asl application form deadline: may 15
TRANSCRIPT

Page1
Parent/GuardianInformation__________________________________________
PrimaryParent/Guardian
Name:______________________________
Address:_________________________________________________
DateofBirth(mm/dd/yyyy):_____/_____/_______
EmailAddress:____________________________________________
HomePhoneNumber:______-______-__________
CellPhoneNumber:______-_______-__________
BusinessPhoneNumber:______-______-_________
SecondaryParent/Guardian
Name:______________________________
Address:_________________________________________________
DateofBirth(mm/dd/yyyy):_____/_____/_______
EmailAddress:____________________________________________
HomePhoneNumber:______-______-__________
CellPhoneNumber:______-_______-__________
BusinessPhoneNumber:______-______-_________
ASLApplicationFormDeadline:May15Submitto:[email protected]

Page2
DelegateInformation_________________________________________________
Name:___________________________________
PreferredName:________________
Gender(circleone):M/F
Height:_________
Weight:_________
HairColor:_________
EyeColor:_________
T-ShirtSize(circleone):Youth:Small/Medium/Large
Adult:Small/Medium/Large/XL/XXL
GradeEnteringintheFall:________
CurrentSchool:_____________________________________
SchoolEnteringintheFall(ifapplicable):__________________________________
SchoolType(circleone):Public/Private/Homeschool/Other
EthnicOrigin(Circleallthatapply):
• AmericanIndian/AlaskanNative
• Asian
• Black/AfricanAmerican
• Hawaiian/PacificIslander
• Hispanic/Latino
• White
• TwoormoreEthnicities
DateofBirth(mm/dd/yyyy):____/____/________
DelegateEmailAddress:___________________________
DelegateCellPhone:______-_______-__________

Page3
Pleaseindicateanyspecialinformationweshouldbeawareof(circleallthatapply):
• Medication
• MedicalCondition
• Life–ThreateningAllergy
• Allergy
• Asthma
• SpecialNeeds
• DietaryRestrictions
• Other
• None
HaveYouPreviouslyAttendedanMLWprogram?Yes/No
If“Yes”,whichprogramdidyouattend?_________________
HowdidyouhearaboutMLW?(circleone)
• School• Friends• MASC/StudentGovernment• LeadershipMaryland• Newspaper/Campguides• FormerDelegatesand/orStaff• MLWWebsite• Facebook• CampFair• Other
InterviewAvailability_________________________________________________Partofyourapplicationisaphoneinterview.Onthelinesnexttothedaysoftheweek,pleaselistthehoursthatyou,thedelegate,aretypicallyavailablefora15to20-minuteintervieweachday.Weekdayinterviewscantakeplaceintheeveningsandweekendinterviewscanhappenduringtheday.Pleaselistthewindowoftimethatyouaretypicallyavailable.
Monday Saturday Tuesday Sunday Wednesday Thursday Friday

Page4
SponsorshipInformation______________________________________________
Areyoureceivingasponsorship(meaningyourtuitionisbeingpartiallyorfullypaidforbysomeoneelse)fromyourschoolorotherorganization?(circleone)Yes/No
If“Yes”,pleasecompletetheinformationbelow:
SponsoredtoattendMLWby:______________________________
Amountofsponsorship:_______________
ContactNameforSponsorship:_____________________________
EmailforSponsorship:___________________________
PhoneforSponsorship:______-______-__________
MedicalQuestionnaire________________________________________________
DuetonewregulationswewillrequireallapplicantstocompleteandsubmitallMedicalforms(availablewiththerestofoursupplementalforms).Ifanyoftheformsdonotpertaintoyourchild,simplymarkN/Aontheformbeforesubmitting.
EmergencyContacts_____________________________________________________________
Pleaseindicatetwoalternativepeopletocontactifthefamilyisnotavailable.
PrimaryEmergencyContact:_________________________
RelationtoDelegate:________________
PrimaryPhone:______-______-__________
SecondaryPhone______-______-__________
SecondaryEmergencyContact:____________________________
RelationtoDelegate:__________________
PrimaryPhone:______-______-__________
SecondaryPhone:______-______-_________

Page5
HealthcareProviderContactInformation____________________________________________
Delegate'sPhysician:____________________________
PhysicianPhone:______-______-__________
PhysicianAddress:__________________________
Nameoffamilydentist/orthodontist:____________________
Dentist/OrthodontistPhone:______-______-__________
Dentist/OrthodontistAddress:______________________
HealthInformation______________________________________________________________
Doesyourchildhaveanymedicalconditions,psychologicalconditions,behavioralconditions,medications,dietaryrestrictions,allergies,orspecialneedsthatweneedtobeawareof?(circleone)
Yes/No
Pleaseexplainanymedicalconditions,psychologicalconditions,behavioralconditions,medications,dietaryrestrictions,allergies,orspecialneedsthatweneedtobeawareof:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Doesyourchildhaveanymedicationallergies?(circleone)Yes/No
Pleaseexplainanymedicationallergies:__________________________________________________________________________________________________________________________________________________________________________
Doesyourchildhaveanyfoodorotherallergies?(circleone)Yes/No
Pleaseexplainanyfoodorotherallergies:__________________________________________________________________________________________________________________________________________________________________________
Doesyourchildhavedietaryrestrictionsorotherneeds?(circleone)Yes/No
Pleaseexplainanydietaryrestrictionsorotherneeds:__________________________________________________________________________________________________________________________________________________________________________

Page6
ImmunizationInformation________________________________________________________
DoesthedelegateresidewithintheUnitedStates?(circleone)Yes/No
If“Yes”,pleasecompletetheinformationbelow:
State/Territorywherethedelegateresides:__________________________
Isthedelegateexemptfromimmunizations?(circleone)Yes/No
If“Yes”,pleaselistthem:________________________________________________________
If“No”,pleaseprovidethecountryinwhichthedelegateresides:_______________________
PleaseNote:AllInternationalDelegatesarerequiredtocompleteandsubmitanInternationalimmunizationform,availablethroughthisURL:
https://phpa.health.maryland.gov/OIDEOR/IMMUN/Shared%20Documents/MDH_896_form.pdf
InsuranceInformation___________________________________________________________
Isthedelegatecoveredbymedical/hospitalinsurance?(circleone)Yes/No
If“Yes”,pleasecompletetheinformationbelow:
InsuranceCompany:_______________________________________
InsurancePhoneNumber:______-______-__________
PolicyNumber:_______________________________
GroupNumber:_______________________________
IDNumber:__________________________________
If“No”,pleasereadandsignthesectiononthenextpage:

Page7
Thereisnomedicalinsuranceineffecttocovermyabove-namedson/daughterforanyillnesses,injuries,orotheradversehealthoutcomesthathe/shemayexperience.I,therefore,herebyagreetoassumedirectandcompletefinancialresponsibilityforanyandallmedicalcareofanykindthatmyabove-mentionedson/daughterreceiveswhileattendingMarylandLeadershipWorkshops,Inc.’s2018summerresidentialleadershipprograms.
Further,IherebyagreetoreimburseMarylandLeadershipWorkshops,Inc.foranyandallcosts,medicalexpenses,andothersumsthatMarylandLeadershipWorkshops,Inc.advancesthatrelatetothemedicaltreatmentofmyson/daughterwhilehe/sheisattendingMarylandLeadershipWorkshops,Inc.’s2018summerprograms.
____________________________________________________________________
Parent/LegalGuardianSignature PrintedName Date
ScholarshipInformation_______________________________________________
Ifapplyingforascholarshipfor2018,pleasecontactmatt@leadershipmd.orgtoobtainascholarshipapplication.
Parent/LegalGuardianEmploymentInformation__________________________
PrimaryParent/Guardianemployer:__________________________________________
SecondaryParent/Guardianemployer:_____________________________________________
Page8
BehavioralQuestionnaire_____________________________________________
ThesectionprovidedonthefollowingpageasksforinformationthatisimportantforustoensureyourchildhasasuccessfulweekatMLW.YouranswerstothesequestionsARENOTafactorintheacceptanceofyourchildintoourprogram.Pleasebehonestandforthrightsothatourstaffcanbestpreparetoworkwithyourchild.
Ifyourchildhasamentalorphysicalhealthdiagnosisorissue,howdoesitaffectthemonaday-to-daybasis?Whatdoweneedtoknow?
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Hasyourchildeverbeenhospitalizedduetobehavioralissues?Ifyes,pleaseexplain:
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Hasyourchildeverbeenawayfromhomewithoutfamilyforaweek?(circleone)Yes/No
Doesyourchildrelateeasilytoothers,oristhatoftenachallenge?
_____________________________________________________________________________________
Doesyourchildenjoyparticipatinginlargegroupactivities?Oraretheyhappierbeingalone/insmallgroups?
_____________________________________________________________________________________
Whenyourchildisfrustrated,angry,upsetorsad,howdotheyhandletheseemotions?
__________________________________________________________________________________________________________________________________________________________________________
Whattechniquesaresuccessfulforhandlinginappropriatebehaviorsbyyourchild,shouldthosebehaviorsarise?
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Describeyourchild'spersonality.Whatdotheyenjoy/notenjoydoing?
_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Page9
CustodialInformation________________________________________________
Doesanyoneotherthantheadultslistedinthisapplicationhavepermissiontopickyourchildupfromcamp?(oldersiblings,extendedfamilymembers,friends,etc.)
(circleone)Yes/No
If“Yes”,pleaseenterthenamesandphonenumbersofupto3authorizedpersonsbelow:
AuthorizedPerson1Name:_______________________________________
AuthorizedPerson1PhoneNumber:______-______-__________
AuthorizedPerson2Name:_______________________________________
AuthorizedPerson2PhoneNumber:______-______-__________
AuthorizedPerson3Name:_______________________________________
AuthorizedPerson3PhoneNumber:______-______-__________
Isthereanissueovercustodyofthedelegate?(circleone)Yes/No
If“Yes”,pleaseexplaintheissueovercustody.Beasthoroughaspossiblesothereisnoconfusionwhileyourchildisinourcare:
____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Page10
Waivers____________________________________________________________Parents/Guardians-Pleasereadthisformandreviewwithyourchild.
AttendanceandRefundPoliciesThefollowingrefundscheduleappliesfordelegateswhocanceltheirregistration.·CancellationsbeforeMay1st,willreceivea$500refund.·CancellationsbetweenMay1standJune1st,willreceivea$300refund.·CancellationsafterJune1stcannotberefunded.·RefundswillbeissuedbySeptember30th.Allnecessaryitemsforacompleteapplication,includingsignedmedicalforms,mustbereceivedpriortoMay15th.Areservedspaceintheprogrammaybeforfeitedinordertomakeroomforthedelegateswhoareonthewaitinglistifmaterialisnotreceivedbythedeadline.StudentsparticipatinginMLW’ssummerprogramsmustparticipateintheentireweek-longresidentialexperience.Studentswillnotbepermittedtoarriveattheprogramlateordepartearly.Unfortunately,refundscannotbemadetostudentswho,forunexpectedhealthorotherreasons,mustleavetheprogramearly.MLWreservestherighttoexpelwithoutrefundanystudentwhoviolatesMLW’sRulesandExpectations,violatesMarylandStatelaw,orforothercause.
PermissiontoApplyandAttendIherebygrantpermissionformychildtoapplytoandparticipateinthisprogram.Iacceptandassumeanyandallrisksassociatedwithhis/herattendanceandparticipationintheprogramanditsactivities.Iunderstandthatmychildshouldnotattendthecampifhe/sheisnothealthy.Iunderstandthatmychildmustabidebyprogrampoliciesandtheinstructionsofprogramstaff.Ipermitmychildandhis/herimagetobeinvolvedinactivitiesandmediaeventsthataredesignedtopromotethebenefitsofMarylandLeadershipWorkshops,Inc.,includingbutnotlimitedtophotographs,videotapes,postingimagesontheMLWwebsite,facebookpage,Twitter,Instagramandothersocialmedia,newslettersandpressreleases.Additionally,IherebygrantpermissionforMLWtosharetheschoolnameandemailaddressofmychildwithotherparticipantsinMLWprograms,localschoolsystempersonnel,LeadershipMaryland,andlocalcommunityleadershipassociations.Knowingthesefacts,I,formyself,mychildattendingtheprogram,andanyoneelsewhomightclaimonmyormychild’sbehalf,herebyagreethatMLWisnotresponsibleforlostorstolenitems,accidents,injuries,and/ormedicalordentalexpensesarisingfrommychild’sparticipationintheprogramand,accordingly,Icovenantnottosue,andwaive,releaseanddischargeMLWandanyoneworkingontheirbehalffromanyandallclaimsofliabilityorexpensesofanykindornaturewhatsoeverarisingoutoforrelatingtomychild’sparticipationintheprogram.Ihavecarefullyreadalloftheinformationinthisapplicationformandagreetoallconditions.
Page11
ExpectationsofDelegateRESPECTRespectforoneanotherisofprimaryimportanceinorderforalldelegatesandstaffmemberstolearnandgrowthroughouttheweek.Treatotherswithrespectfulbehaviorsothatyoumayexpectthesameinreturn.Respectfulbehaviorincludes:·RespectrequestsmadebyMLWstaffmembersandcampusemployees.·Avoidtheuseofprofanity/obscenelanguage.·RespecttheprivacyofMLWparticipantsandothergroupswhomaybeusingthecampus.·Avoidtouchingofotherpeopleandtheirbelongings(thisincludesfightsandtheft).·Respectallideasandbeliefsandavoidtheuseofderogatorycommentstowardsothers.ATTENDANCEItisexpectedthatyouwillattendallscheduledactivities.Wehavemanyfunandchallengingactivitiesforyouandexpectthatyouwillbeapartofeachone.Eatingthreebalancedmealsaday,drinkingplentyofliquids,andgettingenoughsleepwillensurethatattendingallactivitieswillbenoproblem.Incaseofanemergencyoranycircumstancepreventingparticipationinactivities,notifyastaffmemberimmediately!
RulesandProcedurestoFollowforaSAFEandFUNweekINANDAROUNDDORMITORIESTherewillbenoguysongirls’hallsandnogirlsonguys’hallsunlessapprovedinadvanceforanofficialactivity.Thisincludesstairwellsthatleadfromsuchhalls,whicharelabeled“offlimits.”Commonareasareopentoalldelegates.Nooutsidevisitorsarepermittedatanytimeduringtheweekwithoutpriorpermissionfromtheprogramdirector.Intheeventofafire,pullthefirealarmandexitthebuildingquickly,knockingonthedoorsthatyoupass.Checkinwithyourassignedstaffmemberatthedesignatedmeetinglocation.Intheeventofanothertypeofemergency,contactthestaffmemberwhoisonDormDuty.His/hernamewillbepostedonyourhalleachday.Donotpropopenoutsidedoorsatanytime.

Page12
CHECK-INANDLIGHTSOUTCheck-inwilloccureverynightatthetimeindicatedintheguidebookyoureceiveatregistration.Youmustcheckinwithastaffmemberfromyourhallbythestatedtime.Wewillgiveyoutimetogetreadyforbed,andwewillusuallyscheduleahallmeetingaftercheck-in.LightsmustbeTURNEDOFFatthetimedesignatedinyourguidebook.Althoughyoumaybeaccustomedtostayingupabitlater,rememberthatthisweekisveryactiveanddemandsyourfullenergyeveryday.Youwillneedyoursleeptofullyparticipateinallactivities.AROUNDTHECAMPUSAtregistration,youwillreceiveanMLWbuttonwithyournameonit.Thisbuttonmustbewornatalltimesunless,ofcourse,youareintheshowerorsleeping.Youmustalsowearshoesatalltimesexceptwhenshoweringandsleeping(althoughyoumaywanttowearshowershoes).YoumayNOTleavecampusatanytimeorforanyreason.Ifyouareuncertainofcampusboundaries,askastaffmember.Commercialpropertieslocatednearthecampusarenotpartofthecampus.Ifyouhaveforgottenanecessityitem,givetheofficestaffmoneyandawrittendescriptionoftheitem,andtheywillsecureitforyou.Ifyouaredrivingyourselftotheprogram,pleaseinformtheMLWExecutiveDirectorAnitaAndersonatanita@leadershipmd.orgsothatparkingandotherarrangementscanbemadeforyou.DoNOTwalkaloneanywhere—alwaystakeabuddywithyou.TOBACCO,ALCOHOL,ANDOTHERDRUGSThepossessionand/oruseofdrugs,alcohol,andtobaccoisabsolutelyforbiddenatalltimesduringtheweek.Nooverthecounterorprescriptionmedicationisallowedindormrooms.AllmedicationistobeturnedintothehealthconsultantatregistrationandwillbeavailablebycomingtotheMLWonsiteoffice.Onlydelegateswithformssignedbyahealthpractitionerwillbeallowedtotakeoverthecounterorprescriptionmedication.
INAPPROPRIATEBEHAVIORANDCONSEQUENCESTheseexpectationsareintendedtoallowalldelegatesandstaffmemberstohaveasafeandsuccessfulweek.Anybehaviordescribedinthisdocumentoratthediscretionofastaffmemberthatthreatensorjeopardizesthesafetyofotherpersonsortheirenjoymentoftheprogramwillnotbetolerated.TheMLWdirectorsandstaffmaytakeanyofthefollowingactionsasaconsequencefordelegateswhodonotmeettheexpectationsoutlinedabove:·Aconferencewiththedelegateandastaffmember.·Aconferencewiththedelegateandaprogramdirector.·Aphonecallhomeinformingaparent/guardianoftheincident.·Adelegate-writtenletterofapologytotheoffendedparty.·Thewithholdingofparticipationinsocialactivities.·Removalfromtheprogram(aparent/guardianwillberequestedtopickupthestudent).
Page13
MEDICATIONANDHEALTHCARERELEASE
PARENTALRELEASEANDACKNOWLEDGMENT:Igivepermissiontoauthorizedpersonneltocarryoutsuchemergencydiagnosticandtherapeuticproceduresasmaybenecessaryformyson/daughter,andalsopermitsuchprocedurestobecarriedoutat,andby,localhospital(s)intheeventthatmyson/daughteristakenthereforemergencycare.Iagreetothereleaseofanyrecordsnecessaryforinsurancepurposes.IgrantpermissiontoMarylandLeadershipWorkshops,Inc.toarrangeanyrelatedtransportationnecessarytocareformychild.Iunderstandthatanymedicalexpenseswillbedirectlybilledtomyinsurancecompanyorme.Icertifythatallmedicalandhealthhistoryinformationprovidedinthisapplicationiscompleteandaccuratetothebestofmyknowledge.IherebyreleaseandholdharmlessMarylandLeadershipWorkshops,Inc.anditsagents,servants,contractorsandemployeesfromanyandallliabilitythatmayresultfrommedicalcareofmyson/daughter.Ifurthercertify,thatunlessindicatedontheDelegateMedicationForm,myson/daughteriscapableofself-administeringanyprescribedmedication(s)andIassumeallresponsibilityandliabilitystemmingfrommydecisiontohavemychildself-administermedication(s).Intheeventthatthereisnomedicalinsuranceineffecttocovermyabove-namedson/daughterforanyillnesses,injuries,orotheradversehealthoutcomesthathe/shemayexperience.Iherebyagreetoassumedirectandcompletefinancialresponsibilityforanyandallmedicalcareofanykindthatmyabove-mentionedson/daughterreceiveswhileattendingMarylandLeadershipWorkshops,Inc.’s2018summerresidentialleadershipprograms.Further,IherebyagreetoreimburseMarylandLeadershipWorkshops,Inc.foranyandallcosts,medicalexpenses,andothersumsthatMarylandLeadershipWorkshops,Inc.advancesthatrelatetothemedicaltreatmentofmyson/daughterwhilehe/sheisattendingMarylandLeadershipWorkshops,Inc.’s2018summerprograms.
MychildandIhavereadandunderstandthepolicies,expectations,andrulesstatedaboveandacknowledgethatviolationofanyoftheserulesmayresultindismissal.
DelegateFirstandLastName:___________________________________________________________
DelegateSignature:__________________________________________________Date:______________
Parent/GuardianFirstandLastName:______________________________________________________
Parent/GuardianSignature:___________________________________________Date:______________

Page14
MLWPACKINGLIST
• Enoughcomfortable,weatherappropriateclothingfortheweek.Yourclothesfortheweekshouldbeschool-appropriate;ifyouwouldn’tbeallowedtowearitatschool,pleasedonotbringittoMLW.MLWstaffanddelegatesallwearcasual,comfortableclothing.It’sagoodideatobringshorts,t-shirts,jeans,sneakers,andasweatshirt,aswe’llbedoingactivitiesbothinsidetheairconditioningandoutsideinthesummerheat.
• Therewillbeavarietyshow/showcasethatdelegateswillplanandimplement.Pleasebringanyinstruments,equipment,oranythingelsethatwillhelpyoushareyourtalentwiththerestoftheMLWcommunity,ifyoulike.
• Sheetsforanextra-longtwinbed(and/orasleepingbag)andablanket(thedormsareairconditionedsoitcangetcold)
• Pillow
• Towels–bathtowel,handtowel,washcloth
• Toiletries(don’tforgetatoothbrush,toothpaste,handsoap,showersoap,anddeodorant)
• ShowerShoes
• Arainjacket/umbrella
• AlarmClock
• Pensorpencils
• Reusablewaterbottle
• Smallbackpackordrawstringbagtocarryguidebook,pens,etc.
• Athleticequipmentforrecreationtime
• Lightsnacksanddrinksforevenings(optional–MLWwillalsoprovide).
• Anoutfit(shorts,tshirt,oldshoes)thatcangetwetanddirty
• Onebusinesscasualoutfit
• SunscreenandBugSpray,aswedoactivitiesoutdoorsduringthedayanintheevenings.

Page15
TobecompletedbyApplicant:Delegate(Student)Name: RecommenderName: TobecompletedbyRecommender:RecommenderAddress: City/State/Zip: Phone: Emailaddress: RelationshiptoStudent: LengthofTimeYouHaveKnownStudent:
Pleaserateapplicantinthefollowingareasusingascalefrom1-5
(1=notatallstronginthisarea,2=lowinthisarea,3=averageinthisarea,4=goodinthisarea,5=very
stronginthisarea)
Abilitytoworkwithothers 1 2 3 4 5
Self-awareness 1 2 3 4 5
Communicationskills 1 2 3 4 5
Abilitytogiveandreceivefeedback 1 2 3 4 5
Abilitytoempowerandmotivateothers 1 2 3 4 5
ALSApplicationRecommendationFormAlsoavailableonlineatgoo.gl/c8eFxRTotheApplicant:IfyouhaveneverattendedanMLWprogram,pleasegivethisformtobecompletedbysomeonewhocanwriteaboutyourleadershippotential.Besuretocompleteyourinformationbeforegivingtheformtoyourrecommender.Itisalsoagoodideatoprovideaself-addressed,stampedenvelope.TotheRecommender:Pleaseanswerthequestionsbelowbasedonyourinteractionwiththeapplicant.Ifaccepted,thisstudentwillspendaweekwithstudentleadersfromtheMid-Atlanticregion,developinghis/herleadershipskills,implementingaproject,andsettinggoalsforactionathome.Formoreinformation,visitwww.mlw.org.
Page16
Pleaserespondtothefollowingquestionsinordertogiveusadditionalinsightontheapplicant.Ifyou
wouldprefer,youmayuseanadditionalsheetofpapertorecordyouranswers.
1. Whataretheapplicant’sstrengthsandweaknesses?
2. Howdoestheapplicantdemonstrateleadershippotential?
3. HowwouldtheMLWcommunitybeenrichedbytheapplicant’sparticipation?
4. Othercomments:
______________________________________________________ ____________
Signature Date
Pleasereturnthisformdirectlyto:MLW,c/oLeadershipMD.,134HolidayCourt,Suite318,Annapolis,
MD21401orFax:410-841-2104;[email protected]

Page17
DelegateFirstandLastName:
__________________________________________________________________________________
Date:___/____/_____
1. WhydoyouwanttoattendALS?
2. Usingyourownwords,howwouldyoubestdefineordescribe“leadership”?Thinkaboutcharacteristics,skills,qualities,and/orbehaviorsleaderspossessincreatingyourdefinition/description.
3. Usingyourdefinition/descriptionofleadershipfromquestion2,tellusaboutoneinstanceinwhichyoudemonstratedleadership.Describetheskillsandqualitiesyouused,thechallengesyoufaced,andhowyouovercamethosechallenges.
4. ImaginethatyouweretheleaderofacommitteethatwasputinchargeoffixingaseriousissuefacinghighschoolstudentsinMaryland.Whatseriousissuewouldyouchoose?Whywouldyouchoosethisissue?Whatspecificallycouldyourcommitteedotohelp?
5. Describeyourself.Whatareyourinterestsand/ortalents?Whattypesofactivitiesareyouinvolvedwith?Whatdoyouliketodoinyoursparetime?
6. ALSisalearningexperiencedesignedtohelpyougrow.WhataspectofyourleadershippotentialwouldyouliketoworkonwhileatALS?WhatskillswouldyouliketodeveloporpolishwhilehereatALS?
7. WhatisonepieceofadvicethatyouhavefortheupcomingALSstaffaswedesignourprogram?Considerwhattopicsoractivitiesyouwouldlikeustoinclude,howyou’dlikeustoschedulethedays,thingsyouwantustokeepthesameasotherMLWprogramsandthingsyou’dliketochangefromotherMLWprograms.
8. PleaselisttheyearsthatyouhavepreviouslyattendedMLW,theprogramandgroupthatyouwereinforthoseyears,themainideaofyourgroup’sproject,andthemajorconceptsorskillsthatyoutookoutofeachyear.
ALSApplicationStudentLeadershipInsightsQuestionnairePleaseanswerthefollowingquestionsonaseparatesheetofpaperincompletesentences.Youmayeithertypeorwriteneatlyinblueorblackink.Pleaseputyourfullnameatthetopofeachpage.Applicantanswersareusuallyaboutahalf-pagetofullpageinlength,butpleasefeelfreetouseasmuchspaceasyouwouldlike.TheanswerstothesequestionsareafactorusedintheprocesstodeterminewhetheryouareacceptedtoALS.Ifyouareaccepted,thestaffwilluseyouranswerstodesignaprogramtomeetyourneeds.
Page18
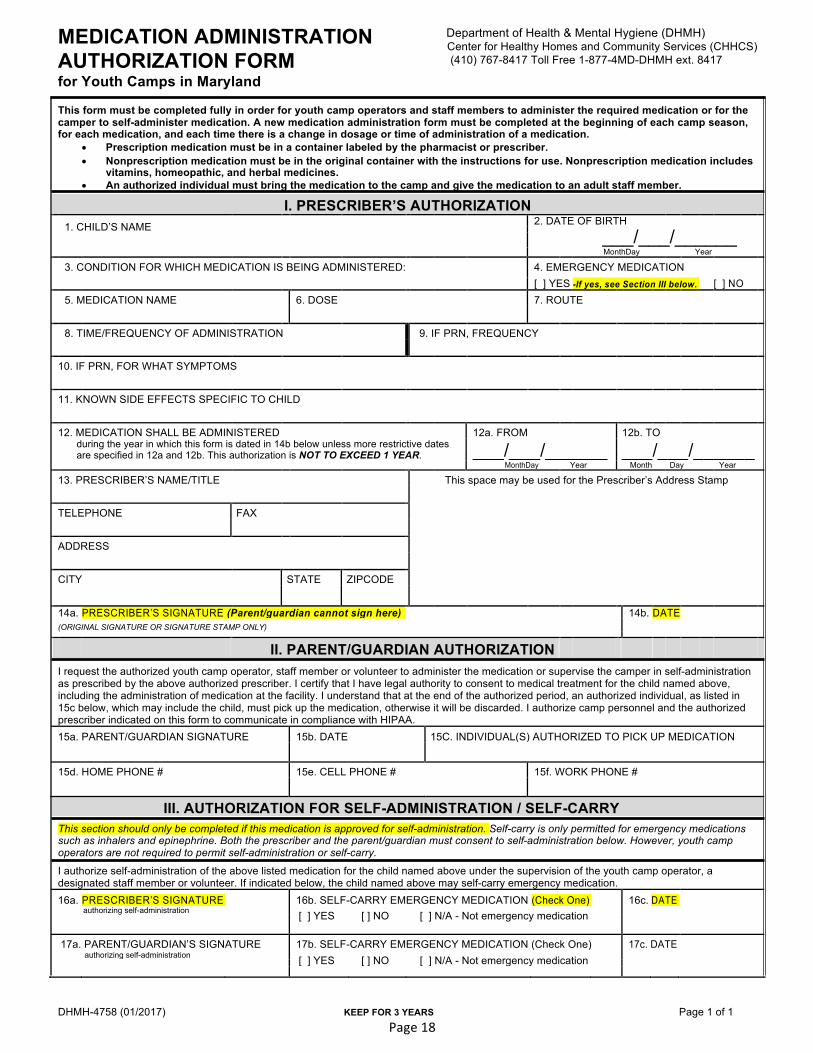
MEDICATION ADMINISTRATION AUTHORIZATION FORM for Youth Camps in Maryland
Department of Health & Mental Hygiene (DHMH) Center for Healthy Homes and Community Services (CHHCS) (410) 767-8417 Toll Free 1-877-4MD-DHMH ext. 8417
This form must be completed fully in order for youth camp operators and staff members to administer the required medication or for the camper to self-administer medication. A new medication administration form must be completed at the beginning of each camp season, for each medication, and each time there is a change in dosage or time of administration of a medication.
• Prescription medication must be in a container labeled by the pharmacist or prescriber. • Nonprescription medication must be in the original container with the instructions for use. Nonprescription medication includes
vitamins, homeopathic, and herbal medicines. • An authorized individual must bring the medication to the camp and give the medication to an adult staff member.
I. PRESCRIBER’S AUTHORIZATION 1. CHILD’S NAME 2. DATE OF BIRTH ___/___/______
MonthDay Year
3. CONDITION FOR WHICH MEDICATION IS BEING ADMINISTERED: 4. EMERGENCY MEDICATION
[ ] YES -If yes, see Section III below. [ ] NO 5. MEDICATION NAME 6. DOSE 7. ROUTE 8. TIME/FREQUENCY OF ADMINISTRATION 9. IF PRN, FREQUENCY 10. IF PRN, FOR WHAT SYMPTOMS 11. KNOWN SIDE EFFECTS SPECIFIC TO CHILD 12. MEDICATION SHALL BE ADMINISTERED 12a. FROM 12b. TO during the year in which this form is dated in 14b below unless more restrictive dates ___/___/______ ___/___/______ are specified in 12a and 12b. This authorization is NOT TO EXCEED 1 YEAR. MonthDay Year Month Day Year
13. PRESCRIBER’S NAME/TITLE This space may be used for the Prescriber’s Address Stamp TELEPHONE FAX ADDRESS CITY STATE ZIPCODE 14a. PRESCRIBER’S SIGNATURE (Parent/guardian cannot sign here) 14b. DATE (ORIGINAL SIGNATURE OR SIGNATURE STAMP ONLY)
II. PARENT/GUARDIAN AUTHORIZATION I request the authorized youth camp operator, staff member or volunteer to administer the medication or supervise the camper in self-administration as prescribed by the above authorized prescriber. I certify that I have legal authority to consent to medical treatment for the child named above, including the administration of medication at the facility. I understand that at the end of the authorized period, an authorized individual, as listed in 15c below, which may include the child, must pick up the medication, otherwise it will be discarded. I authorize camp personnel and the authorized prescriber indicated on this form to communicate in compliance with HIPAA. 15a. PARENT/GUARDIAN SIGNATURE 15b. DATE 15C. INDIVIDUAL(S) AUTHORIZED TO PICK UP MEDICATION
15d. HOME PHONE # 15e. CELL PHONE # 15f. WORK PHONE #
III. AUTHORIZATION FOR SELF-ADMINISTRATION / SELF-CARRY
This section should only be completed if this medication is approved for self-administration. Self-carry is only permitted for emergency medications such as inhalers and epinephrine. Both the prescriber and the parent/guardian must consent to self-administration below. However, youth camp operators are not required to permit self-administration or self-carry. I authorize self-administration of the above listed medication for the child named above under the supervision of the youth camp operator, a designated staff member or volunteer. If indicated below, the child named above may self-carry emergency medication.
16a. PRESCRIBER’S SIGNATURE 16b. SELF-CARRY EMERGENCY MEDICATION (Check One) 16c. DATE authorizing self-administration [ ] YES [ ] NO [ ] N/A - Not emergency medication
17a. PARENT/GUARDIAN’S SIGNATURE 17b. SELF-CARRY EMERGENCY MEDICATION (Check One) 17c. DATE authorizing self-administration [ ] YES [ ] NO [ ] N/A - Not emergency medication
DHMH-4758 (01/2017) KEEP FOR 3 YEARS Page 1 of 1

Page19
MLWDELEGATEMEDICALFORM–OvertheCounterMedicationForm
ThedelegatewillonlybeallowedtohaveOTCmedicineandself-administermedicationonanasneededbasisifthisformisfilledoutcorrectlyandinourfiles.Therefore,pleasefillthisformoutcompletely,signatthebottom,andreturntoMLW(oruploadtoyouronlineaccount)byMay15th.THESEMEDICATIONSWILLBESTOREDINTHEMLWOFFICE,anddelegatescanrequesttotakethemasneeded.
Program: ALS MSEL SHW Journey DelegateName:
Delegate’sAge:___________ Delegate’sWeight:_______________
DrugNameGenericmaybesubstitutedforbrandname
Route/Howitistaken Dosage&Schedule(perlabelinstructionsbyage/weight,unlessotherwiseindicated)
Indications Parent/Guardian/HealthCareProviderPermission(circleone)
Thingstobeawareofwhenonthismedication/Comments
Tylenol(orgeneric)
PO(chewable,elixir,ortabs)PR(suppository)
PerlabelInstructions
PainorFever YesorNo
Ibuprofen PO(chewabletabs,suspension,ortablets)
PerlabelInstructions
PainorFever YesorNo
Robitussin(orgeneric)
PO(syrup) PerlabelInstructions
Cough YesorNo
Pepto-Bismol(orgeneric)
PO(liquidorchewabletabs)
PerlabelInstructions
Upsetstomach,Diarrhea
YesorNo
Kaopectate(orgeneric)
PO(liquidortab) PerlabelInstructions
Diarrhea YesorNo
Children’sMylanta(orgeneric)
PO(chewable) PerlabelInstructions
Upsetstomach YesorNo
Sudafed(orgeneric)
PO(tabsorliquid) PerlabelInstructions
Nasalcongestion,Eustachiantubecongestion
YesorNo
Chlorpheniramine PO(chewabletabs,suspension,ortabs)
PerlabelInstructions
Seasonalallergysymptoms
YesorNo
Zyrtec/Claritin PO PerlabelInstructions
Seasonalallergysymptoms
YesorNo
Dramamine/Bonine(orgeneric)
PO(chewable/regulartabs)
PerlabelInstructions
MotionSickness YesorNo
Dimetapp(orgeneric)
PO(elixirortabs) PerlabelInstructions
Nasalcongestion,Seasonallergy
YesorNo
Benadryl(orgeneric)
PO(elixir,chewable,tab,orpills);topicalointment
PerlabelInstructions
Allergicreactions(hives,insectbite,allergies)
YesorNo
Antibioticointment Topical PerlabelInstructions
Superficialcuts/abrasions
YesorNo
HydrocortisoneCream
Topical PerlabelInstructions
Allergicreactions,contactdermatitis,insectbite
YesorNo
CalamineLotion Topical PerlabelInstructions
Allergicreaction(insectbite,hives)
YesorNo
Vitaminsand/orSupplements*
PO PerlabelInstructions
YesorNo
I,_______________________(parent/guardianname),givepermissionformychildtotakethemedicationslisted“YES”aboveandmychildhastakenathomeatleast1doseofthemedication(s)listedas“YES”above.IdoNOTwantmychildtotakethefollowingmedications: ParentorLegalGuardian’sSignature Date