back pack health worker team
TRANSCRIPT

Back Pack Health Worker TeamBack Pack Health Worker Team

BACK PACK HEALTH WORKER TEAM
●Established in 1998
●Coordinated with health workersfrom Karen, Mon, and Karenni areas.
●Aim to reach IDPs in the least stableconflict zone areas
● Provide primary health care
●Aim to equip communities with theskills and knowledge to address theirown needs while working towards along-term sustainable community-based primary health care system.
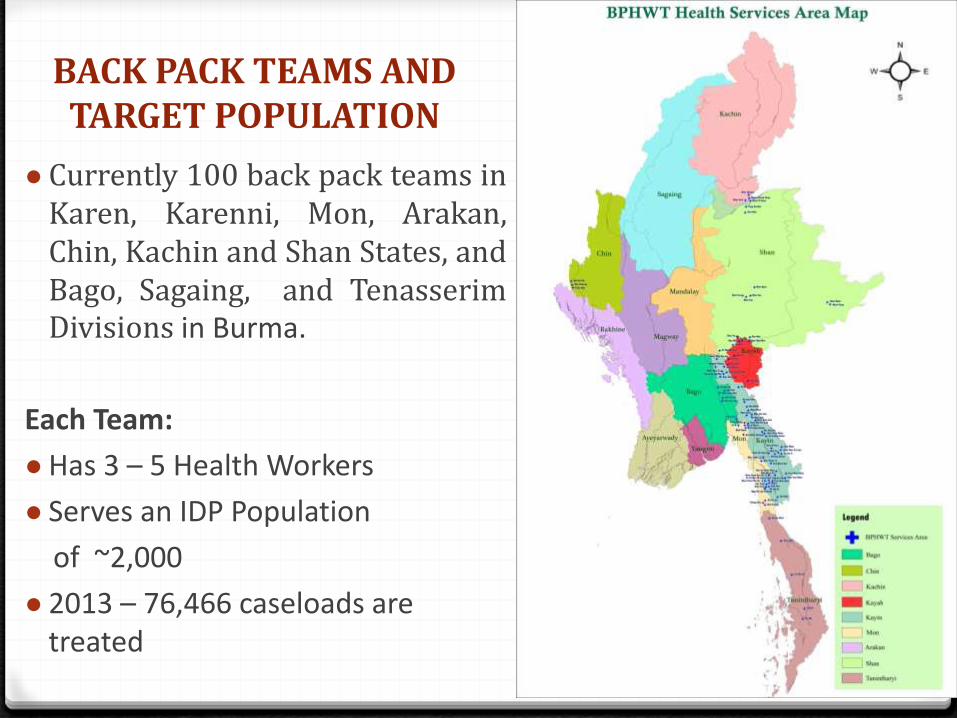
BACK PACK TEAMS AND TARGET POPULATION
● Currently 100 back pack teams inKaren, Karenni, Mon, Arakan,Chin, Kachin and Shan States, andBago, Sagaing, and TenasserimDivisions in Burma.
Each Team:
●Has 3 – 5 Health Workers
● Serves an IDP Population
of ~2,000
● 2013 – 76,466 caseloads are treated
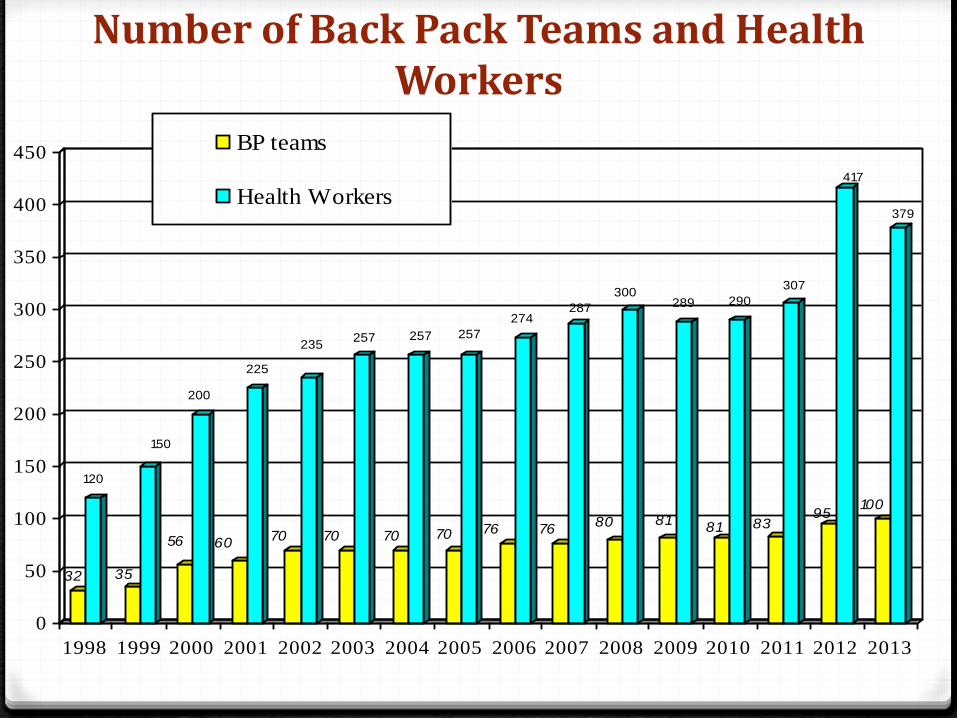
Number of Back Pack Teams and Health Workers
32
120
35
150
56
200
60
225
70
235
70
257
70
257
70
257
76
274
76
287
80
300
81
289
81
290
83
307
95
417
100
379
0
50
100
150
200
250
300
350
400
450
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
BP teams
Health Workers

Organizational Structure and Governance
3 Major Programs
● Medical Care Program
● Community Health Education and
Prevention Program
● Maternal and Child Healthcare Program

Medical Care Program
● Treat common illnesses0 Targets the 6 most prevalent
conditions: Malaria, ARI, Anemia, Worms, Diarrhea and Dysentery
● Provision of medicine and medical materials
● Strengthen existing referral system
● Emergency treatment for war-related injuries


Community Health Education and Prevention Program
● School Health Promotion access
●Community Water and Sanitation Program
●Nutritional Promotion
●Village Health workshops
●Village Health Worker training and workshops

Maternal & Child Healthcare Program
●Trained Traditional Birth Attendant (TTBA) Training
0711 TBAs/TTBAs currently working
●TBA/TTBA Workshops are held every six months
● Provision of TTBA supplies and maternity kits
● 3,508 total deliveries in 2013
● Provide family planning methods
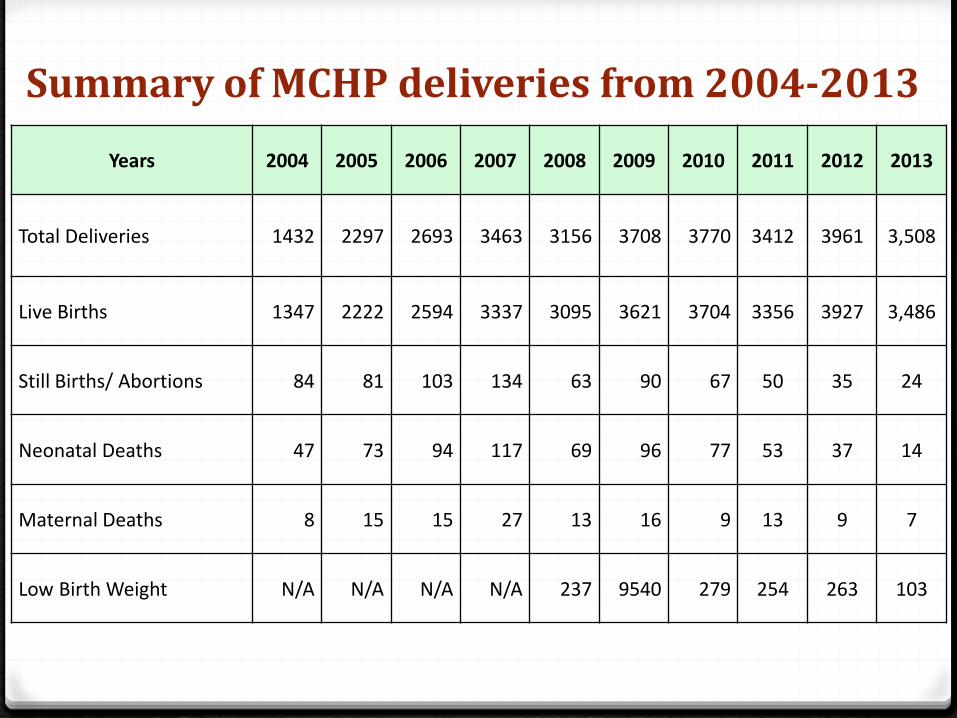
Summary of MCHP deliveries from 2004-2013
Years 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Total Deliveries 1432 2297 2693 3463 3156 3708 3770 3412 3961 3,508
Live Births 1347 2222 2594 3337 3095 3621 3704 3356 3927 3,486
Still Births/ Abortions 84 81 103 134 63 90 67 50 35 24
Neonatal Deaths 47 73 94 117 69 96 77 53 37 14
Maternal Deaths 8 15 15 27 13 16 9 13 9 7
Low Birth Weight N/A N/A N/A N/A 237 9540 279 254 263 103

Obstacles to Program Implementation
●Restricted health worker mobility0 Environment
0 Security
●Data collection0 Dangers
0 Populations are frequently on the move
●Health worker skills and training

Solutions to Obstacles
●Data Collection – solutions for security:
0 No identifying features on forms
0 Consult with local leaders
0 Use walkie-talkies and satellite phones
0 Some translation to local languages
●Health worker skills and training
0 Increase quality and quantity of training
0 Training-of-Trainers courses
0 Village Health Volunteers → Village Health Workers
0 Traditional Birth Attendants → Trained Traditional Birth Attendants

Coordination and collaboration
● Cooperate with local authorities for transportation andcommunication
● Coordinate with local ethnic health organizations to managethe outbreak of diseases, referral of patients and for BasicMedical Training
● Cooperate with IRC (health worker training & capacitybuilding); BRC (external M&E, capacity building, advocacy,networking); MTC (health worker training); CPI (technicalsupport, i.e. HIS & Public Health)

Monitoring and Evaluation
I) Internal monitoring and evaluation:
● Program Management
● Program Development
● Program Effectiveness
0Data Collection & Review
0Health worker performance
0 Field Consultation with village leaders
0 Impact Assessment Survey
II) External monitoring and evaluation:
● 2008 – DCA; BRC/CIDA
● 2010-2011 – BRC/NCA/IRC/Inter Pares
● 2011 (Eastern Burma) – IRC/TBBC

Thank you