assessment of the influence of development …
TRANSCRIPT

1
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES
ON HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES
IN BENIN CITY
BY
DR OMONYEMEN BOSEDE BELLO
DEPARTMENT OF COMMUNITY HEALTH,
UNIVERSITY OF BENIN TEACHING HOSPITAL,
BENIN CITY, EDO STATE.
SUBMITTED TO
THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA
IN PARTIAL FULFILMENT FOR THE REQUIREMENTS
FOR THE AWARD OF FINAL FELLOWSHIP OF THE MEDICAL COLLEGE
IN PUBLIC HEALTH
AUGUST, 2015
DECLARATION

2
I hereby declare that this work is original and was done under appropriate supervision. This
work has not been submitted in part or in full for any other examination or publication.
………………………………….
Researcher
Dr Omonyemen Bosede Bello
CERTIFICATION

3
I certify that this work was carried out by Dr Omonyemen Bosede Bello of the Department
of Community Health, University of Benin Teaching Hospital, Benin City, under my
supervision.
________________________
Supervisor
PROF. O. H. OKOJIE
MBBS, FMCPH, FWACP
Professor/Consultant
Department of Community Health,
University of Benin/University of Benin Teaching Hospital,
Benin City.
Nigeria.
__________________________
Supervisor
DR V. O. OMUEMU
MBBS, MPH, FMCPH, MWACP
Associate Professor/Consultant
Department of Community Health,
University of Benin/University of Benin Teaching Hospital,
Benin City.
Nigeria.
_______________________
Head of Department
DR V. O. OMUEMU
MBBS, MPH, FMCPH, MWACP
Associate Professor/Consultant
Department of Community Health,
University of Benin/University of Benin Teaching Hospital,
Benin City.
Nigeria.
ACKNOWLEDGEMENTS

4
I acknowledge first and foremost the Lord God Almighty for His benevolence in the course
of my study.
My profound and unalloyed gratitude goes to my project supervisors Prof. O. H. Okojie and
Dr. (Mrs.) V. O. Omuemu who both tirelessly and painstakingly supervised this work. My
sincere thanks go to Prof. (Mrs.) E. C. Isah, Prof. V. Wagbatsoma and Prof. (Mrs.) A. N.
Ofili for their motherly advice and support and Dr. A. R. Isara for his mentorship and
contributions to this dissertation. I also wish to extend my gratitude to all my consultants:
Dr. O. A. Adeleye, Dr. J. C. Chiwuzie, Chief (Dr.) S. U. Ighedosa, Dr. V. Y. Adam, Dr. G.
Owoeye, Dr. A. Obi and Dr. E. O. Ogboghodo for their support and encouragement
throughout my training.
I also appreciate my darling husband, Peter for his encouragement and support in making
this work a reality, my beloved children, David, Vicky and Sammy, my sister in-law, Mary
and my dear mum, Mrs F. O. Aimufia for their prayers and support. I am especially grateful
to Dr. Seye Abimbola, my fellow residents and friends for their prayers and encouragement.
Special thanks to my colleagues Dr. Adesuwa Aigbokhaode, Dr. P. W. Okojie, Dr. Greg
Oko-Oboh, Dr. N. Mokogwu, Dr. Obiageli Okwara, Dr. E.Eseigbe and Dr C. Kanu and for
their tireless support and encouragement.
My sincere appreciation goes to the Chairmen, PHC coordinators and the various
community leaders, of Oredo and Ikpoba Okha Local Government Areas for their
permission to carry out this study in their Local Government Areas, and communities. My
sincere thanks also goes to the Edo State focal person of the National Primary Healthcare
Development Agency (NPHCDA), heads of the Primary Health Centres, all the respondents
in this study as well as my research assistants.

5
TABLE OF CONTENTS
Title Page - - - - - - - - - i
Declaration - - - - - - - - - ii
Certification - - - - - - - - - iii
Acknowledgements - - - - - - - - iv
Table of Content - - - - - - - - v
List of Tables - - - - - - - - vii
List of Figures - - - - - - - - ix
List of Abbreviations - - - - - - - - x
Definition of Terms - - - - - - - - xiii
Abstract - - - - - - - - - xvii
Chapter One: Introduction - - - - - - - 1
Background - - - - - - - - 1
Statement of the Problem - - - - - - 8
Justification of the Study - - - - - - 12
Research Questions - - - - - - - 13
Aim and Objectives - - - - - - - 15
Chapter Two: Literature Review - - - - - - 16

6
Chapter Three: Materials and Methods - - - - - 36
Chapter Four: Results - - - - - - - - 60
Chapter Five: Discussion - - - - - - - 115
Conclusion - - - - - - - - - 121
Recommendations - - - - - - - - 123
References - - - - - - - - - 127
Appendices - - - - - - - - - 140

7
LIST OF TABLES
Table 4.1.1 Socio-demographic Characteristics of mothers of under-five children 61
Table 4.1.2 Monthly income of mothers of under-five children 63
Table 4.1.3 Occupational and educational status of the spouse/partners of the mothers
Of under-five children 64
Table 4.1.4 Monthly income of the spouse/partners of the mothers of under-five
Children 65
Table 4.1.5 Socio-demographic characteristics of PHC workers 66
Table 4.2.1 Composition of village and ward development committees 68
Table 4.4.1 Readiness of PHC facilities in terms of Infrastructure, Equipment,
Personnel and Composite scores 82
Table 4.4.2 Correlation between VDCs and WDCs and readiness of PHCs 84
Table 4.4.3 Scores for Functionality of VDCs/WDCs and readiness of PHCs to
deliver some components of the WMHCP 85
Table 4.4.5 Correlation between functionality of VDCs/WDCs and readiness of
PHCs to deliver some components of the WMHCP 86
Table 4.5.1 General utilization of PHC services by the respondents and households 87
Table 4.5.2 Household utilization of maternal health services 89
Table 4.5.3 Utilization of child survival services for the last child 91
Table 4.5.4 Vaccines received in the health centre by the respondent’s last child 92
Table 4.5.5 Household utilization of health education and community mobilization
Services 94
Table 4.6.1 Performance of PHC workers with respect to the delivery of maternal and
Newborn health services 98
Table 4.6.2 Performance of PHC workers with respect to the delivery of child survival
Services
101

8
Table 4.6.3 Performance of PHC workers with respect to the delivery of health
Education and community mobilization services
103
Table 4.7.1 Scores for performance of PHC workers and household utilization of PHC
facilities
107
Table 4.7.2 Correlation (Spearman’s rho) between performance of PHC workers and
Household utilization of PHC facilities
108
Table 4.8.1 Percentage score for household utilization of PHC services and
Composition and functionality of Development Committees
109
Table 4.8.2 Correlation (Spearman’s rho) of composition and Functionality of
development committees with household utilization of PHC services
104

9
LIST OF FIGURES
Fig. 4.2.1 Composition of village development committees 70
Fig. 4.2.2 Composition of ward development committees based on composite
Scores 71
Fig. 4.2.3 Functionality of Village Development Committees 77
Fig. 4.2.4 Functionality of Ward Development Committees 78
Fig. 4.2.5 Composition and functionality of Village Development Committees 79
Fig 4.6.1 Composition and functionality of Ward Development Committees
105
Fig. 4.6.2 Overall performance of PHC workers in the delivery of some components
Of the WMHCP
106

10
LIST OF ABBREVIATIONS
CEMID Centre for Empowerment, Innovation and Development
CHEW Community Health Extension Worker
CHO Community Health Officer
CHW Community Health Worker
CLP Chars Livelihood Programme
CORPS Community Resource Persons
DHS District Health System
DM&HO District Medical and Health Officer
DRF Drug Revolving Fund
Edo SMOH Edo State Ministry of Health
FGD Focus Group Discussion
FMOH Federal Ministry of Health
GPEI Global Polio Eradication Initiative
HEF Health Equity Fund

11
HFOMC Health Facility Operation and Management Committee
IMR Infant Mortality Rate
INLOGOS Institute of Local Governance Studies
IPTP Intermittent Preventive Treatment in Pregnancy
JCHEW Junior Community Health Extension Worker
KII Key Informant Interview
KOD Kirivong Operational District
LGA Local Government Area
MDG Millennium Development Goal
MICS Multiple Indicator Cluster Survey
MMR Maternal Mortality Rate
MSS Midwives Service Scheme
NBS National Bureau of Statistics
NPHCDA National Primary Health Care Development Agency
NPC National Population Commission
NSHDP National Strategic Health Development Plan
PHC Primary Health Care
SSHDP State Strategic Health Development Plan
U5MR Under-five Mortality Rate

12
UNFPA United Nations Population Fund
UNICEF United Nations Children’s Fund
VDC Village Development Committee
VHW Village Health Worker
WDC Ward Development Committee
WHO World Health Organization
WHS Ward Health System
WMHCP Ward Minimum Health Care Package

13
DEFINITION OF TERMS
Active Participation: This is a situation where the people acknowledge their own health
problems, are able to identify the need for their solution or reduction, draw out plans of
action according to priority, and with the resources available, organize and implement the
programmes, and monitor and control their progress, periodically evaluate and do
reprogramming.
Advocacy: The act of taking a position on an issue, and initiating actions in a deliberate
attempt to influence private and public policy choices.
Community: A group of people that have some sense of shared identity and belonging,
often within a given geographic and political context.
Community Development: The planned evolution of all aspects of community well-being
(economic, social, environmental and cultural). It is a process whereby community members
come together to take collective action and generate solutions to common problems.
Community Engagement: The process of working collaboratively with groups of people
affiliated by geographic proximity, special interests, or similar situations with respect to
issues affecting their well-being.
Community Health Workers: A diverse category of health workers who have many
specific names that may be unique to the context in which they work (almost always outside
of fixed health facilities) with formal, but limited training for the tasks they are expected to
perform.

14
Community Mobilisation: A process that uses participatory approaches to motivate groups,
institutions, leaders and members at local levels towards shared knowledge, attitude, actions
and practices that are collectively beneficial to them.
Community Participation: An educational and empowering process in which the people, in
partnership with those who are able to assist them, identify their problems and needs and
increasingly assume responsibilities themselves to plan, manage, control and assess the
collective actions that are proved necessary.
Community Participation in Health: The active involvement of people living together in
some form of social organization and cohesion in the planning, operation and control of
primary health care using local, national and other resources.
Community Participation in Health Development: A process by which partnership is
established between the government and local communities in the planning, implementation
and utilization of health activities in order to benefit from increased local self-reliance and
social control over the infrastructure and technology of Primary health Care.
Community Resource Persons: Community Volunteers including, Traditional Birth
Attendants, Village Health Workers and other community based service providers that have
been duly trained and are recognized by the Local Government.
Composite Score: A score that represents small sets of data points that are highly related to
one another both conceptually and statistically. It is computed from the sum of the scores
from its component measures.
Empowerment: The process of increasing the capacity of individuals or groups to make
choices and to transform those choices into desired actions and outcomes.

15
Functionality: The quality of performing the particular use or set of uses for which
something is designed.
Local Government Area Primary Health Care Management Committee: The committee
that provides overall direction for Primary Health Care in the Local Government Area.
Local Government Area Primary Health Care Technical Committee: The committee
serves as the administrative link between the LGA PHC management committee and the
Village and Ward development committees as well as the health workers.
Primary Health Care: Essential health care based on practical, scientifically sound and
socially acceptable methods and technology made universally accessible to individuals and
families in the community through their full participation and at a cost that the nation can
afford to maintain at every stage of its development in the spirit of self-reliance and self-
determination.
Primary Health Care Managerial Committees: The various committees existing at
different Levels in the Ward Health System, responsible for Primary Health Care
Implementation.
Primary Health Care Managerial Process: The organization and management of
infrastructures that have to exist at various levels (villages, wards and LGAs) for PHC
implementation.
Readiness: A state of preparedness of persons systems or organisations to meet a situation
and carry out a planned sequence of actions.

16
Spouse: A life partner in a marriage, civil union, domestic partnership or common-law
marriage. The term is gender neutral, whereas a males spouse is a husband and a
female spouse is a wife.
Summary score: A score that combines many measures into one overall score even though
the individual measures may address different aspects of a concept. It is computed from the
arithmetic average of the scores from its component measures.
Village Development Committee: The administrative link between communities and
Primary Health facilities at village or community level, responsible for promoting
community participation.
Ward Development Committee: The administrative link between communities and
Primary Health Care facilities at ward level, responsible for promoting community
participation.
Ward Minimum Health Care Package: A set of health interventions and services that
addresses health and health related problems that would result in substantial health gains at
low cost to government and its partners.

17
Abstract
Introduction: Information about Village and Ward Development Committees is limited.
This study examined the composition and functionality of Village and Ward Development
Committees and their influence on household utilization of Primary Health Care services.
Methodology: A descriptive, cross-sectional study design was utilized and respondents
comprised 840 mothers of under-five children, 29 Primary Health Care workers, 3 village
development committees, 4 ward development committees, 5 key informants and 11
Primary Health Centres. A multistage sampling technique was used in the selection of
mothers of under-fives. All the Primary Health Care facility workers in the surveyed wards
were studied, the Village and Ward Development Committees were purposively selected
and all the operational Primary Health Centres in the surveyed wards were studied. Data
were collected using structured, pretested, interviewer-administered questionnaires for
mothers of under-fives and Primary Health Care facility workers. A Focus Group Discussion
guide was used for the various committees and 3 key informant interview guides for the key
informants. Readiness of the Primary Health Care facilities to provide some components of

18
the Ward Minimum Health Care Package was assessed using an observational check-list.
Data were analysed using the Statistical Package for the Social Sciences (SPSS) version 20
and Microsoft Excel with the level of significance set at p < 0.050.
Results: Two (66.7%) of the Village Development Committees were well composed and
functional, while one (33.3%) was only fairly well composed and functional. Two (50.0%)
of the Ward Development Committees were well composed and fairly functional, one
(25.0%) was well composed but poorly functional while one was fairly well composed and
poorly functional. The only factor found to be associated with well composed Village and
Ward Develoment Committees was inauguration by officials of the National Primary Health
Care Development Agency, while the main factor associated with their functionality was
absence of financial remuneration. In the three communities with functional Village
Development Committees, two of the Primary Health Care facilities were fairly ready while
one was not ready to deliver maternal, newborn, child survival and health
education/community mobilization services. There was little or no correlation between
functionality of the Village Development Committees and readiness of the Primary Health
Care facilities to deliver some components of the Ward Minimum Health Care Package (rho
= -0.058, p = 0.913). Overall, majority 645 (76.8%) of the households showed poor
utilization of Primary Health Care facilities, 129 (15.4%) showed fair utilization, while 64
(7.6%) showed good utilization. Overall, 12 (41.4%), 13 (44.8%) and 4 (13.8%) of the PHC
workers had poor, fair and good performances respectively in the delivery of
maternal/newborn, child survival and health education/community mobilization services.
There was a weak positive correlation between household utilization of Primary Health Care
services and performance of Primary Health Care workers (rho = 0.400, p = 0.600). There
was no correlation between composition of development committees and utilization of

19
Primary Health Care services (rho = 0.000, p = 1.000). There was a strong positive
correlation between functionality of development committees and household utilization of
PHC services (rho = 0.500, p = 0.667).
Conclusion: Functional village and ward development committees positively influence
household utilization of Primary Health Care services. Provision of sitting allowance for
members of VDCs/WDCs will promote their functionality.
Key words: Development Committees, Households, Utilization, Primary Health Care
services.
CHAPTER ONE
1.0 INTRODUCTION
1.1 BACKGROUND
Primary Health Care (PHC) was adopted as a tool for achieving “Health For All” by the
member nations of the World Health Organization (WHO) at the international conference
on PHC held at Almaty (formerly Alma Ata), Kazakhstan (formerly Kazakh Soviet Socialist
Republic) from 6th – 12thSeptember 1978.1 At that conference, universal access to care and
coverage on the basis of need, political commitment and a health care system that will
address the major health problems of the people (essential health care) were identified as
guiding principles for the successful implementation of PHC. Equitable distribution of
health resources in such a way that provides accessibility and coverage to the entire
population at a cost they can afford, community participation, health promotion, use of
appropriate technology and intersectoral collaboration were also identified as guiding

20
principles.2,3 Community participation has been acknowledged as the most important of
these principles, since “people have a right and duty to participate individually and
collectively in the planning and implementation of their health care”.1,4,5
In order to promote active community participation, Village and Ward Development
Committees have been established in many developing countries and they serve as the
management structures for PHC at the village and ward levels. In Nigeria, the goal of the
management process in PHC is “to establish and sustain functional development committees
at all levels to achieve health for all Nigerians.”6 The Village Development Committees’
(VDCs’) function is to identify and prioritize village needs, providing a forum for contact
between the villagers and the politicians and local authorities.7 Village or Ward
Development committees are umbrella organizations that serve as representatives of the
entire people, acting as a front for the entire village or ward.8
These Village and Ward Development committees form the managerial structures for the
Ward Health System.9,10 The Ward Health System through its Ward Health Services is
responsible for delivery of health care services to a political ward. This system operates at
the Local Government level in Nigeria and consists of the ward health services and its
managerial structure.10 The structure for health care service delivery at the ward level is the
Ward Health Centre which provides integrated PHC services to cover all PHC components.
It also provides referral services, to the Primary Health Clinics and Health Posts in the
communities that make up the ward. The Village and Ward Development Committees serve
as the managerial structures at the village and ward levels respectively, supervising the
activities of the PHC workers. At the village level, the Village Development Committees
(VDCs) supervise the activities of the Junior Community Health Extension Workers

21
(JCHEWs) who ought to spend 90% of their work time in the communities, supervising the
activities of the community resource persons who in turn spend 100% of their time in the
community.9
The Ward Development Committees (WDCs) supervise the activities of the Community
Health Extension Workers (CHEWs) and Community Health Officers (CHOs), who ought
to spend 40% of their work time paying regular and scheduled visits to their communities.9
The VDCs and WDCs also help in planning for the health activities in the village and ward
respectively. In Nigeria, these and other functions are outlined in the ‘Guidelines for the
Functioning of the Primary Health Care system in Nigeria’, developed by the National
Primary Health Care Development Agency.9
The VDCs in a ward, report to the WDC through their representatives serving in the WDC,
while the WDC through their representatives report to the PHC Technical Committee at the
Local Government level, which is in turn responsible to the LGA PHC Management
Committee.10 The PHC Technical and the PHC Management Committees are responsible for
the overall planning, monitoring and evaluation of health activities in the Local
Government. Their functions are also outlined in the ‘Guidelines for the Functioning of the
Primary Health Care System in Nigeria’.
The aim of the Ward Health System is to promote full and active community participation at
the grass root level in order to sustain an effective and efficient delivery of PHC services in
the ward.10 These services are outlined in the Ward Minimum Health Care Package. This
package consists of six interventions; Control of communicable diseases, Child survival,
Maternal and newborn care, Nutrition, Non-communicable disease prevention and Health
education and Community mobilization.11 Household members’ utilization of these services

22
can be a measure of community participation. Studies have shown that utilization of health
services is influenced by the availability of these services in the health facilities and the
readiness of these facilities to deliver such services.12–14 However utilization of services
alone without involvement of the community in planning, implementation, monitoring and
evaluation of these services will amount to passive participation.15 In addition to utilizing
the services, involvement in planning for the services, monitoring the day to day delivery of
the services and evaluating the services against a background of predetermined objectives
are good indices of active participation.16 These managerial processes ought to be carried
out by the Village and Ward Development Committees who are the representatives of their
communities.
1.2 STATEMENT OF THE PROBLEM
One of the major challenges of PHC implementation is improving community participation.
In many developing countries, participation of communities in planning, monitoring and
evaluation of health services has diminished. Community management structures (e.g.
VDCs and WDCs) have broken down or are non-existent; the link between health delivery
systems and the communities they serve has disappeared. In most countries, community
health workers and extension workers are no longer in place.17
Community participation, though the most important principle of Primary Health Care has
remained one of the weakest in terms of implementation.18 In the African region, monitoring
and evaluation of the implementation of National Health-for-All strategies were carried out
in 1988, 1991 and 1994. The findings revealed that the implementation of the strategy had
achieved some significant results; however, there were weaknesses in community
participation among other areas.17

23
In sub-Saharan Africa, it appears that the political will exists at national levels, in terms of
participatory approaches to health care, yet, when reviewing both governmental documents
and the professional health literature, there is little documentary evidence of actual
participation by communities.7 Even when there is participation, this often only takes place
when free labour is needed, such as to construct a health facility. Consultation on
community needs and plans is usually absent and even where consultation with and
participation of the general population through the village health committees do exist, such
as in VDCs, and village-based meetings, the consultation may not really be accessible.7
In the absence of effective community participation, community members are not able to
exert administrative supervision over health services, and participate in community
development activities. In addition, access to health care, health care coverage, knowledge
of and participation in health promoting activities will be limited.19 Consequently, there will
be lack of ownership and sustainability of health interventions leading to poor and even
negative reversals in health indices. In Nigeria, part of the reason why the PHC gains of the
1980s were not sustained was the failure to develop adequate ownership of primary health
care by the communities.20 The efforts to encourage and support the formation of Village
and Ward Health Committees were largely abandoned across the nation and primary health
services and facilities were left to dissatisfied health workers. The Local Government
system, intended to give a powerful voice to every community member, does not function as
such. Health facility committees, if they function at all, do not regularly include community
representation.20 In Edo State, community participation has been limited in scope,
organization and impact.18

24
Ward Development Committees are key implementers of the Ward Health System which
has been adopted as the strategy for providing efficient and effective services with wide
coverage in Nigeria.10 However WDCs and VDCs which form the backbone of the
management structure of the WHS have largely been non-functional.21,22 This has
contributed to limited access and poor utilization of health care services, contributing to the
poor health indices in the country (MMR = 545/100,000,23 U5MR = 128/1,000,24 IMR =
69/1,00024). In Nigeria, as at 2001, 89% of the LGAs were estimated to have PHC
management committees and only 27% of these committees were functional.22 PHC
management committees oversee and coordinate the activities of VDCs and WDCs,
consequently, where the PHC Management and Technical Committees are non-functional,
the activities of the VDCs and the WDCs will be uncoordinated, the capacity of the
community representatives will not be built to effectively carry out their functions. This will
ultimately result in poor community participation with its attendant consequences.
The village and ward development committees form the link between the community and
the Primary health care workers who are responsible for delivering health care services to
the community. Empirical studies have shown that community health workers are effective
in improving utilization of PHC services.25–27 In many parts of Nigeria however, there is a
dearth of qualified personnel in PHC facilities and even when they are available many lack
training on essential life-saving skills.28–30 This has resulted in unavailability of 24 hour
services in many PHC facilities, poor utilization of PHC facilities in favour of unskilled
health practitioners which has largely contributed to the poor health indices in the country.
Utilization of PHC services is directly affected by the readiness of PHC facilities to deliver
health services in terms of adequate staffing and equipment. In Nigeria, readiness of PHC
facilities to deliver basic or comprehensive Emergency Obstetric Care is well below

25
average. In North East Nigeria in 2012, only 28% of Primary Health Care facilities were
adequately staffed and equipped to deliver basic or comprehensive EmOC.14 In North West,
South West and South-South Nigeria, prior to the launch of the midwives service scheme in
2009, less than 5% of Primary Health Care facilities had adequate staffing and equipment
for Basic and Comprehensive Emergency Obstetric Care.12,28,31 This low level of facility
readiness in PHCs has contributed to poor utilization of PHC services by women of child
bearing age thus contributing to the poor maternal health indices in the country and
consequent poor progress towards the attainment of MDG 5.
Lack of community participation has been implicated as being contributory to the evident
ineffectiveness of child health programmes leading to insufficient progress towards the
attainment of MDG 4.32 Globally, of the 68 priority countries targeted for child survival
improvements in 2010, 41% were deemed to have made insufficient progress and 38% made
no progress as at 2008.33 Nigeria being one of these countries was deemed to have made
insufficient progress between 2000 and 2008 towards the attainment of MDG 4 with an
annual reduction rate of only 1.3%.34
Poor community participation among other factors has been shown to contribute to low
immunization coverage in Nigeria, with coverage rates for BCG, Polio, DPT, measles,
Hepatitis B and Yellow fever being 61.7%, 46.1%, 42.6%, 49.2%, 34.0% and 40.4%
respectively.35,36 Low rates of immunization have in turn been associated with poor
knowledge and attitude towards immunization.37–40 This has resulted in the resurgence of
vaccine preventable diseases in the country which could further worsen the country’s high
infant mortality rate of 69/1000 and under five mortality rate of 128/1000.24,41,42 Studies
have shown, that worldwide, improved breastfeeding rates have been associated with peer

26
counseling.43–46 The low rates of breast feeding in Nigeria have been linked with poor
community participation in the form of peer counseling.47 Despite the fact that breast
feeding is the most inexpensive and effective intervention in the reduction of childhood
mortality, the rates of exclusive breastfeeding under 6 months and continued breastfeeding
up to 2 years in Nigeria are 15.1% and 34.5% respectively.36 This low rate of exclusive
breastfeeding has contributed to diarrhoeal diseases and malnutrition in infants and under-
fives. Malnutrition can lead to poor school performance and drop out. It also threatens the
future ability of the girl-child to bear healthy children and perpetuates a generational cycle
of poverty.48 Malnutrition also undermines economic growth as 2-3% of a country’s national
income can be lost to malnutrition.49 It is projected that Nigeria will have 1.6 million
additional stunted children by 2015.50
Despite average to good knowledge of antenatal care among women of childbearing age in
many parts of Nigeria,51–54 utilization of antenatal care services is still sub-optimal.51–56 In
Benin City high maternal mortality ratio has been linked with non-utilization of ANC
services.57 Low utilization of antenatal care services could account for increased maternal
morbidity and mortality as it results in late detection or non-detection of complications in
pregnancy. This has contributed to the country’s insufficient progress towards achieving
MDG 533,58 with a maternal mortality ratio of 545/100,000. This is not surprising as only
38.1% of births are attended by a skilled health provider with only 35.8% of deliveries
taking place in a health facility.24 High maternal mortality may contribute to physical,
emotional, psychological and cognitive deprivation in children as well as reduction in per
capita GDP, thus worsening the vicious cycle of poverty, ignorance and disease.59
1.3 JUSTIFICATION OF THE STUDY

27
In Nigeria, government has shown some political will to strengthen community participation
in Primary Health Care by lending policy support to the principle through the National
Health Policy and the National and State Strategic Health development plans. Recently,
WDCs were reactivated by the NPHCDA in collaboration with the SURE-P initiative.
However it is not yet known how functional these reactivated ward committees are.
This study is intended to reveal factors that are associated with the composition and
functionality of Development Committees in Benin City and it is expected that the
information generated will serve as a useful tool in the hands of the NPHCDA, the SURE–P
initiative, NGOs and other interested donor agencies towards the activation of development
committees that are still inactive, both in Benin City as well as Edo state. It will also serve
as a contribution to knowledge in this area.
This study is to highlight the level of utilization of Primary Health Care services in Benin
City as well as the association between utilization and performance of PHC workers on one
hand, and that between utilization and functional development committees on the other
hand. This information will add to existing knowledge on PHC services utilization as well as
and serve as a basis for making recommendations to the Development Committees, the
Local Government and the NPHCDA.
In Benin City, few studies have been published on the readiness of PHC facilities to deliver
health services, in terms of infrastructure, adequate staffing and equipment. An assessment
of Primary Health Care facility readiness in Benin City therefore will help to fill this
knowledge gap. It will also serve to provide information on the relationship between facility
readiness and utilization of PHC services in Benin City thus providing information for
evidence based recommendations to the State and Local Governments. Finally, this study

28
could also serve as a basis for further studies in other parts of the country to fill the current
knowledge gap on the relationship between functional development committees and
utilization of PHC services.
1.4 RESEARCH QUESTIONS
This study attempted to answer the following questions:
1) Are development committees in Edo State well composed and functional?
2) What factors are associated with establishment of well composed and functional
committees?
3) How ready are health facilities located in villages or wards with functional
Development Committees, to provide some of the minimum ward health package
services (in terms of adequate staffing and equipment)?
4) To what extent do household members in Benin City utilize Primary Health Care
services?
5) How are PHC workers performing in delivering some components of the minimum
ward health Package?
6) Is this performance positively related to utilization of the facilities by members of the
communities?
7) Is there evidence of better utilization of services in wards or villages with well-
composed and functional committees?

29
1.5 AIM AND OBJECTIVES
General Objective: To assess the influence of development committees on household
utilization of Primary Health Care services in Benin City, with a view to gaining some
insight into the effectiveness of Primary Health Care managerial structures in Benin City.
Specific Objectives
1. To assess the composition and functionality of Village and Ward Development
Committees and the factors associated with their establishment in Benin City
2. To determine the readiness of health facilities in villages or wards with functional
Village or Ward Development Committees, to deliver some of the Ward Minimum
Health Care Package services in Benin City (in terms of adequate staffing and
equipment).
3. To assess household members’ utilization of Primary Health Care services in Benin
City

30
4. To assess the performance of primary health care workers with respect to the
delivery of some components of the ward minimum health care package in Benin
City
5. To determine the relationship between performance of the PHC workers and
household utilization of PHC facilities in Benin City
6. To ascertain the relationship between utilization of PHC services and well composed
and functional development committees.
CHAPTER TWO
2.0 LITERATURE REVIEW
2.1 Guidelines for Development Committees: The guidelines cover the strategies for
the formation of the various managerial committees, their composition, their roles and
responsibilities and their terms of reference.
Village and Ward Development Committees
Strategy for formation: The committee members will be selected by members of the
community.
Composition: The village head will be appointed as the patron of the VDC while the ward
head, the autonomous clan head shall be appointed as patron of the WDC. The members of
the VDC will comprise representatives of various groups in the community such as women
groups, youth groups, farmers’ groups etc. A respectable person elected by the members of

31
the committee will serve as chairman, an elected literate member will serve as secretary and
a trusted member of the committee will serve as treasurer. The members of the WDC will
consist of representatives of the VDCs in the ward. The chairman, secretary and treasurer
will be elected by the members of the committee. At least 20% of the committee members
should be women.
Roles and Responsibilities: For both village and ward development committees, these
include identification of health related needs, planning for welfare, identification of human
resources and allocating same as appropriate for PHC programmes, supervision of
developed work plans, determination of exemptions from drug payments and pricing of
drugs, supervision of VHWs/TBAs among others. The VDC shall forward local community
health plans to the WDCs. The WDCs will ensure the proper functioning of the Ward Health
Centres.
Terms of Reference: Both VDCs and WDCs shall meet monthly, record minutes of
meeting, have the minutes of meeting duly signed after adoption at subsequent meetings and
comply with the quorum set for meetings. The treasurer should record and keep all monies
and record all expenditure. Where there is a bank account the signatories shall be the
committee chairman and secretary. The VDC shall send minutes of meetings to the WDC.
The WDC shall monitor the drug revolving fund at ward and facility levels. For the WDC,
where there is a bank account, signatories to the account will be the committee chairman,
treasurer, and a mandatory signatory who is a government official.
LGA PHC Management Committee:
Each LGA should have an LGA PHC Management Committee. The objective of the
committee is to provide overall direction for PHC in the LGA.

32
Composition: The members should comprise, the Chairman of the LGA, the Supervisory
councilor for health, the LGA Secretary, the LGA PHC coordinator who should serve as the
secretary of the committee, a representative of CHO Training Institutions, principal of
School of Health Technology, representative of health-related occupational
groups/associations, the Chief (or most senior) Community Health Officer in the LGA,
Community Development Officer for the LGA, the Medical Officer in-charge of the
secondary health facility, chairmen of Ward Development Committees, ward councilors,
representatives of international Organizations having PHC programmes in the LGA, heads
of other health-related departments in the LGA (Education, Agriculture, Works, etc.),
representatives of NGOs, representatives of women/youth Groups, representative of
religious Groups, representative of private health practitioners in the LGA, representative of
health related departments (Agriculture, Education, Works).
Terms of Reference: Provision of overall direction for PHC service delivery in the LGA
including control of endemic communicable diseases (HIV/AIDS/STD, TB, Malaria,
onchocerciasis, etc.), planning for and managing PHC services in the LGA, health
manpower development for the LGA, provision of the Operational Guideline for the LGA
resource mobilisation for PHC. Terms of Reference also include quarterly meetings,
recording of minutes of meeting, adoption of minutes of meeting with signing of adopted
minutes by the chairman and secretary. The quorum set for starting meetings should also be
complied with.
LGA PHC Technical Committee:
There should be a PHC technical committee at the LGA level.

33
Composition: PHC Coordinator who will be the chairman of the committee, all assistant
PHC coordinators, program managers in the LGA.
Roles and Responsibilities: The committee shall plan and budget for implementation of
activities of PHC department and present same to the LGA PHC Management committee,
identify training needs for Health Workers and make proposals to the LGA PHC
Management Committee, design minimum acceptable performance standard for monitoring
LGA PHC services and develop monitoring indicators, monitor activities of health workers,
design supervisory checklist for LGA PHC services, Identify health related needs of
communities within the Local Government Areas, Plan for mobilization of local and
external resources to enhance PHC activities, provide feedback to committees at all levels,
monitor drug revolving fund for the health services at the LGA level, discuss Primary Health
Care Management Information System (PHCMIS) report and take appropriate action, give
feedback of data collected at LGA PHC Management Committee meeting/facility
staff/community, review progress of PHC in the LGA and evaluate their indicators.
Terms of Reference: In carrying out the above functions, the committee shall: meet
regularly; weekly or at minimum monthly, record minutes of meetings; adopt minutes of
meetings and ensure that the Chairman and Secretary sign them; comply with the quorum
set for starting meetings.
2.2 Composition and Functionality of Development Committees and Associated
Factors
In Nigeria, the government has long ago showed willingness to be committed to the
principle of community participation in PHC. The 1988 National Health Policy included
provision for the creation of PHC management and technical committees at local

34
government level, ward development committees a t t h e w a r d l e v e l and
community/village development committees at the community/village levels. In 2001, a
survey of 202 Local Government Areas (LGAs) spread across the six geopolitical zones in
Nigeria revealed that 89% of the LGAs had PHC Management Committees, of which only
27% were functional; having met at least once in the last three months before the visit.
Similarly, 75% of the LGAs had formed PHC Technical Committees and only 44% had met
at least once in the last 3 months before the survey.22 In 2013, the NPHCDA, in collaboration
with the SURE-P initiative reactivated ward development committees in the wards where the SURE-P
project is being sponsored. However, there is yet no objective evidence as to how functional these
committees are.
A report on Fiji Island published by the WHO in 2008 covered the progress of PHC in the
Island nation from 1978 to 2008.60 Findings were based on key informant interviews. It was
revealed that in Notagadravu, a village in Fiji, there were very effective village committees
which had regular meetings with the community and always involved them in their decision
making processes. This resulted in benefits such as reduced sickness and fatal disease and
improved environmental conditions. On the other hand, villages that had no village
committees were found to have poor health standards compared with those that had proper
committees. In these villages with poor health standards, lack of enabling government
policy, resulting in trained health workers not being encouraged to work with communities
was identified as a factor that hindered community participation through effective village
committees. Movement of community leaders out of the village to look for better jobs was
also identified as a factor that hindered the effectiveness of village committees. In this study,
though no mention was made of guidelines for the formation of VDCs, it was stated that

35
communities with effective or functional VDCs had positive health benefits while those with
no VDCs had poor health standards.
In another descriptive cross-sectional study carried out in Nepal between December 2008
and January 2009, to assess Village Development Committee governance and the use of
block grants, a representative sample of 202 VDCs, from 25 representative districts was
studied. Household respondents and other key informants were also surveyed and data were
collected using questionnaires, Focus Group Discussions and Key Informant Interviews.61
Findings revealed that the effectiveness of the VDCs was negatively affected by the fact that
most of the VDC secretaries were politically appointed and not democratically elected.
Consequently, these secretaries were usually overburdened with multiple responsibilities
and therefore unable to perform their function of effectively promoting community
participation. In addition, due to the fact that these VDC secretaries were political
appointees, there was little consultation with communities when deciding on development
programmes. Twenty five percent of the VDC secretaries said that the dominant type of
VDC planning consultations were formal meetings with the local politicians while 36% of
them said that the politicians’ recommendations was the main basis for deciding which
projects to fund from the block grants received from the government. In addition frequent
transfers and security concerns in conflict affected areas also reduced their effectiveness in
promoting community participation. This study was in contrast to the one in Fiji Island
described above, where functional village committees always involved the community in
their decision-making processes, thus promoting effective community participation.
A similar descriptive crosssectional study was carried out in Bangladesh in 2014, by the
Chars Livelihood Programme (CLP) with the aim of investigating the effectiveness and

36
sustainability of VDCs after CLP phased out of their working area and to understand the
factors contributing to VDC sustainability.62 Data were collected using both questionnaires
and qualitative methods (FGDs and KIIs). A multistage sampling method was used for the
questionnaire survey, which involved 82 respondents and 42 VDCs. Factors that contributed
positively to the effectiveness of VDCs, included presence of committed members who had
strategies in place to recruit new members, thus ensuring stability of the VDCs. Having clear
objectives at the time of formation of the committees and working towards them, also
contributed to effectiveness of the committees. Cordial relationship between the members of
the community and the VDCs also promoted their effectiveness. Acknowledgement of the
importance of the VDCs by the members of the community also promoted the effectiveness
of the committees. Factors that militated against the effectiveness of the committees
included the view that CLP support was necessary for VDCs to continue as evidenced by the
expectation of financial incentives and low feelings of VDC ownership from community
members. The lack of a strategic phase out plan and lack of an income generating source
also negatively affected the effectiveness of the VDCs. It is worthy of note that while in the
Fiji Island study, movement of community leaders outside the community hindered the
effectiveness of the VDCs, in the Bangladesh study, a factor contributing to the success of
the VDCs was the fact that they had committed members who had strategies in place to
recruit new members.
Another similar study was conducted in 2008 in South Africa which aimed at assessing the
role of Ward Committees in enhancing participatory local governance. Six ward
development committees, selected from three municipalities were studied and data were
collected using qualitative methods (focus group discussions, in-depth interviews and
participant observation).63 Findings revealed that each of the six committees had a

37
minimum of 33% female representation, most ward committee members and ward
councillors had a reasonably clear understanding of what their roles were. In most cases, the
nomination and election processes appeared to have been relatively unproblematic from the
respondents’ perspectives and more or less in line with the process envisaged in national
guidelines. In most of the committees there was inadequate representation of the different
sectors of the community. Only two (33.3%) of these committees were able to meet
regularly and had some sense of common purpose and achievement to their meetings and
other activities carried out by them. In this study, there was compliance of the committees
with the guidelines for their formation but inadequate community representation. The other
studies above did not mention guidelines for formation, female and community
representation.
2.3 Readiness of Primary Health Care Facilities in Villages or Wards with
Functional Development Committees to Deliver some of the Ward Minimum Health
Care Package Services
One of the critical pathways to improving the poor health indices in our country is by
increasing access to skilled care especially in the rural areas where about 70% of the
population resides. An important component of access is the availability of the facilities,
manpower and medicines required for the delivery of these services. It has been shown that
facilities that were ready for service delivery were better utilized than their counterparts
which were not ready.14 It is believed that functional Primary Health Care Committees
(VDCs and WDCs) will promote readiness of PHC facilities to deliver health services.
A descriptive crosssectional study was conducted in Nepal in 2011 to assess the influence
of active engagement and capacity building of Health Facility Operation and Management

38
Committees (HFOMC) on good governance at peripheral public health facilities.64 The
study assessed a health facility management strengthening programme which was being
implemented in 13 districts. Baseline and monitoring data were collected retrospectively
from the records of the programme implementers from July 2008 to October 2011. Results
showed that there were increases in health facility opening days and availability of technical
staff. Furthermore, health services became more inclusive. The HFOMC is similar to the
WDC and consists of representatives from the health facility, VDCs and women and
disadvantaged groups in the district. This study revealed that functional HFOMC had a
positive influence on the readiness of PHC facilities to deliver services.
Another descriptive crosssectional study was conducted in Mkuranga district, Tanzania in
2007, to explore the views of the villagers on the existence and functioning of local PHC
committees, VHWs, skilled staff at government health facilities and their responsiveness to
community health needs.65 Data were collected using qualitative methods (FGDs, KIIs and
in-depth interviews) as well as quantitatively, using semi-structured questionnaires. Findings
revealed low awareness of VDCs and WDCs among household members and health service
staff. Responses from household respondents also revealed that 55% of the 40 household
respondents were dissatisfied with their poorly functioning PHC committees. Reasons for
dissatisfaction in 13.6% of those dissatisfied was the acute and long term shortage of clinical
staff, while in 4.5%, the reason was the poor state of the health facility building. Thus it can
be deduced from this study that villages with poorly functioning PHC committees were also
not ready for service delivery in terms of health manpower and infrastructure.
In 2013, a similar study was conducted in 6 states in Nigeria (three northern states –
Kaduna, Nassarawa and Benue and three southern states – Lagos, Bayelsa and Abia).66 The

39
aim of the study was to examine how the decentralization of health system governance
influences the retention of health workers in rural communities in Nigeria. Data were
collected using in-depth interviews and focus group discussions. Findings revealed that
through community health committees, rural communities positively influenced the
retention of health workers by providing social, financial and housing support to health
workers. Furthermore, communities also took the initiative to co-finance and co-manage
PHC services in order to ensure that PHC facilities were functional. From this study,
functional community health committees such as VDCs and WDCs positively influenced the
readiness of PHCs to deliver services in terms of availability of manpower as well as
facilities and infrastructure.
Another similar study was conducted in Enugu State Nigeria in 2002 to compare the level of
availability and rational drug use in PHCs with operational Bamako Initiative (BI) Drug
Revolving Fund (DRF) programmes with PHCs where such programmes were not yet
operational. Twenty one PHCs with operational BI DRF programmes and 12 PHCs without
such programmes were studied.67 Crosssectional data were collected from the listing of
available drugs at the time of the survey, data were also collected from health centre records.
Findings revealed that an average of 35.4 essential drugs were available in the BI health
centres compared with 15.3 essential drugs in the non-BI health centres out of a possible
total of 39 essential drugs required at the health centre level. This difference was statistically
significant. The presence of an operational BI programme could be used as a proxy for
functional development committees. This is because Bamako Initiative programmes
function against a background of community participation through active WDCs and
VDCs.68 Thus indirectly, this study reveals that PHCs located in communities with

40
functional development committees were more ready for service provision in terms of
essential drugs compared with those which were located in communities without functional
development committees.
The literature reviewed above revealed that the presence of a functional village development
committee had a positive influence on the readiness of their health facilities to deliver PHC
services, on the contrary, PHCs located in communities without functional development
committees were not ready for PHC service delivery.
2.4 Utilization of Primary Health Care Services
Utilization of healthcare services is still low in Nigeria and use of primary health care
services is even lower. Among women who had live births in Nigeria from 2008 to 2010,
only 36% delivered in a health facility. In the same period, only 9.2% of users of
contraceptives aged 15 – 49 years obtained their commodities from a government health
centre.24
An analysis of data obtained from the 2005 National HIV/AIDS and Reproductive Health
Survey (NARHS) was carried out to identify individual, household and community factors
that were significantly associated with utilization of maternal care services among 2,148
women of reproductive age (15-49 years), who had had babies during the five years
preceding the survey.69 The survey covered all the 36 states of Nigeria and the FCT.
About 60% of the respondents used antenatal services at least once during their most recent
pregnancy. The percentage of last births whose delivery was assisted by qualified medical
personnel (doctor, nurse or nurse-midwife) was 43.4% while only two fifths (41.2%)
received postnatal care. For the antenatal care indicator, the most significant individual-level

41
predictors of use of antenatal care services were a minimum of post-secondary level of
education (OR = 5.03), approval of family planning (OR = 1.64), age at birth of last child
between 25 – 34years (OR =1.18, OR2 = 0.99): the relationship between age at last birth
and use of ante natal services appears to be curvilinear, the negative coefficient associated
with the square of age indicates that use of postnatal services initially increases with age up
to a threshold and decreases thereafter. Belonging to a household with a high socio-
economic status (OR = 5.86) was also a predictor of use of ANC services. This study, was a
nationally representative one, thus, use of PHCs was also included. Findings revealed fair
use of ANC services and poor use of delivery and ANC services. Although this study was
not specifically focused on utilization of PHC services, national findings from nationally
representative studies like the NDHS show that use of PHC services is even less than that of
other public health facilities..
A descriptive cross sectional study was carried out in 2013, in Giwa, a semi-urban
community in North-Western Nigeria, to determine, the mothers' perspective of barriers to
utilization of maternal health services and the changes that they believed would improve
these services.70 One hundred and fifty women of child bearing age (15 – 49 years) who had
delivered in the 24 months preceding the survey, and had been permanent residents in the
community for at least 12 months before that delivery were selected using multistage
sampling and data were collected using a structured interviewer-administered
questionnaire.70 Results revealed that the proportion that utilized preconception care was
2.7%, ANC 98.7%, delivery 24.0%, postnatal care 35.3% and family planning service
14.0%. Among the 148 respondents who attended antenatal clinics, 66.9% attended four or
more times while the remaining did so less than four times. With respect to place of

42
delivery, only 24.0% delivered in a health facility. This study was carried out in a semi-
urban community, hence it can be safely assumed that PHC facilities were included in this
study. The finding of almost 100% utilization of ANC services, is in contrast to the findings
of the NARHS above where only 60% of women used ANC services. It also contrasts with
findings from NDHS 2013 where in the North Western Nigeria, only 41.0% of pregnant
women received care from a skilled provider in the five years preceding the survey.24
In another descriptive crosssectional study carried out in 2013, which assessed the
reproductive health knowledge and utilization of maternal health care services among 1,000
married women of reproductive age (14 - 49 years) living in Kano State, northern Nigeria,
42.2% of urban and 40.2% of rural respondents were aware of and used ANC services
offered at primary and/or secondary facilities in Kano state.56 Sixty five percent of urban
and 33.6% of the rural respondents said they were aware of and used family planning
services offered by health facilities. Reasons given by respondents for not utilizing ANC
services included ill health, (81.1%) husband’s refusal (69.1%), long distance from the
health facility (48.4%), lack of money (16%) and the belief that a pregnant woman should
go to the hospital only on account of ill health. Thirty percent of respondents delivered their
children at home or at the TBA’s place while 65.8% women delivered in hospitals. Findings
from this study showed poor utilization of ANC services, family planning and delivery
services in the rural areas and fair utilization of family planning and delivery services in the
urban areas.
In another similar study carried out in Ibadan, Nigeria, in 2010, to assess the factors that
determine the utilization of ANC services, 400 women of child-bearing age accessing health
care services in the PHCs in selected LGAs were interviewed using semi-structured

43
questionnaires.71 Findings revealed that majority (76.8%) of the respondents attended
antenatal clinics. Bivariate analysis revealed that age equal to or greater than 25 years (p =
0.045), Yoruba tribe (p = 0.001), religion other than Christianity (p = 0.039), being married
(p = 0.011), minimum of secondary education (p = 0.001), professional occupations (p =
0.001), spouse with minimum of secondary education (p = 0.001), spouse with professional
occupation (p = 0.001), residence in an urban area (p = 0.0001) and respondents’ personal
involvement in taking decisions concerning her own health (p = 0.014), were all
significantly associated with utilization of ANC services. However after multiple regression,
only place of residence (OR = 2.177, 95% CI, 1.081-4.382), religion (OR = 2.398, 95% CI,
1.264-4.557) and age (OR = 2.236, 95% CI, 1.106-4.107) were found to be the statistically
significant predictor variables. This study showed good utilization of PHC services in terms
of ANC services utilization. This contrasts with the Kano study described above where there
was poor utilization of ANC services. Findings from this study agree with the findings from
NDHS 2013, where 87.2% of pregnant women in Oyo State, utilized ANC services in the
five years preceding the survey.
Another descriptive cross sectional study was carried out in 2013 in Irepodun/Ifelodun local
government area (LGA) in Ekiti State, southwest Nigeria. The aim was to assess knowledge
and utilization of Intermittent Preventive Treatment for malaria among pregnant women
(IPTp) attending antenatal clinics in primary health care centers in rural southwest,
Nigeria.72 About 27% of the 209 respondents were reported to have received at least one
dose of IPTp during the index pregnancy and all were among those who had heard of IPTp
(52.3%).

44
Pregnant women who registered in the 1st and 2nd trimester (p = 0.02) and those who were
able to define IPTp correctly (p < 0.001) were significantly more likely to use IPTp. The
number of women who received IPTp increased as the number of pregnancies increased up
to the third pregnancy and decreased thereafter (p = 0.01). Majority of the women 116
(77.0%) did not have a sure source of monthly income. However, 29 out of 48 who
volunteered the amount they earned monthly earned less than N10,000 monthly (< $100
USD) and these group of women were more likely not to use IPTp (p < 0.001). There was
no significant association between gestational age, age of respondents, and length of time
(minutes) spent trekking to the clinic and IPTp use (p > 0.05). Use of IPTp was poor (less
than 50%) in this study. This study differs from the others described above, in that its aim
was not merely to assess the use of ANC, but a specific component of ANC. Specific
components of ANC were assessed in NDHS 2013, but use of IPTp was not.
A descriptive cross-sectional survey was conducted in September 2006, in Sabongida-Ora,
Edo State to assess knowledge of immunization among mothers of children aged 12–23
months and vaccination coverage.73 Vaccination coverage against all the seven childhood
vaccine preventable diseases was 61.9% although it was significantly higher (p = 0.002)
amongst those who had a vaccination card (131/188, 69.7%) than in those assessed by
maternal history (79/151, 52.3%). Multiple logistic regression showed that mothers'
knowledge of immunization (p = 0.006) and vaccination at a privately funded health facility
(p < 0.001) were significantly correlated with the rate of full immunization. Sabongida-Ora
is a rural community in Edo State, thus it can be assumed that the PHC facilities in that
community were also assessed. Findings of this study are very different from those of
NDHS 2013 where vaccination coverage against all the seven childhood vaccine preventable
diseases was 1.8% among those whose immunization cards were seen and 57.2% among

45
those whose cards were not seen.24 While in the other studies described above, utilization of
maternal health services were assessed in this study utilization of a child health service was
assessed.
2.5 Performance of Primary Health Care Workers with respect to the Delivery of
some Components of the Ward Minimum Health Care Package Services and
Household Utilization of PHC Facilities in Benin City.
Various cadre of Community Health Workers (CHWs) constitute the majority of the
workforce of Primary Health Care Facilities in Nigeria.4 Community Health Workers are
most effective when supported by a clinically skilled health workforce, particularly for
maternal care, and deployed within the context of an appropriately financed primary health
care system. However, CHWs have also notably proven crucial in settings where the overall
primary health care system is weak, particularly in improving child and neonatal health.
They also represent a strategic solution to address the growing realization that shortages of
highly skilled health workers will not meet the growing demand of the rural population.74
Some of the universal features of CHWs include their comparatively limited training,
diverse typologies and titles that may or may not be directly related to their roles and their
primary focus on communities.75 CHWs can play important roles in responding to many
diseases and in promoting immunization and breast feeding, resulting in positive effects on
child, neonatal and adult morbidity and mortality. In maternal and child services, CHWs
provide ante- and postnatal care, advise on family planning and childhood nutrition, increase
facility-based deliveries, conduct home visits, formulate birth plans, facilitate home
deliveries and respond to obstetric emergencies.75 There is some evidence that CHWs could
be a less costly approach for the delivery of certain services such as malaria case

46
management among others. The World Health Organization has endorsed task shifting to
allow lower cadres of health workers assume greater responsibility in health care delivery.76
In 2004, a descriptive cross sectional study was carried out in Riyadh City, Saudi Arabia, to
identify the factors influencing utilization of public and private PHC services. Five hundred
respondents 18 years or older were selected from one public PHC centre and two
dispensaries using stratified random sampling and data was collected using a structured self-
administered questionnaire. Results showed that waiting time was significantly associated (p
< 0.001) with the choice of whether to use a public or a private facility.77 This study shows
that performance of healthcare staff in the area of time management is important in
determinant of health facility utilization.
Another descriptive cross sectional study was conducted in Iran in 2010 to explore the
perceptions of CHWs regarding their contribution to rural health. Data was collected
qualitatively by means of face-to-face interviews with CHWs in 18 provinces.78 A total of
91 interviews were undertaken in the 18 study provinces. Participants were asked questions
concerning recruitment, training, tasks and responsibilities, support, and supervision. CHWs
(Behvarzes’) perceptions about barriers to effective program delivery and suggestions for
improvement were also sought. Findings showed that the CHWs were involved in rendering
services in Child health care, maternal health care, communicable and non-communicable
disease management and care of the elderly among others. Respondents reported that trust-
based relationships with rural communities, an altruistic motivation to serve rural people,
and sound health knowledge and skills were the most important factors facilitating
successful implementation of the CHW program in Iran. In contrast, high workload and the
lack of a support system were mentioned as barriers to effective performance. From this

47
study in Iran, the successful implementation of the CHW programme, which resulted in
good utilization of PHC services was linked with good performance of the CHWs in terms
of sound health knowledge and skills as well as good health-worker-patient relationship. On
the other hand, high workload and lack of support system were identified as hindrances to
effective performance.
Another study (a pilot study) was carried out between 2008 and 2010 in Warangal district of
Andhra Pradesh, India with the aim to strengthen monitoring, supervision and community
participation for performance enhancement of PHC.79 Ten PHC centres were selected for the
study in consultation with the District Medical and Health Officer (DM&HO); two from
each of the five subdivisions in the district. Five of them rendered 24 hour services while the
other 5 rendered only day time services from 9am to 5 pm. Findings revealed that health
care workers performance positively affected utilization of the health centres and facilities.
Prior to the pilot study, the poor services by the healthcare workers had been reported to be a
major factor influencing poor utilization of the health care services.79 This pilot study found
out that improved communication and interaction by the PHC workers with members of the
community helped to improve utilization of PHC services. There was improvement in
percentage performance for immunization from 81% in 2008-2009 to 86% in 2009-2010,
average out-patient attendance increased from 85% in 2008-2009 to 101 % in 2009-2010
and for couples using birth-spacing methods from 22% to 38%. This is similar to the study
in Iran, described above where good health-worker-patient relationship contributed
positively to the utilisation of PHC services.
A similar study was conducted in 2011, in Roma, a community within the Maseru district in
Lesotho, with the aim of assessing the effectiveness of Primary Health Care in Lesotho.

48
Village health workers, nurses, chiefs and out-patients were selected using quota sampling.80
Qualitative methods (focus group discussions and key informant interviews) were used for
data collection. Secondary data were also collected from PHC facility records. Findings
from qualitative interviews revealed good performance of PHC workers in terms of
immunization and patient care. PHC records also showed improvement in the coverage of
some PHC components from 2004 to 2008 as follows: maternal and child care; from 39% to
61%, immunization; from 30% to 64%, health education; from 15% to 58% and promotion
of nutrition; from 4% to 12%. Like the study in Iran described above, this study assessed
performance of health workers in terms of delivery of some components of PHC, which is
one of the objectives of the proposed study. Thus findings from this study will serve as
useful comparisons with findings from the proposed study.
A community-based intervention study was carried out in Mtwara district, in the south-east
region of Tanzania from June 2004 to November 2006, to evaluate the effectiveness of a
community-based intervention package for Safe Motherhood.81 Mtwara is one of the least
developed regions in the country and the majority of its population are poor subsistence
farmers earning below 1 US$ per day and hence living below the poverty line. This
intervention package relied heavily on the involvement of community volunteers, called
Safe Motherhood Promoters (SMPs). Quantitative and qualitative tools were used for data
collection. The results showed a significant improvement in the utilization of a skilled
attendant with variation across the villages. Deliveries with skilled attendants significantly
increased from 34.1% at baseline to 51.4% in 2006 (ρ < 0.05), against a background of
almost a static situation at regional level which was 36% in 2004 at baseline and at post-
intervention in 2006. The primigravida mothers who booked ANC early, between 4 to 16

49
weeks, increased significantly (ρ < 0.01) from 18.7% (12 out of 64) at baseline in November
2004, to 56.9% (41 out of 72) at final assessment in November 2006. Findings from this
study showed that well trained PHC workers resulted in significant increase in the utilization
of PHC facilities.
Another descriptive cross sectional study was carried out in 2008 among 313 traders in
Igboora and Idere in Ibarapa Central LGA, South Western Nigeria. The aim of the study was
to identify their health problems as well as health seeking behaviour and associated factors.
A total population study of all traders above 18 years was done using an interviewer-
administered semi-structured questionnaire. Data was analysed using SPSS version 16
software. It was discovered that previous education about illness by health workers was
significantly associated with health facility use (p= 0.001).82 This study therefore shows that
good performance by PHC workers as regards health education was positively associated
with use of the health facility.
Another descriptive cross sectional study was carried out in 2012 in Enugu among 300
women of child-bearing age. The aim was to find out their knowledge and perception about
health services offered in the PHC facilities and the factors militating against the efficient
and effective use of the services. A multi-stage sampling method was used, data was
collected using an interviewer-administered semi-structured questionnaire, and was analysed
using Epi-Info version 3.3 software. Poor staff attitude (46.3%) and unavailability of doctors
(35.7%) among others, were found to be factors that militated against the use of PHC
services.83
From the studies cited above, effective delivery of maternal health care and immunization
services, well trained health workers, prior health education by health workers and short

50
waiting time were all positively associated with use of health facilities. On the other hand,
poor staff attitude and unavailability of doctors were associated with poor utilization of
health facilities. This study assessed performance of health care workers in terms of delivery
of some components of the WMHCP.
2.6 Utilization of PHC Services and Well Composed and Functional Development
Committees
Some studies have shown that well composed and functional village (or community) and
ward (or district) development committees promote utilization of PHC services.
A study was conducted in Kirivong Operational District (KOD) Cambodia between May
2003 and December 2005 to assess the ability of local structures to provide financial access
to public sector health services for the poorest.84 In KOD, Health Equity Funds (HEF) were
set up by an International Non-governmental Organisation and managed by pagoda-
associated volunteers who raised funds for pagodas (Buddhist temples) and their inhabitants
(Buddhist monks). The HEF in KOD were different from those of other districts in that there
was very little dependence on external support. In KOD there were 4 administrative districts,
31 communities, 290 villages, 91 pagodas, 4 mosques and 20 public sector health centres.
Data were collected from the health facilities at baseline, after 20 months and at the end of
the 2nd year. Findings revealed that for the equity fund beneficiaries, there was an increase in
the number of deliveries assisted by qualified staff from 2.3/1000 population at the end of
the initial 20 months to 4.4/1000 at the end of the 2nd year. The district in which this study
was conducted was predominantly Buddhist, and the pagoda-associated volunteers were an
existing local structure which can be likened to our ward development committees because
the volunteers were representatives of the different Buddhist Communities. Thus the study

51
shows that the activities of a functional district committee through their involvement in the
management of health equity funds, resulted in increased utilization of primary health care
services.
A descriptive cross-sectional study was conducted in Nkoranza district, Ghana in 2014 to
determine the influence of community based health insurance schemes on the use of in-
patient care in Ghana. Secondary data were obtained retrospectively from the records of the
community based health insurance scheme covering a period of 17 years (1981 – 1998); ten
years before the introduction of the scheme and 7 years after the introduction of the scheme.
Findings revealed that there was a significant increase in the number of admissions after the
introduction of the scheme (p < 0.05). It was also shown that the scheme had a significant
positive influence on the number of hospital admissions. (p < 0.05).85 Community based
financing is a way in which communities actively participate in their own health care by
being involved in the financing as well as the management of health insurance schemes.86
Functional WDCs and VDCs play an important role in convincing the members of the
community to participate in health care activities, including such a scheme. Thus in this
study, the success of the community-based health insurance scheme and consequent positive
influence on PHC utilization can be attributed to well-functioning VDCs and WDCs.
Findings from this study are similar to those of the study in Cambodia described above,
where community based financing in the form of health equity funds was also associated
with increased utilization of healthcare services.
In 2002, a descriptive cross-sectional study was carried out in Kogi and Lagos states,
Nigeria which aimed to analyse the decentralized delivery of PHC services and to
understand how existing institutional arrangements impacted service delivery outcomes.

52
Data were collected in 30 LGAs from 252 health facilities and over 700 health workers via
key informant interviews, record reviews and use of questionnaires. Findings revealed that
community participation was significantly associated with greater productivity per staff in
providing in-patient deliveries, immunization and out-patient consultation.87
The agents of community participation are well functioning VDCs and WDCs. As shown
above in the section on performance of PHC services and household utilization of PHC
services, good performance of PHC workers is associated with better utilization of PHC
services. Thus by extension, this study shows that well-functioning VDCs and WDCs are
positively associated with utilization of PHC services.
Another study was conducted in 2004 in Oji River LGA in Enugu State, South East Nigeria
to determine the utilization of maternal and child health care services in health centres
before and after the introduction of the Bamako Initiative programme in South East Nigeria.
The study consisted of a descriptive cross-sectional component which was conducted in
December 2001 and a longitudinal retrospective component which spanned from January
1989 to December 2001. Data were collected from 405 women in 405 different households
who had at least one child not older than 12 months using interviewer-administered
structured questionnaires as well as from health centre records. Findings revealed that there
was an overall upward trend for ANC attendance, deliveries, as well as measles and OPV1
immunizations.88 The Bamako Initiative which was adopted by Nigeria in 1988, is a strategy
to strengthen PHC, one of its five components being community participation through
functional village, ward and LGA level committees.89 Since functional VDCs and WDCs
help to drive any successful Bamako Initiative programme, the increase in PHC services
utilization in this study can indirectly be attributed to functional VDCs and WDCs.

53
The studies described in this section showed directly or indirectly that well-functioning
VDCs and WDCs were associated with better utilization of PHC services.
CHAPTER THREE
3.0 MATERIALS AND METHODS
3.1 Study Area
The study was conducted in Benin City, the capital of Edo State, located in the South-South
geopolitical zone of Nigeria. It occupies a strategic position as the gateway to eastern,
western, southern and northern parts of Nigeria. Benin City comprises of three Local
Government Areas namely; Oredo, Egor and Ikpoba-Okha and serves as the headquarters of
Oredo LGA. It lies within latitudes 6ᵒ26’N and 6ᵒ31’N and longitudes 5ᵒ35’E and 5ᵒ41’E
with an average elevation of 77.8 meters above sea level. It has a population of 1,086,882,
the population of the three Local Government Areas in Benin City (Oredo, Egor and Ikpoba-
Okha) being 374,515; 340,287 and 372,080 respectively with a male to female ratio of
approximately 1:1 in all three LGAs.90 The predominant tribe in Benin City is Benin while
the predominant religion is Christianity.

54
Oredo, Egor and Ikpoba Okha LGAs have 12, 10 and 10 wards respectively. There are 40
government owned Primary Health Care facilities in Benin City with 12, 8 and 20, in Oredo,
Egor and Ikpoba Okha LGAs respectively. All the PHC facilities in Oredo and Ikpoba Okha
LGA are Primary Health Centres, similarly 6 out of the 8 PHC facilities in Egor LGA are
Primary Health Centres.
Ten out of the twelve Primary Health Centres in Oredo LGA are in Iyekogba ward (Ward 2)
while New Benin and Ikpema wards have one PHC each. The remaining 9 wards in Oredo
LGA have no Primary Health Care facilities. In Iyekogba ward, 8 out of the 10 PHCs are
operational. The operational PHCs in Ward 2 are: Oredo, Ugbor, Ekae, Evbuodia, Utagban,
Aruogba, Emwinyomwanru and Igogogi PHCs. In Ikpoba Okha LGA, the 20 Primary
Health Centres are distributed across 9 of the wards. These wards are Ute, oregbeni,
Ogbeson, Ukhiri, Evbomodu, Ugbekun, Irhinwinrin, ogheghe and Ologbo wards. Only
Evbuoriaria ward has no PHC.
In Oredo LGA, there are 11 WDCs and 3 VDCs. Each of the 12 wards in Oredo LGA except
Iyekogba ward has a WDC. Iyekogba ward, because of its large size has 3 VDCs instead of
a single WDC. The VDCs in ward 2 are located in Evbuodia, Utagban and Ekae
communities. In Ikpoba Okha LGA, there are 4 Ward Development Committees located in
Ute, Oregbeni, Ugbekun and Ologbo wards. All the WDCs and VDCs in Oredo and Ikpoba-
Okha LGAs were inaugurated by officials of the NPHCDA. However in Egor LGA, no
WDC has been inaugurated by the NPHCDA.
3.2 Study Design: The study was a descriptive cross sectional study
3.3 Scope of Study

55
This study assessed the composition and functionality of development committees. The
criteria for this assessment was based on the guidelines outlined in the ‘NPHCDA National
Guidelines for Development of Primary Health Care System in Nigeria’.9 Household
utilization of PHC service was also assessed. The assessment of household utilization of
PHC services in Benin City was based on the Ward Minimum Health Care Package.91 This
package comprises six interventions as follows: Control of Communicable Diseases, Child
Survival, Maternal and Newborn Care, Nutrition, Non-communicable Disease Prevention
and Health Education and Community Mobilization.
The assessment of utilization of PHC services covered three of the domains of the Ward
Minimum Health Care Package as follows: Child Survival, (breastfeeding, complementary
feeding, immunization, ORS for management of diarrhea) Maternal Care (Antenatal care,
delivery and post-natal care) Newborn Care and Health Education and Community
Mobilization. For child survival, only utilization of immunization services was assessed, as
the others sub-domains are components of key household practices to be adopted by the
mothers of the under-fives and not necessarily in themselves services rendered by the PHC
facilities. This assessment was done using the household questionnaire. An assessment of
the readiness of PHC facilities to deliver these domains of the Ward Minimum Health Care
Package was also carried out using a checklist. The first two domains were chosen because
issues of maternal newborn and child health are of serious Public Health importance in
Nigeria as well as globally as evidenced by MDGs 4 and 5. The choice of the third domain
was informed by the fact that health education and community mobilization are directly
linked with community participation.
3.4 Study Population: This consisted of:
56
1. Mothers of under five children in selected communities in Benin City
2. Community Health Officers (CHOs), nurse/midwives, Community Health Extension
workers (CHEWs), Junior CHEWs and doctors in selected communities in Benin
City.
3. Village Development Committee members in selected communities in Benin City.
4. Ward Development Committee members in selected wards in Benin City.
5. Key persons in the community such as Community Chiefs, Local Government
Chairmen and Local Government PHC coordinators in selected communities and
Local Government Areas in Benin City.
6. Primary Health Care facilities in selected LGAs in Benin City.
3.5 Selection Criteria
3.5.1 Inclusion Criteria
Mothers of under-five children: Mothers of under-five children residing in wards with
both an NPHCDA inaugurated Ward Development Committee and at least one Primary
Health Centre were included in the study.
Any mother of one or more under-five children who had lived in the community for a
minimum of 6 months was included in the study.
Community Health Officers (CHOs), nurse/midwives, Community Health Extension
workers (CHEWs), Junior CHEWs and doctors: These cadre of PHC facility workers in
selected PHC facilities that had been on the job for at least 6 months and gave their consent
were interviewed.

57
Village Development Committees Members: Members of VDCs that had been in
existence for at least 6 months were included. Some members were purposively selected for
Focus Group Discussions.
Ward Development Committees Members: Members of WDCs that had been in existence
for at least 6 months were included. Some members were purposively selected for FGDs.
Key persons in the community: Key persons such as Community Chiefs, Local
Government Chairmen, Local Government PHC coordinators and a zonal representative of
NPHCDA that had occupied their current position for at least 6 months were included
Primary Health Care Facilities: All PHC facilities in the selected wards were studied.
Information about the facilities was obtained from the heads of the facilities or their
representatives.
3.5.2 Exclusion criteria
Wards without NPHCDA-inaugurated VDCs/WDCs as well as PHC facilities were
excluded.
Mothers of Under-fives who were visitors to the surveyed communities were excluded from
the study.
3.6 Sample Size Determination for mothers of under-five children
Sample size was determined using Cochran’s formula for studying proportions in cross
sectional studies92 as follows:
Where n = desired sample size for a population greater than 10,000

58
Z = Standard Normal Deviate usually set at 1.96 which corresponds to 95% confidence
level.
p = proportion of people in the target population estimated to have a characteristic of
interest.
d = Degree of precision desired usually set at 0.05
However to compensate for the design effect, D, which is 1 for simple random sampling and
1-2 for other sampling techniques; in order to compensate for deviation from the simple
random sampling procedure, the formula is modified as shown below93:
In this study, the characteristic of interest was the proportion of household members that had
ever utilized PHC services in the Niger Delta region of Nigeria; p = 0.5894
D = 2.0 for multistage sampling technique
Substituting in the formula
Calculating for a 10% non-response rate
Where nf = final minimum sample size
NRR = Non-response rate
Final minimum sample size = 833.

59
However data were collected from 840 mothers of under-fives.
3.7 Sampling Technique for mothers of under-five children
A multistage sampling technique consisting of three stages was used in selecting the mothers
of under-five children. Oredo and Ikpoba-Okha LGAs were used because they were the only
ones with both PHC facilities and NPHCDA-inaugurated WDCs. In Oredo LGA, only 3
wards had both PHC facilities and NPHCDA-inaugurated WDCs, while in Ikpoba-Okha
LGA only 4 wards had both PHC facilities and NPHCDA-inaugurated WDCs.
Stage 1: Selection of Wards
Two wards each were selected from the 3 wards in Oredo and the 4 wards in Ikpoba-Okha
LGAs which had both Primary Health Centres and NPHCDA inaugurated WDCs. This was
done by simple random sampling, using balloting. Thus Iyekogba and Ikpema wards were
selected in Oredo LGA, while Ugbekun and Oregbeni wards were selected in Ikpoba-Okha
LGA. Two wards were chosen from each LGA because they provided more VDCs/WDCs
for assessing the relationship between utilization of PHC services and well composed and
functional VDCs and WDCs.
Stage 2: Selection of Communities
From each of the four wards selected above, one community each was selected, making a
total of four communities. To do this a list of the communities in each ward was obtained

60
from the Social Development Department of the Local Government secretariat and one
community was selected from each ward by simple random sampling using balloting.
However, in Iyekogba ward simple random sampling using computer generated random
numbers was done because of the large number of communities (48). The random numbers
were generated using Win-pepi software. Thus four communities were selected and coded as
communities A, B, C and D; from Iyekogba and Ikpema wards in Oredo LGA and Ugbekun
and Oregbeni wards in Ikpoba Okha LGA respectively.
Stage 3: Selection of Mothers of under-five children
In each of the 4 communities, two main clusters separated by a major street were identified
and 1 cluster was selected by simple random sampling, using balloting. All the eligible
mothers of under-five children in households in the selected clusters were interviewed. Any
house in the selected communities which had at least one household, with one or more
mothers of under-fives who met the selection criteria was eligible for the study. The eligible
mothers were identified by asking them preliminary questions based on the selection criteria.
They were asked if they were visitors or permanent residents in the community, and how
long they had resided in the community, if they were permanent residents. Permanent
residents who had lived in the community for a minimum of 6 months were interviewed.
3.8 Selection of the other respondents
3.8.1. PHC facility workers
All the PHC facility workers (CHOs, nurses/midwives, CHEWs, JCHEWs and doctors) in
the four selected communities were interviewed. The four communities were selected as
described in stages 1 and 2 of section 3.7 above. The PHC facility workers were interviewed

61
using the PHC questionnaire. Repeated visits were made to the PHC facilities until all the
workers were interviewed.
3.8.2 Members of VDCs and WDCs
In the LGAs surveyed, (Oredo and Ikpoba-Okha), ten members of each of the VDCs and
WDCs in the wards with both PHC facilities and NPHCDA-inaugurated Development
Committees were interviewed. There were 3 VDCs and 4 WDCs that met this criterion. The
ten members were purposively selected from each of the VDCs and WDCs in the surveyed
LGAs. The selected members included available members of the executive and other
committed members. A total seven FGDs were thus held with the members of the
Development Committees using the FGD guide.
3.8.3 Key Informants: They were all purposively selected on the basis on their roles in the
PHC system. In the 2 LGAs surveyed, the PHC Coordinators were selected as key
informants because they are the heads of the PHC system at the LGA level and are in charge
of coordinating all PHC activities in the LGA. The Zonal representative of the NPHCDA
was selected because she is the local representative of the NPHCDA, the body designated to
co-ordinate the PHC system in Nigeria. One community leader was selected from each of
the two LGAs. They were selected because they represent the communities and are
knowledgeable about all PHC-related community activities. Thus a total of five key
informants were interviewed using the Key Informant Interview guides.
3.9 Data Collection
3.9.1 Tools for Data Collection
A combination of quantitative and qualitative data collection tools were used to collect data
relevant to the study objectives.

62
Quantitative Data Collection Tools: This consisted of questionnaires as follows:
1. Household Questionnaire
2. PHC workers’ questionnaire
3.9.2 Quantitative Data Collection Methods
3.9.2.1 The household questionnaire survey:
A purpose-designed, semi-structured interviewer-administered questionnaire with open and
closed ended questions was administered to the mothers of under-five children (Appendix
1). This questionnaire consisted of five sections. The first section was on the socio-
demographic characteristics, the second section was on general utilization of Primary Health
Care services and associated factors, the third was on utilization of maternal health services,
the fourth section was on utilization of child-survival services and the fifth was on
utilization of health education and community mobilization services.
3.9.2.2 The Primary Health Care Workers’ Questionnaire Survey: Data were collected
using a semi-structured interviewer-administered questionnaire with open and closed ended
questions, designed by the researcher (Appendix 2). The questionnaire was adapted from
relevant sections of the ‘Minimum Standards for Primary Health Care in Nigeria’.95 It
consisted of sections on the socio-demographic profile of the respondents, delivery of
maternal and newborn, child health and health education and community mobilization

63
services. It was administered to all the health care workers that met the inclusion criteria in
the four PHC facilities in the surveyed communities.
3.9.3 Qualitative Data Collection Tools: These consisted of a Focus Group Discussion
Guide (Appendix 3), three Key Informant Interview Guides (Appendices 4-6) and an
Observational Check List (Appendix 7).
3.9.4 Qualitative Data Collection Methods
3.9.4.1 Focus Group Discussion: One Focus Group Discussion each was held with
members of the 3 Village Development Committees in Iyekogba ward and members of the 4
Ward Development Committees in the wards where the survey was conducted, giving a total
of 7 FGDs. The WDCs were selected purposively based on their presence in the wards
where the survey was conducted. New Benin WDC, being the only other Ward
Development Committee in ward 2 with a PHC, was also included. In each of the
committees, ten out of twenty members, were purposively selected for the FGDs to include
both male and female as well as members holding elective positions. The purpose of the
focus group discussions was to explore the members understanding of their roles as
development committee members, the extent to which they had been able to perform their
roles and factors influencing the functioning of their committees.
Each of the focus group discussion sessions was conducted by the researcher and two
assistants who simultaneously took notes and did audio recording. It was conducted with an
interactive guide designed to meet the objectives of this study. Opening, topical and probing

64
questions designed to stimulate interest in the group process and to elicit the participants’
initial perceptions about the general theme were asked. The general topical themes for the
discussions included: Meaning of a Development Committee, (VDC and WDC), functions
of a development committee, factors affecting the functions of a development committee, as
well as achievements and challenges of the committees.
The sitting arrangement at each session was such that allowed for easy eye contact and
hearing between the principal facilitator and the participants. The participants were
encouraged to talk freely and spontaneously. Each discussion lasted for about 60 minutes
after which light refreshment was served to participants. No financial or other incentives
were offered to participants. This was to prevent any bias from occurring. The notes and
recordings were transcribed within 48 hours, using thematic analysis to identify recurrent
themes in the committee members’ responses.
3.9.4.2 Key Informant Interviews: Key Informant Interviews were conducted using the Key
Informant Interview guides which were used to guide discussions with Key Informants. The
Key Informants that were interviewed included the 2 Medical officers of Health of Oredo
and Ikpoba Okha LGAs who also represented their respective Local Government Chairmen,
the zonal NPHCDA focal person, and 2 community leaders, one each from Oredo and
Ikpoba Okha LGAs. Thus a total of 5 key informants were interviewed. These key informant
interviews were conducted to assess the awareness of the key informants of the existence of
the Development committees, their knowledge concerning the roles of development
committees, their knowledge and perceptions of the activities of the committees their
awareness of the achievements or challenges of these committees.

65
3.9.4.3 Observation: Observations were carried out using the Observational Check List for
assessment of facility readiness to deliver Primary Health Care Services. The check list
assessed the readiness of the PHCs to deliver the components of the WMHCP covered in
this study, in terms of infrastructure, furnishings, medical equipment, personnel and hours of
operation. It was utilized in 11 Primary Health Centres, 8 of which were in ward 2
(Iyekogba ward), Oredo LGA while the each of other 3 were in Ikpema ward, Oredo LGA,
and Ugbekun and Oregbeni wards, Ikpoba-Okha LGA.
3.9.5 Specific objectives and the tools that were used to achieve them
Objectives Tools
1. To assess the composition and
functionality of development
committees in Benin City.
FGD guide for VDCs and WDCs
2. To determine the factors that are
associated with the establishment of
well composed and functional
development committees in Benin
City.
FGD guide for VDCs and WDCs
KII Guides

66
3 To determine the readiness of health
facilities in villages or wards with
functional development committees
to deliver some of the ward
minimum health care package
services in Benin City.
Observational check list for PHC
facilities
4 To assess household members’
utilization of Primary Health Care
services in Benin City
Household questionnaire
Objectives Tools
5 To assess the performance of
primary health care workers with
respect to the delivery of some
components of the ward minimum
health care package in Benin City
PHC workers questionnaire
6 To determine the relationship
between performance of the PHC
workers and household utilization of
PHC facilities in Benin City
PHC workers questionnaire
Household questionnaire

67
7. To determine the relationship
between utilization of PHC services
and well composed and functional
development committees.
Household questionnaire
FGD guide for VDCs and WDCs
3.10 Research Assistants: A team of five research assistants consisting of 500 level
medical students from the University of Benin, were recruited to assist in data collection
during the survey. They were trained for two days by the primary researcher to enhance
uniformity in data collection in terms of validity and repeatability.
3.11 Pretesting: The questionnaires were pretested in Ekpoma in Esan West LGA of Edo
State. This helped to enhance validity as well as reliability of the survey instruments.
3.12 Data Management
3.12.1 Data Analysis: The questionnaires were screened for completeness by the primary
researcher, coded and the data were entered into the Statistical Package for the Social
Sciences (IBM SPSS) Version 20. Quantitative data were analysed using this software. An
initial univariate analysis was carried out for all variables to check their distribution.
Summary statistics like the mean and standard deviation were computed for quantitative
variables like age. Total and percentage scores for PHC utilization, performance of PHC
workers, readiness of PHCs, composition and functionality of VDCs/WDCs were computed.

68
Bivariate analysis was carried out using Spearman’s test of correlation with the level of
significance set at p < 0.050. This test was used because the number of items per variable
used for the analyses were few (less than 10). For this number of items, use of a parameric
test (Pearson’s test of correlation) would violate the basic assumption of the Central Limit
Theorem required for the use of such tests. Rank correlation coefficients of 0.000, 0.001 to
0.090, 0.100 to 0.499, 0.500 to 0.949, 0.950 to 1.000 were classified as no, little or no, weak
and strong or perfect correlation respectively. Positive correlation coefficients were
interpreted as positive relationships in which increase in one variable resulted in increase in
the other, while negative correlation coefficients were interpreted as negative relationships
in which increase in one variable led to decrease in another and vice versa. Bivariate
analyses were carried out between readiness of PHCs and functionality of VDCs/WDCs,
performance of PHC workers and utilization of PHC services, composition of development
committees and utilization of PHC services and functionality of development committees
and utilization of PHC services.
Transcripts from qualitative interviews were read several times by the primary researcher,
within 48 hours of the interviews, to identify themes and categories. A coding frame was
developed and transcripts were coded. The coding helped in the analysis of the different
themes that emerged from the transcripts. Validity of information obtained from the
qualitative interviews was enhanced by coding consistency check by an independent coder
and triangulation where data obtained from the qualitative interview were compared with
those obtained from the quantitative survey.
Data were presented using simple frequency tables, descriptive statistics like mean and
standard deviation and charts. Information obtained from bivariate analyses were presented

69
using contingency tables. Data obtained using qualitative data collection tools were
presented as prose.
3.12.2 Scoring System for Utilization of PHC Services
There were 30 questions on utilization of PHC services. Of these, 17 were used for the
scoring. The 13 questions that either addressed the factors associated with utilization or were
introductory in nature were not used for scoring. For the questions that had yes/no answers
or only one correct answer, each correct answer attracted a score of 1 mark, and each wrong
answer a score of 0. For questions with sub-questions, each correct answer to a sub-question
also attracted a score of 1 mark, and each wrong response a score of 0. For those that
required listing of items, a score of 1 was allocated for each correct item mentioned, with the
maximum score being equal to the number of items required. Composite scores were
computed for general utilization of PHC services and utilization of maternal health, child
survival and health education/community mobilization services. The maximum obtainable
scores for each of the domains were 7, 3, 12 and 8 marks respectively. The percentage
composite scores for each of the domains were computed and 70% and above was graded as
good utilization, 50 to 69.9% was graded as fair utilization and a score of less than 50% was
graded as poor utilization for each of the 4 domains. The summary percentage scores for all
the four domains were calculated by computing the averages of the percentage scores in
each of the 4 domains. Summary percentage scores for utilization of PHC services in the
four domains were categorized into poor, fair and good utilization for scores in the range of
(0.0 – 49.9) %, (50.0 – 69.9) % and ≥70% respectively.

70
The questions used for scoring utilization were tested for reliability using a test-retest
correlation method. They showed a high degree of reliability, with a Pearson’s correlation
coefficient of 0.925 (p < 0.001).
3.12.3 Scoring System for Performance of PHC Workers
In the PHC workers’ questionnaire 77 questions addressed performance. Of these questions,
24 assessed whether or not an activity was carried out and for each of these, a score of 1 was
allocated for positive answers and a score of 0 for negative answers. Twenty one questions
assessed how health interventions were carried out, the number of times some health
interventions were carried out and number of cases managed. For these questions, scores in
the range of 0 to 4 marks were obtainable. For interventions that were not carried out
according to standard procedure, no score was awarded. For methods of health interventions,
marks were awarded based on the number of ways an intervention could possibly be carried
out. A maximum of 3 marks was awarded for interventions carried out according to standard
procedures in up to 3 different ways at some time in the past. For number of times an
intervention was carried out, the frequencies were split into four groups. The group with the
lowest range was allocated a score of 1 while that with the highest range was allocated a
score of 4. Seven questions required listing the answers, and for each item correctly listed, a
score of 1 was awarded, with the maximum score being equal to the number of items
required. Composite scores for performance were computed for delivery of services in each
of the domains assessed (maternal/newborn, child survival and health education/community
mobilization). The maximum obtainable scores for performance in each of the domains were
75, 26 and 12 respectively. Composite scores in each of the domains were computed by
summing up the scores obtained for the questions used in assessing that domain. Percentage

71
composite scores were computed. For each of the four domains, performance was
categorized into poor, fair and good, for percentage scores in the range of (0.0 – 49.9) %,
(50.0 – 69.9) % and ≥70% respectively. Summary scores for performance in all four
domains were calculated by computing the average of the percentage scores in each of the
four domains. Thus, performance in the delivery of PHC services in all four domains was
categorized as poor, fair and good respectively for summary scores in the range of (0.0 –
49.9) %, (50.0 – 69.9) % and ≥70% respectively.
The questions used for scoring performance were tested for reliability using a test-retest
correlation method, and showed a high degree of reliability, with a Pearson correlation
coefficient of 0.993 (p < 0.001).
3.12.4 Scoring System for PHC Facility Readiness
The observational checklist assessed the infrastructure, equipment/furnishings and
personnel/hours of operation. The PHC facilities were scored based on the presence or
absence of the items on the observational checklists for PHC facilities. For all the Primary
Health Care facilities, a score of 2 was given where the infrastructure or facility was present
and functional, a score of 1 was given where it was present but non-functional while a score
of 0 was given where the infrastructure or facility was absent. Where the checklist specified
a given number of equipment, facilities or infrastructure, a score of 1 was given for each
item that was present and functional up to a maximum of the number specified and a score
of zero was given where the item was completely absent. Where the facility was present but
non-functional, a score of 0.5 was given for each item. In the case of the Primary Health
Centre that ought to render 24-hour services, a score of 1 was given if they rendered services
from 8am to 4pm (i.e. morning shift only), a score of 2 was given if they rendered service

72
from 8am to 8pm (i.e. morning and afternoon shift) and a score of 3 was given if they
rendered service from 8am to 8am (i.e. morning, afternoon and night shifts). The maximum
scores obtainable for each of the 3 domains (infrastructure, equipment/facilities and
personnel/hours of operation) were 67, 216 and 42 respectively. Composite scores in each of
the domains were computed by summing up the scores obtained for the questions used in
assessing that domain. Percentage composite scores were computed for each of the domains
and readiness of the PHC facilities to deliver some components of the WMHCP was
classified into ‘not ready’, ‘fairly ready’ and ready for percentage composite scores in the
range of (0.0 – 49.9) %, (50.0 – 69.9) % and ≥70% respectively. Summary scores for
readiness of the PHC facilities to deliver some components of the WMHCP were calculated
by computing the average of the percentage composite scores for all the 3 domains.
Summary scores for PHC facility readiness in all 3 domains were categorized into ‘not
ready’, ‘fairly ready’ and ready for scores in the range of (0.0 – 49.9) %, (50.0 – 69.9) %
and ≥70% respectively.
3.12.5 Scoring system for composition and functionality of Development Committees
There were 17 criteria for well composed and functional VDCs and WDCs; 6 for the
composition, and 11 for the functions of the committees. For the first four criteria on
composition of the committees, a mark of 2 was awarded for each criterion that was
fulfilled. The fifth criterion on composition had to do with representation of the different
sectors of the community or ward and the sixth was the representation of the various
communities in the ward or the streets/units in the community. For the fifth criterion, a
maximum score of 14 was obtainable for the VDCs/WDCs, 2 scores each for educational,
commercial, agricultural, orthodox health sector, traditional health sector, religious, and
youth. The scores obtainable for representation of the communities or streets were awarded

73
based on the proportion represented. For less than 50%, 50 – 69.9% and 70% or greater
representation, scores of 1, 2 and 3 respectively were awarded. Thus the maximum score
obtainable for composition was 25. There were 11 questions on the functions of the
committees. Two marks each were awarded for each function that was present. Thus for
functionality a maximum of 22 marks was obtainable for both VDCs and WDCs.
Composite scores for composition were computed by summing up the scores obtained for
each of the criteria on composition. The scores obtained were converted to percentages. Any
committee scoring 70% or more was graded as well composed, those scoring 50 – 69.9%
were graded as fairly well composed, while those scoring 0 – 49.9% were graded as poorly
composed. Composite scores for functionality were computed by summing up the scores
obtained for each of the criteria on functionality. Scores were converted to percentage scores
and any committee scoring 70% or more was graded as functional, those scoring 50 – 69.9%
were graded as fairly functional, while those scoring 0 – 49.9% were graded as poorly
functional.
3.12.6 Classification of Occupation: The International Labour Organisation (ILO)
International Standard Classification of Occupations (ISCO) based on skill levels was used
as follows96:
Skill Level 1: Many occupations at this skill level may require physical strength and/or
endurance. Some may require basic skills in numeracy and literacy. Occupational groups
classified under this skill level include elementary occupations and armed forces
occupations. In this study, occupations classified under this skill level included: cooks,
cleaners, laundry men/women and small scale farmers.

74
Skill Level 2: Occupations at this skill level typically require the performance of tasks such
as operating machinery and electronic equipment; driving vehicles, maintenance and repair
of electrical and mechanical equipment and manipulation and ordering and storage of
information. Occupational groups classified under this skill level include clerical support
workers, services and sales workers, skilled agricultural, forestry and fishery workers, craft
sand related trades workers, and plant and machine operators and assemblers. In this study,
occupations included in this skill level included: hair dressers, tailors, drivers, mechanics,
plumbers, welders, and other similar occupations.
Skill Level 3: Occupations at this skill level typically involve the performance of complex,
technical and practical tasks that require and extensive body of factual technical and
procedural knowledge in a specialized field. Occupations at this skill level generally require
a high level of literacy and numeracy and well developed interpersonal communication
skills. The occupational groups classified under this skill level are the technicians and
associate professionals. In this study, occupations classified under this sill level included:
nurses, business managers, clerical staff, computer operators, among others.
Skill Level 4: Occupations at this skill level typically involve the performance of tasks that
require complex problem-solving, decision-making and creativity based on an extensive
body of theoretical and factual knowledge in a specialized field. The tasks performed
typically include analysis and research to extend the body of human knowledge in a
particular field, diagnosis and treatment of disease, imparting knowledge to others, and
design of structures or machinery and of processes for construction and production.
Occupations at this skill level generally require extended levels of literacy and numeracy,
and excellent interpersonal communication skills. The occupational groups classified under

75
this skill level are professionals, managers and armed forces occupations. In this study,
occupations classified under this skill level included: doctors, engineers, secondary school
teachers, medical laboratory scientists, computer scientists, business managers, among
others.
3.12.7 A summary of specific objectives and their outcome measures
Specific Objectives Outcome measures

76
1 To assess the composition and
functionality of development
committees in Benin City
Composite and summary scores for composition
(obtained from criteria for well composed VDCs
WDCs [Appendix 8])
Composite and summary scores for functionality
(obtained from criteria for functional VDCs and
WDCs [Appendix 8])
2 To determine the factors
associated with the
establishment of well composed
and functional Development
Committees
Findings were obtained from (FGDs and KIIs)
3 To determine the readiness (in
terms of adequate staffing and
equipment) of health facilities in
villages or wards with functional
Development Committees to
deliver some of the WMHCP
services in Benin City
Composite and summary scores for readiness
obtained from scores for infrastructure,
equipment/facilities and personnel/hours of
operation.
Specific Objectives Outcome measures

77
4 To assess household members’
utilization of PHC services in
Benin City.
Composite and summary scores for utilization
derived from scores from 4 domains of utilization:
utilization of general PHC services, maternal health,
child survival and health education/community
mobilization services
5 To assess the performance of
PHC workers with respect to the
delivery of some components of
the WMHCP in Benin City
Composite and summary scores for performance
derived from the scores for each of the 3 domains
assessed: (performance in the delivery of
maternal/newborn, child survival and health
education/community mobilization services).
6 To determine the relationship
between performance of PHC
workers and household
utilization of PHC services in
Benin City
Spearman’s rank correlation coefficient and its p
value. This was used to determine the presence of a
positive or negative relationship or the absence of
any relationship.
7 To determine the relationship
between utilization of PHC
services and well composed and
functional Development
Committees
Spearman’s rank correlation coefficient. This was
used to determine the presence of a positive or
negative relationship or the absence of any
relationship.
3.13 ETHICAL CONSIDERATIONS: Ethical clearance was obtained from the Ethics
and Research Committee of the University of Benin Teaching Hospital. Assent was

78
obtained from the LGA chairmen, the LGA PHC Coordinators and the heads of the various
PHCs where the study was carried out. In addition, assent was obtained from the various
heads of the communities where questionnaires were administered or FGDs carried out.
Written informed consent was obtained from each respondent. The respondents were
assured of confidentiality and told that at any time they wished to discontinue participation
they were free to do so without fear of untoward consequences.
Confidentiality was assured by making use of codes for all the units of the sub-sets of the
study population. The communities were identified with alphabets, the mothers of under-
fives, PHC workers, VDCs, WDCs and PHCs were identified by serial numbers. Their
identities were not disclosed to anyone not involved in the research. The 4 communities
surveyed were coded as A, B, C, D, the mothers of under-five as 1 – 840, the PHC workers,
as 1 – 29, the VDCs as 1 - 3, the WDCs as 1 – 4 and the PHCs as 1 – 11.
Respondents who were found to be ill during the course of the study were given medical
attention by the researcher and referred to PHC facility, where necessary. Cases seen during
the survey included malaria, upper respiratory tract infections and hypertension. Those with
hypertension who were already being managed by qualified medical personnel were
counselled on the need for lifestyle changes and compliance with medication. In addition
study participants were educated concerning maternal, newborn and child health issues.
The study posed minimal risk of harm or injury to the respondents and any probable risk that
may have been associated with the disclosure of information obtained during the study was
minimized by the use of codes for the units of the different sub-sets of the study population.
Data was stored safely and was made accessible to only those involved in the research.

79
3.14 LIMITATIONS OF THE STUDY
Data from the household survey, Focus Group Discussions and Key Informant Interviews
were based on self-report and this may have been subject to information (response and
recall) bias. However, this limitation was minimized by good questionnaire design, careful
questionnaire administration by the researcher and trained research assistants, as well as
triangulation of data collected from quantitative and qualitative sources.
CHAPTER FOUR
4.0 RESULTS

80
A total of 840 mothers of under-five children participated in the household survey and a
total of 29 PHC workers, participated in the PHC workers’ performance survey. Selected
members of 3 VDCs and 4 WDCs participated in the FGDs, and 11 health facilities were
assessed for readiness. The results of the study are presented in sections as listed below:
Section 4.1: Socio-demographic characteristics of the respondents.
Section 4.2: Composition and functionality of Development Committees.
Section 4.3: Factors associated with the establishment of well composed and functional
Development Committees.
Section 4.4: Readiness of health facilities in villages and wards with functional
Development Committees to deliver some of the Ward Minimum Health Care Package
services.
Section 4.5: Household members’ utilization of Primary Health Care services.
Section 4.6: Primary Health Care facility workers’ performance with respect to the delivery
of some components of the Ward Minimum Health Care package.
Section 4.7: Relationship between performance of the Primary Health Care facility workers
and household utilization of PHC facilities.
Section 4.8: Relationship between utilization of PHC services and well composed and
functional development committees.
Section 4.1 Socio-demographic characteristics of the respondents
Table 4.1.1: Socio-demographic characteristics of mothers of under-five children

81
Variables Frequency (n = 840) Percent
Age group (years)
15 – 24 112 13.3
25 – 34 541 64.4
35 – 44 173 20.6
45 – 49 14 1.7
Mean age = 30.6 ± 5. 5 years
Marital Status
Married 694 82.6
Cohabiting 121 14.4
Separated 10 1.2
Single 6 0.7
Widowed 5 0.6
Divorced 4 0.5
Religion
Christianity 815 97.0
Islam 20 2.4
African Traditional Religion 5 0.6
Educational Status
No formal education 12 1.4
Primary uncompleted 24 2.9
Primary completed 112 13.3
Secondary uncompleted 198 23.6
Secondary completed 315 37.5
Tertiary uncompleted 23 2.7
Tertiary completed 156 18.6
Occupational Status
Skill level 1 12 1.4
Skill level 2 625 74.4
Skill level 3 22 2.6
Skill level 4 77 9.2
Unemployed 104 12.4
Table 4.1.1 contd: Socio-demographic characteristics of mothers of under-five children
Variables Frequency (n = 840) Percent
Ethnicity

82
Benin 346 41.2
Esan 153 18.2
Igbo 130 15.5
Afenmai 63 7.5
Urhobo 35 4.2
Delta Ibo* 35 4.2
Yoruba 30 3.6
Calabar** 20 2.4
Isoko 9 1.1
Ijaw 7 0.8
Ogoni 4 0.5
Others*** 8 1.0
* refers to Ika, Ukwani, Anioma, Asaba.
** refers to Efik, Ibibio, Ogoja, Eket, Annang.
*** refers to Idoma, Igala, Hausa, Itsekiri, Kanuri.
A higher proportion, 541 (64.4%) of the mothers of under-fives were in the age group, 25 –
34 years, with a mean age of 30.6 ± 5.5 years. Majority, 694 (82.6%) were married, while 6
(0.7%) were single. Almost all 815 (97.0%) the respondents were Christians. A larger
proportion, 315 (37.5%) of the respondents completed secondary level of education, 198
(23.6%) of the respondents did not, while only a small proportion 12 (1.4%) had no formal
education. Majority 625 (74.4%) of the respondents were in occupations categorized under
skill level 2.
Table 4.1.2: Monthly Income of Mothers of Under-five Children
Monthly Income Range (N) Frequency Percent

83
<18,000 488 71.6
18,000-50,999 163 23.9
51,000-120,999 26 3.8
≥121,000 5 0.7
Total 682 100.0
Out of a total of 840 respondents, 104 (12.4%) were unemployed, with no regular source of
income, and 54 (6.4%) were unwilling to divulge their income. Out of the remaining that
divulged their income, a majority 488 (71.6%) earned below an average of N18,000, while
only a very small proportion, 5 (0.7%) earned up to N121,000 or greater monthly.
Table 4.1.3: Occupational status and educational status of the spouses/partners of the
mothers of under-five children

84
Variable Frequency (n = 815) Percent
Occupational status
skill level 1 31 3.8
skill level 2 603 74.0
skill level 3 65 8.0
skill level 4 100 12.3
Unemployed 16 1.9
Educational status
No formal education 4 0.5
Primary uncompleted 13 1.6
Primary completed 59 7.2
Secondary uncompleted 73 9.0
Secondary completed 410 50.3
Tertiary uncompleted 27 3.3
Tertiary completed 229 28.1
Of the 840 mothers of under-fives, 815 (97%) were either married or co-habiting. The
remaining 25 (3%) were separated, divorced, widowed or single. Majority, 603 (71.8%) of
the spouses/partners were in occupations categorized under skill level 2, while a small
proportion 31 (3.7%), was employed at skill level 1. A higher proportion, 410 (50.3%) of the
respondents’ spouses completed their secondary education while only a small proportion, 4
(0.5%) had no formal education.
Table 4.1.4: Monthly income of spouses/partners of the mothers of under-five
children
Monthly Income (N) Frequency Percent

85
<18,000 183 24.3
18,000 - 50,999 380 50.4
51,000 - 120,999 148 19.6
≥121,000 43 5.7
Total 754 100.0
Of the 815 respondents’ spouses/partners, 16 (2.0%) were unemployed and 45 (5.5%) did
not divulge their income to their spouses/partners. For the 754 (92.5%) whose income were
revealed, half, 380 (50.4%) earned a monthly income in the range of N(18,000 – 50,999); a
quarter, 183 (24.3%) below N18,000 while a small proportion, 43 (5.7%) earned up to or
above N121,000.00, monthly.
Table 4.1.5: Socio-demographic characteristics of Primary Health Care workers
Variable Frequency (n = 29) Percent
Age (years)

86
26 – 35 14 48.3
36 – 45 9 31.0
46 – 55 4 13.8
56 – 65 2 6.9
Mean age = 37.9 ± 9.5 years
Designation
SCHEW 13 44.8
Nurse/Midwife 9 31.0
JCHEW 3 10.3
CHO 2 6.9
Medical Officer 2 6.9
Marital Status
Single 4 13.8
Married 25 86.2
Ethnic group
Benin 18 62.1
Esan 5 17.2
Afenmai 2 6.8
Igbo 2 6.8
Ijaw 1 3.4
Yoruba 1 3.4
A higher proportion, 14 (48.3%) of the PHC workers were in the 26 – 35 year age bracket,
followed by a third, 9 (31.0%) in the 36 – 45 year bracket. The mean age of the PHC facility
workers was 37.9 ± 9.5 years. A little less than half, 13 (44.8%) of them were SCHEWs,
about a third, 9 (31.0%) were nurses/midwives while only 2 (6.9%) were doctors.
Majority 25 (82.6%) of the healthcare workers were married and a higher proportion 18
(62.1%) of the healthcare workers were Benin.

87
Section 4.2: Composition and Functionality of Village and Ward Development
Committees
Table 4.2.1 Composition of Village and Ward Development Committees

88
Variable Frequency n (%)
VDC (n = 3) WDC (n = 4)
Female membership (%)
≥ 20 2 (66.7) 4 (100.0)
< 20 1 (33.3) 0 (0.0)
Elected Chairman
Yes 3 (100.0) 4 (100.0)
Elected Secretary
Yes 3 (100.0) 4 (100.0)
Elected Treasurer
Yes 3 (100.0) 4 (100.0)
Street/community representation (%)
≥ 70 3 (100.0) 4 (100.0)
Sector Representation
Education
Yes 2 (66.7) 3 (75.0)
No 1 (33.3) 1 (25.0)
Commercial
Yes 2 (66.7) 4 (100.0)
No 1 (33.3) 0 (0.0)
Agricultural
Yes 3 (100.0) 4 (100.0)
Orthodox health
Yes 3 (100.0) 4 (100.0)
Traditional Health
Yes 2 (66.7) 1 (25.0)
No 1 (33.3) 3 (75.0)
Religious
Yes 2 (66.7) 1 (25.0)
No 1 (33.3) 3 (75.0)
Youth
Yes 3 (100.0) 3 (75.0)
No 0 (0.0) 1 (25.0)
From the findings of the FGD, 2 (66.7%) of the VDCs had female members constituting
20% or more of the total membership. The 3 (100.0%) VDCs had elected chairmen,
secretaries and treasurers and for all of them 70% or more of their streets or units were

89
represented. With respect to the educational, commercial, traditional health and religious
sectors, 2 (66.7%) of the VDCs had representatives; while for the agricultural, orthodox
health and youth sectors, all 3 VDCs had representatives.
The 4 (100%) WDCs had female members constituting 20% or more of the total
membership, 3 (75%) had representatives for the educational and youth sector, all 4 (100%)
of them had representatives for the commercial, agricultural and orthodox health sectors
while only 1 (25%) had representatives for the traditional health and religious sectors.

90
Fig 4.2.1 Composition of Village Development Committees
Two (66.7%) of the VDCs were well composed, while 1 (33.3%) was fairly well composed.
None was poorly composed.

91
Fig 4.2.2 Composition of Ward Development Committees
Three (75%) of the WDCs were well composed while 1 (25%) was fairly well composed.
None was poorly composed.

92
Focus Group Discussions and Key Informant Interviews on Functionality of VDCs and
WDCs
Frequency of Meetings
Findings from the FGDs revealed that two of the three VDCs (66.7%), had been having
monthly meetings, while for 1 (33.3%) of them, the frequency had dwindled to once in 6
months. Of the 4 WDCs, 3 (75%) were meeting monthly, while for 1 (25%) of them, the
frequency of meetings had also reduced to once in every six months. For those who held
meetings once every month, some of their members had stopped attending meetings because
of lack of financial incentives from the Local Government authorities. Those whose
meetings had dwindled to once in six months also gave lack of financial incentives as a
major reason for not holding meetings. Most of the discussants were of the opinion that
meetings would be more regular if there was money to convene the meetings, buy stationery
and provide some form of refreshment during the meetings. The following statement made
by one of the discussants aptly expressed the view of the generality of the FGD participants
regarding frequency of meetings.
“It is not easy to hold meetings because you have to make calls, which cost money, and
some of our members, they are very busy”
A male member of WDC 1
In addition to the view expressed above, some older discussants who no longer earned an
income spoke of their difficulty in attending meetings. This was as a result of inability to get
to the meeting venue because of lack of funds. In the words of one of the discussants:

93
“Most of the people don’t come again because there is no money involved. There is no
source of our income again, we’re no longer working, how can we hold meeting when no
money for paper to write, nothing to eat, nothing to drink?”
A male member of WDC 3
Taking of minutes during meetings and sending of minutes of meetings to the LGA
committees
All the VDC and WDC members took minutes during their meetings, but in WDC 1,
minutes were not taken most of the time because their meetings were usually brief due to
poor attendance. However, most of the discussants agreed that they did not forward their
minutes of meeting to the LGA committees. They were strongly of the opinion that since
their committees did not receive any financial support from the LGAs, they could not take
up the additional financial burden of transporting themselves to the LGA secretariat to
submit minutes of meetings. In the words of one of the WDC members:
“We cannot use our transport to go and submit minutes of WDC meetings to the LGA
headquarters when they are not paying us, no we cannot!”
A female member of WDC 4
Other reasons given for not submitting minutes of meeting to the LGA PHC committees
included the unwelcoming attitude of the LGA officials and lack of awareness of who to
report to. The PHC coordinators of the two LGAs however said that none of the committees
had been sending minutes to the LGA committees. One of them was of the opinion that the
committees probably preferred to send their minutes of meetings to the zonal office of the
NPHCDA. In his words:

94
“The WDCs do not bring their reports to the PHC Management Committee. They submit
their reports to NPHCDA directly because NPHCDA has been the one paying them their
sitting allowance or some monthly stipends.”
PHC coordinator, Ikpoba-Okha LGA
Relaying plans to the community
Two (66.7%) of the VDCs and 3 (75.0%) of the WDCs relayed their plans to the community
monthly while for 1 (33.3%) VDC and 1 (25.0%) WDC, the last time they communicated
any plans to the community members was 6 months prior to the FGD. Some of the VDCs
and WDCs relayed their plans to the community during community meetings while others
did so by delegating some members to go from house to house.
Identification of health needs in the communities and wards
All the Development committees had been involved in identifying health needs in their
communities and mobilizing the community for health actions. However in some of the
committees, community mobilization activities had been dormant for a while due to
discouragement as a result of lack of financial incentives from the Local Government and
failure of the Local Government authorities to the meet the identified needs. Common health
needs identified by most of the committees were: need for more staff, provision of 24 hour
services, security and more affordable medicines, in the PHC facilities. For WDC 1, in
addition to the above needs, members expressed a strong desire for the structural expansion
of their PHC in order for it to accommodate more beds.

95
Involvement in the Essential Drug Programme
Only one of the Development Committees had been involved in the Essential Drug
Programme of its PHC facility. However, it played no part in the fixing of prices and was
only involved in securing exemptions or postponement of payments for some indigent
members of the community. The members of this committee complained that by the time
many of the drugs got to the Health Centre, they had almost expired. In the words of one of
the VDC members:
“Most of the drugs they are bringing are almost expired drugs. When they invited us to
one seminar, I complained that they start bringing drugs a month to expiration. It nearly
caused problems between me and matron because I always insist that she should return
such drugs to the LGA headquarters.”
Chairman of VDC 2
Supervision of PHC facility workers and VHWs.
Most of the VDCs and WDCs were involved in the supervision of their PHC facility
workers and the Village Health Workers. The WDC which was not involved in supervision
of health workers attributed it to lack of a means of identification as a WDC member. They
said that such a means of identification, would prevent them from being embarrassed by
anyone in the course of carrying out their supervisory functions.

96
Representation of the VDCs and WDCs in their respective Health Centre Management
Committees
Most of the VDCs and WDCs were not represented in the Health Centre Management
Committees of the PHC facilities in their respective communities and wards. They were also
not involved in health care decision making in their communities and wards.
Keeping of financial records
Most of the committees, had no financial records, the common reason being that they had no
sources of finance. A few of them who sourced funds among themselves and from some
public spirited persons in the community kept financial records, but none of the committees
had a bank account.

97
Fig 4.2.3 Functionality of Village Development Committees
The 3 (100.0%) VDCs were all functional.

98
Fig 4.2.4 Functionality of Ward Development Committees
Two (50%) of the WDCs were fairly functional and 2 (50%) were poorly functional.

99
Fig 4.2.5 Composition and functionality of Village and Ward Development Committees
Two (66.7%) of the VDCs were well composed and functional while one (33.3%) of them
was fairly well composed and functional. Two (50.0%) of the WDCs were well composed
and fairly functional, one (25.0%) was well composed and functional and 1 (25%) was fairly
well composed and poorly functional.

100
Section 4.3: Factors associated with the establishment of well composed and functional
Development Committees
From all the FGDs, the only factor associated with the predominantly well composed
VDCs/WDCs was inauguration by the NPHCDA representatives.
All seven FGDs revealed that a major factor associated with poor functionality of VDCs and
WDCs was inadequate financial support from the Local Government. Other factors
identified were: non-incorporation of the VDCs and WDCs by the LGA authorities, as part
of the managerial structure of the PHC system, non-response by the Local Government to
the demands of the committees as regards the health needs of their communities and
insufficient training of members of the committees as regards their functions as members.
The following statement by a member of one of the WDCs, expressed the views of many of
the FGD discussants concerning financial support.
“The turn-out is reducing because people are not encouraged to continue coming. That’s
why they are not coming. They will not leave what they are doing at home and start
coming for a meeting when there is nothing to gain from it.”
A representative of the PHC in WDC 4
The Key Informants also expressed the view that lack of financial support was a hindrance
to the proper functioning of the VDCs and WDCs. In the words of one of the PHC
coordinators:
“When the WDCs in my LGA were constituted by the NPHCDA they were functioning
because they were getting some stipends and allowances but at present they are not

101
meeting, and much contribution cannot come from that angle for now except when they
start funding them.”
PHC Coordinator, one of the LGAs
The zonal representative of NPHCDA also confirmed that some of the VDCs and WDCs
were not holding regular meetings due to lack of financial support.
“For them to even have their monthly meeting, some of them will be waiting for someone
to give them money. Sometimes, they say they don’t have sitting allowance, because of
that some of them do not hold their monthly meetings as they are supposed to.”
A representative of NPHCDA
The fact that the VDCs and WDCs had not been incorporated into the PHC managerial
system was revealed in the following statement made by one of the PHC coordinators.
“Since I came on board 3 years ago, we have not really held any meeting with the WDCs.”
PHC Coordinator, one of the LGAs
This fact was underscored by the other PHC coordinator who was of the view that the VDCs
and WDCs did not need to report to the LGA, as expressed in the following statement.
“We have told our matrons that they should be doing monthly reports to us and this
should capture the activities of the VDCs and WDCs. The committee itself does not need
to report to us.”
PHC Coordinator, one of the LGAs

102
Section 4.4: Readiness of health facilities in villages and wards with functional
Development Committees to deliver some of the Ward Minimum Health Care Package
services.
Table 4.4.1 Readiness of PHC facilities for service delivery
Variable Frequency (n = 11) Percent
Infrastructure
Ready 1 9.1
Fairly Ready 8 72.7
Not Ready 2 18.2
Equipment and Furnishings
Fairly Ready 4 36.4
Not Ready 7 63.6
Personnel and Hours of Operation
Fairly Ready 4 36.4
Not Ready 7 63.6
Overall Readiness
Fairly Ready 6 54.5
Not Ready 5 45.5
In terms of infrastructure, only 1 health facility (9.1%) was ready for the delivery of
maternal/newborn, child survival and community mobilization/health education services,
while majority 8 (72.7%) were fairly ready. With regard to equipment and furnishings, a
larger proportion, 7 (63.6%) was not ready while 4 (36.4%) were fairly ready. As regards
personnel and hours of operation, 4 (36.4%) were fairly ready while most, 7 (63.6%) were
not ready to deliver PHC services. In terms of overall readiness, 6 (54.5%) was fairly ready
while 5 (45.5%) were not ready for the delivery of PHC services.

103
Table 4.4.2: Functionality of VDCs/WDCs and Readiness of their PHCs to deliver
some components of the WMHCP
VDC/WDC and PHC codes Functionality of VDC/WDC Readiness of PHC
VDC 1/PHC 5 Functional Not ready
VDC 2/PHC 6 Functional Fairly ready
VDC 3/PHC 3 Functional Fairly ready
WDC 1/PHC 9 Fairly functional Not ready
WDC 3/PHC 10 Poorly functional Fairly ready
WDC 4/PHC 11 Fairly functional Not ready
Of the three communities with functional VDCs (VDCs 1, 2 and 3), two had fairly ready
PHC facilities (PHCs 3 and 6), while one of them had a PHC facility that was not ready to
deliver some components of the WMHCP (PHC 5). The two wards with fairly functional
WDCs (WDCs 1 and 4) both had PHCs facilities that were not ready for PHC service
delivery (PHCs 9 and 11) while the ward that had a poorly-functional WDC (WDC 3), had a
PHC facility that was fairly ready to deliver some components of the WMHCP (PHC 10).

104
Table 4.4.3: Scores for Functionality of VDC/WDCs and readiness of PHCs to deliver
some components of the WMHCP
VDC/WDC and PHC Codes Composite scores
for Functionality of
VDCs/WDCs (%)
Summary scores for
Readiness of PHCs (%)
VDC 1/PHC 5 90.9 57.3
VDC 2/PHC 6 90.9 55.4
VDC 3/PHC 3 75.0 55.3
WDC 1/PHC 9 50.0 29.7
WDC 3/PHC 10 40.9 64.1
WDC 4/PHC 11 54.6 48.7
Mean (%) = 67.1 ± 21.6; 51.8 ± 11.9
VDCs 1, 2 and 3 had composite scores of 90.9%, 90.9% and 75.0% respectively for
functionality while their corresponding PHCs (PHCs 5, 6 and 3) had summary scores of
57.3%, 55.4%, and 55.3% respectively for readiness to deliver maternal/newborn, child
survival and health education/community mobilization services. WDCs 1, 3 and 4 had
composite scores of 50.0%, 40.9% and 54.6% respectively for functionality while their
corresponding PHCs (PHCs 9, 10 and 11) had summary scores of 29.7%, 64.1% and 48.7%
respectively for readiness to deliver maternal/newborn, child survival and health
education/community mobilization services. The mean composite score for VDC/WDC
functionality was (67.1 ± 21.6) % while the mean summary score for PHC facility readiness
was (51.8 ± 11.9) %.

105
Table 4.4.4: Correlation between functionality of VDCs/WDCs and readiness of PHCs
to deliver some components of the WMHCP
Variables (n = 6) VDC/WDC
Functionality
PHC readiness p value
VDC/WDC Functionality 1.000 -0.058
PHC readiness -0.058 1.000 0.913
There was little or no correlation, (rho = -0.058, p = 0.913) between functionality of
VDCs/WDCs and readiness of their PHCs to deliver maternal/newborn, child survival and
health education/community mobilization services.

106
Section 4.5: Household members’ utilization of Primary Health Care services
Table 4.5.1: General utilization of PHC Services by respondents and their households
Variable Frequency (n = 840) Percent
Ever used PHC services
for personal illness
Yes 202 24.0
No 638 76.0
Ever used PHC services
for children’s illness
Yes 300 35.7
No 540 64.3
Usual place of health care
for the household
Pharmacy/Chemist 286 34.0
Health Centre 165 19.6
General hospital 158 18.8
Home (self-medication) 120 14.3
Private hospital 98 11.7
Others* 13 1.5
Place of healthcare
during last illness episode
Pharmacy / Chemist 333 39.6
Home (self-medication) 182 21.7
General hospital 119 14.2
Health centre 115 13.7
Private hospital 70 8.3
Maternity clinic 15 1.8
Others** 6 0.7
Place of healthcare
during child's last illness
Pharmacy/Chemist 355 42.3
Health centre 206 24.5
General hospital 162 19.3
Private hospital 76 9.0
Home 18 2.1
Maternity 11 1.3
Others*** 12 1.5
* refers to maternity (n = 7), teaching hospital (n = 5) and trado-medical healing homes (n = 1)
** refers to teaching hospital (n =1) and trado-medical healing homes (n = 5)
*** refers to church (n = 6), teaching hospital (n =3) and trado-medical healing homes (n = 3)

107
Of the 840 respondents, a majority 638 (76.0%) had never used the PHC services for illness
episodes and a higher proportion 540 (64.3%) of the respondents had never used the PHC
services for their children’s illness episodes. A little over a third of the respondents 286
(34.0%) usually visited chemists/pharmacies for their health care needs. During their last
illness episode, more than a third 333 (39.6%) of the respondents accessed health care from
chemists and pharmacies while only 115 (13.7%) of the respondents accessed health care in
the Health Centres. The last time an under-five was ill, a little over two fifths 355 (42.3%) of
the respondents accessed treatment from the chemist/pharmacy while only about a fourth
206 (24.5%) accessed treatment from Health Centres.

108
Table 4.5.2: Utilization of maternal health services by mothers of under-five children
Variable Frequency Percent
Use of ANC services during the last pregnancy (n = 840)
Yes 796 94.8
No 44 5.2
Place of ANC during the last pregnancy (n = 796)
Private hospital 318 39.9
General hospital 214 26.9
Primary Health Centre 180 22.6
Teaching hospital 44 5.5
Maternity 26 3.3
TBA 14 1.8
Place of last delivery (n = 840)
private hospital 358 42.6
General Hospital 162 19.3
Primary Health Centre 114 13.6
Home 66 7.9
Maternity 64 7.6
Teaching Hospital 39 4.6
TBA 37 4.4
Use of Post natal services after last delivery (n = 840)
Yes 503 59.9
No 337 40.1
Place of post natal care after last delivery (n = 503)
Private hospital 176 35.0
General hospital 133 26.4
Primary Health Centre 116 23.1
Teaching hospital 34 6.8
Maternity 24 4.8
TBA 20 4.0
Majority of the respondents 796 (94.8%) made use of antenatal services during their last
pregnancy; two fifths 318 (39.9%) accessing these services in private hospitals while only
about a fifth (22.6%) accessed the services in PHCs. A higher proportion of the respondents
358 (42.6%), had their last delivery in private hospitals with only 114 (13.6%) delivering in
PHCs.

109
Over half of the respondents 503 (59.9%), made use of post natal care services after their
last delivery with about a third 176 (35.0%), utilizing private hospitals, while only about a
fifth 116 (23.1%) used the PHCs.

110
Table 4.5.3 Utilization of child survival services by the last children of the mothers of
under-fives
Variable Frequency Percent
Ever been vaccinated (n = 840)
Yes 830 98.8
No 10 1.2
Immunization card seen (n = 830)
Yes 228 27.5
No 602 72.5
Fully immunized for age (n = 830)
Yes 777 93.6
No 53 6.4
Health Centre as place where all vaccines were accessed
(n = 830)
Yes 455 54.8
No 375 45.2
Ever received Vitamin A supplementation (n = 840)
Yes 491 58.5
No 349 41.5
Place where Vitamin A supplementation was accessed
(n = 491)
Health Centre 286 58.2
General Hospital 68 13.8
Private Hospital 60 12.2
Home 48 9.8
Teaching hospital 17 3.5
School 8 1.6
Church 4 0.8
Almost all the respondents 830 (98.8%), had vaccinated their last child and a majority 777
(93.6%) had fully immunized them for age. A little over half of the respondents 455
(54.8%), accessed all the vaccines from the Health Centre and almost three fifths (58.5%),
had accessed Vitamin A supplementation for their last child at least once. Of the respondents
whose children had received vitamin A supplementation, a higher proportion 286 (58.2%),
received it in the Primary Health Centres.

111
Table 4.5.4: Reception of vaccines in the Health Centre by respondent’s last child and
vaccines received
Variables Frequency Percent
Health Centre as place where all vaccines were
accessed (n = 830)
Yes 455 54.8
No 375 45.2
Vaccines accessed in the Health Centre by those
who didn’t receive all their vaccines from the
Health Centre (n = 375)
BCG
Yes 87 23.2
No 288 76.8
OPV 0
Yes 97 25.9
No 278 74.1
OPV 1
Yes 91 24.3
No 284 75.7
OPV 2
Yes 74 19.7
No 301 80.3
OPV 3
Yes 51 13.6
No 324 86.4
Penta 1
Yes 72 19.2
No 303 80.8
Penta 2
Yes 72 19.2
No 303 80.8
Penta 3
Yes 63 16.8
No 312 83.2
Measles
Yes 56 14.9
No 319 85.1
Yellow Fever
Yes 51 13.6
No 324 86.4
Among the 840 respondents, majority 830 (98.8%) had vaccinated their last child at least
once. Of these, less than half 375 (45.2%) of their children did not access all the vaccines in

112
the Health Centre. Among those who did not access all their vaccines in the Health Centre,
about a quarter, 97 (25.9%), 87 (23.2%) and 91 (24.3%), received OPV 0, BCG and OPV1
respectively in the Health Centre while only about one sixth, 63 (16.8%), 56 (14.9%),
received Penta 3 and measles vaccines respectively in the Health Centre.

113
Table 4.5.5: Household utilization of health education and community mobilization
services
Variables Frequency Percent
Receipt of health education in the PHC (n = 840)
Yes 483 57.5
No 357 42.5
Health education topics received* (n = 483)
Exclusive Breastfeeding 308 65.5
Family Planning 296 63.0
Immunization Of Children 231 49.1
Child Care And Nutrition 219 45.8
Personal Hygiene 123 26.2
Adequate Nutrition 20 4.3
Pregnancy Care 6 1.3
Home Management of Malaria 2 0.4
Others** 3 0.6
Provision of community based health care services by
PHC workers (n =840)
Yes 366 43.6
No 474 56.4
Community based health care services rendered by PHC
workers* (n = 366)
Immunization 343 93.7
Health education 16 4.4
Sensitisation on the use of the PHC facility 11 3.0
Vit A administration 6 1.6
Mobilisation for house to house immunization 4 1.1
Free malaria treatment 2 0.5
Distribution of free diapers 1 0.3
Post natal care 1 0.3
*Multiple response
**refers to Ebola signs and symptoms, exercise and environmental sanitation
Over half of the respondents 483 (57.5%), had received health education in the PHCs. The
topics most frequently taught were exclusive breastfeeding, 308 (65.5%) and family
planning, 296 (63.0%). Less than half of the respondents 366 (43.6%), agreed that PHC

114
workers provided community based health care services. Immunization was mentioned by
the majority, 343 (93.7%) as a community based health care received.

115
Fig. 4.5.1: Level of utilization of some components of the Ward Minimum Health Care
Package by household members
Majority of the respondents, 715 (85.1%) and 721 (85.8) showed poor utilization of general
PHC services and maternal health services respectively. Also, a little over half of the
respondents, 469 (55.8%) showed poor utilization of health education/community
mobilization services but almost three fifths, 482 (57.4%) showed good utilization of child
survival services.

116
Fig. 4.5.2 Overall level of utilization of PHC services by household members
Overall, majority 645 (76.8%) of the respondents showed poor utilization of PHC services,
129 (15.4%) showed fair utilization while 64 (7.6%) showed good utilization of PHC
services.

117
Section 4.6 Performance of PHC workers with respect to the delivery of some
components of the Ward Minimum Health Care Package Services
Table 4.6.1: Performance of PHC workers in the delivery of maternal and newborn
health services
Variable Frequency Percent
Referral of pregnant women from the community to the Health
Centre in the last 3 months (n = 29)
Yes 13 44.8
No 16 55.2 Conduct of Antenatal Clinics (n = 29)
Yes 25 86.2
No 4 13.8
Management of pregnant women with severe infection (n = 29)
Yes 4 13.8
No 25 86.2
Management of women with severe infection after miscarriage or
abortion (n = 29)
No 29 100.0
Management of pregnant women with severe PIH (n = 29)
Yes 4 13.8
No 25 86.2
Taking of deliveries (n = 29)
Yes 24 82.8
No 5 17.2
Management of pregnant women with severe infection after delivery
(n = 29)
Yes 2 6.9
No 27 93.1
Basic resuscitation of the newborn (n = 29)
Yes 24 82.8
No 5 17.2
Newborn care in the last three months (n = 29)
Yes 24 82.8
No 5 17.2
Post natal care (n = 29)
Yes 19 65.5
No 10 34.5
Family planning counselling services in the last three months (n = 29)
Yes 28 96.6
No 1 3.4

118
Out of the 29 PHC facility workers, less than half of them 13 (44.8%), had referred a
pregnant woman from the community to the Health Centre in the last three months before
the survey. Majority 25 (86.2%), conducted antenatal clinics, however, only 4 (13.79%) had
ever managed pregnant women with severe infection. None of them had ever managed a
woman with severe infection after miscarriage or abortion, 2 (6.9%) had managed women
with severe infection after delivery while 4 (13.8%) had managed women with severe
pregnancy-induced hypertension. A majority, 24 (82.8%) took deliveries and had
administered newborn care in the last three months before the survey and of these less than
half had performed basic resuscitation of the new born. Almost two thirds, 19 (65.5%) of the
PHC workers rendered post natal services.

119
Table 4.6.2 Performance of PHC workers in the delivery of child survival services
Variable Frequency Percent
Conduct of exclusive breastfeeding counselling
(n =29)
Yes 27 93.1
No 2 6.9
Assisting mothers to initiate breast feeding (n = 29)
Yes 28 96.6
No 1 3.4
Visits to the home of the newborn to encourage
continued EBF (n = 28)
Yes 14 50.0
No 14 50.0
Conduct of growth monitoring sessions
Yes 26 89.7
No 3 10.3
Delivery of health talks on nutrition (n = 29)
Yes 27 93.1
No 2 6.9
Management of malnutrition in children (n = 29)
Yes 13 44.8
No 16 55.2
Provision of routine immunization (n = 29)
Yes 28 96.6
No 1 3.4
Participation in immunization campaigns (n = 29)
Yes 26 89.7
No 3 10.3
Almost all the respondents, 27 (93.1%) had counselled women on exclusive breastfeeding at
some time in the past. Most of them, 28 (96.6%) had helped a mother to initiate exclusive
breastfeeding and of these, half, 14 (50.0%) had gone to the home of a newborn to
encourage continued exclusive breastfeeding. Majority, 26 (89.7%) of the respondents had
been involved in growth monitoring, almost all of them, 27 (93.1%) had previously given a
health talk on nutrition, but less than half, 13 (44.8%) had ever managed a child with

120
malnutrition. Nearly all of them, 28 (96.6%) had assisted with the provision of routine
immunization at some time in the past and a majority 28 (89.7%) had participated in
immunization campaigns.

121
Table 4.6.3: Performance of PHC workers in the delivery of health education and
community mobilization services
Variable Frequency Percent
Health education in the Health Centre in the last three months
(n = 29)
Yes 27 93.1
No 2 6.9
Number of health education topics taught (n =27)
1 1 3.7
2 2 7.4
3 24 88.9
Health education topics taught* (n = 27)
Nutrition 18 66.7
Personal hygiene 18 66.7
Immunization 13 48.1
Family Planning 13 48.1
Exclusive Breastfeeding 11 40.7
Pregnancy care and use of ANC services 3 11.1
Environmental sanitation 3 11.1
Awareness of community mobilization (n = 29)
Yes 28 96.6
No 1 3.4
Previous involvement in community mobilization (n = 28)
Yes 19 67.9
No 9 32.1
Involvement in community mobilization in the last three
months (n = 19)
Yes 14 73.7
No 5 26.3
Time of last community mobilisation activity (n = 19)
1 week ago 3 15.8
1 month ago 6 31.6
2 months ago 4 21.1
3 months ago 1 5.3
12 months ago 3 15.8
3 years ago 1 5.3
5 years ago 1 5.3
*Multiple response

122
Nearly all the PHC facility workers, 27 (93.1%) had conducted health education sessions in
the PHC facility in the last three months prior to the survey. Majority 24 (88.9%) mentioned
up to 3 topics on which they had previously educated their patients. Most of them, 18
(66.7%) mentioned nutrition and personal hygiene as topics they had taught. Almost all the
health workers 28 (96.6%), had heard about community mobilization, of which over half, 19
(67.9%) had been involved in it at some time in the past. Of those who had previously been
involved in community mobilization, a majority, 14 (73.7%) had carried out some form of
community mobilization in the three months just prior to the survey.

123
Fig 4.6.1: Performance of PHC workers in the delivery of maternal/newborn, child
survival and health education/mobilization services
All the PHC facility workers 29 (100.0%), performed poorly in the delivery of maternal and
newborn services. However, in the delivery of child survival services, two fifths, 12
(41.4%), had good performance and in the delivery of health education and community
mobilization services, half of them, 15 (51.7%) also had good performance.
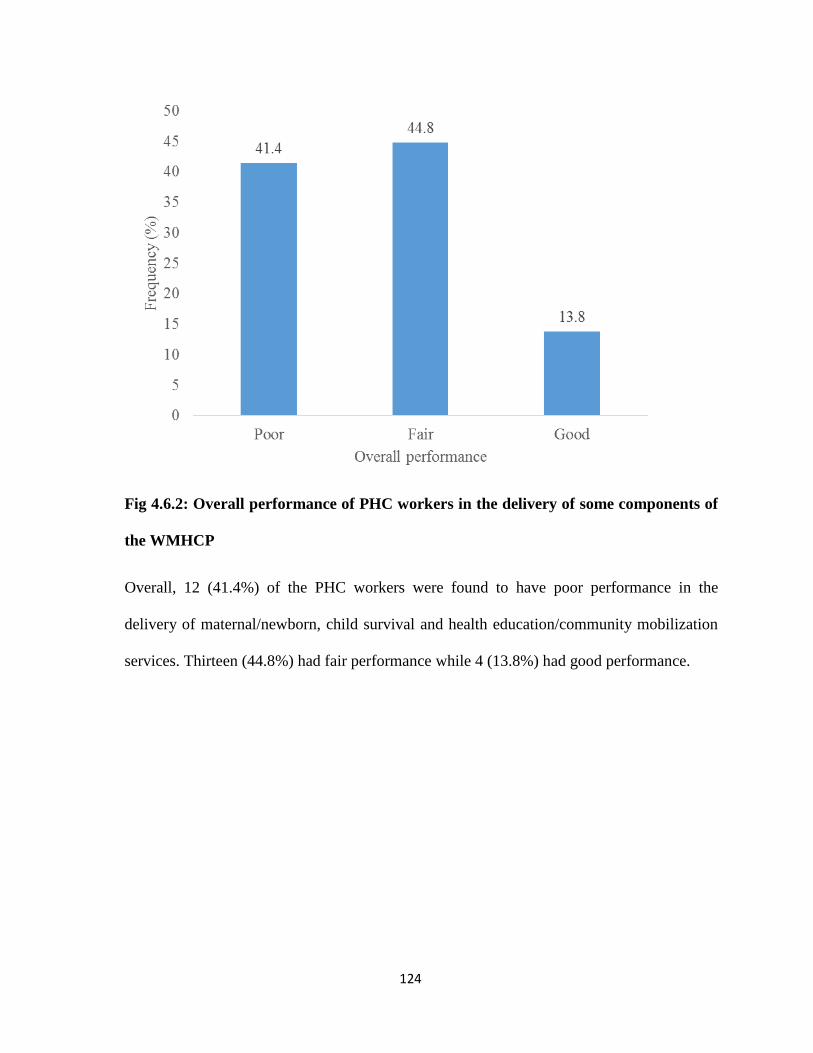
124
Fig 4.6.2: Overall performance of PHC workers in the delivery of some components of
the WMHCP
Overall, 12 (41.4%) of the PHC workers were found to have poor performance in the
delivery of maternal/newborn, child survival and health education/community mobilization
services. Thirteen (44.8%) had fair performance while 4 (13.8%) had good performance.

125
Section 4.7: Relationship between performance of PHC workers and household
utilization of PHC facilities
Table 4.7.1: Scores for performance of PHC workers and household utilization of PHC
facilities
Summary scores (%)
Community/PHC Codes Household utilization
PHC workers’
performance
Community 1/PHC 1 20.7 53.4
Community 2/PHC 9 28.4 48.3
Community 3/PHC 10 38.3 51.6
Community 4/PHC 11 44.8 53.9
Mean (%) = 33.1 ± 10.6; 51.8 ± 2.8
Communities 1 – 4 had summary scores for utilization, of 20.7%, 28.4%, 38.3% and 44.8%
respectively. The mean summary score was (33.1 ± 10.6) %. The workers in their
corresponding PHCs, (PHCs 1, 9, 10 and 11) had composite performance scores 53.4%,
48.3%, 51.6% and 53.9% respectively. The mean summary scores for household utilization
of PHC facilities and PHC workers’ performance were (33.1 ± 10.6) % and (51.8 ± 2.8) %,
respectively.

126
Table 4.7.2: Correlation (Spearman’s rho) between performance of PHC workers and
household utilization of PHC facilities
Variables (n = 4) PHC workers’
performance
Household
utilization of PHC
facilities
p value
PHC workers’
performance
1.000 0.400
Household
utilization of PHC
facilities
0.400 1.000 0.600
A weak positive correlation (r = 0.400) was found between performance of PHC workers
and household utilization of PHC services. This however was not statistically significant
(p = 0.600).

127
Section 4.8: Relationship between utilization of PHC services and well composed and
functional Development Committees
Table 4.8.1: Percentage Scores for household utilization of PHC services, composition
and functionality of Development Committees
Composite scores (%)
Community/WDC
codes
Summary scores for
household utilization (%)
WDC
composition
WDC
functionality
Community 2/WDC
1
28.4 84.0 50.0
Community 3/WDC
3
38.3 68.0 40.9
Community 4/WDC
4
44.8 84.0 54.6
Mean = 37.2 ± 8.3 78.7 ± 9.2 48.5 ± 7.0
Communities 2, 3 and 4 had summary utilization scores of 28.4%, 38.3% and 44.8%
respectively. Their corresponding WDCs (WDCs 1, 3 and 4) had composite scores of
84.0%, 68.0% and 84.0% respectively for composition; and 50.0%, 40.9%, and 54.6%
respectively for functionality. For these communities, the mean summary score for
household utilization of PHC services was (37.2 ± 8.3) % while the mean composite scores
for composition and functionality were (78.7 ± 9.2) % and (48.5 ± 7.0) % respectively.

128
Table 4.8.2: Correlation (Spearman’s rho) of composition and functionality of
Development Committees with household utilization of PHC services
Variables (n = 3) Household
utilization of PHC
facilities
WDC composition WDC functionality
Household
utilization of
PHC facilities
1.000
WDC
composition
0.000 (p = 1.000) 1.000
WDC
functionality
0.500 (p = 0.667) 0.944 (p = 0.214) 1.000
There was no correlation between WDC composition and household utilization of PHC
services (rho = 0.000, p = 1.000). There was a strong correlation between WDC
functionality and household utilization of PHC services which however was not statistically
significant (rho = 0.500, p = 0.667). There was a very strong correlation between WDC
composition and functionality but this was not statistically significant
(rho = 0.944, p = 0.214).

129
CHAPTER FIVE
5.0 DISCUSSION
It is believed that well composed and functional Village and Ward Development committees
are important in the Primary Health Care system, as they serve as a go-between the
community on one hand, and the PHC facility and Local Government authorities on the
other hand. This study has revealed some facts about the composition and functionality of
VDCs and WDCs in Benin City as well as their influence on household utilization of PHC
services.
Over half of the mothers of under-five children were aged 25 - 34 years. This is at variance
with the findings of NDHS 2013, where less than 20% of the women were in this age
group.24 The variation is probably due to the fact that in Edo State where female literacy rate
is about 90%, the age of marriage and subsequent childbirth is high.97 This is corroborated
by the finding that over half of the respondents had a minimum of secondary education
(completed). More-so in the face of current harsh economic realities, females now marry
later because even when they are ready for marriage, many of their suitors are not
economically ready. Female literacy is a very important factor in the promotion of the health
and wellbeing of children and indeed the entire family. It is easier for a literate woman to
understand and adopt health promoting practices such as use of antenatal care, skilled birth
attendants, family planning, immunization, insecticide treated nets, oral rehydration solution
among others. The importance of female literacy in relation to health is underscored by the
second and third millennium development goals.
Majority of the women being married is a reflection of the respect for the marriage
institution that is still prevalent in this part of the world. However, the finding that about

130
1.5% of the respondents were cohabiting is an indication, that our traditional beliefs about
the marriage institution are probably being gradually eroded, most probably due to
influences from the developed nations. Marriage connotes faithfulness to one partner and
this has health-promoting benefits both for the mother and the children. Faithfulness to one
faithful partner largely reduces the incidence of sexually transmitted infections including
HIV/AIDS. The current global trend towards sexual freedom which undermines traditional
beliefs about the marriage institution and monogamous relationships should therefore be
strongly resisted by individuals, families, communities and societies who still uphold these
traditional values.
Majority of the respondents were Christians and this can be attributed to the fact that Benin
City is a predominantly Christian society. Benin City, being the ancestral home of the Benin
people, as well as a cosmopolitan society; it is not surprising that the largest proportion of
the respondents were Benin and over half of the respondents were from other ethnic groups
within and outside Edo State such as Esan, Afenmai, Igbo e.t.c.
As regards occupation, the largest proportion of respondents belonged to skill level 2. This
is a reflection of the fact that over half of the respondents had either completed their
secondary education or dropped out of secondary school. Secondary school level of
education can only suffice for jobs at this skill level. The finding that a higher proportion of
the mothers of under-fives, had a minimum of secondary education is however a welcome
indication that they had attained basic literacy. Female education is necessary for the welfare
of the children and overall welfare of the home. An educated woman is better able to
appreciate and adopt health interventions that are beneficial to herself as well as the family.
Adoption of interventions such as pre-conceptional care, antenatal, delivery, post natal care,

131
family planning, immunization, exclusive breastfeeding, oral rehydration therapy among
others has been shown to contribute positively to reduction in child mortality and
improvement in maternal health. These will in turn promote the attainment of the fourth and
fifth MDGs.
The high rate of unemployment in Nigeria, with unemployment rates of up to 27.9% in Edo
State is also reflected by the finding that over a tenth of the mothers of under-fives were
unemployed.98 Majority of those who were employed had a monthly income of less than
eighteen thousand naira, corroborating statistics that show that over 60% of Nigerians are
poor.99 Where there is a high female unemployment rate, there is reduced financial access to
healthcare interventions such as antenatal care, skilled birth attendants at delivery, post natal
care, immunization, and management of common childhood illnesses. This can result in
problems such as preterm delivery, obstructed labour and its complications, small-for-date
infants, neonatal deaths and delayed cognitive development in children as a result of
inadequate maternal nutrition in pregnancy. Findings from the Nigeria Multiple Indicator
Cluster Survey reveal that both education and wealth status of mothers positively influence
health outcomes of their children.36 It is therefore imperative that all the tiers of government
should deploy more resources to reduce the present rates of unemployment in the country, so
as to harness the positive health effects of improved financial access to health care.
Majority of the spouses/partners of the mothers of under-fives were employed at skill level
2, similar to what was found among a larger proportion of the respondents. This similarity in
the skill level of the respondents and their spouses may be attributable to the fact that people
from similar social classes usually intermarry. The predominant skill level is most likely a
consequence of the dominant educational status which was secondary completed.

132
Employment of a higher proportion of spouses and their partners at this skill level implies a
low level of income for the families and consequent limited financial access to health care
services. In order to mitigate the negative health effects arising from limited financial access
to health care, measures that reduce out-of-pocket expenditure on health such as the
National Health Insurance Scheme should be adopted by the Edo State Government, since
the enabling policy environment already exists.
Interestingly, almost a third of the spouses or partners had completed their tertiary
education, but this level of education was not reflected in the proportion of spouses
employed at skill levels 3 and 4, as this proportion was only about a fifth of the total. The
difference may be attributable to the high unemployment rate in the country, with higher
rates in Edo State.98 The finding that majority of the respondents’ spouses or partners had a
higher income range than them is probably attributable to the fact that rates of
unemployment is lower for men. Similar findings were presented in the 2010 Nigeria
Poverty Profile.99
A larger proportion of the PHC facility workers were aged 26 – 35 years, with a mean age of
about 38 years. This is in keeping with the finding that a larger proportion of the PHC
workers were SCHEWs. The fact that most of the work force were in the older age group as
well as in the senior cadre of CHEWs may be attributable to the fact that employment into
the State Government service has been low for some years; resulting in the presence of
fewer workers in the junior compared to the senior cadres. The junior CHEWs are supposed
to spend up to 90% of their time rendering community based service, however their being
few in number will result in a situation of inadequate community based services. The results
of the study also showed this, as less than half of the mothers of under-five children had ever

133
received community based health care services. Inadequate community based health care
services will in turn reduce the effectiveness of the PHC system which aims at bringing
healthcare to the doorstep of the people. The survey was carried out in Benin City, hence it
was not surprising to find out that a larger proportion of the PHC workers were Benin. This
is in line with the principle of community participation which encourages the employment of
indigenous people in the PHC facilities.
A higher proportion of the Village and Ward Development committees was well composed.
This could be attributed to the fact that they were all constituted by the officials of the
NPHCDA who were abreast with the guidelines for constituting these committees. The
finding of a higher proportion of well composed VDCs and WDCs is similar to those in a
study conducted in South Africa in 2008, where all the VDCs were well composed, with
good female representation and duly elected officials.63 However, this finding is at variance
with those of a study conducted in Nepal where the VDCs were poorly composed as
evidenced by VDC secretaries who were politically appointed instead of being duly
elected.61
Well composed VDCs and WDCs with good representation of the units and communities in
the communities and wards respectively as well as good representation of the various sectors
is a basic requirement for a functional development committee. However, this alone is not
sufficient to make a development committee functional as shown by findings from this
study. The fact that all the VDCs were functional but none of the WDCs was functional may
be attributable to the existence of stronger community structures and a stronger sense of
commitment at the village than at ward level. This finding of VDC functionality is similar
to findings in studies conducted in Fiji and Bangladesh where the VDCs had regular

134
monthly meetings, and regular interaction with members of the community.60,62 Functional
development committees promote community participation in health, both in terms of
utilization of health care facilities as well as involvement in the planning and
implementation of health programmes. This usually results in a strong sense of community
ownership and consequent sustainability of health programmes. Half of the WDCs were
poorly functional, this is similar to findings in a study conducted in Nepal, where their
VDCs were poorly-functional as evidenced by failure to carry out their normal functions and
very little consultation with the community.64 Poorly functional development committees do
not promote community participation and ownership of health programmes, thus impeding
their sustainability and impact.
Majority of the WDCs were well composed but this did not translate into their being
functional. Unlike studies in Fiji and Nepal which attributed ineffectiveness of VDCs to
movement of community leaders outside the village and political appointment of the VDC
secretary, a study done in Bangladesh identified the desire for remuneration as a factor that
hindered the effectiveness of their VDCs.60–62 This finding was similar to findings in this
study where the major factor militating against the functionality of the VDCs/WDCs was
lack of remuneration. The felt need for remuneration by VDC and WDC members is
probably attributable to the level of poverty in the society. In a situation where people are
hardly able to afford their basic necessities, expecting them to use their meagre resources as
well as their time and effort for community work may be asking for too much. Measures
should be put in place by the LGA authourites and the NPHCDA to address this need for
remuneration so as to improve the effectiveness of the development committees. Other
factors found to be associated with poor functionality of the WDCs were hinged on the
failure of the PHC Coordinators and the LGA committees to incorporate them into the PHC

135
managerial system. This failure may have resulted from the fact that despite the presence of
policy support to the idea of community participation through VDCs and WDCs, the key
implementers of this policy at the level of the Local Government are yet to fully appreciate
its importance. This is supported by the findings of a study conducted in Lagos, Nigeria,
where key implementers of the Ward Health System (WHS) including PHC coordinators
were found to have inadequate knowledge about the WHS.100 A good grasp of the
importance of the VDCs/WDCs by these key implementers will most probably lead to
increased support of the activities of these committees. This in turn will most likely
contribute to improved functionality. Functional VDCs and WDCs will promote
improvement in maternal, newborn and child health through their community mobilization
activities. Their effective supervision of the PHC workers will most likely result in
improvement in their performance, thus further promoting the use of the PHCs by members
of the community, with a resultant positive effect on the health status of mothers and
children in particular, and the entire community in general.
None of the communities with functional VDCs was ready for the delivery of the
components of the WMHCP assessed. This could be attributed to the fact a functional VDC
or WDC may not be able to influence the state of readiness of a PHC facility especially in a
situation where members of the VDCs are not financially endowed or politically influential.
This finding can also be attributed to the disconnect between the VDCs/WDCs and the local
government officials as evidenced by the finding that minutes were not being forwarded by
any of the village or ward committees to the PHC committees as well as the relative lack of
awareness of the PHC coordinators about the activities of their VDCs/WDCs. It may also be
attributed to the fact that most of the committees were not involved in decision-making
processes of the PHC facilities as most of them were not represented in the health facility

136
committees. This disconnect between the VDCs/WDCs and the LGA management
committees, on one hand as well as the management of the PHC facilities on the other hand
may account for absence of any correlation between functionality of VDCs/WDCs and
readiness of the PHC facilities.
This finding is at variance with findings of studies carried out in Nepal and six states in
Nigeria (Kaduna, Nasarawa, Benue, Lagos, Bayelsa and Abia), where community
committees had a positive influence on the readiness of PHCs to deliver health services.64,66
In the study done in Kaduna, Nasarawa, Benue, Lagos, Bayelsa and Abia states in Nigeria,
the committees provided financial and housing support to health workers, as well as co-
financing and co-managing PHC services. Functional VDCs and WDCs have the potential to
positively influence the readiness of PHC facilities to deliver health services if they can
generate financial resources and if necessary integration with the activities of the PHC
facility management and the LGA management system exists.
Overall utilization of PHC facilities was poor for the majority of household members. This
may be attributed to the fact that none of the PHCs was ready for service delivery in terms
of equipment and facilities as well as adequate staffing. In particular, use of ANC services
was poor, as only about one fifth of the respondents used the PHC facilities for ANC. Use of
delivery and post natal care services was also poor, being corroborated by the finding that
about half of the PHC workers had taken only one to ten deliveries in the last three months
prior to the survey while only one third of they agreed that they rendered post natal care.
The poor use of ANC and delivery services may also be attributed to inadequate staffing of
the PHCs as well as unavailability of the required equipment/facilities. In particular, the fact
that most of the PHC facilities didn’t render 24 hour services probably also militated against

137
their use for delivery services. Immunization was the service most often used by households.
This is probably due to the fact that this service was available in most of the PHCs. In
addition, immunization services are more affordable in PHC facilities than in private
hospitals and less time is spent in accessing it in PHC facilities compared to secondary
health facilities.
The predominantly poor utilization of PHC services by respondents and their households, is
in keeping with findings in studies carried out in Kaduna and Kano States of Nigeria where
the use of delivery and post natal services was poor.56,70 This is also in consonance with
findings from the 2005 National HIV/AIDS reproductive and health survey as well as the
2013 National Demographic and Health Surveys in Nigeria, both of which revealed poor use
of public health facilities for antenatal, delivery and postnatal care.24,101 In this study, about
half of the respondents’ last children received all their vaccines in the PHC facilities which
is in keeping with the 2013 NDHS which revealed that all basic vaccinations were received
by 52.2% of children in Edo State.24
PHC facilities provide health care services where the people live and work. For millions of
Nigerians who by reason of their income level, cannot afford private hospitals or secondary
health facilities, unavailability of adequate PHC facilities, will result in their resorting to
traditional birth attendants or other unqualified personnel resulting in increased morbidity
and mortality both for the mothers and their children, especially the under-fives. As at 2014,
report on the MDGs from the National Bureau of Statistics showed improvement in both
maternal and child health indices with reduction in under-five mortality rate, infant mortality
rate and maternal mortality rates to 89/1000, 58/1000 and 243/100,0000 respectively.102
Improvement in equipment and manpower at the level of the Primary Health Centre, will

138
improve utilization of PHC facilities and thus further help improve the maternal and child
health indices, thus taking us closer to the attainment of the MDGs.
The fact that overall, two fifths of the PHC workers showed poor performance and only
about a tenth showed good performance, may be attributed to the unavailability of
equipment and facilities as shown by the finding that two thirds of the PHCs were not ready
for service delivery in terms of equipment and facilities. The higher proportion of CHEWs
as compared with nurse/midwives in the PHCs probably accounts for the poor performance
of all the PHC workers in the delivery of maternal/newborn services. This is corroborated by
the finding that two thirds of the PHC facilities were not ready for service delivery in terms
of adequate staffing. There was a weak positive correlation between performance of the
PHC workers and utilization of PHC services. This may have arisen from the predominantly
good performances in the delivery of child survival and health education and community
mobilization services resulting in more of the households utilizing child survival services.
The absence of any statistically significant correlation between performance of PHC
workers and utilization of PHC services may be due to the small number of units used in the
test of significance. However, this does not negate the importance of the positive correlation
observed, as all the health facilities in the wards surveyed were utilized in the analysis.
Similar to what was found in this study, positive relationships were observed between PHC
worker performance and utilization of community based health care services in studies
conducted in Iran, India and Lesotho.78–80 In these studies, improved performance in some
PHC services like immunization, health education and delivery services was associated with
better utilization of PHC services. However, no statistical tests of significance were carried
out. Studies carried out in Tanzania, Ibarapa in Oyo state, Nigeria and Enugu State Nigeria,

139
showed statistically significant associations between the performance of PHC workers and
utilization of health services.81–83
Provision of the required equipment/facilities in the PHCs will promote good performance
by PHC workers which will in turn encourage utilization of PHC services, with a resultant
reduction in morbidity and mortality especially among women and under-fives. This will
lead to further improvement in maternal and child health indices. However, this is more
likely to occur against a background of availability of an adequate number health care
personnel of the right cadres.
There was no correlation between utilization of PHC services and composition of the
VDCs/WDCs. This may be explained by the fact that even though a committee is well
composed, the well composed nature of the committee may in itself not be related to
utilization of health services if other factors like functionality of the committees and
availability of equipment, infrastructure and adequate staffing in the PHCs are not in place.
A strong positive correlation (rho = 5) was found between utilization and functionality.
Even though only half of the WDCs were fairly functional and the other half poorly
functional, their activities probably had a positive effect on PHC utilization by household
members thus contributing to the strong positive correlation. This finding may be an
indication that if circumstances were better, with functional development committees being
fully integrated into the decision making processes of the PHCs, a stronger relationship may
be observed. The absence of statistical significance is probably due to the fact that the
number of units available for the test were few. A larger study would probably yield
statistically significant results. This finding of a positive relationship between functionality
of WDCs and utilization of PHC services is similar to those in studies conducted in

140
Cambodia, Ghana and Enugu state Nigeria, where functional village committees were
associated with increased utilization of delivery, in-patient, antenatal and immunization
services.84,85,88
Functional VDCs who not only carry out their stipulated activities but are well integrated
into the decision-making processes of their PHCs and LGA committees, will most likely
result in better utilization of PHC facilities with the attendant positive outcomes of reduced
morbidity and mortality especially as it relates to maternal and child health issues and
consequent further improvement in maternal and child health indices in Benin City.

141
CONCLUSION
Majority of the VDCs were well composed and functional. Majority of the WDCs were also
well composed but none was functional.
The only factor associated with well composed Development Committees was inauguration
by the NPHCDA representatives while the main factor associated with poor functionality of
the Development Committees was inadequate financial support from the LGA authorities.
Over half of the PHCs were not ready for the delivery of maternal/newborn, child survival
and health education/community mobilization services, while the others were fairly ready. In
the communities with functional development committees, majority of the PHCs were fairly
ready for the delivery of PHC services.
Majority of the respondents and their households showed poor utilization of PHC services.
About half of the PHC facility workers had poor performance with respect to the delivery of
maternal and newborn, child survival and health education/community mobilization services
while most of the others had fair performance.
There was a weak positive relationship between performance of PHC workers and
household utilization of PHC services.
There was no relationship between the composition of development committees and
household utilization of PHC services. However, there was a strong positive relationship
between functionality of development committees and household utilization of PHC
services.

142
RECOMMENDATIONS
The following recommendations are made based on findings from the study.
The State Government
1. There should be provision of adequate equipment and furnishings for the Primary
Health Care facilities to promote readiness for the delivery of maternal/newborn,
child health and health education/community mobilization services. Government
can partner with corporate organisations like banks and non-governmental
organisations in the provision of these equipment and furnishings.
2. There should be employment of more staff, of the right cadre to man the PHC
facilities. In particular more nurses, midwives and community health officers should
be employed to improve on the capacity of the PHC facilities to provide maternal
health services.
The Local Government
3. There should be training and retraining of health workers so as to improve their
performance in the provision of maternal, newborn, child survival, health education
and community mobilization services.
4. The PHC Management and Technical committees should incorporate the Village and
Ward Development committees into the managerial structure of the PHC system in
in order to promote the functionality of these committees.
5. Sitting allowance should be provided for members of the VDCs and WDCs by the
Local Government Chairman so as to defray costs of convening the meetings,

143
transportation and other opportunity cost. Corporate organisations should be
encouraged to take up as part of their social responsibilities, the payment of sitting
allowance to VDC/WDC to promote their functionality.
6. More effort should be made to mitigate or solve the health problems identified by the
VDCs and WDCs in their communities and wards respectively. This will show them
that they are recognized and that their work is appreciated, thus improving their
morale and promoting functionality.
7. Essential drugs should be supplied to the PHC facilities at least 6 months to their
expiration dates in order to promote the delivery of effective services by PHC
workers.
8. Members of the VDCs and WDCs should be incorporated into the drug revolving
systems in the LGAs in order for these committees to better fulfill their prescribed
functions.
9. There should be quarterly attendance of one or two representatives of the PHC
technical committees at the meetings of their respective VDCs/WDCs to boost the
morale of the members thereby promoting their functionality.
Village and Ward Development Committees
10. The officials of the VDCs and WDCs should regularly reach out to defaulting
members in order to encourage continued participation.
11. Minutes of meetings should be forwarded on a monthly basis to the PHC technical
and Management committees so that they are made officially aware of the activities
of the VDCs and WDCs

144
The South-South Zone of the National Primary Health Care Development Agency
12. There should be collaboration with the Local Government in the provision of sitting
allowance for the VDCs /WDCs.
The Primary Health Care Facility Workers
13. Efforts should be made at self-improvement in the provision of maternal, newborn,
child survival, health education and community mobilization services, in order to
improve performance. This could be achieved through self-sponsored trainings.
The mothers of under-five children and their households
14. The available services in the PHC facilities should be utilized as often as the need
arises.

145
REFERENCES
1. World Health Organization. Declaration of Alma-Ata: international conference on
primary health care, Alma-Ata, USSR, September 6-12, 1978. [cited 2013 October
4]. Available from: http://www.who.int/hpr/NPH/docs/declaration_almaata
2. Olise P. Primary Health Care for sustainable development: history of Primary Health
Care. Abuja, Nigeria: Ozege publications; 2007:19
3. Calnan R and Rodger GL. Primary Health Care : a new approach to health care
reform. Notes for Remarks by President-Elect and President of the Canadian Nurses
Association to the Senate Standing Committee on Social Affairs, Science and
Technology. 2002. [cited 2013 Nov 5]. Available from: www.cna-nurses.ca.
4. Obionu C.N. Primary Health Care for developing countries: basic concepts. 2nd ed.
Enugu, Nigeria: Evanseenio printing and publishing; 2007:2
5. Roy S., Sharma BBL. Community participation in Primary Health Care. Heal. Popul.
Issues. 1986; 9(4):165–91.
6. Federal Republic of Nigeria. National Primary Health Care Development Agency.
NPHCDAbriefing manual on theMDG-DRGfunded Midwives'Service Scheme .
Abuja: NPHCDA; 2009:47
7. Levers LL, Magweva FI, Mpofu E. A literature review of district health systems in
east and southern Africa : Facilitators and barriers to participation in health.
EQUINET Discussion Paper 40 [cited 2013 Dec 13] Available from:
http://www.gsdrc.org/go
8. Federal Republic of Nigeria, National Primary Health Care Development Agency.
The MDG-DRG funded Midwives Service Scheme: concept, process and progress.
2nd ed. Abuja: NPHCDA; 2012:68

146
9. Federal Republic of Nigeria, National Primary Health Care Development Agency.
National guidelines for development of Primary Health Care system in Nigeria. 4th
revised ed. Abuja: NPHCDA; 2012:31 - 97
10. Federal Republic of Nigeria, National Primary Health Care Development Agency.
Introduction to the Ward Health System: briefing package for sensitization on the
Ward Health System. Abuja: NPHCDA; 2006:5 - 8
11. Oakley P. Community involvement in health development: an examination of the
critical issues. Geneva: WHO; 1989:15
12. Odogwu K, Audu O, Baba Lafia S, Bawa U, Tukur B, Ejembi C, Adaji S, Shittu O.
Availability and utilization of emergency obstetric care services in three
communities in Kaduna State, Northern Nigeria. Afr J Reprod Health.
2010;14(3):83-8.
13. Ramarao S, Caleb L, Khan ME, Townsend JW. Safer maternal health in rural Uttar
Pradesh : do primary health services contribute? Health Policy and Planning.
2001;16(3):256-63.
14. Marchant T and Schellenberg J. Measuring skilled attendance at birth using linked
household, health facility, and health worker surveys in Ethiopia, North-East
Nigeria, and Uttar Pradesh, India. Lancet. 2013;381(June):S88-S98.
15. Kreuter MW, Lezin NA, Kreuter MW, Green LW. Community health promotion:
ideas that work. 2nd ed.Sudbury MA: Jones and Bartlett publishers; 2003. pp 59 - 62
16. Bjaras G. Haglund BJA, Rifkin SB. A new approach to community participation
assessment. Health Promot Int. 1991;6(3):199–206.
17. World Health Organization, Regional Committee for Africa. Revitalizing health
services using the Primary Health Care approach in the African region. Addis Ababa:

147
WHO; 2006. World Health Organization Regional Office for Africa. Report of the
regional director. 56th session. AFR/RC56/12. [cited 2013 Dec 20]. Available from
www.who.int
18. Edo State Government, State Ministry of Health. Edo State Government 2010 - 2020
Strategic Plan. Benin: SMOH; 2010:8
19. Alakija W. Essentials of community health, primary health care and health
management: community participation and community mobilisation. Benin City:
Medisuccess publications; 2000:151
20. Federal Republic of Nigeria, National Primary Health Care Development Agency.
Policies and priorities for Primary Health Care development in Nigeria; 2010:14
21. World Health Organization. The Nigerian Health System. 2008:21–30. [cited 2013
Nov 13] Available from: www.who.int/pmnch/countries/nigeria-plan-chapter-3.pdf.
22. Adeniyi JO, Ejembi CL, Igbinosun P, Muhammed D, Nwagbo FE, Ogundeji MO.
Report of the National Health Care Needs Assessment Survey. Abuja: National
Primary Health Care Development Agency. 2001. [cited 2014 Jan 23] Available
from: www.who.int.pmnch/countries/
23. National Population Commission and ICF Macro. Nigeria demographic and health
survey 2008. Abuja, Nigeria: NPC and ICF Macro; 2009:237
24. National Population Commission and ICF International. Nigeria demographic and
health Survey 2013. Abuja, Nigeria: NPC and ICF International; 2014:92-153
25. Findley SE, Uwemedimo OT, Doctor HV, Green C, Adamu F, Afenyadu GY. Early
results of an integrated maternal newborn, and child health program, Northern
Nigeria, 2009 to 2011. BMC Public Health. 2013;13:1034.

148
26. Hall J. Effective community-based interventions to improve exclusive breast feeding
at four to six months in low- and low-middle-income countries: a systematic review
of randomised controlled trials. Midwifery. 2011;27(4):497–502.
27. Ahmed T, Ahmed AMS, Mahfuz M, Abdullah K, Cravioto A SD. Systematic review
of management of childhood severe malnutrition. Lancet. 2008;372:417–40.
28. Ijadunola KT, Fatusi AO, Orji EO, Adeyemi AB, Owolabi OO, Ojofeitimi EO,
Omideyi AK, Adewuyi AA. Unavailability of Essential Obstetric Care Services in a
Local Government Area of South West Nigeria. J Health Popul Nutr. 2007;25(1):94-
100.
29. Ameh C, Msuya S, Hofman J, Raven J, Mathai M, van den Broek N. Status of
emergency obstetric care in six developing countries five years before the MDG
targets for maternal and newborn health. PLoS One. 2012;7(12):e49938.
30. Ehiri JE, Oyo-Ita AE, Anyanwu EC, Meremikwu MM, Ikpeme MB. Quality of child
health services in primary health care facilities in south-east Nigeria. Child Care
Health Dev. 2005;31(2):181-91.
31. Mezie-okoye MM, Adeniji FO, Tobin-west CI, Babatunde S. Status of Emergency
Obstetric Care in a Local Government Area in South South Nigeria. J Reprod Heal.
2012;16(September):170-9.
32. Bryce J, Victora CG, Habitcht JP, Black RE, Scherpbier RW. Programmatic
pathways to child survival. Health Policy Plan. 2005;20(Suppl 1):i15–i17.
33. Bryce J, Daelmans B, Dwivedi A, Fauveau V, Lawn JE, Mason E, Newby H,
Requejo J, Salama P, Shankar A, Starrs A, wardlaw T. Countdown to 2015 for
maternal, newborn and child survival:the 2008 report on tracking coverage of
interventions. Lancet. 371;(9620)2008:1247–58.

149
34. World Health Organisation and United Nations Childrens Fund. Countdown to 2015
Decade report (2000–2010); 2010.[cited 2014 Feb 3] Available from
www.countdown2015mnch.org/
35. Itimi K, Dienye PO, Ordinioha B. Community participation and childhood
immunization coverage: a comparative study of rural and urban communities of
Bayelsa State, south-south Nigeria. Niger Med J. 2012;53(1):21-5
36. Federal Republic of Nigeria, National Bureau of Statistics, United Nations Children'
s Fund, United Nation's Population Fund. Nigeria Multiple Indicator Cluster Survey
2011. Abuja: NBS; 2013:51
37. Adeiga A, Omilabu SA, Audu RA, Sanni F, Lakehinde GP, Balogun O, Olagbaju O.
Infant immunization coverage in difficult-to-reach area of Lagos metropolis. African
Journal of Clinical and Experimental Microbiology. 2005;6(3):227-31
38. Wonodi C, Stokes-prindle C, Aina M, Oni G, Olukowi T, Ali Pate M, Privor-Dumm
L, Levine O. Landscape analysis of routine immunization in Nigeria: identifying and
addressing barriers to routine immunization coverage. Baltimore: International
Vaccine Access Centre, John Hopkins School of Public Health; 2012:2008-11. [cited
2014 Feb 3]. Available from www.jhsph.edu/ivac.
39. Oluwadare C. The social determinants of routine immunisation in Ekiti State of
Nigeria. Ethno-Med. 2009;3(1):49–56.
40. Wondifon EA. Myths and Misconceptions as Barriers to Uptake of Immunization
Services in Nigeria. J. Vaccines Vaccin. 2013;04(07):4–7.
41. Weldegebriel GG, Gasasira A, Harvey P, Masresha B, Goodson JL, Ali Pate M,
Abanida E, Chevez A. Measles resurgence following a nationwide measles

150
vaccination campaign in Nigeria, 2005-2008. J. Infect. Dis. 2011;204 (Suppl:1):226–
S231.
42. Bill and Melinda Gates Foundation. Polio: strategy overview. 2012 [cited 2014 Jan
15]. Available from: www.gatesfoundation.org/
43. Morrow AL, Guerrero ML, Shults J, Calva JJ, Lutter C, Bravo J, Ruiz-Palacios G,
Morrow RC, Butterfoss FD. Efficacy of home based peer counselling to promote
exclusive breastfeeding: a randomised controlled trial. Lancet.
1999;353(9160):1226–31.
44. Grummer-Strawn LM, Rice SP, Dugas K, Clark LD, Benton-Davis S. An evaluation
of breastfeeding promotion through peer counseling in Mississsipi WIC clinics.
Maternal and Child Health J. 1997;1(1):35-8
45. Tylleskär T, Jackson D, Meda N, Engebretsen IM, Chopra M, Diallo AH, Doherty T,
Ekström EC, Fadnes LT, Goga A, Kankasa C, Klungsøyr JI, Lombard C,
Nankabirwa V, Nankunda JK, Van de Perre P, Sanders D, Shanmugam R,
Sommerfelt H, Wamani H, Tumwine JK. Exclusive breastfeeding promotion by
peer counsellors in sub-saharan Africa (PROMISE-EBF): a cluster randomised trial.
Lancet 2011;378(9789):420–7.
46. Haider R, Ashworth A, Kabir I HS. Effect of community-based peer counselors on
exclusive breast feeding practices in Dhaka, Bangladesh: a randomized controlled
trial. Lancet 2000;356(9242):1643–7.
47. Qureshi AM, Oche OM, Sadiq UA, Kabiru S. Using community volunteers to
promote exclusive breastfeeding in Sokoto State, Nigeria. Pan Afr. Med. J.
2011;10:8.

151
48. United Nations Childrens Fund. Progress for Children: a report card on child
nutrition. No. 4. Geneva: UNICEF. 2006. [cited 2013 Dec 14] Available from:
www.unicef.org/publications/index
49. Save the Children Everyone. Two summits to tackle the hidden malnutrition crisis: a
call to action to end global hunger and malnutrition. 2012:1–5. [cited 2014 Jan 15]
Available from: www.savethechildren.org.uk/
50. Save the Children Everyone. A life free from hunger: tackling child malnutrition.
2008:1–8. [cited 2014 Jan 15] Available from:www.savethechildren.org.uk/
51. Adewoye KR, Musa IO, Atoyebi OA, Babatunde OA. Knowledge and utilization of
antenatal care services by women of child bearing age in Ilorin-East Local
Government Area, North Central Nigeria. Int. J. Sci. Technol. 2013;3(3):188–93.
52. Fagbamigbe AF, Akanbiemu FA, Adebowale AS, Olumide AM, Korter G. Practice,
knowledge and perceptions of antenatal care services among pregnant women and
nursing mothers in Southwest Nigeria. International Journal of Maternal and Child
Health 2013;1(1):7–16.
53. Akanbiemu FA, Olumide AM, Fagbamigbe AF, Adebowale AS. Effect of perception
and free maternal health services on antenatal care facilities utilization in selected
rural and semi-urban communities of Ondo State, Nigeria. British journal of
Medicine & Medical Research. 2013;3(3):681–97.
54. Igbokwe CC. Knowledge and attitude of pregnant women towards antenatal services
in Nsukka Local Government Area of Enugu State, Nigeria. J. Res. Educ. Psychol.
2012;3(1):70–8.
55. Olayinka A, Joel A, Bukola D. Factors influencing utilization of antenatal care
services among pregnant women in Ife Central LGA , Osun State Nigeria, National

152
Hospital Abuja, Nigeria. Advances in Applied Science Research. 2012;3(3):1309-
15.
56. Yar'Zeva IS, Said IY. Knowledge and barriers in utilization of maternal health care
services in Kano State, northern Nigeria. Eur. J. Biol. Med. Sci. Res. 2013;1(1):1–14.
57. Abe E, Omo-Aghoja LO. Maternal mortality at the Central Hospital, Benin City
Nigeria: a ten year review. Afr. J. Reprod. Health. 2008;12(3):17–26.
58. Millenium Development Goals Nigeria. Countdown strategy 2010-2015: achieving
the MDGs; 2010. [cited 2014 Jan 23 ]. Available from: www.mdgs.gov.ng.
59. Kirigia JM, Oluwole D, Mwabu GM, Gatwiri D, Kainyu LH.. Effects of maternal
mortality on gross domestic product (GDP) in the WHO African region. Afr J of
Health Sci. 2006;13(1-2):86–95.
60. Jerety J. Primary health care: Fiji’s broken dream. Bull World Health Organ.
2008;86(3):166–7.
61. Institute of Local Governance Studies-Nepal. Assessment of Village Development
Committee governance and the use of block grants. Kathmandu; 2009. [cited 2014
February 16] Available from: www.undp.org/.../governance/
62. Haneef C, Pritchard M, Hannan M, Alam Z RM. A study into the effectiveness and
sustainability of Village Development Committees. Bangladesh; 2014. [cited 2014
Feb 13]. Available from: www.clp-bangladesh.org/
63. Smith T. The role of ward committees in enhancing participatory local governance
and development in South Africa: evidence from six ward committee case studies.
2008 . [cited 2014 January 18] Available from www.mlgi.org.za/

153
64. Gurung G, Tuladhar S. Fostering good governance at peripheral public health
facilities: an experience from Nepal. Rural Remote Health. 2013;13:2042. [cited
2014 October 30] Available from: http://www.rrh.org.au.
65. Mubyazi GM, Mushi AK, Shayo E, Mdira K, Ikingura J. Local Primary Health Care
committees and community-based health workers in Mkuranga District, Tanzania:
does the public recognize and appreciate them? Ethno-Med. 2007;1(1):27-35.
66. Abimbola S, Olanipekun T, Igbokwe U, Negin J, Jan S, Martiniuk A, Ihebuzor N,
Aina M. How decentralisation influences the retention of primary health care
workers in rural Nigeria. Global Health Action. 2015;1(5):1-11.
67. Uzochukwu BSC, Onwujekwe OE, Akpala CO. Effect of the Bamako-Initiative drug
revolving fund on availability and rational use of essential drugs in primary health
care facilities in South-East Nigeria. Health Policy Plan. 2002;17(4):378-83.
68. World Health Organisation, Regional Committee for Affrica. Review of the
implementation of the Bamako Initiative. Windhoek, Namibia: WHO; 1999. World
Health Organization, Regional Office for Africa. Report of the Regional Director.
49th session. AFR/RC/49/13. [cited 2014 October 30]. Available from:
www.afro.who.int/.../5233-fortyninth-session-of-who-regional-committ...
69. Babalola S, Fatusi A. Determinants of use of maternal health services in Nigeria -
looking beyond individual and household factors. BMC Pregnancy and Childbirth.
2009;9:43.
70. Suleman HI, Mohammed NS, Muhammed SI. Barriers to utilisation of maternal
health services in a semi-urban community in northern Nigeria. Niger Med J.
2013;54(1):27–32.

154
71. Dairo MD, Owoyokun KE. Factors affecting the utilization of antenatal care services
in Ibadan, Nigeria. Benin J. post Grad. Med. 2010;12(1):3-13
72. Akinleye SO, Falade CO, Ajayi IO. Knowledge and utilization of intermittent
preventive treatment for malaria among pregnant women attending antenatal clinics
in primary health care centers in rural southwest , Nigeria: a cross-sectional study.
BMC Pregnancy Child Birth. 2009;9:28.
73. Odusanya OO, Alufohai EF, Meurice FP, Ahonkhai VI. Determinants of vaccination
coverage in rural Nigeria. BMC Public Health. 2008;8:381.
74. The earth institute Columbia University. One Million Community Health Workers:
technical taskforce report. 2013. [cited 2014 Feb 1] Available from:
1millionhealthworkers.org/
75. Lehmann U, Sanders D. Community health workers :what do we know about them?
The state of the evidence on programmes, activities, costs and impact on health
outcomes of using community health workers. Geneva: WHO. 2007. [cited 2014 Jan
15] Available from: www.who.int/healthsystems/
76. World Health Organisation. Task shifting to tackle health worker shortages. 2010:1–
12. [cited 2014 Jan 17] Available from: www.who.int/healthsystems/
77. Al-Ghanim S. Factors influencing the utilisation of public and private Primary
Health Care services in Riyadh City. JKAU: Econ & Adm 2004;19(1):3-27.
78. Javanparast S, Baum F, Labonte R, Sanders D. Community health workers’
perspectives on their contribution to rural health and well-being in Iran. Am. J.
Public Health. 2011;101(12):2287–92.

155
79. Murthy N, Campbell P, Vasan A, Latha SH and Prasanna A. Performance
Enhancement of Primary Health Care in Andhra Pradesh: findings from the Pilot.
Foundation for Research in Health Systems. 2010:3-25.
80. Obioha EE and Molale MG. Functioning and Challenges of Primary Health Care (
PHC ) Program in Roma Valley, Lesotho. Ethno Med. 2011;5(2):73-88.
81. Mushi D, Mpembeni R, Jahn A. Effectiveness of community based Safe Motherhood
promoters in improving the utilization of obstetric care: the case of Mtwara rural
district in Tanzania. BMC Pregnancy Childbirth. 2010;10:14.
82. Ige K, Nwachukwu C. Health Care Seeking Behaviour Among Market Traders In
Ibarapa Central Local Government, Nigeria. Internet J Heal. 2008;9(2).[cited 2014
October 14]. Available from: https://ispub.com/IJH/9/2/9674
83. Christiandolus E. Health Consumers’ perception on increasing Primary Health Care
services utilization and quality enhancement at the Primary Health Centers in Enugu
, Enugu State , Nigeria. Sci Rep. 2012;1:530.
84. Jacobs B, Price N, Sam SO. A sustainability assessment of a health equity fund
initiative in Cambodia. Int J Heal Plann Mgmt. 2007;22:183-203.
85. Fosu R, Opoku-Asante K, Adu-Gyanfi K. Influence of community financing health
insurance schemes on in-patient care in Ghana: the case of Nkoranza scheme. Dev
Ctry Stud. 2014;4(8):53-64.
86. Carrin G. Community based Health Insurance Schemes in Developing Countries:
facts , problems and perspectives. Geneva: WHO; 2003. World Health Organization,
Discussion Paper number 1, 2003. [cited 2014 October 20]. Available from:
http://apps.who.int/iris/bitstream/10665/69023/1/EIP_FER_DP.E_03.1.pdf.

156
87. Gupta MD, Gauri V, Khemani S. Decentralized delivery of primary health services
in Nigeria: survey evidence from the states of Lagos and Kogi. Mozambique: Human
Development Sector, Africa Region, The World Bank; 2004.Africa region human
development working paper series. [cited 2014 October 14]. Available from:
www1.worldbank.org/publicsector/decentrallization/…/Khemani.doc
88. Uzochukwu BSC, Onwujekwe OE, Akpala CO. Did the Bamako Initiative improve
the utilization of maternal and child health-care services in Nigeria ?: A case study of
Oji River Local Government Area in Southeast Nigeria. J Heal Popul Dev Ctries.
2004. [cited 2014 october 20]. Available from: http://www.jhpdc.unc.edu/.
89. Anaemene BU. Health Diplomacy under Structural Adjustment Programe : A view
from Nigeria. International Affairs and Global Strategy. 2013;15:48-59. [cited 2014
October25].Availablefrom:www.iiste.org/journals/index.php/IAGS/article/viewFile/
8016/8301.
90. Federal Government of Nigeria. Constitution of the Federal Republic of Nigeria:
legal notice on publication of 2006 census final results. 2007:94(24): B184.
91. Federal Government of Nigeria, National Primary Health Care Development
Agency. Ward minimum health care package 2007 - 2012. Abuja: NPHCDA;
2007:10
92. Cochran WG. Sample survey techniques: the estimation of sample size. 3rd ed. New
York: John wiley and Sons; 1977:75
93. Suresh K, Chandrashekara S. Sample size estimation and power analysis for clinical
research studies. J. Hum. Reprod. Sci. 2012;5(1):7–13.
94. Onokerhoraye AG. Access and utilization of modern health care facilities in the
petroleum-producing region of Nigeria: the case of Bayelsa state. Havard School of

157
Public Health 1999;02115(162).[cited 2014 Feb 3] Available from:
www.hsph.harvard.edu/
95. Federal Government of Nigeria, National Primary Health Care Development
Agency. Minimum standards for Primary Health Care in Nigeria. Abuja: NPHCDA;
2013:47-50
96. International Labour Organisation. International standard classification of
occupations. Geneva: ILO; 2012:12-15
97. Federal Government of Nigeria, National Bureau of Statistics. Report of the national
literacy survey. Abuja: NBS; 2010:14-22
98. Federal Government of Nigeria, National Bureau of Statistics. Unemployment
rates in Nigeria by state. Abuja: NBS; 2011. [cited 2015 July 14] Available from
www.nigerianstat.gov.ng/pages/data/socioeconomicdata/
99. Federal Government of Nigeria, National Bureau of Statistics. Nigerian poverty
profile 2010. Abuja: NBS; 2012:9-15
100. Abosede OA, Campbell PC, Olufunlayo T, Sholeye OO. Establishing a sustainable
Ward Health System in Nigeria : are key implementers well informed ?
Community Med Heal Educ. 2012;2(7):1-5
101. Federal Government of Nigeria, Federal Ministry of Health. National HIV &
AIDS and Reproductive Health Survey (NARHS Plus II 2012). Abuja: FMOH;
2013. [cited 2015 July 15] Available from:
www.unaids.org/sites/default/files.../NGA_narrative_report
102. Federal Government of Nigeria, National Bureau of Statistics. The millenium
development goals performance tracking survey, 2015 report. Abuja: NBS; 2015:18-
24

158
APPENDIX 1
HOUSE HOLD QUESTIONNAIRE
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES ON
HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES IN
BENIN CITY
Good day Madam, I am Dr (Mrs.) Omonyemen Bosede Bello, a Senior Registrar in the Department
of Community Health, University of Benin Teaching Hospital, Benin City.
I am carrying out a survey titled, ‘Assessment of the Influence of Development Committees
on Household Utilization of Primary Health Care Services in Benin City’ This questionnaire
seeks information on the extent to which household members in Benin City utilize primary
health care services as well as factors which affect their utilization of these services. This
information will serve as a basis for making recommendations to relevant stakeholders with
the aim of improving utilization of health services.
To this end therefore, I would like to ask you some questions. The answers you give will not be
shown to anyone that is not involved in this research and we do not require your name. Your answers
will only assist us in learning more about utilization of health services in Benin City. I therefore seek
your consent cooperation in doing this. Thank you.
______________________ ______________________
Signature of respondent Signature of researcher
SOCIODEMOGRAPHIC PROFILE OF RESPONDENTS
1. Age ____________________
2. Sex male ( ) female ( )
3. Place of residence _________________________
4. Occupation ______________
5. Occupation of spouse______________
6. Marital Status: Single ( ) Married ( ) Divorced ( ) Separated ( ) Cohabiting ( )
7. If the answer to no 6 is married, tick the type of marriage
a. Monogamous ( ) b. Polygamous ( )
8. Religion Christianity ( ) Islam ( ) ATR ( ) Others please
specify_____________
9. Ethnic group________________________
10. Educational level attained: no formal education ( ) primary uncompleted ( ) primary
completed ( ) secondary uncompleted ( ) secondary completed ( ) tertiary uncompleted ( )
tertiary completed ( )
11. Educational level of spouse:
a. No formal education ( ) primary uncompleted ( ) primary completed ( ) secondary
uncompleted ( ) secondary completed ( ) tertiary uncompleted ( )

159
12. Monthly Income range:
a. <N18, 000 ( ) N18, 000 – N50, 000 ( ) N51, 000 – N120, 000 ( )>N120,000
b. <216,000 ( ) 216,000 – 600,000 ( ) 601,000 – 1,440, 000 ( ) > 1,440,000 (annual)
13. Monthly Income range of spouse:
a. <N18, 000 ( ) N18, 000 – N50, 000 ( ) N51, 000 – N120, 000 ( )>N120,000
b. <216,000 ( ) 216,000 – 600,000 ( ) 601,000 – 1,440, 000 ( ) > 1,440,000 (annual)
HOUSEHOLD MEMBERS’ UTILIZATION OF PHC SERVICES AND ASSOCIATED
FACTORS
14. Have you ever gone to the health centre when you were ill? Yes ( ) No( )
15. If the answer to 14 is no, why not? [Multiple Response]
a. The health centre is too far. Yes ( ) No ( ) b.The waiting time in the health centre is
too long Yes ( ) No ( ) c.Health workers are unfriendly
Yes ( ) No ( ) d.The staff in the health centre are incompetent Yes ( ) No ( ) e.
Treatment at the health centre is too expensive Yes ( ) No ( ) f. Others please
specify
_________________________________________________________________
16. Has your spouse ever gone to the health centre when he was ill? Yes ( ) No ( )
17. If the answer to 17 is no, why not? [Multiple Response]
a. The health centre is too far. Yes ( ) No ( ) b. The waiting time in the health centre
is too long. Yes ( ) No ( ) c. Health workers are unfriendly Yes ( )
No ( ) d. The staff in the health centre are incompetent. Yes ( ) No ( ) e. Treatment
at the health centre is too expensive. Yes ( ) No ( ) f. Others
pleasespecify____________________________________________________
18. Have your children ever been taken to the health Centre when they were ill?
Yes ( ) No ( )
19. If the answer to 19 is no, why not? [Multiple Response]
a. The health centre is too far Yes ( ) No ( ) b.The waiting time in the health centre is
too long Yes ( ) No ( ) c.Health workers are unfriendly
Yes ( ) No ( ) d.The staff in the health centre are incompetent
Yes ( ) No ( ) e. Treatment at the health centre is too expensive
Yes ( ) No ( ) f.Others please specify_________________________
20. When a member of your household falls sick, where do you usually seek health care?
a. We apply self-remedy b. Health centre c. Chemist d. maternity e. native doctor f. Prayed
only. Others please specify_________________________________
21. If the answer to 21 is not b what are your reasons?
a. The health centre is too far Yes ( ) No ( ) b.The waiting time in the health centre is
too long Yes ( ) No ( ) c.Health workers are unfriendly
Yes ( ) No ( ) d.The staff in the health centre are incompetent
Yes ( ) No ( ) e. Treatment at the health centre is too expensive
Yes ( ) No ( ) f.Others please specify_________________________
22. What did you do the last time you were ill?
a. Applied self-remedy b.Went to the health centre c. Went to the chemist

160
d. Went to the maternity e.Went to the native doctor f. Prayed only g. Others please
specify _______________________________________________
23. Where did your spouseaccess treatment the last time he was ill?
a. At the health centre b. at the chemist c. at the maternity d. At the native doctor
e. In church Others please specify ______________________________________
24. Where did you access treatment the last time any of your children was ill?
a. At the health centre b. at the chemist c. at the maternity d. At the native doctor
e. In church Others please specify ______________________________________
HOUSEHOLD UTILIZATION OF MATERNAL HEALTH SERVICES
25. How old is your last child?
26. Did you attend antenatal clinics during the pregnancy? Yes ( ) No ( )
27. Where did you access antenatal care? a. Primary Health Centre ( ) b. General Hospital (
) c. Teaching Hospital ( ) d. Maternity ( ) e. TBA ( ) f. Private Hospital ( ) Others
please specify_____________________________________________________________
28. Where did you deliver?
a. Primary Health Centre ( ) b. General Hospital ( ) c. Teaching Hospital ( ) d.
Maternity ( ) e. TBA ( ) Home ( ) f. Private Hospital ( ) Others please
specify_____________________________________________________________
29. Did you access post natal care? Yes ( ) No ( )
30. If the answer to question 29 is Yes, where did you access post natal care?
a. Primary Health Centre ( ) b. General Hospital ( ) c. Teaching Hospital ( ) d.
Maternity ( ) e. TBA ( ) f. Others please
specify_____________________________________________________________
HOUSEHOLD UTILIZATION OF CHILD-SURVIVAL SERVICES
31. Has your last child ever been immunized Yes ( ) No ( )
(Immunization card seen) Yes ( ) No ( )
32. If the answer to 31 is no, why not? a. Child was sick ( )
b. I didn’t have the time ( ) c. The health centre is too far ( ) d. Vaccines not
available in the health centre ( ) f. Others please specify
__________________________________
33. If the answer to 31 is Yes, Is this child fully immunized for age? Yes ( ) No ( )
(Immunization card seen) Yes ( ) No ( )
34. If the answer to 31 is no, why is this child not fully immunized for age?
a. I didn’t have the time ( ) c. The health centre is too far ( ) d. Vaccines not available
in the health centre ( )
e. Others please specify __________________________________
35. Did the child receive all of his/her vaccinations in the health centre? Yes ( )No ( )
If the answer to 35 is No,
36. Which ones did the child receive in the health centre?

161
a. OPV0 ( ) OPV1 ( ) OPV2 ( ) OPV3 ( ) BCG ( ) DPT1 ( ) DPT2( )
DPT3 ( ) HBV1 ( ) HBV2 ( ) HBV3 ( ) PENTA1 ( ) PENTA 2 ( ) PENTA3 (
) Measles ( ) Yellow fever ( )
37. Has this child ever received vitamin A supplementation? Yes ( ) No ( )
38. If the answer to 37 is no, why not?
a. I didn’t have the time ( ) c. The health centre is too far ( ) d. Vitamin A not
available in the health centre ( )
39. If the answer to37 is Yes, where did he receive it? A. Health centre ( ) b. at home c. in
church d. in school Others please specify __________________________________
HOUSEHOLD UTILZATION OF HEALTH EDUCATION AND COMMUNITY
MOBILISATION SERVICES
40. Have you ever received health talks in the PHC? Yes ( ) No ( )
41. If the answer to 40 is yes, Please list four topics that you have been taught
______________________________________________
______________________________________________
______________________________________________
______________________________________________
42. Have any of the PHC workers in your community ever come to administer healthcare in
your home? Yes ( ) No ( )
43. If the answer to 42 is yes, what activities did the carry out in the community?
________________________________________________________________
________________________________________________________________

162
APPENDIX 2
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES ON
HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES IN
BENIN CITY
PRIMARY HEALTH CARE WORKERS’ QUESTIONNAIRE
Good day Sir/Madam, I am Dr (Mrs.) OmonyemenBosede Bello, a Senior Registrar in the
Department of Community Health, University of Benin Teaching Hospital, Benin City.
I am carrying out a survey titled:‘Assessment of the Influence of Development Committees on
Household Utilization of Primary Health Care Services in Benin City’. This aspect of the survey will
help us to understand how the Primary Health Care workers in Benin City help to promote household
utilization of Primary Health Care services. The study is not being sponsored by any government
agency and is not out to find out who is defaulting on his/her job. Its ultimate aim is to contribute to
improving household utilization of PHC services in Benin City, thus positively impacting the health
of the people in Benin City. To this end therefore, I would like to ask you some questions. The
answers you give will not be shown to anyone that is not involved in this research and we do not
require your name. Your answers will only assist us in learning more about how PHC workers in
Benin City perform in delivering PHC services and how this influences utilization of these services. I
therefore seek your consent cooperation in doing this. Thank you.
______________________ ______________________
Signature of respondent Signature of researcher
Code for the Primary Health Centre ___________________________________
Type of Primary Health Centre _______________________________________
SOCIODEMOGRAPHIC PROFILE OF RESPONDENTS
1. Age ____________________
2. Sex male ( ) female ( )
3. Occupation ______________
4. Cadre of health worker __________________________
5. Marital status. Single ( ) Married ( ) Divorced ( ) Separated ( ) Cohabiting ( )
6. If married, type of marriage. Monogamous ( ) Polygamous ( )
7. Designation a. Village Health Worker b. Traditional Birth Attendant c. Community
Resource Person d. Junior Community Health Extension Worker e. Community Health
Extension Worker f. Nurse g. Nurse/Midwife h. Community Health Officer i. Doctor
8. Others please specify ___________________________________

163
9. Religion: Christianity ( ) Islam ( ) ATR ( ) Others please
specify_____________
10. Ethnic group________________________
11. Educational level attained:
a. No formal education () primary uncompleted ( ) primary completed ( )secondary
uncompleted ( ) secondary completed ( ) tertiary uncompleted ( )tertiary completed()
12. Educational level of spouse:
a. No formal education ( ) primary uncompleted () primary completed ( )secondary
uncompleted ( ) secondary completed ( ) tertiary uncompleted ( ) tertiary completed( )
MATERNAL AND NEWBORN HEALTH SERVICES
13. In the last 3 months have you referred any pregnant woman in the community to the health
centre?
a. Yes ( ) No ( )
14. If the answer to question 13, is yes, how many have you referred?
a. ________________________________
15. Do you conduct Antenatal care for pregnant women? Yes ( ) No ( )
16. If the answer to the above is no, why do you not conduct antenatal care?
a. ______________________________________________________________
b. ______________________________________________________________
17. If the answer to the above is yes, mention 4 things you do in the antenatal clinic
a. ______________________________________________________________
b. ______________________________________________________________
c. ______________________________________________________________
d. ______________________________________________________________
18. Have you ever been involved in managing a pregnant woman with severe infection? Yes ( )
No ( )
19. If yes to 18, how many cases have you managed in the last 3 months? ________________
20. If the answer to question 19 is yes, how did you treather?
a. parenteral antibiotics ( ) b. oral antibiotics ( ) Others please
specify_________________________________________
21. If no to 18, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) We do not have the required manpower ( ) Other
please specify __________________________
22. Have you ever been involved in managing a woman with severe infection after miscarriage
or abortion? Yes ( ) No ( )

164
23. If yes to 22, how many cases have you managed in the last 3 months? ________________
24. If no to 22, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) We do not have the required manpower ( ) Other
please specify __________________________
25. Have you ever been involved in managing a woman with severe infection after delivery?
Yes ( ) No ( )
26. If yes to 25, how many cases have you managed in the last 3 months? ________________
27. If no to 25, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) We do not have the required manpower ( ) Other
please specify __________________________
28. Have you ever been involved in the management of a woman with severe pregnancy induced
hypertension, with or without convulsions? Yes ( ) No ( )
29. If yes to 28, how many cases have you managed in the last 3 months? ________________
30. If no to 28, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) We do not have the required manpower ( ) Other
please specify __________________________
31. Do you take deliveries Yes ( ) No ( )
32. If no to question 31, why don’t you take deliveries? ( ) We do not have the required
facilities ( ) I do not have the required skill ( ) I have never had a labour case ( )
33. Other please specify __________________________
34. If the answer to 31 is yes, how many deliveries have you taken in the last 3 months?
__________________________________________________
35. If the answer to 31 is yes, what do you administer to contract the uterus after each delivery?
Oxytocin ( ) Ergometrine ( ) Misoprostol ( ) Other please specify _________________
36. Have you managed a woman with retained placenta in the last three months? Yes ( ) No (
)
37. If yes to 36, how many cases have you managed in the last 3 months? ________________
38. If yes 36 is Yes what did you do?
a. perform manual removal of the placenta? Referred to the general hospital ( ) Other
please specify _________________________________________
39. If no to 36, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) I do not have the required skill ( ) Other please
specify __________________________
40. Have you ever managed a labour case that required assisted vaginal delivery months?Yes (
) No ( )
41. If yes to 40, how many cases have you managed in the last 3 months? ________________
42. If yes 40 what did you do?
a. Vacuum extraction ( ) forceps delivery ( ) Referred to the general hospital Other
please specify ( )________________________________________
43. If no to 40, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) I do not have the required skill ( ) Other please
specify __________________________
44. Have you ever managed a woman with retained products of conception? Yes ( ) No ( )
45. If yes to 44, how many cases have you managed in the last 3 months? ________________
46. If the answer to number 44 is Yes, what did you do?
a. Curettage b. used carman’s syringe c. referred to the general hospital ( )
Other please specify _______________________________________

165
47. If no to 44, why you never managed such a case? No such case has ever presented ( ) We
do not have the required facilities ( ) I do not have the required skill ( ) Other please
specify __________________________
48. Have you been been involved in caring for the newborn in the last three months?
a. Yes ( ) No ( )
49. Mention 4 important things you must do in caring for the newborn
a. _______________________________________________
b. _______________________________________________
c. _______________________________________________
d. _______________________________________________
50. Have you performed basic resuscitation of the newborn in the last three months?
Yes ( ) No ( )
51. Do you render post natal care services Yes ( ) No ( )
52. If no to question 51, why not? We do not have the required facilities ( ) I do not have the
required skill ( ) Post natal cases do not come ( ) Other please specify
____________________________________
Please answer always, most of the time, rarely or never to questions 53 and 54
53. I render post natal care services in the health facility
a. Always ( ) most of the time ( ) rarely ( ) Never ( )
54. I render post natal care services in the home of the newborn
a. Always ( ) most of the time ( ) rarely ( ) Never ( )
55. Have you ever counselled women on family planning? Yes ( ) No ( )
56. How many times in the last 3 months have you done this?
a. __________________________________________________________
57. Name three modern family planning methods
a. ______________________________________________
b. ______________________________________________
c. ______________________________________________
CHILD SURVIVAL SERVICES
58. Have you ever counselled pregnant women on exclusive breast feeding?
Yes ( ) No ( )
59. If the answer to question 58, is yes, where did this counselling take place?
a. In the health centre ( ) In the women’s meeting ( ) In the Church ( ) In the
women’s homes ( ) Others please specify ____________________________
60. In the last three months, how many times have you counselled pregnant women on exclusive
breast feeding? _____________________________________________________________
61. Have you ever helped a mother to initiate breast feeding?Yes ( ) No ( )
62. If the answer to question 61 is no, why not? ___________________________________
a. ________________________________________________________________
63. If the answer to question 61 is yes, how soon after birth should breastfeeding be initiated?
____________________________________________________________
64. If you helped to initiate breastfeeding for a newborn, have you ever gone to the home of the
newborn to encourage the mother on the need to continue exclusive breast feeding?

166
a. Yes ( ) No ( )
65. Have you ever monitored the growth of a child? Yes ( ) No ( )
66. If yes to 65, how many have you monitored in the last 3 months? _____________________
67. Where did this growth monitoring take place? a. In the health centre ( ) b. In the child’s
home c. Others please specify ( )
68. If the answer to question 65 is yes, mention the name of the chart used for growth
monitoring _________________
69. Mention 2 measurements we can use to assess the growth of a child
a. __________________________________________________________
b. __________________________________________________________
70. Have you ever given health talks on nutrition education? Yes ( ) No ( )
71. Have you ever managed any child with malnutrition? Yes ( ) No ( )
72. If the answer to 71 is yes, mention 3 things you did to manage the patient.
a. _________________________________________________
b. _________________________________________________
c. _________________________________________________
73. Have you ever assisted in the provision of routine immunization? Yes ( ) No ( )
74. If the answer to question 73, is no, why not? I do not have the required skill ( ) We do not
have vaccines ( ) Other please specify __________________________
75. Have you ever participated in immunization campaigns? Yes ( ) No ( )
76. If the answer to question 75 is yes, which of the campaigns have you participated in?
Local immunization days ( ) National immunization days ( ) Mop up campaigns ( )
Others please specify ( ) _______________________________________________
77. Have you ever identified an adverse event following immunization?
Yes ( ) No ( )
78. If the answer to question 77 , is yes, which adverse event have you identified?
Fever ( ) rigor ( ) vomiting ( ) Others please specify
_____________________________________________________
79. If the answer to question 77 is yes, how did you manage the adverse event?
___________________________________________________________
80. Have you ever identified a case of Acute Flaccid Paralysis? Yes ( ) No ( )
81. If the answer to 80 is yes what did you do ?
________________________________________________________
HEALTH EDUCATION AND COMMUNITY MOBILIZATION SERVICES
82. In the last three months have you conducted health education sessions in the health centre?
Yes ( ) No ( )
83. If the answer to question 82, is No, why not? No patients ( ) Don’t know how to do it ( )
Other please specify ( ) _______________________________________________
84. If the answer to question 82 is yes, list three topics on which you have previously health
educated patients
a. ____________________________________
b. _____________________________________
c. _____________________________________
85. Have you ever heard of community mobilization? Yes ( ) No ( )
86. In the last three months have you been involved in mobilising the community for health
actions? Yes ( ) No ( )

167
87. If the answer to question 86 is yes, list 3 health activities for which you have previously been
involved in mobilisingyour community.
a. _______________________________________________________
b. ________________________________________________________
c. ________________________________________________________
88. When did your last community mobilisation activity occur? _______________
89. What was the outcome of this community mobilisation activity?____________________
_______________________________________________________________________

168
APPENDIX 3
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES ON
HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES
IN BENIN CITY
FOCUS GROUP DISCUSSION GUIDE FOR DEVELOPMENT COMMITTEES
Interviewer: Dr (Mrs.) O.B. Bello Date:_________ Place:____________ Time:____________
Group: Village/Ward Development committee
INTRODUCTION
Good day, my name is DrOmonyemenBosede Bello, I am a Senior Registrar in the Department of
Community Health, University of Benin Teaching Hospital, Benin City. Thank you for being a part
of this focus group. The aim of this meeting is to create an avenue for interaction such that
information about your functions as a group can be obtained in greater detail. This will enable me
provide answers to my study on “Assessment of the influence of development committees on
household utilization of Primary Health Care services in Benin City”. The major questions I desire to
answer as I carry out my study relate to how your committee came into being, the composition of the
committee, the functions as well as your challenges and achievements as a group.
Now I would like us to begin by moving around and introducing ourselves one to another.
Introductions should include your names, what you do for a living and any other thing you would
like us to know about you. Thanks a lot for taking time out of your busy schedules to participate in
this discussion. Like we said earlier on we will be taking notes and doing a voice recording of the
sessions for the purpose of further analysis. Thank you.
QUESTIONS
1. What is the name of this committee?
2. In which year was the committee formed?
3. Who are the members of this committee?
4. How many women are in this committee?
5. Do you have elected officials?
6. What are the positions held in this committee?
7. How were the officials of this committee selected?
8. How often does the committee meet?
9. What do you discuss during your meetings?
10. Are minutes taken during the meetings?
11. What do you understand your function to be as a committee?
12. Have you been able to identify health needs in the community?
13. Does your PHC have an essential drug programmme?
14. Are you involved in the management of the essential drug programme?
15. Are you involved in the supervision of health workers in the community and PHC?
16. Is this committee represented in the health centre committee(s)

169
17. Is this committee represented in the WDC/LGA PHC management committee?
18. Are reports on the activities of this committee sent to the next level of the PHC
managerial system?
19. How do you communicate your decisions and plans to the community?
20. What are your sources of finance?
21. Do you have financial records?
22. Do you think you are fulfilling your functions as a committee? If so in what ways?
23. If no, why do you think you’re failing to fulfill your functions?
24. What have been your achievements as a committee?
25. What are your challenges?
CONCLUSION
Thank you very much for your readiness to share your thoughts and experiences and for
participating in this focus group. The information you have provided has been very helpful. This
information will be used to help us gain a better understanding of the workings of the village
development committee in your community.

170
APPENDIX 4
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES ON
HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES
IN BENIN CITY
KEY INFORMANT INTERVIEW GUIDE (1)
KEY INFORMANTS: LGA chairmen, Supervisory councilors for health and PHC Coordinators.
Introducing the interview:
Good morning/afternoon. I am DrOmonyemenBosede Bello from Department of Community
Health, UBTH. I will be carrying out a study titled “Assessment of the influence of
development committees on household utilization of primary health care services in Benin
City”Some of the objectives of the study are to assesshow the development committees
function and to ascertain if communities with functional development committees utilize
PHC facilities optimally. Before asking questions, I want to assure you that I will safeguard
the identities of all respondents of this study. If I use any of your statements in the report, I
will cite the source of the statement only as: LGA chairmen/Supervisory councilor for
health/PHC Coordinator without reference to the particular LGA or Ward. This interview
should take about 45–60 minutes.
Male____ Female_______
Position of respondent _______________________________
Date of interview: __________________________________
Time started: ________________________________________
Time ended: ________________________________________
Interviewer/facilitator: ________________________________
1) Can you please tell me what you understand by the term Village development
committee?

171
2) Can you please tell me what you understand by the term+ Ward development
committee?
3) Can you please tell me what you understand by the term LGA PHC Management
committee?
4) Can you please tell me what you understand by the term LGA PHC Technical
committee?
5) Does this LGA have any of these Development Committees?
6) Is the LGA PHC management committee existent and functional?
7) Can you mention some of their members (office not name)
8) Is the LGA PHC technical committee existent and functional?
9) Can you mention some of their members (office not name)
10) What factors do you think may be responsible for the proper functioning (or absence
of it) in these Development Committees?
11) What do you know about the activities of VDCs and WDCs in this LGA?
12) What do you think are the achievements of the VDCs and WDCs?
13) What do you think are the challenges of these committees?
Thank you very much for taking out time for this interview.

172
APPENDIX 5
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES ON
HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES
IN BENIN CITY
KEY INFORMANT INTERVIEW GUIDE (2)
KEY INFORMANT: NPHCDA Representative from the zonal office
Introducing the interview:
Good morning/afternoon. I am DrOmonyemenBosede Bello from Department of Community
Health, UBTH. I will be carrying out a study titled “Assessment of the influence of
development committees on household utilization of primary health care services in Benin
City”Some of the objectives of the study are to assesshow the development committees
function and to ascertain if communities with functional development committees utilize
PHC facilities optimally. Before asking questions, I want to assure you that I will safeguard
the identities of all respondents of this study. If I use any of your statements in the report, I
will cite the source of the statement only as: NPHCDA representativewithout reference to the
particular person. This interview should take about 45–60 minutes.
Male____ Female_______
Position of respondent _______________________________
Date of interview: __________________________________
Time started: ________________________________________
Time ended: ________________________________________
Interviewer/facilitator: ________________________________
1) Can you please tell me what you understand by the term Village development
committee?
2) Can you please tell me what you understand by the term Ward development
committee?

173
3) Can you please tell me what you understand by the term LGA PHC Management
committee?
4) Can you please tell me what you understand by the term LGA PHC Technical
committee?
5) Which of the LGAs in Benin City have WDCs?
6) Have all these WDCs been inaugurated by the NPHCDA?
7) Do VDCs exist in our communities in Benin City?
8) If yes to 7, in which communities do VDCs exist in Benin City?
9) Have they been inaugurated?
10) Is the LGA PHC management committee existent and functional?
11) Is the LGA PHC technical committee existent and functional?
12) What factors promote proper functioning of these committees?
13) What factors hinder the proper functioning of these committees?
14) What are the achievements of the WDCs in Benin City?
15) What do you are the achievements of the VDCs in Benin City?
16) What are the challenges of WDCs?
17) What are the challenges of WDCs?
Thank you very much for taking out time for this interview.

174
APPENDIX 6
ASSESSMENT OF THE INFLUENCE OF DEVELOPMENT COMMITTEES ON
HOUSEHOLD UTILIZATION OF PRIMARY HEALTH CARE SERVICES
IN BENIN CITY
KEY INFORMANT INTERVIEW GUIDE (3)
KEY INFORMANT: Community Leaders
Introducing the interview:
Good morning/afternoon. I am Dr Omonyemen Bosede Bello from Department of
Community Health, University of Benin Teaching Hospital. I am carrying out a study titled
“Assessment of the influence of development committees on household utilization of primary
health care services in Benin City” Some of the objectives of the study are to assess how the
development committees function and to ascertain if communities with functional
development committees utilize PHC facilities well enough. Before asking questions, I want
to assure you that I will safeguard the identities of all respondents of this study. If I use any of
your statements in the report, I will cite the source of the statement only as: Community
leader without reference to the particular community. This interview should take about 45–60
minutes.
Male____ Female_______
Position of respondent _______________________________
Date of interview: __________________________________
Time started: ________________________________________
Time ended: ________________________________________
Interviewer/facilitator: ________________________________
1) Can you please tell me what you understand by the term Village development
committee?

175
2) Can you please tell me what you understand by the term Ward development
committee?
3) Can you please tell me what you understand by the term LGA PHC Management
committee?
4) Can you please tell me what you understand by the term LGA PHC Technical
committee?
5) Do you have a VDC in this community?
6) If yes to 5, does your VDC meet regularly?
7) Does your VDC have representatives in the WDC?
8) Does your VDC submit minutes of their meetings to the WDC?
9) How has your VDC contributed to solving health and development problems in the
community? (Achievements)
10) What are the factors that promote the proper functioning of the VDC?
11) What are the factors that hinder the proper functioning of your VDC?
Thank you very much for taking out time for this interview.

176
APPENDIX 7
OBSERVATIONAL CHECKLIST FOR FACILITY-READINESS OF
PRIMARY HEALTH CENTRES TO DELIVER PHC SERVICES
INFRASTRUCTURE/HUMAN
RESOURCES/EQUIPMENT/DRUGS
Present Absent
COMMENT Functional/
Number
Non
functional/
Number
Infrastructure
5 rooms
Functional Doors
Windows with nets
Clean water source: at least a motorized borehole
Connection to national grid
Alternative power source
Sanitary waste collection point
Waste disposal site
Functional separate male and female toilet facilities
with water supply within the premises
Signpost visible from both entry and exit points
Fencing
Gate house
Generator house
Staff accommodation: 2 bedroom apartments
Rooms and Space to accommodate
Client observation area
2 Consulting rooms
2 Delivery rooms
Maternity/lying-in section
Injection and dressing area
In-patient ward section
Laboratory
Pharmacy and dispensing unit
Medical Records area
Injection/dressing area
Minor procedures room
Food demonstration area
Kitchen
Staff station
Store
Toilet facilities (male and female)
Waiting/reception area
Furnishings and Equipment
Female Ward
1 Angle poised lamp
4 medium artery forceps
2 Stainless steel bedpans
2 stainless steel bowls with stand
2 ceiling fans
2 good plastic chairs

177
OBSERVATIONAL CHECKLIST FOR FACILITY-READINESS OF PRIMARY HEALTH
CENTRESTO DELIVER PHC SERVICES CONTD
2 stainless steel covered bowls for cotton wool
2 graduated medicine cups
2 dissecting forceps
2 Dressing scissors
1 dressing trolley
2 drinking mugs
2 Dust bins with pedal
1 medium sized galipot
2 packs of disposable gloves (100 pcs/pack)
6 hospital beds with mattress and mackintosh
1 stainless steel instrument tray
1 forceps jar
1 kerosene lamp
4 large kidney dishes
1 length measure for babies
1 Long bench
6 Mercury sphygmomanometers
4 hand breast pumps with rubber bulbs
1 refridgerator
1 screen
1 Mackintosh sheet
1 Littman stethoscope
1 stitch removal or suture scissors
1writing table
2 sets of Sims Vaginal speculum
Labour Room
4 medium artery forceps
2 stainless steel adult bedpans
1 Stainless steel bowl with stand
2 delivery couches
1pair of dissecting forceps
1 dressing trolley
2 enema cans
2 episiotomy scissors
2 aluminiumfoetal stethoscopes
4 packs of disposable gloves (100pcs/pack)
4 sponge holding forceps
1 Littman stethoscope
2 Sims vaginal speculum
1 wall clock
1 water container with tap
2 screens
Soap/disinfectant dispenser
1 angle poised lamp
1 manual vacuum extractor
1 suction pump
1 baby weighing scale
3 urinary catheters
1pack of umbilical cord clamps (100 pcs)
2 drip stands

178
OBSERVATIONAL CHECKLIST FOR FACILITY-READINESS OF PRIMARY HEALTH
CENTRESTO DELIVER PHC SERVICES CONTD
1 suture kit
1 set of Oro pharyngeal airway (7 pcs)
10 plastic aprons
Family Planning
1 pack of Disposable gloves (100 pcs)
1 instrument tray
1 stainless steel
1 medium sized stainless kidney dish
1 mercury sphygmomanometer
1 pair of dissecting forceps
1 small sized sterilizer
1 angle poised lamp
1 IUD kit
1 pedal bin
1 stainless steel bowl with stand
1 stainless instrument trolley
1 gynae couch
1 Auvards speculum
1 tenaculum forceps
Infant and Child Welfare
2 baskets with lids for ORS materials
1 Ceiling fan
2 Plastic chairs
1 Stainless covered bowl for cotton wool
Plastic bowls
Spoons
First Stage Room
3 Stainless bed pans
1 stainless steel bowl with stand
1 Stainless covered bowl for cotton wool
1 Pedal dustbin
1 Foetal stethoscope
1 stainlesss galipot
1 pack of disposable latex gloves (100 pcs/pck)
2 hospital beds with mattress and mackintosh
1 Mecury Sphygmomanometer
1 Kerosene pressure lamp
4 Mackintosh sheets
2 sponge holding forceps
1 Littman stethoscope
1 Office table
1 Seward weighing scale
2 sets of Oro pharyngeal airway (7pcs/set)
2 bedside cabinets
Antenatal/Interview Room
2 Ceiling fans
1 Examination couch
2 Foetal stethoscopes
1 stainless steel galipot

179
OBSERVATIONAL CHECKLIST FOR FACILITY-READINESS OF PRIMARY HEALTH
CENTRESTO DELIVER PHC SERVICES CONTD
20 packs of Latex gloves (100 pcs/pack)
1height measuring stick
1 reflex hammer
3 long wooden benches
2 Mackintosh sheets
1 pack of nail scrubbing brushes (12/pack)
1 pen torch
1 Mercury sphygmomanometer
1 stethoscope
2 tables
2 oral thermometers
6 tongue depressors
1 Soap/disinfectant dispenser
1 angle poised lamp
1 stainlesss steel bowl with stand
1 dressing trolley
20 packs of urine dipstick for sugar and albumin
(100pcs/pack)
50 ANC gowns for patients
1 Wall clock
1 door name plate
Nutrition
10 Spoons
10 Stainless drinking mugs
2 Gas cylinders
4 knives
1 gas cooker
1 seward weighing scale
2 blenders and mills
1 stainless tray
10 plates
4 water containers
4 buckets with lid
2 chopping boards
6 cooking spoons
2 Kerosene stoves
2 utility tables
1 set of cooking pots (6pcs/set)
Sterlization
1 bucket autoclave
1 tape dispenser
1 Scrub brush dispenser
1 autoclave tape
2 Storage cabinets
6 sets of sterilizing drums (3 pcs/set)
1 soap/disinfectant dispenser
1 pack of nail scrubbing brushes (12 pcs/pack)
1 wall clock

180
OBSERVATIONAL CHECKLIST FOR FACILITY-READINESS OF PRIMARY HEALTH
CENTRESTO DELIVER PHC SERVICES CONTD
1 door name plate
Personnel
1 Medical officer if available
1 CHO
4 Midwives or nurse mid wives
3 Community Health Extension Workers
1 Pharmacy technician
6 Junior Community Health Extension Workers
1 Medical records officer
1 Laboratory technician
2 Health attendants/assistants
2 Security personnel
1 General maintenance staff
Hours of operation
24 hour services
JCHEWs 60% in the health facility and 40% in the
communities
CHEWs: 80% in the facility and 20% in the
communities
Standing order for CHEWs and JCHEWs
Essential drug list
Other Requirements
1 mobile phone or communication radio
1 motor cycle
1 bicycle

181
APPENDIX 8
CRITERIA FOR WELL COMPOSED AND FUNCTIONAL VILLAGE AND WARD
DEVELOPMENT COMMITTEES
a. COMPOSITION:
1. At least 20% of the members should be female
2. The committee should have a chairman elected by members
3. The committee should have a secretary elected by members
4. The committee should have a treasurer elected by members
5. Representatives of the different sectors of the community or ward should be present in
the committee e.g. health sector, educational sector, traders, farmers etc.
6. The different communities in the ward and the different streets in the community
should be well represented.
b. FUNCTIONS
They should:
7. Meet at least once a month
8. Have identified health needs in the community
9. Relay their plans and decisions to members of the community at least once a month
10. Mobilize the community for health actions regularly
11. Take minutes during all meetings which should be signed
12. Have up to date financial records (if any)
13. Be involved in the essential drug programme of the PHC facility through its drug
revolving fund sub committee
14. Supervise the activities of village health workers or PHC workers

182
15. Send reports of its activities on a monthly basis to the next level of the PHC
managerial system (WDC or LGA PHC technical committee)
16. Be represented in the health committees of the Primary Health Centres
17. Be involved in health care decision-making in the villages and wards

183

184

185

186

187

188
A crosssection of the Focus Group Discussion with members of VDC 1
A Crosssection of the Focus Group Discussion with members of WDC 3

189
Dr Bello collecting data from a health worker in one of the Primary Health Centres
Dr Bello, two community leaders and one of the research assistants