b.8 oral candidiasis
DESCRIPTION
b.8 Oral CandidiasisTRANSCRIPT

Oral candidiasis andangular cheilitisdth_1320 230..242
Victoria Sharon & Nasim FazelDepartment of Dermatology, University of Davis, Sacramento, California
ABSTRACT: Candidiasis, an often encountered oral disease, has been increasing in frequency. Mostcommonly caused by the overgrowth of Candida albicans, oral candidiasis can be divided into severalcategories including acute and chronic forms, and angular cheilitis. Risk factors for the development oforal candidiasis include immunosuppression, wearing of dentures, pharmacotherapeutics, smoking,infancy and old age, endocrine dysfunction, and decreased salivation. Oral candidiasis may be asymp-tomatic. More frequently, however, it is physically uncomfortable, and the patient may complain ofburning mouth, dysgeusia, dysphagia, anorexia, and weight loss, leading to nutritional deficiency andimpaired quality of life. A plethora of antifungal treatments are available. The overall prognosis of oralcandidiasis is good, and rarely is the condition life threatening with invasive or recalcitrant disease.
KEYWORDS: angular cheilitis, angular cheilosis, candidosis, oral candidiasis, thrush
Introduction
Oral candidiasis, the most common fungal infec-tion in humans, has resurged in frequencythroughout the United States. This has been at-tributed to the increasing prevalence of humanimmunodeficiency virus (HIV), administration ofcorticosteroids and a variety of other immuno-suppressive medications, expanded use ofbroad-spectrum antibiotics, an enlarging elderlypopulation with oral prostheses, and an increasein obesity and resultant diabetes mellitus (1).Although oral candidiasis poses a very low mortal-ity risk, it can be physically uncomfortable, and thepatient may complain of burning mouth, dysgeu-sia, dysphagia, anorexia, and weight loss, leading tonutritional deficiency and impaired quality of life.In the immunocompromised host, there is a risk oftracheal or esophageal extension, which may leadto painful erosions. Systemic dissemination andfungemia from oral candidiasis, although rare, canoccur in susceptible and debilitated hosts.
Candida can be a commensal organism in theoral cavity, and its isolation in the absence of clini-cal correlation does not indicate active infection.The pseudohyphal growth of Candida is fosteredby elevated intraoral temperatures. In healthy chil-dren and adults, carriage of Candida is asymptom-atic. The areas of the mouth most heavily colonizedby Candida are the posterior dorsal tongue, palate,and buccal mucosa (2). The prevalence of carriageof Candida varies from 45 to 65% in healthy infants,and 30–55% in normal adults (3). Colonized infantsare often exposed in utero or during passagethrough the vaginal canal. Candida carriage occursin up to 65% of denture wearers, 78% of hospital-ized elderly, and greater than 90% of patients withHIV or individuals receiving chemotherapy (2–6).
Candidal carriage occurs more frequently inwomen, during the summer months, in patientswith more acidic saliva, in pregnancy, and in thosewith blood group O (7–9). Candidal counts aremost elevated in the mornings and decrease withmeals and brushing. In denture wearers, however,this finding is reversed. Thus, carriage is lowest inthe mornings and increases throughout the day,corresponding to the length of time dentures havebeen worn. In edentulous patients who wear theirdentures overnight, candidal counts are again
Address correspondence and reprint requests to: VictoriaSharon, MD, Department of Dermatology, University ofCalifornia, Davis, 3301 C Street, Suite 1400, Sacramento, CA95816, or email: [email protected].
230
Dermatologic Therapy, Vol. 23, 2010, 230–242Printed in the United States · All rights reserved
© 2010 Wiley Periodicals, Inc.
DERMATOLOGIC THERAPYISSN 1396-0296

highest in the morning. These findings support thetheory that Candida adheres to dentures, and theorganism has indeed been detected in increasednumbers on denture surfaces compared to mucosa(10). Therefore, with the exception of edentulouspatients, early-morning candidal samples are mostaccurate for comparing individual differences incarriage (7).
Denture stomatitis, identified by erythema andedema of the denture-fitting surfaces of the mouth,occurs in up to 65% of patients with dentures (11).The predominant cause of denture stomatitis iscandidal colonization of the denture-coveredareas, although mechanical irritation, allergy todenture material, and non-candidal infectionshave been identified as alternate causes. The mainreservoir for candidal colonization in thesepatients is the fitting denture surface as Candidaoften attaches to plastic or orthodontic surfaces,either directly or by a layer of plaque that adheresto the polymethylmethacrylate base (12).
Although candidal carriage in the oral cavitymay be a normal phenomenon, candidiasis is aresult of Candida overgrowth (5). The mostcommon pathogenic species of candidiasis isCandida albicans, occurring in 50–60% of cases.Other important pathogens include Candida gla-brata (15–20%), Candida parapsilosis (10–20%),Candida tropicalis (6–12%), Candida pseudotropi-calis (<5%), Candida guilliermondii (<5%),Candida krusei (<5%), Candida lusitaniae (<5%),Candida dubliniensis (<5%), and Candida stella-toidea (<5%) (5,13). Less commonly identifiedstrains are more frequently found in immunosup-pressed populations. Greater than 15% of oral can-didiasis is caused by non-albicans species in thosewith HIV, most often C. dubliniensis. Similarly,46% of cases of oral candidiasis in patients withmalignancy are caused by non-albicans species(14–17).
Options for treating oral candidiasis are avail-able in a variety of forms including rinses, suspen-sions, creams, ointments, lozenges, capsules, andtablets. Topical treatment in healthy patients or inthe immunocompromised host with mild diseaseis preferable to systemic therapy. However, theunique environment of salivary flushing and theaction of oral musculature result in decreasedtherapeutic drug concentration, mandating a needfor frequent dosing. Inconvenient dosing sched-ules combined with the occasional unpalatabletaste lead to noncompliance and frequent treat-ment failure. A variety of systemic therapies aregenerally reserved to treat refractory or high-riskdisease.
Risk factors
Any circumstance predisposing an individual toincreased oral candidal carriage presents a poten-tial risk for developing active infection, particularlyin the setting of transient immunosuppression.Risk factors for active infection can be classifiedinto endogenous and exogenous components.Endogenous factors include infancy and old age,pregnancy, immunocompromised states, diabetesmellitus, other endocrinopathies resulting inchronically elevated serum glucose, Sjögrensyndrome-induced xerostomia, vitamin deficien-cies, and poor overall health (7). Exogenous riskfactors encompass poor nutritional diet, the useof specified pharmacotherapeutics, cigarettesmoking, ill-fitting oral prostheses, chronic localirritation or trauma, local radiation, and malig-nancy with chemotherapy treatment (5,15). Theserisk factors are summarized in Table 1, and dis-cussed in further detail below.
Extreme ages of life confer decreased immunity,and hence an increased risk for the growth ofopportunistic pathogens. Diminished saliva pro-duction has been hypothesized to promote thegrowth of Candida by decreasing clearance of thefungus in areas of colonization (5). Saliva not onlydilutes and clears candidal species from the oralcavity, but via its proteins, among which arelysozyme, lactoferrin, sialoperoxidase, and anti-Candida antibodies, discourages proliferation(5,7). Transient immunosuppression and immuno-deficiency syndromes predispose to active infec-tion secondary to an inability of the individual tomount an innate or adaptive immune response.Impaired phagocytosis, oxidative destruction,cytokine production, or antibody formation canlead to impaired clearance of Candida.
In patients with HIV, Candida is the most fre-quent oral opportunistic infection. Infection typi-cally occurs at times of decreased CD4 counts,although it has been reported to arise at all stagesof HIV infection (15,18). Although asymptomaticcandidal carriage has been shown by some to beincreased at all stages of HIV infection, symptom-atic candidiasis predominantly occurs at CD4counts below 500 cells/mm3, with a larger increaseseen below 200 cells/mm3 (19). Symptomatic can-didiasis has been found in up to 90% of patientswith HIV, half of whom develop acquired immuno-deficiency syndrome within 3 years (20). Althoughoral candidal infections are primarily a nuisance inimmunocompetent individuals, they can lead tomore worrisome complications in patients withHIV, such as esophageal candidiasis (1). It is there-
Oral candidiasis and angular cheilitis
231

fore important for the clinician to perform a thor-ough oral examination in the patient with HIV, asoral candidiasis can be a harbinger of worseningimmunosuppression. Highly active antiretroviraltherapy in patients with HIV correlates withdecreased recovery of Candida from the oropha-ryngeal tract and decreased symptomatic oral can-didiasis (21).
Many pharmacotherapeutics confer an in-creased risk of active candidal infection. Antibiot-ics, such as tetracycline and minocycline, alter thenormal flora of the oral cavity, promoting candidal
growth (7,22,23). The use of antibiotic mouth-washes may also increase the risk of active infec-tion. Anticholinergics may cause xerostomialeading to diminished salivary flow and impairedclearance of candidal species. Oral or inhaled cor-ticosteroids and other immunosuppressive medi-cations, including chemotherapy in the settingof malignancy, impair the ability of the immunesystem to battle candidal antigens.
Smoking has been associated with increasedcandidal carriage in some studies, but not in others(3,24). Its role as an etiologic agent in predisposingan individual to active Candida infection is contro-versial, with several studies clearly showing anincreased risk of active infection in particularimmunosuppressed populations (25).
Chronic local irritation, poorly fitting oral pros-theses, epithelial dysplasia, prior local radiation,and oral malignancy disrupt the intact epithelium,resulting in a damaged epithelial barrier, facilitat-ing candidal invasion of the stratum corneum andstratum spinosum (26).
Classification
Candidiasis of the oral cavity can be broadly cat-egorized as primary or secondary. The formerdescribes candidal infections only involving theoral or perioral tissues, whereas the latter charac-terizes systemic candidiasis that secondarilyinvolves the oral cavity (1,7). Primary oral candidi-asis has been traditionally subdivided into acutepseudomembranous candidiasis, acute atrophiccandidiasis, chronic hyperplastic candidiasis,chronic atrophic candidiasis, median rhomboidglossitis, angular cheilitis, and linear gingivalerythema (FIG. 1) (5).
Acute pseudomembranous candidiasis
Acute pseudomembranous candidiasis (exudativecandidiasis, thrush) is responsible for at least one-third of cases of oral candidiasis (5). In particularpopulations, it has been reported to represent upto two-thirds of symptomatic candidiasis (19).When clinically symptomatic, the patient maynotice a burning sensation in the mouth, a sourtaste or difficulty tasting food, or discomfort andeasy bleeding in the affected areas. Thrush oftenappears as confluent, loosely attached, whitepseudomembranous plaques resembling milkcurd, which frequently involve the buccal mucosa,
Table 1. Risk factors for oral candidiasis andangular cheilitisa
Endogenous riskfactors Exogenous risk factors
Extremes of age (infants,elderly)
Poor oral hygiene
Immunodeficiency Overclosure(occlusion)HIV or AIDS
Oral prosthesesSevere combinedimmunodeficiency Poorly fitting
denturesMyeloperoxidasedeficiency Mouth guardsHyper IgE syndrome Dental traysChronic granulomatousdisease
Disrupted mucosalbarrier
Chediak–Higashisyndrome
Trauma
DiGeorge syndromeBurn
Nezelof syndromeChronic local irritation
Endocrine abnormalitiesSurgery
Diabetes mellitusRadiation
Hyperadrenalism(Cushing syndrome)
Medications
Hypothyroidism
Antibiotics
Pregnancy
Anticholinergics
Systemic illnesses
Antihistamines
Malignancy
Chemotherapeutics
Blood dyscrasias
Immunosuppressiveagents
UremiaXerostomicpsychotropicmedicationsXerostomia (Sjögren
syndrome) Systemic or inhaledcorticosteroidsOral contraceptives
SmokingProlonged
hospitalizationPoor diet
Vitamin deficiencies(iron, folate, B12)High carbohydratecontent
aAdapted from Scully et al. (7).
Sharon & Fazel
232

tongue, oropharynx, hard palate, and soft palate(FIG. 2) (5). Scraping of these pseudomembraneswith a tongue depressor, blade, or gauze reveals anunderlying erythematous base. Microscopic evalu-ation demonstrates hyphal forms, bacteria, inflam-matory cells, and sloughed epithelial cells (27).
Conditions that predispose to thrush include,but are not limited to, immune defects, HIV, corti-costeroid inhalers, endocrine abnormalities, and
malignancy (27). Although thrush may occuracutely, its presence can persist for months inpatients with HIV or in those using corticosteroidinhalers. The differential diagnosis includes leuko-plakia, lichen planus, other lichenoid eruptions,pemphigus, mucous membrane pemphigoid, per-sistent food debris, and squamous cell carcinoma.
Acute atrophic candidiasis
Acute atrophic candidiasis (erythematous candidi-asis, antibiotic sore mouth) may be associated witha burning oral sensation, and the patient may com-plain of a sore tongue or lip (1,5). Erythematouscandidiasis involving the palate is quite common,particularly in HIV-positive patients, and is oftenoverlooked (FIG. 3) (1,7). Erythematous patchesmay also be found on the buccal mucosa, and lesscommonly the mid-posterior dorsal tongue(median rhomboid glossitis), which can appearbright red because of loss of the filiform papillae.Erythematous candidiasis can arise after the whitepseudomembranes of thrush are shed, or mayalternatively arise de novo (1,28). It has been pos-tulated that acute pseudomembranous candidiasisand erythematous candidiasis represent a con-tinuum of the same pathological process (1).
The differential diagnosis includes atrophiclichen planus, oral mucositis, and nutritional defi-ciencies of vitamin B12, folate, and ferritin (5).
Chronic hyperplastic candidiasis
Chronic hyperplastic candidiasis has been referredto as candidal leukoplakia, owing to the possibilityof progression to dysplasia or malignancy in some
Primary oral candidiasis
Chronic atrophic
Chronic hyperplastic
Candida -associated
Acute atrophic
Acutepseudomembranous
Denture stomatitisThrush “Antibiotic sore mouth”
Candidal leukoplakia • Actinic cheilitis
• Median rhomboid glossitis
• Linear gingival erythema
FIG. 1. Traditional classification of primary oral candidiasis.
FIG. 2. Acute pseudomembranous candidiasis. Courtesy ofErrol Craig, MD, PhD, Walnut Creek, CA.
Oral candidiasis and angular cheilitis
233

cases, if left untreated (1,5,7). Chronic hyperplasticcandidiasis is one of the least common forms oforal candidiasis. Lesions generally occur on thebuccal mucosa, and less commonly on the lateralsides of the tongue, as small or large well-circumscribed translucent-to-white homogeneousor speckled firm plaques or nodules (5). Unlikethrush, these plaques are resistant to removal bygentle scraping. Chronic hyperplastic candidiasismay resolve with smoking cessation (5). Histologi-cally, these lesions reveal candidal hyphae withina hyperplastic epithelium. Epithelial dysplasia isnot present. However, in cases of oral malignancy,Candida invasion may occur secondary to a dis-rupted or altered epithelium.
The differential diagnosis of chronic hyperplas-tic candidiasis is similar to that of acutepseudomembranous candidiasis.
Chronic atrophic candidiasis
Chronic atrophic candidiasis (denture stomatitis),as distinguished from acute atrophic candidiasis,occurs in areas occluded by dentures, such as thehard palate, and presents as erythema and edemabetween the dentures and oral mucosa (2).Restricted salivary flow may predispose to this dis-tribution. Twenty to sixty percent of denture
wearers are affected (5,27). Symptoms includeburning or a sore mouth. Patients with angularcheilitis may have unrecognized chronic atrophiccandidiasis (7).
Three clinical presentations have beendescribed in chronic atrophic candidiasis. In type I,local inflammation manifests as pinpoint hyper-emic macules. Type II appears as diffuse erythemaof part or the entirety of the denture-occluded area.Type III, or the granular type, most often involvesthe central hard palate or alveolar ridge formingpapillary hyperplasia (1,29). Confirmatory diagno-sis can be obtained by swabbing and staininginvolved tissue.
The differential diagnosis of chronic atrophiccandidiasis includes mechanical irritation, allergyto denture material, and bacterial infection (30).
Median rhomboid glossitis
Median rhomboid glossitis (glossal central papil-lary atrophy) appears clinically as a chronic, sym-metric, red, elliptic or rhomboid-shaped patch onthe mid-posterior dorsal tongue anterior to the cir-cumvallate papillae (5). On occasion, these lesionsappear exophytic (1). Biopsies of median rhom-boid glossitis reveal Candida in over 80% of lesions,and many cases resolve after treatment withtopical antifungal therapy (5). Smoking and the useof inhaled corticosteroids are most often associ-ated with median rhomboid glossitis.
Angular cheilitis
Angular cheilitis (perlèche, angular stomatitis)manifests as bilateral, bright red erythematous fis-sures at the angles of the mouth and can occur atany age (FIG. 4). Angular cheilitis may be fosteredby both local as well as systemic factors. Angularcheilitis has been associated with intraoralCandida infection of the pseudomembranous orerythematous types, cutaneous Staphylococcus orStreptococcus infection, isolated nutritional defi-ciencies, particularly with vitamin B12 or iron, andmouth breathing (5). In young children, angularcheilitis is associated with habitual lip licking,thumb sucking, or biting of the corners of themouth, whereas in older patients it occurs fromsagging at the commissures of the mouth (31).Wrinkles or congenital excessive-angle skin foldsat the oral commissures impart an increased riskfor angular cheilitis by creating a chronic, moist,intertriginous environment which fosters candidalovergrowth. The long-term use of ill-fitting den-tures accentuates this wrinkling by causing resorp-
FIG. 3. Acute atrophic candidiasis. Note minor componentof pseudomembranes at the periphery. Courtesy of ErrolCraig, MD, PhD, Walnut Creek, CA.
Sharon & Fazel
234

tion of the bone on which the dentures lay,reducing the vertical height of the lower face (5).These conditions result in saliva trapping or exces-sive saliva at the angles of the mouth. Incorrect useof dental floss can lead to local mechanical trauma,predisposing to angular cheilitis (32).
Angular cheilitis has also been associated withdiseases that cause enlarged lips, such as orofacialgranulomatosis. Cases of angular stomatitis relatedto staphylococcal infection have been in somecases shown to result from nasal carriage withspread to the angles of the mouth (33). Exfoliativecheilitis, presenting predominantly with crackingof the lower lip, has been associated with Candida,particularly in HIV-positive patients (34). Angularstomatitis refractory to treatment or chronicallyrecurring in a non-denture wearer should promptevaluation for HIV or another underlying immunedefect (7).
The treatment of angular cheilitis is most appro-priately tailored to its cause. Angular cheilitis sec-ondary to Candida infection should be treated withtopical antifungal creams (5). In patients with HIVgiven topical therapy for angular cheilitis, relapsesoccur more frequently than in those treated withsystemic antifungal therapy (35). To treat angularcheilitis caused by overclosure, petrolatum or lipbalm can be used as a mechanical barrier. In casesassociated with bacteria, topical mupirocin 2%ointment three to four times daily until resolution
can be helpful (36). Angular cheilitis resulting fromdeep orofacial grooves may be amenable to softtissue augmentation with fillers at the oral com-missures to correct the anatomic defect (37).
Linear gingival erythema
Linear gingival erythema manifests as a beefy reddiscrete line or punctate erythema of at least 2 mmwidth along the gingival margin (38). It mayencompass many teeth, or as little as one tooth,and can be accompanied by pain and bleeding (1).Although first described in patients with HIV, it hasalso been reported in healthy children (1). Thiscondition may be misdiagnosed as gingivitis. Somereports in the literature indicate that linear gingivalerythema may signify disease progression in HIV-positive individuals (39). To prevent progression tonecrotizing periodontitis, it is important to aggres-sively treat linear gingival erythema (40). Cases inwhich Candida is isolated should receive antifun-gal therapy. Patients should be instructed toperform proper hygiene techniques and rinsetwice daily with chlorhexidine gluconate 0.12%mouthwash. Concomitant dental referral is highlyrecommended for periodontal scaling and debri-dement (41).
Cheilo-candidiasis, chronic multifocalcandidiasis, and chronic mucocutaneouscandidiasis
Two additional variants, cheilo-candidiasis andchronic multifocal candidiasis, do not fit into thetraditional categories of oral candidiasis. Cheilo-candidiasis is an ulcerating lesion of the lowervermilion border of the lip. Chronic multifocal can-didiasis is characterized by erythematous plaquesin two or more areas of the mouth, most commonlyidentified in older male tobacco smokers. By defi-nition, lesions must be present for greater than 4weeks in the absence of known risk factors (1,30).Antifungal therapy is usually successful in treatingchronic multifocal candidiasis, although recur-rences are common without smoking cessation(30).
Chronic mucocutaneous candidiasis refers to aset of rare syndromes, at times with an identifiableimmune defect, in which the patient has persistentmucocutaneous findings including thrush and/or angular cheilitis, hyperkeratotic dystrophicnails, as well as acral and scalp involvementwith erythematous, hyperkeratotic, serpiginousplaques. These are syndromes that include autoim-mune polyendocrine syndrome type 1, in which
FIG. 4. Angular cheilitis. Courtesy of Errol Craig, MD, PhD,Walnut Creek, CA.
Oral candidiasis and angular cheilitis
235
chronic mucocutaneous candidiasis is followed bythe appearance of hypoparathyroidism and hypoa-drenalism (42). Symptoms usually begin early inlife and are often refractory to antifungal treatment(30).
Diagnosis
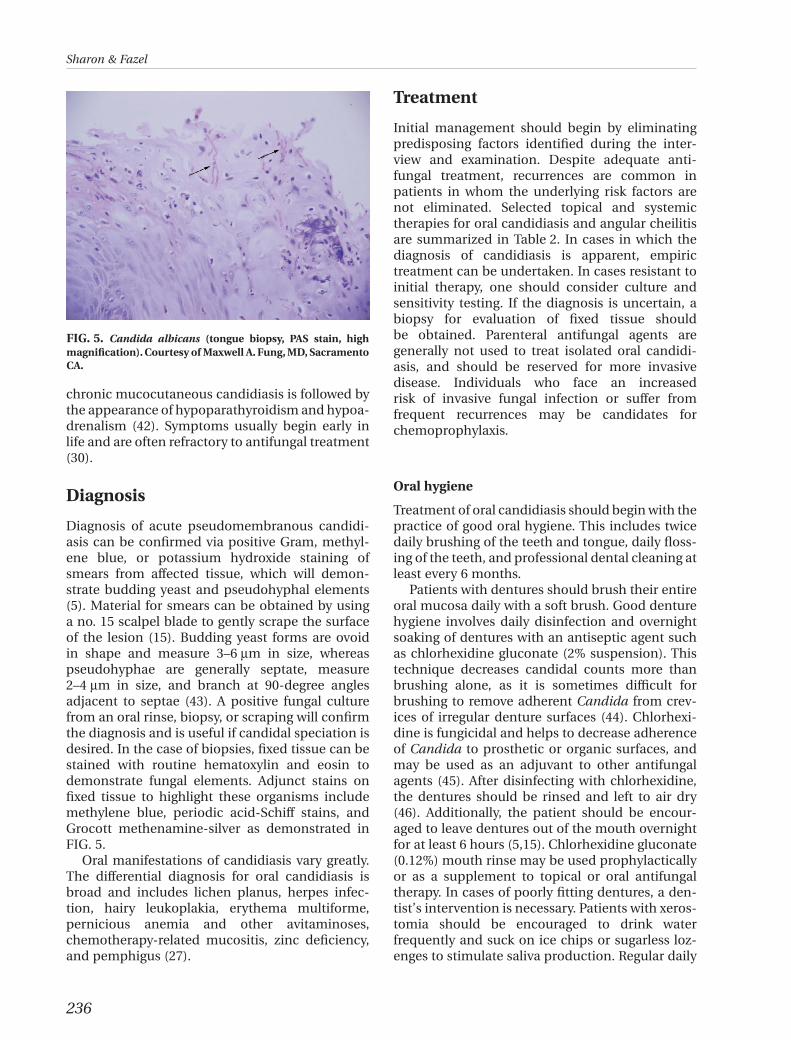
Diagnosis of acute pseudomembranous candidi-asis can be confirmed via positive Gram, methyl-ene blue, or potassium hydroxide staining ofsmears from affected tissue, which will demon-strate budding yeast and pseudohyphal elements(5). Material for smears can be obtained by usinga no. 15 scalpel blade to gently scrape the surfaceof the lesion (15). Budding yeast forms are ovoidin shape and measure 3–6 mm in size, whereaspseudohyphae are generally septate, measure2–4 mm in size, and branch at 90-degree anglesadjacent to septae (43). A positive fungal culturefrom an oral rinse, biopsy, or scraping will confirmthe diagnosis and is useful if candidal speciation isdesired. In the case of biopsies, fixed tissue can bestained with routine hematoxylin and eosin todemonstrate fungal elements. Adjunct stains onfixed tissue to highlight these organisms includemethylene blue, periodic acid-Schiff stains, andGrocott methenamine-silver as demonstrated inFIG. 5.
Oral manifestations of candidiasis vary greatly.The differential diagnosis for oral candidiasis isbroad and includes lichen planus, herpes infec-tion, hairy leukoplakia, erythema multiforme,pernicious anemia and other avitaminoses,chemotherapy-related mucositis, zinc deficiency,and pemphigus (27).
Treatment
Initial management should begin by eliminatingpredisposing factors identified during the inter-view and examination. Despite adequate anti-fungal treatment, recurrences are common inpatients in whom the underlying risk factors arenot eliminated. Selected topical and systemictherapies for oral candidiasis and angular cheilitisare summarized in Table 2. In cases in which thediagnosis of candidiasis is apparent, empirictreatment can be undertaken. In cases resistant toinitial therapy, one should consider culture andsensitivity testing. If the diagnosis is uncertain, abiopsy for evaluation of fixed tissue shouldbe obtained. Parenteral antifungal agents aregenerally not used to treat isolated oral candidi-asis, and should be reserved for more invasivedisease. Individuals who face an increasedrisk of invasive fungal infection or suffer fromfrequent recurrences may be candidates forchemoprophylaxis.
Oral hygiene
Treatment of oral candidiasis should begin with thepractice of good oral hygiene. This includes twicedaily brushing of the teeth and tongue, daily floss-ing of the teeth, and professional dental cleaning atleast every 6 months.
Patients with dentures should brush their entireoral mucosa daily with a soft brush. Good denturehygiene involves daily disinfection and overnightsoaking of dentures with an antiseptic agent suchas chlorhexidine gluconate (2% suspension). Thistechnique decreases candidal counts more thanbrushing alone, as it is sometimes difficult forbrushing to remove adherent Candida from crev-ices of irregular denture surfaces (44). Chlorhexi-dine is fungicidal and helps to decrease adherenceof Candida to prosthetic or organic surfaces, andmay be used as an adjuvant to other antifungalagents (45). After disinfecting with chlorhexidine,the dentures should be rinsed and left to air dry(46). Additionally, the patient should be encour-aged to leave dentures out of the mouth overnightfor at least 6 hours (5,15). Chlorhexidine gluconate(0.12%) mouth rinse may be used prophylacticallyor as a supplement to topical or oral antifungaltherapy. In cases of poorly fitting dentures, a den-tist’s intervention is necessary. Patients with xeros-tomia should be encouraged to drink waterfrequently and suck on ice chips or sugarless loz-enges to stimulate saliva production. Regular daily
FIG. 5. Candida albicans (tongue biopsy, PAS stain, highmagnification). Courtesy of Maxwell A. Fung, MD, SacramentoCA.
Sharon & Fazel
236

use of saliva substitutes is recommended. Sial-ogogues can also be employed to increase salivaryflow (47).
Topical antifungal agents
In cases of mild candidiasis, topical antifungalagents are the first line of therapy (1,48). Althoughthey often work quite well, treatment can beunsuccessful for a variety of reasons. The need forfrequent dosing, unpleasant taste, and consequentnoncompliance, as well as short contact timebetween the antifungal agent and the affected oraltissue, contribute to treatment failures.
Gentian violet
Gentian violet, a traditional topical fungicidalagent, was first used in the 1920s to treat oropha-
ryngeal candidiasis (2). It is an antiseptic agent thathas both anti-candidal and anti-staphylococcalproperties.
Gentian violet, 1.5 mL of a 0.5% solution twicedaily, is comparable to treatment with oral keto-conazole and may be superior to nystatin mouthrinses (49). Side effects include purple staining ofskin and clothes, skin irritation, and ulceration ofmucous membranes (50).
Nystatin
Nystatin, a polyene antifungal agent, has been oneof the most widely used topical antifungals (51). Itbinds to ergosterol, a sterol specific to fungal cellmembranes, forming artificial pores to alter mem-brane permeability (30). This results in the seepageof cellular components and eventual loss of cellviability.
Table 2. Medical treatment of oral candidiasis and angular cheilitisa,b
Agent Form Adult dosePregnancyrisk Adverse effects
Gentian violet Solution 1.5 mL BID C Purple staining; mucosal ulceration; skinirritation
Nystatin Suspension 100,000 U QID B/C Local skin irritation; adverse taste; nauseaand vomiting at high dosesCream TID-QID
Tablet 100,000 U TIDLozenge 100,000 U up to 5¥/day
7- to 14-day courseAmphotericin B Cream TID-QID 7–14 days B Minimal gastrointestinal absorption
Suspension 100 mg/mLClotrimazole Cream 1%, BID-TID ¥ 3–4 weeks B Local skin irritation; gastrointestinal upset
Solution 1%, TID-QID ¥ 2–3 weeks CTroche 10 mg, 5¥/day ¥ 14 days
Miconazole Cream 2%, BID ¥ 2–3 weeks C Skin irritation, burning, and macerationOintment 2%, BID ¥ 2–3 weeksOral gel 2%, TID-QID ¥ 2–3 weeks
Ketoconazole Cream 2%, BID-TID ¥ 2–4 weeks C Skin irritation and headacheTablet 200 mg QD-BID ¥ 2 weeks Nausea and vomiting; hepatotoxicity;
drug–drug interactionsFluconazole Tablet 50–200 mg QD or QW C Gastrointestinal upset; hepatotoxicity;
drug–drug interactionsItraconazole Capsule 100–200 mg QD-TID C Gastrointestinal upset; hepatotoxicity;
drug–drug interactionsSolution �loading dose of 200 mgTID ¥ 3 days
Posaconazole Suspension 100 mg BID ¥ 1 dayfollowed by 100 mg
C Gastrointestinal upset; hepatotoxicity;drug–drug interactions; neutropenia
QD ¥ 13 daysFor severe disease: 400 mg
BID ¥ 3 days followed by400 mg
QD-BID ¥ 4 weeks
aAdapted from Ellepola & Samaranayake (30).bOnly selected antifungal therapy presented.QD indicates once daily; QW, once weekly; BID, twice daily; TID, three times daily; QID, four times daily.
Oral candidiasis and angular cheilitis
237

Nystatin is available in several forms including a50% sucrose oral suspension, vaginal tablet, cream,ointment, and lozenge (pastille). Shortcomings ofthe oral suspension (100,000 U/mL, prescribedfour times daily for 7–14 days) include a shortcontact time, mild gastrointestinal disturbance,increased risk of dental caries, or worseningglucose intolerance. Vaginal tablets (100,000 U) areunflavored and lack a carbohydrate base, support-ing their use as an alternative formulation inpatients at risk for dental caries or in those withdiabetes. One tablet three times daily for 2 weeksshould be used. The lozenge (100,000 U), one totwo taken by mouth five times daily for 7–14 days,has a pleasant taste and provides a longer durationof action, if dissolved slowly (15). However, its highsugar content puts the patient at risk for develop-ing secondary caries and may exacerbate underly-ing diabetes mellitus. In patients with xerostomia,lozenges may be difficult to dissolve.
If the patient cannot tolerate the taste of nysta-tin, or if nausea and vomiting occur, alternativeagents such as clotrimazole troches may be usedinstead.
Nystatin and chlorhexidine, when combined,inactivate each other forming chlorhexidine–nystatin complexes and should not be used con-comitantly (52).
Amphotericin B
Amphotericin B, like nystatin, is a polyene antifun-gal medication. As an oral agent, it is poorlyabsorbed via the gastrointestinal tract. It is oftenadministered intravenously in the case of systemicfungal infections. Although less popular than nys-tatin because of decreased familiarity and associa-tion with significant adverse systemic effects whenadministered intravenously, amphotericin B canbe used to adequately treat Candida of the oralcavity and is available in the United States as acream, lotion, and ointment (1). The patient shouldbe instructed to apply amphotericin B to theaffected areas three to four times daily for up to 2weeks (1,30).
Clotrimazole
Clotrimazole is a fungistatic topical imidazoleantifungal agent that prevents the synthesis ofergosterol in the fungal cell membrane. It ismanufactured as an oral or vaginal troche, cream,and solution, and has the advantage of both anti-candidal and anti-staphylococcal activities (1,30).Clotrimazole troches have a more palatable taste
than nystatin, but are also formulated with a dex-trose base and, like nystatin, increase the risk fordental caries (15).
Clotrimazole cream should be applied to theinvolved area of the oral mucosa or angles of themouth two to three times daily for 3 weeks. Whenusing the topical solution, the patient should beinstructed to swish and spit one teaspoonful threeto four times daily for 3 weeks. If the troche (10 mg)is preferred, the patient should hold it in the mouthwith a 15- to 30-minute dissolution time five timesdaily (2,48). However, frequent dosing, particularlywith the troche and solution, is associated withpoor adherence.
Clotrimazole troches (10 mg) three times dailyhave been successful for the prophylaxis of oralcandidal infections in leukemic patients receivingchemotherapy (53).
Adverse reactions are for the most part limitedto gastrointestinal upset and minor local skinirritation.
Miconazole
Miconazole is an imidazole antifungal agent thathas anti-candidal and anti-staphylococcal proper-ties. Like clotrimazole, it may be used for the treat-ment of angular cheilitis (1,30). For the treatmentof oral candidiasis, miconazole is available in gel(Zeasorb-AF), cream, ointment, and lacquer for-mulations. The cream should be applied to theaffected area twice daily for 2–3 weeks, and the gelshould be applied three to four times daily for 2–4weeks. The lacquer may be painted over denture-fitting surfaces in patients with a history of denturestomatitis, thus slowly delivering anti-candidaltherapy for prolonged periods of time. Decreasednumbers of Candida on these surfaces with oneapplication have been documented (54). Prior tolacquer application, the patient should thoroughlybrush the occlusal denture surfaces under coldrunning water. It is recommended that the patientpaint each denture with 1 g of lacquer (containing55 mg/g of miconazole) and permit the lacquer todry for 1 hour prior to denture insertion. Thisshould be repeated two more times at Days 7 and14 (55).
Miconazole is well tolerated. Side effects arelimited to nausea and local skin irritation whenused topically.
Ketoconazole
Ketoconazole, like clotrimazole and miconazole,is an imidazole antifungal medication. However,
Sharon & Fazel
238

ketoconazole does not possess antibacterial activ-ity. It is available topically as a 2% cream. Thepatient should apply the cream two to three timesdaily to affected areas for 14–28 days. Topical keto-conazole is well tolerated, and side effects arelimited to skin irritation and headache.
Systemic oral antifungal agents
Systemic azoles are used to treat oral candidiasisrefractory to treatment with topical antimycoticagents or in patients who are immunocompro-mised or at risk of disseminated disease (5).Parenteral antimycotic agents such as flucytosine,amphotericin B, and the echinocandins (e.g.,caspofungin) are generally reserved for the treat-ment of invasive candidiasis (48).
Azoles are divided into the imidazoles (clotrima-zole, miconazole, ketoconazole) and triazoles(fluconazole, itraconazole, posaconazole, vori-conazole) (30,48). Azoles are fungistatic and blockthe synthesis of ergosterol in fungal cell mem-branes by inhibiting the 14a-demethylation oflanosterol (56). Imidazoles also disturb fungal oxi-dative enzymes, resulting in a lethal accumulationof hydrogen peroxide (30).
Systemic antifungals, such as ketoconazole anditraconazole, are potent inhibitors of the cyto-chrome P-450 hepatic metabolism pathways. Theycan result in harmful drug–drug interactions andhepatitis, and may be associated with birth defects(18). Therefore, a patient’s existing medication listshould be reviewed for potential adverse drug–drug interactions.
Ketoconazole
Oral ketoconazole is a weak base and is bestabsorbed at normal acidic gastric pH. Absorption isdecreased with the concomitant use of antacids,histamine-receptor blockers, or proton pumpinhibitors. In conditions with impaired gastricsecretion and in patients with achlorhydria,absorption is decreased thus limiting effectiveness.
Ketoconazole (200 mg tablet) is administeredonce or twice daily for 2 weeks (1). The mostcommon adverse effects are nausea and vomiting.Ketoconazole can suppress cytochrome P-450-mediated metabolism of several medications suchas cyclosporine, leading to increased activemetabolites (57). Ketoconazole can block steroidsynthesis, decrease the production of testosterone,and cause hair loss. It may also be teratogenic andis advisable to avoid in pregnancy. Idiosyncratichepatotoxicity may occur, and can be asymptom-
atic, manifesting as reversible elevations of serumaspartate and alanine aminotransferases (30). Fatalnephrotoxicity and hepatotoxicity have beenreported. Care should be taken when prescribingthese agents to patients with liver or kidney impair-ment. A hepatic function panel may be monitoredperiodically in anyone receiving prolonged therapybeyond 2 weeks or in high-risk populations such asthose with known liver impairment (58). Currently,routine hepatic monitoring is not universally rec-ommended unless the patient develops signs ofhepatotoxicity including nausea, vomiting, anor-exia, abdominal pain, fatigue, jaundice, or darkurine.
Fluconazole
Fluconazole is a water-soluble triazole that, unlikeketoconazole, is well absorbed from the gas-trointestinal tract at any gastric pH (56). Its oralbioavailability is approximately 90% of intravenousadministration (48). It is only weakly plasmaprotein bound and therefore has good uptake intotissue (1). Distinct from other azoles, fluconazoleis minimally metabolized and is excreted via thekidney 80% unchanged, therefore negligibly affect-ing hepatic metabolism (1,30,59). It may be pre-scribed in doses of 50, 100, 150, or 200 mg, or3 mg/kg daily for 7–14 days for oral candidiasis,with a 200 mg loading dose (1,48). Overall, flucona-zole is well tolerated and generates only mild sideeffects related to gastrointestinal discomfort andheadache. In rare instances, fluconazole may beassociated with abnormal liver enzymes. Althoughthere is no universal consensus, some authorssuggest obtaining a baseline hepatic functionpanel with periodic monthly monitoring (60).Animal studies have suggested an association withfetal malformation (61). Fluconazole has fewerdrug–drug interactions than does ketoconazole.However, a complete list of potential drug interac-tions should be identified prior to administration.
There is an increasing trend toward fluconazole-resistant candidal species (C.krusei and C.glabrata)(15,18). Fluconazole resistance has been detected inexcess of 20% in some studies (62,63). Higher dosesof fluconazole (up to 600 mg daily) or alternativeazoles may be necessary in such cases (30).
Fluconazole may be used for chronic suppres-sion of oropharyngeal candidiasis in doses of 50 or100 mg daily, 100 or 200 mg three times weekly,150 mg weekly, or as needed (48,64,65). Continu-ous prophylaxis with fluconazole does not result inhigher resistance rates than as needed dosing fororal candidiasis (66).
Oral candidiasis and angular cheilitis
239

Itraconazole
Itraconazole is a lipophilic triazole and is particu-larly beneficial for the treatment of fluconazole-resistant candidal strains such as C. krusei or C.glabrata, with response rates of 64–80% (30,67).The capsule form requires acidic pH for absorption(1). The patient should be instructed to take itra-conazole capsules with food, as its bioavailabilityis two- to threefold increased when compared toingestion on an empty stomach (68). Acidic bever-ages (carbonated beverages, cranberry juice) canheighten gastrointestinal absorption (69). Thesolution form (10 mg/mL) has approximately 30%greater bioavailability than the capsule, and doesnot require acidic pH for absorption (68). The solu-tion and capsule formulations may be prescribedat doses of 100–200 mg daily for 14 days. A loadingdose of 200 mg by mouth three times daily for 3days should be administered in cases of severerecalcitrant oropharyngeal disease (48).
Itraconazole is hepatically metabolized andexcreted via the biliary tract. It is generally welltolerated, although adverse effects include asymp-tomatic hepatitis, hypokalemia, headache, dizzi-ness, and gastrointestinal disturbance (1).
Posaconazole
Posaconazole is an extended-spectrum triazolereserved for fluconazole-resistant candidal strainsor refractory disease. Improvement was noted in75% of patients with refractory oropharyngeal can-didiasis (70). It is formulated as a suspension(40 mg/mL). A loading dose of 100 mg should begiven twice daily for the first day, followed by a doseof 100 mg daily for 13 days (71). In refractory orcomplicated cases, posaconazole 400 mg twicedaily for 3 days, followed by 400 mg daily or twicedaily for 25–28 days may be necessary (48). Posa-conazole has a greater bioavailability when admin-istered with food.
Posaconazole is metabolized by the liver. Com-pared to other azole agents, it exerts a limited effecton cytochrome P-450 isozymes. Posaconazole isgenerally well-tolerated. Most common adverseeffects involve gastrointestinal upset, althoughneutropenia was noted in 7% of patients (71).
Prophylaxis
Prophylactic anti-candidal treatment is indicatedfor patients who have recurrent oral candidiasis,who are receiving prolonged antibiotic treatment,
or who are immunosuppressed (transplant, che-motherapy, systemic immunosuppressives, HIV,low CD4 counts). Continuous antifungal therapyreduces intraoral candidal counts and resultantinfections (5). In patients receiving bone marrowtransplants, chlorhexidine has been shown to beeffective in decreasing the risk of oral candidiasis(72).
There is no collective consensus on a standardprophylactic regimen for oral candidiasis. Themost appropriate therapy depends on the speciesof Candida isolated, as well as the underlying pre-disposing conditions, frequency of recurrences,and ongoing antibiotic or immunosuppressivetherapy. Recommended regimens include, but arenot limited to, rinsing with chlorhexidine glucon-ate 0.12% mouthwash twice daily, using clotrima-zole troches (10 mg) three times daily, oradministering fluconazole 50 or 100 mg daily, or200 mg between one and three times weekly(11,53,73).
Conclusion
Oral candidiasis and angular cheilitis are fre-quently encountered in clinical practice. Althoughacute pseudomembranous oral candidiasis isreadily recognized, other forms of oral candidiasismay present a greater diagnostic challenge. Oralcandidiasis may be a clue to concurrent unidenti-fied systemic diseases. In many patients, candidi-asis can cause oral discomfort, leading todecreased oral intake predisposing to nutritionaldeficiency.
Uncomplicated oral candidiasis and angularcheilitis generally respond to treatment, althoughrelapses often occur because of reduced compli-ance, poor oral hygiene, and failure to address pre-disposing factors. Treatment should be tailored tothe individual patient’s needs and preferences.
The prognosis of oral candidiasis in mostpatients is good. In immunosuppressed or debili-tated populations, however, oropharyngeal can-didiasis places the host at risk for developinginvasive disease. Therefore, it is important to rec-ognize and treat oral candidiasis.
References
1. Samaranayake LP, Keung Leung W, Jin L. Oral mucosalfungal infections. Periodontol 2000 2009: 49: 39–59.
2. Vazquez JA, Sobel JD. Mucosal candidiasis. Infect Dis ClinNorth Am 2002: 16: 793–820, v.
3. Arendorf TM, Walker DM. The prevalence and intra-oraldistribution of Candida albicans in man. Arch Oral Biol1980: 25: 1–10.
Sharon & Fazel
240

4. Wilkieson C, Samaranayake LP, MacFarlane TW, Lamey PJ,MacKenzie D. Oral candidosis in the elderly in long termhospital care. J Oral Pathol Med 1991: 20: 13–16.
5. Akpan A, Morgan R. Oral candidiasis. Postgrad Med J 2002:78: 455–459.
6. Abu-Elteen KH, Abu-Alteen RM. The prevalence ofCandida albicans populations in the mouths of completedenture wearers. New Microbiol 1998: 21: 41–48.
7. Scully C, el-Kabir M, Samaranayake LP. Candida and oralcandidosis: a review. Crit Rev Oral Biol Med 1994: 5: 125–157.
8. Barlow AJ, Chattaway FW. Observations on the carriage ofCandida albicans in man. Br J Dermatol 1969: 81: 103–106.
9. Arendorf TM, Walker DM. Oral candidal populations inhealth and disease. Br Dent J 1979: 147: 267–272.
10. Davenport JC. The oral distribution of Candida in denturestomatitis. Br Dent J 1970: 129: 151–156.
11. Pankhurst CL. Candidiasis (oropharyngeal). Clin Evid(Online) 2009: March 18.
12. Pereira-Cenci T, Del Bel Cury AA, Crielaard W, Ten Cate JM.Development of Candida-associated denture stomatitis:new insights. J Appl Oral Sci 2008: 16: 86–94.
13. Vazquez JA, Sobel JD. Candidiasis. In: Dismukes WE,Pappas PG, Sobel JD, eds. Clinical mycology. New York, NY:Oxford University Press, 2003: 143–187.
14. Wingard JR. Importance of Candida species other than C.albicans as pathogens in oncology patients. Clin Infect Dis1995: 20: 115–125.
15. Greenspan D. Treatment of oropharyngeal candidiasis inHIV-positive patients. J Am Acad Dermatol 1994: 31: S51–55.
16. Barchiesi F, Morbiducci V, Ancarani F, Scalise G. Emer-gence of oropharyngeal candidiasis caused by non-albicans species of Candida in HIV-infected patients. Eur JEpidemiol 1993: 9: 455–456.
17. Habif TP. Superficial Fungal Infections. In: Habif TP, ed.Clinical dermatology, 4th ed. Amsterdam: Elsevier HealthSciences, 2004: 409–456.
18. Darouiche RO. Oropharyngeal and esophageal candidiasisin immunocompromised patients: treatment issues. ClinInfect Dis 1998: 26: 259–274.
19. Liu X, Liu H, Guo Z, Luan W. Association of asymptomaticoral candidal carriage, oral candidiasis and CD4 lympho-cyte count in HIV-positive patients in China. Oral Dis 2006:12: 41–44.
20. Samaranayake LP. Oral mycoses in HIV infection. Oral SurgOral Med Oral Pathol 1992: 73: 171–180.
21. Martins MD, Lozano-Chiu M, Rex JH. Declining ratesof oropharyngeal candidiasis and carriage of Candidaalbicans associated with trends toward reduced rates ofcarriage of fluconazole-resistant C. albicans in humanimmunodeficiency virus-infected patients. Clin Infect Dis1998: 27: 1291–1294.
22. Ozog DM, Gogstetter DS, Scott G, Gaspari AA. Minocycline-induced hyperpigmentation in patients with pemphigusand pemphigoid. Arch Dermatol 2000: 136: 1133–1138.
23. Goulden V, Glass D, Cunliffe WJ. Safety of long-term high-dose minocycline in the treatment of acne. Br J Dermatol1996: 134: 693–695.
24. Oliver DE, Shillitoe EJ. Effects of smoking on the prevalenceand intraoral distribution of Candida albicans. J Oral Pathol1984: 13: 265–270.
25. Soysa NS, Ellepola AN. The impact of cigarette/tobaccosmoking on oral candidosis: an overview. Oral Dis 2005: 11:268–273.
26. Cannon RD, Holmes AR, Mason AB, Monk BC. OralCandida: clearance, colonization, or candidiasis? J DentRes 1995: 74: 1152–1161.
27. Janik MP, Heffernan MP. Yeast Infections: Candidiasis andTinea (Pityriasis) Versicolor. In: Wolff K, Goldsmith LA, KatzSI, Gilchrest BA, Paller AS, Leffell DJ, eds. Fitzpatrick’s der-matology in general medicine. New York, NY: McGraw-HillMedical, 2008: 1822–1830.
28. Samaranayake LP, Holmstrup P. Oral candidiasis andhuman immunodeficiency virus infection. J Oral PatholMed 1989: 18: 554–564.
29. Golecka M, Oldakowska-Jedynak U, Mierzwinska-Nastalska E, Adamczyk-Sosinska E. Candida-associateddenture stomatitis in patients after immunosuppressiontherapy. Transplant Proc 2006: 38: 155–156.
30. Ellepola AN, Samaranayake LP. Oral candidal infectionsand antimycotics. Crit Rev Oral Biol Med 2000: 11: 172–198.
31. Appleton SS. Candidiasis: pathogenesis, clinical character-istics, and treatment. J Calif Dent Assoc 2000: 28: 942–948.
32. Kahana M, Yahalom R, Schewach-Millet M. Recurrentangular cheilitis caused by dental flossing. J Am Acad Der-matol 1986: 15: 113–114.
33. MacFarlane TW, Helnarska SJ. The microbiology of angularcheilitis. Br Dent J 1976: 140: 403–406.
34. Reichart PA, Weigel D, Schmidt-Westhausen A, Pohle HD.Exfoliative cheilitis (EC) in AIDS: association with Candidainfection. J Oral Pathol Med 1997: 26: 290–293.
35. Pons V, Greenspan D, Debruin M. Therapy for oropharyn-geal candidiasis in HIV-infected patients: a randomized,prospective multicenter study of oral fluconazole versusclotrimazole troches. The multicenter study group. J AcquirImmune Defic Syndr 1993: 6: 1311–1316.
36. de Wet PM, Rode H, van Dyk A, Millar AJ. Perianal candido-sis – a comparative study with mupirocin and nystatin. IntJ Dermatol 1999: 38: 618–622.
37. Chernosky ME. Collagen implant in management of per-leche (angular cheilosis). J Am Acad Dermatol 1985: 12:493–496.
38. Odden K, Schenck K, Koppang H, Hurlen B. Candidal infec-tion of the gingiva in HIV-infected persons. J Oral PatholMed 1994: 23: 178–183.
39. Velegraki A, Nicolatou O, Theodoridou M, Mostrou G,Legakis NJ. Paediatric AIDS-related linear gingivalerythema: a form of erythematous candidiasis? J OralPathol Med 1999: 28: 178–182.
40. Barr CE. Periodontal problems related to HIV-1 infection.Adv Dent Res 1995: 9: 147–151.
41. Reznik DA. Oral manifestations of HIV disease. Top HIVMed 2005: 13: 143–148.
42. Shikama N, Nusspaumer G, Hollander GA. Clearing theAIRE: on the pathophysiological basis of the autoimmunepolyendocrinopathy syndrome type-1. Endocrinol MetabClin North Am 2009: 38: 273–288, vii.
43. Hinshaw M, Longley BJ. Fungal Diseases. In: Lever WF,Elder DE, eds. Lever’s histopathology of the skin. Philadel-phia, PA: Lippincott Williams & Wilkins, 2009: 597–600.
44. Odman PA. The effectiveness of an enzyme-containingdenture cleanser. Quintessence Int 1992: 23: 187–190.
45. Lal K, Santarpia RP 3rd, Pollock JJ, Renner RP. Assessmentof antimicrobial treatment of denture stomatitis using an invivo replica model system: therapeutic efficacy of an oralrinse. J Prosthet Dent 1992: 67: 72–77.
46. Douglas LJ. Surface composition and adhesion of Candidaalbicans. Biochem Soc Trans 1985: 13: 982–984.
Oral candidiasis and angular cheilitis
241
47. Aframian DJ, Helcer M, Livni D, Robinson SD, Markitziu A,Nadler C. Pilocarpine treatment in a mixed cohort of xeros-tomic patients. Oral Dis 2007: 13: 88–92.
48. Pappas PG, Kauffman CA, Andes D, et al. Clinical practiceguidelines for the management of candidiasis: 2009 updateby the Infectious Diseases Society of America. Clin InfectDis 2009: 48: 503–535.
49. Nyst MJ, Perriens JH, Kimputu L, Lumbila M, Nelson AM,Piot P. Gentian violet, ketoconazole and nystatin inoropharyngeal and esophageal candidiasis in Zairian AIDSpatients. Ann Soc Belg Med Trop 1992: 72: 45–52.
50. Balabanova M, Popova L, Tchipeva R. Dyes in dermatology.Clin Dermatol 2003: 21: 2–6.
51. Epstein JB. Antifungal therapy in oropharyngeal mycoticinfections. Oral Surg Oral Med Oral Pathol 1990: 69: 32–41.
52. Barkvoll P, Hurlen B. Conventional treatment of oral can-didiasis – new aspects. Nor Tannlaegeforen Tid 1989: 99:116–119.
53. Cuttner J, Troy KM, Funaro L, Brenden R, Bottone EJ. Clot-rimazole treatment for prevention of oral candidiasis inpatients with acute leukemia undergoing chemotherapy.Results of a double-blind study. Am J Med 1986: 81: 771–774.
54. Konsberg R, Axell T. Treatment of Candida-infecteddenture stomatitis with a miconazole lacquer. Oral SurgOral Med Oral Pathol 1994: 78: 306–311.
55. Dias AP, Samaranayake LP, Lee MT. Miconazole lacquer inthe treatment of denture stomatitis: clinical and microbio-logical findings in Chinese patients. Clin Oral Investig 1997:1: 47–52.
56. Como JA, Dismukes WE. Oral azole drugs as systemic anti-fungal therapy. N Engl J Med 1994: 330: 263–272.
57. Gupta AK, Sauder DN, Shear NH. Antifungal agents: anoverview. Part I. J Am Acad Dermatol 1994: 30: 677–698;quiz 698–700.
58. Hay RJ. Risk/benefit ratio of modern antifungal therapy:focus on hepatic reactions. J Am Acad Dermatol 1993: 29:S50–54.
59. Brammer KW, Coakley AJ, Jezequel SG, Tarbit MH. The dis-position and metabolism of [14C]fluconazole in humans.Drug Metab Dispos 1991: 19: 764–767.
60. Gupta AK, Sauder DN, Shear NH. Antifungal agents: anoverview. Part II. J Am Acad Dermatol 1994: 30: 911–933;quiz 916–934.
61. Aleck KA, Bartley DL. Multiple malformation syndrome fol-lowing fluconazole use in pregnancy: report of an addi-tional patient. Am J Med Genet 1997: 72: 253–256.
62. Maenza JR, Merz WG, Romagnoli MJ, Keruly JC, Moore RD,Gallant JE. Infection due to fluconazole-resistant Candida
in patients with AIDS: prevalence and microbiology. ClinInfect Dis 1997: 24: 28–34.
63. Maninder J, Usha A. Isolation, characterization and anti-fungal susceptibility pattern of Candida species causingoropharyngeal candidiasis in HIV positive patients. JCommun Dis 2008: 40: 177–181.
64. Leen CL, Dunbar EM, Ellis ME, Mandal BK. Once-weeklyfluconazole to prevent recurrence of oropharyngeal can-didiasis in patients with AIDS and AIDS-related complex:a double-blind placebo-controlled study. J Infect 1990:21: 55–60.
65. Corvo R, Amichetti M, Ascarelli A, et al. Effects of flucona-zole in the prophylaxis of oropharyngeal candidiasis inpatients undergoing radiotherapy for head and necktumour: results from a double-blind placebo-controlledtrial. Eur J Cancer Care (Engl) 2008: 17: 270–277.
66. Goldman M, Cloud GA, Wade KD, et al. A randomized studyof the use of fluconazole in continuous versus episodictherapy in patients with advanced HIV infection and ahistory of oropharyngeal candidiasis: AIDS Clinical TrialsGroup Study 323/Mycoses Study Group Study 40. ClinInfect Dis 2005: 41: 1473–1480.
67. Saag MS, Fessel WJ, Kaufman CA, et al. Treatment offluconazole-refractory oropharyngeal candidiasis withitraconazole oral solution in HIV-positive patients. AIDSRes Hum Retroviruses 1999: 15: 1413–1417.
68. Barone JA, Koh JG, Bierman RH, et al. Food interaction andsteady-state pharmacokinetics of itraconazole capsules inhealthy male volunteers. Antimicrob Agents Chemother1993: 37: 778–784.
69. Lange D, Pavao JH, Wu J, Klausner M. Effect of a cola bev-erage on the bioavailability of itraconazole in the presenceof H2 blockers. J Clin Pharmacol 1997: 37: 535–540.
70. Skiest DJ, Vazquez JA, Anstead GM, et al. Posaconazolefor the treatment of azole-refractory oropharyngeal andesophageal candidiasis in subjects with HIV infection. ClinInfect Dis 2007: 44: 607–614.
71. Vazquez JA. Role of posaconazole in the management oforopharyngeal and esophageal candidiasis. Ther Clin RiskManag 2007: 3: 533–542.
72. Ferretti GA, Ash RC, Brown AT, Largent BM, Kaplan A,Lillich TT. Chlorhexidine for prophylaxis against oral infec-tions and associated complications in patients receivingbone marrow transplants. J Am Dent Assoc 1987: 114: 461–467.
73. Just-Nubling G, Gentschew G, Meissner K, et al. Flucona-zole prophylaxis of recurrent oral candidiasis in HIV-positive patients. Eur J Clin Microbiol Infect Dis 1991: 10:917–921.
Sharon & Fazel
242

Copyright of Dermatologic Therapy is the property of Wiley-Blackwell and its content may not be copied or
emailed to multiple sites or posted to a listserv without the copyright holder's express written permission.
However, users may print, download, or email articles for individual use.