board papers/2015/06... · web viewthe trust has one side room in berrow ward (side room 3) which...
TRANSCRIPT

INFECTION PREVENTION AND CONTROL
DIRECTOR OF INFECTION PREVENTION AND CONTROL
ANNUAL REPORT
April 2014-March 2015
Chris Perry
Director of Infection Prevention and Control (DIPC)
Selena Luff
Lead Nurse Infection Prevention and Control
April 2015
1

Contents Page 1. Executive Summary 3
2. Introduction 4
3. Overview of Progress 2014-2015 6
4. Infection Prevention and Control Arrangements 7
5. HCAI statistics and surveillance 8
6. Untoward incidents including outbreaks 12
7. Hand hygiene and aseptic protocols 14
8. Antimicrobial Stewardship 15
9. Infection Prevention And Control Policies 16
10. Education and training 16
11. Decontamination 17
12. Estates 18
13. Cleaning services 19
14. Infection Prevention And Control Plans And Ambitions 2015/16 21
2

WESTON AREA HEALTH NHS TRUST
INFECTION PREVENTION AND CONTROL ANNUAL REPORT – 2014/15
1.0 EXECUTIVE SUMMARY There were 2 Trust apportioned Meticillin Resistant Staphylococcus aureus (MRSA) bloodstream
infections in 2014/15. Post infection reviews were carried out which highlighted improvements were needed in Doctors’ awareness of MRSA topical treatment prescription and agreeing levels of care for seriously ill patients.
The Trust did not meet its Clostridium difficile (CDI) objective of no more than 17 Trust apportioned cases in 2014/5, finishing the year with 20 cases. Each case is now reviewed and assessed by our Commissioners as being avoidable or unavoidable and only 7 of the 20 cases were deemed to be avoidable.
There were 11 Trust apportioned Meticillin Sensitive Staphylococcus aureus (MSSA) bloodstream infections reported in 2014/15 against our locally agreed target not to exceed 3 cases. Post infection reviews identified trends in 4 of the cases that were related to peripheral vascular devices and this is where we will focus some work in 2015/16.
The Trust experienced a high level of Norovirus throughout 2014/15, leading to 21 separate ward closures. These outbreaks caused a major operational impact on the Trust, particularly in December 2014 when there was an unprecedented demand for our services. Each outbreak was managed in line with national guidance with the affected area being closed to admissions and strict hygiene and enhanced cleaning instigated.
Two categories of Surgical Site Infection Surveillance were included in the 2014/15 programme; repair of neck of femur and large bowel surgery. The infection rate for the neck of femur repair category for quarter 3 (July – September 2014) was above the national average; this was investigated and actions taken to prevent recurrence. No further infections have been reported.
Hand hygiene compliance remained good during 2014/15, with an average compliance rate of 95%. Validation audits concurred with this compliance rate.
To ensure that Infection Prevention and Control remains embedded throughout the organisation, monthly IPC performance reports have been established to disseminate this information Trust wide.
The Infection Prevention and Control team completed a comprehensive annual programme of work, including a programme of HCAI surveillance, policy review, audit, education and training.
Plans and ambition for 2015/16 include achieving zero MRSA infections and to have no avoidable cases of Clostridium difficile infection; to reduce MSSA bloodstream infections by 50% and the prevalence of urinary catheters by 20%.
3

2.0 INTRODUCTION
Welcome to the Weston Area Health NHS Trust’s Infection Control Report for 2014/15. The purpose of this report is to provide assurance that the Trust implements successful management, prevention and control of infection as a key factor in the quality and safety of the care of our patients and in the safety and well being of our staff and visitors.
Control of infection is an essential activity for all healthcare providers as the nature of hospital treatments increases risk of infection through exposure to other patients, and use of invasive devices, such as drips, which break the skin (one of the body’s most important defences against infection). Whilst healthcare associated infection is caused by many micro-organisms (germs) the ones most commonly associated with healthcare activity are MRSA, MSSA and Clostridium difficile (CDI). MRSA and MSSA belong to the same family of germs, although MRSA has become resistant to some of the antibiotics that are commonly used to treat infection. MRSA and MSSA can cause infections in wounds, skin, invasive devices and the blood (bacteraemia). Clostridium difficile is an infection of the bowel and is linked to use of antibiotics. Preventing healthcare associated infection focuses on the following actions:
Only admitting patients when necessary and discharging as soon as possible as risk of infection increases with length of stay in hospital
High standards of cleaning Hand hygiene and use of gloves and aprons Isolation in a single room when patients have transmissible infections Only using drips and drains when necessary and removing these as soon as they are no longer
needed Only using antibiotics when absolutely essential and for the shortest time possible
The Trust Board has collective responsibility for the prevention and control of infection in order to minimise, and where possible, eradicate the risks of infection. The Trust Board receives assurance that the Trust has mechanisms in place for this through bi-monthly performance updates and a quarterly infection control report to the Quality and Governance Committee. The Director of Infection Prevention and Control for the period of this report was the Director of Nursing who is a member of the Quality and Governance Committee. The Director reported on a regular basis directly to the Chief Executive. The Infection Control Committee is chaired by the Director of Infection Prevention and Control. The Committee produces an annual report for the Board and an annual plan for Board approval.
The Trust is committed to the exemplary application of infection prevention and control practice within all areas. This is achieved by ensuring that all staff are provided with access to infection control advice from a fully resourced Infection Control Team and Occupational Health Service, have access to personal protective equipment, training and policies. Individual and corporate responsibilities for infection
4

control are as stipulated in all job descriptions and contracts of employment with individual annual monitoring through the appraisal systems and personal development plans.
The policies and arrangements outlined above are to encourage, support and foster a culture of Ward to Board responsibility for the control and prevention of infection, with the intention of continually improving the quality and safety of patient care, and ensuring the full confidence of the local population in the quality of care the Trust delivers. The policies and arrangements accord with the aims and objectives of national policy and strategy.
Christine Perry
Director Infection Prevention and Control
5

3.0 OVERVIEW OF PROGRESS FOR 2014/15
We set ourselves 10 ambitious objectives for 2014/15 with progress set out in the table below.
We said we would…. How we didComply with the requirements of the Code of Practice for the Prevention and Control of Healthcare Associated Infection
We achieved thisWe declared overall compliance to these requirements throughout 2014/15.
Meet national targets for reduction of infection and to reduce further the incidence of Clostridium difficile infections; reduction of MRSA/MSSA bacteraemias will include a focus on invasive devices
We did not achieve thisWe reported 20 total and 7 avoidable CDI infections against a plan of no more than 17. We reported 2 MRSA blood stream infections against a plan of zero and 11 MSSA blood stream infections against a plan of no more than 3.
Undertake surveillance of surgical site infection, including post discharge surveillance, in 3 categories
We partly achieved thisWe managed to complete continuous surveillance in the neck of femur surgery category and 3 out of the 4 quarters of large bowel surgery.
Implement a flu prevention programme and vaccinate 75% or more of front line staff.
We partly achieved thisWe vaccinated 67% of staff. This was the highest vaccination rate in the local area
Develop an antimicrobial management group to implement national requirements for best practice in antimicrobial stewardship
We achieved thisCompliance to antibiotic prescribing has risen from 34% to 92% over the year
Develop and implement best practice in the diagnosis of and treatment of Urinary Tract Infections and Pneumonia using clinical pathways.
We achieved thisClinical pathways for these are in use across the Trust
Introduce the Carbapenemase-producing Enterobacteriaceae toolkit
We achieved thisStaff have access to this resource and assess patients correctly on admission
Embed the use of monthly practice improvement audits, proactively implementing changes as necessary.
We achieved thisThe results of this are included in overall performance dashboards for wards and departments
Reduce the percentage of patients with indwelling urethral catheters (and associated infections) to below the national average
We did not achieve thisIn the March 2015 national safety thermometer survey 25% of our patients had catheters compared to 17% nationally
Reduce the incidence of contamination incidents reported (sharp injuries and splashes) by 33% compared to 2013/4.
We did not achieve this36 injuries were reported in 2013/14 and 42 in 2014/15
6

4.0 INFECTION PREVENTION AND CONTROL ARRANGEMENTS
4.1 Infection Prevention and Control Team
The Infection Prevention and Control Team (IP&C Team) underwent a number of changes to personnel and roles during the year. At year end the Team consisted of:
Christine Perry – Director of Infection Prevention and Control Dr Ram Lakshmipathy – Infection Control Doctor (11 PAs) Dr Isabel Baker – Microbiologist Decontamination and Antimicrobial Lead (10.5 PAs) Selena Luff – Lead Infection Prevention and Control Nurse – 1.0 wte Angela Lovell – Infection Prevention and Control Nurse – 1.0 wte Laura Aparacio – Antimicrobial Pharmacist (temporary post to end of March 2015) – 1.0 wte Gemma Summerhayes – Administrator (role shared with safeguarding and tissue viability) – 1.0
wte
Plans are in place for 2015/16 to strengthen the clinical and administrative support as well as to ensure appropriate antimicrobial pharmacist support.
4.2 Infection Prevention and Control Committee
The Committee meets quarterly. Members of the Committee are:
Director of Nursing / Director of Infection Prevention and Control (Chair) Medical Director (Deputy Chair) Infection Control Doctor / Consultant Medical Microbiologist Antimicrobial Pharmacist Infection Prevention and Control Nurses Head of Governance Divisional Representatives – Head of Nursing from each Division Matron Representative Theatre/Endoscopy representative Facilities Manager/Housekeeper Decontamination Lead / Head of Estates Member of Patient Council
The duties of the Committee are:
Oversee and direct all Infection Prevention and Control activity within the Trust and provide the Chief Executive with relevant information and advice.
Oversee and direct all decontamination and environmental decontamination activity within the Trust and provide the Chief Executive with relevant information and advice
7
Interpret and advise on national Infection Prevention and Control policy, relating it to the local situation. Ensure NHS core standards, and Department of Health recommendations on infection prevention and control are implemented.
Review infection surveillance data, monitor performance and make recommendations for further action Introduce,
Maintain and approve infection prevention and control policies and guidelines that promote a quality patient experience.
Ensure the Trust meets its statutory requirements in relation to Infection Prevention and Control and the decontamination of medical and surgical equipment, eg Health Act 2008 – Code of Practice and Care Quality Commission outcome 8.
Ensure that training and supervision systems are in place for all staff and contractors working within the Trust and that those systems are regularly monitored.
Recommend an annual infection prevention and control programme; monitor and review the progress of the programme and produce an annual report.
The annual committee review demonstrated that all these duties had been achieved.
5.0 HCAI STATISTICS AND SURVEILLANCE
5.1 MRSA (Meticillin Resistant Staphylococcus aureus) bloodstream infections
All MRSA bloodstream infections are reported nationally and are assigned as being related to the Trust or not related to the Trust (that is acquired in community or other settings) following a post infection review.
0
5
10
15
20
25
2006/7 2007/8 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15
MRSA Reported Cases by Year
Non-WAHT cases
WAHT cases
8

Full investigations were carried out for the two cases reported in 2014/15. The investigations highlighted improvements were needed in Doctors’ awareness of MRSA topical treatment prescription and also the empirical treatment needed for these patients and agreeing levels of care for seriously ill patients.
There is a programme of screening for MRSA in place when patients are admitted as emergency patients or for planned surgery. Compliance for emergency patients is 94% and for planned patients is 98%.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15Planned 100% 95% 95% 100% 100% 95% 100% 100% 90% 100% 100% 100%Emergency 90% 95% 100% 100% 95% 80% 100% 100% 90% 85% 95% 95%
MRSA Screening Compliance 2014/15
New national guidance was issued in 2014/15 suggesting a return to risk based screening as opposed to the more full screening currently undertaken by the Trust. Minor changes only to the Trust’s screening programme have been agreed following this national change which will only apply to those patients who attend for day procedures.
5.2 MSSA (Meticillin Sensitive Staphylococcus aureus) bloodstream infections
The same reporting and investigation for MSSA bloodstream infections is carried out as for MRSA infections.
There has been a marked increase in the cases of MSSA infection this year. Post infection reviews for these cases have shown the need to focus on insertion and care of invasive devices such as catheters and drips. A programme of focused work has been undertaken and will continue into 2015/16.
9

0
5
10
15
20
25
30
35
2010/11 2011/12 2012/13 2013/14 2014/15
MSSA Reported Cases by Year
Non-WAHT cases
WAHT cases
5.3 Clostridium difficile infections (CDI)
In 2014/15 a new process was put in place nationally whereby each CDI that occurred after a patient has been in hospital for more than three days was reviewed and assessed by our Commissioners as being avoidable or unavoidable. Of the 20 total cases reported by the Trust in 2014/15, only seven of these were deemed to be avoidable.
0
50
100
150
200
250
2007/8 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15
CDI Reported Cases by Year
Non-WAHT cases
WAHT cases
10

To prevent CDI the following actions were put in place during 2014/15:
Increased focus on antimicrobial prescribing with compliance to policy improved from 34% to 92%
Replacement of reusable bed pans and disinfection equipment with disposable products Implementation of a revised diarrhoea risk assessment tool Agreement of a policy to use probiotics as a preventative measure during winter months when
antibiotic use tends to be higher Increased collaboration with GPs and other community colleagues to reduce the use of
antibiotics outside of hospital
5.4 E. coli blood stream infections
Most strains of E. coli form part of the bacteria normally in the bowel, however, they can cause urinary tract and blood stream infections. Of the 128 infections reported, 85% were admitted from the community with the infection.
5.5 Carbepenemase Producing Enterobacteriaceae (CPE)
CPEs are a group of bacteria that usually live harmlessly in the gut of humans or animals but have become very resistant to some antibiotics. As with E. coli, they can cause infections of the urine system and the blood stream.
Due to the serious nature of these bacteria, it is now a requirement to report patients that are admitted to the hospital, or who have these bacteria identified in specimens sent to the hospital laboratory. In 2014/5 the Trust reported one case which was managed appropriately with the correct isolation and effective antibiotics.
5.6 Surgical Site Infection Surveillance
It is a mandatory requirement for NHS Trusts in England to complete one category of orthopaedic surgical site infection surveillance for a minimum of a three month period each year, using the National Surgical Site Infection Surveillance service (NSSIS). This service is co-ordinated by the Communicable Disease Surveillance Centre at Public Health England in Colindale.
Continuous surveillance into neck of femur surgery was undertaken; a higher than expected level of infection was reported during the July- September surveillance quarter. This was investigated and actions taken to prevent reoccurrence. No further infections have been reported in this surveillance category. Large bowel surgery was monitored for three quarters of the year; rates of infection were reported in line with the national average.
Results of the surveillance are disseminated to the Medical Director, Consultant Surgeons and Divisional Management who take appropriate actions as required. They are also reported at the Infection Prevention and Control committee on a quarterly basis.
11

5.7 Catheter Associated Urinary Tract Infection
A monthly snap shot survey of patients with urine infections related to catheter use is undertaken as part of national reporting to the NHS Safety Thermometer. In 2014/15 a total of 58 patients were identified in this survey as having a catheter associated urine infection with only 3 of these patients developing the infection whilst in hospital.
6.0 UNTOWARD INCIDENTS INCLUDING OUTBREAKS
6.1 Outbreaks
The Trust experienced a high level of Norovirus throughout 2014/15, resulting in a number of ward closures as set out in the table below. There were a total of 21 outbreaks that affected 296 patients, 66 staff with 7 different wards closed for a total of 193 days.
Ward Date ward closed
Date ward opened
No of patients affected
No of staff affected
No of days ward closed
Kewstoke 24.08.2014 30.08.2014 14 5 6Kewstoke 08.09.2014 16.09.2014 21 7 8Uphill 11.09.2014 03.09.2014 11 5 8Berrow 01.10.2014 10.10.2014 12 0 9Harptree 26.11.2014 02.12.2014 10 1 6Berrow 28.11.2014 05.12.2014 18 10 7Harptree 08.12.2014 12.12.2014 9 0 4Kewstoke 12.12.2014 17.12.2014 12 2 5Uphill 12.12.2014 22.12.2014 19 4 10Berrow 15.12.2014 23.12.2014 19 4 8Cheddar 19.12.2014 24.12.2014 9 1 5Uphill 30.12.2014 13.01.2015 12 2 14Berrow 31.12.2014 12.01.2015 15 1 12Kewstoke 01.01.2015 16.01.2015 17 1 15Hutton 06.02.2015 24.02.2015 19 3 18Berrow 17.02.2015 24.02.2015 11 4 7Uphill 02.03.2015 17.03.2015 19 5 15Stroke 03.03.2015 14.03.2015 13 2 11
Kewstoke 05.03.2015 16.03.2015 17 6 11Uphill 25.03.2015 30.03.2015 8 1 5Stroke 26.03.2015 04.04.2015 11 2 9Total - - 296 66 193
12

Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-150
10
20
30
40
50
60
70
6 8 515 11
824
20
9 7
20
76
4
8
18
16
Number of days ward closed
StrokeHuttonCheddarHarptreeBerrowHarptreeUphillKewstoke
Month
Days ward closed
This presented many operational challenges for the Trust as well as significant pressure on the housekeeping staff to undertake enhanced cleaning during periods of ward closure and deep cleans of whole wards before re-opening.
In addition to the IP&C Team reviewing management outbreak, the Trust was supported by the Trust Development Agency with review by their infection control expert advisers. The internal and external reviews recommended some changes to the cleaning regime, which were implemented in December 2014 and continued focus on clinical practice on closed wards. The alcohol hand sanitising agent was changed in early 2015 to one that has increased effectiveness against the gastroenteritis viruses. Although correct application of national guidelines to prevent and manage Norovirus outbreaks was in place, it was necessary for the Trust to adopt additional measures, such as longer ward closures, to effectively halt the outbreaks.
The high levels of Norovirus were also present across the health community in North Somerset. The Trust is actively working with colleagues across the health system to enhance our preparedness for gastroenteritis outbreaks.
6.2 MRSA and CDI deaths
In 2014/15 there were 0 deaths where MRSA was identified as the primary cause of death and 0 deaths where CDI was identified as the primary cause.
6.3 Serious incidents requiring investigation
In addition to the two MRSA blood stream infections reported as serious incidents, the Norovirus outbreak in December 2014 was also reported due to its impact on the running of the Trust. There was one further serious incident reported where an item of medical equipment was not completely decontaminated between use. No patient harm occurred and procedures were amended as a result of this to prevent any further occurrence.
13

7.0 HAND HYGIENE AND ASEPTIC PROTOCOLS
7.1 Hand hygiene
Hand hygiene is considered to be the most important infection prevention measure. Alcohol hand gels are available at the patients’ chair or bedside as this is the point where hand hygiene is recommended by the World Health Organisation. The Trust also provides alcohol hand gel at the entrances to the hospital, wards and departments for optional use by staff and visitors. All staff are expected to be ‘bare below the elbows’ (that is not wearing watches, bracelets or stoned rings) and with short sleeves or long sleeves rolled up when they are in direct contact with a patient or their immediate environment.
Compliance to hand hygiene is monitored in wards and department monthly. Compliance for 2014/15 is outlined in the chart below.
Apr-14
May-14
Jun-14Jul-1
4
Aug-14
Sep-14
Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Mar-15
Total
annual
0%
20%
40%
60%
80%
100%
120%97% 97% 98% 95% 99% 95% 98% 96% 99%
74%91%
99% 95%
Trust Hand Hygiene Audit
Trust Hand Hygiene Audit
A new audit tool was implemented in Jan 15
7.2 Aseptic Protocols
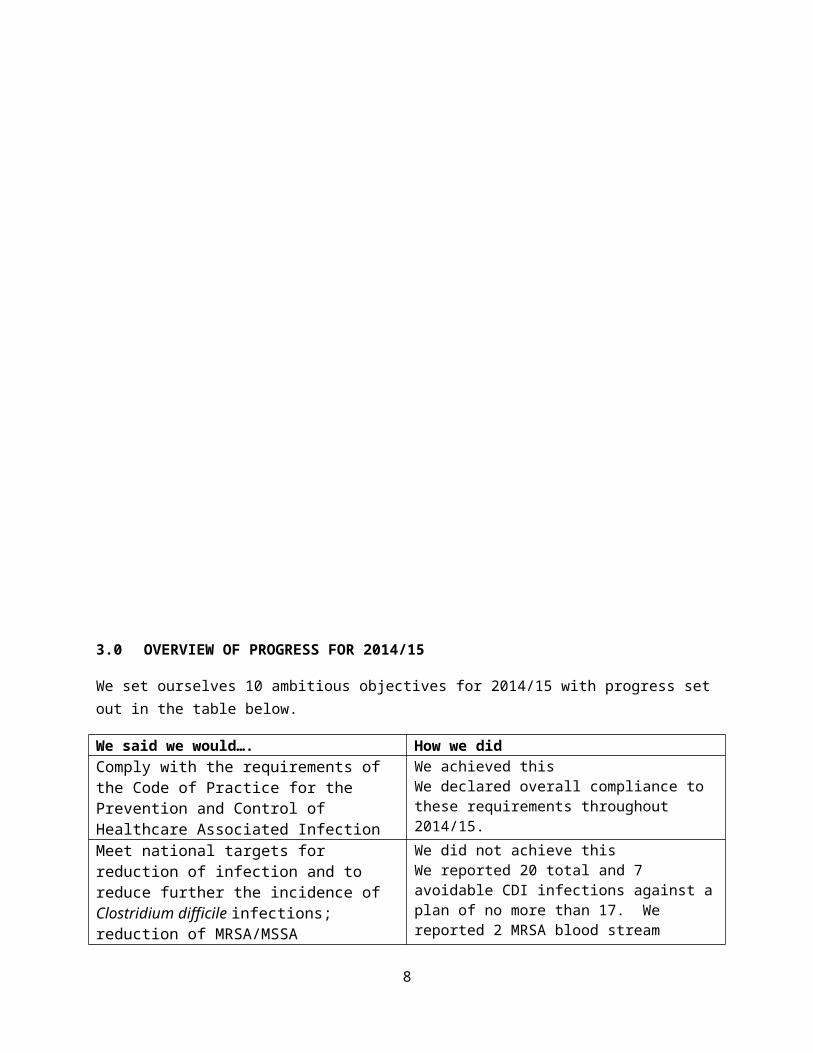
Adherence to aseptic technique when accessing a site on the body susceptible to infection is essential to prevent infection. This includes wounds and drips and drains. Care of devices such as drips, drains and catheters is part of the Trust’s training programme. Insertion and management of invasive devices is audited monthly by Ward Sisters or one of their staff designated to support infection prevention. The results of these audits are shown in the chart below.
14

Apr-14
May-14
Jun-14Jul-1
4
Aug-14
Sep-14
Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Mar-15
0%
20%
40%
60%
80%
100%
120%
Device Compliance
PVC Insertion & Ongoing Care Urinary Catheter Ongoing Care
Month
To improve care further, the Trust commenced an enhanced audit and training for aseptic non-touch technique (ANTT) in January 2015; this will continue in the 2015/16 programme of work.
8.0 ANTIMICROBIAL STEWARDSHIP
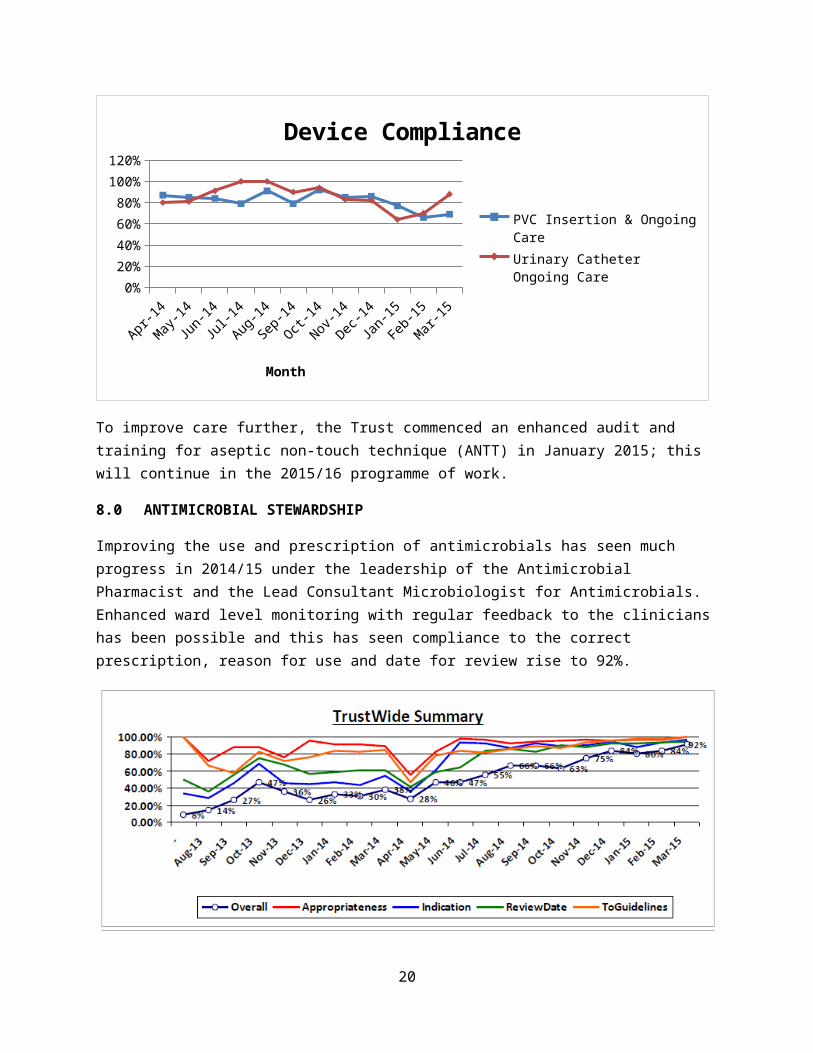
Improving the use and prescription of antimicrobials has seen much progress in 2014/15 under the leadership of the Antimicrobial Pharmacist and the Lead Consultant Microbiologist for Antimicrobials. Enhanced ward level monitoring with regular feedback to the clinicians has been possible and this has seen compliance to the correct prescription, reason for use and date for review rise to 92%.
An Antimicrobial Stewardship Committee has been established and a strategy for Antimicrobial Stewardship has been produced and approved by the Trust’s Quality and Governance Committee.
The following antimicrobial prescribing policies were reviewed in 2014/15:
15

Medical Critical Care (ITU) Obstetric and Gynaecological Management of urinary tract infection Collaborative Care IV to oral switch
New guidelines were introduced for the prescription and monitoring of gentamicin, teicoplanin and vancomycin.
An application for smartphones with the antibiotic guidelines was introduced, to improve access to these.
Training and education for clinicians and pharmacists has been increased, and closer collaboration with Primary care established. We participated in the European Antibiotic Awareness Day on the 18 th November with a Trust wide campaign to raise awareness.
The improvements in this area have been possible through additional resourcing to support a full time antimicrobial pharmacist post. With the cessation of this additional funding, options to ensure the maintenance of the improvements are being considered.
9.0 INFECTION PREVENTION AND CONTROL POLICIES
IP&C guidelines and policies are available for staff access through the Trust Intranet. The following policies were revised or implemented in 2014/15:
Meningitis Control of Legionella Transmissible Spongiform
Encephalopathy (CJD) Hand hygiene Isolation Standard Precautions Viral Haemorrhagic Fevers (including
Ebola)
Decontamination of Mattresses Seasonal Influenza Aseptic Technique Insertion and Care of Central Lines Insertion and Care of Peripheral Lines CPE Blood Cultures Decontamination Operational Policy
10.0 EDUCATION AND TRAINING
Attendance at IP&C training is mandatory for staff with update on a two-yearly basis with compliance levels set at 90%. The 90% standard has not been achieved throughout 2014/5 as demonstrated below.
16

AprilMay June
July
August
Septem
ber
October
November
December
January
February
March
Total
Annual83.00%
84.00%
85.00%
86.00%
87.00%
88.00%
89.00%
90.00%
88.1%87.6%
88.7% 88.5%
86.7%
85.7% 86.0%85.2%
87.0%86.4%
87.2% 87.5%0.870000000000001
Training compliance
Quarter 1Quarter 2Quarter 3Quarter 4Total %
The IP&C Team works closely with the Trust’s training team to deliver the programme and to improve the compliance level.
The IP&C Team undertake local training sessions and are supported in local awareness and training by ward/department based link nurses. The link nurses have met together as a group on 7 occasions in 2014/15 and have contributed to IP&C prevention activities through:
monthly auditing of hand hygiene practices/ infection prevention practices promoting 5th May Hand Hygiene Day using flash cards for compliance and the Glo box on
wards attending and assisting with the Isolating Iris teaching room in August and participation in the
influenza campaign.
They have received educational/teaching sessions on the following subjects:
multi resistant organisms wound infections aseptic non-touch technique catheter associated urinary tract infections deep cleans and decontamination influenza
11.0 DECONTAMINATION
The Decontamination Lead for the Trust is Jeff Legge, Head of Estates. The Trust Authorising Engineer is Tom Hall. Decontamination activities are reported through the IP&C Committee. The Trust contracts with Nuffield Hospitals for an off-site sterilization service. This contract is monitored regularly and there have been no incidents of concern with this contract.
17

Decontamination of Endoscopes was audited by an external IP&C adviser following the serious incident noted above. The service was found to be overall compliant with the standards set, with recommendations made for changes to documentation, review of competence recording and update of operating protocols.
The Pathology Sterilizer is managed by the Head of Pathology Services with confirmation that the appropriate testing and maintenance has been carried out in year.
11.1 Washer Disinfectors
As further measures to prevent cross contamination the washer disinfector machines which decontaminated patient wash bowls, bed pans and urinals were removed from ward sluices in February 2015. These have now been replaced with disposable bowls and related products. Each ward has been fitted with an industrial macerator which pulps down the disposable products which is then flushed into the water drainage system. The remaining washer disinfector within the Theatre complex will be removed as part of the upcoming refurbishment.
12.0 ESTATES
12.1 Ventilation System Compliance
Following an instruction from Estates & Facilities Management a ventilation survey was completed of both Cheddar and Hutton wards and their respective side rooms. The report confirms that the hospital relies on natural air movement for ventilation around the majority of wards. Cheddar ward side rooms have some comfort cooling ventilation, but these rooms should not be classed as either negative or positive pressure rooms. The Trust has one side room in Berrow ward (side room 3) which is used as a negative pressure room but does not meet the full specification of HTM-03. If this room is to be used as a negative pressure room there will be a requirement to up-grade this room to the current HTM-03 ventilation standard.
The Trust has recently appointed an Authorised Engineer Ventilation (AEV) who will complete an audit of the existing Trust ventilation systems and processes.
A programme of work is being produced by Estates & Facilities to clean the air intake and extract grills across the main hospital site, once this programme is finalised this will form part of the planned maintenance programme and be included on Planet-FM for implementation.
12.2 Progress with Legionella & Pseudomonas Prevention
As part of the Trust compliance for water management a water safety group was established. This group will review current best practice to ensure that the Trust has a proactive water management process in place. This group will take responsibility for evaluating the current and proposed inspection and testing regime introduced by the Estates & Facilities Management department.
18

A chlorine dosing system (Abulox) was introduced to minimise the risks of Legionella and Pseudomonas aeruginosa production which are both water borne bacteria. These bacteria can pose serious harm to patients if they are not controlled. Prior to the introduction of Abulox and after its initial installation, filtered showerheads were in use as a further preventative measure. This pre dosing provision is a proactive measure in monitoring the water quality throughout the water systems across the Trust.
Both Legionella and Pseudomonas are under a 6 monthly external consultant testing.
12.3 Central Waste Storage Area
The sluice rooms within ward areas were deemed non-compliant due to lack of space and resulting in poor segregation of clean and dirty items. To resolve this issue it was agreed that a central waste and used linen storage area should be built centrally in the hospital. This work was completed in January 2015 and the central waste store is situated on level one adjacent to pathology.
12.4 Theatre Refurbishment
Main theatres within the Trust have not been subject to full renovation of refurbishment since they were installed during the 1980s.
An infection prevention and control audit completed during 2013 identified a number of risks requiring remedial building alteration to provide appropriate flow of clean and dirty instruments and waste.
The refurbishment commenced in March 2015 and once completed all the issues raised in the audit will be addressed including:
Forming new dirty utility room, including fitting new door set and sanitary ware. Replacement of all air handling units Replacement of ultra clean canopies Replacement of service lift Replacement of cill boards Replacement of all flooring Wall repairs & decoration including wall protection
13.0 CLEANING SERVICES
13.1 Management Arrangements
The cleaning management is completely in-house. Cleaning staff are managed by the Facilities Team, with an average 2.48 WTE cleaning staff per ward. There is a process for responding to urgent calls to deep clean bed spaces or side rooms 24 hours a day, although the pressure on this service has been such in 2014/15 that the present arrangements require review.
19
13.2 Monitoring Arrangements
Monitoring arrangements are not currently in line with the National Specifications of Cleaning, although cleaning specifications are. The ‘Credit 4 Cleaning’ Software is used to carry out monthly environmental and cleanliness audits in very high risk areas. The average cleaning score for 2014/15 in high risk areas was 92%. Ward Sisters carry out monthly cleanliness audits of their ward areas with the average cleaning score for 2014/15 being 93%.
13.3 Budget Allocation
The cleaning budget is allocated through Facilities. There has been no reduction in budget for 2014/15 and a slight increase has been agreed for 2015/16.
13.4 Patient Led Assessment of the Care Environment (PLACE) Assessments 2014
The most recent nationally available PLACE self-assessment was carried out in the Trust on the 20 th March 2014 and results are as follows.
Weston Area Health NHS Trust England AverageCleanliness 99.10% 97.25%Food and Hydration 93.52% 88.79%Privacy, Dignity and Well being 86.74% 87.73%Condition, Appearance and Maintenance
96.06% 91.97%
13.5 User Satisfaction
The House Keeping Team carry out regular surveys of patient satisfaction. The results of these show:
92% rated the overall cleaning standards of the ward area were scored either good or excellent. 94% rated the cleanliness of their bed area were scored as either good or excellent. 92% rated the cleanliness of the ward toilets and bathrooms as either good or excellent 99% of patients rated the housekeeping staff very friendly.
20

13.6 Deep Cleaning Programme
An annual deep clean programme of wards is carried out by a deep clean of a specific area of each ward being carried out daily; this is monitored by the Housekeeping Supervisory Team. In addition to these planned deep cleans, the Housekeeping Team carried out the following deep cleans in 2014/15.
Number of cleansSingle rooms 2268Ward Bays 24Whole Wards 20
14.0 INFECTION PREVENTION AND CONTROL PLANS AND AMBITIONS 2015/16
Reducing healthcare associated infections remains a priority objective for the Trust in 2015/16. Key ambitions for 2015/16 will be:
Achieving zero MRSA blood stream infections Reducing MSSA blood stream infections by 50% Achieving no more than 18 Clostridium difficile infections Reducing the number of sharps injuries by 25% Reducing the prevalence of urinary catheters in use across the Trust by 20% Monitoring the number of surgical site infections in neck of femur, large bowel and breast
surgery Achieving over 90% training compliance Continuing to monitor and achieve a high compliance to hand hygiene Continuing the roll out of ANTT training and competence checks Assurance that all ventilation and airflows meet the requirements of HTM 03-01 Maintain an effective antimicrobial stewardship programme
21