arrhythmia ed cme
DESCRIPTION
arrhythmia; pulseless arrest, tachyarrhythmia and bradyarrhythmiaTRANSCRIPT

CARDIAC ARRHYTHMIA
Dr Afifah

OBJECTIVES
• To recall basic heart anatomy and heart electrical system
• To be able to recognise and treat life threatening arryhthmias
– ALS approach

CONTENTS
• Heart anatomy • Normal rhythm • Overview – ALS algorithm • Pulseless arrest arrhythmia • Arrhythmia with pulse
– Bradyarrhythmias – Tachyarrhythmias
*Pathology and management – NCORT/ALS guideline • Medications • ECG quiz

ANATOMY OF THE HEART


6

HEART BEAT
• Pumping action that moves blood INTO, THROUGH, and AWAY from the heart
• Heart’s elecrical system:
– SA node
– AV node
– Bundle of His
– Purkinje fiber
• Normal HR: 60-100

8

NORMAL RHYTHM

• Originated from SA node
• Normal P
• Followed by normal QRS complex
• HR 60 - 100
Normal Sinus Rhythm (NSR)


WHAT IS ARRHYTHMIA?
• Any cardiac rhythm, regular or irregular, that is not driven by sinus node or,
• Any abnormality of the cardiac rhythm, even if the sinus node is the primary pacemaker

ALS ALGORITHM CARDIAC ARRHYTHMIA
13

14
Arrhtyhmia
Pulseless
Non shockable
Shockable
With pulse
Tachycardia
Unstable Stable
Wide QRS complex
Regular
Irregular
Narrow QRS complex
Regular
Irregular
Bradycardia
Unstable
Stable

PULSELESS ARREST NO PULSE

PULSELESS ARREST
• Shockable
– VF
– Pulseless VT
• Non shockable
– PEA
– Asystole


18


07-Dec-12




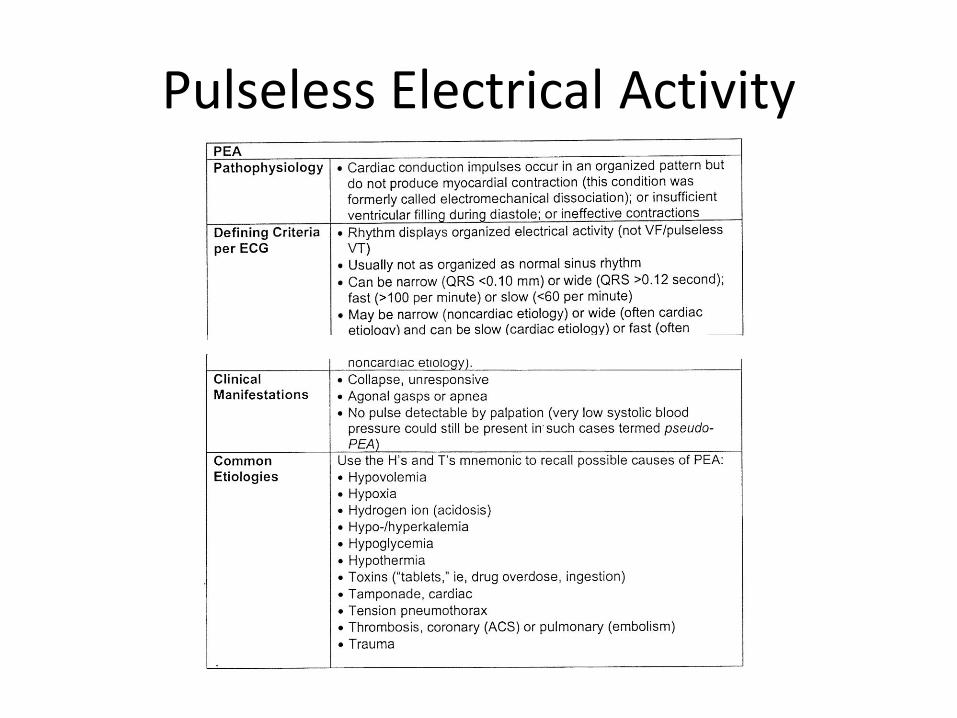
Pulseless Electrical Activity


Mx – Pulseless arrest

Shockable rhythm Mx?


Pulseless Arrest Treatment Sequences (VF & Pulseless VT)

07-Dec-12

Non shockable rhythm Mx?

Pulseless Arrest Treatment Sequences (PEA & Asystole)

DEFIBRILLATION
• Does not restart the heart.
• It stunts the heart and briefly terminates all electrical activities include VF and VT.
• Defibrillators:
– Manual biphasic- 200 J
– Manual monophasic- 360 J
• After delivering shock, resume CPR immediately

Importance of early defibrillation

Defibrillation

AED
• Automated External Defibrillator
• computerized medical device which can check a person’s heart rhythm.
• It can recognize a rhythm that requires a shock.
• It can advise the rescuer when a shock is needed.
• The AED uses voice prompts, lights and text messages to tell the rescuer the steps to take.

AED

REVERSIBLE CAUSES
• 5Hs
• 5Ts

REVERSIBLE CAUSES
• Hypothermia
• Hypokalaemia/hyperkalaemia
• H ion (acidosis)
• Hypotension
• Hypoxia
• Tension pneumothorax
• Tamponade, cardiac
• Thrombosis, cardiac/pulmonary
• Trauma
• Toxin

BRADYARRHYTHMIA
WITH PULSE

• Rhythm with heart rate <60 bpm
• The key clinical questions are: – Are there “serious” sign or symptoms?
– Are the signs and symptoms related to slow heart rate?
• Look for S/S of bradycardia (indicates poor perfusion) – Symptoms- chest pain, shortness of breath, reduced
consciousness, weakness, dizziness and presyncope or syncope.
– Signs- hypotension, CCF
BRADYCARDIA

How to recognize Atrioventricular (AV) Block?


46

2nd Degree AV Block
• Type 1 (Mobitz l - Wenckebach)
• Type 2 (Mobitz ll)


49


51


53

Junctional bradycardia

Sinus arrest

Mx - bradycardia



07-Dec-12

Transcutaneous Pacing (TCP)
• Treatment of choice in symptomatic bradycardia with signs of poor perfusion.
• TCP delivers pacing impulses to the heart through the skin by using cutaneous electrodes.
• Conscious patient require analgesia for discomfort unless delay for sedation will cause / contribute to deterioration

Transcutaneous Pacing (TCP) Technique:
Step Action
1 Place pacing electrodes on the chest per package
instruction.
2 Turn the pacer on.
3
Set the demand rate to approx. 60/min. this rate can be
adjusted up or down (based on ptn’s clinical response)
once pacing is established.
4
Set the current milliamperes (mA) output 2 mA above the
dose at which consistent capture is observed (safety
margin).

TACHYARRHYTHMIA
WITH PULSE

TACHYCARDIA
• Rhythm with heart rate >100 bpm.
• Has many potential causes
• May be symptomatic or asymptomatic
• The key of management is to determine whether pulses are present or not.
• If pulses are present, determine whether the patient is stable or unstable.




67



70





Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
The “Re-Entry” Mechanism of Ectopic Beats & Rhythms
Electrical Impulse
Cardiac
Conduction
Tissue
Tissues with these type of circuits may exist:
• in microscopic size in the SA node, AV node, or any type of heart tissue
• in a “macroscopic” structure such as an accessory pathway in WPW

Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
Premature Beat Impulse
Cardiac
Conduction
Tissue
1. An arrhythmia is triggered by a premature beat
2. The beat cannot gain entry into the fast conducting
pathway because of its long refractory period and
therefore travels down the slow conducting pathway
only
Repolarizing Tissue
(long refractory period)
The “Re-Entry” Mechanism of Ectopic Beats & Rhythms

3. The wave of excitation from the premature beat
arrives at the distal end of the fast conducting
pathway, which has now recovered and therefore
travels retrogradely (backwards) up the fast pathway
Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
Cardiac
Conduction
Tissue
The “Re-Entry” Mechanism of Ectopic Beats & Rhythms

4. On arriving at the top of the fast pathway it finds the
slow pathway has recovered and therefore the wave of
excitation ‘re-enters’ the pathway and continues in a
‘circular’ movement. This creates the re-entry circuit
Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
Cardiac
Conduction
Tissue
The “Re-Entry” Mechanism of Ectopic Beats & Rhythms

Atrial Re-entry
• atrial tachycardia
• atrial fibrillation
• atrial flutter
Atrio-Ventricular Re-entry
• Wolf Parkinson White
• supraventricular tachycardia
Ventricular Re-entry
• ventricular tachycardia
Atrio-Ventricular Nodal Re-entry
• supraventricular tachycardia
Re-entry Circuits as Ectopic Foci and Arrhythmia Generators

How to recognize Tachyarrhythmias?
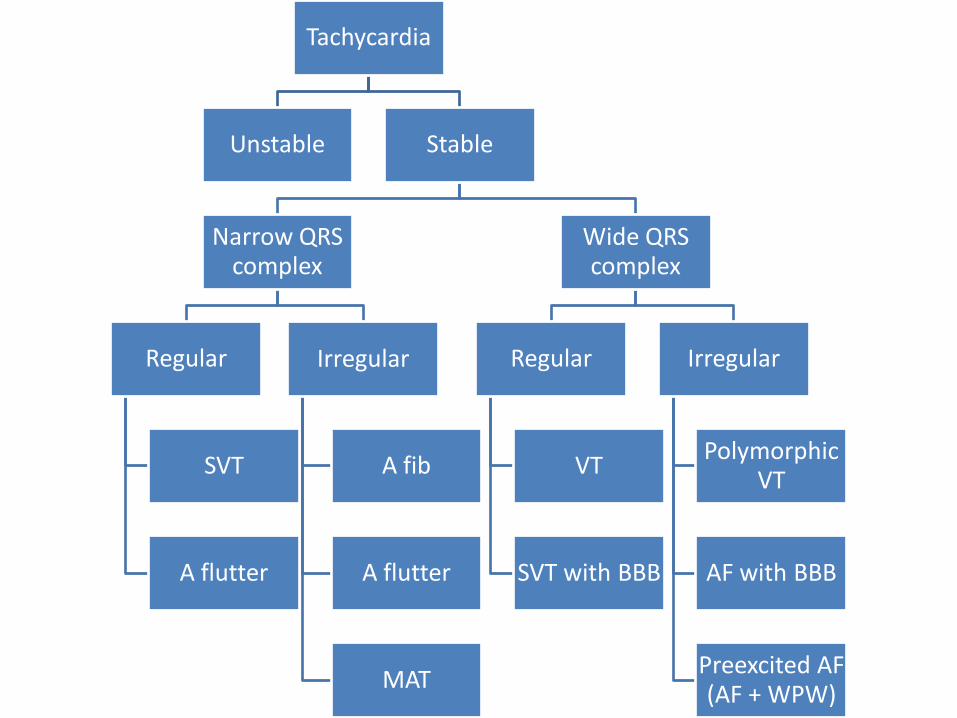
Tachycardia
Unstable Stable
Narrow QRS complex
Regular
SVT
A flutter
Irregular
A fib
A flutter
MAT
Wide QRS complex
Regular
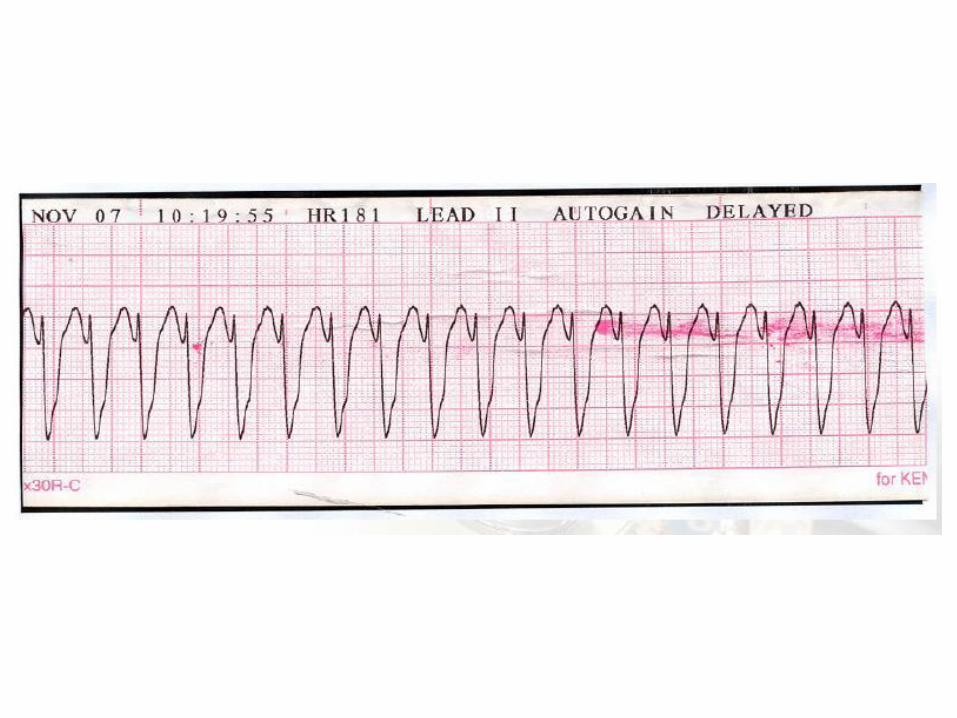
VT
SVT with BBB
Irregular
Polymorphic VT
AF with BBB
Preexcited AF (AF + WPW)






ATRIAL TACHYCARDIA
• Abnormal P waves morphology
• Atrial rates 100-250 beats/min
• Ventricular rhythm usually regular
• Variable ventricular rate




Mx - tachycardia

Tachycardia with pulse
Unstable Stable

Perform immediate synchronized cardioversion in Unstable
Tachycardia patients…

Unsynchronized vs Synchronized Shocks
• Unsynchronized shock
– Electrical shock delivered as soon ‘SHOCK’ button is pushed
– Shock may fall randomly anywhere within cardiac cycle
– Should use higher energy level than synchronized cardioversion
– When to use?
• Pulseless arrest

Unsynchronized vs Synchronized Shocks
• Synchronized cardioversion – Deliver shock at the peak of QRS complex (highest
point of R wave)
– Deliver lower energy than defibrillation
– Can avoid delivery of shock during cardiac repolarization (T wave) which can precipitate VF.
– Remember: low-energy shock should always be delivered as synchronized shock to avoid precipitating VF



MEDICATIONS

ADRENALINE
• Catecholamines • Actions:
– Increases contractile force of the heart (increase cardiac output)
– Increases conduction of SA node, AV node and ventricle (increase HR)
– Increases systemic vascular resistance through periphjeral vasoconstriction (increase perfusion pressure)
• Indications: – Cardiac arrest: 1mg every 3-
5minutes
– Symptomatic bradycardia: infusion at 2-10mcg/min
• Adverse effects: – Hypertension after resuscitation
– Ventricular irritability -tachyarrhythmias
– Tissue necrosis if extravasation
– Increase myocardial O2 demand – risk of ischaemia and MI, CVA

ATROPINE
• Anticholinergic agent (parasympatholytic)
• Antagonise parasymphatetic neurotransmitter acetylcholine at muscarinic receptors
• Blocks effect of vagus nerve on both SA and AV nodes increasing sinus automaticity and facilitating AV node conduction
• Indications: – Symptomatic bradycardia:
0.5mg every 3-5minutes up to max 3mg
• Side effects: – Tachycardia
– Palpitations
– Paradoxical bradycardia (if dose < 0.5mg)
– Hypertension (rare)

DOPAMINE
• Chemical precursor of noradrenaline that stimulates both alpha and beta adrenergic receptors – Causes peripheral
vasonstriction (BP)
– Increases myocardial contractility (CO)
• Indications: – 2nd line for symptomatic
bradycardia: 2-20mcg/kg/min
• Side effects: – Tachycardia
– Tachyarrhythmias
– Excessive peripheral vasoconstriction (higher dose)

ADENOSINE
• Purine nucleotide
• Slows transmission across AV node but little effect on others
• Highly effective in terminating paroxysmal SVT
• Short acting - half life: 5s
• Indications: – SVT: 6 + 12 + 12mg
• How to administer?
• Side effects: – Transient bradycardia,
asystole
– Hypotension
– Chest pain
– Dyspnoea
– Bronchospasm (caution in asthma)
– Transient flushing

AMIODARONE
• Antiarrhyhthmic
• Acts on Na, K, Ca channels
• Poses alpha and beta adrenergic blocking properties
• Adverse effects: – Hypotension, bradycardia,
heart block
• Indications: – Refractory VF/pulseless VT:
300mg IV bolus, 2nd dose 150mg
– Unstable tachyarrhythmias: 300mg IV over 10-20mins after failed cardioversion x3
– Stable tachycarrhythmias: 300mg IV over 20-60mins
– Maintenance infusion: 900mg IV over 24hrs

LIGNOCAINE
• Ca channel blocker
• Actions: – Raises fibrillatory threshold –
enhances effect of DC shock
– Suppresses automaticity and shortens effective refractory period and action potential duration – slows down HR
– Inhibits reentry mechanism – halts arrhythmias
• Indications: – Refractory VF/pulseless VT: 1-
1.5mg/kg IV, additional dose 0.5-0.75mg/kg. repeat 5-10mins up to 3mg/kg
• Side effects/precautions: – Can cause slurred speech,
altered consciousness, muscle twitching, seizure
– Hypotension, bradycardia, HB, asystole
– Widening of QRS complexes

MAGNESIUM
• Important in maintaining membrane stability
• Low Mg may cause myocardial hyperexcitability
• Indications:
– Cardiac arrest due to torsade de pointes: 1-2g IV bolus
– Stable torsade de pointes/hypomagnesaemia: loading 1-2g in 50cc D5% over 5-60mins, followed with 0.5 – 1g/hr infusion

ECG QUIZ





















Thank you