assessment and management of heart failure after left ... · stay, bleeding, reoperation, worsening...
TRANSCRIPT

1161
Case Presentation: A 56-year-old man with a history of ischemic
cardiomyopathy and New York Heart Association functional class IV heart failure (HF) requiring intravenous ino-tropic therapy underwent uncompli-cated implantation of a continuous-flow left ventricular assist device (LVAD) as bridge to heart transplantation (HT). The patient was weaned off inotropic support during the first week after sur-gery and had progressive improvement in functional status. He was discharged home on maintenance antithrombotic therapy with aspirin 325 mg once daily and warfarin targeted to an interna-tional normalized ratio of 2.0 to 3.0. Eight weeks after LVAD implantation, he developed progressive dyspnea on exertion, recurrent pedal edema, and a 7-pound weight gain. Physical exami-nation revealed conjunctival pallor, a palpable carotid pulse, jugular venous pressure of 14 cm H
2O, and 2+ pitting
edema bilaterally. A rapid and targeted assessment of recurrent HF is essential in this LVAD patient because of multi-ple, potentially life-threatening causes that necessitate divergent treatments.
LVAD Therapy in Advanced HF
The US Food and Drug Administration first approved implantable LVADs as a bridge to transplantation in 1994.1 Although HT remains the gold stan-dard therapy for selected patients with end-stage HF, the stable donor base of <2500 hearts per year in North America limits its widespread appli-cability.2 The landmark Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) trial established the first-generation, pulsatile-flow HeartMate (HM) XVE LVAD as a viable, life-prolonging treatment in patients who were not candidates for HT, a strategy known as destination therapy (DT). However, survival 2 years after implantation was still only 23%, in part because of the high rates of mechanical pump failure.
The advent of continuous-flow LVADs has provided a more durable long-term treatment that improves quality of life and survival.3 The continuous- flow HM II LVAD has a markedly lower rate of device failure
(0.06 versus 0.51 events per patient-year) and overall lower complication rates than the pulsatile HM XVE. Furthermore, survival at 2 years was 58% with the HM II compared with 24% with the HM XVE. Continued improvements have come with increas-ing experience, and 2-year actuarial survival for continuous-flow LVADs is now 70%.4 This has made DT a viable option for a much larger number of patients and accommodated longer waiting times for bridge-to-transplan-tation patients. Consequently, there has been a significant increase in both the number of LVADs implanted for DT and the use of continuous-flow LVADs, which now account for virtually 100% of DT implants in the United States.
A shift in use to less critically ill patients has occurred as a result of these improvements in survival and durability, again expanding the eligible patient population. The Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) database classifies a patient’s clinical profile on a scale from 1 to 7, with 1 being the most
(Circulation. 2014;129:1161-1166.)© 2014 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.113.002836
From the Cardiovascular Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School (M.A.B., M.M.G.), and VA Boston Healthcare System (M.A.B.), Boston, MA.
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/lookup/suppl/doi:10.1161/CIRCULATIONAHA. 113.002836/-/DC1.
Correspondence to Michael M. Givertz, MD, Cardiovascular Division, Brigham and Women’s Hospital, 75 Francis St, Boston, MA 02115. E-mail [email protected]
Assessment and Management of Heart Failure After Left Ventricular Assist Device ImplantationMichael A. Burke, MD; Michael M. Givertz, MD
CLINICIAN UPDATE
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from

1162 Circulation March 11, 2014
critically ill.4 The majority of patients in the REMATCH and HM II DT tri-als were classified as INTERMACS profile 1 (critical cardiogenic shock) or 2 (progressive decline), whereas the more recent Evaluation of the HeartWare Left Ventricular Assist Device for the Treatment of Advanced Heart Failure (ADVANCE) trial using the continuous-flow HeartWare ven-tricular assist device enrolled a major-ity of INTERMACS profile 3 (stable but inotrope-dependent) patients.5 The currently enrolling Randomized Evaluation of VAD Intervention Before Inotropic Therapy (REVIVE-IT)1 and Risk Assessment and Comparative Effectiveness of Left Ventricular Assist Device and Medical Management (ROADMAP; NCT01452802) trials aim to enroll even less sick patients with INTERMACS profiles of 4 to 7.
Various new, smaller, and more durable devices are in development. They no longer require an externalized driveline and are implantable intraperi-cardially or intraventricularly. These advances promise further expansion of the population of patients eligible for this technology. Not surprisingly, the number of centers implanting LVADs is also expanding, including non-HT pro-grams.4 Although encouraging, these changes have resulted in a burgeoning population of patients presenting with post-LVAD complications. Knowledge of how to triage and manage these patients is increasingly important for emergency medicine physicians, gen-eral cardiologists, and internists as the population of LVAD patients continues to expand.
Recurrent HF After LVAD Implantation
Persistent HF early after LVAD implantation is common, occurring in at least 20% to 25% of patients.6 Right ventricular (RV) dysfunction is the most common cause of early postop-erative HF and can be attributable to preexisting RV disease, perioperative RV injury, or excessive volume resus-citation. Early postoperative RV failure is defined as the requirement for a RV
assist device or continued use of ino-tropes >14 days after implantation and is associated with increased length of stay, bleeding, reoperation, worsening renal function, impaired quality of life, and increased mortality.7 Additional causes of early post-LVAD HF include inappropriate LVAD pump speed, mis-alignment of the LVAD inflow can-nula, and LVAD thrombosis. Because providers specializing in mechanical circulatory support will manage most of these causes during the surgical admission, their workup and treatment are not covered further in this update. Readers are referred to comprehensive management guidelines.6
Recurrent HF late after successful LVAD implantation is also common, although the incidence is uncertain. For the purposes of this update, we define late HF as HF occurring >4 weeks after LVAD implantation in a patient with resolution of early postoperative RV dysfunction and other acute periopera-tive issues. HF late after LVAD implan-tation can be attributable to either LV or RV failure, each in turn resulting from LVAD-related or non–LVAD-related causes (Table 1).
Recurrent left-sided HF can occur with LVAD thrombosis, obstruction of the LVAD inflow or outflow can-nula (as a result of kinking or, rarely, thrombosis), motor dysfunction, or fracture of the percutaneous driveline, which connects the implanted LVAD motor to the external system control-ler (see Figure 1 in Reference 8).8 Each of these malfunctions reduces LVAD pump output, which, if significant, can lead to HF attributable to inadequate
forward flow. An inappropriately low LVAD pump speed can also cause HF as a result of inadequate LV unload-ing or worsening mitral regurgitation. Non–LVAD-related causes of late, left-sided HF include aortic valve insuffi-ciency (AI) and severe anemia caused by gastrointestinal bleeding.
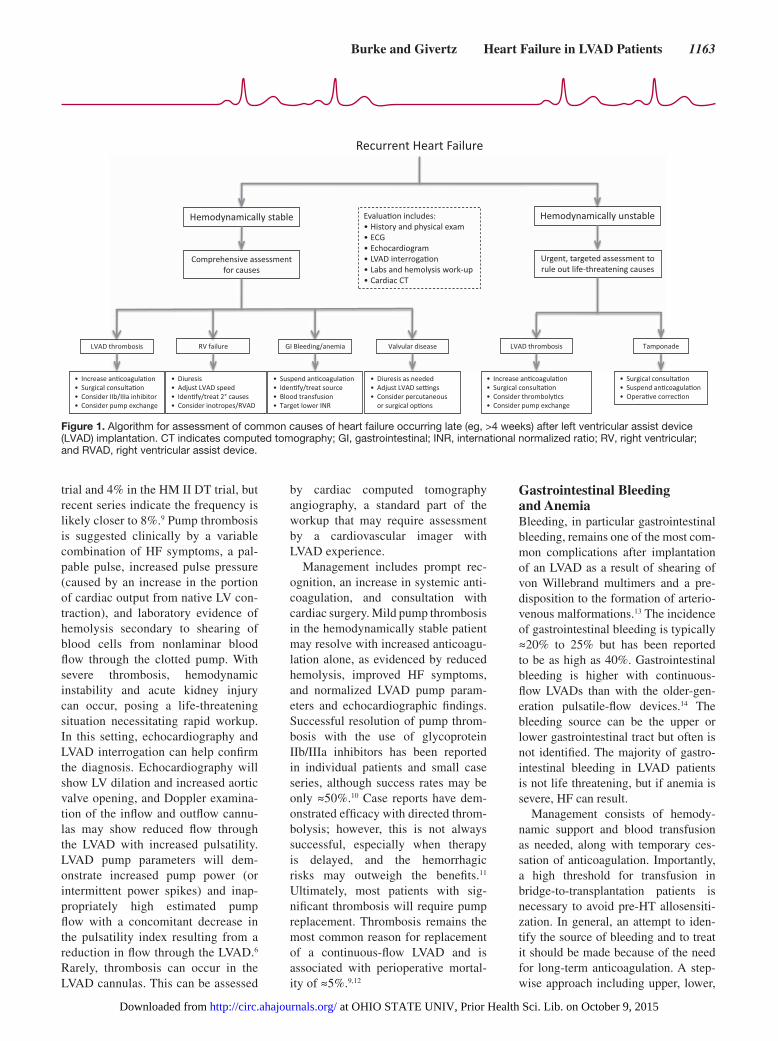
New or recurrent right-sided HF can be caused by inappropriately high LVAD pump speed. This results in shift of the septum toward the LV that distorts RV geometry, which in turn reduces RV systolic function and causes worsening tricuspid regurgita-tion (TR). Inappropriately high pump speed can also result in excessive car-diac output, increasing venous return to an already impaired RV. Recurrent primary RV failure can also be attribut-able to new or worsening primary RV myocardial dysfunction or tricuspid valve disease, ventricular arrhythmias, persistent pulmonary hypertension, pulmonary embolism, or rarely late cardiac tamponade. A systematic eval-uation for differentiating potential causes of recurrent HF in the patient with an LVAD can lead to timely and appropriate treatment (Figure 1).
Specific Causes and Treatment of Recurrent
HF After LVADLVAD Pump ThrombosisThrombosis of the LVAD pump is the most concerning cause of recurrent HF because it can cause death if not iden-tified and managed promptly. Pump thrombosis occurred in 2% of patients in the HM II bridge-to-transplantation
Table 1. Causes of Late Heart Failure After LVAD Implantation
LV Failure RV Failure
LVAD related Pump thrombosisInflow or outflow cannula obstructionPercutaneous lead or motor failurePump speed too low
Cardiac tamponadePump speed too high
Non–LVAD related New/worsening aortic insufficiencyGastrointestinal bleeding with severe anemia
Intrinsic RV dysfunctionPersistent pulmonary hypertensionPulmonary embolismNew/worsening tricuspid regurgitationVentricular arrhythmias
LV indicates left ventricle; LVAD, left ventricular assist device; and RV, right ventricle.
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from
Burke and Givertz Heart Failure in LVAD Patients 1163
trial and 4% in the HM II DT trial, but recent series indicate the frequency is likely closer to 8%.9 Pump thrombosis is suggested clinically by a variable combination of HF symptoms, a pal-pable pulse, increased pulse pressure (caused by an increase in the portion of cardiac output from native LV con-traction), and laboratory evidence of hemolysis secondary to shearing of blood cells from nonlaminar blood flow through the clotted pump. With severe thrombosis, hemodynamic instability and acute kidney injury can occur, posing a life-threatening situation necessitating rapid workup. In this setting, echocardiography and LVAD interrogation can help confirm the diagnosis. Echocardiography will show LV dilation and increased aortic valve opening, and Doppler examina-tion of the inflow and outflow cannu-las may show reduced flow through the LVAD with increased pulsatility. LVAD pump parameters will dem-onstrate increased pump power (or intermittent power spikes) and inap-propriately high estimated pump flow with a concomitant decrease in the pulsatility index resulting from a reduction in flow through the LVAD.6 Rarely, thrombosis can occur in the LVAD cannulas. This can be assessed
by cardiac computed tomography angiography, a standard part of the workup that may require assessment by a cardiovascular imager with LVAD experience.
Management includes prompt rec-ognition, an increase in systemic anti-coagulation, and consultation with cardiac surgery. Mild pump thrombosis in the hemodynamically stable patient may resolve with increased anticoagu-lation alone, as evidenced by reduced hemolysis, improved HF symptoms, and normalized LVAD pump param-eters and echocardiographic findings. Successful resolution of pump throm-bosis with the use of glycoprotein IIb/IIIa inhibitors has been reported in individual patients and small case series, although success rates may be only ≈50%.10 Case reports have dem-onstrated efficacy with directed throm-bolysis; however, this is not always successful, especially when therapy is delayed, and the hemorrhagic risks may outweigh the benefits.11 Ultimately, most patients with sig-nificant thrombosis will require pump replacement. Thrombosis remains the most common reason for replacement of a continuous-flow LVAD and is associated with perioperative mortal-ity of ≈5%.9,12
Gastrointestinal Bleeding and AnemiaBleeding, in particular gastrointestinal bleeding, remains one of the most com-mon complications after implantation of an LVAD as a result of shearing of von Willebrand multimers and a pre-disposition to the formation of arterio-venous malformations.13 The incidence of gastrointestinal bleeding is typically ≈20% to 25% but has been reported to be as high as 40%. Gastrointestinal bleeding is higher with continuous-flow LVADs than with the older-gen-eration pulsatile-flow devices.14 The bleeding source can be the upper or lower gastrointestinal tract but often is not identified. The majority of gastro-intestinal bleeding in LVAD patients is not life threatening, but if anemia is severe, HF can result.
Management consists of hemody-namic support and blood transfusion as needed, along with temporary ces-sation of anticoagulation. Importantly, a high threshold for transfusion in bridge-to-transplantation patients is necessary to avoid pre-HT allosensiti-zation. In general, an attempt to iden-tify the source of bleeding and to treat it should be made because of the need for long-term anticoagulation. A step-wise approach including upper, lower,
Figure 1. Algorithm for assessment of common causes of heart failure occurring late (eg, >4 weeks) after left ventricular assist device (LVAD) implantation. CT indicates computed tomography; GI, gastrointestinal; INR, international normalized ratio; RV, right ventricular; and RVAD, right ventricular assist device.
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from

1164 Circulation March 11, 2014
and video endoscopy, followed by push or balloon enteroscopy and tagged red blood cell scanning, is necessary. HF is typically mild and self-limited, resolv-ing with restoration of an adequate hematocrit. Some have advocated the use of the somatostatin analog octreo-tide, although data in LVAD patients are mixed and extremely limited. Once bleeding has resolved, anticoagulation should be reinstituted with a lower target international normalized ratio. Gastrointestinal bleeding can be recur-rent, and in rare cases, patients have been managed off anticoagulation.
Primary RV DysfunctionFailure of the RV is the most common cause of late HF after LVAD implan-tation. In the HM II DT trial, late RV failure, defined as reinstitution of ino-tropes >14 days after implantation, occurred in 7% of patients.7 Late RV failure can be due primarily to intrin-sic RV disease or can be secondary to a number of causes, including ven-tricular arrhythmias, progressive TR, pulmonary hypertension, or pulmo-nary embolism. Initial workup should focus on ruling out other causes of HF, in particular ventricular assist device malfunction or thrombosis.
With LVAD support, ventricular arrhythmias are generally not life-threatening but, when sustained or repetitive, can cause RV dysfunction and recurrent HF.15 Antiarrhythmic or ablative therapies are usually war-ranted. Rarely, refractory arrhythmias may require the addition of RV assist device support. Pulmonary hyperten-sion, which is nearly ubiquitous in the advanced HF population, improves significantly with LVAD therapy, even when defined as “fixed” before ven-tricular assist device implantation.16 However, the time to reversal var-ies from days to months. Therefore, patients with persistent pulmonary hypertension after LVAD implantation are at risk for early or late RV failure resulting from sustained RV afterload in the setting of increased RV pre-load and preexisting RV dysfunction. Treatment with phosphodiesterase type
5 inhibitors can improve pulmonary hemodynamics in those with persistent pulmonary hypertension after LVAD,17 but it is unclear whether there is any clinical benefit. Standard HF therapies, including diuresis and, in severe cases, inotropes, are used as supportive ther-apy when overt HF is present.
Primary RV myocardial dysfunction in the absence of a secondary cause poses a greater challenge. Initial treat-ment with diuresis is warranted, but for those with progressive myocardial dysfunction, reinstitution of inotropic therapy may be necessary. The use of inotropic therapy is associated with reduced survival and worse quality of life and should be avoided if possible. In those eligible for HT, RV support with a durable RV assist device is indi-cated for refractory HF, but this option is not approved for DT. Therefore, a major goal of the pre-LVAD workup is to identify patients at risk for RV fail-ure.18 Despite the availability of several different risk scores, RV failure after LVAD implantation has proved diffi-cult to predict.
Valvular Heart DiseaseNew or worsening AI can also result in late-onset HF. AI after LVAD implan-tation is common, occurring in up to 38% of patients, and is associated with a worse prognosis.19 As a result, preexisting AI greater than mild in
severity should be corrected at the time of LVAD implantation.20 Despite this, AI frequently occurs de novo after LVAD surgery and is progres-sive with continued LVAD support as a result of changes in hemodynamics across the aortic valve and in the aortic root. Significant AI increases LV pre-load and LVAD flow while paradoxi-cally reducing forward cardiac output and thus can cause LV failure despite adequate LVAD function. Changes in medical therapy and device speed are usually ineffective, and refractory AI causing HF must be treated invasively. First-line treatment is surgical, either with oversewing of the aortic valve or valve replacement. Percutaneous aortic valve closure or replacement can also be performed successfully in those who are at excessive risk for surgery.
Severe TR resulting in RV failure is typically attributable to worsening of preexisting TR in the setting of either progressive primary RV dysfunction and dilation or high LVAD pump speed that causes septal shift and altered RV geom-etry. Preexisting TR is associated with worse outcomes after LVAD surgery. As with preexisting AI, the best treat-ment is prevention by performing tricus-pid valve surgery at the time of LVAD implantation. Tricuspid valve annulo-plasty may reduce the incidence of post-LVAD HF.20 Management of worsening TR post-LVAD implantation begins with
Table 2. Pertinent Laboratory Values at Baseline, Admission, and Follow-Up
Parameter Baseline Admission Follow-Up
Sodium, mmol/L 136 136 139
HCO3, mmol/L 22 22 25
BUN, mg/dL 14 26 21
Creatinine, mg/dL 0.91 2.15 1.49
ALT, U/L 30 30 21
Total bilirubin, mg/dL 0.3 1.6 0.3
LDH, U/L 470 5230 416
Hemoglobin, g/dL 10.5 6.9 11.2
Free hemoglobin, mg/dL 3.3 26.5 5.5
Hematocrit, % 33.3 21.5 34.9
Haptoglobin, mg/dL <8 <8 <8
INR (Target) 2.0-3.0 1.8 2.9
ALT indicates alanine aminotransferase; BUN, blood urea nitrogen; HCO3, bicarbonate; INR, international
normalized ratio; and LDH, lactate dehydrogenase.
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from
Burke and Givertz Heart Failure in LVAD Patients 1165
conservative therapies that target a poorly functioning RV or a reduction in LVAD pump speed to mitigate septal shift. If this is not successful, surgical valve repair may need to be considered.
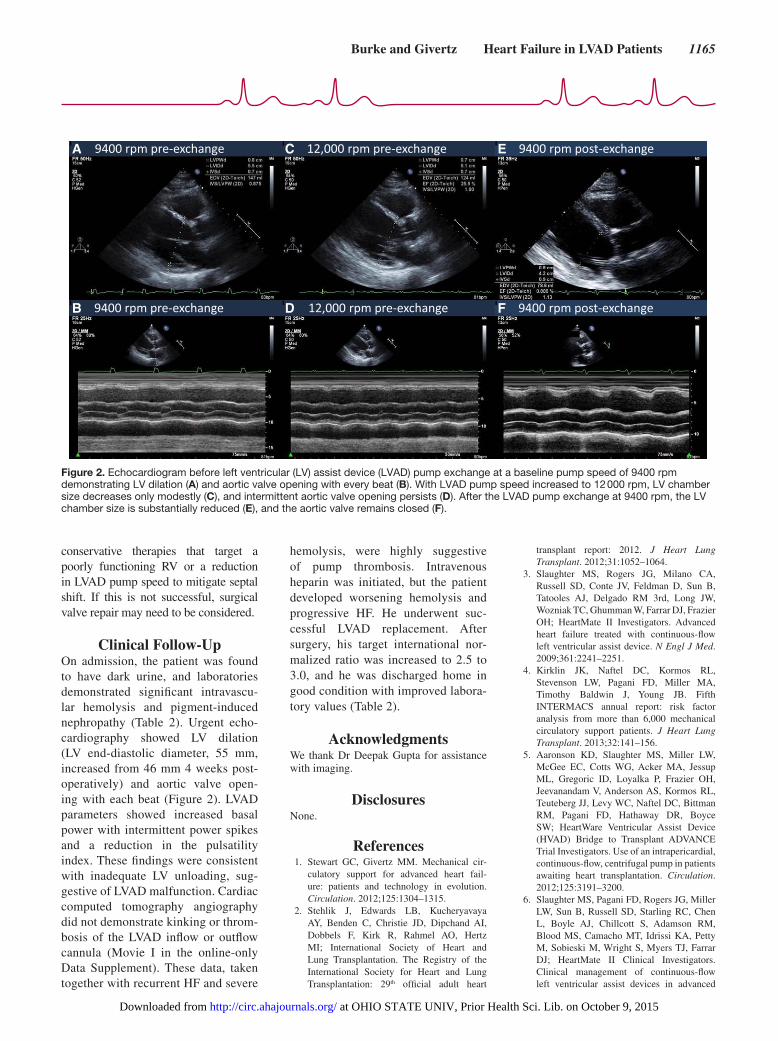
Clinical Follow-UpOn admission, the patient was found to have dark urine, and laboratories demonstrated significant intravascu-lar hemolysis and pigment-induced nephropathy (Table 2). Urgent echo-cardiography showed LV dilation (LV end-diastolic diameter, 55 mm, increased from 46 mm 4 weeks post-operatively) and aortic valve open-ing with each beat (Figure 2). LVAD parameters showed increased basal power with intermittent power spikes and a reduction in the pulsatility index. These findings were consistent with inadequate LV unloading, sug-gestive of LVAD malfunction. Cardiac computed tomography angiography did not demonstrate kinking or throm-bosis of the LVAD inflow or outflow cannula (Movie I in the online-only Data Supplement). These data, taken together with recurrent HF and severe
hemolysis, were highly suggestive of pump thrombosis. Intravenous heparin was initiated, but the patient developed worsening hemolysis and progressive HF. He underwent suc-cessful LVAD replacement. After surgery, his target international nor-malized ratio was increased to 2.5 to 3.0, and he was discharged home in good condition with improved labora-tory values (Table 2).
AcknowledgmentsWe thank Dr Deepak Gupta for assistance with imaging.
DisclosuresNone.
References 1. Stewart GC, Givertz MM. Mechanical cir-
culatory support for advanced heart fail-ure: patients and technology in evolution. Circulation. 2012;125:1304–1315.
2. Stehlik J, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dipchand AI, Dobbels F, Kirk R, Rahmel AO, Hertz MI; International Society of Heart and Lung Transplantation. The Registry of the International Society for Heart and Lung Transplantation: 29th official adult heart
transplant report: 2012. J Heart Lung Transplant. 2012;31:1052–1064.
3. Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, Sun B, Tatooles AJ, Delgado RM 3rd, Long JW, Wozniak TC, Ghumman W, Farrar DJ, Frazier OH; HeartMate II Investigators. Advanced heart failure treated with continuous- flow left ventricular assist device. N Engl J Med. 2009;361:2241–2251.
4. Kirklin JK, Naftel DC, Kormos RL, Stevenson LW, Pagani FD, Miller MA, Timothy Baldwin J, Young JB. Fifth INTERMACS annual report: risk factor analysis from more than 6,000 mechanical circulatory support patients. J Heart Lung Transplant. 2013;32:141–156.
5. Aaronson KD, Slaughter MS, Miller LW, McGee EC, Cotts WG, Acker MA, Jessup ML, Gregoric ID, Loyalka P, Frazier OH, Jeevanandam V, Anderson AS, Kormos RL, Teuteberg JJ, Levy WC, Naftel DC, Bittman RM, Pagani FD, Hathaway DR, Boyce SW; HeartWare Ventricular Assist Device (HVAD) Bridge to Transplant ADVANCE Trial Investigators. Use of an intrapericardial, continuous-flow, centrifugal pump in patients awaiting heart transplantation. Circulation. 2012;125:3191–3200.
6. Slaughter MS, Pagani FD, Rogers JG, Miller LW, Sun B, Russell SD, Starling RC, Chen L, Boyle AJ, Chillcott S, Adamson RM, Blood MS, Camacho MT, Idrissi KA, Petty M, Sobieski M, Wright S, Myers TJ, Farrar DJ; HeartMate II Clinical Investigators. Clinical management of continuous-flow left ventricular assist devices in advanced
B
E
D
C
F
A
Figure 2. Echocardiogram before left ventricular (LV) assist device (LVAD) pump exchange at a baseline pump speed of 9400 rpm demonstrating LV dilation (A) and aortic valve opening with every beat (B). With LVAD pump speed increased to 12 000 rpm, LV chamber size decreases only modestly (C), and intermittent aortic valve opening persists (D). After the LVAD pump exchange at 9400 rpm, the LV chamber size is substantially reduced (E), and the aortic valve remains closed (F).
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from

1166 Circulation March 11, 2014
heart failure. J Heart Lung Transplant. 2010;29(suppl):S1–S39.
7. Kormos RL, Teuteberg JJ, Pagani FD, Russell SD, John R, Miller LW, Massey T, Milano CA, Moazami N, Sundareswaran KS, Farrar DJ; HeartMate II Clinical Investigators. Right ventricular failure in patients with the HeartMate II continuous-flow left ventricu-lar assist device: incidence, risk factors, and effect on outcomes. J Thorac Cardiovasc Surg. 2010;139:1316–1324.
8. Givertz MM. Cardiology patient pages: ven-tricular assist devices: important informa-tion for patients and families. Circulation. 2011;124:e305–e311.
9. Starling RC, Moazami N, Silvestry SC, Ewald G, Rogers JG, Milano CA, Rame JE, Acker MA, Blackstone EH, Ehrlinger J, Thuita L, Mountis MM, Soltesz EG, Lytle BW, Smedira NG. Unexpected abrupt increase in left ventricular assist device thrombosis. N Engl J Med. 2014; 370:33–40.
10. Potapov EV, Stepanenko A, Krabatsch T, Hetzer R. Managing long-term complica-tions of left ventricular assist device therapy. Curr Opin Cardiol. 2011;26:237–244.
11. Kamouh A, John R, Eckman P. Successful treatment of early thrombosis of HeartWare left ventricular assist device with intraven-tricular thrombolytics. Ann Thorac Surg. 2012;94:281–283.
12. Stulak JM, Cowger J, Haft JW, Romano MA, Aaronson KD, Pagani FD. Device exchange after primary left ventricular assist device implantation: indications and outcomes. Ann Thorac Surg. 2013;95:1262–1267.
13. Eckman PM, John R. Bleeding and throm-bosis in patients with continuous-flow ventricular assist devices. Circulation. 2012;125:3038–3047.
14. Crow S, John R, Boyle A, Shumway S, Liao K, Colvin-Adams M, Toninato C, Missov E, Pritzker M, Martin C, Garry D, Thomas W, Joyce L. Gastrointestinal bleeding rates in recipients of nonpulsatile and pulsatile left ventricular assist devices. J Thorac Cardiovasc Surg. 2009;137:208–215.
15. Garan AR, Yuzefpolskaya M, Colombo PC, Morrow JP, Te-Frey R, Dano D, Takayama H, Naka Y, Garan H, Jorde UP, Uriel N. Ventricular arrhythmias and implantable cardioverter-defibrillator therapy in patients with continuous-flow left ventricular assist devices: need for primary prevention? J Am Coll Cardiol. 2013;61:2542–2550.
16. Etz CD, Welp HA, Tjan TD, Hoffmeier A, Weigang E, Scheld HH, Schmid C. Medically refractory pulmonary hyperten-sion: treatment with nonpulsatile left ven-tricular assist devices. Ann Thorac Surg. 2007;83:1697–1705.
17. Tedford RJ, Hemnes AR, Russell SD, Wittstein IS, Mahmud M, Zaiman AL,
Mathai SC, Thiemann DR, Hassoun PM, Girgis RE, Orens JB, Shah AS, Yuh D, Conte JV, Champion HC. PDE5A inhibitor treat-ment of persistent pulmonary hypertension after mechanical circulatory support. Circ Heart Fail. 2008;1:213–219.
18. Wilson SR, Mudge GH Jr, Stewart GC, Givertz MM. Evaluation for a ventricular assist device: selecting the appropriate can-didate. Circulation. 2009;119:2225–2232.
19. Pak SW, Uriel N, Takayama H, Cappleman S, Song R, Colombo PC, Charles S, Mancini D, Gillam L, Naka Y, Jorde UP. Prevalence of de novo aortic insufficiency during long-term support with left ventricular assist devices. J Heart Lung Transplant. 2010;29:1172–1176.
20. Feldman D, Pamboukian SV, Teuteberg JJ, Birks E, Lietz K, Moore SA, Morgan JA, Arabia F, Bauman ME, Buchholz HW, Deng M, Dickstein ML, El-Banayosy A, Elliot T, Goldstein DJ, Grady KL, Jones K, Hryniewicz K, John R, Kaan A, Kusne S, Loebe M, Massicotte MP, Moazami N, Mohacsi P, Mooney M, Nelson T, Pagani F, Perry W, Potapov EV, Eduardo Rame J, Russell SD, Sorensen EN, Sun B, Strueber M, Mangi AA, Petty MG, Rogers J; International Society for Heart and Lung Transplantation. The 2013 International Society for Heart and Lung Transplantation guidelines for mechan-ical circulatory support: executive summary. J Heart Lung Transplant. 2013;32:157–187.
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from

SUPPLEMENTAL MATERIAL
Assessment and Management of Heart Failure Following Left Ventricular Assist
Device Implantation Michael A. Burke, MD and Michael M. Givertz, MD
Supplemental Video Cardiac computed tomography angiography demonstrating no obstruction to flow in either the LVAD inflow or outflow cannula.

Michael A. Burke and Michael M. GivertzImplantation
Assessment and Management of Heart Failure After Left Ventricular Assist Device
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2014 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.113.002836
2014;129:1161-1166Circulation.
http://circ.ahajournals.org/content/129/10/1161World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2014/05/23/129.10.1161.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at OHIO STATE UNIV, Prior Health Sci. Lib. on October 9, 2015http://circ.ahajournals.org/Downloaded from