balancing cost- effectiveness with other values: the nice experience stirling bryan department of...
TRANSCRIPT

Balancing cost-effectiveness with other
values: the NICE experience
Stirling Bryan
Department of Health Economics

Overview
Introduction to the National Institute for Health & Clinical Excellence (NICE)
Cost-effectiveness analysis as a key driver of NICE decisions
The NICE equity and social value principles
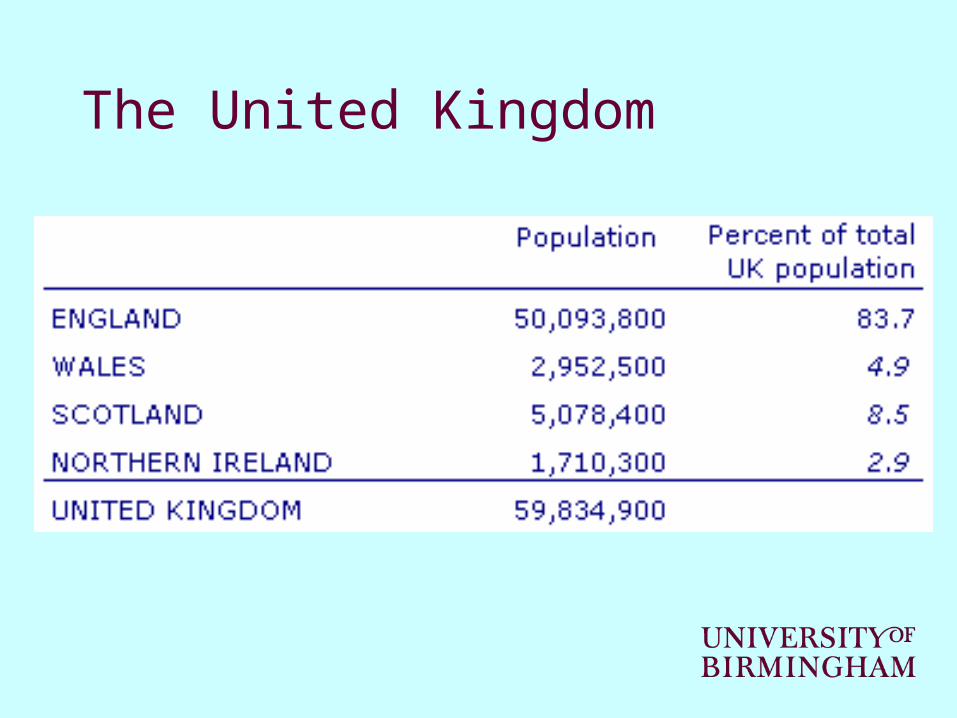
The United Kingdom
NICE Programmes
Technology appraisals– Criteria include both clinical and cost effectiveness
Clinical guidelines– Criteria include both clinical and cost effectiveness
Public health guidance– Criteria include both effectiveness and cost effectiveness
Interventional procedures– Guidance on safety and efficacy

Technology ‘coverage’ decisions in England
Local level – main budget holders are the PCTs but wide variety of decision-making bodies
National level – NICE– coverage decisions based on explicit criteria,
informed by evidence review and economic evaluation
– submissions received from independent academic team, the sponsor of the technology, and other expert bodies

SubmissionsSubmissions
11stst Committee meeting Committee meeting preliminary preliminary
recommendationsrecommendations
PublicationPublication
22stst Committee meeting Committee meeting final guidancefinal guidance
Consultation Consultation on preliminary on preliminary recommendationsrecommendations
AppealAppeal (or not)(or not)
ReferralReferral
[14 months]
AssessmentAssessmentConsultationConsultationon evidenceon evidence
Review
14 weeks
13 weeks
4 weeks
4 weeks

NICE Appraisal Committee membership (n=28)
Area of expertise Number of Committee members (per branch)
Medical (e.g. GP, physician, surgeon)
12 (43%)
Other clinical (e.g. nurse, pharmacist)
4 (14%)
Methodologists (e.g. health economist, statistician)
5 (18%)
Managers 3 (11%)
Patient ‘advocate’ 2 (7%)
Manufacturer ‘representative’ 2 (7%)

NICE ‘reference case’ for CEAElement of health technology assessment
Reference case
Comparator Alternative therapies routinely used in the NHS
Perspective on costs Perspective on outcomes Type of economics evaluation Synthesis of evidence on outcomes Measure of health benefits Description of health states for calculation of QALYs
NHS and PSS All health effects on individuals Cost-effectiveness analysis Based on a systematic review Quality-adjusted life-years (QALYs) Health states described using a standardised and validated generic instrument

Example CEA: anakinra for RA
Results Cost QALYs With Anakinra £14,523 3.840 Without Anakinra £2,841 3.729 Difference £11,682 0.111 ICER (cost per quality-adjusted life-year)
£105,000
Guidance: “Anakinra should not normally be used as a treatment for rheumatoid arthritis. It should only be given to people who are taking part in a study on how well it works in the long term.”
The importance of CEA at NICE
Secretary of State’s Direction to NICE:– NICE should consider … “The broad balance of clinical
benefits and costs”
Bryan et al (2007):– “I think economic evaluation was regarded as being
important from day one.”– “It [the CEA] seems to me to be the clincher really. If it’s too
high then it’s not going to get funded.”
NICE social value principle 2:– NICE “must take into account the relative costs and benefits
of interventions (their 'cost effectiveness') when deciding whether or not to recommend them.”
The drug itself has no side effects … but the number of health economists needed to prove its
value may cause dizziness and nausea
The US and this debate …
Britain Stirs Outcry by Weighing Benefits of Drugs Versus Price
Millions of patients around the world have taken drugs introduced over the past decade to delay the worsening of Alzheimer's disease. …
But this year, an arm of Britain's government health-care system, relying on some economists' number-crunching, said the benefit isn't worth the cost. It issued a preliminary ruling calling on doctors to stop prescribing the drugs.
THE WALL STREET JOURNAL November 22, 2005; Page A1
Committee procedures: the threshold
There is a feeling when we get beyond £30,000 per QALY we’re running into trouble.
I do sometimes have reservations about the figure of £30,000 per QALY. Where does the figure come from? Who determines where the cut-off point should be?
My biggest criticism … is basically we are funding things at a level that actually the NHS cannot afford – that the [cost per] QALY figure is far too high, it should be much lower.
Bryan et al (2007)
Birch & Gafni (2007) ‘Economists’ dream or nightmare?’ HEPL
“The efficiency of adopting the new intervention depends crucially on where the additional resources required to support the new intervention are to be taken from and at what opportunity cost.”
NICE and procedural justice
Framework: 'accountability for reasonableness‘ (Daniels & Sabin, 2002)
– Publicity– Relevance– Challenge and revision– Regulation

NICE ‘reference case’ and distributive justice
Element of health technology assessment
Reference case
Method of preference elicitation for health state valuation Source of preference data Discount rate Equity position
Choice-based method (for example, time trade-off; standard gamble, not rating scale) Representative sample of the public An annual rate of 3.5% on both costs and health effects An additional QALY has the same weight regardless of the other characteristics of the individuals receiving the health benefit
NICE’s social value principles
Principle 3– Decisions about whether to recommend interventions should
not be based on evidence of their relative costs and benefits alone. NICE must consider other factors when developing its guidance, including the need to distribute health resources in the fairest way within society as a whole.
Principle 4– If NICE decides not to recommend use of an intervention
with a cost per QALY gained within or below the range £20,000 to £30,000 per QALY gained, or decides it will recommend use of an intervention within or above this range, it must explain the reasons why.
NICE’s social value principles
Principle 5– Although NICE upholds the right of individuals to make their
own decisions about their care, this should not lead NICE to recommend interventions that are not effective and cost effective for the NHS as a whole.
Principle 7– NICE can recommend that use of an intervention is
restricted to a particular group (e.g. people under or over a certain age) but only in certain circumstances. There must be clear evidence about the increased effectiveness of the intervention in this subgroup, or other reasons relating to fairness for society as a whole, or a legal requirement to act in this way.
Procedural and distributive justice coming together
Principle 6– NICE should consider and respond to comments it
receives about its draft guidance, and change it where appropriate. But NICE must always use its own judgement to ensure that what it recommends is cost effective and takes account of the need to distribute health resources in the fairest way within society as a whole.

Informationprocessing
The ‘workings’ of the Committee
Practical issuesrelating to economic
analyses
Appraisal Committee composition
Conceptual challenges
Committeeprocedures
Political
Concepts & processes
Practical
QALYsEquity
concerns
Roles ofCommittee members

Conceptual challenge: QALYs
The positives of QALYs:
They really do allow us to begin to compare hearing aids to insulin pumps to MS drugs. Now there are a lot of problems with them … but without that it becomes very difficult to do anything meaningful in terms of decision making.
The problem, drawing on the example of MND:
When people with MND are looking forward over that really quite dire prospect, … having a few weeks or a few months of better quality of life … might be valued much more highly than just assigning a QALY weight.
Conceptual challenge: equity
No strong evidence currently on which to base equity weighting:
I think there’s a sort of recognition at the moment, that we have no basis for doing the weighting.
Some implicit weighting is being done:
At the end of each of these discussions people say, ‘well we have no basis for doing this so let’s just treat a QALY as a QALY regardless’. But where that isn’t true, I think, is in relation to children … although people don’t necessarily explicitly state it, I think everybody tends to give it more weight.

And to conclude …
“While we recognise that there are aspects of NICE’s methods that could stand building, on balance we think that UK health economists should sleep more soundly at night for its presence …
Gold & Bryan (2007)
More in … Bryan S, Williams I, McIver S. Seeing the NICE side of cost-
effectiveness analysis: A qualitative investigation of the use of cost-effectiveness analysis in NICE technology appraisals. Health Economics 2007;16(2):179-193
Williams I, Bryan S, McIver S. How should cost-effectiveness analysis be used in health technology coverage decisions? Evidence from the NICE approach. Journal of Health Services Research & Policy 2007;12(2):73-79
Williams I, Bryan S. Cost-effectiveness analysis and formulary decision making in England. Social Science & Medicine 2007;65:2116-2129
Gold M, Bryan S. Some reasons to be cheerful about NICE. Health Economics, Policy and Law 2007;2(2):209-216