caffeine use, hours of sleep, and academic … · cause a cycle of inadequate sleep and caffeine...
TRANSCRIPT

CAFFEINE USE, HOURS OF SLEEP, AND ACADEMIC PERFORMANCE OF UNDERGRADUATE COLLEGE STUDENTS
A thesis submitted to the Kent State University College
of Education, Health, and Human Services in partial fulfillment of the requirements
for the degree of Master of Science
By
Danielle L. Gabrish

ii
May 2017
A thesis written by
Danielle L. Gabrish
B.S., Ball State University, 2015
M.S. Kent State University, 2017
Approved by
_________________________, Director, Master’s Thesis Committee Natalie Caine-Bish _________________________, Member, Master’s Thesis Committee Eun-Jeong (Angie) Ha _________________________, Member, Master’s Thesis Committee Tanya Falcone
Accepted by
_________________________, Director, School of Health Sciences Lynne E. Rowan _________________________, Interim Dean, College of Education, Health and Human Mark Kretovics Services

GABRISH, DANIELLE L., M.S., May 2017 Nutrition
CAFFEINE USE, HOURS OF SLEEP, AND ACADEMIC PERFORMANCE OF UNDERGRADUATE COLLEGE STUDENTS (124 pp)
Director of Thesis: Natalie Caine-Bish, Ph.D., RD., LD.
The primary objective of this study is to assess the difference in hours of sleep
and academic performance between caffeine users and non-caffeine users.
Participants were chosen based on current enrollment as a student for the spring 2017
semester at Kent State University. Students included both male and female of any age
and any more credits per semester at a Kent State. Exclusion criteria included students
reporting a history of a sleep disorder and participants not currently enrolled at Kent State
University. The study consists of a four section anonymous, Qualtrics online survey with
a series of questions regarding caffeine consumption, sleep, and academics. The total
amount (mg) of caffeine consumed and total sleep duration was determined for each
participant. Lastly, participants manually entered in their cumulative GPA. Data was
then collected and analyzed using SPSS statistical software using significance p<0.05.
An univariate ANOVA was used to compare both hours of sleep and GPA to the five
levels of caffeine consumption (non-caffeine, low, moderate, high and very high). A t-
test was used to compare both the hours of sleep and GPA between caffeine consumers

and non-consumers. A t-test was also used to compare both sex (males and females) and
grade level (freshman, sophomore, junior, and seniors) to the amount (mg) of caffeine
consumed. Results found that non-consumers have longer sleep duration (p=0.002) and
higher GPA compared to the consumers group (p< 0.001), non-caffeine consumers have
longer sleep duration compared to the high level of caffeine consumption (p=0.041), and
that males consume a greater amount (mg) of caffeine than females (p=0.024). There
were no significant differences (p>0.05) between the different levels of intake and GPA
and in grade levels and amount (mg) of caffeine consumed.

iii
ACKNOWLEDGMENTS
There are many individuals I would like to acknowledge in helping create this
thesis. I would like to first thank Dr. Natalie Caine-Bish for agreeing to be my advisor
and spending countless hours editing and providing feedback during the construction of
this thesis. Your insight, guidance, and patience were not overlooked. I would also like
to recognize the effort from my committee members Dr. Angie Ha and Tanya Falcone,
whom gave me incredible advice and feedback. I appreciate the time each committee
member took to help me in this process, especially when your schedules were so full. I
would also like to recognize my statistician Han Zhang, who took me on in such a short
amount of time. Lastly, I would like to thank the other dietetic interns at Kent State
because of their support for one another throughout the entire thesis process.

iv
TABLE OF CONTENTS
Page ACKNOWLEDGEMENTS ............................................................................................... iii LIST OF FIGURES .......................................................................................................... vii
LIST OF TABLES ........................................................................................................... viii CHAPTER I. INTRODUCTION ........................................................................................................ 1 Statement of the Problem .............................................................................................. 4 Purpose Statement ......................................................................................................... 6 Hypotheses .................................................................................................................... 6 Operational Definitions ................................................................................................. 7
II. REVIEW OF LITERATURE ...................................................................................... 8 Definition of Caffeine ................................................................................................... 8 Background Information on Caffeine ........................................................................ 8 Absorption .................................................................................................................. 9 Metabolism .............................................................................................................. 10 Excretion .................................................................................................................. 11 Sources of Caffeine ...................................................................................................... 13 Intake of Caffeine Sources in the College Population ............................................. 17 Coffee ................................................................................................................... 17 Soda ...................................................................................................................... 18 Tea ........................................................................................................................ 19 Energy drinks ....................................................................................................... 19 Alcohol ................................................................................................................. 20 Foods .................................................................................................................... 21 Regulations .............................................................................................................. 21 Recommendations of Daily Caffeine Intake ................................................................ 23 Current Average Caffeine Intake ............................................................................ 25 Reasons for Caffeine Use ......................................................................................... 27 Mental energy and performance .......................................................................... 27 Mood .................................................................................................................... 28 Sensory appeal ..................................................................................................... 29 Partying and social contexts ................................................................................. 29 Benefits of Caffeine Use .......................................................................................... 30 Cognitive and behavioral effects ......................................................................... 30 Mood .................................................................................................................... 31

v
Exercise and athletic performance ....................................................................... 31 Neurotransmitters ................................................................................................. 32 Negative Effects of Caffeine .................................................................................... 32 Cognitive and behavioral side effects .................................................................. 33 Caffeine withdrawal ............................................................................................. 33 Caffienism ............................................................................................................ 34 Cardiovascular ..................................................................................................... 35 Infertility .............................................................................................................. 35 Osteoporosis ......................................................................................................... 36 Dehydration .......................................................................................................... 36 Prevalence of Caffeine Overdose ............................................................................. 37 Definition of Sleep ....................................................................................................... 39 Sleep Cycles ............................................................................................................. 39 Circadian Preference ................................................................................................ 40 Function of Sleep .................................................................................................... 41 Current Average Hours and Recommendation of Sleep for College Students ........ 42 Consequences of Sleep Deprivation ........................................................................ 43 Factors Affecting Sleep ............................................................................................ 45 Stress .................................................................................................................... 45 Caffeine use ......................................................................................................... 46 Alcohol ................................................................................................................. 47 Smoking ............................................................................................................... 48 Environmental ...................................................................................................... 49 Definition of Academic Performance .......................................................................... 49 Use of Grade Point Average in Assessing Academic Achievement ........................ 50 Caffeine and Academic Performance ...................................................................... 51 Sleep and Academic Performance ........................................................................... 52 III. METHODOLOGY .................................................................................................. 54 Research Design .......................................................................................................... 54 Research Sample ......................................................................................................... 55 Procedures ................................................................................................................... 55 Research Measures ...................................................................................................... 56 Statistical Analysis ...................................................................................................... 57
IV. JOURNAL ARTICLE ............................................................................................. 58 Introduction ................................................................................................................. 58 Methodology ............................................................................................................... 60 Research Design ....................................................................................................... 61 Research Sample ...................................................................................................... 61 Procedures ................................................................................................................ 62

viiii
Research Measures ................................................................................................... 62 Statistical Analysis ................................................................................................... 63 Results ......................................................................................................................... 64 Demographic Details of Participants ....................................................................... 65 Significant Differences in Sleep Between Caffeine Consumers and Non-consumers ........................................................................................................ 66 Significant Differences in Sleep and Levels of Caffeine Consumption .................. 66 Significant Differences in GPA Between Caffeine Consumers and Non-consumers ........................................................................................................ 68 Differences in GPA and Levels of Caffeine Consumption ..................................... 68 Significant Differences in Sex and Caffeine Consumption ..................................... 69 Differences in Grade Levels and Caffeine Consumption ........................................ 70 Discussion ................................................................................................................... 71 Caffeine Consumption ............................................................................................. 71 Sleep ...................................................................................................................... 71
Academic performance ......................................................................................... 74 Sex ......................................................................................................................... 76 Grade levels .......................................................................................................... 76
Applications ................................................................................................................ 78 Limitations .................................................................................................................. 80 Conclusion .................................................................................................................. 81
APPENDICES .................................................................................................................. 83 APPENDIX A. SURVEY EMAILS ........................................................................... 84 APPENDIX B. SURVEY QUESTIONNAIRE ........................................................... 87 APPENDIX C. CONSENT FORM ............................................................................. 93 REFERENCES ................................................................................................................. 96

vii
LIST OF FIGURES
Figure Page
1. Caffeine Pathway .................................................................................................. 13
2. Significant Difference in Mean Hours of Sleep Between Caffeine Consumers
versus Non-Caffeine Consumers ......................................................................... 66
3. Mean Hours of Sleep for Each Level of Caffeine Consumption in Undergraduate
College Students .................................................................................................. 67
4. Significant Differences of Mean Cumulative GPA Between Caffeine Consumers
and Non-consumers .............................................................................................. 68

viii
LIST OF TABLES
Table Page
1. Caffeine Content of General Food and Beverages ............................................... 15
2. Caffeine Content of Medications, Snacks, and Supplements .............................. 16
3. Frequency and Percentage of Sex (n=2876), Grade Level (n=2868), and Ethnicity
(n=2876) of Caffeine Consumers and Non-Consumers of Undergraduate College
Students ................................................................................................................ 65
4. Mean GPA and Significance between Levels of Caffeine Consumption in
Undergraduate College Students (n=876) ........................................................... 69
5. Significant Difference Between Sex and Amount of Caffeine (mg) Consumed .. 69
6. Frequency, Percentage, Mean, and Standard Deviation of Total Caffeine (mg)
Consumed in Grade Levels of Undergraduate Students ...................................... 70

1
CHAPTER I
INTRODUCTION
Insufficient sleep and varying sleep schedules have been widely reported in the
college population, with 28% of students reporting daytime sleepiness (Tran et al., 2014)
and 25% of students reporting less than six and a half hours per night (Lund et al., 2010;
Tsai, 2004). Inadequate sleep can lead to daytime sleepiness and sleep deprivation
(Bulboltz, Brown, & Soper, 2001; Gaultney, 2010; Pilcher, Douglass, & Sadowsky,
1997). In the college population, stress can occur due to intrapersonal, environmental,
interpersonal, and academic reasons (Ross, Niebling, & Heckert, 1999). Academic and
emotional stress, tension and worry are the most common reasons for decreased duration
and quality of sleep in college students but also include social situations, cosleeping, and
excess noise (Buysse et al., 1988; Ginsberg, 2006; Lund et al., 2010; Plaford, 2009; Tsai
& Li, 2004). To help cope with this sleep loss and be able to fulfill academic duties,
students often rely on caffeine (Lazarus, 1993; Lieberman et al., 2015; Thoitis, 1995).
Caffeine is used by approximately 92% of college students, 65% using caffeine on a daily
basis, with an average of 159 to 849.86 mg caffeine consumed per day (Lieberman et al.,
2015; McIlvain, Noland & Bickel, 2011). During times of increased academic stress,
63% of college students have reported an increase in their caffeine intake (Oaten and
Cheng, 2005; Tannous & Kalash, 2014).

2
Sleep is a physical and mental necessity for basic human functioning. For college
students, seven to nine hours of sleep per night is recommended; some individuals may
need as little as six hours and up to 10-11 hours of sleep per night (Hirshkowitz et al.,
2015). Inadequate sleep, less than six hours per night, can lead to acute or chronic sleep
deprivation. On average, college students sleep approximately seven hours per night.
Twenty-five percentage of students report receiving less than six and a half hours of sleep
per night while 29.4% report sleeping at least eight hours. This number varies on the
weekends and weekdays, with more sleep being acquired on weekends (Lund et al.,
2010). Sleep deprivation is harmful on the health of an individual and can effect the
consolidation of memory, alertness and mood, cardiovascular system, immune system,
hormone, temperature, and glucose regulation (Colten & Altevogt, 2006; Horne, 1988;
Lund et al., 2010; Plaford, 2009).
Caffeine is a central nervous system (CNS) stimulant and mild diuretic found in
over 60 species of plants (Heckman et al., 2010; Institute of Medicine (U.S.) Committee
on Military Nutrition Research, 2001; Katan & Schouten, 2005; Mahan & Escott-Stump,
2008; Parliment, Ho, & Schieberle, 2000; Somogyi, 2010; Merriam Webster; Winston,
Hardwick & Jaberi 2005). It works through the competitive binding of adenosine
receptors, effecting dopamine, serotonin, and norepinephrine (Basheer, Strecker,
Thakker, & Mccarley, 2004; Gupta & Gupta, 1999; Institute of Medicine (U.S.)
Committee on Military Nutrition Research, 2001; National Center for Biotechnology
Information, n.d.; Winston, Hardwick & Jaberi, 2005). While caffeine can be found
naturally or artificially in a number of products, the most common include coffee, tea,
3
soda, and chocolate (FDA 2010; Heckman et al., 2010; Nawrot et al., 2003; Winston et
al., 2005).
Caffeine is not a nutrient and its intake is not required for a healthy diet, but it is
generally considered safe in moderate amounts (<400mg/day) (USDA, 2015). Caffeine
causes a series of physiological changes, including increased secretion of the stress
hormone cortisol (Al'Absi et al., 1998; Lovallo et al., 2006; Randall, 2011). At low to
moderate caffeine consumption, perceived benefits include improved cognitive and
behavioral effects, enhanced mood, and potentially increased neuroprotection against
certain disease (Garrett & Griffiths, 1997; Guerreiro et al., 2008; Gupta & Gupta, 1999;
Institute of Medicine (U.S.) Committee on Military Nutrition Research, 2001; Parliment,
Ho, & Schieberle, 2000; Schardt, 2015; Tieges et al., 2007; Uchida, Kadowaki-Horita, &
Kanda, 2014). Higher doses of caffeine can cause various, negative side effects including
restlessness, excitement, tremors, dizziness, headaches, and insomnia (UNEP, 2013) and
very high doses may cause nausea, vomiting, convulsions, tachycardia, and even death
(Gilman, Rall, T.W., Nies, A.S., & Taylor, 1990; Institute of Medicine (U.S.) Committee
on Military Nutrition Research, 2001; Winston et al., 2005).
The role of sleep has been shown to be very important to perform academically,
but the upcoming stress of exams often leads to decreased sleep quality (Abraham &
Scaria, 2015; Gaultney, 2010; Zunhammer, Eichhammer, & Busch, 2014). Poor quality
and quantity of sleep in college students has a negative impact on the performance of
students (Abraham & Scaria, 2015; Becker et al., 2008; Gaultney, 2010). Caffeine’s
effect on increasing the stress hormone cortisol and its impact on the sleep cycles may

4
cause a cycle of inadequate sleep and caffeine consumption and, therefore, long-term
sleep deprivation. This cycle may have a substantial effect on the academic achievement
of students, since a decrease in quality of sleep has been shown to negatively effect
academic performance. Recent studies have shown a negative correlation between
energy drink consumption and decreased grade point averages (Champlin, Pasch, &
Perry, 2016; Pattison, Rusin, & Bai, 2016; Pettit & Debarr, 2011). This is further an
issue for the large percentage of students reporting decreased sleep as well as increased
caffeine consumption during times of academic stress.
Statement of the Problem
Caffeine consumption is high in the college-aged population due to the appeal of
caffeine’s perceived effects on improved performance, counteracted fatigue, and elevated
mood (Gupta & Gupta, 1999; Kristiansen et al., 2005; Parliment, Ho, & Schieberle, 2000;
Winston et al., 2005). Caffeine intake has been found to be up to 850 mg/day in college
students (McIlvain, Noland & Bickel, 2011) while the recommendation for adults is a
moderate intake of <400 mg/day (Mayo Clinic; Johns Hopkins). Caffeine also increases
the release of the stress hormone cortisol, which may be problematic for those that use
caffeine to cope and the high percentage of students reporting an increase in caffeine
consumption during times of academic stress (Al'Absi et al., 1998; Lieberman et al.,
2015; Oaten and Cheng, 2005; Tannous & Kalash, 2014). Recent research has even
indicated that there is a negative correlation between grade point average and both the

5
dosage and intake frequency of energy drinks consumed (Champlin, Pasch, & Perry,
2016; Pattison, Rusin, & Bai, 2016; Pettit & Debarr, 2011).
Caffeine has an effect on both the REM and NREM sleep cycle, resulting in
decreased sleep quality and/or increased sleep latency (Carrier et al., 2009; James, 1991a;
Karacan et al., 1976; Nicholson & Stone, 1980; Smith, 2002). To make up for this lack
of sleep, individuals may rely on caffeine the next day to counteract the daytime
sleepiness, leading to a cycle of caffeine use and sleep deprivation (Winston, Hardwick,
& Jaberi, 2005; Champlin, Pasch, & Perry, 2016; Schardt, 2015). This sleep deprivation
is common in college students, with over 48% having short sleep time and 28% reporting
daytime fatigue, which poses problems on the mental and physical health (Curcio,
Ferrara, & De Gennaro, 2006; Dickelmann and Born, 2010; Lund et. al., 2010; Plaford,
2009; Tsai & Li, 2004). Students with low overall sleep quality tend to have lower
GPA’s compared to those who report adequate sleep quality (Curcio, Ferrara, & De
Gennaro, 2006; Dewald et. al., 2010; Taylor, et. al., 2011; Orzech, Salafsky, & Hamilton,
2011).
While caffeine may be used to keep a student energized to perform academic
duties, its use affects the sleep cycle, causing the quality of sleep to suffer. Sleep quality
is essential in the academic setting and when decreased, leads to poorer performance and
reduced grade point averages (Abraham & Scaria, 2015; Becker, Adams, Orr, & Quilter,
2008; Gaultney, 2010). While studies have a shown an effect of caffeine on sleep and of
sleep on academic performance, there is a lack of research assessing the relationship
between all three variables. With the high amount of college students consuming caffeine

6
and reported insufficient sleep, the impact of these on academic performance needs to be
further researched.
Purpose Statement
The purpose of this study is to assess the difference in hours of sleep and
academic performance between caffeine users and non-caffeine users.
Hypotheses
H1= There is a difference in the hours of sleep between caffeine users versus non-caffeine
users
H2= There is a difference among the different levels of caffeine consumed and hours of
sleep.
H3= There is a difference in academic performance between caffeine users versus non-
caffeine users
H4= There is a difference among the different levels of caffeine consumed and academic
performance.
H5= There is a difference between the sex and amount of caffeine (mg consumed).
H6= There is a difference between grade levels and amount of caffeine (mg consumed).
7
Operational Definitions
College undergraduate students- full and part-time undergraduate male and female
students enrolled and registered for classes for the 2017 spring semester at Kent State
University.
Grade Level- The current grade status (freshman, sophomore, junior, or senior) of the
Kent State University student.
Level of Caffeine Consumption- The categorized total amount (mg) of caffeine
consumed daily.
Very high caffeine consumer- Intake of > 750 mg of caffeine per day
High caffeine consumer- Intake of 501-750 mg of caffeine per day
Moderate caffeine consumer- Intake of 201-500 mg of caffeine per day
Low caffeine consumer- Intake of 5-200 mg of caffeine per day
Non-caffeine consumer- The absence of caffeine intake from dietary sources and
forms
Hours of sleep- The approximate duration (hours) of sleep per night.
Academic performance- The educational performance demonstrated by the student as
assessed by current cumulative grade point average.

8
CHAPTER II
REVIEW OF LITERATURE
Definition of Caffeine
Caffeine is a 1,3,7-trimethylxanthine, whose chemical structure, C8H10N4O2, is
similar to the purines (Institute of Medicine (U.S.) Committee on Military Nutrition
Research, 2001; Oestreich-Janzen, 2016) that can be defined as a “white, bitter crystalline
alkaloid compound” that is used medicinally as a stimulant of the central nervous system
and also as a diuretic (Institute of Medicine (U.S.) Committee on Military Nutrition
Research, 2001; Parliment, Ho, & Schieberle, 2000; Somogyi, 2010; Merriam Webster;
Winston, Hardwick & Jaberi 2005).
Background Information on Caffeine
Caffeine is the most internationally used psychoactive substance (Fredholm 1995;
Heckman, Weil, & Gonzalez, 2010; Institute of Medicine (U.S.) Committee on Military
Nutrition Research, 2001; Winston et al., 2005). Caffeine is consumed daily by
approximately 90% of individuals worldwide, and 80% in the U.S. (Food and Drug
Administration [FDA], 2007). In the U.S., approximately 95-98% of caffeine consumed
coming from beverages and 1.7-4.2% from foods (Somogyi, 2010). While caffeine is
widely known for its “stimulant properties,” it is not clear how this action is preformed
(Daly, 1993; Fredholm, Arslan, Johansson, Kull, & Svenningsson, 1997; Garrett &

9
Griffiths, 1997; Nehlig, Deval, & Debry 1992). The most commonly accepted
mechanism is that caffeine’s similar structure to adenosine allows it to bind to A1 and A2
receptor sites, blocking the binding of adenosine (Basheer, Strecker, Thakker, &
Mccarley, 2004; Gupta & Gupta, 1999; National Center for Biotechnology Information,
n.d.; Nawrot et al., 2003; Winston, Hardwick & Jaberi, 2005). As cited in the U.S.
National Library of Medicine (n.d.), caffeine also “competitively inhibits
phosphodiesterase, which is the enzyme that degrades cyclic 3',5'-adenosine
monophosphate (AMP).” This competitive blocking causes an “indirect” effect of other
neurotransmitters, including ACh, gamma-aminobutyric acid (GABA), dopamine,
serotonin, and norepinephrine (Institute of Medicine (U.S.) Committee on Military
Nutrition Research, 2001). Caffeine dilates peripheral blood vessels and stimulates all
areas of the central nervous system, including “medullary, vagal, vasomotor, and
respiratory centers” especially when taken in higher doses (U.S. National Library of
Medicine. (n.d.). This stimulation of the respiratory center can lead to vasoconstriction
and an elevated respiratory rate (U.S. National Library of Medicine, n.d.).
Absorption
Approximately 90% of caffeine is “removed from the stomach” after twenty
minutes of absorption and 99% of caffeine is absorbed within one hour after ingestion
from the stomach/intestines, but can also be absorbed directly from the lining of the
mouth (Oestreich-Janzen, 2016; Preedy, 2012). The liver processes caffeine and allows
absorption into the bloodstream (Preedy, 2012). Once absorbed, the caffeine is circulated

10
throughout the body’s “fluid and cells,” including the brain, in which it is thought to
move freely from blood to the brain, allowing effects on the central nervous system
(CNS) (Institute of Medicine (U.S.) Committee on Military Nutrition Research, 2001;
Lorist & Tops, 2003; Oestreich-Janzen, 2016; Preedy, 2012). Certain caffeine sources
are absorbed more quickly, such as chewing gum, gel patches for the skin, and “vapor
sticks,” which ate similar to e-cigarettes (Oestreich-Janzen, 2016).
Metabolism
After absorption, caffeine then binds to plasma proteins, peaking approximately
15-120 minutes after ingestion (Institute of Medicine (U.S.) Committee on Military
Nutrition Research, 2001; UNEP Publications, 2003). According to Gropper, Smith, &
Groff (2009), caffeine “increases blood flow to the kidneys” and “stimulates” the adipose
tissue to release fatty acids.” The liver breaks down caffeine into the following
percentage of metabolites- 84% paraxanthine, 12% theobromine, and 4% theophylline
(Gonzalez de Mejina & Ramirez-Mares, 2014; Kalow & Tang, 1993; UNEP Publications,
2003). Caffeine is N3-demethylated into paraxanthine through catalyzation of
cytochrome P450 (also called CPY), which consists of two subtypes- 1A2 (the primary
isoenzyme) and 2E1 (Guerreiro, 2008; U.S. National Library of Medicine, n.d.). Uric
acid and uracil derivatives (such as 5-acetylamino-6-formylamino-3-methyluracil,
theobromine and paraxanthine) are formed through this demethylation as well as
“hydroxylation of the eighth position” (U.S. National Library of Medicine, n.d.; UNEP
Publications, 2003). The liver is the organ excreting the caffeine metabolites, with only

11
2% non-metabolized caffeine being excreted by the kidneys (Preedy, 2012). As cited by
Preedy (2012), “caffeine blocks the adenosine receptors, inhibits cAMP
phosphodiesterase activity, mobilizes calcium intracellularly, and binds to
benzodiazepine receptors.” This chain of events is what makes caffeine is a central
nervous system stimulant. CYP1A2 activity differs genetically in each person, which is
why caffeine metabolism varies on an individual basis (Butler et al., 1992; Guest,
Jamnik, Womack, & El-Sohemy, 2015; Whoriskey, 2015). Also, during pregnancy,
caffeine metabolism is decreased, creating higher serum concentrations (UNEP
Publications, 2003).
There is a difference of metabolism varies based on sex, age, and smoking
(Nawrot et al., 2003). Women typically have 20-30% shorter caffeine half-life than
males (Nawrot et al., 2003). During pregnancy, the half-life of caffeine begins at four
hours in the first trimester and increases to approximately 18 hours by the third trimester
(Nawrot et al., 2003). The half-life of caffeine is two times shorter in smokers (Nawrot
et al., 2003). The half-life of caffeine in infants ranges 50 to 100 hours and slowly
declines until age 6 months, where the half-life is approximately the same as adults
(Nawrot et al., 2003). Until 9 months of age, infants cannot metabolize caffeine very
well, resulting in 85% being excreted.
Excretion
In the liver, caffeine is broken down via demethylation (Oestreich-Janzen, 2016).
Caffeine is oxidized to uric acid, its imidazole ring is cleaved, and then it is further
broken down to ammonia where it can then be “exhaled as carbon dioxide” (Oestreich-

12
Janzen, 2016). Most of the caffeine is excreted in the urine as the metabolite
paraxanthine with hardly any of the caffeine excreted intact (Institute of Medicine (U.S.)
Committee on Military Nutrition Research, 2001; Kalow & Tang, 1993; Oestreich-
Janzen, 2016). More than 95% of caffeine is excreted via urination, with small amounts
excreted via bile, saliva, semen, and breast milk (UNEP Publications, 2003). The half-
life of caffeine in humans varies in studies- from one and a half hours up to nine and a
half hours, averaging five hours (Institute of Medicine (U.S.) Committee on Military
Nutrition Research, 2001; Lorist & Tops, 2003; Smith, 2002) and two and a half to four
and a half hours in another source (UNEP Publications, 2003). Infants and fetuses have
less P450 activity than adults, thus allowing them to have a more extended half life
compared to adults (Preedy, 2012). A study conducted by Patwardhan, Desmond,
Johnson, and Schenker (1980) found that the half-life for 250 mg of caffeine was
approximately 6.2 hours for both men and women. Certain factors affect the clearance of
caffeine. Oral contraceptives almost double the half-life of caffeine, while the use of
nicotine increases the clearance rate by 30-50% (Abernethy & Todd, 1985; Lorist &
Tops, 2003; Patwardhan et al., 1980; Preedy, 2012). Alcohol consumption decreases
caffeine metabolism as seen in a study by George et al. (1986), where 50 grams of
alcohol a day increased the half life by 72% and decreases clearance by 36%. Figure 1
shows the movement of calcium to different parts of the body and the routes to organs.

13
Figure 1. Caffeine Pathway (Gonzalez de Mejina & Ramirez-Mares, 2014)
Sources of Caffeine
Over 60 species of plants contain caffeine (Somogyi, 2010; Heckman et al., 2010;
Katan & Schouten, 2005; Mahan & Escott-Stump, 2008). Cocoa, coffee beans, and tea
are the most “commonly cultivated,” while guarana, kola nuts, and yerba mate generally
has their caffeine removed and used as additive in commercial products (Frary, Johnson,
& Wang, 2005; Heckman et al., 2010; Parliment, Ho, & Schieberle, 2000; Rosenfeld,
Mihalov, Carlson, & Mattia, 2014; Somogyi, 2010). Commercial sources with caffeine
added often uses caffeine taken from decaffeination process of coffee or with synthetic
caffeine, also called anhydrous caffeine (Somogyi, 2010). Commercial beverage sources
include soda, energy drinks, energy shots, and caffeinated alcoholic beverages, and
14
certain snacks such as chips, gum, and mints (Somogyi, 2010). Of the various sources,
coffee, tea, chocolate, and soft drinks are consumed most often (FDA 2010; Heckman et
al., 2010; Nawrot et al., 2003; Winston et al., 2005). Snacks and baked goods may also
contain caffeine if they contain a natural source of caffeine such as foods containing
chocolate (Somogyi, 2010). Table 1 lists various caffeine sources and the amount of
caffeine (mg) from foods and beverages.
Stimulant drinks, also known as energy drinks, was introduced in 1987 (Finnegan,
2003) and some brands have higher caffeine content than “natural sources” of caffeine
(Pettit & DeBarr, 2011; Somogyi, 2010). Roberts (2006) explains that energy drinks
typically have around, or maybe a little less, caffeine than soda, but the other ingredients
that are added-sugar, herbal stimulants (guarana and ginseng), and taurine- creates a
“synergistic effect.” Also, taurine itself increases the effects of caffeine on the body
(Roberts, 2006). These stimulant beverages have become more popular, where 26.3
million gallons were sold in 2001 and increased to 354.5 million gallons in 2009
(Beverage World, 2010). While energy drinks can vary significantly in the amount of
caffeine, the 2008 Beverage Marketing Corporation, as cited by Somogyi (2010), states
that the average content is “50 mg caffeine per 100 ml serving.”
Another source is caffeine powder, which is made of up 100% caffeine and is
available to consumers online (FDA, 2015). One teaspoon of caffeine powder is equal to
approximately 28 cups of coffee (FDA, 2015). Pharmaceuticals such as diet pills,
diuretics, proprietary analgesics, and cold and flu “remedies” may also contain caffeine
(Somogyi, 2010; Winston et al., 2005). Some common names for these pharmaceuticals

15
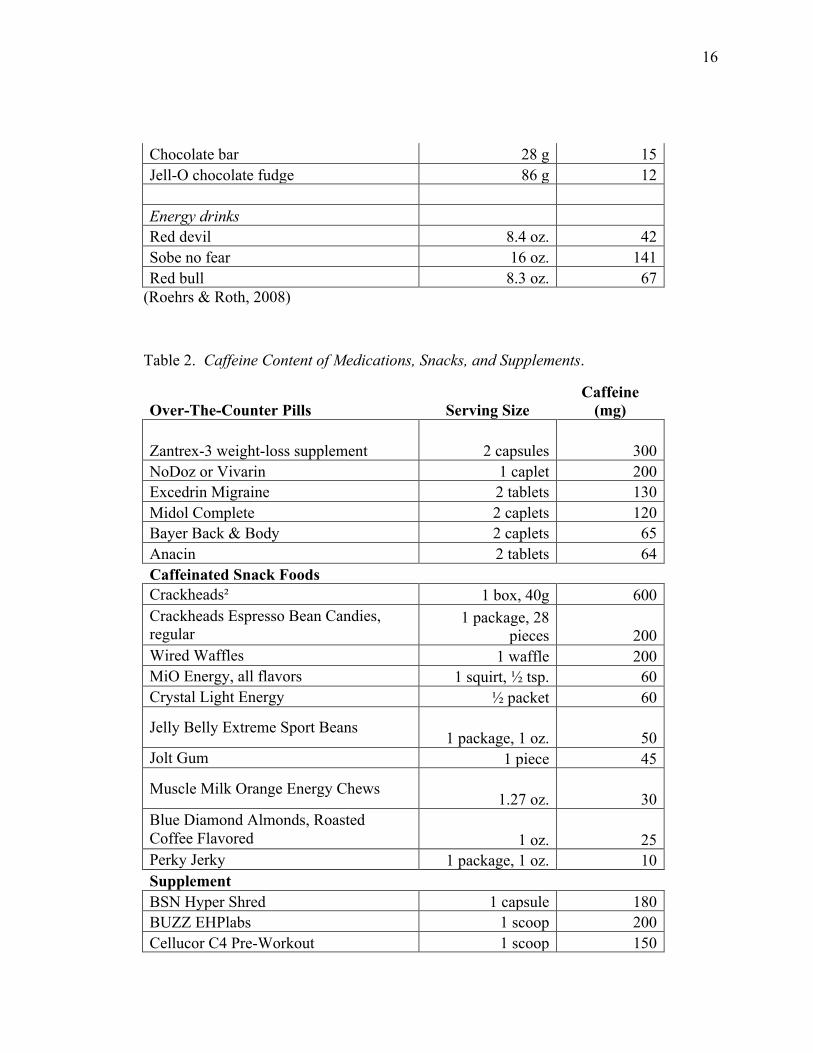
are Excedrin and NoDoz/Vivarin (Mahan & Escott-Stump, 2008). Table 2 lists various
caffeine sources and amount (mg) used in pharmaceuticals, snack foods and supplements.
There are other, non-edible caffeine products on the market. ThinkGeek manufactured a
soap product that contains caffeine called Shower Shock Caffeinated Soap. The
manufacturer claims it contains “12 servings/showers per 4 ounce bar with 200
milligrams of caffeine per serving” (ThinkGeek, n.d.)
Table 1. Caffeine Content of General Food and Beverages.
Product Serving Size Caffeine
(mg) Coffees Brewed-graved 8 oz. 80-135 Instant 8 oz. 40-108 Drip 7 oz. 115-175 Espresso 2 oz. 100 Starbucks, regular 16 oz. 259 Decaffeinated 8 oz. 5-6. Teas Leaf teas 7 oz. 50-60 Instant 7 oz. 30 Bottles 8 oz. 40-80 Soft drinks Jolt 12 oz. 71 Mountain dew 12 oz. 58 Mellow Yellow 12 oz. 53 Coca-Cola 12 oz. 45 Dr. Pepper 12 oz. 41 Pepsi Cola 12 oz. 37 RC Cola 12 oz. 36 Candies & desserts Chocolate baking 28 g (10 oz.) 25 Chocolate chips 43 g (1/4 cup) 15
16
Chocolate bar 28 g 15 Jell-O chocolate fudge 86 g 12 Energy drinks Red devil 8.4 oz. 42 Sobe no fear 16 oz. 141 Red bull 8.3 oz. 67
(Roehrs & Roth, 2008)
Table 2. Caffeine Content of Medications, Snacks, and Supplements.
Over-The-Counter Pills Serving Size Caffeine
(mg)
Zantrex-3 weight-loss supplement 2 capsules 300 NoDoz or Vivarin 1 caplet 200 Excedrin Migraine 2 tablets 130 Midol Complete 2 caplets 120 Bayer Back & Body 2 caplets 65 Anacin 2 tablets 64 Caffeinated Snack Foods
Crackheads² 1 box, 40g 600 Crackheads Espresso Bean Candies, regular
1 package, 28 pieces 200
Wired Waffles 1 waffle 200 MiO Energy, all flavors 1 squirt, ½ tsp. 60 Crystal Light Energy ½ packet 60
Jelly Belly Extreme Sport Beans 1 package, 1 oz. 50
Jolt Gum 1 piece 45
Muscle Milk Orange Energy Chews 1.27 oz. 30
Blue Diamond Almonds, Roasted Coffee Flavored 1 oz. 25 Perky Jerky 1 package, 1 oz. 10 Supplement
BSN Hyper Shred 1 capsule 180 BUZZ EHPlabs 1 scoop 200 Cellucor C4 Pre-Workout 1 scoop 150

17
GNC Amp (Pre-Post) 3 tablets 400 GNC Raw Ravage 1 scoop 200 Juggernaut HP 1 scoop 150 Muscle Marinade 1 scoop 300 Muscle Pharm Assault 1 scoop 300 MuscleXplosion 1 pouch 60 Oxyelite Pro 1 capsule 100 Pre JYM 1 scoop 300 SportMax Preworkout Shot 1 bottle 140
(Caffeine Informer, 2016; Center for Science in the Public Interest, n.d.)
Intake of Caffeine Sources in the College Population
The most popular sources of caffeine in United States colleges are coffee, soda,
tea, and chocolate (NACS, 2012; National Association of College Stores, 2012; Tannous
& Kalash, 2014; Traylor & Summers, n.d.). Other sources consumed also energy drinks
and other food products (Attila & Çakir, 2011). Alcohol mixed with caffeinated
beverages is also common in college students (O’Brien, McCoy, Rhodes, Wagoner &
Wolfson, 2008; Marczinski, 2011).
Coffee. In the college population, coffee is the most commonly consumed source
of caffeine, where 41% of college students reported coffee as being the most difficult
source of caffeine to give up (Traylor & Summers, n.d.). The percentages of college
students daily coffee use is sporadic in the literature, ranging from 57 to 71% for 18-24
year olds (Frary et al., 2005; Mitchell et al., 2003; Traylor and Summers (n.d.). Another
study found that 43% of college students reported hot coffee use, 21% “specialty coffee
drinks,” 15% iced coffee drink (National Association of College Stores [NACS], 2012).

18
Zagat’s 2015 Coffee Survey asked American’s what their favorite type of coffee, 24%
said a regular cup of coffee, 17% latte, 12% cappuccino, 8% espresso, 8% americano, 5%
flavored latte, 5% iced coffee, and 21% said other. A study by Tannous and Kalash
(2014) found that 97% of students reported consuming caffeinated products and
beverages- 9.7% consumed Nescafé, 12.4% cappuccino, 9.8% coffee, and 3.3%
consumed espresso. As to where American’s purchase their coffee, 43% make it at home
or get it from work, 26% get it from a large national chain, 22% from a small or
independent chain, and 9% reported getting it from “other” (Zagat, 2015). When
comparing genders, a seven-day beverage recall of college students found that females
consumed more hot coffee (37% female; 32% male) and more specialty coffee drinks
(25% female; 16% male) than males (Cozart & Riddle, 2011).
The true caffeine content of coffee can vary greatly depending on the environment
the coffee was grown, and roasting, brewing, and grounding method (Roberts, 2006). A
study conducted at the University of Florida (2003) periodically sampled the caffeine
content of coffees from various shops. When sampling the same Starbucks 16 oz., it was
found that the same beverage ranged from 259mg to 564 mg of caffeine. While
decaffeinated coffee has the caffeine extracted, not all of the caffeine can be eliminated
from the product, thus the end product still contain traces of caffeine. The same Florida
study (2003) found up to 18 mg caffeine per 16oz cup of decaf coffee.
Soda. According to Schardt (2015), 70% of sodas on the market contain caffeine.
Soda is the second most commonly consumed caffeine source in the college population,
with a range of 15% (Tannous & Kalash, 2014) to 70% of students reporting
19
consumption on a daily basis (Frary et al., 2005; Mitchell et al., 2013; Traylor &
Summers, n.d.). In a study conducted by Cozart and Riddle (2011), 52% of students
reported drinking soda in the past week, with 24% drinking diet soda. The same study
also found that females consumed more diet soft drinks (25% female; 20% male) while
males consumed more non-diet soft drinks (61% male; 58% female) (Cozart & Riddle,
2011).
Tea. The daily caffeinated tea consumption in the college population varies, with
sources reporting 12% (Frary et al., 2005), 13.6% (Tannous & Kalash, 2014) up to 54%
(Balaghi, Faramarzi, Mahdavi, & Ghaemmaghami, 2011; Mitchell et al., 2013). In a
study by National Association of College Stores (2012), 27% college students drank hot
tea, 25% drank flavored iced tea, and 14% drank unflavored tea in the previous seven
days. Females tend to consume more hot tea per week than males (22% female; 16%
male) (Cozart & Riddle, 2011).
Energy drinks. Energy drink consumption has been reported as 6.7% (Tannous &
Kalash, 2014), 9% (Mitchell et al., 2013), 13-14% (NACS, 2012; Traylor & Summers,
n.d) and 48% (Attila & Çakir, 2011). Fifty-one percent of participants in one study
reported never using energy drinks (Attila & Çakir, 2011). Caffeine Informer (2016)
compiled the most popular energy drinks based on sales. The most popular was Red bull,
then Monster, then Rockstar, then Amp and NOS, Full throttle, and lastly Xyience
Xenergy (Top Selling Energy, 2016). Another study found that the most popular type of

20
energy drink in the college population is also Red bull (51.7% preferred) (Attila & Çakir,
2011).
Most studies indicate that males consume more energy drinks in comparison to
females (Hidiroglu et al., 2015; Lohsoonthorn et al., 2012; Tannous & Kalash, 2014),
where in a seven day beverage recall, 24% of men reported using energy drinks and
women only 15% (Cozart & Riddle, 2011). Research suggests that males are 1.5 times
more likely to use energy drinks than women (Attila & Çakir, 2011). Females typically
consumed more sugar-free varieties of energy drinks (35%) in comparison to men (12%)
(Malinauskas, Aeby, Overton, Carpenter-Aeby, & Barber-Heidal, 2007). However, a
study by Malinauskas et al. (2007) found that females drank significantly more energy
drinks (53%) in comparison to males (42%).
Alcohol. Caffeine is often mixed with caffeinated products, such as energy drinks to
decrease the flavor of alcohol or not feel/appear drunk, and to become drunk (O’Brien,
McCoy, Rhodes, Wagoner & Wolfson, 2008; Marczinski, 2011). When partying, 54% of
college students mix alcohol and energy drinks (Malinauskas et al., 2007). One study
found that of the 68% of the college students drinking alcohol in the past 30 days, 24%
had drank alcohol mixed with an energy drink at least once (O’Brien et al., 2008). Males,
Caucasians, fraternity/sorority members, intramural athletes, and underage students were
most likely to consume alcohol mixed with energy drinks (O’Brien et al., 2008;
Marczinski, 2011). Those that consumed alcohol and energy drink mixtures reported
higher alcohol consumption during those drinking occasions (O’Brien et al., 2008). In a
study by Berger, Fendrich, and Fuhrmann (2013) found that three out of four students in

21
the study consumed alcohol mixed with energy drinks in their lifetime, and two of these
three consumed this in the past year. However, another study found a lower amount
(44%) reported amount of students consuming alcohol mixed with energy drinks in their
lifetime, and only 9% reported consuming this in the past two weeks (Marczinski, 2011).
Attila & Çakir (2011) found that 37.2% of students reported drinking energy drinks with
alcohol and that one third of the current energy drink users first tried energy drinks at a
bar.
Foods. Other products that contain caffeine include caffeinated gums, chocolate or
mocha-flavored products, or products containing coffee or chocolate. This may include
ice cream/frozen yogurt (Schardt, 2016), baked goods, puddings, and candy bars. A
seven-day recall revealed that 45% of college students consumed cookies/pastries, 38%
consumed ice cream/frozen treats, and 32% of students consumed candy bars (NACS,
2012). The caffeinated gum called Stay Alert Military Caffeine Energy Gum is often
used in the military to keep soldiers awake and more alert during long
operations/missions, in which one pack of gum contains five pieces, each containing
100mg of caffeine (Weinberg, 2013). Caffeine in the gum form allows for a much more
rapid absorption (five times faster) than caffeinated beverage or foods (Weinberg, 2013).
Regulations
There are different regulations between products containing caffeine being
labeled as conventional foods versus dietary supplements (Rosenfeld et al., 2014). The
difference lies in the “ingredient regulation, labeling, and good manufacturing processes”
22
(Rosenfeld et al., 2014). In soda, caffeine is considered generally recognized as safe
(GRAS) in levels less than 200 parts per million (2% of weight) or 71 mg of caffeine per
12 fluid ounces (Rosenfeld et al., 2014). Any retail food products must list their
ingredients by their “common name,” and these must be listed on their product’s
packaging when it is greater than or equal to 2% of the ingredients by weight; this
includes caffeine Rosenfeld et al., 2014). Caffeine is not required to be on food labels
because it is not a “nutrient” but when added to food, caffeine must be listed in the
ingredients on food label packaging (FDA, 2016; Roberts, 2006). Dietary supplements,
such as energy shots and energy drinks, are not required to list the amount of caffeine
(USDA, 2015). However, dietary supplements containing caffeine in “proprietary
blends,” the total amount of the blend is the only thing that must be listed (Rosenfeld et
al., 2014). The Center for Science in the Public Interest petitioned to the FDA in 1997 to
mandate the labeling of caffeine content per serving that is found in caffeine-containing
foods and drinks, however the petition is still rendered as “active” and undecided by the
FDA (Schardt, 2015).
The combination of alcohol and caffeine is not generally recognized as safe
because, when mixed together, the effects of intoxication are lowered (USDA, 2015). In
2010, the FDA issued “warning” statements to four companies, discussing that the added
caffeine in their alcoholic, caffeinated malt products were an “unsafe food additive”
(FDA, 2010). According to Attila & Çakir (2011), the mixing of energy drinks with
alcohol with strenuous physical activity can lead to sudden cardiac death.

23
Recommendations of Daily Caffeine Intake
Caffeine is not a nutrient and, therefore, not essential in the diet. The current
Dietary Guidelines for Americans (2015) state that non-caffeine consumers are “not
encouraged” to add caffeine into their regular, daily diet. The recommendation is to limit
caffeine to low to moderate intakes. Studies and reports vary in their “classifications” of
what is considered “low,” “moderate,” and “high” caffeine doses and intake. Overall, it
is stated that single doses of caffeine <200 mg (two cups of coffee or less) is considered
non-harmful in adults (European Food Safety Authority, 2015; Mayo Clinic). For
pregnant women, it is recommended that caffeine is limited to 200 mg/day (12 oz cup of
coffee) since caffeine crosses the placenta (March of Dimes, 2015). Breastfeeding
mothers are recommended to limit caffeine to no more than two to three cups/day since
small amount of caffeine enter into breast milk (March of Dimes, 2015).
Low intake has been described as <100 mg (Nehlig, Deval, & Debry, 1992),
<250mg/day (Winston et al., 2005), and 20-200 mg/day (Garrett & Griffiths, 1997). Low
doses of caffeine are thought to cause the benefits of caffeine (Daly & Fredholm, 1998).
Caffeine intake between 20 and 200 mg has been noted to increase “well-being,
happiness, energy, alertness, and sociability” (Schardt, 2015). Doses up to 2 µg/ml are
considered low and stimulate the central nervous system (UNEP Publications, 2003).
Moderate intake has been described as 250-750 mg/day (Winston et al., 2005),
100-200 mg/day (Drug Abuse Warning Network [Dawn], 2011), 200-300 mg/day (Mayo
Clinic) and 400 mg/day (USDA, 2015). Five cups of coffee a day (<400 mg) or five soda
or tea beverages that contain caffeine (110-345 mg/day) (Gonzalez de Mejia & Ramirez-

24
Mares, 2014). The general findings are that caffeine can have a positive effect on
individuals with the consumption of 200-300 mg/day (Garrett & Griffiths, 1997; Smith,
2002). In the military, soldiers are advised to consume 100-200 mg (considered a
moderate dose) of caffeine when tired to increase “alertness and performance” (Schardt,
2015). In some individuals, caffeine intake greater than 200 mg/day can cause negative
side effects, such as jitteriness, anxiety, nervousness, and upset gastrointestinal
discomfort (Schardt, 2015).
Women that are actively trying to conceive are recommended to limit caffeine use
to less than 300 mg/day (Gonzalez de Mejia & Ramirez-Mares, 2014) and breastfeeding
mothers are recommended an upper limit of caffeine intake of 200-300 mg (Preedy,
2012). Research has found that >300 mg caffeine/day may result in negatively effect the
reproduction of women and the development of the baby (Dlugosz & Bracken, 1992). It
has been proposed that 300 mg caffeine/day may lead to a decrease in birth weight
(UNEP Publications, 2003). Pregnant women consuming caffeine in moderate doses
(less than five to six mg caffeine/kg body weight) is not thought to result in any negative
implications on the neonate/fetus Christian and Brent (2001).
High intake has been described as 200-800 (Garrett & Griffiths, 1997), >300 mg
(Nehlig et al., 1992), >500 mg/day (Mayo Clinic), and >750 mg/day (Winston et al.,
2005). A study by Tieges et al. (2007) found that both “low doses” of caffeine (3 mg/kg
bodyweight) and “high doses” (6 mg/kg bodyweight) result in faster response times and
reduced errors during an electronic “task switching” activity compared to non-caffeinated
participants. Doses exceeding 999 mg caffeine may lead to serious side effects, such as
25
convulsions, tachycardia, nausea, vomiting, and even death (Gilman, Rall, Nies, &
Taylor, 1990; Institute of Medicine (U.S.) Committee on Military Nutrition Research,
2001; Winston et al., 2005). UNEP Publications (2003) reports that 10-30 µg/ml can lead
to adverse effects, such as restlessness, excitement, tremors, dizziness, headaches, and
insomnia, while doses of five gm/ml caffeine is thought to be fatal.
Current Average Caffeine Intake
Caffeine intake has increased over the years, where intake has been reported as
165 mg/day in 2013 compared to 120 mg/day in 1999 (Mitchell et al., 2013). Over 95%
of adults consume caffeine from various sources, 70-90% of which are from coffee and
tea (USDA, 2015). Somogyi (2010) reports that the United States’ caffeine consumption
has remained constant, with adults (22 years of age and older) consuming approximately
300 mg/day per person between 2003 and 2008, with 13 to 21 year olds consuming
approximately 100 mg/day. Nawrot et al. (2003) report the average, daily caffeine intake
in the United States is 3 mg/kg body weight; this would be 205 mg caffeine for a 150 lbs
individual. As cited by Somogyi (2010), the National Coffee Association survey found
the average of 3.3 cups of coffee/day per capita in 2009, compared to 3.0 cups/day in
2003. As cited by Somogyi (2010), EuroMonitor International reported that as of 2013,
the coffee consumption in America was 3.1 kg dry coffee per capita. Only 36% of
Americans report they do not consume caffeine (Saad, 2015). There have been
differential data on the average consumption of caffeine in the United States, with one
study reporting 103.4 mg/day for females and 110.5 mg/day in males 14-21 years old

26
(Somogyi, 2010). A study conducted by McIlvain, Noland & Bickel (2011), found that
65% of the students surveyed reported daily intake of caffeinated beverages and that the
average caffeine intake of the participants was 849.86 mg/day (12.08 mg/kg body weight)
while another study found that 18-24 year olds had a mean intake of 122mg/day (1.7
mg/kg body weight/day) (Mitchell et al., 2013). Another study had self-reported caffeine
of participants ranging from 261 mg to 760 mg per day (Tieges, Snel, Kok, Plat, &
Ridderinkhof, 2007). Lieberman et al. (2015) found that 92% of college students
consumed caffeine, with an average of 159 mg/day for all students surveyed and 173
mg/day for caffeine users. In a study assessing caffeine consumption in 1994-1996 and
1998, 87% of females and 91% of males 18-34 years old consumed caffeine based on
“two-day dietary intake data” where the mean intake of caffeine was 166 mg/day for
females and 199 mg/day for males; (Frary et al., 2005). This higher caffeine intake in
males compared to females has been noted in other studies as well (Lieberman et al.,
2015; Pettit & DeBarr, 2011). There is also a pattern of increased caffeine consumption
with age (Lieberman et al., 2015; Mitchell, Knight, Hockenberry, Teplansky, & Hartman,
2013; Zagat, 2015), with 28% of college students reporting an increase of caffeine from
the previous year (Traylor & Summers, n.d.). Students 21 to 24 years old had a higher
percentage of ingesting caffeine more than three times a day, while 17 to 20 year olds
consumed the least amount of caffeine (Tannous & Kalash, 2014). A study of college
students in Thailand found that females increased their use of stimulants as they aged, but
results did not show “a clear pattern” on whether men increased stimulant use with age
(Lohsoonthorn et al., 2012). The highest caffeine-consuming age group being 50-59
27
years old for both males and females with an intake of 295.6 mg and 225.3 mg caffeine
per day in 2005-2006 (Somogyi, 2010).
Reasons for Caffeine Use
There are many perceived effects of caffeine that lends its appeal to consumers.
These include behavioral and psychological enhancements and providing energy to allow
students to study longer, improve attention via feeling more awake, counteract fatigue,
and boost mood (Attila & Çakir, 2011; Gupta & Gupta, 1999;; Hidiroglu, Tanriover,
Unaldi, Sulun, & Karavus, 2013; Usman et al., 2015). Caffeine is also used in social
circumstances and because of taste preferences (Attila & Çakir, 2011; Tannous & Kalash,
2014).
Mental energy and performance. Caffeine is consumed for many reasons, often
revolving around its perceived effects of “improving cognitive performance, mood, and
counteracting fatigue” (Gupta & Gupta, 1999; Kristiansen, Levy-Milne, Barr, & Flint,
2005; Lieberman et al., 2015; Parliment, Ho, & Schieberle, 2000; Snel & Lorist, 2011;
Usman, Bhomba, Jawaid, & Zaki, 2015; Winston et al., 2005). Twenty-two percent of
students reported that the main reason for their caffeinated beverage consumption was to
sense increased alertness (Tannous & Kalash, 2014).
Caffeine is also used when having to make long drives (Attila & Çakir, 2011;
Malinauskas et al., 2007). Studies show that caffeine helps to increase alertness on long
car drives when the drivers had insufficient sleep (Schardt, 2015). Caffeine is also
utilized in the military to help “maintain alertness and performance” in those sleep
28
deprived (Schardt, 2015). Caffeine is also used as a means to increase performance in
sports and athletics (Attila & Çakir, 2011; Usman et al., 2015). As seen in Table 2, many
workout supplements contain caffeine. Caffeinated gum or freeze-dried coffee have been
used in the military, especially for soldiers who have very long hours of operation
(Weinberg, 2013). Gum is used due to the quicker absorption compared to caffeinated
beverages or food products. When looking specifically at the use of caffeine in
academics, one study found that 17.6% of students used caffeine to endure long,
academic work shifts (Tannous & Kalash, 2014) and another study showed that students
reported caffeine use for studying and for major projects (Malinauskas et al., 2007).
Looking specifically at energy and stimulant drinks, reasons for consumption are
most commonly due to perceived benefits, including improved mental or physical
performance (Attila & Çakir, 2011; Hidiroglu, Tanriover, Unaldi, Sulun, & Karavus,
2013; Usman et al., 2015). A study conducted by Malinauskas et al. (2007) found that
for both men and women of the study, the top two reasons for consuming energy drinks
was due to insufficient energy (68% male; 67% female) and to increase energy (69%
male; 62% female).
Mood. Tannous & Kalash, 2014 found that 13.3% of the caffeine consumers
indicated that they consumed caffeinated products because it enhanced their mood and
6.6% used caffeine to diminish anxiety (Tannous & Kalash, 2014). The use of energy
drinks is also related to the desire to feel more energetic (Attila & Çakir, 2011).
Prevention of caffeine withdrawal is another reason but has been proposed that this is

29
related to the desire to improve the user’s mood (Lieberman et al., 2015; Parliment, Ho,
& Schieberle, 2000).
Sensory appeal. There is also a sensory aspect that drives the use of caffeinated
foods and beverages. These included “curiosity of taste and effects” (Attila & Çakir,
2011; Hidiroglu, Tanriover, Unaldi, Sulun, & Karavus, 2013; Parliment, Ho, &
Schieberle, 2000), to replace lost body fluid/thirst (Kristiansen et al., 2005; Lieberman et
al., 2015 Usman et al., 2015), and flavor preference (Tannous & Kalash, 2014; Usman,
2015).
Partying/social contexts. Caffeine, especially as energy drinks, is commonly
consumed in social situations, such as when partying (Attila & Çakir, 2011; Lieberman et
al., 2015; Parliment, Ho, & Schieberle, 2000; Usman et al., 2015). Fifty-four percent of
the students that consumed energy drinks in one study reported it was with alcohol while
partying, and noted that 49% of these users claimed three or more energy drinks were
typically consumed during these situations (Malinauskas et al., 2007). Fourteen percent
of students reported that a bar was the first place they had ever consumed an energy
drink. Those that drink alcohol were also two and a half times more likely to consume
energy drinks than non-users (Attila & Çakir, 2011). Students report also using energy
drinks to help treat hangovers and as a social pastime (Malinauskas et al., 2007; Tannous
& Kalash, 2014).

30
Benefits of Caffeine Use
The benefits of caffeine consumption are more substantial in individuals that do
not consistently consume caffeine (Gropper, Smith, & Groff, 2009; Schardt, 2015).
Cognitive and behavioral effects. According to Kanarek and Lieberman (2011),
the cognitive effects of caffeine can be seen more consistently in sleep-deprived
individuals, but not than those that are well-rested. Possible behavioral benefits of
caffeine include “spontaneous motor activity, learning, and memory” (Borota et al.,
2014), and “mental and cognitive performance, vigilance, and endurance” (Gupta &
Gupta 1999). This includes producing clearer thoughts more quickly, decreasing fatigue,
improving “mental association,” “faster reaction and response times,” and enhanced
alertness (Garrett & Griffiths, 1997; Gupta & Gupta, 1999; Institute of Medicine (U.S.)
Committee on Military Nutrition Research, 2001; Parliment, Ho, & Schieberle, 2000;
Schardt, 2015; Tieges et al., 2007). Individual’s personalities may also contribute to the
effectiveness of caffeine on human performance. Those that have a lower level of
baseline arousal in the morning have shown to have a more significant increase in
performance after the administration of caffeine compared to those that have a higher
baseline arousal (Gupta & Gupta, 1999). As cited by Snel & Lorist (1998), It has been
suggested that caffeine’s benefit in task performance is limited to “simple and moderately
complex tasks” in which caffeine used for more complex tasks may worsen performance.
There are differential speculations on the benefits of caffeine use, where some

31
researchers theorize that the seemingly beneficial aspects of caffeine are due to the “relief
of caffeine deprivation” for habitual users (Gupta & Gupta, 1999; James, 1994).
Mood. Some research indicated an improvement of mood and feelings of well-
being in moderate doses of caffeine (Garrett & Griffiths, 1997; Schardt, 2015;
Lieberman, Tharion, Shukitt-Hale, Speckman, and Tulley (2002) found that mood was
improved in a dose-dependent manner. It has been proposed that this mood improvement
may be related to the “anticipated” effects of caffeine or the reversal of withdrawal rather
than the actual mechanism of action (Gupta & Gupta, 1999; James & Rogers, 2005;
Parliment, Ho, & Schieberle, 2000). Other studies have also found no effect of caffeine
on positive mood alterations at 100 and 200 mg dosages (Svensson, Persson, & Sjöberg,
1980; Swift & Tiplady, 1988). However, a study conducted Stern, Chait, and Johanson
(1989) found that individuals who ingested a high dose of caffeine reported positive
mood change. It is suggested that the lack of findings in the elevation of mood during
caffeine administration may be due to the “masking of negative moods” as a result of
caffeine withdrawal (Smith, 2002).
Exercise and athletic performance. Since it has been shown that caffeine
metabolism differs on an individual, genetic basis, caffeine has different effects per
athlete (Butler et al., 1992; Guest, Jamnik, Womack, & El-Sohemy, 2015; Whoriskey,
2015). Researchers have found that individuals undergoing training have increased free
fatty acids, metabolism, and adrenaline when consuming caffeine at rest in comparison to
those not training (LeBlanc, Jobin, Cote, Samson, & Labrie, 1985). The results of short-

32
term, intense exercise is sporadic in research, with some studies showing no benefit to
caffeine use (Perkins & Williams, 1975), while other showing moderate and some
significant benefits (Flinn, Gregory, McNaughton, Tristram, & Davies, 1990).
Neurotransmitters. Caffeine has an effect on some neurotransmitters, including
catecholamines, acetylcholine, serotonin, and amino acids (Gupta & Gupta, 1999). When
caffeine and acetylcholine (ACh) precursor choline are “administered together,” short-
term memory retention increased in rats by “increasing the “synthesis” of the ACh
neurotransmitter (Gupta & Gupta, 1999). Caffeine has a protectant role for neurons and
may prevent diseases such as Parkinson’s (Guerreiro et al., 2008; Uchida, Kadowaki-
Horita, & Kanda, 2014) and Alzheimer’s disease (Maia & de Mendonca, 2002). This is
thought to be caused through the antagonist effect on the adenosine A2A receptor,
resulting in an increase of cortical dopamine to increase motor performance and working
memory in those with Parkinson’s disease (Uchida, Kadowaki-Horita, & Kanda, 2014).
A study by Guerreiro et al., (2008) concluded that the metabolite paraxanthine provides
“neuro-protection from cell death of selective nigrostriatal dopaminergic neurons.”
Negative Effects of Caffeine
Due to the variability of metabolism, the effects of caffeine differ amongst
individuals ((Butler et al., 1992; Guest, Jamnik, Womack, & El-Sohemy, 2015;
Whoriskey, 2015). Overall, caffeine may affect the body in many ways, such as causing
bone loss (Mahan & Escott-Stump, 2008), delayed conception (Bolùmar, Olsen,
Rebagliato, Bisanti, & the European Study Group on Fertility and Subfecundity, 1997;

33
Nawrot et al., 2003; Stanton & Gray, 1995), mood changes (Gupta & Gupta 1999), and
sleep disruptions (James, 1991a).
Negative cognitive and behavioral side effects. In general, negative side effects
include gastrointestinal distress, aggressiveness, depression, anxiety, irritability,
tremulousness/jitteriness, and sleep loss/insomnia (Botella & Parra, 2003; Gupta & Gupta
1999; Journal of the American Medical Association [JAMA], 2001; Schardt. 2015).
Caffeine is often consumed by college students as a means to cope with stress, however,
studies have shown that caffeine increases the stress hormone cortisol and
adrenocorticotropic hormone (which regulates the release of cortisol) (Al'Absi et al.,
1998; Lovallo et al., 2006; Randall, 2011) Non-caffeine consumers are generally less
stressed compared to caffeine users (Richards & Smith, 2015). A study by Lovallo,
Farag, Vincent, Thomas, and Wilson (2006) found that ingesting caffeine periodically
during the day resulted in increased cortisol levels throughout the day. The study also
highlighted this cortisol increase may be cause by the stimulation of the CNS in males
and that in females, “may interact with their peripheral metabolic mechanism” (Lovallo
et al., 2006).
Caffeine withdrawal. Research suggests that caffeine may cause dependency
because of its natural component as a stimulant, therefore, leading to withdrawal
symptoms, (Schardt, 2015; Winston et al., 2005). According to Schardt (2015),
individuals who began consuming caffeine daily showed distinct “effects on the body” in
less than a week. Common symptoms of caffeine withdrawal include headaches, nausea,

34
vomiting, depression, irritability, inability to sleep, confusion, anxiety, tremors, and
fatigue. (Finnegan 2003; McIlvain, Noland, & Bickel, 2011; Nehlig, 2004). Other
symptoms listed included fatigue, drowsiness, unable to concentrate (Traylor &
Summers, n.d.), gastrointestinal disturbance, nervousness, aggression, hot flashes, heart
palpitations, and increased blood pressure (Tannous & Kalash, 2014). In a study
performed by Traylor & Summers (n.d.), 40% of college students surveyed had difficulty
concentrating with caffeine cessation, 31% of students considered themselves addicted to
caffeine, and 31% reported had experiences strong caffeine cravings. It has been
proposed that the relief of this caffeine withdrawal causes the perceived benefit of mood
improvement (Gupta & Gupta, 1999; James 1994).
Tolerance may occur in individuals that habitually and chronically consume caffeine
(Champlin, Pasch, & Perry, 2016) because the “depressant effects” can outweigh
caffeine’s “stimulating” component and decrease the brain’s “receptiveness” to caffeine
(Gupta & Gupta, 1999; Parliment, Ho, & Schieberle, 2000).
Caffeinism. “Caffienism” may occur when high doses of caffeine are consumed.
Caffeinism is when high doses, around 1000-1500mg, of caffeine are consumed, leading
to “a pharmacological state of acute or chronic toxicity” (Pilette, 1983) and causes a
“physical dependence” for caffeine (Smith 2002; Winston et al., 2005). Symptoms
include difficulty sleeping/insomnia, agitation, excitement, and “rambling thoughts and
speech” (Winston et al., 2005; McIlvain, Noland, & Bickel, 2011). Doses around 10-14
gm caffeine are thought to be fatal (Hodgman, 1998).
35
Cardiovascular. Caffeine also may cause cardiac arrhythmias (Katan &
Schouten, 2005), headaches (Hering-Hanit & Gadoth, 2003), and increase homocysteine
levels (Katan & Schouten, 2005). High doses of caffeine can result in more serious side
effects, including increased heart rate, convulsions, nausea, vomiting, and “increased
respiration” (Gilman, Rall, Nies, & Taylor, 1990; Institute of Medicine (U.S.) Committee
on Military Nutrition Research, 2001; Winston et al., 2005). A study conducted by
Passmore, Kondowe, and Johnston (1987) found that 360 mg of caffeine administered to
healthy, male adults resulted in an increased systolic and diastolic pressure, and a late
increase in heart rate (three to four hours after administration). The increase in systolic
pressure was dose-dependent, while the diastolic was not (Passmore, Kondowe, &
Johnston, 1987). Individuals with no tolerance to caffeine may experience temporary
spikes in blood pressure, while regular or chronic users do not experience these same
elevations in blood pressure or heart rate (Weinberg & Bealer, 2004). However, there is
contradicting evidence of caffeine’s correlation of heart attacks and hyperlipidemia
(Weinberg & Bealer, 2004) and of caffeine’s effect on heart rhythm or blood pressure in
those with a normal blood pressure (UNEP Publications, 2003). As cited by UNEP
Publications (2003), there is no link between cardiovascular disease and the consumption
of caffeine in moderate doses but findings have indicated that short-term administration
(250 mg caffeine) elevated systolic blood pressure.
Infertility. Approximately 72% of pregnant women consume caffeine on a
regular basis (James, 1991b). High caffeine intake consumed daily has shown to delay
conception in women (Bolùmar, Olsen, Rebagliato, Bisanti, & the European Study Group

36
on Fertility and Subfecundity, 1997; Nawrot et al., 2003; Stanton & Gray, 1995).
However, the effect of caffeine on reproduction in research has conflicting results in the
delayed of conception or infertility (UNEP Publications, 2003).
Osteoporosis. Caffeine is also thought to play a role in the development of
osteoporosis, especially in cola beverages (Mahan & Escott-Stump, 2008). Calcium’s
absorption by the kidney is decreased after caffeine intake, leading to “increased urinary
losses” (Gropper, Smith, & Groff, 2009). It is also thought that caffeine consumption
may increase the secretion of calcium in the gut, leading to further calcium loss (Gropper,
Smith, & Groff, 2009). Gonzalez de Mejia & Ramirez-Mares (2014) state that “adding
two tablespoons of milk to their coffee” may counterbalance the calcium losses from
caffeine in those that are at risk of developing osteoporosis.
Dehydration. There is differential information on whether or not caffeine leads
to dehydration. Generally, studies have found that the diuretic effect is dose dependent,
where low to moderate doses of caffeine do not cause acute diuresis, but high doses do
(Passmore, Kondowe, & Johnston, 1987). Neuhauser-Berthold, Beine, Verwied, &
Luhrmann PM (1997) found that six cups of coffee (642 mg caffeine) caused a negative
fluid balance by increasing the 24 hours urine excretion of the participants by 41%.
However, these results may not be completely accurate, as the researchers noted that the
bioelectrical impedance analysis overestimated the males’ total body water and
underestimated the females’ (Neuhauser-Berthold et al., 1997). A diuretic effect was
seen in individuals, who do not consume caffeine habitually, when they consumed high

37
doses of caffeine (250-300 mg) (Maughan & Griffin, 2003). It is thought that consuming
caffeine regularly would build up a tolerance to caffeine’s diuretic effect (Caffeine
Metabolism, n.d.; Maughan & Griffin, 2003). A meta-analysis found that 300 mg of
caffeine caused a minor diuretic effect, with females being more susceptible than males
(Zhang et al., 2015). Caffeine consumption is also related to greater sodium excretion
and decreased potassium (Passmore, Kondowe, & Johnston, 1987), where one study
found sodium excretion was higher in the group consuming coffee compared to the
water-drinking group (Killer, Blannin, & Jeukendrug, 2014). Multiple studies have found
no evidence to support the previous notions that caffeine has an acute diuretic affect in
healthy adults, however, caffeine consumption may affect chronic hydration (Armstrong
et al., 2005; Zhang et al., 2015). Caffeine may even contribute to hydration when
consumed in a beverage, such as coffee (Killer, Blannin, & Jeukendrug, 2014).
Prevalence of Caffeine Overdose
High doses of caffeine may lead to overdose and toxicity, symptoms being
restlessness, excitement, sleeping difficulties, frequent urination, and headaches
(McIlvain, Noland, & Bickel, 2011). Approximately 83% of college students reported
having one or more of these toxicity symptoms, with a mean of nearly three and a half
(McIlvain et al., 2011).
Emergency department (ED) hospitalizations have also increased. In 2005, there
were 1,128 ED visits related to energy drinks; this number increased, with 16,053 ED
visits in 2008 and 13,114 visits in 2009 (Dawn Report, 2011). Sixty-four percent of the

38
total patients were male, 45% of these visits were individuals aged 18 to 25 years and
32% aged 26 to 39 years (Dawn Report, 2011). Besides energy drink consumption by
itself, 52% of individuals aged 18 to 25 were hospitalized for the combination of energy
drinks with illicit drugs, alcohol, or pharmaceuticals. From the total data, 16% of the ED
visits were related to energy drinks combined with alcohol, with 20% of males and 10%
of females receiving the ED visits from this combination (Dawn Report, 2011). The
American Association of Poison Control Centers’ annual National Poison Data System
(NPDS) report states that in 2013, 1,112 cases involving energy drinks with caffeine
coming containing any sources (ie guarana, kola nut, tea, cocoa, etc.), in which 149 were
ages 12 to 19 years old and 181 is over twenty years of age (Mowry, Spyker, Cantilena,
McMillan, & Ford, 2014). An extreme case of excessive energy drink consumption
likely resulted in acute hepatitis in a 50-year-old man whom consumed four to five
energy drinks daily for three weeks (Harb, Taylor, Khullar, & Sattari, 2016). His
symptoms upon admittance to the hospital were jaundice, upper abdominal pain, nausea,
vomiting, malaise, dark urine, yellowing of the sclera (white portion of the eye), and
anorexia. While the hospital found he had “evidence of a chronic hepatitis C infection
and transaminitis, physicians believe the acute hepatitis was secondary to the high intake
of energy drinks (Harb et al., 2016). There were 1,392 “reported events” due to “adverse
effects” of dietary supplements containing caffeine between December 31, 2012 and
January 1, 2012 (Rosenfeld et al., 2014). There have been two fatalities from the use of
caffeine powder reported by the FDA (2015).

39
Definition of Sleep
Carskadon and Dement (2011) define sleep is a “reversible behavioral state of
perceptual disengagement from and unresponsiveness to the environment.” Oxford
University Press (2016) defines sleep as “a condition of body and mind which typically
recurs for several hours every night, in which the nervous system is inactive, the eyes
closed, the postural muscles relaxed, and consciousness practically suspended.”
Sleep Cycles
Sleep is a cycle of four stages of non-rapid eye movement sleep (NREM)
followed by rapid eye movement (REM) sleep (Carskadon & Dement, 2011; Dickelmann
& Born, 2010). NREM sleep is a “deeper state of sleep” with “delta waves” and “low
levels of autonomic physiological activity” (Colten & Altevogt, 2006). NREM is
measured using electroencephalographic (EEG) recordings, which display how each
stage of NREM affects the brain’s activity (Colten & Altevogt, 2006). Stage one is the
transition from wake to sleep and lasts around one to seven minutes. Stage two is a
“slightly deeper sleep” compared to stage one. Stage three is short in the first cycle of
sleep and “produces more slow-wave activity” and contains 20% to 50% of the brain’s
activity as shown on the EEG. Stage four is has a duration around 20 to 40 minutes, with
an activity of 50% or higher. Stages three and four is often referred as “deep sleep”,
“delta sleep”, or “slow wave sleep” where an individual needs more “intense stimuli” to
wake up in comparison to the previous two stages (Carkadon & Dement, 2011; Colten &
Altevogt, 2006).

40
REM (rapid eye movement) sleep is incorporated into NREM sleep periodically
during the normal cycle and shows up as “increased forebrain and midbrain neuronal
activity” (Colten & Altevogt, 2006). During REM, dreams occur and the body’s muscles
are paralyzed (Colten & Altevogt, 2006; Plaford, 2009). REM sleep is thought that long-
term memory storage of experiences and learning occurs (Plaford, 2009). Each cycle of
sleep varies, with the first NREM-REM sleep cycle being the shortest, lasting
approximately 70-100 minutes, while the following cycles are 90-120 minutes (Carkadon
& Dement, 2011). Humans spend approximately 75-80% of their sleep in NREM and
around 20-25% in REM (Colten & Altevogt, 2006).
Circadian Preference
The National Sleep Foundation (2015) defines circadian rhythm as “the
mechanism that helps govern your sleep and wake time and describes the timing and
duration of sleep.” The circadian clock is described as an internal biological clock
controlled by the brain that regulates the alertness throughout the day, timing of sleep,
wakefulness, as well as other processes (Horne, 1988). Chronotypes for the sleep-wake
cycle may be categorized as “morning,” “intermediate,” or “evening” and is generally
measured via body temperature, which increases during “wakefulness” and decreases
during sleep (Horne, 1988; Horne & Östberg, 1976). Social and behavioral
commitments, regulation of sleep, and one’s natural circadian pacemaker are factors that
contribute to circadian preference of each individual (Digdon, 2010; Gaultney, 2010). In

41
early adulthood, which includes college students, chronotype preference shift towards
most predominately to evening (Taylor, Clay, Bramoweth, Sethi, & Roane, 2011).
Between the three chronotypes, there is a significant difference in the time the
individual goes to sleep and the “peak” performance time (Horne & Östberg). On the
other hand, the overall duration of sleep was not significant among the three chronotypes,
approximately seven and a half for each (Horne & Östberg, 1976). Evening types go to
bed approximately 99 minutes later and wake up approximately 120 minutes later in
comparison to morning type chronotypes (Horne & Östberg, 1976). The peak time of
intermediate and morning have similar “peak times” but intermediate chronotypes go to
bed and arise “approximately median” between the morning and evening types (Horne &
Östberg, 1976).
Males tend to be more of an evening chronotype compared to females (Digdon,
2010; Lund, Reider, Whiting, & Prichard 2010; Schneider et al., 2014; Tran et al., 2014).
Evening types, in comparison to intermediate and morning chronotypes, have a greater
chance of developing issues with health, including sleep and psychiatric disturbances,
increased daytime sleepiness, and difficulty “adjusting to sleep practices” (Digdon, 2010;
Schneider et al., 2011; Taylor et al., 2011; Tran et al., 2014) and more likely to
characterize themselves as being “poor sleepers” (Digdon, 2010).
Function of Sleep
Sleep is important for psychological and physiological health (Colten & Altevogt,
2006; Lund, 2010 et al.; Plaford, 2009). Sleep is essential for basic functioning,

42
including alertness, “handling emotions,” and “cognitive performance” (Kilgore, 2010).
When an individual is not getting the necessary hours of sleep or has poor quality of
sleep, their quality of life is reduced; sleep is a “predictor of illness” for the future (Lund
et al., 2010; Buysse, Reynolds, Monk, Berman, & Kupfer, 1988). Sleep strengthens the
immune system’s response, thereby increasing the body’s ability to fight infections
(Plaford, 2009).
Memory consolidation is when learned information can become “integrated and
stored” for long-term memory (Curcio, Ferrara, & De Gennaro, 2006; Dickelmann &
Born, 2010). Sleep, mostly during REM sleep, is when this memory consolidation occurs
and allows for the storage of learned material and experiences to be stored (Dickelmann
& Born, 2010). Therefore, insufficient sleep or poor quality of sleep restricts the ability
to consolidate and process memory (Dickelmann & Born, 2010; Plaford, 2009; Walker,
2008), ultimately leading to potential negative impacts on a students’ academic
performance (Champlin, Pasch, & Perry, 2016; Gaultney, 2010).
Current Average Hours and Recommendation of Sleep for College Students
The amount Americans reporting insufficient sleep, less than six hours per night,
has increased by 13% from 2001 to 2001 (National Sleep Foundation: Sleep in America
Poll, 2009; National Sleep Foundation: Sleep in America Poll, 2009). This lack of sleep
affects the performance of individuals, making them less likely to “work well and
efficiently” (National Sleep Foundation: Sleep in America Poll, 2009). The amount of
sleep needed may vary between individuals, so there is not a set, “optimal” number of

43
hours of sleep, however, eight hours of sleep per night has shown to have substantial
benefits in regards to memory (Dickelmann & Born, 2010). Appointed sleep experts of
the National Sleep Foundation (NSF) created sleep recommendations for each age
bracket. These experts recommended that young adults, ages 18 to 25, have seven to nine
hours of sleep per night, where 10 to 11 hours per night may be recommended for certain
individuals, but sleep should not be less than six hours nor greater than 11 hours per night
Hirshkowitz et al., 2015). According to Lund et al. (2010), college students get
approximately 7 hours of sleep per night with 25% of students reporting less than six and
a half hours per night and almost 30% getting eight or more hours per night. Sleep
schedules were irregular, with 20% of students reporting that in the past month they
stayed up all night and 35% reported staying up until three in the morning at least once a
week (Lund et al., 2010). Sleep schedules varied by grade level in college students.
Freshman and sophomores tended to go to bed and wake up later and juniors and seniors
went to bed and woke up earlier (Lund et al., 2010).
Consequences of Sleep Deprivation
The college population often experiences “sleep deprivation” and “daytime
sleepiness,” (Bulboltz, Brown, & Soper, 2001; Gaultney, 2010) with approximately 28%
of students reporting daytime sleepiness (Tran et al., 2014). Sleep deprivation can occur
due to either acute situations or cumulative sleep loss (Plaford, 2009). Cumulative sleep
loss can occur when an individual is sleeping six to seven hours of sleep or less a night
over long periods of time (Plaford, 2009). Females, in comparison to men, are more

44
susceptible to sleeping difficulties, including a longer amount of time to fall asleep, have
higher incidences of disrupted sleep, and report lower quality of sleep (Tsai & Li, 2004;
Bulboltz, Brown, & Soper, 2001).
Receiving less than seven hours of sleep per night is one characteristic of “sleep loss”
and/or “poor sleep quality” and may lead to the common symptoms of excessive daytime
sleepiness, depressed mood, poor memory and poor concentration (Colten & Altevogt,
2006). Memory consolidation occurs during sleep, therefore, the storage of experiences,
including learning, is impaired (Plaford, 2009). Cardiovascular, endocrine, immune, and
nervous system are affected by sleep loss (Colten & Altevogt, 2006; Horne, 1988; Lund
et al., 2010). Negative emotions and increased stress are reported in individuals that have
poor sleep quality. These “negative emotions” include anger, confusion, depression,
tiredness, and tension (Colten & Altevogt, 2006; Lund et al., 2010; Plaford, 2009).
Sleep deprivation also plays a role in obesity (Colten & Altevogt, 2006; Plaford,
2009). Body temperature decreases with acute sleep deprivation because body
temperature regulation is disrupted (Plaford, 2009). To counteract this, the body’s
metabolism increases, resulting in increased desire to eat (Plaford, 2009). Also,
insufficient sleep affects metabolism and suppresses the body’s ability to regulate blood
sugar and, therefore, increases the risk of diabetes (Colten & Altevogt, 2006; Plaford,
2009). The immune system is also affected by sleep deprivation (Colten & Altevogt,
2006; Plaford, 2009). There is a relationship between the reports of “low sleep quality”
and “incidences of physical illness” in college students (Lund et al., 2010). The
relationship between disrupted circadian clock and immune system leads to the increase

45
in immune system susceptibility when sleep is disturbed (Plaford, 2009). Chronic
inadequate sleep may pose serious, long-term problems. These include in increased risk
of sleep disorders, hypertension, heart attack, stroke, and depression (Colten & Altevogt,
2006). Individuals with sleep disorders may have similar consequences of sleep loss,
which may also include “excessive daytime sleepiness” and difficulty falling and/or
staying asleep (Colten & Altevogt, 2006).
Factors Affecting Sleep
Sleep is affected by numerous variables including stress Delannoy, Mandai,
Honoré, Kobayashi, & Sequeira, 2015), caffeine use (Schardt, 2015), alcohol (Harvard
Medical, 2007; National Sleep Foundation, n.d.), smoking (Lohsoonthorn et al., 2012;
Wetter & Young, 1994) and other environmental factors.
Stress. Stress and sleep are connected in that lack of sleep can cause stress and
stress can cause lack of sleep. According to Wagner, Lorion, and Shipley (1983), school
pressures, psychological struggles and identity resolution are main stressors in college
students. According to the American Psychological Association (n.d.), 21% of adults
report that their stress increases when the length and quality of sleep decreases. Younger
generations also are reporting poorer sleep habits compared to older generations; 31% of
18 to 34 year olds compared to 23% of 35 to 40 year olds, 22% of 49-67 year olds, and
14% of 68 years and older (American Psychological Association, n.d.). College students
who worry were significantly more likely to report decreased sleep. Wagner et al. (1983)
found that stressors that reduce sleep in college students arise from school pressures, the

46
presence of psychological conflicts, and identity resolution. Having negative emotions
during the day has also found to impact the REM stage of sleep and increase activity of
the sympathetic nervous system compared to individuals with more positive pre-sleep
emotions (Delannoy, Mandai, Honoré, Kobayashi, & Sequeira, 2015).
Caffeine use. Due to caffeine’s effect on the central nervous system and blocking of
adenosine, it is often used to provide energy and decrease fatigue (Schardt, 2015). This is
beneficial for the users that use caffeine in order to restore energy or “improve
performance and alertness” when sleep deprived (Parliment, Ho, & Schieberle, 2000;
Schardt, 2015). However, there is a substantial effect of caffeine on sleep. Preedy
(2012) states that caffeine “likely has implications for day-to-day performance, behavior,
and health” in relation to its affect on sleep. A study by Whittier et al. (2013) found that
students who consumed “stimulant beverages” were more 1.37 times more likely to
report “excessive daytime sleepiness.” Another study found that students consuming one
caffeinated beverage per week were 1.60 times more likely than non-caffeine consumers
to report poor quality of sleep (Lohsoonthorn et al., 2012). Students using stimulant
drinks had high instances of “daytime dysfunction from sleep” and an increase in the
amount of time to fall asleep (Lohsoonthorn et al., 2012). There is a correlation between
amount of stimulant beverages and quality of sleep, where the greater amount of
stimulant beverages were consumed, the higher incidences of poor sleep quality
(Lohsoonthorn et al., 2012). The American Sleep Foundation’s Sleep Study Poll (2009)
found that over half of Americans report they are “at least somewhat likely” to use
caffeinated beverages during the day to combat sleepiness. The amount of Americans

47
using caffeine for this purpose has increased by 16% from 2001 to 2009 (National Sleep
Foundation: Sleep in America, 2001).
Even low concentrations of caffeine can affect the sleep-wake cycle, thereby affecting
both the REM and NREM stages of sleep (James, 1991a). Nicholson and Stone (1980)
found that hours after the ingestion of 300 mg of caffeine, the “early stages” of NREM
and REM sleep were reduced. In the majority of people, sleep can be disturbed if
caffeine is consumed three to five hours before bed; they may wake up periodically
throughout the night, causing low sleep quality and, therefore, fatigue the next day
(Schardt, 2015). Effects of caffeine are dose-dependent, where large doses consumed in
the late evening have shown to extend the time it takes to fall asleep at bedtime and
decreases the amount of time asleep (Carrier et al., 2009; Karacan et al., 1976; Smith,
2002). To counteract the fatigue from caffeine-induced sleep disturbance, individuals
may consume caffeine the next day, thereby creating a vicious cycle (Schardt, 2015).
Overtime, this change to the sleep cycle due to long-term caffeine consumption may
potentially cause insomnia, leading to chronic sleep deprivation (Winston, Hardwick, &
Jaberi, 2005; Champlin, Pasch, & Perry, 2016).
Alcohol. Alcohol is consumed for a number of reasons, such as conformity, coping,
reinforcement (either positive or negative), or social influences (Kenney, Paves,
Grimaldi, & LaBrie, 2014). The National Sleep Foundation (n.d.) reported that 20% of
Americans use alcohol to help them fall asleep at night, although alcohol consumed
before bed results in a decrease in quality of sleep (Roehrs & Roth, 2001). Researcher’s

48
believe that perhaps the decrease in the quality, not as necessarily amount, of sleep led to
more daytime sleepiness, which in turn, hindered the academic performance of students
(Howell, Jahrig, & Powell, 2004; Singleton & Wolfson, 2008). Alcohol decreases REM
sleep, disturbs an individual’s circadian rhythm, and decreases restorative sleep via the
activation of both delta and alpha activity (Harvard Medical, 2007; National Sleep
Foundation, n.d.). 53.8% of college students that drank alcohol in the previous month
reported poor sleep quality (average of 8 drinks per week for males and 5 for females)
(Kenney, Paves, Grimaldi, & LaBrie, 2014). Students that consumed a “moderate”
amount of alcohol (one to 19 drinks per month) had a 39% greater chance of having
daytime dysfunction incidences due to sleepiness but were less likely to report short sleep
duration (Lohsoonthorn et al., 2012). Students that consumed more than 19 alcoholic
beverages per month were three times more likely to report daytime dysfunction due to
sleepiness (Lohsoonthorn et al., 2012).
Smoking. Students that smoke cigarettes tend to take longer to fall asleep, have
more difficulty completing everyday tasks due to sleepiness, and report overall poor sleep
quality compared to those who have never smoked (Lohsoonthorn et al., 2012; Wetter &
Young, 1994). While the sleep latency was greater in smokers than non-smokers,
smokers were less likely to report short sleep duration (Lohsoonthorn et al., 2012). Since
nicotine is a stimulant, it can make falling asleep more difficult for users, especially when
using nicotine before bed (Diaz, 2016; Philips & Danner, 1995; Wetter & Young, 1994).
Due to the addictive component of nicotine, sleep cycles may be disrupted if the
individual experiences withdrawal, which may cause them to wake up throughout the

49
night (Diaz, 2016; Philips & Danner, 1995; Wetter & Young, 1994). Disordered
breathing is also more prevalent in smokers and can decrease the quality of sleep.
Another possible reason is any possible psychological troubles” (Wetter & Young, 1994).
Cigarette smokers were also more likely to report daytime sleepiness compared to non-
smokers (Philips & Danner, 1995)
Environmental. An individual’s direct environment can also have a negative
impact on sleep. Factors that can prevent or disrupt sleep include “excess noise,”
sleeping with others, and social obligations (Lund et al., 2010; Muzet, 2007). Light is
also an external factor that influences sleep. Exposure to light late in the night can
leading to changes in circadian patterns and can decrease the quality of sleep (Harvard
Medical, 2007). The temperature of the room may also impact sleep, in which the “ideal
sleep temperature” varies among individuals (Harvard Medical, 2007).
Definition of Academic Performance
The terms “academic performance” and “academic achievement” can be used
interchangeably. Steinmayr, Meißner, Weidinger, and Wirthwein (2014) state that
academic achievement signifies the results of performance, which show the “extent” of
an individual’s success towards particular goals to which were the “focus of activities in
instructional environments,” specifically in school, college, and university. Academic
success can be defined as “a gathering of “personal characteristics” including “mental
ability, academic skills, motivation, and goals,” and environmental characteristics
(Muuss, 1996). Walberg’s theory of academic achievement is that the “learning

50
outcome” is dependent on a student’s mental personalities and their “cognitive,
behavioral, and attitudinal influences” from their environment (Reynolds & Walberg,
1992).
Use of Grade Point Average in Assessing Academic Achievement
Cumulative grade point average (CGPA) is characterized by the grades “A, B, C,
D, and F’s,” each corresponding to a given, “numerical measurement” and scaled from
0.00 to 4.00 (Best College Values, n.d.). Grade point average (GPA) is considered
traditional and often used when measuring academic in order to assess the student’s
ability to “enter” higher education (Karthigeyan & Nirmala, 2012; Steinmayr et al., 2014;
York, Gibson, & Rankin, 2015). Feldman & Kubota (2014) state that GPA is an
important indicator of success in college and that it may affect a student’s financial aid in
the short term and helps to predict career success long-term. According to Masrom and
Usat (2015), GPA provides a “greater insight” into the academic performance of students
both individually and in “groups.” GPA and grades are thought to be useful by easily
assessed for institutions, grades are based off of specific course levels, and also easy to
“evaluate programs” within a given “institution” (York, Gibson, & Rankin, 2015).
Minimum GPA’s have been set by many institutions to maintain “good academic
standing,” where below GPA or grades below that minimum may lead to academic
consequences (Olin College, n.d.).
There is a difference in academic performance among genders. In both high
school and college, females consistently have a higher mean GPA than males (Astin,
51
1971; Astin & McCornack & McLeod, 1988). This difference in GPA can be due to
different reasons. These include type/difficulty of major (Gallini, 1982; Turner &
Bowen, 1999) and skills, in which females also tend to have certain skills, including
“organization, self-discipline, attentiveness, dependability, and seeking help from others”
(Riegle-Crumb, 2007; Jacob 2002). Jacobs (1999) states that females tend to enroll in
colleges that have higher acceptance rates and looser admission rates. However, a study
by Ari, Atalay, & Aljamhan (2010) found that the GPA for both males and females had
improved exit GPA (compared to entrance GPA), suggesting that there is no gender
difference in the improvement of academic performance during college.
Caffeine and Academic Performance
There has been an increase in research of the relationship between energy drink
consumption and academic performance in the past decade (Champlin, Pasch, & Perry,
2016; Hidiroglu, 2013; Pattison, Rusin & Bai, 2016; Pettit & DeBarr, 2011). Sixty-three
percent of students reported their consumption of caffeine increases during time of
academic stress (Oaten and Cheng, 2005; Tannous & Kalash, 2014). College students
that have a high intake of energy drinks also had higher reports of “perceived stress” than
their peers with lower “perceived stress” (Pettit & DeBarr, 2011). In a study conducted
by Hidiroglu et al. (2013), students reported their expectations of energy drinks to
enhance their mental performance were met. This expectations clashed with findings
from other studies, which found that the “frequency” of energy drink consumed was
52
“inversely related” to the grade point average of first year undergraduate college students
(Champlin, Pasch, & Perry, 2016; Pattison, Rusin & Bai, 2016; Pettit & Barr, 2011).
Sleep and Academic Performance
As cited by Pettit & Debarr, (2011), the American College Health Association
states that the most common threats to academic performance are sleep, stress, anxiety,
and depression. Academic and emotional stress, tension and worry are also listed as the
most common reasons for decreased quality or duration of sleep in college students
(Buysse et al., 1988; Ginsberg, 2006; Lund et al., 2010; Plaford, 2009; Tsai & Li, 2004).
Poor quality and quantity of sleep in college students negatively impacts performance and
grade point average (Abraham & Scaria, 2015; Becker, Adams, Orr, & Quilter, 2008;
Gaultney, 2010). Researchers found a positive correlation between sleep times and
amount of alcohol consumed, grades were weakly (negatively) associated with sleep
duration, suggesting that when the quality, not as much quantity, of sleep is negatively
correlated with academic performance via increased daytime sleepiness (Singleton &
Wolfson, 2008). Howell et al. (2004) found that while sleep quality is not correlated with
GPA, those with lower sleep quality in addition to a full workload performed worse on
performance measures This is shown through the reported reduction in quality of sleep
one month before an exam, where 29% of college students reported “poor sleep” during
this time (Zunhammer, Eichhammer, & Busch, 2014). Cognitive and behavioral
performance in the “academic setting” is negatively affected by the reduction of duration

53
and quality of sleep by potentially increasing daytime sleepiness (Curcio, Ferrara, & De
Gennaro, 2006; Dewald, Meiher, Oort, Kerkhof, & Bogels, 2010).
The body’s immune system requires sleep in order to function properly. Students
with inadequate sleep have a greater occurrence of missed class related to physical illness
(Lund et al., 2010; Plaford, 2009) and had poorer performance due to “episodes of falling
asleep” during class (Lund et al., 2010). Students with the evening chronotype have been
reported to have a significantly lower GPA compared to the intermediate and morning
types Taylor et al., 2011). This is a problem considering that the total duration of sleep is
often reduced in college students due to late school bedtimes (Abraham & Scaria, 2015).

54
CHAPTER III
METHODOLOGY
Research Design
The study design was a comparative study with five levels of type of caffeine
consumer (non-caffeine consumer, low caffeine consumer, moderate caffeine consumer,
high caffeine consumer and very high caffeine consumer). When assessing the first
hypothesis, the caffeine users and non-caffeine users are the dependent variable and the
hours of sleep is the independent variable. When assessing the second hypothesis, the
different levels of caffeine consumed is the dependent variables and hours of sleep is the
independent variable. When assessing the third hypothesis, GPA is the dependent
variable and caffeine users and non-caffeine users are the independent variables. When
assessing the fourth hypothesis, GPA is the dependent variable and the dependent
variables are the levels of caffeine consumed. When assessing the fifth hypothesis, sex is
the independent variable and the amount of caffeine (mg) consumed is the dependent
variable. When assessing the sixth hypothesis, grade level is the independent variable
and the amount of caffeine (mg) consumed is the dependent variable. For demographic
analyses- grade level, sex, and ethnicity were the independent variable while caffeine
consumption was the dependent variable.

55
Research Sample
The email list was provided by the Registrars office and consisted of students who
were undergraduates and current Kent State University students as of the spring 2017
semester. This included both male and female of any age and could be either full-time or
part-time at a Kent State. During the survey, students were excluded if they were
graduate students, students under 18 years of age, or individuals diagnosed with a sleep
disorder.
Procedures
The Kent State University Institutional Review Board (IRB) approved the thesis
topic, and then the Registrar’s Office gave permission and an email list of 31, 585 current
Kent State University undergraduate part-time and full time students. The survey was
then sent out to students via email through Qualtrics. Upon opening the survey,
participants were asked a series of questions regarding their status as a student and
sleeping behaviors that may identify them as having a sleep disorder to ensure inclusion
criteria. Participants having any exclusion criteria or did not agree to the informed
consent was thanked and then dismissed from continuing the survey. The survey was
accessible from February 9, 2017 to February 23, 2017. One email reminder was sent out
to participants February 16th. To determine caffeine intake, the amounts of caffeine
consumed, per Excel spreadsheet uploaded by the participant to Qualtrics, was summed
and entered into SPSS software for analysis. To determine hours of sleep, reported fall
asleep-wake times were subtracted from one another for both weekend and weekday,

56
averaged, and entered into SPSS software for analysis.
Research Measures
An online Caffeine Consumption, Sleep, and Academic Performance
Questionnaire with four sections were used. The questionnaire was developed by Pfaff
(2013) and was an updated survey based on the Caffeine Consumption Questionnaire
(CCQ) originally created by R. E. Landrum (1992). Updates were made to the caffeine
consumption section to incorporate newer sources of caffeine and be shortened to allow
students to type in their caffeine beverage if not listed from the shortened list, and can be
seen in Appendix B. The survey was available to students through Qualtrics survey
creation website online. To begin the survey, students had to agree to the consent form,
which can be seen in Appendix C.
Part I had seven questions and consisted of demographic information and
questions regarding academic status, number of credit hours per semester, and asked
about any history of a sleeping disorder. Part II had three questions and consisted of a
caffeine consumption questionnaire, to determine amount of caffeine consumed and how
long the participant has been using caffeine. Participants had to download the Excel
attachment with a list of various sources of caffeine. From this list, the student must
specify- on one typical day- the type of caffeine source consumed, amount of servings of
that particular source, and the time it was consumed and then re-upload the Excel
document to Qualtrics. This would then allow the sum of the amount of caffeine
consumed per day to be calculated. An example was provided on the survey to

57
demonstrate how to fill out the Excel document using a Brand (other) source for if the
source of caffeine they consumed was not on the caffeine source list. Part III had five
questions and consisted of a sleep questionnaire to determine the sleep/wake times of
students. Part IV had three questions and consisted of an academic questionnaire for
participants to record cumulative GPA, which they will type in themselves, the amount of
credit hours they are taking, and if they believe their caffeine intake increases during
times of academic stress.
Statistical Analysis
Data was analyzed using SPSS version 24 statistical software using significance
as p<0.05. Data includes demographic information, amount of caffeine consumed, hours
of sleep, and cumulative GPA. P-value of p< 0.05 was selected a priori. An univariate
ANOVA was used to determine differences between the five levels of caffeine
consumption for cumulative GPA and reported hours of sleep. These five levels
consisted of non-consumer (<5 mg caffeine), low (5-200 mg caffeine), moderate (201-
500 mg caffeine), high (501-750 mg caffeine), and very high (>750 mg caffeine). A t-
test was used to assess the difference between the two levels of caffeine consumer
(caffeine consumer and non-consumer) between reported hours of sleep and differences
between caffeine consumers and non-consumers for cumulative GPA. Post hoc analysis
was performed for calculations with significant differences.
58
CHAPTER IV
JOURNAL ARTICLE
Introduction
Caffeine is not a nutrient and, therefore, its consumption is not required in a
healthy diet. However, caffeine consumption is high in the college populations for its
perceived benefits in increasing energy and alertness, counteracting fatigue, improving
behavioral and cognitive performance, and mood enhancement (Gupta & Gupta, 1999;
Kristiansen, Levy-Milne, Barr, & Flint, 2005; Lieberman et al., 2015; Malinauskas et al.,
2007; Parliment, Ho, & Schieberle, 2000; Snel & Lorist, 2011; Usman Bhomba, Jawaid,
& Zaki, 2015; Winston et al., 2005). Approximately 92% of students consume caffeine
and 65% using caffeine daily (Lieberman et al., 2015; McIlvain, Noland & Bickel, 2011).
Coffee is the most popular source of caffeine, with soda, tea, and chocolate, energy
drinks, and certain medicines also being used regularly. While moderate caffeine intake
(<400 mg/day) is generally recognized as safe for the general population (United States
Department of Agriculture [USDA], 2015), the average amount of daily caffeine (mg)
consumed varying from 159 mg/day to 849.86 mg/day (Lieberman et al., 2015; McIlvain,
Noland & Bickel, 2011). Higher doses of caffeine can cause various, negative side
effects including restlessness, excitement, tremors, dizziness, headaches, and insomnia
(UNEP, 2013) and very high doses may cause nausea, vomiting, convulsions,

59
tachycardia, and even death (Gilman, Rall, T.W., Nies, A.S., & Taylor, 1990; Institute of
Medicine (U.S.) Committee on Military Nutrition Research, 2001; Winston et al., 2005).
Sleep is a physical and mental necessity for basic human functioning. It is
recommended that the typical college student receive no less than seven and no more than
nine hours of sleep per night (Hirshkowitz et al., 2015). While the average reported sleep
duration is seven hours per night, 25% of students report receiving less than six and a half
hours, with only 29.4% report sleeping at least eight hours (Lund et al., 2010).
Inadequate sleep, less than six hours per night, can lead to acute or chronic sleep
deprivation. To make up for this lack of sleep, individuals may rely on caffeine the next
day to counteract the daytime sleepiness. However, even in small doses caffeine (100
mg) affects both the rapid eye movement (REM) and non-rapid eye movement (NREM)
sleep cycle (James, 2001; Smith, Smith, Miners, McNeil, & Proudfoot, 2000). This sleep
disruption results in decreased quality and duration of sleep, causing daytime sleepiness
the next day (Carrier et al., 2009; James, 1991a; Karacan et al., 1976; Nicholson & Stone,
1980; Smith, 2002). Therefore, the cycle of sleep loss, daytime fatigue, and caffeine
continues, leading to a cycle of caffeine use and sleep deprivation (Winston, Hardwick, &
Jaberi, 2005; Champlin, Pasch, & Perry, 2016; Schardt, 2015).
The role of sleep has been shown to be very important to perform academically,
but the upcoming stress of exams often leads to decreased sleep quality (Abraham &
Scaria, 2015; Gaultney, 2010; Zunhammer, Eichhammer, & Busch, 2014). Poor quality
and quantity of sleep in college students have a negative impact on the performance and
grade point average of students (Abraham & Scaria, 2015; Becker et al., 2008; Gaultney,

60
2010). While caffeine may be used to keep a student energized to perform academic
duties, its effects have been shown to be less than optimal in certain studies where the
increase of energy drinks results in lower grade point averages (GPA’s) (Champlin,
Pasch, & Perry, 2016; Pattison, Rusin, & Bai, 2016; Pettit & Debarr, 2011). There is a
lack of research assessing the relationship between all the variables- caffeine, sleep, and
academic performance. With the high numbers of students reporting insufficient sleep
and the excessive amounts (mg) of caffeine consumed, the effect of these variables on the
academic performance of students needs to be assessed.
The purpose of this study is to assess the difference in hours of sleep and
academic performance between caffeine users and non-caffeine users in undergraduate
full and part-time students. It was hypothesized that there will be a difference in GPA
and hours of sleep exists between type of caffeine consumer (non-caffeine and caffeine
consumer) and between the five levels of caffeine consumption (non-consumer, low,
medium, high, and very high). Also, there will be a difference in amount of caffeine
(mg) consumed between both sex and grade level (freshman, sophomore, junior, and
senior).
Methodology
Research Design
The study design was a comparative study with five levels of type of caffeine
consumer (non-caffeine consumer, low caffeine consumer, moderate caffeine consumer,
high caffeine consumer and very high caffeine consumer). When assessing the first

61
hypothesis, the caffeine users and non-caffeine users are the dependent variable and the
hours of sleep is the independent variable. When assessing the second hypothesis, the
different levels of caffeine consumed is the dependent variables and hours of sleep is the
independent variable. When assessing the third hypothesis, GPA is the dependent
variable and caffeine users and non-caffeine users are the independent variables. When
assessing the fourth hypothesis, GPA is the dependent variable and the dependent
variables are the levels of caffeine consumed. When assessing the fifth hypothesis, sex is
the independent variable and the amount of caffeine (mg) consumed is the dependent
variable. When assessing the sixth hypothesis, grade level is the independent variable
and the amount of caffeine (mg) consumed is the dependent variable. For demographic
analyses- grade level, sex, and ethnicity were the independent variable while caffeine
consumption was the dependent variable.
Research Sample
The email list was provided by the Registrars office and consisted of students who
were undergraduates and current Kent State University students as of the spring 2017
semester. This included both male and female of any age and could be either full-time or
part-time at a Kent State. During the survey, students were excluded if they were
graduate students, students under 18 years of age, or individuals diagnosed with a sleep
disorder

62
Procedures
The Kent State University Institutional Review Board (IRB) approved the thesis
topic, and then the Registrar’s Office gave permission and an email list of 31, 585 current
Kent State University undergraduate part-time and full time students. The survey was
then sent out to students via email through Qualtrics. Upon opening the survey,
participants were asked a series of questions regarding their status as a student and
sleeping behaviors that may identify them as having a sleep disorder to ensure inclusion
criteria. Participants having any exclusion criteria or did not agree to the informed
consent was thanked and then dismissed from continuing the survey. The survey was
accessible from February 9, 2017 to February 23, 2017. One email reminder was sent out
to participants February 16th. To determine caffeine intake, the amounts of caffeine
consumed, per Excel spreadsheet uploaded by the participant to Qualtrics, was summed
and entered into SPSS software for analysis. To determine hours of sleep, reported fall
asleep-wake times were subtracted from one another for both weekend and weekday,
averaged, and entered into SPSS software for analysis.
Research Measures
An online Caffeine Consumption, Sleep, and Academic Performance
Questionnaire with four sections were used. The questionnaire was developed by Pfaff
(2013) and was an updated survey based on the Caffeine Consumption Questionnaire
(CCQ) originally created by R. E. Landrum (1992). Updates were made to the caffeine
consumption section to incorporate newer sources of caffeine and be shortened to allow

63
students to type in their caffeine beverage if not listed from the shortened list. The
survey was available to students through Qualtrics survey creation website online.
Part I had seven questions and consisted of demographic information and
questions regarding academic status, number of credit hours per semester, and asked
about any history of a sleeping disorder. Part II had three questions and consisted of a
caffeine consumption questionnaire, to determine amount of caffeine consumed and how
long the participant has been using caffeine. Participants had to download the Excel
attachment with a list of various sources of caffeine. From this list, the student must
specify- on one typical day- the type of caffeine source consumed, amount of servings of
that particular source, and the time it was consumed and then re-upload the Excel
document to Qualtrics. This would then allow the sum of the amount of caffeine
consumed per day to be calculated. An example was provided on the survey to
demonstrate how to fill out the Excel document using a Brand (other) source for if the
source of caffeine they consumed was not on the caffeine source list. Part III had five
questions and consisted of a sleep questionnaire to determine the sleep/wake times of
students. Part IV had three questions and consisted of an academic questionnaire for
participants to record cumulative GPA, which they will type in themselves, the amount of
credit hours they are taking, and if they believe their caffeine intake increases during
times of academic stress.
Statistical Analysis
Data was analyzed using SPSS version 24 statistical software using significance
64
as p<0.05. Data includes demographic information, amount of caffeine consumed, hours
of sleep, and cumulative GPA. P-value of p< 0.05 was selected a priori. An univariate
ANOVA was used to determine differences between the five levels of caffeine
consumption for cumulative GPA and reported hours of sleep. These five levels
consisted of non-consumer (<5 mg caffeine), low (5-200 mg caffeine), moderate (201-
500 mg caffeine), high (501-750 mg caffeine), and very high (>750 mg caffeine). A t-
test was used to assess the difference between the two levels of caffeine consumer
(caffeine consumer and non-consumer) between reported hours of sleep and differences
between caffeine consumers and non-consumers for cumulative GPA. Post hoc analysis
was performed for calculations with significant differences.
Results
A convenience sample of 3,246 participated in the survey from the original 31,
585 emails sent. From this original sample, 18 participants were removed from study for
disagreeing with the consent form. Twenty-four students who reported their age was less
than 18 years old were removed from the study. Thirty-one graduate level students were
removed from the survey. Two hundred and fifteen participants were removed from the
survey for reporting a sleep disorder. Fourteen participants were removed for not being a
current, enrolled Kent State University student. This left 2,944 participants that met the
inclusion criteria.

65
Demographic Details of Participants
Of participants, age ranged from 18 to 62 years with the mean age of 21.9 ± 5.8
years (n=2,749). As depicted in Table 3, majority of participants were female (n=2,143,
74.5%), of white or Caucasian ethnicity (n=2528, 87.9%), with the grade level of
participants was being highest in freshman (n= 773, 27%), followed by seniors (n=760,
26.5%), sophomores (n=684, 23.8%), and lastly juniors (n=651, 22.7%).
Table 3. Frequency and Percentage of Sex (n=2876), Grade Level (n=2868), and Ethnicity (n=2876) of Caffeine Consumers and Non-Consumers of Undergraduate College Students n %
Sex Male 773 27.0
Female 2143 72.7 Grade level
Freshman 773 27.0 Sophomore 684 23.8
Junior 651 22.7 Senior 760 26.5
Ethnicity Hispanic or Latino 71 2.5
Non-Hispanic or Latino 7 0.2 American Indian or Alaska Native 8 0.3
Asian 62 2.2 Black or African American 126 4.4
Native Hawaiian or Other Pacific Islander 3 0.1 White or Caucasian 2528 87.9
Other 71 2.5

66
Significant Differences in Sleep Between Caffeine Consumers and Non-consumers
Differences between hours of sleep between caffeine consumers (n=1340) and
non-consumers (n=442) are shown in Figure 2., whereby there was a significant
difference in sleep between non-consumers (7.93 ± 1.49) and caffeine consumers (7.66 ±
1.58) (p= 0.002).
Figure 2. Significant Difference in Mean Hours of Sleep Between Caffeine Consumers versus Non-Caffeine Consumers
Significant Differences in Sleep and Levels of Caffeine Consumption
There were significant differences between sleep and levels of caffeine
consumption. Post Hoc analysis revealed the difference in sleep was significant (p =
0.041) between non-caffeine consumers (7.93 ± 1.49) and high caffeine consumers (7.42
0 1 2 3 4 5 6 7 8 9 10
Consumer
Non-consumer
MeanHoursofSleep*Significantdifferencesbetweenvariables(p=0.002)
*TypeofCaff
eine
Con
sumer

67
± 1.40) (Figure 3). There were no other significant differences of hours of sleep among
low (7.95 ± 1.43), moderate (7.58 ± 1.50), or very high (7.36 ± 1.74), of caffeine
consumption (p>0.05): non-caffeine to low consumers (p<0.001); non-caffeine to
moderate consumers (p=0.069); non-caffeine to very high consumers (p=0.065); low
consumers to moderate consumers (p=0.200); low consumers to high consumers
(p=0.087); low consumers to very high consumers (p=0.102); moderate consumers to
high consumers (p=0.922); moderate consumers to very high consumers (p=0.871); or
high consumers to very high consumers (p=0.100).
Figure 3. Mean Hours of Sleep for Each Level of Caffeine Consumption in Undergraduate College Students Note:
Non-consumer: <5 mg (total) caffeine per day Low consumer: 5-200 mg (total) caffeine per day
Moderate: 201-500 mg (total) caffeine per day High consumer: 501-750 mg (total) caffeine per day
Very high consumer: >750 mg (total) caffeine per day
a a
012345678910
Non-Consumer Low Moderate High VeryHigh
MeanHo
urso
fSleep
LevelofCaffeineConsumpEon*LeFerssignifysignificancebetweengroups(a,p=0.041)

68
Significant Differences in GPA Between Caffeine Consumers and Non-consumers
A t-test analysis revealed a significant difference in GPA between caffeine
consumers and non-caffeine consumers (p<001). As depicted in Figure 4, the majority of
students were self-reported caffeine consumers (n=1313, 75%), with a mean GPA of 3.30
± 0.54 compared to 3.46 ± 1.12 GPA of non-consumers.
Figure 4. Significant Differences of Mean Cumulative GPA Between Caffeine Consumers and Non-consumers.
Differences in GPA and Levels of Caffeine Consumption
There were no significant differences between the levels of caffeine consumers on
GPA with frequency, percentages, means, and standard deviations as shown in Table 4.
Post Hoc analysis revealed no differences between non-consumers to low consumers
(p=1.00); non-consumers to moderate consumers (p =0.807); non-consumers to high
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
Non-consumer
Consumer
MeanCumulaEveGPA*Significantdifferencesbetweenvariables(p<0.001)
*Typeofcaff
eine
Con
sumer

69
consumers (p =0.177); non-consumers to very high consumers (p =0.207); low
consumers to moderate consumers (p =0.938); low consumers to high consumers
(p=0.360); low consumers to very high consumers (p =0.346); moderate consumers to
high consumers (p =0.709); moderate consumers to very high consumers (p =0.653); or
high consumers to very high consumers (p =0.999).
Table 4. Mean GPA and Significance between Levels of Caffeine Consumption in Undergraduate College Students (n=876) Consumer n % Mean ± Standard Deviation (points)
Non-Consumer 437 49.9 3.46 ± 1.11 Low 125 14.3 3.45 ± 0.48
Moderate 180 20.5 3.38 ± 0.45 High 81 9.2 3.23 ± 0.73
Very High 51 5.8 3.19 ± 0.53 %= percentage as defined by frequency
Significant Differences in Sex and Caffeine Consumption
Table 5 depicts the significant differences (p<0.05) between sexes in the amount
of caffeine (mg) consumed. A 2-tailed t-test found that males consume a significantly
greater amount of caffeine compared to females (p= 0.024).
Table 5. Significant Difference Between Sex and Amount of Caffeine (mg) Consumed (n=471) *Sex n % Mean ± Standard Deviation (mg)
Male 118 25.1 464 ± 447.85 Female 353 74.9 363 ± 308.77
%= percentage as defined by frequency *Signifies significant differences (p=0.024)

70
Differences in Grade Levels and Caffeine Consumption
There were no significant differences in the amount of caffeine consumed (mg)
amongst any grade level (p>0.05) as shown in Table 6. There were no significant
differences between freshmen and sophomores (p =0.994); freshmen and juniors (p
=0.582); freshmen and seniors (p =0.889); sophomores and juniors (p =0. 374);
sophomores and seniors (p =0. 710); or juniors and seniors (p =0.893).
Table 6. Frequency, Percentage, Mean, and Standard Deviation of Total Caffeine (mg) Consumed in Grade Levels of Undergraduate Students
Grade Level n % Mean ± Standard Deviation (mg) Freshman 87 49.9 364 ± 324.27
Sophomore 104 14.3 351 ± 383.81 Junior 111 20.5 428 ± 385.73
Senior 170 5.8 398 ± 336.84 Total 472 388 ± 350.71
%= percentage as defined by frequency

71
Discussion
The purpose of this study is to assess the difference in hours of sleep and
academic performance between caffeine users and non-caffeine users. The results from
the present study indicated: 1) non-caffeine consumers had a significantly higher amounts
(hours) of sleep than caffeine consumers, therefore the first hypothesis was accepted; 2)
non-caffeine consumers had a significantly higher amount (hours) of sleep than high-
intake consumers, but since there were no other significant differences amongst the levels
of caffeine consumers, the second hypothesis was only partially met; 3) there was a
significant difference in GPA between caffeine consumers and non-consumers; therefore,
the third hypothesis was accepted; 4) there was no significant difference between
different levels of caffeine consumption on GPA, therefore, the fourth hypothesis was
rejected; 5) males consumed significantly higher amounts of caffeine than females;
therefore the fifth hypothesis was accepted; 6) there was no difference between the grade
levels (freshman, sophomore, juniors, and seniors) and amount of caffeine consumed,
therefore the sixth hypothesis was rejected.
Caffeine Consumption
The affect of caffeine consumption on sleep, academic performance, sex, and
grade level are not equally significant.
Sleep. The present results of this comparative study between caffeine consumers
and non-consumers indicate that non-caffeine consumers have longer sleep duration than
caffeine consumers. This generally agrees with previous research where caffeine been

72
not only been found to decrease the length of sleep time, but also decreases the sleep
quality, leading to daytime fatigue (Lohsoonthorn et al., 2012; Whittier et al., 2013).
James (1991a) concluded that caffeine, even in small amounts, has been known to affect
the sleep cycle, resulting in decreased duration and quality of sleep. This can be related
to the present findings, where the sleep cycle of caffeine consumers might be negatively
affected by their caffeine intake, resulting in shorter sleep duration than the non-caffeine
group.
This concept can also be related to the comparison between the five levels of
caffeine consumers, where small quantities of caffeine can affect the sleep cycle, it may
be predicted that larger doses would interrupt sleep more substantially. This may then
explain the significant difference of sleep duration between non-consumers and high
consumers. However, this notion does not reflect the results of present study, which
found no difference between non-caffeine consumers and low consumers. Several
studies have found that the effects of caffeine are dose-dependent, where large doses
consumed in the late evening have shown to extend the time it takes to fall asleep at
bedtime and decreases the amount of time asleep (Carrier et al., 2009; Karacan et al.,
1976; Smith, 2002). Given that the non-consumer and low consumer have no difference
in sleep duration, it is possible that the dose-dependent factor may not start impacting
sleep until moderate amounts are consumed, as evidenced by the difference in sleep
between moderate consumers and the low and non-consumers. Anxiety is a well-known
side effect of caffeine consumption, starting as low as 200 mg doses of caffeine for some
individuals (Schardt, 2015). In previous research, anxiety is a common reason for

73
decreased quality or quantity of sleep (Buysse et al., 1988; Ginsberg, 2006; Lund et al.,
2010; Plaford, 2009; Tsai & Li, 2004). This being said, the increase of caffeine
consumed may have induced students’ anxiety, resulting in a greater lack of sleep. High
caffeine ingestion (10-30 µg/ml or >750 mg caffeine) has been linked to symptoms such
as difficulty sleeping and insomnia, which again agrees with the present results of the
significant differences between non-consumer vs. consumers and non-consumers and
high consumers (McIlvain, Noland, & Bickel, 2011; UNEP Publications, 2003; Winston
et al., 2005). The lack of significance between high and very high consumers was not
surprising because these two levels have similar negative effects, any of which may
hinder academic performance.
According to the American Psychological Association (n.d.), 21% of adults report
that their stress increases when their length and quality of sleep decreases. Caffeine is
often used to cope with this stress, but since caffeine releases the stress hormone cortisol,
stress and worry may be further increased, both of which are factors affecting sleep in the
first place (Buysse et al., 1988; Ginsberg, 2006; Lund et al., 2010; Plaford, 2009; Tsai &
Li, 2004). Therefore, the use of caffeine may further, negatively impact the duration of
sleep among caffeine consumers compared to non-caffeine users as well as cause even
more anxiety in the moderate, high, and very high caffeine consumer groups. High
caffeine intake also has a slight diuretic effect, in which frequent urination during the
night may occur, shortening the amount of sleep for the high and very high consumers
(McIlvain, Noland, & Bickel, 2011; Passmore, et al., 1987; Neuhauser-Berthold et al.,
1997). This being said, it was surprising that there was not a larger difference between

74
non-caffeine users and very high (>750mg). This is likely because the effects of caffeine
on sleep at the high dose resulted in similar effects as with the very high caffeine doses,
even though the amout of caffeine was much higher. It is possible that after a certain
level of caffeine is consumed, caffeine’s effect on sleep plateaus, resulting in similar
sleep duration.
Academic performance. In the present study, GPA of the non-caffeine
consumer group was significantly higher than the caffeine consumer group. These
findings agree with previous studies that found that GPA is lower in those that consumed
caffeinated beverages (energy drinks) (Champlin, Pasch, & Perry, 2016; Pettit & Barr,
2011). Present results show that the non-caffeine consumer and the low-caffeine (5-200
mg) consumer group had similar GPA’s. Based on previous research, an explanation for
this could be that low doses of caffeine (20-200 mg) generally reflect benefits, including
increased positive moods, energy, alertness, and sociability” (Garrett & Griffiths, 1997;
Schardt, 2015; Smith, 2002).
In terms of caffeine versus non-caffeine consumer, it is possible that since the
GPA of both the high and very high caffeine intake group was much lower than the non-
consumer’s GPA, it was able to bring down the average of the caffeine consumer group
enough to have a significant difference between the caffeine consumer and non-
consumers. The sleep duration results may also play a role in the significant difference in
GPA between non-caffeine users and caffeine users in the present study. Receiving less
than seven hours of sleep per night is one characteristic of sleep loss and poor sleep
quality and may lead to the common symptoms of excessive daytime sleepiness,

75
depressed mood, poor memory and poor concentration (Colten & Altevogt, 2006). Also,
memory consolidation occurs during sleep, so if the hours of sleep are cut short, the
student has less time to store their experiences, including learning, (Plaford, 2009). Since
caffeine had a significant impact on sleep between users and non-users and sleep has a
widely known effect on academic performance, caffeine may have had an indirect impact
on academic performance, explaining why the present results showed non-caffeine
consumers had significantly higher GPA’s than caffeine consumers.
When looking at the insignificant differences between the five levels of caffeine
consumption and GPA, there are several explanations for each category. Doses up to 300
mg (which falls within the moderate consumer level) have also been found to have these
same benefits as low caffeine consumption, however the negative effects of caffeine have
also been reported at doses above 200 mg (Garrett & Griffiths, 1997; Schardt, 2015;
Smith, 2002). These negative side effects include increased anxiety, jitteriness, insomnia,
nervousness, dizziness, headaches, and gastrointestinal distress, nausea, vomiting, and
even difficulty concentrating (Gilman, Rall, T.W., Nies, A.S., & Taylor, 1990; Institute
of Medicine (U.S.) Committee on Military Nutrition Research, 2001; UNEP Publications,
2003; Winston et al., 2005). The fact that doses in the moderate consumption category
may benefit some and negatively impact others may explain why the decrease in GPA of
this group was only slightly lower than the non-caffeine and low caffeine consumers
groups. A large amount of studies have found that individuals experience negative side
effects when caffeine is consumed in high doses (Botella & Parra, 2003; Gupta & Gupta
1999; Journal of the American Medical Association [JAMA], 2001; Schardt. 2015).
76
This, therefore, gives insight into the results of the present study, where the high and very
high caffeine consumer groups had lower GPA’s compared to the non-consumer and low
consumer groups (the moderate intake group seemed to be more of a neutral between the
lower intakes and higher intakes).
Sex. The result of the present study confirms previous research that males tend to
consume more caffeine than females (Lieberman et al., 2015; Pettit & DeBarr, 2011). In
comparing males vs. females, literature has documented 103.4 mg/day vs. 110.5 mg/day
(Somogyi, 2010), 199 mg/day vs. 166 mg/day (Frary et al., 2005 of 295.6 mg/day vs.
225.3 mg/day (Somogyi, 2010). Males do typically weigh more than females, and
therefore caffeine consumed per body weight may be a factor in why males consume
higher amounts of caffeine (mg). In defense of this argument, males were also found to
consume caffeine more frequently, with 91% of males compared to 87% of females
consuming caffeine in a two-day dietary intake survey (Frary et al., 2005). While the
half-life of caffeine is the same in both males and females, oral contraceptives almost
double the half-life of caffeine (Abernethy & Todd, 1985; Lorist & Tops, 2003;
Patwardhan et al., 1980;). Therefore, if any females were using these medications during
the study, their caffeine intake may have been lower due to the prolonged time the
caffeine was in their system.
Grade levels. For each grade level, there was a large variability in the amount
(mg) of caffeine consumed by students. The present study showed no difference in the
amount of caffeine consumed (mg) among freshman, sophomore, juniors, and seniors.
This does not reflect previous studies that found an increase of caffeine with age and

77
grade levels. One study states that 28% of college students reporting an increase in
caffeine consumption than the previous year (Traylor & Summers, n.d). One justification
for this increase is that workloads and difficulty of classes typically increases with grade
level, in which caffeine intake has been shown to increase with academic stress (Oaten
and Cheng, 2005; Tannous & Kalash, 2014). Therefore, the lack of significant
differences between amount of caffeine consumed and grade level may be due to the
timing of the survey. The survey was distributed early into the semester, and it may be
predicted that the workload was lighter, with lower amounts of academic stress as
compared to later in the semester when there are more midterms, projects, and final
examinations. Tannous and Kalash (2014) found that 17 to 20 year old students
consumed the least amount of caffeine in their study, while students age 21 to 24 years
had a significantly higher percentage of caffeine intake. However, caffeine is thought to
increase with age and so the small age difference used in the present study may be too
short to reflect the long-term increases in caffeine noted in other studies (Frary et al.,
2005; Lieberman et al., 2015; Mitchell et al., 2013; Somogyi, 2010; Zagat, 2015). The
overall, mean caffeine consumption of the present study was 364mg freshmen, 351mg
sophomores, 428mg juniors, and 351mg seniors, with a total average of 374mg
caffeine/day. While one previous study had similar results as the current findings, with
an average intake of 300 mg caffeine/day, past research generally disagrees with the
amount of caffeine consumed daily (Somogyi, 2010). The current findings were higher
than some of the other research, which found an average, daily caffeine intake of 165 mg
(Mitchell et al., 2013), 173 mg (Lieberman et al., 2015), and 183 mg (Frary et al., 2005).
78
The current study did have a lower mean caffeine intake than one study, which reported
the average daily intake to be 850 mg caffeine (McIlvain et al., 2011).
Applications
Stress, inadequate sleep and caffeine use are common in the college population. As
seen in the present study, the use of caffeine has negative effects on both the grade points
average and sleep duration of students. A high percentage of participants reported
consuming caffeine, and many were consuming caffeine doses above the recommended
limit, thus making it important to address the issues and negative effects of caffeine.
Therefore, education on time management, sleep hygiene, and healthy consumption is
critical in maintaining the health of this population. Sleep deprivation is linked to both
acute and chronic problems. Overall, the effect of inadequate sleep may directly impact
the ability of the student to learn and perform efficiently in the academic setting. Long-
term consequences of sleep loss is related to obesity, reduced immune system function,
and cardiovascular issues. Thus, educating students on the importance of sleep hygiene
will help the students reach their academic potential and decrease the risk of developing
future health problems due to chronic sleep deprivation.
A greater emphasis on the importance of moderation of caffeine use can help
decrease the negative side effects of high caffeine consumption. Not only is high
caffeine consumption linked to infertility, osteoporosis, and possible cardiovascular
problems, but also the contents of commonly consumed caffeine sources may contribute
to future health problems. Many regularly consumed sources contain high amounts of

79
sugar and fat, such as flavored coffees, sweetened teas, soda, and chocolates. With the
high frequency of these products being consumed daily, consumers must be more aware
of the negative impacts of these added calories and its contribution to obesity.
Stress is a common encounter for not only college students, but also working adults.
The juggling of deadlines, exams, and personal responsibilities can result in decreased
sleep quality and duration. The cycle of inadequate sleep and the use of caffeine to cope
with the stress are unhealthy and continue to be a problem in society. By teaching time
management skills, emphasizing the importance of sleep, and more effective ways to
cope with stress, the cycle of sleep deprivation and caffeine use may be relieved.
Integration of time management, sleep hygiene, and moderation of caffeine intake
should begin at the freshman level, where students may experience substantial changes in
these three subjects when transitioning from home to a college campus. By incorporating
a stress management component to freshman orientation, each of these topics can be
addressed along with their implications on overall health and academic performance. In
addition, dorm hall visits or on-campus seminars for all grade levels held by a
knowledgeable party may be considered for interested students to attend and receives
information on these topics. This would allow for a smaller group size, where students
have a greater opportunity to ask questions and have greater interaction amongst their
peers. Many universities are already implementing health education programs. Ball
State University has a health, alcohol, and drug education program that has trained peer
health educators go to sororities, fraternities, and dorms to present health information.
These health topics may include healthy eating, caffeine, stress management, sleep

80
hygiene, and more. Other colleges also have similar programs that can be presented per
request. A few examples of these schools include Indiana University-Purdue University
Indianapolis, Davidson College, and University of Missouri-Kansas City. The University
of New Hampshire has a stress management program that offers many different
workshops, including meditation, poetry/expressive writing, color therapy, and more.
Berkeley University also offers workshops for health education with topics including
alcohol education and stress and resilience. Even with these programs already being in
place, the incidences of reported high caffeine intake, stress, and lack of sleep
demonstrates the need to reassess and improve college and university’s current programs.
Limitations
The demographic information was not distributed equally, with greater amounts of
females (75%) and white/Caucasian ethnicity participating in the survey. Participants in
the study were generally of good academic standing. A larger demographic area could
allow more insight on the effects of caffeine and sleep on academic performance in
diverse populations with a more variable GPA range.
The participants’ current state of academic stress was not addressed in the survey,
which may affect the have affected reported caffeine intake, such as if one student had an
upcoming exam and their caffeine intake was higher than their usual. Future studies
would benefit from reporting caffeine consumption across an entire semester to better
assess caffeine intake patterns as academic stress changes. Also, understanding and
assessing other types of stress, besides academic, that students undergo may provide

81
more insight that can be related to sleep disturbances, caffeine intake, and its affect on
academic performance.
The survey used in the present research collected duration of sleep only when looking
at academic performance. Research has shows that the quality of sleep has a greater
impact on academic performance than just the duration. Similar studies in the future may
consider incorporating questions to assess the quality of the participant’s sleep per night.
Another limitation of the present study is that the true amount of caffeine
consumption (mg) was difficult to determine. A set number was used for certain sources
of caffeine (i.e. brewed, cold brewed, percolated, etc.) when a specific brand was not
named. The true level of caffeine in those sources may vary considerably depending on
brewing method, number of coffee beans/scoops used, and the brand used. Having more
specific documentation on the sources of caffeine in future studies can help researchers
obtain a more accurate, total amount of caffeine consumed.
Conclusion
This research study confirmed that in undergraduate students, those consuming
caffeine received significantly less hours of sleep per night compared to students
reporting no caffeine intake, especially between non-caffeine consumers versus those
consuming high levels of caffeine (500-570 mg caffeine/day). The GPA of non-caffeine
consumers was significantly higher than that of caffeine consumers. These results pose a
problem with current college practices in regards to caffeine use and insufficient sleep.
Since caffeine is often used by college students in the academic setting, education is
82
needed not on just the negative side effects of caffeine use, but its impact on sleep and
therefore, academic performance.

APPENDICES
APPENDIX A
SURVEY EMAILS
85
Appendix A
Survey Emails
Original Email for Survey Link
Dear Student, My name is Danielle Gabrish and I am conducting research on the difference between caffeine use, sleep, and academic performance in undergraduate college students. The survey is web-based and answers are strictly anonymous. The survey will take approximately 5-7 minutes. Participation is voluntary and refusal to take part in the study involves no penalty. Participants may withdraw from the study at any time without penalty. Your time and participation is much appreciated. Sincerely, Danielle Gabrish
Follow this link to the Survey: Take the survey
Or copy and paste the URL below into your internet browser: https://kent.qualtrics.com/SE?Q_DL=0xk0crZXWrNGh7L_6RnNwFutsUqqQmh_MLRP_eKIef0b2srJWbvT&Q_CHL=email

86
Reminder Email for Survey Link
Dear Student, My name is Danielle Gabrish and I am conducting research on the difference between caffeine use, sleep, and academic performance in undergraduate college students. If you have already completed this survey, I thank you for your participation and you may disregard this email. The survey is web-based and answers are strictly anonymous. The survey will take approximately 5-7 minutes. Participation is voluntary and refusal to take part in the study involves no penalty. Participants may withdraw from the study at any time without penalty. Your time and participation is much appreciated. Sincerely, Danielle Gabrish
Follow this link to the Survey: Take the survey
Or copy and paste the URL below into your internet browser: https://kent.qualtrics.com/SE?Q_DL=9yjXOhX7Q5Gz1JP_6RnNwFutsUqqQmh_MLRP_9NxXYYqyML2BvZH&Q_CHL=email

APPENDIX B
SURVEY QUESTIONNAIRE

88
Appendix B
Survey Questionnaire
Caffeine use, sleep, and academic performance in undergraduate college students Q19 Informed consent m I agree (1) m I disagree (2) Condition: I disagree Is Selected. Skip To: End of Survey. Part I: Demographic Information Q1 Age ___ Q2 Sex m Male (1) m Female (2)
Q3 Ethnicity m Hispanic or Latino (1) m Non-Hispanic or Latino (2) m American Indian or Alaska Native (3) m Asian (4) m Black or African American (5) m Native Hawaiian or Other Pacific Islander (6) m White or Caucasian (7) m Other (8) ____________________ Q4 Are you currently a student enrolled at a Kent State University? m Yes (1) m No (2) If No Is Selected, Then Skip To End of Survey Q18 What is your grade level? m Freshman (1) m Sophomore (2) m Junior (3) m Senior (4) m Graduate (5) If Graduate Is Selected, Then Skip To End of Survey

89
Q5 How many credit hours are you taking this semester? ___ Q6 Have you ever been diagnosed with a sleeping disorder? m Yes (1) m No (2) If Yes Is Selected, Then Skip To End of Survey Part II: Caffeine Consumption Questionnaire Q8 Do you consume caffeine? m Yes (1) m No (2) If No Is Selected, Then Skip To End of Block Q9 at what age did you start consuming caffeinated beverages/diet pills (excludes chocolate products)? ___ Q11 Please open the attachment "Caffeine Source List" below and type in the number of servings of the caffeinated product and the time(s) when they are typically consumed in one average day. If the beverage/product is not listed, please type in the specific name along with the quantity and time consumed. Re-upload once form is complete. Caffeine Source List EXAMPLE: Serving size Caffeine Source Servings Consumed Time(s) Brand (other): Starbuck's Iced Coffee 1 grande 10:30 AM
Serving size Caffeine Source Servings Consumed Time(s)
12 oz. (small) Coffee
Regular brewed, drip (Maxwell, Folgers, Eight O' Clock)
Regular, instant (crystallized coffee that dissolves in hot water)
Cold-brew coffee Decaffeinated, brewed Decaffeinated, instant Instant
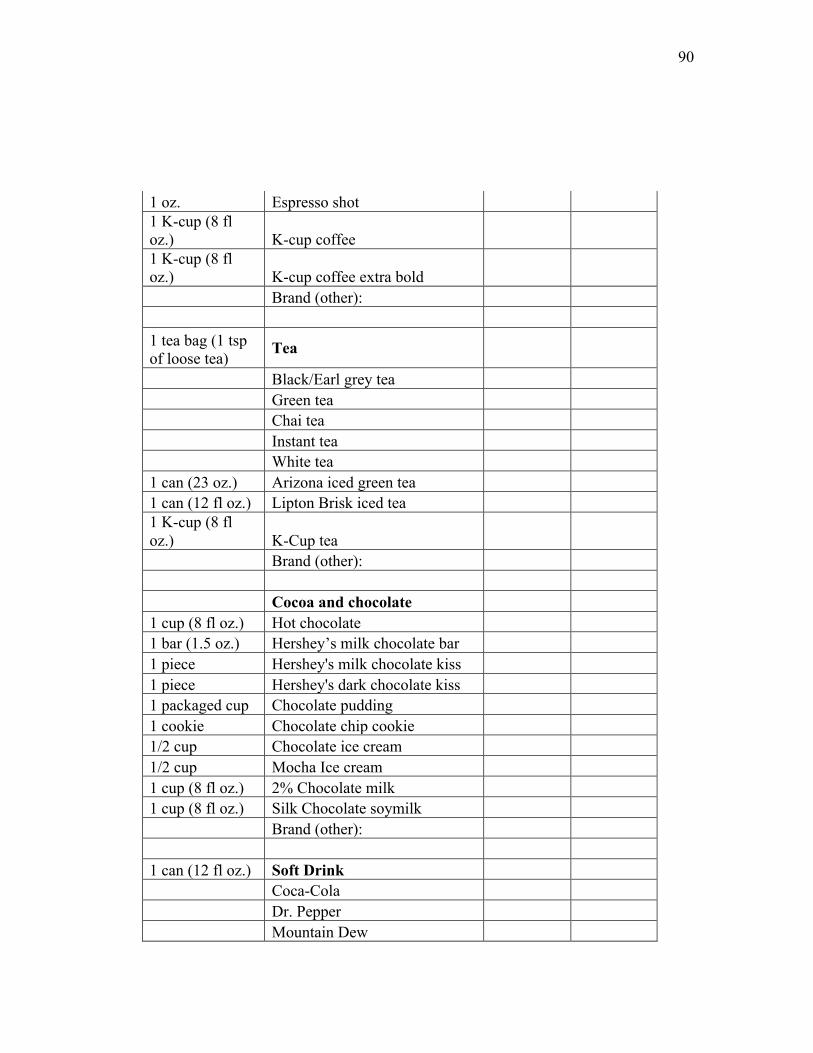
90
1 oz. Espresso shot 1 K-cup (8 fl oz.) K-cup coffee 1 K-cup (8 fl oz.) K-cup coffee extra bold Brand (other): 1 tea bag (1 tsp of loose tea)
Tea
Black/Earl grey tea Green tea Chai tea Instant tea White tea 1 can (23 oz.) Arizona iced green tea 1 can (12 fl oz.) Lipton Brisk iced tea 1 K-cup (8 fl oz.) K-Cup tea Brand (other): Cocoa and chocolate 1 cup (8 fl oz.) Hot chocolate 1 bar (1.5 oz.) Hershey’s milk chocolate bar 1 piece Hershey's milk chocolate kiss 1 piece Hershey's dark chocolate kiss 1 packaged cup Chocolate pudding 1 cookie Chocolate chip cookie 1/2 cup Chocolate ice cream 1/2 cup Mocha Ice cream 1 cup (8 fl oz.) 2% Chocolate milk 1 cup (8 fl oz.) Silk Chocolate soymilk Brand (other): 1 can (12 fl oz.) Soft Drink Coca-Cola Dr. Pepper Mountain Dew

91
Mr. Pibb Tab Pepsi Cola RC Cola Mello Yello Root Beer Brand (other): Energy Drinks 8.4 fl oz. Red Bull 1 can (16 fl oz.) Monster 1 can (16 fl oz.) Rockstar 1 can (16 fl oz.) NOS 1 can (16 fl oz.) Amp 1 can (16 fl oz.) Full Throttle 1 can (8 fl oz.) V8 C-Fusion + Energy 1 can (8 fl oz.) Mountain Dew Kick Start 1 can (16 fl oz.) Venom 1 can (16 fl oz.) Xyience Xenergy 1 container (6 fl oz.)
5 hour energy
Brand (other): Over-The-Counter Pills 2 capsules Zantrex weight loss supplement 1 capsule Noz Doz 1 capsule Vivarin 2 tablets Excedrin migraine 2 capsules Midol complete 2 capsules Bayer back and body 2 tablets Anacin Brand (other): Supplements 1 scoop BPI 1.M.R. 1 capsule BSN Hyper Shred

92
1 scoop Cellucor C4 or C5 Extreme
1 scoop Cellucor C4 Pre-workout/mass/ripped
1 scoop Muscle Pharm Assault 1 scoop MuscleTech Neurocore 1 scoop Pre JYM 1/16 teaspoon Pure caffeine powder
B-complex supplement brand:
Brand (other):
Part III: Sleep Questionnaire Q13 What time do you typically fall asleep on weekdays? _____ Q14 What time do you typically wake up on weekdays? _____ Q15 What time do you typically fall asleep on weekends? _____ Q16 What time do you typically wake up on weekends? _____ Q17 How long does it take you to fall asleep once you've laid down? _____ Q18 What is your cumulative grade point average (GPA)? _____ Q19 How many of your credit hours are online? _____ Q20 Do you feel your caffeine intake increases during times of academic stress (i.e. upcoming exams)? m Yes (1) m No (2)

APPENDIX C
CONSENT FORM
94
Appendix C
Consent Form
Differences Between Caffeine Use, Hours of Sleep, and Academic Performance of Undergraduate College Students
“Difference between caffeine use, hours of sleep, and academic performance” is a web-based survey to analyze the differences between. Before taking part in this study, please read the consent form below and click on the "I Agree" button at the bottom of the page if you understand the statements and willingly consent to participate in the study.
Consent Form
The study involves a web-based experiment designed to help identify the effects of caffeine on sleep and academic performance. The study is being conducted by Danielle Gabrish of Kent State University, and it has been approved by the Kent State University Institutional Review Board. No deception is involved, and the study involves no more than minimal risk to participants (i.e., the level of risk encountered in daily life). This survey will take approximately 5-7 minutes and answers are strictly anonymous. The study consists of four sections. Participants begin by answering demographic and exclusion criteria questions. After, the participants will answer a series of caffeine consumption questions, including filling out a table on their typical intake of listed caffeine sources. Participants will then answer a sleep questionnaire to assess sleep and wake times. Lastly, participants will answer academic questions, in which their cumulative grade point average will be entered.
All responses are treated as confidential, and in no case will responses from individual participants be identified. Rather, all data will be pooled and published in aggregate form only. Participants should be aware, however, that the experiment is not being run from a "secure" https server of the kind typically used to handle credit card transactions, so there is a small possibility that responses could be viewed by unauthorized third parties (e.g., computer hackers).
Individuals’ participation in this study does not include any compensation (i.e. monetary or class credit). The study is restricted to a specific population and will not be assessable to visitors of this website. Participation is voluntary; refusal to take part in the study involves no penalty. Participants may withdraw from the study at any time without penalty. If participants have further questions about this study or their rights, or if they wish to lodge a complaint or concern, they may contact the principal investigator, Associate

95
Professor Natalie Caine-Bish, at (330)-672-2197; or the Kent State University Institutional Review Board, at (330) 672-0709.
If you are 18 years of age or older, understand the statements above, and freely consent to participate in the study, click on the "I Agree" button to begin the experiment.
I Agree I Do Not Agree

REFERENCES
97
REFERENCES
Abernethy, D.R. & Todd, E.L. (1985). Impairment of caffeine clearance by chronic use of low-
dose oestrogen-containing oral contraceptives. European Journal of Clinical
Pharmacology, 28(4), 425-428. doi:10.1007/BF00544361
Abraham, A. & Scaria, J. (2015). Influence of sleep in academic performance- An integrated
review of literature. Journal of Nursing and Health Science. (4)4:78-81.
Al'Absi, M. Lovallo, W.R., Mckey, B., Sung, B.H., Whitsett, T.L., & Wilson, M.F. (1998).
Hypothalmic-pituitary-adrenocortical responses to psychological stress and caffeine in
men at high and low risk for hypertension. Psychosomatic Medicine, 60(4), 521-527
American College Health Association. (2009). National College Health Assessment: Fall 2009.
Retrieved on 6 March 2017 from http://www.acha-ncha.org/reports_ACHA-
NCHAII.html
ACHA-NCHAII.html. Accessed March 29, 2010.
American Psychological Association. (n.d.). Stress and Sleep. Retrieved from
http://www.apa.org/news/press/releases/stress/2013/sleep.aspx
Ari, A., Atalay, O.T. & Aljamhan, E. (2010). From admission to graduation: the impact of
gender on student academic success in respiratory therapy education. J Allied Health,
39(3), 175-178

98
Armstrong, L.E., Pumerantz, A.C., Roti, M.W., Judelson, D.A., Watson, G., Dias, J.C.,…
Kellogg, M. (2005). Fluid, electrolyte, and renal indices of hydration during 11 days of
controlled caffeine consumption. International Journal of Sport Nutrtion and Exercise
Metabolism, 15, 252-265. Retrieved from
http://www.sportsnutritionworkshop.com/files/32.spnt.pdf
Astin, A. W. (1971). Predicting academic performance in college: Selectivity data for 2300
American colleges. New York: Free Press.
Astin, A.W. & Panos, R.J. (1969). The educational and vocational development of college
students. Washington, DC: American Counsel on Education
Attila, S. & Çakir, B. (2011). Energy-drink consumption in college students and associated
factors. Nutrition, 27(3), 316–322. doi:10.1016/j.nut.2010.02.008
Balaghi, S., Faramarzi, E., Mahdavi, R., & Ghaemmaghami, J.(2011). Fluids intake and
beverage consumption pattern among university students. Health Promotion
Perspectives, 1(1), 54-61. doi: 10.5681/hpp.2011.005
Ball State University. Health, alcohol, and drug education. Accessed on 9 February 2017 from
http://cms.bsu.edu/about/administrativeoffices/healtheducation
Basheer, R., Strecker, R., Thakkar, M., & Mccarley, R. (2004). Adenosine and sleep/wake
regulation. Progress in Neurobiology, 73(6), 379-396. doi:
10.1016/j.pneurobio.2004.06.004
99
Becker, C.M., Adams, T., Orr, C., & Quilter, L. (2008). Correlates of quality of sleep and
academic performance. The Health Educator, 40(2), 82-89. Retrieved from
https://eric.ed.gov/?id=EJ863513
Berkeley University of California. University health services. Accessed on 9 February 2017 from
https://uhs.berkeley.edu/hpservices
Best College Values. What is a good college GPA? Retrieved from
http://www.bestcollegevalues.org/what-is-a-good-gpa/. Accessed on 21 Nov. 2016.
Beverage World. (2010). State of the Industry, 14.
Borota, D., Murray, E., Keceili, G., Chang, A., Watabe, J.M., Ly, M., … Yassa, M.A. (2014).
Post-study caffeine administration enhances memory consolidation in humans. Nature
Neuroscience, 17, 201-203. doi: 10.1038/nn.3623
Botella, P. & Parra, A. (2003). Coffee increases state anxiety in males but not in females.
Hum Psychopharmacol, 18(2), 141-3. doi: 10.1002/hup.444
Buboltz, W. C., Brown, F., & Soper, B. (2001). Sleep habits and patterns of college students: A
preliminary study. Journal of American College Health, 50(3), 131-135. doi: 11765249
Bolùmar, F., Olsen, J., Rebagliato, M., Bisanti, L., & the European Study Group on Fertility and
Subfecundity. (1997). Caffeine intake and delayed conception: A European multicenter
study on fertility and subfecundity. Journal of Epidemiology, 145, 4, 324-334

100
Berger, L., Fendrich, M., & Fuhrmann, D. (2013). Alcohol mixed with energy drinks: Are there
associated negative consequences beyond hazardous drinking in college students?
Addictive Behavior, 38(9), 2428–2432. doi:10.1016/j.addbeh.2013.04.003.
Butler, M.A., Lang, N.P., Young, J.F., Caporaso, N.E., Vineis, P., Hayes, R.B.,… Kadlubar, F.F.
(1992). Determination of CYP1A2 and NAT2 phenotypes in human populations by
analysis of caffeine urinary metabolites. Pharmacogenetics 2(3), 116-127.
Buysse, D.J., Reynolds, C.F., Monk, T.H., Berman, S.R., & Kupfer, D.J. (1998). The Pittsburg
quality index: A new instrument for psychiatric practice and research. Psychiatry
Research, 28, 193-213.
Caffeine Informer. (n.d.). Caffeine Content of Drinks. Retrieved on 4 January 2017 from
http://www.caffeineinformer.com/the-caffeine-database
Caffeine Informer. (n.d.). Caffeine Metabolism. Retrieved on 28 February 2017 from
https://www.caffeineinformer.com/caffeine-metabolism
Caffeine Informer. (2016). Caffeine in Workout Supplements. Retrieved on 20 February 2017
from http://www.caffeineinformer.com/caffeine-in-workout-supplements
Caffeine Informer (2016). Top Selling Energy Drink Brands. Retrieved on 5 May 2017 from
https://www.caffeineinformer.com/the-15-top-energy-drink-brands

101
Campus health: Health Education. Indiana-Purdue University Indianapolis. Accessed on 9
February 2017 from https://www.iupui.edu/
Carrier, J., Paguet, J., Fernandez-Bolanos, M., Girourd, L., Roy, J., Selmaoui, B., & Filipini, D.
(2009). Effects of caffeine on recovery sleep: A double challenge to the sleep-wake cycle
in aging. Sleep Medicine, 10(9), 1016-1024. doi:10.1016/j.sleep.2009.01.001
Carskadon, M.A., & Dement, W.C. (2011). Monitoring and staging human sleep. In M.H.
Kryger, T. Roth, & W.C. Dement (Eds.), Principles and Practice of Sleep Medicine, 5,
16-26.
Center for Science in the Public Interest. (n.d.). Caffeine Chart. Retrieved on 20 February 2014
from https://cspinet.org/eating-healthy/ingredients-of-concern/caffeine-chart
Champlin, S.E., Pasch, K.E., & Perry, C.L. (2016). J Primary Prevent, (4)37: 345-359.
doi:10.1007/s10935-016-0437-4
Coffee & Health. Sources of caffeine. Retrieved from http://coffeeandhealth.org/topic-
overview/sources-of-caffeine/
Colten, H.R., & Altevogt, B,M. (2006). Institute of Medicine (US) Committee on Sleep Medicine
and Research. Washington (DC), National Academies Press (US).

102
Cozart, L. & Riddle, E. (2011). Insights into your core consumer on campus [PowerPoint slides].
Retrieved from OnCampus Research website:
https://www.nacs.org/LinkClick.aspx?fileticket=_tB1l3GJewg%3D&tabid=3010&mid=4
179
Curcio, G., Ferrara, M. De Gennaro, L. (2006). Sleep loss, learning capacity and academic
performance. Sleep Medicine Reviews, 10, 323-337. doi: 10.1016/j.smrv.2005.11.001
Daly, J.W. (1993). Mechanism of action of caffeine. Caffeine, Coffee, and Health, Garattini, S.,
Ed., Raven Press, New York, 97.
Daly, J.W. & Fredholm, B.B. (1998). Caffeine: An atypical drug of dependence. Drug and
Alcohol Dependence, 51(1-2), 199-206. http://dx.doi.org/10.1016/S0376-8716(98)00077-
5
Davidson College. Health Education. Accessed on 9 February 2017 from
https://www.davidson.edu/student-life/health-and-counseling/health-education
Delannoy, J., Mandai, O., Honoré, J., Kobayashi, T., & Sequeira, H. (2015). Diurnal Emotional
States Impact the Sleep Course. PLoS One, 10(11), e 0142721. doi:
10.1371/journal.pone.0142721
Diaz, K. (2016). Smoking and sleep. American Sleep Association. Retrieved from
https://www.sleepassociation.org/blog-post/smoking-and-sleep/
103
Drug Abuse Warning Network. (2011). Emergency department visits involving energy drinks.
Substance Abuse and Mental Health Services Administration, 89, 1-5. Retrieved from
http://oas.samhsa.gov.
Dewald, J.F., Meiher, A.M., Oort, F.J., Kerkhof, G.A., & Bogels, S.M. (2010). The influence of
sleep quality, school duration and sleepiness on school performance in children and
adolescents: A meta-analytic review. Sleep Med Reviews, 14, 179-189. doi:
10.1016/j.smrv.2009.10.004
Dickelmann, S. & Born, J. (2010). The Memory function of sleep . Nature Reviews Neuroscience
11, 114-126. doi:10.1038/nrn2762
Digdon, N. L. Circadian preference and college students; beliefs about sleep education.
Chronobiology International, 27(2), 297-317. doi: 10.3109/07420520903502895
Epstein, J. (2010). Grades on the rise. Inside Higher Ed. Retrieved from
https://www.insidehighered.com/news/2010/03/05/grades. Accessed on 22 Nov. 2016
European Food Safety Authority. (2015). Scientific opinion on the safety of caffeine. EFSA
Journal, 13(15), 4102.
Flinn, S., Gregory, J., McNaughton, L.R., Tristram, S. & Davies, P. (1990). Caffeine ingestion
prior to incremental cycling to exhaustion in recreational cyclists. Int J Sports Med.,
11(3), 188-193

104
Food and Drug Administration. (2007). Medicines in my home: Caffeine and your body.
Retrieved from https://www.fda.gov/downloads/ucm200805.pdf
Frary, C.D., Johnson, R.K., & Wang, M.Q. (2005). Sources and intakes of caffeine in the diets of
persons in the United States. Journal of the American Dietetic Association, 1, 110-113
Fredholm, B.B. (1995). Adenosine, adenosine receptors and the actions of caffeine.
Pharmacology & Toxicology, 76, 93-101. doi: 10.1111/j.1600-0773.1995.tb00111.x
Fredholm, B.B., Arslan, G., Johansson, B., Kull, B. & Svenningsson P. (1997). Adenosine A2A
receptors and the actions of caffeine. The Role of Adenosine in the Nervous System,
Okada Y., Ed. Elsevier Elsevier, Amsterdam, 51
Gallini, J. (1982). Evidence of an adaptive level grading practice through a causal approach.
Journal of Experimental Education, 50, 188-194
Garrett, B.E. & Griffiths, R.R. (1997). The role of dopamine in the behavioral effects of caffeine
in animals and humans. Pharmacol. Biochem. Behav., 57(3), 533-541
Gaultney, J. F. (2010). The prevalence of sleep disorders in college students: Impact on academic
performance. Journal of American College Health, 59(2), 91.
doi:10.1080/07448481.2010.483708
George, J., Murphy, T., Roberts, R., Cooksley, W.G.E., Halliday, J.W., & Powell, L.W. (1986).
Influence of alcohol and caffeine consumption on caffeine elimination. Clinical and

105
Experimental Pharmacology and Physiology, 13(10), 731-736. doi: 10.1111/j.1440-
1681.1986.tb02414.x
Gilman, A.G., Rall, T.W., Nies, A.S., & Taylor, P. (1990). Goodman and Gilman’s: The
pharmacological bases of therapeutics in two volumes. New York: McGraw-Hill, 625
Ginsberg, J. (2006). Academic worry as a predictor of sleep disturbance in college students.
Journal of Young Investigators.
Gonzalez de Mejina, E. & Ramirez-Mares, M.V. (2014). Impact of caffeine and coffee on our
health. Trends in Endocrinology and Metabolism, 25(10), 491. doi:
10.1016/j.tem.2014.07.003
Gropper, S. S., Smith, J. L., & Groff, J.L. (2009). Advanced nutrition and human metabolism
(5th ed.). Belmont, CA: Wadsworth, Cengage Learning
Guerreiro, S., Toulorge, D., Hirsch, E., Marien, M., Sokoloff, P., & Michel, P.P. (2008).
Paraxanthine, the primary metabolite of caffeine, provides protection against
dopaminergic cell death via stimulation of ryanodine receptor channels. Molecular
Pharmacology, 74(4), 980–989. doi:10.1124/mol.108.048207
Guest, N., Jamnik, J., Womack, C., El-Sohemy, A. (2015). Genetic variation related to caffeine
metabolism or response during exercise. Journal of the International Society of Sports
Nutrition, 12(1),53. Retrieved from http://www.jissn.com/content/12/S1/P53

106
Gupta, B.S. & Gupta, U (1999). Caffeine and behavior: Current views and research trends. CRC
Press, 22, 1-231
Harb, J.N., Taylor, Z.A., Khullar, V. & Sattari, M. (2016). Rare cause of acute hepatitis: A
common energy drink BMJ Case Report. doi: 10.1136/bcr-2016-216612
Harvard Medical (2007). External factors that affect sleep. Retrieved from
http://healthysleep.med.harvard.edu/healthy/science/how/external-factors.
Heckman, M. A., Weil, J., & Gonzalez de Mejia, E. (2010). Caffeine (1, 3, 7-trimethylxanthine)
in foods: A comprehensive review on consumption, functionality, safety, and regulatory
matters. Journal of Food Science, 75(3), R77-87. doi:10.1111/j.1750-3841.2010.01561.x
Hering-Hanit, R. & Gadoth, N. (2003). Caffeine-induced headache in children and adolescents.
Cephalalgia, 23(5), 332-335.
Hidiroglu, S., Tanriover, O., Unaldi, S., Sulun, S., & Karavus, M. (2013). A survey of energy-
drink consumption among medical students. J Pal Medical Association, 63(7), 842-845
Hirshkowitz, M., Whiton, K., Albert, S.M, Alessi, C., Bruni, O., DonCarlos, L., … Hillard, A.
(2015). National Sleep Foundation’s updated sleep duration recommendations: final
report. Sleep Health: Journal of the National Sleep Foundation, 1(4), 40-43. doi:
http://dx.doi.org/10.1016/j.sleh.2015.10.004

107
Hodgman, M.J. (1998). Caffeine. Wexler P, ed. Encyclopedia of Toxicology. San Diego:
Academic Press, 209-210
Horne, J.A. & Östberg, O. (1976). A self-assessment questionnaire to determine morningness-
eveningness in human circadian rhythms. International Journal of Chronobiology, 4, 97-
110
Horne, J. (1988). Why We Sleep. New York: Oxford University Press.
Howell, A.J., Jahrig, J.C., & Powell, R.A. (2004). Sleep quality, sleep propensity and academic
performance. Percept. Motor Skills 99(2),525-535
Jacob, B.A. (2002). Where the boys aren't: Non-cognitive skills, returns to school and the gender
gap in higher education. Economics of Education Review, 21(6), 589-598
Jacobs, J.A. (1999). Gender and the stratification of colleges. The Journal of Higher Education,
70(2),161-187
JAMA 100 years ago. (2001). Journal of the American Medical Association, 4, 285, 384.
doi:10.1001/jama.285.4.384
James, J.E. (1991a). Caffeine and Health. Academic Press: London, Ed.
James, J.E. (1991b). Human reproduction. Caffeine and Health, edited by J. E. James. London:
Academic Press, pp. 219–244.

108
James, J.E. (1994). Does caffeine enhance or merely restore degraded psychomotor
performance? Neuropsychobiology, 30, 306.
James, J.E. & Rogers, P.J. (2005). Effects of caffeine on performance and mood: withdrawal
reversal is the most plausible explanation. Psychopharmacology, 182(1), 1-8.
doi:10.1007/s00213-005-0084-6
Johnson, S.J., Alford, C., Verster J.C., & Stewart, K. (2015). Motives for mixing alcohol with
energy drinks and other non-alcoholic beverages and its effects on overall alcohol
consumption among U.K. students. Appetite, 1(96), 588-97. doi:
10.1016/j.appet.2015.10.007.
Kalow,W. & Tang, B.K. (1993). The use of caffeine for enzyme assays: A critical-appraisal.
Clinical Pharmacology and Therapeutics, 53(5), 505-514.
Karacan, I., Thornby, J.I., Anch, M., Booth, G.H., Williams, R.L., Salis, P.J. (1976). Dose-
related sleep disturbances induced by coffee and caffeine. Clin Pharm Ther, 20, 682–689
Karthigeyan, K. & Nirmala, K. (2012). Academic achievement in English: An analysis through
gender lens. Journal of Educational Studies, 2(2), 144-157
Katan, M.B. & Schouten, E. (2005). Caffeine and arrhythmia. The America Journal of Clinical
Nutrition, 81(3), 539-540.

109
Kenney, S.R., Paves, A.P., Grimaldi, E.M., & LaBrie, J.W. (2014). Sleep quality and alcohol risk
in college students: Examining the moderating effects of drinking motives. Journal of
American College Health, 62(5), 301–308. doi: 10.1080/07448481.2014.897953
Killer, S.C., Blannin, A.K., & Jeukendrug, A.E. (2014) No evidence of dehydration with
moderate daily coffee intake: A counterbalanced cross-over study in a free-living
population. Coffee Ingestion and Fluid Balance, 9(1), e84154.
doi:10.1371/journal.pone.0084154
Killgore W.D.S. (2010). Effects of sleep deprivation on cognition. Progress in Brain Research,
185, 105-129. doi:10.1016/B978-0-444-53702-7.00007-5
Kovacs, B. 2008. Sources of Caffeine. Retrieved from http://www.Medicinenetcom
Kristiansen, M., Levy-Milne, R., Barr, S., & Flint, A. (2005) Dietary supplement use by varsity
athletes at a Canadian university. Int J Sport Nutr Exerc Metab., 15, 195–210. doi:
Institute of Medicine (U.S.).Committee on Military Nutrition Research. (2001). Caffeine for the
Sustainment of Mental Task Performance: Formulations for Military Operations.
Washington, D.C.: National Academy Press.
LeBlanc, J., Jobin, M., Côté, J. Samson, P., & Labrie, A. (1985). Enhanced metabolic response
to caffeine in exercise-trained human subjects. Journal of Applied Physiology, 59(3),
832-837
110
Lieberman, H., Marriott, B., Judelson, D., Glickman, E., Geiselman, P., Giles, G., Mahoney, C.
(2015). Intake of caffeine from all sources including energy drinks and reasons for use in
U.S. college students. Journal of the Foundation of American, 29(1).
Lieberman, H.R., Tharion, W.J., Shukitt-Hale, Speckman, K.L. & Tulley, R. (2002). Effects of
caffeine, sleep loss, and stress on cognitive performance and mood during U.S. Navy
SEAL training. Psychopharmacology, 164(3), 250–261. doi: 10.1007/s00213-002-1217-9
Lohsoonthorn, V., Khidir, H., Casillas, G., Lertmaharit, S., Tadesse, M.G., Pensuksan,
W.C.,…Williams, M.A. (2012). Sleep quality and sleep patterns in relation to
consumption of energy drinks, caffeinated beverages, and other stimulants among Thai
college students. Sleep Breath doi: 10.1007/s11325-012-0792-1
Lovallo, W.R., Farag, N.H., Vincent, A.S., Thomas, T.L., and Wilson, M.F. (2006).
Cortisol responses to mental stress, exercise, and meals following caffeine intake in men
and women. pharmacology, Biochemistry and Behavior 83(3), 441-447. doi:
10.1016/j.pbb.2006.03.005
Lund, H.G., Reider, B.D., Whiting, A.B. & Prichard, J.R. (2009). Sleep patterns and predictors
or disturbed sleep in a large population of college students. Journal of Adolescent Health.
doi: 10.1016/j.jadohealth.2009.06.016
Mahan, K. L., & Escott-Stump, S. S. (2008). Krause’s food & nutrition therapy (12th ed.). St.
Louis, MS: Saunders, Elsevier
111
Maia, L., de Mendonca, A. (2002) Does caffeine intake protect from Alzheimer’s disease? Eur J
Neurol 9(4), 377-382
Malinauskas, B.M., Aeby, V.G., Overton, R.F., Carpenter-Aeby, T., & Barber-Heidal, K. (2007).
A survey of energy drink consumption patterns among college students. Nutrition
Journal, 6(35). doi:10.1186/1475-2891-6-35
March of Dimes. (2015). Caffeine in pregnancy. Retrieved from
http://www.marchofdimes.org/pregnancy/caffeine-in-pregnancy.aspx#
Marczinski, C.A. (2011). Alcohol mixed with energy drinks: Consumption patterns and
motivations for use in U.S. college students. International Journal of Environmental
Research and Public Health, 8(8), 3232-3245; doi:10.3390/ijerph8083232
Masrom, M. & Usat, S. (2015). Use of online social networking and academic performance of
students. Encyclopedia of Information Science and Technology (3rd ed.). doi:
10.4018/978-1-4666-5888-2.ch259 Maughan, R.J. & Griffin, J. (2003). Caffeine
ingestion and fluid balance: A review. Journal of Human Nutrition and Dietetics, 16(6),
411-420. Doi: 10.1046/j.1365-277X.2003.00477.x
Mayo Clinic. Caffeine: How much is too much? Retrieved from
http://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/in-
depth/caffeine/art-20045678. Accessed on 18 Nov. 2016.

112
McCornack, R.L. & McLeod, M.M. (1988). Gender bias in the prediction of college course
performance. Journal of Educational Measurement, 25(4), 321-331
McIlvain, G.E., Noland, M.P., Bickel, R. (2011). Caffeine consumption patterns and beliefs of
college freshman. American Journal of Health Education, (42)4: 235-243.
Merriam Webster. Caffeine. Retrieved on 11 Nov. 2016 from http://www.merriam-
webster.com/dictionary/caffeine
Mitchell, D.C, Knight, C.A., Hockenberry, J., Teplansky, R., & Hartman, T.J. (2013). Beverage
caffeine intakes in the U.S. Food and Chemical Toxicology, 63(2014), 136-142. doi:
10.1016/j.fct.2013.10.042
Mowry, J.B., Spyker, D.A., Cantilena, L.R., McMillan, N., & Ford, M. (2014). 2013 Annual
report of the american association of poison control centers’ national poison data system
(NPDS): 31st annual report. Clinical Toxicology, 52, 1032-1282. doi:
10.3109/15563650.2014.987397
Muuss, R. (1996). Theories of adolescence (6th ed.). New York: McGraw-Hill.
Muzet, A. (2007). Environmental noise, sleep, and health. Sleep Medicine Reviews, 11(2), 135-
142. doi: http://dx.doi.org/10.1016/j.smrv.2006.09.001
National Association of College Stores. (2012). Student watch: Trends of student consumers
[PDF document]. Retrieved from www.nacs.org/research

113
National Center for Biotechnology Information. (n.d.). Caffeine. PubChem Compound Database.
Accessed on 17 November, 2016 from https://pubchem.ncbi.nlm.nih.gov/compound/2519
National Sleep Foundation. (n.d.). How alcohol affects the quality—and quantity—of sleep.
Retrieved from https://sleepfoundation.org/sleep-topics/how-alcohol-affects-sleep
Nehlig, A., Deval, J.L., & Debry, G. (1992). Caffeine and the central nervous system:
Mechanisms of action, biochemical metabolic and psychostimulant effect. Brain Res.
Rev., 17, 139.
Neuhauser-Berthold, Beine S., Verwied S.C., & Luhrmann P.M. (1997). Coffee consumption
and total body water homeostasis as measured by fluid balance and bioelectrical
impedance analysis. Ann Nutr Metab., 41(1), 29-36.
Nicholson, A.N. & Stone, B.M. (1980). Heterocyclic amphetamine derivatives and caffeine on
sleep in man. Br. J. Clin. Pharmac., 9(2), 195-203. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1429858/
O’Brien, M.C., McCoy, T.P., Rhodes, S.D., Wagoner, A., & Wolfson, M. (2008). Caffeinated
cocktails: Energy drink consumption, high-risk drinking, and alcohol-related
consequences among college students. Society for Academic Emergency Medicine, 15(5),
453-460. doi:10.1111/j.1553-2712.2008.00085.x
114
Oaten, M. & Cheng, K. (2005). Academic examination stress impairs self-control. Journal of
Social and Clinical Psychology, 24(2), 254-279.
Olin College. Student academic performance. Retrieved from http://www.olin.edu/course-
catalog/academic-policies/student-academic-performance/. Accessed on 22 Nov. 2016.
Orzech, K.M., Salafsky, D.B., & Hamilton, L. (2011). The state of sleep among college students
at a large public university. Journal of American College Health, 8(7), 612-619. doi:
10.1080/07448481.2010.520051
Oxford University Press. Sleep. Retreived from
https://en.oxforddictionaries.com/definition/sleep. Accessed on 22 Nov. 2016.
Parliment, T.H., Ho, C., and Schieberle, P. (2000). Caffeinated beverages: Health benefits,
physiological effects, and chemistry. American Chemical Society. [ACS Symposium
series] 754, 2-46s
Passmore, A.P., Kondowe, G.B., & Johnston, G.D. (1987). Renal and cardiovascular effects of
caffeine: A dose-response study. Clinical Science, 72(6), 749-756. doi:
10.1042/cs0720749

115
Pattison, S., Rusin, Y., & Bai, Y. (2016) Caffeine consumption among college students: Its effect
on sleep hours and academic achievement. Journal of the Academy of Nutrition and
Dietetics, 116(9), A-13
Patwardhan, R.V., Desmond, P.V., Johnson, R.F., & Schenker, S. (1980). Impaired elimination
of caffeine by oral-contraceptive steroids. Journal of Laboratory and Clinical Medicine,
95(4), 603-608
Perkins, R. & Williams, M.H. (1975). Effect of caffeine upon maximal muscular endurance of
females. Med Sci Sports, 7(3), 221-224
Pettit, M. L., & DeBarr, K. A. (2011). Perceived stress, energy drink consumption, and academic
performance among college students. Journal of American College Health, 59(5), 335–
341
Phillips, A.B. & Danner, F.J. (1995). Cigarette Smoking and Sleep Disturbance. Arch Intern
Med., 155(7), 734-737. doi:10.1001/archinte.1995.00430070088011
Pfaff, C. (2013). Sleep habits and caffeine use in college students: A convenience sample. Kent
State University College and Graduate School of Education, Health, and Human Services
Pilcher, J.J., Douglass, G.R., & Sadowsky, B. (1997). Sleep quality versus sleep quantity:
Relationships between sleep and measures of health, well-being, and sleepiness in college
students. Journal of Psychosomatic Research, 42(6), 583-596.

116
Pilette, W.L. (1983). Caffeine: Psychiatric grounds for concern. J. Psycho. Nurs. Ment. Health
Serv., 21, 19.
Plaford, G.E. (2009). Sleep and learning: The magic that makes us healthy and smart. Maryland:
Lanham: Rowman & Littlefield.
Preedy, V.R. (2012). Caffeine: Chemistry, analysis, function, and effects. Cambridge, UK: Royal
Society of Chemistry.
Randall, M. (2011). The physiology of stress: Cortisol and the hypothalamic-pituitary-adrenal
axis. Dartmouth Undergraduate Journal of Science. Retrieved from
http://dujs.dartmouth.edu/2011/02/the-physiology-of-stress-cortisol-and-the-
hypothalamic-pituitary-adrenal-axis/#.WL8tJBBREwU
Reynolds, A. R., & Walberg, H. J. (1992). A process model of mathematics achievement and
attitude. Journal of Research in Mathematics, 23(4), 306-328. doi: 10.2307/749308
Richards, G. & Smith, A. (2015). Caffeine consumption and self-assessed stress, anxiety, and
depression in secondary school children. J Psychopharmacol, 29(12), 1236–1247. doi:
10.1177/0269881115612404
Riegle-Crumb, C. (2007). More girls go to college: Academic and social factors behind the
female postsecondary advantage. Working paper. Accessed on 10 February 2017 from
http://theop.princeton.edu/workingpapers.html

117
Roberts, L. (2006). Amped up. Orlando Sentinel. Retrieved from
http://articles.orlandosentinel.com/2006-03-28/news/CAFFEINE_1_caffeine-pancake-
syrup-energy-drinks#
Roehrs, T. & Roth, T. (2001). Sleep, sleepiness, and alcohol use. Journal of the National
Institute on Alcohol Abuse and Alcoholism, 25(2), 101-109. Retrieved from
https://pubs.niaaa.nih.gov/publications/arh25-2/101-
109.htm?utm_source=io9+Newsletter&utm_campaign=6d29bbd775-UA-142218-
29&utm_medium=email
Roehrs, T. & Roth, T. (2008). Caffeine: Sleep and daytime sleepiness. Sleep Medicine Reviews,
12, 153-162. doi: 10.1016/j.smrv.2007.07.004
Ross, S.E., Niebling, B.C., Heckert, T.M. (1999). Sources of stress among college students.
College Student Journal, 33(2), 6
Saad, L. (2015). Americans’ coffee consumption is steady, few want to cut back. Gallup.
Retrieved from http://www.gallup.com/poll/184388/americans-coffee-consumption-
steady-few-cut-back.aspx
Schardt, D. (2015). Beware of these effects of caffeine on the body. Nutrition Action
Healthletter. Retrieved from http://www.nutritionaction.com/daily/caffeine-in-
food/beware-of-these-effects-of-caffeine-on-the-body/
118
Schardt, D. (2016). Can you get a caffeine buzz from chocolate cocoa: Chocolate vs. coffee-
flavored desserts. Nutrition Action Healthletter. Retrieved from
http://www.nutritionaction.com/daily/caffeine-in-food/how-much-caffeine-is-in-
chocolate/
Schneider, M.L., Vasconcellos, D.C., Dantas, G., Levandovski, R., Caumo, W., Allebrandt K.V.,
… Hidalgo, M.P. (2011). Morningness-eveningness, use of stimulants, and minor
psychiatric disorders among undergraduate students. Int J Psychol., 46(1), 18-23. doi:
10.1080/00207594.2010.513414
Smith, A. (2002). Effects of caffeine on human behavior. Food and Chemical Toxicology, 40,
1243-1255. http://dx.doi.org/10.1016/S0278-6915(02)00096-0
Smith, P.F., Smith, A., Miners, J., McNeil, J., & Proudfoot, A. (2000). The safety aspects of
dietary caffeine. Australia: Report from the Expert Working Group, 202-223. Retrieved
from
https://www.foodstandards.gov.au/publications/Documents/safety%20aspects%20of%20
dietary%20caffeine.pdf
Snel, J. & Lorist, M.M. (1998). Nicotine, Caffeine, and Social Drinking: Behavior and Brain
Function. Amsterdam, The Netherlands: Hardwood Academic Publishers.
Somogyi, L.P. (2010). Caffeine intake by the U.S. population. The Food and Drug
Administration.

119
Stanton, C.K. & Gray, R.H. (1995). Effects of Caffeine Consumption on Delayed Conception
Am J Epidemiol, 142(12), 1322-1329. https://doi.org/10.1093/oxfordjournals.aje.a117600
Steinmayr, R., Meißner, A., Weidinger, A.F., & Wirthwein, L. (2014). Academic achievement.
Oxford University Press. http://dx.doi.org/10.1093/obo/9780199756810-0108
Stern, K.N., Chait, L.D., & Johanson, C.E. (1989). Reinforcing and subjective effects of caffeine
in normal human volunteers. Psychopharmacology, 98(1), 81-88.
doi:10.1007/BF00442010
Svensson, E. Persson, L.O., &, Sjöberg L. (1980). Mood effects of diazepam and caffeine.
Psychopharmacology, 67(1), 73-80. doi:10.1007/BF00427598
Swift, C.G., & Tiplady, B. (1988). The effects of age on the response to caffeine.
Psychopharmacology, 94(1), 29-31. doi:10.1007/BF00735876
Tannous, M. & Kalash, Y.A. (2014). Prevalence of caffeinated-beverage consumption by
university students in North Lebanon. Public Health Research, 4(5), 173-178. doi:
10.5923/j.phr.20140405.04
Taylor, D.J., Clay, K.C., Bramoweth, A.D., Sethi, K., & Roane, B.M. (2011). Circadian
preference in college students: Relationships with physiological functioning and
academics. Chronobiology International, 28(6), 541–547. doi:
10.3109/07420528.2011.580870

120
ThinkGeek. (n.d.) Shower Shock Caffeinated Soap. Accessed on 5 Feb. 2015 from
http://www.thinkgeek.com/product/5a65/
Thoits, P.A. (1995) Stress, coping, and social support processes: Where are we? What next? J
Health Soc Behav, 35, 53–79.
Tieges, Z., Snel, J., Kok, A., Plat, N., & Ridderinkhof, R. (2007). Effects of caffeine on
anticipatory control processes: Evidence from a cued task-switch paradigm.
Psychopsychology, 44, 561-578. doi: 1 0.1111/j.1469-8986.2007.00534.x
Tran, J., Lertmaharit, S., & Lohsoonthorn, V., Pensuksan, W.C., Rattananupong, T., Tadesse,
M.G., …Williams, M.A. (2014). Daytime sleepiness, circadian preference, caffeine
consumption and use of other stimulants among Thai college students. J Public Health
Epidemiol. 8(6), 202-210. doi: 10.5897/JPHE2014.0620
Traylor, A. &Summers (n.d.). [Poster illustration of Caffeine consumption among college
students]. Texas Christian University. Retrieved from
www.srs.tcu.edu/previous_posters/Nutritional_Sciences/2012/89-Traylor-Dart.pdf
Tsai, L. & Li, S. (2004). Sleep patterns in college students: Gender and grade differences.
Journal of Psychosomatic Research, 56(2), 231-237. doi:10.1016/S0022-3999(03)00507-
5
Turner, S.E. & Bowen, W.G. (1999). Choice of major: The changing (unchanging) gender gap.
Industrial Labor Relations Review, 52(2), 289-313.

121
U.S. Food and Drug Administration. Consumer advice on pure powdered caffeine. (2015).
Retrieved from
http://www.fda.gov/food/recallsoutbreaksemergencies/safetyalertsadvisories/ucm405787.
htm
U.S. Food and Drug Administration. Serious concerns over alcoholic beverages with added
caffeine. (2010). Retrieved from
http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm233987.htm
U.S. Food and Drug Administration. (2016). Why isn’t the amount of caffeine a product
contains required on a food label? Retrieved from
http://www.fda.gov/AboutFDA/Transparency/Basics/ucm194317.htm
U.S. National Library of Medicine. (n.d.). HSDB: Caffeine. Toxicology Data Network. Retrieved
from https://toxnet.nlm.nih.gov/cgi-bin/sis/search2/f?./temp/~rq3kQ7:1
Uchida, S., Kadowaki-Horita, T.,& Kanda, T. (2014). Chapter eight: Effects of the adenosine
A2A receptor antagonist on cognitive dysfunction in Parkinson's disease. International
Review of Neurobiology, 119, 169-189. http://dx.doi.org/10.1016/B978-0-12-801022-
8.00008-8
UNEP Publications. (2003). OECD SIDS: Caffeine (CAS 58-08-2). Retrieved from
http://www.inchem.org/documents/sids/sids/CAFEINE.pdf

122
United States Department of Agriculture. (2015). 2015-2020 dietary guidelines for Americans,
8th edition. Retrieved from http://health.gov/dietaryguidelines/2015/guidelines/
University of Missouri-Kansas City. Student health and wellness. Accessed on 9 February 2017
from http://info.umkc.edu/studenthealth/health-education-services/
University of New Hampshire. Office of health education and promotion. Accessed on 9
February 2017 form https://www.unh.edu/health-services/ohep/educational-programs
Usman, A., Bhombal, S.T., Jawaid, A., & Zaki, S. (2015). Energy drink practices among medical
students of a private sector university of Karachi, Pakistan. J Pak Med Assoc., 65(9),
1005-1007
Wagner, K.D., Lorion, R.P., & Shipley, T.E. (1983) Insomnia and psychosocial crisis: Two
studies of Erikson's developmental theory. Journal of Consulting and Clinical
Psychology 51(4), 595-603
Walker, M.P. (2008). Cognitive consequences of sleep and sleep loss. Sleep Medicine, 9(1), s29-
s34. http://dx.doi.org/10.1016/S1389-9457(08)70014-5
Weinberg, B.A. (2013). Caffeinated: Developed by USA as “first strike rations” for our troops
and issued to Israeli soldiers. World of Caffeine. Retrieved from
http://worldofcaffeine.com/2013/01/31/caffeinated-gum-developed-by-usa-issued-to-
israeli-soldiers/

123
Weinberg, B.A. & Bealer, B.K. (2001). The world of caffeine: The science and culture of the
world’s most popular drug. New York, NY: Routledge.
Wetter, D.W. & Young, T.B. (1994). The relation between cigarette smoking and sleep
disturbance. Preventative Medicine, 23(3), 328-334.
http://dx.doi.org/10.1006/pmed.1994.1046
Whittier, A., Sanchez, S.E., Castaneda, B., Sanchez, E., Yanez, D., Williams, M.A. (2014).
Eveningness chronotypes, daytime sleepiness, caffeine consumption and use of other
stimulants among Peruvian university students. Journal of Caffeine Research, 4(1), 21-
27.
Whoriskey, P. (2015). A government panel said drinking coffee is harmless. Why that might be
wrong. The Washington Post. Retrieved from
https://www.washingtonpost.com/news/wonk/wp/2015/11/23/scientists-say-this-years-
big-announcement-on-coffee-was-wrong/?utm_term=.f0bfac002f86
Winston A.P., Hardwick E., & Jaberi N. (2005). Neuropsychiatric effects of caffeine. Advance in
Psychiatric Treatment, 11(6), 432-439. doi: 10.1192/apt.11.6.432
York, T.T., Gibson, C., & Rankin, S. (2015). Defining and measuring academic success.
Practical Assessment, Research & Evaluation, 20(5), 1-20. Retrieved from
http://eric.ed.gov/?id=EJ1059739
Zagat (2015). 2015 Coffee Survey Results. Retrieved from https://www.zagat.com/coffee-trends#

124
Zhang, Y., Coca, A., Casa, D.J., Antonio, J., Green, J.M., & Bishop. P. A. (2015). Caffeine and
diuresis during exercise: A meta-analysis. Journal of Science and Medicine in Sport,
18(2015), 569-574. http://dx.doi.org/10.1016/j.jsams.2014.07.017
Zunhammer, M., Eichhammer, P., & Busch, V. (2014). Sleep quality during exam stress: The
role of alcohol, caffeine and nicotine. PloS one, 9(10), e109490. doi:
10.1371/journal.pone.0109490