bleeding physio
TRANSCRIPT
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 414
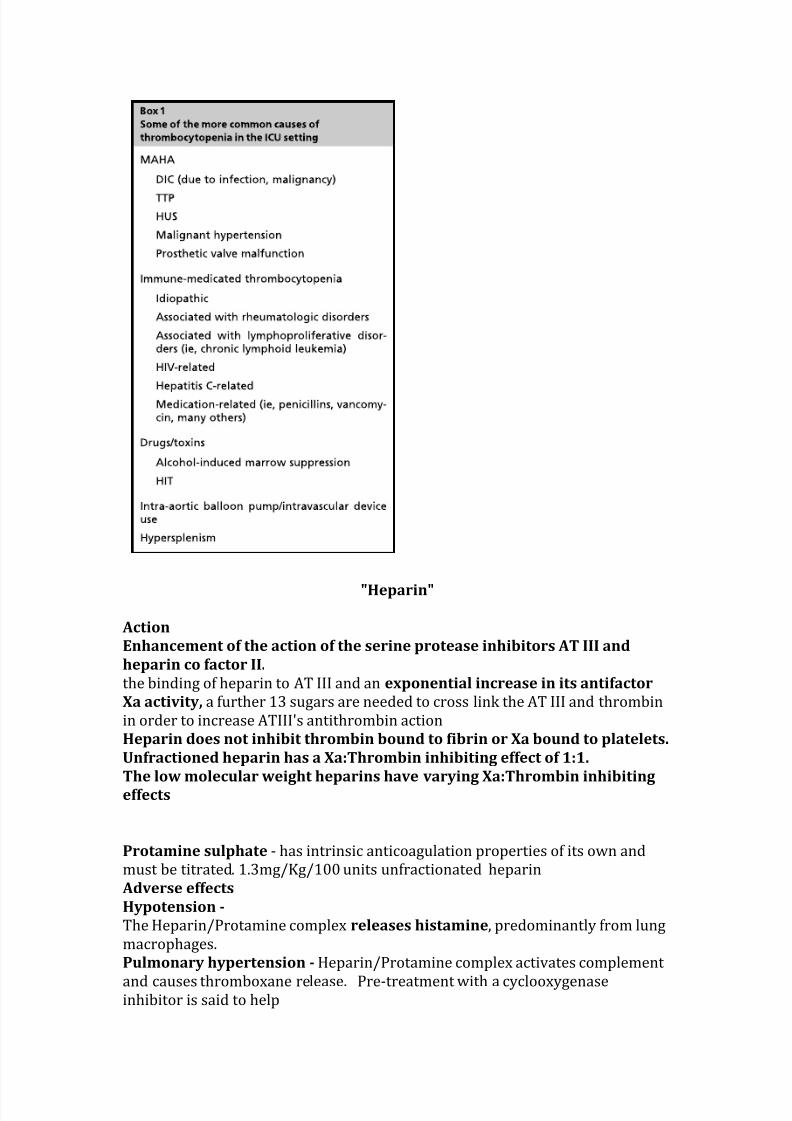
Heparin
Action
Enhancement of the action of the serine protease inhibitors AT III and
heparin co factor II
the binding of heparin to AT III and an exponential increase in its antifactor
Xa activity a further 13 sugars are needed to cross link the AT III and thrombin
in order to increase ATIIIs antithrombin action
Heparin does not inhibit thrombin bound to fibrin or Xa bound to platelets
Unfractioned heparin has a XaThrombin inhibiting effect of 11
The low molecular weight heparins have varying XaThrombin inhibiting
effects
Protamine sulphate - has intrinsic anticoagulation properties of its own and
must be titrated 13mgKg100 units unfractionated heparin
Adverse effects
Hypotension -
The HeparinProtamine complex releases histamine predominantly from lung
macrophages
Pulmonary hypertension - HeparinProtamine complex activates complement
and causes thromboxane release Pre-treatment with a cyclooxygenaseinhibitor is said to help
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 514
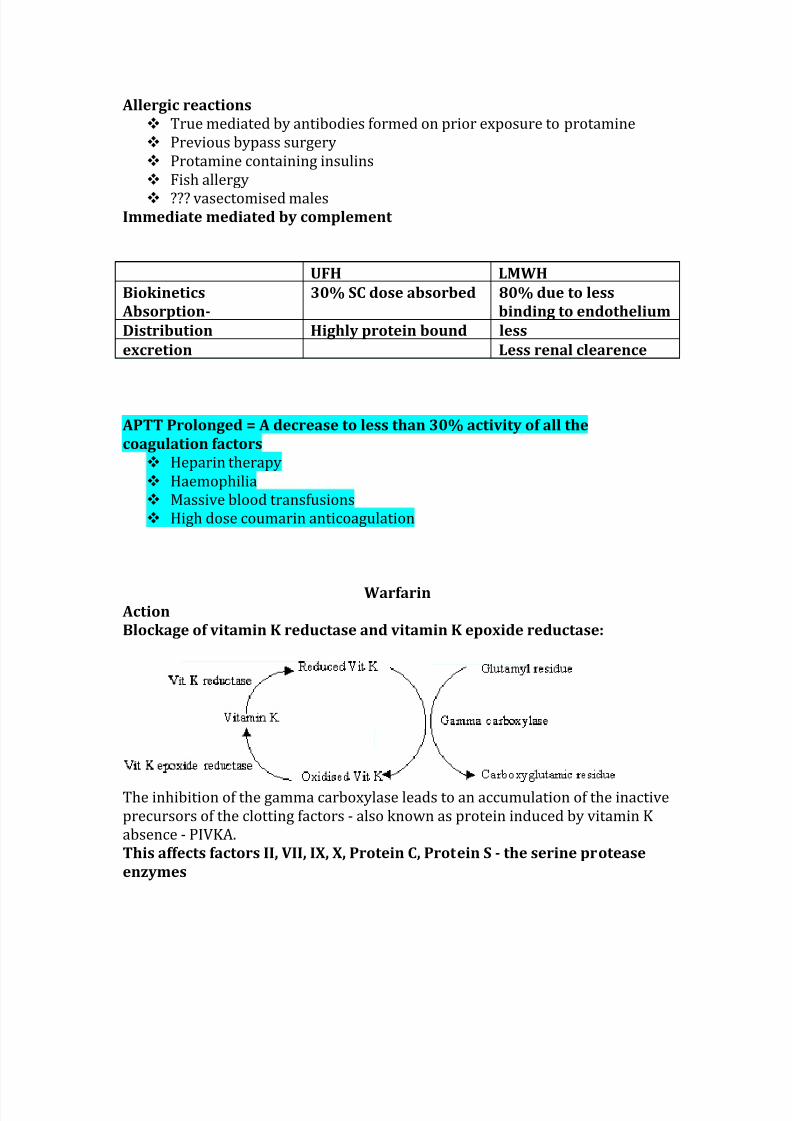
Allergic reactions
True mediated by antibodies formed on prior exposure to protamine
Previous bypass surgery
Protamine containing insulins
Fish allergy
vasectomised malesImmediate mediated by complement
UFH LMWH
Biokinetics
Absorption-
30 SC dose absorbed 80 due to less
binding to endothelium
Distribution Highly protein bound less
excretion Less renal clearence
APTT Prolonged = A decrease to less than 30 activity of all the
coagulation factors
Heparin therapy
Haemophilia
Massive blood transfusions
High dose coumarin anticoagulation
Warfarin Action
Blockage of vitamin K reductase and vitamin K epoxide reductase
The inhibition of the gamma carboxylase leads to an accumulation of the inactive
precursors of the clotting factors - also known as protein induced by vitamin K
absence - PIVKA
This affects factors II VII IX X Protein C Protein S - the serine protease
enzymes
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 614
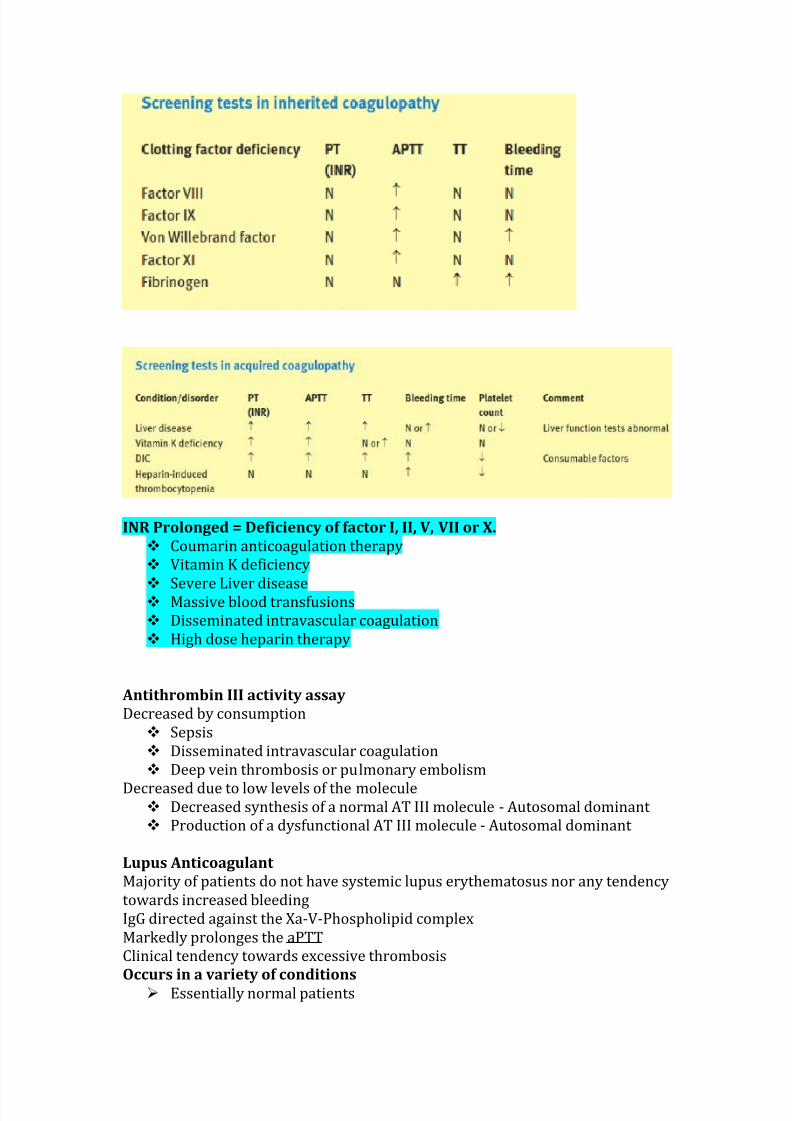
INR Prolonged = Deficiency of factor I II V VII or X
Coumarin anticoagulation therapy
Vitamin K deficiency
Severe Liver disease
Massive blood transfusions
Disseminated intravascular coagulation
High dose heparin therapy
Antithrombin III activity assay
Decreased by consumption
Sepsis
Disseminated intravascular coagulation
Deep vein thrombosis or pulmonary embolism
Decreased due to low levels of the molecule Decreased synthesis of a normal AT III molecule - Autosomal dominant
Production of a dysfunctional AT III molecule - Autosomal dominant
Lupus Anticoagulant
Majority of patients do not have systemic lupus erythematosus nor any tendency
towards increased bleeding
IgG directed against the Xa-V-Phospholipid complex
Markedly prolonges the aPTT
Clinical tendency towards excessive thrombosis
Occurs in a variety of conditions
Essentially normal patients
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 414
Heparin
Action
Enhancement of the action of the serine protease inhibitors AT III and
heparin co factor II
the binding of heparin to AT III and an exponential increase in its antifactor
Xa activity a further 13 sugars are needed to cross link the AT III and thrombin
in order to increase ATIIIs antithrombin action
Heparin does not inhibit thrombin bound to fibrin or Xa bound to platelets
Unfractioned heparin has a XaThrombin inhibiting effect of 11
The low molecular weight heparins have varying XaThrombin inhibiting
effects
Protamine sulphate - has intrinsic anticoagulation properties of its own and
must be titrated 13mgKg100 units unfractionated heparin
Adverse effects
Hypotension -
The HeparinProtamine complex releases histamine predominantly from lung
macrophages
Pulmonary hypertension - HeparinProtamine complex activates complement
and causes thromboxane release Pre-treatment with a cyclooxygenaseinhibitor is said to help
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 514
Allergic reactions
True mediated by antibodies formed on prior exposure to protamine
Previous bypass surgery
Protamine containing insulins
Fish allergy
vasectomised malesImmediate mediated by complement
UFH LMWH
Biokinetics
Absorption-
30 SC dose absorbed 80 due to less
binding to endothelium
Distribution Highly protein bound less
excretion Less renal clearence
APTT Prolonged = A decrease to less than 30 activity of all the
coagulation factors
Heparin therapy
Haemophilia
Massive blood transfusions
High dose coumarin anticoagulation
Warfarin Action
Blockage of vitamin K reductase and vitamin K epoxide reductase
The inhibition of the gamma carboxylase leads to an accumulation of the inactive
precursors of the clotting factors - also known as protein induced by vitamin K
absence - PIVKA
This affects factors II VII IX X Protein C Protein S - the serine protease
enzymes
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 614
INR Prolonged = Deficiency of factor I II V VII or X
Coumarin anticoagulation therapy
Vitamin K deficiency
Severe Liver disease
Massive blood transfusions
Disseminated intravascular coagulation
High dose heparin therapy
Antithrombin III activity assay
Decreased by consumption
Sepsis
Disseminated intravascular coagulation
Deep vein thrombosis or pulmonary embolism
Decreased due to low levels of the molecule Decreased synthesis of a normal AT III molecule - Autosomal dominant
Production of a dysfunctional AT III molecule - Autosomal dominant
Lupus Anticoagulant
Majority of patients do not have systemic lupus erythematosus nor any tendency
towards increased bleeding
IgG directed against the Xa-V-Phospholipid complex
Markedly prolonges the aPTT
Clinical tendency towards excessive thrombosis
Occurs in a variety of conditions
Essentially normal patients
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 414
Heparin
Action
Enhancement of the action of the serine protease inhibitors AT III and
heparin co factor II
the binding of heparin to AT III and an exponential increase in its antifactor
Xa activity a further 13 sugars are needed to cross link the AT III and thrombin
in order to increase ATIIIs antithrombin action
Heparin does not inhibit thrombin bound to fibrin or Xa bound to platelets
Unfractioned heparin has a XaThrombin inhibiting effect of 11
The low molecular weight heparins have varying XaThrombin inhibiting
effects
Protamine sulphate - has intrinsic anticoagulation properties of its own and
must be titrated 13mgKg100 units unfractionated heparin
Adverse effects
Hypotension -
The HeparinProtamine complex releases histamine predominantly from lung
macrophages
Pulmonary hypertension - HeparinProtamine complex activates complement
and causes thromboxane release Pre-treatment with a cyclooxygenaseinhibitor is said to help
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 514
Allergic reactions
True mediated by antibodies formed on prior exposure to protamine
Previous bypass surgery
Protamine containing insulins
Fish allergy
vasectomised malesImmediate mediated by complement
UFH LMWH
Biokinetics
Absorption-
30 SC dose absorbed 80 due to less
binding to endothelium
Distribution Highly protein bound less
excretion Less renal clearence
APTT Prolonged = A decrease to less than 30 activity of all the
coagulation factors
Heparin therapy
Haemophilia
Massive blood transfusions
High dose coumarin anticoagulation
Warfarin Action
Blockage of vitamin K reductase and vitamin K epoxide reductase
The inhibition of the gamma carboxylase leads to an accumulation of the inactive
precursors of the clotting factors - also known as protein induced by vitamin K
absence - PIVKA
This affects factors II VII IX X Protein C Protein S - the serine protease
enzymes
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 614
INR Prolonged = Deficiency of factor I II V VII or X
Coumarin anticoagulation therapy
Vitamin K deficiency
Severe Liver disease
Massive blood transfusions
Disseminated intravascular coagulation
High dose heparin therapy
Antithrombin III activity assay
Decreased by consumption
Sepsis
Disseminated intravascular coagulation
Deep vein thrombosis or pulmonary embolism
Decreased due to low levels of the molecule Decreased synthesis of a normal AT III molecule - Autosomal dominant
Production of a dysfunctional AT III molecule - Autosomal dominant
Lupus Anticoagulant
Majority of patients do not have systemic lupus erythematosus nor any tendency
towards increased bleeding
IgG directed against the Xa-V-Phospholipid complex
Markedly prolonges the aPTT
Clinical tendency towards excessive thrombosis
Occurs in a variety of conditions
Essentially normal patients
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 414
Heparin
Action
Enhancement of the action of the serine protease inhibitors AT III and
heparin co factor II
the binding of heparin to AT III and an exponential increase in its antifactor
Xa activity a further 13 sugars are needed to cross link the AT III and thrombin
in order to increase ATIIIs antithrombin action
Heparin does not inhibit thrombin bound to fibrin or Xa bound to platelets
Unfractioned heparin has a XaThrombin inhibiting effect of 11
The low molecular weight heparins have varying XaThrombin inhibiting
effects
Protamine sulphate - has intrinsic anticoagulation properties of its own and
must be titrated 13mgKg100 units unfractionated heparin
Adverse effects
Hypotension -
The HeparinProtamine complex releases histamine predominantly from lung
macrophages
Pulmonary hypertension - HeparinProtamine complex activates complement
and causes thromboxane release Pre-treatment with a cyclooxygenaseinhibitor is said to help
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 514
Allergic reactions
True mediated by antibodies formed on prior exposure to protamine
Previous bypass surgery
Protamine containing insulins
Fish allergy
vasectomised malesImmediate mediated by complement
UFH LMWH
Biokinetics
Absorption-
30 SC dose absorbed 80 due to less
binding to endothelium
Distribution Highly protein bound less
excretion Less renal clearence
APTT Prolonged = A decrease to less than 30 activity of all the
coagulation factors
Heparin therapy
Haemophilia
Massive blood transfusions
High dose coumarin anticoagulation
Warfarin Action
Blockage of vitamin K reductase and vitamin K epoxide reductase
The inhibition of the gamma carboxylase leads to an accumulation of the inactive
precursors of the clotting factors - also known as protein induced by vitamin K
absence - PIVKA
This affects factors II VII IX X Protein C Protein S - the serine protease
enzymes
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 614
INR Prolonged = Deficiency of factor I II V VII or X
Coumarin anticoagulation therapy
Vitamin K deficiency
Severe Liver disease
Massive blood transfusions
Disseminated intravascular coagulation
High dose heparin therapy
Antithrombin III activity assay
Decreased by consumption
Sepsis
Disseminated intravascular coagulation
Deep vein thrombosis or pulmonary embolism
Decreased due to low levels of the molecule Decreased synthesis of a normal AT III molecule - Autosomal dominant
Production of a dysfunctional AT III molecule - Autosomal dominant
Lupus Anticoagulant
Majority of patients do not have systemic lupus erythematosus nor any tendency
towards increased bleeding
IgG directed against the Xa-V-Phospholipid complex
Markedly prolonges the aPTT
Clinical tendency towards excessive thrombosis
Occurs in a variety of conditions
Essentially normal patients
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 514
Allergic reactions
True mediated by antibodies formed on prior exposure to protamine
Previous bypass surgery
Protamine containing insulins
Fish allergy
vasectomised malesImmediate mediated by complement
UFH LMWH
Biokinetics
Absorption-
30 SC dose absorbed 80 due to less
binding to endothelium
Distribution Highly protein bound less
excretion Less renal clearence
APTT Prolonged = A decrease to less than 30 activity of all the
coagulation factors
Heparin therapy
Haemophilia
Massive blood transfusions
High dose coumarin anticoagulation
Warfarin Action
Blockage of vitamin K reductase and vitamin K epoxide reductase
The inhibition of the gamma carboxylase leads to an accumulation of the inactive
precursors of the clotting factors - also known as protein induced by vitamin K
absence - PIVKA
This affects factors II VII IX X Protein C Protein S - the serine protease
enzymes
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 614
INR Prolonged = Deficiency of factor I II V VII or X
Coumarin anticoagulation therapy
Vitamin K deficiency
Severe Liver disease
Massive blood transfusions
Disseminated intravascular coagulation
High dose heparin therapy
Antithrombin III activity assay
Decreased by consumption
Sepsis
Disseminated intravascular coagulation
Deep vein thrombosis or pulmonary embolism
Decreased due to low levels of the molecule Decreased synthesis of a normal AT III molecule - Autosomal dominant
Production of a dysfunctional AT III molecule - Autosomal dominant
Lupus Anticoagulant
Majority of patients do not have systemic lupus erythematosus nor any tendency
towards increased bleeding
IgG directed against the Xa-V-Phospholipid complex
Markedly prolonges the aPTT
Clinical tendency towards excessive thrombosis
Occurs in a variety of conditions
Essentially normal patients
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 614
INR Prolonged = Deficiency of factor I II V VII or X
Coumarin anticoagulation therapy
Vitamin K deficiency
Severe Liver disease
Massive blood transfusions
Disseminated intravascular coagulation
High dose heparin therapy
Antithrombin III activity assay
Decreased by consumption
Sepsis
Disseminated intravascular coagulation
Deep vein thrombosis or pulmonary embolism
Decreased due to low levels of the molecule Decreased synthesis of a normal AT III molecule - Autosomal dominant
Production of a dysfunctional AT III molecule - Autosomal dominant
Lupus Anticoagulant
Majority of patients do not have systemic lupus erythematosus nor any tendency
towards increased bleeding
IgG directed against the Xa-V-Phospholipid complex
Markedly prolonges the aPTT
Clinical tendency towards excessive thrombosis
Occurs in a variety of conditions
Essentially normal patients
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414

7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 714
Lupus 5-10 of patients
Infectious diseases
Rheumatoid arthritis
Lymphoma
Prostatic cancer
Acquired immunde deficiency syndrome Drug exposure - chlorpromazine procainamide and antibiotics
Laboratory tests to isolate the lupus anticoagulant
Cardiolipin adsorption
Reptilase Test
Dilute aPTT
Kaolin clotting time
Platelet neutralisation procedure
Thrombin is added to plasma and the time taken to form a clot is recorded
Normal is less than 15 seconds
Prolonged due to inhibition of thrombin
Heparin
Fibrin degradation products
Lupus anticoagulant
Prolonged due to abnormal fibrinogen
ACT Prolonged times may be due to
Heparin effect
Hypothermia
Platelet dysfunction
Haemodilution
Cardioplegic solutions
Hypofibrinogenaemia
Factor deficiencies
High Risk of Pre-operative Thrombosis
Venous thrombosis
An acute episode of Deep vein thrombosis within the last three
months
Multiple previous acute episodes of deep vein thrombosis
Hereditary thrombophilic state
Active carcinoma
Atrialarterial thrombosis
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414

7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 814
Clinical criteria
Previous cerebrovascular accident
Female over the age of 75 years
Hypertensive patients
Left ventricular dysfunction
Congestive Cardiac Failure Trans-oesophageal criteria
Complex aortic plaque
Existing left atrial thrombus
Dense spontaneous echocardiographic contrast
Mechanical Heart Valve
Previous valvular thrombosis
Caged-ball (Star-Edwards) and tilt (Bjork-Shiley) type valves in the mitral
position
Bleeding Time
1211Data Interpretation ndash Venkatesh
A-Z
- standard incision made on forearm using a pricking device or a template- BP cuff inflated to 40mmHg- incision dabbed with filter paper every 30 seconds until bleeding time stops- normal value = 2-9 minutes- infrequently used co susceptible to much variation- if prolonged -gt platelet function problem
-gt wWD-gt aspirin-gt heparin-gt post cardiopulmonary bypass-gt uraemia-gt post-haemodialysis-gt beta-lactam antibiotic use-gt NSAIDS
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414

7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 914
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1014
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1114
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414

7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1214
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1314
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414
7302019 Bleeding Physio
httpslidepdfcomreaderfullbleeding-physio 1414