case study: post mi torsade arrest almero oosthuizen uct/us emergency medicine 1 april 2009
TRANSCRIPT
CASE STUDY:POST MI TORSADE ARREST
ALMERO OOSTHUIZENUCT/US EMERGENCY MEDICINE
1 APRIL 2009
PATIENT BACKGROUND
• Mrs. AS, 70y female• PMH:– Hypertension, 40py smoker (COPD)– No previous ischemic events
• Medication:– Ridaq 12,5mg od– Currently using amoxil and paracodol for ‘flu’
• No allergies
PRESENTING COMPLAINT
• Presented to VHW ED at 16h10• 15h00 - Generalised weakness; legs felt numb;
vomited twice; appeared confused; could not understand speech or speak clearly
• 15h30 – Chest discomfort; sweating; tremulous. Lasted 30min, then came and went
• Also c/o leg discomfort ; 2 weeks of productive cough
PHYSICAL EXAM 1
• General:– Frail, poor concentration, slightly slurred speech– HR 75 ; BP 140/82 ; Temp 36,7 ; RR 24 ; Hb 11
• CVS:– Regular pulse ; limb pulses not documented ; no
failure ; no murmurs ; JVP not documented
• Chest:– No abnormalities documented
PHYSICAL EXAM 2
• Abd:– No abnormalities documented
• CNS– GCS 14 (slightly confused); power both legs 4/5– Nil more documented
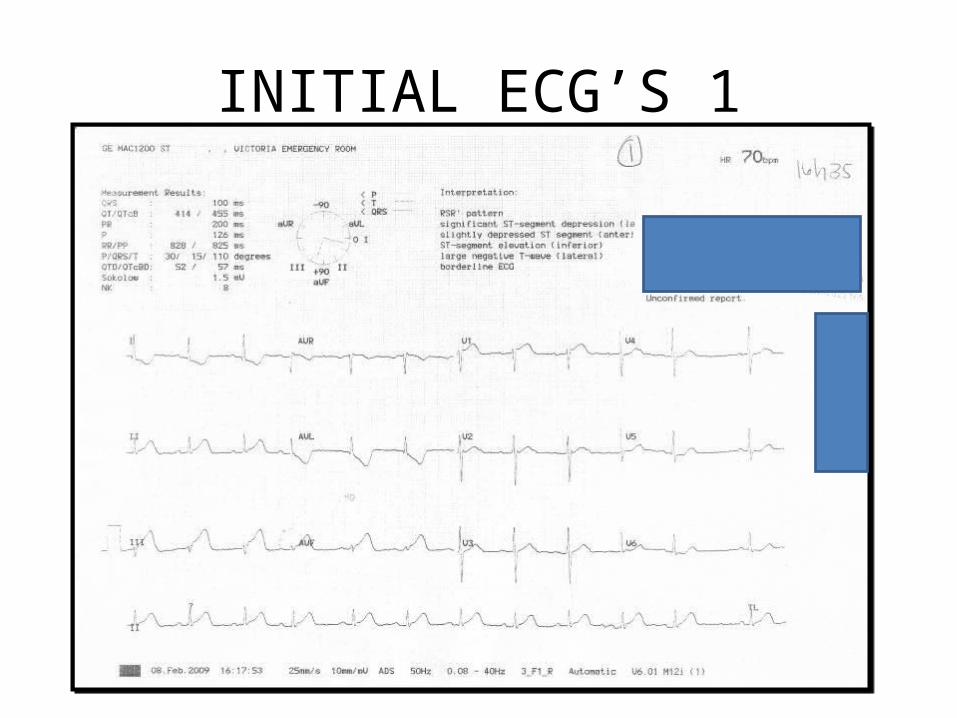
INITIAL ECG’S 1
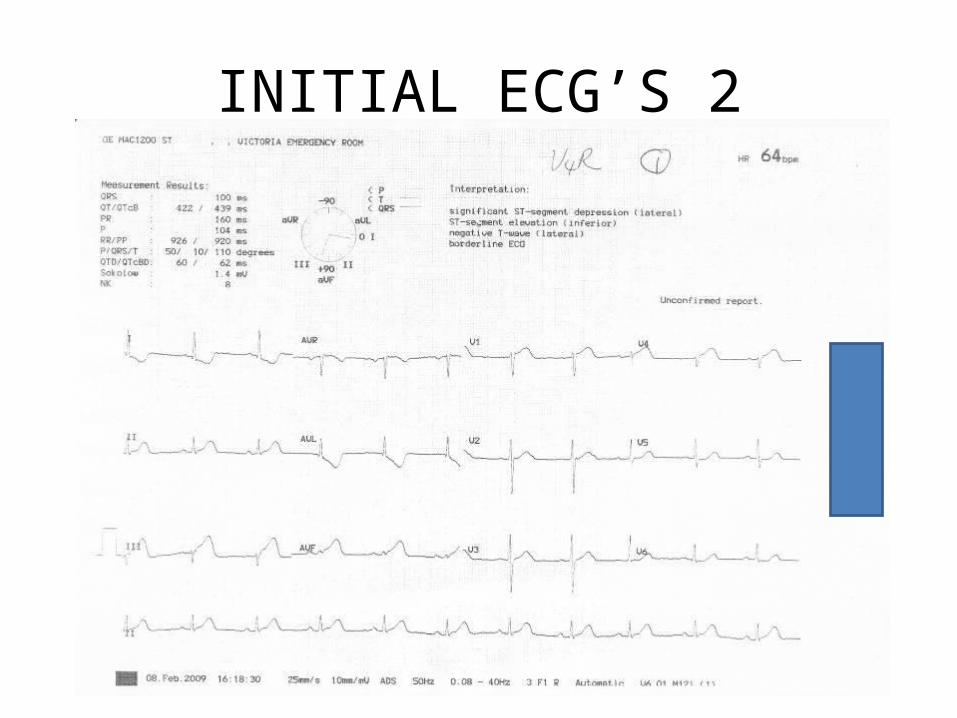
INITIAL ECG’S 2
INITIAL ASSESMENT
• Casualty Officer (2’nd year intern) notes– ?MI ; ?TIA ; ?LRTI
• Central question: In light of possible IC event, is it safe to strep patient?
INITIAL MANAGEMENT
• O2 ; Aspirin 300mg ; Morphine 4mg ; Isordil sl• Trop T (neg)• Casualty officer referred the patient to
medical registrar (actually a cosmo)– Recommended they phone GSH cardiology– Said he’d be down as soon as possible
• GSH Cardiology– “we don’t give advice re thrombolysis over the
phone” AAARGHH! Intern! AAARGHH!
THEN…
• Patient now comfortable and pain free• Spoke to medics again– Recommended ED hold off on strep until they
have reviewed patient
19h00
• Patient became unresponsive (noticed immediately by attending nurse) and pulseless
• CPR commenced at once with chest compressions, and patient rushed to resuscitation area (cpr en route, transit time about 20 sec)
RESUSCITATION 1
• BVM vent 2:30 high quality chest compressions ongoing
• Monitor attached within 40 seconds of initial arrest
• Arrest rhythm: Torsade du Pointes• Immediate async. biphasic cardio version at
200J• CPR commenced, adrenalin 1mg IV ordered,
but not given yet
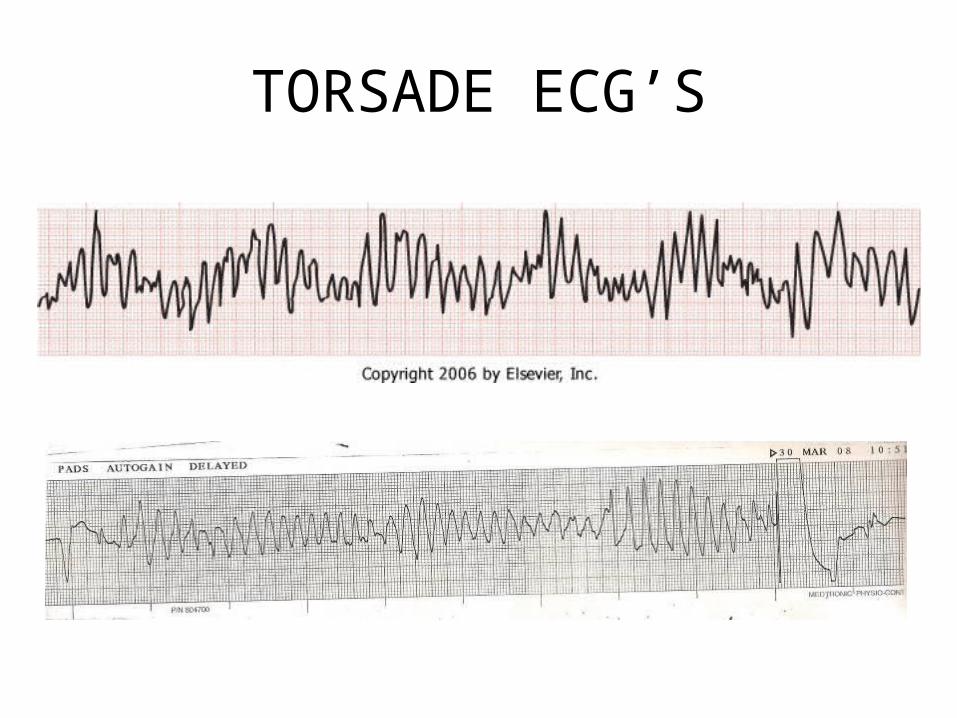
TORSADE ECG’S
RESUSCITATION 2
• During first cycle of chest compressions post shock, patient displayed signs of ROSC– Moaning, moving
• Good pulse felt; rhythm = AF with incomplete RBBB at 75bpm
• Patient woke up and was conversant within about two minutes, complaining of ‘sore ribs’
• By this time the medic arrived at last
SUBSEQUENT CARE
• Post resuscitation care consisted of O2 via face mask and ongoing cardiac monitoring
• 2g MgSO4 infused IV over 5 minutes
• After discussion with the medical consultant, thrombolysis with streptokinase was started once the patient had been transferred to ICU.
NEXT MORNING
• Stable post strep course in ICU• Bilateral, severe PVD noted• Critical ischemia of right leg• Transferred to GSH ICU• Right leg embolectomy and fasciotomy, with
eventual right sided BKA (septic, non healing wound)
• Transferred back to VHW on 25-2-2009, and is doing well!
FINAL ASSESSMENT
• Inferior STEMI with RV extension– Possible intermittent complete AV block with
bradycardia– Complicated by Torsade arrest– Post version/strep AF
• Acute limb ischemia (right leg)– Initial embolectomy– Eventual right BKA
• Probably never had a ‘TIA’
PEARLS
• ACS patients are not stable patients– They should be intensively monitored
• Difficult management decisions on sick or complicated patients like this should be made by the most senior person available
• Torsade with arrest is still arrest: initial treatment remains good CPR and early cardio version. Other treatments may then be considered

Pause Dependent (Acquired) • Drug induced: 1A and 1C antidysrhythmics, phenothiazines,
cyclic antidepressants, organophosphates, antihistamines.• Electrolyte abnormalities: hypokalemia, hypomagnesemia,
hypocalcemia (rarely)• Diet related: starvation, low protein• Severe bradycardia or atrioventricular block• Hypothyroidism• Contrast injection• Cerebrovascular accident (especially intraparenchymal)• Myocardial ischemia
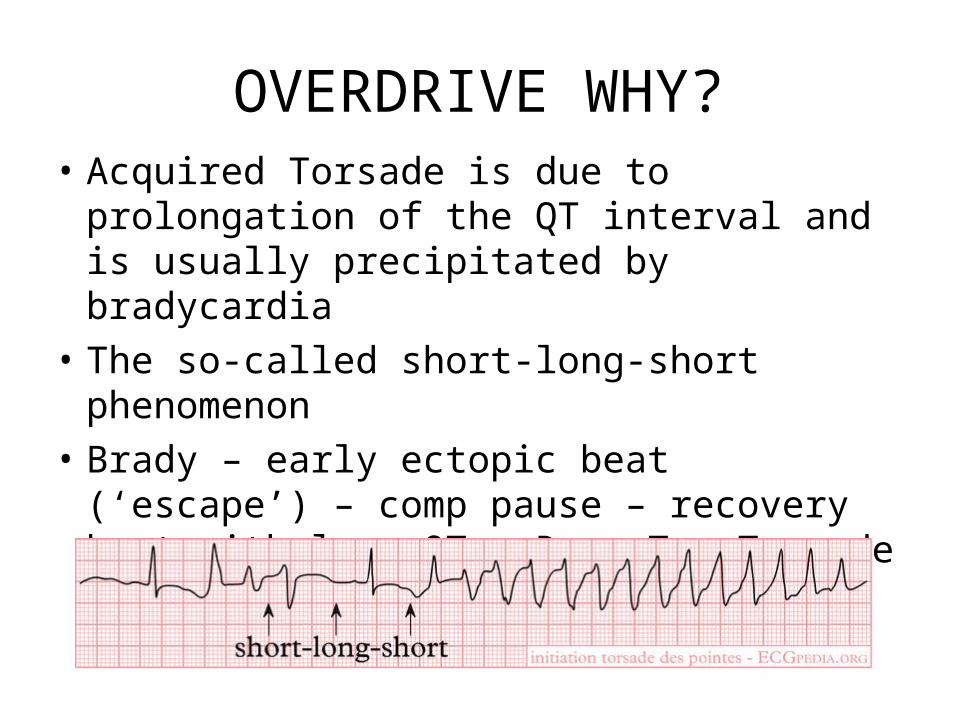
OVERDRIVE WHY?• Acquired Torsade is due to prolongation of
the QT interval and is usually precipitated by bradycardia
• The so-called short-long-short phenomenon• Brady – early ectopic beat (‘escape’) – comp
pause – recovery beat with long QT - R on T - Torsade
OVERDRIVE WHY?
• Speeding up the rate will shorten ventricular repolarisation
• This decreases the effective QT (and therefore vulnerable time) interval and decreases the chances of an early ectopic beat
• Voila!
OVERDRIVE WHAT?
• NB: Overdrive to prevent recurrent TdP vs. Overdrive to convert resistant TdP
• Electrical overdrive to a ventricular rate of about 100 – 120– Discussion of technique during lecture
• Chemical overdrive with Isoproterenol– 2 to 10 mcg/kg/min– Titrate to increase HR till VT suppressed
Adrenergic Dependent
Congenital Jervell and lange-Nielsen syndrome (deafness, autosomal recessive)
Romano-Ward syndrome (normal hearing, autosomal dominant)
Sporadic (normal hearing, no familial tendency)
Mitral valve prolapse.
Acquired Cerebrovascular disease (especially subarachnoid hemorrhage)
Autonomic surgery: radical neck dissection, carotid endarterectomy, truncal vagotomy
TORSADE: MANAGEMENT
• Unstable: Unsynchronized cardio version– Sync not effective due to variable R wave amplitude,
morphology and axis• Other options– Correct precipitant– MgSO4 1-2g IV in 10 ml D5W as a push for everyone
(may also consider K supplementation)– Consider lidocaine or amiodarone (effectiveness not
demonstrated)• Class 1A and 1C contraindicated
REFERENCES
• ACLS resource text (ACLS EP)• 5 Minute emergency medicine consult, Rosen
and Barkin• Textbook of Emergency Medicine, Rosen and
Barkin• Emedicine.com