antiretroviral therapy 2015 paul a. pham pharm.d. bcps
TRANSCRIPT

Antiretroviral Therapy 2015
Paul A. Pham Pharm.D. BCPS

Conflict of Interest
MADAP consultant
CDC OI guidelines committee member
HIV renal guidelines member
Janssen Advisory Board 2014

Objectives
Updated 2015 DHHS guidelines Rationale for recommendations on
1) when to start, 2) what to start with,
3) what to change to
Pharmacology of Antiretrovirals– Adverse Drug Reactions– Drug-drug Interactions– Resistance Mutations

When to Start ARTCurrent 2015 DHHS recommendation: ART is for ALL HIV-infected patients. CD4 Count (cells/µL)
Data Benefit
<350 RCT Mortality and Morbidity Benefit
350-500 non-RCT, Cohort Studies, secondary analysis of RCT
Morbidity benefit and perhaps mortality
>500 Cohort StudiesRCT ongoing
Morbidity benefit and perhaps mortality.NA-ACCORD94% increase in relative risk of death w/ deferred ART
– HIV-associated nephropathy– Rapidly declining CD4 count (>100 cell/mm3 per year)
and high viral load (>100,000 c/mL)– HBV and HCV co-infection– Acute HIV– Pregnancy– AIDS defining conditions (ex. HIV-associated dementia)– Acute OI
Urgency of ART

Importance of ART during an acute OI282 pts randomized to early (within 14 days) vs. deferred
Median time to ART 12d vs. 45 d
PCP-63%, Crypto meningitis-12%, Bacterial Infection-12%
Fewer AIDS progression/deaths (OR = 0.51; 95% CI = 0.27-0.94) with
early ART
Zolopa AR Plos one 2009

Goals of therapy HIV RNA below limit of detection (ie, <20-75 copies/mL, depending on assay)
1) reduce HIV-associated morbidity and mortality
2) restore and preserve immunologic function
3) prevent HIV transmission.
Expected Virologic Response*
Time Viral Load
1 week Decrease 0.75-1.0 log10/mL
4 weeks Decrease 1.3-2.0 log10/mL; <5000 c/mL
8-16 weeks <5000 c/mL
24** <20 c/mL
*Faster VL response in the first month observed with InSTI-based regimens ** Most patient should be undetectable at 24 weeks. VL response rate may be slower with higher baseline VL and low CD4 count

Monitoring Before and During ARTTest Baseline ART
initiationWeek 2-8
Every 3-6 months
Viral failure/Clinically indicated
CD4 count + + q3-6 mo first 2 years of ART-viremia on ART; CD4 <200q12h mo if CD4 300-500If CD4 >500 VL <20 c/ml: optional
+
VL + + Q4-8 weeks until VL <20then q3-6mo
+ +
Genotype* + + +
*Transmitted resistance in 6-16%In absence of therapy (selective pressure), resistance mutations may decline over time and become undetectable, but may persist and cause treatment failure when ART is startedTreatment history is very important when off ART

26 FDA Approved ARVs

ARVs Mechanism of Action
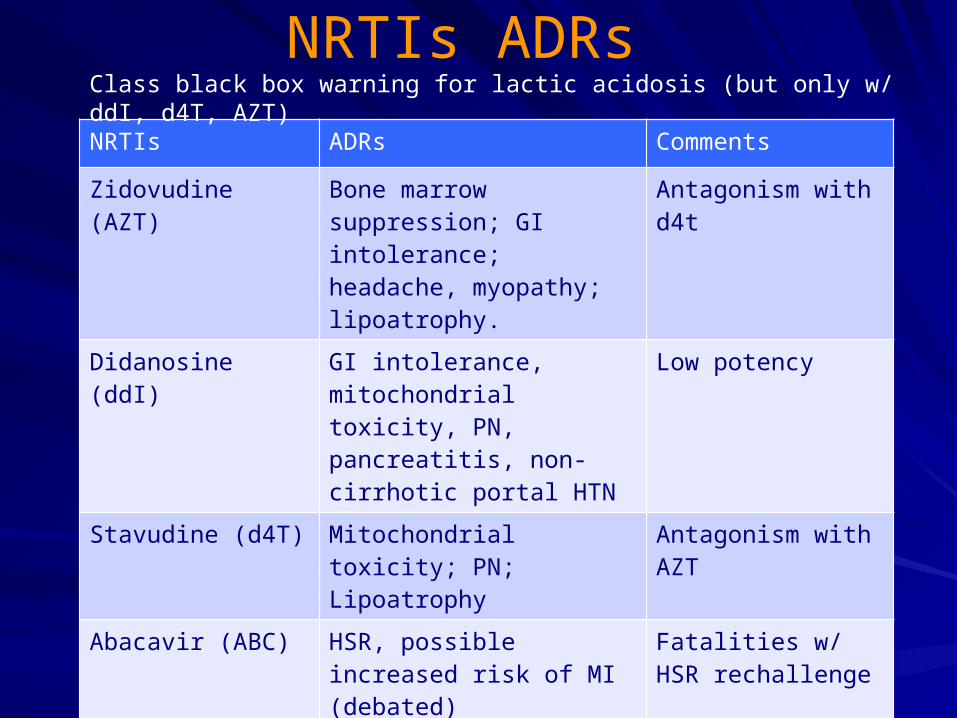
NRTIs ADRs
NRTIs ADRs Comments
Zidovudine (AZT) Bone marrow suppression; GI intolerance; headache, myopathy; lipoatrophy.
Antagonism with d4t
Didanosine (ddI) GI intolerance, mitochondrial toxicity, PN, pancreatitis, non-cirrhotic portal HTN
Low potency
Stavudine (d4T) Mitochondrial toxicity; PN; Lipoatrophy
Antagonism with AZT
Abacavir (ABC) HSR, possible increased risk of MI (debated)
Fatalities w/ HSR rechallenge
Tenofovir (TDF) Nephrotoxicity; Decrease in bone density
HBV flare w/ d/c
Lamivudine (3TC) Well tolerated HBV flare w/ d/c
Emtricitabine (FTC) Well tolerated; skin hyperpigmentation
HBV flare w/ d/c
Class black box warning for lactic acidosis (but only w/ ddI, d4T, AZT)

Protease Inhibitors ADRsPIs ADRs* Comments
Saquinavir (SQV) PR and QTc prolongation (avoid w/ QTc >450 ms); fat accumulation
Low potency; low absorption
Indinavir (IDV) Nephrolithiasis; fat accumulation Avoid
Nelfinavir (NFV) Secretory diarrhea; fat accumulation Low potency
Fosamprenavir (FPV)
Rash; nephrolithiasis (rare); fat accumulation
Cross-resistance with DRV
Lopinavir/r (LPV/r) GI (n/v/d); PR and QTc prolongation; fat accumulation.
Higher rates of GI intolerance compared to ATV/r and DRV/r
Atazanavir (ATV) Indirect bilirubin elevation; nephrolithiasis; PR prolongation; rash
Lipid friendly
Tipranavir (TPV/r) GI intolerance; hepatitis; intracranial hemorrhage; rash
Sulfa moiety
Darunavir/r (DRV/r) Rash Lipid friendly; Sulfa moiety
Class adverse events: GI intolerance, hepatitis, hyperlipidemia

NNRTIs ADRs
NNRTIs ADRs Comments
Nevirapine (NVP)
Severe rash (SJS, TEN) and hepatitis
Women CD4>250 and men CD4 >400 are at increased risk
Delavirdine (DLV)
Rash Low potency
Efavirenz (EFV)
CNS side effects (insomnia, dizziness, confusion, depression); hyperlipidemia
False+ THC and Benzo; teratogenic (first 8 weeks)
Etravirine (ETR)
Generally well tolerated; HSR (rash, hepatitis)
Must d/c with HSR
Rilpivirine (RPV)
Dose dependent QTc prolongation; CNS side effects
Monitor drug-drug interaction with CYP3A4 inhibitors.
Class ADRs: rash; hepatitis

Integrase Inhibitors ADRs
InSTI ADRs Comments
Raltegravir (RAL) CK elevation (+/- rhabdomyolysis); rash; LFT elevation; GI intolerance
Must d/c w/ increased LFTs and rash
Elvitegravir (EVG) GI intolerance Scr elevation (0.14+/-0.13 mg/dL with COBI boosting with no change in GFR
Dolutegravir (DTG) CK elevation; insomnia Scr elevation w/ no change in GFR by iohexal
Generally well tolerated w/ lower discontinuation than PI/r- and EFV-based ART

Entry Inhibitors ADRs
• Enfuvirtide (T-20): injection site reaction (induration, pain, erythema). Rotate injection sites.
• Maraviroc (MVC): Generally well tolerated. CK elevation; myalgia; orthostatic hypotension (CrCL <30ml/min and CYP3A inhibitor)

Not Recommended Due to Toxicity
AZT-GI intolerance, bone marrow suppression, mitochondrial toxicity d4T-mitochondrial toxicity, peripheral neuropathy ddI-mitochondrial toxicity, peripheral neuropathy, pancreatitis NVP-rash (including TEN and SJS) and hepatitis IDV/r-nephrolithiasis RTV 600 mg twice-daily-severe GI intolerance-N/V/D

ADRs due to Drug-Drug Interactions
“statin” PIs Effect of on “statin” PK
Simvastatin SQV/RTVNFV
AUC Increased by 3059%AUC increased by 506%
Lovastatin All PI May significantly increase lovastatin
Gerber JG et al. CROI 2004 abst.603; Hsyu PH et al. ICAAC 2000 abst 425
• Equivalent to giving simvastatin 600mg/d !!
• Atorvastatin (up to 40 mg), rosuvastatin (up to 20 mg), or pitavastatin (up to 4 mg) can be given to PIs

0.001
0.01
0.1
1
10
0 6 12 18 24 30 36 42 48
Time (hours)
Dru
g c
on
cen
trat
ion
(m
g/m
L)
Beneficial CYP3A4 Inhibition LPV/r single-dose pharmacokinetics
LPV400mg +100mg RTV
LPV 400mg alone
Data on File

PIs Drug InteractionsPIs Interacting Drug Comments
Saquinavir (SQV)Indinavir (IDV)Nelfinavir (NFV)Fosamprenavir (FPV)Lopinavir/r (LPV/r)Tipranavir (TPV/r)Darunavir(DRV/r or /c)Atazanavir(ATV/r or /c)
All substrate and inhibitor of 3A4
Amiodarone, quinidine, dofetilide, propafenone, bepridilPimozide, fentanyl, oral midazolam, triazolam
Significant increase of the interacting drugs.Contraindicated
PPI, H2 blocker, antacid Avoid ATV
Rifampin Contraindicated. Use rifabutin
Rifabutin Rifabutin 150 mg once daily (higher than FDA approved dose). Monitor RBT levels.
RTV=COBI >>LPV/r=DRV/r= TPV/r>IDV=NFV=APV=ATV>>SQV

NNRTIs Drug InteractionsNNRTIs Interacting Drug Comments
Nevirapine (NVP)3A4Efavirenz (EFV)2B6>3A4
Etravirine (ETR)3A4, 2C9,2C19
Tacrolimus, sirolimus
Simvastatin
Methadone
Clopidogrel
Tacrolimus, sirolimus, cyclosporine
Simvastatin AUC 58%. Titrate to effect
Methadone up to 50%. Must titrate.
Conversion to active clopidogrel metabolite may be inhibited by ETR. Avoid if possible.
Rilpivirine (RPV)3A4
Macrolide, PI/r May significantly increase RPV. Monitor QTc
Antacid, PPI, H2 blockers
Decreased RPV levels. Avoid

InSTI Drug InteractionsInSTI Interacting Drug Comments
Raltegravir (RAL)Glucuronidation
Rifampin Increase RAL to 800 mg BID
Dolutegravir (DTG)Glucuronidation>> CYP3A4
Rifampin, EFV, FPV, TPV
Etravirine
Must increase DTG 50 mg bidUse only if no InSTI mutations
DTG and ETR can only be co-administered in if given with PI/r.
Elvitegravir/c (EVG/c or /r)CYP3A4
CYP3A4 substrate All interactions with PIs apply
Al and Mg antacid: EVG, RAL, DTG: decreased by ~50-70%. Give EVG or DTG >2hrs before antacid

NRTIs, MVC, T-20 Drug Interactions
NRTIs Interacting drug Comments
Zidovudine (AZT)Didanosine (ddI)Stavudine (d4T)Abacavir (ABC)Lamivudine (3TC)Emtricitabine (FTC)
Tenofovir (TDF)
MaravirocCYP3A4
T-20
PI/r and COBI Increased TDF levels
EFV, ETR, phenytoin, phenobarbital, carbamazepine
Increase MCV to 600 mg bid
PI/r, macrolides, azoles Decrease MCV to 150 mg bid
No significant interaction

Food-drug Interactions w/ ARVsAntiretrovirals Food Effect Recommendation
Rilpivirine AUC ~40% lower in a fasted state Administer wth food (BUT not protein shake 50% lower)
Etravirine Improves absorption. Fasted state: AUC decreased 50%
Administer with food
Nelfinavir AUC 2‑ to 5‑fold higher when given with food.
Administer with a minimum of 500 Kcal with 20% fat meal.
Tipranavir/r AUC increased by 31% with high fat meal.
Administer with food
Atazanavir (+rtv or cobi)
Darunavir (+ rtv or cobi)
AUC increased by 70% (w/unboosted), 33 (w/rtv), and 28% (w/cobi) with light meal.
AUC increased by 30% (w/rtv) and 70% (w/cobi)
Administer with food.
Administer with food
EVG/Cobi/TDF/FTC EVG AUC increased 34% Administer with food
Efavirenz AUC increased by 22% and 50% with low fat and high fat meals.
Take on empty stomach during the first 2 weeks to minimize the risk of CNS side effects.
IDV/r, LPV/r, FPV/r, SQV/r,, MVC, NVP; RAL; DTG; All NRTIs (except ddI);
No significantly affected Administer with or without food.

DHHS Guidelines, April 2015: What to Start
DHHS Guidelines for Antiretroviral Therapy in Adults and Adolescents, April 2015.
Demoted: EFV- and ATV/r-based regimen
INSTI based DTG (QD) + TDF/FTC (AI)
RAL + TDF/FTC (AI)
EVG/COBI/TDF/FTC; only if pre-ART CrCl >70 mL/min (AI)
DTG/ABC/3TC; only if HLA-B*5701 negative (AI)
PI based DRV/r (QD) + TDF/FTC (AI)

SINGLE: Dolutegravir + ABC/3TC vs. EFV/TDF/FTC
Week
EFV/TDF/FTC QD
DTG 50 mg + ABC/3TC QD
BL 2 4 8 12 16 24 32 40 48
0
10
20
30
40
50
60
70
80
90
100
Pro
po
rtio
n (
%)
wit
h <
50 c
/mL
DTG+ABC/3TC: 88%
EFV/TDF/FTC: 81%
WK 48 difference in response (95% CI): +7.4% (+2.5% to +12.3%); p=0.003
● DTG + ABC/3TC QD superior to EFV/TDF/FTC at Wk 48 (1o endpoint)
Walmsley S, et al. N Engl J Med 2013;369:1807-18

Outcome (snapshot) at Week 48
DTG 50 mg +ABC/3TCn=411n (%)
EFV/TDF/FTC(N=419)
n (%)
Virologic success 364 (88) 338 (81)
Virologic nonresponse 21 (5) 26 (6)
Data in window not <50 c/mL 6 (1) 5 (1)
Discontinued for lack of efficacy 7(2) 9 (2)
Discontinued for other reason while not <50 c/mL 8 (2) 12 (3)
No virologic data at Week 48 29 (7) 55 (13)
Discontinued because of AE or death* 9 (2) 40 (10)
Discontinued for other reasons 20 (5) 14 (3)
Missing data during window but on study 0 1 (<1)
SINGLE: DTG + ABC/3TC vs. EFV/TDF/FTC: Disposition
*Deaths: n=2, both on EFV/TDF/FTC: n=1 primary cause of death (sepsis) judged unrelated to study drug but complicated by renal failure judged possibly related to EFV/TDF/FTC; n=1 not related to EFV/TDF/FTC (pneumonia).
Walmsley S, et al. N Engl J Med 2013;369:1807-18

ACTG A5257ATV/r vs. DRV/r vs. RAL (+TDF/FTC)
Virologic failure at 96 weeks (equivalent): RAL 10%ATV 13%DRV 15%
High incidence of discontinuation due to toxicity in ATV/r-treated patients (16% vs. 1% RAL and 5% /DRV/r)
Landovitz RL et al. CROI 2015

Comparing the Integrase InhibitorsAgent Advantages Disadvantages
Raltegravir • Longest experience• Fewest drug interactions
• Twice daily dosing• No coformulation
Elvitegravir • Single-tablet regimen (EVG/cobi/TDF/FTC)
• Once-daily dosing
• Requires COBI or RTV boosting
• Multiple COBI drug interactions (similar to RTV)
• Not recommended with CrCL <70 ml/min
Dolutegravir • Single-table regimen (DTG/ABC/3TC)
• Potency demonstrated with ABC/3TC
• Once-daily dosing• Higher barrier to resistance
(compared to RAL)• Few drug interactions• Active against some RAL-
and EVG-resistant virus
• Coformulated only with ABC/3TC
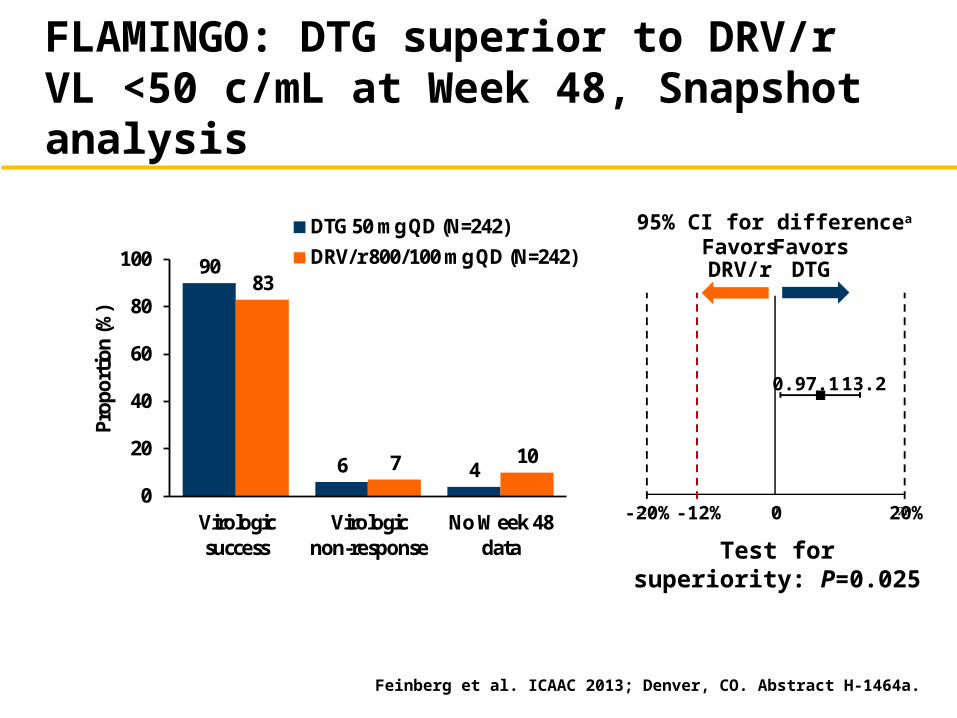
FLAMINGO: DTG superior to DRV/r VL <50 c/mL at Week 48, Snapshot analysis
Feinberg et al. ICAAC 2013; Denver, CO. Abstract H-1464a.
90
6 4
83
7 10
0
20
40
60
80
100
Virologicsuccess
Virologicnon-response
No Week 48data
Prop
ortio
n (%
)
DTG 50 mg QD (N=242)DRV/r 800/100 mg QD (N=242)
95% CI for differencea
FavorsDRV/r
FavorsDTG
-20% 0 20%
7.10.9 13.2
-12%
Test for superiority: P=0.025

DTG 50 mg QD(N=242)
DRV/r 800 mg/100 mg QD
(N=242)
Virologic success 217 (90%) 200 (83%)
Virologic non-response 15 (6%) 18 (7%)Data in window not <50 c/mL 6 (2%) 11 (5%)Discontinued for lack of efficacy 1 (<1%) 1 (<1%)Discontinued for other reason while not <50 c/mL 3 (1%) 5 (2%)Change in ART 5 (2%) 1 (<1%)
No virologic data at Week 48 10 (4%) 24 (10%)Discontinued due to AE or death 3 (1%) 9 (4%)Discontinued for other reasons 6 (2%) 11 (5%)Missing data during window but on study 1 (<1%) 4 (2%)
FLAMINGO: Proportion with VL <50Snapshot Outcomes
Feinberg et al. ICAAC 2013; Denver, CO. Abstract H-1464a.

When Should DRV/r + TDF/FTC be used?
• Must start ART before resistance test available (e.g setting of an acute OI)
• Patients with a history of non-adherence and possible resistance. Re: higher barrier to resistance.

Lesson Learned from SWITCHMRK
ART-experienced pts w/ VL <50 c/mL on a stable LPVr-based regimen. Pts had median of 5 previous ARVs.
Randomized to switch LPV/r to RAL (n=350) or continue on LPV/r (n=352) while remaining on same background ART, which included at least 2 NRTI.
At week 24, RAL (84.4%) vs LPV (90.6%) pts had HIV RNA <50; treatment difference -6.2 % (95%CI -11.2 to -1.3)
Teaching point: Before switching to a regimen with lower barrier to resistance, get a complete ART and resistance history.
Enron JJ et al. Lancet 2010

DHHS Guidelines, April 2015: Alternatives (2nd line)
NNRTI based EFV/TDF/FTC (BI)
RPV/TDF/FTC; only if pre-ART HIV RNA <100,000 copies/mL and CD4 >200 cells/µL (BI)
PI based ATV/c + TDF/FTC; only if pre-ART CrCl >70 mL/min (BI)
ATV/r + TDF/FTC (BI)
(DRV/c or DRV/r) + ABC/3TC (BIII for DRV/c, BII for DRV/r)
DRV/c + TDF/FTC; only if pre-ART CrCl >70 mL/min (BII)

Cobicistat vs. RTV boosting
Pros: co-formulation with DRV, ATV, EVG
Cons:– Not recommended with CrCL <30 ml/min– Unable to overcome induction properties of
EFV, ETR, NVP (compared to RTV).DRV/cobi not recommended with EFV, ETR, NVP
ATV/cobi not recommended with ETR or NVP
Must increase ATV to 400mg with cobi when given with EFV (treatment-naïve patients only);

Initial Regimens: 3rd Line “other”INSTI based RAL + ABC/3TC (CII)
NNRTI based EFV + ABC/3TC; only if pre-ART HIV RNA <100,000 copies/mL (C1)
PI based (ATV/c or ATV/r)a + ABC/3TC; only if pre-ART HIV RNA <100,000 copies/mL (CIII for ATV/c and CII for ATR/r)
LPV/r (QD or BID) + ABC/3TC; only if HLA-B*5701 negative (C1)
LPV/r (QD or BID) + TDF/FTC (C1)

ACTG 5202 TDF/FTC vs. ABC/3TC + EFV OR ATV/r
Early termination by DSMB in the ≥100,000 c/mL group due to higher rate of virologic failure in ABC/3TC treated pts (14% among ABC/3TC recipients vs. 7% among TDF/FTC recipients) (hazard ratio [HR] = 2.33; p = .0003).
No difference between ABC/3TC and TDF/FTC in pts w/ baseline VL <100K.
No difference between ATV/r and EFV arm
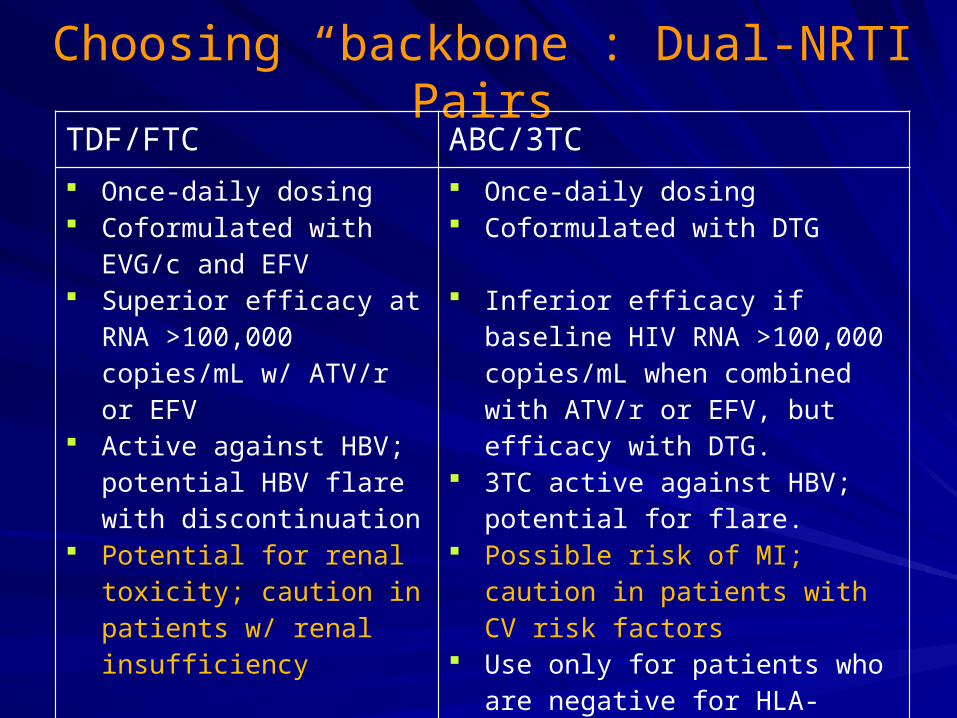
Choosing “backbone”: Dual-NRTI PairsTDF/FTC ABC/3TC
Once-daily dosing Coformulated with EVG/c
and EFV Superior efficacy at RNA
>100,000 copies/mL w/ ATV/r or EFV
Active against HBV; potential HBV flare with discontinuation
Potential for renal toxicity; caution in patients w/ renal insufficiency
Once-daily dosing Coformulated with DTG
Inferior efficacy if baseline HIV RNA >100,000 copies/mL when combined with ATV/r or EFV, but efficacy with DTG.
3TC active against HBV; potential for flare.
Possible risk of MI; caution in patients with CV risk factors
Use only for patients who are negative for HLA-B*5701 (risk of hypersensitivity reaction if positive HLA-B*5701 and fatalities with rechallenge)

What to give a Pt w/ a recent MI and CrCL 20ml/min?
DRV/r + RAL; only if pre-ART HIV RNA <100,000 copies/mL and CD4 >200 cells/µL (C1) (Raffi F et al. NEAT001/ANRS143 CROI abstract 84LB, 2014)
DRV/r + RAL vs. DRV/r + TDF/FTC-Treatment failure at 96 weeks: RAL 17.8% and TDF/FTC 13.8%,(difference 4·0%, 95% CI -0·8 to 8·8).
-With CD4 <200, RAL+DRV/r was inferior to TDF/FTC+DRV/r (p=0.02).
-With VL >100K , RAL+DRV/r did not do as well (p = 0.09).
LPV/r (BID) + 3TC (BID) (C1)
Most would use DRV/r+RAL+3TC or FTC

Virologic Failure, Definitions
Virologic failure:
Inability to achieve or maintain and undetectable HIV viral load
Virologic “blip”:
An isolated detectable HIV RNA level ( between 20-200 copies/mL) that is followed by a return to virologic suppression
No evolution of resistance during a “blip”

Management of Virologic FailureCauses for virologic failure: – 1) Adherence (with or without resistant mutations);
sub therapeutic ARV levels (drug-drug interactions, absorption)
– 2) transmitted drug resistance
Best time to obtain resistance test– While patient is taking the failing regimen (selective
pressure), or within 4 weeks of treatment discontinuation
– If >4 weeks since ARV discontinuation, resistance testing may still provide useful information (if mutations detected). Not helpful if no mutations detected.

NRTIs Resistant Mutations3TC 65R,184VIABC 65R/E/N, 74V, 115F, 184VAZT 41L, 67N, 70R, 210W, 215Y/F, 219Q/Ed4T 41L, 65R/E/N, 67N, 70R, 210W, 215Y/F, 219Q/EddI 65R/E/N, 74VFTC 65R/E/N, 184V/ITDF 65R/E/N, 70E
multi-NRTI resistance (TAMS) 41L, 67N, 70R, 210W, 215Y/F, 219Q/E (Pan resistance)multinucleoside Q151m plus 62V, 75I, 77L, 116Y, 151M (TDF susceptibility retained)multinucleoside 69 insertion 41L, 62V, 69 insert, 70R, 210W, 215Y/F, 219Q/E (Pan resistance)
184V-high level 3TC and FTC resistance; ABC-decreased susceptibility; TDF-hyper susceptibility
K65R-intermediate resistance to ddI, TDF (improved w/184V), 3TC, and FTC.
ABC (worse w/ 184V)
L74V-intermediate resistance to ddI, low level resistance to ABC (worse w/ 184V),

PIs Resistant Mutations
• No single mutation causes high level resistance• Cross resistance between PIs: 82A/F/T/S, 84V, 90M• DRV mutation score
With 0-2, 3, or ≥ 4 of 47V, 54M, 74P & 84V DRV mutations at baseline, the virologic response (< 500 c/mL at 24 weeks) was 50%, 22%, and 10% respectively.

NNRTIs Resistant Mutations
K103N-high level resistance to EFV and NVP; ETR and RPV susceptible
ETR mutation score (based on DUET)3 points: 181I/V; 2.5 points: 101P, 100I, 181C, 230L; 1.5 points: 138A, 106I, 190S, 179F; 1 point: 90I, 179D, 101E, 101H, 98G, 179T, 190A. 0-2 points: 74% response; 2.5-3.5 points: 52% response; 4+ points: 38% response
With RPV resistance, there is 89% cross-resistance to ETR

InSTIs Resistant Mutations
DTG associated with less resistance in clinical trials. The most common DTG-resistance mutation is T97A. Other mutations are E138K/A, G140S/A, Q148H/R/K
RAL: 3 pathways to resistance with mutations in integrase gene: (1) N155H + (E92Q,V151I, T97A, G163R, L74M) and (2) Q148K/R/H + (G140S/A, E138K)(3) Y143R/H/C Cross-resistance between RAL and EVG; cross-resistance w/ DTG if Q148H or G140S (+ L74I/M, E92Q, T97A, E138A/K, G140A, N155H)

Entry Inhibitors Resistant Mutations
MVC: R5 tropism shifts with disease progression 80/20 vs. 50/50
Check tropism when ready to start MVC

ART in Treatment- Experienced Patients
New regimen should contain at least 2 (preferably 3) fully active agents – Based on ARV history, resistance testing– Consider new ARV in a different class
It is a SIN to add 1 active drug to a failing regimen-resistance will develop quickly.
Consult with experts

Factors Affecting ARV SelectionPATIENT-Adherence (social support, IVDU ect)-CD4 count-Acute OI-HCV and HBV co-infection-Co-morbidities (CV risk factor, renal function, concurrent medications ect)-HLA*B5701
VIRUS-Viral load (>100K vs. <100K)-Resistance Mutations-CCR5 vs. CXCR4 tropic
ARV-Good Potency-Minimal Side Effects-Manageable Drug-Drug Interactions-High Barrier to resistance
The Perfect ARV regimen
Summary
All HIV-infected should receive ART
Urgent treatment needed in setting of Acute OI
Know your patient’s ARV treatment history, genotype, level of adherence before choosing “the perfect ART regimen”
The first regimen is the best regimen (choose wisely)
Clinical trials are favoring InSTI-based regimens

The Good News
June 5, 1981
Today

The Bad NewsThe Continuum of HIV Care - US
MMWR (60), 2011
US- 850,000 (72%) have detectable HIV
100%
75%
50%
25%
80%
77%
66% 89
%
77%

Role of the Clinical Pharmacist
Adherence counseling
Side effects and drug-drug interactions management
ART selection and dosing based on renal function, concurrent medications, and resistance profile