cco rational options in breast cancer : how molecular understanding informs treatment
TRANSCRIPT

John R. Mackey, MD, FRCP(C)TRIO DirectorProfessor Division of Medical OncologyDepartment of OncologyUniversity of AlbertaCross Cancer InstituteEdmonton, AlbertaCanada
Rational Options in Breast Cancer: How Molecular Understanding Informs Treatment
This program is supported by educational grants from
In association with Translational Research in Oncology

clinicaloptions.com/oncologyTranslational Research 2012
About These Slides
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
Our thanks to the presenters who gave permission to include their original data
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options
clinicaloptions.com/oncologyTranslational Research 2012
Program Faculty
Program DirectorDennis J. Slamon, MD, PhDTRIO ChairmanChief, Division of Hematology/OncologyDavid Geffen School of Medicine at UCLALos Angeles, California
FacultyJohn R. Mackey, MD, FRCP (C)TRIO DirectorProfessor Division of Medical OncologyDepartment of OncologyUniversity of AlbertaCross Cancer InstituteEdmonton, AlbertaCanada

clinicaloptions.com/oncologyTranslational Research 2012
Faculty Disclosures
John R. Mackey, MD, FRCP(C), has no significant financial relationships to disclose.
Dennis J. Slamon, MD, PhD, has disclosed that he has received consulting fees from Genentech, GlaxoSmithKline, and Roche.

clinicaloptions.com/oncologyTranslational Research 2012
Outline
The challenge of molecular complexity in breast cancer
Where we are today
Where we need to go
– Defining and addressing the problem in Darwinian terms
– Heterogeneity and selection

clinicaloptions.com/oncologyTranslational Research 2012
Challenge of Early-Stage Breast Cancer
Despite surgery, cytotoxic chemotherapy, hormonal therapy, and/or regional radiotherapy, ~ 30% of patients will eventually experience disease recurrence
The biologic reasons for recurrence and resistance to treatment are poorly understood
Recurrent breast cancer is usually lethal

clinicaloptions.com/oncologyTranslational Research 2012
Breast Cancer Biology in 2012: A Pragmatic View
ENDOCHEMO
CHEMO
CHEMOTRAZENDO
CHEMOTRAZ
ERNegativePositive
Po
siti
veN
egat
ive
HE
R2

clinicaloptions.com/oncologyTranslational Research 2012
Why This Pragmatic View Fails . . .
Early breast cancer is much more complex than we thought
MBC is much more complex than early breast cancer

clinicaloptions.com/oncologyTranslational Research 2012
Somatic Rearrangement in Breast Cancer Genomes 24 primary breast cancers
– Each show unique pattern of DNA rearrangements
No recurrent rearrangement identified
Basal breast cancers (and some others) were genetically chaotic
– Nature, 2009
Stephens PJ, et al. Nature. 2009;462:1005-1010.
clinicaloptions.com/oncologyTranslational Research 2012
Mutational Evolution in a Lobular Breast Tumor Primary breast cancer had 5 mutations (and
subpopulations with an additional 6 mutations)
At relapse 9 yrs later, this cancer had 32 mutations
None of these 32 mutations were seen in a panel of 192 breast cancers (ie, every cancer is unique)
– Nature 2009
Shah SP, et al. Nature. 2009;461:809-813.

clinicaloptions.com/oncologyTranslational Research 2012
Challenge of Intratumor Heterogeneity
Solid tumors are heterogeneous and evolve to metastasize and evade drug therapy
Intratumoral heterogeneity presents substantial challenges to individualizing treatment
– N Engl J Med, 2012
Gerlinger M, et al. N Engl J Med. 2012;366:889-892.

clinicaloptions.com/oncologyTranslational Research 2012
Single Cancer’s Family Tree: Phylogenetic Relationships of Tumor Regions
UbiquitousShared primaryShared metastasisPrivate
Normal tissue
VHL
KDM5C (missense and frameshift)mTOR (missense)
SETD2 (frameshift)
SETD2 (missense)KDM5C (splice site)
SETD2 (splice site)
?
PreM
R4a
R4b
PreP
R9 R8R2R1
R3R5
M2bM1
M2a

clinicaloptions.com/oncologyTranslational Research 2012
Breast Cancer: The Problem
Every breast cancer is genetically unique
Each tumor represents multiple evolving clones
We need to reduce this complexity!
What are the commonalities?

clinicaloptions.com/oncologyTranslational Research 2012
Growth factor self-sufficiency
Hanahan D, et al. Cell. 2000;100:57-70.
Cancer
Insensitivity to anti-growth signals
Evading apoptosis
Tissue invasion and metastasis
Sustained angiogenesis
Limitless replication potential
Hallmarks of Malignancy

How Do Current Standard Adjuvant Therapies Address
the Problem?

clinicaloptions.com/oncologyTranslational Research 2012
Growth factor self-sufficiency
Hanahan D, et al. Cell. 2000;100:57-70.
Cancer
Insensitivity to antigrowth
signalsEvading apoptosis
Tissue invasion and metastasis
Sustained angiogenesis
Limitless replication potential
Trastuzumab, aromatase inhibitors, tamoxifen
Taxanes
Trastuzumab
Standard Adjuvant Therapy in Breast Cancer

clinicaloptions.com/oncologyTranslational Research 2012
Addressing Replication With Cytotoxic Chemotherapy We have reached a plateau: TAC = ddAC-P
“New” cytotoxics have not improved outcomes in breast cancer
– Capecitabine, vinorelbine, gemcitabine of no proven benefit

clinicaloptions.com/oncologyTranslational Research 2012
Addressing the Hallmark of Growth Factor Self-Sufficiency HER2-directed therapies
– State of the art
– On the horizon

clinicaloptions.com/oncologyTranslational Research 2012
HER2-Positive Breast Cancer
Decision of adjuvant therapy depends on
– Optimal efficacy
– Optimal safety
– Optimal quality of life
– Which regimen has best risk-to-benefit ratio?

clinicaloptions.com/oncologyTranslational Research 2012
NCCTG N9831
1 yr of trastuzumab
4 × AC 12 × paclitaxel 90 mg/m2
HER2+
NSABP B-31
HER2+
1 yr of trastuzumab
4 × AC 4 × paclitaxel 175 mg/m2HERA
2 yrs of trastuzumab
HER2+(IHC or FISH)
Accepted CT:AC, EC, FAC, FEC, ET, AT,
CMF
1 yr of trastuzumab
Observation
BCIRG 006
HER2+
4 × AC60/600 mg/m2
4 × docetaxel100 mg/m2
6 × T and platinum salts75 mg/m2 75 mg/m2 or AUC 6
1 yr of trastuzumab
N = 32221 yr of trastuzumab
AC → T
AC → TH
TCH
(IHC or FISH)
(IHC or FISH)
(FISH)
4 Positive Adjuvant Trastuzumab Trials

clinicaloptions.com/oncologyTranslational Research 2012
Trastuzumab: Safety
Only incremental safety concern is cardiotoxicity
FDA has reviewed each of the registration trials source documentation and recalculated CHF rates using standardized criteria

clinicaloptions.com/oncologyTranslational Research 2012
FDA product monograph, May 2008.
Study, % Trastuzumab Control
B-31/NCCTG 2 0.4
HERA 2 0.3
BCIRG 006
AC → TH 2 0.4
TCH 0.4 0.4
Incidence of CHF in Adjuvant Breast Cancer Studies
clinicaloptions.com/oncologyTranslational Research 2012
Sequential Trastuzumab Is Inferior to Concurrent Trastuzumab NCCTG N9831 phase III study
Treatment: AC followed by
– Paclitaxel
– Paclitaxel plus sequential trastuzumab
– Paclitaxel plus concurrent trastuzumab
DFS superior at 5 yrs with concurrent trastuzumab
– 80.1% with sequential vs 84.4% with concurrent
Perez EA, et al. J Clin Oncol. 2011;29:4491-4497.

clinicaloptions.com/oncologyTranslational Research 2012
What Regimen Provides the BestRisk-to-Benefit Ratio?
TCH

clinicaloptions.com/oncologyTranslational Research 2012
4 × AC60/600 mg/m2
4 × T100 mg/m2
6 × T and carboplatin75 mg/m2 AUC 6
1 yr of trastuzumab
N = 3222
1 yr of trastuzumab
AC → T
AC → TH
TCH
HER2+(central FISH)
N+ or high risk N-
4 × AC60/600 mg/m2
4 × T100 mg/m2
Stratified by nodes and HRS
Slamon D, et al. SABCS 2009. Abstract 62.
Phase III BCIRG 006 Trial: Adjuvant Trastuzumab in HER2+ Breast Cancer

clinicaloptions.com/oncologyTranslational Research 2012
Slamon D, et al. N Engl J Med. 2011;365:1273-1283.
100
80
60
40
20
00 12 24 36 48 60 72 84
Mos
DF
S (
%)
AC-T plustrastuzumab
TCHAC-T
93
8781
88
78
86
75
849287 84 81
BCIRG 006 Trial of Adjuvant Trastuzumab in HER2+ Breast Cancer: 5-Yr DFS

clinicaloptions.com/oncologyTranslational Research 2012
BCIRG 006 Trial of Adjuvant Trastuzumab in HER2+ Breast Cancer: Grade 3/4 AEsAE, % AC-T
(n = 1050)AC-TH
(n = 1068)TCH
(n = 1056)
Arthralgia 3.2 3.3 1.4*
Myalgia 5.2 5.2 1.8*
Fatigue 7.0 7.2 7.2
Hand-foot syndrome 1.9 1.9 0.0*
Stomatitis 3.5 2.9 1.4*
Diarrhea 3.0 5.6 5.4
Nausea 5.9 5.7 4.8
Vomiting 6.2 6.7 3.5*
Irregular menses 27.0 24.3 26.5
*Statistically significant AC-TH vs TCH.
Slamon D, et al. N Engl J Med. 2011;365:1273-1283.

clinicaloptions.com/oncologyTranslational Research 2012
Adjuvant Trastuzumab in HER2+ Breast Cancer: Grade 3/4 Hematologic AEsAE, % AC-T
(n = 1050)AC-TH
(n = 1068)TCH
(n = 1056)
Neutropenia 63.3 71.5 65.9
Leucopenia 51.8 60.3 48.2*
Febrile neutropenia 9.3 10.9 9.6*
Neutropenic infection 11.1 11.9* 11.2
Anemia 2.4 3.1* 5.8
Thrombocytopenia 1.6 2.1 6.1
Leukemia, n (%) 6 pts (0.6) 1 pt (0.1) 1 pt (0.1)
*Statistically significant AC-TH vs TCH.
Slamon D, et al. N Engl J Med. 2011;365:1273-1283.

clinicaloptions.com/oncologyTranslational Research 2012
Slamon D, et al. N Engl J Med. 2011;365:1273-1283.
Adjuvant Trastuzumab in HER2+ Breast Cancer: Mean LVEF Changes Favor TCH
66
65
62
61
59
00 12 24 36 48
Mea
n L
VE
F (
%)
Mos Since Randomization
64
63
60
58
AC-TH (n = 1042)
TCH (n = 1030)
AC-T (n = 1014)

clinicaloptions.com/oncologyTranslational Research 2012
Clinical Event, n (%) AC-T AC-TH TCH
Distant recurrence 188 124 144
Grade 3/4 CHF 7 21 4
Acute leukemia 6 1 1
Total 201 146 149
Slamon D, et al. N Engl J Med. 2011;365:1273-1283.
Adjuvant Trastuzumab in HER2+ Breast Cancer: Risk-to-Benefit Ratio

clinicaloptions.com/oncologyTranslational Research 2012
State-of-the-Art Adjuvant Therapy for HER2+ Early Stage Breast Cancer Nonanthracycline TCH regimen has the most favorable
risk-to-benefit ratio
– Exploits synergistic interaction
– Avoids cardiotoxicity
– No leukemogenicity
– Superior efficacy to sequential trastuzumab strategies
– Equivalent efficacy to anthracycline/trastuzumab/taxane combinations
– Better quality of life (Au, et al.; submitted)

clinicaloptions.com/oncologyTranslational Research 2012
What Is on the Horizon for HER2+ Early Breast Cancer? Biology informs the new adjuvant trials
Trastuzumab predominantly restores sensitivity to apoptosis
Lapatinib primarily reduces proliferation
Synergy between trastuzumab and lapatinib
Synergy between trastuzumab and pertuzumab
HER2 amplification increases VEGF production

clinicaloptions.com/oncologyTranslational Research 2012
NucleusNucleus
RbRb myc
maxmyc
max
PI3KPI3K
HER2HER2
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
CyclinsCyclinsCyclinsCyclins
CdksCdksCdksCdks
p27p27//p16p16p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
VEGFVEGFVEGFVEGF
HER2 Amplification Drives Proliferation
HER2HER2

clinicaloptions.com/oncologyTranslational Research 2012
NucleusNucleus
RbRb myc
maxmyc
max
PI3KPI3K
HER2HER2
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
cyclinscyclinscyclinscyclins
Cdk’sCdk’sCdk’sCdk’s
p27p27//p16p16p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
VEGFVEGFVEGFVEGF
HER2 Amplification Suppresses Apoptosis
HER2HER2

clinicaloptions.com/oncologyTranslational Research 2012
NucleusNucleus
RbRb myc
maxmyc
max
PI3KPI3K
HER2HER2
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
cyclinscyclinscyclinscyclins
Cdk’sCdk’sCdk’sCdk’s
p27p27//p16p16p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
HER2HER2
Chang J, et al. SABCS 2008.

clinicaloptions.com/oncologyTranslational Research 2012
Growth factorsGrowth factors
NucleusNucleus
RbRb myc
maxmyc
max
PI3KPI3K
HER2HER2HER 1,3,4HER 1,3,4
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
cyclinscyclinscyclinscyclins
Cdk’sCdk’sCdk’sCdk’s
p27p27//p16p16p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
Chang J, et al. SABCS 2008.

clinicaloptions.com/oncologyTranslational Research 2012
Trastuzumab 4 mg/kg IV (loading dose) → 2 mg/kg once wkly
× 11 wks ±Paclitaxel 80 mg/m2
IV once wkly × 12 wks
ClinicalTrials.gov. NCT00490139.
ALTTO Phase III Study: Lapatinib ± Trastuzumab in HER2+ Breast Cancer
Women withcentrally
determinedHER2+
invasive breastcancer
(N = 8000planned)
Surgery, (neo)
adjuvant anthracycline
-based therapy for 4 cycles; LVEF ≥ 50
Trastuzumab 8 mg/kg IV (loading dose) → 6 mg/kg every 3 wks for 1 yr ±
Paclitaxel 80 mg/m2 IV once wkly × 12 wks
Lapatinib 1500 mg/kg PO QD× 51 wks ±Paclitaxel 80 mg/m2 IV once wkly × 12 wks
Trastuzumab 8 mg/kg (loading dose) → 6 mg/kg every 3 wks for 1 yr
Lapatinib 1000 mg PO QD × 51 wks ±Paclitaxel 80 mg/m2 IV once wkly × 12 wks
Lapatinib 1500 mg orally QD ×
34 wks
6-wkwash-out

clinicaloptions.com/oncologyTranslational Research 2012
NucleusNucleus
RbRb myc
maxmyc
max
PI3KPI3K
HER2HER2HER 1,3,4HER 1,3,4
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
cyclinscyclinscyclinscyclins
Cdk’sCdk’sCdk’sCdk’s
p27p27//p16p16p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
Growth factorsGrowth factors
clinicaloptions.com/oncologyTranslational Research 2012
NucleusNucleus
RbRb myc
maxmyc
max
PI3KPI3K
HER2HER2HER 1,3,4HER 1,3,4
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
cyclinscyclinscyclinscyclins
Cdk’sCdk’sCdk’sCdk’s
p27p27//p16p16p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
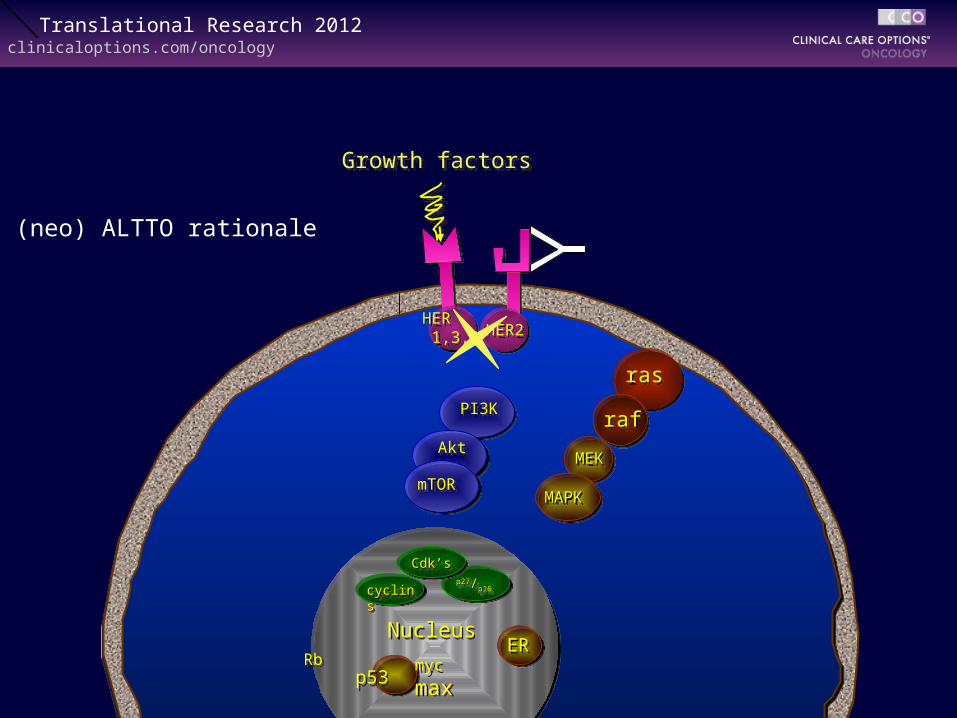
(neo) ALTTO rationale
Growth factorsGrowth factors

clinicaloptions.com/oncologyTranslational Research 2012
ALTTO in Perspective
Promising results in combination arm
– In M1 disease, lapatinib plus trastuzumab active as salvage therapy
– Neoadjuvant potential
Due to pharmacokinetic interaction with paclitaxel, 43% of patients receiving lapatinib/trastuzumab discontinued[1]
1. Hudis, et al. ASCO 2008.2. Dieras V, et al. ASCO 2010. Abstract 1049.

clinicaloptions.com/oncologyTranslational Research 2012
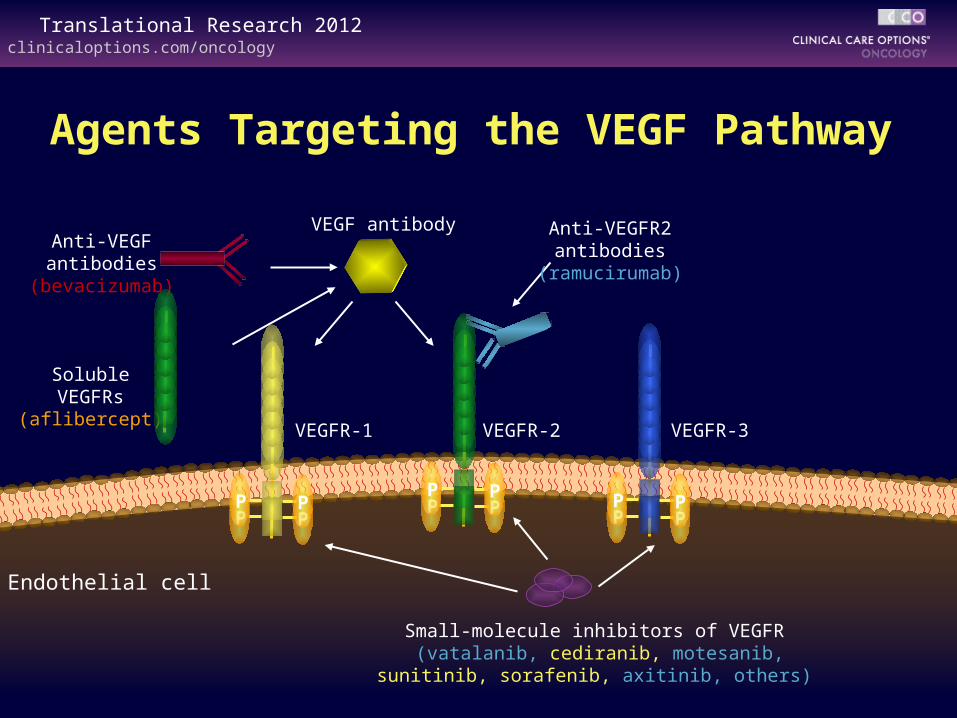
Addressing the Hallmark of Sustained Angiogenesis Angiogenesis: physiologic process of new blood vessel
formation
Principally driven by interactions between VEGFs and 3 high-affinity VEGFRs
clinicaloptions.com/oncologyTranslational Research 2012
VEGFR-3VEGFR-2VEGFR-1
Endothelial cell
VEGF antibody
PP
PP P
PPP
PP
PP
Anti-VEGFantibodies
(bevacizumab)
Anti-VEGFR2antibodies
(ramucirumab)
Small-molecule inhibitors of VEGFR (vatalanib, cediranib, motesanib,
sunitinib, sorafenib, axitinib, others)
SolubleVEGFRs
(aflibercept)
Agents Targeting the VEGF Pathway

clinicaloptions.com/oncologyTranslational Research 2012
Antiangiogenic Agents: Class Toxicities
Hypertension
Clotting
Bleeding
CHF (when combined with anthracyclines)
Financial
Agent-specific toxicities
– Motesanib: cholecystitis
– Sunitinib, pazopanib: pigmentation changes
– Tyrosine kinase inhibitors: fatigue

clinicaloptions.com/oncologyTranslational Research 2012
Ramucirumab
Fully humanized antibody directed against VEGFR2
Potential for immune-mediated destruction of angiogenic vessels
Circumvents insoluble VEGF activation of VEGFR2

clinicaloptions.com/oncologyTranslational Research 2012
TRIO-012 Ramucirumab Study
Patient population
– Women with HER2-negative, unresectable, locally recurrent, or MBC with or without measurable lesions
– No previous chemotherapy for metastatic or locally recurrent and inoperable breast cancer
Study plan
RA
ND
OM
IZA
TIO
N
Follow-up
Progressivedisease
or unacceptable
toxicityor
withdrawnconsent
Docetaxel 75 mg/m² IV q3w
Blinded ramucirumab 10 mg/kg IV q3w
…..
…..
2/3
1/3Docetaxel 75 mg/m² IV q3w
Blinded placebo IV q3w
Mackey J, et al. Clin Breast Cancer. 2009;9:258-261.

Adjuvant Antiangiogenic Therapy?

clinicaloptions.com/oncologyTranslational Research 2012
HER2 Biology
NucleusNucleus
PI3KPI3K
HER2HER2HER 1,3,4HER 1,3,4
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
AktAkt
mTORmTOR
Sur
viva
l
Prol
ifera
tion VEGFVEGFVEGFVEGF
Growth factorsGrowth factors

clinicaloptions.com/oncologyTranslational Research 2012
BETH: Bevacizumab With Trastuzumab Adjuvant Therapy in HER2+ Breast Cancer CIRG/TRIO 011: phase III translational study (planned
N = 3509) based on the following
– Adjuvant trastuzumab is effective
– Preclinical observations that HER2 transfection leads to VEGF overexpression and increased angiogenesis
– HER2 and VEGF are independent prognostic factors
– Clinical efficacy of the 2 antibodies trastuzumab and bevacizumab from phase I and II studies
– The ability to add bevacizumab to the noncardiotoxic backbone (TCH) from the BCIRG 006 study
– Averel trial showed efficacy of this combination in MBC
Fully accrued, results expected in 2013ClinicalTrials.gov. NCT00625898.

clinicaloptions.com/oncologyTranslational Research 2012
Growth factor
Growth factor
NucleusNucleusRbRb myc
maxmyc
max
PI3KPI3K
HER2HER2HER1,3,4HER1,3,4
rasras
rafraf
MEKMEKMEKMEK
MAPKMAPKMAPKMAPK
cyclinscyclinscyclinscyclins
Cdk’sCdk’sCdk’sCdk’sp27p27//p16p16
p27p27//p16p16
ERER
p53p53
AktAkt
mTORmTOR
VEGFVEGFVEGFVEGF
BETH Phase III Study of Trastuzumab + Bevacizumab in Breast Cancer: Rationale

clinicaloptions.com/oncologyTranslational Research 2012
6 × TC
1 yr of trastuzumab
TCHB(Group 1B)
1 yr of bevacizumab
RT
6 × TC
1 yr of trastuzumab
TCH(Group 1A) RT
BETH Phase III Study: Chemotherapy + Trastuzumab ± Bevacizumab
Primary endpoint: IDFS
Secondary endpoints: DFS, OS, RFI, DRFI, toxicity
HER2+, N+, or high-risk N-
Stratified by Ns and HRS
(N ~ 3500)
ClinicalTrials.gov. NCT00625898.

clinicaloptions.com/oncologyTranslational Research 2012
Take-Home Messages: HER2+ Research
New approaches in the adjuvant setting
– Double-hit HER2 pathway (ALLTO; APHINITY)
– Inhibit both HER2 and angiogenesis (BETH)
TRIO is launching new trials exploring synergistic agents
– TRIO 016: panobinostat (HDAC inhibitor)
– TRIO 019: everolimus (mTOR inhibitor)
– TRIO 0xx: T-DM1

How Are Ongoing Adjuvant Trials Addressing the Problem?

clinicaloptions.com/oncologyTranslational Research 2012
Growth factor self-sufficiency
Hanahan D, et al. Cell. 2000;100:57-70.
Cancer
Insensitivity to antigrowth
signalsEvading apoptosis
Tissue invasion and metastasis
Sustained angiogenesis
Limitless replication potential
Lapatinib, neratinib, pertuzumab, T-DM1
BevacizumabDenosumab
EverolimusMetformin
Hallmarks of Malignancy

What Will Future Adjuvant Therapies Look Like?

clinicaloptions.com/oncologyTranslational Research 2012
Growth factor self-sufficiency
Cancer
Insensitivity to antigrowth
signalsEvading apoptosis
Tissue invasion and metastasis
Sustained angiogenesis
Limitless replication potential
Src inhibitors, PI3K/Akt inhibitorsT-DM1, lapatinib
DenosumabAnti-integrin therapies
ASA
Telomerase inhibitors
PARP inhibitorsRb inhibitors
Dichloroacetate
RamucirumabBevacizumab
Physical exerciseMetforminEverolimusEntinostat
My Predictions for Adjuvant Therapy

clinicaloptions.com/oncologyTranslational Research 2012
Breast cancer
– A collection of multiple clones of malignant cells with divergent genotypes and phenotypes expected to demonstrate Darwinian evolution under the selection pressure of systemic therapy
The Molecular Reality of Breast Cancer

clinicaloptions.com/oncologyTranslational Research 2012
Prediction-Based Adjuvant Treatment Algorithm Molecular diagnosis (full genome, epigenome, and
quantitative transcriptome sequencing)
– Bioinformatic identification of post-alteration targets
Pick from the menu: “à la carte” hallmark inhibitors
Iteration: on relapse and after each progression, repeat biopsy and repeat the process

clinicaloptions.com/oncologyTranslational Research 2012
July 1, 2031
Dear Dr. Mackey:
Ultigenomics has determined your patient’s T2N1 primary breast cancer has the following phenotype, and intervention is recommended:
Tumor
– PI3K-activating mutation: PiKtrimicin
– HER2 pathway activation: T-DM1
– Telomerase activation: Tipglu
This will reduce your pt’s estimated 10-yr risk of recurrence from 63% to 4%
Stroma
– VEGFR pathway activation: ramucirumab
– Bone tropism: denosumab

clinicaloptions.com/oncologyTranslational Research 2012
How Do We Get There From Here?

clinicaloptions.com/oncologyTranslational Research 2012
Making Progress . . .
Progress in adjuvant therapy will require greater understanding of disease biology and subsequent development of targeted therapies
Ongoing and planned adjuvant trials are likely to make major improvements in breast cancer survival—please discuss participation with your patients
Please contribute to the design and conduct of biology-based breast cancer trials

clinicaloptions.com/oncologyTranslational Research 2012
Take-Home Messages
Every breast cancer is genetically unique
MBCs are more complex than primary breast cancers
Breast cancer is heterogeneous and evolves in response to treatment – we are pitted against Darwinian selection
There are commonalities among this complexity
Understanding the molecular biology of a specific breast cancer informs treatment in 2012

Go Online for More CCO Coverage of Chicago 2012!
Capsule Summaries of all the key data, plus CME-certified Slidesets exploring the clinical implications of these findings
Downloadable slides: for use as a study resource or in your noncommericial presentations
clinicaloptions.com/oncology