case 12: speaker notesmedu.s3.amazonaws.com/3819c3ee/core 12 workshop speaker... · web viewdo you...
TRANSCRIPT

Slide 1
Slide 2
Slide 3
Slide 4
Slide 5 Spend a moment on this very important slide. This is where we prompt and engage the learners to TELL us explicitly what seemed a difficult concept and what ELSE they want to know. We need to be explicit to encourage learners to NAME their unmet needs. This ensures learner agency in their education (Learner centered, rather than teacher centered)

Slide 6
Slide 7 Anticipate they will say US, but may also say CT & MR, Ultrasound is portable, and does not requires sedation.Q: What is US good to detect? A: Hydrocephalus, germinal matrix hemorrhage, congenital anomaliesQ: What are some limitations with Ultrasound in cranial imaging? A: Requires open sutures as acoustic window for sound. So patient must be an infant.Q: When might you need more than Ultrasound? A: Require greater detail to work out complicated findingsQ: If Ultrasound doesn’t answer all the questions, what will you prefer to do next? A: MR generallyQ: Why? A: Avoids the radiation that comes with CT
Slide 8 A little anatomy…Q: What anatomic plane is this image? How do you know? A: Coronal. Right side and left side are mirror image or symmetrical, so that means this CANNOT be sagittal. Symmetrical images in brain will be either axial or coronal.
We’ll work through the anatomy and then, you’ll know the answer.
Slide 9 Q: Where is the anterior fontanelle? We can also use other fontanelles if they are open.
Slide 10 Q: Where is the fontanelle? Here.Q: Why is the fontanelle important when cranial ultrsound is done? A: This is the acoustic window through which we can introduce sound energy. Ultrasound does not penetrate through the skull bones, so we go through fontanelle which is not covered by bone.

Slide 11 So let’s think about where the fontanelle is located and use that knowledge and this image to figure out the rest of the anatomy… We know that sound waves propagate in a straight line from the transducer, so
Q: What might make sense for the structures shown here in yellow?
Slide 12 So let’s think about where the fontanelle is located and use that knowledge and this image to figure out the rest of the anatomy… We know that sound waves propagate in a straight line from the transducer, so
Q: What might make sense for the structures shown here in yellow? A: These are the bilateral thalami and the midbrain.
Q: if we see the thalami above the midbrain in the image, is this axial or is it coronal? A: has to be coronal.
Slide 13 Q: So, what would this structure in aqua have to be?
Slide 14 Q: So, what would this structure in aqua have to be? A: Since we worked out this image is coronal, it has to be the Pons. Are you surprised to see that with ultrasound, it is possible to see details of the posterior fossa from the fontanelle?
Slide 15 Q: What is the ultrasound lingo for a really dark black structure in an image? Remember the language of imaging?
Q: Which of the following is the most correct way to describe on any ultrasound image an area with a darker gray to black color and no specks within it?Choose from:• Hypo-attenuating• Hypo-intense• Anechoic (correct response)• Hypoechoic
Remember that ultrasound deals with echoes, and the language in the radiology reports you will receive reflects that.

Slide 16 Q: What are the black structures ?? (next slide for answer)
Slide 17 Q: What are the anechoic (black, no internal echoes) structures ?? A: These are the ventricles and the midline cavum septum
Slide 18 Q: What is the structure crossing midline above the cavum and lateral ventircles?
Slide 19 Q: What is the structure crossing midline above the cavum and lateral ventircles? A: Corpus callosum
Slide 20 Here is a blank slide if you are using annotation on an iPad and want to have students identify anatomy. (Can hide this slide if wished)

Slide 21 Q: What is different in this image? A: Transducer has been turned 90 degrees on the fontanelle, and now we have a sagittal (actually parasagittal) image. There are a few things very important to know in cranial ultrasound that will be mentioned in reports you get, so let’s quickly run through them.
Q: What is the anechoic crescentic structure? A: Lateral ventricle. The ultrasonographer will orient in parasagittal planes using the lateral ventricle to bring important landmarks into view.
Slide 22 Q: What is the crescentic anechoic structure? A: Lateral ventricle. The ultrasonographer will orient in parasagittal planes using the lateral ventricle to bring important landmarks into view.
Slide 23 These normal landmarks include the caudate, the thalamus, and a distinct groove between them. The choroid plexus is visible in the atrium of lateral ventricle in routine neonatal cranial ultrasound.
Q: Why is the caudo-thalamic groove so important? A: This is the site where hemorrhage in the germinal matrix frequently occurs. Germinal matrix runs along this dotted yellow line.
Slide 24
Slide 25 Normal image on left upper part of screen. Cranial ultrasound at 31 week gestation in two different babies.Ask learners to see if they can compare and contrast what they see in the normal and abnormal images.
A: There are heterogeneous, predominantly hypoechoic masses on both ventricles and ventricular enlargement
Q: What do you think this is? A: These are germinal matrix hemorrhages with hydrocephalus, a condition that particularly affects premature infants.

Slide 26 Normal image on left upper part of screen. Cranial ultrasound at 31 week gestation in two different babies. Contrast what you see in the normal and abnormal images.
(Allow learners to describe, prompt them to practice correct use of the ultrasound “dialect” of language of imaging)
Q: Where is the blood? A: In the abnormal image, we see the germinal matrix bleed at caudothalamic groove, better localized on sagittal.Q: What effect does this have on child’s long-term neurologic and cognitive outcome? A: Depends on the grade of the hemorrhage. Lower grades have good prognosis: the highest grade has much poorer prognosis. Radiologists use a grading system (1-4) that depends on where is the blood, and whether baby develops hydrocephalus or not.
Slide 27 Q: How is the likelihood of germinal matrix hemorrhage related to gestational age at birth? A: risk is higher when gestational age is lower.Q: where do they think the blood is on this image? How is this different from the last patient? See next slide for labelsA: This is an example of a Grade 4 hemorrhage. There is blood in enlarged ventricles and involvement of the brain parenchyma.
Slide 28 Showing the comparison with the normal if needed
Slide 29 Q: How is the likelihood of germinal matrix hemorrhage related to gestational age at birth? A: risk is higher when gestational age is lower.
This is an example of a Grade 4 hemorrhage. There is blood in enlarged ventricles (red) and involvement of the brain parenchyma (pink).
Slide 30 Q: How will you initially examine a child with limited hip abduction? A: Barlow: Adduct the flexed hip and press posteriorly on knee – attempt to dislocate hip. Ortolani: Abduct and push leg anteriorly at greater trochanter, attempt to relocate hip.Q: What are clinical indications for hip imaging in an infant? A: Clicky hip, asymmetric groin creases, breech presentation, family history of hip dysplasia, late onset of walking.Q: Is imaging needed in this case? A: YES. What might you consider? US if less than 4 months, Radiography if older than 4-6 months.Q: How do you know which imaging in which patients? A: ACR AC Developmental Dysplasia of the Hip –Child

https://acsearch.acr.org/docs/69437/Narrative/
Further reading: World J Orthop. 2013 Apr 18;4(2):32-41. doi: 10.5312/wjo.v4.i2.32. Print 2013 Apr 18. Developmental dysplasia of the hip in the newborn: A systematic review.
Slide 31 Compare the configuration of the normal and abnormal acetabulum and hip locationsQ: How do you characterize the hip in the abnormal? A: out too far laterally, up too far.Q: Which has the deeper acetabulum? A: The normal has a deep acetabulum, tucked well under the iliac bone. The abnormal acetabulum is shallow, and allows hip to slide out and up.
Slide 32 • Was this the right exam to do? A. Yes, according to the ACR AC, if the child is 4-6 months of age or older (when the when femoral head ossification centers appear) , with clinical findings suspicious for DDH (Clicky hip, asymmetric groin creases, breech presentation, family history of hip dysplasia, late onset of walking).
Q. What is wrong? A. bilateral abnormal hip location.Q. So how do we determine if this radiograph is normal or not?
Slide 33 Use this slide to make the point to learners that the region in yellow is the nonossified cartilaginous portion of the femoral heads that we don’t see that on the radiographs and the blue is the ossified.
Slide 34 First a little anatomy. Note the pseudoacetabulum on the left = the area on the ilium which the femoral head is articulating with .
Slide 35 For radiographic analysis of infants’ hip joints, the radiologist draws a variety of lines and angles that serve to characterize if the acetabulum is normally deep, keeping the femoral head of the hip joint properly located, or if it is abnormally shallow and likely to be unstable causing hip dysplasia as the child grows. Naming and explanation of these lines is not in the scope of our objectives, just so they know that we take some measurementss.
Nice short Radiopaedia article on how the analysis is done with illustrations is here: http://radiopaedia.org/articles/developmental-dysplasia-

of-the-hip
Slide 36 Compare the configuration of the normal and abnormal acetabulum and hip locations
Q: How do you characterize the hip in the abnormal? A: out too far laterally, up too far.Q: Which has the deeper acetabulum? A: The normal has a deep acetabulum, tucked well under the iliac bone. The abnormal acetabulum is shallow, and allows hip to slide out and up.
Slide 37Q. What is this? A. Missed opportunity to prevent debilitating disease. A cautionary tale. This child had bilateral hip dysplasia that was not treated.Q. How do we prevent this crippling deformity? A. Screening exams and early use of appropriate treatment.
Slide 38 Questions like that can be a challenge if you don’t have a good resource for evidence based clinical decision support, but no worries we have that, remember the ACR Appropriateness Criteria. Easy to find.Don’t spend more than 30 seconds on these 2 slides. Point out that variant scenarios exist and there are different recommendations for them, mainly US versus X-ray with a 4 month age cutoff for US.
Slide 39 Don’t spend more than 30 seconds on these 2 slides. Point out that variant scenarios exist and there are different recommendations for them, mainly US versus X-ray with a 4 month age cutoff for US.
Slide 40 Child is positioned lateral decubitus with the knees and hips flexed, and the transducer is placed on the lateral aspect of the child’s buttock, over the hip joint and iliac bone. (NOTE: The child with the ultrasound is younger than the x–ray. Remember, we cannot do the US after the hip ossifies.) See if they can spot femoral head and ilium on the ultrasound

Slide 41 May want to use this slide to orientate learners. Corresponding anatomy is shown with a red line
Slide 42 This is a normal hip US. Nice normal steep acetabulumIn ultrasound, we report an ‘alpha angle’ which should be >60. We also say how deep the femoral head is seated in the acetabulum (should be >50% covered)If you want, you could describe how we ‘stress’ the hip to see if it is stable.
Slide 43 This hip has mild DDH with shallow acetabulum – more than half the femoral head is out of the acetabulum. Also the alpha angle is 45 degrees. Do you see the hyperechoic echoes that are reflected from developing ossified bone in the femoral head ossification centers? This means that the next exam has to be x-ray…
Q: How do you want to treat this? A: Try a Pavlik harness and recheck.
Slide 44 The most common treatment option. Casting and surgery are also used in more severe cases.
Slide 45 Q: What diagnoses do you worry about? A: Intussusseption, (viral gastroenteritis, malrotation, Meckel’s diverticulum, Gyn pathology, appendicitis)Q: How do you want toinitially investigate these hypotheses? A: Most centers would start with ultrasound, if available. If not, radiography is typically used.

Slide 46 An example of normal is provided on the left of the slide for comparison.
Q: What do you think about the distribution of bowel gas in our patient. A: Asymmetric . We don’t see much gas on the right. Loops we do see are a little dilated.Q: What is the worry? A: with intermittent severe abdominal pain and bloody stools, evaluation for intussusseption must be done.Q: How sensitive and specific do you think x-rays are for this? A: Not so good, and Ultrasound is increasingly used in diagnosis.
Radiographs in Intussusseption– Absence of bowel gas in the RLQ– Intraluminal convex filling defect in partially air-filled bowel loop (commonly at hepatic flexure)– Frequently normal (50%)
Slide 47 Q: What kind of intussusseption is depicted here? A: Ileo-colicQ: What is the most common site of intussusseption in children this age? A: Ileo-colicQ. What is the mechanism of intussusseption? A. loop of bowel, usually ileum, telescopes into more distal bowel, often cecum, and drags with it the mesentery and vessels. Tight squeeze in the distal bowel can compromise venous and perhaps arterial vessels, bowel necrosis is threatened.
Slide 48 Normal ultrasound in a portion of a child’s colon.
Q: What is the hypoechoic-anechoic portion? A: Normal colonic lumen, delimited by the normal laminar layers that are referred to as the “gut signature” where we see multiple layers of bowel wall. Normal bowel wall thickness is less than 2.5 mm for small bowel, and for the colon it is normally less than 2 mm. Peristalsis should be visible in healthy bowel segments, and the segments should be compressible.
Slide 49 Here are images of Lucky’s proximal colon. Compare to the normal image from another child.Image has intussusseption showing the of the entry of the portion of ileum (intussusseptum) that is abnormally within the colonic lumen (intussussipiens).Q: What part of bowel is usually affected? A: Ileocolic most commonQ: What is the usual pathologic lead point in children? A: 90% of all pediatric intussusceptions have NO pathologic lead pointQ: When are children most likely to have intussusseption? A: Usually in the first 2 years of life, 40% from 3-6 months, Rare in neonatesQ: What are the Symptoms of intussusseption? A: Pain, 90%; Vomiting, 90%; Mass, 60%; Blood per rectum, 60%

Slide 50 Here are images of Lucky’s proximal colon. See if they can identify the colon and ileum
1st image has intussusseption showing the of the entry of the portion of ileum (intussusseptum) that is abnormally within the colonic lumen (intussussipiens).2nd image cross section of the intussusseption, showing the ring of surrounding bowel and the telescoped portion of bowel and the mesentery and associated mesenteric lymph node. Target, donut or cinnamon bun sign. (Make separate slide)
Slide 51 This cross section of an ileo-colic intussusseption has been likened to a cinnamon bun, and some call it the “Cinnamon Bun Sign” on ultrasound.
Slide 52 Reduction enema.Q: What is the idea behind doing an enema as a therapeutic measure in intussusseption? A: exertion of intraluminal pressure in the colon will (hopefully) push the telescoped bowel back into positions.
Air enema is preferred, but some places still use or positive contrast (something radiodense. Examples are iodine containing water soluble contrast or even a barium suspension) with fluoro monitoring. Saline reduction under ultrasound monitoring is not yet mainstream, but is an emerging method that eliminates radiation.
Slide 53

Slide 54 (Orient learners to the reversed fluoroscopic gray scale where the air is light gray and bone is dark)
Q: What do we see? A: Air in the descending and transverse colon. The round meniscus is air outlining the intussusseptum in the distal transverse colon. (Point it out for learners, as this will likely not be obvious to the novice learner).
Slide 55 The intussusseptum has now been reduced as far as the iliocecal valve
Slide 56 Q: How do we know when the reduction attempt has been successful? A: When the air or barium reaches the ileum and begins filling small bowel loops located centrally in the child’s abdomen.Q. Can intussusseption recur? A. Yes, about 10-25% of time it does. So, it is important to admit and observe 24 h. Important to consult surgery, so they are aware of the patient, because if hydrostatic reduction is NOT successful, the surgical team needs to be ready to go to the OR quickly.Surgery is done for cases of intussusseption not reducible by radiological means.
Slide 57 Q: What diagnoses do you worry about?Q: How do you want to investigate these hypotheses?
Slide 58 Here is what the ACR/AC says. Use imaging in this way if patient has clinical context described by the variant title. Note that US is the top choice in this group, if available, with CT as the next most appropriate stepReinforce that CT scans are becoming a major source of radiation exposure in children and should be avoided if US available

Slide 59 Here are images from Lucky’s RLQ ultrasound.
Q: What are the findings? A: Dilated appendix, Hyperemia, Appendicolith, Surrounding fat stranding. Let’s see the image with some annotation
Slide 60 Here we can see all those abnormal findings.Q: What is the diagnosis? A: Appendicitis
(Image annotations drawn by Jeff Otjen )
Slide 61 Unfortunately, ultrasonographers cannot always find the appendix, and this is a different child, a little older than Lucky who had to get a CT.
Q: What are some reasons ultrasound may fail to find the appendix? A: Gas in bowel may obscure acoustic window, severe pain/tenderness, operator error, US may be NOT available. OBESE CHILDREN.Q: What are the findings in these images? A: An appendicolith in a child with appendicitis. Periappendiceal fat reticulation/stranding, dilated appendix with thick enhancing wall.Q: How do you know this is a child? A: The triradiate cartilage remains unfused in the acetabulae.
Slide 62 Q: What happened to this child? A: CT scan shows abscess formation in a child with appendicitis complicated with rupture. CT scan shows a rim enhancing complex fluid collection with an ovoid calcification (appendicolith) within.
Slide 63 Q: What diagnoses are you going to think about? A: if scrotal, think torsion, if not as clearly scrotal, might also include appendicitisQ: How will you proceed? A: Clarify that this I actually groin and abdominal painQ: Ideally, what imaging strategy is best? A: Ultrasound is most appropriate for both scrotal pain and abdominal pain in children

Slide 64 Appropriate Imaging in this setting is easy to remember, as there is only one variant tor Acute onset scrotal pain, child or adult.
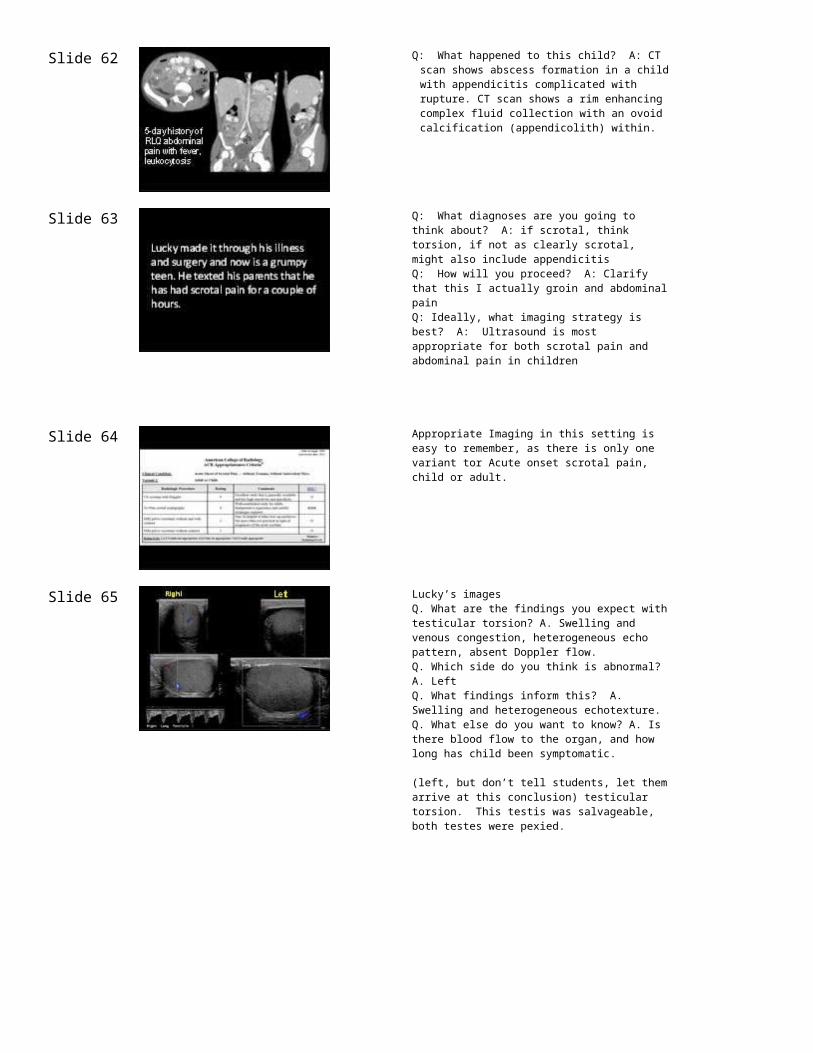
Slide 65 Lucky’s imagesQ. What are the findings you expect with testicular torsion? A. Swelling and venous congestion, heterogeneous echo pattern, absent Doppler flow.Q. Which side do you think is abnormal? A. LeftQ. What findings inform this? A. Swelling and heterogeneous echotexture.Q. What else do you want to know? A. Is there blood flow to the organ, and how long has child been symptomatic.
(left, but don’t tell students, let them arrive at this conclusion) testicular torsion. This testis was salvageable, both testes were pexied.
Slide 66Q. How do these patients present? A. abdominal pain and scrotal pain that is severe. Vomiting.Q. Why do we care? A. torsion is an emergency that threatens the organ and future fertility.Q. Who gets it? A. It is more common in children but occurs also in post pubertal males.
Important take home point :Time is of the essence. The salvage rates are approximately 100 % at 3 hours, 83-90 % at 5 hours, 75 % at 8 hours, and 50-70 % at 10 hours. The salvage rates decrease to 10 to 20 % when the testicle remains torsed for more than 10 hours. After 24 hours, salvage of a testicle is rare unless there has been intermittent detorsion.
Slide 67
Slide 68 Q: What is the abnormality? A: vey conspicuous heterogeneous echoes in the left testicle. This left testicle is not salvageable, and had to be removed due to nonviability.

Slide 69 Q: What do you worry about? A: This clinical presentation raises concern for epiglottitis.Q: What vaccination history should be sought? A: H. flu. Incidence has dropped 10-fold since vaccination has become standard care.Q: What is it important NOT to do in this clinical setting? A: do NOT lie the child down, do NOT open their mouth or look with a tongue depressor, as the child may acutely obstruct the airway.Q: Who will you call? A: Pediatric anesthesiaQ: What imaging might you order IF (and ONLY if) the child is stable? A: Soft tissue neck.
Slide 70 A: Lucky has Epiglottic thickening, and his Neck is flexed.
Have students show the normal epiglottis, vallecula, and aryepiglottic folds. Point out the true and false cords and laryngeal ventricle.
Slide 71 Q: What are the findings? (Ask students to point out the soft tissue structures that distort the upper airway, so they can exercise their skills in analyzing a soft tissue neck image.) A: Enlarged palatine tonsils. Lingual tonsils are normal… Adenoids are largish but palatine tonsils (the ones you would see on exam) are huge.
Slide 72
Slide 73
Slide 74