case scenario group 1
TRANSCRIPT

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 1/12
Case Scenario Group 1
History/Information:This patient is a 60-year-old male who was admitted to the hospital with fever andweight loss of 10kg in the past month. He also has night sweats and fatigue. Hisadmitting diagnosis is left renal cell cancer. Preoperatively, the patient received
ferrous sulfate, epoetin alfa, and vitamin C. The patient is on hydrochlorothiazide25mg once daily for hypertension. The patient has smoked one pack per day sinceage 24 and admits to two cups of caffeinated coffee per day. His BP on admissionwas 136/84 and his preoperative labs revealed Hgb 14, Hct 40%, slightly elevatedBUN/Creatinine ratio and an elevated Alkaline Phosphate. The patient is a Jehovah’sWitness. The patient was transferred back to the floor following a left nephrectomy.His surgical course was uneventful. His vital signs have been stable for the past fourhours. He has been dozing but responds to verbal stimulation. He was medicated forpain one hour ago.
Healthcare Provider’s Orders:• Admitting Diagnosis: Renal Cell Carcinoma, Status Post Left Nephrectomy• Transfer to Medical-Surgical Unit• Condition: Serious• Vital signs per fl oor routine• Complete bedrest• IV 0.9% NS at 150mL/hour• NPO• Clamp nasogastric tube• Discontinue nasogastric tube when alert and oriented, able to lift head off pillowand positive bowel sounds• Urinary catheter• Notify healthcare provider if urine output less than 50mL/hour• Cough and deep breathe, incentive spirometry every 1-2 hours• Oxygen at 50% via face mask• Continuous cardiac and pulse oximetry monitoring• Notify healthcare provider if SpO2 less than 90%• Continuous sequential compression stockings• Cefazolin 2g IV every 8 hours x 2 doses• Sucralfate 1g PO/NG every 6 hours• Epoetin alfa 40,000units SQ now• Ferrous sulfate 324mg PO three times daily• Vitamin C 500mg PO every day• Folate 1mg PO every day• Morphine sulfate 2mg IV every 1 hour prn pain• Chest x-ray, CBC, Electrolytes, BUN, Creatinine, Glucose, ABG STAT

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 2/12

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 3/12
The gastrointestinal tract (GI tract), also called the digestive tract, alimentary canal or gut, isthe system of organs within multicellular animals that takes in water and food, extracts energyand nutrients from the food, and expels the remainder as waste. The major functions of the GItract are digestion and excretion.
Digestion refers to the process of metabolism whereby a biological entity applies both mechanicaland chemical procedures to reduce a substance to component parts that are then absorbed intothe body and distributed throughout via the circulatory system (Silverthorn 2004). Excretion is theprocess of eliminating the waste products of metabolism and other non-useful materials.
The digestive process involves the cooperative work of many body components, includingthe heart, brain, liver , and pancreas. For example, the heart directs blood to the area and the liver and pancreas secrete digestive enzymes. The process also reflects individuality. For instance,some individuals can digest milk or eat peanuts, while others may have an allergy to one or bothof these, and people enjoy different tastes.
The GI tract differs substantially from animal to animal. For instance, some animals have multi-chambered stomachs, while some animals' stomachs contain a single chamber. In anormal human adult male, the GI tract is approximately 6.5 meters (20 feet) long and consists of the upper and lower GI tracts. The tract may also be divided into foregut, midgut, and hindgut,reflecting the embryological origin of each segment of the tract.
In humans, the gastrointestinal tract is a long tube with muscular walls comprising four differentlayers: inner mucosa, submucosa, muscularis externa, and the serosa (see histology section). Itis the contraction of the various types of muscles in the tract that propel the food.
The GI tract can be divided into an upper and a lower tract. The upper GI tract consists of themouth, pharynx, esophagus, and stomach. The lower GI tract is made up of the intestines and the
anus.
Upper gastrointestinal tract
The upper GI tract consists of the mouth, pharynx, esophagus, and stomach.
The mouth comprises the oral mucosa, buccal mucosa, tongue, teeth, and openings of the salivary glands. The mouth is the point of entry of the food into the GI tract and the sitewhere digestion begins as food is broken down and moistened in preparation for further transit through the GI tract.
Behind the mouth lies the pharynx, which leads to a hollow muscular tube calledthe esophagus or gullet. In an adult human, the esophagus (also spelled oesphagus) isabout one inch in diameter and can range in length from 10-14 inches (NR 2007).
Food is propelled down through the esophagus to the stomach by the mechanism of peristalsiscoordinated periodic contractions of muscles in the wall of the esophagus. Theesophagus extends through the chest and pierces the diaphragm to reach the stomach,which can hold between 2-3 liters of material in an adult human. Food typically remains in thestomach for two to three hours.
The stomach, in turn, leads to the small intestine.
8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 4/12
The upper GI tract roughly corresponds to the derivatives of the foregut, with theexception of the first part of the duodenum (see below for more details.)
Lower gastrointestinal tract
The lower GI tract comprises the intestines and anus.
Bowel or intestine
The small intestine, approximately 7 meters (23 feet) feet long and 3.8centimeters (1.5 inches) in diameter, has three parts (duodenum, jejunum, and ileum). Itis where most digestion takes place. Accessory organs, such asthe liver and pancreas help the small intestine digest, and more importantly, absorbimportant nutrients needed by the body. Digestion is for the most part completed in thesmall intestine, and whatever remains of the bolus have not been digested are passedonto the large intestine for final absorption and excretion.
duodenum – the first 25 centimeters (9.84 inches)
jejunum and ileum – combined are approximately 6 meters (19.7 feet) inlength
The large intestine – (about 1.5 meters (5 feet) long with a diameter of about 9centimeters (3.5 inches) also has three parts:
cecum (the appendix is attached to the cecum)
The colon (ascending colon, transverse colon, descending colon andsigmoid flexure) is where feces are formed after absorption is completed
The rectum propels feces to the final part of the GI tract, the anus
The anus, which is under voluntary control, releases waste from the body through thedefecation process
Accessory organs to the GI tract help in digestion by releasing powerful enzymes and other fluidsthat breakdown macromacules into smaller molecules that can be absorbed by the digestivesystem. Two such organs are the liver and pancreas.
The liver secretes bile into the small intestine via the biliary system, employing the gall bladder asa reservoir. Apart from storing and concentrating bile, the gall bladder has no other specificfunction. The pancreassecretes an isosmotic fluid containing bicarbonate and several enzymes,including trypsin, chymotrypsin, lipase, pancreatic amylase, and nucleolytic enzymes(deoxyribonuclease and ribonuclease), into the small intestine.
The primary purpose of the gastrointestinal tract is to break food down into nutrients, which can
be absorbed into the body to provide energy. First food must be ingested into the mouth to be
mechanically processed and moistened. Secondly, digestion occurs mainly in the stomach and
small intestine where proteins, fats and carbohydrates are chemically broken down into their basic building blocks. Smaller molecules are then absorbed across the epithelium of the small
intestine and subsequently enter the circulation. The large intestine plays a key role in
reabsorbing excess water. Finally, undigested material and secreted waste products are excreted
from the body via defecation (passing of faeces).
In the case of gastrointestinal disease or disorders, these functions of the
gastrointestinal tract are not achieved successfully. Patients may develop symptoms
8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 5/12
of nausea, vomiting, diarrhoea, malabsorption, constipation or obstruction.
Gastrointestinal problems are very common and most people will have experienced
some of the above symptoms several times throughout their lives.
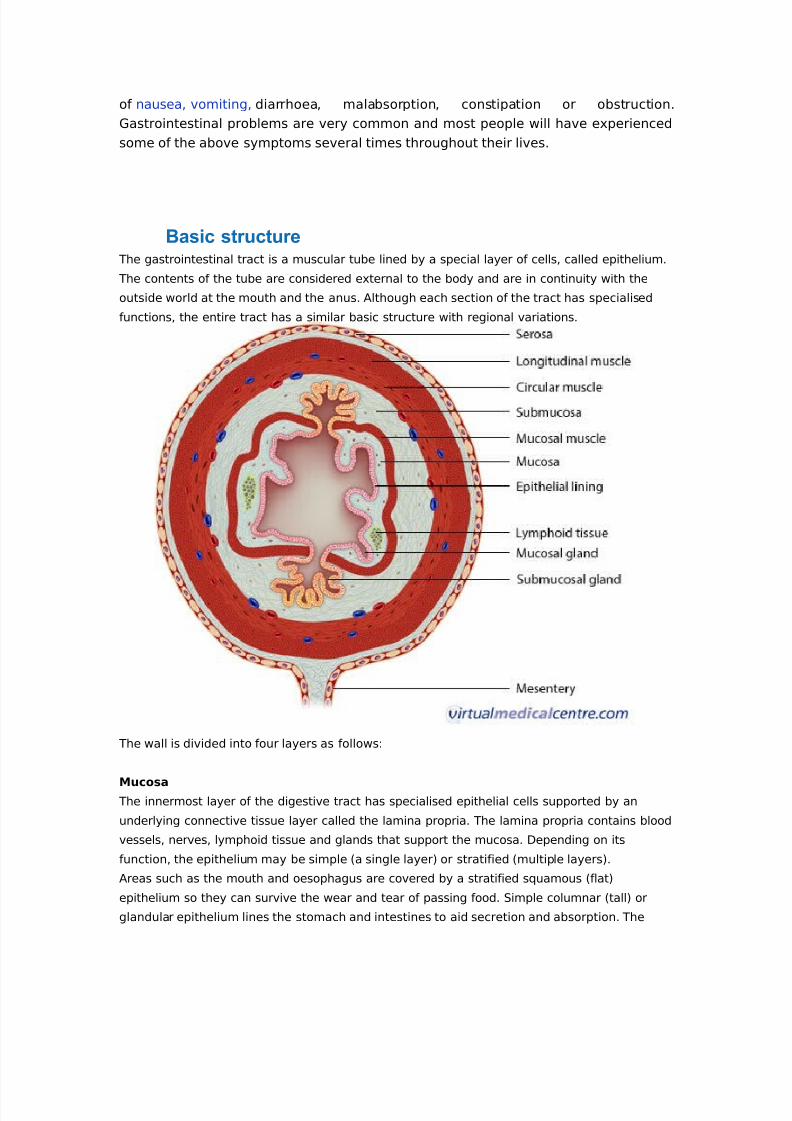
Basic structureThe gastrointestinal tract is a muscular tube lined by a special layer of cells, called epithelium.
The contents of the tube are considered external to the body and are in continuity with the
outside world at the mouth and the anus. Although each section of the tract has specialised
functions, the entire tract has a similar basic structure with regional variations.
The wall is divided into four layers as follows:
MucosaThe innermost layer of the digestive tract has specialised epithelial cells supported by an
underlying connective tissue layer called the lamina propria. The lamina propria contains blood
vessels, nerves, lymphoid tissue and glands that support the mucosa. Depending on its
function, the epithelium may be simple (a single layer) or stratified (multiple layers).
Areas such as the mouth and oesophagus are covered by a stratified squamous (flat)
epithelium so they can survive the wear and tear of passing food. Simple columnar (tall) or
glandular epithelium lines the stomach and intestines to aid secretion and absorption. The

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 6/12
inner lining is constantly shed and replaced, making it one of the most rapidly dividing areas of
the body! Beneath the lamina propria is the muscularis mucosa. This comprises layers of
smooth muscle which can contract to change the shape of the lumen.
Submucosa
The submucosa surrounds the muscularis mucosa and consists of fat, fibrous connective tissue
and larger vessels and nerves. At its outer margin there is a specialized nerve plexus called
the submucosal plexus or Meissner plexus. This supplies the mucosa and submucosa.
Muscularis externa
This smooth muscle layer has inner circular and outer longitudinal layers of muscle fibres
separated by the myenteric plexus or Auerbach plexus. Neural innervations control the
contraction of these muscles and hence the mechanical breakdown and peristalsis of the food
within the lumen.
Serosa/mesentery
The outer layer of the GIT is formed by fat and another layer of epithelial cells called
mesothelium.
Individual components of the gastrointestinal system
Oral cavity
The oral cavity or mouth is responsible for the intake of food. It is lined by a stratified
squamous oral mucosa with keratin covering those areas subject to significant abrasion, such
as the tongue, hard palate and roof of the mouth. Mastication refers to the mechanical
breakdown of food by chewing and chopping actions of the teeth. The tongue, a strong
muscular organ, manipulates the food bolus to come in contact with the teeth. It is also the
sensing organ of the mouth for touch, temperature and taste using its specialised sensors
known as papillae.
Insalivation refers to the mixing of the oral cavity contents with salivary gland secretions. The
mucin (a glycoprotein) in saliva acts as a lubricant. The oral cavity also plays a limited role in
the digestion of carbohydrates. The enzyme serum amylase, a component of saliva, starts the
process of digestion of complex carbohydrates. The final function of the oral cavity is
absorption of small molecules such as glucose and water, across the mucosa. From the mouth,
food passes through the pharynx and oesophagus via the action of swallowing.
Salivary glands
Three pairs of salivary glands communicate with the oral cavity. Each is a complex gland with
numerous acini lined by secretory epithelium. The acini secrete their contents into specialised
ducts. Each gland is divided into smaller segments called lobes. Salivation occurs in response
to the taste, smell or even appearance of food. This occurs due to nerve signals that tell the

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 7/12
salivary glands to secrete saliva to prepare and moisten the mouth. Each pair of salivary
glands secretes saliva with slightly different compositions.
Parotids
The parotid glands are large, irregular shaped glands located under the skin on the side of the
face. They secrete 25% of saliva. They are situated below the zygomatic arch (cheekbone) and
cover part of the mandible (lower jaw bone). An enlarged parotid gland can be easier felt when
one clenches their teeth. The parotids produce a watery secretion which is also rich in proteins.
Immunoglobins are secreted help to fight microorganisms and a-amylase proteins start to
break down complex carbohydrates.
Submandibular
The submandibular glands secrete 70% of the saliva in the mouth. They are found in the floor
of the mouth, in a groove along the inner surface of the mandible. These glands produce a
more viscid (thick) secretion, rich in mucin and with a smaller amount of protein. Mucin is a
glycoprotein that acts as a lubricant.
Sublingual
The sublinguals are the smallest salivary glands, covered by a thin layer of tissue at the floor
of the mouth. They produce approximately 5% of the saliva and their secretions are very sticky
due to the large concentration of mucin. The main functions are to provide buffers andlubrication.
Oesophagus
The oesophagus is a muscular tube of approximately 25cm in length and 2cm in diameter. It
extends from the pharynx to the stomach after passing through an opening in the diaphragm.
The wall of the oesophagus is made up of inner circular and outer longitudinal layers of muscle
that are supplied by the oesophageal nerve plexus. This nerve plexus surrounds the lower

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 8/12
portion of the oesophagus. The oesophagus functions primarily as a transport medium
between compartments.
Stomach
The stomach is a J shaped expanded bag, located just left of the midline between the
oesophagus and small intestine. It is divided into four main regions and has two borders called
the greater and lesser curvatures. The first section is the cardia which surrounds the cardial
orifice where the oesophagus enters the stomach. The fundus is the superior, dilated portion of
the stomach that has contact with the left dome of the diaphragm. The body is the largest
section between the fundus and the curved portion of the J.
This is where most gastric glands are located and where most mixing of the food occurs.
Finally the pylorus is the curved base of the stomach. Gastric contents are expelled into the
proximal duodenum via the pyloric sphincter. The inner surface of the stomach is contracted
into numerous longitudinal folds called rugae. These allow the stomach to stretch and expand
when food enters. The stomach can hold up to 1.5 litres of material. The functions of the
stomach include:
1. The short-term storage of ingested food.
2. Mechanical breakdown of food by churning and mixing motions.
3. Chemical digestion of proteins by acids and enzymes.
4. Stomach acid kills bugs and germs.
5. Some absorption of substances such as alcohol.
Most of these functions are achieved by the secretion of stomach juices by gastric glands in
the body and fundus. Some cells are responsible for secreting acid and others secrete
enzymes to break down proteins.
Small intestine
The small intestine is composed of the duodenum, jejunum, and ileum. It averages
approximately 6m in length, extending from the pyloric sphincter of the stomach to the ileo-
caecal valve separating the ileum from the caecum. The small intestine is compressed into
numerous folds and occupies a large proportion of the abdominal cavity.
The duodenum is the proximal C-shaped section that curves around the head of the pancreas.
The duodenum serves a mixing function as it combines digestive secretions from the pancreas
and liver with the contents expelled from the stomach. The start of the jejunum is marked by a
sharp bend, the duodenojejunal flexure. It is in the jejunum where the majority of digestion and
absorption occurs. The final portion, the ileum, is the longest segment and empties into the
caecum at the ileocaecal junction.

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 9/12
The small intestine performs the majority of digestion and absorption of nutrients. Partlydigested food from the stomach is further broken down by enzymes from the pancreas and bile
salts from the liver and gallbladder. These secretions enter the duodenum at the Ampulla of
Vater. After further digestion, food constituents such as proteins, fats, and carbohydrates are
broken down to small building blocks and absorbed into the body's blood stream.
The lining of the small intestine is made up of numerous permanent folds called plicae
circulares. Each plica has numerous villi (folds of mucosa) and each villus is covered by
epithelium with projecting microvilli (brush border). This increases the surface area for
absorption by a factor of several hundred. The mucosa of the small intestine contains several
specialised cells. Some are responsible for absorption, whilst others secrete digestive enzymes
and mucous to protect the intestinal lining from digestive actions.
Large intestine
The large intestine is horse-shoe shaped and extends around the small intestine like a frame. It
consists of the appendix, caecum, ascending, transverse, descending and sigmoid colon, and
the rectum. It has a length of approximately 1.5m and a width of 7.5cm.
The caecum is the expanded pouch that receives material from the ileum and starts to
compress food products into faecal material. Food then travels along the colon. The wall of the
colon is made up of several pouches (haustra) that are held under tension by three thick bands
of muscle (taenia coli).
The rectum is the final 15cm of the large intestine. It expands to hold faecal matter before it
passes through the anorectal canal to the anus. Thick bands of muscle, known as sphincters,
control the passage of faeces.

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 10/12
The mucosa of the large intestine lacks villi seen in the small intestine. The mucosal surface is
flat with several deep intestinal glands. Numerous goblet cells line the glands that secrete
mucous to lubricate faecal matter as it solidifies. The functions of the large intestine can be
summarised as:
1. The accumulation of unabsorbed material to form faeces.
2. Some digestion by bacteria. The bacteria are responsible for the formation of intestinal
gas.
3. Reabsorption of water, salts, sugar and vitamins.
Liver
The liver is a large, reddish-brown organ situated in the right upper quadrant of the abdomen.
It is surrounded by a strong capsule and divided into four lobes namely the right, left, caudateand quadrate lobes. The liver has several important functions. It acts as a mechanical filter by
filtering blood that travels from the intestinal system. It detoxifies several metabolites
including the breakdown of bilirubin and oestrogen. In addition, the liver has synthetic
functions, producing albumin and blood clotting factors. However, its main roles in digestion
are in the production of bile and metabolism of nutrients. All nutrients absorbed by the
intestines pass through the liver and are processed before traveling to the rest of the body.
The bile produced by cells of the liver, enters the intestines at the duodenum. Here, bile salts
break down lipids into smaller particles so there is a greater surface area for digestive
enzymes to act.
Gall bladder
The gallbladder is a hollow, pear shaped organ that sits in a depression on the posterior
surface of the liver's right lobe. It consists of a fundus, body and neck. It empties via the cystic
duct into the biliary duct system. The main functions of the gall bladder are storage and
concentration of bile. Bile is a thick fluid that contains enzymes to help dissolve fat in the
intestines. Bile is produced by the liver but stored in the gallbladder until it is needed. Bile is

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 11/12
released from the gall bladder by contraction of its muscular walls in response to hormone
signals from the duodenum in the presence of food.
Pancreas
Finally, the pancreas is a lobular, pinkish-grey organ that lies behind the stomach. Its head
communicates with the duodenum and its tail extends to the spleen. The organ is
approximately 15cm in length with a long, slender body connecting the head and tail
segments. The pancreas has both exocrine and endocrine functions. Endocrine refers to
production of hormones which occurs in the Islets of Langerhans. The Islets produce insulin,
glucagon and other substances and these are the areas damaged in diabetes mellitus. The
exocrine (secretrory) portion makes up 80-85% of the pancreas and is the area relevant to the
gastrointestinal tract.
It is made up of numerous acini (small glands) that secrete contents into ducts which
eventually lead to the duodenum. The pancreas secretes fluid rich in carbohydrates and
inactive enzymes. Secretion is triggered by the hormones released by the duodenum in the
presence of food. Pancreatic enzymes include carbohydrases, lipases, nucleases and
proteolytic enzymes that can break down different components of food. These are secreted in
an inactive form to prevent digestion of the pancreas itself. The enzymes become active once
they reach the duodenum.
Co l o rectal cancer is a disease in which normal cells in the lining of the colon or rectum
begin to change, start to grow uncontrollably, and no longer die. These changes usually
take years to develop; however, in some cases of hereditary disease, changes can
occur within months to years. Both genetic and environmental factors can cause the
changes. Initially, the cell growth appears as a benign (noncancerou

8/7/2019 Case Scenario Group 1
http://slidepdf.com/reader/full/case-scenario-group-1 12/12
polyp that can, over time, become a cancerous tumor. If nottreated or
removed, apolyp canbecome apotentially life-
threateningcancer.
Recognizingand removing
precancerouspolyps beforethey becomecancer can
preventcolorectal
cancer.