aristolochic acid nephropathy: from bed to benchside
TRANSCRIPT

Aristolochic acid nephropathy: frombed to benchside
F. Debelle, JL. Vanherweghem, J. Nortier
Erasme university hospital Experimental nephrology unitUniversité Libre de Bruxelles
Revisiting AAN…

Revisiting AAN…
1. The Belgian outbreak of « Chinese-herb nephropathy »
2. A worldwide problem
3. Clinical and experimental toxicityof AA
4. Perspectives of research

July 92June 92April 92Dialysis
Creat. 3.0*Renal biopsy**
Creat. 3.8*Renal Biopsy**
Creat. 3.7*Renal Biopsy**
Jan 92
March 92
Creat. 0.8*Creat. 1.1*1989May 90March 91Nov 91
Case n°3Case n°2Case n°1
Exposure to Chinese herbs * mg/dl** Renal biopsy: interstitial fibrosis
1. « Chinese-herb nephropathy »

Vanherweghem JL et al.
Rapidly progressive interstitial renal fibrosis in young women: association with slimming regimenincluding Chinese herbs
Lancet (1993) 341:387-91
Courtesy Dr Baleriaux


«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)

«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)

«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)

«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)
Aristolochic acid I + II(R=OCH3 / H)

«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)
Aristolochic acid I + II(R=OCH3 / H)

«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)
Aristolochic acid I + II(R=OCH3 / H)
Aristolochia fangchi

«Stephania Tetrandra»
Han Fang-Ji
Vanhaelen et al. Lancet (1994)
Aristolochic acid I + II(R=OCH3 / H)
Aristolochia fangchi
Guang Fang-Ji

Potential toxicity of herbal and plant products
Huxtable RJ. Drug Safety (1990)
Potential toxicity of herbal and plant products
Huxtable RJ. Drug Safety (1990)
1. Correct identification … but unknown orunderestimated toxicity
Potential toxicity of herbal and plant products
Huxtable RJ. Drug Safety (1990)
1. Correct identification … but unknown orunderestimated toxicity
2. Accidental contamination or deliberately modified composition

Potential toxicity of herbal and plant products
Huxtable RJ. Drug Safety (1990)
1. Correct identification … but unknown orunderestimated toxicity
2. Accidental contamination or deliberately modified composition
3. Misidentification of the plant or substitution by another more toxic compound

Muniz Martinez et al. Nephrol Dial Transplant (2002)

End-stage CHN: evolution of renal replacement therapies
A nnées de su iv i1 9 9 0 1 9 9 2 1 9 9 4 1 9 9 6 1 9 9 8 2 0 0 0 2 0 0 2 2 0 0 4 2 0 0 6
Pat
ient
s A
AN
en
IRT
0
10
20
30
40
50 D ia lys ésT ra n sp la n té sD é c é d é sN b c u m u la tif d e p a tie n ts
Follow-up (years)

Autoradiogram of specific AA-relatedDNA adducts in renal tissue
Schmeiser HH, Arlt VM. Cancer Res (1996)
Arlt VM. Mutagenesis (2002)

Autoradiogram of specific AA-relatedDNA adducts in renal tissue
Schmeiser HH, Arlt VM. Cancer Res (1996)
Arlt VM. Mutagenesis (2002)
AA biotransformation (cytochrome P450)

Revisiting AAN…

Revisiting AAN…
1. The Belgian outbreak of « Chinese-herb nephropathy »
2. A worldwide problem3. Clinical and experimental
nephrotoxicity of AA
4. Perspectives of research

The Chenonceaucastle
The green cabinet, Catherine de Médicis’s study

The Brussels
« Aristolochia Tapestry »
(15th century)

Complementary and Alternative Medical (CAM) Therapies
AcupunctureRelaxation techniquesMassageReflexology…
Folk remediesHerbal medicines
= alternative to or complementary to « Western » conventional medicine

The escalating use of alternative therapies
very popular: 47 % of the adult US population (1997), expenditure over $ 21 billion, < 40% disclosed to physicians,
79% of patients perceived the combination to be superior to either one alone
« natural » plant origin safe !!!
traditional medicines: equal official status with Western medicine (Africa, Asia)
dietary supplements (not regulated by the FDA) easy available, over-the-counter, low cost
Eisenberg DM et al. NEJM 1993; JAMA 1998; Arch Int Med 2001

A pharmacy of traditional herbal medicine (Hangzhou, China)
Courtesy Dr F. Debelle
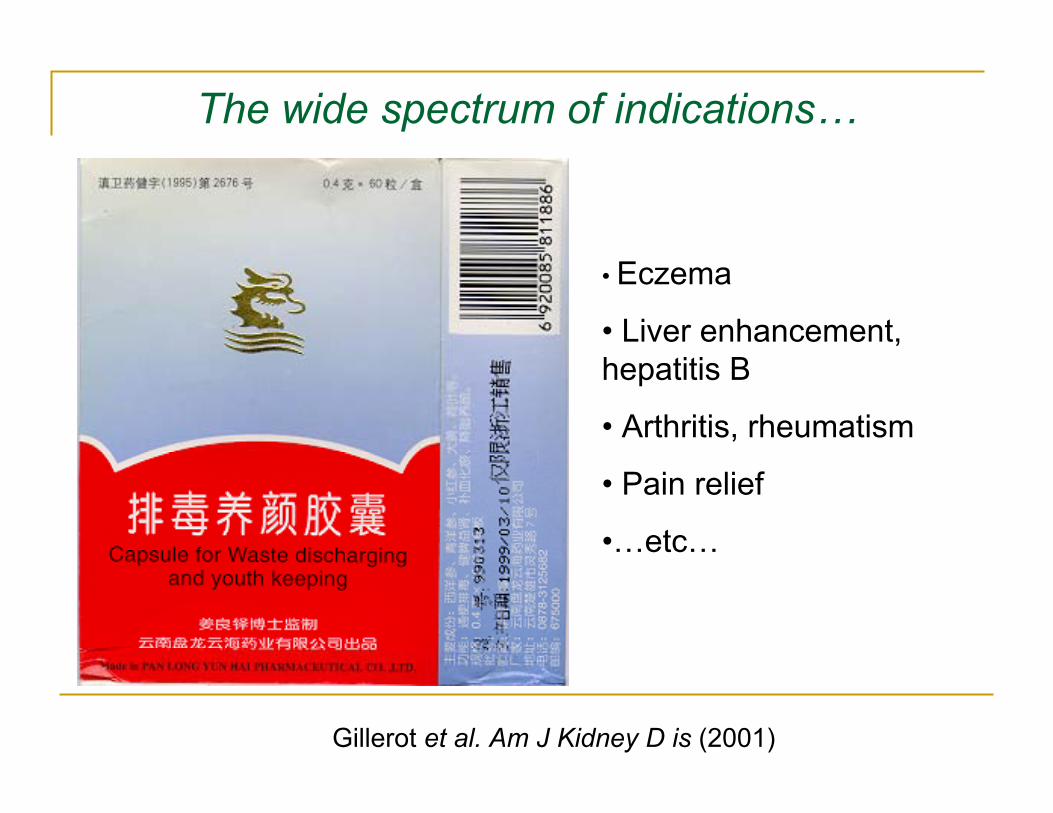
The wide spectrum of indications…
Gillerot et al. Am J Kidney D is (2001)
• Eczema
• Liver enhancement, hepatitis B
• Arthritis, rheumatism
• Pain relief
•…etc…

Aristolochia manshuriensisAristolochia fangchi
Guang Fang-Ji Guan Mutong

FDA recommendations (2001)
Carcinogenicity to humans recognized by the International Agency for Research on Cancer (2002) and the National Toxicology Program (2008)

…
…
…
Gold LS, Slone TH. N Engl J Med (2003)
1 http://www.cfsan.fda.gov/~dms/ds-bot.html

AAN cases around the world
Debelle et al Kidney Int. (2008)
Aristolochia clematitis

Courtesy of Dr B. Jelakovic

The two faces of Janus ?
Chinese herb nephropathy(1992)
SimilaritiesSimilarities
SimilaritiesSimilarities
Renal interstitial fibrosis andurothelial carcinoma
Renal interstitial fibrosis andurothelial carcinoma
Renal interstitial fibrosis, urothelial carcinoma and AA-
related DNA adducts
Renal interstitial fibrosis, urothelial carcinoma and AA-
related DNA adducts
Aristolochic acidspecific DNA
adducts
Aristolochic acidspecific DNA
adducts
Aristolochic acid nephropathy (1996 - )
Aristolochic acid –Balkan endemic nephropathy
(2007 - )
Balkan endemic nephropathy(1956)

Revisiting AAN…

Revisiting AAN…
1. The Belgian outbreak of « Chinese-herb nephropathy »
2. A worldwide problem
3. Clinical and experimental nephrotoxicity of AA
4. Perspectives of research

Clinical presentation of AAN
Depierreux et al. Am J Kidney Dis 1994
Cosyns et al. Kidney Int 1994

The proximal tubule = target of AA
Markers of structural and functional injury:-- brush border enzymuria
-- microproteinuria
Nortier et al. Kidney Int (1997)

Lebeau C et al. Kidney Int (2001)
Control
10 µmol AA
20 µmol AA
20 µmol AA+ 24h recovery
Control
10 µmol AA20 µmol AA
20 µmol AA+ 24h recovery
ControlControl
ControlControl
15 µM CdCl15 µM CdCl22
15 µM CdCl15 µM CdCl22
0.1% DMSO0.1% DMSO 20 µM AA20 µM AA
0.1% DMSO0.1% DMSO 20 µM AA20 µM AA
Aristolochic acid impedes endocytosis and induces DNA adducts in proximal tubule cells

AA-associated urothelial malignancies
Cosyns et al. Am J Kidney Dis (1999) Nortier et al. N Engl J Med (2000)
Right ureteral tumorRight ureteral tumor

Ureteronephrectomies / AAN patients
2249Total
N Engl J Med 2000; 342: 1686
1839ULB
Am J Kidney Dis 1999; 33: 1011
410UCL
ReferenceN. urothelialcarcinoma
N. patientsCenter
Prevalence +/- 40% !

Alive with no evidence of diseaseLow grade pTa-1
Sudden deathLow grade pTa-1
Dead in generalizationPT3N1-1
Alive with no evidence of disease-pTis5
Alive with no evidence of diseaseHigh grade pTapTis + pTa1
Alive with no evidence of diseaseLow grade pTapTis2
Dead from hepatocarcinomaLow grade pTapTis1
Alive with no evidence of diseaseHigh grade pTa + pTis
pTa1
Alive with no evidence of diseasepTispTis3
Alive with no evidence of diseaseHigh grade pT1pTis1
Alive with no evidence of diseasepTisT11
Dead in generalizationpTisT21
Dead in generalizationHigh grade pT1T31
OutcomeBladderPelvis and/or Ureter
Number of patients

Experimental AAN

Experimental AAN
Chronic AA toxicity in rabbits: A model of Chinese herbsnephropathy?
Cosyns JP et al. Kidney Int (2001)

Experimental AAN
Chronic AA toxicity in rabbits: A model of Chinese herbsnephropathy?
Cosyns JP et al. Kidney Int (2001)
Aristolochic acids induce chronicrenal failure with interstitial fibrosis in salt-depleted rats
Debelle FD et al. JASN (2002)

Experimental AAN
Chronic AA toxicity in rabbits: A model of Chinese herbsnephropathy?
Cosyns JP et al. Kidney Int (2001)
Aristolochic acids induce chronicrenal failure with interstitial fibrosis in salt-depleted rats
Debelle FD et al. JASN (2002)
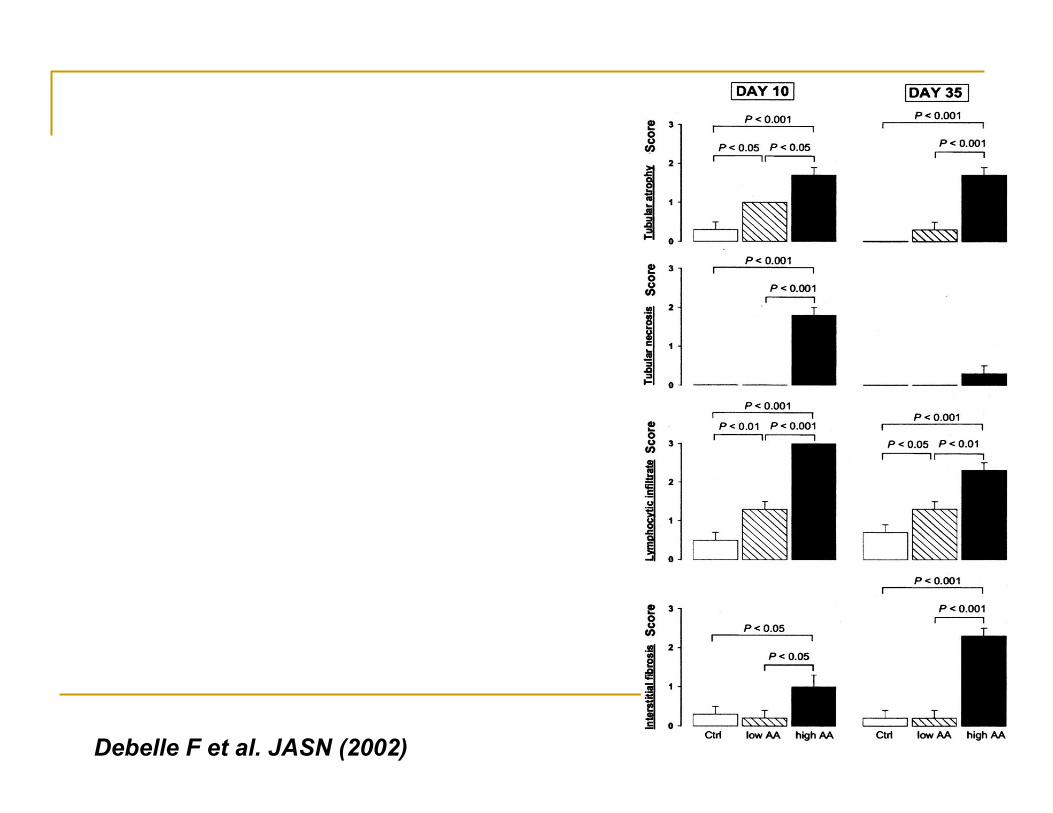
Debelle F et al. JASN (2002)

Debelle F et al. JASN (2002)

Debelle F et al. JASN (2002)
CONTROL

Debelle F et al. JASN (2002)
CONTROL
AA 10 mg/kg

Debelle F et al. JASN (2002)
CONTROL
AA 10 mg/kg Day 35

Debelle F et al. JASN (2002)
CONTROL
AA 10 mg/kg Day 35AA 10 mg/kg Day 35
« The severity of the tubulointerstitial damage determines the functional prognosis »
Schainuck et al. Hum Pathol (1970)
« The severity of the tubulointerstitial damage determines the functional prognosis »
Schainuck et al. Hum Pathol (1970)
« The severity ofdetermines the f
Schainuck

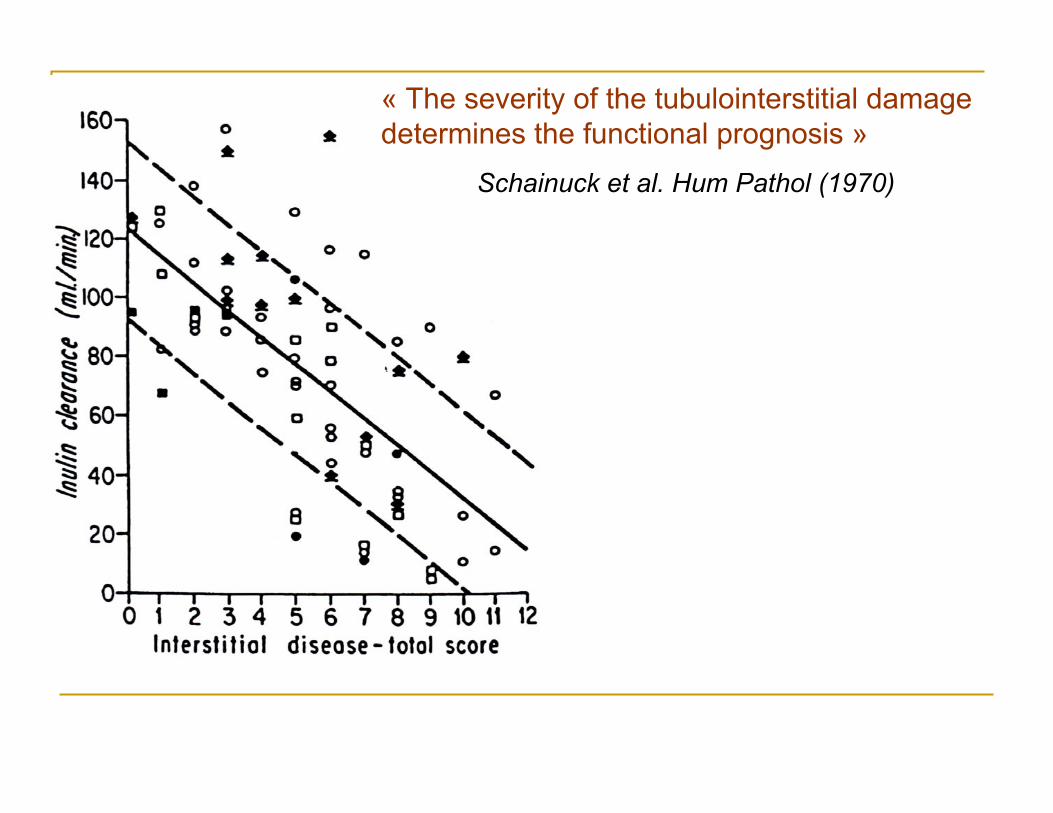
« The severity of the tubulointerstitial damage determines the functional prognosis »
Schainuck et al. Hum Pathol (1970)
« The severity ofdetermines the f
Schainuck
« Injury and matrix remodellingpredict progression »
Halloran P. Necker Seminars (2009)

« The severity of the tubulointerstitial damage determines the functional prognosis »
Schainuck et al. Hum Pathol (1970)
« The severity ofdetermines the f
Schainuck
« Injury and matrix remodellingpredict progression »
Halloran P. Necker Seminars (2009)

« The severity of the tubulointerstitial damage determines the functional prognosis »
Schainuck et al. Hum Pathol (1970)
« The severity ofdetermines the f
Schainuck
« Injury and matrix remodellingpredict progression »
Halloran P. Necker Seminars (2009)
Early events promotingfibrosis ?

AA group (10 mg of AA/ kg of bw, sc)
Control group (AA vehicle, sc)
1 2 3 4 5 7 10 14 18 35
Acute phase Chronic phase
Acclimatization
Days of sacrifice
Experimental design
Pozdzik A et al. Kidney Int (2008) Lebeau et al. Nephrol Dial Transplant (2005)

Tubulointerstitial lesions
AA rats: Day 35
X200
X200
*
Control: Day 35
X40
X40 X40
X200 X200
AA rats: Day 5Control: Day 5

Semiquantitative score of tubulointerstitial injury
Phases: Acute Chronic
*p<0.05, **p<0.01, ***p<0.005 AA vs control group
Acute Chronic

Control: Day 3 AA rat: Day 3
x400
x400
AA rat: Day 35
PTEC proliferation Ki-67 immunostaining
Time (days)1 2 3 4 5 7 10 14 18 35
Ki-6
7+ tu
bula
r nuc
lei /
fiel
d
0
10
20
30
40ControlsAA rats
***
***
***
*
***
***
***
*** ***
Phases: Acute Chronic
*p<0.05, **p<0.01, ***p<0.005 AA vs control group
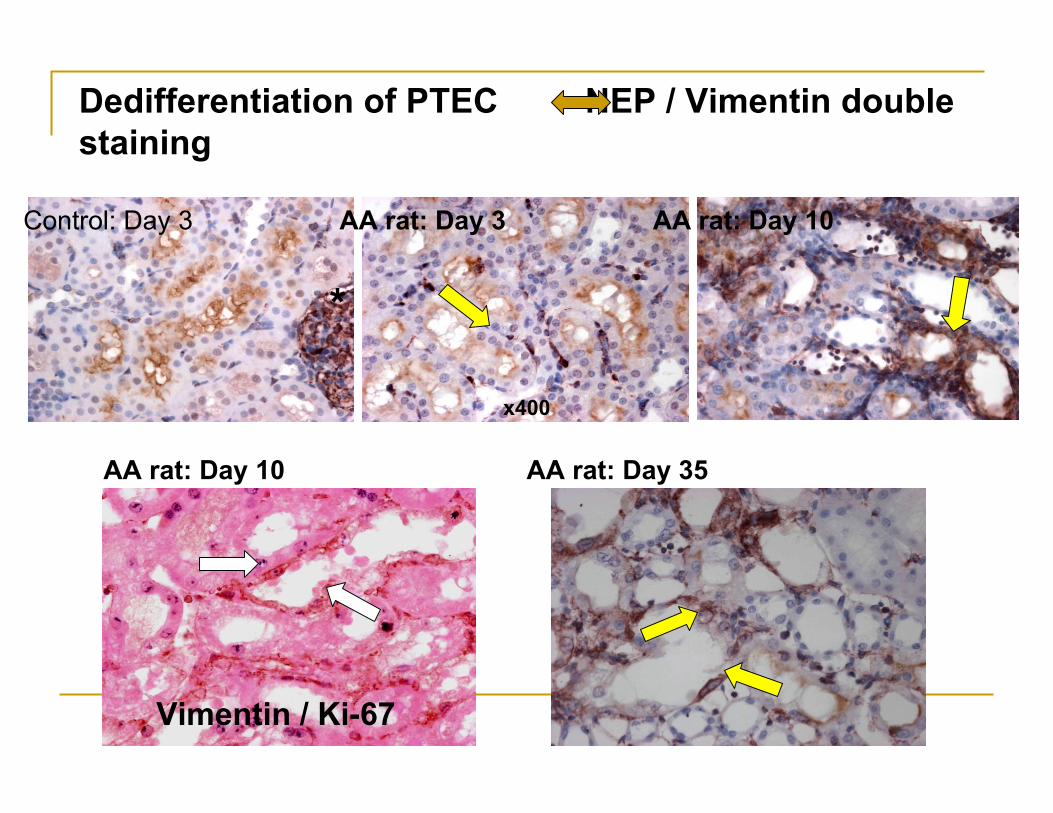
Dedifferentiation of PTEC NEP / Vimentin double staining
*
Control: Day 3 AA rat: Day 3 AA rat: Day 10
x400
x400
AA rat: Day 10 AA rat: Day 35
Vimentin / Ki-67

Key events of epithelial to mesenchymal transition (EMT)
Zvaifler . Arthritis Research & Therapy 2006
TGF-β alone is capable of inducing epithelial cells to undergo all four steps

Tubular basement membrane integrity Jones stainingControl: Day 2 AA rat: Day 2
x400
x400
AA rat: Day 5
Time (days)1 2 3 4 5 10 35
Base
men
t mem
bran
e de
nuda
tion
scor
e
0
1
2
3 ControlsAA rats
*******Phases: Acute Chronic
*p<0.05, **p<0.01, ***p<0.005 AA vs control group

X 200
Myofibroblast phenotype: α-SMA immunostaining
Control: Day 35 AA rat: Day 35
X 400
A. Pozdzik et al. Kidney Int (2008)

X 200
Myofibroblast phenotype: α-SMA immunostaining
Control: Day 35 AA rat: Day 35
X 400
A. Pozdzik et al. Kidney Int (2008)

X 200
Myofibroblast phenotype: α-SMA immunostaining
Control: Day 35 AA rat: Day 35
X 400
A. Pozdzik et al. Kidney Int (2008)
Activation of resident fibroblasts peritubular fibrosis

Renal tissue expression of TGF-βControl: Day 3 AA rat: Day 3
X400
X400
AA rat: Day 10 AA rat: Day 35

Urinary excretion rate of proinflammatory and profibrosing cytokines
Variables Day 10 Day 35
(ng/mmol Cr) Controls AA rats Controls AA rats
IL-1α 8.35 (4.65-9.26)
47.9 b
(23.7-126)8.31
(5.76-17.0)45.7 b
(41.3-87.2)
TNF-α 0.19 (0.00-0.38)
0.00 (0.00-12.4)
0.00(0.00-0.05)
0.28 a
(0.00-1.05)
IFN-γ 0.08 (0.08-1.01)
0.23(0.00-2.19)
0.00 (0.00-0.28)
0.96 a
(0.07-1.54)
MCP-1 119(84.2-145)
219 b
(148-482)74.7
(36.7-110)286 b
(230-490)
IL-4 3.56(0.00-6.00)
9.3(0.00-16.2)
3.31(0.00-3.52)
13.1 b
(3.80-20.7)
Active TGF-β 0.81(0.00-1.91)
56.1 b
(3.20-156)2.20
(1.52-8.41)31.1 b
(9.77-135)
a P < 0.05, b P < 0.005. Pozdzik et al. Nephrol Dial Transplant 2008


Distribution of the monocyte/macrophage infiltrate Semiquantitative score

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrate

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDi

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q
Outer stripe of outer medulla (OSOM)

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q
Outer stripe of outer medulla (OSOM)
Inner stripe of outer medulla (ISOM)

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q
Outer stripe of outer medulla (OSOM)
Inner stripe of outer medulla (ISOM)
ED
-1 im
mun
omar
quag
e(a
mas
/ cha
mp)
0
5
1 0
1 5
2 0
2 5T é m o in sR a ts A A* *
* *
* *
* * * ** *
* *
*
Cortex
Distribution of the monoSemiquan

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q
Outer stripe of outer medulla (OSOM)
Inner stripe of outer medulla (ISOM)
ED
-1 im
mun
omar
quag
e(a
mas
/ cha
mp)
0
5
1 0
1 5
2 0
2 5T é m o in sR a ts A A* *
* *
* *
* * * ** *
* *
*
Cortex
Distribution of the monoSemiquan
*p<0.05, **p<0.01, AA vs controls. N = 6 rats/group

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q
Outer stripe of outer medulla (OSOM)
Inner stripe of outer medulla (ISOM)
ED
-1 im
mun
omar
quag
e(a
mas
/ cha
mp)
0
5
1 0
1 5
2 0
2 5T é m o in sR a ts A A* *
* *
* *
* * * ** *
* *
*
Cortex
Distribution of the monoSemiquan
*p<0.05, **p<0.01, AA vs controls. N = 6 rats/group
ED
-1 im
mun
omar
quag
e (a
mas
/ cha
mp)
0
5
1 0
1 5
2 0
2 5
* * * ** *
* *
* *
* ** *
*
Outer stripe of outer medulla (OSOM)

Distribution of the monocyte/macrophage infiltrate Semiquantitative scoreSemiquantitative score
Phases: Aiguë Chronique Distribution of the monocyte/macrophage infiltrateDistribution of the mono
Cortex q
Outer stripe of outer medulla (OSOM)
Inner stripe of outer medulla (ISOM)
ED
-1 im
mun
omar
quag
e(a
mas
/ cha
mp)
0
5
1 0
1 5
2 0
2 5T é m o in sR a ts A A* *
* *
* *
* * * ** *
* *
*
Cortex
Distribution of the monoSemiquan
*p<0.05, **p<0.01, AA vs controls. N = 6 rats/group
ED
-1 im
mun
omar
quag
e (a
mas
/ cha
mp)
0
5
1 0
1 5
2 0
2 5
* * * ** *
* *
* *
* ** *
*
Outer stripe of outer medulla (OSOM)
T e m p s ( jo u r s )1 2 3 4 5 7 1 0 1 4 1 8 3 5
ED
-1 im
mun
mar
quag
e(a
mas
/ cha
mp)
0
1
2
3
4
5
* **
*
Inner stripe of outer medulla (ISOM)

Interstitial T lymphocytesAnti-CD3 Anti-CD20
Control AA Control AA
X400
Anti-CD45RC Anti-CD8Control AA Control AA

Revisiting AAN…

Revisiting AAN…
1. The Belgian outbreak of « Chinese-herb nephropathy »
2. A worldwide problem
3. Clinical and experimental nephrotoxicity of AA
4. Perspectives of research

Translational nephrology is ongoing !

Translational nephrology is ongoing !
Physiopathological mechanisms of renal fibrosis, including the potential role of immunocompetentcells

Translational nephrology is ongoing !
Physiopathological mechanisms of renal fibrosis, including the potential role of immunocompetentcells
• Therapeutic strategies to reduce the onset
and/or progression of fibrosis

Translational nephrology is ongoing !
Physiopathological mechanisms of renal fibrosis, including the potential role of immunocompetentcells
• Therapeutic strategies to reduce the onset
and/or progression of fibrosis

Translational nephrology is ongoing !
Physiopathological mechanisms of renal fibrosis, including the potential role of immunocompetentcells
• Therapeutic strategies to reduce the onset
and/or progression of fibrosis
From bench to bedside…

Thank you to…
Nephrology,Pathology andUrology depts, Erasme university hospital, ULBExperimental nephrology unit, ULBInstitute of Pharmacy, ULBInserm U785, Paul BrousseGerman Cancer Institute, Heidelberg, GermanyMolecular Toxicology Unit, Sutton, UKNephrology dept, AZ-VUB