cco melanoma
TRANSCRIPT

Targeted Therapy for BRAF V600–Mutant Melanoma
This program is supported by educational grants from
in association with
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
About These Slides
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
Faculty
Keith T. Flaherty, MDDirector of Temeer Center for Targeted TherapyMassachusetts General Hospital Cancer CenterBoston, Massachusetts
Keith T. Flaherty, MD has disclosed that he has received consulting fees from GlaxoSmithKline, Novartis, and Roche/Genentech.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
Incidence of Key Driver Oncogenes in Melanoma BRAF ~ 50%
NRAS ~ 20%
CKIT ~ 1%
– Primarily mucosal and acral lentiginous
GNAQ/GNA11 ~ 1%
– Almost exclusively uveal
Nikolaou VA, et al. J Invest Dermatol. 2012;132:854-863. Smalley KS, et al. Semin Oncol. 2012;39:204-214.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
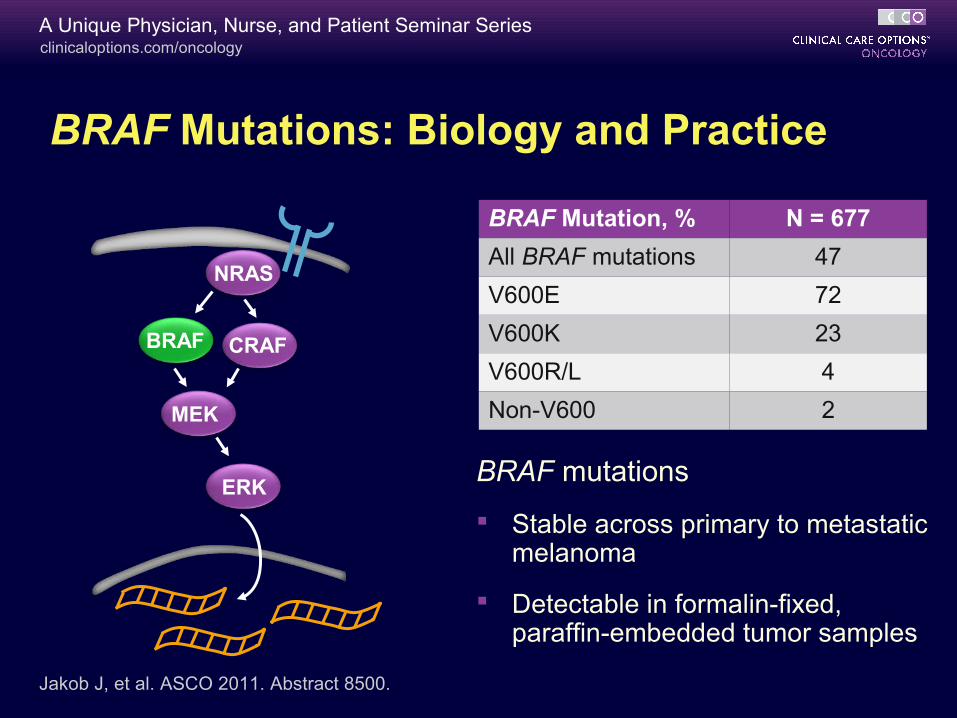
BRAF Mutations: Biology and Practice
BRAF mutations
Stable across primary to metastatic melanoma
Detectable in formalin-fixed, paraffin-embedded tumor samples
BRAF Mutation, % N = 677
All BRAF mutations 47
V600E 72
V600K 23
V600R/L 4
Non-V600 2
Jakob J, et al. ASCO 2011. Abstract 8500.
NRAS
CRAFBRAF
MEK
ERK
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
BRAF Mutation Testing
BRAF mutations are present throughout melanoma disease progression
– If metastasis biopsy not available, most recent melanoma surgery sample adequate (eg, lymph node)
BRAF mutation testing is commercially available
– FDA-approved tests
– Cobas 4800 BRAF V600 Mutation Test (vemurafenib)
– THxID BRAF Kit (dabrafenib with or without trametinib)
NCCN. Clinical practice guidelines in oncology: melanoma. v.1.2014.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
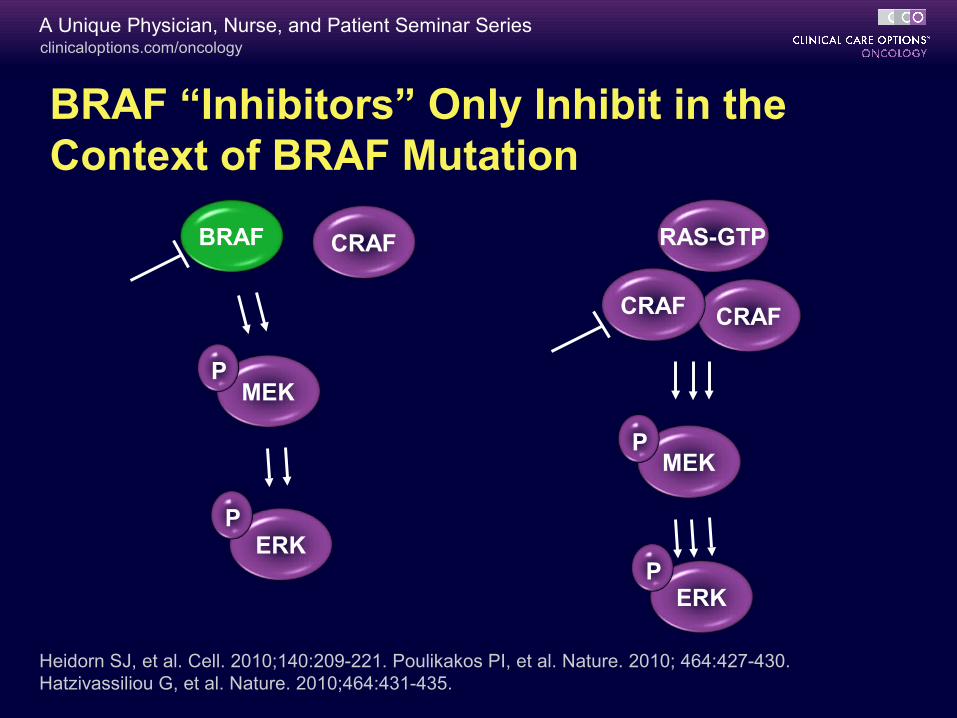
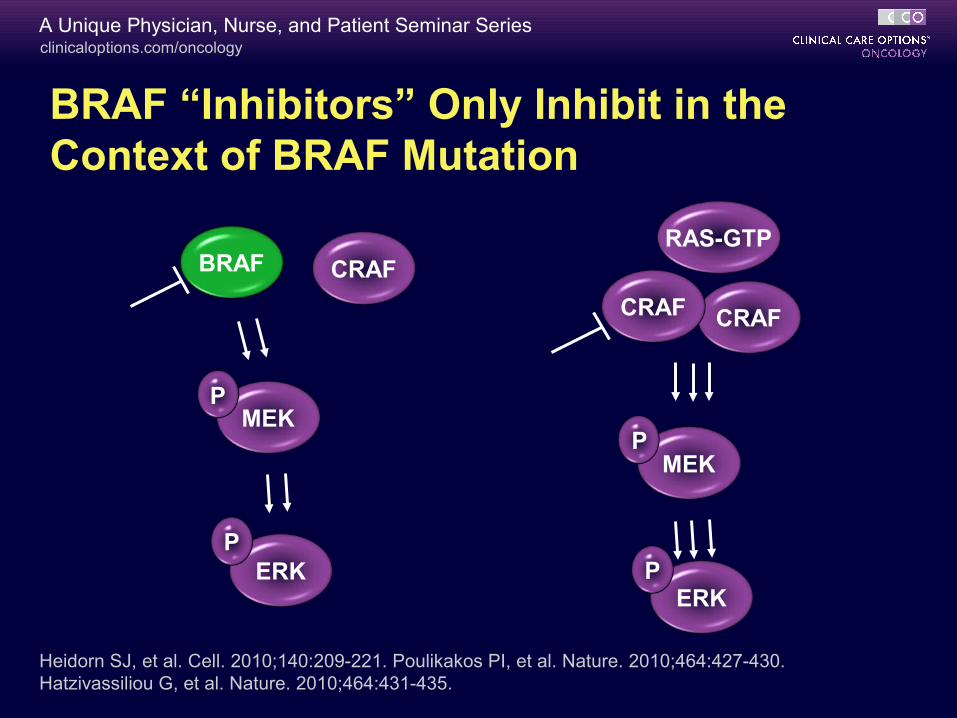
BRAF “Inhibitors” Only Inhibit in the Context of BRAF Mutation
CRAFBRAF
MEK
ERK
P
P
CRAF
MEK
ERK
P
P
CRAF
Heidorn SJ, et al. Cell. 2010;140:209-221. Poulikakos PI, et al. Nature. 2010; 464:427-430. Hatzivassiliou G, et al. Nature. 2010;464:431-435.
RAS-GTP

clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
BRAF-Mutant Melanoma Initial Therapy
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
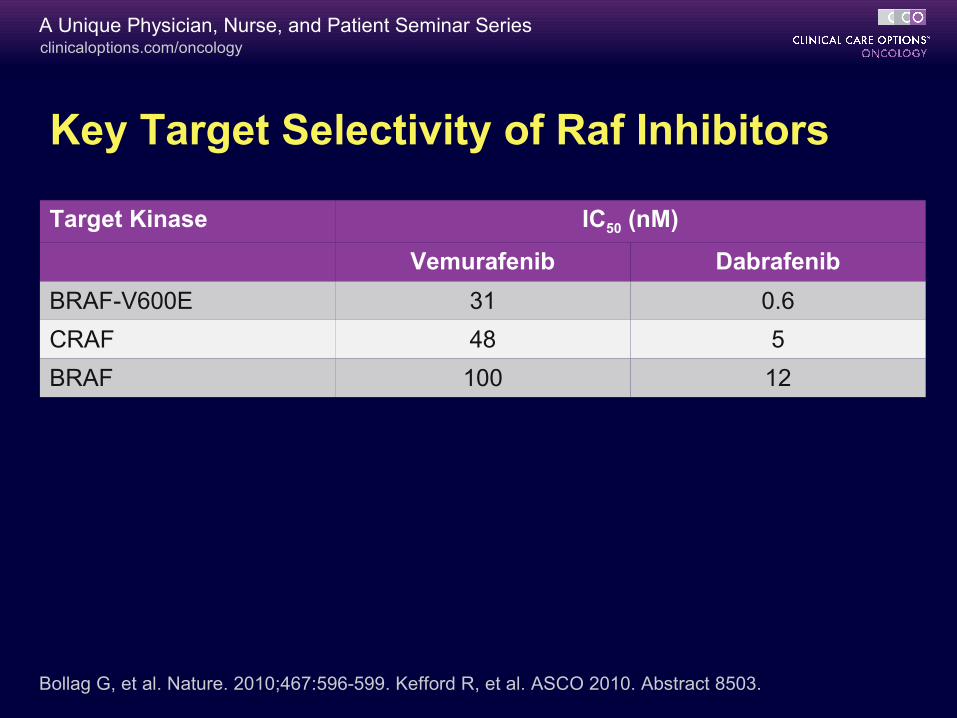
Key Target Selectivity of Raf Inhibitors
Target Kinase IC50 (nM)
Vemurafenib Dabrafenib
BRAF-V600E 31 0.6
CRAF 48 5
BRAF 100 12
Bollag G, et al. Nature. 2010;467:596-599. Kefford R, et al. ASCO 2010. Abstract 8503.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
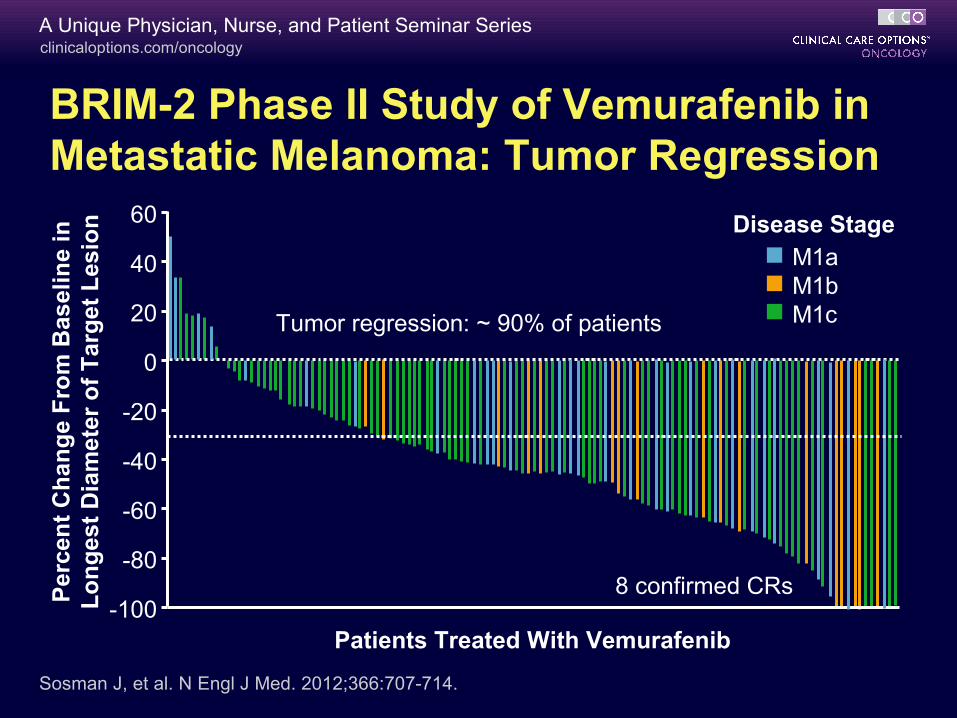
Sosman J, et al. N Engl J Med. 2012;366:707-714.
Tumor regression: ~ 90% of patients
8 confirmed CRs
BRIM-2 Phase II Study of Vemurafenib in Metastatic Melanoma: Tumor Regression
60
40
20
0
-20
-40
-60
-80
-100
Per
cen
t C
han
ge
Fro
m B
asel
ine
in
Lo
ng
est
Dia
met
er o
f T
arg
et L
esio
n
Patients Treated With Vemurafenib
Disease StageM1aM1bM1c
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
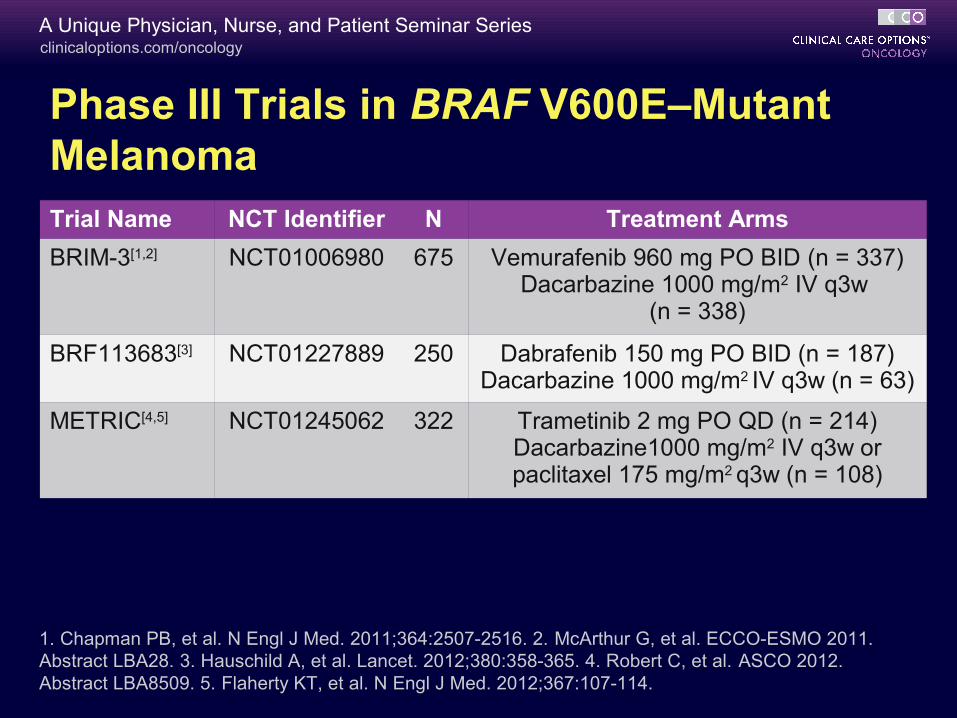
1. Chapman PB, et al. N Engl J Med. 2011;364:2507-2516. 2. McArthur G, et al. ECCO-ESMO 2011. Abstract LBA28. 3. Hauschild A, et al. Lancet. 2012;380:358-365. 4. Robert C, et al. ASCO 2012. Abstract LBA8509. 5. Flaherty KT, et al. N Engl J Med. 2012;367:107-114.
Phase III Trials in BRAF V600E–Mutant MelanomaTrial Name NCT Identifier N Treatment Arms
BRIM-3[1,2] NCT01006980 675 Vemurafenib 960 mg PO BID (n = 337)Dacarbazine 1000 mg/m2 IV q3w
(n = 338)
BRF113683[3] NCT01227889 250 Dabrafenib 150 mg PO BID (n = 187)Dacarbazine 1000 mg/m2 IV q3w (n = 63)
METRIC[4,5] NCT01245062 322 Trametinib 2 mg PO QD (n = 214)Dacarbazine1000 mg/m2 IV q3w or paclitaxel 175 mg/m2 q3w (n = 108)
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
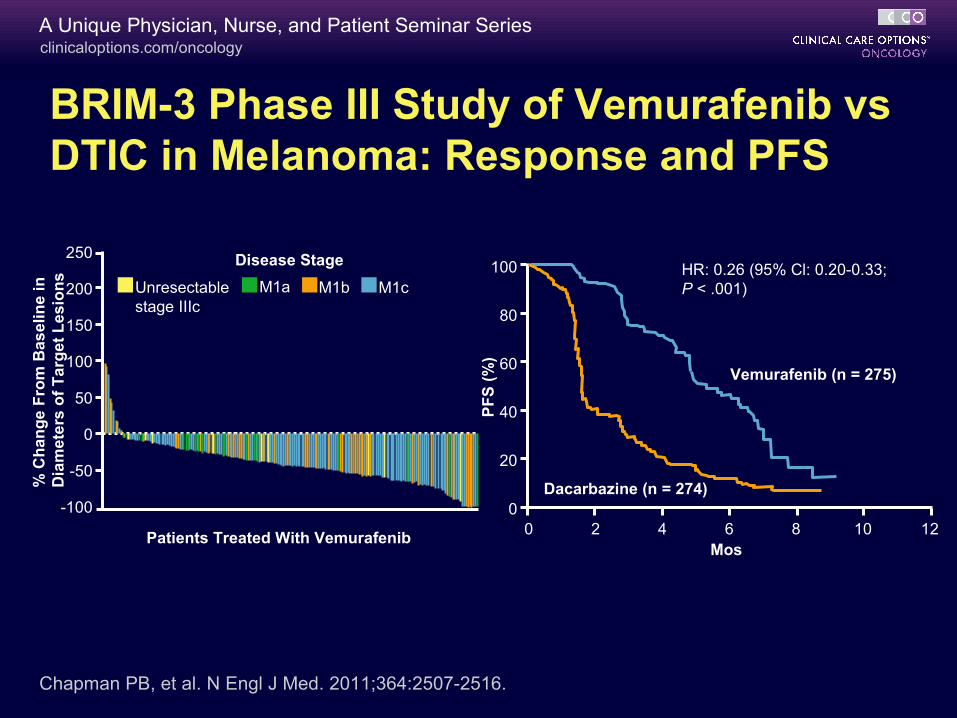
Chapman PB, et al. N Engl J Med. 2011;364:2507-2516.
250
200
150
100
50
0
-50
-100
% C
ha
ng
e F
rom
Ba
se
lin
e i
n
Dia
me
ters
of
Ta
rge
t L
es
ion
s
Patients Treated With Vemurafenib
Unresectable stage IIIc
M1a M1b M1c
Disease Stage 100
80
60
40
20
00 2 4 6 8 10 12
Mos
PF
S (
%)
HR: 0.26 (95% Cl: 0.20-0.33; P < .001)
Vemurafenib (n = 275)
Dacarbazine (n = 274)
BRIM-3 Phase III Study of Vemurafenib vs DTIC in Melanoma: Response and PFS
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
Mos
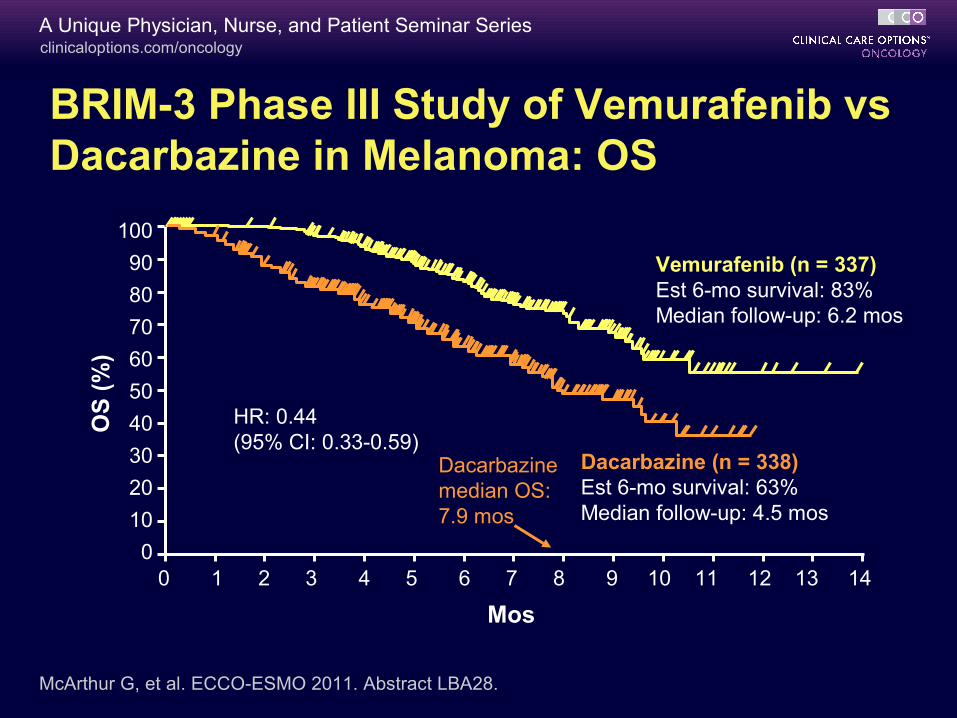
Vemurafenib (n = 337)Est 6-mo survival: 83%Median follow-up: 6.2 mos
Dacarbazine (n = 338)Est 6-mo survival: 63%Median follow-up: 4.5 mos
OS
(%
)
HR: 0.44 (95% CI: 0.33-0.59)
Dacarbazine median OS: 7.9 mos
McArthur G, et al. ECCO-ESMO 2011. Abstract LBA28.
BRIM-3 Phase III Study of Vemurafenib vs Dacarbazine in Melanoma: OS
100
90
80
70
60
50
40
30
20
10
00 1 2 3 4 5 6 7 8 9 10 11 12 13 14
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
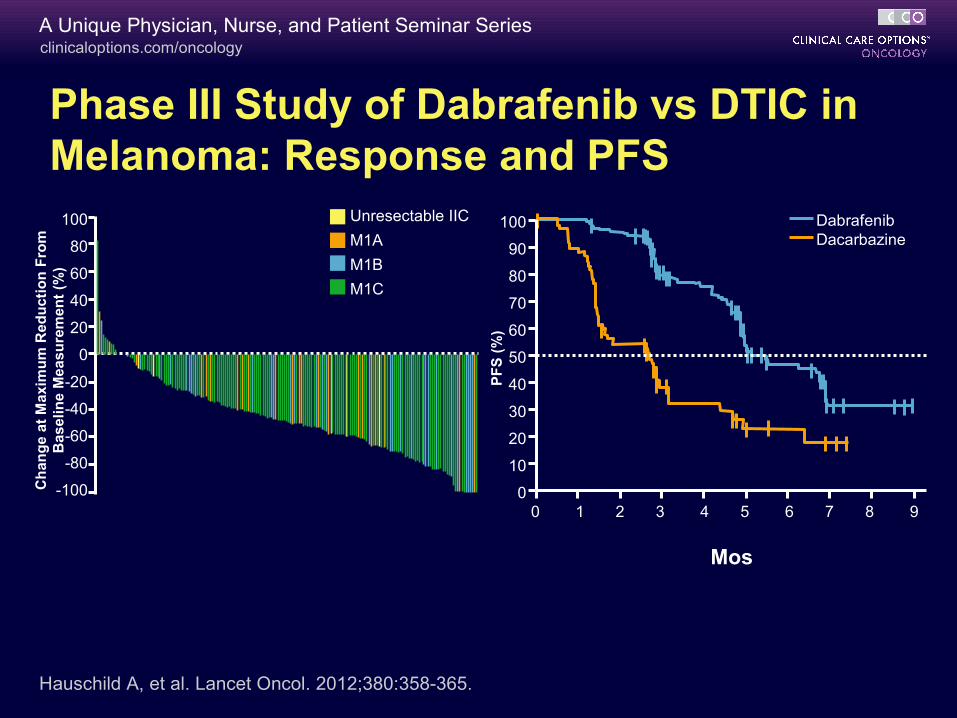
Phase III Study of Dabrafenib vs DTIC in Melanoma: Response and PFS
Hauschild A, et al. Lancet Oncol. 2012;380:358-365.
Unresectable IIC
M1A
M1B
M1C
100
80
60
40
20
0
-20
-40
-60
-80
-100Ch
ang
e at
Max
imu
m R
edu
ctio
n F
rom
B
asel
ine
Mea
sure
men
t (%
)
100
90
80
70
60
50
40
30
20
10
0P
FS
(%
)0 1 2 3 4 5 6 7 8 9
DabrafenibDacarbazine
Mos
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
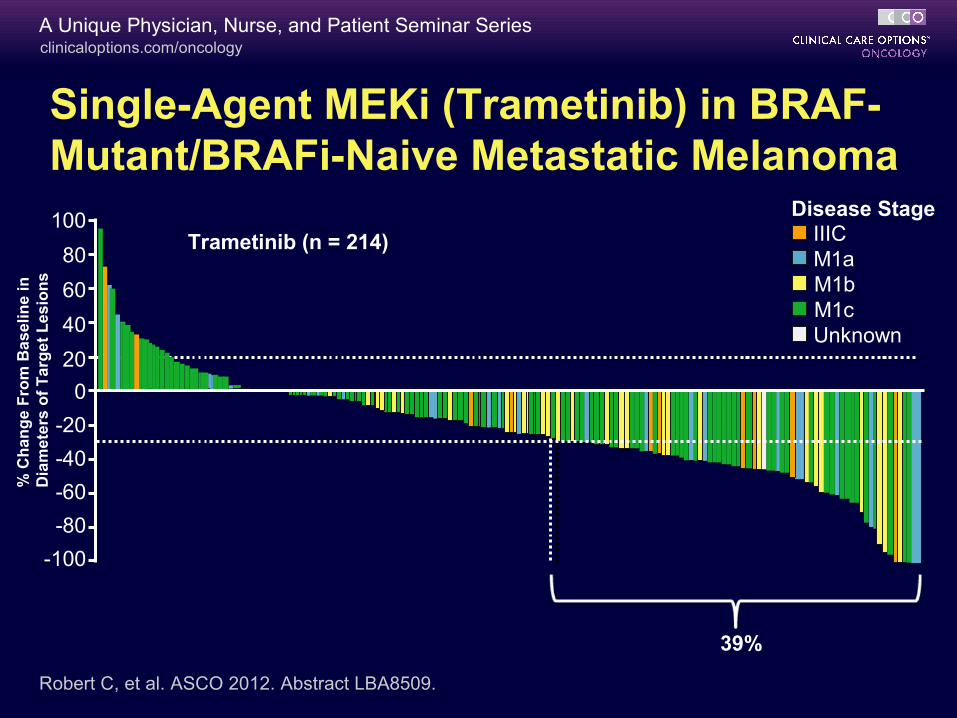
Trametinib (n = 214)
Confirmed RR: 22% (95% CI: 16.6-28.1)
Single-Agent MEKi (Trametinib) in BRAF-Mutant/BRAFi-Naive Metastatic Melanoma
Robert C, et al. ASCO 2012. Abstract LBA8509.
Disease Stage
39%
M1cM1bM1aIIIC
Unknown
100
80
60
40
20
0
-20
-40
-60
-80
-100
% C
ha
ng
e F
rom
Ba
se
lin
e i
n
Dia
me
ters
of
Ta
rge
t L
es
ion
s
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
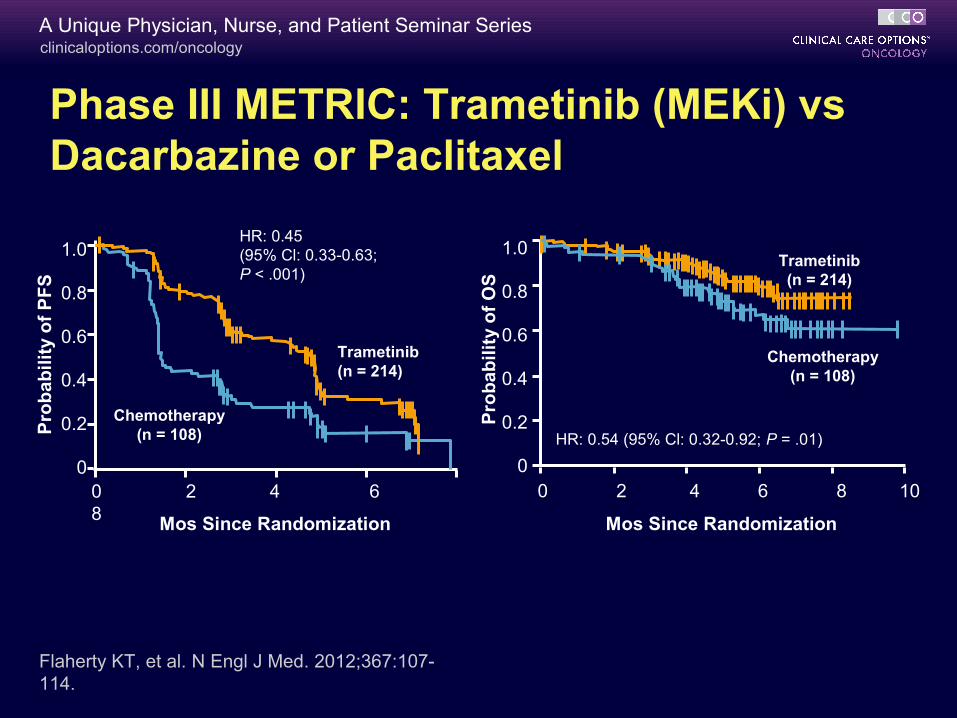
Phase III METRIC: Trametinib (MEKi) vs Dacarbazine or Paclitaxel
Flaherty KT, et al. N Engl J Med. 2012;367:107-114.
1.0
0.8
0.6
0.4
0.2
00 2 4 6 8 Mos Since Randomization
Pro
bab
ilit
y o
f P
FS
HR: 0.45 (95% Cl: 0.33-0.63; P < .001)
Trametinib(n = 214)
Chemotherapy(n = 108)
Pro
bab
ilit
y o
f O
S
1.0
0.8
0.6
0.4
0.2
00 2 4 6 8 10
Trametinib(n = 214)
Chemotherapy(n = 108)
HR: 0.54 (95% Cl: 0.32-0.92; P = .01)
Mos Since Randomization
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
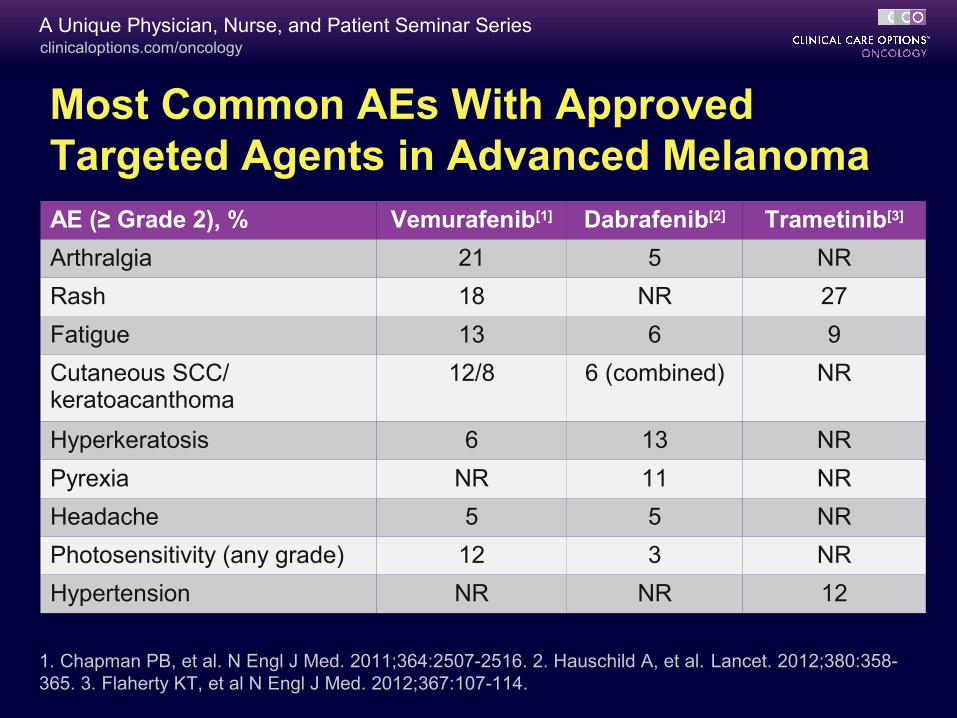
Most Common AEs With Approved Targeted Agents in Advanced MelanomaAE (≥ Grade 2), % Vemurafenib[1] Dabrafenib[2] Trametinib[3]
Arthralgia 21 5 NR
Rash 18 NR 27
Fatigue 13 6 9
Cutaneous SCC/ keratoacanthoma
12/8 6 (combined) NR
Hyperkeratosis 6 13 NR
Pyrexia NR 11 NR
Headache 5 5 NR
Photosensitivity (any grade) 12 3 NR
Hypertension NR NR 12
1. Chapman PB, et al. N Engl J Med. 2011;364:2507-2516. 2. Hauschild A, et al. Lancet. 2012;380:358-365. 3. Flaherty KT, et al N Engl J Med. 2012;367:107-114.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
Vemurafenib + Ipilimumab: Hepatotoxicity
Phase I study in patients with BRAF V600–mutant melanoma
– Dose-limiting grade 3 aminotransferase elevation in 4 pts
– Lowering dose of vemurafenib still produced elevated aminotransferase levels
– Hepatic adverse events asymptomatic and reversible
– Other adverse events of the combination: grade 2 temporal arteritis, grade 3 rash
– Study has been closed to further accrual
Ribas A, et al. N Engl J Med. 2013;368:1365-1366.

clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
Resistance to BRAF Inhibitors
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
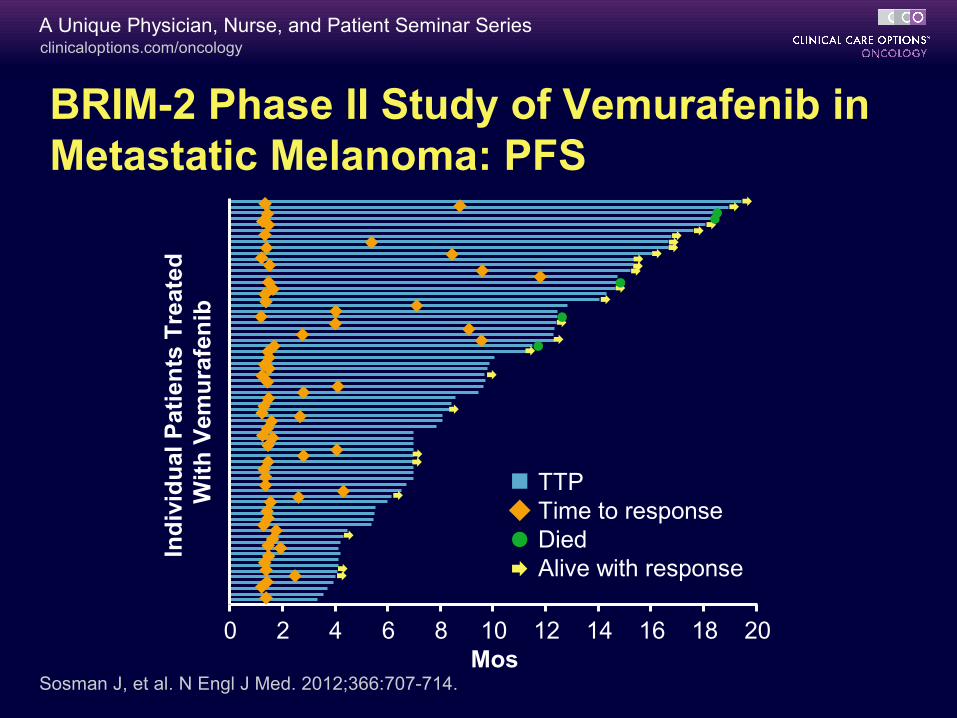
Sosman J, et al. N Engl J Med. 2012;366:707-714.
BRIM-2 Phase II Study of Vemurafenib in Metastatic Melanoma: PFS
Ind
ivid
ual
Pat
ien
ts T
reat
ed
Wit
h V
emu
rafe
nib
TTPTime to responseDiedAlive with response
Mos0 202 4 6 8 10 12 14 16 18
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
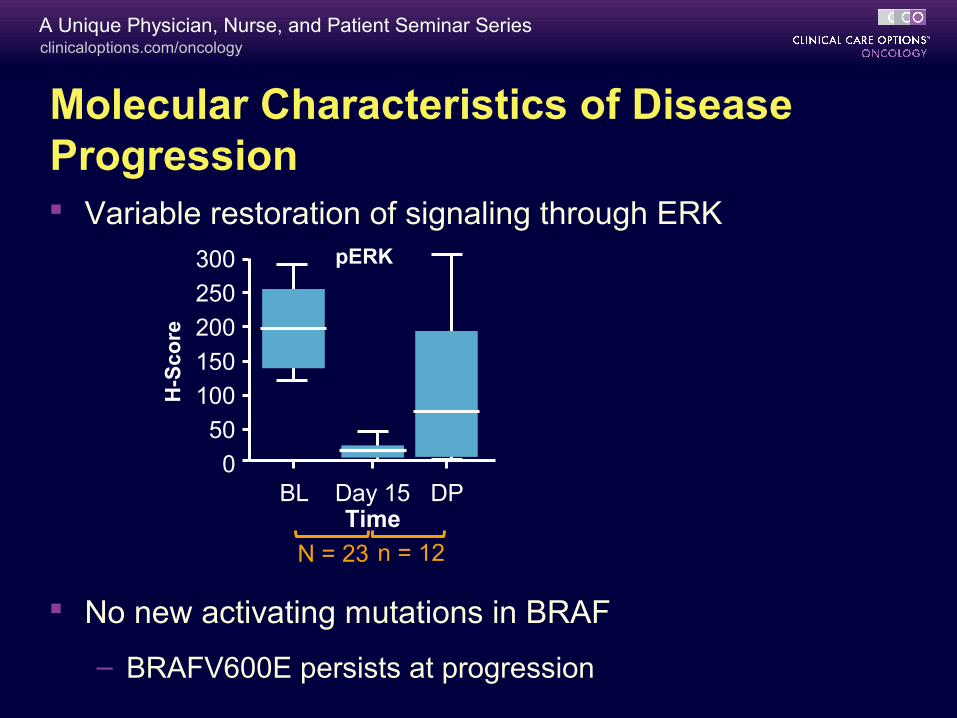
Molecular Characteristics of Disease Progression Variable restoration of signaling through ERK
No new activating mutations in BRAF
– BRAFV600E persists at progression
300
250
200
150
100
50
0
H-S
core
BL Day 15 DP
pERK
Time
N = 23 n = 12
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
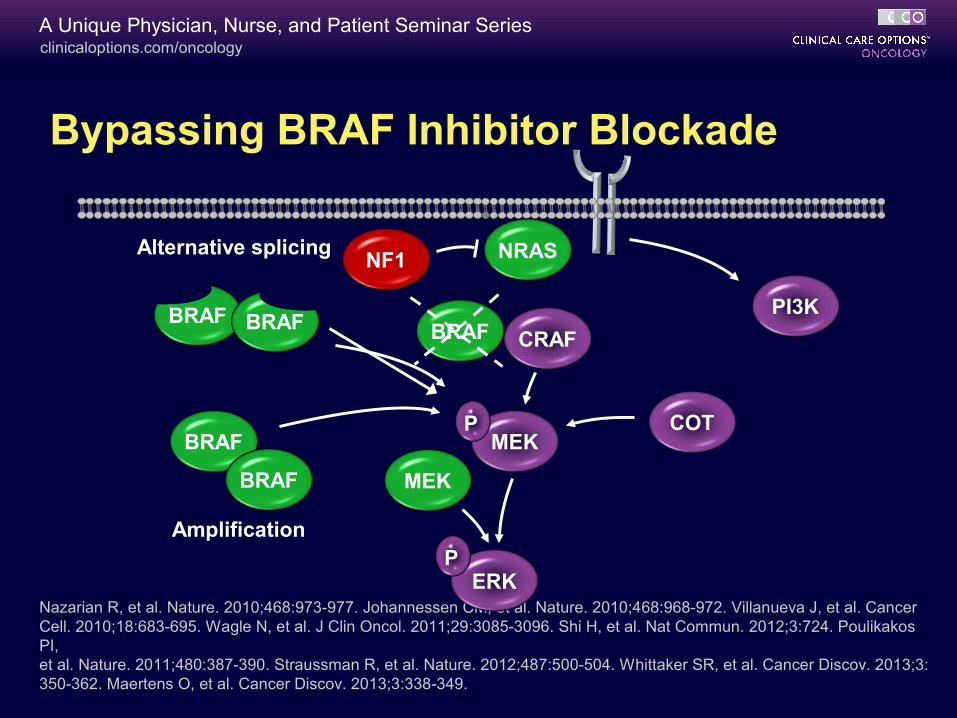
Bypassing BRAF Inhibitor Blockade
Nazarian R, et al. Nature. 2010;468:973-977. Johannessen CM, et al. Nature. 2010;468:968-972. Villanueva J, et al. Cancer Cell. 2010;18:683-695. Wagle N, et al. J Clin Oncol. 2011;29:3085-3096. Shi H, et al. Nat Commun. 2012;3:724. Poulikakos PI, et al. Nature. 2011;480:387-390. Straussman R, et al. Nature. 2012;487:500-504. Whittaker SR, et al. Cancer Discov. 2013;3: 350-362. Maertens O, et al. Cancer Discov. 2013;3:338-349.
CRAFBRAF
MEK
ERK
P
P
BRAF BRAF
BRAF
BRAF
NRAS
COT
MEK
Alternative splicing
Amplification
PI3K
NF1
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
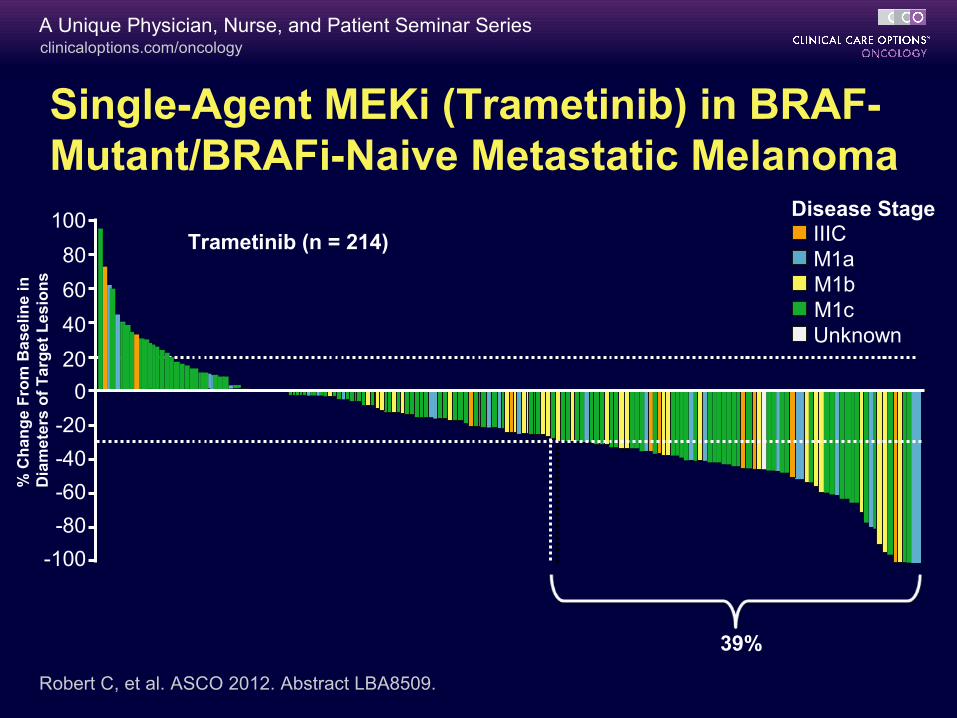
Single-Agent MEKi (Trametinib) in BRAF-Mutant/BRAFi-Naive Metastatic Melanoma
Robert C, et al. ASCO 2012. Abstract LBA8509.
Disease Stage
39%
Trametinib (n = 214)
Confirmed RR: 22% (95% CI: 16.6-28.1)
M1cM1bM1aIIIC
Unknown
100
80
60
40
20
0
-20
-40
-60
-80
-100
% C
ha
ng
e F
rom
Ba
se
lin
e i
n
Dia
me
ters
of
Ta
rge
t L
es
ion
s
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
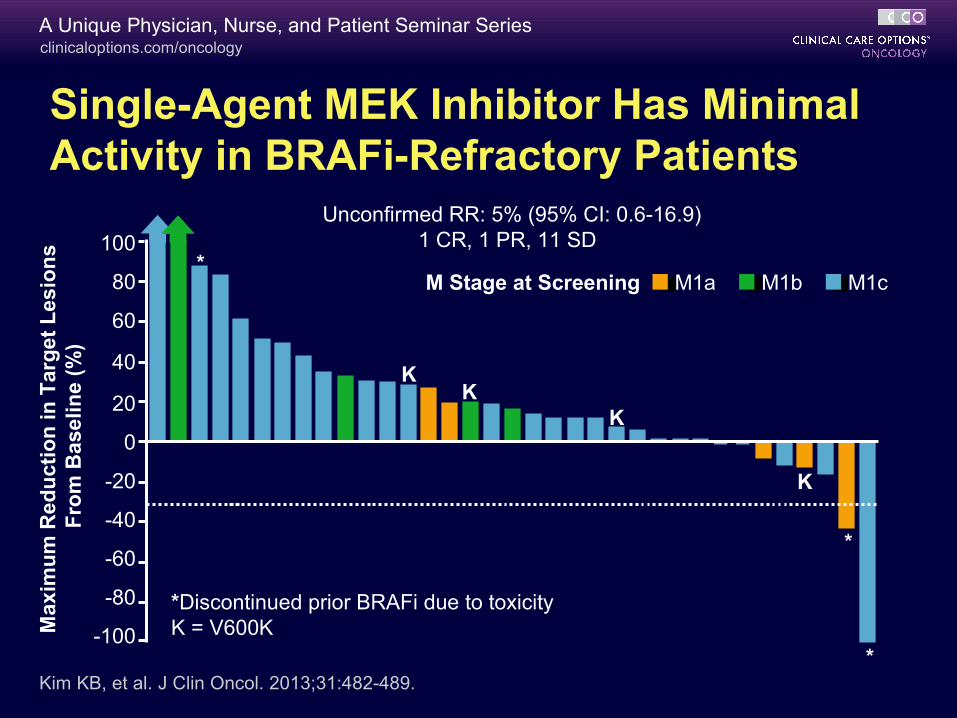
Single-Agent MEK Inhibitor Has Minimal Activity in BRAFi-Refractory Patients
Unconfirmed RR: 5% (95% CI: 0.6-16.9) 1 CR, 1 PR, 11 SD
*Discontinued prior BRAFi due to toxicityK = V600K
M1cM1a M1bM Stage at Screening
KK
K
K
*
Max
imu
m R
edu
ctio
n in
Tar
get
Les
ion
s F
rom
Bas
elin
e (%
)
*
*
Kim KB, et al. J Clin Oncol. 2013;31:482-489.
100
80
60
40
20
0
-20
-40
-60
-80
-100
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
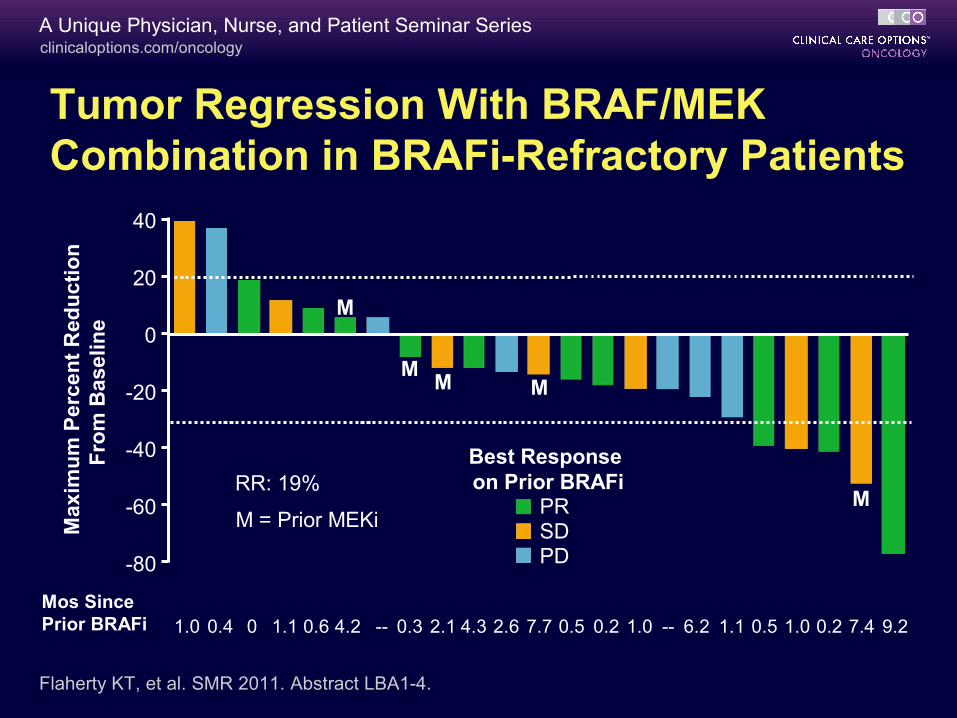
Tumor Regression With BRAF/MEK Combination in BRAFi-Refractory Patients
Max
imu
m P
erce
nt
Red
uct
ion
Fro
m B
asel
ine
Mos Since Prior BRAFi
PRSDPD
Best Response on Prior BRAFiRR: 19%
M = Prior MEKi
Flaherty KT, et al. SMR 2011. Abstract LBA1-4.
--80
--60
--40
--20
0
20
40
1.0 0.4 0 0.6 4.2 -- 0.3 2.1 4.3 2.6 7.7 0.5 0.2 1.0 -- 6.2 0.5 1.0 0.2 7.4 9.21.1 1.1
M
MM M
M
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
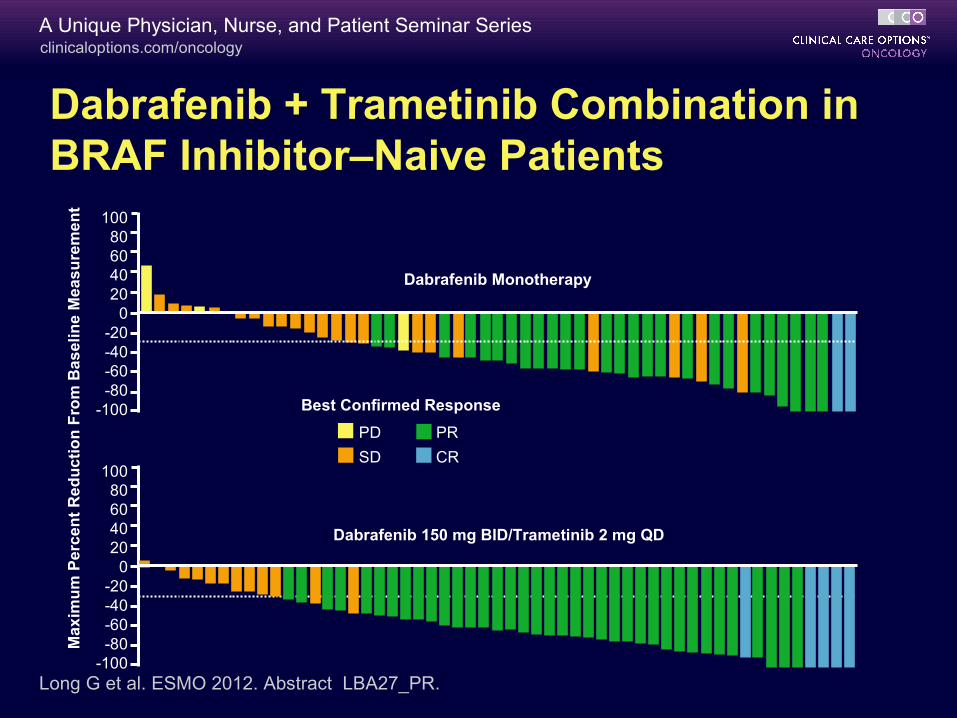
Dabrafenib + Trametinib Combination in BRAF Inhibitor–Naive Patients
Ma
xim
um
Pe
rce
nt
Re
du
cti
on
Fro
m B
as
eli
ne
Me
as
ure
me
nt
Best Confirmed Response
CR
PRPD
SD
Dabrafenib 150 mg BID/Trametinib 2 mg QD
Long G et al. ESMO 2012. Abstract LBA27_PR.
10080604020
0-20-40-60-80
-100
10080604020
0-20-40-60-80
-100
Dabrafenib Monotherapy
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
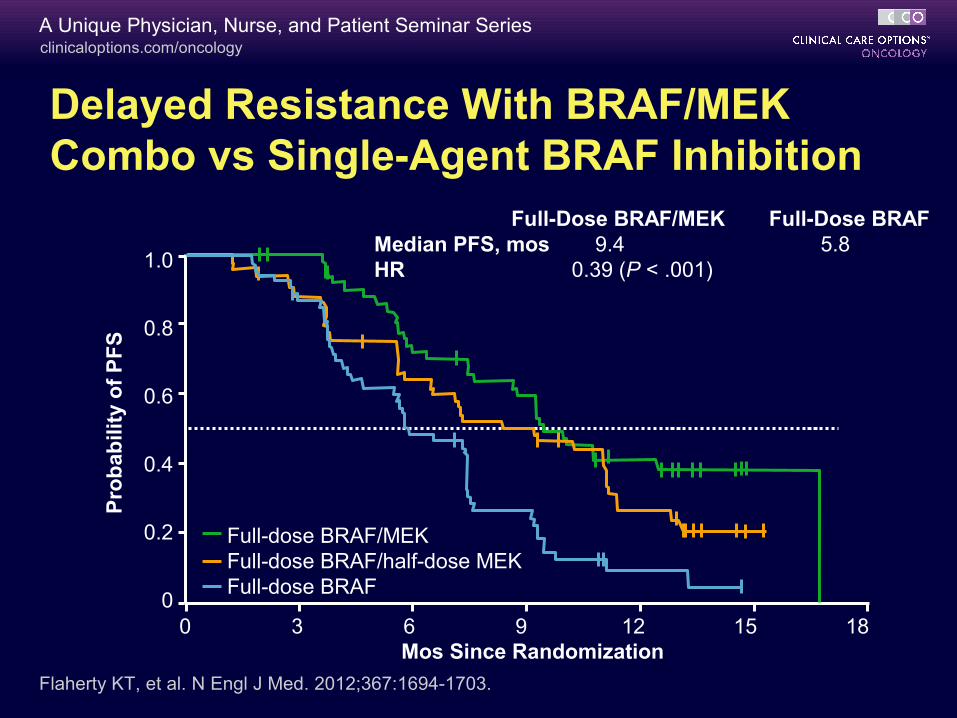
Delayed Resistance With BRAF/MEK Combo vs Single-Agent BRAF Inhibition
Flaherty KT, et al. N Engl J Med. 2012;367:1694-1703.
Full-dose BRAF/MEKFull-dose BRAF/half-dose MEKFull-dose BRAF
Full-Dose BRAF/MEK Full-Dose BRAFMedian PFS, mos 9.4 5.8HR 0.39 (P < .001)1.0
0.8
0.6
0.4
0.2
00 3 6 9 12 15 18
Mos Since Randomization
Pro
bab
ility
of
PF
S
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
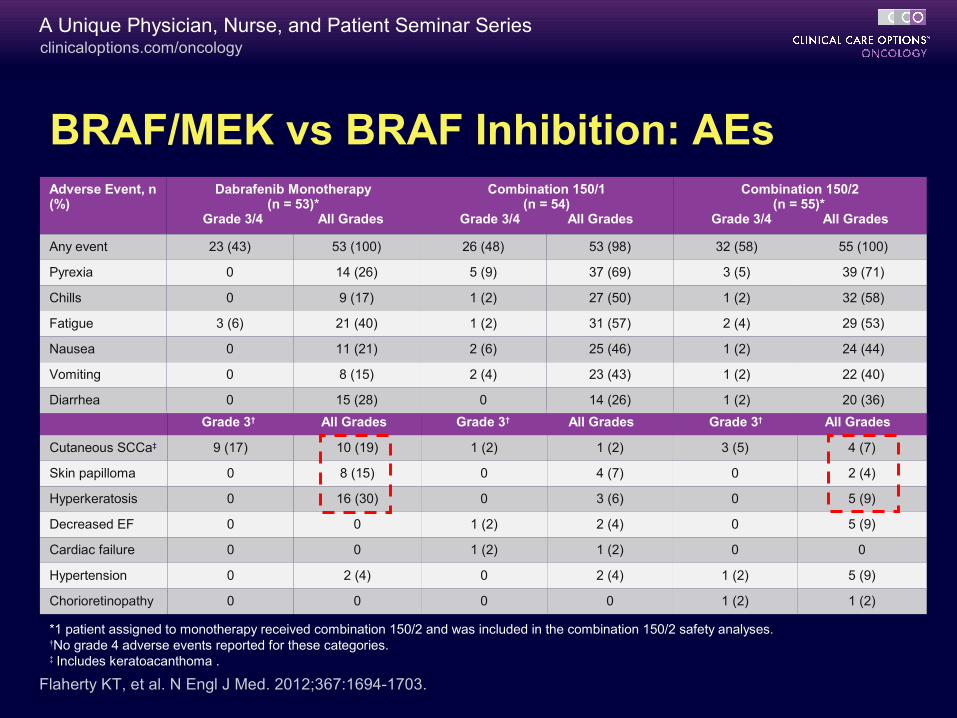
Grade 3† All Grades Grade 3† All Grades Grade 3† All Grades
Cutaneous SCCa‡ 9 (17) 10 (19) 1 (2) 1 (2) 3 (5) 4 (7)
Skin papilloma 0 8 (15) 0 4 (7) 0 2 (4)
Hyperkeratosis 0 16 (30) 0 3 (6) 0 5 (9)
Decreased EF 0 0 1 (2) 2 (4) 0 5 (9)
Cardiac failure 0 0 1 (2) 1 (2) 0 0
Hypertension 0 2 (4) 0 2 (4) 1 (2) 5 (9)
Chorioretinopathy 0 0 0 0 1 (2) 1 (2)
BRAF/MEK vs BRAF Inhibition: AEs
Flaherty KT, et al. N Engl J Med. 2012;367:1694-1703.
Adverse Event, n (%)
Dabrafenib Monotherapy(n = 53)*
Grade 3/4 All Grades
Combination 150/1(n = 54)
Grade 3/4 All Grades
Combination 150/2(n = 55)*
Grade 3/4 All Grades
Any event 23 (43) 53 (100) 26 (48) 53 (98) 32 (58) 55 (100)
Pyrexia 0 14 (26) 5 (9) 37 (69) 3 (5) 39 (71)
Chills 0 9 (17) 1 (2) 27 (50) 1 (2) 32 (58)
Fatigue 3 (6) 21 (40) 1 (2) 31 (57) 2 (4) 29 (53)
Nausea 0 11 (21) 2 (6) 25 (46) 1 (2) 24 (44)
Vomiting 0 8 (15) 2 (4) 23 (43) 1 (2) 22 (40)
Diarrhea 0 15 (28) 0 14 (26) 1 (2) 20 (36)
*1 patient assigned to monotherapy received combination 150/2 and was included in the combination 150/2 safety analyses.†No grade 4 adverse events reported for these categories.‡ Includes keratoacanthoma .
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
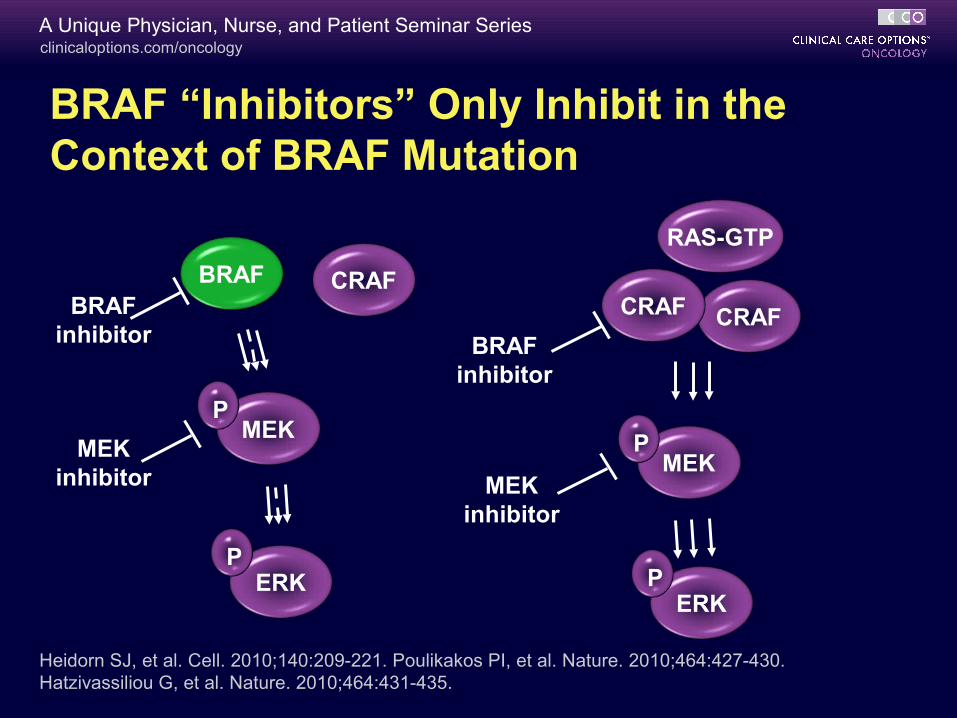
BRAF “Inhibitors” Only Inhibit in the Context of BRAF Mutation
CRAFBRAF
MEK
ERK
P
P
CRAF
MEK
ERK
P
P
CRAF
RAS-GTP
Heidorn SJ, et al. Cell. 2010;140:209-221. Poulikakos PI, et al. Nature. 2010;464:427-430. Hatzivassiliou G, et al. Nature. 2010;464:431-435.
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
CRAFBRAF
MEK
ERK
P
P
CRAF
MEK
ERK
P
P
CRAF
RAS-GTP
BRAF inhibitor BRAF
inhibitor
MEKinhibitor MEK
inhibitor
Heidorn SJ, et al. Cell. 2010;140:209-221. Poulikakos PI, et al. Nature. 2010;464:427-430. Hatzivassiliou G, et al. Nature. 2010;464:431-435.
BRAF “Inhibitors” Only Inhibit in the Context of BRAF Mutation
clinicaloptions.com/oncologyA Unique Physician, Nurse, and Patient Seminar Series
Conclusions
For 50% of patients with melanoma, BRAF and MEK inhibition have been validated as new therapies
Building on BRAF or BRAF/MEK inhibition will proceed in 2 directions:
– Further optimizing MAPK-targeted therapy
– Combination targeted therapy antagonizing pathways essential for melanomagenesis
Go Online for More CCO Coverage of Melanoma!
Interactive Case Challenges to compare your management decisions to those of the expert faculty
Downloadable slides for your own noncommercial presentations or use as a self-study resource
clinicaloptions.com/oncology