnaris; FDI = first dorsal interosseous; NA = not available; Tri = triceps.
Fig. 1. Case 5. Photographs showing unilateral muscular atrophy of the right hand intrinsic (C) and flexor muscle group of the right forearm, except for the brachioradialis muscle (A and B).
Fig. 2. Case 6. Preoperative sagittal (A and B) and axial (C and D) CT myelograms showing spinal cord compression more in the flexed neck position than in the extended neck position by forward displace-ment of the posterior wall of the lower cervical dura mater. Note the spinal cord indentation produced by the dura mater (arrowhead, D).
H. Ito, K. Takai, and M. Taniguchi
4 J Neurosurg: Spine / September 5, 2014
ated literature in the MRI era. Two reviewers (K.T., M.T.) searched the PubMed database for all relevant English-language case reports and case series, published between 1990 and 2013, using text word–based searches with the terms “((((Hirayama disease) OR cervical flexion myelop-athy) AND surgery) AND (“1990”[Date - Publication]: “2013”[Date - Publication])) AND English[Language].” Case reports and case series treated without spinal de-compression, including those treated with musculotendi-nous transfer, were excluded.
This study protocol was approved by the Institutional Review Board at the Tokyo Metropolitan Neurological Hospital. Because this was a retrospective and noninva-sive study, written patient informed consent was not ob-tained. Instead, a public notice that provided information on this study was posted on the Tokyo Metropolitan Neu-rological Hospital website.
ResultsThe clinical and radiological findings of the 6 pa-
tients are summarized in Table 1, and clinical outcomes are shown in Table 2. After surgery, abnormal forward displacement of the posterior wall of the lower cervical dura mater was prevented in the flexed neck position (Fig. 3). Therefore, the anteroposterior diameters of the dural canal were significantly expanded in the flexed neck posi-tion (7.2 ± 2.2 mm preoperatively vs 9.8 ± 1.7 mm post-operatively, p = 0.001, paired t-test [Table 2, Fig. 4]). Grip strength of the upper extremities significantly improved (20 ± 14 kg preoperatively vs 26 ± 15 kg postoperatively, p = 0.001, paired t-test [Table 2]), not only in the hand affected with muscular atrophy, but also in the opposite hand without atrophy. However, no significant changes were observed in muscular atrophy in any case. No sig-nificant difference was observed between pre- and post-
Fig. 3. Case 6. Illustrations (A–C), intraoperative photographs (E–H), and axial T2-weighted MR image (D) demonstrating the surgical techniques. The vertebral arches were split in the midline, and bilateral gutters were made (A and E). Note the marked engorgement of the extradural venous plexus (white asterisks, A and F). A posterior dural incision was performed after double-door opening (B and G), and duraplasty was performed using the autologous nuchal fascia (black asterisks, B and H). Dural tenting sutures were placed between the dura and yellow ligaments to lift the dura mater to the vertebral arches (arrows, B–D). After duraplasty, small pieces of the autologous bone graft were placed between the spinous processes, which were then closed medially and secured with sutures (C and D). Copyright Keisuke Takai. Published with permission.

J Neurosurg: Spine / September 5, 2014
Decompression of “tight dural canal in flexion”
5
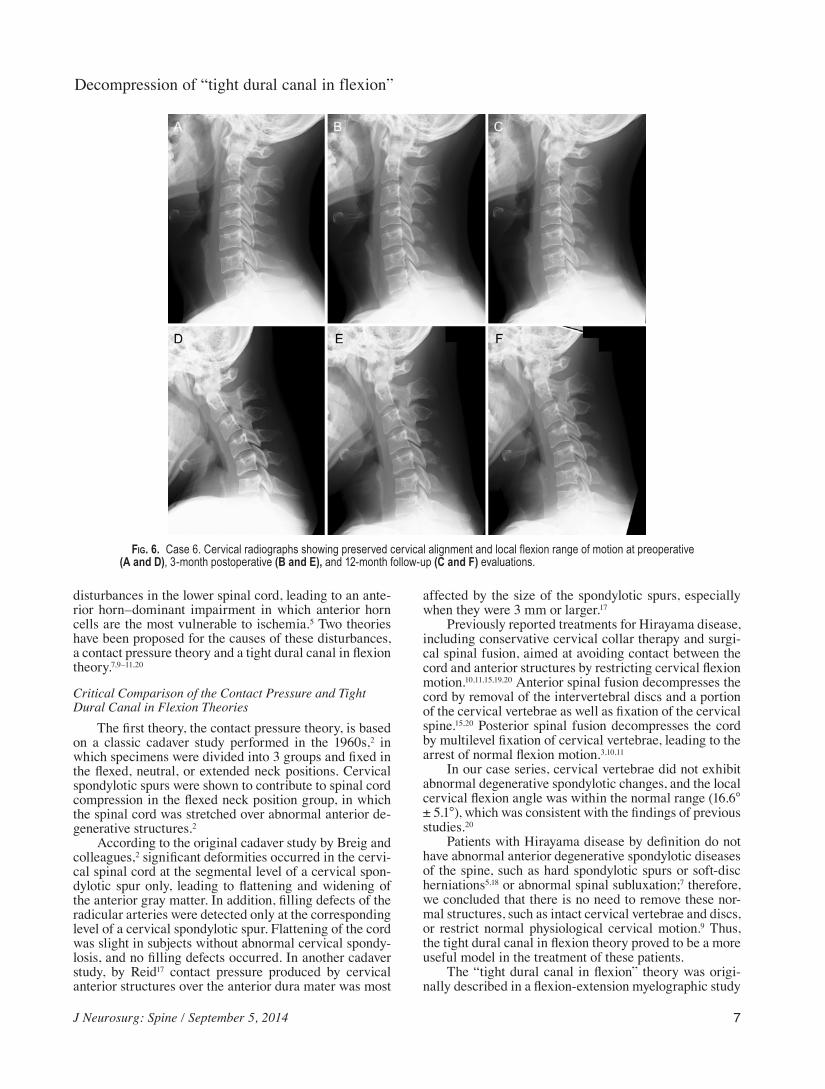
operative cervical alignment in the neutral neck position (7.7° ± 8.1° preoperatively vs 9.0° ± 7.7° postoperatively, p = 0.74, paired t-test [Table 2, Fig. 6]), or between the pre- and postoperative cervical local flexion angle in the flexed neck position at the corresponding levels of lami-noplasty (16.6° ± 5.1° preoperatively vs 15.0° ± 9.4° post-operatively, p = 0.8, paired t-test [Table 2, Fig. 6]). No perioperative surgical complications were noted, except for transient CSF leakage, which was resolved 1 week af-ter lumbar drainage.
Our systematic review identified a total of 37 cases
from 7 reports (Table 3). Twenty-six cases (70%) were treated with multilevel anterior or posterior fusion only, 5 cases (14%) were treated with duraplasty via laminectomy or laminoplasty without spinal fusion, and 6 cases (16%) were treated with combined duraplasty and spinal fusion. After surgical decompression, significant improvements in or stabilization of grip strength was noted in all 7 re-ports, regardless of decompression procedures. Overall, there have been few objective data regarding postopera-tive biomechanical assessments of the cervical spine in-cluding cervical alignment and ROM. In the largest series,
Fig. 4. Case 2. Preoperative axial (A) and sagittal (C) T2-weighted MR images revealing spinal cord compression in the flexed neck position by forward displacement of the posterior wall of the lower cervical dura mater. Axial images of the C-5, C5–6, C-6, C6–7, C-7, and C7–T1 levels are arranged from the top to the bottom (A). Note the marked passive engorgement of the extradural venous plexus (asterisks, A and C). Postoperative axial (B) and sagittal (D) T2-weighted MR images show significant expansion of the dural canal. Axial images of C-5, C5–6, C-6, C6–7, C-7, and C7–T1 levels are arranged in a similar manner (B). Note the dura mater lifted to the vertebral arch (arrows, B) and the absence of forward displacement in the flexed neck position (arrowheads, D).
H. Ito, K. Takai, and M. Taniguchi
6 J Neurosurg: Spine / September 5, 2014
in which 12 cases were treated with anterior fusion, cer-vical alignment was maintained, but local flexion ROM significantly decreased as a result of spinal fixation. In 2 reported cases treated with duraplasty via laminectomy without fusion, although postoperative imaging revealed that flexion ROM was maintained in the illustrative cases, objective measurements were not provided. One major delayed surgical complication was reported in a patient treated with anterior fusion (Table 3). The patient devel-oped severe kyphotic changes at an adjacent level above the anterior fusion site, which were evident 3 months after surgery and had markedly progressed by 7 months. The patient required second and third reconstruction surger-ies by means of anterior and posterior fusion procedures, which resulted in the correction of kyphosis with C3–7 immobilization.
DiscussionIn the present study, we assessed 6 cases of Hirayama
disease in which patients were treated with a newly devel-oped nonfusion technique for a tight dural canal in flex-ion—cervical duraplasty with tenting sutures via double-door laminoplasty (Fig. 3, Table 1). In these patients, we arrested forward displacement of the posterior dura ma-ter in the flexed neck position, which led to expansion of the cervical dural canal without spinal fusion. The spinal cord was decompressed without our having to remove the anterior structures of the normal cervical spine or restrict local flexion motion, which was also within the normal range (Figs. 4 and 6, Table 2). After this procedure, the grip strength of the upper extremities significantly im-proved (Table 2).
To the best of our knowledge, the present study is the first reported case series in which successful decompres-sion of a tight dural canal in flexion was achieved without spinal fusion in young patients with Hirayama disease.
The etiology of Hirayama disease is still being de-bated. Patients with Hirayama disease have circulation TA
BLE
2: S
umm
ary o
f pos
tope
rativ
e cha
nges
in th
e clin
ical
and
radi
olog
ical
findi
ngs o
f 6 p
atie
nts w
ith H
iraya
ma d
iseas
e*
Case
No.
Rang
e of
D-Pl
asty
via
Lami
nop
Op T
ime
(hrs)
Bloo
d Lo
ss (m
l)
Preop →
Postop
Changes
Surg
ical
Comp
licati
ons
FU
Perio
d (m
os)
Cana
l Diam
eter a
t C-6
(m
m)C2
–7 A
lignm
ent (
°)Lo
cal F
lexion
ROM
(°)
Grip
Stre
ngth
(rt/lt
[kg])
Mus
cle
Atro
phy
1C4
–67.5
718
6.7 →
9.3
2 → 17
13 →
1034/7 →
37/10
unch
ange
dno
ne75
2C5
–78
226
5.6 →
8.4
3 → 8
19 →
2021/25 →
30/34
unch
ange
dCS
F lea
k†70
3C4
–67.2
533
84.7
→ 7.6
1 → 8
23 →
1018/3 →
16/4
unch
ange
dno
ne69
4C3
–66
220
8.3 →
10.5
17 →
1210 →
296/30 →
12/41
unch
ange
dno
ne27
5C3
–66.
2527
611 →
12.1
4 → −5
NA6/1
9 → 14
/33
unch
ange
dno
ne24
6C4
–66.7
516
66.8 →
10.7
19 →
1418 →
650/24
→ 56/25
unch
ange
dno
ne12
mean
± S
D7.2
± 2.2 →
9.8 ±
1.7
7.7 ± 8.1 →
9.0 ±
7.7
16.6 ± 5.1
→ 15
.0 ± 9.4
20 ± 14
→ 26
± 15
p valu
e 0.0
010.7
40.
80.0
01
* D-
plasty
= du
rapla
sty; F
U =
follo
w-up
; lami
nop =
lami
nopla
sty.
† Le
akag
e req
uiring
lumb
ar dr
ainag
e.
Fig. 5. Drawings showing radiographic parameters: cervical align-ment (C2–7) in the neutral neck position (A) and cervical local flexion angle at the corresponding levels of laminoplasty in the flexed neck position (B).
J Neurosurg: Spine / September 5, 2014
Decompression of “tight dural canal in flexion”
7
disturbances in the lower spinal cord, leading to an ante-rior horn–dominant impairment in which anterior horn cells are the most vulnerable to ischemia.5 Two theories have been proposed for the causes of these disturbances, a contact pressure theory and a tight dural canal in flexion theory.7,9–11,20
Critical Comparison of the Contact Pressure and Tight Dural Canal in Flexion Theories
The first theory, the contact pressure theory, is based on a classic cadaver study performed in the 1960s,2 in which specimens were divided into 3 groups and fixed in the flexed, neutral, or extended neck positions. Cervical spondylotic spurs were shown to contribute to spinal cord compression in the flexed neck position group, in which the spinal cord was stretched over abnormal anterior de-generative structures.2
According to the original cadaver study by Breig and colleagues,2 significant deformities occurred in the cervi-cal spinal cord at the segmental level of a cervical spon-dylotic spur only, leading to flattening and widening of the anterior gray matter. In addition, filling defects of the radicular arteries were detected only at the corresponding level of a cervical spondylotic spur. Flattening of the cord was slight in subjects without abnormal cervical spondy-losis, and no filling defects occurred. In another cadaver study, by Reid17 contact pressure produced by cervical anterior structures over the anterior dura mater was most
affected by the size of the spondylotic spurs, especially when they were 3 mm or larger.17
Previously reported treatments for Hirayama disease, including conservative cervical collar therapy and surgi-cal spinal fusion, aimed at avoiding contact between the cord and anterior structures by restricting cervical flexion motion.10,11,15,19,20 Anterior spinal fusion decompresses the cord by removal of the intervertebral discs and a portion of the cervical vertebrae as well as fixation of the cervical spine.15,20 Posterior spinal fusion decompresses the cord by multilevel fixation of cervical vertebrae, leading to the arrest of normal flexion motion.3,10,11
In our case series, cervical vertebrae did not exhibit abnormal degenerative spondylotic changes, and the local cervical flexion angle was within the normal range (16.6° ± 5.1°), which was consistent with the findings of previous studies.20
Patients with Hirayama disease by definition do not have abnormal anterior degenerative spondylotic diseases of the spine, such as hard spondylotic spurs or soft-disc herniations5,18 or abnormal spinal subluxation;7 therefore, we concluded that there is no need to remove these nor-mal structures, such as intact cervical vertebrae and discs, or restrict normal physiological cervical motion.9 Thus, the tight dural canal in flexion theory proved to be a more useful model in the treatment of these patients.
The “tight dural canal in flexion” theory was origi-nally described in a flexion-extension myelographic study
Fig. 6. Case 6. Cervical radiographs showing preserved cervical alignment and local flexion range of motion at preoperative (A and D), 3-month postoperative (B and E), and 12-month follow-up (C and F) evaluations.

H. Ito, K. Takai, and M. Taniguchi
8 J Neurosurg: Spine / September 5, 2014
TABL
E 3:
A sy
stem
atic
revi
ew o
f the
repo
rted
serie
s of H
iraya
ma d
iseas
e tre
ated
with
spin
al de
com
pres
sion*
Auth
ors &
Yea
rNo
of
Case
s
Posto
pera
tive C
hang
es
Comp
licati
ons
FU
Perio
d (m
os)
Oper
ative
Pro
cedu
reSp
inal C
anal
or
Cord
Diam
eter
Mea
n C2–
7 Al
ignme
nt M
ean F
lexion
ROM
M
ean G
rip S
treng
th (kg
)M
uscle
Atro
phy
Lin et
al., 2
010
4AF
NANA
decr
ease
d†im
prov
ed in
2 ca
ses
sligh
tly im
prov
ed in
2 ca
ses
none
40Lin
et al
., 201
01
D-pla
sty vi
a lam
inec
w/
o fus
ionNA
NAma
intain
ed‡
unch
ange
dim
prov
edno
ne39
Arre
se et
al.,
20
091
D-pla
sty vi
a lam
inec
w/
o fus
ioninc
reas
ed in
flexio
n§NA
maint
ained
‡un
chan
ged
unch
ange
dno
ne24
Patel
et al
., 200
91
D-pla
sty vi
a lam
inec
w/
PF
NAsli
ght k
ypho
sisNA
impr
oved
NAno
ne3
Wat
anab
e et a
l.,
20
0512
AFinc
reas
ed in
neut
ral
maintain
ed, −4.7
°
→ −1
.5°decreased, 11.8° →
2.2°
improved, 16.3 →
18.6
unch
ange
dno
ne63
Fujim
oto et
al.,
20
023
D-pla
sty vi
a lam
inop
w/
o fus
ionNA
NANA
impr
oved
in 3
case
sun
chan
ged,
later
wor
sene
d
in 2 c
ases
none
41
Kohn
o et a
l.,
19
9910
AF in
7 ca
ses,
PF in
3 cas
esNA
seve
re ky
phos
is in
1
case
decr
ease
d†improved, 20.0
→ 26
.4im
prov
ed in
1 ca
se, s
lightl
y
impr
oved
in 1
case
reco
nstru
ctive
ops i
n 1 ca
se¶
45
Konn
o et a
l.,
19
975
D-pla
sty vi
a lam
inop
w/
PF
incre
ased
in
ne
utra
lNA
NAimproved, 9.3 →
18.3
sligh
tly im
prov
ed in
5 ca
ses
none
24
* AF
= an
terior
fusio
n; lam
inec =
lami
necto
my; P
F =
poste
rior f
usion
. † Po
stoperative ima
ging s
howe
d a de
creased fl
exion
ROM
in the illustrative ca
se (obje
ctive measureme
nts were n
ot provide
d).
‡ Po
stoperative ima
ging s
howe
d main
taine
d flexion
ROM
in the illustrative ca
se (obje
ctive measureme
nts were n
ot provide
d).
§ Po
stoperative ima
ging s
howe
d an increased sp
inal canal dia
meter
in the fl
exed ne
ck po
sition
in the illustrative ca
se (obje
ctive measureme
nts were n
ot provide
d).
¶ Se
vere
kyph
osis
prog
ress
ed se
vera
l mon
ths a
fter a
nterio
r fus
ion an
d req
uired
seco
nd an
d thir
d rec
onstr
uctiv
e sur
gerie
s in 1
case
.

J Neurosurg: Spine / September 5, 2014
Decompression of “tight dural canal in flexion”
9
in 1987.7 The posterior surface of the lower cervical dura mater was shown to migrate forward more in the flexed neck position than in the neutral and extended neck posi-tions. Abnormal forward displacement of the dura mater was shown to compress the cervical spinal cord against normal anterior vertebral bodies, even though there was no cervical spondylosis and the cervical flexion ROM was within normal limits. A tight dural canal was attrib-uted to uneven growth of the spine and dura.9
After the introduction of MRI, abnormal forward displacement of the dura mater and flattening of the spi-nal cord could easily be identified using flexion MRI.12,13 Considerable attention has recently been paid to these neuroradiological findings because they have high sen-sitivity and specificity in the diagnosis of Hirayama dis-ease. Although forward displacement of the dura mater also occurs in normal control subjects, flattening, widen-ing, and distortion in the spinal cord do not occur, be-cause forward displacement is generally 1 mm on aver-age. On the other hand, forward displacement of the dura mater has been recently shown to be several times greater in patients with Hirayama disease than in normal sub-jects.12 As a result, the spinal cord is compressed against normal anterior structures by the abnormally shifted dura mater, even though there is no spondylosis or subluxation in the cervical spine.6 Anterior dural shifting has also been shown to contribute to enlargements of the poste-rior epidural space, leading to passive posterior epidural vertebral plexus engorgement in the flexed neck position without epidural pressure changes.16
In the largest reported case series study on surgical spinal fusion in patients with Hirayama disease, the local cervical flexion angle at the corresponding levels of the lower cervical spine was “corrected” from 11.8° ± 7.0° to 2.2° ± 2.9° by anterior fusion.20 Although grip strength significantly increased after surgery in this series, it is rea-sonable to conclude that in the patients in this case series, the removal of normal anterior structures and fixation of normal cervical motion contributed to the prevention of cervical flexion motion, which had an indirect influence on forward displacement of the posterior dura mater be-cause forward displacement of the dura occurs only in the flexed neck position. Although the cervical flexion angle was preserved in an equal measure with the preoperative value in our series and the spinal cord shifted anteriorly in the flexed neck position, grip strength increased by 30% of preoperative values because the dura did not shift anteriorly and the spinal cord was free from compression by the dura mater. In a previous study, a patient required additional reconstructive surgeries after anterior fusion because delayed severe kyphotic changes occurred at an adjacent level above the fusion site.10 Our series was not complicated by adjacent-level kyphosis or restenosis dur-ing the follow-up period. The immobilization of normal physiological movement may lead to adjacent-level prob-lems in the long term.
We believe that significant expansion of the dural canal in the flexed neck position by duraplasty is theo-retically reasonable if the anteriorly shifted posterior dura mater contributes to cervical flexion myelopathy. Not only duraplasty, but also dural tenting sutures to lift the
dura to the vertebral arches, prevented forward displace-ment of the dura mater in the flexed neck position, result-ing in significant expansion of the dural canal by 2.6 mm on average (36% of preoperative diameter), which was 2 times greater than previous findings.11 Passive engorge-ment of the posterior epidural venous plexus also disap-peared following surgery (Fig. 4). Although Case 2 devel-oped a CSF fistula, it was resolved after lumbar drainage. Therefore, it was important to keep the arachnoid intact when the dural incision was made to prevent a CSF fis-tula. The clinical improvements observed in grip strength by our method support evidence that a tight dural canal in flexion induced by forward displacement of the lower cervical dura mater contributes largely to segmental my-elopathy in patients with Hirayama disease.
LimitationsThis study has some limitations. Because the inci-
dence of Hirayama disease is very low, this study was limited to a small number of patients, and assessments of the outcomes of patients treated by our technique were not compared prospectively with those of patients treated with other medical or surgical techniques. Therefore, fur-ther well-designed studies are needed using larger num-bers of patients.
ConclusionsCervical duraplasty with tenting sutures via lamino-
plasty led to spinal cord decompression with the preserva-tion of cervical alignment and local physiological motion in young patients with Hirayama disease without major complications. The clinical improvements achieved by our method support the theory that a tight dural canal in flexion largely contributes to segmental myelopathy in pa-tients with Hirayama disease.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Conception and design: Takai, Taniguchi. Acquisition of data: all authors. Analysis and interpretation of data: Takai. Drafting the article: Takai, Ito. Critically revising the article: Takai. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Takai. Statistical analysis: Takai. Study supervision: Takai, Taniguchi. Medical illus-trations: Takai.
References
1. Arrese I, Rivas JJ, Esteban J, Ramos A, Lobato RD: A case of Hirayama disease treated with laminectomy and duraplasty without spinal fusion. Neurocirugia (Astur) 20:555–558, 2009
2. Breig A, Turnbull I, Hassler O: Effects of mechanical stresses on the spinal cord in cervical spondylosis. A study on fresh cadaver material. J Neurosurg 25:45–56, 1966
3. Fujimoto Y, Oka S, Tanaka N, Nishikawa K, Kawagoe H, Baba I: Pathophysiology and treatment for cervical flexion myelopa-thy. Eur Spine J 11:276–285, 2002
4. Hirayama K, Tokumaru Y: Cervical dural sac and spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology 54:1922–1926, 2000

H. Ito, K. Takai, and M. Taniguchi
10 J Neurosurg: Spine / September 5, 2014
5. Hirayama K, Tomonaga M, Kitano K, Yamada T, Kojima S, Arai K: Focal cervical poliopathy causing juvenile muscular atrophy of distal upper extremity: a pathological study. J Neu-rol Neurosurg Psychiatry 50:285–290, 1987
6. Hou C, Han H, Yang X, Xu X, Gao H, Fan D, et al: How does the neck flexion affect the cervical MRI features of Hirayama disease? Neurol Sci 33:1101–1105, 2012
7. Iwasaki Y, Tashiro K, Kikuchi S, Kitagawa M, Isu T, Abe H: Cervical flexion myelopathy: a “tight dural canal mecha-nism.” Case report. J Neurosurg 66:935–937, 1987
8. Jeffreys RV: The surgical treatment of cervical myelopathy due to spondylosis and disc degeneration. J Neurol Neuro-surg Psychiatry 49:353–361, 1986
9. Kato Y, Kataoka H, Ichihara K, Imajo Y, Kojima T, Kawano S, et al: Biomechanical study of cervical flexion myelopathy using a three-dimensional finite element method. Laboratory investigation. J Neurosurg Spine 8:436–441, 2008
10. Kohno M, Takahashi H, Ide K, Yamakawa K, Saitoh T, Inoue K: Surgical treatment for patients with cervical flexion my-elopathy. J Neurosurg 91 (1 Suppl):33–42, 1999
11. Konno S, Goto S, Murakami M, Mochizuki M, Motegi H, Moriya H: Juvenile amyotrophy of the distal upper extremity: pathologic findings of the dura mater and surgical manage-ment. Spine (Phila Pa 1976) 22:486–492, 1997
12. Lai V, Wong YC, Poon WL, Yuen MK, Fu YP, Wong OW: Forward shifting of posterior dural sac during flexion cervical magnetic resonance imaging in Hirayama disease: an initial study on normal subjects compared to patients with Hirayama disease. Eur J Radiol 80:724–728, 2011
13. Lehman VT, Luetmer PH, Sorenson EJ, Carter RE, Gupta V, Fletcher GP, et al: Cervical spine MR imaging findings of pa-tients with Hirayama disease in North America: a multisite study. AJNR Am J Neuroradiol 34:451–456, 2013
14. Levine DN: Pathogenesis of cervical spondylotic myelopathy. J Neurol Neurosurg Psychiatry 62:334–340, 1997
15. Lin MS, Kung WM, Chiu WT, Lyu RK, Chen CJ, Chen TY: Hirayama disease. Clinical article. J Neurosurg Spine 12: 629–634, 2010
16. Patel TR, Chiocca EA, Freimer ML, Christoforidis GA: Lack of epidural pressure change with neck flexion in a patient with Hirayama disease: case report. Neurosurgery 64:E1196–1197, 2009
17. Reid JD: Effects of flexion-extension movements of the head and spine upon the spinal cord and nerve roots. J Neurol Neu-rosurg Psychiatry 23:214–221, 1960
18. Tashiro K, Kikuchi S, Itoyama Y, Tokumaru Y, Sobue G, Mu-kai E, et al: Nationwide survey of juvenile muscular atrophy of distal upper extremity (Hirayama disease) in Japan. Amyo-troph Lateral Scler 7:38–45, 2006
19. Tokumaru Y, Hirayama K: [Cervical collar therapy for juve-nile muscular atrophy of distal upper extremity (Hirayama disease): results from 38 cases.] Rinsho Shinkeigaku 41:173–178, 2001 (Jpn)
20. Watanabe K, Hasegawa K, Hirano T, Endo N, Yamazaki A, et al: Anterior spinal decompression and fusion for cervical flex-ion myelopathy in young patients. J Neurosurg Spine 3:86–91, 2005
Manuscript submitted October 24, 2013.Accepted July 21, 2014.Please include this information when citing this paper: published
online September 5, 2014; DOI: 10.3171/2014.7.SPINE13955.Address correspondence to: Keisuke Takai, M.D., Ph.D., Depart-
ment of Neurosurgery, Tokyo Metropolitan Neurological Hospital, 2-6-1, Musashidai, Fuchu, Tokyo 183-0042, Japan. email: takai-nsu @umin.ac.jp.