assessing opportunities to improve performance measures focused on major depressive disorder sarah...
TRANSCRIPT

Assessing opportunities to improve performance measures focused on
major depressive disorder
Sarah Sampsel, MPHResearch Scientist
June 2008

2Academy HealthJune 2008
NCQA: Committed to Measurement, Transparency,
AccountabilityQuality measurement means:•Use of objective measures based on evidence•Results that are comparable across organizations•Impartial third-party evaluation and audit•Public Reporting
NCQA’s quality programs include:•Accreditation of health plans using performance data•HEDIS clinical measures•CAHPS consumer survey•Measurement of quality in provider groups•Physician Recognition
3Academy HealthJune 2008
Study Purpose
• Assess effects of proposed changes to HEDIS Antidepressant Medication Management measure– In HEDIS since 1999– Eligible population identification concerns
• Length of negative diagnosis history• Length of negative medication history
– Opportunities to improve optimal practitioner contacts rate• Inclusion of care management
• National monitoring of quality has not resulted in improvements in care…can revisions in a nationally standardized performance measure result in improvement?
4Academy HealthJune 2008
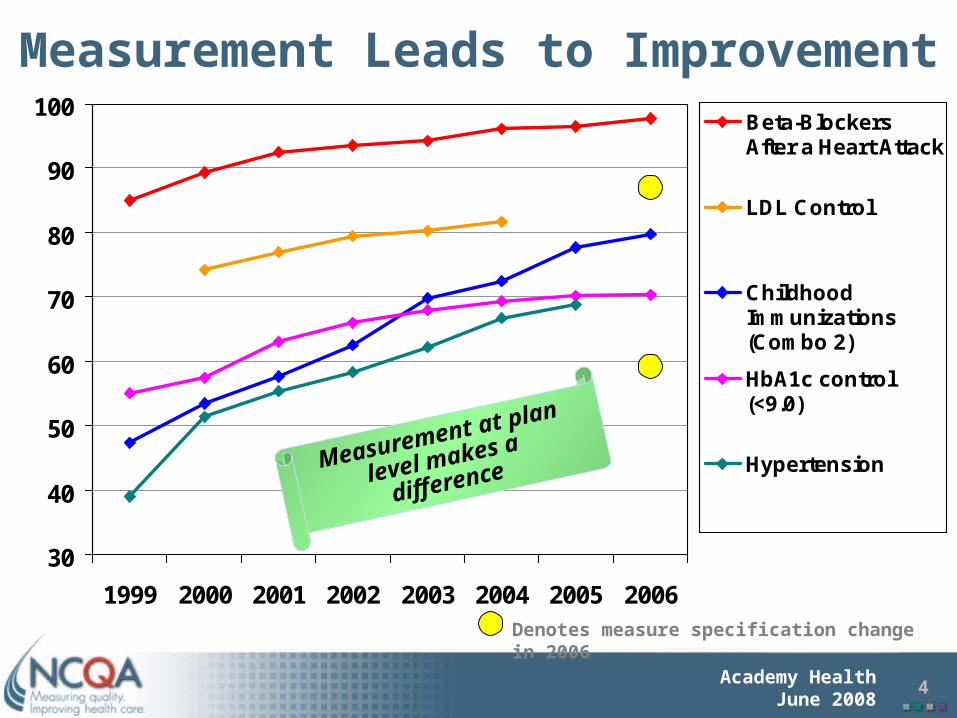
Measurement Leads to Improvement
30
40
50
60
70
80
90
100
1999 2000 2001 2002 2003 2004 2005 2006
Beta-BlockersAfter a Heart Attack
LDL Control
ChildhoodImmunizations(Combo 2)
HbA1c control(<9.0)
Hypertension
Denotes measure specification change in 2006
Measurement at plan
level makes a difference

5Academy HealthJune 2008
State of Health Care Quality 2007State of Health Care Quality 2007
0
10
20
30
40
50
60
70
2003 2004 2005 2006 2007
Optimal Contacts Acute Phase Continuation Phase
Antidepressant Medication Management – Commercial Rates
6Academy HealthJune 2008
HEDIS® Antidepressant Medication Management Measure
• Eligible population: health plan members, 18 years and older, with a new diagnosis of major depressive disorder and a new prescription for an antidepressant. Three rates: – Optimal practitioner contacts: members who
had three visits within 12 weeks (84 days)– Effective acute phase treatment: members
who remain on an antidepressant for 84 days– Effective continuation phase treatment:
members who remain on an antidepressant for at least 180 days

7Academy HealthJune 2008
Study Design
• Three health plans• Membership: 244,794 – 492,005• 3980 total members in eligible
population •Diagnosis of major depression•Prescription for anti-depressant•18 – 85 years
• Patient level data•Current and past diagnoses and visit dates•Current and past prescriptions•Care management utilization

8Academy HealthJune 2008
Population Characteristics
0
10
20
30
40
50
60
70
Gender
Male Female
0
5
10
15
20
25
30
35
40
45
Age Group
18-34 yrs 35-44 yrs 45-54 yrs55-64 yrs 65+

9Academy HealthJune 2008
Prior Diagnosis and Prescription within Past Year
n % Population with prior Dx
n % Population with Prior Rx
A (N=418) 40 9.57% 113 27.03%
B (N=733) 97 13.23% 201 27.42%
C (N=2829)
243
8.59% 741 26.19%
Commercial(N=3738)
352
9.42% 997 26.67%
Medicaid(N=240)
28 11.67% 58 24.17%
Total (N=3980)
380
9.55% 1055
26.51%

10Academy HealthJune 2008
What happens if negative history criteria are lengthened? Eligible
Population Effect SizesNegative History Criteria
Total Eligible
Population
N % Differenc
eCurrent SpecNeg Dx = 120Neg Rx = 90
3980 -- --
Neg Dx = 120Neg Rx = 120
3360 620 -15.6%
Neg Dx = 150Neg Rx = 150
3250 730 -18.3%
Neg Dx = 180Neg Rx = 180
3163 817 -20.5%

11Academy HealthJune 2008
Effects on Measure Rates (Aggregated)
Negative History Criteria
Optimal
Contacts
Acute Phase
Continuation Phase
Current SpecNeg Dx = 120Neg Rx = 90
12.34% 61.43% 45.38%
Neg Dx = 120Neg Rx = 120
15.99% 57.16% 41.62%
Neg Dx = 150Neg Rx = 150
15.79% 57.01% 41.37%
Neg Dx = 180Neg Rx = 180
15.65% 57.06% 41.39%
12Academy HealthJune 2008
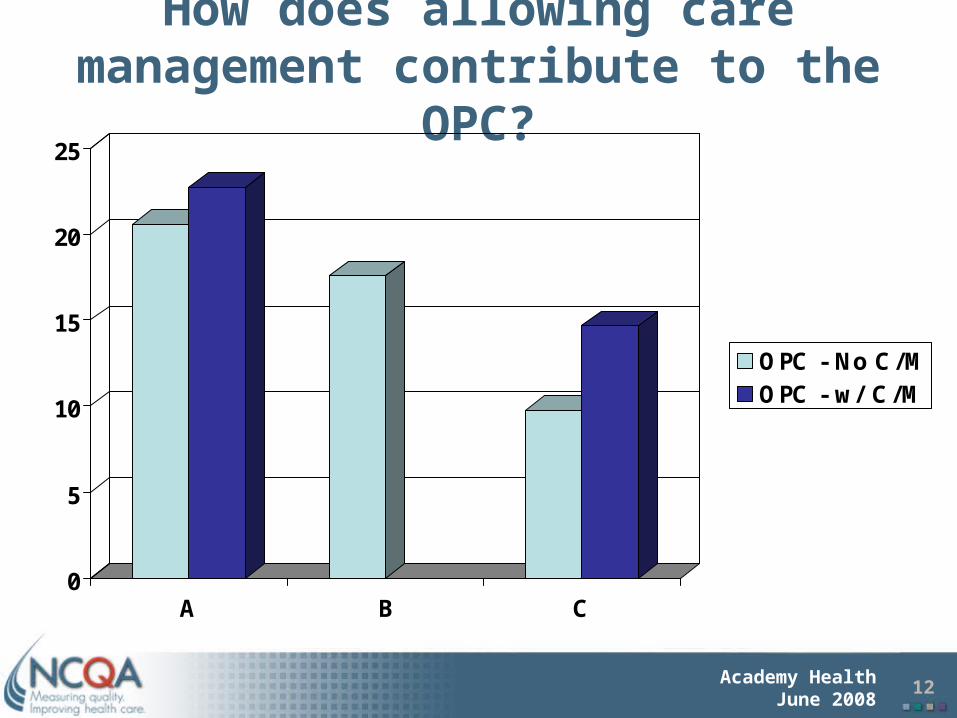
How does allowing care management contribute to the
OPC?
0
5
10
15
20
25
A B C
OPC - No C/MOPC - w/ C/M
13Academy HealthJune 2008
Conclusions
• While revisions to the eligible population specifications would increase the specificity of identification; they do not meaningfully impact measure rates
• Adding care management did not meaningfully impact improvements in optimal practitioner contacts rate– Optimal practitioner contacts rate will be retired for
HEDIS 2009
• There are opportunities to refocus efforts to improve measurement in this area– Assessment and monitoring– Use of standardized assessment tool– Expand to broader population
14Academy HealthJune 2008
Acknowledgements
• NCQA Staff– Zakiya Pierre– Sarah Hudson Scholle– Phil Renner– Greg Pawlson– Lisa Nern
• NCQA Behavioral Health Measurement Advisory Panel (BHMAP)
• Field-test sites