btb - computerised cbt. gps moodjuice beating the blues brief therapy psychology step 1 step 2 step...
TRANSCRIPT
BtB - Computerised CBT
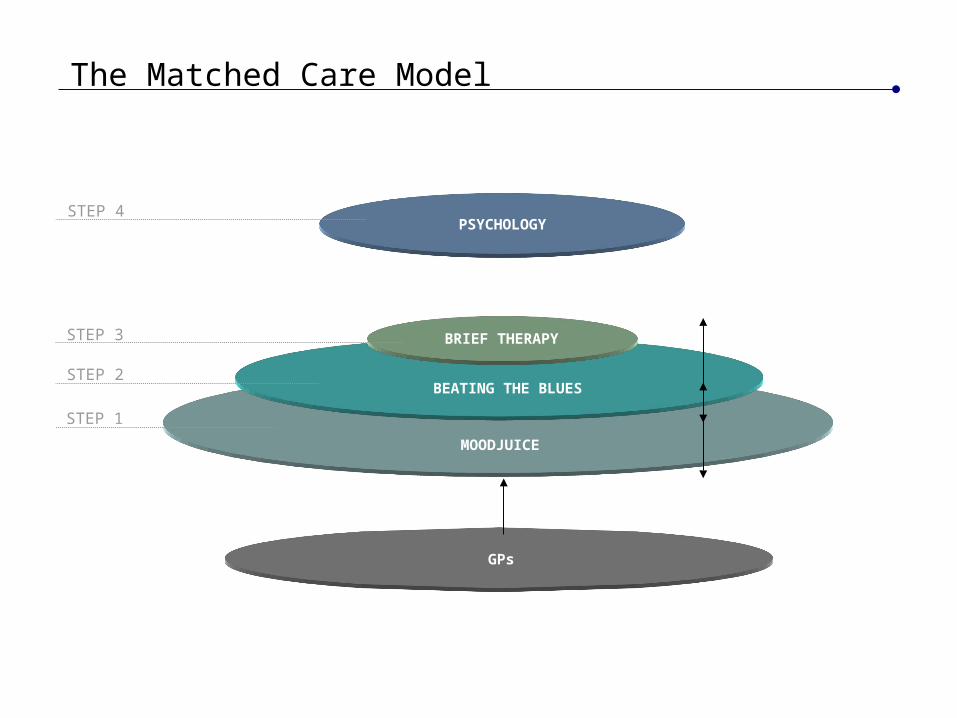
GPs
MOODJUICE
BEATING THE BLUES
BRIEF THERAPY
PSYCHOLOGY
STEP 1
STEP 2
STEP 3
STEP 4
The Matched Care Model
0.00
0.50
1.00
1.50
2.00
2.50
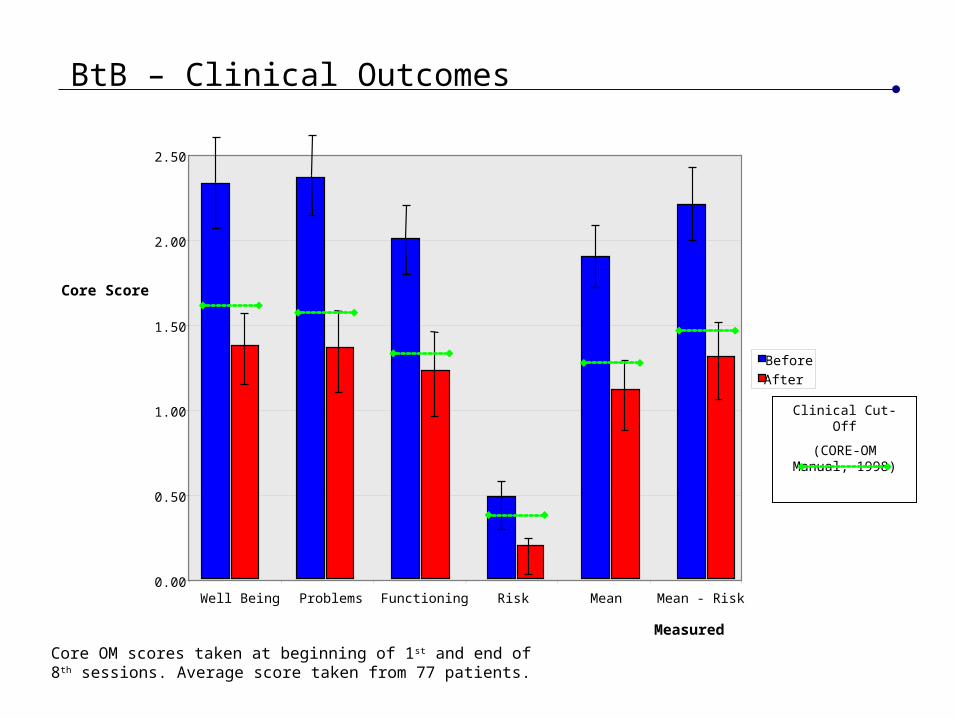
Well Being Problems Functioning Risk Mean Mean - Risk
Before
After
Clinical Cut-Off
(CORE-OM Manual, 1998)
Core OM scores taken at beginning of 1st and end of 8th sessions. Average score taken from 77 patients.
Measured
Core Score
BtB – Clinical Outcomes
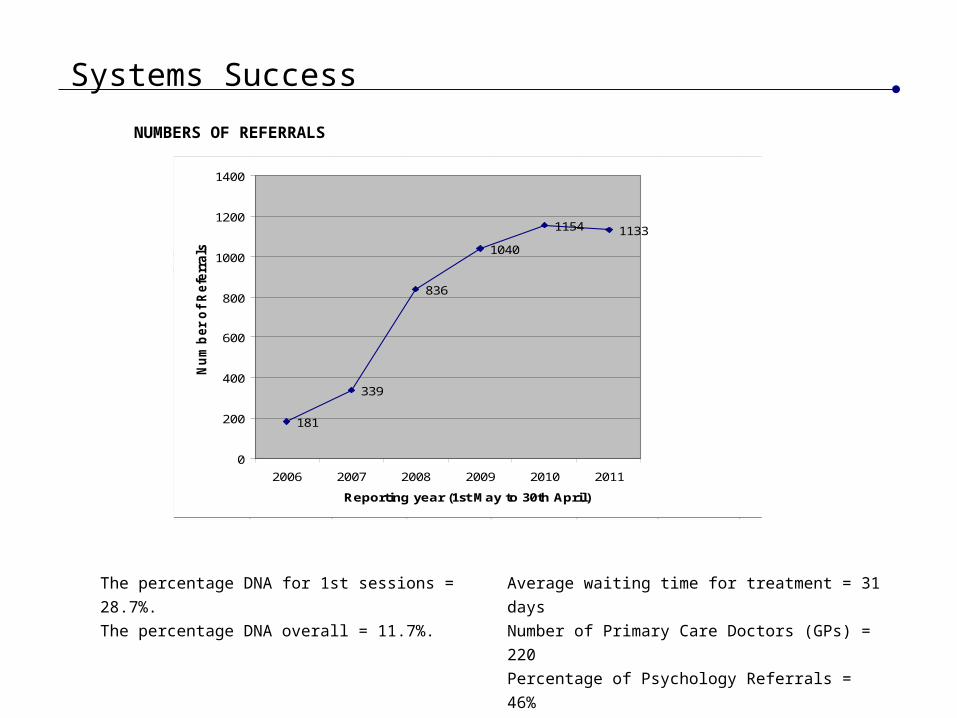
Systems Success
30/04/2006 30/04/2007 30/04/2008 30/04/2009 30/04/2010 30/04/2011181 339 836 1040 1154 1133
30/04/2006 30/04/2007 30/04/2008 30/04/2009 30/04/2010 30/04/2011Average Waiting Days 34 42 33 29 31 32Average Days between referral and appointment letter sent24 26 13 11 9 11
181
339
836
1040
1154 1133
0
200
400
600
800
1000
1200
1400
2006 2007 2008 2009 2010 2011
Reporting year (1st May to 30th April)
Nu
mb
er
of
Refe
rrals
NUMBERS OF REFERRALS
Average waiting time for treatment = 31 days
Number of Primary Care Doctors (GPs) = 220
Percentage of Psychology Referrals = 46%
The percentage DNA for 1st sessions = 28.7%.
The percentage DNA overall = 11.7%.
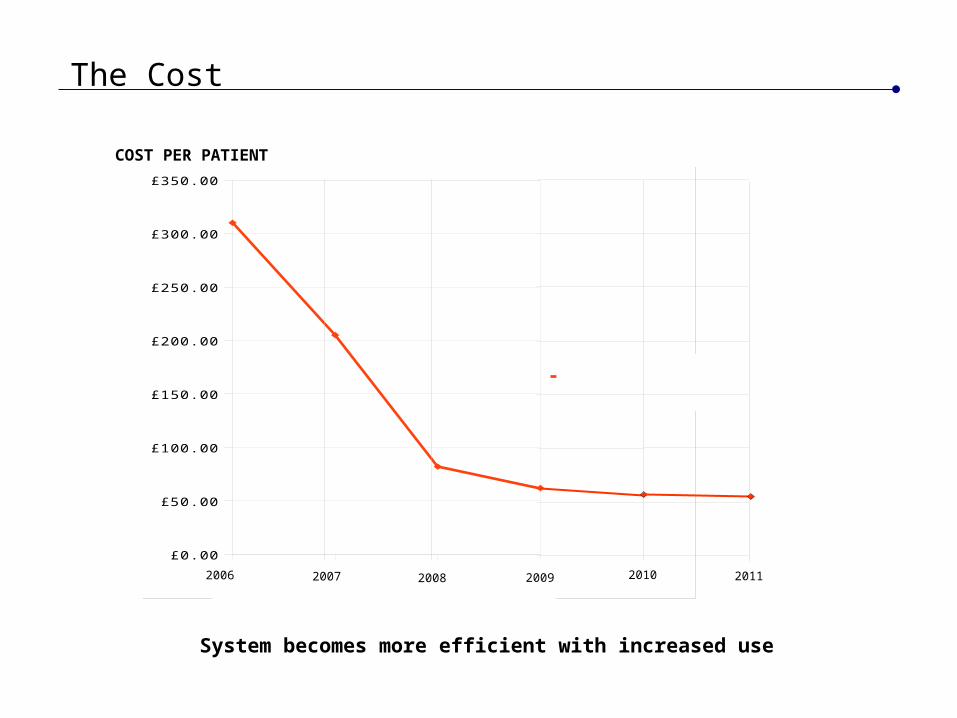
The Cost
System becomes more efficient with increased use
1 2 3 4
£0.00
£50.00
£100.00
£150.00
£200.00
£250.00
£300.00
£350.00
Column B
2009 20102006 2007 2008 2009 2011
COST PER PATIENT
Where to Start
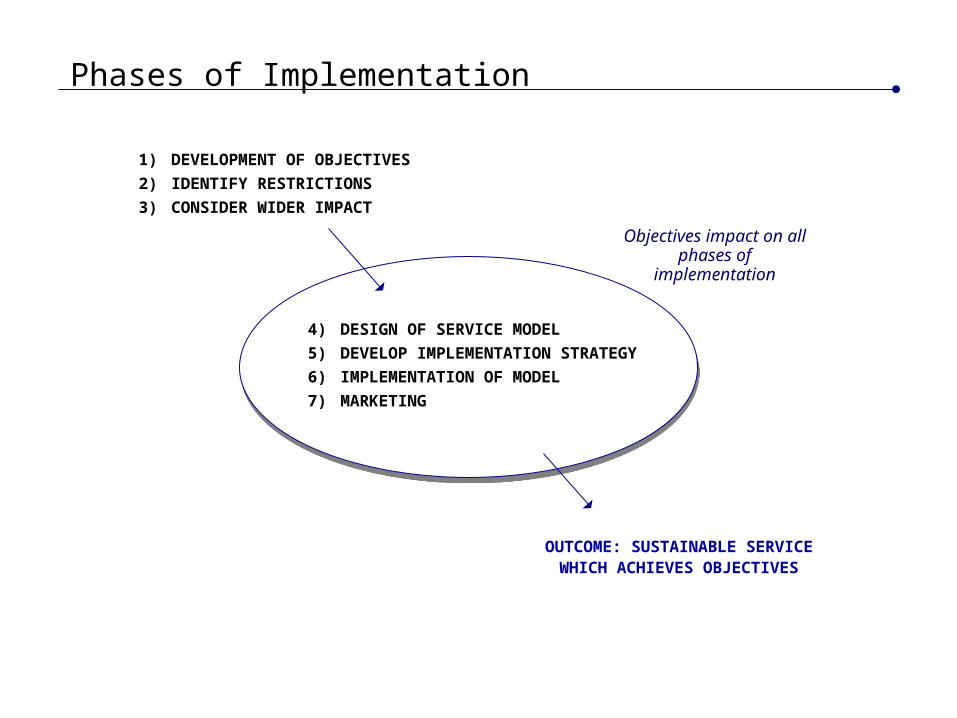
Phases of Implementation
4) DESIGN OF SERVICE MODEL
5) DEVELOP IMPLEMENTATION STRATEGY
6) IMPLEMENTATION OF MODEL
7) MARKETING
1) DEVELOPMENT OF OBJECTIVES
2) IDENTIFY RESTRICTIONS
3) CONSIDER WIDER IMPACT
OUTCOME: SUSTAINABLE SERVICE WHICH ACHIEVES OBJECTIVES
Objectives impact on all phases of
implementation
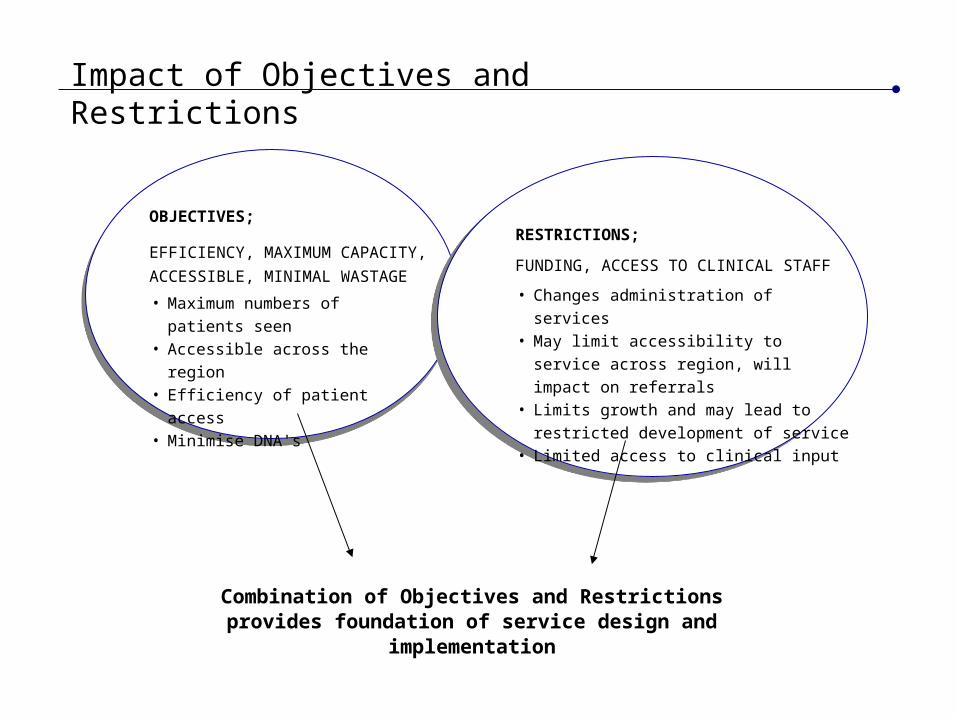
Impact of Objectives and Restrictions
• Maximum numbers of patients seen• Accessible across the region• Efficiency of patient access• Minimise DNA's
OBJECTIVES;
EFFICIENCY, MAXIMUM CAPACITY,
ACCESSIBLE, MINIMAL WASTAGE• Changes administration of services• May limit accessibility to service across
region, will impact on referrals• Limits growth and may lead to restricted
development of service• Limited access to clinical input
RESTRICTIONS;
FUNDING, ACCESS TO CLINICAL STAFF
Combination of Objectives and Restrictions provides foundation of service design and implementation
Example Models
Forth Valley and Tayside – Aims; efficiency, maximum capacity, accessible
Locations distributed across region
Clinical responsibility remaining with referrer
Different clinical models applied in psychology and GP’s
Phased developments with capacity expanding due to needs and readiness of service
Target time for referral to appointment
System working to maximum levels of patient throughput allowed by targets
Service part of matched/stepped care systems for added patient support
Additional Aim in Tayside – minimal wastage of treatments
Assign further appointment to patients that DNA
A Working Service
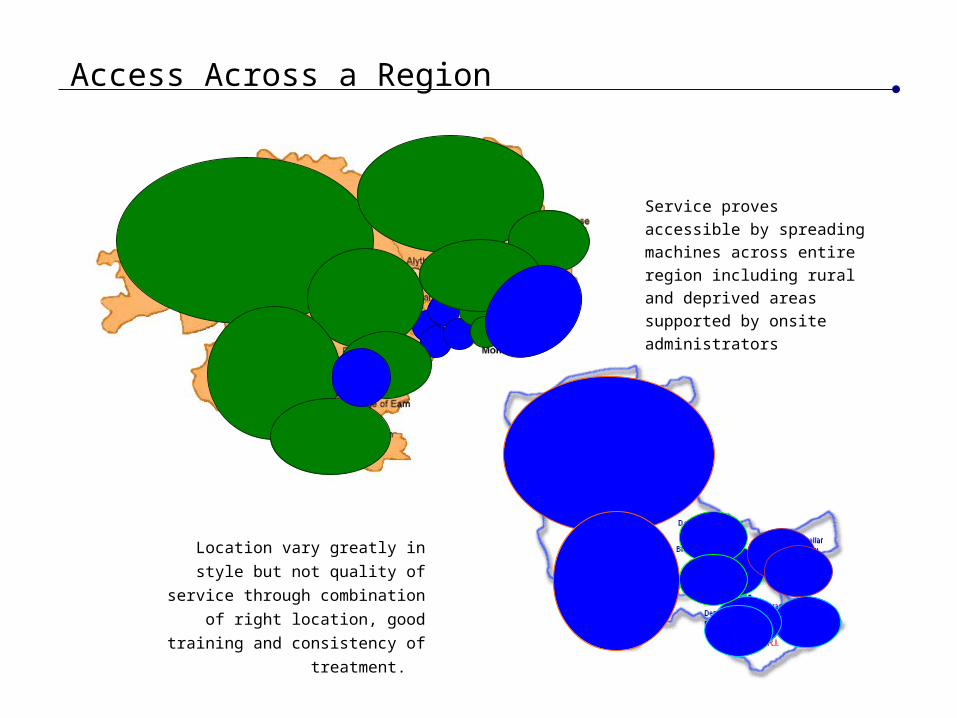
Access Across a Region
Location vary greatly in style but not
quality of service through combination
of right location, good training and
consistency of treatment.
Service proves accessible by
spreading machines across
entire region including rural and
deprived areas supported by
onsite administrators
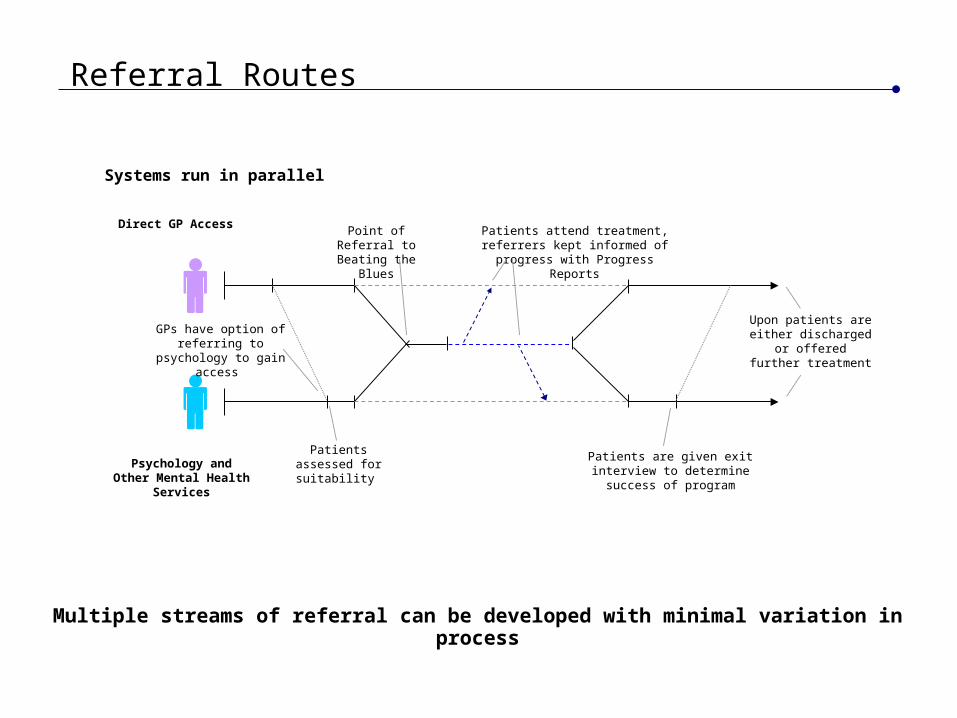
Referral Routes
Systems run in parallel
Direct GP Access
Psychology and Other Mental Health Services
Point of Referral to Beating the
Blues
Patients attend treatment, referrers kept informed of progress with
Progress Reports
GPs have option of referring to psychology to
gain access
Patients assessed for suitability
Patients are given exit interview to determine success of program
Upon patients are either discharged or
offered further treatment
Multiple streams of referral can be developed with minimal variation in process
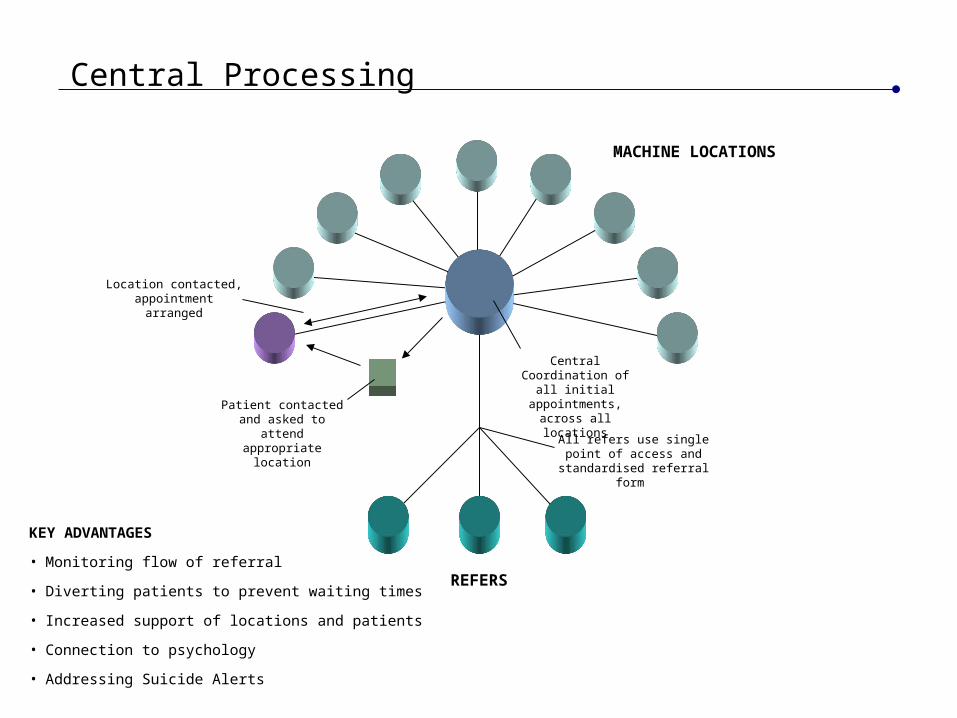
Central Processing
KEY ADVANTAGES
• Monitoring flow of referral
• Diverting patients to prevent waiting times
• Increased support of locations and patients
• Connection to psychology
• Addressing Suicide Alerts
REFERS
All refers use single point of access and standardised
referral form
Central Coordination of all initial appointments,
across all locations
MACHINE LOCATIONS
Patient contacted and asked to attend
appropriate location
Location contacted, appointment arranged
Key Aspects for Success
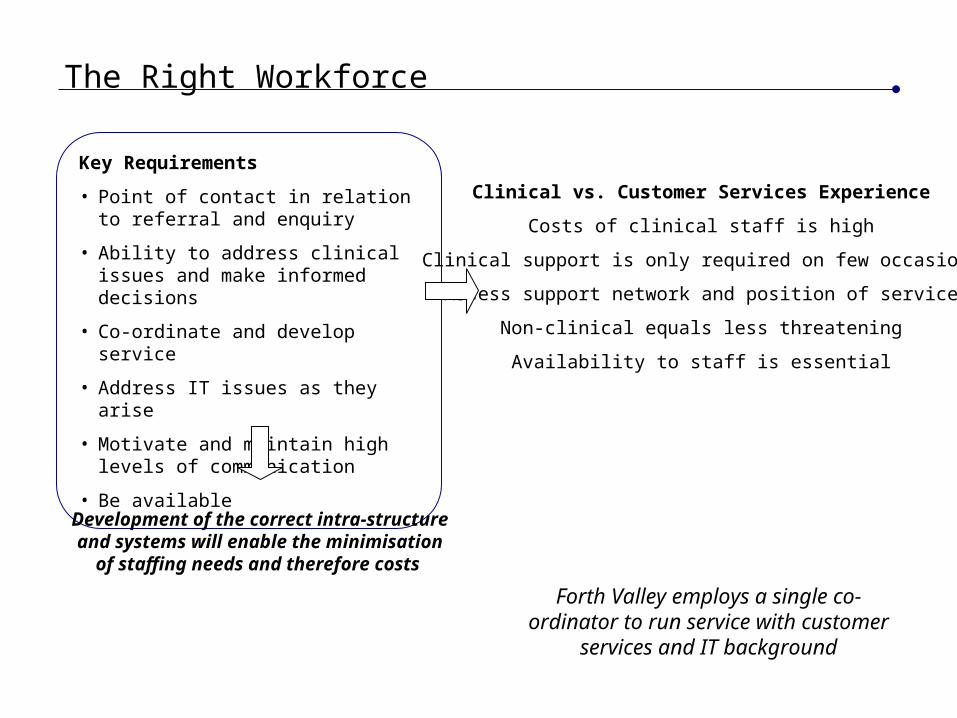
The Right Workforce
Clinical vs. Customer Services Experience
Costs of clinical staff is high
Clinical support is only required on few occasions
Assess support network and position of service
Non-clinical equals less threatening
Availability to staff is essential
Key Requirements
• Point of contact in relation to referral and enquiry
• Ability to address clinical issues and make informed decisions
• Co-ordinate and develop service
• Address IT issues as they arise
• Motivate and maintain high levels of communication
• Be available
Development of the correct intra-structure and systems will enable the minimisation
of staffing needs and therefore costs
Forth Valley employs a single co-ordinator to run service with customer
services and IT background
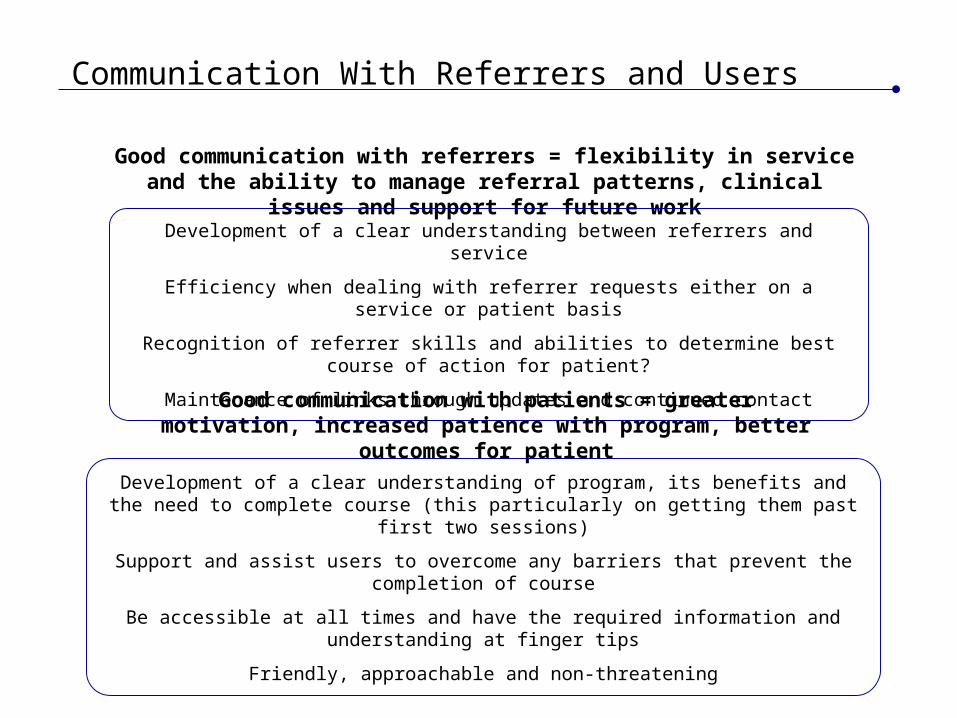
Communication With Referrers and Users
Good communication with referrers = flexibility in service and the ability to manage referral patterns, clinical issues and support for future work
Development of a clear understanding between referrers and service
Efficiency when dealing with referrer requests either on a service or patient basis
Recognition of referrer skills and abilities to determine best course of action for patient?
Maintenance of links through updates and continued contact
Good communication with patients = greater motivation, increased patience with program, better outcomes for patient
Development of a clear understanding of program, its benefits and the need to complete course (this particularly on getting them past first two sessions)
Support and assist users to overcome any barriers that prevent the completion of course
Be accessible at all times and have the required information and understanding at finger tips
Friendly, approachable and non-threatening
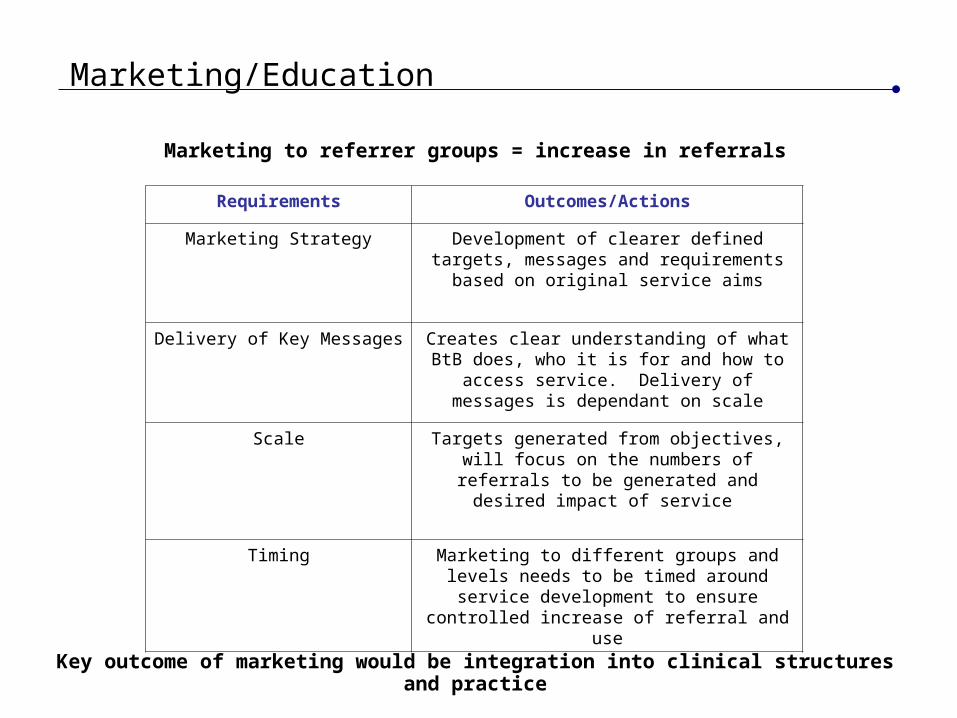
Marketing/Education
Marketing to referrer groups = increase in referrals
Requirements Outcomes/Actions
Marketing Strategy Development of clearer defined targets, messages and requirements based on original
service aims
Delivery of Key Messages Creates clear understanding of what BtB does, who it is for and how to access service. Delivery
of messages is dependant on scale
Scale Targets generated from objectives, will focus on the numbers of referrals to be generated and
desired impact of service
Timing Marketing to different groups and levels needs to be timed around service development to ensure
controlled increase of referral and use
Key outcome of marketing would be integration into clinical structures and practice
Our Advice
Genuine commitment to development and running service
Dedicated team with right individuals to implement and then run service
Allow focus to remain on patient by ensuring efficiency of process and administration
Do not over complicate the service and administration systems
Clearly defined responsibilities
Develop clear lines of communication with referrers and patients
Look to integrate service into exists structures
Get the right clinical and managerial support structures in place before you start
Do not underestimate complexity and subtly of task, having the right understanding and drive to develop the service within those involved is essential
Approaching the service with the right mind set is essentialClearly define objectives and requirements before thinking about logistics of service
The Local Impact
It has doubled the number of people receiving psychological therapy – 1100 new referrals a year to BtB
The waiting time for individual therapy has decreased. Before the start of the system, it was up to 2.5
years, now it is no more than 6 months
The waiting time for other forms of psychological therapy (non-individual) is lower than this, meaning
that a far higher proportion of people are meeting the 18 week waiting time target for psychological
treatment
Audit of BtB has revealed that referrals are appropriate and treatment is effective
The mild to moderate system is now having a significant impact on the population of Forth Valley.
There are about 12000 new case of depression and anxiety in per year about 2000 (or 1 in 6) are
receiving specialist psychological treatment, in addition to the people accessing Moodjuice (a total of
110,000 self-help resources are delivered through Moodjuice a year)
Preliminary data suggests that BtB is helping reduce the increase in antidepressant prescribing by GPs
Features of the Forth Valley Matched Care Model comments from Head of Primary Care Psychology
Greatest impact was achieved by integrating mild to moderate stepped care into existing service models and local structures such as GP Enhance Service.