are we doing harm to our patients? - home | rgpeo ... pa… · strength and balance exercises so...
TRANSCRIPT

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Dawn Skelton Professor of Ageing and Health
Institute of Applied Health Research
School of Health & Life Sciences
Are we doing harm to our
patients? Importance of motivation, support and consistent messages for falls
prevention Part 1

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Presentation Aims
• Effective falls prevention
interventions and potential harm if
fidelity not followed
• Importance of falls per unit of
activity
• Sedentary behaviour and
frailty/sarcopenia
• Hospital acquired immobility vs risk
of falls?
• Consistent messages to change
behaviour from the whole team!
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
”Just like the Olympic athlete,
the elderly person must
perform, frequently and
consistently, at the very limit
of their physical ability. The
85-year-old can therefore
benefit from the study of
athletic training methods...”
(Professor Archie Young, 1997)

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Wide range of abilities and needs

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Fear of Falling
• Fear and lack of confidence in balance predict – Deterioration in physical functioning – Decreases in physical activity, indoor and
outdoor – Increase in fractures – Admission to Institutional Care
(Arfken 1994, Vellas 1997, Cumming 2000, Horne 2011)
“It’s the fear that restricts me. In my mind I know that I can’t [walk outside]. The fear of falling and not having the strength to go out, that stops me from going out…” (Female, 60yrs)
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
What makes the difference?
• Greatest effects of exercise on fall rates
(38% reduction) from interventions
including:
– Highly challenging balance training
– High dose (50+ hours)
– Progressive strength training
– No walking program
• These types of exercise also reduce fear of
falling
Sherrington et al., JAGS 2008, NSWPHB 2011
Kendrick Cochrane Review FoF 2014
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Secondary falls prevention exercise
• Otago Home Exercise Programme (OEP)
– 1 yr; 3 x p/w; 6 home visits and telephone
support
– 6 mths; 3 x p/w (1 p/w group, 2 p/w home)
exercise instructor
– Effects on strength and balance more pronounced
when run in a group
• Falls Management Exercise Programme
(FaME/PSI)
– 9 mths; 3 x p/w (one group, two home); includes
floorwork;
– Increases habitual physical activity as well
Falls Injuries
Cost effective >80s Cost neutral >65s
Cognitive Function
Falls Quality of Life
Bone Mineral Density Change of residence
Coping strategies Long lies
41% of falls services in
the UK employ a
trained OEP Leader
54% of falls services in
the UK employ a
trained PSI (RCP Audit
2012)
(Campbell 1997; Robertson 2001; Campbell 2005; Liu_Ambrose 2008; Kyrdalen 2014; Skelton 2005, 2008)
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
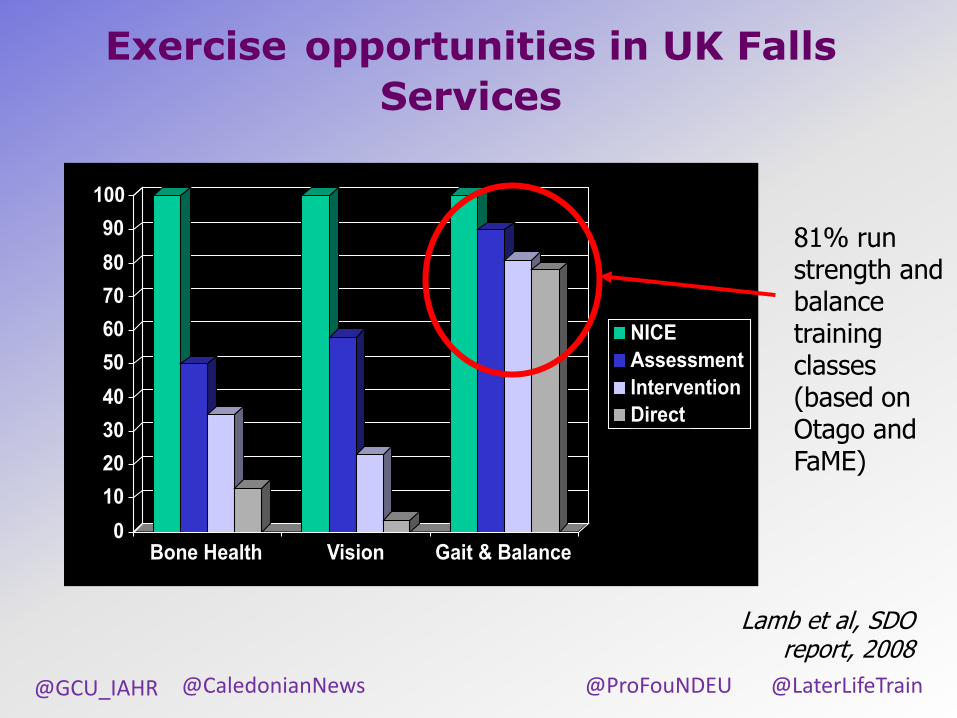
Exercise opportunities in UK Falls
Services
0
10
20
30
40
50
60
70
80
90
100
Bone Health Vision Gait & Balance
NICE
Assessment
Intervention
Direct
81% run strength and balance training classes (based on Otago and FaME)
Lamb et al, SDO report, 2008
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Lack of fidelity….
• More than half the class seated
• Average duration 8 weeks and frequency once per week! = 8 hours!
• Little strength progression
– Ankle weights often not increased
– Max 2 therabands progression
Highly challenging balance?
Ineffective dose ?
Lack of strength
progression ?
No services record falls as outcomes, only strength and balance – all showed improvements BUT….
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Question to you….
• Please all stand up…
• Sit down if you are NOT involved in delivery or referral to exercise to prevent falls….
• Does the exercise intervention really progress strength training and challenge balance (most of session in standing)? Sit down if not….
• Sit down if the exercise intervention is less than 50 hours in length
OH DEAR
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Risks if duration too short ?
FaME showed a significant reduction
in falls after 9 months (RR 0.53) in
those with a history of 3 or more
falls in last year (frail)
BUT DURING INTERVENTION
• Exercisers slightly increased risk
of falls compared to controls
(RR 1.19)
• although less likely to have injurious
fall (RR 0.51)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Intervention Follow-up
Re
lati
ve
Ris
k
Increased confidence, strength and balance - but not yet ready to
integrate it all into ability to prevent a trip?

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Challenges?
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Transitioning onto other exercise
opportunities
• Vital
– to meet effective dose requirements (>50 hours)
• Important
– to encourage an active lifestyle beyond rehabilitation
– to ensure a change in exercise habits and continue to improve social involvement
– to ensure the opportunities continue to improve strength and balance (eg. not seated!)
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
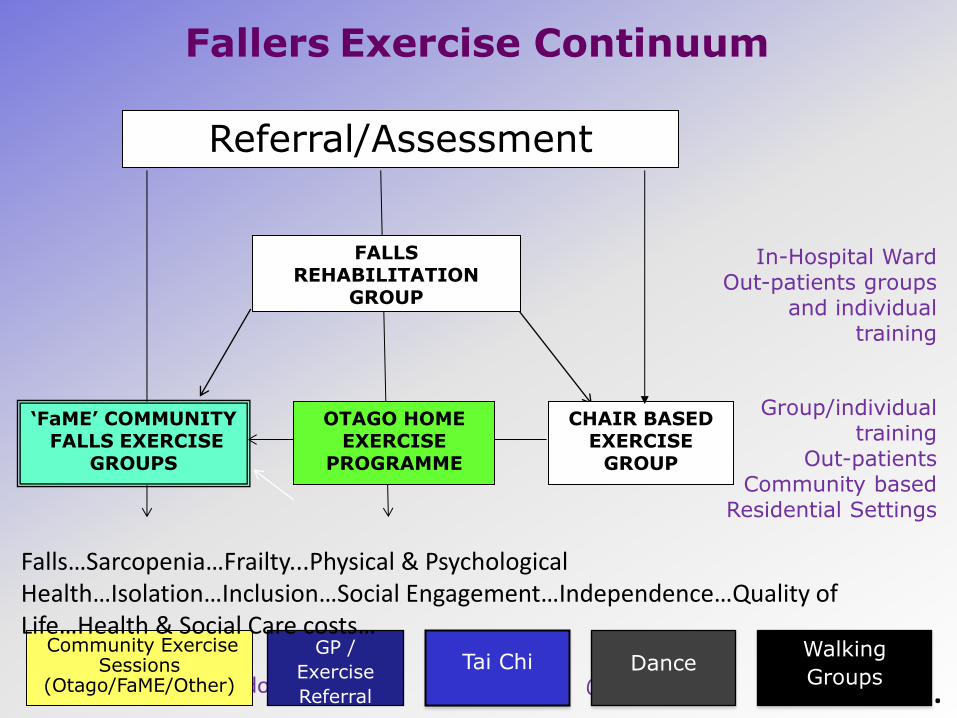
Fallers Exercise Continuum
CHAIR BASED EXERCISE
GROUP
Referral/Assessment
Community Exercise Sessions
(Otago/FaME/Other)
OTAGO HOME EXERCISE
PROGRAMME
FALLS REHABILITATION
GROUP
‘FaME’ COMMUNITY FALLS EXERCISE
GROUPS
In-Hospital Ward Out-patients groups
and individual training
Group/individual training
Out-patients Community based
Residential Settings
GP /
Exercise
Referral
Tai Chi
Walking
Groups
Falls…Sarcopenia…Frailty...Physical & Psychological Health…Isolation…Inclusion…Social Engagement…Independence…Quality of Life…Health & Social Care costs…
Dance
….
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Table Task
List 3 activity/exercise opportunities within a 15 minute walk/30 min drive (from) that includes strength and balance work within the programme and …..
•Has an experienced/qualified/empathetic teacher/instructor/leader
•Is at a sustainable price?
•You are confident to recommend
How do you know?
If you can’t think of any – how are we going to change this?

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
• Older people who are fearful avoid activity.
• Some reduce activity in order to reduce their exposure to hazards – a behavioural response that some professionals use as well!
• We can stop falls, by not moving at all!
• But what effect does this have on mental health, isolation, loneliness and depression?
• Do some interventions reduce risk by reducing activity/exposure to risk?
The importance of falls per unit of activity

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
• More falls in home exercise group than in the control group • Performance based mobility improved more in the intervention
group than the control group
• ? More falls just because increased activity (exposure to risk?) • Is this still a bad outcome?

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Otago exercises for visually impaired older people
• 6 month study, registered blind older people
• Occupational Therapist gave Otago prescription then visited them at home once, peer mentor visited at home three times plus telephone support
• Activity recorded subjectively with PhoneFITT questionnaire and objectively with ActivPal
• 86.7% of participants reported in their exercise diaries they exercised on average three times a week.
• BUT…
Waterman et al. In press Age
Ageing 2016

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Social desirability?
? Compensation, they were doing strength and balance exercises so decided did not need to walk as much?
? They perceived activity was risky unless it was the ‘safe exercises’
Waterman et al. In press Age
Ageing 2016
What will be the long term effect of the Otago intervention in these individuals? Probably an increased risk of falls as they decondition

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Is it possible to increase activity and decrease falls ?
Iliffe S et al. Health Technology Assessment 2014
6 months of FaME in low risk older adults? Still effective? FaME increased moderate to vigorous physical activity by 15 mins/day. Up to 12 months post intervention. By 24 months effect discontinued. FaME reduced falls by 26% (IRR 0.74) Up to 12 months post intervention. By 24 months effect discontinued. No increase in falls at beginning of intervention
MVPA increased
by 105 mins per
week
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
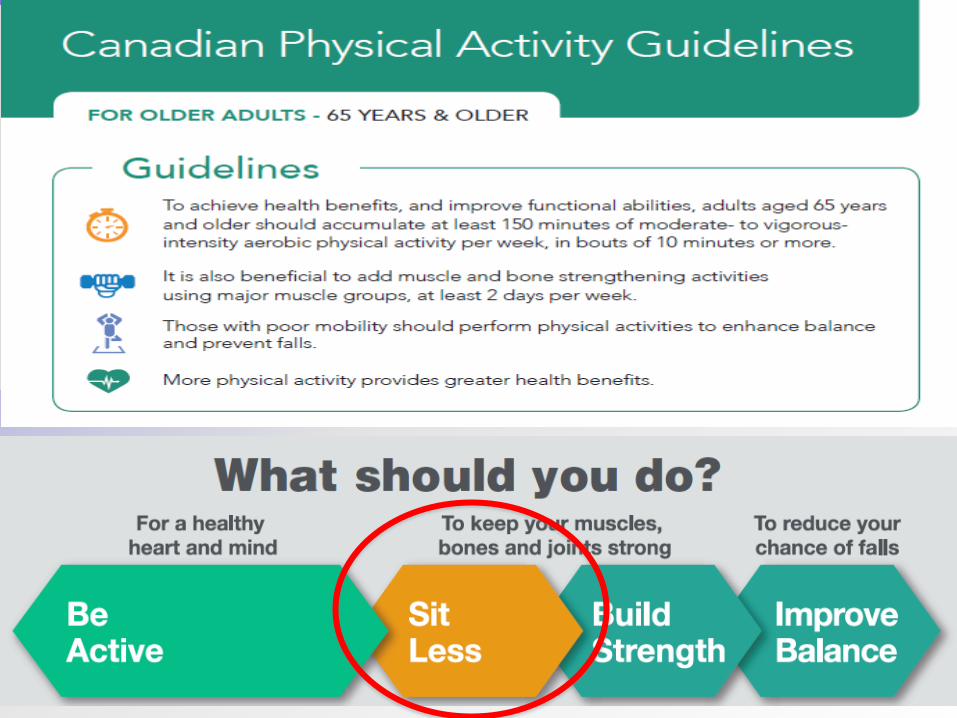
Falls prevention must be more than strength and balance
• If some people compensate by being less physically active because they are doing strength and balance exercise what is the longer term effect?
• We have to have the conversation – these exercises have to be in addition to moving more often…
• Sedentary behaviour leads to poor outcomes
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
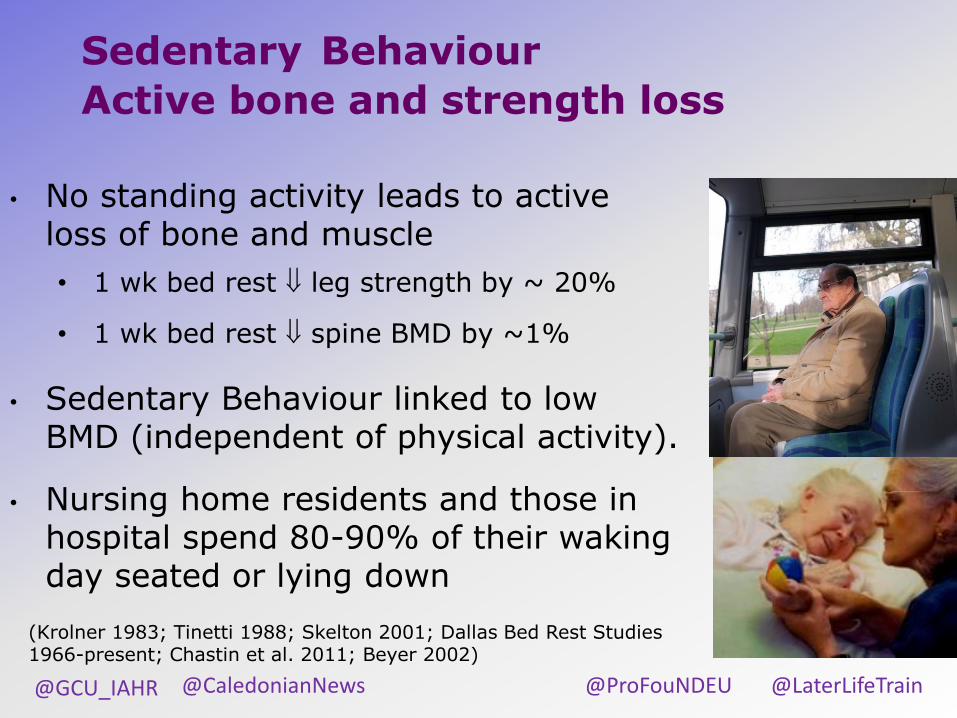
Sedentary Behaviour
Active bone and strength loss
• No standing activity leads to active loss of bone and muscle
• 1 wk bed rest leg strength by ~ 20%
• 1 wk bed rest spine BMD by ~1%
• Sedentary Behaviour linked to low BMD (independent of physical activity).
• Nursing home residents and those in hospital spend 80-90% of their waking day seated or lying down
(Krolner 1983; Tinetti 1988; Skelton 2001; Dallas Bed Rest Studies 1966-present; Chastin et al. 2011; Beyer 2002)
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
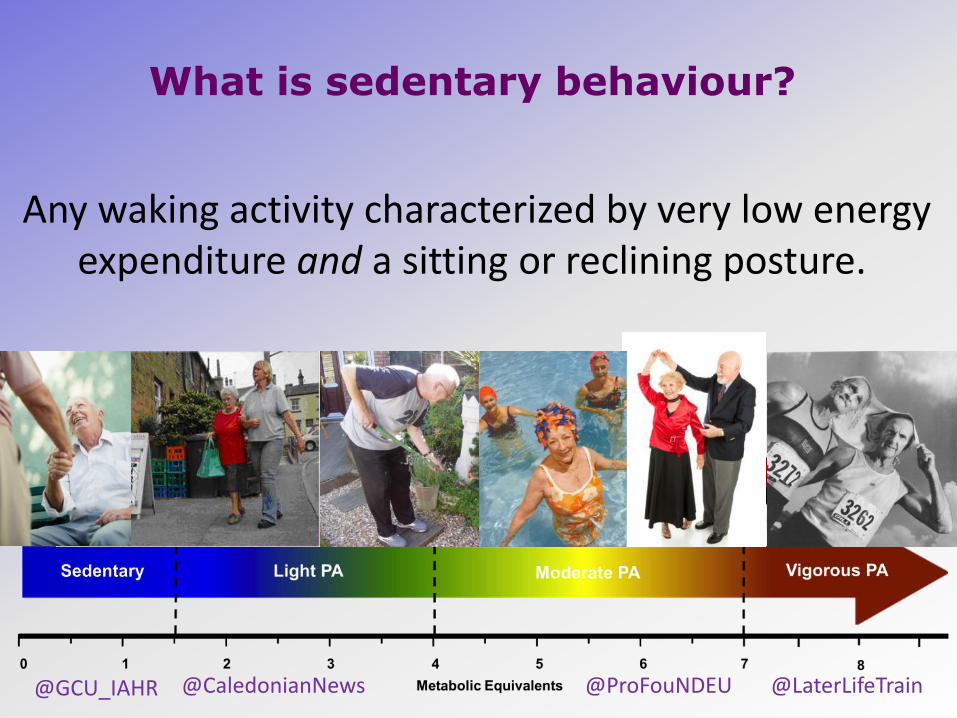
What is sedentary behaviour?
Any waking activity characterized by very low energy expenditure and a sitting or reclining posture.
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
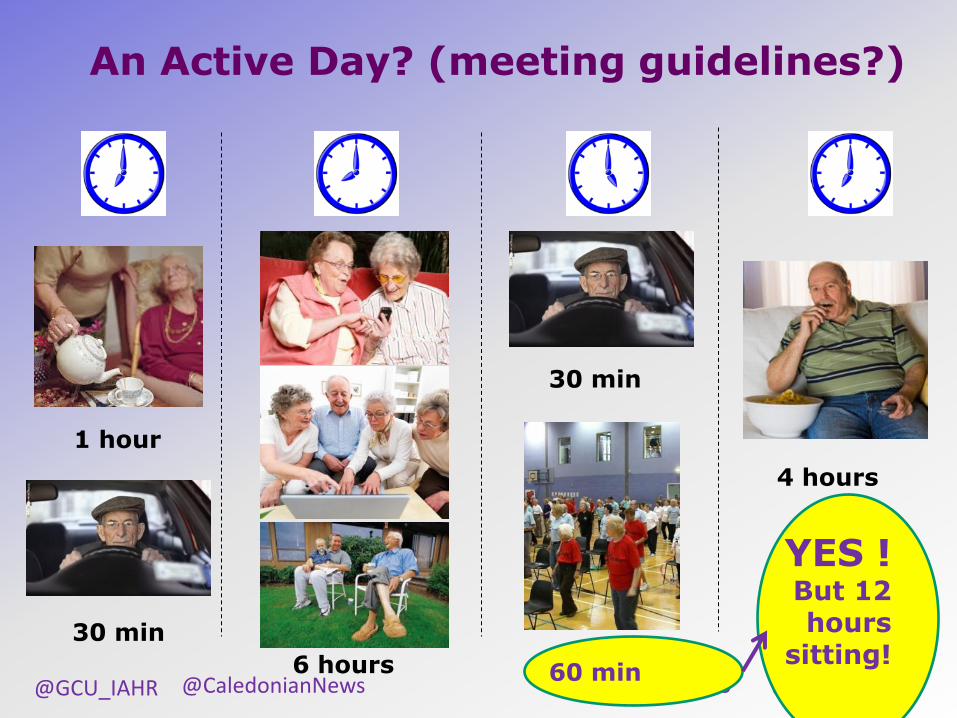
An Active Day? (meeting guidelines?)
6 hours
30 min
30 min
30 min
4 hours
YES ! But 12 hours
sitting! 60 min
1 hour

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
0
2
4
6
8
10
12
Self Report:
Sitting
Self Report: TV Self Report:
Screen
Accelerometry
Ho
urs P
er D
ay
Male
Female
How long do older people sit for?
Harvey, Chastin, Skelton (2014) JAPA
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Sedentary behaviour health risks
Older adults who meet PA guidelines but are
sedentary rest of their time have a 42%
increased risk of all-cause mortality
Older adults who are sedentary and physically
inactive have a 127% increased risk of all-cause
mortality Martinez-Gomez et al (2013) BMC Med. 22: 47
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Sedentary behaviour health risks
In older adults (>60 years old), sedentary behaviour has been found to be significantly associated with:
Sedentary behaviour is also linked to musculoskeletal pain and can affect quality of life, social inclusion and engagement
• Higher plasma glucose • Higher BMI and waist:hip ratio • Higher cholesterol • Reduced muscle strength • Reduced bone density
Gennuso et al (2013) Med Sci Sports Exerc.; Skelton (2001) Age Ageing; Chastin et al (2014) Bone.; WHO (2010) Global Recommendations on Physical Activity for Health

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Acute effects of sitting - 45 mins sitting in a hot room (30°C)
• 26 women
• 70+ years
• 30°C vs 20°C
• 45 mins sitting
• Thin clothing
• Higher BP
• Increased postural hypotension
• Shorter distance walked in 6 mins (reduced stamina)
Stotz, Rapp, Skelton et al. Int. J. Environ. Res. Public Health 2014

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Acute effects of sitting - 45 mins sitting in a cold room (15°C)
• 88 women
• 70+ years
• 15°C vs 20°C
• 45 mins sitting
• Thin clothing
• 5% lower muscle power
• 10% lower sit to stand velocity
• 3.5% lower walking speed
Lindemann, Skelton et al. Age Ageing, 2014.

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
Table Task
• Stand up and talk to the person to your right side
• One idea on how to break up long periods of sitting (>1 hour) in your work setting?
• One idea on how to break up long periods of sitting (>1 hour) in the older people you work with?
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
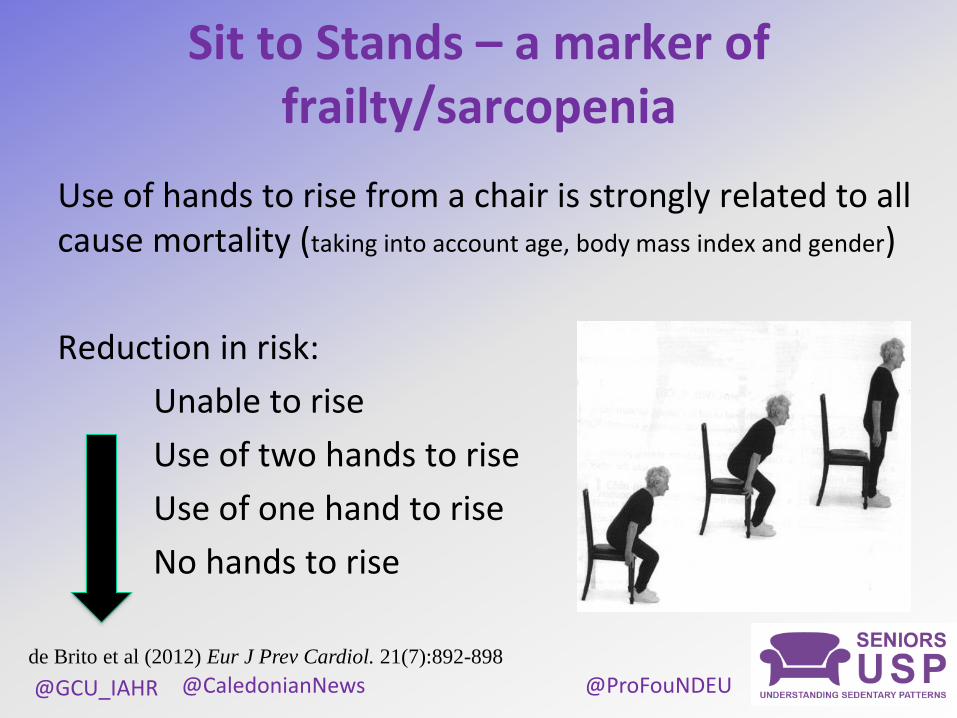
Sit to Stands – a marker of frailty/sarcopenia
Use of hands to rise from a chair is strongly related to all cause mortality (taking into account age, body mass index and gender)
Reduction in risk:
Unable to rise
Use of two hands to rise
Use of one hand to rise
No hands to rise
de Brito et al (2012) Eur J Prev Cardiol. 21(7):892-898

@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
@GCU_IAHR @ProFouNDEU @LaterLifeTrain
@CaledonianNews
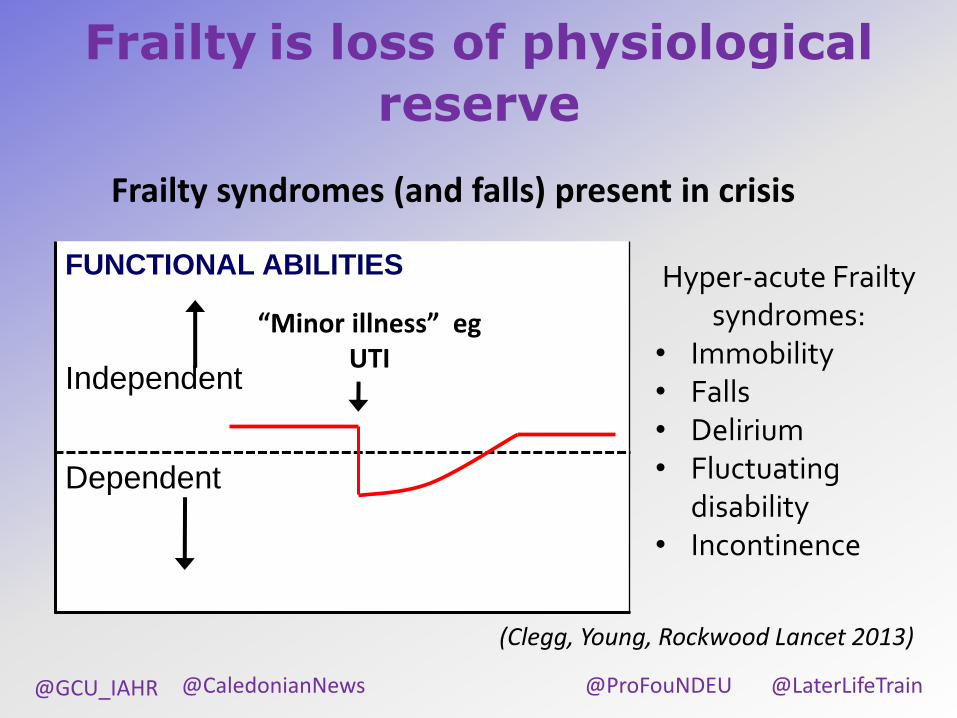
Frailty is loss of physiological
reserve
FUNCTIONAL ABILITIES
Independent
Dependent
“Minor illness” eg UTI
Frailty syndromes (and falls) present in crisis
Hyper-acute Frailty syndromes:
• Immobility • Falls • Delirium • Fluctuating
disability • Incontinence
(Clegg, Young, Rockwood Lancet 2013)