back to local coverage determinations (lcds) for palmetto...
TRANSCRIPT

SearchHome Medicare Medicaid CHIP About CMS Regulations & Guidance Research, Statistics, Data & Systems Outreach & Education
People with Medicare & Medicaid Questions Careers Newsroom Contact CMS Acronyms Help Email Print
Back to Local Coverage Determinations (LCDs) for Palmetto GBA (01192, MAC - Part B)
Local Coverage Determination (LCD) for Nervous System Studies - Autonomic Function,Nerve Conduction and Electromyography (L28282)Select the ’Print Record’, ‘Add to Basket’ or ‘Email Record’ buttons to print the record, to add
it to your basket or to email the record.
Section NavigationSelect Section Go
Contractor Information
Contractor NamePalmetto GBA
Contractor Number01192
Contractor TypeMAC - Part B
Back to Top
LCD InformationDocument Information
LCD ID NumberL28282
LCD TitleNervous System Studies - Autonomic Function, Nerve Conduction andElectromyography
Contractor's Determination NumberJ1B-08-0054-L
AMA CPT/ADA CDT Copyright StatementCPT only copyright 2002-2012 American Medical Association. All Rights Reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS/DFARS Apply to Government Use. Fee schedules,relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not
Primary Geographic JurisdictionCalifornia - Southern
Oversight RegionRegion X
Original Determination Effective DateFor services performed on or after 09/02/2008
Original Determination Ending Date
Revision Effective DateFor services performed on or after 05/31/2012
recommending their use. The AMA does not directly or indirectly practice medicine ordispense medical services. The AMA assumes no liability for data contained or not contained herein. The Code on Dental Procedures and Nomenclature (Code) is published in Current Dental Terminology (CDT). Copyright ©American Dental Association. All rights reserved. CDT and CDT-2010 are trademarks of the American Dental Association.
Revision Ending Date
CMS National Coverage PolicyTitle XVIII of the Social Security Act (SSA), §1862(a)(1)(A), states that no Medicarepayment shall be made for items or services that “are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member.”
Title XVIII of the Social Security Act, §1862(a)(7) and 42 Code of Federal Regulations, §411.15, exclude routine physical examinations.
Title XVIII of the Social Security Act, §1833(e), prohibits Medicare payment for any claim lacking the necessary documentation to process the claim.
Code of Federal Regulations 42 CFR §410.32 states that all diagnostic tests must be ordered by a physician who is treating the beneficiary, and test results must be used in the management of the beneficiary’s specific medical problem.
Code of Federal Regulations 42 CFR §410.33 states that all procedures performed in an independent diagnostic testing facility (IDTF) must be ordering by a treating physician who had a relationship with the beneficiary prior to the performance of the testing and who uses the results in the management of the beneficiary’s specific medical problem.
CMS Manual System, Pub 100-02, Medicare Benefits Policy Manual, Chapter 15, §80 explains that diagnostic tests falling under 1861(s)(3), are not under the “incident to” services created by 1861(s)(2). Supervision requirements for diagnostic tests originally appeared in Change Release 850 (CR 850) and are periodically updated in the Physician Fee Schedule Database. By regulation, Nurse Practitioners, Clinical Nurse Specialists, andPhysician Assistants may perform diagnostic tests (pursuant to state law), and are treated as a physician for the ordering of tests, but are not a “physician” for the purpose of technician supervision.
CMS Manual System, Pub 100-08, Medicare Program Integrity Manual, Chapter 3, §3.2.3 Requesting Additional Documentation During Prepayment and Postpayment Review.
CMS Manual System, Pub 100-08, Medicare Program Integrity Manual, Chapter 13,§13.5.1 address when necessary contractors shall describe the circumstances under which a proposed LCD for the service is considered reasonable and necessary.
HCFA (Health Care Financing Administration) Ruling 95-1 explains application of the Limitation of Liability provision (§1879) and use of community standards in determinations regarding medical necessity (see especially §§5 and 6). See also criteria in 42 CFR 411.406 for determining that a provider, practitioner, or other supplier knew that items or services were excluded from coverage as custodial care or as not reasonable andnecessary.
Medicare Modernization Act, §306, Recovery Audit Contractors (RACs). The RAC shall
comply with all National Coverage Determinations (NCDs), Coverage Provisions in Interpretive Manuals, national coverage and coding articles, local coverage determinations (LCDs) and local coverage/coding articles in their jurisdiction.
CMS Manual System, Pub 100-08, Medicare Program Integrity Manual, Chapter 3, §3.4.1.3; Diagnosis Code Requirements.
Indications and Limitations of Coverage and/or Medical NecessityREGULATORY GUIDELINES FOR MEDICARE DIAGNOSTIC TESTS
Tests of the nervous system that are covered in this policy are: Nerve Conduction Studies (NCS), Electromyography (EMG), Autonomic Function Tests (AFT), and Somatosensory Evoked Potentials (SSEP).
Coverage rules in this LCD are those followed by the contractor and by CMS authorized Recovery Audit Contractor(s) in this jurisdiction, during both primary review and appeals.
•
Diagnostic tests are a distinct benefit of Medicare and not an “incident-to” service.Because of this, Medicare has special supervision guidelines for diagnostic tests which may be different than “incident-to” services.
•
Clinical diagnostic tests can only be ordered by the treating physician or by aconsulting physician; ordering physician includes non-physician practitioners such as nurse practitioners and physician assistants.
•
Diagnostic tests are only payable by Medicare when they are necessary and used in the diagnosis or treatment of a specific disease by the treating physician.
•
The ordering physician, with appropriate expertise and training must first clinically assess the patient in person, including completion of a thorough history and physical examination consistent with the nature and complexity of the patient’s presenting complaint. When the ordering physician is a consultant (e.g. the patient has been referred by a family practitioner to a neurologist), the consulting physician should perform a history and physical examination typical of a consulting medical specialist. The ordering physician then decides which of the available diagnostic tests might provide useful diagnostic information. As part of a payment review, documentation of this full patient assessment made prior to testing may be requested of the ordering physician by the contractor.
OVERVIEW OF ELECTRODIAGNOSTIC TESTS
Electrophysiologic tests assess the physiology and/or functional status of the cranial and peripheral nerves, anterior horn cells and spinal nerve roots, the neuromuscular junction, muscles and the autonomic nervous system. Electrodiagnostic studies (EDX) use equipment which electrically stimulates nerves and which also amplifies and displays electrical signals generated by nerves and muscles. These studies include motor and sensory nerve conduction studies, needle electromyography (for muscle cell activity),repetitive nerve stimulation tests, and blink reflex studies, among others. Autonomic nerve studies are designed to locate causes which result in abnormal cardiovascular status, such as drops in blood pressure, increases or decreases in heart rate, as well as hyperhidrosis (excessive perspiration) and changes in skin color/temperature.
Electromyography studiesFor appropriate patients, when testing is medically necessary after a thorough evaluation, electrodiagnostic studies will aid in the specific diagnosis of disease and in selection of treatment:

Identify normal and abnormal functioning of sensory and motor nerves, muscles, and neuromuscular junctions (NMJ).
•
Localize regions of abnormal functioning. •Define the type of abnormal functioning, such as axonal versus demylinating differential diagnosis.
•
Determine the distribution of abnormalities.•Determine the severity of abnormalities.•Localize correct areas for intramuscular administration of agents such as botulinumtoxin.
•
EMG studies may require multiple fine needle insertions in multiple muscles and are often associated with patient discomfort and pain. Individuals performing the test continually refer to a screen where electrical waveforms generated by muscle fibers are displayed, and are simultaneously hearing auditory results of these waves amplified through a speaker. Interpretation of the test will occur simultaneously with its performance and may influence elements of the remainder of the test. Individuals performing the test decide during the test the optimal number of nerves and muscles to be tested to insure an adequate study.
Dynamic testsOnce undertaken, electrodiagnostic examinations are “dynamic” tests. The decision onwhich nerves or muscles are to be tested is dependent on the clinical diagnoses being considered and the findings obtained as the examination is being conducted. As testing is performed, information generated may determine if additional testing of the same or other anatomic regions would also be reasonable and necessary for diagnosis or therapy. Therefore, considerable expertise is required of the technician and physician. 30-50% of patients required electromyographic studies in their evaluation for carpal tunnel surgery(Storm, 2005). Higher accuracy of carpal tunnel diagnostics is found when forearm/wrist conduction is available among the tests used (Jablecki, 2002). EMG such as 95860 must be personally performed by a physician or by a physical therapist certified by the American Board of Physical Therapy Specialties (ABPTS) as a Clinical Electrophysiologic Certified Specialist, per CMS regulations (see below).
PROFESSIONAL PERSONNEL
PhysiciansNo absolute restrictions are placed on the specialty of physicians performing or supervising electrodiagnostic tests (except for an IDTF). Physicians must however have a depth of knowledge competent to perform the tests in a reasonable manner (preferably, but not required, with relevant training in neurology, rehabilitation medicine, orthopedic surgery, etc) and to assess and train personnel working with them. In contrast to neurologic populations, unselected practice patient populations have a low incidence of complex conditions requiring advanced neurodiagnostic tests.
Non-physician PractitionersUnder Medicare, when performing diagnostic testing themselves, within their scope and/or supervision regulations, non-physician practitioners (NPP; physician assistant, nursepractitioners, etc) are considered a “physician.” But, for the purpose of supervising a technician for a diagnostic test, NPPs are not considered a “supervising physician.”
CMS Supervision RequirementsDiagnostic tests are a distinct benefit under 1862(s)(3) of the SSA, as explained in the Benefit Policy Manual, Chapter 15, Section 80. Supervision levels are assigned by CMS (in the annual Physician Fee Schedule database) to each CPT code for clinical diagnostic tests, while the definitions for the numeric supervision levels (such as “7A”) are in the

Benefit Policy Manual, Section 80.
Level 2 & 3CPT code 95921 may be performed under direct (office suite) physician supervision, CPT code 95922, 95923 may be performed under personal (in-room) physician supervision.
Level 6A/66 testsCPT codes 95860-95870, 95872, per CMS, may be performed personally by a physician or by a physical therapist (PT) with special certification by the ABPTS as a Clinical Electrophysiologic Certified Specialist. For all except 95872 (level 66), such a PT may supervise a licensed PT without such certification.
Level 21CPT codes 95925, 95926, 95927 may be performed by a physician, by a technician underpersonal supervision of the physician, or by a certified technician under direct supervision.
Level 7A testsCPT code 95900, 95903, 95904, CMS defines Level 7A tests as performed by a physician, or a physical therapist (PT) with special certification by the ABPTS as a Clinical Electrophysiologic Certified Specialist, or by a physical therapist under direct (office suite)supervision of a physician, or by a nationally certified technician under general (or higher) supervision of a physician. Read closely, the CMS rules for Level 7A fail to describe any additional category of non-credentialed technician under the direct or personal supervision of the physician. However, this seems to be the practice of Medicare contractors and is therefore allowed by this A/B MAC. For the service to be reasonable and necessary, a non-credentialed technician must be trained and competent to perform complex testing andunderstand the test results during the dynamic management of the test. CMS states that covered services must be furnished by qualified personnel and “furnished in accordance with accepted standards of medical practice.
Physical Therapist Global BillingPhysical therapists in private practice may bill for the technical and professional components for testing allowed by the supervision rules above.
Technician does not "order" TestA technician may not perform any services that are not ordered by an ordering physician that is, a treating or consulting physician.
IDTFsFor IDTF services, both the supervising physician and technician must be credentialed. For an IDTF technician, only the registered supervising physician of the IDTF can supervise the IDTF technician. The supervising physician of an IDTF is almost never the ordering physician (e.g., he would have had a previous and ongoing physician management role for the patient).
INDICATIONS FOR NERVE CONDUCTION STUDIES
2006 Policy RevisionsRevisions to this policy reflect 2005/2006 data, that testing for many conditions, including “diabetic neuropathy” and “carpal tunnel syndrome” reached 20X national averages in parts of California despite similar national coverage in terms of CPT and ICD-9-CM codes alone. This drives several responses, which may include Program Safeguard Contractor investigations, contractor Medical Review investigations, contribution to CERT error rates, Recovery Audit Contractor recoupments, provider education articles, and revised LCDs. Additional clarification of Medicare’s medical necessity conditions is provided. In addition, we stress that the interpretation of EDX studies is complex, the range of normal (and

normal aging) is broad, and the tests are sensitive to factors such as temperature. Theclinical conditions where, despite its limitations, EDX testing is medically required are limited, not widespread.
NCS are performed to assess the integrity of, and to diagnose diseases of, the peripheral nervous system. Specifically, they assess the speed (conduction velocity and/or latency), size (amplitude), and shape of the response. Pathological findings include conductionslowing, conduction block, no response, and/or low amplitude response. NCS can be ordered to assess the degree of demyelination and axon loss in the segments of the nerve studied when these are required for differential diagnosis after detailed examination. NCS results should document the nerves evaluated, the distance between the stimulation and recording sites, the conduction velocity, latency values and amplitude. The temperature of the studied limb must be controlled.
Performance of NCS involves the use of electrodes, both stimulating and recording. Motor, sensory and mixed nerve conductions are sometimes required to be done in the same session. For many diagnostic problems where the etiology and diagnosis are uncertain and EDX studies are therefore required, a nerve conduction study often is followed by or proceeded by a needle electrode examination (electromyography).
2008 Policy RevisionsNerve conduction testing limited to use as an adjunct to physical examination for the initial identification of the presence of peripheral neuropathy, accomplished with discriminatory devices that use fixed anatomic templates and computer-generated reports, is covered. The process for utilizing a point of care device is not identical to the process for conductingconventional nerve conduction studies (NCS). Documentation addressing the need to evaluate the patient for peripheral neuropathy must be maintained by the practitioner and made available to Medicare upon request. Documentation should also include the name of the device, such as NC-Stat®. Medicare does not expect this testing to be used routinely on all patients.
Sensory neuropathyCare of diabetic neuropathy in the feet and elsewhere is very important. Routine EDX studies are not required simply by the presence of diabetes. Unlike hemoglobin A1c testing or retinal testing, similar periodic EDX testing is not established in well-recognized national protocols for effective diabetic care. The value of incidental EDX testing or tracking in diabetics, including those with loss of sensation, has not been established to improvehealth outcomes over careful neurologic physical exam testing. EDX testing is appropriate for specific, complex clinical situations where diabetic neuropathy and entrapment or neurologic diagnoses must be further investigated. Examples include investigation of lumbar radiculopathies, carpal entrapment, and diagnostic differentials established by a detailed physical exam and history. While EDX studies have been used in Phase III clinical trials to test drug effectiveness, no current diabetic neuropathy drugs have FDA requirements for EDX monitoring during their use. Medicare’s benefits for routine foot care in diabetics or other neuropathic patients do not require EDX testing before coverage, but are fulfilled by physical exam testing for loss of protective sensation.
Entrapment NeuropathyMedical review data analysis shows the medically unbelievable use of EDX studies in general practice and IDTF-based EDX testing, such that virtually no patients whatever proceeded to carpal tunnel therapy or surgery except for a minute subset who had subsequent double-testing by a neurologic or orthopedic surgeon before therapeutic care.This is not a critique of any individual non-specialist, but a population study of actual claims. EDX testing for carpal tunnel syndrome has been the subject of numerous clinical guidelines and must follow a complete physical exam, history, and clinical treatment plan which can include minimal intervention or rest as a clinically reasonable therapeutic stage before costly EDX testing. (D’Arcy, 2000; Jablecki, 2002; AANEM, 2002). According to the

NIH (2006), “Initial treatment generally involves resting the affected hand and wrist for at least 2 weeks, avoiding activities that may worsen symptoms, and immobilizing the wrist in a splint to avoid further damage from twisting or bending. If there is inflammation, applying cool packs can help reduce swelling. “ There is no suggestion whatever that early treatment has been established to hinge on costly and elaborate EDX testing. Further, “although 30 percent of frequent computer users complain of hand paresthesias, only 10 percent meet clinical criteria for carpal tunnel syndrome, and nerve conduction studies are abnormal in only 3.5 percent of these persons” (emphasis added, Viera, 2003). Accordingto the University of Maryland, “Many people have abnormal electrodiagnostic test results but have no classic symptoms or even no symptoms at all. Furthermore, about 15% of the population has symptoms consistent with CTS, but most do not show test results indicating the disorder. (UMM, 2002) “ Katz (2006) also found a high incidence of non-clinical “abnormalities” in “stat” EDX testing of unselected populations. Therefore, a low threshold for initiation of EDX studies will simply result in tests which are not reasonable and necessary and not payable by Medicare. One outline of appropriate diagnostics includes the following (NIH, 2006; see also Jablecki, 2002:
A physical examination of the hands, arms, shoulders, and neck can help determine if the patient's complaints are related to daily activities or to an underlying disorder, and can rule out other painful conditions that mimic carpal tunnel syndrome. Thewrist is examined for tenderness, swelling, warmth, and discoloration. Each finger should be tested for sensation, and the muscles at the base of the hand should be examined for strength and signs of atrophy. Routine laboratory tests and X-rays can reveal diabetes, arthritis, and fractures.
Physicians can use specific tests to try to produce the symptoms of carpal tunnelsyndrome. In the Tinel test, the doctor taps on or presses on the median nerve in the patient's wrist. The test is positive when tingling in the fingers or a resultant shock-like sensation occurs. The Phalen, or wrist-flexion, test involves having the patient hold his or her forearms upright by pointing the fingers down and pressing the backs of the hands together. The presence of carpal tunnel syndrome is suggested if one or more symptoms, such as tingling or increasing numbness, is felt in the fingers within 1 minute. Doctors may also ask patients to try to make a movement that brings on symptoms.
Vague DiagnosisTests for vague conditions like “skin sensation disturbance” should also be undertaken only after a detailed history and physical and careful development of a credible and professional differential diagnosis, from which EDX testing follows as a medically necessary differential test.
Evident DiagnosisIn some cases, the etiology (e.g. known drug effect or herpetic neuralgia) and symptoms of a condition are so clearly a sensory neuropathy that additional testing is not clinicallynecessary.
Repeat TestingRepeat testing is not usually required. Asymptomatic patients do not require testing and symptomatic patients with established diagnoses ordinarily will be followed clinically rather than repetitive (monthly, quarterly, etc) EDX testing.
Equipment for Nerve Conduction Studies and EMG
General professional standards apply for all equipment, which must be FDA approved.
FDA clearance generally does not require testing of utility in any specific clinical scenarios in the Medicare population. (For example, an MRI scanner is approved to image the body, not for specific medically necessary clinical situations or at any specific repeat intervals; these are determined by Medicare). This LCD does not proscribe individual FDA-cleared EDX testing devices by brand name. However, this LCD follows the same general principles used by other Medicare contractors.
Psychophysical measurements (current, vibration, and thermal perceptions) even though they may involve delivery of a stimulus, are not covered as separately payable from a general examination. Psychophysical sensory threshold testing is not covered by a NCD (160.23).
Indications for Electromyography
The EMG portion of electrodiagnostic testing is always performed by a physician or a physical therapist with special training and certification to perform these tests. Needle EMG refers to the recording and study of electrical activity of a muscle. The EMG examination usually follows the NCS examination, but may precede it, depending on the circumstances. It involves the use of a very thin needle electrode placed into the muscle tomeasure the muscle’s electrical characteristics at rest and during activity. This procedure is often painful for the patient. The EMG interpretation includes analysis of oscilloscope tracings and the characteristic sounds produced by electrical potentials. The final interpretation of the study is a synthesis by the electrodiagnostic physician of the patient’s history, physical exam, and all components of the electrodiagnostic studies. EMG and NCS examinations usually provide complementary findings.
Medical necessary number of testsPlease see the table contained in the Utilization Guidelines section of this policy that contains the maximum numbers of tests usually needed to reach a diagnosis. This table is excerpted from the “Recommended Policy for Electrodiagnostic Medicine” from the American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM). Although not quoted in full in this LCD, this policy of the AANEM represents a majorrecognized guideline for clinical practice. The Association’s guidelines are a major source of information for reasonable and necessary decisions made by contractors regarding CMS’s very explicit usage of association guidelines for the medical necessity decisions. The web site for AANEM is at www.aanem.org.
An example from this policy would be the recommendation that to diagnose Carpel Tunnel Disease, unilateral, no more than 3 motor NCS tests should be necessary to reach a diagnosis. In some cases, fewer numbers of tests than shown in the table are adequate to reach a diagnosis.
The AANEM guidelines reflect tests per patient per diagnosis; see Utilization Guidelines. See also clinical guidelines of the American Academy of Neurology (Jablecki et al., 2002).
Indications for Autonomic Function Tests
Autonomic Nervous System Testing (ANS) measures alterations in the R-R interval of the electrocardiogram (ECG) in response to parasympathetic and sympathetic system stimulation. Autonomic disorders may be congenital or acquired – primary or secondary. Most are diagnosed clinically, with laboratory and formal diagnostic testing playing an adjunctive or confirmatory role. Testing may also be appropriate to monitor disease progression when there is a change in clinical status, or to evaluate a patient’s response to specific treatment for an autonomic disorder.

The aim of such testing is to correlate signs and symptoms of possible autonomic dysfunction with objective measurement in a way that is clinically useful. Appropriate application and interpretation of these tests requires significant knowledge, training andexpertise such as that generally found at dedicated neurodiagnostic laboratories and academic facilities. For example, proper interpretation requires that test results be compared with findings in age matched control subjects, and that individual laboratories develop their own reference values based on the particular testing protocols employed and patient populations being tested. Equipment to noninvasively measure cardiorespiratory and circulatory parameters and to measure sweat production is commercially available. Proper testing is time consuming, averaging 1 hour per patient. Adequate baseline acclimatization and proper positioning of subjects are crucial. Efforts should be made to keep the patients as comfortable as possible to limit pain-induced artifacts.
Drugs can have substantial effects on the results of ANS testing and are a common cause of falsely abnormal results. Patients should refrain from caffeine, nicotine, and alcohol at least 3 hours prior to testing. All medications with adrenergic and anticholinergic properties need to be discontinued at least 48 hours prior to the study. These would include but arenot necessarily limited to the following: chlorpromazine, thioridazine, the tricyclic and tetracyclic antidepressants, bupropion, mirtazapine, venlafaxine, clonidine, alpha-blockers, beta-blockers, calcium channel blockers, opiates, topical capsaicin and diphenhydramine (diphenhydramine is commonly found in over the counter products for sleep and for cold symptoms).
CPT code 95921 includes heart rate response to deep breathing with recorded R-R interval, Valsalva ratio and 30:15 ratio. To determine the heart rate response to deepbreathing the patient is supine with the head elevated to 30 degrees. The patient breathes deeply at six respirations per minute, allowing 5 seconds for each inspiration and expiration. The minimal and maximal heart rates within each respiratory cycle and the mean variation are determined. The E to I ratio or index is calculated as the sum of the six longest R-R intervals of each of the six respirations divided by the sum of the six shortest R-R intervals. Other standardized calculation methods are also available. To determine the Valsalva ratio the patient begins supine with head slightly elevated. The patient thenstrains against 40mmHg for 15 seconds by blowing into a mouthpiece attached to asphygmomanometer. Following cessation of the Valsalva strain, the patient relaxes and breathes at a normal rate. The ECG is monitored during the strain and at 30-45 seconds afterwards. Maximum and minimum heart rates are obtained respectively at about 1 second after cessation of strain, and then 15-20 seconds later. This is repeated three times, and the largest simple heart rate ratio is considered the best reflection of autonomic function. The Valsalva ratio is the longest to the shortest R-R interval at 15-20 seconds after and at 1 second after Valsalva respectively. To determine the 30:15 ratio the patient lies supine for 20 minutes, and then rises to the standing position. The 30:15 ratio is the ratio of the R-R interval at 30 seconds (longest interval) to that at 15 seconds (shortest interval) upon standing. This ratio is an index of the integrity of parasympathetic cholinergic (cardiovagal) function.
CPT 95922 code includes measurement of beat-to-beat blood pressure and R-R intervalchanges during Valsalva maneuver and at least 5 minutes of passive tilt. This testing involves continuous heart rate recording and requires photoplethysmographic beat-to-beat blood pressure recording. Analysis of heart rate and blood pressure responses reflects the integrity of vasomotor adrenergic innervation.
These tests are payable as reasonable and necessary to evaluate symptoms of vasomotor instability such as hypotension, orthostatic tachycardia and hyperhidrosis, generally after more common causes have been excluded by other testing. Autonomic function testing will be reimbursed as reasonable and necessary only when used for one or more of the following indications and when directed at establishing a more accurate or definitivediagnosis or contributing to clinically relevant medical decision-making:
1. To diagnose the presence of autonomic neuropathy in a patient with signs or symptoms suggesting a progressive autonomic neuropathy.2. To evaluate the severity and distribution of a diagnosed progressive autonomicneuropathy.3. To differentiate the diagnosis between certain complicated variants of syncopes from other causes of loss of consciousness.4. To evaluate inadequate response to beta-blockade in vasodepressor syncope.5. To evaluate distressing symptoms in the patient with a clinical picture suspicious for distal small fiber neuropathy in order to diagnose the condition.6. To differentiate the cause of postural tachycardia syndrome.7. To evaluate change in type, distribution or severity of autonomic deficits in patients with autonomic failure.8. To evaluate the response to treatment in patients with autonomic failure who demonstrate a change in clinical exam.9. To diagnose axonal neuropathy or suspected autonomic neuropathy in the symptomatic patient.10. To evaluate and treat patients with recurrent unexplained syncope to demonstrate autonomic failure, generally after more common causes have been excluded by other standard testing.
Equipment for Autonomic Nervous System Studies
General professional standards apply for all equipment. Unknown algorithms untested on the Medicare population in systematic trials do not constitute the professional component of diagnostic testing. Equipment with FDA clearance for heart rate variability measurements in response to paced respirations and exercises that tests only heart rate variability does not meet the full range of testing parameters required for the performance of 95921 and 95922, and does not ensure full test requirements, such as blood pressuremonitoring and blood oxygen levels; nor do they incorporate proper testing conditions, such as the use of a tilt table. Providers may be asked to supply information on the equipment used to perform autonomic nervous system studies, to ensure that all studies performed meet the requirements of the procedure.
Somatosensory Evoked Potentials (SSEP)
Somatosensory evoked potentials have been defined by Levatt (2006) as follows:
Evoked potentials are the electrical signals generated by the nervous system inresponse to sensory stimuli. Auditory, visual, and somatosensory stimuli are used commonly for clinical evoked potential studies. Somatosensory evoked potentials (SSEPs) consist of a series of waves that reflect sequential activation of neural structures along the somatosensory pathways. While SSEPs can be elicited by mechanical stimulation, clinical studies utilize electrical stimulation of peripheral nerves, which gives larger and more robust responses. The stimulation sites typically used for clinical diagnostic SSEP studies are the median nerve at the wrist, the common peroneal nerve at the knee, and/or the posterior tibial nerve at the ankle. Recording electrodes are placed over the scalp, the spine, and peripheral nerves proximal to the stimulation site.
As clearly described by Burneo (2006) and others, in many circumstances standard NCS or EMG studies are preferable to SSEP for peripheral nervous system disorders. SSEP are indicated only under special circumstances. SSEPs may be useful in some spinal cord trauma conditions including surgical monitoring. SSEP may assist in cortical mapping

during neurologic surgery. MRI has largely supplanted SSEP testing in conditions such as multiple sclerosis. SSEPs are not generally useful in most neurodegenerative disorders although on occasional special clinical circumstances and differential diagnoses may occur. In all cases, a clear clinical use or differential diagnosis must be present and findings must be interpreted carefully.
Limitations
For clarity of text, most limitations are also included in the appropriate part of the Indications section.
Nervous system studies must be ordered by a treating physician and must be both reasonable and necessary for the management of the patient. Test results must be required for and used in the management of the patient.
Nervous system studies should not be performed when a neurological diagnosis can be made clinically and when localization, distribution, and progression of the disease will not aid in the selection or duration of treatment options (such as diabetic distal symmetric sensory polyneuropathy). This does not exclude clinical situations where electrodiagnostic study is a key to rule in/rule out a secondary condition (e.g. entrapment neuropathy) or is a necessary factor in allowing the treating physician to counsel the patient.
The number of nerves to be tested should be the minimum number necessary to address the clinical issue without unnecessary testing. In almost all studies, this will appropriately include evaluation of 1 or more nerves that have normal test results.
In nerve conduction studies, each nerve tested is billed as an individual unit. It isinappropriate to “inch” up or down a nerve and bill for more than one unit.
For ANS tests, syndromes of autonomic dysfunction for which autonomic testing might add valuable clinical information are relatively rare. Generally, only after excluding more common causes of “autonomic” signs or symptoms (e.g., hypotension, hyperhidrosis, orthostatic tachycardia), including incorrect/inappropriate medication dosing, may formal autonomic testing be indicated to exclude or confirm rarer autonomic disorders. The use of these tests to screen patients without signs or symptoms of autonomic dysfunction, including patients with diabetes, hepatic or renal disease, is not covered. Testing for the sole purpose of monitoring disease intensity or treatment efficacy in diabetes, hepatic or renal disease is not considered reasonable and necessary.
For all diagnoses listed in the ICD-9-CM section of this LCD, the usage of an ICD-9-CM diagnosis alone does not guarantee that the services rendered are clinically necessary. The ICD-9-CM diagnoses section list conditions that may be payable assuming all other conditions of this LCD are met and assuming that the evaluation, testing, and follow-up management are consistent with good community practice.
Back to Top
Coding Information
Bill Type Codes:
Contractors may specify Bill Types to help providers identify those Bill Types typically used to report this service. Absence of a Bill Type does not guarantee that the policy does not apply to that Bill Type. Complete absence of all Bill Types indicates that

coverage is not influenced by Bill Type and the policy should be assumed to apply equally to all claims.
999x Not Applicable
Revenue Codes:
Contractors may specify Revenue Codes to help providers identify those Revenue Codes typically used to report this service. In most instances Revenue Codes are purely advisory; unless specified in the policy services reported under other Revenue Codes are equally subject to this coverage determination. Complete absence of all Revenue Codes indicates that coverage is not influenced by Revenue Code and the policy should be assumed to apply equally to all Revenue Codes.
99999 Not Applicable
CPT/HCPCS Codes
Nerve Conduction Studies (NCS)* The process for utilizing point of care devices like NC-Stat® is not identical to the processconducting conventional nerve conduction studies (NCS),therefore, CPT code 95905 shouldfor these type services.
95900 NERVE CONDUCTION, AMPLITUDE AND LATENCY/VELOCITY STUDY, EACH NERVE; MOTOR, WITHOUT F-WAVE STUDY
95903 NERVE CONDUCTION, AMPLITUDE AND LATENCY/VELOCITY STUDY, EACH NERVE; MOTOR, WITH F-WAVE STUDY
95904 NERVE CONDUCTION, AMPLITUDE AND LATENCY/VELOCITY STUDY, EACH NERVE; SENSORY
95934 H-REFLEX, AMPLITUDE AND LATENCY STUDY; RECORD GASTROCNEMIUS/SOLEUS MUSCLE
95936 H-REFLEX, AMPLITUDE AND LATENCY STUDY; RECORD MUSCLE OTHER THAN GASTROCNEMIUS/SOLEUS MUSCLE
95937 NEUROMUSCULAR JUNCTION TESTING (REPETITIVE STIMULATION, PAIRED STIMULI), EACH NERVE, ANY 1 METHOD
95999 UNLISTED NEUROLOGICAL OR NEUROMUSCULAR DIAGNOSTIC PROCEDURE
Electromyography (EMG)
95860 NEEDLE ELECTROMYOGRAPHY; 1 EXTREMITY WITH OR WITHOUT RELATED PARASPINAL AREAS
95861 NEEDLE ELECTROMYOGRAPHY; 2 EXTREMITIES WITH OR WITHOUT RELATED PARASPINAL AREAS
95863 NEEDLE ELECTROMYOGRAPHY; 3 EXTREMITIES WITH OR WITHOUT RELATED PARASPINAL AREAS
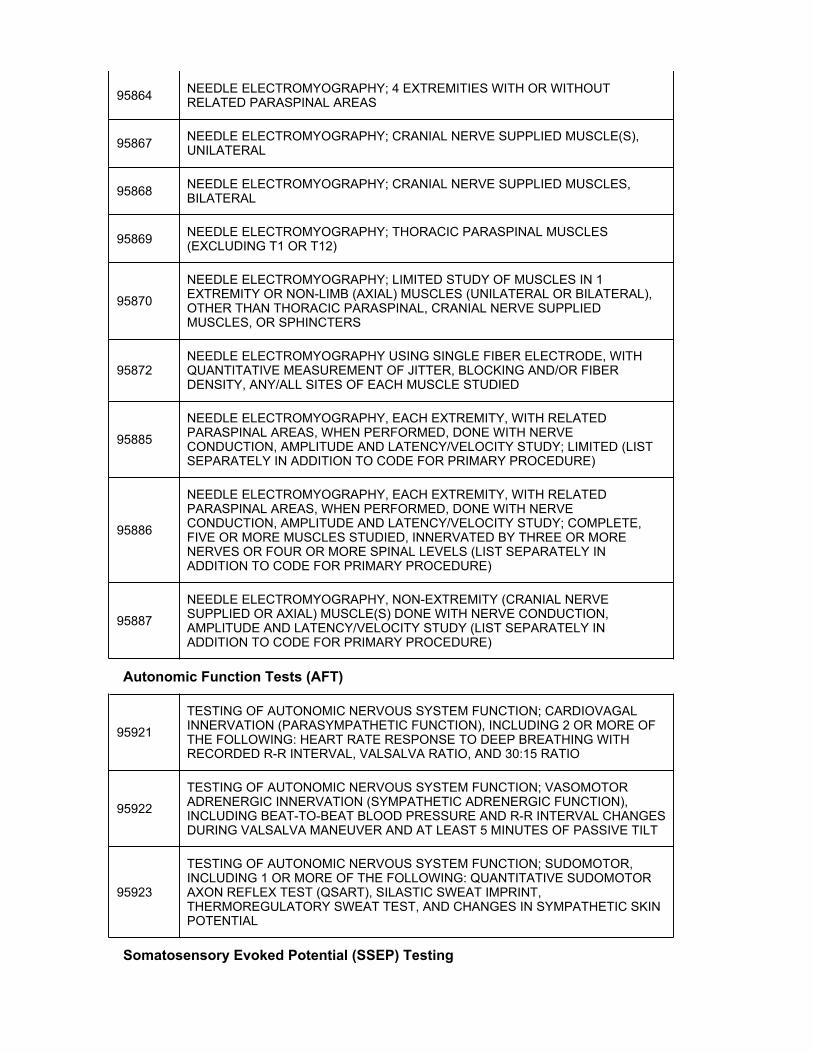
95864 NEEDLE ELECTROMYOGRAPHY; 4 EXTREMITIES WITH OR WITHOUT RELATED PARASPINAL AREAS
95867 NEEDLE ELECTROMYOGRAPHY; CRANIAL NERVE SUPPLIED MUSCLE(S), UNILATERAL
95868 NEEDLE ELECTROMYOGRAPHY; CRANIAL NERVE SUPPLIED MUSCLES, BILATERAL
95869 NEEDLE ELECTROMYOGRAPHY; THORACIC PARASPINAL MUSCLES (EXCLUDING T1 OR T12)
95870
NEEDLE ELECTROMYOGRAPHY; LIMITED STUDY OF MUSCLES IN 1 EXTREMITY OR NON-LIMB (AXIAL) MUSCLES (UNILATERAL OR BILATERAL), OTHER THAN THORACIC PARASPINAL, CRANIAL NERVE SUPPLIEDMUSCLES, OR SPHINCTERS
95872NEEDLE ELECTROMYOGRAPHY USING SINGLE FIBER ELECTRODE, WITH QUANTITATIVE MEASUREMENT OF JITTER, BLOCKING AND/OR FIBERDENSITY, ANY/ALL SITES OF EACH MUSCLE STUDIED
95885
NEEDLE ELECTROMYOGRAPHY, EACH EXTREMITY, WITH RELATED PARASPINAL AREAS, WHEN PERFORMED, DONE WITH NERVE CONDUCTION, AMPLITUDE AND LATENCY/VELOCITY STUDY; LIMITED (LIST SEPARATELY IN ADDITION TO CODE FOR PRIMARY PROCEDURE)
95886
NEEDLE ELECTROMYOGRAPHY, EACH EXTREMITY, WITH RELATED PARASPINAL AREAS, WHEN PERFORMED, DONE WITH NERVE CONDUCTION, AMPLITUDE AND LATENCY/VELOCITY STUDY; COMPLETE, FIVE OR MORE MUSCLES STUDIED, INNERVATED BY THREE OR MORE NERVES OR FOUR OR MORE SPINAL LEVELS (LIST SEPARATELY IN ADDITION TO CODE FOR PRIMARY PROCEDURE)
95887
NEEDLE ELECTROMYOGRAPHY, NON-EXTREMITY (CRANIAL NERVE SUPPLIED OR AXIAL) MUSCLE(S) DONE WITH NERVE CONDUCTION, AMPLITUDE AND LATENCY/VELOCITY STUDY (LIST SEPARATELY IN ADDITION TO CODE FOR PRIMARY PROCEDURE)
Autonomic Function Tests (AFT)
95921
TESTING OF AUTONOMIC NERVOUS SYSTEM FUNCTION; CARDIOVAGAL INNERVATION (PARASYMPATHETIC FUNCTION), INCLUDING 2 OR MORE OFTHE FOLLOWING: HEART RATE RESPONSE TO DEEP BREATHING WITH RECORDED R-R INTERVAL, VALSALVA RATIO, AND 30:15 RATIO
95922
TESTING OF AUTONOMIC NERVOUS SYSTEM FUNCTION; VASOMOTOR ADRENERGIC INNERVATION (SYMPATHETIC ADRENERGIC FUNCTION),INCLUDING BEAT-TO-BEAT BLOOD PRESSURE AND R-R INTERVAL CHANGES DURING VALSALVA MANEUVER AND AT LEAST 5 MINUTES OF PASSIVE TILT
95923
TESTING OF AUTONOMIC NERVOUS SYSTEM FUNCTION; SUDOMOTOR, INCLUDING 1 OR MORE OF THE FOLLOWING: QUANTITATIVE SUDOMOTOR AXON REFLEX TEST (QSART), SILASTIC SWEAT IMPRINT, THERMOREGULATORY SWEAT TEST, AND CHANGES IN SYMPATHETIC SKINPOTENTIAL
Somatosensory Evoked Potential (SSEP) Testing

95925SHORT-LATENCY SOMATOSENSORY EVOKED POTENTIAL STUDY, STIMULATION OF ANY/ALL PERIPHERAL NERVES OR SKIN SITES, RECORDING FROM THE CENTRAL NERVOUS SYSTEM; IN UPPER LIMBS
95926SHORT-LATENCY SOMATOSENSORY EVOKED POTENTIAL STUDY, STIMULATION OF ANY/ALL PERIPHERAL NERVES OR SKIN SITES, RECORDING FROM THE CENTRAL NERVOUS SYSTEM; IN LOWER LIMBS
95927
SHORT-LATENCY SOMATOSENSORY EVOKED POTENTIAL STUDY, STIMULATION OF ANY/ALL PERIPHERAL NERVES OR SKIN SITES, RECORDING FROM THE CENTRAL NERVOUS SYSTEM; IN THE TRUNK OR HEAD
95938
SHORT-LATENCY SOMATOSENSORY EVOKED POTENTIAL STUDY, STIMULATION OF ANY/ALL PERIPHERAL NERVES OR SKIN SITES, RECORDING FROM THE CENTRAL NERVOUS SYSTEM; IN UPPER AND LOWER LIMBS
95939 CENTRAL MOTOR EVOKED POTENTIAL STUDY (TRANSCRANIAL MOTOR STIMULATION); IN UPPER AND LOWER LIMBS
ICD-9 Codes that Support Medical Necessity
Usage of an ICD-9-CM diagnosis alone does not guarantee that the services rendered are clinically necessary. The ICD-9-CM diagnoses section list conditions that may bepayable assuming all other conditions of this LCD are met and assuming that theevaluation, testing, and follow-up management are consistent with good communitypractice.
CPT Codes applicable for these ICD-9 codes 95900, 95903, 95904, 95934, 95936, 95937, 95999, 95860 95861, 95863, 95864,95867, 95868, 95869, 95870, 95872, 95885, 95886, 95887, 95921, 95922, 95923.
005.1 BOTULISM FOOD POISONING
037 TETANUS
053.13 POSTHERPETIC POLYNEUROPATHY
138 LATE EFFECTS OF ACUTE POLIOMYELITIS
192.0 MALIGNANT NEOPLASM OF CRANIAL NERVES
192.2 MALIGNANT NEOPLASM OF SPINAL CORD
192.3 MALIGNANT NEOPLASM OF SPINAL MENINGES
192.8 MALIGNANT NEOPLASM OF OTHER SPECIFIED SITES OF NERVOUS SYSTEM
198.3 SECONDARY MALIGNANT NEOPLASM OF BRAIN AND SPINAL CORD
198.4 SECONDARY MALIGNANT NEOPLASM OF OTHER PARTS OF NERVOUS SYSTEM

225.1 BENIGN NEOPLASM OF CRANIAL NERVES
225.3 BENIGN NEOPLASM OF SPINAL CORD
225.4 BENIGN NEOPLASM OF SPINAL MENINGES
225.8 BENIGN NEOPLASM OF OTHER SPECIFIED SITES OF NERVOUS SYSTEM
237.70 NEUROFIBROMATOSIS UNSPECIFIED
237.71 NEUROFIBROMATOSIS TYPE 1 VON RECKLINGHAUSEN'S DISEASE
237.72 NEUROFIBROMATOSIS TYPE 2 ACOUSTIC NEUROFIBROMATOSIS
237.73 SCHWANNOMATOSIS
237.79 OTHER NEUROFIBROMATOSIS
249.60SECONDARY DIABETES MELLITUS WITH NEUROLOGICAL MANIFESTATIONS, NOT STATED AS UNCONTROLLED, ORUNSPECIFIED
249.61 SECONDARY DIABETES MELLITUS WITH NEUROLOGICAL MANIFESTATIONS, UNCONTROLLED
250.60 - 250.63
DIABETES WITH NEUROLOGICAL MANIFESTATIONS, TYPE II OR UNSPECIFIED TYPE, NOT STATED AS UNCONTROLLED - DIABETES WITH NEUROLOGICAL MANIFESTATIONS, TYPE I [JUVENILE TYPE],UNCONTROLLED
255.2 ADRENOGENITAL DISORDERS
265.1 OTHER AND UNSPECIFIED MANIFESTATIONS OF THIAMINE DEFICIENCY
269.1 DEFICIENCY OF OTHER VITAMINS
272.5 LIPOPROTEIN DEFICIENCIES
331.6 CORTICOBASAL DEGENERATION
333.0 OTHER DEGENERATIVE DISEASES OF THE BASAL GANGLIA
333.2 MYOCLONUS
333.6 GENETIC TORSION DYSTONIA
333.71 ATHETOID CEREBRAL PALSY
333.81 BLEPHAROSPASM
333.82 - 333.84 OROFACIAL DYSKINESIA - ORGANIC WRITERS' CRAMP

333.89 OTHER FRAGMENTS OF TORSION DYSTONIA
334.0 - 334.4 FRIEDREICH'S ATAXIA - CEREBELLAR ATAXIA IN DISEASES CLASSIFIED ELSEWHERE
334.8 OTHER SPINOCEREBELLAR DISEASES
334.9 SPINOCEREBELLAR DISEASE UNSPECIFIED
335.0 WERDNIG-HOFFMANN DISEASE
335.10 SPINAL MUSCULAR ATROPHY UNSPECIFIED
335.11 KUGELBERG-WELANDER DISEASE
335.19 - 335.24 OTHER SPINAL MUSCULAR ATROPHY - PRIMARY LATERAL SCLEROSIS
335.29 OTHER MOTOR NEURON DISEASES
335.8 OTHER ANTERIOR HORN CELL DISEASES
335.9 ANTERIOR HORN CELL DISEASE UNSPECIFIED
336.0 - 336.3 SYRINGOMYELIA AND SYRINGOBULBIA - MYELOPATHY IN OTHER DISEASES CLASSIFIED ELSEWHERE
336.8 OTHER MYELOPATHY
336.9 UNSPECIFIED DISEASE OF SPINAL CORD
337.00 IDIOPATHIC PERIPHERAL AUTONOMIC NEUROPATHY, UNSPECIFIED
337.09 OTHER IDIOPATHIC PERIPHERAL AUTONOMIC NEUROPATHY
337.1 PERIPHERAL AUTONOMIC NEUROPATHY IN DISORDERS CLASSIFIED ELSEWHERE
337.20 - 337.22 REFLEX SYMPATHETIC DYSTROPHY UNSPECIFIED - REFLEX SYMPATHETIC DYSTROPHY OF THE LOWER LIMB
337.29 REFLEX SYMPATHETIC DYSTROPHY OF OTHER SPECIFIED SITE
337.3 AUTONOMIC DYSREFLEXIA
337.9 UNSPECIFIED DISORDER OF AUTONOMIC NERVOUS SYSTEM
340 MULTIPLE SCLEROSIS
341.0 NEUROMYELITIS OPTICA
341.1 SCHILDER'S DISEASE
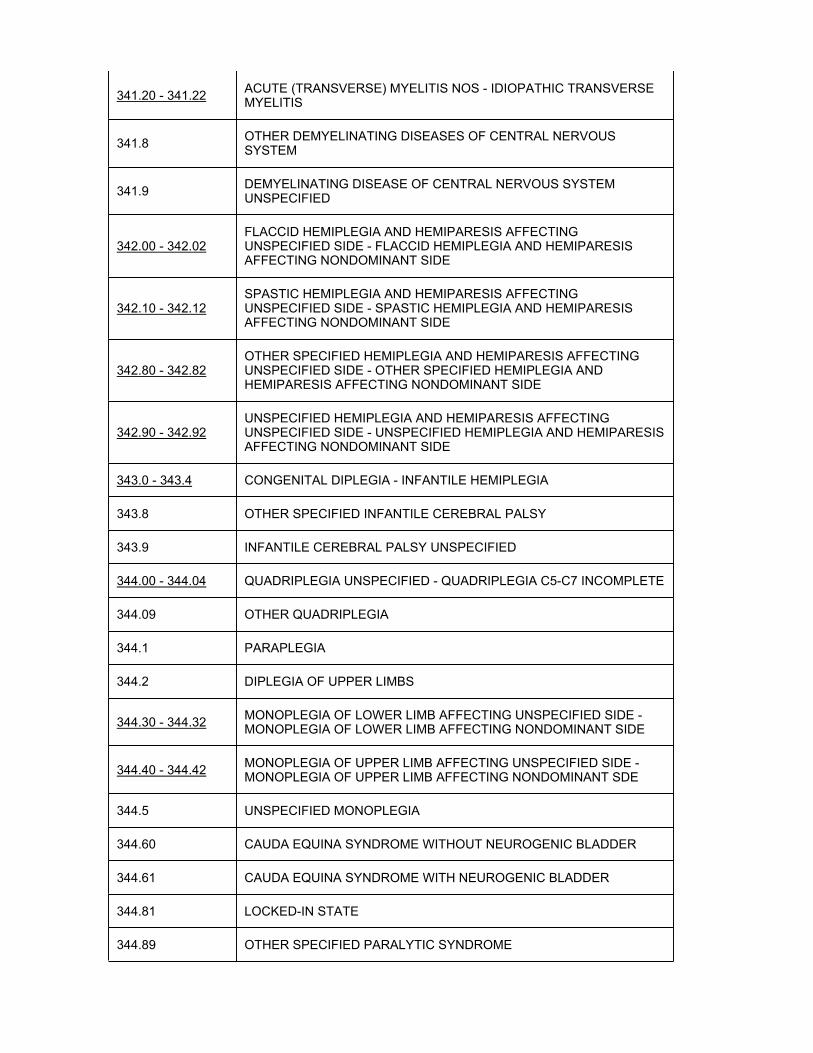
341.20 - 341.22 ACUTE (TRANSVERSE) MYELITIS NOS - IDIOPATHIC TRANSVERSE MYELITIS
341.8 OTHER DEMYELINATING DISEASES OF CENTRAL NERVOUS SYSTEM
341.9 DEMYELINATING DISEASE OF CENTRAL NERVOUS SYSTEM UNSPECIFIED
342.00 - 342.02FLACCID HEMIPLEGIA AND HEMIPARESIS AFFECTING UNSPECIFIED SIDE - FLACCID HEMIPLEGIA AND HEMIPARESIS AFFECTING NONDOMINANT SIDE
342.10 - 342.12SPASTIC HEMIPLEGIA AND HEMIPARESIS AFFECTING UNSPECIFIED SIDE - SPASTIC HEMIPLEGIA AND HEMIPARESIS AFFECTING NONDOMINANT SIDE
342.80 - 342.82OTHER SPECIFIED HEMIPLEGIA AND HEMIPARESIS AFFECTING UNSPECIFIED SIDE - OTHER SPECIFIED HEMIPLEGIA ANDHEMIPARESIS AFFECTING NONDOMINANT SIDE
342.90 - 342.92UNSPECIFIED HEMIPLEGIA AND HEMIPARESIS AFFECTING UNSPECIFIED SIDE - UNSPECIFIED HEMIPLEGIA AND HEMIPARESIS AFFECTING NONDOMINANT SIDE
343.0 - 343.4 CONGENITAL DIPLEGIA - INFANTILE HEMIPLEGIA
343.8 OTHER SPECIFIED INFANTILE CEREBRAL PALSY
343.9 INFANTILE CEREBRAL PALSY UNSPECIFIED
344.00 - 344.04 QUADRIPLEGIA UNSPECIFIED - QUADRIPLEGIA C5-C7 INCOMPLETE
344.09 OTHER QUADRIPLEGIA
344.1 PARAPLEGIA
344.2 DIPLEGIA OF UPPER LIMBS
344.30 - 344.32 MONOPLEGIA OF LOWER LIMB AFFECTING UNSPECIFIED SIDE -MONOPLEGIA OF LOWER LIMB AFFECTING NONDOMINANT SIDE
344.40 - 344.42 MONOPLEGIA OF UPPER LIMB AFFECTING UNSPECIFIED SIDE -MONOPLEGIA OF UPPER LIMB AFFECTING NONDOMINANT SDE
344.5 UNSPECIFIED MONOPLEGIA
344.60 CAUDA EQUINA SYNDROME WITHOUT NEUROGENIC BLADDER
344.61 CAUDA EQUINA SYNDROME WITH NEUROGENIC BLADDER
344.81 LOCKED-IN STATE
344.89 OTHER SPECIFIED PARALYTIC SYNDROME
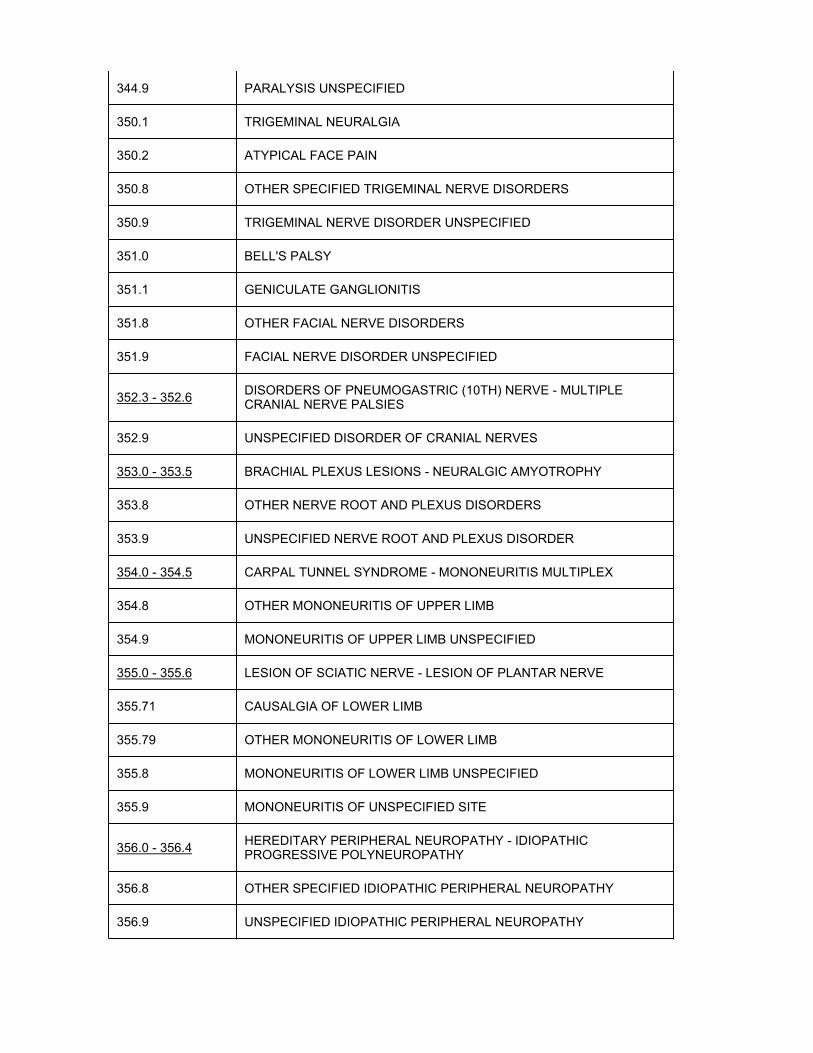
344.9 PARALYSIS UNSPECIFIED
350.1 TRIGEMINAL NEURALGIA
350.2 ATYPICAL FACE PAIN
350.8 OTHER SPECIFIED TRIGEMINAL NERVE DISORDERS
350.9 TRIGEMINAL NERVE DISORDER UNSPECIFIED
351.0 BELL'S PALSY
351.1 GENICULATE GANGLIONITIS
351.8 OTHER FACIAL NERVE DISORDERS
351.9 FACIAL NERVE DISORDER UNSPECIFIED
352.3 - 352.6 DISORDERS OF PNEUMOGASTRIC (10TH) NERVE - MULTIPLE CRANIAL NERVE PALSIES
352.9 UNSPECIFIED DISORDER OF CRANIAL NERVES
353.0 - 353.5 BRACHIAL PLEXUS LESIONS - NEURALGIC AMYOTROPHY
353.8 OTHER NERVE ROOT AND PLEXUS DISORDERS
353.9 UNSPECIFIED NERVE ROOT AND PLEXUS DISORDER
354.0 - 354.5 CARPAL TUNNEL SYNDROME - MONONEURITIS MULTIPLEX
354.8 OTHER MONONEURITIS OF UPPER LIMB
354.9 MONONEURITIS OF UPPER LIMB UNSPECIFIED
355.0 - 355.6 LESION OF SCIATIC NERVE - LESION OF PLANTAR NERVE
355.71 CAUSALGIA OF LOWER LIMB
355.79 OTHER MONONEURITIS OF LOWER LIMB
355.8 MONONEURITIS OF LOWER LIMB UNSPECIFIED
355.9 MONONEURITIS OF UNSPECIFIED SITE
356.0 - 356.4 HEREDITARY PERIPHERAL NEUROPATHY - IDIOPATHIC PROGRESSIVE POLYNEUROPATHY
356.8 OTHER SPECIFIED IDIOPATHIC PERIPHERAL NEUROPATHY
356.9 UNSPECIFIED IDIOPATHIC PERIPHERAL NEUROPATHY

357.0 - 357.7 ACUTE INFECTIVE POLYNEURITIS - POLYNEUROPATHY DUE TO OTHER TOXIC AGENTS
357.81 CHRONIC INFLAMMATORY DEMYELINATING POLYNEURITIS
357.82 CRITICAL ILLNESS POLYNEUROPATHY
357.89 OTHER INFLAMMATORY AND TOXIC NEUROPATHY
357.9 UNSPECIFIED INFLAMMATORY AND TOXIC NEUROPATHIES
358.00 MYASTHENIA GRAVIS WITHOUT (ACUTE) EXACERBATION
358.01 MYASTHENIA GRAVIS WITH (ACUTE) EXACERBATION
358.1 MYASTHENIC SYNDROMES IN DISEASES CLASSIFIED ELSEWHERE
358.2 TOXIC MYONEURAL DISORDERS
358.30 LAMBERT-EATON SYNDROME, UNSPECIFIED
358.31 LAMBERT-EATON SYNDROME IN NEOPLASTIC DISEASE
358.39 LAMBERT-EATON SYNDROME IN OTHER DISEASES CLASSIFIED ELSEWHERE
358.8 OTHER SPECIFIED MYONEURAL DISORDERS
358.9 MYONEURAL DISORDERS UNSPECIFIED
359.0 CONGENITAL HEREDITARY MUSCULAR DYSTROPHY
359.1 HEREDITARY PROGRESSIVE MUSCULAR DYSTROPHY
359.21 - 359.24 MYOTONIC MUSCULAR DYSTROPHY - DRUG INDUCED MYOTONIA
359.29 OTHER SPECIFIED MYOTONIC DISORDER
359.3 - 359.6 PERIODIC PARALYSIS - SYMPTOMATIC INFLAMMATORY MYOPATHY IN DISEASES CLASSIFIED ELSEWHERE
359.71 INCLUSION BODY MYOSITIS
359.79 OTHER INFLAMMATORY AND IMMUNE MYOPATHIES, NEC
359.81 CRITICAL ILLNESS MYOPATHY
359.89 OTHER MYOPATHIES
359.9 MYOPATHY UNSPECIFIED
378.00 - 378.08 ESOTROPIA UNSPECIFIED - ALTERNATING ESOTROPIA WITH OTHER NONCOMITANCIES

378.10 - 378.18 EXOTROPIA UNSPECIFIED - ALTERNATING EXOTROPIA WITH OTHER NONCOMITANCIES
378.20 - 378.24 INTERMITTENT HETEROTROPIA UNSPECIFIED - INTERMITTENT EXOTROPIA ALTERNATING
378.30 - 378.35 HETEROTROPIA UNSPECIFIED - ACCOMMODATIVE COMPONENT IN ESOTROPIA
378.40 - 378.45 HETEROPHORIA UNSPECIFIED - ALTERNATING HYPERPHORIA
378.50 - 378.56 PARALYTIC STRABISMUS UNSPECIFIED - TOTAL OPHTHALMOPLEGIA
378.60 - 378.63 MECHANICAL STRABISMUS UNSPECIFIED - LIMITED DUCTION ASSOCIATED WITH OTHER CONDITIONS
378.71 - 378.73 DUANE'S SYNDROME - STRABISMUS IN OTHER NEUROMUSCULAR DISORDERS
378.81 - 378.87 PALSY OF CONJUGATE GAZE - OTHER DISSOCIATED DEVIATION OF EYE MOVEMENTS
378.9 UNSPECIFIED DISORDER OF EYE MOVEMENTS
458.0 ORTHOSTATIC HYPOTENSION
458.1 CHRONIC HYPOTENSION
478.30 - 478.34 UNSPECIFIED PARALYSIS OF VOCAL CORDS - COMPLETE BILATERAL PARALYSIS OF VOCAL CORDS
478.75 LARYNGEAL SPASM
530.0 ACHALASIA AND CARDIOSPASM
585.5 CHRONIC KIDNEY DISEASE, STAGE V
585.6 END STAGE RENAL DISEASE
625.6 STRESS INCONTINENCE FEMALE
646.40 - 646.44 PERIPHERAL NEURITIS IN PREGNANCY UNSPECIFIED AS TO EPISODE OF CARE - POSTPARTUM PERIPHERAL NEURITIS
710.3 - 710.5 DERMATOMYOSITIS - EOSINOPHILIA MYALGIA SYNDROME
721.0 - 721.3 CERVICAL SPONDYLOSIS WITHOUT MYELOPATHY - LUMBOSACRAL SPONDYLOSIS WITHOUT MYELOPATHY
721.41 SPONDYLOSIS WITH MYELOPATHY THORACIC REGION
721.42 SPONDYLOSIS WITH MYELOPATHY LUMBAR REGION

721.5 KISSING SPINE
721.6 ANKYLOSING VERTEBRAL HYPEROSTOSIS
721.8 OTHER ALLIED DISORDERS OF SPINE
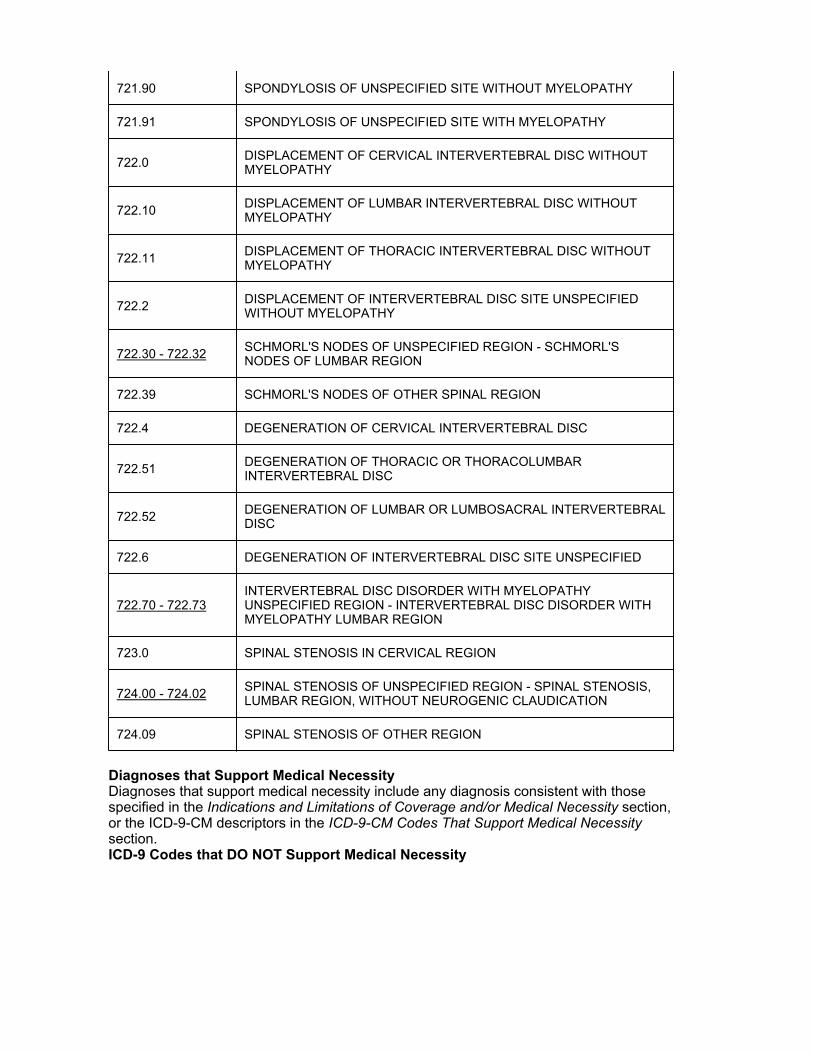
721.90 SPONDYLOSIS OF UNSPECIFIED SITE WITHOUT MYELOPATHY
721.91 SPONDYLOSIS OF UNSPECIFIED SITE WITH MYELOPATHY
722.0 DISPLACEMENT OF CERVICAL INTERVERTEBRAL DISC WITHOUT MYELOPATHY
722.10 DISPLACEMENT OF LUMBAR INTERVERTEBRAL DISC WITHOUT MYELOPATHY
722.11 DISPLACEMENT OF THORACIC INTERVERTEBRAL DISC WITHOUT MYELOPATHY
722.2 DISPLACEMENT OF INTERVERTEBRAL DISC SITE UNSPECIFIED WITHOUT MYELOPATHY
722.30 SCHMORL'S NODES OF UNSPECIFIED REGION
722.31 SCHMORL'S NODES OF THORACIC REGION
722.32 SCHMORL'S NODES OF LUMBAR REGION
722.39 SCHMORL'S NODES OF OTHER SPINAL REGION
722.4 DEGENERATION OF CERVICAL INTERVERTEBRAL DISC
722.51 DEGENERATION OF THORACIC OR THORACOLUMBAR INTERVERTEBRAL DISC
722.52 DEGENERATION OF LUMBAR OR LUMBOSACRAL INTERVERTEBRAL DISC
722.6 DEGENERATION OF INTERVERTEBRAL DISC SITE UNSPECIFIED
722.70 - 722.73INTERVERTEBRAL DISC DISORDER WITH MYELOPATHY UNSPECIFIED REGION - INTERVERTEBRAL DISC DISORDER WITHMYELOPATHY LUMBAR REGION
722.80 - 722.83 POSTLAMINECTOMY SYNDROME OF UNSPECIFIED REGION -POSTLAMINECTOMY SYNDROME OF LUMBAR REGION
722.90 - 722.93OTHER AND UNSPECIFIED DISC DISORDER OF UNSPECIFIED REGION - OTHER AND UNSPECIFIED DISC DISORDER OF LUMBAR REGION
723.0 SPINAL STENOSIS IN CERVICAL REGION
723.1 CERVICALGIA

723.4 BRACHIAL NEURITIS OR RADICULITIS NOS
723.5 TORTICOLLIS UNSPECIFIED
724.00 - 724.02 SPINAL STENOSIS OF UNSPECIFIED REGION - SPINAL STENOSIS, LUMBAR REGION, WITHOUT NEUROGENIC CLAUDICATION
724.03 SPINAL STENOSIS, LUMBAR REGION, WITH NEUROGENIC CLAUDICATION
724.09 SPINAL STENOSIS OF OTHER REGION
724.1 - 724.5 PAIN IN THORACIC SPINE - BACKACHE UNSPECIFIED
724.9 OTHER UNSPECIFIED BACK DISORDERS
725 POLYMYALGIA RHEUMATICA
728.0 INFECTIVE MYOSITIS
728.2 MUSCULAR WASTING AND DISUSE ATROPHY NOT ELSEWHERE CLASSIFIED
728.85 SPASM OF MUSCLE
728.87 MUSCLE WEAKNESS (GENERALIZED)
728.9 UNSPECIFIED DISORDER OF MUSCLE LIGAMENT AND FASCIA
729.1 MYALGIA AND MYOSITIS UNSPECIFIED
729.2 NEURALGIA NEURITIS AND RADICULITIS UNSPECIFIED
729.5 PAIN IN LIMB
729.82 CRAMP OF LIMB
732.7 OSTEOCHONDRITIS DISSECANS
736.05 WRIST DROP (ACQUIRED)
736.06 CLAW HAND (ACQUIRED)
736.09 OTHER ACQUIRED DEFORMITIES OF FOREARM EXCLUDING FINGERS
736.70 - 736.76 UNSPECIFIED DEFORMITY OF ANKLE AND FOOT ACQUIRED -OTHER ACQUIRED CALCANEUS DEFORMITY
736.79 OTHER ACQUIRED DEFORMITIES OF ANKLE AND FOOT
741.90 SPINA BIFIDA UNSPECIFIED REGION WITHOUT HYDROCEPHALUS

741.91 SPINA BIFIDA CERVICAL REGION WITHOUT HYDROCEPHALUS
741.92 SPINA BIFIDA DORSAL (THORACIC) REGION WITHOUT HYDROCEPHALUS
741.93 SPINA BIFIDA LUMBAR REGION WITHOUT HYDROCEPHALUS
742.51 DIASTEMATOMYELIA
742.8 OTHER SPECIFIED CONGENITAL ANOMALIES OF NERVOUS SYSTEM
780.02 TRANSIENT ALTERATION OF AWARENESS
780.2 SYNCOPE AND COLLAPSE
780.72 FUNCTIONAL QUADRIPLEGIA
780.79 OTHER MALAISE AND FATIGUE
781.0 ABNORMAL INVOLUNTARY MOVEMENTS
781.2 ABNORMALITY OF GAIT
781.3 LACK OF COORDINATION
781.4 TRANSIENT PARALYSIS OF LIMB
781.7 TETANY
781.94 FACIAL WEAKNESS
781.99 OTHER SYMPTOMS INVOLVING NERVOUS ANDMUSCULOSKELETAL SYSTEMS
782.0 DISTURBANCE OF SKIN SENSATION
784.42 DYSPHONIA
784.49 OTHER VOICE AND RESONANCE DISORDERS
785.0 TACHYCARDIA UNSPECIFIED
787.60 FULL INCONTINENCE OF FECES
787.61 INCOMPLETE DEFECATION
788.21 INCOMPLETE BLADDER EMPTYING
788.30 - 788.39 URINARY INCONTINENCE UNSPECIFIED - OTHER URINARY INCONTINENCE
794.17 NONSPECIFIC ABNORMAL ELECTROMYOGRAM (EMG)

806.00 - 806.09CLOSED FRACTURE OF C1-C4 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY - CLOSED FRACTURE OF C5-C7 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY
806.10 - 806.19OPEN FRACTURE OF C1-C4 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY - OPEN FRACTURE OF C5-C7 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY
806.20 - 806.29CLOSED FRACTURE OF T1-T6 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY - CLOSED FRACTURE OF T7-T12 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY
806.30 - 806.39OPEN FRACTURE OF T1-T6 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY - OPEN FRACTURE OF T7-T12 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY
806.4 CLOSED FRACTURE OF LUMBAR SPINE WITH SPINAL CORD INJURY
806.5 OPEN FRACTURE OF LUMBAR SPINE WITH SPINAL CORD INJURY
806.60 - 806.62CLOSED FRACTURE OF SACRUM AND COCCYX WITH UNSPECIFIED SPINAL CORD INJURY - CLOSED FRACTURE OF SACRUM ANDCOCCYX WITH OTHER CAUDA EQUINA INJURY
806.69 CLOSED FRACTURE OF SACRUM AND COCCYX WITH OTHER SPINAL CORD INJURY
806.70 - 806.72OPEN FRACTURE OF SACRUM AND COCCYX WITH UNSPECIFIED SPINAL CORD INJURY - OPEN FRACTURE OF SACRUM ANDCOCCYX WITH OTHER CAUDA EQUINA INJURY
806.79 OPEN FRACTURE OF SACRUM AND COCCYX WITH OTHER SPINAL CORD INJURY
806.8 CLOSED FRACTURE OF UNSPECIFIED VERTEBRA WITH SPINAL CORD INJURY
806.9 OPEN FRACTURE OF UNSPECIFIED VERTEBRA WITH SPINAL CORD INJURY
951.4 INJURY TO FACIAL NERVE
951.6 INJURY TO ACCESSORY NERVE
951.8 INJURY TO OTHER SPECIFIED CRANIAL NERVES
952.00 - 952.09 C1-C4 LEVEL SPINAL CORD INJURY UNSPECIFIED - C5-C7 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY
952.10 - 952.19 T1-T6 LEVEL SPINAL CORD INJURY UNSPECIFIED - T7-T12 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY
952.2 - 952.4LUMBAR SPINAL CORD INJURY WITHOUT SPINAL BONE INJURY -CAUDA EQUINA SPINAL CORD INJURY WITHOUT SPINAL BONEINJURY

952.8 MULTIPLE SITES OF SPINAL CORD INJURY WITHOUT SPINAL BONE INJURY
952.9 UNSPECIFIED SITE OF SPINAL CORD INJURY WITHOUT SPINAL BONE INJURY
953.0 - 953.5 INJURY TO CERVICAL NERVE ROOT - INJURY TO LUMBOSACRAL PLEXUS
953.8 INJURY TO MULTIPLE SITES OF NERVE ROOTS AND SPINAL PLEXUS
953.9 INJURY TO UNSPECIFIED SITE OF NERVE ROOTS AND SPINAL PLEXUS
954.0 INJURY TO CERVICAL SYMPATHETIC NERVE EXCLUDING SHOULDER AND PELVIC GIRDLES
954.1 INJURY TO OTHER SYMPATHETIC NERVE EXCLUDING SHOULDER AND PELVIC GIRDLES
954.8 INJURY TO OTHER SPECIFIED NERVE(S) OF TRUNK EXCLUDING SHOULDER AND PELVIC GIRDLES
954.9 INJURY TO UNSPECIFIED NERVE OF TRUNK EXCLUDING SHOULDER AND PELVIC GIRDLES
955.0 - 955.9 INJURY TO AXILLARY NERVE - INJURY TO UNSPECIFIED NERVE OF SHOULDER GIRDLE AND UPPER LIMB
956.0 - 956.5 INJURY TO SCIATIC NERVE - INJURY TO OTHER SPECIFIED NERVE(S) OF PELVIC GIRDLE AND LOWER LIMB
956.8 INJURY TO MULTIPLE NERVES OF PELVIC GIRDLE AND LOWER LIMB
956.9 INJURY TO UNSPECIFIED NERVE OF PELVIC GIRDLE AND LOWER LIMB
957.0 INJURY TO SUPERFICIAL NERVES OF HEAD AND NECK
957.1 INJURY TO OTHER SPECIFIED NERVE(S)
957.8 INJURY TO MULTIPLE NERVES IN SEVERAL PARTS
957.9 INJURY TO NERVES UNSPECIFIED SITE
994.8 ELECTROCUTION AND NONFATAL EFFECTS OF ELECTRIC CURRENT
Somatosensory Evoked Potential (SSEP) Testing CPT codes applicable for these ICD-9 codes 95925, 95926, 95927, 95938, 95939.
170.2 MALIGNANT NEOPLASM OF VERTEBRAL COLUMN EXCLUDING SACRUM AND COCCYX
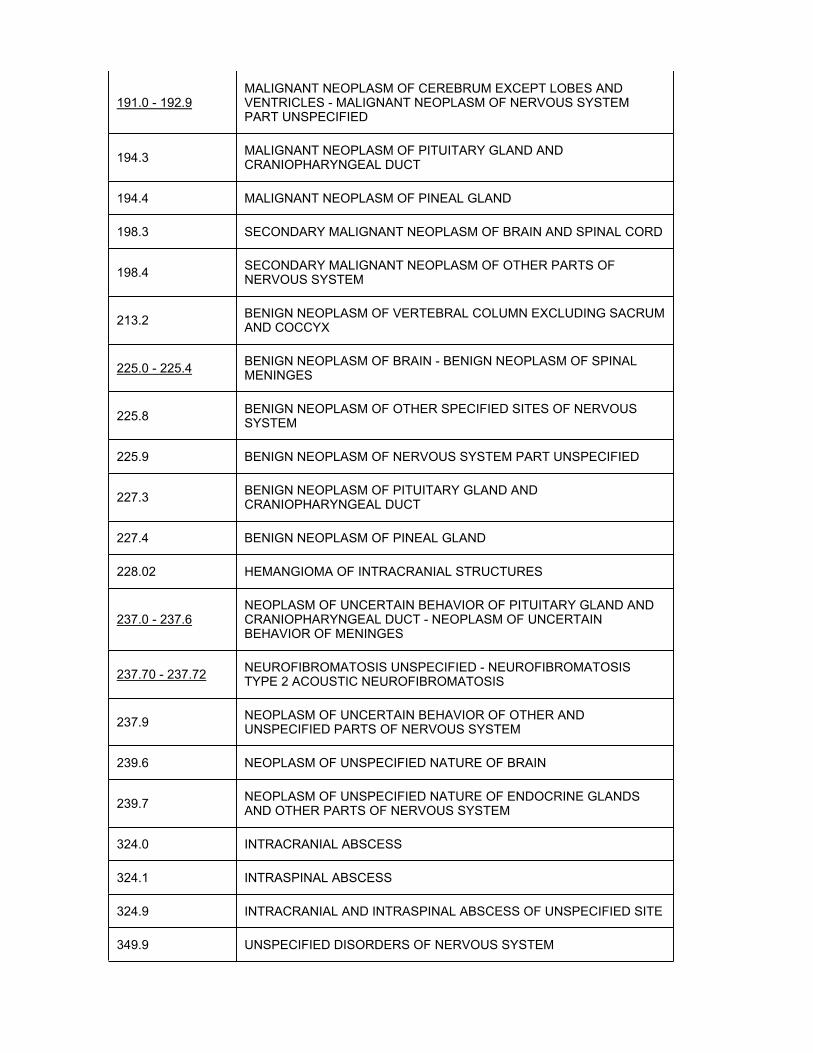
191.0 - 192.9MALIGNANT NEOPLASM OF CEREBRUM EXCEPT LOBES AND VENTRICLES - MALIGNANT NEOPLASM OF NERVOUS SYSTEM PART UNSPECIFIED
194.3 MALIGNANT NEOPLASM OF PITUITARY GLAND AND CRANIOPHARYNGEAL DUCT
194.4 MALIGNANT NEOPLASM OF PINEAL GLAND
198.3 SECONDARY MALIGNANT NEOPLASM OF BRAIN AND SPINAL CORD
198.4 SECONDARY MALIGNANT NEOPLASM OF OTHER PARTS OF NERVOUS SYSTEM
213.2 BENIGN NEOPLASM OF VERTEBRAL COLUMN EXCLUDING SACRUM AND COCCYX
225.0 - 225.4 BENIGN NEOPLASM OF BRAIN - BENIGN NEOPLASM OF SPINAL MENINGES
225.8 BENIGN NEOPLASM OF OTHER SPECIFIED SITES OF NERVOUS SYSTEM
225.9 BENIGN NEOPLASM OF NERVOUS SYSTEM PART UNSPECIFIED
227.3 BENIGN NEOPLASM OF PITUITARY GLAND ANDCRANIOPHARYNGEAL DUCT
227.4 BENIGN NEOPLASM OF PINEAL GLAND
228.02 HEMANGIOMA OF INTRACRANIAL STRUCTURES
237.0 - 237.6NEOPLASM OF UNCERTAIN BEHAVIOR OF PITUITARY GLAND AND CRANIOPHARYNGEAL DUCT - NEOPLASM OF UNCERTAIN BEHAVIOR OF MENINGES
237.70 - 237.72 NEUROFIBROMATOSIS UNSPECIFIED - NEUROFIBROMATOSIS TYPE 2 ACOUSTIC NEUROFIBROMATOSIS
237.9 NEOPLASM OF UNCERTAIN BEHAVIOR OF OTHER AND UNSPECIFIED PARTS OF NERVOUS SYSTEM
239.6 NEOPLASM OF UNSPECIFIED NATURE OF BRAIN
239.7 NEOPLASM OF UNSPECIFIED NATURE OF ENDOCRINE GLANDS AND OTHER PARTS OF NERVOUS SYSTEM
324.0 INTRACRANIAL ABSCESS
324.1 INTRASPINAL ABSCESS
324.9 INTRACRANIAL AND INTRASPINAL ABSCESS OF UNSPECIFIED SITE
349.9 UNSPECIFIED DISORDERS OF NERVOUS SYSTEM

350.1 TRIGEMINAL NEURALGIA
350.2 ATYPICAL FACE PAIN
350.8 OTHER SPECIFIED TRIGEMINAL NERVE DISORDERS
350.9 TRIGEMINAL NERVE DISORDER UNSPECIFIED
351.0 BELL'S PALSY
351.1 GENICULATE GANGLIONITIS
351.8 OTHER FACIAL NERVE DISORDERS
351.9 FACIAL NERVE DISORDER UNSPECIFIED
352.0 - 352.6 DISORDERS OF OLFACTORY (1ST) NERVE - MULTIPLE CRANIAL NERVE PALSIES
352.9 UNSPECIFIED DISORDER OF CRANIAL NERVES
353.0 - 353.6 BRACHIAL PLEXUS LESIONS - PHANTOM LIMB (SYNDROME)
353.8 OTHER NERVE ROOT AND PLEXUS DISORDERS
353.9 UNSPECIFIED NERVE ROOT AND PLEXUS DISORDER
433.01 OCCLUSION AND STENOSIS OF BASILAR ARTERY WITH CEREBRAL INFARCTION
433.11 OCCLUSION AND STENOSIS OF CAROTID ARTERY WITH CEREBRAL INFARCTION
433.21 OCCLUSION AND STENOSIS OF VERTEBRAL ARTERY WITH CEREBRAL INFARCTION
433.31 OCCLUSION AND STENOSIS OF MULTIPLE AND BILATERAL PRECEREBRAL ARTERIES WITH CEREBRAL INFARCTION
433.81 OCCLUSION AND STENOSIS OF OTHER SPECIFIED PRECEREBRAL ARTERY WITH CEREBRAL INFARCTION
433.91 OCCLUSION AND STENOSIS OF UNSPECIFIED PRECEREBRAL ARTERY WITH CEREBRAL INFARCTION
437.3 CEREBRAL ANEURYSM NONRUPTURED
437.5 MOYAMOYA DISEASE
720.0 ANKYLOSING SPONDYLITIS
721.0 - 721.8 CERVICAL SPONDYLOSIS WITHOUT MYELOPATHY - OTHER ALLIED DISORDERS OF SPINE
721.90 SPONDYLOSIS OF UNSPECIFIED SITE WITHOUT MYELOPATHY
721.91 SPONDYLOSIS OF UNSPECIFIED SITE WITH MYELOPATHY
722.0 DISPLACEMENT OF CERVICAL INTERVERTEBRAL DISC WITHOUT MYELOPATHY
722.10 DISPLACEMENT OF LUMBAR INTERVERTEBRAL DISC WITHOUT MYELOPATHY
722.11 DISPLACEMENT OF THORACIC INTERVERTEBRAL DISC WITHOUT MYELOPATHY
722.2 DISPLACEMENT OF INTERVERTEBRAL DISC SITE UNSPECIFIED WITHOUT MYELOPATHY
722.30 - 722.32 SCHMORL'S NODES OF UNSPECIFIED REGION - SCHMORL'S NODES OF LUMBAR REGION
722.39 SCHMORL'S NODES OF OTHER SPINAL REGION
722.4 DEGENERATION OF CERVICAL INTERVERTEBRAL DISC
722.51 DEGENERATION OF THORACIC OR THORACOLUMBAR INTERVERTEBRAL DISC
722.52 DEGENERATION OF LUMBAR OR LUMBOSACRAL INTERVERTEBRAL DISC
722.6 DEGENERATION OF INTERVERTEBRAL DISC SITE UNSPECIFIED
722.70 - 722.73INTERVERTEBRAL DISC DISORDER WITH MYELOPATHY UNSPECIFIED REGION - INTERVERTEBRAL DISC DISORDER WITHMYELOPATHY LUMBAR REGION
723.0 SPINAL STENOSIS IN CERVICAL REGION
724.00 - 724.02 SPINAL STENOSIS OF UNSPECIFIED REGION - SPINAL STENOSIS, LUMBAR REGION, WITHOUT NEUROGENIC CLAUDICATION
724.09 SPINAL STENOSIS OF OTHER REGION
Diagnoses that Support Medical NecessityDiagnoses that support medical necessity include any diagnosis consistent with thosespecified in the Indications and Limitations of Coverage and/or Medical Necessity section, or the ICD-9-CM descriptors in the ICD-9-CM Codes That Support Medical Necessitysection.ICD-9 Codes that DO NOT Support Medical Necessity
ICD-9 Codes that DO NOT Support Medical Necessity Asterisk Explanation
Diagnoses that DO NOT Support Medical NecessityDiagnoses that do not support medical necessity include any diagnosis inconsistent withthe Indications and Limitations of Coverage and/or Medical Necessity section, or the ICD-9-CM descriptors in the ICD-9-CM Codes That Support Medical Necessity section.
Back to Top
General Information
Documentations RequirementsSupportive documentation evidencing the condition and treatment is expected to bedocumented in the medical record and be available upon request. This A/B MAC mayrequest pertinent confirmatory information from the ordering provider as well as the billing (rendering) provider.
Usually the physician interpreting the test has also supervised the test, as part of the supervision involves evaluating both the quality and the extent of testing performed.
The following may be considered inadequate documentation: narrative reports alluding to “normal” or “abnormal” results without numerical data, descriptions of F-wave without reference to corresponding motor conduction data, pattern-setting unilateral H-reflex measurements, or separate E/M consultation charges without a documented request from the referral source.
Ordinarily, stand-alone electrodiagnostic studies-in the absence of a reasonably complete neurological exam with a presumptive diagnosis-will not be reimbursed. Symptoms-only are not adequate for presumptive diagnoses needing electrodiagnostic testing. It is theclinical picture and presumptive diagnoses that dictate the reasonableness and necessity of electrodiagnostic testing.
Appendices
Utilization GuidelinesFor Autonomic Function Studies:
Appropriate diagnostic testing may be performed once for patients to confirm or exclude specific autonomic disease.
•
For patients with an identified autonomic disorder, frequency of testing depends on changes in clinical status or response to intervention.
•
Providers who perform these tests on an unusually high proportion of their patients, or at frequencies exceeding once per patient per year, may be subject to medical review.
•
For Nerve Conduction and Electromyography:
The table below, recommended by the AANEM, is a guideline for the utilization of electrodiagnostic tests. The number of tests performed should be the maximum needed to establish an accurate diagnosis in 90% of patients, taking into account the possibility of more than one clinical diagnosis and coexisting medical and neuromuscular problems. In simple, straightforward cases, fewer tests will be necessary. This is particularly true when results of the most critical tests are normal. Common neurological conditions that can be diagnosed clinically do not usually require electrodiagnostic testing unless the diagnosis is

in question or treatment options are being evaluated for effectiveness.
In certain complex cases, the maximum numbers in the table will be insufficient for the physician to arrive at a complete diagnosis. In cases where there are borderline findings,additional tests may be required to determine if the findings are significant.
In the small number of cases that require testing in excess of the numbers listed in the table, the physician should be able to provide supplementary documentation to justify the additional testing. Such documentation should explain what other differential diagnostic problems needed to be ruled out in that particular situation. Very rarely, multiple simultaneous diagnoses will be investigated, which would in sum exceed the guidelines below.
Repeated electrodiagnostic tests are typically useful only:
To confirm an initial test or for a second opinion. •To repeat a test with equivocal results. •To monitor marked clinical changes in a condition. •To follow conditions that are expected to respond to surgical or medical treatments. •To evaluate a new set of symptoms. •To evaluate recovery from an injury.•
The following table is excerpted from the “Recommended Policy for Electrodiagnostic Medicine” from the American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM). This table provides the maximum number of tests necessary in 90% of cases (AANEM). Some patients may require less.
1.Nerve Conduction Studies, CPT codes 95900, 95903, 95904
A. Motor NCS with and/or without F wave
Carpel tunnel – unilateral- 3Carpel tunnel – bilateral- 4Radiculopathy - 3Mononeuropathy - 3Polyneuropathy/mononeuropathy multiplex - 4 Myopathy - 2Motor neuropathy (e.g., ALS) - 4Plexopathy - 4Neuromuscular junction - 2Tarsal tunnel syndrome – unilateral- 4Tarsal tunnel syndrome – bilateral- 5Weakness, fatigue, cramps, or twitching – focal- 3Weakness, fatigue, cramps, or twitching – general- 4Pain, numbness, or tingling (unilateral) - 3Pain, numbness, or tingling (bilateral) - 4
B. Sensory NCS
Carpel tunnel – unilateral- 4 Carpel tunnel – bilateral- 6Radiculopathy - 2Mononeuropathy - 3Polyneuropathy/mononeuropathy multiplex - 4

Myopathy - 2Motor neuropathy (e.g., ALS) - 2Plexopathy - 6Neuromuscular junction - 2Tarsal tunnel syndrome – unilateral- 4Tarsal tunnel syndrome – bilateral- 6Weakness, fatigue, cramps, or twitching – focal- 4Weakness, fatigue, cramps, or twitching – general- 4Pain, numbness, or tingling (unilateral) - 4Pain, numbness, or tingling (bilateral) - 6
2. Needle Electromyography, CPT codes 95860, 95861, 95863, 95864, 95867-95870
Carpel tunnel – unilateral- 1Carpel tunnel – bilateral- 2Radiculopathy - 2Mononeuropathy- 1Polyneuropathy/mononeuropathy multiplex - 3Myopathy - 2Motor neuropathy (e.g., ALS) - 4Plexopathy - 2Neuromuscular junction - 2Tarsal tunnel syndrome – unilateral- 1Tarsal tunnel syndrome – bilateral- 2Weakness, fatigue, cramps, or twitching – focal- 2Weakness, fatigue, cramps, or twitching – general- 4Pain, numbness, or tingling (unilateral) - 1 Pain, numbness, or tingling (bilateral) - 2
3. Other Electromyographic Studies, CPT codes 95934, 95936, 95937
Carpel tunnel – unilateral- **Carpel tunnel – bilateral- **Radiculopathy - 2Mononeuropathy - 2Polyneuropathy/mononeuropathy multiplex - 2 Myopathy - ** Motor neuropathy (e.g., ALS) - ** Plexopathy - 2 Neuromuscular junction - **Tarsal tunnel syndrome – unilateral- ** Tarsal tunnel syndrome – bilateral- ** Weakness, fatigue, cramps, or twitching – focal- **Weakness, fatigue, cramps, or twitching – general- ** Pain, numbness, or tingling (unilateral) - 2 Pain, numbness, or tingling (bilateral) - 2
** No specific number was indicated by the AANEM.
According to guidelines established by the AANEM, repeat electrodiagnostic consultation is sometimes necessary and reasonable limits can be set for the frequency of repeatstudies. The following numbers of tests per 12 month period, per diagnosis, per physician are acceptable when medically necessary:

1. Two tests for carpal tunnel-unilateral or bilateral, radiculopathy, mononeuropathy,polyneuropathy, myopathy, and NMJ disorders.2. Three tests for motor neuronopathy and plexopathy.
Autonomic Function Tests and Evoked Potential Studies
For autonomic function testing (CPT codes 95921-95923) and evoked potential studies (CPT codes 95925-95927), data shows that nearly all patients required only a single study; only 2-3% of all patients receiving these tests had conditions which required two or three studies. For example, a practice giving 2-5 tests for all patients would be extremely unusual and far outside community norms.
Sources of Information and Basis for DecisionCPT 2006 Standard Edition; American Medical Association
2006 ICD-9-CM Professional for Physicians; St. Anthony Publishing/Medicode Publications
LCD from Trailblazer Medicare, Electrodiagnostic Studies (NCS/EMG)
AANEM, Proper performance and interpretation of electrodiagnostic studies. Muscle Nerve Jan 2006;33(3):436-9. Association guidelines are specifically given by CMS asappropriate guidance for its contractors (HCFA Ruling 95-1, Section 5). See Also: Recommended Policy for Electrodiagnostic Medicine (2002 Update), AmericanAssociation of Neuromuscular and Electrodiagnostic Medicine (AANEM), AmericanAcademy of Neurology, and American Academy of Physical Medicine and Rehabilitation. (AANEM), web site: www.aanem.org. Accessed 2/7/2012.
AANEM. Practice parameters for EDX testing in carpal tunnel syndrome. Muscle Nerve.May 2002;25(6):918-22.
Aminoff MJ. Electromyography in Clinical Practice: Clinical and Electrodiagnostic Aspectsof Neuromuscular Disease. 3rd ed. New York: Churchill Livingstone; 1998.
Burneo JG, Barkley GL, Chawla J. Somatosensory evoked potentials: Clinical applications. 1998. Available at: http://emedicine.medscape.com/article/1139393-overview. Updated May/2010. Accessed 2/7/12.
Campbell WW. Essentials of Diagnostic Medicine. New York: Lippincott Williams & Wilkins; 1998.
D’Arcy CA, McGee S. Does this patient have carpal tunnel syndrome. JAMA. 2000;283(23)3110-7.
Goetz CG. Textbook of Clinical Neurology. 1st ed. Philadelphia, PA: W.B. Saunders Company. 1999:452-4;991-2.
Low PA. Testing the autonomic nervous system. Semin Neurol. 2003;23(4):407-21.Review.
Jablecki CK, Andary MT, Floeter MK, et al. Practice parameter: Electrodiagnostic studies in carpal tunnel syndrome. Neurology. 2002;58:1589-92.

Jaradeh SS, Prieto TE. Evaluation of the autonomic nervous system. Phys Med Rehabil Clin N Am. May 2003;14(2):287-305. Review.
Katz RT. NC-Stat as a screening tool for carpal tunnel syndrome. J Occup Environ Med.Aug 2006;48:414-8.
Levatt AD. Somatosensory evoked potentials: General Principles. Neuro. 2006. Available at: http://emedicine.medscape.com/article/1139906-overview. Updated Feb 3, 2012.Accessed 2/7/2012.
Mathias CJ. Autonomic Disorders and Their Recognition,[editoral]. NEJM. March 1997;336(10):721-724.
NIH Carpal Tunnel Fact Sheet Available at:http://www.ninds.nih.gov/disorders/carpal_tunnel/detail_carpal_tunnel.htm#69003049.Accessed 02/7/2012.
Storm S, Beaver SK, Giardino N, et al. Compliance with electrodiagnostic guidelines for patients undergoing carpal tunnel release. Arch Phys Med Rehabil. Apr 2005;86(4):8-11.
Viera AJ. Management of carpal tunnel syndrome. Am Fam Physician. Jul 2003; 68(2):265-72. Available at: http://www.aafp.org/afp/20030715/265.html. Accessed02/07/2012.
Association of California Neurologists
Contractor Medical Consultants
California Physical Therapy Association
American Physical Therapy Association, Section on Clinical Electrophysiology
American Board of Physical Therapy Specialists
NOTE: Some of the websites used to create this policy may no longer be available.
Advisory Committee Meeting NotesThis policy does not reflect the sole opinion of the contractor or Contractor MedicalDirector. Although the final decision rests with the contractor, this policy was developed in cooperation with advisory groups, which include representatives from the affected provider community.
Contractor Advisory Committee meeting dates:
California -Hawaii -Nevada -
Start Date of Comment Period
End Date of Comment Period
Start Date of Notice Period06/16/2008
Revision History NumberRevision #16
Revision History Explanation

Revision #16 effective for dates of service on or after 05/31/2012Revision made: Under ICD-9 codes that Support Medical Necessity placed the CPT codes that are applicable for those two sections of ICD-9 codes for clarification purposes for the providers.
Revision #15 effective for dates of service on or after 02/16/2012.Revision made: Under Sources of Information and Basis for Decision updated web site address for Levatt AD. Somatosensory evoked potentials: General Principles from www.emedicine.com/Neuro/Topic 640.htm towww.emedicine.medscape.com/article/1139906-overview. Accessed dates on applicable reference web sites were accessed for availability and accuracy.
Revision #14 effective for dates of service on or after 01/01/2012Revisions made: CPT/HCPCS Codes added CPT codes 95885, 95886 and 95887 to Group 2, Electromyography (EMG); added CPT Codes 95938 and 95939 to Group 4, Somatosensory Evoked Potential (SSEP) Testing. This revision is the result of CR 7540 2012 Annual CPT/HCPCS Update.
Revision #13 effective for dates of service on or after 10/01/2011Revisions made: Under CMS National Coverage Policy revised Publication 100-08, Program Integrity Manual Chapter 3, §§3.4.1.2 and 3.4.1.1,G to §§3.2.3 and 3.4.1.3,A;Requesting additional Documentation During Prepayment and Postpayment Review andDiagnosis Code Requirement respectively. Under ICD-9 Codes that Support MedicalNecessity added 331.6, 358.30, 358.31 & 358.39. This LCD is being revised due to the annual FY 2012 ICD-9-CM code update. This revision will become effective 10/01/2011.
Revision #12, effective for dates of service on or after 03/17/2011Revisions made: Under Documentation Requirements the third paragraph was removed that stated, "For documentation, the recording and compiling of test findings are the technical component. When performed separately from the professional component, the technical component is coded with Modifier-TC. The professional component is the process of developing and making a diagnosis and prognosis. When performed separately from the technical component, the professional component is coded with Modifier-26."
Revision #11, effective for dates of service on or after 1/13/2011.Revision made: Under CMS National Coverage Policy updated citation Pub. 100-08, Medicare Program Integrity Manual, Chapter 3, §3.4.1.1 E to G. Under sources of Information and Basis for Decision removed the following sources as they are no longer able to be located: LCD from Kansas/Nebraska, Western Missouri, Nerve Conduction Studies and Electromyography; LCD from Empire Medicare, Autonomic Nervous System Tests; LCD from Noridian Medicare, Nerve Conduction Studies and Electromyography (J3, 2006); Non-Medicare policies were reviewed, e.g. Cigna, Aetna, Wellmark, and others. Corrected the name of the LCD from Trailblazer Medicare from Nerve Conduction Studies – EMGs to Electrodiagnostic Studies (NCS/EMG). Added month and issue number to article titled, “Proper performance and interpretation of Electrodiagnostic studies”. Added month and issue number to article titled “Practice parameters for EDXtesting in carpal tunnel syndrome”. Corrected citation for book titled Electromyography in Clinical Practice: Clinical and Electrodiagnostic Aspects of Neuromuscular Disease. Added authors names to article title “Somatosensory evoked potentials: Clinical Applications,” and replaced web site address with correct address and included when this article was updated and date the article was accessed. Completed citation for book titled, Essentials of Diagnostic Medicine. Added additional author’s name and included issue number for article titled, “Does this patient have carpal tunnel syndrome. Corrected title of book for Textbook of Clinical Neurology, added author’s initials and added the publishing city and state. Added two additional authors names to article titled “Practice parameter: Electrodiagnostic studies in carpal tunnel syndrome.” Added month of publication to

article titled “Evaluation of the autonomic nervous system.” Added month of publication to article titled “NC-Stat as a screening tool for carpal tunnel syndrome.” Added authors’ names to article titles Compliance with Electrodiagnostic guidelines for patients undergoing carpal tunnel release” and corrected title of article, added month and issue number of publication. Removed citation titled “University of Maryland. How is carpaltunnel syndrome diagnosed?” as this web site no longer exists. Removed citation titled “Washington University St Louis. Autonomic Disorders. Neuromuscular Disease Center, Washington University School of Medicine, “as this citation and website are no longer available. Added article publication information for article titled “Management of carpal tunnel syndrome” and updated article accessed date.
Revision #10, effective for dates of service on or after 10/01/2010.Revision made: Under ICD-9 Codes that Support Medical Necessity ICD-9 codes 237.73, 237.79, 724.03, 787.60 & 787.61 were added, 787.6 was deleted and 724.02 had a descriptor change. These changes were the result of Medicare Contractor Annual Update of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) CR 7006, Transmittal 2017.
Revision #9 effective for dates of service on or after 05/20/2010.Revision made -under ICD-9 codes that support medical necessity added ICD-9 code 951.6 to support medical necessity for EMG.
Revision #8 effective for dates of service on or after 01/01/2010Revisions made: Annual 2010 CPT/HCPCS update, under CPT/HCPCS codes, Nerve Conduction Studies, paragraph 1 added CPT code 95905 to the sentence and removed 95999. The following CPT codes descriptors were revised 95937 in Group 1, 95860 and 95870 in Group 2, 95921 and 95923 in Group 3.
Revision #7 effective for dates of service on or after 10/01/2009.Revisions made: Under "ICD-9 Codes that Support Medical Necessity", the following ICD-9 codes were added to support the medical necessity of CPT codes 95900, 95903, 95904, 95934, 95936, 95937, 95860, 95061, 95863, 95864, 95867, 95868, 95869, 95870, 95872, 95921, 95922, 95923: 359.71, 359.79, 784.42. ICD-9 code 784.49 descriptor was revised per CMS Manual System, Pub. 100-04, Medicare Claims Processing, Chapter 23, §10.2; Annual Update of the International Classification of Diseases, Ninth Revision,Clinical Modification (ICD-9-CM), CR 6520, Transmittal 1770, dated July 10, 2009.
Revision #6, effective for dates of service on or after 06/04/2009Revision made: Under “Indications and Limitations of Coverage and/or Medical Necessity” subtitle ‘IDTFs’ removed reference of the IDTF LCD which has been retired.
Revision #5, 02/26/2009This LCD is being revised to implement the streamlining of the Part B LCDs per the published article “Palmetto Team to Streamline Part B LCDs in Jurisdiction 1 (J1).” Thisarticle can be viewed at www.PalmettoGBA.com by searching for the above article name. This revision will become effective on 02/26/2009.
Revision #4, 12/18/2008Correction of typographical error from previous contractor for CPT codes under Indications and Limitation of Coverage and/or medical necessity, subheading Level 6A/66 tests, CPT Codes 96860-96870 and 96872 changed to 95868-95870 and 95872.
Revision #3, 12/18/2008Under CMS National Coverage Policy added Chapter 13 to the cited reference, CMS Manual System, Pub 100-08, Medicare Program Integrity Manual. Under Indications and Limitations of Coverage and/or Medical Necessity-Dynamic Tests deleted the following

verbiage, "The available diagnostic services must include ability to test orthodromic andantidromic studies of proximal and distal segments, and when neuromuscular dysfunction is a key part of the differential diagnosis must include the ability to perform a needle electrode examination (electromyography) to avoid repetition of the study set when EMG is available..." Under Indications and Limitations of Coverage and/or Medical Necessity-Indications for Nerve Conduction Studies added the section titled, "2008 Policy Revision." Under Indications and Limitations of Coverage and/or Medical Necessity-Equipment for Nerve Conduction Studies and EMG deleted verbiage regarding testing by hand-held devices and surface electrodes and diagnostic studies that provide delayed interpretation(telephonic and internet)as substitutes for nerve conduction studies. In the last paragraph of this section changed "an" to "a". Under the CPT/HCPCS Codes-Nerve ConductionStudies (NCS) section added the asterisk and the verbiage regarding CPT code 95999. Under the CPT/HCPCS Codes-Nerve Conduction Studies (NCS) section added CPT code 95999. Under Ulilization Guidelines removed verbiage that read, " This Medicare contractor supports the following language of the Recommended Policy ofElectrodiagnostic Medicine of the American Association of Neuromuscular andElectrodiagnostic Medicine, American Academy of Neurology, and American Academy of Physical Medicine and Rehabilitation: “It is appropriate for only one attending physician to perform or supervise all the components of the electrodiagnostic testing (e.g., history taking, physical examination, supervision and/or performance of the electrodiagnostic test, and interpretation) for a given patient and for all the testing to occur on the samedate of service. The reporting of NCS and EMG study results should be integrated into a unifying diagnostic impression. In contrast, dissociation of NCS and EMG results into separate reports is inappropriate unless specifically explained by the physician. Performance and/or interpretation of NCS separately from that of the needle EMG component of the test should clearly be the exception (e.g., when testing for an acute nerve injury) rather than an established practice pattern for a given practitioner.” Under Sources of Information and Basis for Decision the references were placed in the AMA citation format. This revision becomes effective 12/18/2008.
**Under CPT/HCPCS Codes section the verbiage for CPT codes 95861, 95863, 95864 and 95922 was revised as per the 2009 CPT/HCPCS Updates. This revision becomes effective 01/01/2009.
Revision #2, 10/1/2008FY 2009 Annual ICD-9-CM code update. Under ICD-9-CM Codes that Support Medical Necessity added 249.60, 249.61, 337.00, 337.09 and 780.72. ICD-9-CM code 337.0 was made invalid and deleted from this LCD. Under CMS National Coverage Policy added CMS Publication 100-08 (Program Integrity Manual) Chapter 13, 5.1. Corrected SSA citation and Publication 100.08 (Program Integrity Manual) citation in the National Coverage Policy section of the LCD. Removed duplicative Federal Regulations and CMS manual citations within the Indications and Limitations of Coverage and Documentation Requirement sections of the LCD. Under Sources of Information and Basis for Decision the references were placed in the AMA citation format. This revision becomes effective10/01/2008.
Revision #1, 09/02/2008This LCD is being revised to add Bill Type 999X because the automated system transcription process was incomplete.
08/08/2009 - This policy was updated by the ICD-9 2009-2010 Annual Update.
11/15/2009 - The description for CPT/HCPCS code 95937 was changed in group 111/15/2009 - The description for CPT/HCPCS code 95860 was changed in group 211/15/2009 - The description for CPT/HCPCS code 95870 was changed in group 211/15/2009 - The description for CPT/HCPCS code 95921 was changed in group 311/15/2009 - The description for CPT/HCPCS code 95923 was changed in group 3
09/06/2010 - This policy was updated by the ICD-9 2010-2011 Annual Update.
11/21/2010 - For the following CPT/HCPCS codes either the short description and/or the long description was changed. Depending on which description is used in this LCD, there may not be any change in how the code displays in the document:95860 descriptor was changed in Group 295861 descriptor was changed in Group 295863 descriptor was changed in Group 295864 descriptor was changed in Group 295869 descriptor was changed in Group 295870 descriptor was changed in Group 295872 descriptor was changed in Group 2
Reason for ChangeNarrative Change
Related DocumentsThis LCD has no Related Documents.
LCD AttachmentsThere are no attachments for this LCD.
Back to Top
All Versions
Updated on 05/31/2012 with effective dates 05/31/2012 - N/A Updated on 02/08/2012 with effective dates 01/01/2012 - 05/30/2012Updated on 12/02/2011 with effective dates 01/01/2012 - N/AUpdated on 12/02/2011 with effective dates 01/01/2012 - N/AUpdated on 09/14/2011 with effective dates 10/01/2011 - 12/31/2011Updated on 02/25/2011 with effective dates 03/17/2011 - 09/30/2011Updated on 01/07/2011 with effective dates 01/13/2011 - 03/16/2011Updated on 11/21/2010 with effective dates 10/01/2010 - 01/12/2011Updated on 09/10/2010 with effective dates 10/01/2010 - N/ASome older versions have been archived. Please visit the MCD Archive Site to retrieve them.
Read the LCD DisclaimerBack to Top
Department of Health & Human Services Medicare.gov USA.govWeb Policies & Important Links Privacy Policy Freedom of Information Act No Fear ActCenters for Medicare & Medicaid Services, 7500 Security Boulevard Baltimore, MD 21244
64