antrectomy - - get a free blog here
TRANSCRIPT

Antrectomy
Daniel T. Dempsey, MD, and Abhijit Pathak, MD
The antrum serves important hormonal and motorfunctions. The antral mucosa is the primary source of
gastrin, a major stimulus for acid production by the pari-etal cells. Antral gastrin production is shut off by lumenalacid. When doing an antrectomy, it is particularly impor-tant to be certain that all antral tissue is removed distallywhen planning a Billroth II or Roux reconstruction. Inthese situations, antral tissue left on the duodenal stumpwill secrete gastrin unremittingly because it will no longerbe exposed to acid. This syndrome of “retained antrum” isan important cause of hypergastrinemia and acid hyper-secretion in the remaining stomach. Recurrent or mar-ginal ulceration may result.
The antrum also plays a major role in the triturationand subsequent gastric emptying of solid foods. Antralresection is generally associated with accelerated gastricemptying of liquids, and may be associated with delayedemptying of solids. Symptoms of dumping may or maynot be present. Antrectomy refers to the resection of theantrum and the pylorus and usually involves removing atleast 30% of the stomach. Distal or hemigastrectomy gen-erally refers to resection of about 50% of the caudal stom-ach, including the antrum and pylorus. These operationsare functionally identical, except in the latter in which theproximal margin of resection is extended cephalad.
PATIENT SELECTION
The most common benign indications for antrectomy ordistal gastrectomy are duodenal ulcer, gastric ulcer, andlarge benign gastric tumors (leiomyoma, lipoma). Otherindications include perforation or stricture from traumaor caustic ingestion. Relative contraindications includecirrhosis, extensive scarring of the proximal duodenum(obligating a difficult or tenuous duodenal closure), andprevious operation on the proximal duodenum (eg, cho-ledochoduodenostomy).
DUODENAL ULCER
In selected patients, antrectomy is still a good operationfor intractable or obstructing duodenal ulcer disease. A
truncal or selective vagotomy is added. The advantage ofthe latter is that the extragastric visceral innervation ispreserved and long term side effects such as gallstonesand postvagotomy diarrhea may be less.
It must be recognized that operative intervention forintractable duodenal ulcer disease should be very unusualnowadays, since over 95% of duodenal ulcers are knownto be associated with Heliobacter pylori infection,NSAIDs, or gastrinoma. If these causes have been ex-cluded or treated appropriately, the surgeon should bewary of the patient referred for “intractable duodenalulcer.” This patient may be quite different from the largenumber of patients in the surgical literature who areknown to have done well with vagotomy and antrectomyin the era before effective pharmacologic acid suppression(eg, cimetidine) and before recognition of the role of H.pylori. We feel strongly that if vagotomy and antrectomyare applied indiscriminately today as the operation ofchoice for intractable duodenal ulcer, the incidence ofpoor surgical outcomes (Visick 3 and 4) will be muchhigher than predicted in the existing literature. Medicaltherapy has healed all the easy patients, and the ones whoare referred for elective surgery for intractable or non-healing duodenal ulcer currently are the difficult patientswho may not do well with gastric resection; in this pop-ulation, nonresective procedures should be strongly con-sidered.
Most patients hospitalized today for gastric outlet ob-struction from duodenal ulcer disease have H. pylori in-fection that should be treated. Nonetheless, most suchpatients will require some invasive treatment for theirobstruction. In the low-risk surgical patient with ob-structing duodenal ulcer disease, antrectomy and selec-tive vagotomy is a good operation. This is especially truein the noncompliant patient population in whom eradi-cation of H. pylori and chronic treatment with antisecre-tory medication (if necessary for recurrent ulcer) is lesslikely to be successful. Results of highly selective vagot-omy and drainage for obstructing duodenal ulcer havebeen good, but recurrent or marginal ulceration is morecommon than after antrectomy.
GASTRIC ULCER
Distal gastrectomy (which also includes proximal resec-tion) to include the gastric ulcer remains the electiveoperation of choice for gastric ulcer. The same admoni-tions discussed above regarding intractability apply. But
From the Department of Surgery, Temple University, Philadelphia, PA.Address reprint requests to Dr. Daniel T. Dempsey, 301 South 8th Street,
Philadelphia, PA 19107.© 2003 Elsevier Inc. All rights reserved.1524-153X/03/0502-0011$30.00/0doi:10.1053/otgn.2003.35361
86 Operative Techniques in General Surgery, Vol 5, No 2 (June), 2003: pp 86–100
unlike duodenal ulcer, with a nonhealing gastric ulcer,the specter of malignancy lurks and makes long-termnonsurgical management less appealing. Resection is alsoan attractive option in many patients with a stable gastriculcer who require urgent operation for bleeding or perfo-ration; gastrectomy gets rid of the ulcer, which may bemalignant in 5 to 10% of such patients. In contrast, resec-tion is less commonly done today in the emergency set-ting for perforation or bleeding from duodenal ulcer.
BENIGN TUMORSWedge resection with negative margins is adequate treat-ment for benign gastric tumors such as leiomyoma (stro-mal tumors), lipoma, or adenoma. But when these benignneoplasms are large and located in the antrum or prepy-loric region, formal distal gastrectomy is often more prac-tical, because it avoids excessive lumenal narrowing. Fro-zen section should always be obtained to assure negativemargins and benignity.
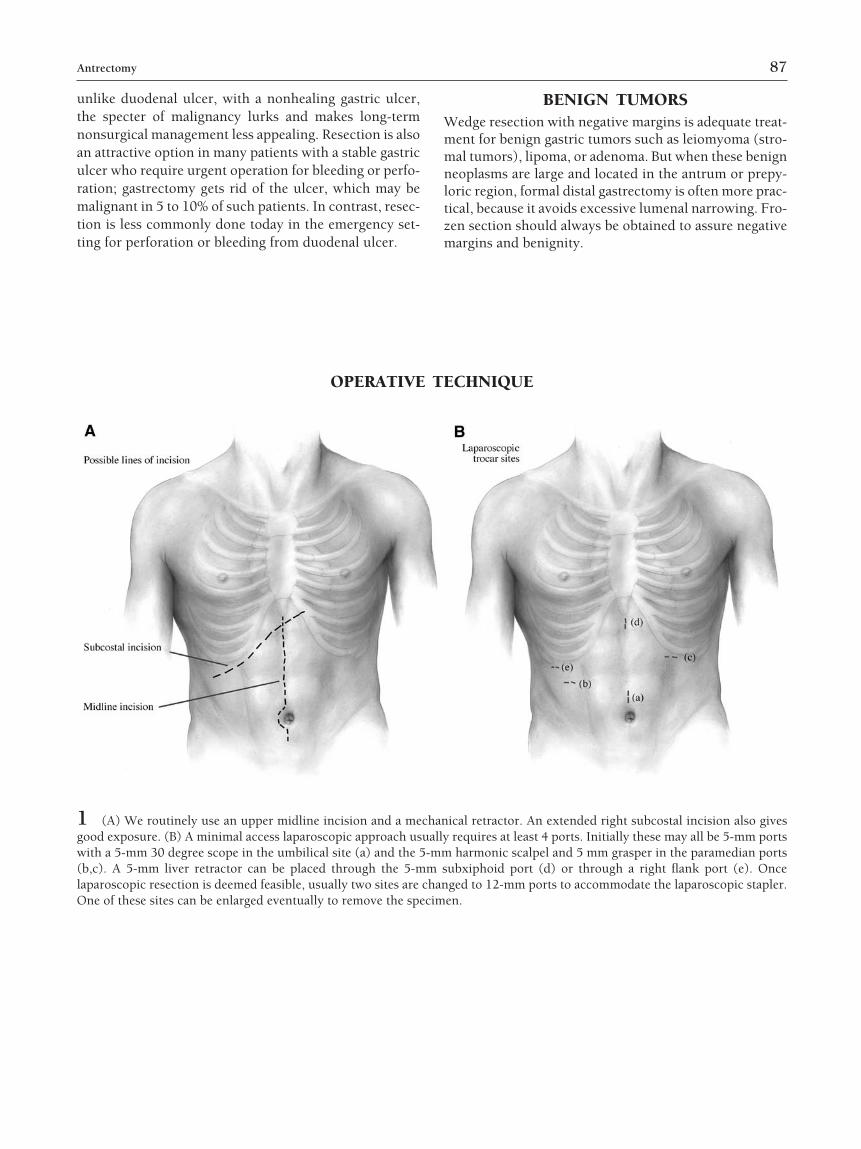
1 (A) We routinely use an upper midline incision and a mechanical retractor. An extended right subcostal incision also givesgood exposure. (B) A minimal access laparoscopic approach usually requires at least 4 ports. Initially these may all be 5-mm portswith a 5-mm 30 degree scope in the umbilical site (a) and the 5-mm harmonic scalpel and 5 mm grasper in the paramedian ports(b,c). A 5-mm liver retractor can be placed through the 5-mm subxiphoid port (d) or through a right flank port (e). Oncelaparoscopic resection is deemed feasible, usually two sites are changed to 12-mm ports to accommodate the laparoscopic stapler.One of these sites can be enlarged eventually to remove the specimen.
OPERATIVE TECHNIQUE
87Antrectomy
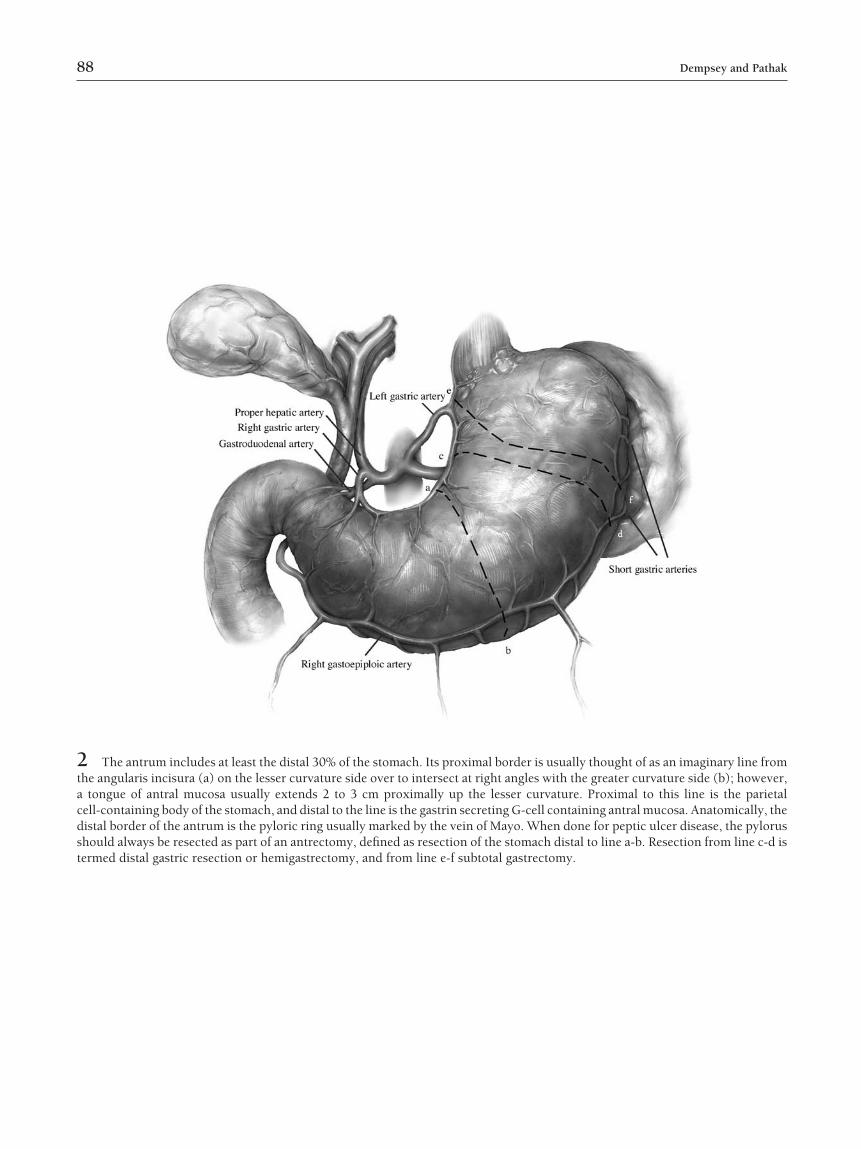
2 The antrum includes at least the distal 30% of the stomach. Its proximal border is usually thought of as an imaginary line fromthe angularis incisura (a) on the lesser curvature side over to intersect at right angles with the greater curvature side (b); however,a tongue of antral mucosa usually extends 2 to 3 cm proximally up the lesser curvature. Proximal to this line is the parietalcell-containing body of the stomach, and distal to the line is the gastrin secreting G-cell containing antral mucosa. Anatomically, thedistal border of the antrum is the pyloric ring usually marked by the vein of Mayo. When done for peptic ulcer disease, the pylorusshould always be resected as part of an antrectomy, defined as resection of the stomach distal to line a-b. Resection from line c-d istermed distal gastric resection or hemigastrectomy, and from line e-f subtotal gastrectomy.
88 Dempsey and Pathak
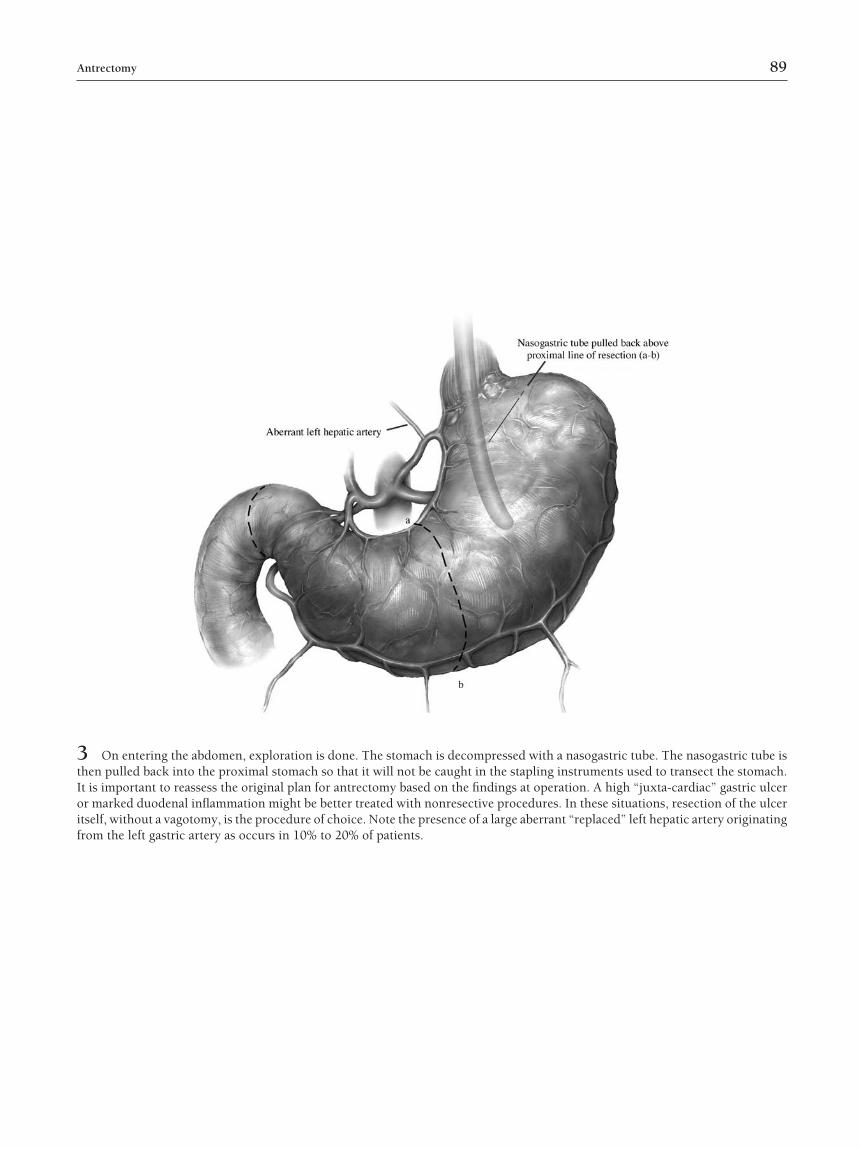
3 On entering the abdomen, exploration is done. The stomach is decompressed with a nasogastric tube. The nasogastric tube isthen pulled back into the proximal stomach so that it will not be caught in the stapling instruments used to transect the stomach.It is important to reassess the original plan for antrectomy based on the findings at operation. A high “juxta-cardiac” gastric ulceror marked duodenal inflammation might be better treated with nonresective procedures. In these situations, resection of the ulceritself, without a vagotomy, is the procedure of choice. Note the presence of a large aberrant “replaced” left hepatic artery originatingfrom the left gastric artery as occurs in 10% to 20% of patients.
89Antrectomy

4 The avascular gastrohepatic ligament (lesser omentum) is opened and the lesser sac entered at about the level of the incisuraangularis. If the posterior stomach is free, the fingers of the operator’s left hand can push up on the greater curvature attachments,facilitating entry into the lesser sac from this side of the stomach. Alternatively, if the lesser sac is obliterated or if the lesser curvatureis thickened or inflamed, the lesser sac is entered initially from the greater curvature side of the stomach, usually below the spleenat about the midpoint of the lesser curvature. The right gastroepiploic vessels are divided and ligated here, and a Penrose drain orcatheter passed around the mid-stomach for manipulation. It is often easier to free the greater gastric curvature down toward thepylorus by staying just outside the right gastroepiploic vessels in the gastrocolic ligament, ligating small omental branches (x).Often, the lesser curvature dissection can be facilitated by palpating the plane between the lesser curvature and the liver with the aidof the surgeon’s nondominant hand in the lesser sac, as introduced from the greater curvature side. Occasionally such an approachwill render the omentum ischemic, necessitating resection. The surgeon should pay attention to the location of the middle colicvessels during this dissection, because inflammation and scarring especially in the obese patient may predispose these vessels toinjury. Alternatively, the distal greater curvature may be mobilized by staying inside the gastroepiploic arcade, ligating the multiplesmall branches to the stomach (o).
90 Dempsey and Pathak
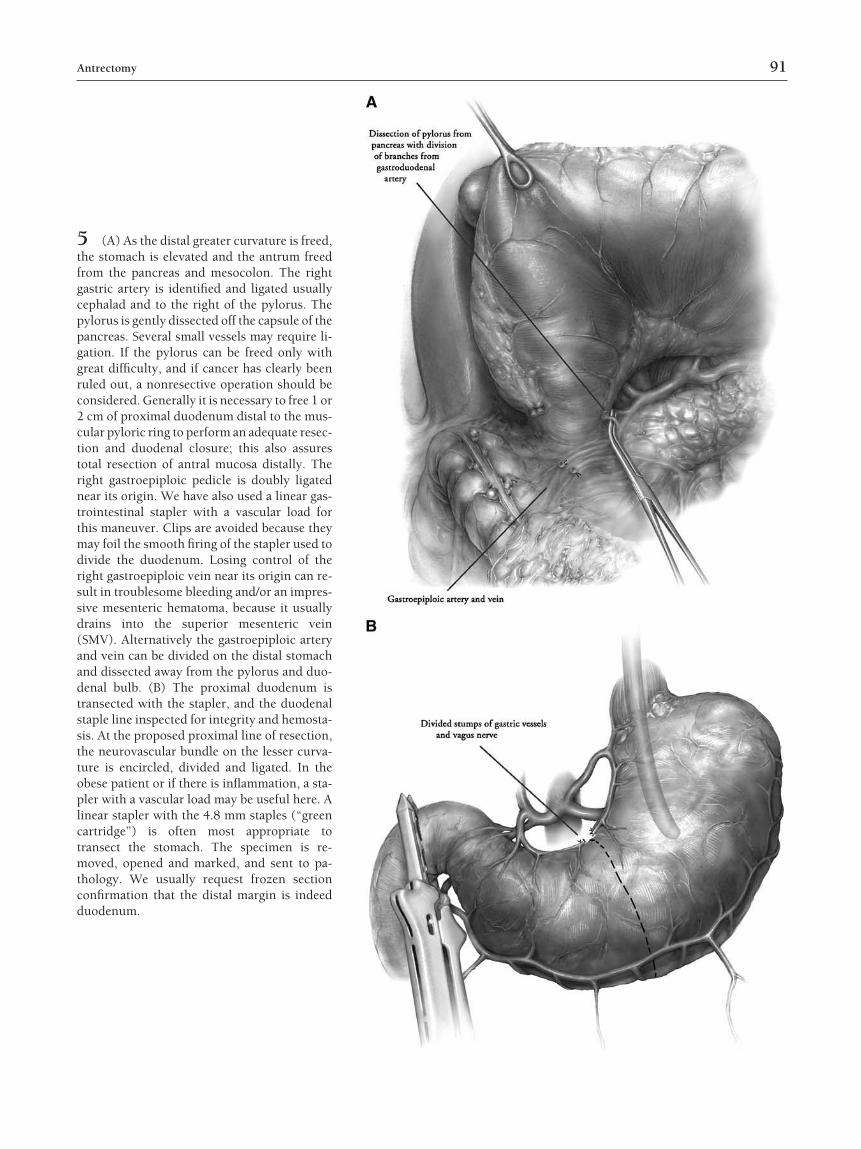
5 (A) As the distal greater curvature is freed,the stomach is elevated and the antrum freedfrom the pancreas and mesocolon. The rightgastric artery is identified and ligated usuallycephalad and to the right of the pylorus. Thepylorus is gently dissected off the capsule of thepancreas. Several small vessels may require li-gation. If the pylorus can be freed only withgreat difficulty, and if cancer has clearly beenruled out, a nonresective operation should beconsidered. Generally it is necessary to free 1 or2 cm of proximal duodenum distal to the mus-cular pyloric ring to perform an adequate resec-tion and duodenal closure; this also assurestotal resection of antral mucosa distally. Theright gastroepiploic pedicle is doubly ligatednear its origin. We have also used a linear gas-trointestinal stapler with a vascular load forthis maneuver. Clips are avoided because theymay foil the smooth firing of the stapler used todivide the duodenum. Losing control of theright gastroepiploic vein near its origin can re-sult in troublesome bleeding and/or an impres-sive mesenteric hematoma, because it usuallydrains into the superior mesenteric vein(SMV). Alternatively the gastroepiploic arteryand vein can be divided on the distal stomachand dissected away from the pylorus and duo-denal bulb. (B) The proximal duodenum istransected with the stapler, and the duodenalstaple line inspected for integrity and hemosta-sis. At the proposed proximal line of resection,the neurovascular bundle on the lesser curva-ture is encircled, divided and ligated. In theobese patient or if there is inflammation, a sta-pler with a vascular load may be useful here. Alinear stapler with the 4.8 mm staples (“greencartridge”) is often most appropriate totransect the stomach. The specimen is re-moved, opened and marked, and sent to pa-thology. We usually request frozen sectionconfirmation that the distal margin is indeedduodenum.
91Antrectomy
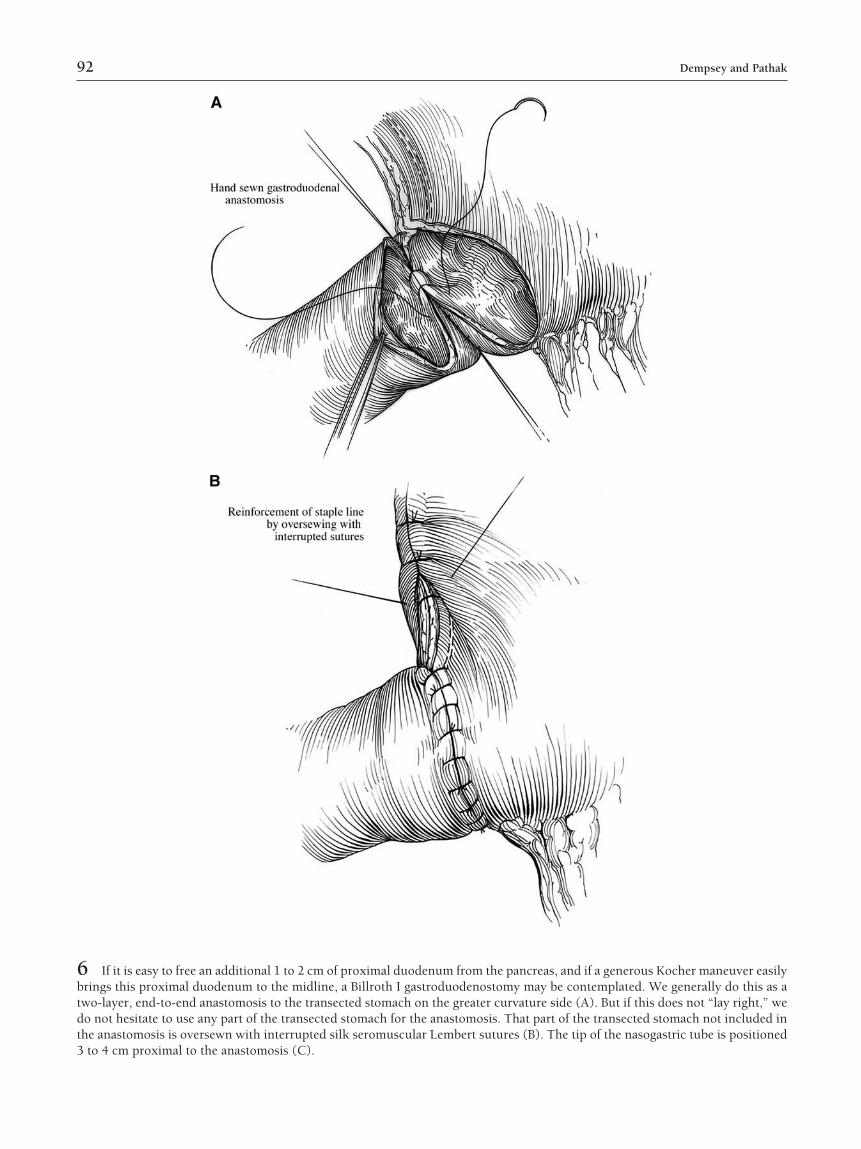
6 If it is easy to free an additional 1 to 2 cm of proximal duodenum from the pancreas, and if a generous Kocher maneuver easilybrings this proximal duodenum to the midline, a Billroth I gastroduodenostomy may be contemplated. We generally do this as atwo-layer, end-to-end anastomosis to the transected stomach on the greater curvature side (A). But if this does not “lay right,” wedo not hesitate to use any part of the transected stomach for the anastomosis. That part of the transected stomach not included inthe anastomosis is oversewn with interrupted silk seromuscular Lembert sutures (B). The tip of the nasogastric tube is positioned3 to 4 cm proximal to the anastomosis (C).
92 Dempsey and Pathak
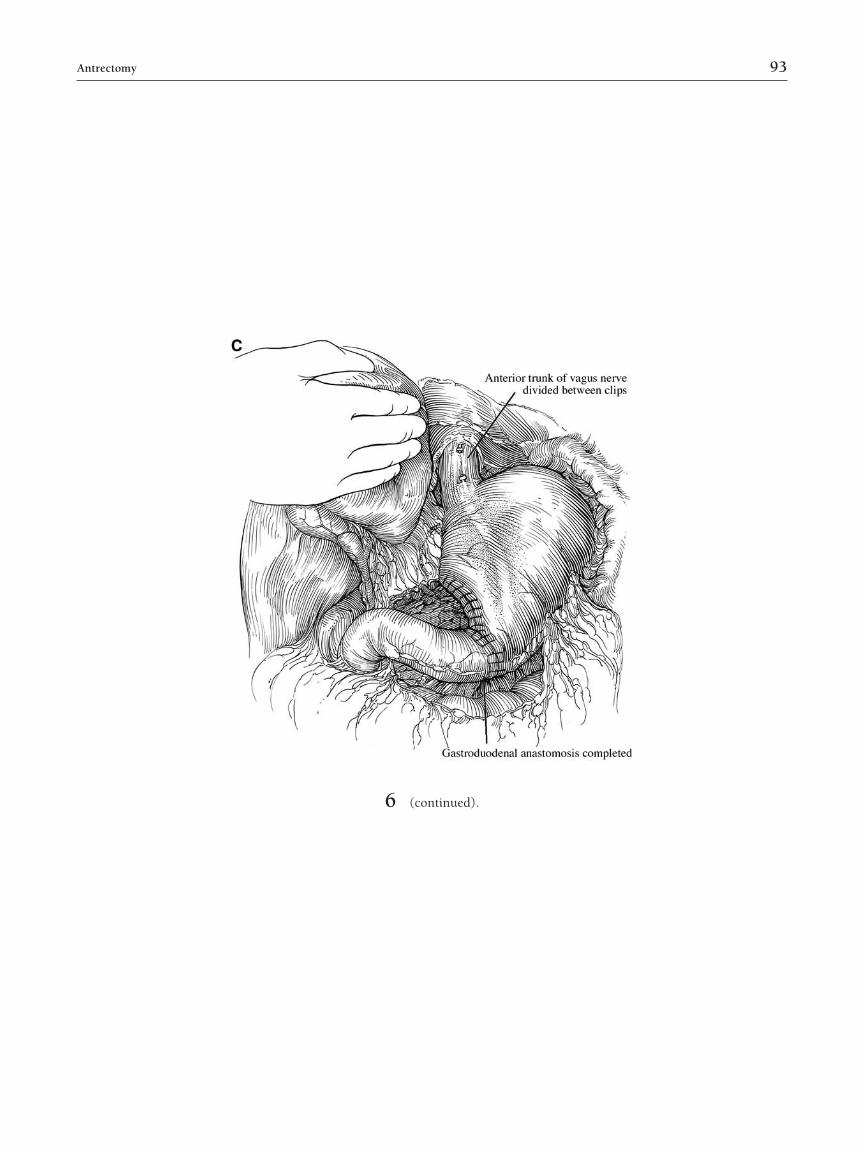
6 (continued).
93Antrectomy
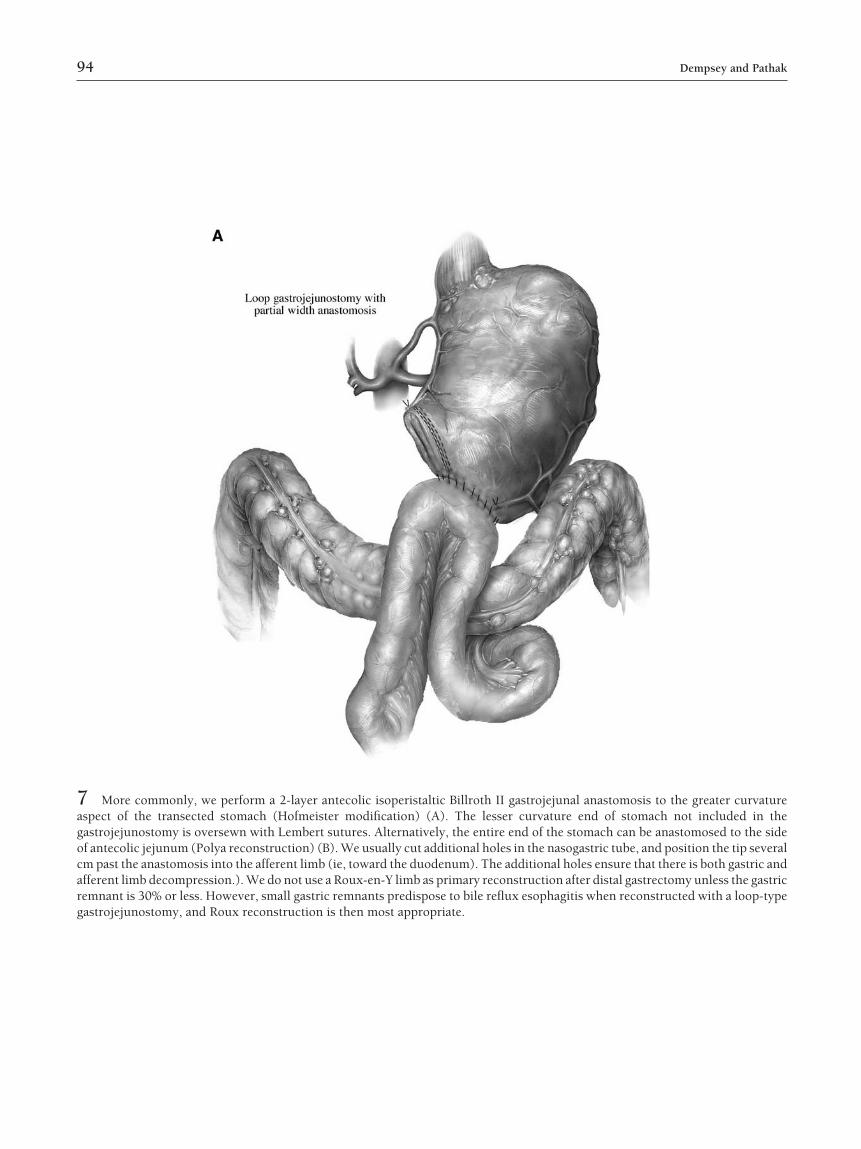
7 More commonly, we perform a 2-layer antecolic isoperistaltic Billroth II gastrojejunal anastomosis to the greater curvatureaspect of the transected stomach (Hofmeister modification) (A). The lesser curvature end of stomach not included in thegastrojejunostomy is oversewn with Lembert sutures. Alternatively, the entire end of the stomach can be anastomosed to the sideof antecolic jejunum (Polya reconstruction) (B). We usually cut additional holes in the nasogastric tube, and position the tip severalcm past the anastomosis into the afferent limb (ie, toward the duodenum). The additional holes ensure that there is both gastric andafferent limb decompression.). We do not use a Roux-en-Y limb as primary reconstruction after distal gastrectomy unless the gastricremnant is 30% or less. However, small gastric remnants predispose to bile reflux esophagitis when reconstructed with a loop-typegastrojejunostomy, and Roux reconstruction is then most appropriate.
94 Dempsey and Pathak
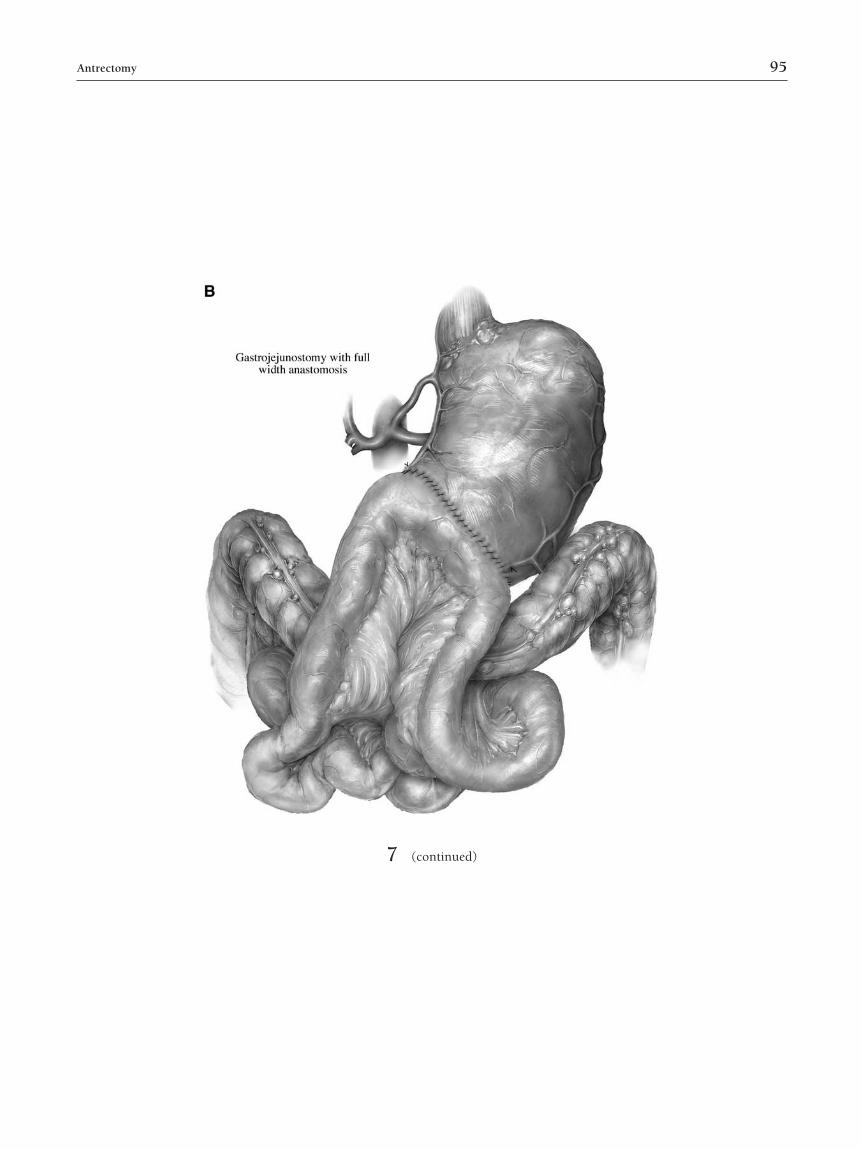
7 (continued)
95Antrectomy
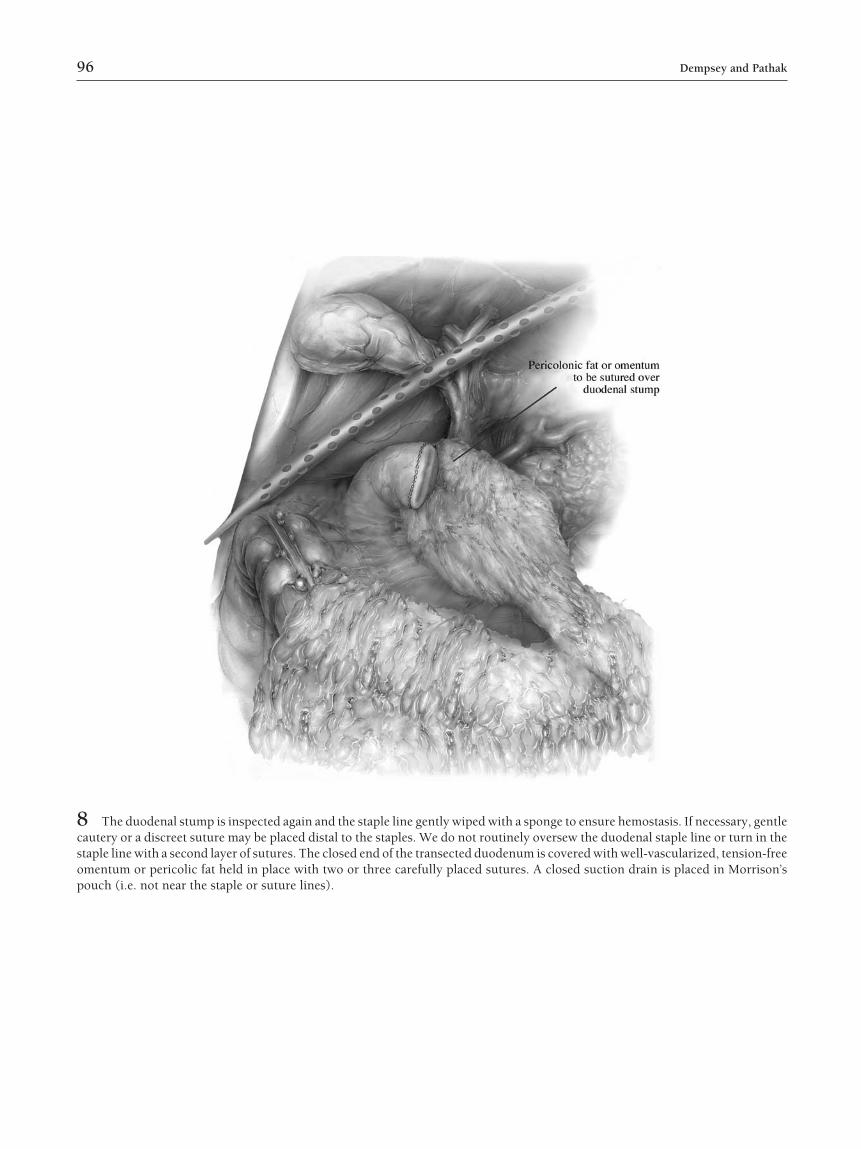
8 The duodenal stump is inspected again and the staple line gently wiped with a sponge to ensure hemostasis. If necessary, gentlecautery or a discreet suture may be placed distal to the staples. We do not routinely oversew the duodenal staple line or turn in thestaple line with a second layer of sutures. The closed end of the transected duodenum is covered with well-vascularized, tension-freeomentum or pericolic fat held in place with two or three carefully placed sutures. A closed suction drain is placed in Morrison’spouch (i.e. not near the staple or suture lines).
96 Dempsey and Pathak
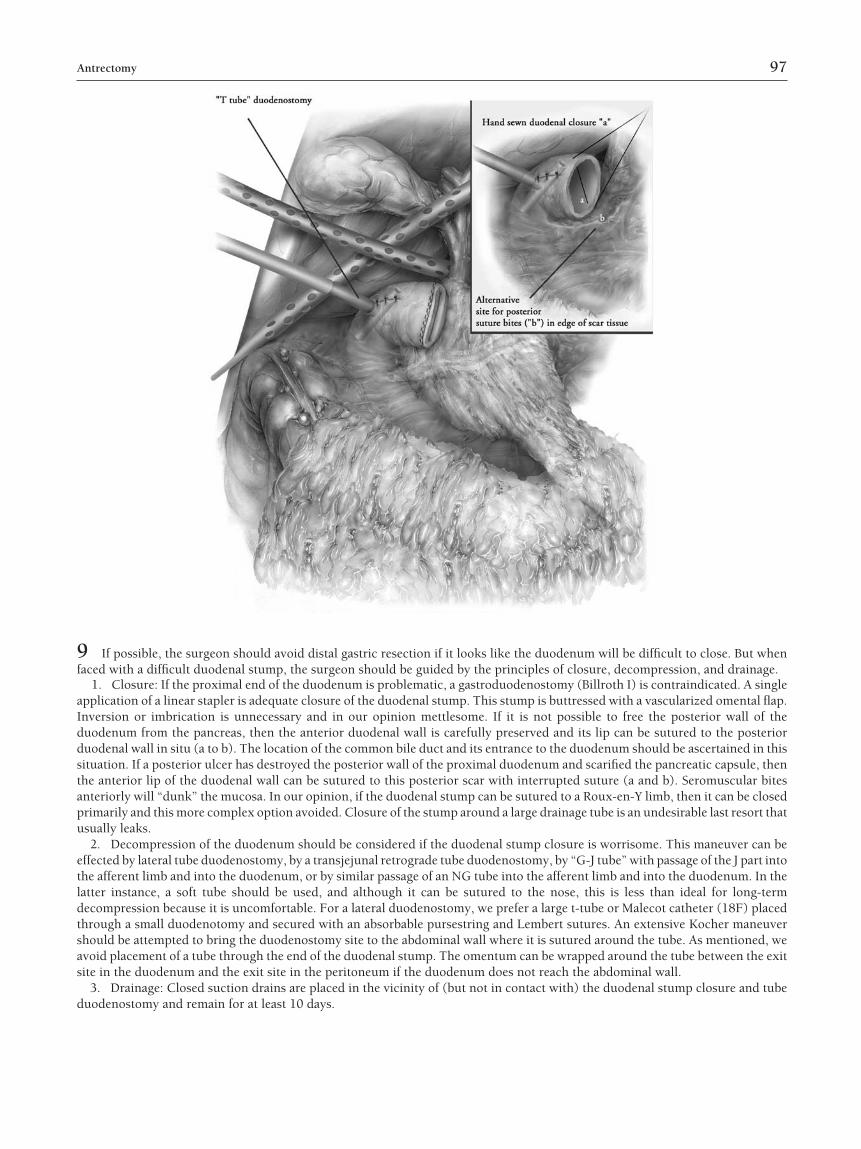
9 If possible, the surgeon should avoid distal gastric resection if it looks like the duodenum will be difficult to close. But whenfaced with a difficult duodenal stump, the surgeon should be guided by the principles of closure, decompression, and drainage.
1. Closure: If the proximal end of the duodenum is problematic, a gastroduodenostomy (Billroth I) is contraindicated. A singleapplication of a linear stapler is adequate closure of the duodenal stump. This stump is buttressed with a vascularized omental flap.Inversion or imbrication is unnecessary and in our opinion mettlesome. If it is not possible to free the posterior wall of theduodenum from the pancreas, then the anterior duodenal wall is carefully preserved and its lip can be sutured to the posteriorduodenal wall in situ (a to b). The location of the common bile duct and its entrance to the duodenum should be ascertained in thissituation. If a posterior ulcer has destroyed the posterior wall of the proximal duodenum and scarified the pancreatic capsule, thenthe anterior lip of the duodenal wall can be sutured to this posterior scar with interrupted suture (a and b). Seromuscular bitesanteriorly will “dunk” the mucosa. In our opinion, if the duodenal stump can be sutured to a Roux-en-Y limb, then it can be closedprimarily and this more complex option avoided. Closure of the stump around a large drainage tube is an undesirable last resort thatusually leaks.
2. Decompression of the duodenum should be considered if the duodenal stump closure is worrisome. This maneuver can beeffected by lateral tube duodenostomy, by a transjejunal retrograde tube duodenostomy, by “G-J tube” with passage of the J part intothe afferent limb and into the duodenum, or by similar passage of an NG tube into the afferent limb and into the duodenum. In thelatter instance, a soft tube should be used, and although it can be sutured to the nose, this is less than ideal for long-termdecompression because it is uncomfortable. For a lateral duodenostomy, we prefer a large t-tube or Malecot catheter (18F) placedthrough a small duodenotomy and secured with an absorbable pursestring and Lembert sutures. An extensive Kocher maneuvershould be attempted to bring the duodenostomy site to the abdominal wall where it is sutured around the tube. As mentioned, weavoid placement of a tube through the end of the duodenal stump. The omentum can be wrapped around the tube between the exitsite in the duodenum and the exit site in the peritoneum if the duodenum does not reach the abdominal wall.
3. Drainage: Closed suction drains are placed in the vicinity of (but not in contact with) the duodenal stump closure and tubeduodenostomy and remain for at least 10 days.
97Antrectomy
SUMMARY
Laparoscopic staplers with interchangeable gastrointesti-nal and vascular cartridges, and the ultrasonic shears havemade laparoscopic antrectomy a more attractive surgicaloption. A periumbilical camera port and three or fourworking ports are used. A 30 degree angled laparoscope isessential, and it should be moved to other ports as neces-sary for optimal visualization. Although the importantparts of the operation are the same whether it is doneopen or laparoscopically, there are some important differ-ences in the conduct of the procedure:
1. The stomach is decompressed and then the NGtube is pulled way back to avoid stapling, since it is vir-tually impossible to palpate laparoscopically.
2. The proximal gastric margin is usually transectedearly. This maneuver facilitates elevation of the antrumoff the pancreas and mesocolon. An endoscopic staplerwith a vascular load can be used on the neurovascularbundle on the greater and lesser curvature, and a gastro-intestinal cartridge with either 3.2 or preferably 4.8 mmstaples on the stomach.
3. Just proximal to the pylorus, the right gastroepip-
loic vessels may be divided with clips or the vascularstapler, and then dissected away from the pylorus andproximal duodenum with the harmonic scalpel.
4. The proximal duodenum is divided with the lapa-roscopic stapler, and then the right gastric pedicle is di-vided.
5. A double staple technique is used for reconstruc-tion with an antecolic Billroth II gastrojejunostomy. TheNG tube is gently reintroduced with the tip only a few cmpast the gastroesophageal junction (“3 lines showing atthe nose”), and position confirmed with x-ray in the re-covery room. No attempt is made to put the tube throughthe anastomosis, and the tip should be proximal enoughin the stomach that it is not near the anastomosis.
Intraoperative ComplicationsAntrectomy for benign disease is usually a straightfor-ward operation. However intraoperative problems canarise, and the prudent surgeon will anticipate and avoidthese. Significant bleeding is usually the result of venousinjury from blunt dissection or excessive traction. Twopotential trouble spots are the gastroepiploic vein at its
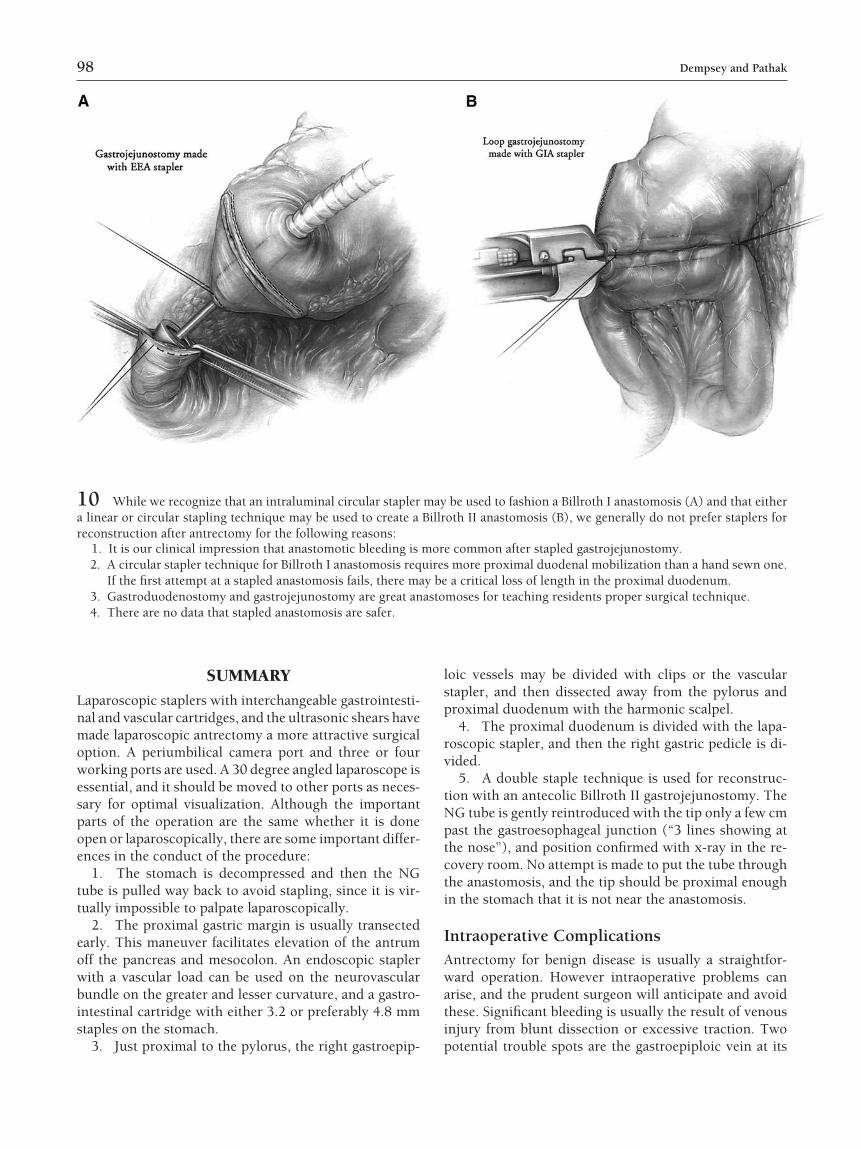
10 While we recognize that an intraluminal circular stapler may be used to fashion a Billroth I anastomosis (A) and that eithera linear or circular stapling technique may be used to create a Billroth II anastomosis (B), we generally do not prefer staplers forreconstruction after antrectomy for the following reasons:
1. It is our clinical impression that anastomotic bleeding is more common after stapled gastrojejunostomy.2. A circular stapler technique for Billroth I anastomosis requires more proximal duodenal mobilization than a hand sewn one.
If the first attempt at a stapled anastomosis fails, there may be a critical loss of length in the proximal duodenum.3. Gastroduodenostomy and gastrojejunostomy are great anastomoses for teaching residents proper surgical technique.4. There are no data that stapled anastomosis are safer.
98 Dempsey and Pathak

junction with the superior mesenteric vein, and the leftgastric vein (coronary vein) near its junction usually withthe portal vein. It is important not to make the injuryworse by hasty or rough dissection in an attempt to ex-pose the source of bleeding. Gentle pressure will controlthe hemorrhage indefinitely, and discreet controlled dis-section will reveal the venous defect that can be repairedreadily with a 5–0 polypropylene suture. Bleeding fromthe splenic capsule can usually be controlled with cauteryand topical hemostatic agents. If staplers with a vascularload are used during gastrectomy, the staple lines shouldalways be irrigated and gently abraded to check the ade-quacy of hemostasis. It is not uncommon that additionalmaneuvers are required. We avoid placing hemo-clips inproximity to where we plan to transect or anastomosewith staplers.
The difficult duodenal stump, more often talked aboutthan seen nowadays, is best avoided by not doing anantrectomy in the face of significant scarring and/or in-flammation in the proximal duodenum (see Fig 9).
Injury to other organs during antrectomy should beunusual. Dissection is distal to the spleen, making injuryto this organ infrequent. Injudicious traction on theomentum can occasionally cause a capsular tear, but sple-nectomy is rarely necessary. If pancreatic injury is sus-pected, drainage is mandatory. Before drain removal, theeffluent is analyzed for amylase content. Adhesions fromprevious operation or gastroduodenal inflammation orscarring may predispose the colon to injury. Rarely thetransverse colon can be rendered ischemic by injury tothe middle colic artery and partial colectomy may benecessary. For these reasons, preoperative mechanicalbowel preparation may be prudent when planning gastricresection in selected patients.
Postoperative management and complications
Early ambulation, incentive spirometry, antisecretorymedications, and prophylactic, perioperative antibioticsare routine. The choice of prophylactic antibiotic dependson whether you expect the presence of gastric outlet ob-struction or achlorhydria; in these situations, coverage ofanaerobic organisms is also wise. Oral liquids are startedwhen there is clinical evidence that gastrointestinal func-tion has returned, usually on postoperative day 3 to 5 asheralded by bowel sounds, decreased NG drainage, andpassage of flatus. First we often obtain a limited upper GIstudy with water-soluble contrast to confirm emptying ofthe gastric remnant and to rule out leak. Then liquids maybe started with the NG tube in place and residualschecked, or the tube may be discontinued. Patients areadvised to start oral intake slowly for the first day or twoin an effort to avoid distention of the gastric remnant.Careful reinsertion of the NG tube should be consideredfor persistent vomiting, distention, or hiccups.
Common postoperative complications include atelec-
tasis, pneumonia, wound infection, ileus (including gas-tric stasis), and electrolyte abnormalities. Delayed gastricemptying during the first postoperative month is by itselfalmost never an indication for reoperation. Erythromycinmay be useful in ameliorating this problem; metoclopra-mide, as a kinetic, is not effective when the antrum hasbeen removed.
Less common complications include intraabdominalhemorrhage, suture line bleeding (ie, GI bleed), duodenalstump leak, anastomotic leak, pancreatitis, intraabdomi-nal abscess and internal hernia. Duodenal stump leak maybe managed nonoperatively only if the patient continuesto do well and there is radiologic evidence of adequatedrainage and no intraabdominal collection. Otherwiseearly reoperation to effect the following is wise: close orintubate the leak; buttress this closure with omentum;decompress the duodenum; drain adequately; and place afeeding jejunostomy to allow long-term postduodenal en-teral feeding and the ability to reinfuse duodenal drain-age.
OutcomesThe overall operative mortality rate for antrectomy isaround 2% but is higher in patients with critical organdysfunction, insulin-dependent diabetes, or immunosup-pression. Eighty percent of patients do well (Visick 1 or2), while up to 20% of patients develop some form ofpostgastrectomy and/or postvagotomy complications(Visick 3 or 4). Problems in this latter group includerecurrent ulcer, dumping, diarrhea, gastric stasis, bile re-flux gastritis, bowel obstruction and chronic abdominalpain. If antrectomy is performed judiciously for benigndisease only when necessary, the incidence of poor out-comes will not increase in our modern era.
SUGGESTED READING1. Adkins RB Jr., DeLozier JB 3rd, Scott HW Jr, Sawyers JL: The
management of gastric ulcers. A current review. Ann Surg. 201:741–751, 1985
2. Behrns KE, Sarr MG: Diagnosis and management of gastric emp-tying disorders. Adv Surg 27:233–255, 1994
3. Csendes A, Maluenda F, Braghetto I, et al: Prospective randomizedstudy comparing three surgical techniques for the treatment ofgastric outlet obstruction secondary to duodenal ulcer. Am J Surg166:45–49, 1993
4. Delcore R, Cheung LY: Surgical options in postgastrectomy syn-dromes. Surg Clin No Amer 71:57–75, 1991
5. De Vries BC, Schattenkerk ME, Smith EE, et al: Prospective ran-domized multicentre trial of proximal gastric vagotomy or truncalvagotomy and antrectomy for chronic duodenal ulcer: results after5–7 years. Br J Surg 70:701–703, 1983
6. Donahue PE: Parietal cell vagotomy versus vagotomy-antrectomy:ulcer surgery in the modern era. World J Surg. 24:264–269, 2000
7. Eagon JC, Miedema BW, Kelly KA: Postgastrectomy syndromes.Surg Clin No Amer 72:445–465, 1992
8. Gibril F, Lindeman RJ, Abou-Saif A, et al: Retained gastric antrumsyndrome: a forgotten, treatable cause of refractory peptic ulcerdisease. Dig Dis Sci 46:610–617, 2001
99Antrectomy

9. Goligher JC, Feather DB, Hall R, et al: Several standard electiveoperations for duodenal ulcer: Ten to 16 year clinical results. AnnSurg 189:18–24, 1979
10. Herrington JL Jr: Gastroduodenal ulcer. Overview of 150 paperspresented before the Southern Surgical Association 1888–1986.Ann Surg 207:754–769, 1988
11. Jordan PH Jr, Thornby J: Twenty years after parietal cell vagotomyor selective vagotomy antrectomy for treatment of duodenal ulcer.Final report. Ann Surg 220:283–293, 1994
12. Kaneko K, Kondo H, Saito D, et al: Early gastric stump cancerfollowing distal gastrectomy. Gut 43:342–344, 1998
13. Kendall BJ, Chakravarti A, Kendall E, et al: The effect of intrave-nous erythromycin on solid meal gastric emptying in patients withchronic symptomatic post-vagotomy-antrectomy gastroparesis.Aliment Pharm Therap 11:381–385, 1997
14. Koo J, Lam SK, Chan P, et al: Proximal gastric vagotomy, truncalvagotomy with drainage, and truncal vagotomy with antrectomyfor chronic duodenal ulcer. A prospective, randomized controlledtrial. Ann Surg. 197:265–271, 1983
15. Mayers TM, Orebaugh MG: Totally laparoscopic Billroth I gastrec-tomy. J Amer Coll Surg 186:100–103, 1998
16. McConnell DB, Baba GC, Deveney CW: Changes in surgical treat-ment of peptic ulcer disease within a veterans hospital in the1970s and the 1980s. Arch Surg 124:1164–1167, 1989
17. McFadden DW, Zinner MJ: Reoperation for recurrent peptic ulcerdisease. Surg Clin No Amer 71:77–92, 1991
18. Millat B, Fingerhut A, Borie F: Surgical treatment of complicatedduodenal ulcers: controlled trials. World J Surg 24:299–306, 2000
19. Paimela H, Tuompo PK, Perakyla T, et al: Peptic ulcer surgeryduring the H2-receptor antagonist era: a population-based epide-miological study of ulcer surgery in Helsinki from 1972 to 1987.Br J Surg 78:28–31, 1991
20. Ramirez B, Eaker EY, Drane WE, et al: Erythromycin enhancesgastric emptying in patients with gastroparesis after vagotomy andantrectomy. Dig Dis Sci 39:2295–2300, 1994
21. So JB, Yam A, Cheah WK, et al: Risk factors related to operativemortality and morbidity in patients undergoing emergency gas-trectomy. Br J Surg 87:1702–1707, 2000
22. Xynos E, Vassilakis JS, Fountos A, et al: Enterogastric reflux aftervarious types of antiulcer gastric surgery: Quantitation by99mTC- HIDA scintigraphy. Gastroenterology 101:991–998,1991
100 Dempsey and Pathak