belgian consensus meeting - institute of tropical · pdf file1- concept low risk malaria ......
TRANSCRIPT

BELGIAN
CONSENSUS MEETING
on TRAVEL MEDICINE
June 26, 2015
Belgian
Scientific Study
Group on Travel
Medicine
Pr. A. Van Gompel Dr. U Maniewski (ITG)
Pr. F. Jacobs (Hôp. Erasme, ULB)
Pr. P. Lacor & Dr. L Seyler (UZ-Brussel)
Dr. Ph. Leonard (CHU-ULg)
Pr. W. Peetermans (U.Z. - K.U.Leuven)
Pr. S. Callens(UZ.- U.Gent)
Dr. S. Quoilin (iph.fgov.be)
Dr. P. Soentjens (Belgian Defence)
Pr. B. Vandercam (CHU. St. Luc, UCL)
Pr. Y. Van Laethem & Dr. C Martin (CHU. St. Pierre, ULB) PART 1b malaria version 25/11/15

REPORT
BELGIAN CONSENSUS MEETING on TRAVEL MEDICINE
June 26, 2015 – PART 1b
2015
• The consensus meeting was chaired by A. Van Gompel and Y, Van Laethem
• Secretary of the meeting was P Lacor
• A preliminary PowerPoint, prepared by A. Van Gompel, was presented
• The discussion and recommendations of the meeting are included in this finale presentation.
• The ESSENTIAL SLIDES (pdf-version) & the CONSENSUS BROCHURE (in Dutch and French) highlighting the proposals for changes will been sent to all participants. May be used for teaching.
• These documents will serve as a proposal for approval by the governmental Belgian Health Council – section Vaccinations, on 17-09-2015
• Responsable final redaction : A. Van Gompel

PART 1
• 1.a - Vaccination for Yellow Fever
• 1.b - Malaria
PART 2
• 2.A - Other vaccinations
• 2.B - TD, other infections, ….,
• 2.C - VARIA
2015


Malaria

Only these chapters are updated
They are freely downloadable
http://www.who.int/ith/en/ Only a few chapters are updated 2014 & 2015
WHO 15-06-2015

Malaria
The guidelines for malaria have not really changed in 2015
2015

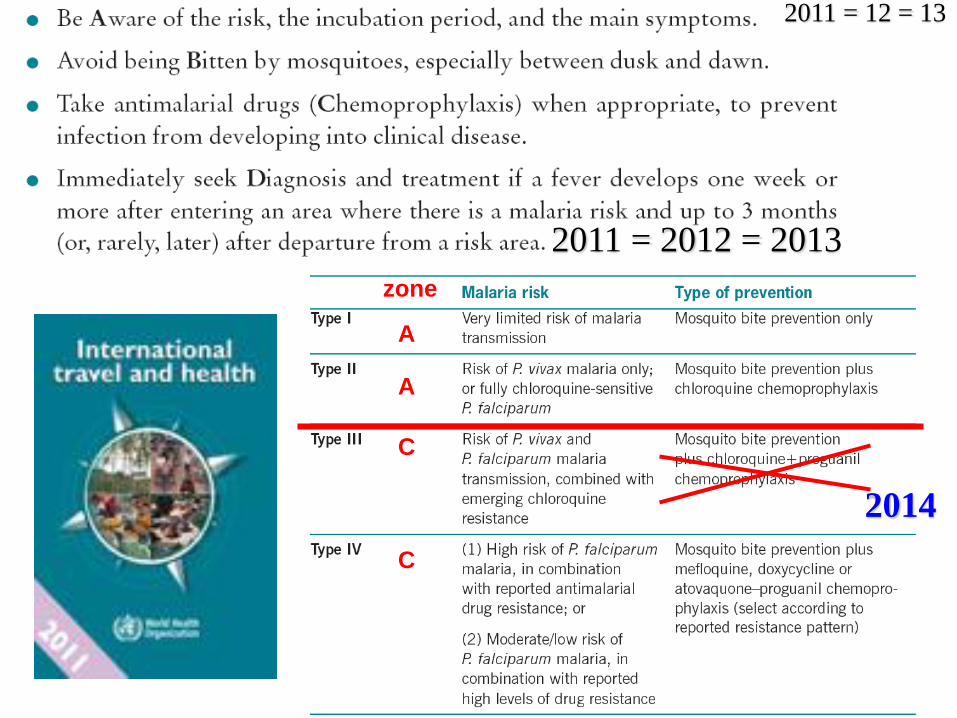
• A: Awareness
• B: Bite prevention
• C: Chemoprophylaxis, if indicated.
• D: Diagnosis
• E: Environment: Avoid outdoor activities in environments
that are mosquito breeding places, especially in late
evenings and at night.
8
ABCDE of
malariaprevention for
travellers
25-11-2015
A
C
C
zone
A
2014
2011 = 2012 = 2013
2011 = 12 = 13

2014
the Belgian guidelines are not changing yet

11
Mosquito bite prevention + think of malaria when T° + /- chemoprophylaxis intermittent or SBET
Alternatively, for travel to rural areas with low risk of malaria infection, mosquito
bite prevention can be combined with stand-by emergency treatment (SBET).
or (very) low risk of P falciparum
A/B
2015

WHO 2014 = 2015

25-11-2015

There is a need to be capable
to give more nuanced
malaria-prevention advice
for many / most regions in
Asia & Latin America:
2015

1- Concept
Low risk malaria areas (< 1 case/1000/year in local population)
“Low risk - Very low risk - Negligible low risk”
2015
2- Many long-term travellers,
not necessarily backpackers only,
have no fixed itinerary, and often stay only briefly in higher risk areas
****************

http://www.sbimc.org/Malaria%20low%20risk%20areas.pdf
2013

Switzerland – Germany – Austria ….SBET only since more than 10-15 years 2014

In low risk malaria areas ?
Switzerland, Germany, Austria
• Mosquito bite prevention
PLUS always
• In case of fever
“think malaria too”
AND always
• SBET = Standby emergency
treatment
– Noodbehandeling
– Traitement d’urgence
Belgium
• Mosquito bite prevention
PLUS always
• In case of fever “think malaria too”
PLUS only in some cases
• SBET
AND / OR only in some cases
• Intermittently chemoprofylaxis “on demand” ??
2015

On-demand malaria chemoprophylaxis
based on regional risk ?
• cfr on demand pacemaker, of on demand omeprazole, ventolin, etc
• better ?
– intermittent risk based malaria
chemoprofylaxe
– intermittent regional risk based malaria
chemoprofylaxis
– on risk malaria chemoprophylaxis
• or ?
– Standby malaria chemoprophylaxis – SBCP
(confusion with SBET ?)
2015

Voumard
When travelling to moderate- to low-risk malaria areas, 85% of interviewees
chose not to take chemoprophylaxis as malaria prevention, although most
(non-Swiss) guidelines recommend it.
… hence 15 % of interviewees chose to take chemoprophylaxis as malaria
prevention, although Swiss guidelines do not recommend it...
They had coherent reasons for their choice.
New recommendations should include shared decision-making to take into
account travellers’ preferences.
Switzerland

Switzerland – Germany – Austria ….SBET only since more than 10-15 years 2015

Let’s take …India

Lectures on Malaria India
NECTM 5 – Bergen Norway
• Malaria-risk for the local population in
India is grossly underestimated by official
WHO – numbers
• However for most travelers the risk is
very low to negligible
Breakpoint = Areas of low transmission = where
the reported malaria case incidence from all
species was < 1 per 1000 (persons within the
local population) per year
• “we should adopt the malariaguidelines of
the German speaking countries”
2014

Lectures on Malaria in India
NECTM5 – Bergen Norway
2014
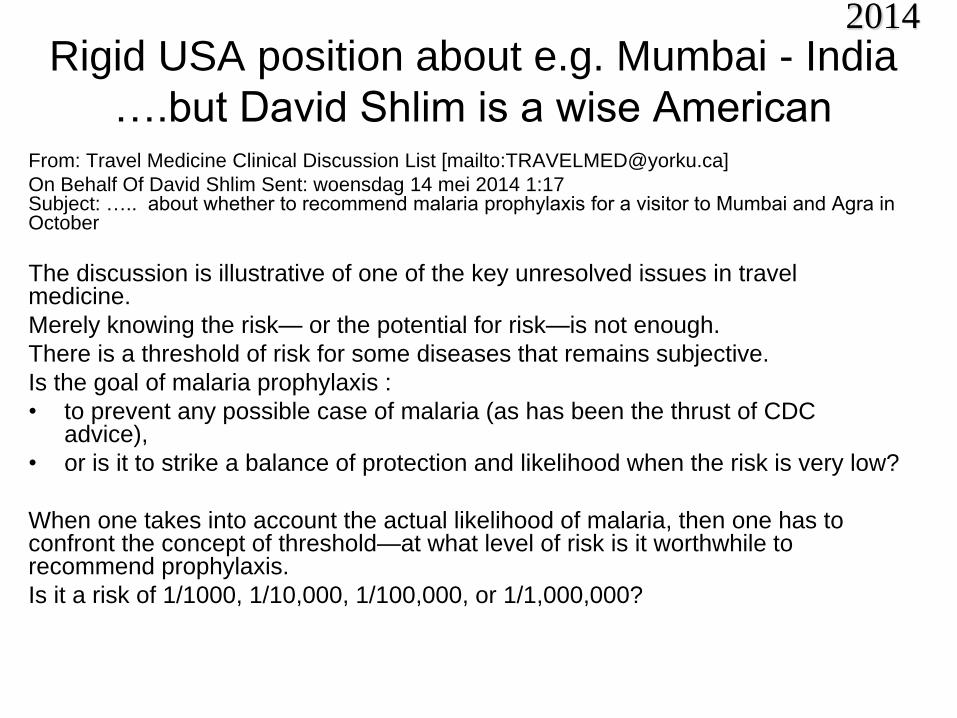
Rigid USA position about e.g. Mumbai - India
….but David Shlim is a wise American From: Travel Medicine Clinical Discussion List [mailto:[email protected]]
On Behalf Of David Shlim Sent: woensdag 14 mei 2014 1:17 Subject: ….. about whether to recommend malaria prophylaxis for a visitor to Mumbai and Agra in October
The discussion is illustrative of one of the key unresolved issues in travel medicine.
Merely knowing the risk— or the potential for risk—is not enough.
There is a threshold of risk for some diseases that remains subjective.
Is the goal of malaria prophylaxis :
• to prevent any possible case of malaria (as has been the thrust of CDC advice),
• or is it to strike a balance of protection and likelihood when the risk is very low?
When one takes into account the actual likelihood of malaria, then one has to confront the concept of threshold—at what level of risk is it worthwhile to recommend prophylaxis.
Is it a risk of 1/1000, 1/10,000, 1/100,000, or 1/1,000,000?
2014

Rigid USA position about e.g. Mumbai - India
….but David Shlim is a wise American From: Travel Medicine Clinical Discussion List [mailto:[email protected]]
On Behalf Of David Shlim Sent: woensdag 14 mei 2014 1:17 Subject: ….. about whether to recommend malaria prophylaxis for a visitor to Mumbai and Agra in October
It would seem that the traveler should be a participant in making a decision about prophylaxis in circumstances that one could call “minimal risk.”
The risk is not zero, but it is so low that some people will elect not to take prophylaxis (and some people will elect to take prophylaxis).
In most of Africa, the risk of malaria is so significant that this type of discussion is not appropriate.
However, in many parts of India, Central and South America, and SE Asia, it is appropriate.
There may be no “right” answer in these situations.
India is a complex risk situation, with the overall number of cases in returning travelers to US on the increase, mainly in the VFR population.
However, it is difficult to find case reports of malaria that occurred in non-VFR travelers who only visited an urban area.
Warmly, David
David R Shlim MD President, ISTM Jackson Hole, Wyoming
2014

2014

2014

2014

2013 2014
2014

2015 Belgium :

… Sri Lanka

WHO 2014
http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0043162
WHO/ITH 2015 Malaria (2015): Limited malaria risk – P. vivax (88%), P. falciparum (12%) – exists throughout the year, except in the districts of Colombo, Galle, Gampaha,
Kalutara, Matara and Nuwara Eliya. No locally acquired cases reported since October 2012. Recommended prevention in risk areas: A

….Viet Nam

WHO 2014
© Tropimed
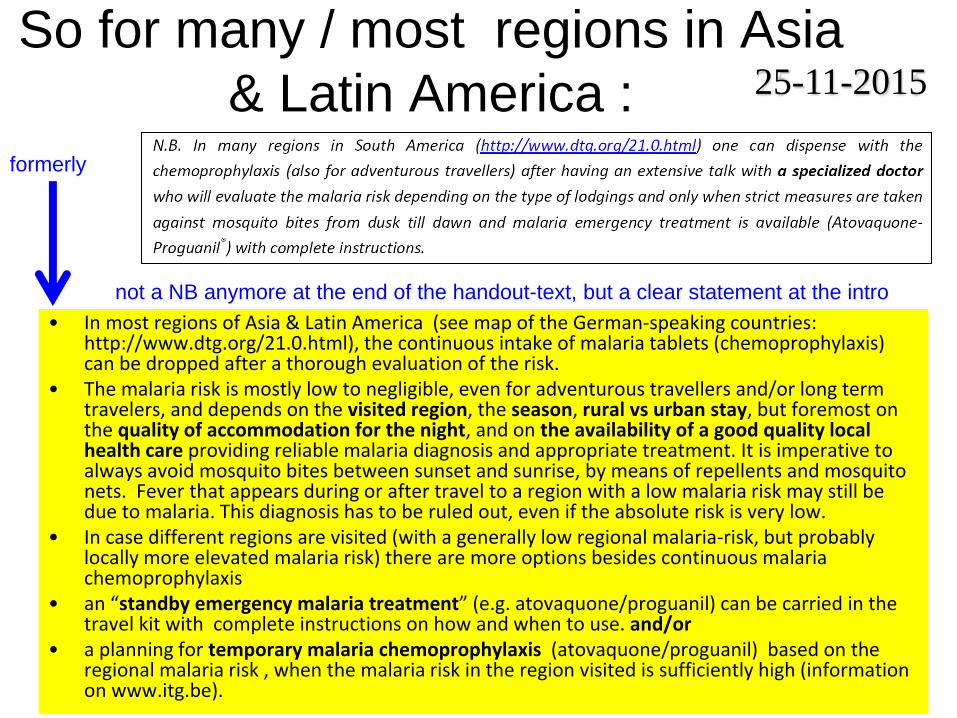
So for many / most regions in Asia
& Latin America :
• In most regions of Asia & Latin America (see map of the German-speaking countries: http://www.dtg.org/21.0.html), the continuous intake of malaria tablets (chemoprophylaxis) can be dropped after a thorough evaluation of the risk.
• The malaria risk is mostly low to negligible, even for adventurous travellers and/or long term travelers, and depends on the visited region, the season, rural vs urban stay, but foremost on the quality of accommodation for the night, and on the availability of a good quality local health care providing reliable malaria diagnosis and appropriate treatment. It is imperative to always avoid mosquito bites between sunset and sunrise, by means of repellents and mosquito nets. Fever that appears during or after travel to a region with a low malaria risk may still be due to malaria. This diagnosis has to be ruled out, even if the absolute risk is very low.
• In case different regions are visited (with a generally low regional malaria-risk, but probably locally more elevated malaria risk) there are more options besides continuous malaria chemoprophylaxis
• an “standby emergency malaria treatment” (e.g. atovaquone/proguanil) can be carried in the travel kit with complete instructions on how and when to use. and/or
• a planning for temporary malaria chemoprophylaxis (atovaquone/proguanil) based on the regional malaria risk , when the malaria risk in the region visited is sufficiently high (information on www.itg.be).
not a NB anymore at the end of the handout-text, but a clear statement at the intro
formerly
25-11-2015

Mefloquine
precautions
& legal obligations !!!
2015

2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015
Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

Roche - Lariam ®
Obligatory patient alert card to share with the clients
2014
2014

2014

2015

2015

Travel medicine Seminar 19 /11/15
“Travel medicine Seminar 20 years later”
MILITAIR HOSPITAAL as in 1995 14.00-14.05 Introduction
14.05-14.35 Yellow Fever Immunization: where are we up to now?
CHARLOTTE MARTIN
14.35-15.05 The last-minute traveler: an update on accelerated vaccine schedules PATRICK SOENTJENS
15.05-15.25 Epidemiologic flashes & edge cutting news / new vaccines
STEVEN CALLENS
15.25-16.00 Coffee break
16.00-16.25 Travellers diarrhea
LUCIE SEYLER
16.25- 16.50 Malaria: when prevention is not clear-cut
ULA MANIEWSKI
16.50-17.15 Traveller's Thrombosis
PETER VERHAMME
17.15-17.45 What did change (drastically) in the last 20 years in travel medicine ?
FONS & YVES
Have a look at http://www.sbimc.org for the pdf’s of the powerpoints of all the lectures since 2009

End Malaria
2013
