changing our approach to stage d heart failure
TRANSCRIPT

�������� ����� ��
Changing our Approach to Stage D Heart Failure
Miriam Becnel, Hector O. Ventura, Selim R. Krim
PII: S0033-0620(17)30109-3DOI: doi: 10.1016/j.pcad.2017.08.003Reference: YPCAD 828
To appear in: Progress in Cardiovascular Diseases
Received date: 6 August 2017Accepted date: 6 August 2017
Please cite this article as: Becnel Miriam, Ventura Hector O., Krim Selim R., Changingour Approach to Stage D Heart Failure, Progress in Cardiovascular Diseases (2017), doi:10.1016/j.pcad.2017.08.003
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Manuscript Title: Changing our Approach to Stage D Heart Failure Authors: Miriam Becnel, PA-C, 1,2 Hector O. Ventura, MD, 1,2,3, Selim R. Krim, MD,1,2,3
From 1Division of Cardiology, John Ochsner Heart and Vascular Institute, 2Section of
Cardiomyopathy & Heart Transplantation, John Ochsner Heart and Vascular Institute,
Ochsner Clinic Foundation, 3The University of Queensland School of Medicine, Ochsner
Clinical School, New Orleans, LA
Short Title: Stage D Heart Failure
Word Count: 3609 (excluding tables and references)
References: 48
Tables: 6
Figures: 2
Financial Disclosures: The authors have no financial or proprietary interest in the
subject matter of this article.
Miriam Becnel, PA-C
Section of Cardiomyopathy & Heart Transplantation
John Ochsner Heart and Vascular Institute
Ochsner Clinic Foundation
1514 Jefferson Highway
New Orleans, LA 70121
Email: [email protected]

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Hector O. Ventura, MD
Section of Cardiomyopathy & Heart Transplantation
John Ochsner Heart and Vascular Institute
Ochsner Clinic Foundation
1514 Jefferson Highway
New Orleans, LA 70121
Email: [email protected]
Selim R. Krim, MD
Section of Cardiomyopathy & Heart Transplantation
John Ochsner Heart and Vascular Institute
Ochsner Clinic Foundation
1514 Jefferson Highway
New Orleans, LA 70121
Email: [email protected]
Address for correspondence:
Selim R. Krim, MD
Section of Cardiomyopathy & Heart Transplantation
John Ochsner Heart and Vascular Institute
Ochsner Clinic Foundation
1514 Jefferson Highway
New Orleans, LA 70121
Email: [email protected]

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Abstract
Despite the tremendous progress made in the management of heart failure (HF), many
patients reach advanced stages. This paper aims to present a practical approach to the
stage D HF patient who is no longer responding to optimal medical therapy. We discuss
all available therapies for this patient population. We also offer some important caveats
with regard to identification, risk stratification, evaluation and treatment including early
patient referral to a center with an advanced HF program. Given the changing
landscape of heart transplantation and an impending change in the allocation system,
we also intend to engage a discussion on the need for a paradigm shift towards left
ventricular assist device therapy in this population.
Key words: heart failure, left ventricular assist device, mechanical circulatory support,
heart transplantation
Abbreviations:
ACC: American College of Cardiology AHA: American Heart Association BP: Blood pressure BTT: Bridge to transplant CO: Cardiac output CO2: Carbon dioxide CPX: Cardiopulmonary exercise testing DT: Destination therapy

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
ECMO: Extracorporeal membranous oxygenation HF: Heart failure HFSS: HF Survival Score HT: Heart transplantation IABP: Intra-aortic balloon pump ICD: Implantable cardioverter-defibrillator INTERMACS: Interagency Registry for Mechanically Assisted Circulatory Support LBM: Lean body mass LVAD: Left ventricular assist device MCS: Mechanical circulatory support NYHA: New York Heart Association OMT: Optimal medical therapy RER: Respiratory exchange ratio RHC: Right heart catheterization SHFM: Seattle HF Model TAH: Total artificial heart UNOS: United Network of Organ Sharing US: United states VE: Minute ventilation VO2: Ventilator oxygen uptake
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Introduction With a worldwide population exceeding 26 million individuals, HF constitutes a
significant burden on the healthcare system. Nearly 6 million HF patients reside in the
United States (US) with over 1 million patients being admitted on a yearly basis.1,2
Owing to a growing and aging population, more patients are reaching advanced stages
of HF despite tremendous progress in available therapies.3 Historically, heart
transplantation (HT) was the only option for stage D HF. With limited donor supply and a
rising need within this population, mechanical circulatory support (MCS) in the form of
the left ventricular assist device (LVAD) has emerged as a viable advanced therapy and
continues to mature through innovation and invention. LVADs are rapidly becoming
standard of care within the field. These devices are being implanted either as a bridge
to transplantation (BTT), destination therapy (DT), or in some cases cardiac recovery.4
Unfortunately not all patients with advanced HF will be candidates for the
aforementioned surgical options, and other treatment options include palliative inotropes
and hospice care.
Clinical recognition of when patients reach end-stage HF can be difficult, but
identifying patients who need advanced HF therapies is often more challenging. Early
patient referral to a center with an advanced HF program is imperative to ensure proper
identification, risk stratification, evaluation and treatment. This paper aims to present a
practical approach to the stage D HF patient. Given the changing landscape of
transplantation and an impending change in the allocation system, we also intend to
engage a discussion on the need for a paradigm shift towards LVAD therapy in this
population.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Early recognition and referral of the stage D HF patient
Timely detection of patient progression from stage C to stage D HF is crucial in
relation to treatment. While there are some variations in how different organizations
define advanced HF, is it universally accepted that all patients with end-stage HF have
become refractory to optimal medical therapy (OMT). It should also be noted that to
deem a patient truly refractory to guideline-directed OMT, any other etiologies that may
explain their symptomatic decline should be explored.5,6 This tell-tale sign should signal
immediate referral to an expert HT center.
Monitoring patients closely for signs and symptoms suggestive of stage D HF is
vital to ensure early detection and prompt referral. Frequent hospitalizations, low or
declining blood pressure (BP), inability to tolerate HF therapy, hyponatremia, frequent
implantable cardioverter-defibrillator (ICD) shocks, or increasing arrhythmia burden are
examples of red flags that should the heighten suspicion of end-stage HF (Table 1).6 In
addition, end-organ damage in the form of worsening creatinine or bilirubin may be
indicative of a low-output state and should never be ignored. Any patient with New York
Heart Association (NYHA) functional class IIIb or IV symptoms, American College of
Cardiology (ACC) and American Heart Association (AHA) stage D HF, or even
individuals with as little as 1 hospitalization for HF in the last 12 months should be
referred for evaluation by an advanced HF cardiologist.6
Although the current classification of patients with NYHA Class IV symptoms
does not accurately define patient clinical risk profile there are other profiling systems
that can be used for risk stratification, such as the Interagency Registry for Mechanically
Assisted Circulatory Support (INTERMACS).7 The INTERMACS profiles (Table 2) are
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
useful in determining candidacy and optimal timing when considering the use of
temporary MCS, durable LVADs, or HT. Some patients may benefit initially from durable
MCS, whereas others may require temporary MCS as a bridge to decision, candidacy,
or recovery.4
Risk stratification
Patients referred for advanced HF treatment options typically undergo initial risk
stratification prior to a full evaluation. This essential step in the process helps to select
patients who warrant and will benefit from these therapies. Risk stratification includes
the use of clinical risk scores, objective functional tests such as cardiopulmonary
exercise testing, and right heart catheterization to assess patient’s hemodynamics.
Clinical risk scores
Risk stratification of patients with HF is crucial for proper prognostication and
recognition of patients who need more advanced therapies. Risk scores typically include
patient characteristics, clinical signs and laboratory tests. Two clinical risk scores are
used commonly in practice when stratifying HF patients. The HF Survival Score (HFSS)
uses 7 parameters and was validated among HF patients who were referred for HT.8,9
The Seattle HF Model (SHFM) includes a 20-variable model that combines clinical,
laboratory and therapeutic data.10,11 Although both models are useful in clinical practice,
only the HFSS was derived and validated in patients referred for HT, and therefore
should be used instead of the SHFM in the advanced HF population. It should be noted
that the SHFM tends to overestimate survival in the stage D HF population as it
originated from ambulatory patient data.10,11

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Cardiopulmonary exercise testing (CPX)
Despite not being available in all centers, cardiopulmonary exercise testing
(CPX) is a key test in assessing patients for advanced HF therapies.12 Two important
CPX variables are usually used for risk stratification and prognosis—peak ventilator
oxygen uptake (VO2) and minute ventilation/carbon dioxide production (VE/VCO2)
slope. Peak VO2 has been shown to be a strong predictor of mortality among HF
patients evaluated for HT.13 A reduced maximal oxygen consumption peak VO2 of less
than 12 mL/kg/min (or less than 14 mL/kg/min for patients using beta blockers) signifies
advanced HF stage and warrants evaluation for HT. A low peak VO2 should always be
interpreted in the context of adequate effort which is defined as a respiratory exchange
ratio (RER) greater than 1.1.12 Owing to significant variability in body composition in our
HF population, correcting peak VO2 for lean body mass (LBM) seems to be a better
discriminator of outcome than traditionally reported total weight adjusted values. In this
regard, a peak VO2 corrected for LBM cutoff of 19 mL/kg/min has shown to be a
superior discriminator of major cardiac events (death and/or urgent HT) than the total
weight-adjusted figure of 14 mL/kg/min in patients with stage D HF.12 The
VE/VCO2 slope is another important variable and when abnormal (VE/VCO2 slope>34)
it provides additional and independent prognostic information. Evaluation of the
VE/VCO2 slope in conjunction with peak VO2 is recommended to optimize
prognostication in patients with HF.14,15,16
Hemodynamic assessment
Right heart catheterization (RHC) is considered the gold standard in evaluating
hemodynamics, particularly the cardiac index and pulmonary pressures, when

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
determining the need for HT. A cardiac index value of less than 2.5 L/min/m2 is
suggestive of advanced disease. The use of RHC is key in diagnostic evaluation of
pulmonary vascular resistance considering that it precludes HT if found to be elevated
and irreversible.17
With regard to LVAD implantation, important hemodynamic parameters identified
as strong markers of post-operative right HF, including right atrial pressure >15 mm Hg,
right atrial pressure to pulmonary capillary wedge pressure ratio>0.63, and right
ventricular stroke work index ≤0.25 mm Hg × l/m2.18,19
Available therapies for stage D HF
Heart transplantation
For the last 4 decades, HT has been the panacea for stage D HF. With improved
immunosuppressive therapies in addition to 1- and 5- year post-HT survival, HT will
likely remain the gold standard treatment for this critically ill patient population.20 Only
2500 HTs are performed annually in the US, and owing to a meager donor pool this is
unlikely to change. As a result, many patients die on the heart transplant list while they
wait for a favorable donor.
Consideration should be made for HT if OMT and cardiac resynchronization
therapy as recommended by current ACC/AHA guidelines have failed to improve patient
symptoms and slow disease progression.21 Assessing for any reversible or surgically
amenable cardiac conditions should be addressed before HT or MCS are considered.
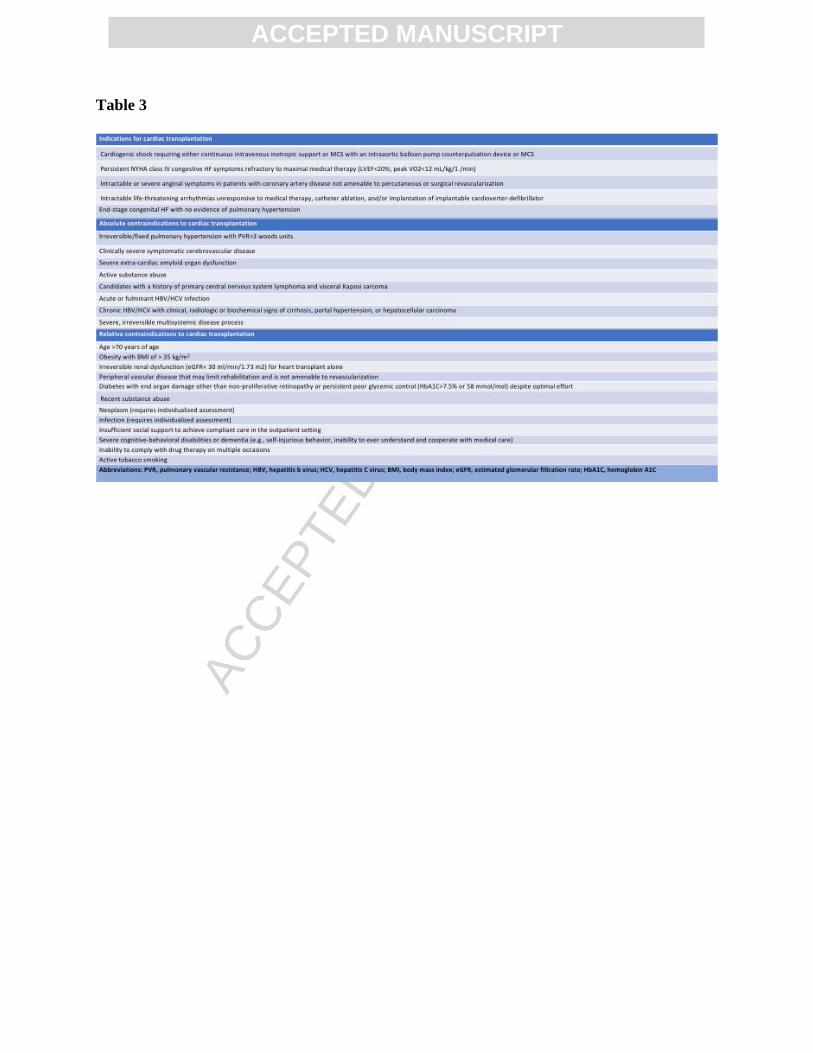
Table 3 summarizes eligibility criteria for HT. By the same token, a thorough
assessment of conditions that may preclude HT should be explored. Examples of
absolute and relative contraindications to HT are listed in Table 3.22,23

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Durable left ventricular assist devices
The use of MCS grew and quickly became a viable option for stage D HF
patients (Table 4) after revealing prolonged survival with the first pulsatile LVAD, the
HeartMate XVE (Abbott Laboratories, formerly Thoratec Corporation, Abbott Park, IL),
in the pivotal 2001 REMATCH trial.24 This device was approved in 1994 for BTT and in
2003 for DT.25 Unfortunately, the associated adverse event profile and large pump size
led to limited durability with device life averaging only 18 to 30 months. Consequently,
pulsatile pumps gave rise to the next generation of continuous-flow LVADs, which
include the axial-flow HeartMate II (Abbott Laboratories, Abbott Park, IL) and the
centrifugal-flow HVAD (HeartWare Inc., Framingham, MA).26 The HeartMate II is
approved for BTT and DT, whereas the HVAD is only approved for BTT at
present.26,27,28 The centrifugal-flow HeartMate 3 (Abbott Laboratories, Abbott Park, IL) is
the newest device under investigation in the US and is seeking both BTT and DT
indications. Additional BTT options include the total artificial heart (TAH) or biventricular
ventricular assist devices (Bi-VAD), which are usually only indicated in a select
population with biventricular failure or refractory ventricular arrhythmias (Figure 1). With
1- and 2-year survival rates of 80% and 70% respectively, the LVAD population is
expected to grow exponentially over the coming years.26,27
Inotrope therapy
Positive inotropic agents are frequently used in the setting of acute
decompensated HF when evidence of pulmonary congestion and signs of
hypoperfusion are present.29 Milrinone and dobutamine are the most widely used
inotropic agents in the US.30 Dobutamine, a ß-adrenergic agonist, is recommended for

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
treatment of patients with low cardiac output (CO) and reduced BP. Concomitant use of
β-blockers with dobutamine is not recommended as it may attenuate the benefit of both
agents. Milrinone, a phosphodiesterase inhibitor, is sometimes preferred over
dobutamine in the setting of significantly elevated systemic and pulmonary vascular
resistance, low CO and hypoperfusion symptoms.31 While inotropes have been shown
to improve both symptoms and hemodynamics, concerns have been raised with the use
of these agents on a long-term continuous basis for patients with refractory HF declined
for definitive therapy (HT or MCS).32,33 Therefore, long-term continuous or intermittent
inotrope infusions should only be recommended as a bridge to decision.
End of life care and palliative therapy
Patients with advanced HF unresponsive to OMT who do not qualify for either HT
or MCS should be offered palliative measures. After exhausting all standard of care
options, hospice should be offered to patients with NYHA class IV symptoms with less
than a 6-month life expectancy.34,35,36,37,38 These services can be performed at home, in
the hospital, or at a specialized hospice center, which can generally provide oral
medications and focus on symptom management. Certain hospice programs may
provide complex treatments, such as intravenous inotropes or continuous positive
airway pressure ventilation. 34,35 It is only with continued engagement of the clinician and
meticulous management of fluid status that quality of life can be fully maximized in
hospice care. A noteworthy topic specific to end-of-life within this patient population is
ICD deactivation. While this may make for a difficult discussion, thoughtfully counseling
patients on deactivation is an essential step for these terminal patients as ICD
discharges only exacerbate pain and anxiety. 39
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
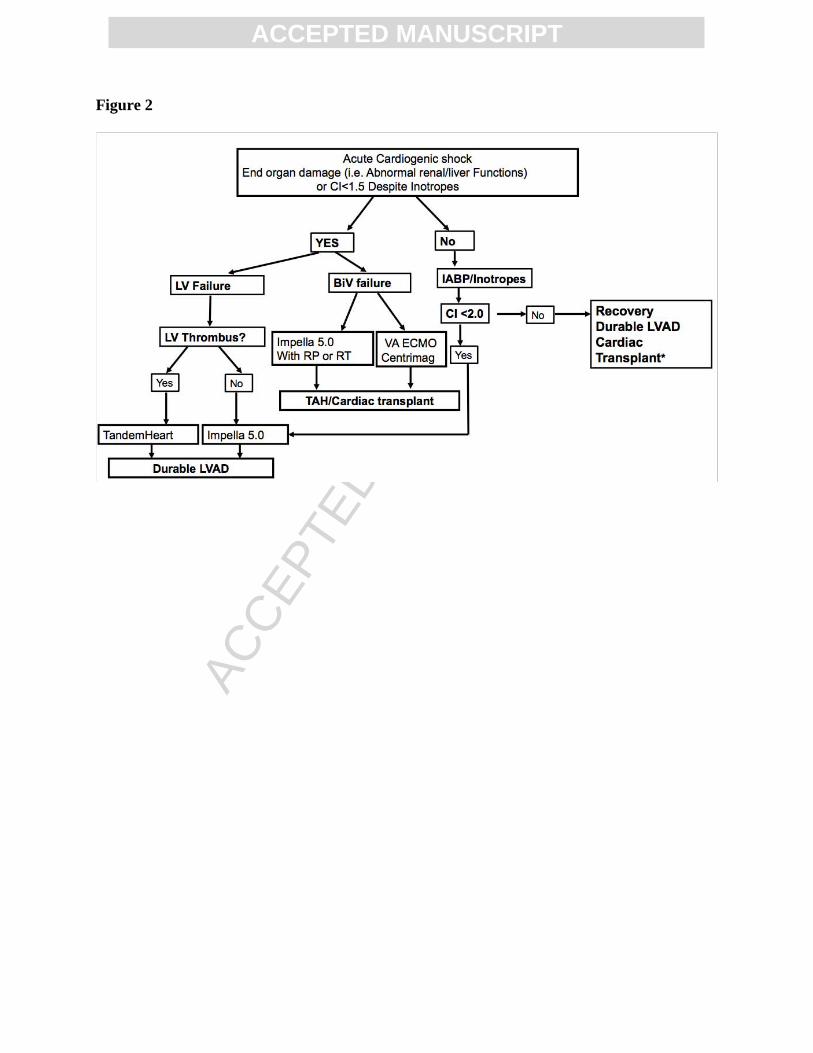
Mechanical circulatory support for the cardiogenic shock patient
Many patients are too sick upon presentation to undergo HT or durable LVADs.
In this regard, temporary MCS may be used as a bridge to more definitive therapy (e.g.,
bridge to durable LVAD or BTT). INTERMACS profile 1 patients are considered “critical
cardiogenic shock” or “crashing and burning” and have held a consistent 15% stake in
the total number of patient’s receiving durable LVADs from 2008 to 2014.7,40,41
INTERMACS 2 patients are patients with “progressive decline” on inotropic therapy, and
accounted for 38% of total implants over the same 6-year time frame.7,41 Given the
overall instability of profile 1 and the foreseeable deterioration in profile 2 patients,
temporizing measures are often pursued. With the aim of reversing end-organ damage,
temporary MCS also allows care teams time to explore whether a more definitive
therapy can be accomplished. In this case, the use of temporary MCS has been coined
“bridge to decision”. While it is still unclear whether reversal of end-organ damage and
stabilization via temporary MCS decreases perioperative risk and mortality, there is
widespread acceptance and use of these devices. Patient and device selection varies
among centers, but ideally should be based on expertise and training, while also being
individually tailored to the patient’s hemodynamic and structural profile. Ease of implant
differs between devices and method (percutaneous versus surgical) determines location
of implant (cardiac catheterization laboratory or operating room). Optimal timing
between temporary device implant and crossover to durable MCS has not been well
defined. Additional data including protocols and algorithms are needed to guide
providers in selecting the most appropriate device for suitable patients at the right time.
Contraindications vary between devices and our proposed algorithm is intended to help

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
guide the selection of support in the cardiogenic shock patient based on their profile
(Figure 2). TABLE 5 highlights temporary counterpulsation, microaxial and centrifugal
pumps currently available for use in the US.
Current heart allocation system and its limitations
Established over a decade ago, the current three-tiered heart allocation system
has led to tremendous decrease in the rate of waiting list mortality and improvement in
post-HT survival.20,23 Based on the severity of medical conditions, the United Network of
Organ Sharing (UNOS) assigns a status to all patients listed for HT.42.43 Those with an
expected survival of less than 1 month are listed 1A, the highest waitlist status. This
gravely ill cohort includes those patients either on high doses of inotropic drugs,
receiving mechanical ventilation or requiring MCS who meet appropriate criteria (e.g.,
LVAD 30-day time, temporary LVAD, RVAD, BiVADs, durable devices with
complications). The next listing tier is status 1B and is assigned to patients who are
stable on lower-dose inotropic therapy or durable mechanical support, and can be
inpatient or outpatient. Status 2, the third tier, are stable ambulatory patients who are
not on inotropic drugs.42,43
Despite improvement in outcomes after the implementation of the 3-tier system,
there are several limitations that remain. For each status within a geographic zone,
hearts are allocated to candidates in order of decreasing time spent at that status in
addition to blood type-matching. One major drawback of the current system is the lack
of clinical differentiation between waitlisted status 1A and 1B candidates.44 In addition,
the rising number of patients listed status 1A and 1B has become a concern and is
primarily attributed due to the increased use of durable MCS.45 This has led experts in
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
the field to question the appropriate designation status of stable LVAD patients.44 This
becomes particularly relevant as recent data has denoted the low risk of adverse events
in stable LVAD patients.46 These events are defined as death or waitlist removal for
being too ill to transplant when compared to other status 1A patients (e.g., dual
inotropes, paracorporeal VADs, congenital heart disease). It is important to note when a
LVAD patient develops a device-related complication that satisfies criteria for 1A listing,
they instantly carry a higher waiting list mortality.46 Consequentially, the continued
expansion of LVAD therapy as BTT will undoubtedly contribute to an increased number
of patients listed UNOS status 1A secondary to device malfunction, thrombosis, and
infection. In turn, the present long-term HT outcomes could be negatively impacted.
Newly proposed heart allocation system and its implications
In response to the conundrum of the present-day allocation structure, the UNOS
heart subcommittee has proposed a new 6-tier system which aims to 1) improve
utilization of the limited supply of donor hearts by modifying geographic distribution and
improve overall access to HT; 2) reduce waiting list mortality by prioritizing sicker
patients and undeserved groups (congenital heart disease, restrictive
cardiomyopathies) without compromising post-HT survival; and 3) decrease the use of
exceptions by better accommodating all candidates within the system. The new
allocation system is summarized in Table 6.43,44
In a nutshell, the sickest patients under the new system are given top priority in
tier 1, including those patients receiving mechanical ventilation and extracorporeal
membranous oxygenation (tier 1), and stable LVAD patients will now fall in tier 4—much
lower when compared to the current 3-tier system. In view of the recent data revealing

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
low mortality rates among stable LVAD patients, our belief is that these changes will
lead to better utilization of available donor hearts and allow sicker patients to receive HT
in an expedited fashion. On the other hand, we feel that tier 3 patients with LVAD
complications such as pump thrombosis or right HF are at a much higher risk for
adverse events and death, and as a result should be given a higher priority.
Furthermore, we believe that those patients sick enough to necessitate a higher level of
temporary MCS (e.g., Impella, TandemHeart, CentriMag) should certainly be assigned
to a higher tier than those only requiring intra-aortic balloon pump support. We also
have serious concerns about assigning patients bridged with extracorporeal
membranous oxygenation (ECMO) to tier 1 knowing the potential increase in post-HT
mortality given their critically ill nature. Lastly, we worry that this newly proposed system
may not solve the previous issue of other disadvantaged groups such as congenital
heart disease and restrictive cardiomyopathies.
Durable MCS: What the future holds
With the upcoming changes in organ allocation, advancement in durable LVAD
technology and management will become more important than ever. With nearly half of
LVAD implants performed as destination therapy, continued amelioration of durable
devices is imperative to prolong survival on support. Bleeding, infection and device
thrombosis are major sources of morbidity and mortality in the present day population.41
Reduction in the frequency of these adverse events should remain a major driver in the
development of better device therapy.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Tunneled drivelines are a major source of infection and are currently used in all
durable LVADs. The driveline exits through the skin to connect to an external power
source, thus making it prone to mechanical complications. Infection risk is likely to be
substantially reduced by way of driveline elimination. A fully implantable system would
also allow patients to submerse in water which would increase patient quality of life.
Frequent hospital admissions for LVAD patients with a subtherapeutic
international normalized ratio is another important issue. Not only do these unnecessary
hospitalizations impact their quality of life, but they also drive the cost-effectiveness of
this therapy down. Many centers have adopted strategies for outpatient bridging of
anticoagulation with low-molecular weight heparin (e.g., enoxaparin). Validation of the
safety and efficacy of such strategies in addition to protocols designed for use in this
population need to be tested at a multicenter level in the ambulatory setting.47
Integration of hemodynamic monitoring capabilities with LVAD technology could
provide a whole new level of care to these patients. Especially true for the centrifugal
type-pumps (e.g., HVAD, HeartMate 3), both hypo- and hyper-volemic conditions can
trigger LVAD alarms and often the culprit driving the condition is difficult to ascertain.
Adding this type of feature to the next generation device would complement the existent
resources in evaluation and management of these patients. Ideally, this data would be
remotely accessibly, which has the potential to decrease hospital readmissions and cost
if providers were able to triage and manage patients without necessitating inpatient
evaluation.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
The most recent device under investigation employs new magnetic levitation and
artificial pulse technology in an attempt to mimic native cardiac contractility in hopes of
reducing bleeding and thrombosis complications.48 The future of durable LVADs
remains promising, and it is only through experience and refining technology that patient
survival will continue to improve.
Conclusion
In light of improvement in LVAD outcomes and the continued limited organ
supply we propose a paradigm shift in the management of advanced stage D HF
patients. First and foremost, we believe that all patients with refractory HF should be
promptly referred and evaluated for durable LVADs. Second, only patients deemed to
not be candidates for LVAD therapy or those who develop complications post-VAD
implant (e.g., gastrointestinal bleeding, driveline infection, pump thrombosis, RV failure)
should be offered HT. This approach, albeit controversial, may reduce the current
number of patients listed as a status 1A or 1B for HT. It would also allow for sicker and
traditionally disadvantaged populations (congenital heart disease, infiltrative
cardiomyopathies, refractory arrhythmias) to get transplanted in a timely fashion. Third,
although the new allocation system aims to reduce waiting list mortality by prioritizing
sicker patients, we have significant concerns with regard to post-HT outcomes in
patients receiving ECMO as a BTT given the lack of data in this population. Despite the
impressive survival benefit provided by LVAD therapy, the unacceptably high short-and
long-term adverse event profile remains a key hindrance. In conclusion, more research
is crucial and necessary to better understand and subsequently reduce these events in
order to make this technology a viable, permanent and cost-effective alternative to HT.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
References 1. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics—2011
update: A report from the american heart association. Circulation 2011;123:e18-
e209.
2. Ambrosy PA et al. The Global Health and Economic Burden of Hospitalizations for
Heart Failure. Lessons Learned From Hospitalized Heart Failure Registries. J Am Coll
Cardiol. 2014;63:1123–1133.
3. Cowie MR et al. Improving care for patients with acute heart failure. 2014. Oxford
PharmaGenesis. ISBN 978-1-903539-12-5. Available online at:
http://www.oxfordhealthpolicyforum.org/reports/acute-heart-failure/improving-care-for-
patients-with-acute-heart-failure
4. Mancini D, Colombo PC. Left Ventricular Assist Devices: A Rapidly Evolving
Alternative to Transplant. J Am Coll Cardiol. 2015;65(23): 2542-2555.
5. Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA
guidelines for the diagnosis and management of heart failure in adults: A report of the
american college of cardiology foundation/american heart association task force on
practice guidelines: Developed in collaboration with the international society for heart
and lung transplantation. Circulation 2009;119:1977-2016
6. Yancy CW, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological
therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the
management of heart failure: a report of the American College of Cardiology
Foundation/American Heart Association Task Force on Clinical Practice Guidelines and

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
the Heart Failure Society of America. J Card Fail. 2016. DOI:
http://dx.doi.org/10.1016/j.cardfail.2016.07.001
7. Stevenson LW, Pagani FD, Young JB, et al. INTERMACS profiles of advanced heart
failure: the current picture. J Heart Lung Transplant. 2009;28(6):535-541.
8. Aaronson KD, Schwartz JS, Chen TM, et al. Development and prospective validation
of a clinical index to predict survival in ambulatory patients referred for cardiac
transplant evaluation. Circulation1997;95:2660-7
9. Goda A, Lund LH, Mancini D. The heart failure survival score outperforms the peak
oxygen consumption for heart transplantation selection in the era of device therapy. J
Heart Lung Transplant2011;30:315-25
10. Gorodeski EZ, Chu EC, Chow CH, et al. Application of the seattle heart failure
model in ambulatory patients presented to an advanced heart failure therapeutics
committee. Circ Heart Fail 2010;3:706-14.
11. Kalogeropoulos AP, Georgiopoulou VV, Giamouzis G, et al. Utility of the seattle
heart failure model in patients with advanced heart failure. J Am Coll Cardiol
2009;53:334-42.
12. Milani RV, Lavie CJ, Mehra MR. Cardiopulmonary exercise testing: how do we
differentiate the cause of dyspnea? Circulation. 2004;110:e27- e31.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
13. Mancini DM, Eisen H, Kussmaul W, et al. Value of peak exercise oxygen
consumption for optimal timing of cardiac transplantation in ambulatory patients with
heart failure. Circulation.1991;83:778–786.
14. Milani RV, Mehra MR, Reddy TK, Lavie CJ, Ventura HO. Ventilation/ carbon dioxide
production ratio in early exercise predicts poor functional capacity in congestive heart
failure. Heart. 1996;76:393-396.
15. Arena R, Myers J, Abella J, et al. Development of a ventilatory classification system
in patients with heart failure. Circulation. 2007;115:2410–2417
16. Ferreira AM, Tabet JY, Frankenstein L, et al. Ventilatory efficiency and the selection
of patients for heart transplantation. Circ Heart Fail. 2010;3:378–386.
17. Mehra MR, Kobashigawa J, Starling R, et al. Listing criteria for heart
transplantation: International society for heart and lung transplantation guidelines for the
care of cardiac transplant candidates--2006. J Heart Lung Transplant 2006;25:1024-42
18. Kormos R.L., Teuteberg J.J., Pagani F.D., et al., for the HeartMate II Clinical
Investigators (2010) Right ventricular failure in patients with the HeartMate II
continuous-flow left ventricular assist device: incidence, risk factors, and effect on
outcomes. J Thorac Cardiovasc Surg 139:1316–1324.
19. Fitzpatrick J.R. 3rd.,Frederick J.R., Hsu V.M., et al. (2008) Risk score derived
from pre-operative data analysis predicts the need for biventricular mechanical
circulatory support. J Heart Lung Transplant 27:1286–1292.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
20. Lietz K, Miller LW. Improved survival of patients with end-stage heart failure listed
for heart transplantation: Analysis of organ procurement and transplantation
network/U.S. united network of organ sharing data, 1990 to 2005. J Am Coll
Cardiol 2007;50:1282-90
21. Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA
guidelines for the diagnosis and management of heart failure in adults: A report of the
american college of cardiology foundation/american heart association task force on
practice guidelines: Developed in collaboration with the international society for heart
and lung transplantation. Circulation 2009;119:1977-2016
22. Butler J, Khadim G, Paul KM, et al. Selection of patients for heart transplantation in
the current era of heart failure therapy. J Am Coll Cardiol 2004;43:787-93
23. Stehlik J, Edwards LB, Kucheryavaya AY, et al. The registry of the international
society for heart and lung transplantation: Twenty-eighth adult heart transplant report--
2011. J Heart Lung Transplant2011;30:1078-94
24. Rose EA, Gelijns AC, Moskowitz AJ, et al., for the Randomized Evaluation of
Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH)
Study Group. Long-term use of a left ventricular assist device for end stage heart
failure. N Engl J Med. 2001;345(20):1435-1443.
25. Miller LW, Pagani FD, Russell SD, et al; HeartMate II Clinical Investigators. Use of a
continuous-flow device in patients awaiting heart transplantation. N Engl J Med.
2007;357(9):885-896.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
26. Starling RC, Naka Y, Boyle AJ, et al. Results of the post-U.S. Food and Drug
Administration-approval study with a continuous flow left ventricular assist device as a
bridge to heart transplantation: a prospective study using the INTERMACS (Interagency
Registry for Mechanically Assisted Circulatory Support). J Am Coll Cardiol.
2011:57(19):1890-1898.
27. Slaughter MS, Pagani FD, Rogers JG, et al. Clinical management of continuous-
flow left ventricular assist devices in advanced heart failure. J Heart Lung Transplant.
2010;29(4 Suppl): S1-S38.
28. Lietz K, Long JW, Kfoury AG, et al. Outcomes of left ventricular assist device
implantation as destination therapy in the post-REMATCH era: implications for patient
selection. Circulation. 2007;116(5):497-505
29. Upadya S, Lee FA, Saldarriaga C, Verma S, Sedrakyan A, Nystrom K, et al. Home
continuous positive inotropic infusion as a bridge to cardiac transplantation in patients
with end-stage heart failure. J Heart Lung Transplant. 2004;23:466-72.
30. Gorodeski EZ, Chu EC, Reese JR, et al. Prognosis on chronic dobutamine or
milrinone infusions for stage D heart failure. Circ Heart Fail 2009;2:320-4.
31. Cuffe MS, Califf RM, Adams KF, et al. Short-term intravenous milrinone for acute
exacerbation of chronic heart failure: A randomized controlled trial. JAMA
2002;287:1541-47.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
32. Anderson JL, Hemodynamic and clinical benefits with intravenous milrinone in
severe chronic heart failure: results of a multi-center study in the United States. Am
Heart J 1991;121:1956-64.
33. Mehra MR, Ventura HO, Kapoor C, Stapleton DD, Zimmerman D, Smart FW. Safety
and clinical utility of long-term intravenous milrinone in advanced heart failure. Am J
Cardiol 1997;80:61-4.
34. Goodlin SJ, Hauptman PJ, Arnold R, Grady K, Hershberger RE, Kutner J, et al.
Consensus statement: Palliative and supportive care in advanced heart failure. J Card
Fail. 2004;10:200-9.
35. Zapka JG, Moran W, Goodlin S, et al. Advanced heart failure: prognosis,
uncertainty, and decision making. Congset Heart Fail. 2007;13(5):268–74.
36. LeMond LM, Allen LA, Palliative care and hospice in advanced heart failure. Prog
Cardiovasc Dis. 2011;54(2):168–78.
37. Goodlin SJ, Palliative care in congestive heart failure. J Am Coll Cardiol.
2009;54(5):386–96.
38. Ryder M, Beattie J, O’Hanlon R, et al. Multidisciplinary heart failure management
and end-of-life care. Curr Opinion Supp Pall Care. 2011;5(4):317–21.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
39. Sherazi S, McNitt S, Aktas M, et al. End-of-life care in patients with implantable
cardioverter defibrillators: A MADIT-II Substudy. Pacing and Clin Electrophys.
2013;36(10):1273–9.
40. Cheng R, Ramzy D, Azarbal B, et al. Device Strategies for Patients in INTERMACS
Profiles 1 and 2 Cardiogenic Shock: Double Bridge With Extracorporeal Membrane
Oxygenation and Initial Implant of More Durable Devices. Artificial Organs.
2016;41(3):224-232. doi:10.1111/aor.12758.
41. Kirklin JK, Naftel DC, Pagani FD, Kormos RL, Stevenson LW, Blume ED, et al.
Seventh INTERMACS annual report: 15,000 patients and counting. The Journal of
Heart and Lung Transplantation. 2015;34:1495-504.
42. 2009 annual report of the U.S. organ procurement and transplantation network and
the scientific registry of transplant recipients: Transplant data 1999-2008. U.S.
department of health and human services, health resources and services
administration, healthcare systems bureau, division of transplantation, rockville, MD.
Available online: http://www.ustransplant.org/annual_reports/current/
43. Organ procurement and transplantation network (OPTN). Organ distribution:
Allocation of hearts and heart-lungs. Department of health and human services, health
resources and services administration, healthcare systems bureau, division of
transplantation. Available
online: http://optn.transplant.hrsa.gov/policiesAndBylaws/policies.asp

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
44. Meyer DM, Rogers JG, Edwards LB, Callahan ER , Webber SA, Johnson MR, Vega
JD, Zucker MJ, Cleveland JC Jr. The Future Direction of the Adult Heart Allocation
System in the United States. American Journal of Transplantation 2015; 15: 44–54
45. Taghavi S, Jayarajan SN, Komaroff E, et al. Continuous flow left ventricular assist
device technology has influenced wait times and affected donor allocation in cardiac
transplantation. J Thorac Cardiovasc Surg 2014;147:1966-71
46. Pinney SP. Timing isn’t everything: Donor heart allocation in the present LVAD era.
J Am Coll Cardiol 2012; 60: 52–53.
47. Sandner SE, Riebandt J, Haberl T, et al. Low-molecular-weight heparin for anti-
coagulation after left ventricular assist device implantation. J Heart Lung
Transplant 2014;33:88-93.
48. Heatley G, Sood P, Goldstein D, et al. Clinical trial design and rationale of the
Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory
Support Therapy With HeartMate 3 (MOMENTUM 3) investigational device exemption
clinical study protocol. The Journal of Heart and Lung Transplantation. 2016;35(4):528-
536.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE TITLES/LEGENDS
Table 1. SIGNS AND SYMPTOMS OF STAGE D HF. Adapted from ACC/AHA
guidelines (Yancy et al6)
Table 2. INTERMACS CLASSIFICATION
Table 3. CURRENT INDICATIONS AND CONTRAINDICATIONS OF CARDIAC
TRANPLANTATIONS
Table 4. INDICATIONS AND CONTRAINDICATIONS OF LVAD THERAPY
Table 5. CURRENTLY AVAILABLE TEMPORARY MCS DEVICES IN THE US
Table 6. NEW HEART ALLOCATION SYSTEM. Adapted from Meyer et al.44
Figure 1. PROPOSED ALGORITHM FOR ADVANCED HEART FAILURE THERAPIES
⌘Infiltrative cardiomyopathies (e.g. Cardiac amyloidosis, Sarcoidosis, HFpEF with
refractory Angina), *LVAD complications: pump thrombosis, pump malfunction,
pump stop, driveline infection
Figure 2. MCS AS A BRIDGE THERAPY FOR THE CARDIOGENIC SHOCK PATIENT.
*Infiltrative cardiomyopathies (e.g. Cardiac amyloidosis, Sarcoidosis, small
ventricles)

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 1
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 2

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 1

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 2
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 3

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 4

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 5

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 6

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Conflict of interest: None.