child survival and population growth - unicef
TRANSCRIPT
Child survival and population growth
In briefThe world's population doubled to 5 billion between 1950 and 1987,and is expected to reach 6.3 billion by the year 2000. Thereafter, globalpopulation could reach anywhere between 8 and 14 billion, depend-ing on how quickly the world arrives at the level of replacementfertility, before stablilizing sometime in the late twenty-first or earlytwenty-second century.
Contrary to popular belief, accelerated child survival strategies,when combined with direct family planning measures, actually resultin slower population growth, thereby making a stable and lower totalworld population attainable earlier.
The effects of major improvements in child survival on world populationgrowth are often misunderstood. One assumption is that any reduction inchild mortality rates must automatically add to population and populationgrowth rates and that any reduction in the number of children dying eachyear would increase total world population, now and in the future.
In fact, the opposite is the case. Actions which extend child andmaternal health services and expand educational opportunities for girlsand women help to both increase child survival and reduce fertility, makingfor lower population growth rates in the longer run.
When combined with direct family planning efforts, actions to acceler-ate child survival are likely to lead to slower population growth and, there-fore, the earlier attainment of a stable and lower world population thanwould be the case if family planning or child survival measures were takenindependently of each other.
This interactive relationship is the essential logic for stressing thecomplementarity of vigorously pursuing child survival and family planningas key elements of maternal child health and human advancement.
39
Population growth -the facts and
figures
World population was about 300 million 2,000 years ago. It then took some1,500 years for population to double. By 1750, world population began torise steadily at the then unprecedented rate of about 0.5 per cent per year.The most rapid increase occurred in what are today's developed countries,mainly in Europe. Growth was slower elsewhere. By 1900, world popula-tion had doubled again, reaching 1.7 billion.
Population growth continued to accelerate in the course of the presentcentury, reaching a 1.5 per cent annual growth rate by 1950 and a peak rateof 2 per cent around 1965. Total population doubled yet again, going from2.5 billion in 1950 to 5 billion in 1987. Developing countries accounted for85 per cent of that growth.
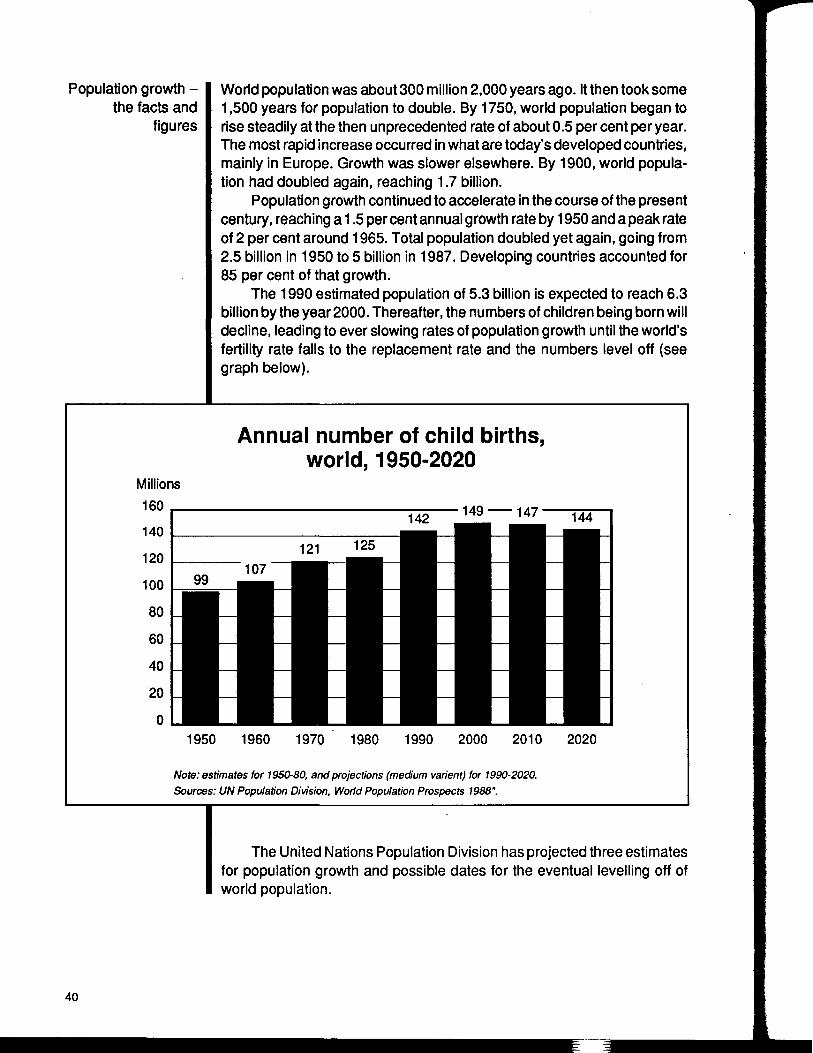
The 1990 estimated population of 5.3 billion is expected to reach 6.3billion by the year 2000. Thereafter, the numbers of children being born willdecline, leading to ever slowing rates of population growth until the world'sfertility rate falls to the replacement rate and the numbers level off (seegraph below).
Annual number of child births,world, 1950-2020
Millions160 __140120
100
80
60
40
20
0
142 149 147' 144
121 125
99107
I •I •
1 •
I I
• •• •I •• •I •• •• •
1950 1960 1970 1980 1990 2000 2010 2020
Note: estimates for 1950-80, and projections (medium varient) for 1990-2020.Sources: UN Population Division, World Population Prospects 1988".
The United Nations Population Division has projected three estimatesfor population growth and possible dates for the eventual levelling off ofworld population.
40
The medium variant assumes that the world will reach replacementfertility by the year 2035, in which case population will stablize at 10.2billion—double today's figure—towards the end of the twenty-first century.
If replacement fertility, however, is reached 30 years later, eventualworld population would be over 14 billion—the Population Division's highvariant. This figure would be attained only in the twenty-second century andwould be almost three times today's population.
In the low variant projection, if replacement fertility is achieved morequickly—by the year 2015—global population would level out at around 8billion, 6 billion lower than the high variant projection.
The synergism between child survival actions and effective family plan-ning programmes means that the two together can bring about populationstabilization at an earlier date and at a lower level than either acting alone.
The interaction ofchild survival and
fertility
Child survivalfactors that affect
fertility
A vigorous programme of child survival and family planning interven-tions pursued over the next 10 years and into the early years of the nextcentury would make an outcome between the lower and the mediumvariants more likely.
The role that child health interventions can play in reducing birth rates andthe role family planning interventions can play in reducing child mortalitydepend on the settings in which the interventions are applied.
The actual fertility consequences of a particular health interventiondepend not only on the type of intervention, but also on the prevalent family-building strategy and the nature and scope of family-planning programmesin the particular location in question. Specifically, the ready availability offamily-planning serviceswas found to intensify any fertility decline resultingfrom improvements in child survival in most settings by providing parentswith greater control over their fertility.
In order to enhance the fertility-reducing effects of child survivalimprovements, programme managers must, therefore, vary the mix ofprogrammatic components in an integrated child health/family-planningpolicy to suit local circumstances.
Child survival can influence fertility levels because of four closely relatedand interacting factors, identified as the physiological, replacement, insur-ance, and confidence factors.
The physiological factor arises when an infant dies which, more oftenthan not, means an end to breastfeeding and its inherent "natural contra-ceptive" effects.
41
Child survivalstrategies thatdirectly reduce
births
The replacement factor arises following the death of a young child,which prompts many couples to replace the loss of a child by a newpregnancy. Studies in Bangladesh show that an infant death reduces theaverage interval between births from more than three years to less thantwo. Families which experience the death of a child are much less likely touse any method of birth planning.
The insurance factor occurs when child death rates are high, sinceparents often insure against an anticipated loss by having more children.Not being aware of the statistical probability of their next child's living ordying, people tend to plan on the basis of the worst that could happen. Thisoften means they over-compensate, making the average family sizegreater than desired.
The confidence factor is the realization by parents that they have thepower to take important decisions to improve their own lives. This isprobably the most important prerequisite for the acceptance of familyplanning. Any change that reinforces parents' confidence in their ability toimprove their own circumstances, therefore, makes the acceptance offamily planning more likely. As almost all the main strategies of the childsurvival revolution offer parents more control, they all increase the likeli-hood of parents opting for smaller families.
Some of the most important means now available for reducing child deathsare also among the most powerful means of reducing births.
Exclusive breastfeeding has a demonstrably significant effect onfertility rates, and WHO studies show a clear relationship between the lengthof time a woman breastfeeds and birth intervals. In population groups witha contraceptive prevalence of less than 10 per cent, there is an almostlinear relationship between the proportion of mothers who breastfeed for 18months and birth intervals that are greater than 2.5 years.
Promoting knowledge about the importance of timing births andproviding the means to act on it is one of the most powerful child survivalstrategies and also reduces birth rates. Most child deaths happen tomothers who are younger than 18 or older than 35, or who have had morethan four children already, or who give birth less than two years after aprevious delivery. Children born in developing countries at the end of a birthinterval of less than two years are, on average, twice as likely to die ininfancy as are children born after a longer interval. According to somestudies, as many as a quarter of all infant deaths and a quarter of allmaternal deaths could be prevented by the well-informed timing of births(see chart on the following page).
Female empowerment, particularly in terms of education, not onlybenefits women, but also improves child health and survival. Educatedmothers are also more likely to opt for smaller families.
42
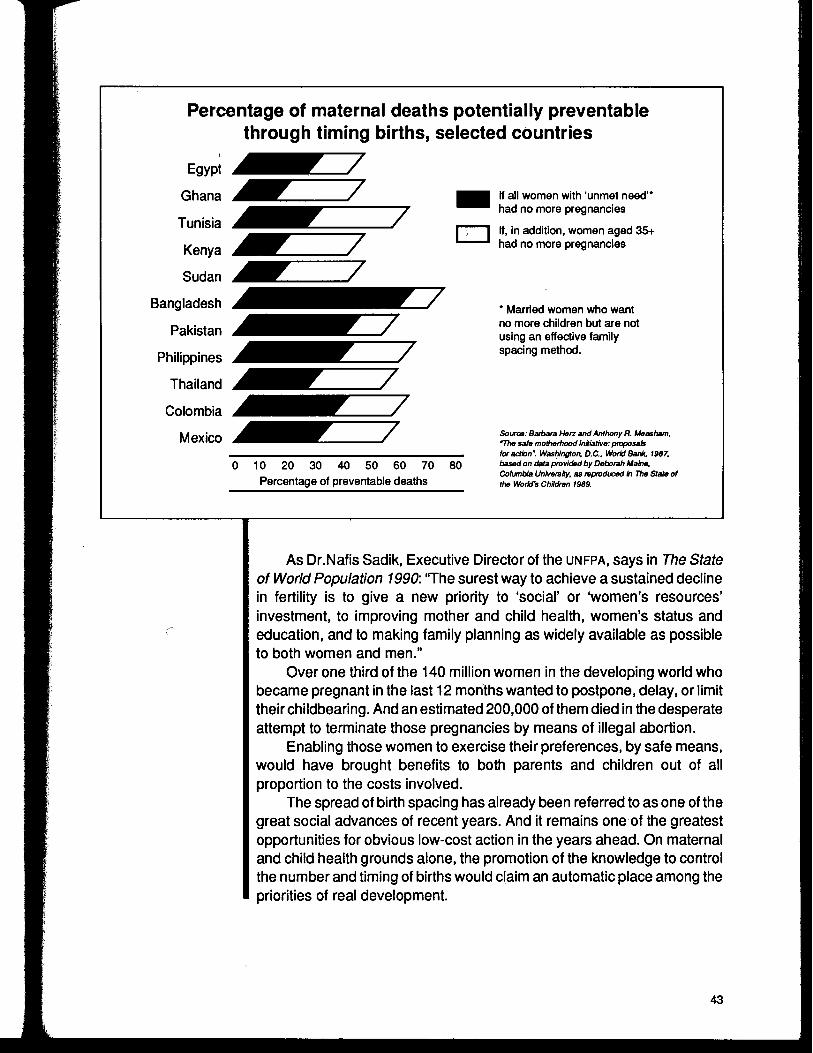
Percentage of maternal deaths potentially preventablethrough timing births, selected countries
EH
If all women with 'unmet need"had no more pregnancies
If, in addition, women aged 35+had no more pregnancies
* Married women who wantno more children but are notusing an effective familyspacing method.
10 20 30 40 50 60 70 80Percentage of preventable deaths
Source/ Barbara Hen and Anthony R. Measham,"The sate motherhood initiative: proposalsfraction: Washington. D.C.. World Bank. 1987.based on data provided by Deborah Maine,Columbia University, as reproduced In The Stale ofthe World's Children 1989.
As Dr.Nafis Sadik, Executive Director of the UNFPA, says in The Stateof World Population 1990: "The surest way to achieve a sustained declinein fertility is to give a new priority to 'social' or "women's resources'investment, to improving mother and child health, women's status andeducation, and to making family planning as widely available as possibleto both women and men."
Over one third of the 140 million women in the developing world whobecame pregnant in the last 12 months wanted to postpone, delay, or limittheir childbearing. And an estimated 200,000 of them died in the desperateattempt to terminate those pregnancies by means of illegal abortion.
Enabling those women to exercise their preferences, by safe means,would have brought benefits to both parents and children out of allproportion to the costs involved.
The spread of birth spacing has already been referred to as one of thegreat social advances of recent years. And it remains one of the greatestopportunities for obvious low-cost action in the years ahead. On maternaland child health grounds alone, the promotion of the knowledge to controlthe number and timing of births would claim an automatic place among thepriorities of real development.
43
Stabilizing thepopulation earlier
Further Reading
The fact that birth spacing also helps to lower rates of populationgrowth, through people themselves choosing to have fewer children, is anenormous dividend for the development effort. But the fundamental casefor making birth spacing available to all couples over the next five years isthat it gives people significantly more control over their own lives—and thatis what real development is about.
The synergism between this array of child survival actions and effectivefamily planning programmes means that the two together can bring aboutpopulation stabilization at an earlier date and at a lower level than eitheracting alone. The 1990s offer a remarkable opportunity to use this syner-gism—as many developing countries are now at the critical "point ofparental confidence" where further reductions in child deaths are likely tobring even greater reductions in births.
The experience of individual countries shows the power of thiscombination. If all countries were to achieve the same under-five deathrates and the same birth rates as Chile or Sri Lanka, for example, then theworld would see approximately 10 million fewer deaths each year—andapproximately 20 million fewer births.
The State of World Population 1990, Dr.Nafis Sadik, Executive Director,UNFPA.
44
PART TWO:
The health of mothers andchildren
45

-%
BLANK?AG£

Primary Health Care
In briefThe goal of health for all by the year 2000 was set more than 12 yearsago. The Primary Health Care (PHC) approach, adopted at the Alma-Ata conference In 1978, Is widely recognized as the key to effectivehealth programmesfor children and mothers, and two major Initiativestaken in the 1980s have strengthened prospects for success in the1990s.
The first is the Child Survival and Development Revolution(CSDR), which has been the leading edge for PHC development Inter-nationally. CSDR has saved millions of young lives, primarily throughthe promotion of Universal Child Immunization (uci) and oralrehydratlon therapy (ORT).
The second Is the Bamako Initiative, which was endorsed byHealth Ministers in sub-Saharan Africa In 1987. The Bamako InitiativeIs addressing the health care crisis in the region with a strategyfocused on, among other things, the decentralization of health ser-vices, community participation In PHC management, and the financ-ing of reliable and rational drug supply systems which are accessibleto all.
Despite the remarkable post war resurgence of economic and socialdevelopment in the 1950s and 1960s, it became obvious by the mid 1970sthat the gap in health status between the "haves" and the "have-nots" inmany countries was widening. The technical knowledge to ensure basichealth care for all existed, but health resources were grossly misallocatedtowards technically complex, urban-based medical care, while largegroups,who lived in rural and remote areas as well as in urban slums, remainedbeyond the reach of any permanent form of health care. It was against thisbackground that a global conference was hosted by WHO, UNICEF, and theUSSR at Alma-Ata in 1978.
47
Alma-Ata andprimary health care
The Alma-Ata conference adopted PHC as a strategy to achieve acceptablelevels of health for all. PHC was defined as "essential health care, based onpractical, scientifically sound, and socially acceptable methods and tech-nology made universally accessible to individuals and families in thecommunity through their full participation and at a cost that the communityand country can afford to maintain at every stage of their development ina spirit of self-reliance and self-determination."
The conference recommended that PHC include at least the following:1.Education concerning prevailing health problems and the methods ofidentifying, preventing, and controlling them; 2. Promotion of food supplyand proper nutrition, and adequate supply of safe water and basic sanita-tion; 3. Maternal and child health care, including family planning; 4.Immunization against the major infectious diseases; 5. Prevention andcontrol of locally endemic diseases; 6. Appropriate treatment of commondiseases; 7. Promotion of mental health; 8. Provision of essential drugs.
The Bamako Initiative responded to a decade of opportunities andconstraints since Alma-Ata, and Africa's especially difficult economicsituation, with a reemphasis on PHC focusing particularly on women andchildren.
Progress in PHC
Alma-Ata set the stage for a revolution in which the concepts of PHCand health for all would become an integral part of social development. TheWorld Health Assembly and the UNICEF Executive Board endorsed thestrategy of PHC in 1979, and in 1980 the United Nations General Assemblyadded its weightto the Alma-Ata resolution by linking Alma-Ata's objectivesto the goals of the Third Development Decade in the 1980s. United NationsMember States were urged to show their solidarity by making the neces-sary resources for PHC available to poorer nations in the spirit of nationaland community self-reliance.
The resolution at Alma-Ata recognized the critical role of communityparticipation, of intersectoral co-ordination of health care, and of the needto ensure universal coverage with the basic elements of PHC. These basicinterventions were to be directed principally towards the health needs ofyoung children and mothers in developing countries, in recognition of theirinordinately high morbidity and mortality rates.
The 12 years since Alma Ata have brought significant advances in theapplication of PHC in many countries—both developing and industrialized.As health care and social systems have reduced disparities and increasedtheir service coverage, morbidity and mortality rates due to infectious andparasitic diseases in particular, have declined significantly. Fertility rateshave also been reduced.
48
Effects ofeconomic crisis
The child survivaland developmentrevolution (CSDR )
Major successes in developing countries have occurred where therehas been the political will to provide services emphasizing universalcoverage, especially in the area of maternal and child health; where therehas been increased community participation and local autonomy in healthcare; and where women's education and a knowledge of health care havesignificantly transformed health behaviour in the home. Emphasis on PHChas also improved health management systems in areas where communi-ties share responsibility with formal government health authorities fordelivering health services.
Where achievements have fallen short, the main causes have beenpolitical, social, or administrative constraints on the decentralization ofpower. Another stumbling block has been economic decline and its impacton systems of financing for PHC.
While the importance of health care financing was recognized at Alma-Ata,discussion on this subject in the final report was rather inconclusive, in partbecause the effects on the world economy of the oil shocks of 1973 and1979 and the third world debt crisis had not fully registered among theinternational health leadership. It quickly became apparent, however, thatthe 1980s was a period of stagnation and recession affecting the poorestcountries most severely, particularly those of sub-Saharan Africa, SouthAsia, and Latin America.
The global economic crisis highlighted basic social and developmen-tal problems stemming from population growth, increasing urbanization,and environmental degradation, in these regions. In many countries, themotivation of health workers declined, and significant numbers migrated toricher countries. There was a virtual breakdown of health managementsystems, especially at the periphery. Supplies of basic medical require-ments became spasmodic and attendance at clinics fell.
The overall deterioration raised the alarm that the goals of health forall through PHC would not be achieved without further urgent internationalaction.
UNICEF'S response in the 1980s was to appeal for CSDR as the leading edgefor PHC development and the means of dealing directly with some majorchildhood diseases and the needs of pregnant women. It was recognizedthat modern communications had the potential to mobilize communitieseverywhere and empower families to become more involved in childsurvival. More effective communications were also seen as a means ofimproving intersectoral action for health.
There have been many achievements under the CSDR, especially inthe field of immunization, and in the use of ORT to prevent deaths from
49
Countries ineconomic and
social difficulties
The BamakoInitiative
diarrhoea! diseases. Successful advocacy for uci not only saved manythousands of lives, but served to raise national consciousness to improveand extend PHC.
Many lessons have been learned from this intensification of effortsunder CSDR. The great potential to harness community resources for socialgoals has been clearly demonstrated. And the relative ease with whichcoverage can be raised in countries with extensive health infrastructurehas highlighted the urgent need to extend the PHC system in countries withpoor infrastructure. The latter need to increase both the number andcapacity of their health workers and to make them more accessible tounderserved communities.
These lessons have profound implications in the 1990s for attainingthe goal of health for all by the year 2000. And the lessons are especiallyimportant for the countries of Africa, south Asia and Latin America that haveserious economic problems.
The health of children and mothers in sub-Saharan Africa is especiallyprecarious. Health care systems reach less than 40 per cent of thepopulation and a significant number of the systems need rehabilitation.There is a shortage of medical supplies and the volume of resourcesdirected to health is either stagnant or has declined in most countries.
Health care workers are very poorly paid and motivation is low. Themanagerial, supervisory, information, and training components of healthcare are quite weak in most countries, and new health problems such asAIDS and chloroquine-resistant malaria have increased the burden oncommunities and health care systems at large. At the same time, newattempts are under way to combat old scourges such as dracunculiasis,onchocerciasis, and micronutrient deficiences.
Faced with these challenges, many countries have demonstrated awill to improve their PHC systems. Political leaders throughout sub-SaharanAfrica have become sensitized to the special problems affecting childrenand women; to the seriousness of population issues; to environmentaldegradation; and to the need to restructure their economies and health andsocial systems in ways that fosteragenuine partnership between communitiesand government. A turning point in this regard was the Lusaka Declarationof 1985 which targeted 1986 as the Year of Immunization for the region.
In September 1987, African Health Ministers attending the 37th regionalmeeting of WHO in Bamako, Mali, addressed the need to redefine Africanhealth policies to meet the goal of health for all by the year 2000.
The Bamako Initiative responded to a decade of opportunities andconstraints since Alma-Ata, and Africa's especially difficult economic
50
Goals for the 1990s
Programmestrategies
Prospects for the1990s
situation, with a reemphasis on PHC focusing particularly on women andchildren. The strategy focused on community participation and the need tomake the fullest use of local, national, and other available resources. It aimsto achieve universal access to PHC through decentralized services andmanagement, from national to district and local levels. It also stressed: theimportance of community involvement in financing health care and servicesin partnership with the central government; community management of theresources generated; the critical importance of regular drug and medicalsupplies, and their rational use; and of ensuring the availability of essentialdrugs and services to the poorest members of society.
Many African countries have taken up this challenge to restructuretheir health systems. External support agencies need to recognize thesignificance of the Initiative and to offer timely assistance.
The principal goal of the 1990s is to reduce mortality among young childrenand mothers. To achieve that, families need ready access to functioningPHC systems and personnel who are competent to handle most of theirbasic needs and refer more serious problems to people with higherqualifications.
Health workers should always be on hand to "heal sometimes and tocomfort always." They should be able to deal effectively with common life-threatenting conditions and to prevent them by supporting protectivemeasures such as community health education, the provision of safe watersupply and sanitation, antenatal care, immunization, breastfeeding andsound weaning practices, and family planning.
These interventions help to establish the credibility of health workersin the community and to guarantee the achievement of their goals.
The strategy for the 1990s should be to emphasize the convergence ofinterventions to solve epidemiologically significant problems through thedevelopment and extension of PHC to all communities. There should beadvocacy for intensified political action; for the flow of resources from themore privileged to the less privileged; and for the empowerment of peopleand communities with the knowledge, information, and technical supportfor decision making. District-level roles must be strengthened to dealeffectively with a range of basic technical problems and surveillance, andto remain sensitive to community needs. Families and communities musthave sufficient health knowledge to take charge of their own needs and toadjust their behaviour as necessary. This last is perhaps the most criticalof all requirements for achieving the goal of health for all through PHC.
This last decade of the twentieth century offers the greatest potential inmodern times for the achievement of social objectives. The virtual end of
51

Further reading
the Cold War has opened the door to genuine collaboration among allnations to deal with major social problems, including the health needs of thepoorest nations.
At the heart of this fundamental change in global relations is the desirefor all nations and communities to be in charge of their own destinies—adesire totally in tune with PHC.
In the field of science and technology, there has never been such avariety of effective interventions that can be applied to the majority of healthproblems. The PHC strategy is the means for integrating these applicationsand technologies for the benefit of all. What is required now is the politicalcommitment to make this happen in every country.
Alma-Ata 1978: Primary Health Care. Report of the International Confer-ence on Primary Health Care, Alma-Ata, USSR, September 6-12, 1978.WHO. Geneva. 1978.
"Annotated Bibliography on Community Financing for Local Health Ser-vices," by Pierre E. Mandl, UNICEF Staff Working Paper No. 3, November,1988.
52
Halving maternal mortality
In briefThe Goal: Between 1990 and the year 2000, reduction of thematernal mortality rate (MMR) by one half.
The health of Infants and children and the health of mothers areIntimately linked. Every year, more than half a million women dieduring pregnancy or childbirth, the vast majority of them In develop-ing countries, doomed by poverty and social Inequity. The conditionsthat take such a toll on women affect their infants and children also.Women debilitated by anaemia, malnutrition, and disease bear in-fants ill-prepared to withstand the traumas of unskilled deliveries,infections, and low birth weight. The toll In mothers' lives is matchedby high Infant mortality rates (IMRS). And infants who survive inherita legacy of III health.
The problem, however, isfarfrom intractable: the MMR drops whenmothers are monitored during pregnancy and those at particular riskof complication—between 5 per cent and 10 per cent of women—areIdentified and given skilled obstetric care; when communities offermothers the services of trained birth attendants and accessiblefacilities; when family planning advice is available and the problemsof women's social inequity are addressed.
More than 500,000 women die each year as a result of pregnancy orchildbirth, all but 6,000 of them in developing countries. In the developingworld overall, nearly 1 in every 200 pregnancies results in the death of themother, a MMR of 450 per 100,000 live births. In those cases where thereis no care or only unskilled care, as many as 1 in every 75 pregnanciesresults in the death of the mother.
Among certain subgroups, the risk of maternal death is particularlyhigh. Young adolescents in Africa and Asia receiving no prenatal care maystand a 5 per cent chance of dying. An African woman's lifetime risk ofdying from pregnancy or childbirth may be 1 chance in 15. A South Asian
53
Underlying causes
woman may have a 1 in 18 chance of dying. By comparison, the risk forwomen in industrialized countries, and even in a few developing countriesin East Asia, has been reduced to the point where pregnant women carryonly one two-hundredth to one five-hundredth that of women in lessdeveloped countries.
Maternal health is intimately linked with infant health and the risks ofinfant mortality. In the least advantaged countries, one half of infant deathsoccur during the first month of life, linked to such factors as neonataltetanus, low birth weight, prematurity, lack of oxygen, birth trauma, andinfections—conditions also associated with poverty and high maternalmortality rates.
Furthermore, among infants who survive birth, the ill health and poornutrition of their mothers, and the poor quality of health care they receiveforeshadow a childhood of disease, nutritional deficiencies, and equallypoor health care.
Without skilled prenatal and delivery care, even well-nourished andeducated women will continue to run a high risk of pregnancy-relateddeath. In the industrialized countries, maternal mortality remained be-tween 200 and 300 per 100,000 live births through the 1930s, and did notfall to fewer than 10 per 100,000 until quality obstetric care became widelyavailable, including improved standards for managing labour and delivery,better handling of complications, the use of antibiotics and blood transfu-sions, and the skilled performance of Caesarian section.
However, the reduction of maternal deaths need not be the exclusiveprivilege of the developed world. In Sri Lanka, where annual maternalmortality between 1950 and 1955 was 550 per 100,000, the rate washalved to 260 per 100,000 peryearfrom 1960 to 1965, and by 1975 to 1980was down to 80.
If the current MMRS remain unchanged, by the year 2000 there will be600,000 maternal deaths per year. Yet, if Sri Lanka's example can befollowed, that figure could be reduced to 300,000 or less.
The risk of a maternal death begins with the health and nutrition of thefuture mother during childhood. A childhood legacy of short stature, lowbody-weight, and anaemia, coupled with early marriage and childbearingbefore social and biological maturity, are major contributors to maternaldeath. The geographic and cultural inaccessibility of family planningservices and the erosion of traditional mechanisms of child spacing allcontribute to the mother's risk.
Only slightly more than half of all deliveries in the developing world(excluding China) are supervised by a trained birth attendant, and no morethan 30 per cent take place in an institutional setting. Even when womenhave physical access to essential and emergency obstetric care, they may
54
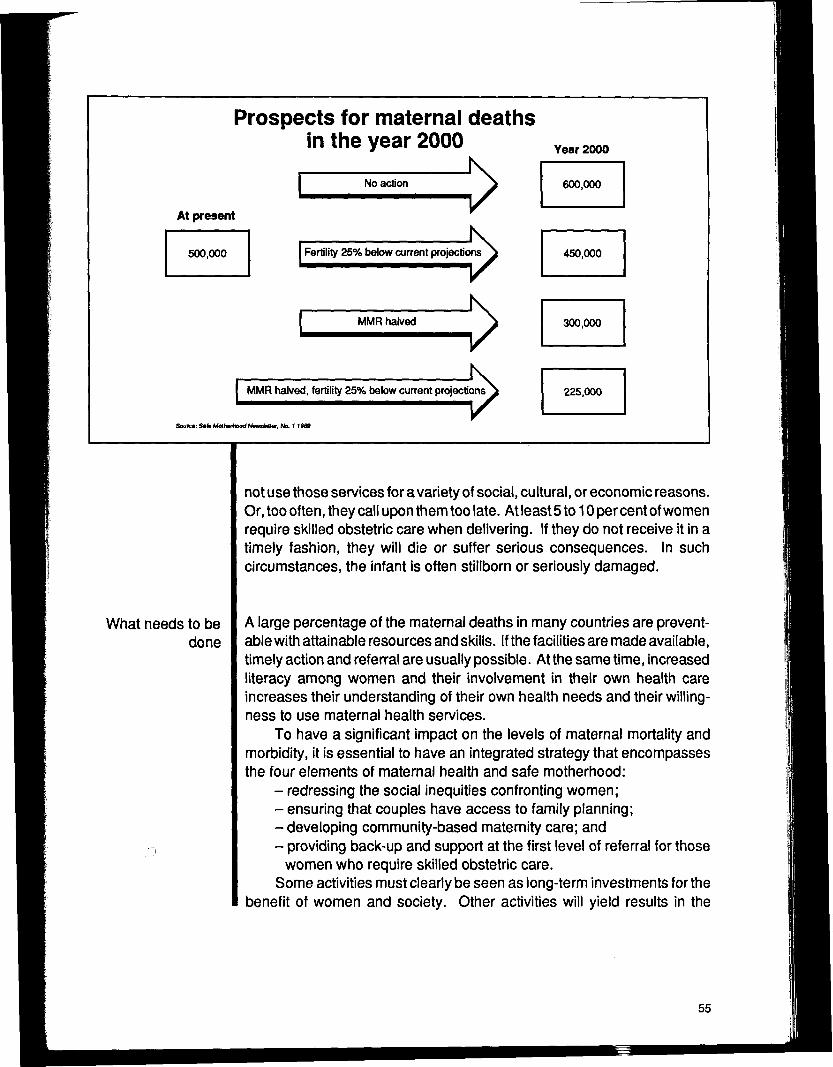
Prospects for maternal deathsin the year 2000 Year2000
No action
At present
Fertility 25% below current projections
MMR halved
0»>
MMR halved, fertility 25% below current projections
Sn/ro:S«feM<*feri»o<fMew»lWter. No. t IM9
ons\
V
What needs to bedone
not use those services for a variety of social, cultural, or economic reasons.Or, too often, they call upon them too late. At least 5 to 10 percent of womenrequire skilled obstetric care when delivering. If they do not receive it in atimely fashion, they will die or suffer serious consequences. In suchcircumstances, the infant is often stillborn or seriously damaged.
A large percentage of the maternal deaths in many countries are prevent-able with attainable resources and skills. If the facilities are made available,timely action and referral are usually possible. At the same time, increasedliteracy among women and their involvement in their own health careincreases their understanding of their own health needs and their willing-ness to use maternal health services.
To have a significant impact on the levels of maternal mortality andmorbidity, it is essential to have an integrated strategy that encompassesthe four elements of maternal health and safe motherhood:
- redressing the social inequities confronting women;- ensuring that couples have access to family planning;- developing community-based maternity care; and- providing back-up and support at the first level of referral for those
women who require skilled obstetric care.Some activities must clearly be seen as long-term investments for the
benefit of women and society. Other activities will yield results in the
55
medium term, paying dividends in the next generation on the investmentsmade in the next few years. Others may produce results almost from thevery beginning.
In the long term, the combination of education, improvement in thesocial status of women, and full access to family planning information andservices would have a large effect on maternal mortality by decreasing therisk attributable to unwanted pregnancy and child-bearing during adoles-cence or at older ages among women who have already given birth severaltimes. Such fertility variables may account for between 15 and 30 per centof maternal mortality.
Governments can adopt the theme that "safe motherhood" and "childsurvival and development" are two sides of the same coin. They canendorse the fourfold strategy of the global movement for maternal healthand safe motherhood: equity, primary health care, essential obstetric carefor those at risk, and family planning.
In the short term, however, efforts to improve community-based familyplanning, prenatal care, and the training of traditional birth attendants(TBAS) would reduce maternal mortality by 8 to 22 per cent, i.e. to 350 per100,000. This estimate is based on the expected effect of partiallydecreasing the infection component of maternal mortality and providingfamily planning to avoid a proportion of the abortion deaths.
TBAS can be taught simple techniques of identifying women withsevere anaemia as well as increased risk of haemorrhage or eclampsia,which together account for 40 to 60 per cent of maternal deaths. Thesecases, however, require referral to a health centre or district hospital for theneeded care.
By strengthening the district level to provide such obstetric functionsas anaesthesia, blood for transfusions, vacuum extraction, and Caesariansections, and if peripheral care were linked to and supervised from thatlevel, maternal mortality could be reduced by 50 to 85 per cent, i.e. to 64per 100,000 live births.
One major remaining obstacle to reducing maternal deaths is thelogistical problem of transporting a woman in need of skilled care. A risk-conscious approach can, in part, overcome that obstacle, since manywomen who require higher-level care can be identified before they go intolabour, and, depending on the degree of risk anticipated, can be sent to adistrict hospital or maternity waiting home in advance of their expecteddelivery dates. Communities can be involved in constructing and maintain-ing such maternity waiting homes.
The impact of such community-based interventions is far greater onneonatal health than on maternal health. Cleanliness during delivery and
56
Cost of halvingmaternal deaths
Research needs
immunization of all women of child-bearing age with tetanus toxoid havebeen shown to reduce neonatal tetanus by 90 per cent to 95 per cent(virtually 100 per cent with immunization). The training of TBAS has reducedperinatal infant deaths from trauma, asphyxia, and sepsis by 40 per centto 60 per cent.
According to World Bank estimates, the cost of an integrated approach tomaternal health care is $1.50 per capita per year, in addition to the cost ofchild health care and essential-drugs programmes. The maternal carecomponent includes community-based prenatal care and family planning,health centres, and the strengthening of first-level referral for essentialobstetric care. The latter would involve minimal upgrading and equippingof district hospitals, serving communities of from 100,000 to 200,000persons.
In many countries the resources for such measures, whether fromnational, bilateral, international, or non-governmental sources, alreadyexist or are attainable. The problem has been that the resources inquestion have neither been targeted to an integrated strategy nor allocatedon the basis of risk.
Estimates can only be made on a country basis for the capital costs ofup-grading and equipping the necessary facilities and of strengtheningtraining programmes for midwives and other health workers.
WHO, World Bank, UNFPA, UNDP, and UNICEF have all made policycommitments to maternal health and safe motherhood. Limited funds havebeen made available by various multilateral and bilateral agencies andfoundations for global-level research, training, and advocacy on thisquestion. In a few countries, the agencies concerned have given priorityto collaborating in and providing funding to programme development formaternal health.
Operational and health systems research on the organization of maternalhealth services is a major priority if maternal health services are to beimproved.
Operational research issues can be approached from three angles:
• The organization and management of services. Examples ofresearch needed include examination of integrated programmesand community participation; studies of relative cost-effectivenessand acceptability of different combinations of maternal health,nutrition, and family planning interventions; studies on how socialsupports affect women's work, nutrition, and energy expenditure;research into distributing maternal health technologies, such asiron folate and antimalarials.
57
Contribution ofthis goal to
sustainable nationaldevelopment
What world leaderscan do to help
achieve this goal
Further reading
Development and adaptation of specific technologies. Priori-ties would include research into such topics as plasma substitutesfor replacing blood loss in shock; the home-based mother's record(HBMR) in self-identification and referral of women at high risk ofcomplications during pregnancy ordelivery; the use of the partographto identify the need for referral or operative intervention; anddevices for detecting severe anemia.
Case and programme management of specific conditions.Topics to be studied would include the use of routine antibiotics incases of prolonged labour or premature rupture of membranes andthe training of TBAS and primary health care (PHC) workers in the useof a simple screening tool for hypertensive disease of pregnancy.
Maternal mortality is an indicator of social inequity and discriminationagainst women. It is an impediment to development and contributes toinfant and child mortality. While many actions that could lower maternaldeath rates fall within the realm of the health sector, all sectors of societybear a responsibility for creating a social climate in which women's needsare accorded a high priority and in which simple but crucial preventivemeasures are no longer withheld through neglect.
Governments can adopt the theme that "safe motherhood" and "childsurvival and development" are two sides of the same coin. They canendorse the fourfold strategy of the global movement for maternal healthand safe motherhood: equity, PHC, essential obstetric care for those at risk,and family planning. Leaders can commit themselves to take decisivesteps to improve maternal health within their countries, drawing upon allfunding sources — national, bilateral and international — and all sectorsconcerned.
Preventing Maternal Deaths. Erica Royston and Sue Armstrong, eds. WHO.Geneva. 1989."Childbearing, Health and Social Priorities: A Survey of 22,774 Consecu-tive Hospital Births in Zaria, Northern Nigeria," by Kelsey A. Harrison, inBritish Journal of Obstetrics & Gynaecology, Vol.92, suppl. No. 5, Oct.1985, pp.1-119.
The Safe Motherhood Initiative: Prospects for Action, by Barbara Herz andAnthony R. Measham. World Bank. Washington. 1987.
58
-52-
BLANKpAGi£

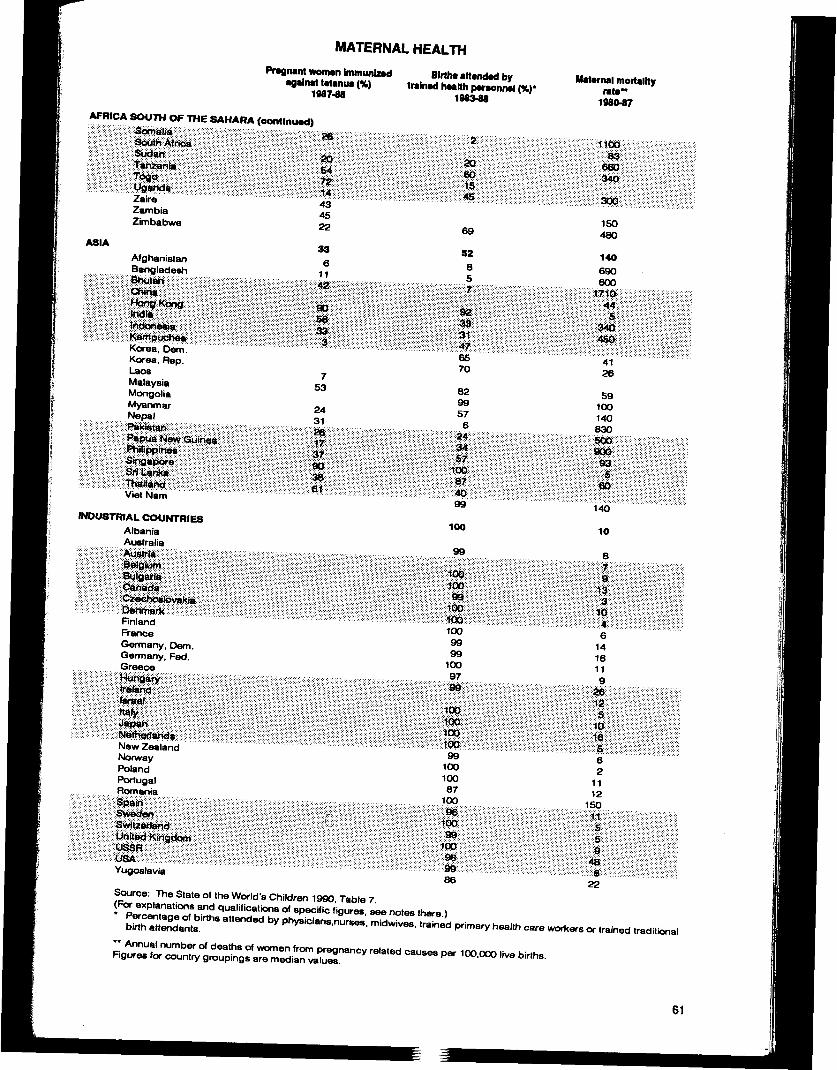
MATERNAL HEALTH
Pregnant woman Immunized•gain* tetanus (%)
196748
Birth* attended bytrained health personnel (%)•
1983-88
Maternal mortalityrata"
1980-87
LATIN AMERICA ft CARIBBEANM^i^f^^iSii^iii^illllilii liiiiiil:iilii:!:!:;:!i:Bl||l::iisililiilii Piiiimm^^ff:!&^^^^mmittmlviii^
CubaDominican Rep.EcuadorEl SalvadorGuatemalaGuyana
8:;;:;:;:;:;:;:;:!:lllllllii pii BIII BiS***S;388^^iiiiili iiiffllll iliSiip;:;:;;:;!;!;!; ^llllliiiiii§ iliillllllilllli
ParaguayPeruTrinidad & TobagoUruguayVenezuela
MIDDLE EAST ft NORTH AFRICAwmmtm#ii$/%^lliiiililill...................5S:S5:::?;:!i:ii:g;S:::Ji' |:!|j |i|S^*(pisIllllllllliliiiiilli'''"'""''"''''''''''''"'"'iSKssssssssliiiDl il;:;:IPliillMil
LebanonLibyan Arab JamairiyaMoroccoOmanSaudi ArabiaSyria
llllll:lill;ii!lll:p:p:;:PS;:; |(iii|pIllilllllii lPliiiiijiii:: :::-:-:-::: : : : : : ^ ^<9H|:|:|:;:|:;:[:|:|:W:|:;
ii:::ii:iii:::;i;|i;::;i!;;: j ;;i3B§ii;
AFRICA SOUTH OF THE SAHARAAngolaBeninBotswana
i|il|||iif | :; lll; Bi;|||pJ||||S ||E| ^ ||| ffi||'•PSPlPpJiiifriiiiiiiiisiliiii iilll Pijiiili Biii iiii iii iiisIP liii i llls ililiiS!
Coted'ivoireEthiopiaGabonGhanaGuineaKenya
m^^mWaiHii^^^^^^^^^mmMmm^iimiiiiiiii^^mmmmmtmii^mmmiti^jm::mmMtl^iimimmmmmijfi^^immiMauritiusMozambiqueNamibiaNigerNigeriaRwandaSenegalSierra Leone
27
iiiimmHim
87S
191857
*BpsiiiiIHiilipliHi
648
6013
34
nipHH!liifiiiiii
12337OSO40
iiii iiilll
iill25197
61:ss*:;15;s;is llispliiililSCpili?l"""46"'
760
0 162
illiil:ii::;:sii;i;sisisillHill
"""65"43
820432450
57
:>::36;:;:liPs:96§1111
5727353496
iJPIS|i:»i|sillll:;lpHi2244989782
64mmiiiii!ilmmiimmm76296O7437
i;:;6|:;SlHii;i;ipiliiilli
154577
siaa??;:;:;:!
iiiiiiiiii'"'so'""""
14924O2528mmm
;:;s|p;ss:;i;::i|ll
•;mm8528
4740225025
72
•mimm
3474
19O7O
110
W®mMmipiiliiilllpl;i!:| lli38088543859
210
H PIiiii;
8O3OO
280WimWiM
420
250||8i|s;
IllililimmiilelllslSall
10OO
17O
s:Z4o::sHiHi;
100
42080021O600450
60
MATERNAL HEALTHPregnant women immunized
against tetanus (%)1987-88
AFRICA SOUTH OF THE SAHARA (continued)
Wiis^^^i^imiiMiiiiii9iM^^^j^^^^^^^^^^^^:
W$injj$iiii^$^M^^^^®^Wjjiji®i$$^ii$!^^ii!!i^i$&W&i$iijiii$®!MK$®iiS$i$®
Zajre • • - • • • •••.....-.•.•.•.--,.,,,.,.,«,.:,.:,,,:«-:,,:
ZambiaZimbabwe
ASIA
AfghanistanBangladesh
Wi-KM^&^i^fimmmimfiiiiiiiiiilpiiiiiliWiMmii^iij^mmimi|l!illl||ipj!:|||;:;:;il:!||llliP;::ilJ»Sp|i|i:i||il;:;iS;ft;:s;:;:|i|;:|:lSiii | ||ll|:|:
Korea, bern'." """"""Korea, Rep.LaosMalaysiaMongoliaMyanmarNepal
|||li|Hli|f|tgi ii;::::;;;;;:i:;;;:s:ig:;:;:;mmmiU^ii^j(j^i^0(M^^ii^^^msMiMmiiiM:i^ii^^m9?imIWiiPliiiliiiliSJ llii;!;
VietNam
INDUSTRIAL COUNTRIESAlbaniaAustralia
mliiiiii^^iiiMiimffiiiiiliii
lift
iiiiHlgfpi**I434522
611fill
lipIliS:i:Wisii
753
2431
i8P;siiii;iiiiiiiiHii|iliil
|liiiiis| |iillllf^f
-fe»l-
BUAJKPAQ£
Immunization goals in the 1990s
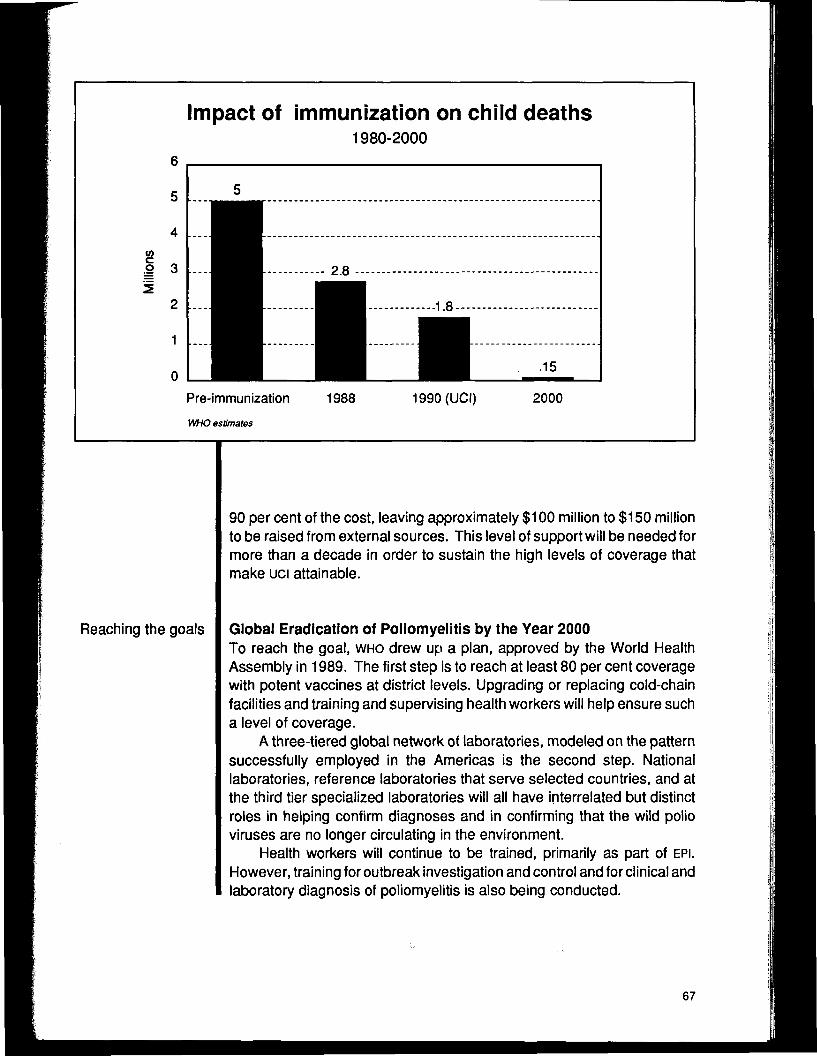
In briefNearly 3 million children in developing countries have been dyingeach year from measles, tuberculosis, whooping cough, tetanus,polio, and diphtheria, all diseases easily prevented by immunization.When Universal Child Immunization (uci) is attained, hopefully by theend of 1990, this toll will be reduced to 1.8 million annual child deaths.
The extraordinary success of uci can be extended even further,reducing the annual death toll to 150,000 by achieving the followinggoals by the year 2000:
• Maintenance of a high level of immunization coverage (at least90 per cent of children under one year of age) against diphthe-ria, pertussis, tetanus, measles, poliomyelitis, tuberculosis,and against tetanus for women of childbearing age.
• Global eradication of poliomyelitis by the year 2000.• Elimination of neonatal tetanus by 1995.• Reduction by 95 per cent in measles deaths and reduction by
90 per cent of measles cases compared to pre-immunizationlevels by 1995, as a major step toward the global eradicationof measles in the longer run.
In the 1970s, smallpox, a disease that had decimated and disfigured entirepopulations across the centuries, was finally eradicated from the earth,through a comprehensive campaign of global immunization.
For the first time, the world united to wipe out a fearsome disease andsix other major killers-measles, tuberculosis, whooping cough, tetanus,polio, and diphtheria-no longer seemed invincible. Encouraged by theunprecedented success of the global campaign against smallpox, WHOestablished the Expanded Programme on Immunization (EPI) to extend theprotection against preventable diseases widely available to children in thedeveloped world to children all over the globe.
63
Universal childimmunization
Still, in the mid-1980s, more than three million children, primarily indeveloping countries, were still dying annually from those same diseases.The interlocking problems of poverty and malnutrition complicate thesolution. Yet the diseases and the enormous toll they take on the mostvulnerable children, families, and nations of the world, can all easily beprevented by vaccination:
• Nearly two million children have been dying each year from suchcomplications of measles as pneumonia, diarrhoea, and ence-phalitis. One immunization at nine months of age (or as early as atsix months, with a newly developed vaccine) can prevent measles.
• Neonatal tetanus kills over three quarters of a million babies in thedeveloping world each year. Unsterile practices at birth cause thenearly always fatal infection of the umbilical cord. Mothers who areimmunized against tetanus either during pregnancy or prior tobecoming pregnant pass immunity to the disease on to theirnewborns. An infant can later receive lasting immunity throughcombined diphtheria/pertussis/tetanus (DPT) vaccinations around6,10, and 14 weeks of age.
• Whooping cough, or pertussis, has been claiming the lives of some600,000 young children each year. It can be prevented by threedoses of the DPT vaccine around 6,10, and 14 weeks of age.
• About 200,000 children contract poliomyelitis each year and 20,000die from it. It can be prevented by three doses of a vaccine givenduring the first year of life.
• Two million children underfive years of age get tuberculosis and anestimated 30,000 die from it. Immunization is achieved with onedose of BCG (anti-tuberculosis) vaccine given after birth.
In 1977, three years after EPI was launched, the World Health Assemblychallenged the countries of the world to achieve uci by the year 1990. Thegoal eventually set was coverage of 80 per cent of the world's children bytheir first birthday with one dose of BCG, three doses of DPT, three doses ofpolio, and one dose of measles vaccines. The ministers of health in Africaset a regional target of 75 per cent, and China set 85 per cent as their levelof coverage.
Many considered such levels of immunization unattainable in 1977.Between 1984 and 1988, however, a great international groundswellpushed the world substantially closer to realizing the goal. In 1985, theUNICEF Executive Board and the United Nations General Assembly af-firmed full support to the goal of uci 1990. They were joined by 74 govern-ments and more than 400 voluntary organizations who pledged to support
64
uci 1990 in commemoration of the fortieth anniversary of the UnitedNations.
Out of these commitments grew high-level international politicalsupport and co-operation between ministries of health, voluntary organiza-tions, and other diverse talents, all necessary to marshal! the requiredresources both nationally and internationally to complete national coldchains and delivery systems and to generate sufficient understanding andmotivation by the public to seek out immunization for their children.
By the end of 1989, BCG coverage for tuberculosis had reached 81 per cent;75 per cent of children received the third dose of polio vaccine; 73 per centreceived their third DFT dose. Coverage against measles was at 71 per cent
The immunizationchallenge for 1990s
By 1987, most countries had established accelerated immunizationprogrammes and were using a variety of strategies to improve immunizationcoverage. National mass campaigns were conducted to promote immu-nization, involving religious leaders, teachers, and other community leadersin advocating immunization. National immunization days, with intensivepublicity and mediasupport, protected millions of children. And meanwhile,health services made immunization a regular component of children'scontacts with the health system. In some countries, immunization becamea prerequisite for admission to schools or for other government services.
A breakthrough-reducing the number of children's lives lost to diseasespreventable by immunization to 150,000-is possible by the year 2000.
The World Health Assembly and the UNICEF Executive Board, target-ing the diseases that exact the heaviest price in children's lives, haveendorsed the following immunization goals to be achieved during thedecade of the 1990s.
• Global eradication of polio by the year 2000;• Elimination of neonatal tetanus by 1995;• Reduction by 95 percent in measles deaths and reduction by 90 per
cent of measles cases in 1995, compared with pre-immunizationlevels as a major step to the global eradication of measles in thelonger run.
If the uci goal of covering 80 per cent of children by the end of 1990is reached, an estimated 1.8 million children will still die annually from thesix major diseases. Achieving the goals above in addition to the goal of uci,however, can reduce the devastating loss each year to 150,000 deaths,and free all children from disabilities due to polio, by the year 2000.
65
uci's success althe end of 1989
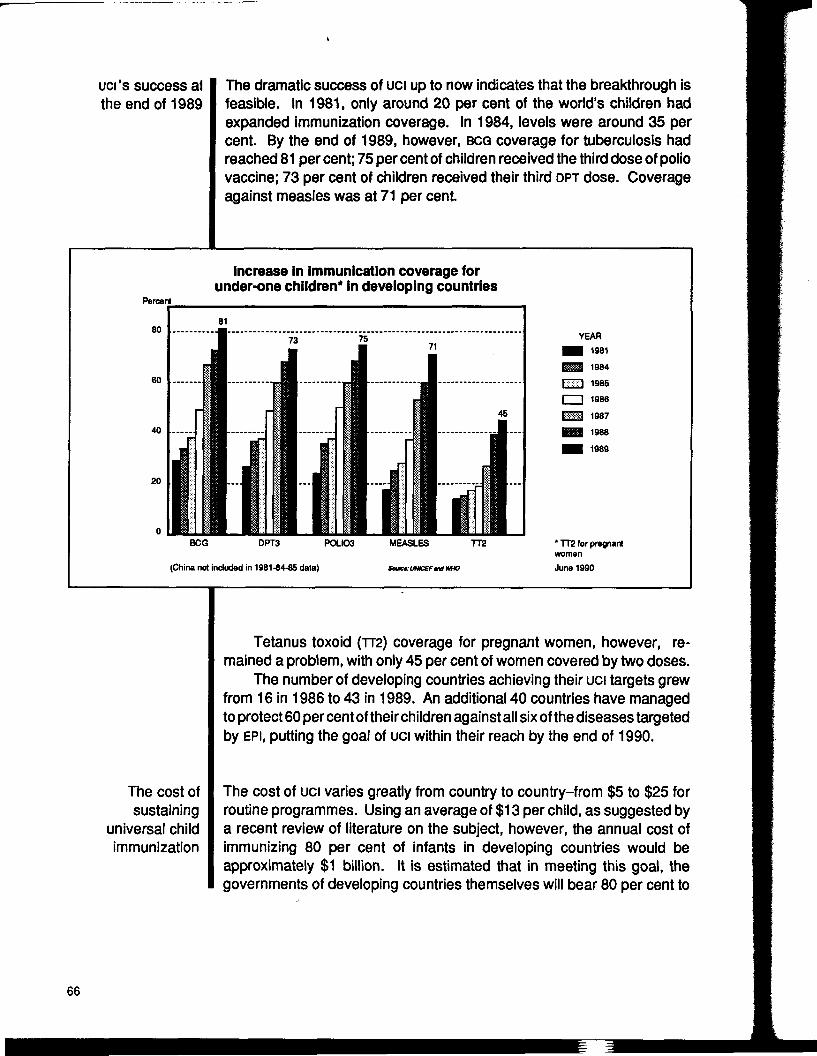
The dramatic success of uci up to now indicates that the breakthrough isfeasible. In 1981, only around 20 per cent of the world's children hadexpanded immunization coverage. In 1984, levels were around 35 percent. By the end of 1989, however, BCG coverage for tuberculosis hadreached 81 per cent; 75 per cent of children received the third dose of poliovaccine; 73 per cent of children received their third DPT dose. Coverageagainst measles was at 71 per cent.
Percent
Increase in immunication coverage forunder-one children* in developing countries
40 .....
20
YEAR• 1981
1984Islxl 1985I——I 1986
E ^ 198719881989
BCG DPT3 POLIO3
(China not included in 1981-84-85 data)
MEASLES TT2
SoacfUHKfFtnlWHO
' TT2 for pregnantwomenJune 1990
The cost ofsustaining
universal childimmunization
Tetanus toxoid (TT2) coverage for pregnant women, however, re-mained a problem, with only 45 per cent of women covered by two doses.
The number of developing countries achieving their uci targets grewfrom 16 in 1986 to 43 in 1989. An additional 40 countries have managedto protect 60 per cent of their children against all six of the diseases targetedby EPI, putting the goal of uci within their reach by the end of 1990.
The cost of uci varies greatly from country to country-from $5 to $25 forroutine programmes. Using an average of $13 per child, as suggested bya recent review of literature on the subject, however, the annual cost ofimmunizing 80 per cent of infants in developing countries would beapproximately $1 billion. It is estimated that in meeting this goal, thegovernments of developing countries themselves will bear 80 per cent to
66
Impact of immunization on child deaths1980-2000
6
5
8.2 3
2
1
0Pre-immunizationWHO estimates
1988 1990(UCI) 2000
Reaching the goals
90 per cent of the cost, leaving approximately $100 million to $150 millionto be raised from external sources. This level of support will be needed formore than a decade in order to sustain the high levels of coverage thatmake uci attainable.
Global Eradication of Poliomyelitis by the Year 2000To reach the goal, WHO drew up a plan, approved by the World HealthAssembly in 1989. The first step is to reach at least 80 per cent coveragewith potent vaccines at district levels. Upgrading or replacing cold-chainfacilities and training and supervising health workers will help ensure sucha level of coverage.
A three-tiered global network of laboratories, modeled on the patternsuccessfully employed in the Americas is the second step. Nationallaboratories, reference laboratories that serve selected countries, and atthe third tier specialized laboratories will all have interrelated but distinctroles in helping confirm diagnoses and in confirming that the wild polioviruses are no longer circulating in the environment.
Health workers will continue to be trained, primarily as part of EPI.However, training for outbreak investigation and control and for clinical andlaboratory diagnosis of poliomyelitis is also being conducted.
67
Societies are continuing to mobilize to immunize children as part of theuci drive. And national medical establishments are being asked to committheir prestige and political influence to the effort, so government supportremains firm until the last case of polio is diagnosed.
Research and development are improving polio vaccines in terms offormulation, efficacy with fewer doses, and heat stability. Better diagnostictests are being created, and efforts are being made to improve manage-ment efficiency of the eradication effort.
And finally, health workers and families are encouraged to make earlyrehabilitation efforts for children who contract the disease. These effortscan prevent much of the need for surgical treatment. Better guidelines onwhich children require surgical treatment are also being developed, andbraces are being improved.
Elimination of Neonatal Tetanus by 1995Although tetanus will never be fully eradicated-tetanus spores can surviveindefinitely in the environment without a human host-neonatal tetanus hasvirtually disappeared from industrial countries because of aseptic deliverypractices.
In the developing world, however, conditions during births are oftenunsanitary, attendants are frequently untrained, and in many cultures, theumbilical stump is actually treated with materials containing the tetanusorganisms.
The training of birth attendants to ensure clean hands and deliverysurfaces and proper care of the umbilical cord can all reduce the risk ofneonatal tetanus. But only by vaccinating all women who are pregnant orlikely to become pregnant against tetanus will neonatal tetanus be elimi-nated.
In the next five years, the focus will be on ensuring that all pregnantwomen receive two doses of tetanus toxoid prior to delivery. This, togetherwith the emphasis on clean delivery, will hopefully eliminate neonataltetanus during the next five years. By also ensuring that girls receive threedoses of DPT during the first year of life, one dose when they enter school,and two additional doses before they leave school, they and their futurechildren will be protected.
The promotion of tetanus toxoid immunization is part of the SafeMotherhood Initiative established in 1987 by WHO, the World Bank, andUNFPA, and supported by many other organizations.
Reduction by 95 Per Cent in Measles Deaths and Reduction by 90 PerCent of Measles Cases Compared to Pre-lmmunlzatlon Levels by1995 - a Major Step Toward the Global Eradication of Measles In theLonger Run.
68
Research prioritiesfor the 1990s: a
children's vaccine
Because measles is highly infectious, it is difficult to control, even inindustrial countries with many years of high levels of coverage. Indeveloping countries, where health services are often marginal, childrenfrequently malnourished, and living conditions overcrowded and impover-ished, control is much harder. Children are also infected at younger ages,sometimes before they are even nine months old.
Recent research has shown a high titre Edmonston-Zagreb strain ofvaccine to be effective in children as young as six months of age. The EPIGlobal Advisory Group recommended in October 1989 that this vaccine beadministered to children at six months of age in countries and areas whereearly measles is a problem. The vaccine, however, is not yet widelyavailable.
In addition to high levels of immunization coverage in all communitiesof all countries at the earliest age possible, measles surveillance will beemphasized to find cases and control epidemics on a timely basis.
The countries of the English-speaking Caribbean have adopted thegoal of measles elimination by 1995. Their strategy is to immunize allchildren between 12 months and 15 years of age by May 1991, regardlessof their previous immunization status.
A major research and development effort aimed at producing improvedvaccines more closely approaching the "ideal"-a single dose multi-antigenoral vaccine that is stable at ambient temperatures and produces life-longimmunity-is under discussion. The effort would be called, simply, theChildren's Vaccine Project. In addition to the current EPI diseases, it wouldseek to develop protection against pneumonia, hepatitis, influenza,mumps, chickenpox, and diarrhoea due to Rotavirus. Regional variantswould also be sought in order to provide protection to children againsttyphoid, cholera, leprosy, shigella, and dengue.
A heat-stable vaccine would eliminate the need for, and cost of, whatis now known as the "cold chain," the vaccine distribution system thatrequires refrigerators, refrigerated transport, skilled maintenance, and awhole series of logistic measures. If any link in this chain fails, the vaccinecan be rendered useless. An oral vaccine would further eliminate the needfor, and thus the expense and complications of, needles, which requiresterilization and also have the potential for transmitting disease if steriliza-tion is not properly performed.
Reducing the number of required doses-ideally to a single dose-would substantially reduce costs, solve the problem of dropouts, and helpbring disease control and eradication goals within our grasp.
Basic and applied research must be carried out, field efficacy trialsmust be conducted, and production and marketing problems solved beforeall this can become a reality. However, much of the basic research is
69
Further reading
already-or nearly-in hand. What remains to be undertaken is an intensiveinternational collaboration to bring together the elements of modernscience in this effort for children. It would be a very fitting gift to the childrenof the twenty-first century if Heads of State assembled at the World Summitfor Children were to pledge themselves and their research establishmentsto making this a reality within the decade.
Protecting the World's Children: A Call for Action. Report on the FourthInternational Child Survival Conference, Bangkok, Thailand, March 1-3,1990. Available from UNICEF.
Assignment Children: Universal Child Immunization by 1990. UNICEF.Geneva. 1985.
70
~^ > JT^ ^
P- > 2. 7^
-A t
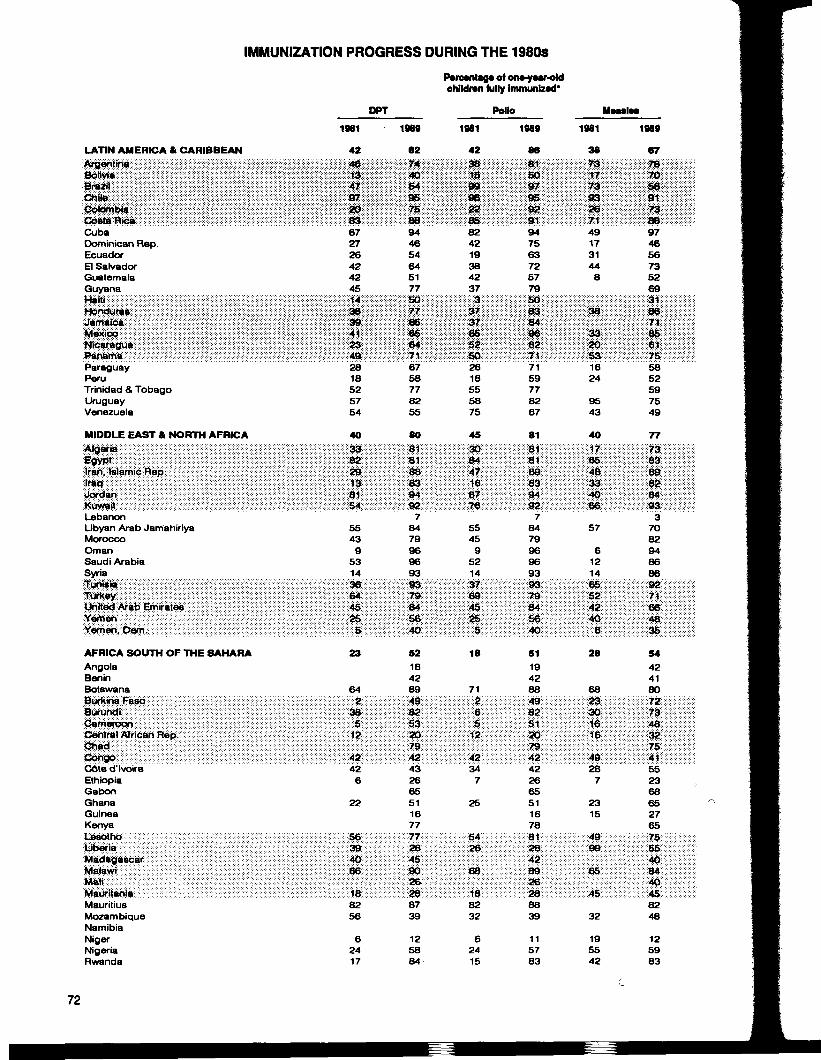
IMMUNIZATION PROGRESS DURING THE 1980SPercentage of one-yeer-oldchildren fully Immunized*
DPT Polio
LATIN AMERICA & CARIBBEANMg&M&mmmm®mmmmmmm
jM^mmmmmmmmmmmmmmmm^^^mmmmmmmmmmmm®mmmmm
CubaDominican Rep.EcuadorEl SalvadorGuatemalaGuyanamwmmmmmmmmmmmmmmmmmm
JAtft^mmmmmmmmmmmmmmmmmmm^Mii^mmmmmmmmmmmmmmmi^^mmmmmmmmmmmm-mmmmmParaguayPeruTrinidad & TobagoUruguayVenezuela
MIDDLE EAST & NORTH AFRICAm&iK^mmmmmmmmmmmmmm:;<rtfii;:;<ilS^$«!i!iil; ^l^iiiiiiirmg^;)S !»llJil;;;;;«^LebanonLibyan Arab JamahiriyaMoroccoOmanSaudi ArabiaSyriaIli fii;;;;;;;;^Mii^iMimiifimwmmsmmm'•ty'iitfnii&n' '-''•''•' '^mmKOwm®mmmmmmmmAFRICA SOUTH OF THE SAHARAAngolaBeninBotswanaWM^;tt&mmmmmmmm®mmmmm^ximmmmmmmmmmmmmmmrnmrnrnmimmmmmmmm^^l^^i^^^^^j^m^^^^M®®^®®®®®m®m®®^^®mj.^iii^mMm®m®®®m®mM®W®nCote d'lvoireEthiopiaGabonGhanaGuineaKenya•K6WM:mmmmmmmmm>mmmmmm.mm^mmmmmmmmiiiiiim.Wim&^mmmmmmmmmmmmmiMmm^mmmmmmmmmm®mmm;mj^mmmmmmmmmmmmmmmmmmmiifti^mtitmmm-mmmm^mmmmmiMauritiusMozambiqueNamibiaNigerNigeriaRwanda
1981
42
mmmmmmm^mm
mmmmmmmm^iimmmmmmmmmm&mm672726424245
mmmmmmmmmmmmmmmmmmim®mmmmmmmmm®mm<mmmmmmmmmmwmimmmmmmmmmmmmmmmmmmmmmmm2818525754
40mmmmmm^mmmy^Ktmm:mmmmmmmmmmmm:mmmmmmmmmmismmmmmmmmmmmmmmmmmmmmmmmSimm:::::::::::-:::::;::::::::::::::::::::K:::::::::::::::::::: !?:::::;::::::::::
55439
5314
mmmmmmm^mmmmmmmmmitmmmmmmmm^mim::::::i^:':;::;:::;:::::::::;:::::;:::::':'::::::::::::::::;:: §:::::::::::;:;::
mmmmmmwzmm23
64
mmmmmmmmmmmimiiimmmmmmmmmmmmmmmmmrnmmmxmi^
426
22
^mmmmmmmi&smmmWmmMmiQ&zmmrnmmmmmwifm*mmmmmmmm;mmmmmmmtf&m
8256
62417
1989
62
mmm*wmmmmmrnm944654645177
iiiisoimmwiimmmmmmm,m.m\mmM
6758778255
80mmmmsssgsSBis;:SssssSiBSf:::;B::Ji?4s«3:J;sssss:s^:gmams&s
78479969693
mmm*mmitmS?ss;wH84:ssssssjjse;;::::lSi:;SK;:40::?
52184289
SSSSSJ49-SiSisisag*?s:*s*:5:553:si:;:l|s;;;:3iC»:;s•mmmzif
432665511677
s:;Ssss;S77;s?'S.ssss28":?H;:;asss:45s:;mmm*~iwmm*mmm*
8739
125884
1981
42mmmmmmmmmmmmmmmmmmmmmmmmmfSmmmmmmmmmmmmmiiiimmm
824219384237mmmmmmmmmwmmmmmmmmmmmm
mmmmmmmmmmmi^mmm
2618555875
45
mmmmj&i^mvfwmmm&mmmmmmmmmmmmmmmmmmm
55459
5214
mmmmmmmmmmmmmmmmmm3®mmsimmmmmmmmmmmmsmmm
18
71
mmmmmmsmmMmmmmmmmmmmmmmmmmimmmm-
347
25
mmrnmstmmm-mmmmmm®mmmmmmmmmmmmmmm
8232
62415
1989
86rnmmmmti&mmmmWimmmmmmmmmmmm
1981
38mmmmmmmmmmMmmmmmmmiiimmmmmmmmmm
1989
67
mmmmmmm^^mmmmmmmmmmmmimmmmmmmmmmmmmmmmmmmmmmmm947563725779
mimm®mmmmmmmmmmmmmmmmmm7159778267
81mmmmmmmmmmmmmmmm^mfmm>mmmmi,mm#zmm
78479969693
®m»sm®mmmmmmmmm.mmmmm
51194288mmmmm:mmmmmmmmmmmmm
mmvmmm•mmtKtmmm
422665511678
mmstmmmmmmmmm®matm®'mmWmmmmmmmfmmeetmm
8839
115783
491731448
: :-SS:>::::::::::::-:-:-: : :::::::::::::?xxx%ijii?;™ffSSV.mmfimmmmm(
mmmmmrnmmmmmmmmmmmMmmmm.1624
9543
40
mmmmmm974656735269mmmmm
mmmmmmmmMmmmmmmmmmmm
SB52597549
77
mmmmmmmmmm&mmm.mmmmmmmmmmmmm
57
61214
mmmmm:mmmmmmmmmmsmmmmmmmmmmmmmmmtmmmm
28
68mmmmm®m®mmmmmmmmmmm.mmmi&mmmmmmmmmm.
287
2315
mmmmmsfmmmmmm®mi^mmmmmmmmmmmmmm4smmmm
32
195542
mmmmm:mi&mmmmmmmmmmmmmmmm
37082948686
:-:-:-:->:-j(j!(*:::v:-:-:-:-:-:-:-:-:-x.::::::::.:.SWf::::;::::::::.:::.:.:.:::::
mmmmmmmmmmmmm;m^mmm54424180mwmmmmmmmmm[m®m®mmmmsgmmmmmmsmmmm
mmMmmmm552368652765•mfswmmmmmmmmmm;mmmmmgjfmmmmm4ommmm:mflgmm®8248
125983
72

IMMUNIZATION PROGRESS DURING THE 1980s
AFf"<JA S°UTH ,?T ™E HARA (continue,
DPT
i|ii!!!||!|8Siiiiiiiiiiiij ^iilPtlig|l|!|!iiW$$$liii$i8$38®$Ji^^Mii$t^^^^w§:Togo • • • • • - • • • - . . • •--••-.•.•.•.•.•.•.•.•.•,,:-.v,:vv.>-,,,,,,,,,,,::::::::::x:
UgandaZaireZambiaZimbabwe
ASIA^i^^is^^^^^^^^^^^^^^^^^^^^e^^^^^^^^^^^^^^M^^^^^m^-^^^^^f^^^^^^;iplliiiiil ^Wjfijfitjjiiiti^mtiztt^msZ^ii^m^^ffiif.!(ttSliiii::|llll||l:|;llllll||Illl|;|Indonesia ' • • • • • • • • • • • • • • • ••••"••••••••••••••••••••• ••••-™<: • wwxxftfixwKampucheaKorea, Dem.Korea, Rep.LaosMalaysiaMongoliaiSjjiijjjiiijii'il^^^^lffi^^iif^^^^iii^Ij$ifi8|!iii ^iii^ff^i^^ii^^^^^^^^^^^^lii^^i^iii^i^^^m^^Ks^im^^^m^m^^iiiiiiiiiiiiiii^^Sr i Lanka • • • • • • • • • • • • • • • • • • • • • •••••••••™™..........;.:.™.^.^^itff^fff^ffff.ThailandViel Nam
INDUSTRIAL COUNTRIES^^^^^^M^^^^f^^m^mfmmiKf^ffffff^^^^jii^m^MXw^isM^^S^^^X^jj^&tiiitiitti^^^jjif^^JiK^^^^^j^^^^^^^^^^^lijiliiiijiiiCanada " "' """ • ' • ' • ' • ' • ' • ' • ' • ' • ' • ' ' • • '•'•'••"™-"™-:-"»«>::.->>:CzechoslovakiaDenmarkFinlandFranceGermany, Dem.^i^^^^if;^^ig}i^mim^mmm^ffi^^l^jS^^iiim^^^^iS^^^^^^^K^^^^i^i^^Si^^^^^^M^^^^^^^a^Maa^Siii^^a^f^^^^^M^i^^MffWfMMim^^^mA^^i^f^;^^WiKSiX9H^i^^^^^^^^^^^Japan ' " " " • • • • • " " ' • • • • • • • • • • • • • • • • • • • • • • • - > • • • • : : ••••••••••m-Vfffi^ymy-w.
NetherlandsNew ZealandNorwayPoland^^j/^ifi^M^mmmmmfmmm^mmwiti^i^^;:::^ijijiif:^fiiiijii^^^^^^^^i^i^Mis'^i^^iii^^^Siffiiiiiiii^^^^^ijiiii^^M9^^ii^^^Miii^^^^^i^^liij^^W^^^fi^^^^^Siiii^KUnited kingdom " " " • • • • • • • •^••-•••••••••••••'••••••••••••••^•-•^•mx'iif^;-^USSRUSAYugoslavia
Source: UNICEF and WHO.•Fully immunized » DPT and Polio, three doses each; Measles, one doseFigures (or country groupings are weighted mean values.
1981
illlllii!!!l!l!illllll
99
184439
48Illllllssisssspi
•IIISSSfSgSHS!wm$$m
52617
5499
mmmiliiisilip!siiSlis;s:il!i?|il
4552
81
PHI5siaS:l;s:;
9585927980
liwsiis::v::::tiikt:::::::;:::::::::>:::>:«t>":::::;:::o:>
|S99:S|SUiUlP::iiiiiiisisSSSJifsS'
9772
95
s»iisii;iillil|'44"""""95
90
1989
s;s::*sssKs:67iimmmimmtmmmfymmmmm.:.:.;.;.;.;.•.-.•-•--.•:•:•:•:•:>?*':•:.;•s*ss!?SS:s!:;:;8B;S;
5560388379
81illllliimm^mmiwmammSSSSSSSiSif?:*;• ; ;• ; .•••••••• •••:•:•:•:•:•""; ••:••.
75225786217269
•:-:-:>:•:•:•:•:•;••••. •••••.v^.i. •.-.•.•.:SSH:H:;:;::::::4:7:;:H:;:;:
iliisiill;:;lililillill;™;:;S:;§::SH8H s
898O68
65
liiiilllliil.Illlllli!!!:Mii&iiZmmsmmymWmttjj&Wif:
859994949694
:mm:t:mm&;li:S;i:;:;;iSil;:!Illlllii
8397708098
mmmimmv®&iiiim&iiimimwmmmm
70799790
ParcmtUg* of ora-ycar-oldchildren fully immunized'
Polio1981
•illSSiSSBjjSSi
iiiliig8
187738
32
tiliii::-:-™mfj:f^f-".™;™::!::::-:-:-:
Illllll
iiillill'^•--•''^••^^^'.jsss;?;?:®;:;:;
51627
6199
illlilmtiggmimim
"49"""22
OS
liiiiiiilllllllijSSSH™::?:™
9597908O90
wmiiiilSlii;:;st6:-;-;:::;:;:;siM:;l:l
97
95
llllll
liiiiii'71'""""95
95
1989
wmm:mmamw%mzi8&
5560388179
lillilmmm^miiimms;s:™-;;;;Ka«is-:'
78225887227269S;S:SSHSsS4jj;ss:
sssss lpss:::x:::-:-:-:-:-::::::"f:ra::::-:ilIl:;5;?3S:::;;llll;sii ||?mm®j$m""""" ""87"""":'X
8068
68
iii» i;liiiiii::::::;::::::::::::::: T::-::::::::::S:EES;:!S9SSisS;:;.HSwsSaSwSwi ff-'-'-K-i-iWawS:-.:-.:::
8598
100959797•;s?;:KS9psgffi
Illlliill;:::::::.x-:-:-.-:yQ:;::::;x:x>
::::::::::::::::;:93;:-::y::::::::
SlMi9597848099
ilii lSili:liipilll::::::::::::y''-'|TJis'::;x::::;:::;:v¥:™-:«:/*»::™m™::;:;« 1;:;:;:;:?P?;:il;li;li;i
87809790
UBMIM1981
BB••:•:•:•:•:•••• ••••••'.•'.•j.-'.-:-:-:-'.-::i:i:i:i:::i:io;-::x?; i:i:i:i:mmmmi
4722232156
N/A
Illllll
iisiiilii1I11IBI
3157
Illlillliiiiiiiiililiiiil
00wmmm.IllllllJiSSiSOsSisSSS
95
70
95llilii!!IBIll'iiii
93
65
SiiimHI
• 52 • • • • • • • • • • • • • • • " • •959695
1989
sssssissag:;;isssssspg•:•:•;•:•••;•::•:•:•:•:•:•:*»:•:•:•
iliiisi?iis:sssssisss;s*ss:4|iis;liiiiii
6260408O75
75
Wiimmilllllii:immmm:-:-:::-:;:;:::::::'i5Q-:::-:-SWiSWsS!?::;:;;::
68205896205058
wmwmmimmmIlillllii:::::::::::::::::::x ::;:::-:;:;
816371
76
•111iillim®mm.••••••••••••••.•-•?*?*-;-:-:-:-:'y
859882874199
mmmmi:Wimim
'^mamm7393608796
wmmmmmmm-jSS IsSSi;
76799892
73
\^•~vr-\
^e§uJ^5<O
-
Control of diarrhoeal diseases
In briefThe Goal: Reduction by 50 per cent, compared with 1990levels, In the deaths due to diarrhoea In children under theage of five years and a 25 per cent reduction In the diarrhoeaIncidence rate.Diarrhoeal diseases are the primary cause of infant and child
mortality in most countries, responsible for over a quarter of all childdeaths world-wide each year.
Yet oral rehydration therapy (ORT)—a simple and Inexpensivemethod of replacing fluids and minerals lost during an episode ofdiarrhoea—could prevent up to two thirds of these deaths.
If cases of diarrhoea are correctly managed—by combining ORTwith continued feeding, increased liquid intake, and the appropriateuse of drugs and intravenous therapy—up to 95 per cent of thesedeaths could be prevented. More and more countries have thecapacity to solve the problem. The challenge now Is to put the controlof these devastating but manageable diseases at the top of everynational political agenda.
On average, children under five years of age in the developing world sufferfrom two to three episodes of diarrhoea a year, and as many as 150 childrenout of every 1,000 in developing nations may die from diarrhoea in the firsttwo years of life. In all, acute diarrhoeal diseases cause an estimated 1.3billion bouts of illness and around 4 million deaths each year in childrenunder five.
In addition, repeated attacks of diarrhoea are a major cause ofmalnutrition and faltering height and weight gain. In a debilitating cycle, anundernourished child can suffer increasingly severe, and possibly morefrequent, attacks of diarrhoea, leading to greater exposure to life-threaten-ing dehydration.
75
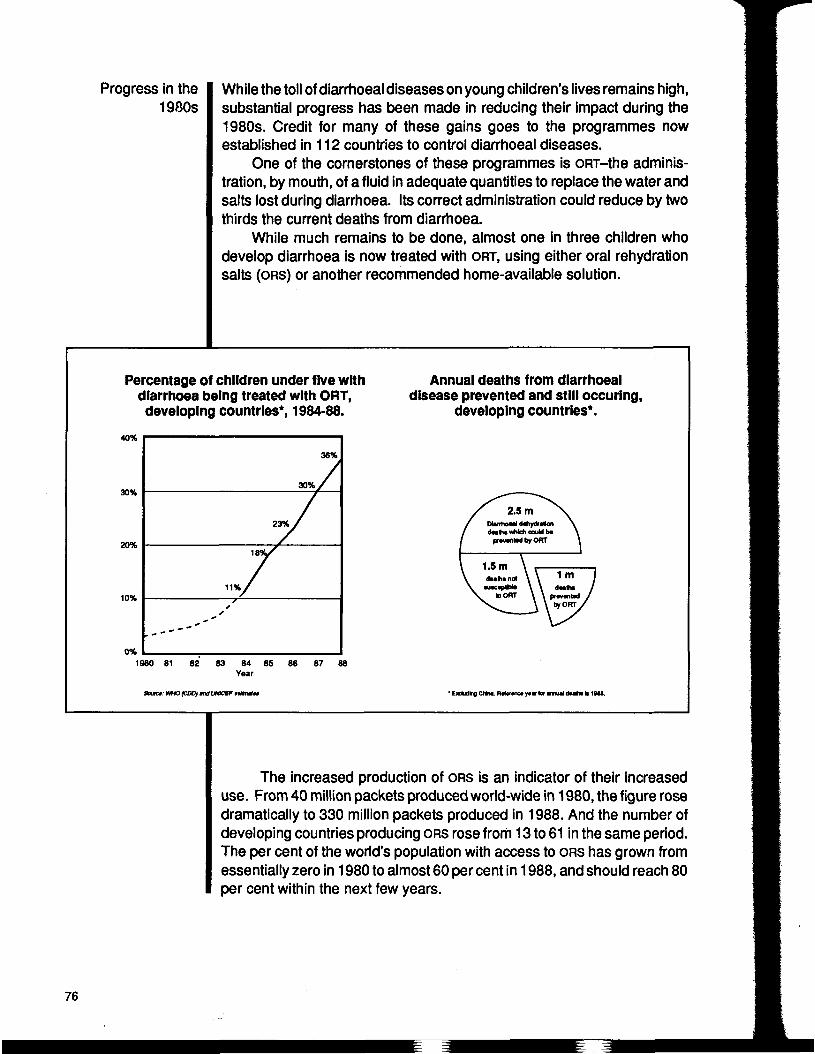
Progress in the1980s
While the toll of diarrhoea! diseases on young children's lives remains high,substantial progress has been made in reducing their impact during the1980s. Credit for many of these gains goes to the programmes nowestablished in 112 countries to control diarrhoea! diseases.
One of the cornerstones of these programmes is ORT-the adminis-tration, by mouth, of a fluid in adequate quantities to replace the water andsalts lost during diarrhoea. Its correct administration could reduce by twothirds the current deaths from diarrhoea.
While much remains to be done, almost one in three children whodevelop diarrhoea is now treated with ORT, using either oral rehydrationsalts (ORS) or another recommended home-available solution.
Percentage of children under five withdiarrhoea being treated with ORT,developing countries*, 1984-88.
Annual deaths from diarrhoea!disease prevented and still occuring,
developing countries*.40%
30%
20%
10%
0%
36%
30%,
11%
1980 81 82 83 84 85 86 87Year
Soam: WHO (CDOJ «x> UWCEF MttMM • OcUhg CNna. nmwio »•« tor nun deatn k 1944.
The increased production of ORS is an indicator of their increaseduse. From 40 million packets produced world-wide in 1980, the figure rosedramatically to 330 million packets produced in 1988. And the number ofdeveloping countries producing ORS rose from 13 to 61 in the same period.The per cent of the world's population with access to ORS has grown fromessentially zero in 1980 to almost 60 per cent in 1988, and should reach 80per cent within the next few years.
76
Managing carecorrectly
Yet diarrhoea in many areas of the world continues to be treatedinappropriately with antidiarrhoeals and antibiotics. In fact, an estimated$1 billion is spent annually on remedies that in many cases are useless oractually harmful.
Thirty per cent or more of admissions to children's hospitals or wardsare due to diarrhoea. A study sponsored by WHO in 14 countries, however,demonstrated that hospital admissions dropped 61 per cent in countrieswhere ORT was effectively promoted.
The correct care of diarrhoea! disease begins at home. At the onset ofdiarrhoea, mothers can immediately begin to administer increased amountsof whatever fluids are available, for example rice water, clear soup, orplainwater.
At the same time, the mother should continue to breastfeed if the childis not yet weaned, and/or continue feeding the child a regular diet in smalleramounts, and usually at more frequent intervals.
The key danger in an episode of diarrhoea is that the child will becomedehydrated. An essential part of correct care for diarrhoea! disease,therefore, is to ensure that mothers can recognize signs of dehydration. Ifa child shows signs of dehydration or if the child does not appear to begetting better, the mother should immediately administer ORS (if available)and seek care from a qualified provider outside the home.
ORS are necessary once dehydration occurs because most fluidsavailable in the home are unable to correct the water and salt imbalancesthat occur in dehydration.
In a very small percentage of cases, when dehydration is severe,intravenous therapy may be necessary. Furthermore, in instances whereblood or mucus are observed in the stool (for example, dysentery orshigella) antibiotics may be appropriate.
Even when dehydration occurs and children are treated in healthcenters with intravenous and antibiotic therapy, breastfeeding and otherfeeding should continue. And after an episode of diarrhoea, carefulnourishment is also crucial to ensure adequate catch-up growth.
About 10 per cent of all cases of childhood diarrhoea last over twoweeks and are classified as persistent. Correct treatment of persistentdiarrhoea will become increasingly important during the 1990s. While only3 per cent to 20 per cent of acute diarrhoea! episodes become persistent,up to 50 per cent of all diarrhoea-associated deaths occur during episodesof persistent diarrhoea.
Research is continuing, but current recommendations on treatingpersistent diarrhoea include appropriate feeding, vitamin supplementa-tion, ORT, and in some cases, the use of antimicrobials and other medicines.
77
Mobilizing support The treatment of childhood diarrhoea in the home and in health facilitiescan be improved in this decade if countries make commitments to thefollowing:
• Increasing the involvement of parents and communities in thehousehold management of diarrhoea. Control of diarrhoea! diseasesmust be promoted as a parent-centered initiative, with parentsdirectly affecting the health and survival of their children. Parents'actions must, of course, be backed up by correct and easilyaccessible health care at all levels, especially that closest to thecommunity.
A study sponsored by the World Health Organization in 14 countriesdemonstrated that hospital admissions dropped 61 per cent in countrieswhere oral rehydration therapy was effectively promoted.
Preventingdiarrhoea
Mobilizing all levels of society to support and promote ORT as thepreferred treatment for childhood diarrhoea. Strengthening thesocial and health-related infrastructures necessary for its wide-spread use must also be given priority attention. Training of healthstaff and other providers of care is an urgent priority.
Continuing advocacy among health professionals to adopt ORT astheir first line treatment for childhood diarrhoea. The resistance ofdoctors and other health personnel to changing existing attitudesand practices has been a formidable obstacle to the effectivepromotion of ORT.
Improving methods for measuring the mortality and morbidity levelsassociated with diarrhoea. ORT use rates should be closely moni-tored; changes in practices known to affect the incidence ofdiarrhoea—including breastfeeding and hygiene practices—alsoneed further development.
The causes of diarrhoea vary from country to country and within countriesas well, but research thus far suggests that the following interventions canhelp reduce substantially the incidence of childhood diarrhoea:
• Helping mothers improve infantfeeding practices, especially breast-feeding and weaning practices;
• Ensuring that water supplies are safe and easily accessible andthat communities use them correctly;
78

Research prioritiesfor the decade
Calculating thecosts
Improving domestic and personal hygiene practices;Promoting measles immunization.
Since persistent diarrhoea is responsible for as many as one of every twodiarrhoea-related deaths, research is needed to identify risk factors for it,as well as to determine the usefulness of advice on nutrition, antimicrobials(oral gentamicin, for example), vitamin supplementation, and other carestrategies.
Comparisons need to be made of the effects of cereal-based vs.glucose-based ORS in young children with noncholera or low-purgingdiarrhoeas, in infants below four months of age, and in severely malnour-ished children.
There is concern as to how cereal-based home rehydration solutionsmay affect food intake and nutritional status during diarrhoea. The impactof cereal-based home rehydration solutions on clinically evident dehydra-tion also needs to be evaluated.
And the success of interventions to prevent diarrhoea, including waysto change behaviours, needs to be examined.
To rehydrate a child in a health facility using ORS costs only about $1. Atthat rate, to cover all diarrhoea! episodes with prepackaged ORS in healthfacilities would cost about $1.3 billion.
Perhaps even more telling are the costs of not addressing the problem:
• Since an average child under five years old has between two andthree episodes of diarrhoea each year, if each episode lastsbetween four and seven days, the child will spend somewherebetween 8 and 21 days each year sick or debilitated by diarrhoea!disease. In Ghana, for example, it is estimated that 14,470 healthydays of life per 1,000 people are lost each year to diarrhoea-relatedailments.
• Not only do children experience illness during these periods, butfamilies (and particularly mothers) are constrained from fully par-ticipating in the social and economic life of their communities. Forfamilies already living on the brink of survival, these constraints canprove devastating.
• While national experience varies widely, it is estimated that globally$1 billion per year is spent on useless or harmful treatments fordiarrhoea. This figure can be expected to increase in the 1990s.
79
Further reading
The toll of diarrhoea! diseases on young children's lives remains high.Fortunately, the solutions are clear and well-defined. Furthermore, thecapacity of most countries to implement them is steadily growing. Thechallenge is to put the control of diarrhoea! diseases at the top of everynational political agenda.
A Simple Solution: How Oral Rehydration Is Averting Child Death FromDiarrhoea! Dehydration, by Glen Williams. New York. UNICEF. 1987.
The Treatment and Prevention of Acute Diarrhoea: Practical Guidelines.Geneva. WHO. 1989.
80

ORAL REHYDRATION THERAPY USE RATES, 1987*
LATIN AMERICA ft CARIBBEAN 30 AFRICA SOUTH OF THE SAHARA (continued)?!S:S;S;5;5;S;:;?;:;:::iilSi|i8r
mM^{f^^^:^^miiim^^m•i^m^^'l^^i^is^mmSl^^^mmM:mmm^mm:mmmmmmm:m
CubaDominican Rep.EcuadorEl SalvadorGuatemalaGuyana
mmmm>mmMmmmmmmm®iiiijj^mmmiiiiiiiiiimmimmii^m^i^ii^mmmi^^;g::i;;;i;i;i::::::::S::::::;::iMe::kriOT::::§;:::;S^;?i;i;i;i;Si;l;l;i;i;l;l;:i^f^ff^ff^
• • • • • • • • • • • • • • • • • • • Paraguay' • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • • •PeruTrinidad & TobagoUruguayVenezuela
MIDDLE EAST & NORTH AFRICAM8;:::;S£?:S;:::;Aii£iEi ^liliiillli lll y'Wil lilllllll i'l'iilillll;:mm-m^tr^w^&m^mm^m^:3::;;;;;:;:;;;;;:;:;:;:;:;:;;;:;::;;:;|:;:;;il;i;lil;;Si Slil
LebanonLibyan Arab JamahiriyaMoroccoOmanSaudi ArabiaSyria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
i;!;l;i;i;£;i'^f^'f^^^iii^imS^^mi^^^^l^'m^!M^^^ft:i^::^^^^M!M!Miil;|ll||l rrt ll|llil;;|i;;;;:;;i|llllli;iiii;i;ii;i;:;i;:;ii:l;;;J;i!
AFRICA SOUTH OF THE SAHARAAngolaBeninBotswanaBurkina Faso
!!!;:!; p:;:::; ^:;:;S;:;:i:;:;;;;;i;:;::: ii(! i«:.:H.;SP
CongoCote d'lvoire
iiiiiiiissiisSssiSis?:?;;:;l:iidi:l:s:ss;:;::s;:iliisSOlSiSHSSS
M$t8:i;l$ii!illilllll;i........^.... . . . . . . . . .
4124261710
-:•;•:-;•:•:•:•*»£•:••.•:-:•:-:•:••.•:•:•:•:•*:>o::.::::::3:V::::::::::::::::::::::::-
lss66;:lll:Sl;illlilelillll1:1111111111:x"::x->:>*>!*»:>xBx:x:x:>::::::::::::::::X7Mi:::::::;:;:::v:::::::;:SSiiH'Sw™:?:?:?:?;;,:,:,:,:|™:,:,:,:,,,:,:
18605628
25
iiiiiiiiiiiiii iiiiiiiii jiSiiiiiS;
;;i:;:;?; il:sssl;:;:;:iSi;iii
101044194331iii iiiii
ssSgsHb'ssssssS:-::::::x:::::::x ::x;:::::::::::::::>:
ll:;:;ll:iiil:-:':-:-:-:-:-:-:-:-is-:-:-:-:-:-:-:-:':-:-:-:-.•.•.-.-.•.•.•.•.•.•o- .•.•.-.•.•.•.•.•.•.•.>.-illijllll
1512264615
is?s!3b:illlllismiiiiismismmmmm^mmm
24
||ll||||||| |ij||||lll|||||||I|W:MMf:M^K^^^ii!ii!i B:::B;:;4s;B;H;5;S?HiH:H:H4
mmmmmmmm^m^mm^mm<ms$$z$3®$i%$$$m m^mmmmW!^MM!w^i$^^i^:!:^ W£Wt^$3i$%
LiberiaMadagascarMalawiMaliMauritaniaMauritius
wmmmmtisi&riffit^mSS^m^y::jiimi§mmmmiimimmmi;|:::|lllll;;;iiiii|i!iiiiiii:i:ilii:|ili;i;•>:-:-:-:-:-:-:-:-:-:-:-:-:-:-:-:-:-:-:->i£«jw™^-'X;- i':-::'x'xox';'x';':'y>:->'-:-: ::•::•::•:•:-;-:-:-:-:-:-:-:-:-:- SWra:.:.:.:.:.;.;.:.:.:.:.;.:::.;;;.;:;;:.::::v.v.v.:.v.;.;.:.:.:
ill; ^"Sierra 'Leone • • • " • • • • • • '• '• '• '• '• '• '• '•SomaliaSouth AfricaSudanTanzaniaTogoUganda
i;l;i;i;i;i;i;l;i;i; ^j;:;:;:;:;:;:;:;|;:;:;:;:|!|;;; ^
;;;iiii ||l||||l||l::||||:||lllllllllWi$^$f$$$i&$iii^i^^^^^
BangladeshBhutanChinaHong KongIndiaIndonesia
mm^mi^-Kamp^^^'Mffi^mM^Mwmmmmmi'6*:;:t^mm:fMmim^^mmiii^Sii^^jjlijmMMM^^^^^ii^a^Wi^iiiSi^^SK^iiIllll!:;iWa1a;pi|l:|:||lilll||:|;
MongoliaMyanmarNepalPakistanPapua New GuineaPhilippines
;;:::;;;:;;;;;;;:;;;;;:;:;:;§:£;:i:i:;:i:i:S;:i:;
fillip;!:;|||||||;; ! lllllll:||:i:j|:;:;i|:
IstlHM*W®$®$®?;-:P;l;Sil:;:lllliiiiiIlllliiSlIlllliil. . . . . . . . . . . . . . g..
242324
H;HHH?HBH}*;Bi;lliS;StllWiJSl:;:;iiliiSa;;;;S!S;S;S;S!?;iiSSSiliiiil•••— -si--
120
2514195
mffrnt-igvliil l:IlllllallIlllilllillllllSI
264050
2372
1111:1111rnmrnmmmms&iiilslliisi;:liill;fiil""""^59 '
2123422024
wfwwatM^msiimwmiietmmfMJK
INDUSTRIAL COUNTRIESNo data available
Source: WHO/CDD/89.31, "Programme for control of diarrhoeal diseases." Interim Programme Report 1988.* Percentage of all cases of diarrhoea in children under five years of age treated with oral rehydration therapy.Figures for country groupings are median values.
81
-oO
p>
S>^
2^ ^
I pc> p
Acute respiratory infections in children
In briefThe Goal: To reduce by 33 per cent the deaths due to acuterespiratory Infections In children under five years.
Each year, acute respiratory infections (ARI), one of the three leadingcauses of death In children under five, claim the lives of over fourmillion young children. Most of these deaths could be preventedsimply through earlier diagnosis and low-cost treatment, and throughimmunization programmes to prevent diseases such as measles andwhooping cough.
In the industrialized world, pneumonia is a relatively rare child-hood respiratory illness. But in developing countries, where malnu-trition and low birth weight are prevalent, large numbers of childrenunder five develop pneumonia and die from it. Children in developingcountries are up to 20 times more likely to die from pneumonia thanare children In the industrialized world.
Studies have proved that correctly managing the care of ARI canreduce the rate of pneumonia-related child deaths by as much as 70per cent. A world that spends millions of dollars on largely ineffectivecough and cold remedies cannot afford to ignore comparably low-cost programmes that produce such dramatic results.
ARI is one of the three leading killers of infants and children in the world.Every year, two billion young children suffer some kind of acute respiratoryinfection. While many of these are self-limiting viral illnesses, such ascoughs and colds, a substantial proportion are life-threatening, particularlyin the developing world. Of the estimated 14.6 million deaths amongchildren under five years of age each year, about 30 per cent are due to ARI.
Pneumonia accounts for most ARI deaths, taking the lives of fourmillion children, mostly in developing countries, annually. In fact, pneumo-
83
Managing carecorrectly
Immunization
nia develops in many children when they get respiratory infections, largelybecause of the prevalence of the two major risk factors—low birth weightand malnutrition. And pneumonia can claim the lives of its victims quickly,often within five days of the onset of symptoms. The risk is greatest toinfants under two months of age.
Cough and cold remedies are the single largest drug expenditure inmost countries around the world. While a few provide symptomatic relief,most are largely ineffective and unnecessary in respiratory infections, andsometimes can even be toxic in children.
The two major strategies of correct case management and immuniza-tion, however, can substantially reduce the deaths due to pneumonia.
Studies in India, Indonesia, the United Republic of Tanzania, Pakistan,Nepal, and the Philippines demonstrate the success of correct casemanagement in cutting the rate of child deaths from pneumonia by as muchas 50 to 70 per cent.
Correct case management, a central strategy in reducing mortalityfrom ARI, involves early recognition of the signs of pneumonia, by familiesor other caretakers, followed by the seeking of care from a trained healthworker, and finally appropriate treatment by that worker.
It is also important for community health workers, who are often thefirst point of contact with sick children, to recognize cases of pneumoniaand refer them for treatment.
Rapid breathing rate is one of the key warning signs of pneumonia.Parents can be helped to recognize changes in respiratory rate and othersigns of pneumonia, and learn to take a child who exhibits them to a clinicor a community health worker.
Health workers can look for diagnostic signs such as chest wallindrawing, observe a child's breathing, and count the breathing rate. If achild is under two months of age and is taking more than 60 breaths aminute, the danger is life-threatening. For children between two monthsand two years old, danger is indicated by a breathing rate of 50 breaths aminute. For children between two years and five years old, 40 inhalationsa minute is the crucial sign.
Health workers can then treat the respiratory infection. The specificcare given will depend on the serverity of the case and the age of the child,very young infants requiring special treatment.
Immunization, the second important strategy to lower the ARI toll, can helpprevent the respiratory infections in children that are caused by pertussis,measles, and diphtheria. Over a third of all ARi-related deaths in developingcountries are caused by these three diseases. Immunizing children
84
Putting ARIprogrammes into
effect
Research prioritiesfor the 1990s
against these diseases is a key component of the Expanded Programmeon Immunization (EPI).
For the most part, national programmes to control ARI are just getting un-derway. Emphasis now is on developing sound national policies and plansof action, phasing programmes appropriately, and developing effectivetraining strategies. Attention needs to be given to the following as nationalprogrammes are further developed:
• Ensuring that antibiotics are used appropriately. They should notbe used to treat simple coughs and colds. At the same time, theinappropriate use of cough and cold remedies needs to be dis-couraged.
• Improving communication so that parents and health workersunderstand each other and the illness. Parents (or other caretakers)need to understand the importance of obtaining rapidly from atrained health worker the right therapy (antibiotics) for the rightchildren (with pneumonia), for the right duration (five days).
• Educating parents and other caretakers on home care of simplecoughs and colds, how to recognize the signs of pneumonia, andwhere to go for help.
• Training health workers to recognize the signs and symptoms ofpneumonia and how to treat it.
• Examining ways to prevent pneumonia through, for example, thebetter understanding of how specific risk factors may promote thedevelopment of pneumonia in young children. Once riskfactors aremore clearly understood, interventions can be developed to mini-mize their impact.
To improve methods of managing the care of pneumonia, a number ofsubjects need to be studied. For example, the clinical signs and agents ofpneumonia among very young infants (less than two to three months old)is a top priority. WHO is organizing a multicentre study in several differentcountries to answer key questions in this area. The ability of differentcategories of health workers to diagnose and treat pneumonia is an areathat needs to be studied. Clinical trials are also needed to determinewhether antibiotic treatment of pneumonia can be simplified. Simpletechnologies to improve diagnosis and treatment—for example, 30-sec-ond and 60-second timers for counting respiratory rates, and oxygenconcentrators—need to be tested and applied.
85

The cost ofprogress
In addition, studies are needed to understand what parents and othercaretakers know about the signs of pneumonia and which signs promptthem to seek help outside the home.
Prevention research could yield valuable insights into the impact ofsuch risk factors as nutritional deficiencies, exposure to cold, and indoor airpollution from fuel and tobacco smoke. Field trials of potential vaccines toprevent the most common pneumonias in young children—specificallypneumonias caused by Streptococcus pneumoniae and Haemophilusinfluenzas—would be of particular value.
The cost of providing correct treatment for API is not excessive. To delivera full course of antibiotics for a case of pneumonia costs about $2. And toprevent a death from pneumonia—based on a case fatality rate of 4 percent estimated by WHO—would cost an estimated $52, without hospital-ization. If a child were hospitalized, then the cost to prevent death wouldbe $72 per case.
Correct case management is a central strategy in reducing mortality fromacute respiratory infections. It involves early recognition of the signs ofpneumonia, by families or other caretakers/ followed by the seeking oftreatment from a trained health worker, and finally appropriate treatmentby that worker.
The costs of not moving aggressively to control ARI are harder toquantify. They are, however, devastating to children, families, and tostruggling nations. API accounts for 30 per cent to 50 per cent of the visitsby children to treatment facilities and between 30 per cent to 40 per centof hospitalizations. An episode of pneumonia, even if not fatal, canseriously affect a child's health and resistance to other infections. Parentsor other caretakers must interrupt other activities to care for the child, andmay spend often scarce resources on unnecessary and sometimes toxicdrugs. And hospitalizing a child costs between $15 and $25 per day in mostcountries, a tremendous strain on national resources.
For the first time in history, pneumonia, one of the most serious causesof child deaths, can be treated inexpensively and effectively by healthworkers in a wide range of settings. Controlling API among young children,however, is not easy. Even more than with many other interventions,effective national programmes depend on functioning health systems,regular supplies of drugs, extensive training efforts, effective referralsystems, and close monitoring and supervision. The challenge is enormousand high-level political support and commitment will be necessary to meet
86
Further reading
it. With four million children succumbing to pneumonia each year, however,action is long overdue.
"Case Management of Acute Respiratory Infections in Children: Interven-tion Studies," Report of a Meeting, 19-21 April 1988, WHO, Geneva.
"Acute Respiratory Infections," UNICEF Executive Board Document, E/ICEF/1990/L7. New York. December 1989.
"Guidelines for UNICEF Assistance to Control Acute Respiratory Infection(ARI) Programmes," UNICEF Programme Paper CF/PD/PRO/I990-002. NewYork. February 1990.
87
oo00
^z<-JCQ
uj
^5
£