biology, epidemiology and control of penicillium marneffei
TRANSCRIPT

1
Abstract:
Penicillium marneffei is a dimorphic fungus that causes fatal systemic mycosis in
immunocompromised patients. The infection Penicilliosis marneffei occurs most
commonly in HIV patients and is currently endemic in South East Asia. The instance
of P. marneffei infection has risen substantially due to the AIDS endemic and has a
100% mortality rate in untreated patient. P. marneffei is the only thermally dimorphic
fungus within its species, producing hyphal growth at 25°C and unicellular yeast
growth at 37°C.
The ability to grow at 37°C facilitates its infectivity in humans. P. marneffei primarily
affects the pulmonary system, disseminating through the blood to other internal
organs. Primary symptoms include weight loss, fever, anaemia and skin lesions
which can be successfully treated with a course of Amphotericin B followed by
Itraconazole. P. marneffei has been successfully extracted from the internal organs
of bamboo rats, however the current mode of transmission into humans is unknown.
It is commonly believed that infectious conidia are inhaled from an environmental
source possibly from the soil. In order to successfully control rates of infection, the
ecological niche of P. marneffei must be uncovered to understand transmission
methods. More interest is required in discovering the environment and the
epidemiology of P. marneffei to reduce the number of fatalities caused by
Penicilliosis infection.
2
1. Introduction:
1.1. Penicillium marneffei:
Penicilliosis marneffei is described as an opportunistic and progressive infection
induced by the fungus Penicillium marneffei. P. marneffei is currently the only known
thermally dimorphic fungus within the Penicillium genus that causes fatal systemic
mycosis in immunocompromised hosts. Patients suffering from human
immunodeficiency virus (HIV) are the most common immunocompromised patients
affected. The infection is currently endemic in South East Asia including Southern
China, Vietnam, Thailand, Taiwan and Hong Kong with the number of instances
increasing due to the prevalence of AIDS in these areas. In northern Thailand, the
disease is ranked third following tuberculosis and cryptococcosis as the most
common opportunistic infection in patients suffering from HIV (Supparatpinyo et al.,
1994).The transmission method of P. marneffei is unknown, however it is suspected
that the infection is transmitted through inhaled conidia produced by an
environmental form of the fungus (Kaewmalakul et al., 2014).This project will discuss
the biology of P. marneffei infection including the mycology, pathology, diagnosis
and treatment of infection. The epidemiology of the infection including possible
reservoirs and methods to control P. marneffei will also be discussed in detail.
1.2. History:
The first isolation of P. marneffei occurred in 1956 from hepatic lesions extracted
from a bamboo rat’s liver (Rhizomys sinesis) at the Pasteur Institute of Indochina,
Vietnam (Segretain 1959). The fungus was named Penicillium marneffei, recently
changed to Talaromyces marneffei (Samson et al., 2011), in respect to Hubert
Marneffe, Pasteur Institute director in Indochina and Paris. The first reported
incidence of P. marneffei in humans occurred in 1959 when the researcher G.

3
Segretain accidently inoculated the fungus into his finger in the laboratory (Segretain
1959). This caused the formation of a nodule after 9 days and also the development
of lymphadenopathy which was successfully treated with oral nystatin (Deng et al.,
1988). In 1973, the group of researchers including DiSalvo reported the first natural
human infection of P. marneffei from a patient living in North Carolina (DiSalvo
1973). The 61 year old minister reported he had worked in Vietnam and was treated
for Hodgkin’s disease where his spleen contained isolates of P. marneffei (Duong
1996). Another 5 cases where reported in 1984 by Jayanetra, in Bangkok (Jayanetra
et al., 1984). From these patients, 2 who had no underlying conditions were treated
with amphotericin B successfully, however the remaining three patients were
misdiagnosed with tuberculosis and died as a result. In the preceding years eight
cases where reported in China with a further 20 cases in the Guangxi region and six
cases reported in Hong Kong (Vanittanakom et al., 2006). The very first reported
incidence of penicilliosis marneffei in a HIV infected patient occurred in 1988 by Piehl
and colleagues causing severe mycosis. Due to the exponential rise in the
prevalence of HIV in Asia, the instance of P. marneffei has risen markedly as these
patients have a high susceptibility to infection (Piehl et al., 1988). Due to the high
frequency of P. marneffei among immunocompromised patients, the infection is now
recognised as an AIDS-indicating disease in many areas including Hong Kong and
Thailand (Cánovas & Andrianopoulos 2007).
1.3. Patients Affected:
HIV positive patients are those mainly infected with penicilliosis due to a weakened
immune system. Infection has been reported in patients who were not HIV positive or
immunocompromised however this instance is rare. A review of the instances in
mainland China from 1984 to 2009 demonstrated that 87.72% of the cases treated

4
were HIV positive (Liu et al., 2013). Prior to the HIV endemic the instance of P.
marneffei infection was relatively rare with only a few cases being described (Lee et
al., 2014). In the Chiang Mai hospital in Thailand, there were 1,115 cases of P.
marneffei infection between 1990 and 1997 alone (Sirisanthana et al.,1998). P.
marneffei infection has been recorded in HIV negative patients that have other
underlying conditions such as tuberculosis, Hodgkin’s disease, systemic lupus
erythematosus, patients recovering from immunosuppressive therapy and even
alcoholism (Wong et al., 2001).
2. Biology:
2.1.Mycology:
Figure 1. (Vanittanakom et al., 2006): Morphologies of P. marneffei species seen
under the microscope. In (A) the hyphal form can be seen with phialides and conidia.
In (B) the cells begin hyphal formation showing branched filaments. In (C) hyphae
have completed arthroconidiogenesis at 37°C. In (D) the yeast cells can be viewed
after incubation at 37°C.

5
The Penicillium group of species is comprised of over 200 fungal species. P.
marneffei is regarded as one of the few species with medical importance within its
genus (Andrianopoulos 2002). The infection is also currently the only fungus within
the Penicillium genus that has been described as a temperature-dependent
thermally dimorphic fungus. At 25°C colonies can be cultured which are filamentous
in form and at 37°C the pathogenic form is expressed as oval shaped unicellular
yeast cells. The lifecycle of the infection is separated into three distinct phases: at
25°C there is filamentous hyphal growth, also at 25°C asexual development
(conidiation) can be seen and at 37°C unicellular yeast growth can be seen
(Kavanagh 2007).
Under suitable nutritional conditions at 25°C, the germination of a conidium occurs
within the first 6 hours through isotrophic growth, forming downy grey colonies and
by 12 hours a germ tube is produced through polarised growth. The germ tube
continues to grow through polarised growth at the apical tip for the formation of a
hypha and through septation cellular compartments are established behind the
apical tip. These sub-apical cells can produce branched cells with a new growth
point through repolarisation. The uncoupling of nuclear and cellular division occurs
where compartments of the actively growing cells contain multiple nuclei
(Andrianopoulos 2002).
In P. marneffei, yeast morphogenesis can occur at 37°C where yeast cells that can
divide by fission, are produced. The ability to grow at 37°C facilitates its infectivity in
humans (Kaewmalakul et al., 2014). Morphogenesis begins 48 hours after
germination giving rise to branched uninucleate hyphae through the coupling of both

6
nuclear and cell division. Hyphal segment that consist of single nuclei are produced
and these pre-arthroconidial cells are easily separated by double septa. The
degradation of material that lies between the double septa occurs after time, the
process of arthroconidiation. These cells can assist the maintenance of the
elongated cell shape, initiate polarised growth and following nuclear division they
divide by fission to produce true yeast cells. The resulting yeast cells are also
capable of dividing by fission at 37°C however, yeast cells grown in vivo have a
different morphology than those in vivo (Cánovas & Andrianopoulos 2007). When
hyphae that have been produced at 25°C enter a temperature of 37°C they can
initiate a comparable morphogenic process that begins with coupling of nuclear and
cell division in the apical cells. This dimorphic transition can be reversed by
decreasing the temperature back to 25°C allowing the uncoupling of nuclear and
cellular division and the yeast cells are polarised forming hyphal cells.

7
Figure 2. (Andrianopoulos 2002): Representation of the P. marneffei lifecycle
including asexual development and dimorphic switching. At 25°C the fungus grows
as a mycelial through hyphal growth and asexual development can produce conidia.
At 37°C the fungus grows as pathogenic yeast cells that divide by fission.
P. marneffei can also initiate asexual development which leads to multicellular
conidiophores containing uninucleate conidia. This process occurs after hyphal
growth at 25 °C and requires specific environmental conditions including light and an
8
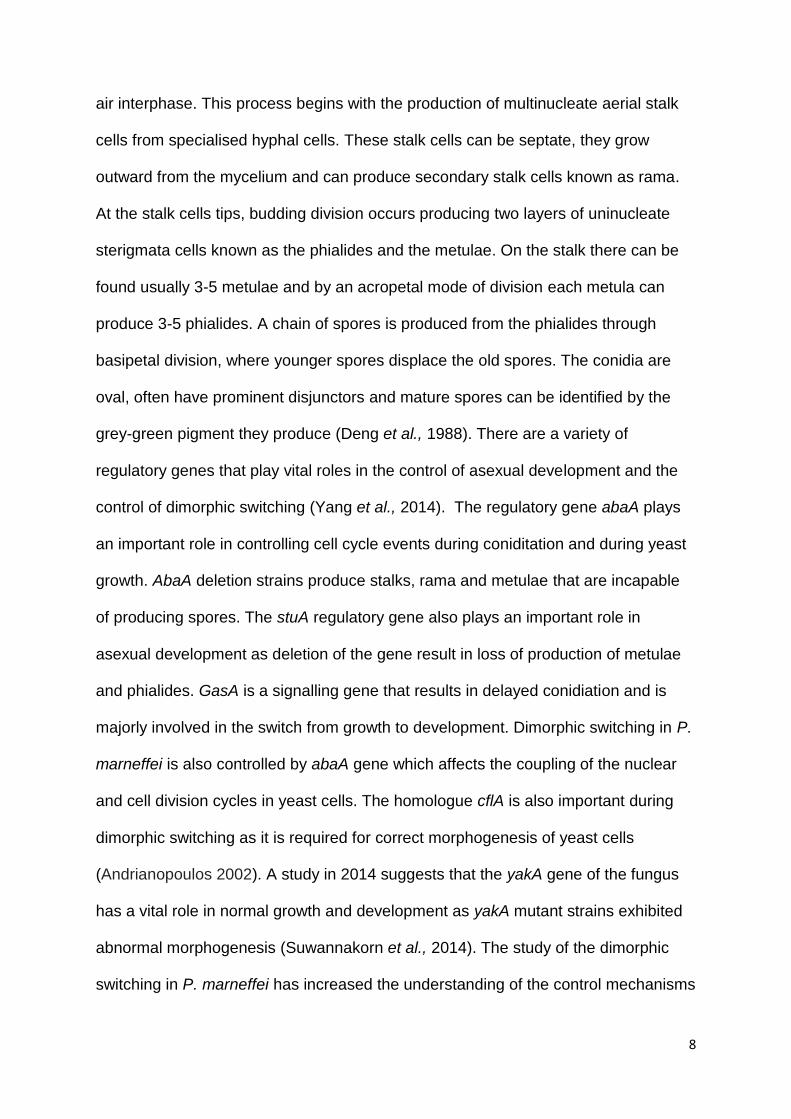
air interphase. This process begins with the production of multinucleate aerial stalk
cells from specialised hyphal cells. These stalk cells can be septate, they grow
outward from the mycelium and can produce secondary stalk cells known as rama.
At the stalk cells tips, budding division occurs producing two layers of uninucleate
sterigmata cells known as the phialides and the metulae. On the stalk there can be
found usually 3-5 metulae and by an acropetal mode of division each metula can
produce 3-5 phialides. A chain of spores is produced from the phialides through
basipetal division, where younger spores displace the old spores. The conidia are
oval, often have prominent disjunctors and mature spores can be identified by the
grey-green pigment they produce (Deng et al., 1988). There are a variety of
regulatory genes that play vital roles in the control of asexual development and the
control of dimorphic switching (Yang et al., 2014). The regulatory gene abaA plays
an important role in controlling cell cycle events during coniditation and during yeast
growth. AbaA deletion strains produce stalks, rama and metulae that are incapable
of producing spores. The stuA regulatory gene also plays an important role in
asexual development as deletion of the gene result in loss of production of metulae
and phialides. GasA is a signalling gene that results in delayed conidiation and is
majorly involved in the switch from growth to development. Dimorphic switching in P.
marneffei is also controlled by abaA gene which affects the coupling of the nuclear
and cell division cycles in yeast cells. The homologue cflA is also important during
dimorphic switching as it is required for correct morphogenesis of yeast cells
(Andrianopoulos 2002). A study in 2014 suggests that the yakA gene of the fungus
has a vital role in normal growth and development as yakA mutant strains exhibited
abnormal morphogenesis (Suwannakorn et al., 2014). The study of the dimorphic
switching in P. marneffei has increased the understanding of the control mechanisms
9
in other fungal pathogens. Understanding the biology of P. marneffei can provide
targets for drugs used during treatment of infection.
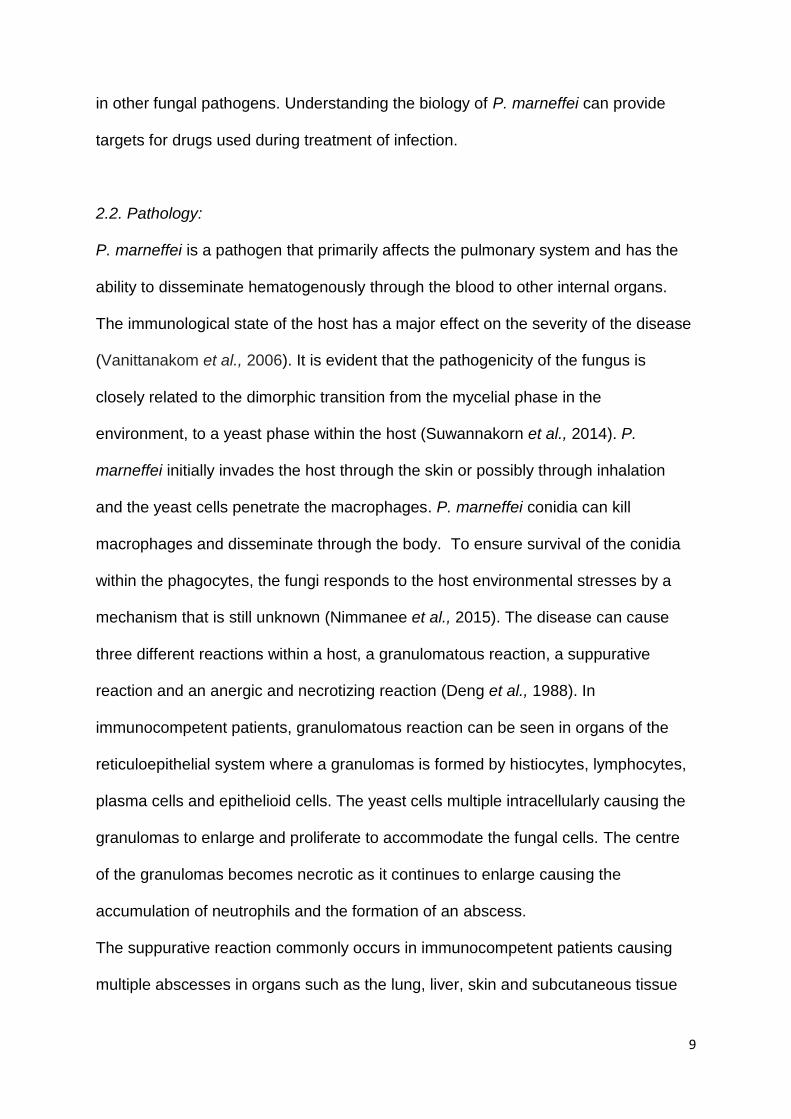
2.2. Pathology:
P. marneffei is a pathogen that primarily affects the pulmonary system and has the
ability to disseminate hematogenously through the blood to other internal organs.
The immunological state of the host has a major effect on the severity of the disease
(Vanittanakom et al., 2006). It is evident that the pathogenicity of the fungus is
closely related to the dimorphic transition from the mycelial phase in the
environment, to a yeast phase within the host (Suwannakorn et al., 2014). P.
marneffei initially invades the host through the skin or possibly through inhalation
and the yeast cells penetrate the macrophages. P. marneffei conidia can kill
macrophages and disseminate through the body. To ensure survival of the conidia
within the phagocytes, the fungi responds to the host environmental stresses by a
mechanism that is still unknown (Nimmanee et al., 2015). The disease can cause
three different reactions within a host, a granulomatous reaction, a suppurative
reaction and an anergic and necrotizing reaction (Deng et al., 1988). In
immunocompetent patients, granulomatous reaction can be seen in organs of the
reticuloepithelial system where a granulomas is formed by histiocytes, lymphocytes,
plasma cells and epithelioid cells. The yeast cells multiple intracellularly causing the
granulomas to enlarge and proliferate to accommodate the fungal cells. The centre
of the granulomas becomes necrotic as it continues to enlarge causing the
accumulation of neutrophils and the formation of an abscess.
The suppurative reaction commonly occurs in immunocompetent patients causing
multiple abscesses in organs such as the lung, liver, skin and subcutaneous tissue

10
by neutrophils and fibrin. Immunocompromised patients are mainly affected by the
anergic and necrotizing reaction in organs such as the lung, skin and liver. Infected
patients show macrophages engorged with proliferation yeast cells which can be
used as a marker for the presence of a progressive and disseminated infection within
the host. Cultures containing P. marneffei have been isolated from a variety of
organs however the blood, skin, bone marrow, liver, lymph nodes and lungs are the
most common organs targeted (Duong 1996).
2.3. Clinical manifestations:
Figure 3. (Qiu et al., 2014): Chest High resolution tomography showing lung lesions
and protrusions on the wall of the patient’s trachea.
Penicilliosis marneffei infection most commonly causes anaemia, weight loss, fever
and skin lesions in HIV patients. The infection can be characterised by the presence
of skin lesions which can be seen in approximately 85 % of patients mainly occurring
on the face and neck (Vanittanakom et al., 2006). Disseminated infection starts with
fever, chills, coughs and pleurisy (inflammation of the membrane of the lungs).
Hepatomegaly, lymphadenopathy, leukocytosis and arthritis has been reported in

11
cases. Over 70% of patients are anaemic and have been recorded with haemoglobin
levels of 10 g/dl or lower. Hepatosplenomegaly is common particularly in children
who are HIV positive and there have been records of bone marrow infection and
genital ulcers (Duong 1996). It is uncommon for the central nervous system to be
affected however there has been reported in Vietnam the development of confusion,
agitation and depressed consciousness in rare cases (Kantipong et al., 1998). A
study in 2013 reported that 10% of penicilliosis patients they examined had P.
marneffei infection in the bone marrow, suggesting bone marrow inspection should
also be considered during treatment (Nong & Liang 2013). The manifestation in HIV
negative patients are relatively similar including the onset of lymoadenopathy,
arthritis, pulmonary infection and osteomyelitis (Wong et al., 2001). These symptoms
are characteristic to other systemic infectious diseases such as tuberculosis,
cryptococcosis and histoplasmosis in patients infected with HIV and may occur along
with penicilliosis (Hilmarsdottir et al, 1993). This makes the diagnosis of P. marneffei
in patients more difficult with misdiagnosis leading to many deaths in the past.
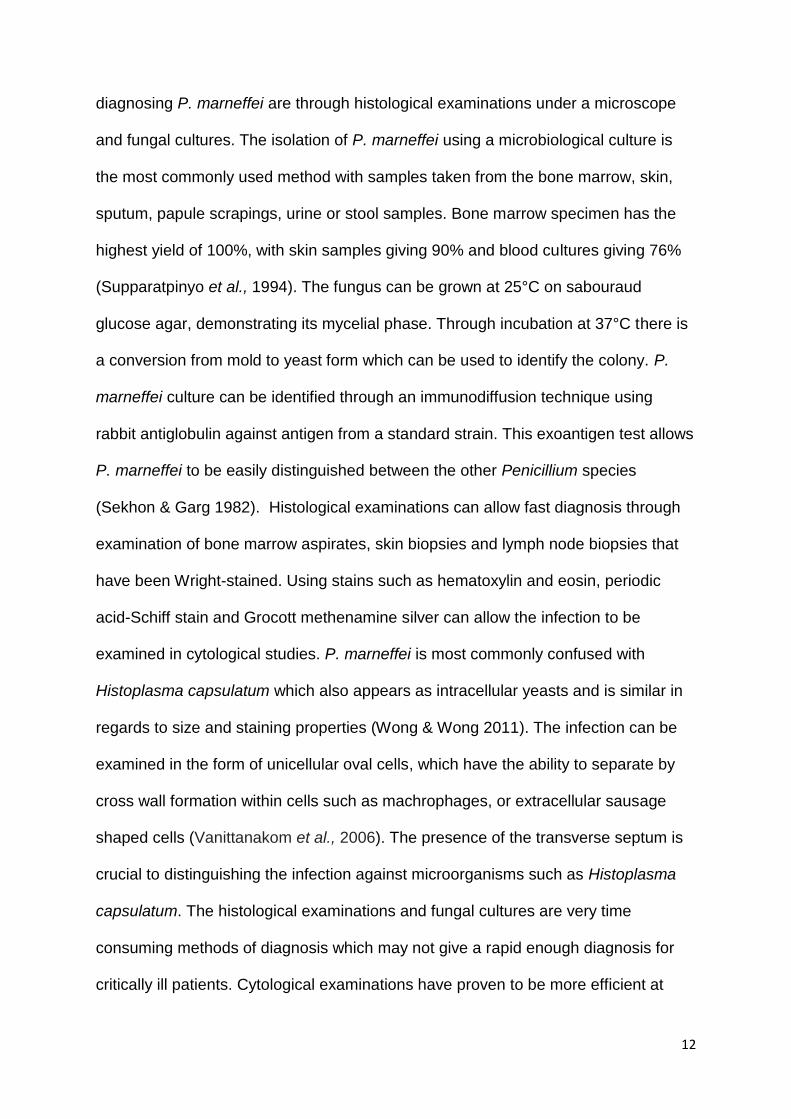
2.4. Diagnosis:
Rapid diagnosis is crucial to begin treatment early and increases the chances of
patient survival (Cao et al., 2009). The diagnosis can be delayed by the slow growth
rate of Penicillium marneffei and its similarities to TB and also non-tuberculous
mycobacterium. The traditional diagnosis method by fungal isolation also requires a
prolonged incubation period. The mould to yeast transition of the infection can be
used as a useful diagnostic tool with the yeast form containing a transverse septum,
which is the marker of binary fission (Jan et al., 2008). The conventional methods of
12
diagnosing P. marneffei are through histological examinations under a microscope
and fungal cultures. The isolation of P. marneffei using a microbiological culture is
the most commonly used method with samples taken from the bone marrow, skin,
sputum, papule scrapings, urine or stool samples. Bone marrow specimen has the
highest yield of 100%, with skin samples giving 90% and blood cultures giving 76%
(Supparatpinyo et al., 1994). The fungus can be grown at 25°C on sabouraud
glucose agar, demonstrating its mycelial phase. Through incubation at 37°C there is
a conversion from mold to yeast form which can be used to identify the colony. P.
marneffei culture can be identified through an immunodiffusion technique using
rabbit antiglobulin against antigen from a standard strain. This exoantigen test allows
P. marneffei to be easily distinguished between the other Penicillium species
(Sekhon & Garg 1982). Histological examinations can allow fast diagnosis through
examination of bone marrow aspirates, skin biopsies and lymph node biopsies that
have been Wright-stained. Using stains such as hematoxylin and eosin, periodic
acid-Schiff stain and Grocott methenamine silver can allow the infection to be
examined in cytological studies. P. marneffei is most commonly confused with
Histoplasma capsulatum which also appears as intracellular yeasts and is similar in
regards to size and staining properties (Wong & Wong 2011). The infection can be
examined in the form of unicellular oval cells, which have the ability to separate by
cross wall formation within cells such as machrophages, or extracellular sausage
shaped cells (Vanittanakom et al., 2006). The presence of the transverse septum is
crucial to distinguishing the infection against microorganisms such as Histoplasma
capsulatum. The histological examinations and fungal cultures are very time
consuming methods of diagnosis which may not give a rapid enough diagnosis for
critically ill patients. Cytological examinations have proven to be more efficient at

13
producing a rapid response and the specimens can be obtained by less invasive
methods. Cytological studies can be undertaken using specimens from lung
aspirates, sputum, neck lymph node aspirates or lung biopsy imprint smears (Jan et
al., 2008). Cytological smears that are stained by a Romanowsky method can
present the characteristic transverse septum of P. marneffei after aspiration and can
be confirmed by a microbiological culture (Wong & Wong 2011). Serologic diagnosis
has been developed to detect specific antibodies used with antigens of the fungus in
order to provide a swift diagnosis (Vanittanakom et al., 2006) however they are not
widely available. Patients that are HIV positive and are infected with P. marneffei
have a significantly higher level of antigen and lower level of antibody in comparison
to patients who are HIV negative with P. marneffei (Wong et al., 2001). A method for
detecting IgG antibodies using a fluorescent antibody test has been developed using
antigens such as conidia and the yeast form of P. marneffei (Yuen et al., 1994). A
high IgG titer can indicate the presence of infection, suggesting this method has the
potential for rapid diagnosis. Aspergillus fumigatus galactomannan can be detected
using a monoclonal antibody by the PAstorex Aspergillus test kit. This
galactomannan assay can be used to detect galactomannan in P. marneffei using a
specific latex agglutination which increased the sensitivity for penicilliosis detection.
This is a highly specific test which can be utilised for efficient detection and is
currently screened for in newly diagnosed HIV patients (Wong & Wong 2011).
Molecular diagnosis methods for P. marneffei detection have been developed with a
specific PCR assay based on oligonucleotide probe of the 18S rRNA gene. This
method has proven to be highly specific and sensitive, however is a complicated
method of diagnosis (Vanittanakom et al., 2006) and is currently not accessible
during clinical use. In 2011, Zhang et al developed a sensitive method of diagnosing
14
P. marneffei by using a multiplex ligation-dependent probe amplification (MLPA)
assay. The group designed three sets of probes used to amplify the internally
transcribed spacer region of P. marneffei rRNA. These probes can simultaneously
detect the gene loci and characterise different fungal strains in the one MLPA
reaction. The MLPA assay is very sensitive and specific and can be completed in
one working day. This method could provide rapid diagnosis and provide information
on the epidemiological studies of the infection (Zhang et al., 2011).
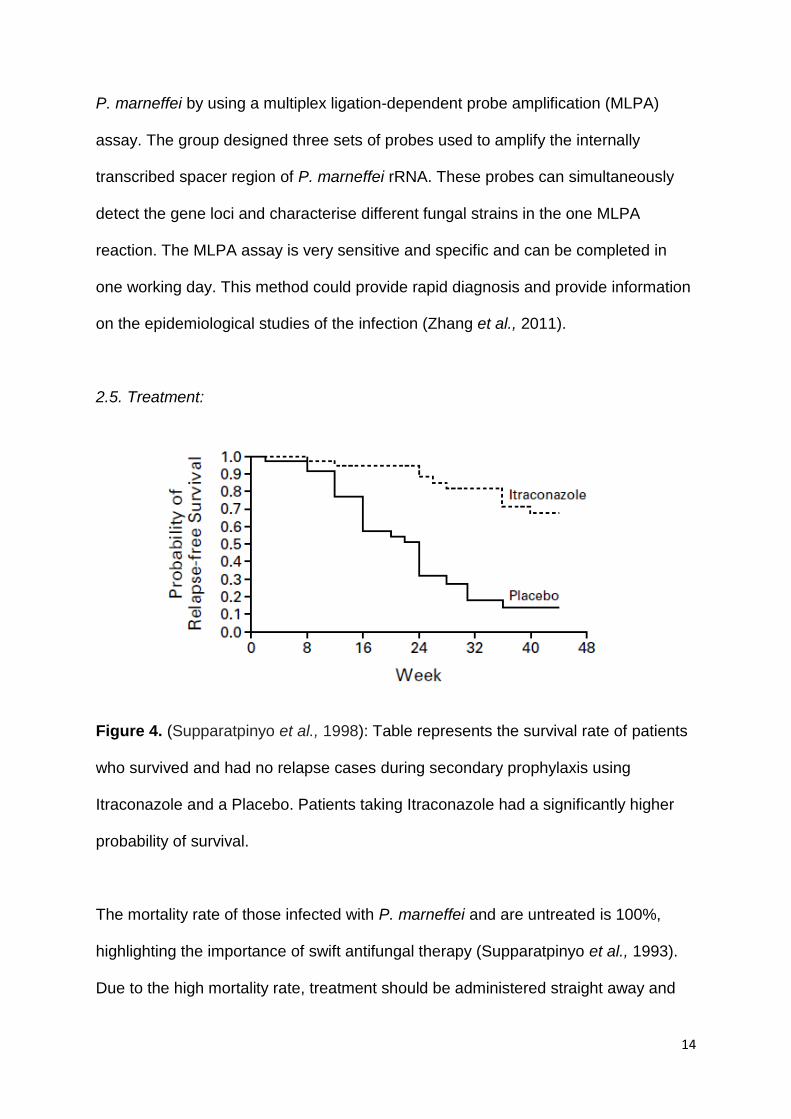
2.5. Treatment:
Figure 4. (Supparatpinyo et al., 1998): Table represents the survival rate of patients
who survived and had no relapse cases during secondary prophylaxis using
Itraconazole and a Placebo. Patients taking Itraconazole had a significantly higher
probability of survival.
The mortality rate of those infected with P. marneffei and are untreated is 100%,
highlighting the importance of swift antifungal therapy (Supparatpinyo et al., 1993).
Due to the high mortality rate, treatment should be administered straight away and
15
not delayed until the results from fungal cultures or samples are obtained. P.
marneffei is known to be highly susceptible to the following group of azoles;
itraconazole, miconazole, voriconazole, ketoconazole and fluconazole, with the latter
being the least effective. Itraconazole has a broad antifungal spectrum, low toxicity
level and has appropriate pharmacokinetic properties. Terbinafine and voriconazole
do have some effect against P. marneffei however there is limited data on their
potential use (Liu et al., 2013). Penicilliosis is also susceptible to amphotericin B
which has proven to be effective and is the standard drug for the most severe cases,
however is associated with high rates of relapse (Sekhon et al., 1992). Amphotericin
B requires a prolonged hospital stay which is inconvenient, is relatively toxic, is
expensive and is known to cause adverse side effects. Some of the side effects
include nausea, headaches, vomiting, and it has been associated with multiple organ
damage such as kidney damage (Supparatpinyo et al., 1998). The recommended
treatment is intravenous amphotericin B at a dosage of 0.6 mg/kg taken daily over
the course of 2 weeks, followed by oral itraconazole at a dose of 200mg taken twice
daily over 10 weeks (Qiu et al., 2014). Secondary prophylaxis with itraconazole has
proven to be efficient at preventing relapse in patients who have received the initial
amphotericin B therapy. The strategy of preventing relapse within patients is more
effective than treating patients who have already relapsed (Supparatpinyo et al.,
1998).

16
3. Epidemiology:
3.1. Endemic Areas:
Figure 5. (google images): Diagram represents the geographic restriction of P.
marneffei infection to South East Asia. The regions affected may contain similar
environmental conditions for the infection to survive and expand.
P. marneffei infection is currently geographically restricted to Southeast Asia
(Gugnani et al., 2007). There have been confirmed cases of infection outside of the
endemic regions in Europe, North America, Africa and Australia in HIV patients
where they reported no recent travel within Asia. These infected individuals suggests
that the infection only requires short term exposure to be contracted by susceptible
hosts and there must be a minimum of one site of infection within the environment in
these regions where tourist can become infected even during a short stay (Chaiwun
et al., 2011). There are two reported cases of penicilliosis marneffei in patients
outside of Asia who reported no history of travel to the endemic area. The first case
was observed in an African from Ghana in 2000 followed by a case in Togo in 2008,
both in HIV positive patients (Patassi et al., 2013). The mode of transmission for both

17
these cases is unknown, however both countries share a border suggesting possible
transmission from the same source. It is suggested that due to the development in
trading between Asian and West Africa, the infection may have travelled by boat.
These cases propose that clinicians should consider P. marneffei in HIV patients that
develop skin lesions, regardless of geographic locations.
The method of transmission of P. marneffei in humans remains a mystery. The
basic ecology of the fungus remains unclear and understanding the ecological niche
of P. marneffei is essential to recovering the mode of transmission. The main issue
of concern is whether penicilliosis marneffei is transmitted by humans through an
animal or environmental source (Vanittanakom et al., 2006).
3.2. Bamboo Rats:
P. marneffei has been successfully extracted from 4 species of rats including
Rhizomys sinensis, Cannomys badius, Rhizomys sumatrensis and Rhizomys
pruinosus, and also from the soil present in the burrows of bamboo rats (Gugnani et
al., 2004). The bamboo rats can be located in the endemic regions, however the
prevalence of infection does vary across Asia (Vanittanakom et al., 2006). There is
little evidence to suggest that humans directly contract penicilliosis marneffei from
these rats, however it is clear that there is a strong association between P. marneffei
and the rodent species (Cao et al., 2011). Infected rats appear healthy, suggesting
that rats are only carriers of the infection (Chaimun et al., 2011). Bamboo rats are
known to live in mountainous regions and have limited contact with humans. Few
humans eat Bamboo rats and P. marneffei cases have been recorded in known
vegetarians (Chariyalertsak et al., 1997). It is widely considered that both humans

18
and rats are commonly infected by an external source in the environment, however it
is also considered that the bamboo rats play a role as an obligate phase in the life
cycle of P. marneffei (Cao et al., 2011). Studies suggest that the rats possibly act as
a vector for human infection by acting as amplifiers of the infectious dispersal stages.
Infection within the rodents may benefit P. marneffei as the body of the host, after
death, can create a nutrient rich environment for aerosol dispersal. Both HIV
patients and bamboo rats are reported to have some genetically similar strains which
could indicate possible co-infection from a common source (Chaiwun et al., 2011).
3.3. Soil as a reservoir:
It is currently still unknown the exact mode of transmission within humans, although
it is assumed that infectious conidia are inhaled within the environment and
disseminates through the lungs (Bulterys et al., 2013). In 1997 a case control study
was conducted by Chariyalertsak, (Chariyalertsak et al., 1997) which indicated that
the bamboo rats were not a risk factor of infection, but rather the patient’s exposure
to possible reservoirs in the environment within the soil. The study included data
from 1988 to 1992 and demonstrated that cases were more likely farmers and
labourers and were also more likely to be younger males. The data was not
statistically significant and it is possible that younger people have an increased
chance of exposure to an environmental source through occupation and recreation
(Chariyalertsak et al., 1997). Investigations of soil samples within Asia have been
conducted in order to determine the natural reservoir of P. marneffei. Deng et al.
(1988) were the first group successful at isolating samples from soil taken from R.
pruinosus species burrows. The second successful isolation attempt was made by

19
Chariyalertsak et al. (1996) from a soil sample taken from the burrow of R.
sumatrensis species (Gugnani et al., 2004). A study conducted in 2008 (Joshi et al.,
2008) presented findings that in sterile soil, P. marneffei can survive for
approximately 4 weeks and only 2-3 days in non-sterile samples. Other attempts to
isolate P. marneffei from soil samples have failed and there is little evidence to prove
that transmission occurs from the soil.
There is significant evidence indicating increased infection among HIV patients
during the rainy season, particularly in Thailand from May to November. A study from
Vietnam reported a 30 % increase in cases of penicilliosis admitted, demonstrating
the seasonal variation of P. marneffei (Le et al., 2011). These patterns of infection
rates can provide a greater understanding of the epidemiology of the fungus
(Chariyalertsak et al., 1996). The study in Thailand suggested the expansions of P.
marneffei reservoirs may be facilitated by precipitation. As cases of P. marneffei
occur in both urban and rural areas, it is difficult to distinguish where the
environmental source is located. A study in Vietnam examined the association
between penicilliosis cases and environmental variables such as humidity,
temperature, wind speed and precipitation (Bulterys et al., 2013). The study
examined data gathered from the Ho Chi Minh City hospital between 2004 and 2010.
The data demonstrated that precipitation and humidity where strongly associated
with the number of penicilliosis. This data suggests that the combination of both
rainfall and humidity may facilitate spore release or fungal growth in the environment.
It is suggested that rainfall should have a greater influence on fungal growth in soil
located deep in the ground, whereas humidity would facilitate fungal growth on areas
that are more exposed to air. More research into the seasonal variation of P.

20
marneffei will lead to greater understanding of the environmental niche and method
of transmission in immunocompromised patients.
The same study from Vietnam also presented findings on the incubation period of P.
marneffei. The strong association between seasonal variations and infection rate
suggests that disseminated disease can occur in a short time after
immunocompromised patients have been exposed to the fungus. Penicilliosis cases
may be due to primary infection, reinfection or reactivation of latent disease
(Chariyalertsak et al., 1997). In cases of penicilliosis within children, primary infection
is the most important problem, with reinfection and reactivation being more important
in adult cases. The study estimates that the incubation period may be between 0 and
3 weeks.
3.4. Possible Reservoirs:
Other possible reservoirs suggested by the case-control study in Thailand are
bamboo plants which are commonly grown and eaten. Bamboo thickets are also the
habitat of R. sumatrensis species of Bamboo rat suggesting that they may possibly
be a common reservoir for infection. Attempts to demonstrate a correlation between
bamboo plants and the infection have not been successful. The possibility of rats
acting as vectors for human transmission suggest that possibly other animals such
as dogs, cats and elephants may play an obligate role in the lifecycle of P. marneffei.
A study in Thailand in 2010 suggested dogs as a reservoir for infection when PCR
samples on nasal swaps obtained from outdoor dogs where positive for P. marneffei
infection. American dogs are known to obtain nasal infections from Penicillium
species and their nasal regions frequently come into contact with nature and soil
21
(Mathews & Sharp 2006). The research showed approximately 13% of the dogs that
samples were taken from were positive with P. marneffei. The dogs may be a
reservoir for infection or may just be carriers, more research is required to confirm
these observations (Chaiwun et al., 2011). The presence of P. marneffei within other
animals that frequently come into contact with tourists such as elephants, is
unknown. Studies of these other animals in Thailand would be valuable to
understanding the epidemiology of the infection.
4. Control:
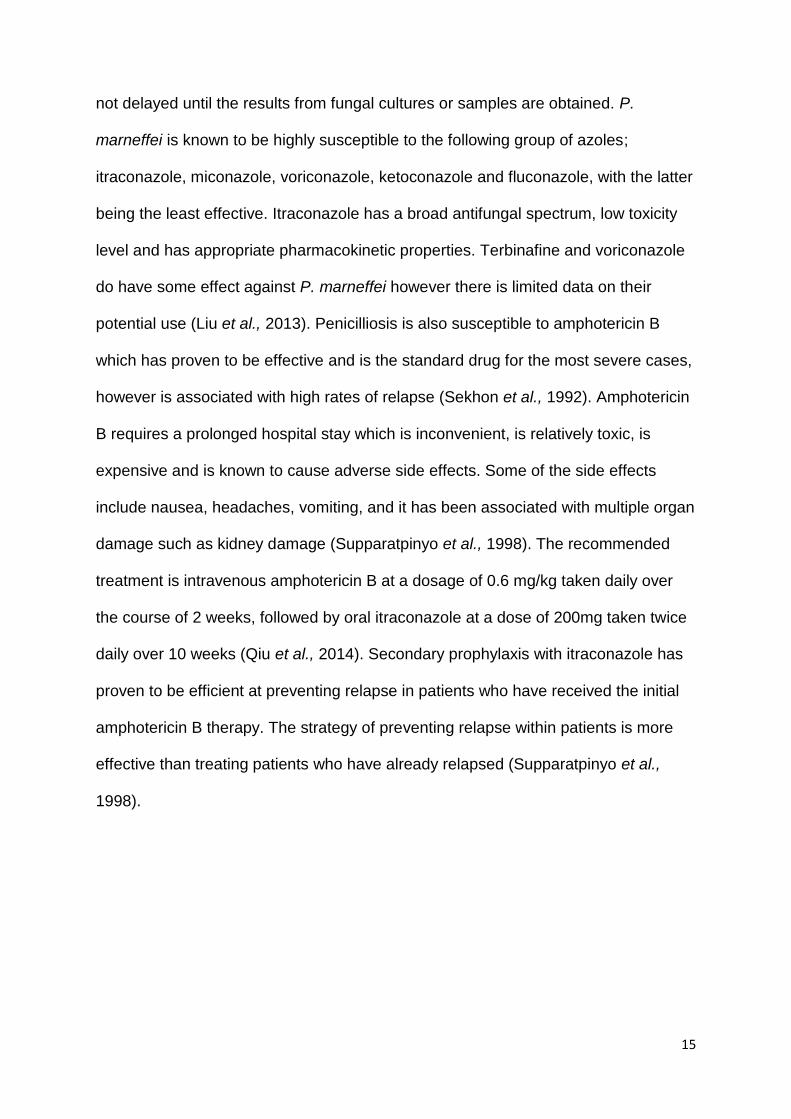
4.1. Methods of Containment:
Figure 6. (Hu et al., 2013): Penicillium marneffei cases have increased exponentially
due to the AIDS epidemic, in the graph a dramatic increase from 2000 to 2009 can
be seen in correlation with the increase in AIDS patients.
It has been noted that in areas where HIV transmission has reduced due to the
introduction of control measures, the cases of P. marneffei have also reduced in
correlation. To effectively control transmission rates of P. marneffei, the prevalence
of HIV must be reduced. There have been numerous projects to help reduced the

22
cases of HIV in the developing world. Needle syringe programmes have effectively
reduced HIV and hepatitis C among drug users. The development of sensitive and
specific HIC screening tests have effectively removed HIV infection from the drug
supply in the developed world and these methods could be employed in the
developing world (Bertozzi et al., 2006). To prevent mother to child transmission, a
course of nevirapine can be administered to mothers throughout labour (Guay et al.,
1999). By discovering the ecological niche of P. marneffei, the mode of transmission
may be uncovered which is essential to controlling the infection. Discovering the
mechanisms of infection will prove vital to reducing the total number of infections and
deaths per year. Quicker diagnosis are essential to reducing mortality rates and this
can be achieved by increasing awareness among physicians. In patients with HIV
and P. marneffei, antifungal therapy should not be postponed until the results from
diagnostic tests are obtained (Supparatpinyo et al., 1992).The instance may be
higher than reported due to misdiagnosis in the past and poor reporting of cases in
national statistics, therefore it is essential to adapt controls measures to ensure the
instance decreases (Hu et al., 2013). Shorter treatment regimens that require
reduced hospital stays could decrease the burden on healthcare systems. The cases
in Togo and Ghana suggests that clinicians should consider P. marneffei infection in
all HIV patients presenting with lesions, regardless of geographic regions as only
early diagnosis and treatment can lead to reduced mortality (Patassi et al., 2013).

23
5. Conclusion:
The instance of P. marneffei infection has increased rapidly in South East Asia due
to the prevalence of HIV. The mortality rate of HIV infected patients who acquire
penicilliosis marneffei is high if diagnosis and treatment are not rapidly administered.
The epidemiology of the infection is still relatively unknown, however studies have
highlighted possible reservoirs that should be investigated. Transmission of the
infection may not be controlled until the natural reservoir of the infection is
discovered. The cases of infection in Togo and Ghana suggest the infection can
survive in environmental conditions found outside of the endemic regions. More
publicity is required to highlight the significance of the disease in order to increase
interest in studying the infection. This project discusses the infection in detail
regarding the biology, epidemiology and control. The complex morphology of P.
marneffei and the poor understanding of the epidemiology highlight the severity of
infection and the necessity for increased research in order to successfully control it.