biochem ass
TRANSCRIPT

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 1/18
SECONDRY METABOLITE
*Ishwar Chandra
[email protected](M.tech Biotechnology, amity institute of biotechnology Amity University)
INTRODUCTION
Secondary metabolites, also known as natural products, are those products (chemical compounds) of
metabolism that are not essential for normal growth, development or reproduction of an organism. In
this sense they are "secondary". The function or importance of these compounds to the organism's
development is usually of ecological nature as they are used as defence against predators (herbivores,
pathogens etc.), for interspecies competition, and to facilitate the reproductive processes. Contrary to
primary metabolites these compounds are not ubiquitous in the living organisms who produce them nor
are they necessarily expressed continuously. Although plants are better known as a source of secondary
metabolites, bacteria, fungi and many marine organisms (sponges, tunicates, corals, snails) are very
interesting sources, too. Secondary metabolites can be classified by their chemical structure or physical
properties into one or more of the following groups: alkaloids, terpenoids, polyketides, aliphatic,
aromatic, and heteroaromatic organic acids, phenols, iridoids , steroids, saponins, peptides, ethereal
oils, resins and balsams. Secondary metabolites are the natural plant products, which are not involved in
the metabolic processes of plants such as photosynthesis. They are also called as secondary plant
products.
Functions
These secondary metabolites help a plant in defense from predators, and sometimes they help in
reproduction processes like pollination. These plant products called as secondary metabolites are
more useful for human mankind as they protect us from many diseases and disorders. Plants
produce a variety of secondary metabolites.
Some of the important secondary metabolites are given below
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 2/18
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 3/18
Plant defense- When there is fungal invasion, plants release hydrogen peroxide which helps the
plant in defense against many antigens. Hydrogen peroxide is produced by a plant and it moves
to the cell wall. Cell wall is the site of invasion. It comes in contact with the enzyme peroxidase
and breaks down pectinase. Thus the foreign harmful substance is rendered useless and hydrogen
peroxide helps in the defense mechanism of plants.
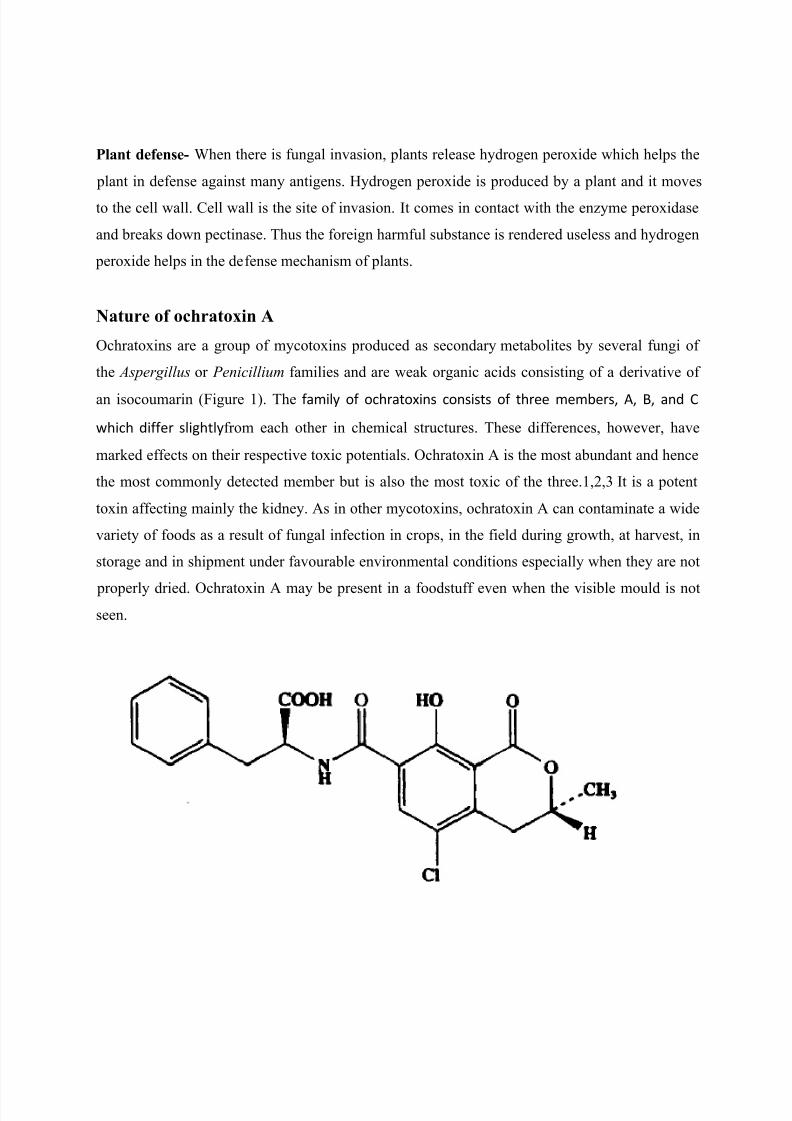
Nature of ochratoxin A
Ochratoxins are a group of mycotoxins produced as secondary metabolites by several fungi of
the Aspergillus or Penicillium families and are weak organic acids consisting of a derivative of
an isocoumarin (Figure 1). The family of ochratoxins consists of three members, A, B, and C
which differ slightlyfrom each other in chemical structures. These differences, however, have
marked effects on their respective toxic potentials. Ochratoxin A is the most abundant and hence
the most commonly detected member but is also the most toxic of the three.1,2,3 It is a potent
toxin affecting mainly the kidney. As in other mycotoxins, ochratoxin A can contaminate a wide
variety of foods as a result of fungal infection in crops, in the field during growth, at harvest, in
storage and in shipment under favourable environmental conditions especially when they are not
properly dried. Ochratoxin A may be present in a foodstuff even when the visible mould is not
seen.

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 4/18
Figure 1. Ochratoxin A
Occurrence and common food products involved
Ochratoxin A is found mainly in cereal and cereal products. This group of commodities has been
reported to be the main contributors to ochratoxin A exposure in exposure assessments carried
out by the European Commission4,5, accounting for 50% of total dietary exposure of ochratoxin
A in European countries (SCOOP task 3.2.7, 2002). Besides cereals and cereal products,
ochratoxin A is also found in arange of other food commodities, including coffee, cocoa, wine,
beer, pulses, spices, dried fruits, grape juice, pig kidney and other meat and meat products of
non-ruminant animals exposed to feedstuffs contaminated with this mycotoxin. Ruminant
animals such as cows and sheep are generally resistant to the effects of ochratoxin A due to
hydrolysis to the non-toxic metabolites by protozoa in the stomachs before absorption into the
blood.
Associated fungal species and geographical distributions
The frequency of the occurrence of the different species of ochratoxinA- producing fungi differs
according to the geographical regions and in the commodities affected. The Penicillium species
that is associated with ochratoxin A production, Penicillium verrucosum,is a common storage
fungus and is the source of ochratoxin A in crops in the cool temperate regions such as Canada,
eastern and north western Europe and parts of South America. It grows only at temperatures
below 30°C and at a lower water activity7. Penicillium species may produce ochratoxin at
temperatures as low as 5°C.In contrast, Aspergillus species appears to be limited to conditions of
high humidity and temperature growing in the tropical and subtropical climates and is the source
of contamination for coffee and cocoa beans, spices, dried vine fruit, grape juice and wine.
Aspergillus ochraceus is the best known species of ochratoxin ±producing Aspergillus. It grows
at moderate temperatures and at a high water activity and is a significant source of ochratoxin Ain cereals. It infects coffee beans usually during sun-drying causing contamination in green
coffee. Aspergillus carbonarius is highly resistant to sunlight and survives sun-drying because of
its black spores and therefore grows at high temperatures. It is associated with maturing fruits
and is the source of ochratoxin A in grapes, dried vine fruits, and wine and is also another source

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 5/18
of ochratoxin A in coffee. Another closely related species, Aspergillus niger, is another minor
source of ochratoxin A production in infected coffee beans and dried vine fruits
.Chemistry and effects of processing.
Ochratoxin A is a moderately stable molecule and is able to survive most food processing to
some extent and may thus occur in consumer products. Processing may involve boiling, baking,
roasting or fermentation, and the degree to which it is destroyed will further depend on other
parameters such as pH, temperature and the other ingredients present. Ochratoxin A is only
partly destroyed during cooking and bread making. Baking and roasting have been reported to
reduce the toxin content by a mere 20%.9,10 However, physical treatment of grain, such as
scouring while cleaning the grain prior to milling, can result in a >50% reduction of ochratoxin
A contamination in the resultant wheat flour. Milling seems to have no or only a minor effect on
the level of ochratoxin A.11
Sources of human exposure
Dietary intake represents the main source of ochratoxin A in human. Human exposure to
ochratoxin A occurs mainly through consumption of contaminated crops or food derived from
animals exposed to contaminated feedstuffs. Occupational exposures from inhalation of dust at
grain storage warehouses are uncommon. Levels of ochratoxin A in human can be measured by
detection of ochratoxin A in human blood and breast milk. A collaborative survey carried out by
13 member states in European Commission in 1995 (SCOOP task 3.2.2) estimated ochratoxin A
intakes in human based on plasma levels of the toxin as a biomarker and found that similar levels
were obtained by estimations from dietary exposure from food surveys. This suggests that the
main sources of ochratoxin A are the known dietary sources covered in the food surveys.
Toxicity and health implications
Metabolism

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 6/18
11. Ochratoxin A is absorbed from the gastrointestinal tract. In mostspecies, ochratoxin A is
absorbed from the stomach as a result of its acidic properties12. Absorption also takes place in
the small intestine particularly in the proximal jejunum. In non-ruminant species such as pigs,
chickens, rabbits and rats,around half of the ingested ochratoxin A may be absorbed.13,14 The
absorbed ochratoxin A is distributed via blood, mainly to the kidneys, and at lower
concentrations to the liver, muscle and fat, with a proportion metabolised into thenon-toxic
metabolite ochratoxin alpha and other less toxic minor metabolites atvarious sites in different
species12, and a significant proportion excretedunchanged. Ochratoxin A has a long serum half -
life in non-ruminant animals andin humans (72-120 h in pigs, 840 h in a human subject) on the
basis of its strong binding to serum macromolecules. In ruminant species such as the cow,
effective hydrolysis of ochratoxin A to the non-toxic ochratoxin alpha takes place in the four
stomachs in the presence of the ruminant protozoa6 rendering the species resistant to the effects
of the toxin. Transfer to the milk has been demonstrated in rats, rabbits and humans. In contrast,
little ochratoxin A is transferred to the milk of ruminants, again due to metabolism of this
mycotoxin by the rumen microflora.
Acute toxicity
The acute toxicity of ochratoxin A is relatively low, although large species differences and
sensitivity are seen with oral LD50 values ranging widely in different species. Oral LD50 values
has been demonstrated to range from 0.2 mg/kg bw in dogs, 1 mg/kg bw in pigs, 3.3 mg/kg bw
in chicken, and 46-58 mg/kg bw in mouse. Dogs and pigs have been reported to be the most
sensitive species15. Effects of acute poisoning such as multifocal haemorrhages in various
organs and fibrin thrombi in the spleen, brain, liver, kidney and heart have been reported
following single dose administration. Nephrosis, hepatic and lymphoid necrosis, and enteritis
with villous atrophy have also been observed in the test species. At present, there are no
documented cases of acute toxicity reported in humans. Chronic toxicity The subchronic and
chronic effects of ochratoxin A are of greatest concern. Ochratoxin A has been shown to be
nephrotoxic, hepatotoxic, teratogenic and immunotoxic to several species of animals and
carcinogenic in mice and rats causing tumours of the kidney and liver.
Nephrotoxicity

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 7/18
In particular, its role in chronic nephropathies has been extensively documented in many
mammalian species. Ochratoxin A is considered the causal agent in nephropathies observed in
several species of agricultural animals, particularly in pigs. It has produced nephrotoxic effects in
all species of single - stomach animals studied so far, even at the lowest level tested (200 g/kg
feed in rats and pigs). Ochratoxicosis in farm animals such as pigs and poultry may lead to
pathological changes in the kidney such as tubular atrophy, interstitial fibrosis and hyalinised
glomeruli. The main target site of ochratoxin A toxicity is the renal proximal tubule, where it
exerts cytotoxic and carcinogenic effects. Significant sex and species differences in sensitivity to
nephrotoxicity have been observed where pigs have been found to be a more sensitive species
compared with rats or mouse. In human, dietary exposure to ochratoxin A in parts of Bulgaria,
Romania and the former Yugoslavia may have association with Balkan endemic nephropathy, a
chronic progressive kidney disease, that is characterised by progressive hypercreatinaemia,
uraemia, hypertension and oedema.
Other toxicities
. Ochratoxin A has been known to cause hepatic damage and hepatic necrosis in experimental
animals. It is a potent teratogen in mice, rats, hamsters and chicken. Both teratogenic and
reproductive effects have been demonstrated. Ochratoxin A has been reported to be an
immunosuppressor and affects the immune system in a number of mammalian species. It was
able to cause inhibition of protein biosynthesis and inhibition of macrophage migration
Carcinogenicity
Ochratoxin A was tested for carcinogenicity by oral administration in mice and rats. Increased
incidence of hepatocellular tumours in mice of each sex, and association with renal-cell
adenomas and carcinomas have been reported in male mice and in rats of each sex fed with
ochratoxin A. In 1993, the International Agency for Research on Cancer (IARC) classified
ochratoxin A as possible human carcinogen (Group 2B) and concluded that there was sufficient
evidence in experimental animals for the carcinogenicity of ochratoxin A and inadequate
evidence in humans for the carcinogenicity of ochratoxin A.19 The doses at which
carcinogenicity were observed in rodents had been reported to be higher than those that caused
nephrotoxicity.
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 8/18
Genotoxicity
Ochratoxin A has been shown to induce DNA damage, DNA repair, and chromosomal
aberrations in mammalian cells in vitro as well as DNA damage and chromosomal aberrations in
mice treated in vivo. However, the mechanism for genotoxicity is unclear and there was no
evidence that it is mediated by direct interaction with DNA.
Observations in humans
Human exposure, as demonstrated by the occurrence of ochratoxin A in blood, and in human
milk, has been observed in various countries in Europe. Ochratoxin A was found more frequently
and high concentrations in blood samples obtained from people living in regions where the fatal
human kidney disease, Balkan Endemic Nephropathy, occurs. A highly significant relationship
has been observed between Balkan endemic nephropathy and tumours of the urinary tract,
particularly with tumours of the renal pelvis and ureters. Nevertheless, similar average
concentrations have been found in some other European countries where this disease is not
observed. The Joint FAO/WHO Expert Committee on Food Additives (JECFA) concluded in
2001 that the epidemiological and clinical data available do not provide a basis for calculatingthe likely carcinogenic potency in human and that Balkan Endemic Nephropathy may involve
other nephrotoxic agents.
Level of safe intake of ochratoxin A
Following the evaluations carried out in 1990, 1995 and 2001 for ochratoxin A, JECFA has
established a provisional tolerable weekly intake (PTWI) of 100 ng/kg bw/wk for this substance
The European Commission¶s Scientific Committee for Food (SCF), after reviewing its opinion
on ochratoxin A, concluded in 1998 that it would be prudent to reduce exposure to ochratoxin A
as much as possible, ensuring that exposures are towards the lower end of the range of tolerable
daily intakes which has been estimated by other bodies, at a level below 5 ng/kg bw/ day.21
Tolerable intake, which can be expressed in daily, weekly (e.g. PTWI) or monthly basis is an
estimate of the amount of a contaminant that can be ingested over a lifetime without appreciable

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 9/18
risk. An intake above PTWI does not automatically mean that health is at risk. Transient
excursion above the PTWI would have no health consequences provided that the average intake
over long period is not exceeded as the emphasis of PTWI is a lifetime exposure.. Values for the
estimated dietary exposures to ochratoxin A in European countries range from 0.13 to 4.6 ng/kg
bw per day (i.e. 0.91 to 32.2 ng/kg bw per week) with the major source being cereal and cereal
products (SCOOP task 3.2.2 and SCOOP 3.2.7). Following the evaluation in 2001 by JECFA,
the mean total intake of ochratoxin A at the international level was estimated to be 45 ng/kg bw
per week based on aggregated data. This was assessed on the basis of data on mean consumption
combined with weighted mean level of contamination
Codex draft limit
In the recent sessions of the Codex Committee of Food Additives and Contaminants (CCFAC),
there had been active discussions on setting the draft maximum level for ochratoxin A in raw
wheat, barley, rye and derived products. A draft maximum level of 5 g/kg is now held at step 7,
pending for JECFA to conduct a more comprehensive risk assessment by 2006. In the 37th
session of CCFAC held in April 2005, ochratoxin A was considered a high priority item for
evaluation by JECFA, with particular reference to ochratoxin A levels in cereals, exposure
assessment, and effects of processing on residual levels in foods.
Legal limits in some countries
Legal limits of ochratoxin A have been set in a number of food commodities including cereals
and cereal products, dried vine fruits, roasted and soluble coffee, wine, grape juice, and foods for
infants and children by the European Commission under EC regulation 466/2001 22 , 472/2002
23 , 24 and 123/200525. The updated limits set for different food items are listed in Annex 1.
Study on ochratoxin A in food
Studies on levels of ochratoxin A in food, so far, have been conducted mainly in the West.
Consequentially, international data accumulated at present are confined principally to the
Western diet. Little is known about levels of ochratoxin A with regards to the rice - based Eastern
diet pertaining to the weather conditions in countries in the East. The present study was carried
out to evaluate the local situation of the levels of ochratoxin A in food, and to estimate the
dietary exposure to ochratoxin A in secondary school students population in Hong Kong in order
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 10/18
to assess if there is any associated health risk. In this study, the potentials for any risks to health
posed by ochratoxin
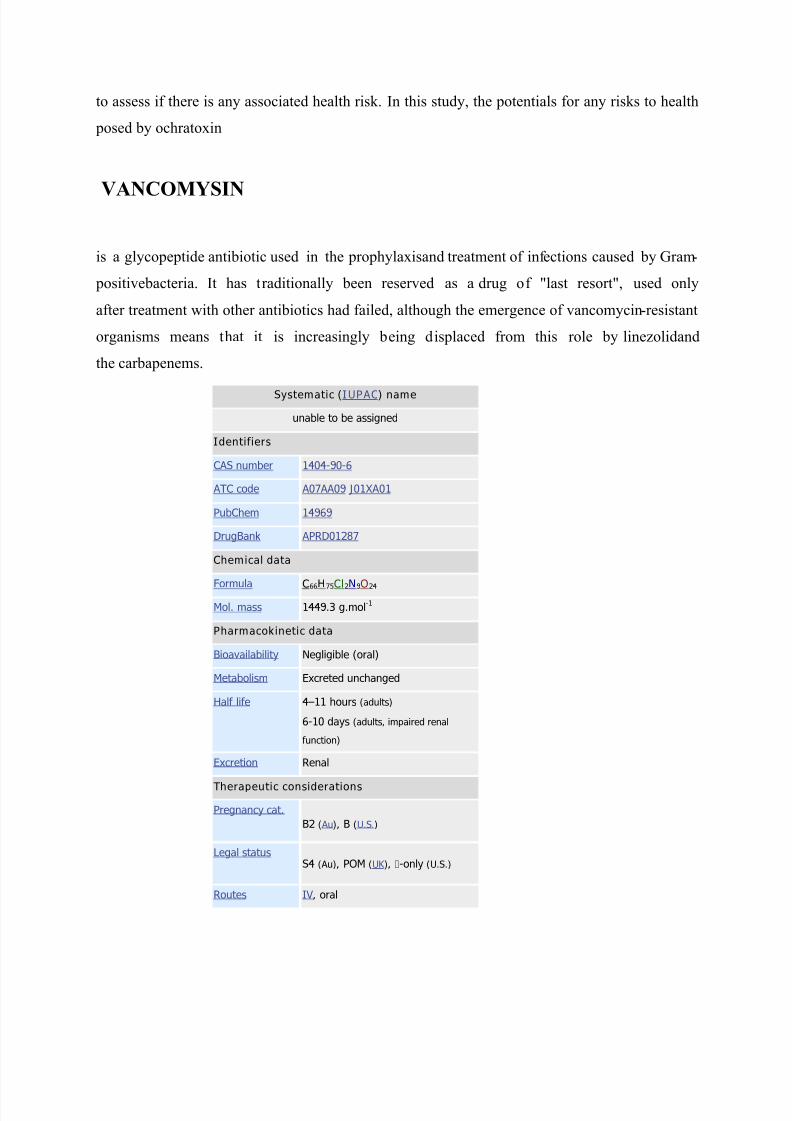
VANCOMYSIN
is a glycopeptide antibiotic used in the prophylaxisand treatment of infections caused by Gram-
positivebacteria. It has traditionally been reserved as a drug of "last resort", used only
after treatment with other antibiotics had failed, although the emergence of vancomycin-resistant
organisms means that it is increasingly being displaced from this role by linezolidand
the carbapenems.
Systematic (IUPAC) name
unable to be assigned
Identifiers
CAS number 1404-90-6
ATC code A07AA09 J01XA01
PubChem 14969
DrugBank APRD01287
Chemical data
Formula
C66H75Cl2N9O24
Mol. mass 1449.3 g.mol-1
Pharmacokinetic data
Bioavailability Negligible (oral)
Metabolism Excreted unchanged
Half life 411 hours (adults)
6-10 days (adults, impaired renal
function)
Excretion Renal
Therapeutic considerations
Pregnancy cat.
B2 ( Au), B (U.S.)
Legal status
S4 (Au), POM (UK ), -only (U.S.)
Routes IV, oral
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 11/18
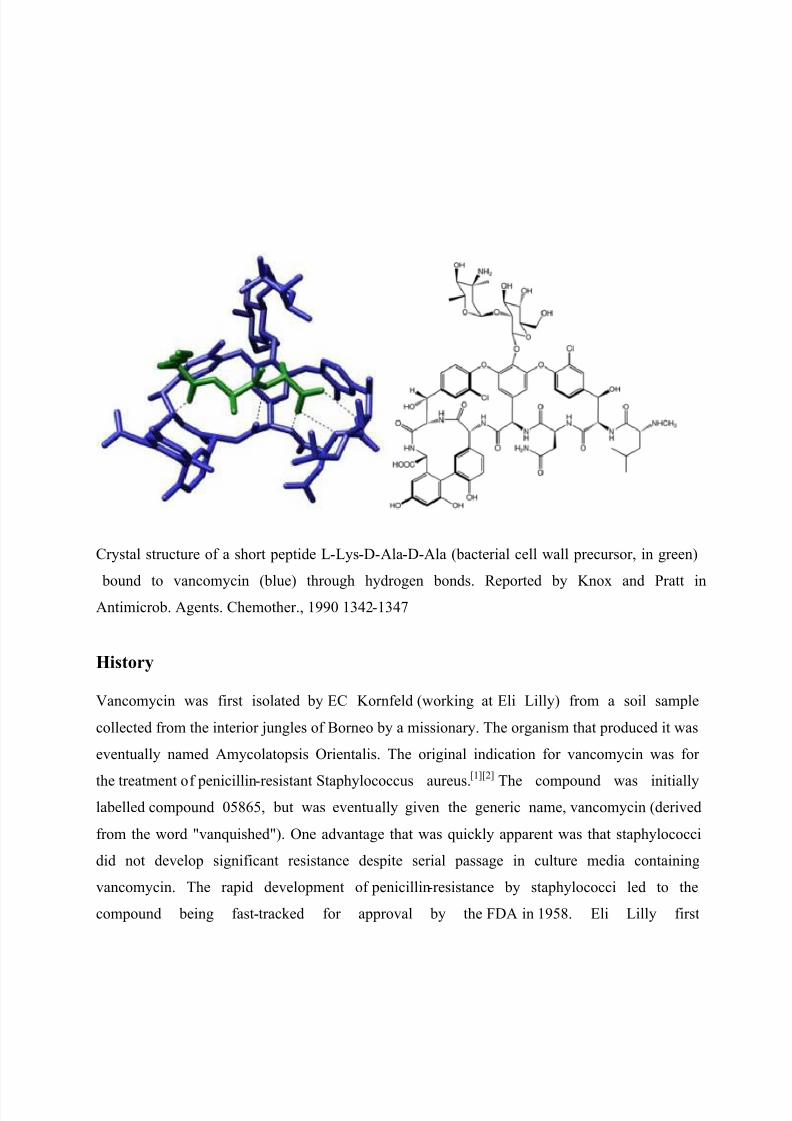
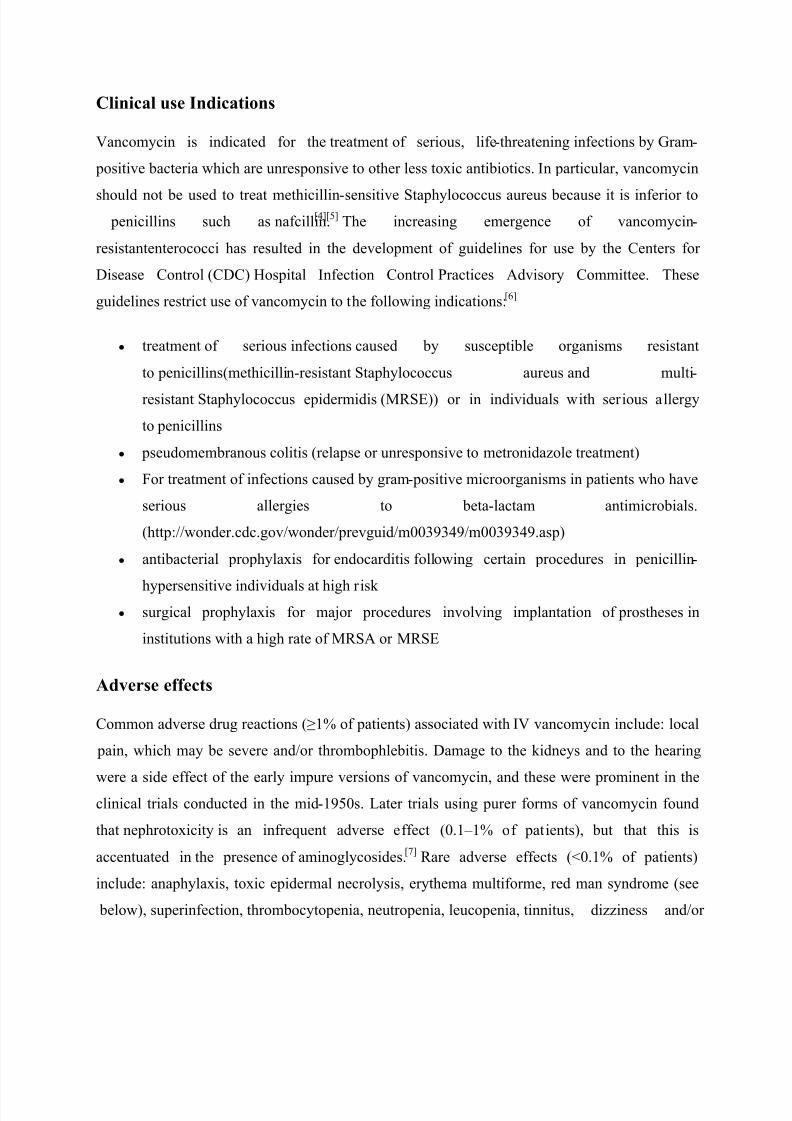
Crystal structure of a short peptide L-Lys-D-Ala-D-Ala (bacterial cell wall precursor, in green)
bound to vancomycin (blue) through hydrogen bonds. Reported by Knox and Pratt in
Antimicrob. Agents. Chemother., 1990 1342-1347
History
Vancomycin was first isolated by EC Kornfeld (working at Eli Lilly) from a soil sample
collected from the interior jungles of Borneo by a missionary. The organism that produced it was
eventually named Amycolatopsis Orientalis. The original indication for vancomycin was for
the treatment of penicillin-resistant Staphylococcus aureus.
[1][2]
The compound was initiallylabelled compound 05865, but was eventually given the generic name, vancomycin (derived
from the word "vanquished"). One advantage that was quickly apparent was that staphylococci
did not develop significant resistance despite serial passage in culture media containing
vancomycin. The rapid development of penicillin-resistance by staphylococci led to the
compound being fast-tracked for approval by the FDA in 1958. Eli Lilly first
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 12/18
marketedvancomycin hydrochloride under the trade name Vancocin.[1]
Vancomycin never
became first line treatment for Staphylococcus aureus for several reasons:
1. The drug must be given intravenously, because it is not absorbed orally.
2. -lactamase-resistant semi-synthetic penicillins such as methicillin (and its
successors,nafcillin and cloxacillin) were subsequently developed.
3. Early trials using early impure forms of vancomycin ("Mississippi mud") which were
found to be toxic to the ears and to the kidneys;[3]
these findings led to vancomycin being
relegated to the position of a drug of last resort.
In 2004, Eli Lilly licensed Vancocin to ViroPharma in the U.S., Flynn Pharma in the UK
andAspen Pharmacare in Australia. The patent expired in the early 1980s and generic versions of
the drug are also available under various trade names.
Pharmacology and chemistry
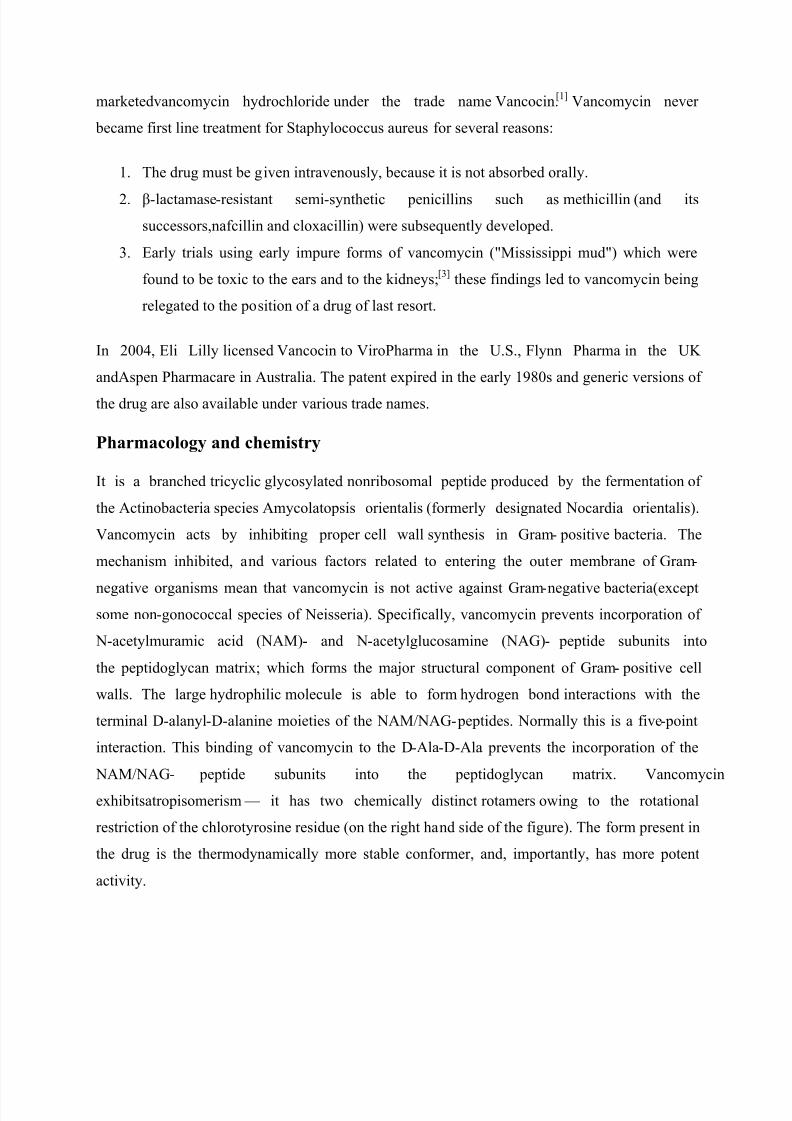
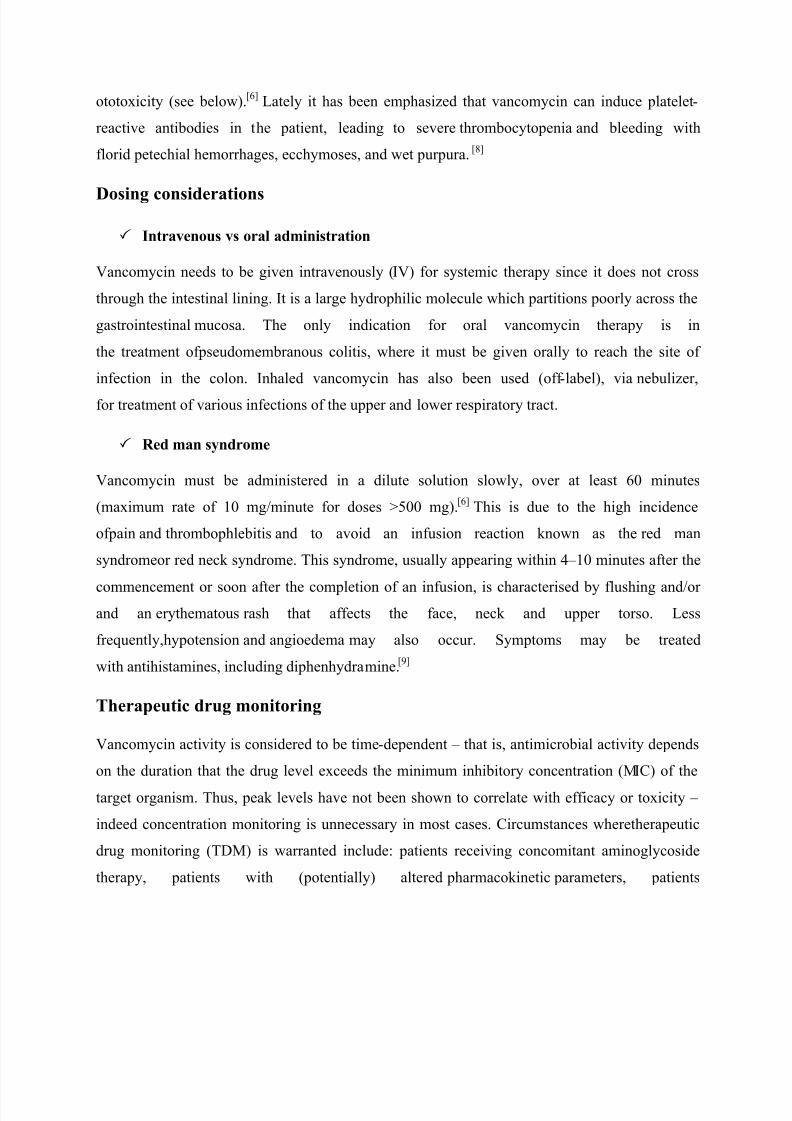
It is a branched tricyclic glycosylated nonribosomal peptide produced by the fermentation of
the Actinobacteria species Amycolatopsis orientalis (formerly designated Nocardia orientalis).
Vancomycin acts by inhibiting proper cell wall synthesis in Gram- positive bacteria. The
mechanism inhibited, and various factors related to entering the outer membrane of Gram-
negative organisms mean that vancomycin is not active against Gram-negative bacteria(except
some non-gonococcal species of Neisseria). Specifically, vancomycin prevents incorporation of
N-acetylmuramic acid (NAM)- and N-acetylglucosamine (NAG)- peptide subunits into
the peptidoglycan matrix; which forms the major structural component of Gram- positive cell
walls. The large hydrophilic molecule is able to form hydrogen bond interactions with the
terminal D-alanyl-D-alanine moieties of the NAM/NAG- peptides. Normally this is a five- point
interaction. This binding of vancomycin to the D-Ala-D-Ala prevents the incorporation of the
NAM/NAG- peptide subunits into the peptidoglycan matrix. Vancomycin
exhibitsatropisomerism ² it has two chemically distinct rotamers owing to the rotational
restriction of the chlorotyrosine residue (on the right hand side of the figure). The form present in
the drug is the thermodynamically more stable conformer, and, importantly, has more potent
activity.
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 13/18
Clinical use Indications
Vancomycin is indicated for the treatment of serious, life-threatening infections by Gram-
positive bacteria which are unresponsive to other less toxic antibiotics. In particular, vancomycin
should not be used to treat methicillin-sensitive Staphylococcus aureus because it is inferior to
penicillins such as nafcillin.[4][5]
The increasing emergence of vancomycin-
resistantenterococci has resulted in the development of guidelines for use by the Centers for
Disease Control (CDC) Hospital Infection Control Practices Advisory Committee. These
guidelines restrict use of vancomycin to the following indications:[6]
y treatment of serious infections caused by susceptible organisms resistant
to penicillins(methicillin-resistant Staphylococcus aureus and multi-
resistant Staphylococcus epidermidis (MRSE)) or in individuals with serious allergy
to penicillins
y pseudomembranous colitis (relapse or unresponsive to metronidazole treatment)
y For treatment of infections caused by gram- positive microorganisms in patients who have
serious allergies to beta-lactam antimicrobials.
(http://wonder.cdc.gov/wonder/prevguid/m0039349/m0039349.asp)
y antibacterial prophylaxis for endocarditis following certain procedures in penicillin-
hypersensitive individuals at high risk y surgical prophylaxis for major procedures involving implantation of prostheses in
institutions with a high rate of MRSA or MRSE
Adverse effects
Common adverse drug reactions (1% of patients) associated with IV vancomycin include: local
pain, which may be severe and/or thrombophlebitis. Damage to the kidneys and to the hearing
were a side effect of the early impure versions of vancomycin, and these were prominent in the
clinical trials conducted in the mid-1950s. Later trials using purer forms of vancomycin found
that nephrotoxicity is an infrequent adverse effect (0.1±1% of patients), but that this is
accentuated in the presence of aminoglycosides.[7]
Rare adverse effects (<0.1% of patients)
include: anaphylaxis, toxic epidermal necrolysis, erythema multiforme, red man syndrome (see
below), superinfection, thrombocytopenia, neutropenia, leucopenia, tinnitus, dizziness and/or
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 14/18
ototoxicity (see below).[6]
Lately it has been emphasized that vancomycin can induce platelet -
reactive antibodies in the patient, leading to severe thrombocytopenia and bleeding with
florid petechial hemorrhages, ecchymoses, and wet purpura. [8]
Dosing considerations
Intravenous vs oral administration
Vancomycin needs to be given intravenously (IV) for systemic therapy since it does not cross
through the intestinal lining. It is a large hydrophilic molecule which partitions poorly across the
gastrointestinal mucosa. The only indication for oral vancomycin therapy is in
the treatment ofpseudomembranous colitis, where it must be given orally to reach the site of
infection in the colon. Inhaled vancomycin has also been used (off -label), via nebulizer,
for treatment of various infections of the upper and lower respiratory tract.
Red man syndrome
Vancomycin must be administered in a dilute solution slowly, over at least 60 minutes
(maximum rate of 10 mg/minute for doses >500 mg).[6]
This is due to the high incidence
ofpain and thrombophlebitis and to avoid an infusion reaction known as the red man
syndromeor red neck syndrome. This syndrome, usually appearing within 4±10 minutes after the
commencement or soon after the completion of an infusion, is characterised by flushing and/or
and an erythematous rash that affects the face, neck and upper torso. Less
frequently,hypotension and angioedema may also occur. Symptoms may be treated
with antihistamines, including diphenhydramine.[9]
Therapeutic drug monitoring
Vancomycin activity is considered to be time-dependent ± that is, antimicrobial activity depends
on the duration that the drug level exceeds the minimum inhibitory concentration (MIC) of the
target organism. Thus, peak levels have not been shown to correlate with efficacy or toxicity ±
indeed concentration monitoring is unnecessary in most cases. Circumstances wheretherapeutic
drug monitoring (TDM) is warranted include: patients receiving concomitant aminoglycoside
therapy, patients with (potentially) altered pharmacokinetic parameters, patients

8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 15/18
on haemodialysis, during high dose or prolonged treatment, and patients with impairedrenal
function. In such cases, trough concentrations are measured.[6][10][11][12]
Toxicity
Vancomycin has traditionally been considered a nephrotoxic and ototoxic drug, based on
observations by early investigators of elevated serum levels in renally impaired patients who had
experienced ototoxicity, and subsequently through case reports in the medical literature.
However, as the use of vancomycin increased with the spread of MRSA beginning in the
seventies, it was recognised that the previously reported rates of toxicity were not being
observed. This was attributed to the removal of the impurities present in the earlier formulation
of the drug, although those impurities were not specifically tested for toxicity.[2]
Nephrotoxicity
Subsequent reviews of accumulated case reports of vancomycin-related nephrotoxicity found
that many of the patients had also received other known nephrotoxins,
particularlyaminoglycosides. Most of the rest had other confounding factors, or insufficient data
regarding the possibility of such, that prohibited the clear association of vancomycin with the
observed renal dysfunction. In 1994, Cantu and colleagues found that the use of vancomycin
monotherapy was clearly documented in only three of 82 available cases in the
literature.[10]
Prospective and retrospective studies attempting to evaluate the incidence of
vancomycin-related nephrotoxicity have largely been methodologically flawed and have
produced variable results. The most methodologically sound investigations indicate that the
actual incidence of vancomycin-induced nephrotoxicity is around 5±7%. To put this into context,
similar rates of renal dysfunction have been reported for cefamandole and benzylpenicillin, two
reputedly non-nephrotoxic antibiotics. Additionally, evidence to relate nephrotoxicity to
vancomycin serum levels is inconsistent. Some studies have indicated an increased rate of
nephrotoxicity when trough levels exceed 10 µg/mL, but others have not reproduced these
results. Nephrotoxicity has also been observed with concentrations within the "therapeutic" range
as well. Essentially, the reputation of vancomycin as a nephrotoxin is over -stated, and it has not
been demonstrated that maintaining vancomycin serum levels within certain ranges will prevent
its nephrotoxic effects, when they do occur.
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 16/18
Ototoxicity
Attempts to establish rates of vancomycin-induced ototoxicity are even more difficult due to the
scarcity of quality evidence. The current consensus is that clearly related cases of vancomycin
ototoxicity are rare. The association between vancomycin serum levels and ototoxicity is also
uncertain. While cases of ototoxicity have been reported in patients whose vancomycin serum
level exceeded 80 µg/mL, cases have been reported in patients with therapeutic levels as well.
Thus, it also remains unproven that therapeutic drug monitoring of vancomycin for the purpose
of maintaining "therapeutic" levels will prevent ototoxicity.
Interactions with other nephrotoxins
Another area of controversy and uncertainty concerns the question of whether, and if so, to what
extent, vancomycin increases the toxicity of other nephrotoxins. Clinical studies have yielded
variable results, but animal models indicate that there probably is some increased nephrotoxic
effect when vancomycin is added to nephrotoxins such as aminoglycosides. However, a dose- or
serum level-effect relationship has not been established.
Antibiotic resistance Intrinsic resistance
There are a few gram- positive bacteria that are intrinsically resistant to vancomycin: these
areLeuconostoc and Pediococcus species, but these organisms are rare causes of disease in
humans.[13]
Most Lactobacillus species are also intrinsically resistant to vancomycin[13]
(the
exception is L. acidophilus[14]
). Most gram-negative bacteria are intrinsically resistant to
vancomycin because of their outer membrane is impermeable to large glycopeptide
molecules[15]
(with the exception of some non-gonococcal Neisseria species).[16]
Acquired resistance
Acquired microbial resistance to vancomycin is a growing problem, particularly within health
care facilities such as hospitals. With vancomycin being the last-line antibiotic for serious Gram-
positive infections there is the growing prospect that resistance will result in a return to the days
when fatal bacterial infections were common. Vancomycin-resistant enterococci (VRE) emerged
in 1987. Vancomycin resistance emerged in more common pathogenic organisms during
the 1990s and 2000s, including vancomycin-intermediate Staphylococcus
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 17/18
aureus(VISA), vancomycin-resistant Staphylococcus aureus (VRSA), and vancomycin-
resistantClostridium difficile.[17][18] There is some suspicion that agricultural use of avoparcin,
another similar glycopeptide antibiotic, has contributed to the emergence of vancomycin-
resistant organisms. One mechanism of resistance to vancomycin appears to be alteration to the
terminal amino acid residues of the NAM/NAG- peptide subunits, normally D-alanyl-D-alanine,
which vancomycin binds to. Variations such as D-alanyl-D-lactate and D-alanyl-D-serine result
in only a 4- point hydrogen bonding interaction being possible between vancomycin and the
peptide. This loss of just one point of interaction results in a 1000-fold decrease in affinity.
InEnterococci this modification appears to be due to the expression of an enzyme which alters
the terminal residue. Three main resistance variants have been characterised to date among
resistant Enterococcus faecium and E. faecalis populations.
y VanA - resistance to vancomycin and teicoplanin, inducible on exposure to these agents
y VanB - lower level resistance, inducible by vancomycin but strains may remain
susceptible to teicoplanin
y VanC - least clinically important, resistance only to vancomycin, constitutive resistance
The development and use of novel antibiotics such as linezolid and daptomycin is expected to
delay, but not halt, the emergence of bacteria resistant to all available antibiotics.
8/8/2019 Biochem Ass
http://slidepdf.com/reader/full/biochem-ass 18/18
References
1. ^ a b
Moellering, RC Jr. (2006). "Vancomycin: A 50-Year Reassessment". Clin Infect
Dis42: S3±S4. PubMed.
2. ^ a b
Donald P. (2006). "Vancomycin: A History". Clin Infect Dis 42: S5-S12. PMID
16323120.
3. ^ Griffith RS. (1981). "Introduction to vancomycin". Rev Infect Dis 3: S2004.
4. ^ Small PM, Chambers HF (1990). "Vancomycin for Staphylococcus aureus endocarditis
in intravenous drug users". Antimicrob Agents Chemother 34: 1227±31. PMI
D 2393284.5. ^ Gonzalez C, Rubio M, Romero-Vivas J, Gonzalez M, Picazo JJ (1999). "Bacteremic
pneumonia due to Staphylococcus aureus: a comparison of disease caused by methicillin-
resistant and methicillin-susceptible organisms". Clin Infect Dis 29: 1171±7. PMID
10524959.
6. Google search
7. Boosrags .com