business case for refurbishment/replacement of theatres … · theatres 1 – 4 craigavon area...
TRANSCRIPT
Business Case for Refurbishment/Replacement ofTheatres 1 – 4 Craigavon Area Hospital
Theatres 1 – 4 Craigavon Area Hospital 2
Document History Document Name: Theatres 1-4 CAH
Status: FINAL - Approved by SMT 5 May 10
Version and Date: V1.0 30 Apr 10
Origin: Acute Planning SHSCT

Theatres 1 – 4 Craigavon Area Hospital 3
Contents
1 EXECUTIVE SUMMARY ..........................................................................6
1.1 Introduction........................................................................................6
1.2 Strategic Fit .......................................................................................6
1.3 Assessment of Need .........................................................................7
1.4 The Economic Case ..........................................................................8
1.5 Procurement ....................................................................................11
1.6 Project Management .......................................................................12
1.7 Project Timetable.............................................................................13
2 INTRODUCTION ....................................................................................14
2.1 Background .....................................................................................14
2.2 Current Situation..............................................................................15
2.3 Project Management Structure ........................................................16
2.4 Document Structure.........................................................................17
3 STRATEGIC CONTEXT .........................................................................18
4 ASSESSMENT OF NEED ......................................................................22
4.1 Condition of Existing Facilities .........................................................23
4.2 Clinical & Estates Risk.....................................................................28
4.3 Demand Assessment ......................................................................31
5 PATIENT PATHWAY..............................................................................45
6 OBJECTIVES AND CONSTRAINTS ......................................................47
6.1 Objectives........................................................................................47
6.2 Constraints ......................................................................................49
7 IDENTIFICATION & SHORTLISTING OF OPTIONS .............................50
7.1 Long List of Options.........................................................................50
8 NON FINANCIAL APPRAISAL OF SHORTLISTED OPTIONS ..............69
8.1 Benefit Criteria.................................................................................69
8.2 Scoring the Options .........................................................................73
9 FINANCIAL APPRAISAL OF SHORTLISTED OPTIONS .......................87
9.1 Capital Costs ...................................................................................88
9.2 Capital Charges...............................................................................88
9.3 Revenue Costs ................................................................................89
9.4 Economic Costs...............................................................................89
Theatres 1 – 4 Craigavon Area Hospital 4
10 ASSESSMENT OF RISK & SENSITIVITY ANALYSIS........................90
10.1 Risks................................................................................................91
10.2 Optimism Bias Adjustment...............................................................93
10.3 Sensitivity Analysis on Non Financial Benefits ................................95
11 IDENTIFICATION OF PREFERRED OPTION....................................97
12 AFFORDABILITY ANALYSIS..............................................................99
12.1 Capital funding requirements..............................................................99
12.2 Revenue Consequences ....................................................................99
13 EQUALITY & HUMAN RIGHTS CONSIDERATIONS .......................100
14 PROCUREMENT ..............................................................................101
15 PROJECT MANAGEMENT & POST PROJECT EVALUATION .......102
15.1 Project Management .....................................................................102
15.2 Post Project Evaluation..................................................................103
15.3 Benefits Realisation Plan...............................................................104
Theatres 1 – 4 Craigavon Area Hospital 5
Tables and Figures
Table 1: Surgical Services at Craigavon Area Hospital ............................................ 14
Table 2: Air Change Rates – Operating Theatres 1 – 4............................................ 24
Table 3: Risk Assessment – Operating Theatres 1 – 4............................................. 29
Table 4: Operating sessions (Theatres 1-5).............................................................. 32
Table 5: Utilisation of Operating Theatres – April to June 2009................................ 33
Table 6: Main Theatre Activity, Craigavon Area Hospital.......................................... 34
Table 7: Independent Sector Activity ........................................................................ 37
Table 8: SHSSB Projected Population Increase ....................................................... 40
Table 9: Surgical Finished Consultant Episodes & Daycases with a Procedure Projected................................................................................................................... 41
Table 10: Long List of Options .................................................................................. 51
Table 11: Short Listing of Options............................................................................. 58
Table 12: Scoring of Short Listed Options ................................................................ 74
Table 13: Capital Costs of Shortlisted Options (inclusive of MIPS inflation and Optimism Bias).......................................................................................................... 88
Table 14: Capital Charges Associated with Shortlisted Options ............................... 88
Table 15: Revenue Consequences of Shortlisted Options ....................................... 89
Table 16: Net Present Costs for Shortlisted Options ................................................ 89
Table 17: Risk Register............................................................................................. 90
Table 18: Summary of Optimism Bias Analysis ........................................................ 93
Table 19:Net Present Costs Adjusted for Optimism Bias.......................................... 94
Table 20: Effect on Ranking of Options by Adjustment of Weightings...................... 95
Table 21: Effect on Ranking of Options by Adjustment of Scores ............................ 96
Table 22: Comparison of Options ............................................................................. 97
Table 23: Affordability Analysis ................................................................................. 99
Table 24: Project Timetable for the Preferred Option ............................................. 103
Figure 1: Main Theatre Activity by Complexity.......................................................... 35
Figure 2: Surgical Finished Consultant Episodes & Daycases with a Procedure ..... 36
Figure 3: Population Projections for SHSSB 2008 - 2021......................................... 40
Figure 4: Forecast Finished Consultant Episodes (Surgical) .................................... 41

Theatres 1 – 4 Craigavon Area Hospital 6
11 EEXXEECCUUTTIIVVEE SSUUMMMMAARRYY 1.1 Introduction
Craigavon Area Hospital is the larger of the Southern Health and Social Care Trust’s two acute hospitals, providing a range of acute services (both emergency and elective) to the catchment population. The hospital was opened some 27 years ago and much of the existing accommodation is still in use and is no longer fit for purpose. There are five main theatres, two trauma and orthopaedic theatres and a day surgery unit with one theatre and an endoscopy room.
The condition of the main theatres has been identified as one of the highest risks to patient safety in terms of infection control issues and also because of the likelihood of major failure due to mechanical and electrical services issues. A business case for the replacement of Theatre 5, the worst of the five main theatres, was approved by the DHSSPS in May 2007 and the new theatre was constructed and has been operational since May 2009.
This business case is for the urgent replacement/upgrading of the remaining four main theatres and support accommodation.
1.2 Strategic Fit
Craigavon Area Hospital was one of the nine acute hospitals identified in Developing Better Services (reducing the number of acute hospitals from 13), it is important that facilities as fundamental as operating theatres are of a standard consistent with the vision set out by the Acute Hospital Review Group. The proposed refurbishment/ replacement of Theatres 1 – 4 will enable the Trust to provide care to patients in line with the broad principles described in Developing Better Services.
The Trust is committed to achieving the targets set out in Priorities for Action and the provision of a modern theatre suite which complies with current estates standards is a fundamental requirement to enable the delivery of acute surgery. This project will therefore be critical to supporting the provision of a safe, timely acute hospital service which meets the targets set out in the Public Service Agreement and ministerial framework.
This project will allow Craigavon Area Hospital, as one of the nine acute hospitals in Northern Ireland, to meet its clinical responsibilities to the level required. Furthermore, improved facilities will allow the Trust to maintain and enhance the level of expertise and experience of professional staff.

Theatres 1 – 4 Craigavon Area Hospital 7
1.3 Assessment of Need
An assessment of need highlights the deficiencies with the current theatre accommodation and clearly demonstrates a requirement to retain five main theatres at Craigavon Area Hospital.
Condition of Existing Facilities
! The theatre ventilation plant (including design configuration and air change rate) does not meet Departmental standards;
! Theatre design does not meet Departmental standards in terms of space, layout or quality of finishes;
! There are significant electrical services issues including only one source of electrical supply; emergency back-up is fully loaded and the distribution network contravenes standards.
Demand Assessment
! The number of allocated theatre sessions is currently 48 per week out of an available 50;
! Main theatre activity has increased over the last three years, particularly in terms of the numbers of more complex surgery. The number of surgical episodes with a procedure carried out has increased from 6,331 in 2005/06 to 9,569 in 2008/09, an increase of 51%;
! Whilst the Trust is currently meeting the Priorities for Action target of 13 weeks for inpatient and daycase treatment, this has required significant use of the independent sector to provide additional capacity. In 2008/09 826 inpatient and 3,005 day case episodes were provided by the independent sector. It is the Regional Health and Social Care Board’s (RHSCB) intent that the use of independent sector should be minimised. In the last quarter of 2009/10 the Trust made significant reductions in the use of independent sector capacity. Only 193 day cases were treated in the independent sector. This achievement resulted from the maximisation of theatre capacity, flexible use of theatres and the provision of sessions in the evening and at the weekend;
! Planned service developments will give rise to the need to increase theatre sessions further, but these can be accommodated within the existing theatre complement;
! Population demographics show a 23.8% increase in the overall number of people in the Southern area by 2021 and more significantly an increase of 43.7% in those aged 65 years and over. This increase will have a considerable impact on the requirement for theatre capacity because a large proportion of inpatient episodes are attributable to the 65+ age group;
Theatres 1 – 4 Craigavon Area Hospital 8
! Projected inpatient surgical activity is forecast to increase to 12,024 finished consultant episodes by 2020/21, a substantial increase of 25% between 2008/09 and 2020/21.
1.4 The Economic Case
A long list of ten options was identified and explored by the Trust. This long list of options was sifted using agreed objectives and constraints to give a short list of five options.
The key objectives are as follows:
! To deliver operating theatre accommodation by 2012 to DHSSPS standards;
! To provide a reliable theatre environment for patients and staff to ensure consistent levels of theatre capacity;
! To provide accommodation with the flexibility/capacity to accommodate the level of emergency and complex procedures as emerging from the presenting population on completion of the project (currently 20% of procedures undertaken in the main theatre complex);
! To ensure there are no unscheduled session cancellations during the period of construction and current capacity is maintained. To minimise the disruption to theatre and other support services;
! To achieve a high satisfaction rating from theatre staff;
! To align with the Trust’s strategic direction and contribute to the development of services within the Trust.
The five short listed options are described in the paragraphs below.
The Southern Trust is currently leasing two volumetric modular theatres with support accommodation. These theatres will be vacated in May 2010 when the new trauma and orthopaedic facility has been commissioned. As the replacement of main theatres 1-4 will be a temporary solution until major redevelopment of the Craigavon Area Hospital site a number of the options considered include the purchase and upgrade of these two volumetric theatres.
Option 2 - Do Minimum – Minimal refurbishment of existing 4 theatres, replacing the ventilation system and upgrading the electrical supply.
This option proposes to conduct the minimum work required to the existing theatres to meet some of the requirements of the Department of Health building guidance. This would involve replacement of the ventilation system and upgrade of the electricity supply. Decant of two theatres at a time and also decant of recovery ward would be required for the duration of the works.
Theatres 1 – 4 Craigavon Area Hospital 9
Option 3 - Purchase 2 volumetric theatres. Extend theatre block into a courtyard & refurbish to provide 2 theatres, new recovery, upgraded staff changing and support accommodation.
This option involves purchasing the 2 volumetric theatres. Two theatres and recovery facilities which comply with the Department of Health building guidance would be provided by building an extension in an adjacent courtyard and refurbishing within the existing main theatre suite. The staff changing facilities would also be upgraded and additional storage would be provided.
Option 7 - Purchase 2 volumetric theatres and construct 2 theatres. Refurbish existing theatre block to provide new recovery, upgraded staff changing and support accommodation.
This option involves purchasing the 2 volumetric theatres. Two theatres and recovery ward which fully comply with the Department of Health building guidance would be constructed. Some minor re-alignment of the hospital ring road would be required. The staff changing facilities would also be upgraded and additional storage would be provided.
Option 8 - Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and support accommodation.
This option involves purchasing the 2 volumetric theatres. A third theatre would be constructed. The fourth theatre would be provided by refurbishing within the existing main theatre building. A new recovery ward, staff changing facilities, storage etc would be provided by refurbishing within the existing main theatre area.
Option 9 - Construct 4 new theatres and new recovery ward. Refurbish existing theatre block to provide upgraded staff changing and additional support accommodation.
This option involves the construction of four theatres and new recovery ward which fully comply with the Department of Health building guidance. The proposed site is currently occupied by the histocytology laboratory and laboratory office accommodation. These 2 units would be re-provided prior to construction commencing. The staff changing facilities would also be upgraded and additional storage would be provided.
Theatres 1 – 4 Craigavon Area Hospital 10
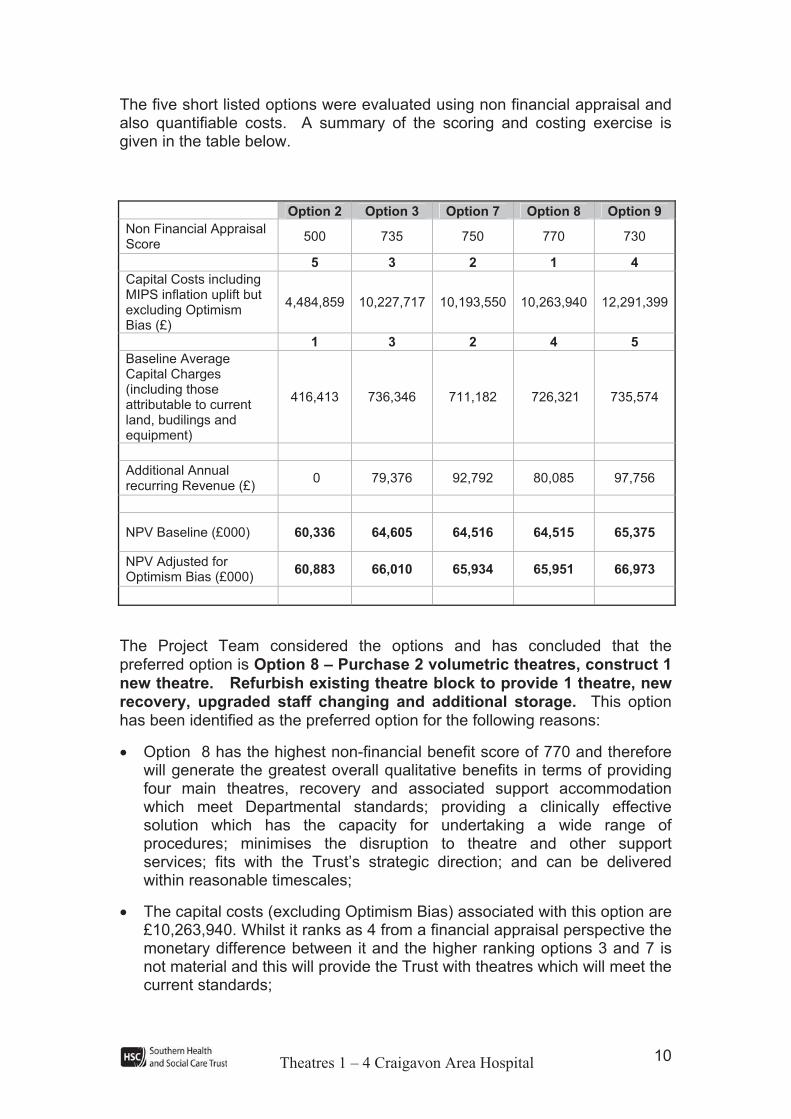
The five short listed options were evaluated using non financial appraisal and also quantifiable costs. A summary of the scoring and costing exercise is given in the table below.
Option 2 Option 3 Option 7 Option 8 Option 9
Non Financial Appraisal Score
500 735 750 770 730
5 3 2 1 4
Capital Costs including MIPS inflation uplift but excluding Optimism Bias (£)
4,484,859 10,227,717 10,193,550 10,263,940 12,291,399
1 3 2 4 5
Baseline Average Capital Charges (including those attributable to current land, budilings and equipment)
416,413 736,346 711,182 726,321 735,574
Additional Annual recurring Revenue (£)
0 79,376 92,792 80,085 97,756
NPV Baseline (£000) 60,336 64,605 64,516 64,515 65,375
NPV Adjusted for Optimism Bias (£000)
60,883 66,010 65,934 65,951 66,973
The Project Team considered the options and has concluded that the preferred option is Option 8 – Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage. This option has been identified as the preferred option for the following reasons:
! Option 8 has the highest non-financial benefit score of 770 and therefore will generate the greatest overall qualitative benefits in terms of providing four main theatres, recovery and associated support accommodation which meet Departmental standards; providing a clinically effective solution which has the capacity for undertaking a wide range of procedures; minimises the disruption to theatre and other support services; fits with the Trust’s strategic direction; and can be delivered within reasonable timescales;
! The capital costs (excluding Optimism Bias) associated with this option are £10,263,940. Whilst it ranks as 4 from a financial appraisal perspective the monetary difference between it and the higher ranking options 3 and 7 is not material and this will provide the Trust with theatres which will meet the current standards;
Theatres 1 – 4 Craigavon Area Hospital 11
! Annual capital charges associated with Option 8 are £726,321. This is less than the capital charges associated with Options 3 and 9 and is not materially higher than those for Option 7;
! Recurring revenue costs associated with Option 8 are lower than those indicated for Option 7 and Option 9 and are not materially different to those for Option 3;
! Net Present Value of Option 8 is £64,515k (risk adjusted NPV £65,951k), given that Option 8 achieved the highest non-financial benefit score this offers the best benefit for investment required.
1.5 Procurement
In line with Health Estates recommendations on best value for money in procurement the Trust has entered into Performance Related Partnering (PRP) frameworks with a design team and a contractor for the design and construction of acute hospital facilities. The appointed Design Team and Contractor are undertaking two projects –
1. Construction of a new trauma and orthopaedics facility at Craigavon Area Hospital. This project is well underway and the building was handed over for Trust commissioning in March 2010;
2. Extension and refurbishment of maternity and neonatal facilities at Craigavon Area Hospital – works commenced in July 2009 and construction is scheduled for completion in May 2010. The Trust is satisfied with the performance of both the design team and the contractor and proposes to re-appoint both for this project.
Theatres 1 – 4 Craigavon Area Hospital 12
1.6 Project Management
It is proposed to implement the organisation and management of this scheme in accordance with the guidance contained in the Capital Investment Manual entitled ‘Project Organisation and Capital Investment Manual: Management of Construction Projects’ issued by the DHSSPS. Relevant expertise and experience will be required from Trust staff and from Health Estates Investment Group.
The proposed project structure is summarised as follows:
Theatres 1 – 4 Craigavon Area Hospital 13
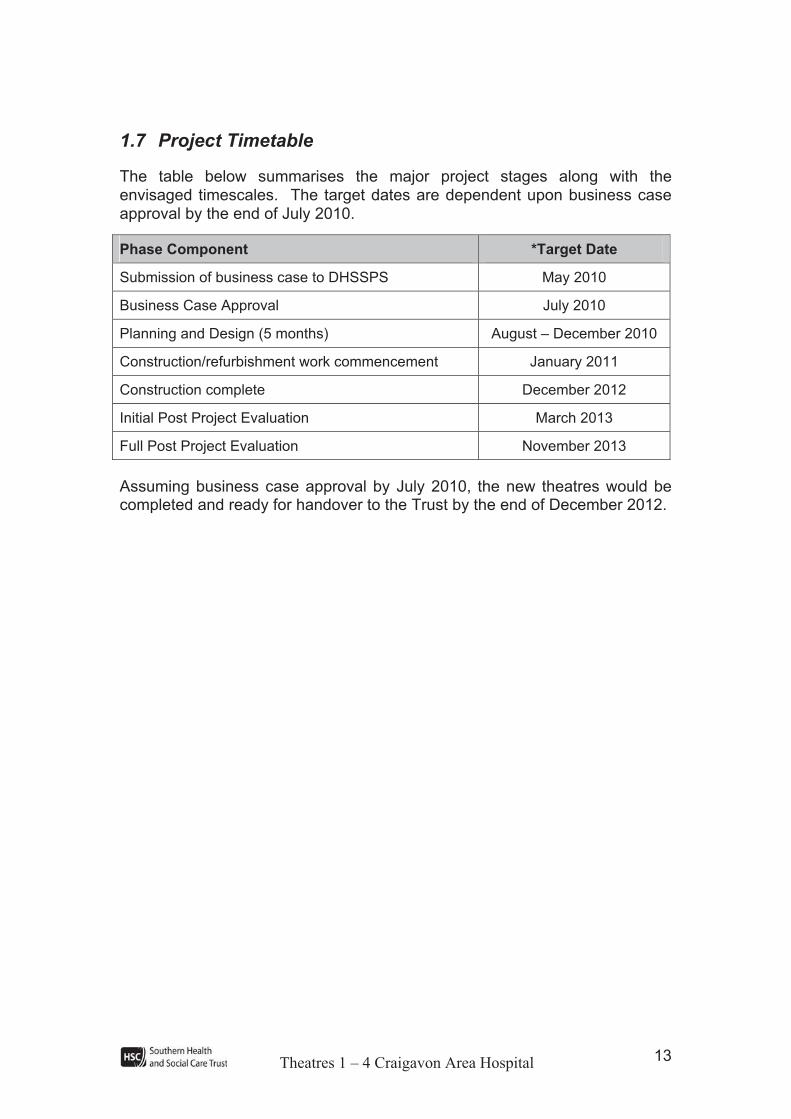
1.7 Project Timetable
The table below summarises the major project stages along with the envisaged timescales. The target dates are dependent upon business case approval by the end of July 2010.
Phase Component *Target Date
Submission of business case to DHSSPS May 2010
Business Case Approval July 2010
Planning and Design (5 months) August – December 2010
Construction/refurbishment work commencement January 2011
Construction complete December 2012
Initial Post Project Evaluation March 2013
Full Post Project Evaluation November 2013
Assuming business case approval by July 2010, the new theatres would be completed and ready for handover to the Trust by the end of December 2012.
Theatres 1 – 4 Craigavon Area Hospital 14
2 INTRODUCTION 2.1 Background
The Southern Health and Social Care Trust (SHSCT) became operational on 1 April 2007 following the amalgamation of Craigavon Area Hospital Group, Craigavon and Banbridge Community, Newry and Mourne and Armagh and Dungannon Health and Social Services Trusts. The Trust is responsible for the delivery of high quality health and social care to a resident population of 348,000, employs approximately 12,000 staff and has an annual budget in the region of £400m. The Trust delivers acute hospital care from two main sites - Craigavon Area Hospital (453 beds) and Daisy Hill Hospital (260 beds). Day surgery, outpatient and diagnostic services are also delivered at South Tyrone Hospital.
This business case focuses exclusively on the main theatre suite on the Craigavon Area Hospital (CAH) site.
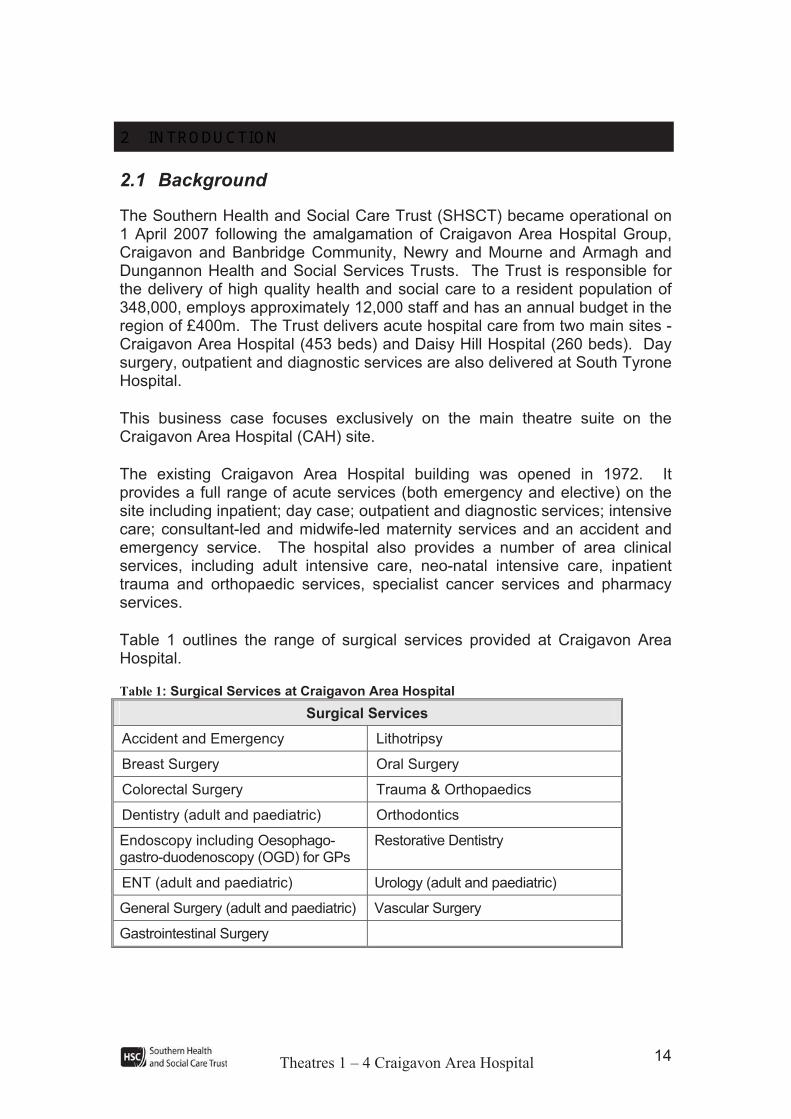
The existing Craigavon Area Hospital building was opened in 1972. It provides a full range of acute services (both emergency and elective) on the site including inpatient; day case; outpatient and diagnostic services; intensive care; consultant-led and midwife-led maternity services and an accident and emergency service. The hospital also provides a number of area clinical services, including adult intensive care, neo-natal intensive care, inpatient trauma and orthopaedic services, specialist cancer services and pharmacy services.
Table 1 outlines the range of surgical services provided at Craigavon Area Hospital.
Table 1: Surgical Services at Craigavon Area Hospital
Surgical Services
Accident and Emergency Lithotripsy
Breast Surgery Oral Surgery
Colorectal Surgery Trauma & Orthopaedics
Dentistry (adult and paediatric) Orthodontics
Endoscopy including Oesophago-gastro-duodenoscopy (OGD) for GPs
Restorative Dentistry
ENT (adult and paediatric) Urology (adult and paediatric)
General Surgery (adult and paediatric) Vascular Surgery
Gastrointestinal Surgery
Theatres 1 – 4 Craigavon Area Hospital 15
2.2 Current Situation
Craigavon Hospital originally had 4 theatres within its theatre suite, however due to increased demand, an endoscopy room was reconfigured in 1991 into a fifth theatre. In 2005 the Trust became concerned about the condition of the theatres and the Health Estates Agency was requested to conduct a survey assessment of the facilities. In the report the Health Estates Agency highlighted a number of areas where the conditions of the theatres were not compliant with current DHSSPS standards. The key problems were grouped as follows:
! Architectural – theatre design does not comply with space standards, layout of rooms in the suites and the quality of finishes;
! Mechanical Services – theatre ventilation plant does not comply with standards in respect of air change rates. For example, air change rates in the sterile preparation areas are approximately 24 ach (air changes per hour) compared to a requirement for 37 changes per hour; and
! Electrical Services – there is an over-dependence on a single source of electricity, the supply to theatres is fully loaded and the power distribution network throughout the theatres contravenes current standards.
Following receipt of the Health Estates report in 2005, the Trust implemented a number of measures to reduce the risks identified above. However these measures could at best be described as short term in nature until a longer term solution could be found.
This business case focuses specifically on the refurbishment/ replacement of Theatres 1 – 4. A separate business case was submitted to examine the options around the replacement of Theatre 5. This business case was approved in May 2007 and the new theatre was constructed and has been operational since May 2009.
In October 2006, the Trust submitted a business case for the refurbishment/ replacement of Theatres 1 – 4, however this previous business case also included provision for a sixth theatre. Following submission of the business case in October 2006, the Trust recognised the tightening funding environment and re-examined their capital priorities. This resulted in a revision to the options being considered and the proposal for a sixth theatre was removed.

Theatres 1 – 4 Craigavon Area Hospital 16
Wider Context
Craigavon Area Hospital Group Trust submitted an Outline Business Case for major redevelopment of the Craigavon Area Hospital site, in August 2005. This was revised to incorporate comments from Departmental advisors and the Trust’s responses to those comments, and it was re-submitted in August 2006. The business case proposed the construction of a new hospital on a different part of the Craigavon Area Hospital site, to meet the acute health and social care needs of the catchment population over the longer term.
In May 2008 the Minister commissioned Health Estates Agency to lead an urgent review of the capital priorities in health, social care and public safety. The Trust submitted a high level paper setting out its capital priorities over the 10 years of the current ISNI planning period (2008/09 – 2017/18). These priorities included major redevelopment of the Craigavon Area Hospital site in 3 phases, with the first phase identified as the Trust’s highest priority for capital investment. The first phase includes the replacement of theatres.
However the deficiencies with the main theatre suite highlighted by Health Estates Agency must be addressed as a matter of urgency. The Trust is therefore progressing this business case as an interim scheme to urgently address the problems in the main theatre suite.
2.3 Project Management Structure
This business case has been developed by a multi-disciplinary Project Board under the auspices of robust and fully inclusive project management structures. The organisational structure for the project and the roles and responsibilities of the individuals and groups involved comply with the requirements of the Capital Investment Manual. The structure is illustrated in Appendix 1, along with the membership of the Project Board and the Project Team.
Theatres 1 – 4 Craigavon Area Hospital 17
2.4 Document Structure
The business case has been structured to provide a clear logic for the proposed development and to explain the financial and non-financial implications. It also sets out the risks associated with the project.
The main document is set out in 14 Chapters.
In addition supporting information is given in 15 appendices.
Chapter 1 Executive Summary (Trust Board Report)
Chapter 2 Introduction
Chapter 3 Strategic Context
Chapter 4 Assessment of Need
Chapter 5 Patient Pathway
Chapter 6 Objectives & Constraints
Chapter 7 Identification and Short Listing of Options
Chapter 8 Non Financial Appraisal of Options
Chapter 9 Financial Appraisal of Options
Chapter 10 Assessment of Risk & Sensitivity Analysis
Chapter 11 Identification of the Preferred Option
Chapter 12 Affordability Analysis
Chapter 13 Equality & Human Rights Considerations
Chapter 14 Procurement
Chapter 15 Project Management & Post Project Evaluation

Theatres 1 – 4 Craigavon Area Hospital 18
3 STRATEGIC CONTEXT Introduction
It is important that all Government expenditure is aligned with the relevant national and local strategic objectives. This section of the report therefore summarises the strategic context as set out in:
! Government/ Departmental Strategies;
! Southern Health and Social Services Board Strategy; and
! Southern Health and Social Care Trust (SHSCT) Principles and Strategic Development Plan.
Government and Departmental Strategies/ Policies
In recent years Government have issued a number of policy documents which impact on the refurbishment/replacement of the operating theatres in Craigavon Area Hospital. These are considered in turn below.
Developing Better Services (DBS)
The overall aim of ‘Developing Better Services’ is to put in place: “a new modern and more effective hospital service … that is set up and resourced to meet the needs of the expected number of patients it serves.”
To achieve this, nine acute hospitals would be developed across Northern Ireland that would provide a full range of care services. Importantly, Craigavon Area Hospital was one of the nine hospitals identified as a provider of acute services.
The report also highlighted that “acute services must be refocused to achieve the concentration of expertise and experience required to deliver the highest possible levels of clinical care.”
This project should therefore allow CAH, as one of the nine acute hospitals in Northern Ireland, to meet its clinical responsibilities to the level required. Furthermore, improved facilities should also allow the Trust to maintain and enhance the level of expertise and experience of professional staff.
Theatres 1 – 4 Craigavon Area Hospital 19
DHSSPS – Acute Hospital Review Group
The Acute Hospital Review Group established by the Department in September 2000 set out in its vision to secure hospital services that were:
! High quality, which through clinical governance, involving audit and quality assurance processes, ensure the best outcome for patients;
! Accessible to everyone, taking full account of the urgency, nature and frequency of patients’ needs;
! Patient-centred and planned to ensure the best balance of safety, quality and convenience for patients;
! Cost-effective and offering value for money;
! Professional, delivered by staff with the right skills and experience, working under appropriate conditions, and in a well-equipped environment; and
! Integrated, as part of a seamless system including primary and secondary care allowing treatment care plans to be developed for individual patients.
As Craigavon Area Hospital (CAH) is one of the nine acute hospitals identified in DBS (reducing the number of acute hospitals from 13), it is important that facilities as fundamental as operating theatres are of a standard consistent with the vision set out by the Acute Hospital Review Group. An acute hospital is set up to deal with many types of disease and injury and includes an accident and emergency department to deal with immediate threats to health. It is typically the major health care facility in its area, and provides intensive and long-term care and specialised facilities for surgery. Therefore the proposed refurbishment/ replacement of Theatres 1 – 4 will enable the Trust to provide care to patients in line with these broad principles.
Southern Health and Social Services Board Strategy
Profile of Future Services
In January 2004, the SHSSB published its ‘Profile of Future Services within the SHSSB’ in response to DBS which outlined the following priority for CAH.
“… the reconfiguration of services across Northern Ireland and the move to make Lagan Valley into a local hospital, along with changes to Tyrone County Hospital, will mean that residents in these localities may in future be admitted for both emergency and planned surgery to Craigavon Area Hospital. As a result, this will be the key hospital for the provision of health and social services to people in a greater number of areas outside Craigavon.”
Theatres 1 – 4 Craigavon Area Hospital 20
The strategic direction outlined above indicates a more prominent role for CAH and emphasises the need for investment in theatre estate to ensure that the hospital is well positioned to manage the additional demands on its service.
Legacy CAHGT Strategic Development Plan
The legacy CAHGT Strategic Development Plan was completed to address the weaknesses in the existing hospital facilities and infrastructure. The plan focuses primarily on the redevelopment of the entire CAH site which it recognises will not be complete until at least 2019/20. As a result interim schemes were proposed to ensure that the Trust could address the following strategic goals and priorities:
! Manage significant backlog maintenance issues and outdated accommodation issues in a facility over 3 decades old
! Ensure compliance with current statutes and regulations;
! Facilitate the provision of more efficient healthcare that meets patient expectations;
! Provide the capacity necessary to meet both current and future healthcare delivery requirements; and
! Improve the environment for patients, staff and the general public.
Given the condition of the existing theatre suite, it is recognised that replacement of these theatres is required to improve the facilities within which patients are treated as part of the interim scheme.
Trust Delivery Plan 2009/10
The Trust Delivery Plan gives a commitment to improving the quality of life of the local population. The Trust’s strategic direction for the development of services has a number of key themes which include:
! Providing quality of care across all dimensions – safety, timeliness, effectiveness, efficiency, equality and patient-centredness.
This project will be critical to supporting the provision of a safe, timely acute hospital service which meets the targets set out in the Public Service Agreement and ministerial framework.

Theatres 1 – 4 Craigavon Area Hospital 21
Conclusion on Strategic Context
The strategic direction of Government and the SHSSB is to provide health services which are:
! Patient-centred;
! Professional and delivered under appropriate conditions;
! High quality;
! Accessible;
! Cost effective; and
! Integrated.
Furthermore, CAH is one of nine acute hospitals for Northern Ireland identified in DBS which is likely to result in increased levels of demand which would have previously been taken by Tyrone County and Lagan Valley. Therefore investment in the theatre infrastructure at Craigavon is consistent with the broad strategic direction outlined in DBS.
Finally, improved facilities should also assist the Trust in maintaining and enhancing the quality of service it provides and improving the expertise and experience of its professional staff.

Theatres 1 – 4 Craigavon Area Hospital 22
4 ASSESSMENT OF NEED Introduction
This section of the appraisal considers the ‘need’ for refurbishment/ replacement of Theatres 1 – 4. The assessment considers the following factors:
! Condition of existing facilities – Health Estates completed a conditions survey of Theatres 1 – 4 in July 2005 and the results indicated a significant shortfall when compared against Departmental requirements/ standards;
! Clinical/ Estates Risk – a risk assessment was undertaken by the legacy CAHGT in terms of the relationship between the condition of facilities and the risk of infection;
! Demand assessment – through available statistical information on the following areas:
- Theatre activity and utilisation;
- Forecast analysis of usage;
- The management of waiting lists;
- Planned service developments; and
- Demographic changes.

Theatres 1 – 4 Craigavon Area Hospital 23
4.1 Condition of Existing Facilities
In developing the Outline Business Case for the redevelopment of the entire hospital site, the Trust identified the need for a number of interim schemes which would be required as a matter of urgency to ensure uninterrupted service delivery until the completion of the new facilities within the site wide development. Refurbishment of the Theatre Suite was identified as one such scheme and as a result the Trust, in partnership with the Health Estates Agency, commissioned the following reports and investigations:
! Health Estates Agency Conditions Report – conducted in July 2005 (this is attached in Appendix 2);
! Independent external investigation relating to infection control – conducted in August 2005 (this is attached in Appendix 3).
These reports/ investigations are now discussed in turn.
Health Estates Agency Conditions Report (July 2005)
In respect of Theatre 1 – 4 the Health Estates Agency Conditions Report examined three areas:
! Mechanical Services;
! Architectural Non-Compliance; and
! Electrical Services.
Taking these areas in turn, the report highlighted the following issues in respect of the Mechanical Services of Theatres 1 – 4:
! The Theatre Ventilation Plant did not comply with current standards as per the DHSSPS Health Technical Memorandum (HTM) 2025. Air change rates in the theatres and sterile preparation rooms were significantly below Hospital Infection Society Guidance;
! Climate Control is limited to heating only (ie. there is no cooling or humidity control); and
! Building services are not fully compliant with the requirements for the control of legionella.
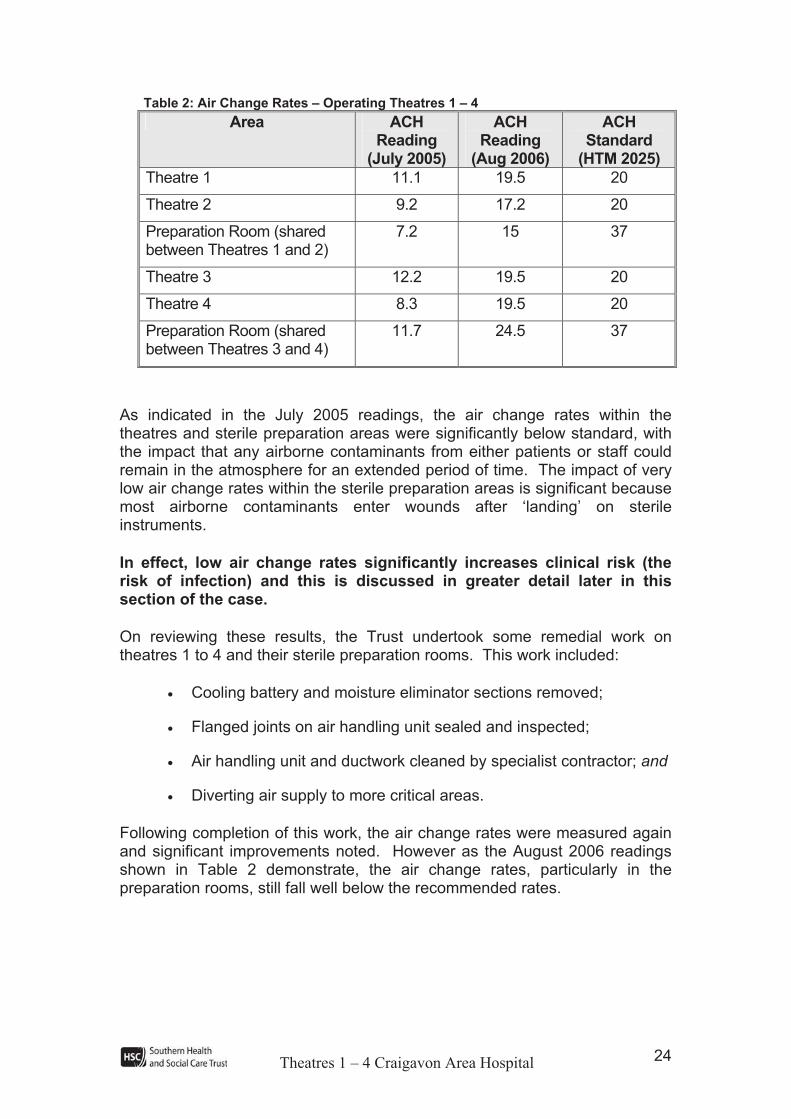
Table 2 sets out the air change rates, measured in air changes per hour (ACH), for theatres 1 – 4 and the adjacent sterile preparation rooms. This is compared to the standard as detailed in HTM 2025.
Theatres 1 – 4 Craigavon Area Hospital 24
Table 2: Air Change Rates – Operating Theatres 1 – 4
Area ACHReading
(July 2005)
ACHReading
(Aug 2006)
ACHStandard
(HTM 2025)
Theatre 1 11.1 19.5 20
Theatre 2 9.2 17.2 20
Preparation Room (shared between Theatres 1 and 2)
7.2 15 37
Theatre 3 12.2 19.5 20
Theatre 4 8.3 19.5 20
Preparation Room (shared between Theatres 3 and 4)
11.7 24.5 37
As indicated in the July 2005 readings, the air change rates within the theatres and sterile preparation areas were significantly below standard, with the impact that any airborne contaminants from either patients or staff could remain in the atmosphere for an extended period of time. The impact of very low air change rates within the sterile preparation areas is significant because most airborne contaminants enter wounds after ‘landing’ on sterile instruments.
In effect, low air change rates significantly increases clinical risk (the risk of infection) and this is discussed in greater detail later in this section of the case.
On reviewing these results, the Trust undertook some remedial work on theatres 1 to 4 and their sterile preparation rooms. This work included:
! Cooling battery and moisture eliminator sections removed;
! Flanged joints on air handling unit sealed and inspected;
! Air handling unit and ductwork cleaned by specialist contractor; and
! Diverting air supply to more critical areas.
Following completion of this work, the air change rates were measured again and significant improvements noted. However as the August 2006 readings shown in Table 2 demonstrate, the air change rates, particularly in the preparation rooms, still fall well below the recommended rates.
Theatres 1 – 4 Craigavon Area Hospital 25
In addition to the above analysis, the following points have been identified to address the problems with the control of legionella. These problems are due to:
! The coldwater storage turnover times.
! The design and condition of the existing Hot Water System.
! Poor temperature monitoring of both hot and cold water systems.
The installation of a new ventilation system is therefore required to resolve these problems. However the HEA has identified that to replace the ventilation system would cause significant disruption to all areas requiring mechanical ventilation as ceilings in these areas would have to be removed to accommodate new ductwork dampers and controls.
The Health Estates Agency also reported on Architectural Non-Compliance.Theatres 1 – 4 are approximately 40 sq metres, against a standard size of 55 sq metres.
Key issues highlighted are discussed below:
! Current theatre design does not meet the Department’s standards as per Health Building Note (HBN) 26 in terms of space, the layout of rooms or quality of finishes (which makes it more difficult to clean the theatre). This impacts on the ability of staff to undertake high-risk/ complex surgery because of deficiencies in theatre space; and
! These deficiencies have a direct impact on control of infection.
The final area examined by the Health Estates Agency was on ElectricalServices. These issues relate to the entire Theatre Suite and the key issues are discussed in turn below:
! Incoming electrical supply to the theatres is via one single source;
! The emergency back-up supply to the theatres is fully loaded;
! The power distribution network throughout the theatre suite contravenes current standards;
! Theatre lighting is, in places, inadequate and non-compliant; and
! The report also highlighted non-compliances for theatre control panel; use of lasers/x-rays; IT and telephone systems; security systems, and; fire detection and alarm system.

Theatres 1 – 4 Craigavon Area Hospital 26
In terms of the proposed enhancements to the electrical system, the current electrical installation provides no electrical safety features as required by modern theatres. Therefore, when proposing to refurbish/ renew existing theatres, electrical safety features should be incorporated as part of any improvement works. Furthermore, HEA has advised that simply installing an additional source and extra standby is not sufficient with regard to the life safety of the patient; upgrading of the entire electrical infrastructure in the Theatre Suite is strongly recommended.
On the basis of the mechanical, architectural and electrical services findings, the Health Estates Agency report recommends that in respect of Theatres 1 to 4, “the 33 year old theatres are in need of major refurbishment in order to comply with current standards”.
Independent external investigation relating to infection control (Hoffman Report)
In addition to the ventilation investigation, by the Health Estates Agency, an independent investigation was undertaken to assess infection control across the entire Theatre Suite. The findings of the investigation are set out below:
! Air change rates were not satisfactory “from an infection control perspective … posing a ‘high’ risk of infection”;
! A higher than expected proportion of fungi were present suggesting the ingress of unfiltered air; and
! Air handling units did not comply with HTM2025 (as noted in the Health Estates Agency Report).
On the basis of these findings, the following recommendations were made:
! The ventilation supply to all theatres needs to be increased to meet the current minimum levels;
! There is substantial ingress of unfiltered air in theatres, entering via the air handling unit. In the short-term this may be decreased by inspection of the integrity of the air handling units and sealing them wherever possible. However replacement of the air handling units (to HTM 2025 standards) is required in order to address design and condition deficiencies;
! Each change to, or modification of, the air supply should be verified by assessment of engineering parameters;
! The present shared preparation configuration is unsatisfactory and there should be modifications made.
Whilst the remedial work has increased air flow throughout theatres 1 and 2, and improved the availability of ‘fresh’ air, there is still no provision for humidity control or cooling.

Theatres 1 – 4 Craigavon Area Hospital 27
As previously noted by the Departmental economists, the HEA report states that the Theatres require refurbishment and the independent external investigation states that the air handling units need replaced. Neither report stated that the existing theatres need replaced. In this regard it is important to note that neither were commissioned to look at the preferred option in relation to risk, cost and continuity of the surgical service. This business case considers the options to resolve the problems highlighted in the HEA report, of which replacement of the theatres is only one option.

Theatres 1 – 4 Craigavon Area Hospital 28
4.2 Clinical & Estates Risk
As noted earlier in Section 4.1 (Table 2), the Air Change Rates, generated by the Theatre Ventilation system, across the 4 theatres were significantly below Departmental standards (HTM 2025). The low air change rates have the impact of significantly increasing clinical risk (ie. increasing the risk of infection).
The Hoffman report (see Appendix 3) sets out in detail the importance of ventilation in terms of infection control, but a summary is provided below. The purpose of operating theatre ventilation is to prevent airborne microbes from entering surgical wounds. This is achieved in ventilated theatres by two approaches:
1) Preventing ingress of contaminated air from other areas in the hospital or theatre suite; and
2) Diluting airborne contamination in critical areas of the theatre suite.
The first approach is accomplished by controlling the direction of airflow between areas of the operating suite and the second by supplying sufficient clean air to critical areas, such that airborne contamination generated in these areas is diluted in turbulent airflow and carried to less critical areas. Most of this airborne contamination comprises micro-organisms dispersed from the skin of people moving around in the theatre.
Airborne contamination can enter the wound by two main routes: it can fall directly into a wound or it can fall onto exposed instruments that will later be used in the wound. The relative proportions of airborne contamination that enter a wound by each of these routes will vary according to:
! the size of the wound;
! the time it is open;
! the area of the exposed instruments; and
! the time the instruments are exposed.
Hoffman has indicated that it is generally considered that airborne contamination of the wound via instruments is more important than the direct route. For this reason, preparation rooms used for instrument layup should be at higher pressure than the operating theatre and should have high air change rates.
Theatres 1 – 4 Craigavon Area Hospital 29
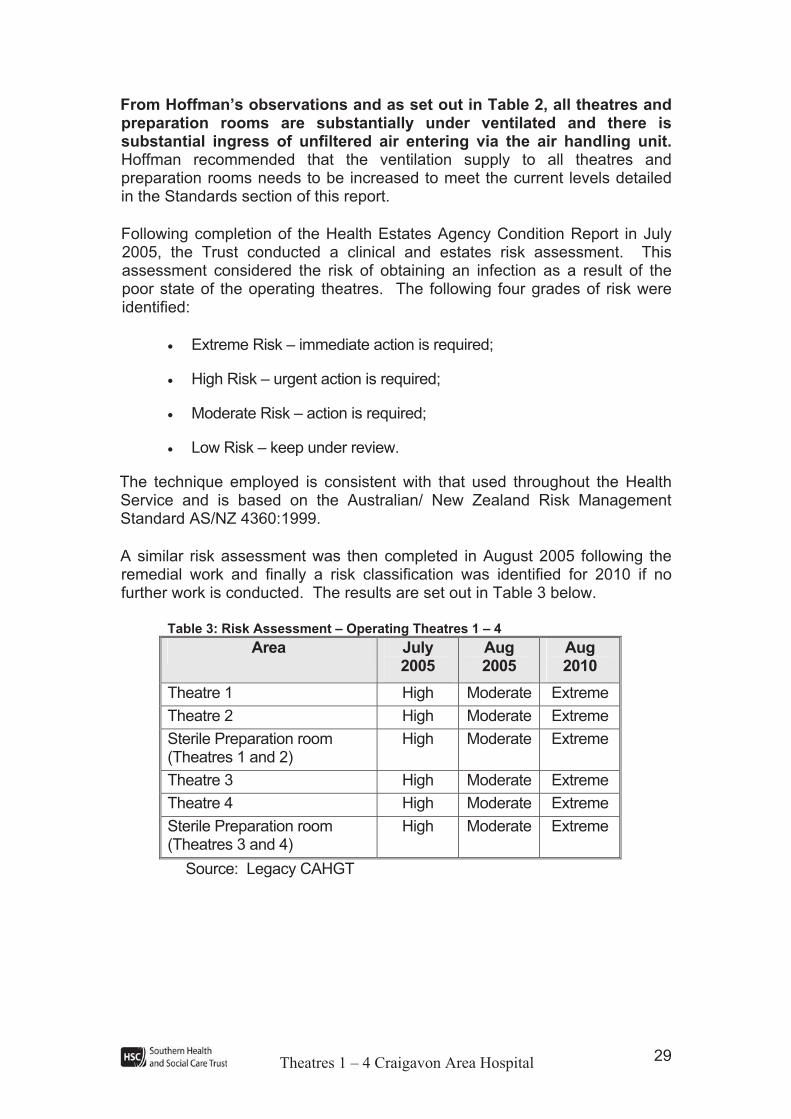
From Hoffman’s observations and as set out in Table 2, all theatres and preparation rooms are substantially under ventilated and there is substantial ingress of unfiltered air entering via the air handling unit. Hoffman recommended that the ventilation supply to all theatres and preparation rooms needs to be increased to meet the current levels detailed in the Standards section of this report.
Following completion of the Health Estates Agency Condition Report in July 2005, the Trust conducted a clinical and estates risk assessment. This assessment considered the risk of obtaining an infection as a result of the poor state of the operating theatres. The following four grades of risk were identified:
! Extreme Risk – immediate action is required;
! High Risk – urgent action is required;
! Moderate Risk – action is required;
! Low Risk – keep under review.
The technique employed is consistent with that used throughout the Health Service and is based on the Australian/ New Zealand Risk Management Standard AS/NZ 4360:1999.
A similar risk assessment was then completed in August 2005 following the remedial work and finally a risk classification was identified for 2010 if no further work is conducted. The results are set out in Table 3 below.
Table 3: Risk Assessment – Operating Theatres 1 – 4
Area July 2005
Aug2005
Aug2010
Theatre 1 High Moderate Extreme
Theatre 2 High Moderate Extreme
Sterile Preparation room (Theatres 1 and 2)
High Moderate Extreme
Theatre 3 High Moderate Extreme
Theatre 4 High Moderate Extreme
Sterile Preparation room (Theatres 3 and 4)
High Moderate Extreme
Source: Legacy CAHGT

Theatres 1 – 4 Craigavon Area Hospital 30
Therefore whilst the remedial work had the impact of reducing the level of risk from High to Moderate, this was only achieved through increasing air flows and cleaning of ductwork. It was not practical to improve the physical condition of the plant and theatres (without significant work being undertaken) so the risk of “age related” failure is unchanged ie. this is only a short term reprieve, if no further work is done then the level of risk is judged to increase to Extreme. The risk assessment therefore shows that a medium term solution is required to prevent the existing theatre suite from becoming an extreme risk area before the new hospital development is completed.
Theatres 1 – 4 Craigavon Area Hospital 31
4.3 Demand Assessment
In this section, an overview is given of current and anticipated future demand for surgery and in turn the ‘need’ for the existing theatres to be replaced. Future demand for surgery, both elective and emergency, is considered within the context of a number of key factors including:
! Theatre utilisation;
! Increase in activity levels at Craigavon Area Hospital resulting in the need to maximise utilisation of operating theatres;
! The need to meet DHSSPS targets in relation to the management of waiting lists for elective surgery;
! Planned service developments;
! Increasing levels of day case surgery; and
! Population Projections.
Theatres 1 – 4 Craigavon Area Hospital 32
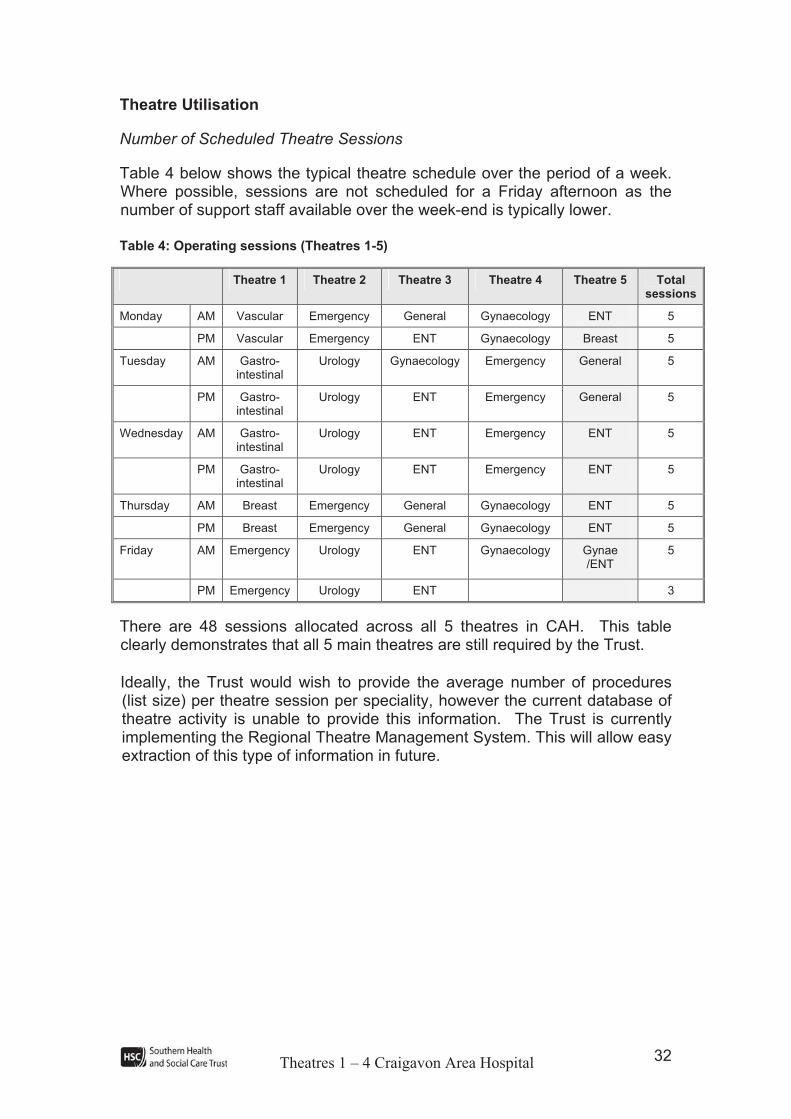
Theatre Utilisation
Number of Scheduled Theatre Sessions
Table 4 below shows the typical theatre schedule over the period of a week. Where possible, sessions are not scheduled for a Friday afternoon as the number of support staff available over the week-end is typically lower.
Table 4: Operating sessions (Theatres 1-5)
Theatre 1 Theatre 2 Theatre 3 Theatre 4 Theatre 5 Total sessions
Monday AM Vascular Emergency General Gynaecology ENT 5
PM Vascular Emergency ENT Gynaecology Breast 5
Tuesday AM Gastro-intestinal
Urology Gynaecology Emergency General 5
PM Gastro-intestinal
Urology ENT Emergency General 5
Wednesday AM Gastro-intestinal
Urology ENT Emergency ENT 5
PM Gastro-intestinal
Urology ENT Emergency ENT 5
Thursday AM Breast Emergency General Gynaecology ENT 5
PM Breast Emergency General Gynaecology ENT 5
Friday AM Emergency Urology ENT Gynaecology Gynae /ENT
5
PM Emergency Urology ENT 3
There are 48 sessions allocated across all 5 theatres in CAH. This table clearly demonstrates that all 5 main theatres are still required by the Trust.
Ideally, the Trust would wish to provide the average number of procedures (list size) per theatre session per speciality, however the current database of theatre activity is unable to provide this information. The Trust is currently implementing the Regional Theatre Management System. This will allow easy extraction of this type of information in future.
Theatres 1 – 4 Craigavon Area Hospital 33
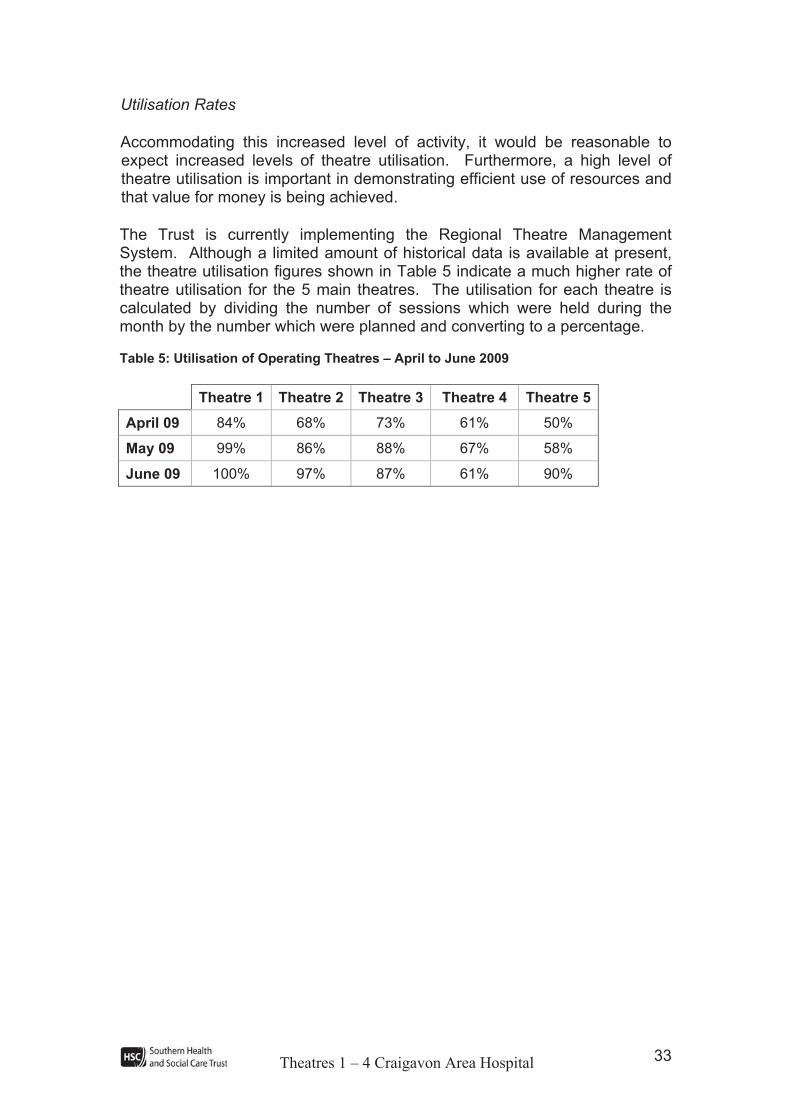
Utilisation Rates
Accommodating this increased level of activity, it would be reasonable to expect increased levels of theatre utilisation. Furthermore, a high level of theatre utilisation is important in demonstrating efficient use of resources and that value for money is being achieved.
The Trust is currently implementing the Regional Theatre Management System. Although a limited amount of historical data is available at present, the theatre utilisation figures shown in Table 5 indicate a much higher rate of theatre utilisation for the 5 main theatres. The utilisation for each theatre is calculated by dividing the number of sessions which were held during the month by the number which were planned and converting to a percentage.
Table 5: Utilisation of Operating Theatres – April to June 2009
Theatre 1 Theatre 2 Theatre 3 Theatre 4 Theatre 5
April 09 84% 68% 73% 61% 50%
May 09 99% 86% 88% 67% 58%
June 09 100% 97% 87% 61% 90%
Theatres 1 – 4 Craigavon Area Hospital 34
Current Activity Levels
Main Theatre Activity
Inpatient activity at CAH has been increasing over the past number of years. Most of this can be attributed to changes in demographics generally and the increase in the number of elderly people, in particular. Other factors include changes in the Trust’s catchment area, which has increased with the reduced number of acute hospitals across Northern Ireland.
When assessing activity levels, it is important to understand the breakdown in terms of the level of complexity of surgical procedures. For example a small increase in complex surgery numbers would have a much more significant impact than a small increase in the number of minor surgical procedures. Surgical procedures have been categorised as follows:
! Complex – for example radical cystectomy (removal of the bladder);
! Major+ – for example cholecystectomy (removal of the gall bladder);
! Major – for example appendectomy (removal of the appendix );
! Intermediate – for example stripping/removal of varicose veins; and
! Minor – for example surgery on ingrown toe nails.
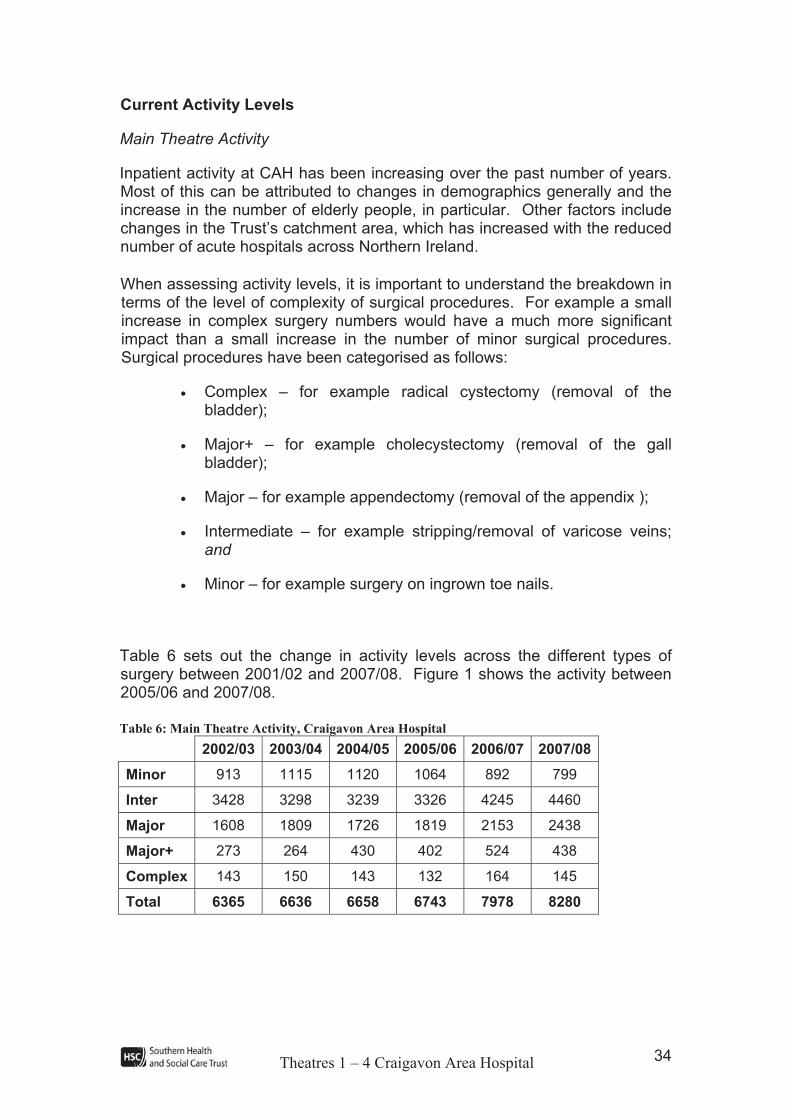
Table 6 sets out the change in activity levels across the different types of surgery between 2001/02 and 2007/08. Figure 1 shows the activity between 2005/06 and 2007/08.
Table 6: Main Theatre Activity, Craigavon Area Hospital
2002/03 2003/04 2004/05 2005/06 2006/07 2007/08
Minor 913 1115 1120 1064 892 799
Inter 3428 3298 3239 3326 4245 4460
Major 1608 1809 1726 1819 2153 2438
Major+ 273 264 430 402 524 438
Complex 143 150 143 132 164 145
Total 6365 6636 6658 6743 7978 8280
Theatres 1 – 4 Craigavon Area Hospital 35
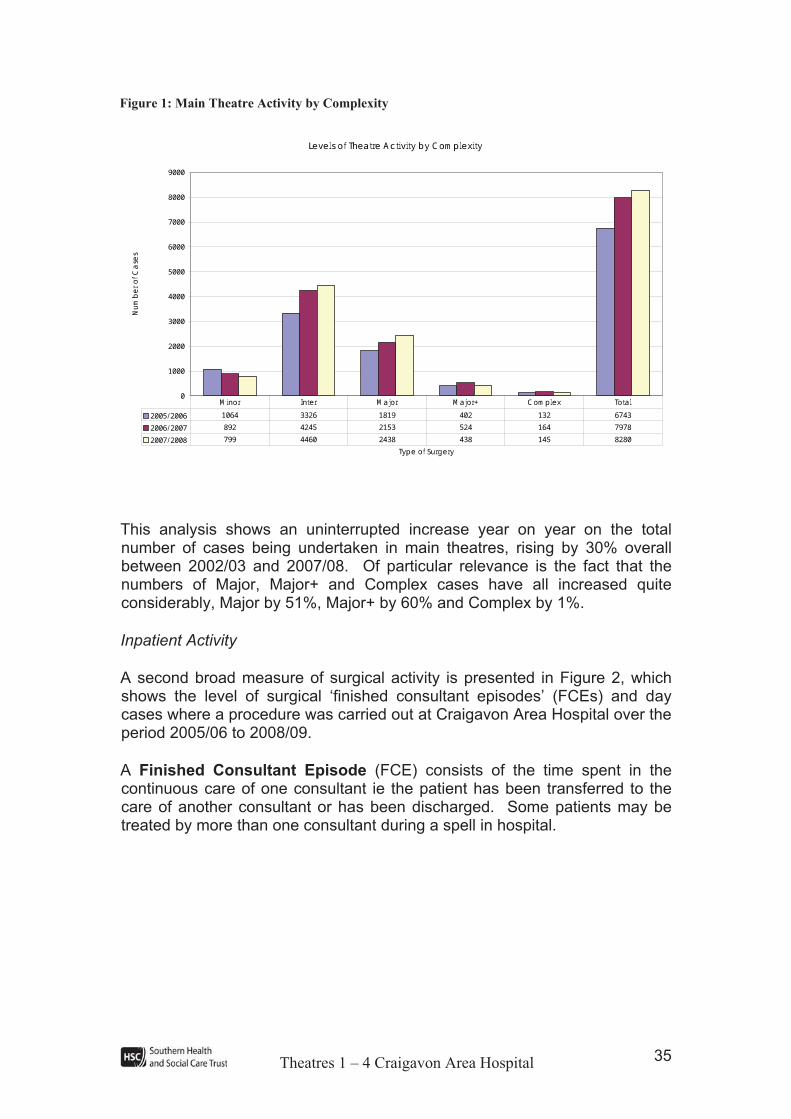
Figure 1: Main Theatre Activity by Complexity
Levels of Theatre Activity by Complexity
0100020003000400050006000700080009000
Type of Surgery
Number o
f Cases
2005/2006 1064 3326 1819 402 132 67432006/2007 892 4245 2153 524 164 79782007/2008 799 4460 2438 438 145 8280Minor Inter Major Major+ Complex Total
This analysis shows an uninterrupted increase year on year on the total number of cases being undertaken in main theatres, rising by 30% overall between 2002/03 and 2007/08. Of particular relevance is the fact that the numbers of Major, Major+ and Complex cases have all increased quite considerably, Major by 51%, Major+ by 60% and Complex by 1%.
Inpatient Activity
A second broad measure of surgical activity is presented in Figure 2, which shows the level of surgical ‘finished consultant episodes’ (FCEs) and day cases where a procedure was carried out at Craigavon Area Hospital over the period 2005/06 to 2008/09.
A Finished Consultant Episode (FCE) consists of the time spent in the continuous care of one consultant ie the patient has been transferred to the care of another consultant or has been discharged. Some patients may be treated by more than one consultant during a spell in hospital.
Theatres 1 – 4 Craigavon Area Hospital 36
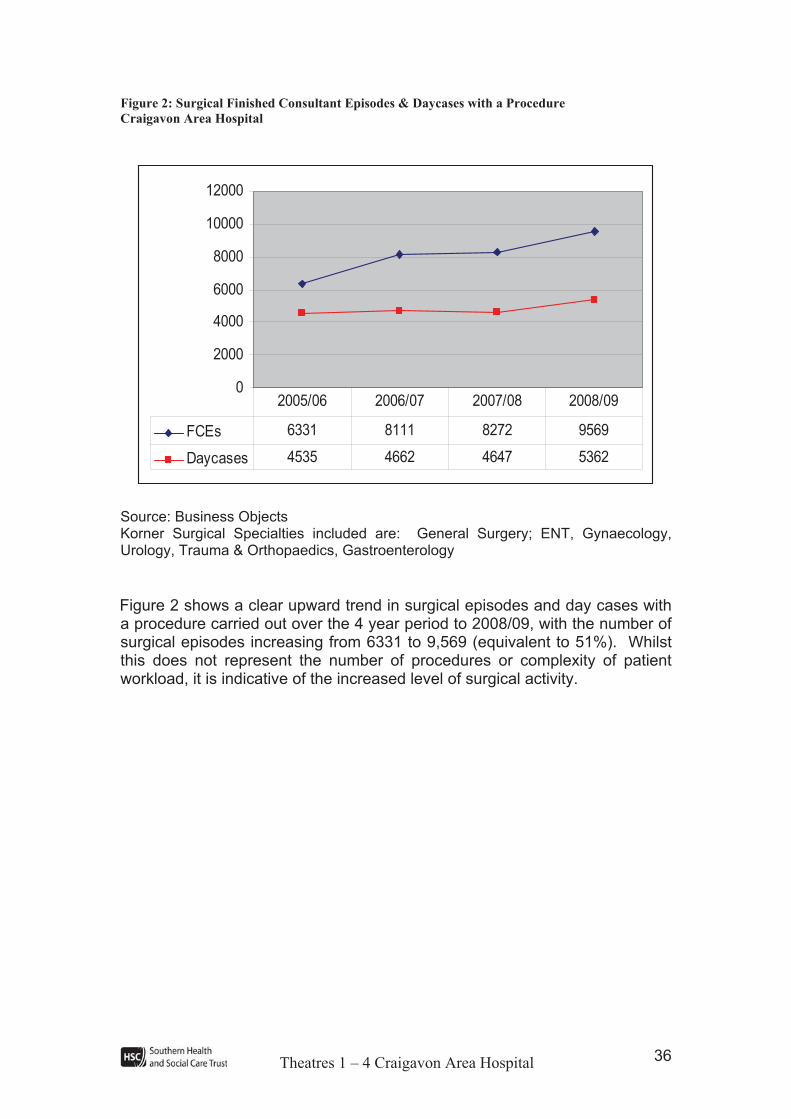
Figure 2: Surgical Finished Consultant Episodes & Daycases with a Procedure
Craigavon Area Hospital
0
2000
4000
6000
8000
10000
12000
FCEs 6331 8111 8272 9569
Daycases 4535 4662 4647 5362
2005/06 2006/07 2007/08 2008/09
Source: Business Objects Korner Surgical Specialties included are: General Surgery; ENT, Gynaecology, Urology, Trauma & Orthopaedics, Gastroenterology
Figure 2 shows a clear upward trend in surgical episodes and day cases with a procedure carried out over the 4 year period to 2008/09, with the number of surgical episodes increasing from 6331 to 9,569 (equivalent to 51%). Whilst this does not represent the number of procedures or complexity of patient workload, it is indicative of the increased level of surgical activity.

Theatres 1 – 4 Craigavon Area Hospital 37
Management of Waiting Time Targets and Independent Sector Activity
Whilst the Trust is currently meeting the Priorities for Action target of 13 weeks for inpatient and daycase treatment, this has required significant use of the independent sector to provide additional capacity. This indicates capacity constraints within the Trust to meet waiting list targets on an ongoing basis. Table 7 shows the high level of independent sector usage by the Trust for 2007/08 and 2008/09.
Table 7: Independent Sector Activity
EpisodesDay Cases
2007/08 ENT 182 16
General Surgery 80 156
General Surgery (Scopes) 1 353
Urology 76 31
Oral Surgery 0 81
Pain Management 0 21
Ophthalmology 0 687
Rheumatology 0 1
Total 339 1346
2008/09 ENT 405 30
General Surgery 156 224
General Surgery (Scopes) 3 1199
Urology 187 498
Gynaecology 58 32
Orthopaedics 17 10
Oral Surgery 0 130
Pain Management 0 92
Ophthalmology 0 790
Total 826 3005
It is the Trust’s intention to reduce the level of activity which is undertaken within the independent sector and a bid has been made for recurring access target funding to increase capacity for endoscopy, orthopaedics, pain management, ENT and gynaecology. These developments will all impact on the requirement for theatre capacity but they can be accommodated within the current theatre complement.
It is the Regional Health and Social Care Board’s (RHSCB) intent that the use of independent sector should be minimised. In the last quarter of 2009/10 the Trust made significant reductions in the use of independent sector capacity. Only 193 day cases were treated in the independent sector during this 3 month period. This achievement resulted from the maximisation of theatre capacity, flexible use of theatres and the provision of sessions in the evening and weekend.
Theatres 1 – 4 Craigavon Area Hospital 38
Service Developments
The Trust continually seeks to modernise current service and to introduce alternative service models such as ‘see and treat’ clinics for appropriate conditions. However, there are a number of planned service developments which will impact on the requirement for theatre capacity at the Trust:
Review of Urology Services
A regional review of Urology services has recently been undertaken and the final report is awaited. The report is expected to recommend a 3 team model for urology services within Northern Ireland. Team South will be based at Craigavon Area Hospital and will provide services for a catchment population of approximately 410,000. It will encompass the Southern area and the lower third of the Western area (Fermanagh). The number of surgeons will increase from the current three to five, with a requirement to provide a minimum of six additional operating sessions across the Trust.
Bowel Screening
PSA Target 1.11 states:
By December 2009, ensure that a comprehensive bowel screening programme for those aged 60 – 69 is in place, with a view to achieving a 10% reduction in mortality from bowel cancer by 2011.
Craigavon Area Hospital has been identified as a Bowel Screening Centre and will be required to provide a dedicated weekly colonoscopy list for bowel screening. This will be a new theatre session in addition to those which are already in place for endoscopic diagnostic procedures.
ENT
The appointment of an additional consultant surgeon is planned to meet an identified capacity gap for this service. This new post will require a further two operating sessions.
Pain Management
The Trust has submitted a proposal to the Southern Commissioning Group for an additional Consultant in Pain Management. The job plan for this post includes a weekly day case session.
Theatres 1 – 4 Craigavon Area Hospital 39
Ophthalmology
The current ophthalmology service at the Southern Trust is delivered on an outreach basis by Belfast Trust. The Trust plans to develop an ophthalmology service with locally employed staff providing outpatient and day surgery sessions. The number of ophthalmology theatre sessions at South Tyrone Hospital will increase from the current 3 per week to 6 each week, giving a requirement for an additional 3 weekly day surgery theatre sessions. This increase in ophthalmology theatre sessions at South Tyrone may require existing sessions to be displaced and re-provided at Craigavon Area Hospital.
Impact of Increased Day Case Rates
PSA Target 9.1 states that:
Each Trust should secure improvements in daycase rates for a defined range of procedures in accordance with Departmental targets for March 2010 and 2011.
The Southern Trust recognises the potential benefits to be gained from optimising the number of elective procedures that can be performed as a day case both from a patient quality and efficiency perspective. The Trust has therefore put in place plans to ensure that the standard can be achieved for the 25 procedures listed in the day case basket.
A separate business case was submitted to the DHSSPS (August 2006) to extend and refurbish the Day Surgery Unit at Craigavon Hospital but funding has not been made available as yet. Therefore, although the Trust will improve its day case rates in accordance with the PSA target, day case patients will continue to be operated on in main theatre sessions until day surgery capacity can be expanded. In the interim there will be little if any reduction in main theatre activity as a result of improving day case rates.
Theatres 1 – 4 Craigavon Area Hospital 40
Impact of Population Projections
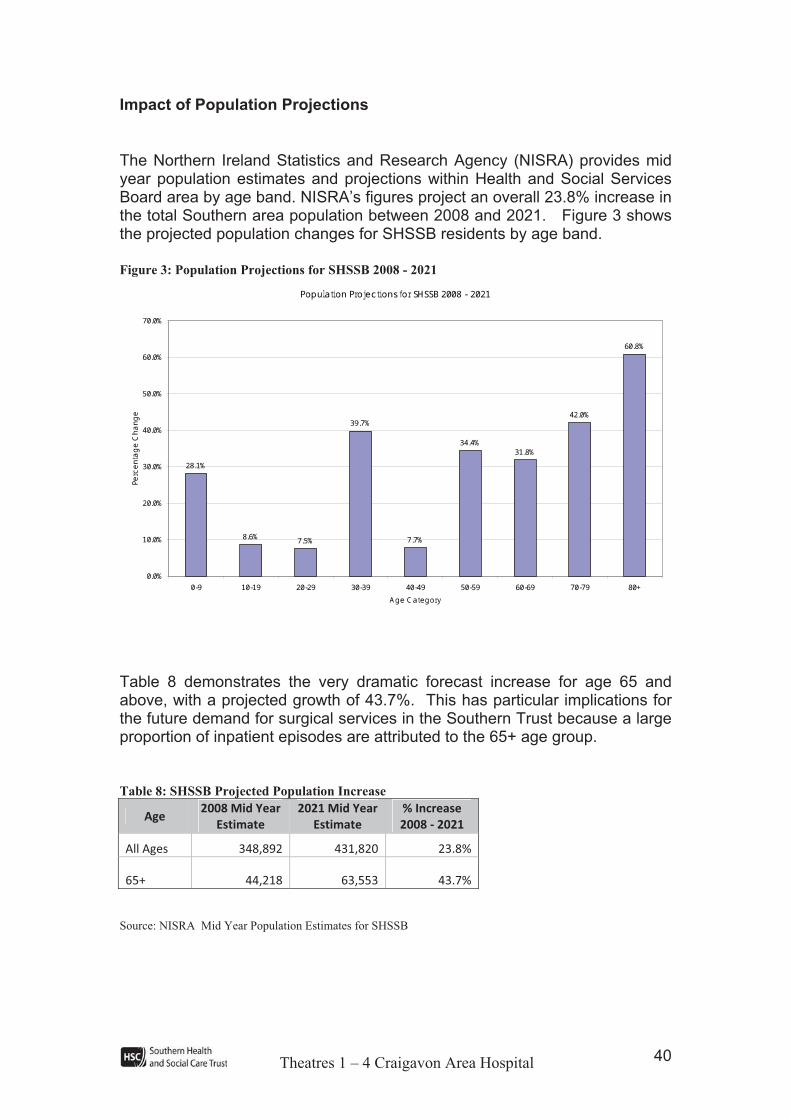
The Northern Ireland Statistics and Research Agency (NISRA) provides mid year population estimates and projections within Health and Social Services Board area by age band. NISRA’s figures project an overall 23.8% increase in the total Southern area population between 2008 and 2021. Figure 3 shows the projected population changes for SHSSB residents by age band.
Figure 3: Population Projections for SHSSB 2008 - 2021
Population Projections for SHSSB 2008 - 2021
8.6% 7.5%
39.7%
7.7%
34.4% 31.8%42.0%
60.8%
28.1%
0.0%10.0%20.0%30.0%40.0%50.0%60.0%70.0%
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 80+Age Category
Percenta
ge Chang
e
Table 8 demonstrates the very dramatic forecast increase for age 65 and above, with a projected growth of 43.7%. This has particular implications for the future demand for surgical services in the Southern Trust because a large proportion of inpatient episodes are attributed to the 65+ age group.
Table 8: SHSSB Projected Population Increase
Age!2008!Mid!Year!
Estimate!
2021!Mid!Year!
Estimate!
%!Increase!
2008!"!2021!
All!Ages! 348,892! 431,820! 23.8%!
65+! 44,218! 63,553! 43.7%!
Source: NISRA Mid Year Population Estimates for SHSSB
Theatres 1 – 4 Craigavon Area Hospital 41
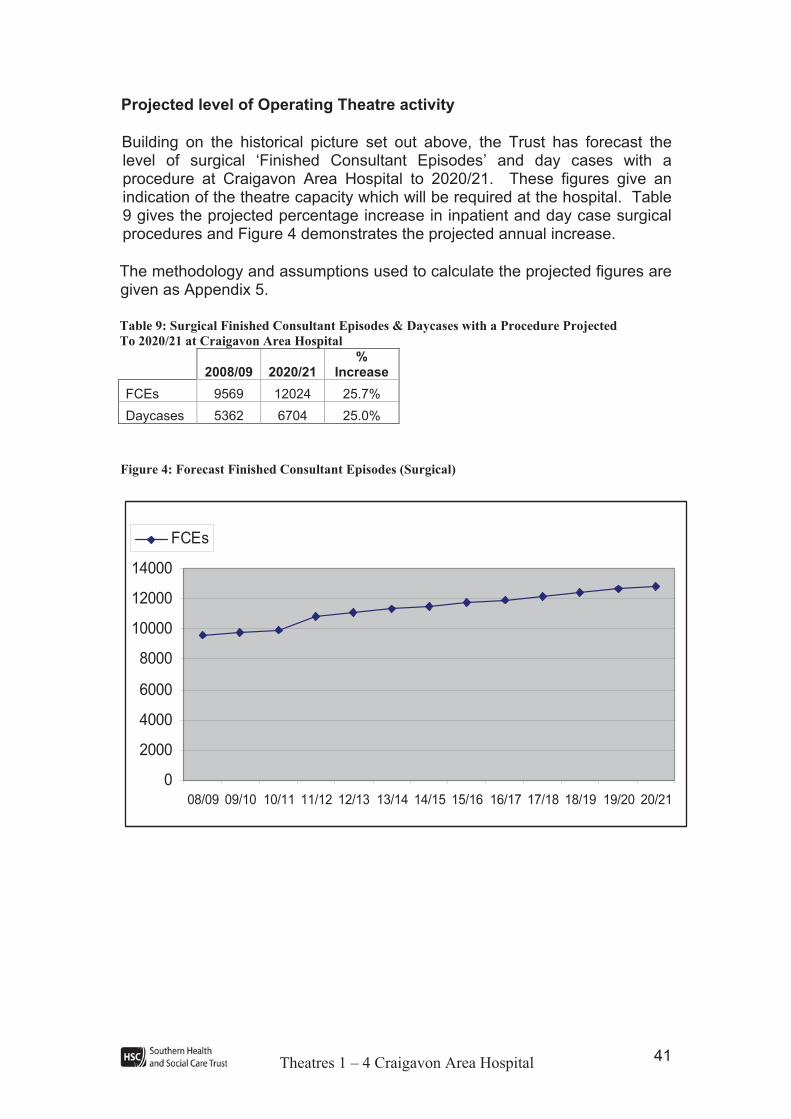
Projected level of Operating Theatre activity
Building on the historical picture set out above, the Trust has forecast the level of surgical ‘Finished Consultant Episodes’ and day cases with a procedure at Craigavon Area Hospital to 2020/21. These figures give an indication of the theatre capacity which will be required at the hospital. Table 9 gives the projected percentage increase in inpatient and day case surgical procedures and Figure 4 demonstrates the projected annual increase.
The methodology and assumptions used to calculate the projected figures are given as Appendix 5.
Table 9: Surgical Finished Consultant Episodes & Daycases with a Procedure Projected
To 2020/21 at Craigavon Area Hospital
2008/09 2020/21 %
Increase
FCEs 9569 12024 25.7%
Daycases 5362 6704 25.0%
Figure 4: Forecast Finished Consultant Episodes (Surgical)
0
2000
4000
6000
8000
10000
12000
14000
08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17 17/18 18/19 19/20 20/21
FCEs

Theatres 1 – 4 Craigavon Area Hospital 42
The longer term demand shows a significant increase in activity. However the Trust believes that in the medium term the increase can be managed within the current theatre complement through maximisation of theatre capacity, implementing ‘The Productive Operating Theatre’ model and by extending the theatre day/week. An outline of the workstreams associated with the Productive Operating Theatre project is given as Appendix 15. The Trust has also the increased networking between its 3 hospitals (Craigavon Area Hospital, Daisy Hill Hospital and South Tyrone Hospital) and the management of patients across this network to improve theatre utilisation. Centralised theatre scheduling has been recently introduced to ensure optimum utilisation of sessions.
In order to comply with national and regional standards and guidelines1 on the care and treatment of children who require elective surgery the Trust is proposing to centralise elective surgery for patients aged 16 and under at Daisy Hill Hospital. These standards and guidelines emphasise the special requirements of paediatric patients in hospital and recommend that children should be managed in separate facilities and be looked after by staff with the appropriate paediatric training and experience.
This proposal is currently out for public consultation. If implemented, it will release some theatre sessions which will be used to absorb increases in theatre activity.
1 The National Framework for Children, Young People and Maternity Service;, The Royal College of Anaesthetists, Guidelines on the Provision of Paediatric Anaesthetic Services; DHSSPSNI proposed
new standards ‘Improving Services for General Paediatric Surgery’ and ‘Improving Services for
Paediatric ENT Surgery’

Theatres 1 – 4 Craigavon Area Hospital 43
Summary of Assessment of Need
Condition of Existing Facilities
! The theatre ventilation plant (including design configuration and air change rate) does not meet Departmental standards (HTM 2025);
! Theatre design does not meet Departmental standards (HBN 26) in terms of space, layout or quality of finishes;
! There are significant electrical services issues including only one source of electrical supply; emergency back-up is fully loaded and the distribution network contravenes standards;
! Remedial works to the theatres have been successful in reducing the risk to MODERATE. However, to prevent the risk rising to EXTREME, primarily due to the failure of aging infrastructure, further significant action is required.
Demand Assessment
! The number of theatre sessions is currently at 48 per week; however usage can be higher depending on the time of the year;
! Main theatre activity has increased over the last three years, particularly in terms of the numbers of more complex surgery. Historical data on surgical FCEs with a procedure at Craigavon Area Hospital has shown a significant increase over the last four years, with the number of surgical FCEs with a procedure increasing from 6,331 in 2005/06 to 9,569 in 2008/09, an increase of 51%;
! Whilst the Trust is currently meeting the PfA target of 13 weeks for inpatient and daycase treatment, this has required significant use of the independent sector to provide additional capacity. In 2008/09 826 inpatient and 3,005 day case episodes were provided by the independent sector. It is the Regional Health and Social Care Board’s (RHSCB) intent that the use of independent sector should be minimised. In the last quarter of 2009/10 the Trust made significant reductions in the use of independent sector capacity. Only 193 day cases were treated in the independent sector. This achievement resulted from the maximisation of theatre capacity, flexible use of theatres and the provision of sessions in the evening and weekend;

Theatres 1 – 4 Craigavon Area Hospital 44
! Planned service developments will give rise to the need to increase theatre sessions within the Trust. These developments include the expansion of urology with the appointment of 2 additional consultant surgeons, the commencement of bowel screening, the expansion of ENT and chronic pain management services, the development of a local ophthalmology service;
! The Trust will increase its day surgery rates in line with the PSA target 1.11. However, this will not significantly affect the level of activity in main theatres due to capacity constraints in the day surgery unit;
! Population demographics show a 23.8% increase in the overall number of people in the Southern area by 2021 and more significantly an increase of 43.7% in those aged 65 years and over. This increase will have a considerable impact on the requirement for theatre capacity because a large proportion of inpatient episodes are attributable to the 65+ age group;
! Projected inpatient surgical activity is forecast to increase to 12,024 FCEs by 2020/21, a substantial increase of 25% between 2008/09 and 2020/21.
Theatres 1 – 4 Craigavon Area Hospital 45
5 PATIENT PATHWAY The operating theatre department comprises:
! 5 general theatres – 4 which are the subject of this proposal and one which has recently been replaced with a new build theatre (theatre 5);
! A dental room;
! An emergency endoscopy room (former theatre 5);
! Two new trauma and orthopaedic theatres are currently being constructed (scheduled for handover at the end of March 2010) adjacent to and linked to the main theatre suite.
All of the theatres listed above are managed as a single, integrated operating department.
There will be 4 theatres provided as part of this scheme. It is proposed that all four theatres will be 55 m2. Two will be general theatres and the remaining 2 theatres will be ultra clean with 18 m2 preparation rooms to facilitate procedures which require a large number of trolleys. This will provide flexibility within the operating theatre department eg the trauma and orthopaedic service will be able to use the two ultra clean theatres, if required. The theatres will be provided with an exit bay which is large enough to park the empty bed belonging to the patient currently in theatre.
There will be 3 main groups of patients arriving at theatres:
! Elective patients arriving straight from home;
! Elective patients coming from a surgical ward;
! Emergency cases coming from a surgical ward or A&E Department.
The majority of elective patients will arrive at the operating theatre department straight from home, having previously been pre-assessed. They will be admitted via the admissions lounge and will be assessed in the lounge by the surgeon and the anaesthetist prior to surgery. They will not go to a surgical ward until after recovery. This will reduce the pressure on surgical wards and enable the Trust to make much more effective use of its surgical bed complement. It is worthy of note that the Trust has implemented best practice in relation to admission on the day for elective procedures and compares favourably with the Northern Ireland average. The most recent figures which are available relate to the quarter ended December 2009. CHKS benchmarking data indicates a NI average of 73.6% of elective inpatients admitted on the day of their procedure compared to a Southern Trust figure of 75.1%.

Theatres 1 – 4 Craigavon Area Hospital 46
Those elective and emergency patients arriving at theatre from a ward will be moved to the anaesthetic room if it is free or to a pre operative holding bay. The holding bays will be equipped with medical gases and will be provided adjacent to the recovery ward to allow for the observation of pre operative patients.
Following surgery patients are transferred from theatre to recovery ward. The recovery ward is open 24 hours, seven days per week. The recovery ward is used by:
! The 5 main theatres (theatres 1-5);
! The dental room;
! The emergency endoscopy room (‘old’ theatre 5);
! The trauma and orthopaedic theatres, out of hours. The T&O theatres do not currently provide an out of hours service and any patients requiring recovery after 9pm or an overnight stay are transferred to the main recovery ward;
! For short term high dependency care (in line with para 3.23 & 3.30 HBN 26)
As far as possible male and female patients will be segregated in recovery. Children will be separated from adults in the recovery area, and accommodation will be provided for parents of children who have to remain in recovery.
The current recovery ward can accommodate up to a maximum of 15 patients, with bed spacing which is considerably less than the recommended 3.6 m2, This is not sufficient and theatre lists have to be carefully planned around the existing recovery capacity, with patients sometimes having to be recovered in theatre, thereby delaying lists. The Trust therefore proposes an 18 bed recovery ward with this scheme.
Theatres 1 – 4 Craigavon Area Hospital 47
6 OBJECTIVES AND CONSTRAINTS Introduction
This section of the business case sets out project objectives for the proposed replacement of theatres 1 to 4. It also details anticipated constraints that will impact on the achievement of the identified objectives.
6.1 Objectives
In terms of service delivery at Craigavon Area Hospital, the Trust is responsible for delivering healthcare in line with the following overarching objectives:
! Safety for patients, staff and the local community through well designed, constructed and maintained facilities that meet regulation and service standards (Measured in terms of alignment with Health Building Notes (HBN) and Health Technical Memoranda (HTM));
! Equity/Accessibility of services regardless of where services are provided (Measured through ensuring all members of the public have access to modern facilities);
! Sustainability of services, through clinical integration, networks and maximisation of synergies (Measured in terms of a full range of surgical procedures including emergency surgery being undertaken in the new facility);
! Affordability and demonstration of value-for-money (Measured in terms of option selection through business case process); and
! Quality services capable of delivering high quality healthcare incorporating best practice and fit for purpose solutions (Measured in terms of alignment with HBN and HTM).
In terms of the specific replacement/upgrading of the existing theatre suite the following overall aim has been identified:
“To provide a suitable theatre suite and associated support facilities until completion of the redevelopment of the Craigavon Area Hospital site.”

Theatres 1 – 4 Craigavon Area Hospital 48
The specific objectives for this project are set out below:
Objective 1: To deliver operating theatre accommodation by 2012 to DHSSPS standards as per:
! Health Building Notes (HBN 26 – Facilities for Surgical Procedures);
! Health Technical Memoranda;
! Laser Protection Agency Guidance;
! Radiation Protection Agency Guidance.
Objective 2: To provide a reliable theatre environment for patients and staff to ensure consistent levels of theatre capacity on completion of the project::
! Provide capacity for 47 sessions per week;
! Maintain utilisation rates at above 85%;
! Meet access targets.
Objective 3: To provide accommodation with the flexibility/capacity to accommodate the level of emergency and complex procedures as emerging from the presenting population on completion of the project (currently 20% of procedures undertaken in the main theatre complex):
! Undertake 20% of emergency and complex surgery work.
Objective 4: To ensure there are no unscheduled session cancellations during the period of construction and current capacity is maintained. To minimise the disruption to theatre and other support services.
Objective 5: To achieve a high satisfaction rating from theatre staff on completion of the project::
! Achieve 95% satisfaction as determined through staff survey.
Objective 6: To align with the Trust’s strategic direction and contribute to the development of services within the Trust:
! The achievement of the day surgery standard of 75% day case rate for the ‘basket’ of 25 procedures;
! The development of bowel screening at the Trust. A key ministerial target was set for the service in 2008/09 (PSA 1.11):
‘By December 2009, a comprehensive bowel screening programme for those aged 60-69 is in place with a view to achieving a 10% reduction in mortality from bowel cancer by 2011’.
Craigavon Area Hospital has been identified as the Southern Trust bowel screening centre and will be required to provide dedicated screening colonoscopy lists;
Theatres 1 – 4 Craigavon Area Hospital 49
! The expansion of the urology service in line with the current regional review of urology;
! The expansion of services including ENT, endoscopy and pain management, to meet identified capacity gaps;
! The development of an integrated ophthalmology service.
6.2 Constraints
The following constraints have been identified in respect of this project:
o Funding – the preferred option must be both accessible and affordable in terms of capital and revenue;
o Existing Estate – The preferred option must make best use of the existing estate and service infrastructure without impeding potential future development of the Craigavon Hospital site;
o Need for theatre Support at all times – in addition to having operating theatres available for use, it is also necessary that the support infrastructure is also in place. Most importantly this includes a suitable ‘Recovery Area’, but also other facilities such as changing rooms for staff. As a result sequencing will be important;
o Infection Control – the sequence of the works programme must mitigate the risk of infection during the construction phase;
o Site Constraints – any proposed replacement theatre must be located adjacent to necessary support infrastructure (eg. the Intensive Care Unit).

Theatres 1 – 4 Craigavon Area Hospital 50
7 IDENTIFICATION & SHORTLISTING OF OPTIONS Introduction
This section of the business case identifies potential solutions - what is referred to as the ‘long list’ of options. A baseline option and a range of alternative options were identified by the Project Team. This long list of potential solutions was then sifted using the identified objectives and constraints to produce a short list of appropriate options for in-depth appraisal.
7.1 Long List of Options
Table 10 summarises the long list of options identified by the Project Board with further detail being provided in the paragraphs that follow.
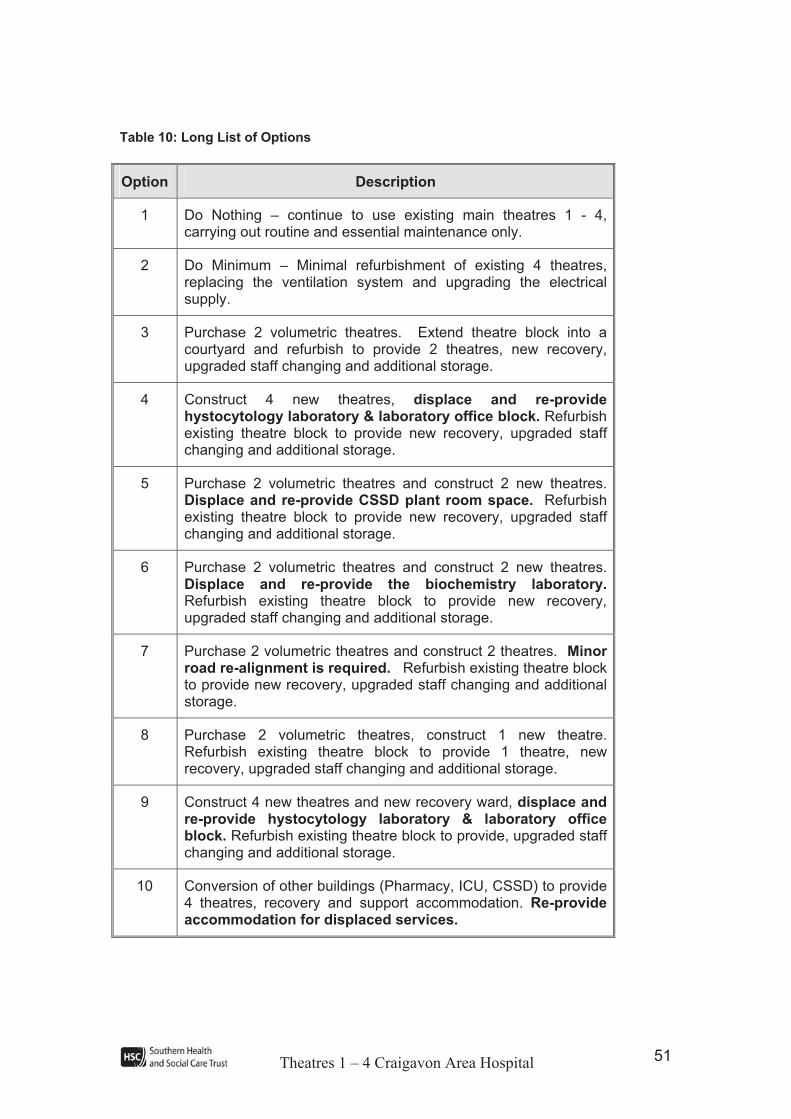
Theatres 1 – 4 Craigavon Area Hospital 51
Table 10: Long List of Options
Option Description
1 Do Nothing – continue to use existing main theatres 1 - 4, carrying out routine and essential maintenance only.
2 Do Minimum – Minimal refurbishment of existing 4 theatres, replacing the ventilation system and upgrading the electrical supply.
3 Purchase 2 volumetric theatres. Extend theatre block into a courtyard and refurbish to provide 2 theatres, new recovery, upgraded staff changing and additional storage.
4 Construct 4 new theatres, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
5 Purchase 2 volumetric theatres and construct 2 new theatres. Displace and re-provide CSSD plant room space. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
6 Purchase 2 volumetric theatres and construct 2 new theatres. Displace and re-provide the biochemistry laboratory.Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
7 Purchase 2 volumetric theatres and construct 2 theatres. Minorroad re-alignment is required. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
8 Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage.
9 Construct 4 new theatres and new recovery ward, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide, upgraded staff changing and additional storage.
10 Conversion of other buildings (Pharmacy, ICU, CSSD) to provide 4 theatres, recovery and support accommodation. Re-provide accommodation for displaced services.

Theatres 1 – 4 Craigavon Area Hospital 52
Volumetric Modular Theatres
Volumetric theatres are steel framed, pre-engineered modular units manufactured within a controlled factory environment that are delivered to site as fitted-out, serviced building modules and craned into position to form a complete healthcare building. Volumetric modular buildings offer the advantages of ability to meet extremely tight programmes and to achieve installation in congested and restricted sites, e.g. over roofs of existing buildings where there is limited space at ground-floor level and within enclosed hospital courtyards. The majority of the building can be constructed off-site with plant located on the roof whilst ground works, foundations and engineering services infrastructure works are carried out on site. Standard (in terms of layout and specification) volumetric modular operating theatres can provide a fast-track, economical solution that is suited to temporary facilities.
The Southern Trust is currently leasing two volumetric modular theatres with support accommodation to enable the trauma and orthopaedic (T & O) service to commence quickly at the Trust. These theatres will be vacated when the construction of the new trauma and orthopaedic facility has been completed and the building commissioned. The new T&O facility will be handed over for Trust commissioning in April 2010. When the business case for the new T & O facility was written it was intended that the lease would be terminated and these buildings would be removed from the site when the T & O service moves to its new accommodation. However as the replacement of main theatres 1-4 will be a temporary solution until major redevelopment of the Craigavon Area Hospital site a number of the options described below include the purchase and upgrade (to the ventilation systems, nurse call and fire alarm systems) of these two volumetric theatres.
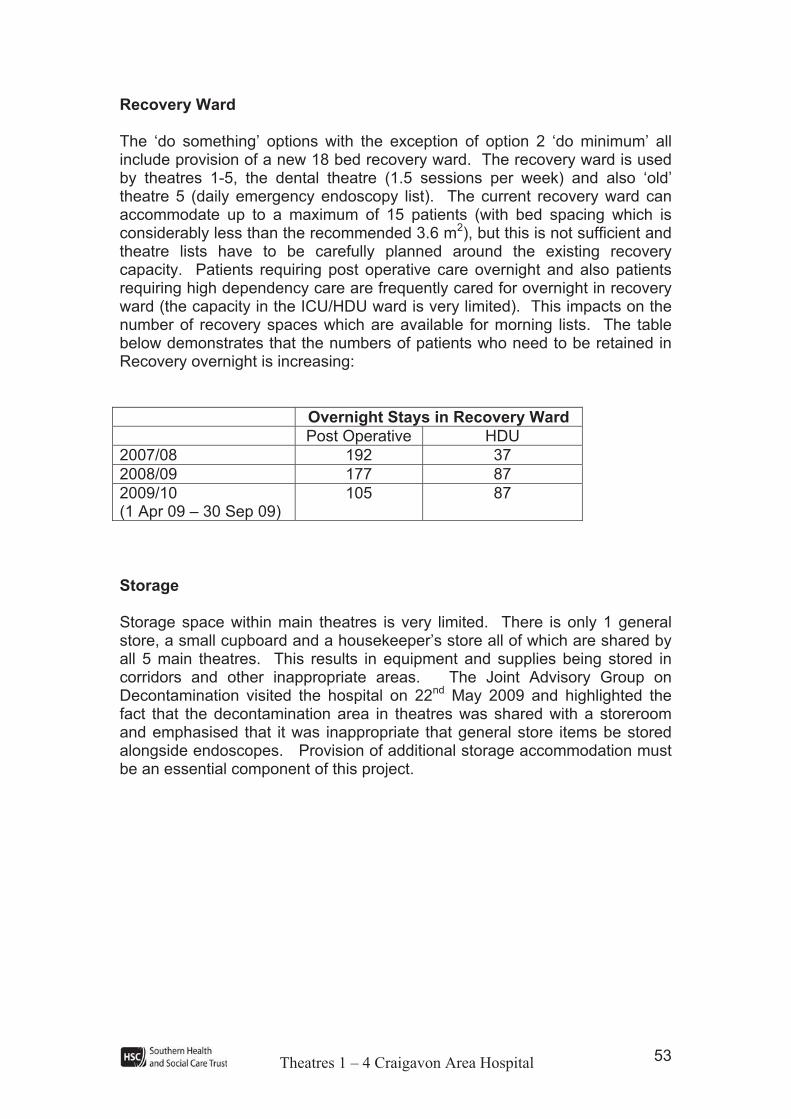
Theatres 1 – 4 Craigavon Area Hospital 53
Recovery Ward
The ‘do something’ options with the exception of option 2 ‘do minimum’ all include provision of a new 18 bed recovery ward. The recovery ward is used by theatres 1-5, the dental theatre (1.5 sessions per week) and also ‘old’ theatre 5 (daily emergency endoscopy list). The current recovery ward can accommodate up to a maximum of 15 patients (with bed spacing which is considerably less than the recommended 3.6 m2), but this is not sufficient and theatre lists have to be carefully planned around the existing recovery capacity. Patients requiring post operative care overnight and also patients requiring high dependency care are frequently cared for overnight in recovery ward (the capacity in the ICU/HDU ward is very limited). This impacts on the number of recovery spaces which are available for morning lists. The table below demonstrates that the numbers of patients who need to be retained in Recovery overnight is increasing:
Overnight Stays in Recovery Ward
Post Operative HDU
2007/08 192 37
2008/09 177 87
2009/10(1 Apr 09 – 30 Sep 09)
105 87
Storage
Storage space within main theatres is very limited. There is only 1 general store, a small cupboard and a housekeeper’s store all of which are shared by all 5 main theatres. This results in equipment and supplies being stored in corridors and other inappropriate areas. The Joint Advisory Group on Decontamination visited the hospital on 22nd May 2009 and highlighted the fact that the decontamination area in theatres was shared with a storeroom and emphasised that it was inappropriate that general store items be stored alongside endoscopes. Provision of additional storage accommodation must be an essential component of this project.

Theatres 1 – 4 Craigavon Area Hospital 54
Option 1 - Do Nothing
This option involves continuing to use the existing theatre suite and undertaking only planned maintenance work as necessary.
Option 2 - Do Minimum – Minimal refurbishment of existing 4 theatres, replacing the ventilation system and upgrading the electrical supply.
This option proposes to conduct the minimum work required to the existing theatres to meet some of the requirements of the HBN and HTM guidance. This would involve refurbishment to the existing four theatres to include the following work:
! Replacement of the ventilation system;
! Upgrade the electricity supply.
It would include removal of ceilings and tracking of walls. Two temporary decant theatres and a temporary recovery ward would be provided and the main theatres would be decanted and refurbished in pairs. Due to capital developments on the Craigavon Hospital site in the vicinity of main theatres (temporary trauma and orthopaedic theatres and ward, new theatre 5, trauma and orthopaedic phase B facility) the available locations for decant accommodation are very limited. The only potential location is on the far side of the laboratory buildings with a clean corridor through the labs reception area.
Option 3 - Purchase 2 volumetric theatres. Extend theatre block into a courtyard & refurbish to provide 2 theatres, new recovery, upgraded staff changing and additional storage.
This option involves purchasing and retaining the 2 volumetric theatres in their present location to replace 2 of the main theatres. Necessary upgrade work to the ventilation system, nurse call and fire alarm systems would be carried out.
The dental theatre, staff rest and office accommodation would be displaced and an extension would be built in an adjacent courtyard to provide a new theatre 3. The 4th theatre would be provided by refurbishing vacated accommodation along with an 18 bed recovery ward, upgraded changing facilities and additional storage. The new theatres and recovery facilities would comply with Health Building Note 26 (HBN 26) and relevant Health Technical Memoranda (HTMs). Old theatre 5 (which has recently been replaced with a new build theatre) would be utilised to provide displaced accommodation. Work would be carried out in phases and 2 theatres and recovery ward would continue to be fully functional within the main theatre block whilst building and refurbishment work is ongoing.

Theatres 1 – 4 Craigavon Area Hospital 55
Option 4 - Construct 4 new theatres, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option involves the construction of four theatres which fully comply with HBN 26 and relevant HTMs located adjacent to the new Theatre 5 and Trauma and Orthopaedic Facility (this is under construction and will be handed over to the Trust in April 2010), to replace the four main theatres. This site is currently occupied by the Histocytology Laboratory and Laboratory office accommodation. These 2 buildings would be re-provided prior to construction commencing. A new 18 bed recovery ward would be provided by refurbishing within the existing main theatre area. The staff changing facilities would also be upgraded and additional storage would be provided.
Option 5 - Purchase 2 volumetric theatres and construct 2 new theatres. Displace and re-provide CSSD plant room space. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option involves purchasing and retaining the 2 volumetric theatres in their present location to replace 2 of the main theatres. Necessary upgrade work to the laminar flow, nurse call and fire alarm systems would be carried out. Two theatres which fully comply with HBN 26 and relevant HTMs would be constructed, one between the volumetric theatres and the current main theatres, taking in part of the CSSD department and the other between new theatre 5 and the Labs buildings. The space lost from CSSD would have to be re-provided.
A new 18 bed recovery ward would be provided by refurbishing within the existing main theatre area. The staff changing facilities would also be upgraded and additional storage would be provided.
Theatres 1 – 4 Craigavon Area Hospital 56
Option 6 - Purchase 2 volumetric theatres and construct 2 new theatres. Displace and re-provide the biochemistry laboratory. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option involves purchasing and retaining the 2 volumetric theatres in their present location to replace 2 of the main theatres. Necessary upgrade work to the ventilation system, nurse call and fire alarm systems would be carried out. Two theatres which fully comply with HBN 26 and relevant HTMs would be constructed together and adjacent to the 2 volumetric theatres between the volumetric theatres and the Biochemistry Laboratory. The Biochemistry Laboratory would be displaced by the new theatres, and would be re-provided.
A new 18 bed recovery ward would be provided by refurbishing within the existing main theatre area. The staff changing facilities would also be upgraded and additional storage would be provided.
Option 7 - Purchase 2 volumetric theatres and construct 2 theatres. Minor road re-alignment is required. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option involves purchasing and retaining the 2 volumetric theatres in their present location to replace 2 of the main theatres. Necessary upgrade work to the ventilation system, nurse call and fire alarm systems would be carried out. Two theatres which fully comply with HBN 26 and relevant HTMs would be constructed, one between the volumetric theatres and the ring road and the other adjacent to the Labs and the new T&O building. Some minor re-alignment of the ring road would be required.
A new 18 bed recovery ward would be provided by refurbishing within the existing main theatre area. The staff changing facilities would also be upgraded and additional storage would be provided.
Option 8 - Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage.
This option involves purchasing and retaining the 2 volumetric theatres in their present location to replace 2 of the main theatres. Necessary upgrade work to the ventilation system, nurse call and fire alarm systems would be carried out. A third theatre would be constructed adjacent to the 2 volumetric theatres and the new theatre 5. The fourth theatre would be provided by refurbishing within the existing main theatre building. Both new theatres would fully comply with HBN 26 and relevant HTMs.
Theatres 1 – 4 Craigavon Area Hospital 57
A new 18 bed recovery ward would be provided by refurbishing within the existing main theatre area. The staff changing facilities would also be upgraded and additional storage would be provided.
Option 9 - Construct 4 new theatres and new recovery ward, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide upgraded staff changing and additional storage.
This option involves the construction of four theatres and new 18 bed recovery ward which fully comply with HBN 26 and relevant HTMs located adjacent to the new Trauma and Orthopaedic Facility on the side furthest away from current main theatres. The new T&O facility is under construction and will be handed over to the Trust for commissioning in April 2010. This site is currently occupied by the histocytology laboratory and laboratory office accommodation. These 2 units would be re-provided prior to construction commencing. The theatre staff changing facilities would also be upgraded and additional storage would be provided.
Option 10 - Conversion of another building — eg Pharmacy, Intensive Care Unit and/ or Central Sterile Service Department to provide 4 theatres, recovery and support accommodation. Re-provide accommodation for displaced services.
This option proposes the conversion of existing buildings (the Pharmacy, ICU and CSSD have been identified as possibilities) into new theatre suites. In all cases, it would be necessary to rebuild the facility/facilities which have been displaced.
The outcome of the preliminary sift of options is shown overleaf with the following symbols:
!! Fully complies with the objective/constraint
! Partially complies with the objective/constraint ? May/may not comply with the objective/constraint
X Fails to comply with the objective/constraint
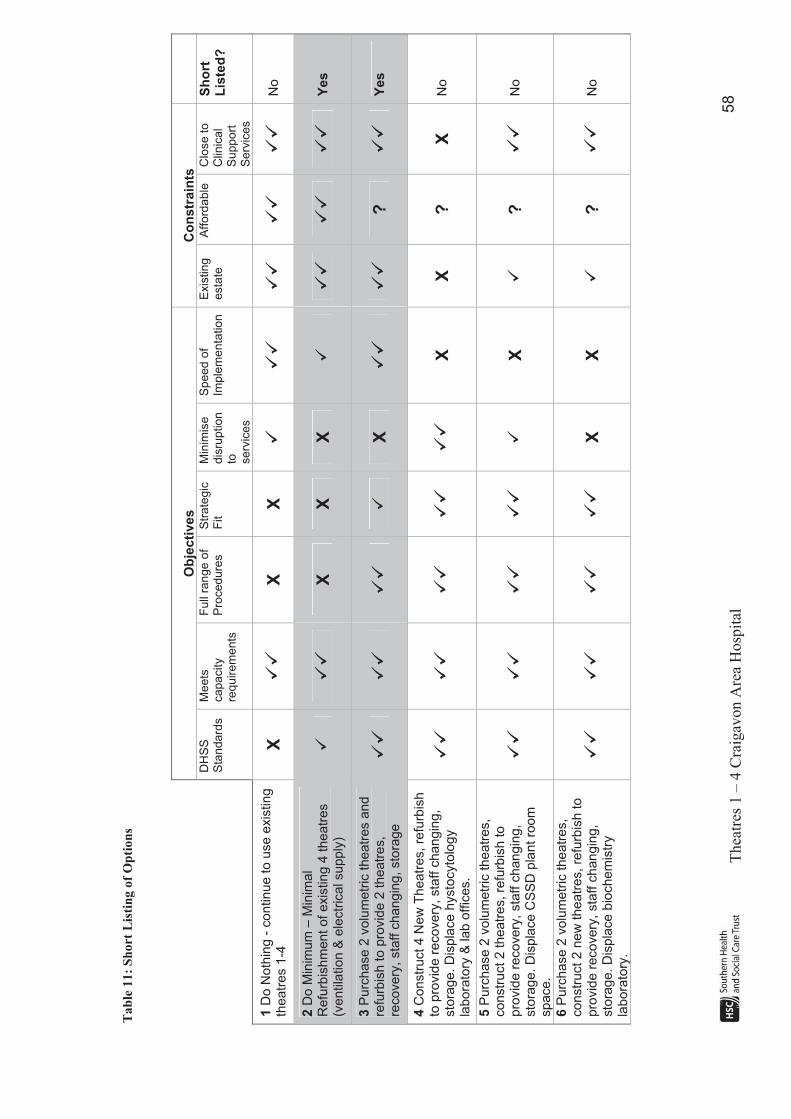
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
58
Ta
ble
11:
Sh
ort
Lis
tin
g o
f O
pti
on
s
Ob
jec
tive
s
Co
nstr
ain
ts
DH
SS
Sta
ndard
s
Meets
capacity
requ
irem
ents
Full
ran
ge o
f P
roced
ure
s
Str
ate
gic
Fit
Min
imis
e
dis
ruption
to serv
ices
Spee
d o
f Im
ple
menta
tion
Exis
ting
esta
teA
fford
able
C
lose t
o
Clin
ical
Supp
ort
S
erv
ices
Sh
ort
Lis
ted
?
1D
o N
oth
ing
- c
on
tinu
e to
use
exis
tin
g
the
atr
es 1
-4X
!!"
X
X
!"
!!"
!!"
!!"
!!"
No
2D
o M
inim
um
– M
inim
al
Refu
rbis
hm
en
t of exis
ting 4
theatr
es
(ventila
tion &
ele
ctr
ical supp
ly)
!"
!!"
XX
X!"
!!"
!!"
!!"
Yes
3P
urc
hase
2 v
olu
me
tric
the
atr
es a
nd
re
furb
ish to p
rovid
e 2
theatr
es,
reco
ve
ry, sta
ff c
ha
ng
ing
, sto
rage
!!"
!!"
!!"
!"
X!!"
!!"
?!!"
Yes
4C
onstr
uct 4 N
ew
Theatr
es, re
furb
ish
to p
rovid
e r
ecovery
, sta
ff c
hangin
g,
sto
rag
e. D
isp
lace
hysto
cyto
log
y
labora
tory
& lab o
ffic
es.
!!"
!!"
!!"
!!"
!!"
X
X
?
X
No
5P
urc
hase
2 v
olu
metr
ic theatr
es,
co
nstr
uct 2 theatr
es, re
furb
ish to
pro
vid
e r
eco
ve
ry, sta
ff c
han
gin
g,
sto
rag
e. D
isp
lace
CS
SD
pla
nt ro
om
sp
ace
.
!!"
!!"
!!"
!!"
!"
X!"
?!!"
No
6P
urc
hase
2 v
olu
metr
ic theatr
es,
constr
uct 2 n
ew
theatr
es, re
furb
ish to
pro
vid
e r
eco
ve
ry, sta
ff c
han
gin
g,
sto
rag
e. D
isp
lace
bio
ch
em
istr
y
labora
tory
.
!!"
!!"
!!"
!!"
X
X
!"
?!!"
No
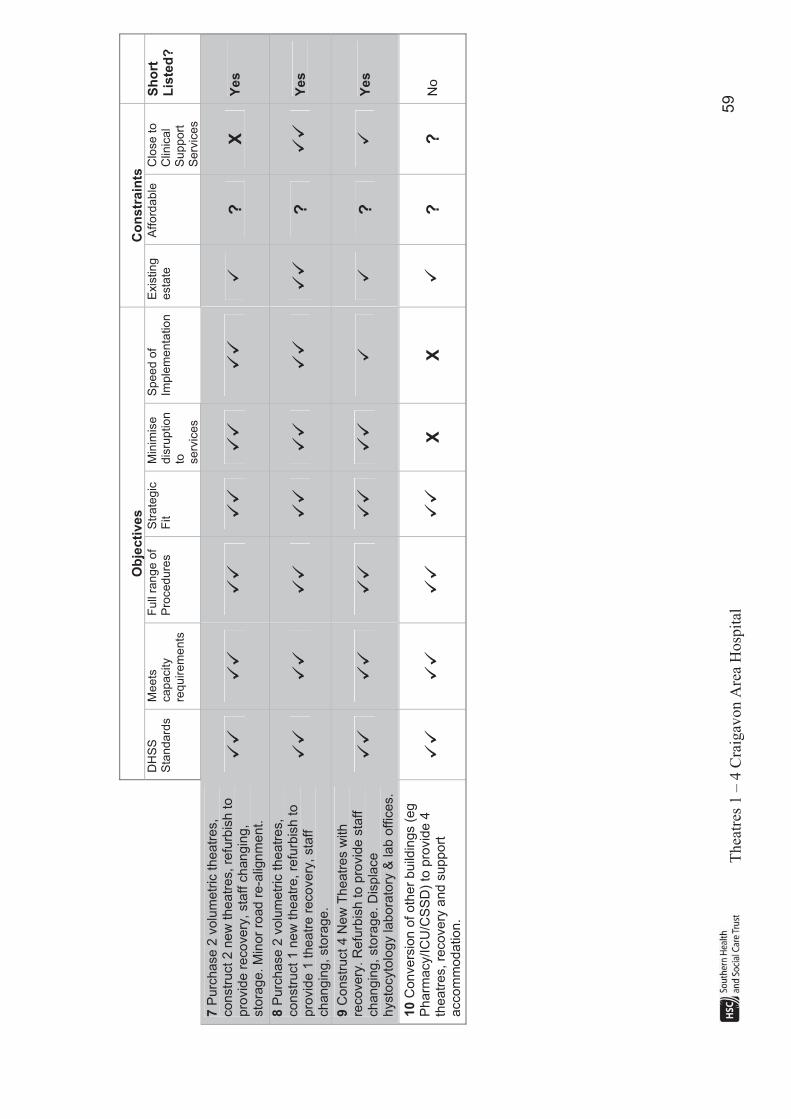
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
59
Ob
jec
tive
s
Co
nstr
ain
ts
DH
SS
Sta
ndard
s
Meets
capacity
requ
irem
ents
Full
ran
ge o
f P
roced
ure
s
Str
ate
gic
Fit
Min
imis
e
dis
ruption
to serv
ices
Spee
d o
f Im
ple
menta
tion
Exis
ting
esta
teA
fford
able
C
lose t
o
Clin
ical
Supp
ort
S
erv
ices
Sh
ort
Lis
ted
?
7P
urc
hase
2 v
olu
metr
ic theatr
es,
constr
uct 2 n
ew
theatr
es, re
furb
ish to
pro
vid
e r
eco
ve
ry, sta
ff c
han
gin
g,
sto
rag
e. M
inor
road
re-a
lign
me
nt.
!!"
!!"
!!"
!!"
!!"
!!"
!"
?X
Yes
8P
urc
hase
2 v
olu
metr
ic theatr
es,
constr
uct 1 n
ew
theatr
e, re
furb
ish to
pro
vid
e 1
thea
tre r
ecovery
, sta
ff
changin
g, sto
rage.
!!"
!!"
!!"
!!"
!!"
!!"
!!"
?!!"
Yes
9C
onstr
uct 4 N
ew
Th
ea
tres w
ith
re
covery
. R
efu
rbis
h to p
rovid
e s
taff
ch
an
gin
g, sto
rag
e. D
isp
lace
hysto
cyto
log
y labora
tory
& lab o
ffic
es.
!!"
!!"
!!"
!!"
!!"
!!"
?!"
Yes
10
Convers
ion
of oth
er
build
ings (
eg
Pharm
acy/IC
U/C
SS
D)
to p
rovid
e 4
th
ea
tres, re
cove
ry a
nd
supp
ort
a
cco
mm
od
atio
n.
!!"
!!"
!!"
!!"
X
X
!"
?
?
No

Theatres 1 – 4 Craigavon Area Hospital 60
The short listing exercise indicates that options 7, 8, and 9 comply with the majority of objectives and constraints and have therefore been carried forward for further evaluation. Option 2 would meet some of the project objectives and is being taken forward as a base case comparator, in accordance with the guidance set out in HM Treasury Green Book (The Green Book, Appraisal and Evaluation in Central Government, Treasury Guidance, 2003). Option 3 has also been short listed. Although it does not meet all of the objectives and constraints, it enables the Trust to evaluate a range of different levels of solution in line with the guidance.
Short Listed Options
Option 2 - Do Minimum – Minimal refurbishment of existing 4 theatres, replacing the ventilation system and upgrading the electrical supply.
This option proposes conducting the minimum work required to the existing theatres to meet some of the requirements of the HBN and HTM guidance. It would involve refurbishment to the existing four theatres to include the replacement of the ventilation system and upgrade the electricity supply. This would enable some of the theatre standards to be met however it would not address the issue of the size of theatres or preparation rooms (refurbished theatres would be 40 sq metres compared to the new HBN standard of a minimum 55 sq metres). Also preparation rooms would continue to be shared between two theatres. This option would therefore not support a full range of surgical procedures. There is no potential to upgrade the existing recovery ward with this option. The current bed spacing is considerably less than the recommended bed spacing of 3.6m for multi bed areas. There would be no upgrade to the staff changing area which is cramped and inadequate and no provision to expand the current inadequate storage.
Clinical adjacencies are good as the theatres remain adjacent to the existing support infrastructure, such as recovery ward and the intensive care unit and existing hospital estate would continue to be utilised
Of major concern to the Trust is the significant disruption which would result from the works within the main theatre suite. Two theatres would have to remain fully operational whilst works are being carried out within the same area. It would also be difficult to locate decant accommodation due to site constraints and the decant accommodation would have to be some distance from the theatre support accommodation and remaining two theatres. This arrangement would lead to operational difficulties and would inevitably impact on the Trust’s ability to provide the current level of theatre services. This would have a knock on effect to achievement of access standards or alternatively significant one-off costs would be incurred if this activity has to be displaced to the independent sector for the period of the refurbishment.
Theatres 1 – 4 Craigavon Area Hospital 61
Option 2 would not release any space to support the development of services within the Trust for example the expansion of urology, ENT, gynaecology and pain management services.
Option 3 - Purchase 2 volumetric theatres. Extend the theatre block into a courtyard & refurbish to provide 2 theatres, new recovery, upgraded staff changing and additional storage.
This option meets some but not all of the project objectives and constraints. The two volumetric theatres and two refurbished theatres would enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and will support a full range of surgical procedures. The necessary support facilities would be provided. A new 18 bed recovery area would be built and would meet the current HBN/HTM requirements including compliance with new bed spacing recommendations for multi bed areas. The staff changing area would be upgraded to provide appropriate accommodation.
Existing hospital estate would continue to be utilised and good clinical adjacencies are maintained as the two volumetric theatres are linked to main theatres.
However this option would result in a high level of disruption to existing theatre services. It could impact on the Trust’s ability to provide the current level of theatre services and therefore has the potential to have an adverse impact on length of stay and the achievement of elective waiting time targets. This is a technically difficult option. It would be necessary to crane materials over occupied buildings into the courtyard to build the extension.
New plant would have to be installed on the roof (of fully functioning theatres) and the existing water tank would have to be removed. Two theatres and recovery ward would continue to be fully functional within the main theatre block whilst work is being carried out.
This option would not release any space to support the development of services within the Trust for example the expansion of urology, ENT, gynaecology and pain management services.
Option 7 - Purchase 2 volumetric theatres and construct 2 theatres. Minor road re-alignment is required. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option meets all of the project objectives and some of the constraints. The two volumetric theatres and two new build theatres will enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and will support a full range of surgical procedures. The necessary support

Theatres 1 – 4 Craigavon Area Hospital 62
facilities will be provided. A new 18 bed recovery area will be created within the existing theatre suite after the theatre activity has moved to the two volumetric and two new build theatres. The new recovery will meet the current HBN/HTM requirements including compliance with new bed spacing recommendations. The staff changing area will be upgraded to provide appropriate accommodation and additional storage will be provided.
The disruption to theatre services will be minimal. Construction of the two new build theatres and upgrade work to the two volumetric theatres can commence when the T & O service transfers to its new facility. Upgrade work to the two volumetric theatres will be completed first and when these have been commissioned sessions from two existing theatres will transfer. The temporary volumetric staff changing and recovery ward units will be removed from the site to enable construction of the two new build theatres (these will no longer be required at that stage). Operating sessions from the two remaining theatres will transfer to the new build theatres when construction and commissioning of these has been completed. Work to construct the new recovery ward and to upgrade the staff changing will not commence until all four theatres have moved.
There is some use of existing estate – the temporary volumetric theatres will be used and recovery, staff changing and other support accommodation will continue to be located within the existing theatre block.
Clinical adjacencies are generally good with this option. However new theatre 4 is some distance from recovery and ICU. This would make monitoring of recovering patients by Anaesthetists in this theatre more difficult (at present the anaesthetists are close to recovery when in theatre and can quickly respond to an emergency situation).
Space would be released within the theatre suite which could be developed to provide other facilities such as an admissions unit to enable elective patients to be admitted to the theatre suite on the day of their procedure. This option would therefore support the development of services within the Trust for example the expansion of urology, ENT, gynaecology and pain management services.
Option 8 - Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage.
This option meets all of the project objectives and the majority of constraints. The two volumetric theatres, the refurbished theatre and the new build theatre will enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and will support a full range of surgical procedures. The necessary support facilities will be provided. A new 18 bed recovery area will be created within the existing theatre suite. The new recovery will meet the current HBN/HTM requirements including compliance with new bed spacing recommendations for multi bed accommodation. The staff changing area will

Theatres 1 – 4 Craigavon Area Hospital 63
be upgraded to provide appropriate accommodation and additional storage will be provided.
The disruption to theatre services will be minimal. Construction of the new build theatre and upgrade work to the two volumetric theatres can commence when the T & O service transfers to its new facility. Upgrade work to the two volumetric theatres will be completed first and when these have been commissioned sessions from two existing theatres will transfer. The temporary volumetric T&O recovery unit would be removed from the site to allow construction of the new build theatre. Operating sessions from a third theatre will transfer to the new build theatre when construction and commissioning of this has been completed. Work to construct the fourth theatre will be undertaken when the first three have moved and following this refurbishment to provide a new recovery ward and to upgrade the staff changing will be undertaken.
There is good use of existing estate as one theatre, recovery ward, staff changing and other support accommodation will continue to be located within the existing theatre block. The temporary volumetric theatres will also continue to be utilised.
Clinical adjacencies are good with this option. The four theatres are located together and the new build theatre adjoins new theatre 5. All are convenient to the new recovery ward and a short distance from ICU.
Space would be released within the theatre suite which could be developed to provide other facilities such as an admissions unit to enable elective patients to be admitted to the theatre suite on the day of their procedure. This option would therefore support the development of services within the Trust for example the expansion of urology, ENT, gynaecology and pain management services.
Option 9 - Construct 4 new theatres and new recovery ward, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide upgraded staff changing and additional storage.
This option meets all of the project objectives and partially meets some of the constraints. The four new build theatres will enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and will support a full range of surgical procedures. The necessary support facilities will be provided. A new 18 bed recovery area will be built and will meet the current HBN/HTM requirements including compliance with new bed spacing recommendations. Staff changing and additional storage will be provided in the new build accommodation.
The disruption to theatre services will be minimal as theatre sessions will not transfer until the construction of the new theatres and recovery ward has been
Theatres 1 – 4 Craigavon Area Hospital 64
completed and the new facilities have been commissioned. There will be some disruption to laboratory services as the histocytology laboratory, laboratory reception, and some laboratory office accommodation occupies the proposed site for the new build theatres and recovery. This accommodation would have to be re-provided and services moved before the site could be cleared for construction. This option will therefore be slower to implement than some of the other options.
There is limited use of existing accommodation – only staff changing and some support accommodation will be located within the existing theatre footprint.
Clinical adjacencies within theatres are generally good with this option. The four new theatres are together and adjacent to recovery ward. The new recovery ward is also convenient to new theatre 5. However the new theatres are much further away from ICU than the current theatres.
Space would be released within the theatre suite which could be developed to provide other facilities such as an admissions unit to enable elective patients to be admitted to the theatre suite on the day of their procedure. This option would therefore support the development of services within the Trust for example the expansion of urology, ENT, gynaecology and pain management services.
Eliminated Options
Options 1, 4, 5, 6 and 10 have been eliminated at the short listing stage. The reasoning is provided in the paragraphs which follow.
Option 1 - Do Nothing
This option does not meet the majority of the project objectives. The HBN and HTM requirements in terms of theatre environment would not be met. Air change rates, theatre size standards and bed spacing in recovery ward would not be improved and therefore the clinical risk would not be reduced. The condition of the theatre suite and associated infrastructure will continue to deteriorate as time progresses, even with scheduled maintenance. The theatre suite will therefore not support more complex and high risk surgery. Ensuring an uninterrupted service would become increasingly difficult as on-going maintenance becomes necessary on a more regular basis.
Option 1 does not provide all the necessary support facilities. Separate preparation rooms would not be provided for each theatre. The current staff changing facilities would not be upgraded and there would be no space to provide additional storage so equipment and consumables would continue to be stored in inappropriate areas.
Theatres 1 – 4 Craigavon Area Hospital 65
This option would not release any space to support the development of services within the Trust for example the expansion of urology, ENT, gynaecology and pain management services.
Given the critical state of the main theatres, the Trust does not consider ‘do nothing’ to be an acceptable course of action. As there is an appropriate ‘do minimum’ option which can be used as a baseline comparator, and with the agreement of the Health Economists at the DHSSPS, option 1 has not been taken forward for further analysis.
Option 4 - Construct 4 new theatres, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option does not meet all of the project objectives, nor comply with all of the constraints. The four new theatres would enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and will support a full range of surgical procedures. The necessary support facilities would be provided. A new 18 bed recovery area would be provided within the current main theatres block and would meet the current HBN/HTM requirements including compliance with new bed spacing recommendations. The current staff changing area would be upgraded to provide appropriate accommodation and additional storage would be provided.
There would be minimal disruption to existing theatres while the new theatres are constructed. The impact of refurbishing existing theatre accommodation to provide a new recovery ward and upgraded staff changing can also be minimised. Although disruption to theatre services would be minimised there would be disruption to laboratory services as new accommodation would have to be built for histocytology laboratory in order to clear the proposed site. This option would also take longer to implement due to the need to build laboratory accommodation first. In addition, laboratory services are currently sited together and this option would result in histocytology being located on another part of the site.
There is very little use of existing accommodation – only recovery, staff changing and some support accommodation would be located within the existing theatre footprint.
Clinical adjacencies are poor with option 4. The new theatres are much further away from recovery and ICU than at present. The distance from recovery ward is of particular concern to clinical staff as this would make monitoring of recovering patients by anaesthetists much more difficult (at present anaesthetists are close to recovery when in theatre and can quickly respond to an emergency situation).
Theatres 1 – 4 Craigavon Area Hospital 66
Option 5 - Purchase 2 volumetric theatres and construct 2 new theatres. Displace and re-provide CSSD plant room space. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option meets some of the project objectives. The two volumetric theatres and two refurbished theatres would enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and would support a full range of surgical procedures. The necessary support facilities would be provided. A new 18 bed recovery area will be built and would meet the current HBN/HTM requirements including compliance with new bed spacing recommendations. The staff changing area would be upgraded to provide appropriate accommodation and additional storage would be provided.
There is some use of existing estate – the temporary volumetric theatres would be used and recovery, staff changing and other support accommodation would continue to be located within the existing theatre block.
Clinical adjacencies are acceptable with this option. Theatres 1 – 4 are close to the new recovery ward. The distance to ICU is acceptable. However the adjacencies between theatres 2, 3 and 4 are not as good as that provided by some of the other options.
There would be relatively little disruption to existing theatres while the new theatres are constructed. The impact of refurbishing existing theatre accommodation to provide a new recovery ward and upgraded staff changing can also be minimised. Although disruption to theatre services would be minimised the disruption to CSSD would be significant as part of the CSSD plant room would be displaced. The CSSD plant has recently been extended to enable the service to meet the decontamination needs for main theatres, day surgery and other clinical areas within the hospital. There is no other suitably located site to re-provide this plant space and therefore this option would in reality involve re-providing the sterile services department at another location. This option would also take longer to implement due to the need to re-provide and move the CSSD department.
Given that there are an acceptable number of other options which will not require such significant disruption to another key department, this option has not been short listed for further evaluation.
Theatres 1 – 4 Craigavon Area Hospital 67
Option 6 - Purchase 2 volumetric theatres and construct 2 new theatres. Displace and re-provide the biochemistry laboratory. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
This option meets some of the project objectives. The two volumetric theatres and two refurbished theatres would enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and will support a full range of surgical procedures. The necessary support facilities would be provided. A new 18 bed recovery area would be built and would meet the current HBN/HTM requirements including compliance with new bed spacing recommendations. The staff changing area would be upgraded to provide appropriate accommodation and additional storage would be provided.
There is some use of existing estate – the temporary volumetric theatres would be used and recovery, staff changing and other support accommodation will continue to be located within the existing theatre block.
Clinical adjacencies are good with this option. Theatres 1 – 4 are located together and are close to the new recovery ward. The distance to ICU is acceptable.
There would be relatively little disruption to existing theatres while the new theatres are constructed. The impact of refurbishing existing theatre accommodation to provide a new recovery ward and upgraded staff changing can also be minimised. Although disruption to theatre services would be minimised the disruption to laboratory services would be significant. Part of the biochemistry laboratory occupies the proposed site for the two new build theatres. The biochemistry analyser is a large piece of equipment which along with its necessary support accommodation requires a significant footprint. This accommodation would have to be re-provided in another suitable location on the hospital site. The analyser processes approximately 750,000 laboratory samples each year. It could not be dismantled and moved either easily or quickly and the resultant downtime would have a high impact on both hospital and primary care services. This option would also take longer to implement due to the need to re-provide biochemistry. For these reasons option 6 has not been shortlisted for further consideration.
Theatres 1 – 4 Craigavon Area Hospital 68
Option 10 - Conversion of another building — eg Pharmacy, Intensive Care Unit and/ or Central Sterile Service Department to provide 4 theatres, recovery and support accommodation. Re-provide accommodation for displaced services.
This option could meet some of the project objectives. Conversion of existing buildings could provide theatres and associated accommodation that would enable the Trust to meet all the HBN and HTM requirements in terms of theatre environment and would support a full range of surgical procedures. The necessary support facilities could be provided.
There is the potential to minimise disruption to existing theatres while the new theatres are constructed. However as this option involves displacing Pharmacy, ICU and/or CSSD this would cause significant disruption to these and other dependent services and would have the potential to adversely affect current clinical adjacencies (such as adjacency of theatres to ICU or CSSD). This option would also take longer to implement due to the need to re-provide displaced departments before building of the new theatre accommodation could take place. For these reasons option 10 has been eliminated.

Theatres 1 – 4 Craigavon Area Hospital 69
8 NON FINANCIAL APPRAISAL OF SHORTLISTED OPTIONS In the previous chapters the long list of potential options for the project was described, the methodology employed to arrive at an appropriate short-list, and reasons for excluding options from the short-list were explained. This chapter evaluates each of the short-listed options based on a non-financial assessment using benefit criteria.
8.1 Benefit Criteria
Benefit criteria are used to select and evaluate the options that have the potential to meet the specific project objectives. Although cost is an important evaluative determinant, it represents only one of a number of issues, which will impact on the value to be provided from that particular option. In addition, it is the case that not all costs or benefits can be measured in monetary terms, as no market value exists for them. Taking into account the objectives of the proposed project, a list of salient benefits has been devised which could accrue from the project if implemented successfully. The criteria employed to select and evaluate the options are given below and explained overleaf.
! Clinical effectiveness;
! Quality of accommodation;
! Strategic fit;
! Avoidance of disruption;
! Speed of Implementation.
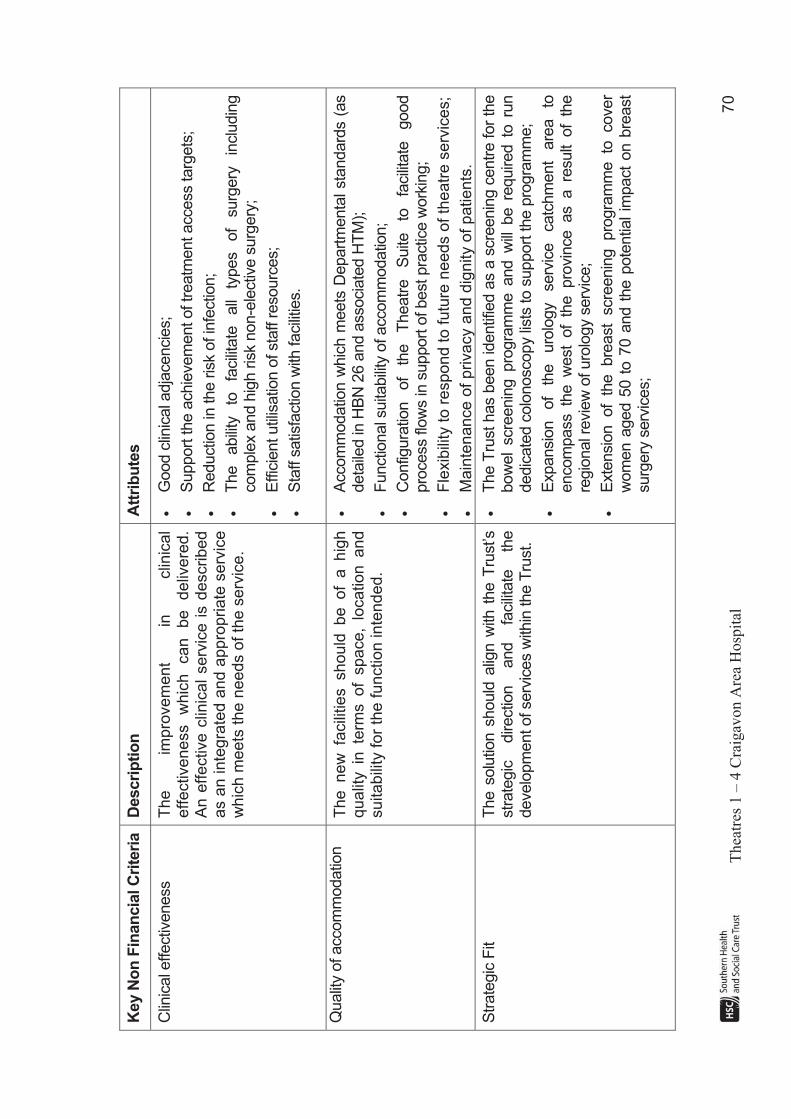
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
70
Key N
on
Fin
an
cia
l C
rite
ria
Descri
pti
on
A
ttri
bu
tes
Clin
ical e
ffectiv
eness
The
impro
vem
ent
in
clin
ica
l effectiveness
whic
h
can
be
deliv
ere
d.
A
n e
ffective c
linic
al
serv
ice i
s d
escribe
d
as a
n inte
gra
ted a
nd a
ppro
priate
serv
ice
whic
h m
eets
the n
eeds o
f th
e s
erv
ice.
!G
ood c
linic
al a
dja
cencie
s;
!S
upport
the a
chie
vem
ent of tr
eatm
ent access targ
ets
;
!R
eductio
n in
the r
isk o
f in
fectio
n;
!T
he
abili
ty
to
facili
tate
all
types
of
surg
ery
in
clu
din
g
com
ple
x a
nd h
igh r
isk n
on-e
lectiv
e s
urg
ery
;
!E
ffic
ient util
isatio
n o
f sta
ff r
esourc
es;
!S
taff s
atis
factio
n w
ith facili
ties.
Qualit
y o
f accom
modatio
n
The new
fa
cili
ties should
be of
a hig
h
qualit
y in
te
rms of
space,
location and
su
ita
bili
ty f
or
the
fu
nctio
n in
ten
de
d.
!A
ccom
modatio
n w
hic
h m
eets
Depart
menta
l sta
ndard
s (
as
deta
iled in
HB
N 2
6 a
nd a
ssocia
ted H
TM
);
!F
unctio
nal s
uita
bili
ty o
f accom
modatio
n;
!C
onfig
ura
tion
of
the
Theatr
e
Suite
to
fa
cili
tate
good
pro
cess flo
ws in
support
of best pra
ctic
e w
ork
ing;
!F
lexib
ility
to
re
sp
on
d t
o f
utu
re n
ee
ds o
f th
ea
tre
se
rvic
es;
!M
ain
tenance o
f privacy a
nd d
ignity o
f patients
.
Str
ate
gic
Fit
The s
olu
tion s
hould
alig
n w
ith t
he T
rust’s
str
ate
gic
directio
n
and
facili
tate
th
e
develo
pm
ent of serv
ices w
ithin
the T
rust.
!T
he T
rust has b
een identif
ied a
s a
scre
enin
g c
entr
e for
the
bow
el
scre
enin
g p
rogra
mm
e a
nd w
ill b
e r
equired t
o r
un
dedic
ate
d c
olo
noscopy li
sts
to s
upport
the p
rogra
mm
e;
!E
xpansio
n
of
the
uro
logy
serv
ice
catc
hm
ent
are
a
to
encom
pass th
e w
est
of
the pro
vin
ce as a re
sult
of
the
regio
nal r
evie
w o
f uro
logy s
erv
ice;
!E
xte
nsio
n of
the bre
ast
scre
enin
g pro
gra
mm
e to
cover
wom
en a
ged 5
0 t
o 7
0 a
nd t
he p
ote
ntia
l im
pact
on b
reast
surg
ery
serv
ices;
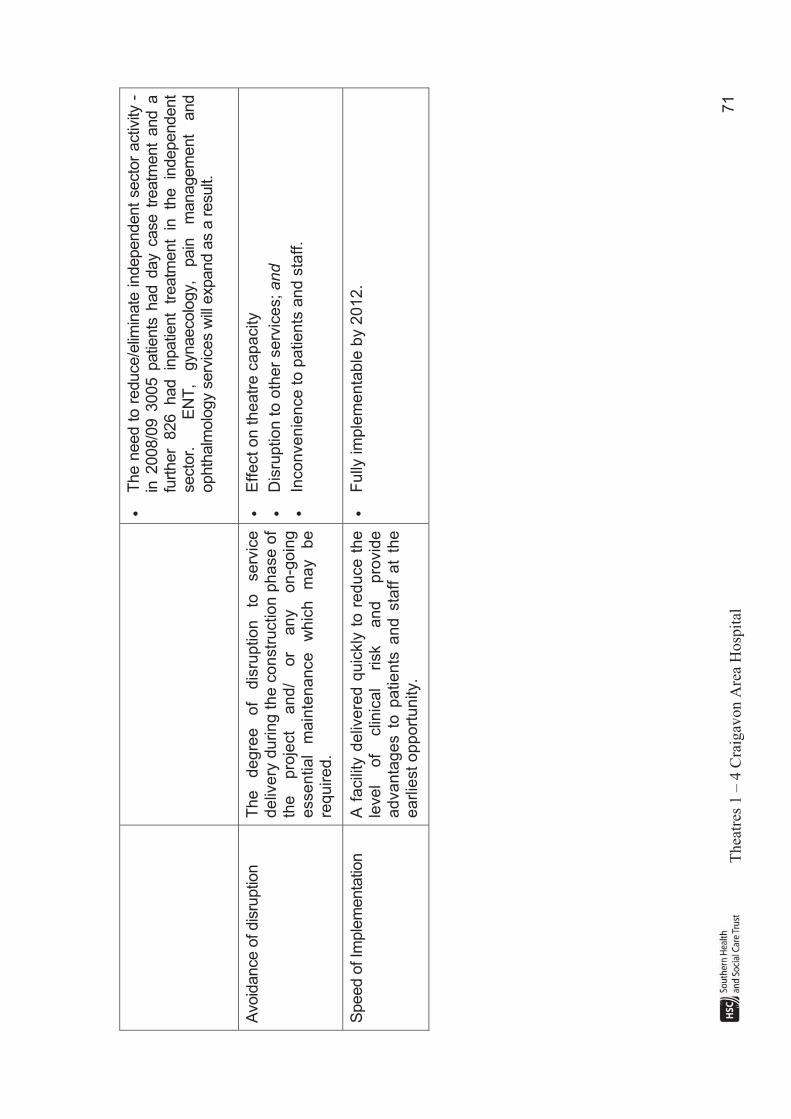
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
71
!T
he n
eed t
o r
educe/e
limin
ate
independent
secto
r activ
ity -
in
2008/0
9 3
005 p
atie
nts
had d
ay c
ase t
reatm
ent
and a
fu
rther
826
had
inpatie
nt
treatm
ent
in
the
independent
secto
r.
E
NT
, gynaecolo
gy,
pain
m
anagem
ent
and
ophth
alm
olo
gy s
erv
ices w
ill e
xpand a
s a
result.
Avoid
ance o
f dis
ruptio
n
The
degre
e
of
dis
ruption
to
serv
ice
deliv
ery
during t
he c
onstr
uction p
hase o
f th
e
pro
ject
an
d/
or
an
y
on
-go
ing
essential
main
tenan
ce
whic
h
may
be
req
uire
d.
!E
ffect
on t
heatr
e c
apacity
!D
isru
ption t
o o
ther
serv
ices; and
!In
co
nve
nie
nce
to
pa
tie
nts
an
d s
taff
.
Speed o
f Im
ple
menta
tion
A f
acili
ty d
eliv
ere
d q
uic
kly
to r
ed
uce t
he
level
of
clin
ical
risk
and
pro
vid
e
ad
va
nta
ge
s t
o p
atie
nts
an
d s
taff
at
the
e
arlie
st
op
po
rtu
nity.
!F
ully
im
ple
me
nta
ble
by 2
01
2.
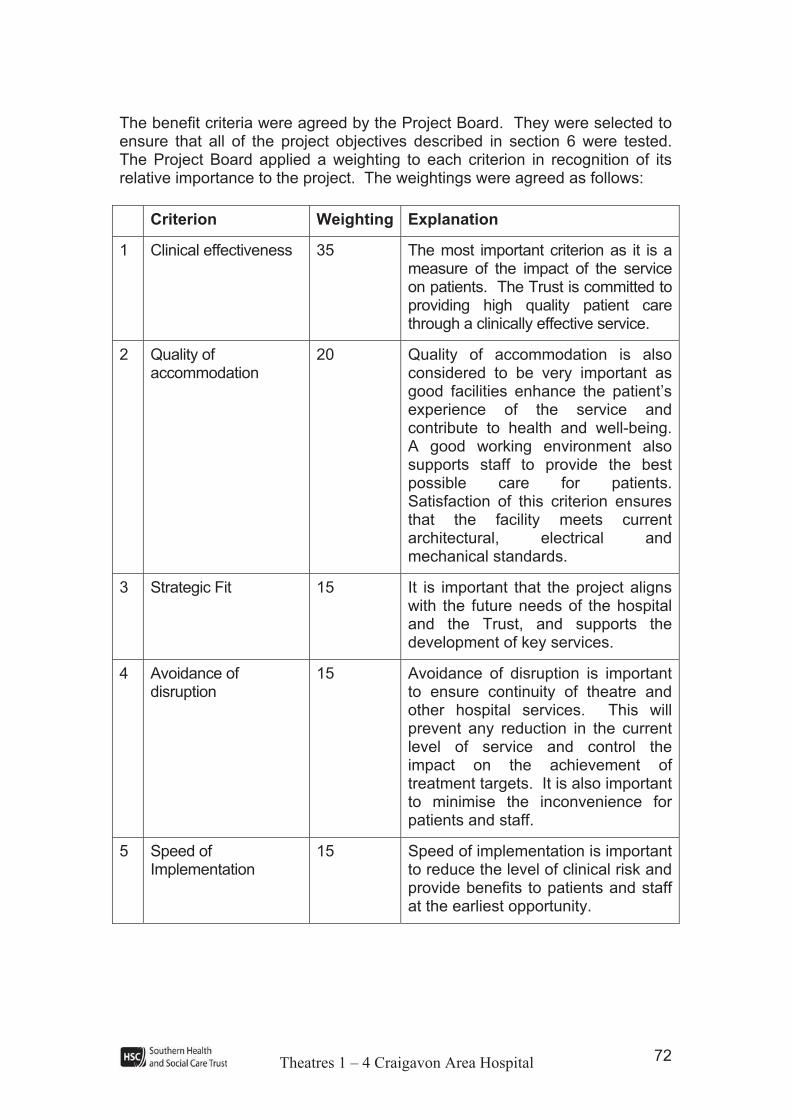
Theatres 1 – 4 Craigavon Area Hospital 72
The benefit criteria were agreed by the Project Board. They were selected to ensure that all of the project objectives described in section 6 were tested. The Project Board applied a weighting to each criterion in recognition of its relative importance to the project. The weightings were agreed as follows:
Criterion Weighting Explanation
1 Clinical effectiveness 35 The most important criterion as it is a measure of the impact of the service on patients. The Trust is committed to providing high quality patient care through a clinically effective service.
2 Quality of accommodation
20 Quality of accommodation is also considered to be very important as good facilities enhance the patient’s experience of the service and contribute to health and well-being. A good working environment also supports staff to provide the best possible care for patients. Satisfaction of this criterion ensures that the facility meets current architectural, electrical and mechanical standards.
3 Strategic Fit 15 It is important that the project aligns with the future needs of the hospital and the Trust, and supports the development of key services.
4 Avoidance of disruption
15 Avoidance of disruption is important to ensure continuity of theatre and other hospital services. This will prevent any reduction in the current level of service and control the impact on the achievement of treatment targets. It is also important to minimise the inconvenience for patients and staff.
5 Speed of Implementation
15 Speed of implementation is important to reduce the level of clinical risk and provide benefits to patients and staff at the earliest opportunity.
Theatres 1 – 4 Craigavon Area Hospital 73
8.2 Scoring the Options
Scoring of the options was carried out by the Project Board. The four short-listed options, along with the ‘do minimum’ option were evaluated using the agreed criteria and the weighted scores detailed in Table 12 were calculated. The maximum score for each criterion was 10.

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
74
Ta
ble
12:
Sco
rin
g o
f S
ho
rt L
iste
d O
pti
on
s 2D
o M
inim
um
3 2
Volu
metr
ic &
2
inte
rnal re
furb
ishm
ent
72 v
olu
metr
ic,
2 n
ew
build
- m
inor
road r
e-
alig
nm
ent
82 v
olu
metr
ic,
1
inte
rnal re
furb
ishm
ent,
1 n
ew
build
9N
ew
build
4
theatr
es &
reco
very
, d
isp
lace
hysto
cyto
la
b &
offic
es
Cri
teri
on
W
eig
ht
Score
S
core
x
Weig
ht
Score
S
core
x
Weig
ht
Score
S
core
x
Weig
ht
Score
S
core
x
Weig
ht
Score
S
core
x
Weig
ht
1
Clin
ica
l E
ffectiveness
40
6
2
40
9
3
60
7
2
80
9
3
60
7
2
80
2
Qualit
y o
f A
ccom
mo
da
tio
n
20
4
8
0
8
16
0
8
16
0
8
16
0
9
18
0
3
Str
ate
gic
Fit
15
5
7
5
5
75
8
1
20
7
1
05
9
1
35
4
Avoid
ance o
f D
isru
ption
15
5
7
5
6
90
8
1
20
7
1
05
7
1
05
5
Sp
ee
d o
f Im
ple
menta
tion
10
3
3
0
5
50
7
7
0
4
40
3
3
0
To
tals
10
05
00
73
57
50
77
07
30
RA
NK
ING
5
32
14

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
75
Exp
lan
ati
on
of
the S
co
res
Cri
teri
on
1 –
Clin
ical E
ffecti
ven
ess
Op
tio
n
Sco
re
Exp
lan
ati
on
2D
o
Min
imum
–
Min
imal
refu
rbis
hm
ent
of
exis
ting
4
theatr
es,
repla
cin
g
the
ventil
atio
n
syste
m
and
upgra
din
g
the
ele
ctr
ical
supply
.
6! C
linic
al
adja
cencie
s a
re g
ood.
The t
heatr
es a
re a
dja
cent
to e
xis
ting s
upport
infr
astr
uctu
re
such a
s r
ecovery
ward
and IC
U;
! In
tegra
tion b
etw
een t
he 4
theatr
es,
new
theatr
e 5
and t
he n
ew
T&
O t
heatr
es i
s g
ood a
nd
good flo
ws w
ithin
the theatr
e c
om
ple
x a
re e
nable
d w
hic
h w
ill facili
tate
the e
ffic
ient util
isatio
n o
f sta
ff;
! T
his
optio
n s
core
d l
ow
er
than t
he o
ther
short
lis
ted o
ptio
ns b
ecause a
lthough t
he r
isk o
f in
fectio
n w
ould
be r
educed d
ue t
o t
he insta
llatio
n o
f new
ventil
atio
n e
quip
ment, e
ach p
air o
f th
eatr
es w
ould
contin
ue t
o s
hare
a p
repara
tion a
rea.
In a
dditi
on,
the 4
theatr
es w
ill s
till only
be 4
0 m
2 w
hic
h is
consid
era
bly
sm
alle
r th
an the c
urr
ent m
inim
um
recom
mended s
ize o
f 55m
2;
! A
lthough a
n im
pro
vem
ent
on t
he c
urr
ent
facili
ties,
sta
ff a
re lik
ely
to b
e less s
atis
fied w
ith t
his
optio
n than w
ith the o
ther
short
liste
d o
ptio
ns.
3P
urc
hase
2
volu
metr
ic
theatr
es.
E
xte
nd
theatr
e
blo
ck
into
court
yard
&
re
furb
ish
to
pro
vid
e
2
theatr
es,
new
re
covery
, upgra
ded sta
ff changin
g and
additi
onal s
tora
ge.
9! C
linic
al
adja
cencie
s a
re g
ood.
The t
heatr
es a
re a
dja
cent
to e
xis
ting s
upport
infr
astr
uctu
re
such a
s r
ecovery
ward
and IC
U;
! In
tegra
tion b
etw
een t
he 4
theatr
es,
new
theatr
e 5
and t
he n
ew
T&
O t
heatr
es i
s g
ood a
nd
good flo
ws w
ithin
the theatr
e c
om
ple
x a
re e
nable
d w
hic
h w
ill facili
tate
the e
ffic
ient util
isatio
n o
f sta
ff;
! R
isk o
f in
fectio
n w
ould
be s
ignifi
cantly
reduced w
ith t
his
optio
n.
In a
dditi
on t
o n
ew
ventil
atio
n
equip
ment
whic
h w
ill f
acili
tate
air c
hange r
ate
s w
hic
h a
re c
om
plia
nt
with
HB
N 2
6,
this
optio
n
will
pro
vid
e th
eatr
es w
hic
h are
com
plia
nt
in
term
s
of
siz
e
and
support
accom
modatio
n
inclu
din
g s
epara
te p
repara
tion r
oom
s for
each theatr
e;
! T
his
optio
n w
ill p
rovid
e a
facili
ty w
hic
h w
ill s
upport
the a
chie
vem
ent of access targ
ets
;
! S
taff w
ill b
e a
ble
to d
eliv
er
a s
erv
ice fro
m m
odern
, fit
for
purp
ose theatr
e a
ccom
modatio
n a
nd
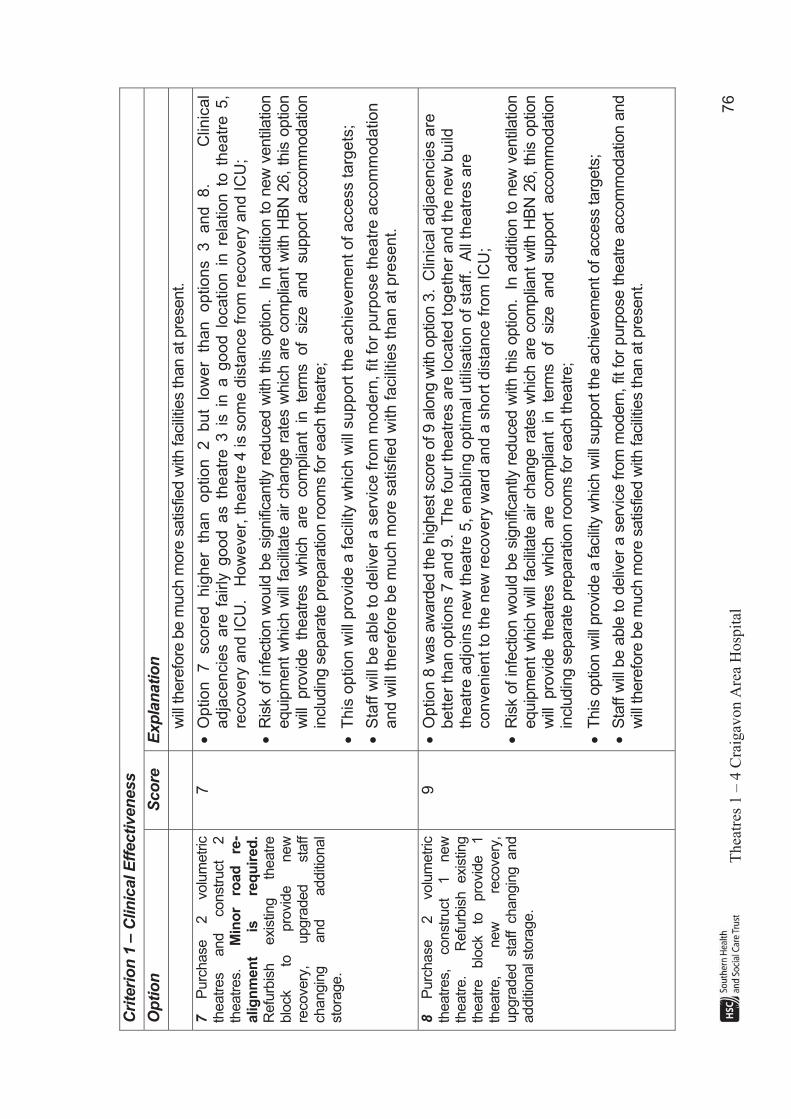
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
76
Cri
teri
on
1 –
Clin
ical E
ffecti
ven
ess
Op
tio
n
Sco
re
Exp
lan
ati
on
will
there
fore
be m
uch m
ore
satis
fied w
ith facili
ties than a
t pre
sent.
7P
urc
hase
2
volu
metr
ic
theatr
es
and
constr
uct
2
theatr
es.
M
ino
r ro
ad
re
-alig
nm
en
t is
re
qu
ired
.R
efu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e
new
re
covery
, upgra
ded
sta
ff
changin
g
and
additi
onal
sto
rage.
7! O
ption
7
score
d
hig
her
than
op
tio
n
2
bu
t lo
we
r th
an
o
ptio
ns
3
an
d
8.
C
linic
al
adja
cencie
s a
re f
airly
good a
s t
heatr
e 3
is i
n a
good l
ocation i
n r
ela
tion t
o t
heatr
e 5
, re
co
ve
ry a
nd
IC
U.
H
ow
eve
r, t
he
atr
e 4
is s
om
e d
ista
nce f
rom
recovery
and I
CU
;
! R
isk o
f in
fectio
n w
ould
be s
ignifi
cantly
reduced w
ith t
his
optio
n.
In a
dditi
on t
o n
ew
ventil
atio
n
equip
ment
whic
h w
ill f
acili
tate
air c
hange r
ate
s w
hic
h a
re c
om
plia
nt
with
HB
N 2
6,
this
optio
n
will
pro
vid
e th
eatr
es w
hic
h are
com
plia
nt
in
term
s
of
siz
e
and
support
accom
modatio
n
inclu
din
g s
epara
te p
repara
tion r
oom
s for
each theatr
e;
! T
his
option
will
pro
vid
e a
facili
ty w
hic
h w
ill s
upport
the a
chie
vem
ent
of
access t
arg
ets
;
! S
taff w
ill b
e a
ble
to d
eliv
er
a s
erv
ice f
rom
modern
, fit
for
purp
ose t
heatr
e a
ccom
modation
and w
ill t
he
refo
re b
e m
uch m
ore
satisfied w
ith f
acili
ties t
han a
t pre
sent.
8P
urc
hase
2
volu
metr
ic
theatr
es,
constr
uct
1
new
th
eatr
e.
Refu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e
1
theatr
e,
new
re
covery
, upgra
ded sta
ff changin
g and
additi
onal s
tora
ge.
9! O
ption 8
was a
ward
ed the h
ighest score
of 9 a
long w
ith o
ptio
n 3
. C
linic
al adja
cencie
s a
re
better
than o
ptions 7
and 9
. T
he f
our
theatr
es a
re locate
d t
ogeth
er
and t
he n
ew
build
th
eatr
e a
djo
ins n
ew
th
eatr
e 5
, enablin
g o
ptim
al utilis
ation o
f sta
ff.
All
theatr
es a
re
convenie
nt
to t
he n
ew
recovery
ward
an
d a
sh
ort
dis
tan
ce
fro
m I
CU
;
! R
isk o
f in
fectio
n w
ould
be s
ignifi
cantly
reduced w
ith t
his
optio
n.
In a
dditi
on t
o n
ew
ventil
atio
n
equip
ment
whic
h w
ill f
acili
tate
air c
hange r
ate
s w
hic
h a
re c
om
plia
nt
with
HB
N 2
6,
this
optio
n
will
pro
vid
e th
eatr
es w
hic
h are
com
plia
nt
in te
rms of
siz
e
and
support
accom
modatio
n
inclu
din
g s
epara
te p
repara
tion r
oom
s for
each theatr
e;
! T
his
optio
n w
ill p
rovid
e a
facili
ty w
hic
h w
ill s
upport
the a
chie
vem
ent of access targ
ets
;
! S
taff w
ill b
e a
ble
to d
eliv
er
a s
erv
ice fro
m m
odern
, fit
for
purp
ose theatr
e a
ccom
modatio
n a
nd
will
there
fore
be m
uch m
ore
satis
fied w
ith facili
ties than a
t pre
sent.
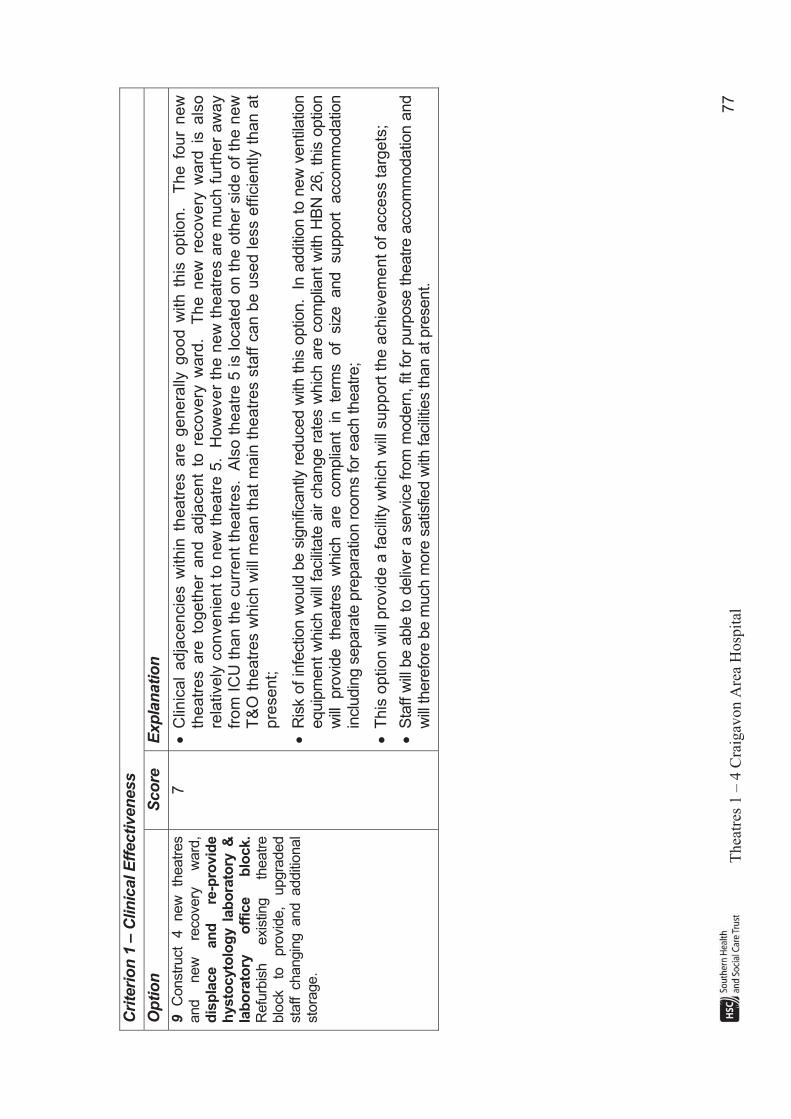
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
77
Cri
teri
on
1 –
Clin
ical E
ffecti
ven
ess
Op
tio
n
Sco
re
Exp
lan
ati
on
9C
onstr
uct
4
new
th
eatr
es
and
new
re
covery
w
ard
,d
isp
lace
an
d
re-p
rovid
e
hysto
cyto
log
y l
ab
ora
tory
&
lab
ora
tory
o
ffic
e
blo
ck.
Refu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e,
upgra
ded
sta
ff changin
g and additi
onal
sto
rage.
7! C
linic
al
ad
jace
ncie
s w
ith
in t
he
atr
es a
re g
en
era
lly g
ood
with
this
op
tio
n.
Th
e f
ou
r n
ew
th
eatr
es a
re t
ogeth
er
and a
dja
cent
to r
ecovery
ward
. T
he n
ew
recovery
ward
is a
lso
re
latively
convenie
nt
to n
ew
theatr
e 5
. H
ow
ever
the n
ew
theatr
es a
re m
uch f
urt
her
aw
ay
from
IC
U t
han t
he c
urr
ent
theatr
es.
Als
o t
he
atr
e 5
is lo
ca
ted o
n t
he o
ther
sid
e o
f th
e n
ew
T
&O
theatr
es w
hic
h w
ill m
ean t
hat
main
theatr
es s
taff c
an b
e u
se
d less e
ffic
iently t
han a
t p
rese
nt;
! R
isk o
f in
fectio
n w
ould
be s
ignifi
cantly
reduced w
ith t
his
optio
n.
In a
dditi
on t
o n
ew
ventil
atio
n
equip
ment
whic
h w
ill f
acili
tate
air c
hange r
ate
s w
hic
h a
re c
om
plia
nt
with
HB
N 2
6,
this
optio
n
will
pro
vid
e th
eatr
es w
hic
h are
com
plia
nt
in
term
s
of
siz
e
and
support
accom
modatio
n
inclu
din
g s
epara
te p
repara
tion r
oom
s for
each theatr
e;
! T
his
option
will
pro
vid
e a
facili
ty w
hic
h w
ill s
upport
the a
chie
vem
ent
of
access t
arg
ets
;
! S
taff w
ill b
e a
ble
to d
eliv
er
a s
erv
ice fro
m m
odern
, fit
for
purp
ose theatr
e a
ccom
modatio
n a
nd
will
there
fore
be m
uch m
ore
satis
fied w
ith facili
ties than a
t pre
sent.
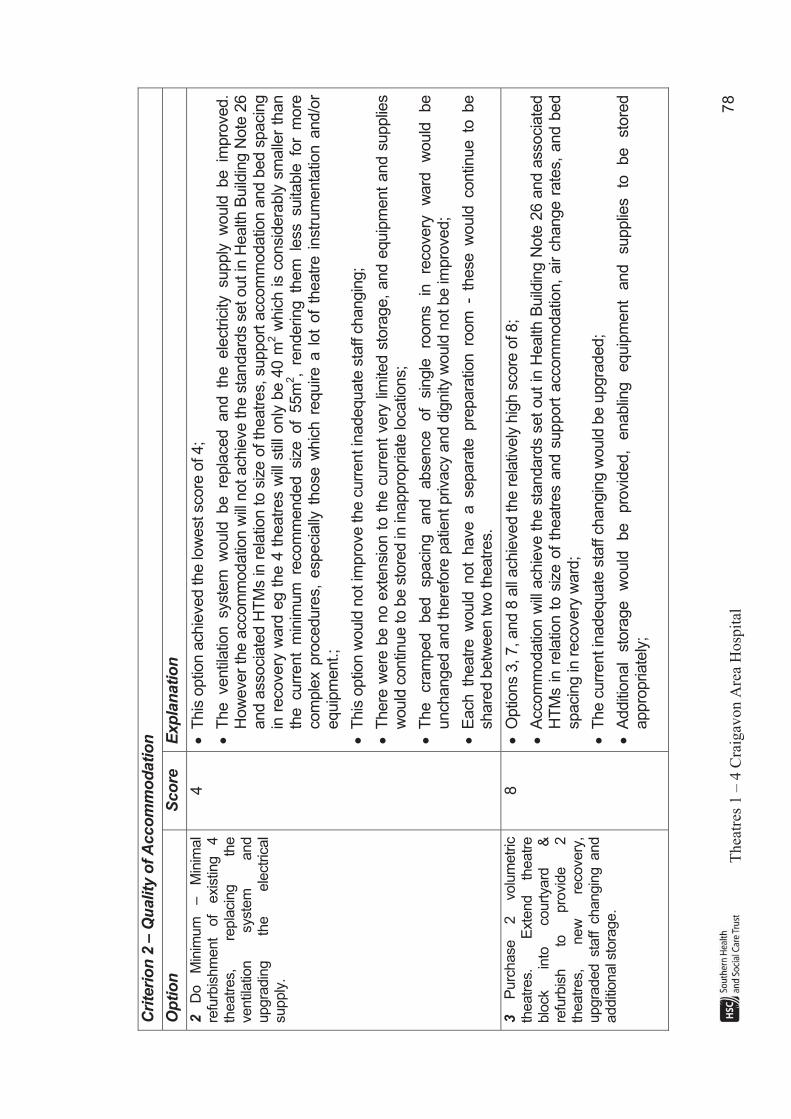
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
78
Cri
teri
on
2 –
Qu
ality
of
Acco
mm
od
ati
on
Op
tio
n
Sco
re
Exp
lan
ati
on
2D
o
Min
imum
–
Min
imal
refu
rbis
hm
ent
of
exis
ting
4
theatr
es,
repla
cin
g
the
ventil
atio
n
syste
m
and
upgra
din
g
the
ele
ctr
ical
supply
.
4! T
his
optio
n a
chie
ved the lo
west score
of 4;
! T
he ventil
atio
n syste
m w
ould
be re
pla
ced and th
e ele
ctr
icity
supply
w
ould
be im
pro
ved.
How
ever
the a
ccom
modatio
n w
ill n
ot achie
ve the s
tandard
s s
et out in
Health
Build
ing N
ote
26
and a
ssocia
ted H
TM
s in r
ela
tion to s
ize o
f th
eatr
es, support
accom
modatio
n a
nd b
ed s
pacin
g
in r
ecovery
ward
eg t
he 4
theatr
es w
ill s
till only
be 4
0 m
2 w
hic
h is c
onsid
era
bly
sm
alle
r th
an
the curr
ent
min
imum
re
com
mended siz
e of
55m
2,
rendering th
em
le
ss suita
ble
fo
r m
ore
com
ple
x p
rocedure
s,
especia
lly t
hose w
hic
h r
equire a
lot
of
theatr
e i
nstr
um
enta
tion a
nd/o
r equip
ment.;
! T
his
optio
n w
ould
not im
pro
ve the c
urr
ent in
adequate
sta
ff c
hangin
g;
! T
here
were
be n
o e
xte
nsio
n t
o t
he c
urr
ent
very
lim
ited s
tora
ge,
and e
quip
ment
and s
upplie
s
would
contin
ue to b
e s
tore
d in
inappro
priate
locatio
ns;
! T
he
cra
mped
bed
spacin
g
and
absence
of
sin
gle
ro
om
s
in
recovery
w
ard
w
ould
be
unchanged a
nd there
fore
patie
nt privacy a
nd d
ignity
would
not be im
pro
ved;
! E
ach th
eatr
e w
ould
not
have a separa
te pre
para
tion ro
om
-
these w
ould
contin
ue to
be
share
d b
etw
een tw
o theatr
es.
3P
urc
hase
2
volu
metr
ic
theatr
es.
E
xte
nd
theatr
e
blo
ck
into
court
yard
&
re
furb
ish
to
pro
vid
e
2
theatr
es,
new
re
covery
, upgra
ded sta
ff changin
g and
additi
onal s
tora
ge.
8! O
ptio
ns 3
, 7, and 8
all
achie
ved the r
ela
tively
hig
h s
core
of 8;
! A
ccom
modatio
n w
ill a
chie
ve t
he s
tandard
s s
et
out
in H
ealth
Build
ing N
ote
26 a
nd a
ssocia
ted
HT
Ms in r
ela
tion t
o s
ize o
f th
eatr
es a
nd s
upport
accom
modatio
n,
air c
hange r
ate
s,
and b
ed
spacin
g in
recovery
ward
;
! T
he c
urr
ent in
adequate
sta
ff c
hangin
g w
ould
be u
pgra
ded;
! A
dditi
onal
sto
rage
would
be
pro
vid
ed,
enablin
g
equip
ment
and
supplie
s
to
be
sto
red
appro
priate
ly;

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
79
Cri
teri
on
2 –
Qu
ality
of
Acco
mm
od
ati
on
Op
tio
n
Sco
re
Exp
lan
ati
on
! P
atie
nt
privacy a
nd d
ignity
would
be i
mpro
ved a
s b
ed s
pacin
g i
n r
ecovery
ward
would
be
exte
nded a
nd s
om
e s
ingle
room
s w
ould
be p
rovid
ed.
7P
urc
hase
2
volu
metr
ic
theatr
es
and
constr
uct
2
theatr
es.
M
ino
r ro
ad
re
-alig
nm
en
t is
re
qu
ired
.R
efu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e
new
re
covery
, upgra
ded
sta
ff
changin
g
and
additi
onal
sto
rage.
8! O
ptio
ns 3
, 7, and 8
all
achie
ved the r
ela
tively
hig
h s
core
of 8;
! A
ccom
modatio
n w
ill a
chie
ve t
he s
tandard
s s
et
out
in H
ealth
Build
ing N
ote
26 a
nd a
ssocia
ted
HT
Ms in r
ela
tion t
o s
ize o
f th
eatr
es a
nd s
upport
accom
modatio
n,
air c
hange r
ate
s,
and b
ed
spacin
g in
recovery
ward
;
! T
he c
urr
ent in
adequate
sta
ff c
hangin
g w
ould
be u
pgra
ded;
! A
dditi
onal
sto
rage
would
be
pro
vid
ed,
enablin
g
equip
ment
and
supplie
s
to
be
sto
red
appro
priate
ly;
! P
atie
nt
privacy a
nd d
ignity
would
be i
mpro
ved a
s b
ed s
pacin
g i
n r
ecovery
ward
would
be
exte
nded a
nd s
om
e s
ingle
room
s w
ould
be p
rovid
ed.
8P
urc
hase
2
volu
metr
ic
theatr
es,
constr
uct
1
new
th
eatr
e.
Refu
rbis
h exis
ting
theatr
e
blo
ck
to
pro
vid
e
1
theatr
e,
new
re
covery
, upgra
ded sta
ff changin
g and
additi
onal s
tora
ge.
8! O
ptio
ns 3
, 7 a
nd 8
all
achie
ved the r
ela
tively
hig
h s
core
of 8;
! A
ccom
modatio
n w
ill a
chie
ve t
he s
tandard
s s
et
out
in H
ealth
Build
ing N
ote
26 a
nd a
ssocia
ted
HT
Ms in r
ela
tion t
o s
ize o
f th
eatr
es a
nd s
upport
accom
modatio
n,
air c
hange r
ate
s,
and b
ed
spacin
g in
recovery
ward
;
! T
he c
urr
ent in
adequate
sta
ff c
hangin
g w
ould
be u
pgra
ded;
! A
dditi
onal
sto
rage
would
be
pro
vid
ed,
enablin
g
equip
ment
and
supplie
s
to
be
sto
red
appro
priate
ly;
! P
atie
nt
privacy a
nd d
ignity
would
be i
mpro
ved a
s b
ed s
pacin
g i
n r
ecovery
ward
would
be
exte
nded a
nd s
om
e s
ingle
room
s w
ould
be p
rovid
ed.
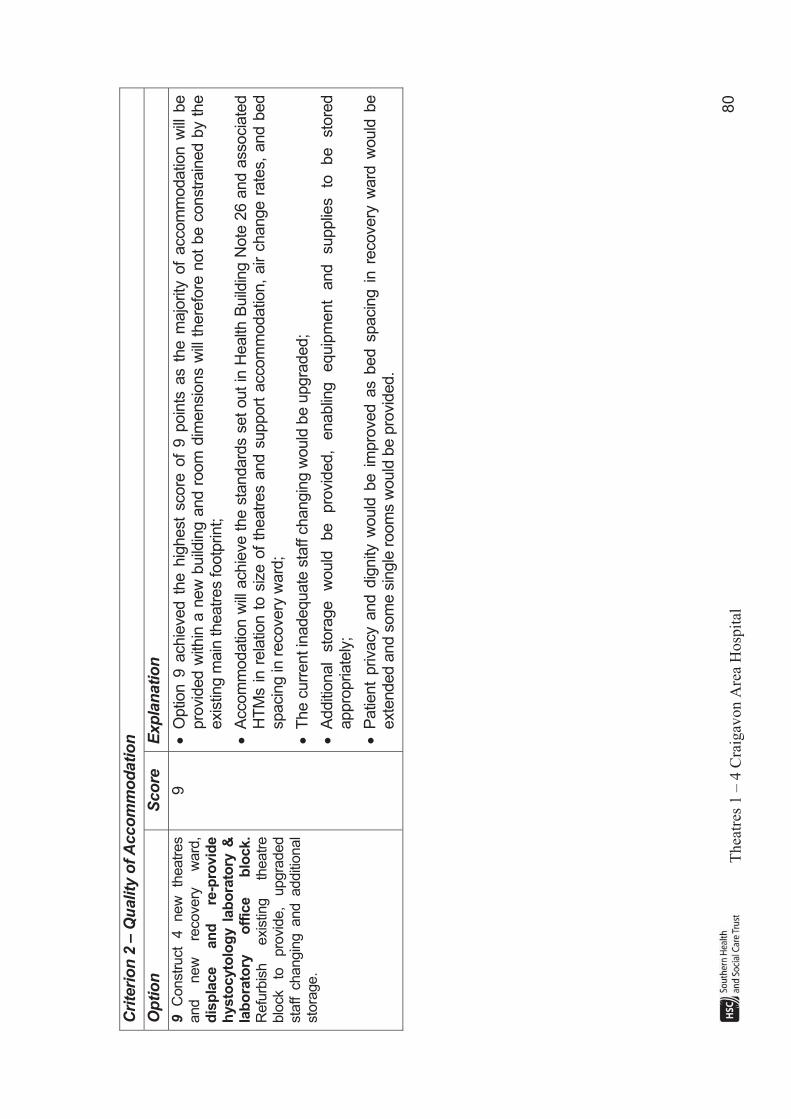
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
80
Cri
teri
on
2 –
Qu
ality
of
Acco
mm
od
ati
on
Op
tio
n
Sco
re
Exp
lan
ati
on
9C
onstr
uct
4
new
th
eatr
es
and
new
re
covery
w
ard
,d
isp
lace
an
d
re-p
rovid
e
hysto
cyto
log
y l
ab
ora
tory
&
lab
ora
tory
o
ffic
e
blo
ck.
Refu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e,
upgra
ded
sta
ff c
hangin
g and additi
onal
sto
rage.
9! O
ptio
n 9
achie
ved t
he h
ighest
score
of
9 p
oin
ts a
s t
he m
ajo
rity
of
accom
modatio
n w
ill b
e
pro
vid
ed w
ithin
a n
ew
build
ing a
nd r
oom
dim
ensio
ns w
ill t
here
fore
not
be c
onstr
ain
ed b
y t
he
exis
ting m
ain
theatr
es footp
rint;
! A
ccom
modatio
n w
ill a
chie
ve t
he s
tandard
s s
et
out
in H
ealth
Build
ing N
ote
26 a
nd a
ssocia
ted
HT
Ms in r
ela
tion t
o s
ize o
f th
eatr
es a
nd s
upport
accom
modatio
n,
air c
hange r
ate
s,
and b
ed
spacin
g in
recovery
ward
;
! T
he c
urr
ent in
adequate
sta
ff c
hangin
g w
ould
be u
pgra
ded;
! A
dditi
onal
sto
rage
would
be
pro
vid
ed,
enablin
g
equip
ment
and
supplie
s
to
be
sto
red
appro
priate
ly;
! P
atie
nt
privacy a
nd d
ignity
would
be i
mpro
ved a
s b
ed s
pacin
g i
n r
ecovery
ward
would
be
exte
nded a
nd s
om
e s
ingle
room
s w
ould
be p
rovid
ed.
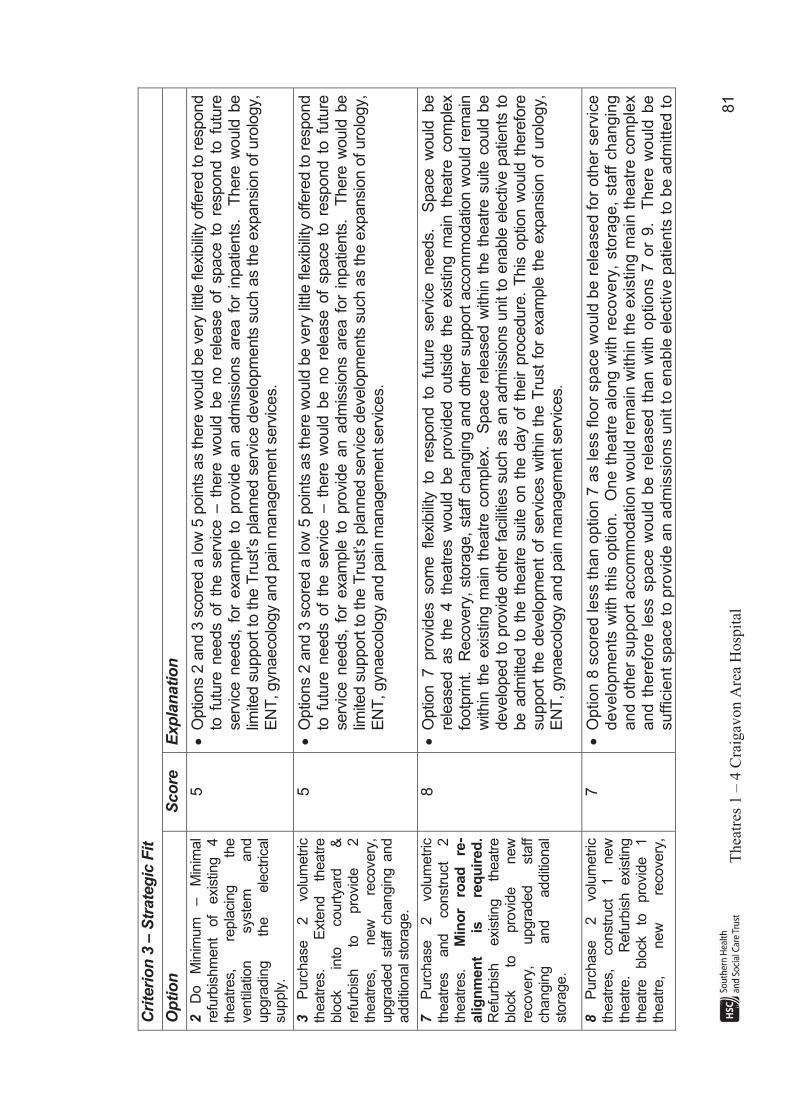
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
81
Cri
teri
on
3 –
Str
ate
gic
Fit
Op
tio
n
Sco
re
Exp
lan
ati
on
2D
o
Min
imum
–
Min
imal
refu
rbis
hm
ent
of
exis
ting
4
theatr
es,
repla
cin
g
the
ventil
atio
n
syste
m
and
upgra
din
g
the
ele
ctr
ical
supply
.
5! O
ptio
ns 2
and 3
score
d a
low
5 p
oin
ts a
s there
would
be v
ery
litt
le fle
xib
ility
offere
d to r
espond
to f
utu
re n
eeds o
f th
e s
erv
ice –
there
would
be n
o r
ele
ase o
f space t
o r
espond t
o f
utu
re
serv
ice n
eeds,
for
exam
ple
to p
rovid
e a
n a
dm
issio
ns a
rea f
or
inpatie
nts
. T
here
would
be
limite
d s
upport
to the T
rust’s
pla
nned s
erv
ice d
evelo
pm
ents
such a
s the e
xpansio
n o
f uro
logy,
EN
T, gynaecolo
gy a
nd p
ain
managem
ent serv
ices.
3P
urc
hase
2
volu
metr
ic
theatr
es.
E
xte
nd
theatr
e
blo
ck
into
court
yard
&
re
furb
ish
to
pro
vid
e
2
theatr
es,
new
re
covery
, upgra
ded s
taff c
hangin
g a
nd
additi
onal s
tora
ge.
5! O
ptio
ns 2
and 3
score
d a
low
5 p
oin
ts a
s there
would
be v
ery
litt
le fle
xib
ility
offere
d to r
espond
to f
utu
re n
eeds o
f th
e s
erv
ice –
there
would
be n
o r
ele
ase o
f space t
o r
espond t
o f
utu
re
serv
ice n
eeds,
for
exam
ple
to p
rovid
e a
n a
dm
issio
ns a
rea f
or
inpatie
nts
. T
here
would
be
limite
d s
upport
to the T
rust’s
pla
nned s
erv
ice d
evelo
pm
ents
such a
s the e
xpansio
n o
f uro
logy,
EN
T, gynaecolo
gy a
nd p
ain
managem
ent serv
ices.
7P
urc
hase
2
volu
metr
ic
theatr
es
and
constr
uct
2
theatr
es.
M
ino
r ro
ad
re
-alig
nm
en
t is
re
qu
ired
.R
efu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e
new
re
covery
, upgra
ded
sta
ff
changin
g
and
additi
onal
sto
rage.
8! O
ptio
n 7 pro
vid
es som
e fle
xib
ility
to
re
spond to
fu
ture
serv
ice needs.
S
pace w
ould
be
rele
ased as th
e 4 th
eatr
es w
ould
be pro
vid
ed outs
ide th
e exis
ting m
ain
th
eatr
e com
ple
x
footp
rint.
Recovery
, sto
rage,
sta
ff c
hangin
g a
nd o
ther
support
accom
modatio
n w
ould
rem
ain
w
ithin
the e
xis
ting m
ain
theatr
e c
om
ple
x.
Space r
ele
ased w
ithin
the t
heatr
e s
uite
could
be
develo
ped t
o p
rovid
e o
ther
facili
ties s
uch a
s a
n a
dm
issio
ns u
nit
to e
nable
ele
ctiv
e p
atie
nts
to
be a
dm
itted t
o t
he t
heatr
e s
uite
on t
he d
ay o
f th
eir p
rocedure
. T
his
optio
n w
ould
there
fore
support
the d
evelo
pm
ent
of
serv
ices w
ithin
the T
rust
for
exam
ple
the e
xpansio
n o
f uro
logy,
EN
T, gynaecolo
gy a
nd p
ain
managem
ent serv
ices.
8P
urc
hase
2
volu
metr
ic
theatr
es,
constr
uct
1
new
th
eatr
e.
R
efu
rbis
h exis
ting
theatr
e
blo
ck
to
pro
vid
e
1
theatr
e,
new
re
covery
,
7! O
ption 8
score
d less t
han o
ption 7
as less f
loor
sp
ace
wo
uld
be
rele
ase
d f
or
oth
er
se
rvic
e
de
ve
lop
me
nts
with
th
is o
ptio
n.
One t
heatr
e a
long w
ith r
ecove
ry,
sto
rag
e,
sta
ff c
ha
ng
ing
and o
ther
support
accom
modation w
ould
rem
ain
with
in t
he
exis
tin
g m
ain
th
ea
tre
co
mp
lex
and t
here
fore
less s
pace w
ould
be r
ele
ased t
han w
ith o
ptions 7
or
9.
There
would
be
su
ffic
ien
t sp
ace
to
pro
vid
e a
n a
dm
issio
ns u
nit t
o e
nable
ele
ctive p
atien
ts t
o b
e a
dm
itte
d t
o
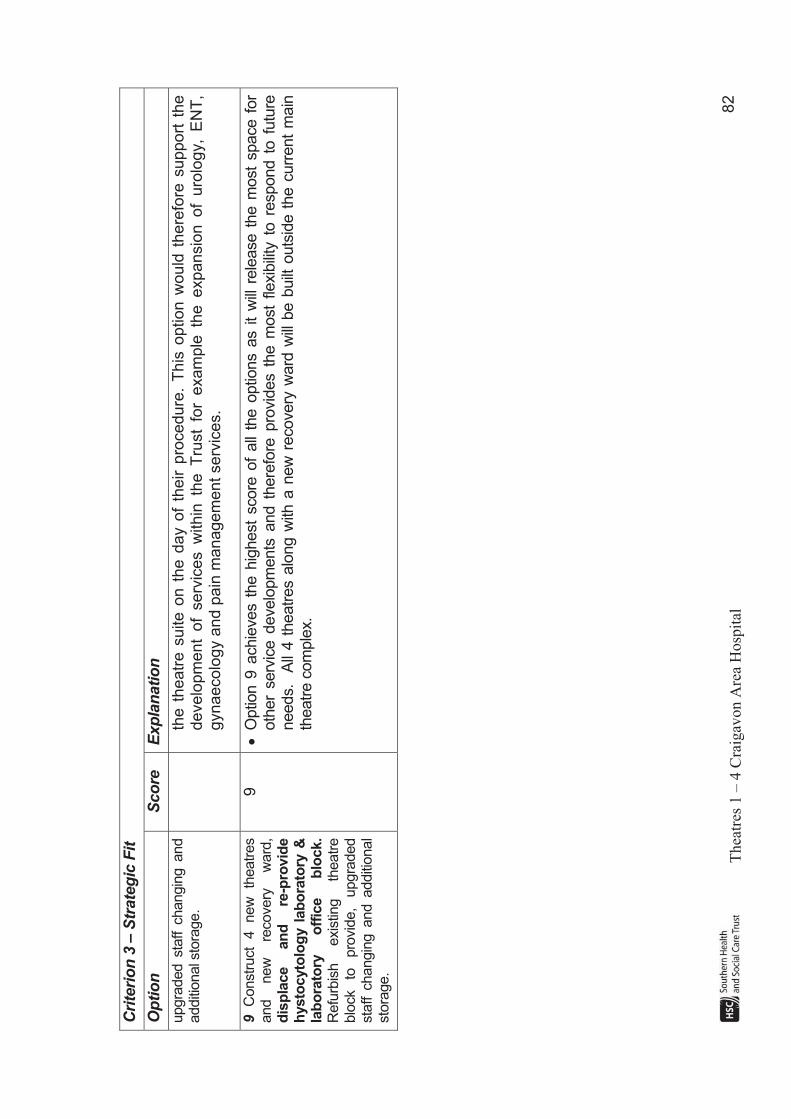
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
82
Cri
teri
on
3 –
Str
ate
gic
Fit
Op
tio
n
Sco
re
Exp
lan
ati
on
upgra
ded s
taff c
hangin
g a
nd
additi
onal s
tora
ge.
the t
heatr
e s
uite o
n t
he d
ay o
f th
eir p
rocedure
. T
his
option w
ou
ld t
here
fore
support
the
develo
pm
ent
of
serv
ices w
ithin
th
e T
rust
for
exam
ple
th
e expansio
n of
uro
logy,
EN
T,
gynaeco
logy a
nd p
ain
managem
ent
serv
ices.
9C
onstr
uct
4
new
th
eatr
es
and
new
re
covery
w
ard
,d
isp
lace
an
d
re-p
rovid
e
hysto
cyto
log
y l
ab
ora
tory
&
lab
ora
tory
o
ffic
e
blo
ck.
Refu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e,
upgra
ded
sta
ff c
hangin
g a
nd a
dditi
onal
sto
rage.
9! O
ptio
n 9
achie
ves t
he h
ighest
score
of
all
the o
ptio
ns a
s i
t w
ill r
ele
ase t
he m
ost
space f
or
oth
er
serv
ice d
evelo
pm
ents
and t
here
fore
pro
vid
es t
he m
ost
flexib
ility
to r
espond t
o f
utu
re
needs.
All
4 t
heatr
es a
long w
ith a
new
recovery
ward
will
be b
uilt
outs
ide t
he c
urr
ent
main
th
eatr
e c
om
ple
x.

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
83
Cri
teri
on
4 –
Avo
idan
ce o
f D
isru
pti
on
Op
tio
n
Sco
re
Exp
lan
ati
on
2D
o
Min
imum
–
Min
imal
refu
rbis
hm
ent
of
exis
ting
4
theatr
es,
repla
cin
g
the
ventil
atio
n
syste
m
and
upgra
din
g
the
ele
ctr
ical
supply
.
5! O
ptio
n 2
achie
ved t
he low
est
score
of
5 b
ecause t
here
will
be s
ignifi
cant
dis
ruptio
n t
o t
heatr
e
serv
ices;
! T
he
theatr
es
would
be
decante
d
in
pairs
alo
ng
with
re
covery
w
ard
to
te
mpora
ry
accom
modatio
n.
The d
ecant
of
theatr
es a
nd t
he m
ove b
ack f
ollo
win
g t
he u
pgra
de w
ork
s w
ill
itself
be very
dis
ruptiv
e and w
ill re
sult
in th
eatr
e dow
n tim
e.
In additi
on,
due to
esta
te
develo
pm
ents
aro
und th
e very
congeste
d th
eatr
e are
a,
the only
pote
ntia
l site
fo
r decant
theatr
es is o
n t
he f
ar
sid
e o
f th
e labora
tory
build
ings w
ith t
he c
onstr
uctio
n o
f a c
lean c
orr
idor
thro
ugh the la
bora
tory
receptio
n a
rea. G
iven the d
ista
nce to s
taff c
hangin
g, sta
ff r
est fa
cili
ties,
theatr
e s
tora
ge a
nd s
upport
accom
modatio
n a
nd IC
U, clin
ical adja
cencie
s w
ill b
e s
ub o
ptim
al.
In
additi
on the tw
o theatr
es r
em
ain
ing in
the m
ain
theatr
e b
lock w
ill b
e s
om
e d
ista
nce fro
m the
tem
pora
ry r
ecovery
ward
;
! T
wo t
heatr
es w
ill c
ontin
ue t
o f
unctio
n w
hils
t w
ork
is g
oin
g o
n w
ithin
the m
ain
theatr
e a
rea.
The p
ote
ntia
l for
unpla
nned d
ow
ntim
e is
consid
ere
d to b
e h
igh.
3P
urc
hase
2
volu
metr
ic
theatr
es.
E
xte
nd
theatr
e
blo
ck
into
court
yard
&
re
furb
ish
to
pro
vid
e
2
theatr
es,
new
re
covery
, upgra
ded sta
ff changin
g and
additi
onal s
tora
ge.
6! O
ptio
n 3
was a
ward
ed a
rela
tively
low
score
of
6 a
s t
here
will
be s
ignifi
cant
dis
ruptio
n t
o
theatr
e s
erv
ices, alth
ough this
is d
eem
ed to b
e le
ss than w
ith o
ptio
n 2
. W
ork
would
be c
arr
ied
out
in a
num
ber
of
phases a
nd f
or
the d
ura
tion o
f th
e p
roje
ct, t
here
would
be w
ork
goin
g o
n
while
tw
o t
heatr
es a
nd r
ecovery
ward
rem
ain
opera
tional
in t
heir c
urr
ent
locatio
n.
Theatr
e
dow
ntim
e is
inevita
ble
with
this
optio
n;
! N
ew
T
hea
tre
1
will
be
pro
vid
ed
by
a
mix
ture
of
exte
nsio
n
into
a
court
yard
an
d
refu
rbis
hm
ent
of
a s
mall
denta
l th
eatr
e a
nd s
taff r
est
and o
ffic
e a
ccom
modation.
Denta
l surg
ery
will
be r
elo
ca
ted t
o o
ld t
heatr
e 5
. S
taff r
est
are
a a
nd S
iste
rs’
offic
e w
ill b
e r
e-
pro
vid
ed i
n p
art
of
the e
xis
ting s
taff c
hangin
g.
The r
em
ain
der
of
the d
ispla
ced o
ffic
e
accom
modation w
ill b
e r
e-p
rovid
ed t
em
pora
rily
in p
ort
acabin
s.

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
84
Cri
teri
on
4 –
Avo
idan
ce o
f D
isru
pti
on
Op
tio
n
Sco
re
Exp
lan
ati
on
! E
xis
ting T
heatr
e 1
will
be r
efu
rbis
hed t
o p
rovid
e a
new
theatr
e 2
.
! T
heatr
es 3
& 4
will
move t
o t
he 2
volu
metr
ic t
he
atr
es.
Exis
tin
g T
he
atr
es 2
, 3
an
d 4
will
be
re
furb
ished t
o p
rovid
e a
recovery
ward
and o
ther
support
accom
modation.
! T
he exis
ting re
covery
are
a and old
T
heatr
e 5
w
ill b
e re
furb
ish
ed
to
p
rovid
e a
d
en
tal
theatr
e,
adm
issio
ns lounge a
nd d
ispla
ced o
ffic
e a
ccom
modation.
7P
urc
hase
2
volu
metr
ic
theatr
es
and
constr
uct
2
theatr
es.
M
ino
r ro
ad
re
-alig
nm
en
t is
re
qu
ired
.R
efu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e
new
re
covery
, upgra
ded
sta
ff
changin
g
and
additi
onal
sto
rage.
8! T
he d
isru
ptio
n to theatr
e s
erv
ices w
ill b
e m
inim
al a
nd there
fore
optio
n 7
achie
ved a
hig
h s
core
of 8.
! W
hen th
e T
&
O
serv
ice tr
ansfe
rs to
its
new
facili
ty upgra
de w
ork
to
th
e tw
o volu
metr
ic
theatr
es w
ill b
e c
arr
ied o
ut
and w
hen t
hese h
ave b
een c
om
mis
sio
ned s
essio
ns f
rom
tw
o
exis
tin
g
the
atr
es
will
tr
an
sfe
r.
Th
e
tem
po
rary
vo
lum
etr
ic
T&
O
sta
ff
ch
an
gin
g
an
d
recovery
units w
ould
be re
moved fr
om
th
e site
to
allo
w constr
uction of
the new
build
th
eatr
es
and
when
constr
uction
and
com
mis
sio
nin
g
of
these
has
been
com
ple
ted
, opera
ting s
essio
ns f
rom
the t
wo r
em
ain
ing t
heatr
es w
ill t
ransfe
r to
new
theatr
e 3
and 4
;
! W
ork
to
constr
uct
the new
re
covery
w
ard
and to
up
gra
de th
e sta
ff changin
g w
ill not
com
mence u
ntil all
four
theatr
es h
ave m
oved.
8P
urc
hase
2
volu
metr
ic
theatr
es,
constr
uct
1
new
th
eatr
e.
Refu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e
1
theatr
e,
new
re
covery
, upgra
ded sta
ff changin
g and
additi
onal s
tora
ge.
7! O
ption 8
achie
ved a
low
er
sco
re t
ha
n o
ptio
n 7
be
ca
use
in
tern
al
refu
rbis
hm
en
t w
ork
to
cre
ate
the f
ourt
h t
heatr
e w
ill t
ake p
lace
wh
ile o
ne t
he
atr
e i
s s
till
opera
tion
al
within
th
e
main
theatr
e s
uite;
! In
com
mon w
ith o
ptions 3
and 7
, w
hen the T
& O
serv
ice tra
nsfe
rs to its
new
facili
ty u
pgra
de
work
to
th
e
two
volu
metr
ic
theatr
es
will
be
carr
ied
out
and
when
these
have
been
com
mis
sio
ned s
essio
ns f
rom
tw
o e
xis
tin
g t
he
atr
es w
ill t
ran
sfe
r;
! T
he
te
mp
ora
ry v
olu
me
tric
T&
O c
ha
ng
ing
un
it w
ou
ld b
e r
em
ove
d f
rom
th
e s
ite
to
allo
w
co
nstr
uctio
n o
f th
e n
ew
bu
ild (
third
) th
ea
tre
. O
pe
ratin
g s
essio
ns f
rom
a t
hird
exis
tin
g

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
85
Cri
teri
on
4 –
Avo
idan
ce o
f D
isru
pti
on
Op
tio
n
Sco
re
Exp
lan
ati
on
theatr
e w
ill t
ransfe
r to
the n
ew
build
the
atr
e w
hen c
on
str
uction a
nd c
om
mis
sio
nin
g o
f th
is
has b
een c
om
ple
ted;
! W
ork
to c
onstr
uct
the f
ourt
h t
heatr
e w
ill b
e u
ndert
aken w
hen t
he
first
thre
e h
ave m
ove
d
and f
ollo
win
g t
his
, re
furb
ishm
ent
to p
rovid
e a
new
recovery
ward
and t
o u
pgra
de t
he s
taff
changin
g w
ill b
e u
ndert
aken.
9C
onstr
uct
4
new
th
eatr
es
and
new
re
covery
w
ard
,d
isp
lace
an
d
re-p
rovid
e
hysto
cyto
log
y l
ab
ora
tory
&
lab
ora
tory
o
ffic
e
blo
ck.
Refu
rbis
h
exis
ting
theatr
e
blo
ck
to
pro
vid
e,
upgra
ded
sta
ff changin
g and additi
onal
sto
rage.
7! O
ptio
n 9
sco
red
7.
Dis
rup
tio
n t
o t
he
atr
e s
erv
ices w
ill b
e m
inim
al as t
heatr
e s
essio
ns w
ill
no
t tr
an
sfe
r u
ntil
the
co
nstr
uctio
n o
f th
e n
ew
th
ea
tre
s a
nd
re
co
ve
ry w
ard
h
as b
ee
n
com
ple
ted
and
the
new
fa
cili
ties
have
be
en
co
mm
issio
ne
d.
Ho
we
ver
the
re
will
b
e
dis
ruption t
o labora
tory
serv
ices a
s t
he h
isto
cyto
log
y la
bo
rato
ry,
lab
ora
tory
re
ce
ptio
n,
an
d
som
e la
bora
tory
offic
e accom
modation occu
pie
s th
e pro
posed site fo
r th
e new
build
th
eatr
es a
nd r
ecovery
. T
his
accom
modation w
ould
have t
o b
e r
e-p
rovid
ed a
nd s
erv
ice
s
moved b
efo
re t
he s
ite c
ould
be c
leare
d f
or
constr
uction.
Curr
ently t
he labora
tory
serv
ices
are
lo
ca
ted
to
ge
the
r.
Th
is o
ptio
n w
ill r
esu
lt i
n l
ab
ora
tory
se
rvic
es b
ein
g s
plit
acro
ss t
wo
lo
ca
tio
ns o
n t
he
site
.

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
86
Cri
teri
on
5 –
Sp
eed
of
Imp
lem
en
tati
on
–
This
crite
rion is
linked d
irectly
to c
onstr
uctio
n/r
efu
rbis
hm
ent tim
escale
s. T
he e
stim
ate
d p
rogra
mm
es for
the s
hort
liste
d o
ptio
ns a
re s
how
n
belo
w. F
ive m
onth
s h
as b
een in
clu
ded for
desig
n for
each o
ptio
n.
!
Optio
n 2
– 3
0 m
onth
s (
score
3)
!
Optio
n 3
– 2
8 m
onth
s (
score
5)
!
Optio
n 7
– 2
6 m
onth
s (
score
7)
!
Optio
n 8
– 2
9 m
onth
s (
score
4)
!
Optio
n 9
– 3
0 m
onth
s (
score
3)
Based o
n these tim
escale
s the s
core
s h
ave b
een a
llocate
d a
s follo
ws:
Tim
elin
e (
mo
nth
s)
0 _
_________ 2
6 _
_________ 2
7 _
_________ 2
8 _
_________ 2
9 _
_________ 3
0
Sco
re 10 _
_________ 7 _
_________ 6 _
__________ 5 _
_________ 4
__________ 3

Theatres 1 – 4 Craigavon Area Hospital 87
9 FINANCIAL APPRAISAL OF SHORTLISTED OPTIONS This section of the business case assesses the quantifiable costs of the shortlisted options, as set out below.
Option Description
2 Do Minimum – Minimal refurbishment of existing 4 theatres, replacing the ventilation system and upgrading the electrical supply.
3 Purchase 2 volumetric theatres. Extend theatre block into a courtyard and refurbish to provide 2 theatres, new recovery, upgraded staff changing and additional storage.
7 Purchase 2 volumetric theatres and construct 2 theatres. Minorroad re-alignment is required. Refurbish existing theatre block to provide new recovery, upgraded staff changing and additional storage.
8 Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage.
9 Construct 4 new theatres and new recovery ward, displace and re-provide hystocytology laboratory & laboratory office block. Refurbish existing theatre block to provide, upgraded staff changing and additional storage.
The costs of each of the options are considered under the following headings:
! Capital Costs;
! Capital Charges;
! Revenue Consequences; and
! Economic Costs (NPVs).
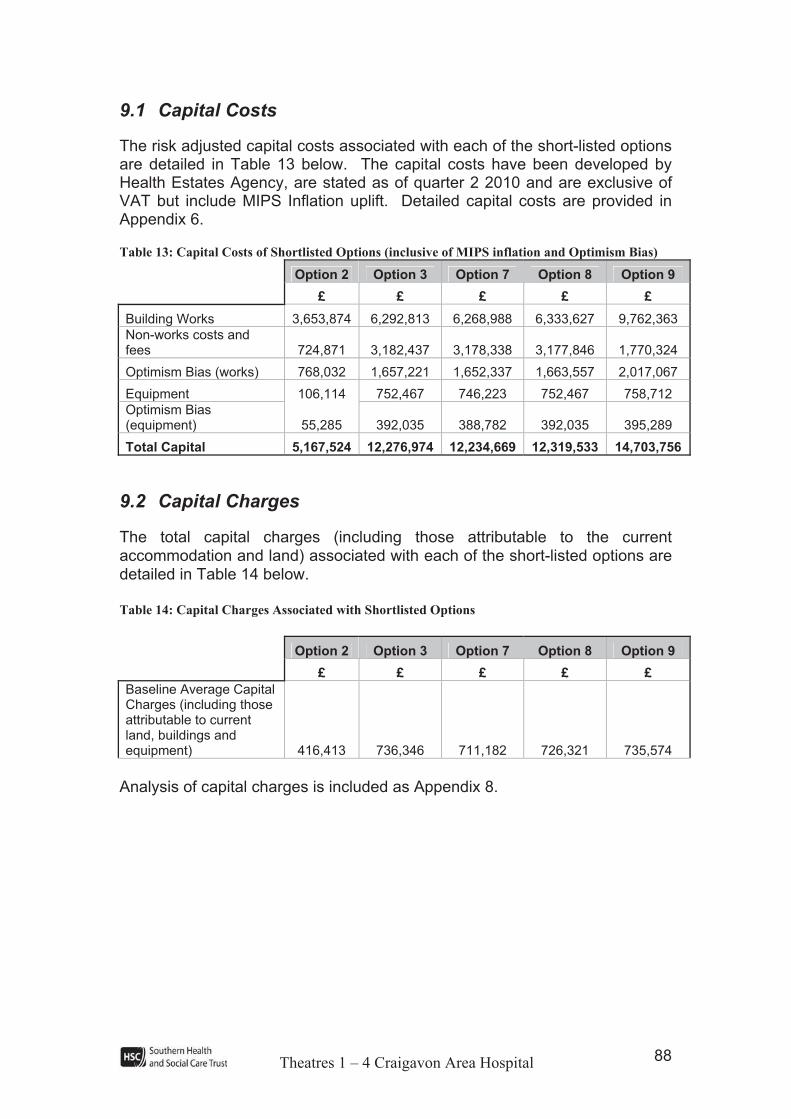
Theatres 1 – 4 Craigavon Area Hospital 88
9.1 Capital Costs
The risk adjusted capital costs associated with each of the short-listed options are detailed in Table 13 below. The capital costs have been developed by Health Estates Agency, are stated as of quarter 2 2010 and are exclusive of VAT but include MIPS Inflation uplift. Detailed capital costs are provided in Appendix 6.
Table 13: Capital Costs of Shortlisted Options (inclusive of MIPS inflation and Optimism Bias)
Option 2 Option 3 Option 7 Option 8 Option 9
£ £ £ £ £
Building Works 3,653,874 6,292,813 6,268,988 6,333,627 9,762,363
Non-works costs and fees 724,871 3,182,437 3,178,338 3,177,846 1,770,324
Optimism Bias (works) 768,032 1,657,221 1,652,337 1,663,557 2,017,067
Equipment 106,114 752,467 746,223 752,467 758,712
Optimism Bias (equipment) 55,285 392,035 388,782 392,035 395,289
Total Capital 5,167,524 12,276,974 12,234,669 12,319,533 14,703,756
9.2 Capital Charges
The total capital charges (including those attributable to the current accommodation and land) associated with each of the short-listed options are detailed in Table 14 below.
Table 14: Capital Charges Associated with Shortlisted Options
Option 2 Option 3 Option 7 Option 8 Option 9
£ £ £ £ £
Baseline Average Capital Charges (including those attributable to current land, buildings and equipment) 416,413 736,346 711,182 726,321 735,574
Analysis of capital charges is included as Appendix 8.
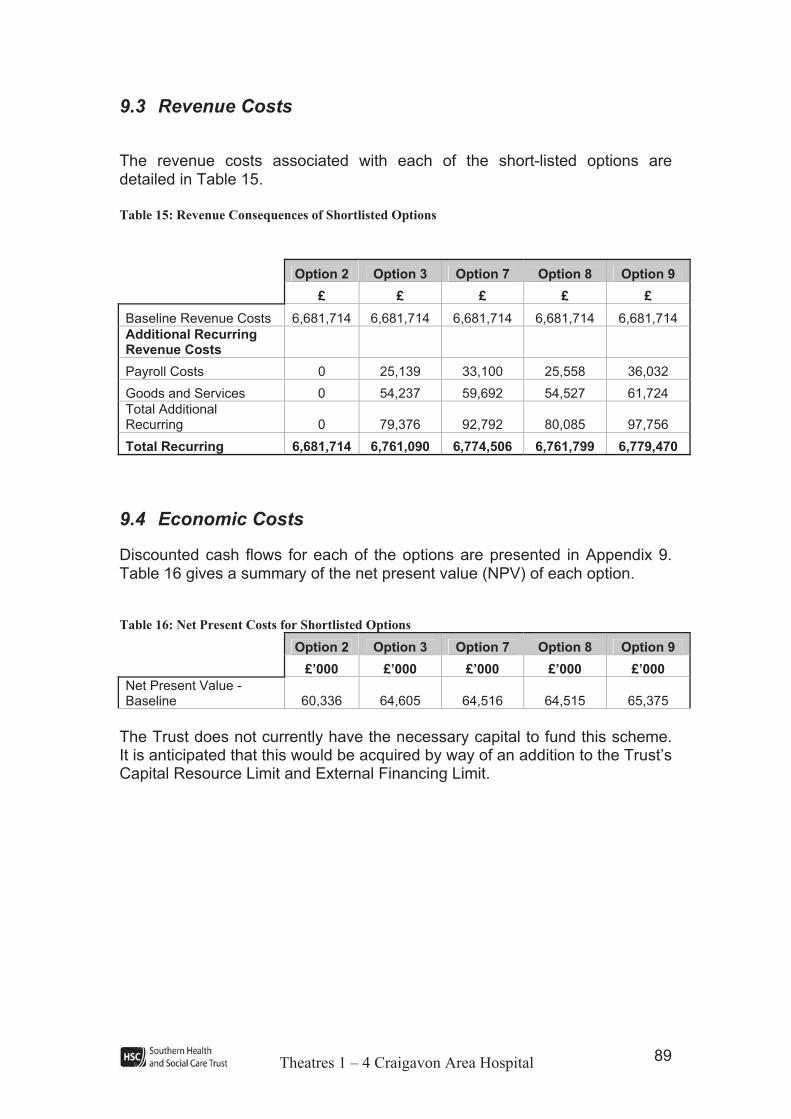
Theatres 1 – 4 Craigavon Area Hospital 89
9.3 Revenue Costs
The revenue costs associated with each of the short-listed options are detailed in Table 15.
Table 15: Revenue Consequences of Shortlisted Options
Option 2 Option 3 Option 7 Option 8 Option 9
£ £ £ £ £
Baseline Revenue Costs 6,681,714 6,681,714 6,681,714 6,681,714 6,681,714
Additional Recurring Revenue Costs
Payroll Costs 0 25,139 33,100 25,558 36,032
Goods and Services 0 54,237 59,692 54,527 61,724
Total Additional Recurring 0 79,376 92,792 80,085 97,756
Total Recurring 6,681,714 6,761,090 6,774,506 6,761,799 6,779,470
9.4 Economic Costs
Discounted cash flows for each of the options are presented in Appendix 9. Table 16 gives a summary of the net present value (NPV) of each option.
Table 16: Net Present Costs for Shortlisted Options
Option 2 Option 3 Option 7 Option 8 Option 9
£’000 £’000 £’000 £’000 £’000
Net Present Value - Baseline 60,336 64,605 64,516 64,515 65,375
The Trust does not currently have the necessary capital to fund this scheme. It is anticipated that this would be acquired by way of an addition to the Trust’s Capital Resource Limit and External Financing Limit.
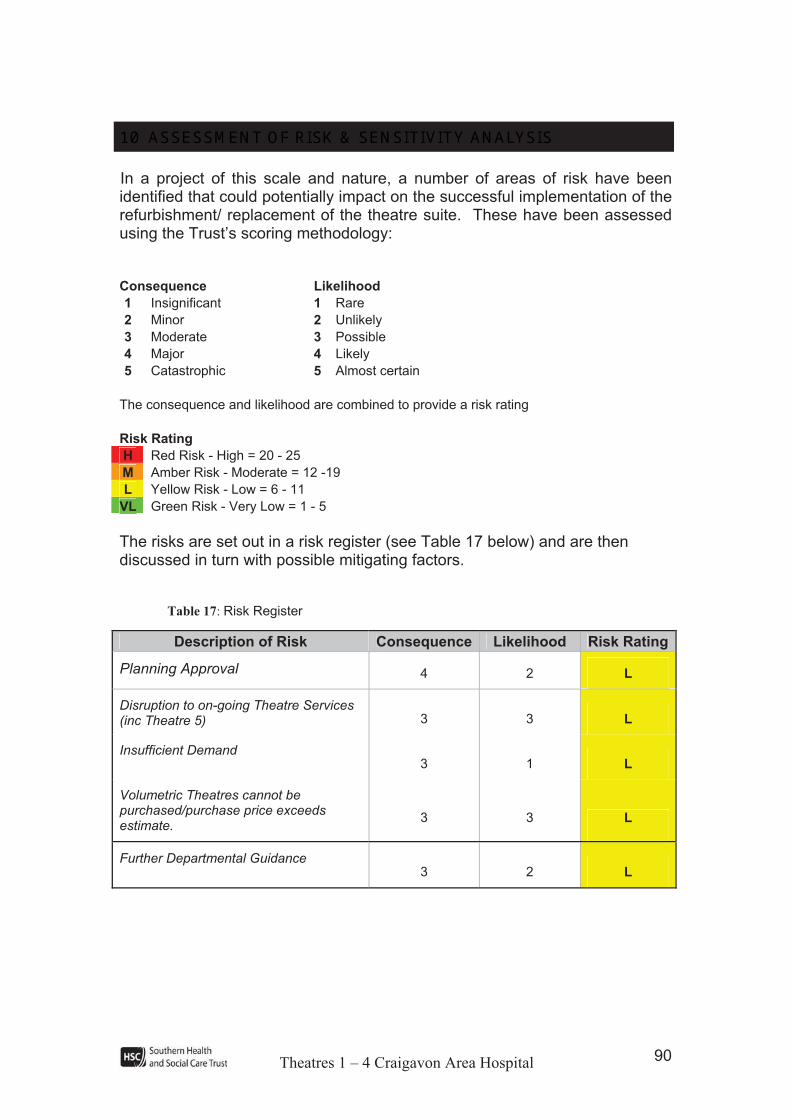
Theatres 1 – 4 Craigavon Area Hospital 90
10 ASSESSMENT OF RISK & SENSITIVITY ANALYSIS In a project of this scale and nature, a number of areas of risk have been identified that could potentially impact on the successful implementation of the refurbishment/ replacement of the theatre suite. These have been assessed using the Trust’s scoring methodology:
Consequence Likelihood
1 Insignificant 1 Rare
2 Minor 2 Unlikely
3 Moderate 3 Possible
4 Major 4 Likely
5 Catastrophic 5 Almost certain
The consequence and likelihood are combined to provide a risk rating
Risk Rating
H Red Risk - High = 20 - 25
M Amber Risk - Moderate = 12 -19
L Yellow Risk - Low = 6 - 11
VL Green Risk - Very Low = 1 - 5
The risks are set out in a risk register (see Table 17 below) and are then discussed in turn with possible mitigating factors.
Table 17: Risk Register
Description of Risk Consequence Likelihood Risk Rating
Planning Approval 4 2 L
Disruption to on-going Theatre Services (inc Theatre 5) 3 3 L
Insufficient Demand 3 1 L
Volumetric Theatres cannot be purchased/purchase price exceeds estimate.
3 3 L
Further Departmental Guidance 3 2 L

Theatres 1 – 4 Craigavon Area Hospital 91
In general, the risks identified refer to all the short listed options equally, however where these risks relate to a specific option this has been highlighted. In addition mitigation factors have been discussed in respect of each risk highlighted.
It is important to recognise that whilst there may be significant risks around the construction of the project, in terms of cost overruns and delays, these are dealt with under ‘Adjustment for Optimism Bias’ which is set out after the discussion on other risks below.
10.1Risks
Planning Approval
This issue is a risk for options which require construction outside the existing hospital building, therefore this risk applies to all options. In the case of option 2, although it involves no new build, there are significant temporary structures required, in the form of modular theatres and a Recovery Suite to be used until the refurbishment work is complete.
In particular the risk is that the construction of new modular theatres and a new recovery suite would not receive planning permission. There are a number of mitigation factors which should be considered:
! The entire Craigavon Area Hospital site has been zoned for hospital use and the proposed location of the new constructions is adjacent to the existing theatre suite;
! This project represents an interim scheme before major redevelopment of the hospital on a different part of the site;
! As similar developments for the new Trauma & Orthopaedics Unit and new Theatre 5 have been granted approval, it would be highly unlikely that planning permission would not be given for this project.
Whilst the impact of not getting planning permission would be high, the likelihood of this occurring is considered to be low.
Disruption to Theatre Services
There is a risk that during the construction period, theatre services could be disrupted. Whilst this risk is largely managed across all ‘Do Something’ options, it is of greater significance to option 2 the ‘Do Minimum’ option and also with option 3. Option 2 requires two temporary theatres and recovery facilities to be erected and then refurbishment work to be undertaken in the existing theatre suite while 2 theatres remain operational. Due to recent building work to the rear of main theatres, temporary accommodation would have to be located on the far side of the laboratory buildings with a clean corridor through the laboratory reception. This would provide an operationally difficult arrangement and therefore the likelihood of disruption with option 2 is

Theatres 1 – 4 Craigavon Area Hospital 92
higher than with the other short listed options. Option 3 also involves work being undertaken in the theatre suite while two theatres remain operational.
The risk of disruption is easier to manage with the other short listed options. Options 7, 8 and 9 involve new build of either one or more theatres which can be undertaken without any significant disturbance to the existing theatres as it is external to the existing suite. In addition, those options which involve purchasing the two volumetric theatres enable two existing theatres to be decanted permanently, early in the project.
Therefore options 7, 8 and 9 provide the lowest risk in this regard.
A further risk equally applicable to all options is in respect of an accidental disruption to utilities. Consultation with the Health Estates Agency has indicated that they have accurate plans of underground services around the main theatre suite therefore minimising the risk of any accidental damage.
Insufficient Demand
As with any capital project, there is a risk that demand for the new theatres may not materialise and utilisation levels could fall. In mitigation, the Assessment of Need section of this business case has highlighted an increasing trend in utilisation and numbers of procedures being completed in recent years. Furthermore, projection data has also forecast a further increase in the number of procedures being undertaken.
Volumetric Theatres Cannot be Purchased/Purchase Price Exceeds Estimate
For options 3, 7 and 8 there is a risk that the company supplying the volumetric theatres may decide not to sell or the purchase price may exceed the estimated price. This would result in the Trust having to purchase theatres from another company for these options and/or additional capital cover being required. The Trust believes this to be a low risk.
Further Departmental Guidance
Whilst Departmental guidance issued in respect of operating theatres is not applicable to theatres currently in use but only the construction of new theatres, other requirements may be issued.
This is a risk which impacts on all options equally and it is a feature of the environment in which Trusts operate and will therefore be managed as appropriate. Good communication will be maintained between the Trust and Health Estates to ensure that if new guidance is issued, then the Trust has ample time to plan for its implementation.

Theatres 1 – 4 Craigavon Area Hospital 93
10.2Optimism Bias Adjustment
The Green Book and the HM Treasury Supplementary Green Book Guidance on Optimism explicitly addresses project risks following a study by Mott MacDonald2 which identified the tendency for project appraisers to be overly optimistic, overstating benefits and understating timescales and costs. To redress this tendency, HM Treasury has developed an approach which requires appraisers to make explicit adjustments to determine a suitably optimism biased adjusted capital cost and NPV for each option.
Based on this guidance, an uplift is required to the capital costs (based on HM Treasury recommended adjustment ranges). There is no specific uplift required for revenue costs.
The Green Book enables optimism bias to be reduced according to the extent to which each of the contributory factors have been managed. Appendix 10 illustrates the risk factors for this project and the extent to which the Trust considers it can mitigate against them. A summary of this evaluation is given in Table 18. The capital and equipment costs used to calculate optimism bias have been uplifted for inflation.
Table 18: Summary of Optimism Bias Analysis
Option 2 Option 3 Option 7 Option 8 Option 9
Capital Cost (£) 4,378,745 9,475,250
9,447,327 9,511,473 11,532,687
Optimism Bias 17.54% 17.49% 17.49% 17.49% 17.49%
OB Adjusted Capital Cost 5,146,777 11,132,471 11,099,664 11,175,030 13,549,754
Works Duration (months) 25 23 21 24 25
Optimism Bias 13.20% 13.14% 13.14% 13.14% 13.14%
OB Adjusted Works Duration 28.3 26 23.8 27.2 28.3
Equipment Cost (£) 106,114 752,467 746,223 752,467 758,712
Optimism Bias 52.10% 52.10% 52.10% 52.10% 52.10%
OB Adjusted Equipment Cost 161,399 1,144,502 1,135,005 1,144,502 1,154,001
Discounted cash flows for each of the options were recalculated following application of these uplift factors. In applying the optimism bias percentage to capital costs, planning contingencies have been removed and the optimism bias applied to the remaining capital costs. Table 19 gives the net present value of each of the options after optimism bias adjustments.
2 Mott MacDonald (2002), Review of Large Public Procurement in the UK, Mott MacDonald (2002)

Theatres 1 – 4 Craigavon Area Hospital 94
Table 19:Net Present Costs Adjusted for Optimism Bias
Option 2 Option 3 Option 7 Option 8 Option 9
£’000 £’000 £’000 £’000 £’000
Baseline Net Present Value 60,336 64,605 64,516 64,515 65,375
Risk adjusted Net Present Value 60,883 66,010 65,934 65,951 66,973

Theatres 1 – 4 Craigavon Area Hospital 95
10.3Sensitivity Analysis on Non Financial Benefits
The sensitivity of the benefits to risk is considered in this section, to determine if this would impact on the preferred option. The aim is to test the robustness of the ranking of the options.
Sensitivity analysis may be carried out on the weights allocated to the benefit criteria to test how the ranking of the options would respond to changes in the weighting. The most important criterion was deemed to be clinical effectiveness. As Table 20 indicates the weighting of clinical effectiveness would have to be decreased by 8 in order to change the option which is ranked first.
Table 20: Effect on Ranking of Options by Adjustment of Weightings
Option 2 Option 3 Option 7 Option 8 Option 9
Weights unchanged 5 3 2 1 4
Increase clinical effectiveness by 4, decrease others by 1
5 2 2 1 4
Increase clinical effectiveness by 8, decrease others by 2 5 2 3 1 4
Decrease clinical effectiveness by 4, increase others by 1
5 4 2 1 3
Decrease clinical effectiveness by 8, increase others by 2
5 4 1 2 3
The potential risks to the project have been outlined in section 10.1. The risk associated with insufficient demand will apply equally to all of the short listed options. An inability to secure planning approval and changes to departmental guidance relating to operating theatres would affect all of the options with the exception of option 2.
The ability to deliver theatre services to both emergency and elective patients for the duration of the project is critical to the functioning of the hospital and the ‘avoidance of disruption’ criterion is deemed to have the greatest degree of uncertainty, although the uncertainty will be mitigated by appropriate planning and phasing of works. All of the options, with the exception of option 9, involve some work within the existing theatre suite while theatre and/or recovery continue to function. Table 21 shows the effect on the ranking by decreasing the score for options 2, 3, 7 and 8 by one point.

Theatres 1 – 4 Craigavon Area Hospital 96
Table 21: Effect on Ranking of Options by Adjustment of Scores
Option 2 Option 3 Option 7 Option 8 Option 9
Scores unchanged 5 3 2 1 4
Decrease option 2 by 1 5 3 2 1 4
Decrease option 3 by 1 5 4 2 1 3
Decrease option 7 by 1 5 2 2 1 4
Decrease option 8 by 1 5 3 2 1 4
Table 21 demonstrates that decreasing the score for ‘avoidance of disruption’ for options 2, 3, 7 or 8 does not change the option which is ranked first. The score for option 8 would need to be decreased by 2 points to change its ranking from first to second. This would imply that option 8 would be equally disruptive to theatre services as option 2, which is clearly not the case.
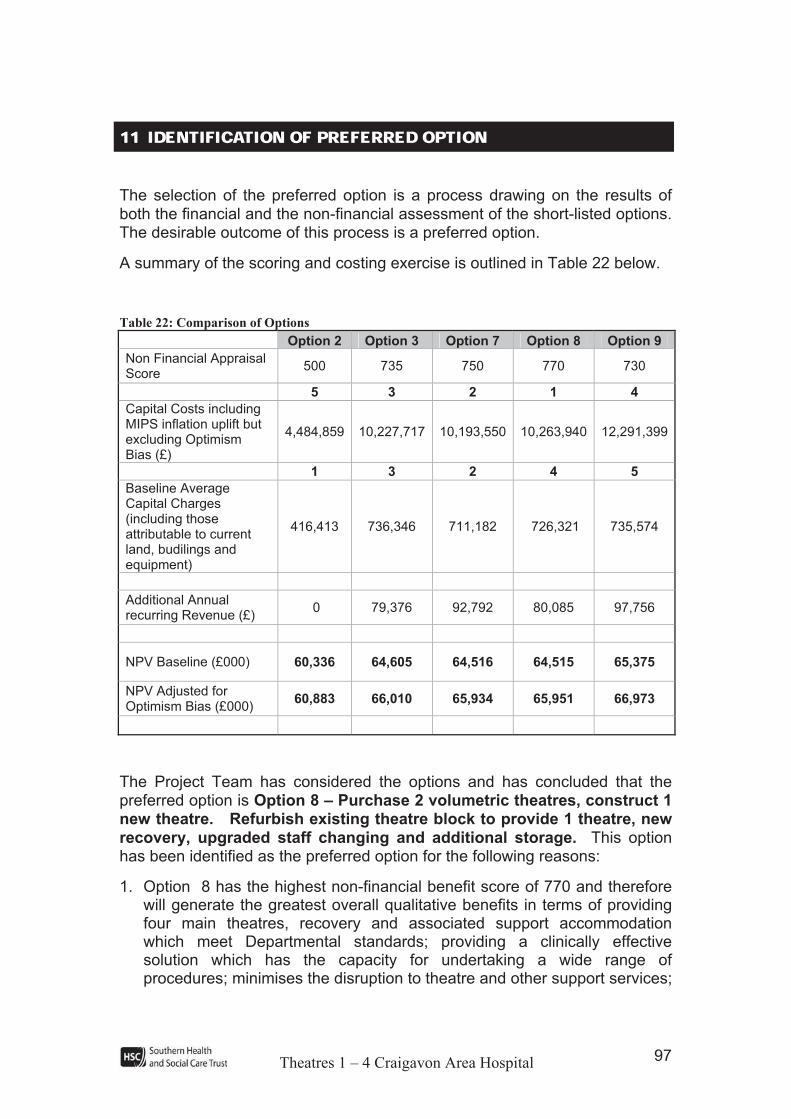
Theatres 1 – 4 Craigavon Area Hospital 97
1111 IIDDEENNTTIIFFIICCAATTIIOONN OOFF PPRREEFFEERRRREEDD OOPPTTIIOONN The selection of the preferred option is a process drawing on the results of both the financial and the non-financial assessment of the short-listed options. The desirable outcome of this process is a preferred option.
A summary of the scoring and costing exercise is outlined in Table 22 below.
Table 22: Comparison of Options
Option 2 Option 3 Option 7 Option 8 Option 9
Non Financial Appraisal Score
500 735 750 770 730
5 3 2 1 4
Capital Costs including MIPS inflation uplift but excluding Optimism Bias (£)
4,484,859 10,227,717 10,193,550 10,263,940 12,291,399
1 3 2 4 5
Baseline Average Capital Charges (including those attributable to current land, budilings and equipment)
416,413 736,346 711,182 726,321 735,574
Additional Annual recurring Revenue (£)
0 79,376 92,792 80,085 97,756
NPV Baseline (£000) 60,336 64,605 64,516 64,515 65,375
NPV Adjusted for Optimism Bias (£000)
60,883 66,010 65,934 65,951 66,973
The Project Team has considered the options and has concluded that the preferred option is Option 8 – Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage. This option has been identified as the preferred option for the following reasons:
1. Option 8 has the highest non-financial benefit score of 770 and therefore will generate the greatest overall qualitative benefits in terms of providing four main theatres, recovery and associated support accommodation which meet Departmental standards; providing a clinically effective solution which has the capacity for undertaking a wide range of procedures; minimises the disruption to theatre and other support services;

Theatres 1 – 4 Craigavon Area Hospital 98
fits with the Trust’s strategic direction; and can be delivered within reasonable timescales;
2. The capital costs (excluding Optimism Bias) associated with this option are £10,263,940. Whilst it ranks as 4 from a financial appraisal perspective the monetary difference between it and the higher ranking options 3 and 7 is not material and this will provide the Trust with theatres which will meet the current standards;
3. Annual capital charges associated with Option 8 are £726,321. This is less than the capital charges associated with Options 3 and 9 and is not materially higher than those for Option 7;
4. Recurring revenue costs associated with Option 8 are lower than those indicated for Option 7 and Option 9 and are not materially different to those for Option 3;
5. Net Present Value of Option 8 is £64,515k (risk adjusted NPV £65,951k), given that Option 8 achieved the highest non-financial benefit score this offers the best benefit for investment required.

Theatres 1 – 4 Craigavon Area Hospital 99
12 AFFORDABILITY ANALYSIS The sections below demonstrate the affordability of the preferred option under the following headings.
12.1 Capital funding requirements
The preferred option selected in the previous section envisages purchasing 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage.
The estimated total capital cost of this scheme (less refreshes) adjusted for Optimism Bias is £12,319,533.
12.2 Revenue Consequences
The revenue consequences of the preferred option, Option 8 - Purchase 2 volumetric theatres, construct 1 new theatre. Refurbish existing theatre block to provide 1 theatre, new recovery, upgraded staff changing and additional storage are summarised in the table below.
Table 23: Affordability Analysis
Average Annual Revenue Costs (RiskAdjusted)
Average Annual Capital
Charges (Risk
Adjusted)
Total
£ £ £
Option 2 – Base Case 6,681,714 462,789 7,144,503
Option 8 – Preferred Option 6,761,799 845,737 7,607,536
Additional Revenue Consequences 80,085 382,948 463,033

Theatres 1 – 4 Craigavon Area Hospital 100
13 EQUALITY & HUMAN RIGHTS CONSIDERATIONSSection 75 of the Northern Ireland Act 1998 requires the Trust, in carrying out its functions relating to Northern Ireland, to have due regard to the need to promote equality of opportunity between persons of different religious belief, political opinion, racial group, age, marital status or sexual orientation; between men and women generally; between persons with a disability and persons without; and between persons with dependants and persons without.
Without prejudice to these obligations the Trust is also required, in carrying out its functions, to have regard to the desirability of promoting good relations between persons of different religious belief, political opinion or racial group.
As part of ensuring compliance with the statutory duty, the SHSCT have produced an Equality Scheme demonstrating their commitment to equality of opportunity and to carrying out Equality Impact Assessments on policies which may have a differential impact on any of the categories noted above. The existence of a differential impact is determined by reference to the following four criteria:
! Is there any evidence of higher or lower participation or uptake by different groups?
! Is there any evidence that different groups have different needs, experiences issues and priorities in relation to the particular policy area?
! Is there an opportunity to better promote equality of opportunity or better community relations by altering the policy or working with others in government or in the larger community? or
! Have consultations in the past with relevant groups, organisations or individuals indicated that particular policies create problems that are specific to them?
The developments proposed within this outline business case have been considered in terms of their equality of opportunity implications against each of the four criteria detailed above. The proposal to provide four theatres and associated support accommodation at Craigavon Area Hospital has limited scope to impact differentially on any of the nine equality groupings, as the standard of care and accommodation for all service users and staff will be improved. The project will provide significantly improved theatre and support accommodation which will enable the Trust to provide a safer, more clinically effective service to all patients who are operated on in the main theatres. Improved privacy and dignity will be facilitated within the new accommodation. It is therefore felt that these proposals will not have an adverse impact on the Trust’s requirement to promote equality of opportunity and good relations between the different equality groups.

Theatres 1 – 4 Craigavon Area Hospital 101
The Human Rights Act 1998
Under the Human Rights Act 1998 the Trust must ensure that the way in which it carries out its functions does not breach the rights of its service users. It is felt that this proposal will not breach any of the Articles covered within the Act.
1144 PPRROOCCUURREEMMEENNTT In line with Health Estates’ recommendations on best value for money in procurement the Trust has entered into Performance Related Partnering (PRP) frameworks with a design team and a contractor for the design and construction of acute hospital facilities. The appointed Design Team and Contractor are currently undertaking two projects –
3. Construction of a new trauma and orthopaedics facility at Craigavon Area Hospital. This project is well underway and the building will be handed over for Trust commissioning in April 2010;
4. Extension and refurbishment of maternity and neonatal facilities at Craigavon Area Hospital – works commenced in July 2009 and construction is scheduled for completion by the end of March 2010.
The Trust is satisfied with the performance of both the design team and the contractor and proposes to re-appoint both for this project.
Theatres 1 – 4 Craigavon Area Hospital 102
1155 PPRROOJJEECCTT MMAANNAAGGEEMMEENNTT && PPOOSSTT PPRROOJJEECCTT EEVVAALLUUAATTIIOONN HM Treasury and Department of Finance and Personnel (DFP) guidance has highlighted the importance of setting up appropriate project management and post project evaluation procedures as part of the appraisal process. In addition, the arrangements for financing the project should also be considered and detailed. These are examined in turn in this section of the report.
15.1Project Management
It is proposed that this project will be managed in line with the DHSSPS guidance ‘Project Organisation and the Capital Investment Manual: Management of Construction Projects’.
The process of document preparation will be managed by the Project Manager with input from the Directorate of Acute Services and Health Estates Agency.
The following roles have been identified:
Project Owner: Gillian Rankin (Acting Director of Acute Services)
Project Director: Martin Kelly (Assistant Director of Corporate Planning)
Trust Project Manager:
Sandra Waddell (Head of Acute Planning)
Health Estates Project Manager:
Michael McCorry (Architect)
Project Board:
Martin Kelly, Assistant Director of Corporate Planning (Chair)
Michael McCorry, Health Estates Project Manager
Sandra Waddell, Trust Project Manager
Alan Metcalfe, Assistant Director of Estates
Jim Austin, Head of Estates Development and Capital Works
Eamon Mackle, Assistant Medical Director
Gillian Rankin, Acting Director of Acute Services
Stephen Hall, Assistant Medical Director
Carol Cassells, Senior Financial Management Accountant
Heather Trouton, Assistant Director, Surgery and Elective Care Division
Ronan Carroll, Assistant Director, Cancer & Clinical Services
Mary McGeough, Head of Anaesthetics, Theatres and ICU

Theatres 1 – 4 Craigavon Area Hospital 103
An outline programme for the project is given as Appendix 14. The table below summarises the major project stages along with the envisaged timescales. The target dates are dependent upon business case approval by the end of July 2010.
Table 24: Project Timetable for the Preferred Option
Phase Component *Target Date
Submission of business case to DHSSPS May 2010
Business Case Approval July 2010
Planning and Design (5 months) August – December 2010
Construction/refurbishment work commencement January 2011
Construction complete December 2012
Initial Post Project Evaluation March 2013
Full Post Project Evaluation November 2013
Assuming business case approval by July 2010, the new theatres would be completed and ready for handover to the Trust by the end of December 2012.
15.2Post Project Evaluation
This section presents the post project evaluation plan. This may be further refined as the project proceeds.
The following post-project evaluation arrangements are in place, however this may be amended as the project proceeds. The post project evaluation will be the responsibility of the Project Board and managed by the Project Director. The evaluation will be undertaken by the relevant business and clinical areas and if necessary will include staff from other HPSS organisations and/ or the DHSSPS.
Construction Phase
The initial stage of the evaluation will be undertaken on completion of the capital project and will seek to address the following questions:
! Was the project completed on time?
- Reasons sought for any delay.
! Was it completed at budget cost?
- Reason sought for any cost increase.
! Is the space and layout of the new theatre suite suitable for the purpose intended? Are there any modifications that need to be undertaken to make it fit for the purpose intended?
! Does the theatre suite meet the needs of the hospital?

Theatres 1 – 4 Craigavon Area Hospital 104
! What are key issues and lessons which can be learned to ensure similar problems do not arise in future?
In addition, the Trust Estates team will also make a number of observations during the commissioning phase relating to site preparation, materials used, site management and relationships with contractors.
Post Construction Phase
Approximately 9 to 12 months following the completion of the project, an assessment will be made of the effectiveness of the proposed theatre suite for carrying out the full range of operating procedures (including high-risk and emergency surgery). The key objective of the evaluation will be to assess if the benefits that are being derived from the project are in line with the Trust’s expectations. The areas to be assessed are set out below:
! The quality of accommodation provided;
! The range of procedures which can be undertaken;
! Improved working practices;
! Clinical effectiveness of the new accommodation;
! Disruptions caused; and
! The speed with which the project was implemented.
15.3Benefits Realisation Plan
The realisation of benefits is an increasingly important aspect of completing business cases. The Benefits Realisation Plan (BRP) for this project is given overleaf. It includes the actions which will be taken, the individual or group responsible and the method by which evaluation of success should be determined.
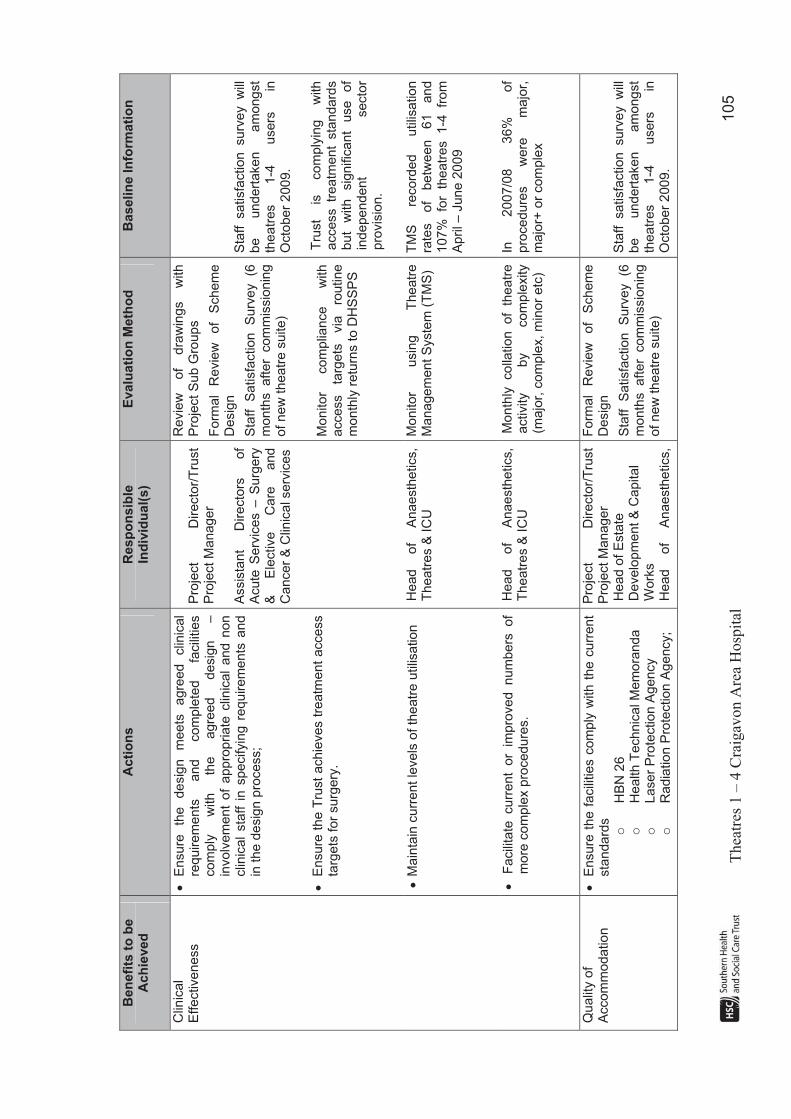
T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
105
Be
nefi
ts t
o b
e
Ac
hie
ve
d
Ac
tio
ns
R
esp
on
sib
leIn
div
idu
al(
s)
Eva
lua
tio
n M
eth
od
B
aselin
e In
form
ati
on
Clin
ica
l E
ffectiveness
!
En
sure
th
e
de
sig
n
mee
ts
agre
ed
clin
ical
requirem
ents
and
com
ple
ted
facili
ties
co
mp
ly
with
th
e
agre
ed
d
esig
n
–
invo
lve
me
nt
of
ap
pro
pria
te c
linic
al
and n
on
clin
ical
sta
ff i
n s
pecifyin
g r
equirem
ents
and
in th
e d
esig
n p
rocess;
!
Ensure
the T
rust
achie
ves t
reatm
ent
access
targ
ets
for
surg
ery
.
Pro
ject
Dir
ecto
r/T
rust
Pro
ject M
anager
Assis
tan
t D
irecto
rs
of
A
cu
te S
erv
ice
s –
Su
rge
ry
&
Ele
ctive
Care
and
Ca
ncer
& C
linic
al se
rvic
es
Revie
w
of
dra
win
gs
with
Pro
ject S
ub
Gro
up
s
Form
al
Revie
w
of
Schem
e
Desig
n
Sta
ff
Satisfa
ction
Surv
ey
(6
month
s after
com
mis
sio
nin
g
of new
theatr
e s
uite)
Monitor
com
plia
nce
with
access
targ
ets
via
ro
utine
month
ly r
etu
rns to D
HS
SP
S
Sta
ff satisfa
ction surv
ey w
ill
be
un
dert
ake
n
am
ong
st
the
atr
es
1-4
u
sers
in
O
cto
be
r 2
00
9.
Tru
st
is
com
ply
ing
with
access tr
eatm
ent
sta
ndard
s
but
with
sig
nific
ant
use
of
ind
epe
nd
en
t secto
r p
rovis
ion
.
! M
ain
tain
curr
ent le
vels
of th
eatr
e u
tilis
ation
Head
of
Anaesth
etics,
Th
ea
tre
s &
IC
U
Mo
nito
r usin
g
The
atr
e
Managem
en
t S
yste
m (
TM
S)
TM
S
record
ed
u
tilis
atio
n
rate
s
of
be
twe
en
6
1
an
d
107%
fo
r th
eatr
es 1-4
fr
om
A
pri
l –
Jun
e 2
00
9
!
Facili
tate
curr
ent
or
impro
ved num
bers
of
mo
re c
om
ple
x p
roced
ure
s.
Head
of
Anaesth
etics,
Th
ea
tre
s &
IC
U
Month
ly colla
tion of
theatr
e
activity
by
co
mple
xity
(majo
r, c
om
ple
x, m
inor
etc
)
In
2007/0
8
36%
of
pro
ce
du
res
were
m
ajo
r,
majo
r+ o
r com
ple
x
Qualit
y o
f A
ccom
mo
da
tio
n
!
Ensure
the f
acili
ties c
om
ply
with t
he c
urr
ent
sta
nda
rds
o
HB
N 2
6
o
He
alth
Technic
al M
em
ora
nd
a
o
Laser
Pro
tection A
gency
o
Radia
tion P
rote
ction A
gency;
Pro
ject
Dir
ecto
r/T
rust
Pro
ject M
anager
Head o
f E
sta
te
Develo
pm
ent &
Capital
Work
s
Head
of
Anaesth
etics,
Form
al
Revie
w
of
Schem
e
Desig
n
Sta
ff
Satisfa
ction
Surv
ey
(6
month
s after
com
mis
sio
nin
g
of new
theatr
e s
uite)
Sta
ff satisfa
ction surv
ey w
ill
be
un
dert
ake
n
am
ong
st
the
atr
es
1-4
u
sers
in
O
cto
be
r 2
00
9.

T
hea
tres
1 –
4 C
raig
avo
n A
rea
Ho
spit
al
106
Be
nefi
ts t
o b
e
Ac
hie
ve
d
Ac
tio
ns
R
esp
on
sib
leIn
div
idu
al(
s)
Eva
lua
tio
n M
eth
od
B
aselin
e In
form
ati
on
!
All
defe
cts
re
solv
ed
prior
to hand over
to
Tru
st
Th
ea
tre
s &
IC
U
Re
vie
w a
t fo
rma
l h
an
do
ve
r m
eeting
Str
ate
gic
Fit
!
Key s
erv
ice d
evelo
pm
ents
facili
tate
d;
!
Re
du
ction
in
th
e
curr
en
t le
ve
ls
of
independent secto
r activity
Tru
st P
roje
ct M
anager
Assis
tan
t D
irecto
r,
Surg
ery
& E
lective C
are
Assessm
en
t o
f im
ple
men
tation
of
key
se
rvic
e d
eve
lop
me
nts
lis
ted
in
sectio
n 4
.3.
Re
vie
w
of
ind
ep
en
de
nt
secto
r activity o
ne y
ear
after
com
ple
tion o
f pro
ject.
In
20
08
/09
8
26
in
pa
tie
nts
a
nd
30
05
day c
ase
pa
tien
ts
had tre
atm
ent in
the IS
.
Avoid
ance o
f D
isru
ption
!
Mo
nito
rin
g o
f in
cid
en
ts d
urin
g th
e p
roje
ct
!
Mo
nito
rin
g
of
un
pla
nn
ed
the
atr
e
sessio
n
cancella
tions d
ue to the p
roje
ct
Health
Esta
tes/T
rust
Pro
ject M
anagers
T
o be re
vie
wed at
month
ly
Pro
ject M
anagers
’ m
eeting
N/A
Speed o
f Im
ple
menta
tion
!
Monitoring o
f th
e p
roje
ct pro
gra
mm
e
Health
Esta
tes/T
rust
Pro
ject M
anagers
T
o be re
vie
wed at
month
ly
Pro
ject M
anagers
’ m
eeting
N/A