cervical cancer screening recommendations 2012, fda panel 2014
TRANSCRIPT

Cervical Cancer Screening Recommendations 2012, FDA Panel 2014

Goals of Screening ( & Management) Prevent Morbidity and mortality from Cervical Cancer Not find HPV infection Not find abnormal cytology
Prevent Overzealous management of precursor lesions likely to regress or disappear for which the risks of management outweight the benefits
The new screening recommendations address
Initial screening primary screening approach
Screening in older women and after hysterectomy
Screening frequency ( interval)
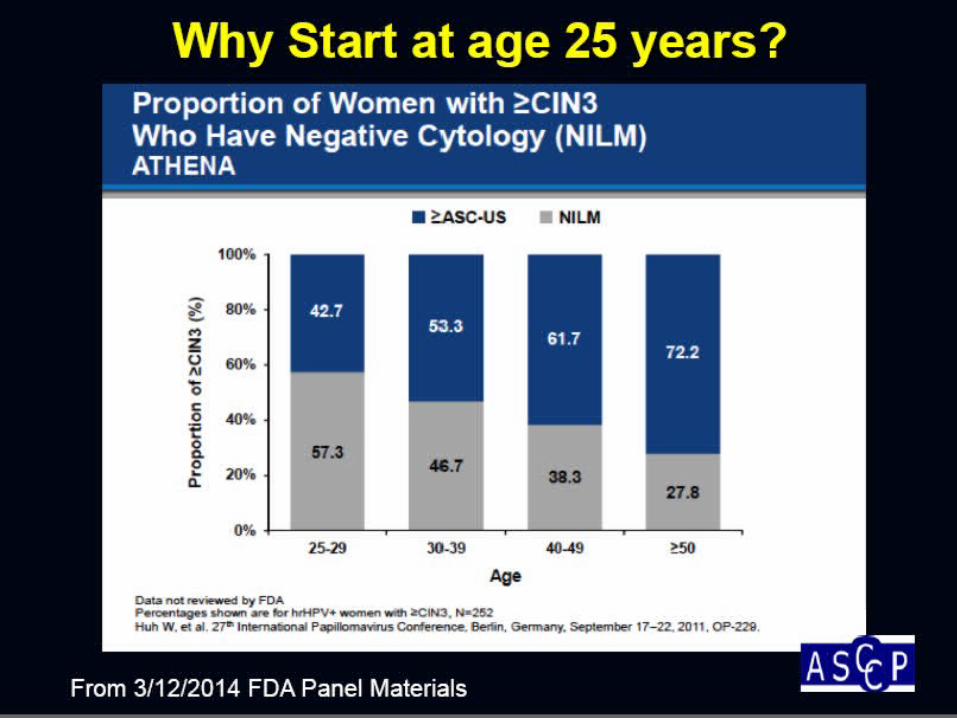
Starting age
Stopping age
Special Population
age-appropriate screening strategies

The frequency of testing is dependent upon the screening test used.
Frequency (Interval)

SCREENING MODALITIES
Pap Test ; conventional or Liquid > = 21 y every 3 year
Co-testing; every 5 year pap smear + hrHPV test ; only ≥ 30 Y
Primary, Stand-alone HPV test ; ≥25 Y every 3 year only FDA Approve: Cobas test

Screening Interval
Risk of developing invasive cancer before next screen should be unlikely

Rationale for Longer Pap Screening Intervals
Sensitivity of Single Pap test 50-70% Cancer risk 1.5/100,000 Cancer risk 4.7/100,000
99,997 women screened unnecesarily to help 3








RISKS OF SCREENING
MISUSE and Harms


2014 NEWS What’s NEW



Other Issues to Consider with Cytology
• Highly subjective test: substantial inter-and intra-laboratory variability and limited reproducibility
• Unable to identify those women who are at future risk of developing cervical cancer precursors
• Unclear how cytology will perform as HPV vaccine uptake rates increase in the US


FDA approval of cobasHPV test, April, 2014 Athena end of trial results
–>40,000 participants ≥ age 25
–Followed up in 3 years if HPV test negative
–Colposcopy if HPV 16+ or 18+
–Cytology if HPV 16 neg. or 18 neg.
Summary of HPV Primary Screening for Cervical Cancer







Education, education, and more education
3 screening options = more confusion?
Concerns raised by the FDA Panel(and others….)

سپاس