antimicrobial resistance in ireland a strategy for the ... · antimicrobial resistance in ireland a...
TRANSCRIPT

Prevention of intravascularcatheter-related infection in Ireland
Item Type Report
Authors SARI Prevention of Intravascular Catheter-related Infection Sub-Committee
Publisher HSE Health Protection Surveillance Centre (HPSC)
Download date 09/09/2018 07:56:48
Link to Item http://hdl.handle.net/10147/303395
Find this and similar works at - http://www.lenus.ie/hse
25-27 Middle Gardiner Street Dublin 1 IrelandTel +353 1 876 5300 Fax +353 1 856 1299 Email [email protected] www.hpsc.ie
This report is also available to download on the HPSC website at www.hpsc.ie
Antimicrobial Resistance in IrelandA Strategy for the Control of S A R I
Prevention of Intravascular Catheter-related Infection in Ireland
SARI Prevention of Intravascular Catheter-related Infection Sub-Committee

Prevention of Intravascular Catheter-related Infection in Ireland
SARI Prevention of Intravascular Catheter-related Infection Sub-Committee
Health Protection Surveillance CentreDecember 2009
Updated February 2010
Published on behalf of SARI by HSE Health Protection Surveillance Centre
ISBN 978-0-9551236-6-5
Antimicrobial Resistance in IrelandA Strategy for the Control of S A R I

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
Contents Foreword 2 SECTION 1: RECOMMENDATIONS AND DEFINITIONS 3
• Summary of Recommendations 3 • Definitions 13 •ClinicalDefinitionsforCatheter-relatedInfection 13 •CDCSurveillanceDefinitions 14
SECTION 2: RATIONALE FOR RECOMMENDATIONS 16
1. Introduction 16
2. General Infection Prevention and Control Principles 19 2.1 Hand Hygiene 19 2.2 Aseptic Technique 19 2.3 Education of Healthcare Workers and Patients 19 3. Central Vascular Catheters (CVC) 21 3.1 Prevention of CVC Infection 21 3.1.1 Hand Hygiene and Aseptic Technique 21 3.1.2 Skin Asepsis 21 3.1.3 Maximal Barrier Precautions 22 3.1.4SelectionofCVC,InsertionSiteandCVCPlacement 23 3.1.5AntimicrobialOintments,LocksandProphylaxis 24 3.1.6 CVC Exit Site Care 26 3.1.7 CVC Replacement 27 3.1.8 CVC Care Bundles 29 3.2 Surveillance 30 3.2.1 Surveillance in Other Countries 30 3.2.2 Setting up Surveillance 30 3.2.3 Surveillance Infrastructure 31 3.2.4CaseDefinitionsandDenominators 31 3.2.5DataCollectionFormsandProtocol 32 3.2.6Examples–CalculationofDevice-associatedInfection 32 3.2.7FeedbackofSurveillanceResults 33 3.3ManagementofCVC-relatedInfection 34 3.3.1ManagementofCVCExitSiteInfection 34 3.3.2ManagementofTunnelInfection/PortAbscess 34 3.3.3ManagementofPositiveCVCTips 34 3.3.4ManagementofCRBSI 34 3.3.5CVCRemovalandGuidewireExchange 40 4. Peripheral Vascular Catheters (PVC) 42 4.1PreventionofPVCInfection 42 4.1.1HandHygiene,AsepticTechniqueandSkinAsepsis 42 4.1.2SelectionofPVCType 42 4.1.3SelectionofPVCSite 42 4.1.4ProcedureforPVCInsertion,PVCFixationandMaintenanceofPatency 43 4.1.5PVCRemovalandReplacement 43 4.1.6PVCCareBundles 44 4.2PVCInfection 45
5. Diagnosis of Catheter associated or related Infection 46 5.1ClinicalDiagnosis 46 5.2LaboratoryDiagnosis 46 6. Considerations for Specific Settings 51 6.1TheEmergencyDepartment 51 6.2 Haemodialysis 51 6.3CriticalCare 54

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-1-
SECTION 3: APPENDICES AND REFERENCE LIST 55 Appendix 1: Committee Membership and Acknowledgements 55 Appendix 2: Consultation Process 56 Appendix 3: Abbreviations 57 Appendix4: AnatomicalPointsofAccessforIntravascularCatheters 58 Appendix 5: Types of Intravascular Catheters 59 Appendix 6: Aseptic Technique 61 Appendix7: PatientInformationLeaflet 62 Appendix 8: CVC Insertion Procedure Guideline 63 Appendix 9: CVC Insertion Pack – Example of Contents 65 Appendix 10: CVC Insertion Checklist 66 Appendix 11: CVC Care Bundle 67 Appendix12: FormforCollectionofDenominatorDataforCRBSISurveillance 69
Appendix13: FormforCollectionofCRBSI–ClinicalandLaboratoryData 70
Appendix14: PVCInsertionProcedureGuideline 71
Appendix 15: Example of a Visual Infusion Phlebitis Score 72
Appendix 16: PVC Care Bundle 73
Reference List 76
Published by Health Protection Surveillance Centre25-27 Middle Gardiner StreetDublin1Tel: 01-8765300Fax:01-8561299
© Health Protection Surveillance Centre 2009ISBN 978-0-9551236-6-5

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-2-
ForewordThe Strategy for the Control of Antimicrobial Resistance in Ireland (SARI) National Committee •established a subcommittee to produce national guidelines on the prevention of intravascular catheter–relatedinfection.NominationswererequestedfromtheIntensiveCareSocietyofIreland(ICSI),InfectiousDiseasesSocietyofIreland(IDSI),IrishNephrologySociety(INA),InfectionPreventionSociety(IPS),IrishSocietyofClinicalMicrobiologists(ISCM),RoyalCollegeofSurgeonsinIreland(RCSI)FacultyofRadiologistsandtheSurveillanceScientistsAssociationofIreland(SSAI).Inaddition,individualswithaninterestinthefieldwereinvitedtoparticipateinthegroup.Themembershipofthesubcommitteeis outlined in Appendix 1.
The terms of reference for the group were to review international best evidence and to make •recommendationsfortheprevention,surveillance,diagnosisandclinicalmanagementofintravascularcatheter-relatedinfectioninIreland.ThecommitteefirstmeetinJuly2008.Membersagreedtheterms of reference as listed above. A draft document was sent for circulation to a wide range of professionalgroups(Appendix2)inFebruary2009.
Thisdocumentisaimedathealthcareprofessionalsandoutlinesrecommendationsfortheprevention,•surveillance,diagnosisandclinicalmanagementofintravascularcatheter-relatedinfectioninIreland.Abbreviations used in this document are outlined in Appendix 3.
This document represents the expert opinion of the sub-committee following a literature review •and consultative process. It was not possible for the sub-committee to grade the evidence available in the literature as outlined by the Scottish Intercollegiate Guidelines Network (SIGN) due to the heterogeneityofevidenceavailable,andotherworkcommitmentsofsub-committeemembers,whichprecluded a more detailed literature review.
Whileweacceptthatsomeaspectsoftherecommendationsmaybedifficulttoimplementinitiallydue•toalackoffacilitiesorinsufficientpersonnel,westronglybelievethattheseguidelinesrepresentbestpractice.
Wheretherearedifficulties,theseshouldbehighlightedtoseniormanagementofthehealthcare•facility,theHealthServicesExecutive(HSE)andtheDepartmentofHealthandChildren(DoHC)sothatmeasuresaretakentoensureimplementation,includingtheprovisionofappropriateresourcesandpersonnel.
The Committee recommends that these guidelines are reviewed and updated in 3-5 years.•

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-3-
Section 1: Recommendations and DefinitionsSuMMARy OF RECOMMENDATIONS A: GENERAL INFECTION PREVENTION AND CONTROL PRINCIPLESRecommendation 1:
Intravascular catheters should only be inserted when there is a clear clinical indication for their use. •Whentheclinicalindicationisnolongerpresent,thecathetermustberemoved.
Recommendation 2: Hand HygieneHand hygiene is the single most important procedure in the prevention of intravascular catheter-•associated or related infections. Hands must be decontaminated before and after accessing or dressing anintravascularcatheter.Palpationoftheinsertionsiteshouldnotbeperformedafterskinasepsis,unless aseptic technique is maintained.
Handscanbedecontaminatedbywashingwithanantimicrobialliquidsoapandwater,orifhandsare•physicallyclean,byanalcoholbasedhandrub.Handsthatarevisiblysoiledorcontaminatedwithdirtor organic material must be washed with liquid soap and water before using an alcohol hand rub.
Recommendation 3: Aseptic TechniqueAseptic technique should be used by all healthcare workers during insertion and maintenance of •intravascular catheters. Aseptic (no touch) technique is a term used to describe a technique that maintains asepsis and is non-touch in nature – the susceptible site should not come into contact with any item that is not sterile. (Appendix 6)
Followinghandhygiene,cleanglovesandanaseptic(notouch)techniqueshouldbeusedwhen•accessinganintravascularcatheterwhentheluer*lockisnotdisconnectedfromthecatheter(e.g.,intravenousdrugadministration,bloodsamplingorconnectingordisconnectingintravenousfluids).
Sterile gloves in addition to aseptic (no touch) technique should be used when a luer needleless •connectorisdisconnected(e.g.,manipulationofacatheter,haemodialysis).
Sterile gloves and aseptic (no touch) technique must be used for changing total parenteral nutrition •(TPN) and central venous catheter (CVC) insertion site dressing change.
Each healthcare facility should develop and implement a standardised protocol for aseptic (no touch) •technique.
*Luer connectionsystemsarethestandardwayofattachingsyringes,catheters,hubbedneedles,IVtubes,andsoontoeachother.Theyconsistofroundmaleandfemaleinterlockingtubes,theycaneitherbe‘luerslip’,orcanhaveanadditionalouterrimofthreadingcalleda‘luerlock’,allowingthemtobemoresecure.
Recommendation 4: Education of Healthcare Workers and PatientsInfectionpreventionandcontrol,includingtheprinciplesofpreventionofcatheter-relatedbloodstream•infection(CRBSI),mustbeanessentialcomponentofthecorecurriculumoftrainingprogrammesofmedical and nursing students at both undergraduate and postgraduate level.
Followingtraining,HCWsmustbeassessedanddocumentedascompetentinusingandconsistently•adhering to appropriate infection prevention and control practices when inserting or maintaining intravascular catheters. Ideally a national competency document would ensure standardisation of trainingandallowforinterchangebetweenhealthcarefacilities(duetostaffmovement);however,thiswouldneedanappropriateinfrastructureintermsofprojectmanagement,ITandeducation.
Onlycompetent,trainedstaff(ortrainingstaffsupervisedbycompetentstaff)shouldinsertand•maintain intravascular catheters.
Beforedischargefromahealthcarefacility,patientswithanintravascularcatheterandtheircarers•mustbeeducatedbyamember(s)ofthepatient’sclinicalmultidisciplinaryteamwithrespecttotheprocedures necessary to safely manage their catheter and to prevent infection. This should include educationonthesignsofinfectionandarelevantinformationleaflet.(Appendix7)
Ongoingqualityassurance/improvement,riskmanagementandsurveillanceprogrammesshould•beinplacetomonitortheincidenceofinfectionassociatedwithintravascularcatheters,toevaluatetheresponsetopatientandstaffeducation,andtoidentifyfutureeducationalneeds.Monitoringcompliance with care bundles are important process measures for evaluation of a CRBSI preventative

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-4-
programme.(Appendix10,11and16)Theseresultsshouldbereviewedandfedbacktorelevantward areas and senior management at regular intervals.
B: CENTRAL INTRAVASCULAR CATHETERS (CVC)B1: PREVENTION OF INFECTION ASSOCIATED WITH CVCs
Recommendation 5: Skin AsepsisIndividual single use sachets of antiseptic solution or individual packages of single use antiseptic-•impregnated swabs or wipes should be used to disinfect the CVC insertion site. Skin must be allowed toairdrypriortofurthermanipulation.Iftheskinisvisiblydirty,itshouldbewashedwithsoapandwater prior to skin asepsis.
In adults and children • ≥2months(assumingnormalgestationatbirth),asinglepatientuseapplicationof alcoholic chlorhexidine gluconate solution (preferably 2% chlorhexidine gluconate in 70% isopropyl alcohol if compatible with the CVC) should be used and must be allowed to air dry;
o ForskindisinfectantpriortotheinsertionofaCVC.
o To disinfect the CVC insertion site during dressing changes.
o Prior to accessing the CVC hub or injection port.
0.5-1% chlorhexidine is the optimal range for neonatal (< 2 months) skin asepsis; however randomised •controlled trials are required to clarify this range.
Anaqueoussolutionof2%chlorhexidinegluconateshouldbeusediftheCVCsmanufacturer’s•recommendations prohibit the use of alcohol with their product.
Single patient use application of alcoholic povidone-iodine solution should be used for patients with a •history of chlorhexidine sensitivity.
HCWshouldensurethatCVCsitecareiscompatiblewithCVCmaterials(e.g.,tubing,hubs,•injectionports,luerneedlelessconnectorsandextensions)andcarefullycheckcompatibilitywiththemanufacturer’srecommendations.ThisassessmentmustbeperformedinadvanceofpurchasingtheCVC/materials. If the CVC/materials are incompatible with 2% chlorhexidine gluconate in 70% isopropyl alcohol,thereshouldbeaclearclinicalbenefittopurchasingtheCVC/materials.Ifnot,analternativeCVC/materials should be sought.
Atthetimeofwriting,itisrecognisedthattherearenolicensedpreparationscontainingchlorhexidine•2%/isopropyl alcohol 70% designed for skin asepsis prior to IV catheter insertion commercially availableinIreland,despitetheiravailabilityinotherjurisdictions.However,clinicaltrialdataandinternationally recognised best practice leads us to strongly advocate the use of products containing this particular combination for skin asepsis. The decision to use unlicensed products should be made in-house,inaccordancewitheachhealthcarefacility’smedicinesmanagementstructuresandpoliciesforthe use of unlicensed medicines.
Recommendation 6: Maximal Barrier PrecautionsMaximal barrier precautions are recommended for insertion of all CVCs and when exchanging a CVC •overaguidewireandmustbeusedbytheoperatorandanypersonwhoentersthesterilefieldtoassistin the procedure.
These precautions include:•
o Strict compliance with hand hygiene by the operator placing the CVC and staff assisting in the procedure.
o Covering the patient with sterile drape(s) from head to toe with an appropriate opening for the site of insertion.
o Theoperatorandstaffassistingintheprocedurewearingthefollowing:cap,(shouldcoverallhair),mask(shouldcoverthenoseandmouthtightly),protectiveeyewear,sterilegownandsterile gloves.

-5-
Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
Recommendation 7: CVC Insertion ProtocolsIt is recommended that each healthcare facility has a written CVC insertion procedure guideline that is •updated regularly. (Appendix 8)
CVC insertion packs containing all the necessary items for CVC insertion are recommended. •(Appendix 9)
It is recommended that a CVC checklist is used to ensure adherence to infection prevention and •control practices at the time of CVC insertion. (Appendix 10) This checklist is used to ensure and document compliance with aseptic technique. CVC insertion should be observed by a HCW who has received appropriate education to ensure that aseptic technique is maintained. The observer will assist inidentifyingbreachesinaseptictechnique,whichifobservedshouldresultintheprocedurebeingaborted and restarted.
Recommendation 8: Selection of CVC Type and Insertion Site • Patients should be assessed prior to CVC insertion as to the appropriate number of lumens that are likelytoberequired.Ifamulti-lumenCVCisused,oneportshouldbeidentifiedanddesignatedexclusively for TPN (if required).
• Inselectinganappropriateinsertionsite,therisksforinfectionshouldbeassessedagainsttherisksofmechanical complications.
• Forpatientslikelytorequirelongtermrenalreplacement,earlyconsiderationofthefuturevascularaccessplanisessentialpriortoCVCinsertion(includingfuturearteriovenous(AV)fistulasite).Inthesepatients the subclavian site should be avoided because of the frequent development of subclavian stenosis which interferes with long term provision of vascular access.
• Portableultrasoundimagingmaybeconsideredforselectedpatientsathighriskofcomplications(e.g.,knownvascularanomaly)orwherevascularaccessislikelytobedifficult(e.g.,children).
• WiththeexceptionofperipherallyinsertedCVCs(PICCs),patientsthatrequireshort-termCVCaccess(< 2 weeks) should have a non tunnelled CVC inserted.
• Forpatientsrequiringregularorcontinuousaccess,atunnelledCVCispreferred.
• Theuseofimplantableportsisrecommendedforpatientswhorequirelong-term,intermittentvascularaccess.
• Inadults,antiseptic/antimicrobialimpregnatedCVCsmaybeconsideredinthefollowingcircumstances:
o Units or patient populations that have a high CRBSI rate despite compliance with basic CRBSI prevention practices.
o Patients with limited venous access and a history of recurrent CRBSI.
o PatientsthatareatheightenedriskforseveresequelaefromaCRBSI(e.g.,patientswithrecentlyimplantedintravasculardevices,suchasaprostheticheartvalveoraorticgraft).
Recommendation 9: Prophylaxis: Antimicrobial Ointments, Antiseptic and Antimicrobial LocksThe application of antimicrobial ointment to the CVC placement site prior to insertion is not •recommended.
AntimicrobiallocksolutionsmaybeusedforthepreventionofCRBSIincertainsubgroupsofpatients,•notablythosewhorequirelongtermvascularaccess(e.g.,haemodialysis,shortbowelsyndrome)andwho have had multiple episodes of CRBSI and have developed these infections despite strict adherence to all other preventative measures. Ongoing surveillance for the emergence of resistant organisms should be performed where antimicrobial lock therapy is used.
The decision to use antimicrobial lock prophylaxis and the choice of antimicrobial agent to be used will •needtobedecidedonaindividualpatientbasis,basedonthepreviouspositivemicrobiologyandinconjunction with the medical microbiologist/infectious diseases physician.
The administration of prophylactic antimicrobials prior to CVC insertion is not recommended.•

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-6-
Recommendation 10: CVC Care and MaintenanceIt is recommended that each healthcare facility has a written CVC care and maintenance guideline that is •updated regularly/as new evidence becomes available.
Handhygiene,aseptictechniqueanddecontaminationoftheCVChub/injectionportshouldbe•performedasinRecommendations2,3and5.
ManipulationsoftheCVC,includingreplacementofdressingsshouldbedocumented.•
Asterile,transparentsemipermeabledressingshouldbeusedtocovertheCVCinsertionsiteandshould•be changed every seven days or sooner if it is no longer intact or if moisture collects under the dressing. Ifasterilegauzedressingisused(e.g.,ifapatienthasprofuseperspirationoriftheinsertionsiteisbleeding or oozing) it should be replaced by a transparent semipermeable dressing as soon as possible.
DressingsusedontunnelledorimplantedCVCinsertionsitesshouldbereplacedeverysevendaysuntil•theinsertionsitehashealed,unlessthereisanindicationtochangethemsooner.
Asterile0.9%sodiumchloridesolutionshouldbeusedtoflushandlockCVClumens.When•recommendedbythemanufacturer,implantedportsoropened-endedCVClumensshouldbeflushedandlockedwithheparinsodiumflushsolutions.Routineuseofsystemicanticoagulantsisnotrecommended to prevent CRBSI. The committee have omitted heparin dosage information in these guidelines. This is because policy may differ between healthcare facilities and patient groups. It is suggestedthatonadoptionoftheseguidelines,theuseofheparinissupportedwithin-houseguidelineswhichtakeintoaccountdosageandproductformulation.Inaddition,specialprovisionshouldbemadeforpatientswithahistoryofheparininducedthrombocytopenia,asheparinshouldnotbeusedinsuchascenario.
Recommendation 11: Daily Review of CVCsAllCVCsshouldberevieweddaily,documentedasreviewedandthosethatarenolongerclinically•indicated promptly removed.
Theinsertionsiteshouldbeexamineddailyfordrainage,tenderness,pain,redness,swelling,suture•integrityandCVCpositionandallfindingsdocumented.Siteappearanceshouldnotbeusedastheonlyindicatorofinfection.Thepatientshouldalsobeexaminedforfeverorothersignsofsepsis(e.g.,tachycardia,tachypnoea,hypotension).
Patients should be encouraged (where possible) to report any changes in their CVC site or any new •discomfort.
Patients transferring from other healthcare facilities with a CVC • in situ must have the device reviewed upon arrival for evidence of any infectious or mechanical complications.
Recommendation 12: CVC ReplacementIftheCVCisnolongeressential,itshouldberemovedpromptly.•
Management of CVC replacement in the context of CVC infection is outlined in Recommendation 16. •
IftheCVCisfractured,itshouldbereplacedandanewCVCinsertedideallyatadifferentsite.•
Becausebreachesinsteriletechniquearemorelikelyduringemergencyprocedures,CVCsinserted•during a medical emergency must be replaced as soon as possible.
Routine replacement of CVCs that are functioning and have no evidence of causing local or systemic •complications (including scheduled guidewire exchanges of CVCs) as a method to reduce CRBSI is not recommended.
Guidewire techniques should not be used to replace CVCs in patients suspected of having CVC infection. •Guidewire assisted CVC exchange to replace a malfunctioning CVC or to exchange an existing CVC should be used only if there is no infection at the CVC site or no suspicion of CRBSI. If after a guidewire exchange,investigationsrevealCRBSI,thenewlyinsertedCVCshouldberemovedandifstillrequiredreinsertedatadifferentsite.InselectedpatientswithtunnelledhaemodialysisCVCsandbacteraemia,CVCexchangeoveraguidewire,incombinationwithantibiotictherapy,mightbeanalternativeasasalvage strategy in patients with limited venous access.
Forguidewireexchanges,thesamemeticulousaseptictechniqueanduseoffullsterilebarriersare•mandatory as outlined in Recommendations 2-3 and 5-9.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-7-
B 2: SURVEILLANCE OF INFECTION ASSOCIATED WITH CVCs Recommendation 13: CRBSI SurveillanceHealthcaremanagersmustsupportsurveillanceactivities,includingsurveillanceofCRBSI.•
Surveillance must start and end with the patient in order to improve patient care. A CRBSI surveillance •programme should be introduced in an healthcare facility as dictated by the specialities and requirementsofthathealthcarefacilityandtheresourcesavailableforsurveillance,todeterminehealthcareassociated(HCA)CRBSIrates,monitortrendsinrates,andassistinidentifyinglapsesininfectionpreventionandcontrolpractices.AreasthatmaybeinvolvedincludeICU/HDU,dialysisunits,haematology/oncologyunits,TPNservicesandinterventionalradiologyunits.Thecommitteehave provided sample forms for CRBSI surveillance. (Appendices 12-13) These forms represent a template and can be used to guide healthcare facilities in the design of their own forms. Each healthcare facility may wish to include additional questions in the template form so that local needs can be met.
A local multidisciplinary steering committee should be established with representatives from the •relevantarea(s)inwhichsurveillanceistocommence(e.g.,ICU,haemodialysis,medicalmicrobiology,infectiousdiseases,infectionpreventionandcontrolandseniormanagement)tohelpdrivethesurveillanceproject,encouragecomplianceandadvisetherelevantarea(s)andhealthcarefacilitymanagement based on surveillance results.
CRBSI rates must be fed back to the relevant area(s) and healthcare facility management on a regular •basis,ideallymonthly,butatleastquarterly.
All clusters of HCA CRBSI and all episodes of HCA CRBSI due to S. aureus must be investigated.•
The introduction of new intravascular catheters should be monitored for an increase in the occurrence •of infection.
Recommendation 14: Case Definitions for CRBSI Surveillance CRBSIprotocolsmustbestandardisedandadheretootherinternationalframeworks(e.g.,CDC/•HELICS)forcomparativeanalysisofCRBSIincidencerates.
Toenableinternationalcomparisonsofsurveillancedata,itisrecommendedthatstandardcases•definitionsareemployed.IntheabsenceofanagreedEuropeanCRBSIcasedefinition,itisrecommendedthatCDCcasedefinitionsareemployed.1
Recommendation 15: Denominators for SurveillanceThe CRBSI rate should be expressed as the number of CRBSIs per 1000 CVC days.•
B3: MANAGEMENT OF CVC-RELATED INFECTIONRecommendation 16:ManagementofCVC-relatedinfectiondependsonthetypeofCVCinvolved,theinfectingorganism,•and the associated complications.
WhenaCVC-relatedinfectionisdocumentedandaspecificpathogenisidentified,systemic•antimicrobial therapy should be adjusted according to antimicrobial susceptibility.
Durationoftreatmentwilldependontheorganismidentified,presenceofbacteraemia,presenceof•complications and whether the line has been removed.
Whendenotingdurationofantibiotictherapyfortreatmentofbloodstreaminfection(BSI),dayoneis•thefirstdayonwhichnegativebloodculturesareobtained.
Exit site infection: Empiric therapy with an appropriate antibiotic should be commenced after blood •cultures are taken and involvement of the tunnel/port pocket outruled (if a tunnelled CVC is present). CVC removal is recommended if antibiotic treatment fails. Exchange of the CVC over a guidewire inthepresenceofanexitsiteinfectionisnotrecommended.Ifbloodculturesarepositive,thentreatment for CRBSI is indicated.
Tunnel infection: Successful therapy of tunnel infections without CVC removal is very unlikely. In •theabsenceofbacteraemia7-10daysofantibioticsmaysuffice.Ifassociatedwithbacteraemia,thepatient should be considered to have complicated CRBSI.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-8-
CRBSI: •
o InpatientswithBSIandanindwellingCVC,itisimportanttoruleoutothersourcesofinfectionto avoid unnecessary CVC removal. Where a patient has a single blood culture for coagulase-negative Staphylococcus spp., additional blood cultures (peripheral and through the CVC) should be obtained.
o Empiricintravenousantimicrobialtherapyshouldbeconsidered,afterculturesareobtained.Ingeneral a glycopeptide antibiotic is recommended for empirical therapy in health care settings in which MRSA is prevalent. Additional gram negative coverage is indicated in patients who are neutropenic or severely ill with sepsis or for suspected infections involving femoral catheters. Antifungal agents (choice depending on local susceptibility patterns) should be considered for empirical treatment when fungaemia is suspected.
o PatientswithcomplicatedCRBSIwillrequire4-6weeksofIVantibiotics.Thisincludespatientswithsuppurativethrombophlebitis,endocarditis,metastaticseeding,orpersistentbacteraemia(>72 hours despite appropriate antibiotics) after removal of the catheter.
o ManagementofCRBSIwhentheinfectingorganismisknownisoutlinedinFigures1and2.
o Repeat blood cultures to document clearance of bacteraemia are recommended.
o In uncomplicated CRBSI due to organisms other than S. aureus, P. aeruginosa, fungi,mycobacteria, Micrococcus spp., Proprionobacterium or Bacillus spp., CVC salvage may be attempted in situations where there is limited vascular access. If bacteraemia is persistent (>72 hours) this should prompt reassessment of the ability to salvage the CVC. Antibiotic lock therapy (ALT)shouldbeusedwhenCVCsalvageisbeingattempted,howeverthisshouldalwaysbeadministered with systemic antibiotic therapy.
Complicated infection
Uncomplicated infection
Non-tunnelled CVC CRBSI
Remove CVC and
treat with systemicantibiotic for 4-6
weeks; (6-8 weeks for osteomyelitis)
Coagulase-negative staphylococci
(except S. lugdunensis)
S. aureus & S. lugdunensis
Enterococcus spp.
Gram negative bacilli
Candida spp.
o Remove CVC* and treat with systemic antibiotic for 5-7 days
o If CVC is retained, treat with systemic antibiotic (+/- antibiotic lock) therapy for 10-14 days
Remove CVC and
treat with systemic
antibiotic for minimum 14
days
Remove CVC and
treat with systemic
antibiotic for 7-14 days
Remove CVC and
treat with systemic
antibiotic for7-14 days
Remove CVC and
treat with antifungal therapy for 14 days after
first negative blood culture
Prolonged or persistent bacteraemia/fungaemia after CVC removal (i.e., occurring >72hours after removal)Evidence of endocarditis Evidence of suppurative thrombophlebitisClinical evidence of a metastatic focus of infectionOsteomyelitis
BSI and fever resolves within 72 hours in a patient without an active malignancy or immunosuppression who
has no other intravascular devices and no evidence of endocarditis or suppurative thrombophlebitis
*Infections may resolve in patients without intravascular/orthopaedic prosthesis/devices with CVC removal alone (and no antibiotic
therapy).BloodculturesshouldberepeatedafterCVCwithdrawaltoconfirmtheabsenceofbacteraemia.
Figure 1: Management of CRBSI associated with non-tunnelled CVCs.
Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-9-
Tunnel infection, port
abscess
Septic thrombosis, endocarditis, osteomyelitis
Coagulase-negative
staphylococci (except
S. lugdunensis)
S. aureus &
S. lugdunensis
Enterococcus spp.
Gram negative bacilli
Candida spp.
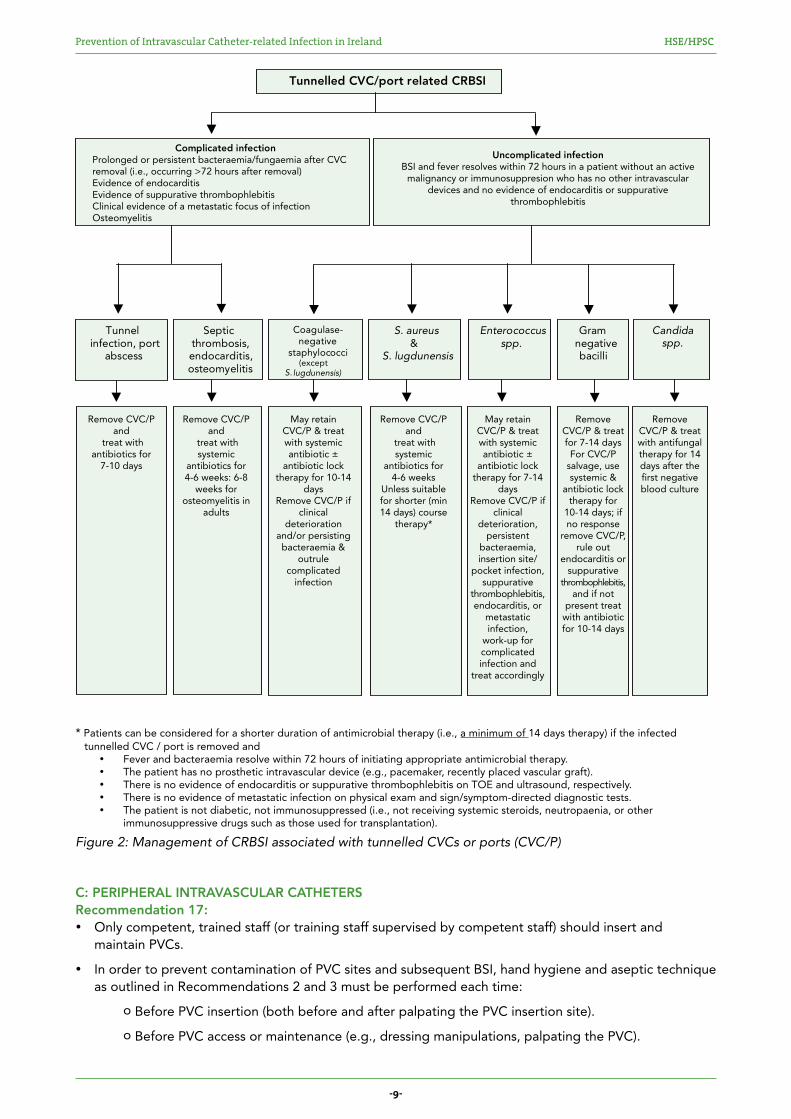
Tunnelled CVC/port related CRBSI
Complicated infection Prolonged or persistent bacteraemia/fungaemia after CVC removal (i.e., occurring >72 hours after removal)Evidence of endocarditis Evidence of suppurative thrombophlebitisClinical evidence of a metastatic focus of infectionOsteomyelitis
Uncomplicated infection BSI and fever resolves within 72 hours in a patient without an active
malignancy or immunosuppresion who has no other intravascular devices and no evidence of endocarditis or suppurative
thrombophlebitis
Remove CVC/P and
treat with antibiotics for
7-10 days
Remove CVC/P and
treat with systemic
antibiotics for 4-6 weeks: 6-8
weeks for osteomyelitis in
adults
May retain CVC/P & treat with systemic antibiotic ±
antibiotic lock therapy for 10-14
daysRemove CVC/P if
clinical deterioration
and/or persisting bacteraemia &
outrule complicated
infection
Remove CVC/P and
treat with systemic
antibiotics for 4-6 weeks
Unless suitable for shorter (min 14 days) course
therapy*
May retain CVC/P & treat with systemic antibiotic ±
antibiotic lock therapy for 7-14
daysRemove CVC/P if
clinical deterioration,
persistent bacteraemia, insertion site/
pocket infection, suppurative
thrombophlebitis, endocarditis, or
metastatic infection,
work-up for complicated infection and
treat accordingly
Remove CVC/P & treat for 7-14 daysFor CVC/P
salvage, use systemic &
antibiotic lock therapy for
10-14 days; if no response
remove CVC/P, rule out
endocarditis or suppurative
thrombophlebitis, and if not
present treat with antibiotic for 10-14 days
Remove CVC/P & treat with antifungal therapy for 14 days after the first negative blood culture
* Patientscanbeconsideredforashorterdurationofantimicrobialtherapy(i.e.,a minimum of 14daystherapy)iftheinfected tunnelled CVC / port is removed and
Feverandbacteraemiaresolvewithin72hoursofinitiatingappropriateantimicrobialtherapy.•Thepatienthasnoprostheticintravasculardevice(e.g.,pacemaker,recentlyplacedvasculargraft).•ThereisnoevidenceofendocarditisorsuppurativethrombophlebitisonTOEandultrasound,respectively.•There is no evidence of metastatic infection on physical exam and sign/symptom-directed diagnostic tests.•Thepatientisnotdiabetic,notimmunosuppressed(i.e.,notreceivingsystemicsteroids,neutropaenia,orother•immunosuppressive drugs such as those used for transplantation).
Figure 2: Management of CRBSI associated with tunnelled CVCs or ports (CVC/P)
C: PERIPHERAL INTRAVASCULAR CATHETERSRecommendation 17: Onlycompetent,trainedstaff(ortrainingstaffsupervisedbycompetentstaff)shouldinsertand•maintain PVCs.
InordertopreventcontaminationofPVCsitesandsubsequentBSI,handhygieneandaseptictechnique•as outlined in Recommendations 2 and 3 must be performed each time:
o Before PVC insertion (both before and after palpating the PVC insertion site).
o BeforePVCaccessormaintenance(e.g.,dressingmanipulations,palpatingthePVC).

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-10-
Followinghandhygiene,cleanglovesandanaseptictechniquemustbeemployed.Handhygienemustalso be performed immediately after removing gloves and after each episode of patient care. All sharps must be disposed of carefully into an approved sharps container.
In adults and children • ≥2months(assumingnormalgestationatbirth),asinglepatientuseapplicationof alcoholic chlorhexidine gluconate solution (preferably 2% chlorhexidine gluconate in 70% isopropyl alcohol if compatible with the PVC) should be used and allowed to air dry;
o ForskindisinfectionpriortotheinsertionofaPVC.
o To disinfect the PVC insertion site during dressing changes.
o Prior to accessing the PVC hub.
0.5-1%chlorhexidineistheoptimalrangeforneonatal(<2months)skinasepsis;however,randomised•controlled trials are required to clarify this range.
The PVC site should not be re-palpated after skin asepsis.•
Select the PVC and insertion site with the lowest risk for complications for the anticipated type and •duration of IV therapy.
Asterile,transparentsemipermeabledressingshouldbeusedtocoverthePVCinsertionsite.Routine•dressing change is not recommended unless the dressing is no longer intact or moisture collects under the dressing.
Whenadherencetoaseptictechniquecannotbeensured(i.e.,whenPVCsareinsertedduringamedical•emergency),thePVCshouldbereplacedassoonaspossible.
Patients transferring from other healthcare facilities with a PVC• in situ should have this device reviewed upon arrival and preferably replaced unless clinically contraindicated.
AllPVCsshouldberevieweddaily,andthosethatarenolongerneededshouldbepromptlyremoved.•Detailsofthereviewandthedecisiontoremoveornotshouldbeclearlydocumented.
All PVCs must be removed promptly when there is clinical evidence that the PVC is infected. •
Inadults,PVCreplacementshouldbeconsideredevery72-96hourstopreventphlebitis.Where•peripheralvenousaccessislimited,thedecisiontoleaveaPVCindwellingbeyond96hoursshoulddependonassessmentofthePVC,skinintegrity,lengthandtypeofprescribedtherapy.Thisassessment should be clearly documented.
Routine replacement of PVCs in children is not recommended. PVCs should be replaced if complications •such as phlebitis occur.
D: DIAGNOSIS OF INTRAVASCULAR CATHETER-RELATED INFECTIONRecommendation 18:Clinicalfindingsaloneareunreliableforestablishingadiagnosisofintravascularcatheter–related•infection,becauseoftheirpoorspecificityandsensitivity.
Two sets of blood cultures should be taken using aseptic technique from all patients with suspected •intravascularcatheter-relatedinfection.ForCVCseitherthroughtheCVCandperipherallyorthroughdifferent lumens of the CVC if blood cultures cannot be drawn from a peripheral vein. Blood cultures should be taken prior to initiation of antimicrobial therapy. The bottles should be appropriately marked toreflectthesitetheculturesweredrawnfrom.
Routineculturingofintravascularcathetertipsisnotrecommended.However,CVCtipsshouldalways•be sent for culture if the CVC is removed and catheter-related infection is suspected. It is essential that every CVC is removed using aseptic technique.
Forsuspectedpulmonaryarterycatheterinfection,theintroducertipshouldbecultured.•
IfanimplantableportisremovedforsuspectedCRBSI,thecathetertipandtheportshouldbesentfor•qualitative culture of the port reservoir contents.
Ifpusispresentatthecatheterexitsite,thesitemustbeswabbedforcultureandremovalofthe•catheter considered. (Recommendations 16 and 17)

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-11-
Growthof>15CFUfromasegmentofthecathetertipbysemiquantitative(roll-plate)cultureorgrowth•of >102 CFUfromacatheterbyquantitative(sonication)brothculturereflectscathetercolonisation.AllsuchisolatesfromCVCtipsarepotentiallysignificantandshouldbeidentifiedtogenuslevelandtospecieslevel,ifclinicallyindicated.Antimicrobialsusceptibilityshouldbeperformedonallclinicallysignificantisolates.
The choice of the precise microbiological method for CRBSI diagnosis may vary locally and should •be made according to technical availability and after discussion between clinicians and medical microbiologists.Inaddition,economicconsiderations,suchascost-effectiveness,mayalsobetakenintoaccount.
Blood culture results that are positive for• S. aureus, coagulase-negativestaphylococci,or Candida spp., intheabsenceofanyotheridentifiablesourceofinfection,shouldincreasethesuspicionforCRBSI.
FordiagnosisofCRBSIthefollowingcriteriashouldbemet:Bacteraemiaorfungaemiainapatientwho•has an intravascular device and >1positivebloodcultureobtainedfromtheperipheralvein,clinicalmanifestationsofinfection(e.g.,fever,chills,and/orhypotension),andnoapparentsourceforBSI(withthe exception of the catheter).
One of the following should be present:
o Apositiveresultofsemiquantitative(>15CFU/cathetersegment)orquantitative(>102CFU/cathetersegment)catheterculture,wherebythesameorganism(species)isisolatedfromacatheter segment and a peripheral blood culture.
o Simultaneousquantitativeculturesofbloodwitharatioof>3:1CFU/mlofblood(catheterversus peripheral blood); differential time to positivity (growth in a blood culture drawn through catheter hub is detected by an automated blood culture system at least 2 hours earlier than a simultaneouslydrawn,peripheralbloodcultureofequalvolume).
E: PREVENTION OF CRBSI IN SPECIFIC SETTINGS
Recommendation 19: The Emergency DepartmentOnly appropriately trained staff (or trainee staff supervised by competent staff) should insert percutaneous •CVCsinEmergencyDepartments.(Recommendation4)
There should be strict adherence to hand hygiene, skin asepsis and aseptic insertion technique.•(Recommendations 2-3 and 5-9)
Ultrasound-guided central venous access should be considered.•
IntravascularcathetersinsertedintheEmergencyDepartmentshouldgenerallyberemovedorreplaced•as early as is practical.
Accurate documentation and record keeping is required for all instances of CVC insertion in the Emergency •Department.ACVCInsertionChecklist(Appendix10)maybeusedtoensurepatientsafety,auditingofclinicalpractice,andthetrackingofinfectivecomplications.
Recommendation 20: HaemodialysisHaemodialysis patients should whenever possible and practical have a primary arteriovenous •(AV)fistulacreatedforvascularaccess.IfitisnotpossibletoachieveafunctioningAVfistulaapolytetrafluoroethylene(PTFE)graftisingeneralpreferabletolongtermcuffedcatheters.
Renal units need to have adequate access to vascular surgeons in order to ensure the timely creation of •primary vascular access.
PatientswithprogressiverenalfailureshouldhaveaprimaryAVfistulacreatedwhentheeGFRis•between17and12aimingtostartsuchpatientswiththeirfirstdialysisthroughafunctioningfistula.
Eachunitshouldkeeprecordsofprimaryfistulaprevalence,PTFEgraftprevalenceandcuffedcatheter•prevalence.
Units should review bacteraemia rates for patients with and without catheters on a regular basis. When •an episode of bacteraemia develops in a dialysis patient a root cause analysis should be undertake to identifythesourceofinfectionandpotentiallymodifiableriskfactors.
AllpatientsshouldbescreenedforprevalenceofMRSAcolonisationregularly(e.g.,threemonthly)and•

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-12-
patients managed as per national guidelines.2
WhenCVCinfectionissuspectedinhaemodialysispatients,twosetsofbloodculturesshouldbetaken•usingaseptictechnique(eitherthroughtheCVCandperipherally,orthroughdifferentlumensoftheCVC if peripheral blood cultures cannot be taken). Peripheral blood cultures should be obtained from vesselsnotintendedforfutureuseincreatingadialysisfistula.Whenaperipheralbloodculturecannotbeobtained,bloodculturesshouldbedrawnduringhaemodialysisfrombloodlinesconnectedtotheCVC.
Empiric antibiotic therapy can be discontinued in patients with suspected CRBSI if both sets of blood •culturesarenegativeandnoothersourceofinfectionisidentified.Ifaperipheralbloodculturecannotbeobtainedandnoclinicalevidenceforanalternatesourceofinfection,thenapositivecatheter-drawnblood culture in a symptomatic haemodialysis patient should lead to continuation of antimicrobial therapy for possible CRBSI.
The infected CVC should be removed in patients with haemodialysis CRBSI due to • S. aureus, Pseudomonas or Candida spp. and a temporary (non-tunnelled catheter) inserted into another anatomical site. A long-term haemodialysis catheter can be placed once repeat blood cultures are negative. Guidewire exchange is recommended only if no alternative sites are available for CVC insertion.
ForCRBSIduetootherpathogens(e.g.,gramnegativebacilliotherthan• Pseudomonas spp. or coagulase-negativestaphylococci),apatientcanbestartedonempiricintravenousantibioticswithoutimmediate catheter removal (provided the patient is clinically stable). If symptoms persist or there evidenceofametastaticinfection,thecathetershouldberemoved.
Surveillance blood cultures should be obtained one week after completing an antibiotic course for •CRBSIifthecatheterhasbeenretained.Ifthebloodculturesarepositive,thecathetershouldberemovedandanew,long-termdialysiscathetershouldbeplacedafterarepeatbloodculturesarenegative.
F: IMPLEMENTION OF THESE GUIDELINESRecommendation 21: Responsibility for the implementation of these guidelinesPreventionofhealthcare-associatedinfection(HCAI)shouldbeprioritisedbytheDepartmentofHealth•andChildren(DoHC),theHealthServicesExecutive(HSE)andallhealthcarestaffinordertoimprovepatientcareandsafetyandtoreduceallHCAI,includingCRBSI.
Implementation of the National Standards for the Prevention and Control of HCAI• 3 will be a key aspect of the prevention and control of intravascular catheter-related infection. Standard 8 (invasive medical device-relatedinfection)outlinesthespecifickeycriteriathatwillbeassessedinthisregard.
The following infrastructural requirements are recommended to institute a programme to prevent •CRBSI:
o An adequately staffed infection prevention and control programme responsible for identifying patientswithCRBSI,includingasurveillancecoordinatorwithappropriateadministrativesupport.
o Information technology to collect and calculate catheter-days as a denominator for computing rates of CRBSI and patient-days to allow calculation of CVC utilisation; Catheter-days from information systems should be validated against a manual method.
o Resources to provide appropriate education and training.
o Adequate laboratory support for timely processing of specimens and reporting of results.
Implementation of these guidelines may require ring-fenced funding to assist healthcare facilities to •meettheserecommendations,specificallysurveillance,laboratory,infectionpreventionandcontrolinfrastructure and personnel.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-13-
Definitions
Clinical Definitions for Catheter-related Infections4
Definition
Catheter Colonisation
Significantgrowthofoneormoremicroorganismsinaquantitativeorsemiquantitativecultureofthecathetertip,subcutaneouscathetersegment,orcatheterhub(Section5)
Phlebitis
Indurationorerythema,warmth,andpainortendernessalongthetract of a catheterised or recently catheterised vein
Exit site InfectionO Microbiological Exudate at catheter exit site yields a microorganism with or without
concomitant bloodstream infection (BSI)
O Clinical Erythema,induration,and/ortendernesswithin2cmofthecatheterexit site; may be associated with other signs and symptoms of infection,suchasfeverorpurulentdrainageemergingfromtheexitsite,withorwithoutconcomitantBSI
Tunnel Infection
Tenderness,erythema,and/orinduration>2cmfromthecatheterexitsite,alongthesubcutaneoustractofatunnelledcatheter,withor without concomitant BSI
Pocket Infection
Infectedfluidinthesubcutaneouspocketofatotallyimplantedintravasculardevice;oftenassociatedwithtenderness,erythema,and/or induration over the pocket; spontaneous rupture and drainage,ornecrosisoftheoverlyingskin,withorwithoutconcomitant BSI
Bloodstream Infection
O Infusate-related Concordant growth of a microorganism from infusate and cultures of percutaneously-obtained blood cultures with no other identifiablesourceofinfection

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-14-
CDC Surveillance Definitions1
1. Laboratory-Confirmed Primary Bloodstream Infection (LCBI)
Laboratoryconfirmedbloodstreaminfection(LCBIcriteria1and2)maybeusedforpatientsofanyage,includingpatients≤1yearofage.LCBImustmeetatleastoneofthefollowingcriteria:
Criteria 1: Patient has a recognised pathogen cultured from one or more blood cultures and Organism cultured from blood is not related to an infection at another site.
Criteria 2: Patient has at least one of the following signs or symptoms: fever (>38oC),chills,orhypotensionand Signs and symptoms and positive laboratory results are not related to an infection at another site and Commonskincontaminant(i.e.,diphtheroids[Corynebacteriumspp],Bacillus[notB anthracis]spp,Propionibacteriumspp,coagulasenegativestaphylococci[includingS. epidermidis],viridansgroupstreptococci,Aerococcus spp,Micrococcus spp) is cultured from two or more blood cultures drawn on separate occasions.
Criteria 3: Patient ≤ 1 year of age has at least one of the following signs or symptoms: fever (>38oC,rectal),hypothermia (37oC,rectal),apnoea,orbradycardiaand Signs and symptoms and positive laboratory results are not related to an infection at another site and Commonskincontaminant(i.e.,diphtheroids[Corynebacterium spp],Bacillus[notB anthracis]spp,Propionibacterium spp,coagulasenegativestaphylococci[includingS. epidermidis],viridansgroupstreptococci,Aerococcusspp,Micrococcus spp) is cultured from two or more blood cultures drawn on separate occasions.
Notes In criterion 1:
Thephrase‘oneormorebloodcultures’meansthatatleastonebottlefromblooddrawnisreportedbythelaboratoryashaving•grownorganisms(i.e.,isapositivebloodculture).Theterm‘recognisedpathogen’doesnotincludeorganismsconsideredcommonskincontaminants(seecriteria2and3foralist•of common skin contaminants). A few of the recognized pathogens are • Staphylococcus. aureus,Enterococcusspp,Escherichia. coli,Pseudomonasspp,Klebsiella spp,Candidaspp,andothers.
In criteria 2 and 3:Thephrase‘2ormorebloodculturesdrawnonseparateoccasions’means(1)thatbloodfromatleast2blooddrawswere•collectedwithin2daysofeachother(e.g.,blooddrawsonMondayandTuesdayorMondayandWednesdaywouldbeacceptableforbloodculturesdrawnonseparateoccasions,butblooddrawsonMondayandThursdaywouldbetoofarapartintimetomeetthis criterion) and (2) that at least 1 bottle from each blood draw is reported by the laboratory as having grown the same common skincontaminantorganism(i.e.,isapositivebloodculture).Abloodculturemayconsistofasinglebottleforapaediatricblooddrawbecauseofvolumeconstraints.Therefore,tomeetthis•partofthecriterion,eachbottlefrom2ormoredrawswouldhavetobeculturepositiveforthesameskincontaminant.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-15-
2. Central Line (CVC)
An intravascular catheter that terminates at or close to the heart or in one of the great vessels whichisusedforinfusion,withdrawalofblood,orhemodynamicmonitoring.
The following are considered great vessels for the purpose of reporting central-line infections andcountingcentral-linedays:aorta,pulmonaryartery,superiorvenacava,inferiorvenacava,brachiocephalicveins,internaljugularveins,subclavianveins,externaliliacveins,andcommonfemoral veins.
NotesAn introducer is considered an intravascular catheter. •Inneonates,theumbilicalartery/veinisconsideredagreatvessel.•Neither[thelocationof]theinsertionsitenorthetypeofdevicemaybeusedtodetermineifalinequalifiesasaCVC.Thedevice•must terminate in one of these vessels or in or near the heart to qualify as a CVC.Pacemaker wires and other non-lumened devices inserted into central blood vessels or the heart are • not consideredcentrallines,becausefluidsarenotinfused,pushed,norwithdrawnthroughsuchdevices.Umbilical Catheter: A central vascular device inserted through the umbilical artery or vein in a neonate. •Temporary CVC: Non-tunnelled catheter. •PermanentCVC:IncludesTunnelledcatheters,includingcertaindialysiscatheters,implantedcatheters(includingports).•
3. CVC-associated Bloodstream Infection (BSI)
ACVC-associatedBSIisaprimaryBSIinapatientthathadacentrallinewithinthe48-hourperiodbefore the development of the BSI.
NotesThere is no minimum period of time that the central line must be in place in order for the BSI to be considered central line-•associated.IftheBSIdevelopswithin48-hoursofdischargefromalocation,itisassociatedwiththedischarginglocation.•
4. Cardiovascular System Infection - Arterial or Venous Infection (CVC-VASC)
Includedarearteriovenousgrafts,shunt,fistula,orintravenouscannulation.Shouldmeetatleastoneof the following criteria:
Patient has organisms cultured from arteries or veins removed during a surgical operation and •blood culture not done or no organisms cultured from blood.
Patient has evidence of arterial or venous infection seen during a surgical operation or •histopathological examination.
Patient has at least one of the following signs or symptoms with no other recognised cause: •fever(>38ºC),pain,erythema,orheatatinvolvedvascularsiteand>15CFUsculturedfromanintravascular cannula tip using a semi quantitative culture method and blood culture not done or no organisms cultured from blood.
Patient has purulent drainage at the involved vascular site and blood culture not done or no •organisms cultured from blood.
Patient aged <1 year has at least one of the following signs or symptoms with no other recognised •cause:fever(>38ºCrectal),hypothermia(<37ºCrectal),apnoea,bradycardia,lethargy,orpain,erythema or heat at involved vascular site and >15 colonies cultured from intravascular cannula tip using semi quantitative method and blood culture not done or no organisms cultured from blood.
5.Device Days
Acountofthenumberofpatientswithaspecificdeviceinthepatientcarelocation.Tocalculatedevicedays,foreachdayofthemonth,atthesametimeeachday,recordthenumberofpatientswhohavethespecificdevice(e.g.,centralline).

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-16-
Section 2: Rationale for Recommendations1. IntroductionA major feature of healthcare-associated infection (HCAI) in the last 20 years has been its association with medicaldevicessuchasintravascularcatheters.Thoughessentialforthecareofpatients,intravascularcatheters represent an avenue by which microorganisms can gain entry to the body. Intravascular catheter-related bloodstream infections (CRBSI) have become a leading cause of health-care-associated (HCA) bloodstream infections (BSI) and are associated with substantial morbidity and mortality. CRBSI represent 10–20% of all nosocomial infection and may complicate the stays of up to 10% of intensive care unit (ICU) patients.5 CRBSI independently increase hospital cost and length of stay.6-9 Over 250 000 CRBSI occur annuallyintheUSwithanattributablemortalityrangingfrom12%to25%incriticallyillpatients,withanadded cost ranging from US$3000 to $56 167.6;10;11IntravascularcathetersrepresentpotentiallymodifiableHCAIriskfactors,thereforeafocusoninfectionpreventionisessentialtoensureappropriatepracticeduring the insertion and subsequent optimal care. Preventative strategies to reduce the prevalence of CRBSI have been effective in other countries and include; education of health-care workers (HCWs) oncorrectcatheterinsertionandmaintenance,routinemonitoringofhealthcarefacilityCRBSIrates,adherencetohandhygiene,theuseofadedicatedinfusiontherapyteam,useofsterilesemipermeabledressingsandremovingtheintravascularcatheterassoonaspossible.(Sections2-4)Preventativeprogrammes,includinginstitutionofappropriatesurveillanceprogrammesnotonlyreducecatheter-relatedinfection,butalsohavesignificantcostsavings.InoneIrishhospital,theintroductionofadedicatedtotalparenteralnutrition(TPN)surveillancecoordinatorresultedinadecreaseof9.8CRBSIperyear,representing a minimum saving of 78,300perannum.12
1.1 Types of Intravascular CathetersA large variety of intravascular catheters exist which can be broadly divided into;1. Central vascular catheters (CVC).2. Peripheral vascular catheters (PVC).
CVCs are intravascular catheters that terminate at or close to the heart or in one of the great vessels and areusedforinfusion,withdrawalofbloodorhemodynamicmonitoring.ThetipofaCVCisplacedclosetoa site feeding a large deep systemic vein (Swan Ganz CVCs are placed in pulmonary arteries) where there is alargevessellumenandhighflowstatelimitingvesselinjuryandthrombosis.Thesevesselsincludeinternaljugular(IJ),subclavian(SC)andfemoralvein(FV)placement.Inexceptionalcircumstances,CVCsmaybeplacedtranslumbarintotheinferiorvenacava,inhepaticveinsandthroughlargecollateralsinthosewith central venous obstruction. A number of different CVCs exist which vary with respect to insertion technique,size,numberoflumensandintravascularcathetermaterials.(Appendix4and5)
Incontrast,thetipofaPVCisplacedinasuperficialsmallsystemicvein,typicallybasilic,cephalic,forearm,handorfootveins.PVCsmayrarelybeplacedinothersuperficialveinsorcollateralveins.
1.2 Clinical Presentation and Diagnosis of Catheter-related InfectionAllintravascularcathetersareassociatedwithariskofinfection.Thisriskvarieswiththetypeofcatheter,insertionsite,experienceandeducationofthecatheterinserter,frequencyofaccessingthecatheter,durationofcatheterplacement,theuseofinfectionpreventionandcontrolstrategiesandcharacteristicsofthe catheterised patient.10 Any patient with an intravascular catheter is potentially at risk for intravascular catheter-related infection however certain populations of patients are at higher risk. These patients include:PatientsintheICU-frequentinsertionofmultipleintravascularcathetersthatarerepeatedlyaccessed,•often required for prolonged periods and may be inserted in emergency situations.Non-ICUpatientswithCVCs,includinghaemodialysispatientsandhaematology/oncologypatients.For•patientswithCVCs,factorsassociatedwithincreasedriskofinfectioninclude;prolongedhospitalisationbeforecatheterisation,prolongeddurationofcatheterisation,heavymicrobialcolonisationattheinsertionsiteorCVChub,internaljugularcatheterisation,neutropaenia,prematurity,TPNandsubstandardcareofthecatheter(e.g.,excessivemanipulationofthecatheterorreducednurse-to-patient ratio).13

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-17-
CVC-relatedinfectionscanpresentwithlocalorsystemicsymptoms.Localinfectionsincludeexitsiteinfection,tunnelinfection,andpocketinfection.(Section3.3)Symptomsmayincludeinduration,erythema,warmth,andpainortendernessatoraroundtheintravascularcatheterexitsite.Localinfectionscanbe associated with systemic symptoms including CRBSI. CRBSI should be considered when a patient with a CVC presents with bacteraemia/fungaemia in the presence of signs and symptoms of systemic infection(e.g.,fever,rigors,hypotension).ProbableCRBSIcanbediagnosedbyoneormorepositivebloodculturesobtainedfromaperipheralvein,whenthereisnoapparentsourcefortheBSIexcepttheintravascularcatheter.However,thediagnosisofCRBSIremainsamajorchallenge.Localcathetersiteinflammationhaspoorsensitivity,whilethepresenceofsystemicsymptomssuchasfeverisnotspecificenough.14;15Therefore,microbiologicalevidenceimplicatingthecatheterasasourceoftheBSIisnecessaryfor establishing a diagnosis of CRBSI. These diagnostic approaches which can be divided into two major groups (those that require catheter removal and those that do not) will be discussed in further detail in Section 5.
PVCsarethedevicesmostfrequentlyusedforvascularaccess.AlthoughtheincidenceofBSIislow,seriouscomplicationscanproduceconsiderablemorbidity.PVCsmaybecomplicatedbyphlebitis,extravasationandcolonisation,allofwhichincreasetheriskofPVCinfectionandBSI.Phlebitisisassociatedwithprolonged placement of a PVC (>72 hours).
1.3 PathogenesisThemicroorganismsmostcommonlyassociatedwithCRBSIincludecoagulasenegativestaphylococci,Staphylococcus aureus,aerobicgramnegativebacilli,andCandida spp. Important pathogenic determinants of catheter-related infection are the material of which the device is made and the intrinsic virulence factors of the infecting organism. Catheters made of polyvinyl chloride or polyethylene are likely lessresistanttotheadherenceofmicroorganismsthanarecathetersmadeofPTFE,orsiliconeelastomer.10 Certainmaterialsaremorethrombogenicthanothers,whichmaypredisposetocathetercolonisation.Inaddition,adherencepropertiesandbiofilmformationbyagivenmicroorganismisalsoimportantinthepathogenesis of infection.
The pathogenesis of CVC infection also varies with the type of CVC. Infection of non-tunneled CVC is due to either extra luminal CVC colonisation (which originates most frequently from the skin and less commonly fromhaematogenousseedingofthetip),orintraluminalCVCcolonisationofthehubandlumen.15 In contrast,contaminationoftheCVChubandintraluminalinfectionisthemostcommonrouteofinfectionoftunneledCVCsorimplantabledevices.Inadditiontoskin,thereisevidencethatmucosalcolonisationisanimportant source of coagulase-negative staphylococcal bacteraemia.16
WithrespecttoPVCs,phlebitisisassociatedwithprolongedplacement(>72hours).Migrationofskinorganisms at the insertion site into the cutaneous PVC tract with colonisation of the tip is the most common route of infection. Occasionally organisms enter intraluminally following contamination of the PVChub.Oncemicroorganismsenter,biofilmformsonthelumensurfaceandasaconsequence,thePVCbecomes infected.
1.4 Irish Epidemiology1.4.1 North-South MRSA Study 199917
The 1999 North-South Study evaluated the epidemiology and management of meticillin resistant S. aureus (MRSA)casesidentifiedinIrishlaboratories.TheprevalenceofMRSAwashigherintheSouth(14.0per100000population)thanintheNorth(11.4per100000population).WhilethemajorityofcasesrepresentedMRSAcolonisation,5%(North)and10%(South)ofcaseshadinvasiveinfection.Patientswithinvasive infection were more likely to have a history of PVC or CVC than those with colonisation only.
1.4.2 Enhanced EARSS SurveillanceThe European Antimicrobial Resistance Surveillance System (EARSS) was established in 1999 in response to the growing threat of antimicrobial resistance in Europe. EARSS comprises a network of over 800 microbiological laboratories serving some 1200 hospitals in 30 countries that collects routinely-generated antimicrobial susceptibility testing data on invasive infections caused by seven important bacterial pathogens: Staphylococcus aureus, Streptococcus pneumoniae,Escherichia coli,Enterococcus faecalis,Enterococcus faecium,Klebsiella pneumoniae and Pseudomonas aeruginosa. The HPSC coordinates
Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-18-
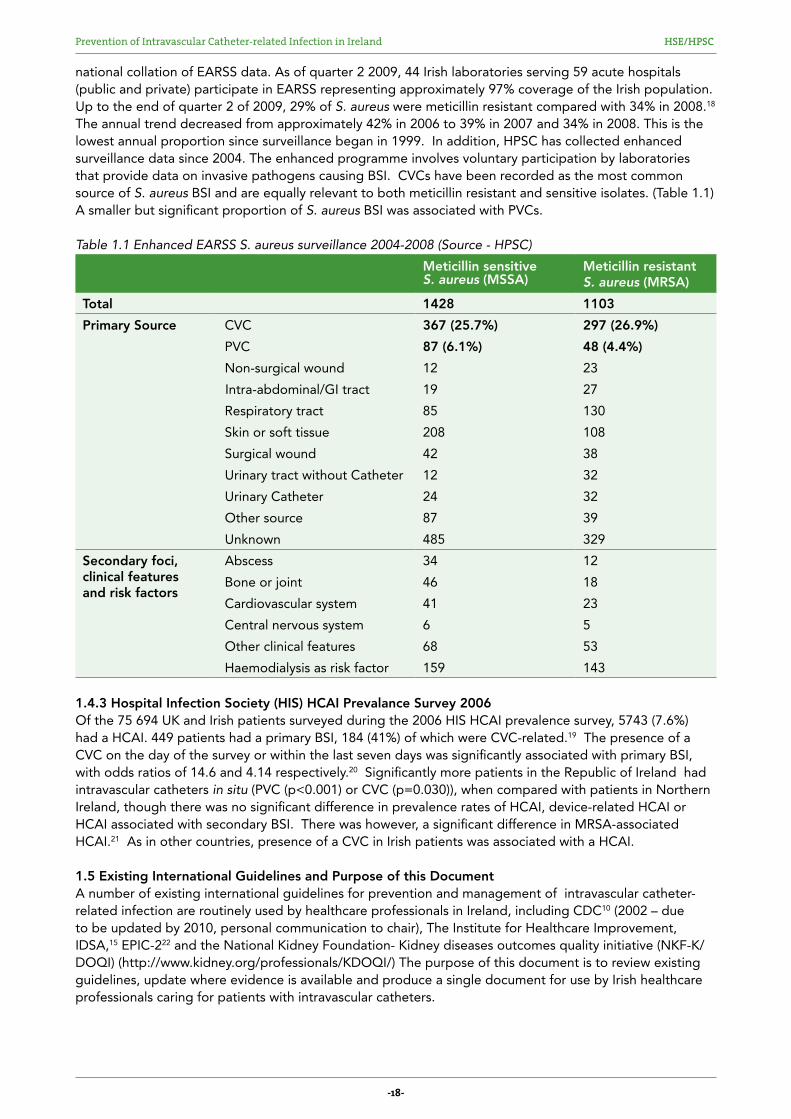
nationalcollationofEARSSdata.Asofquarter22009,44Irishlaboratoriesserving59acutehospitals(public and private) participate in EARSS representing approximately 97% coverage of the Irish population. Uptotheendofquarter2of2009,29%ofS. aureus weremeticillinresistantcomparedwith34%in2008.18 Theannualtrenddecreasedfromapproximately42%in2006to39%in2007and34%in2008.Thisisthelowestannualproportionsincesurveillancebeganin1999.Inaddition,HPSChascollectedenhancedsurveillancedatasince2004.Theenhancedprogrammeinvolvesvoluntaryparticipationbylaboratoriesthat provide data on invasive pathogens causing BSI. CVCs have been recorded as the most common source of S. aureus BSI and are equally relevant to both meticillin resistant and sensitive isolates. (Table 1.1) AsmallerbutsignificantproportionofS. aureus BSI was associated with PVCs.
Table 1.1 Enhanced EARSS S. aureus surveillance 2004-2008 (Source - HPSC)
Meticillin sensitive S. aureus (MSSA)
Meticillin resistant S. aureus (MRSA)
Total 1428 1103
Primary Source CVC 367 (25.7%) 297 (26.9%)
PVC 87 (6.1%) 48 (4.4%)
Non-surgical wound 12 23
Intra-abdominal/GI tract 19 27
Respiratory tract 85 130
Skin or soft tissue 208 108
Surgical wound 42 38
Urinary tract without Catheter 12 32
Urinary Catheter 24 32
Other source 87 39
Unknown 485 329
Secondary foci, clinical features and risk factors
Abscess 34 12
Bone or joint 46 18
Cardiovascular system 41 23
Central nervous system 6 5
Other clinical features 68 53
Haemodialysis as risk factor 159 143
1.4.3 Hospital Infection Society (HIS) HCAI Prevalance Survey 2006Ofthe75694UKandIrishpatientssurveyedduringthe2006HISHCAIprevalencesurvey,5743(7.6%)hadaHCAI.449patientshadaprimaryBSI,184(41%)ofwhichwereCVC-related.19 The presence of a CVConthedayofthesurveyorwithinthelastsevendayswassignificantlyassociatedwithprimaryBSI,withoddsratiosof14.6and4.14respectively.20SignificantlymorepatientsintheRepublicofIrelandhadintravascular catheters in situ (PVC(p<0.001)orCVC(p=0.030)),whencomparedwithpatientsinNorthernIreland,thoughtherewasnosignificantdifferenceinprevalenceratesofHCAI,device-relatedHCAIorHCAIassociatedwithsecondaryBSI.Therewashowever,asignificantdifferenceinMRSA-associatedHCAI.21Asinothercountries,presenceofaCVCinIrishpatientswasassociatedwithaHCAI.
1.5 Existing International Guidelines and Purpose of this DocumentA number of existing international guidelines for prevention and management of intravascular catheter-relatedinfectionareroutinelyusedbyhealthcareprofessionalsinIreland,includingCDC10 (2002 – due tobeupdatedby2010,personalcommunicationtochair),TheInstituteforHealthcareImprovement,IDSA,15 EPIC-222andtheNationalKidneyFoundation-Kidneydiseasesoutcomesqualityinitiative(NKF-K/DOQI)(http://www.kidney.org/professionals/KDOQI/)Thepurposeofthisdocumentistoreviewexistingguidelines,updatewhereevidenceisavailableandproduceasingledocumentforusebyIrishhealthcareprofessionals caring for patients with intravascular catheters.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-19-
2. General Infection Prevention and Control PrinciplesIntravascular catheters should only be inserted when there is a clear clinical indication for their use. When theclinicalindicationisnolongerpresent,thecathetermustberemoved.Hand hygiene is the single most important procedure in prevention of intravascular catheter-associated or related infections.10;23Education-basedpreventiveprogrammes,theuseofaseptictechnique,theoptimalinsertionsite,skinpreparationandappropriateintravascularcathetercareandreplacementalsoplayanimportant role.
2.1 Hand Hygiene Handsmustbedecontaminatedbywashingwithanantimicrobialliquidsoapandwater,orifhandsarephysicallyclean,applyinganalcoholbasedhandrub.24 Hands must be decontaminated before and after accessing or dressing an intravascular catheter.
2.2 Aseptic TechniqueAseptic technique should be used by all HCW during insertion and maintenance of intravascular catheters.(Appendix 6) Aseptic (no-touch) technique is a term used to describe a technique that maintains asepsis and is non-touch in nature.25 The susceptible site should not come in contact with any item that is not sterile;thereforeunsterileglovescanbeused(e.g.,forreconstitutionofmedication),butthekeypartsofthe device must not be touched or come in contact with any unsterile material.25;26 The underlying principles of aseptic (no-touch) technique are:
•Alwaysperformhandhygieneeffectively.•Nevercontaminate‘keyparts’.•Touchnon-keypartswithconfidence.•Takeappropriateinfectiveprecautions.
Theprincipleofaseptic(no-touch)techniqueoperatesonthebasisofidentifyingandprotecting‘keyparts’ ofequipment,whichiftouchedeitherdirectlyorindirectlycouldresultininfection.Thisisachievedbypreventingdirectandindirectcontactof‘keyparts’byanon-touchmethod.Onlysterileequipmentandfluidsareusedandpartsofthecomponentsthatshouldremainsterilearenottouchedorallowedtocomeintocontactwithnon-sterilesurfaces(e.g.,thetipofintravenousconnectors).Inintravenoustherapythekeypartsareusuallythosewhichcomeintocontactwiththeliquidinfusion(e.g.,needles,syringetips,IVlineconnections,exposedCVClumens).Effectivehandhygieneisthemostsignificantprocedureinpreventingcrossinfection.Glovesarenotareplacementforgoodhandhygiene;therefore,staffmustdecontaminate their hands before donning and after removing gloves as described in Section 2.1.
Aswithanystandardisedpractice,itisessentialthatstandardisedprotocols(foruseinallunitswherepatients have intravascular catheters in situ) are developed by healthcare facilities detailing the components of aseptic (no-touch) technique. Staff should be educated and deemed competent before introduction of the protocol. After implementation compliance should be monitored and audited on a regular basis.
The Committee recommends that aseptic technique should be used by all healthcare workers during insertionandmaintenanceofintravascularcatheters.Followinghandhygiene,cleanglovesandanaseptic(no touch) technique should be used when accessing an intravascular catheter if the luer* lock access deviceisnotdisconnectedfromthecatheter(e.g.,intravenousdrugadministration,bloodsamplingorconnectingordisconnectingintravenousfluids).Sterileglovesinadditiontoaseptic(notouch)techniqueshouldbeusediftheluer*lockaccessdeviceisdisconnected(e.g.,manipulationofaline,haemodialysis).Sterile gloves and non touch technique must be used for changing TPN and CVC insertion site dressing change.
*Luer connectionsystemsarethestandardwayofattachingsyringes,catheters,hubbedneedles,IVtubes,andsoontoeachother.Theyconsistofroundmaleandfemaleinterlockingtubes,theycaneitherbe‘luer slip’,orcanhaveanadditionalouterrimofthreading called a ‘luer lock’,allowingthemtobemoresecure.
2.3 Education of Healthcare Workers (HCW) and PatientsInfectionpreventionandcontrol,includingtheprinciplesofpreventionofCRBSI,mustbeanessentialcomponent of the core curriculum of training programmes of medical and nursing students at both

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-20-
undergraduate and postgraduate level. HCW caring for a patient with an intravascular catheter (CVC and PVC) should be trained in:
•Standardprecautions(includingformalhandhygienetraining).•Aseptic(notouch)technique.•Indicationsforintravascularcatheteruse.•Appropriateinsertiontechnique(ifrelevant).•Appropriatecathetercareandmaintenance.•CRBSI:risks,diagnosisandmanagement.
Followingtraining,HCWsmustbeassessedanddocumentedascompetentinusingandconsistentlyadhering to appropriate infection prevention and control practices when inserting or maintaining intravascular catheters. Ideally a national competency document would ensure standardisation of training and allow for interchange between healthcare facilities (due to staff movement); however this would need anappropriateinfrastructureintermsofprojectmanagement,ITandeducation.Itiswellrecognisedthat insertion or maintenance of intravascular catheters by inexperienced staff increase the potential for colonisation and BSI. Only competent staff (or training staff supervised by competent staff) should insert and maintain intravascular catheters. There is a higher rate of infection in haemodialysis patients when new orinexperienceddialysisstaffmanipulatethepatient’svascularaccess.27 Specialised IV teams have shown effectiveness in reducing the incidence of PVC-related infections.28 It is recommended that HCW are periodically assessed with respect to their knowledge of and adherence to preventive measures.13
Patient and carer education also plays a role in the prevention of catheter-related infection; Appendix 7 outlinesapatientinformationleafletthatmaybeusefulinthisregard.Beforedischargefromahealthcarefacility,patientswithanintravascularcatheterandtheircarersshouldbeeducatedbyamember(s)ofthepatient’sclinicalmultidisciplinaryteamwithrespecttoproceduresnecessarytosafelymanagetheirdevice and to prevent infection and on the signs of infection. This training should be documented in the patient’srecordsandthepatient/carershouldsignthattheyhaveunderstoodtheprinciplesofpreventionofintravascularcatheterinfection.Inhaemodialysispatients,poorpersonalhygieneisariskfactorforvascular access site infections29 and is certainly true for all patients with CVCs. Therefore,patientswithpoor personal hygiene habits should be taught how to improve and maintain their personal hygiene.
Educationalprogramsthatprovide,monitor,evaluateandfeedbackareessential.Trackingtheoccurrenceofinfections(e.g.,CRBSIsurveillance,Section3.2)canhelpidentifythesourceandallowcorrectiveactiontobetaken.Morerecently,thedevelopmentandimplementationofcarebundleshasincreasedawareness,adherencetoguidelinesandreducedtheincidenceofcatheter-relatedinfections,howevereducationofHCW is key to the success of implementing and maintaining a care bundle programme. (Sections 3.1.8 and4.1.6)Ongoingqualityassurance/improvement,riskmanagementorsurveillanceprogrammesshouldbeinplacetomonitortheincidenceofinfectionassociatedwithintravascularcatheters,toevaluatetheresponsetopatientandstaffeducation,toidentifygapsinpracticethatwillneedremedialactionandtoidentify future educational needs.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-21-
3. Central Vascular Catheters (CVCs)
3.1 Prevention of CVC Infection3.1.1 Hand Hygiene and Aseptic TechniqueHand hygiene and an aseptic technique are essential to prevent contamination of CVC sites and subsequent BSI. (Sections 2.1 and 2.2)
3.1.2 Skin Asepsis The epidemiology of CVC-related infections clearly shows a predominance of gram positive organisms. There is a worldwide consensus on the use of chlorhexidine as the optimum antiseptic for skin preparation prior to CVC insertion. The concentration of chlorhexidine used in different studies has varied from 0.5% to4%.Thelowestconcentration,0.5%hastypicallybeenusedinneonatalpatientcohorts.Thislowerconcentrationwouldhavesimilarefficacytopovidoneiodinesolutions.The2%chlorhexidinesolutionwasmostcommonlyselectedinarangeofstudies,althoughanumberofauthorsadmitthata1%solutionwasnot regularly available at the commencement of their trial.
Thereisastrongargumenttocombine2%aqueouschlorhexidinewithalcohol,asalcoholhasaninstanteffect and provides better cover for a range of gram-negative organisms or gram-positive organisms with relativelyhighMICvaluesforchlorhexidine(e.g.,Bacillus spp.). Indeed chlorhexidine has no activity against Bacillus spearothermophilus,ATCC7953andanMICof10,000mg/LagainstBacillus subtilis ATCC 9372.30
Acommerciallyavailablechlorhexidineimpregnatedsponge,about2.5cmindiameter,canbeplacedover the CVC insertion site and covered with transparent polyurethane. A meta-analysis including eight randomized trials showed that chlorhexidine impregnated sponges are associated with a trend towards reduction of vascular infection.31 Recent studies have also shown their effectiveness in preventing infection in patients having CVCs inserted for chemotherapy.32 The overall cost effectiveness for all groups would need to be evaluated before making a recommendation for the use of these dressings in all groups with CVCs. Their use is not recommended in neonates less than seven days of age or a gestational age of less than 26 weeks. Recent US guidance advised considering their use in selected groups of patients only which include units or patient populations that have a CRBSI rate higher than the healthcare facility goal despite compliancewithanevidence-basedpreventionbundle,patientswithlimitedvenousaccessandahistoryofrecurrentCRBSIorpatientsareatheightenedriskforseveresequelaefromaCRBSI(e.g.,patientswithrecentlyimplantedintravasculardevices,suchasaprostheticheartvalveoraorticgraft).13
DirectcomparisonofaqueousversusalcoholsolutionsofchlorhexidineforpreventionofCVC-relatedinfection has not been performed. Intellectually the argument for the addition of alcohol seems persuasive and hence the EPIC guideline recommendation for 2% chlorhexidine gluconate in 70% isopropyl alcohol.22 TheCDCguidelinerecommends2%aqueouschlorhexidineandclearlystatethattheirguidelineexcludesbabies < 2 months old.10Forpatientswithahistoryofchlorhexidinesensitivity,theEPICguidelinesrecommend a single patient use application of alcoholic povidone-iodine solution.22
The Committee recommend single patient use of 2% chlorhexidine gluconate in 70% isopropyl alcohol in adults and children ≥ 2 months (assuming normal gestation at birth) as follows:
•SkinasepsispriortotheinsertionofaCVC.•TodisinfecttheCVCinsertionsiteduringdressingchanges.•TodisinfectCVChuborinjectionport.
Skinshouldbeallowedtoairdrypriortofurthermanipulation.Ifskinisvisiblydirty,itshouldbewashedprior to skin asepsis. Single patient use application of alcoholic povidone-iodine solution should be usedforpatientswithahistoryofchlorhexidinesensitivity.Hub/portdecontaminationwith70%alcohol,allowing the hub/port to dry prior to further manipulation is an acceptable alternative to 2% chlorhexidine in 70% isopropyl alcohol.
MostmodernCVCsaregenerallyalcohol-resistant,i.e.,theyarenotdamagedbycontactwithalcohol.However,alcoholandotherorganicsolvents,oil-basedointmentsandcreamsmaydamagesometypesofpolyurethaneandsiliconCVCtubing(e.g.,someCVCsusedinhaemodialysis).HCWshould

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-22-
thereforeensurethatCVC-sitecareiscompatiblewithCVCmaterials(tubing,hubs,injectionports,luerconnectorsandextensions)andcarefullycheckcompatibilitywiththemanufacturer’srecommendations.Themanufacturer’srecommendationsforonlyusingdisinfectantsthatarecompatiblewithspecificCVCmaterials must be followed. This assessment must be performed in advance of purchasing the CVC/materials.IftheCVC/materialsareincompatiblewith2%chlorhexidinegluconatein70%isopropylalcohol,thereshouldbeaclearclinicalbenefittopurchasingtheCVC/materials.Ifnot,alternativeCVC/materialsshouldbesought.Anaqueoussolutionofchlorhexidinegluconateshouldbeusedifthemanufacturer’srecommendations prohibit the use of alcohol with their product.
Atthetimeofwriting,itisrecognisedthattherearenolicensedpreparationscontainingchlorhexidine2%/isopropyl alcohol 70% designed for skin asepsis prior to IV catheter insertion commercially available inIreland,despitetheiravailabilityinotherjurisdictionsincludingtheUK.However,clinicaltrialdataandinternationally recognised best practice leads us to strongly advocate the use of products containing this particular combination for skin asepsis. It is hoped that the commercial incentive for use of these productswillprompttheintroductionofIrishlicensedpreparationsinthenearfuture.Inthemeantime,thedecisiontouseunlicensedproductsshouldbemadein-house,inaccordancewitheachhealthcarefacility’smedicines management structures and policies for the use of unlicensed medicines.
3.1.2.i Neonatal Skin AsepsisNeonatal skin is known to be fragile with premature birth cohorts being particularly vulnerable. A study of 705neonates,whereachlorhexidineimpregnatedspongewasusedforCVCsitecareshowedthat15%of98verylowbirthweightinfantsdevelopedcontactdermatitis,whileonly1.5%of237neonatesweighing>1000 grams developed this complication.33
Absorption of chlorhexidine or alcohol is another concern. Chlorhexidine absorption was investigated in 1970s and 1980s with variable results but generally premature neonates did absorb detectable amounts (range 13 to 1021ng/ml). The upper level of serum chlorhexidine that can be considered safe is unknown. The potential for absorption appears to be reduced when chlorhexidine is applied in aqueous or other non-ethanol based formulations. Wilson et al suggests that the highest tolerable concentration for newborn skin cleansing is 1% chlorhexidine.34Othersideeffectsreportedinclude,transientbradycardia(inabreastfedinfantwherethematernalbreastwassprayedwithchlorhexidine)andburns,somesufficientlysevere to require skin grafting have also been reported from neonatal units. Currently different skin antisepticsarebeingusedinneonatalunitsacrossIreland.AUKsurveyof50tertiary-levelneonatalintensive care units (NICUs) on cutaneous antisepsis prior to insertion of central venous and umbilical catheters revealed a lack of uniformity across the NICUs with regard to the type or concentration of antiseptic solutions currently being used. Antiseptic solutions used included 0.05% chlorhexidine in aqueoussolution(27NICUs),0.015%chlorhexidineand0.15%cetrimideinaqueoussolution(8NICUs),10%povidone-iodineinaqueoussolution(6NICUs),0.5%chlorhexidinein70%alcoholicsolution(5NICUs),1%chlorhexidineinaqueoussolution(3NICUs)and70%alcohol(oneNICU).35Onbalance,itappearsthat0.5-1%chlorhexidineistheoptimalrangeforneonatalskinasepsis;however,randomisedcontrolled trials are required to clarify this range.
The gentle friction caused by scrubbing when performing skin asepsis may damage the immature stratum corneumofimmatureneonates(e.g.below30weeksgestationalage),therefore,itisrecommendedthatthe product should be gently dabbed onto the skin for 10 seconds and the skin allowed to dry. Application ina‘upanddown,backandforth’movementshouldbeavoided.Aftertheprocedure,theskinshouldbecleaned with sterile water and dried throughly.
3.1.3 Maximal Barrier PrecautionsMaximal barrier precautions clearly decrease the odds of developing CRBSI. Two studies show that the odds of developing a CVC infection were higher if maximal barrier precautions were not used.36;37 The componentsofmaximalbarrierprecautionsareoutlinedinFig3.1.Theseprecautionsarethesameasforany other surgical procedure that carries a risk of infection and must be performed by the operator and any personwhoentersthesterilefieldtoassistbeforeplacingaCVC(includingguidewireexchanges).

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-23-
•Handhygiene:StrictcompliancewithhandhygienebytheoperatorplacingtheCVCandfor
those assisting in the procedure (antimicrobial soap or alcohol-based hand rub as outlined in Section 2.1).
•Coveringthepatientfromheadtotoewithasteriledrapewithasmallopeningforthesiteofinsertion.
•Theoperatormustwear: •Cap(thecapshouldcoverallhair). •Mask(themaskshouldcoverthenoseandmouthtightly). •Protectiveeyewear. •Sterilegown. •Sterilegloves.
Fig 3.1 Maximal barrier precautions
3.1.4 Selection of CVC, Insertion Site and CVC PlacementThe indications for CVC insertion may include:
•Infusionofcardiovascularsupports.•Haemodynamicmonitoring.•Highvolumefluidresuscitation.•Haemodialysis.•Poorvenousaccess.•IntravenousadministrationofhyperosmolarandirritatingsolutionsandsolutionsofacidicoralkalinepH,whichmaycauseendothelialdamageandsubsequentphlebitisandthrombusformation(e.g.,chemotherapy,vesicants,TPN).
ThesiteofCVCplacementcaninfluencetheriskofsubsequentBSI.PotentialsitesareoutlinedinAppendix4.Itisrecommendedtousetheinsertionsiteassociatedwiththeleastlikelihoodofinjury(jugular,femoral,subclavian)andtoconsiderportableultrasoundimagingforselectedpatientsathighrisk of complications (e.g.,knownvascularanomaly)orwherevascularaccessislikelytobedifficult(e.g.,young children). In a large randomized trial of ultrasound versus the landmark technique for insertion of jugular CVCs,significantlyfewerinfectionswerefound intheultrasoundgroup,possiblyduetothefewer skin punctures required when ultrasound was used.38 Mermel et al. demonstrated that the great majority of infections develop at the insertion site; other risk factors were use of the jugular insertion site over the subclavian site.36 A similar effect was demonstrated for CVCs used for TPN.39 Recent US guidance recommends avoiding using the femoral vein for central venous access in adult patients on the basis that the femoral access site is associated with greater risk of infection and deep venous thrombosis in adults.13 The increased risk of infection associated with femoral catheters in adults may however be limitedtooverweightpatients(bodymassindexhigherthan28.4).40 In selecting an appropriate insertion site,therisksforinfectionshouldbeassessedagainsttherisksofmechanicalcomplications.Recentprospectiveevidenceshowsthatsubclavian,jugularandfemoralsiteshavesimilarCRBSIratesincriticallyill patients.40-43 When CVCs are inserted in dialysis patients that are likely to require long term renal replacement; the subclavian site should be avoided because of the frequent development of subclavian stenosis which interferes with long term provision of vascular access.
A large variety of CVC types are available as outlined in Appendix 5. The risk of infection with peripherally inserted CVCs (PICCs) in ICU patients is similar to CVCs placed in the subclavian and internal jugular veins.13 A single or double-lumen CVC is recommended unless multiple ports are essential for the managementofapatient.Ifamulti-lumenCVCisused,oneportshouldbeidentifiedanddesignatedexclusivelyforTPN(ifrequired).Ifsingle-lumenaccessisrequired,consideraPICC.Forpatientsrequiringregularorcontinuousaccess,atunnelledCVCispreferred.Theuseofimplantableportsisrecommendedforpatientswhorequirelong-term,intermittentvascularaccess.
Recentguidelinesadviseconsideringtheuseofantiseptic(e.g.,chlorhexidine-silversulfadiazine)orantimicrobial(e.g.,minocycline-rifampicin)impregnatedCVCsinthefollowingcircumstancesinadults:
Units or patient populations that have a CRBSI rate higher than the healthcare facility • goal despite compliance with basic CRBSI prevention practices.
Patients with limited venous access and a history of recurrent CRBSI.•

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-24-
PatientsthatareatheightenedriskforseveresequelaefromaCRBSI(e.g.,patientswithrecently•implantedintravasculardevices,suchasaprostheticheartvalveoraorticgraft).13
It is recommended that each healthcare facility has a written CVC insertion guideline that is updated regularly/as new evidence becomes available. An example of such a guideline is provided in Appendix 8. CVC insertion packs containing all necessary items for aseptic CVC insertion are also recommended. (Appendix 9) These packs should be easily accessible in all units where CVCs are inserted. As recommended previously,CVCshouldonlybeinsertedbyeitherexperiencedHCW(educatedandtrainedintheproperprocedures for insertion and assessed as competent in using and consistently adhering to appropriate infection prevention and control practices) or less experienced HCW under the direct supervision of an experienced HCW. (Section 2.3)
OncetheCVCisinserteditisrecommendedthatCVCplacementisconfirmedwithchestradiology.Ifaccidental insertion of wide-bore CVC into subclavian artery or femoral artery above inguinal ligament occurs the catheter should be left in situ and vascular surgery/interventional radiology consulted for possible endovascular repair with closure device.
3.1.4.i Image Guided Placement and Interventional RadiologyImageguidedplacementisperformedinaradiology/angiographysuitewithsonography,duplexandangiography/fluoroscopicfacility.AvarieyofproceduresasoutlinedinFig3.2canbecarriedout.Theinterventional team consists ofradiologist,radiographerandspecialistnurse.Theteamshouldbecapableof standard and complex line placement and equipped to deal with complications of placement or of long termuse.CVCinsertionshouldtakeplaceinacertifiedventilationunitwithairexchangeinkeepingwithaprocedureunit,containingascrubandpreparationareaanddesignatedcleananddirtyutilityareas.PriortoCVCinsertion,theteamshouldperformfullsterilepreparationincludingsurgicalscrubandsteriletablepreparation.Equipmentanddisposablesusedfortheproceduremustbesterile.Vesselsareidentifiedandtargetedwithfluoroscopy,venographyorvascularsonographyandthelinecourseandtippositionconfirmedwithfluoroscopy.Radiologyreportofprocedurewithsurgicalnotebecomespartofthepatientrecord.Patient monitoring and sedation or general anaesthetic is recorded in the procedure note. Anaesthetic notes maybeincludedinadditionifrequired.Animageisrecordedofaccessandfinallineposition.Aspreviouslyrecommended,eachhealthcarefacilityshouldhaveawrittenCVCinsertionguideline,thatisupdatedregularly/as new evidence becomes available. An example of such a guideline is provided in Appendix 8 and of CVC insertion packs in Appendix 9.
Standard and Complex line placement.•Tip Replacement if dislodged or migrates .•Tunneled line removal.•Tunneled line tract bleeding management.•LineExchange.•Longtermlinestrippingiffibrinsheath.•Venography for non functioning lines.•LineFracture-repairandandretrievalofmigratedfragments.•Thrombolysis.•Diagnosisandmanagmentofcomplicationssuchasarterialandvenousinjury.•
Fig 3.2 Peripheral / Central Line Techniques in an Interventional Unit
3.1.5 Antimicrobial Ointments, Locks and Prophylaxis3.1.5.i Antimicrobial OintmentsThe EPIC group22 reviewed several studies examining the application of antimicrobial ointments to the CVCsite,eitheratthetimeofCVCinsertion,orduringroutinedressingchanges,toreducemicrobialcontaminationofCVCinsertionsites.Reportedefficacyinpreventingcatheter-relatedinfectionsbythispracticeyieldedcontradictoryfindings.TherewasalsoconcernthattheuseofpolyantibioticointmentsthatwerenotfungicidalcouldsignificantlyincreasetherateofcolonisationbyCandida spp. Recent guidelines recommend the application of povidone-iodine or polysporin ointment to haemodialysis catheter insertion sites in patients with a history of recurrent S.aureus CRBSI. Mupirocin ointment is not recommended due to the risks of mupirocin resistance and damage to polyurethane catheters.13

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-25-
3.1.5.ii Antibiotic Antimicrobial LocksAnantimicrobiallocksolutionconsistsofanantimicrobialagent,frequentlymixedwithananticoagulant,whichisusedtofillthelumenoftheintravascularcatheter.Avarietyofantimicrobials(bothsingleagentand in combination) have been studied to evaluate their effectiveness in the prevention of CRBSI. Concerns that their widespread use would lead to the selection of resistant organisms (especially vancomycin resistant organisms) have thus far limited their widespread recommendation.
A meta-analysis of randomized controlled trials evaluating the use of vancomycin for prevention of CRBSI showedastatisticallysignificantreductioninthenumberofCRBSIwithvancomycinlocksolution.However,thisanalysisconsistedofonlysevenstudies(fivestudieswithcancerpatients,onewithneonatesandonewithcancer and neonates with parenteral nutrition). AntimicrobialflusheswerenotshowntocauseastatisticallysignificantreductioninCRBSI.TheauthorsdidnotfindanyreportofcolonisationorBSIwithvancomycin-resistantorganismsandconcludedthatitishighlyunlikelythatmicroorganismsinapatient’smicroflorawoulddevelop resistance to vancomycin from the very low dosage of vancomycin used in the antimicrobial locks.44 Inaretrospectivestudy,Feelyet al.exploredtheefficacyofantibioticlocktherapyinhigh-riskhaemodialysispatientsandidentifiedasubgroupofpatientswiththreeormoredocumentedBSIsovertwoyears,inwhomlocksolutions(gentamicin-heparin,minocycline-ethylenediaminetetraaceticacid(EDTA)orvancomycin-heparin)decreasedtherateofcatheterinfectionsfrom9.1to1.04episodesper1000patient-days.45 Doxycline-EDTAisapossiblealternativetominocycline-EDTA,whichisnolongeravailableonthemarket. Previously,prophylacticuseofavancomycin-heparinlocksolution in high-risk neonates with long-term CVCs was shown to reduce CRBSI.46
A recent meta-analysis evaluating the use of antimicrobial lock solutions for the prevention of CRBSI in haemodialysis patients showed that the use of antimicrobial lock therapy was associated with a reduction inratesofbothCRBSIandcatheterremoval.However,whiletheauthorsconcludethatantimicrobiallocktherapydoesindeedresultinastatisticallysignificantreductioninCRBSI,afinalrecommendationastowhich antimicrobial lock solution to choose (a number of different antimicrobial agents were used in the trials includedinthemeta-analysis:vancomycin,gentamicin,cefazolin,minocycline,cefotaxime)andforhowlong,(range of duration 1-15 weeks) was not addressed. Additional preventative measures (nasal decontamination withmupirocin,topicalchlorhexidine,iodinedressings)usedinconjunctionwithantimicrobiallocktherapywere also necessary to prevent CRBSI.47
Onthebasisoftheavailableevidence,thereappearstobearoleforantimicrobiallocktherapyinpreventionofCRBSI,mostnotablywithrespecttoeradicationofgram-positiveorganisms.Anecdotalandcasereportsonly are available regarding the use of antimicrobial lock prophylaxis for the prevention of gram-negative CRBSI and therefore the use of lock therapy prophylaxis cannot be recommended for this category of patients at present. Antimicrobial lock therapy is not recommeded for the prevention of CRBSI due to Candida spp. andotherfungi,duetomycoticseedingandthepotentialforendocarditis.ArecommendationfortheuseofantimicrobiallocksolutionsforthepreventionofCRBSIcanbemadeforcertainsubgroupsofpatients,notablythosewhorequireindefinitevascularaccess(e.g.,haemodialysis,shortbowelsyndrome)andwhohave had multiple episodes of CRBSI and and have developed these infections despite strict adherence to all other preventative measures. Antimicrobial lock therapy should only be considered for use with long term CVCs. Ongoing surveillance for the emergence of resistant organisms should be performed where antimicrobial lock therapy is used.
The decision to use antimicrobial lock prophylaxis and the choice of antimicrobial agent to be used will need tobedecidedonaindividualpatientbasis,basedontheirpreviouspositivemicrobiologyandinconjunctionwith the medical microbiologist/infectious diseases physician.
3.1.5.iii Non Antibiotic Antimicrobial LocksTherationalbehindtheuseofanticoagulantsinthepreventionofCVCinfectionisthatthrombinandfibrindepositedonCVCsmightserveasnidusformicrobialcolonisation.Anticoagulantflushsolutionsareusedwidely to prevent CVC thrombosis. The majority of heparin solutions contain preservatives with antimicrobial activity,thereforeitisimpossibletoascertainwhetheranydecreaseinCRBSIisasaresultofdecreasedthrombusformation,antimicrobialactivityorboth.Investigationoftetrasodium-EDTA,in vitro and ex vivo (withexplantedinfectedhaemodialysiscatheters)hasshownpromiseinreducingCVC-associatedbiofilmsofclinicallyrelevantmicroorganisms(includingMRSA,S. epidermidis, P. aeruginosa, and C. albicans). Tetrasodium-EDTAisalsoapotentanticoagulantthatcouldreplacetheuseofheparinandeliminatethe

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-26-
risk of heparin-induced thrombocytopenia.48 Other non-antibiotic antimicrobial CVC lock solutions include; tauroline,citrateandcombinationsofboththeseagents.Taurolidineisabroadspectrumagentwithin vitro activity against gram negative and gram positive organisms and Candida spp. and a number of reports appear promising.49-51Likewise,theuseofethanolasalockhasbeenreported.52;53Thereiscurrentlyinsufficientevidencetowarrantroutineuseoftaurolidineorothernon-antibioticantimicrobiallocks,however,studiesareencouraging.Furtherstudyisthereforerequiredbeforetheseagentscanberoutinelyrecommendedtoprevent CRBSI.
3.1.5.iv Systemic Antimicrobial ProphylaxisSystemicantimicrobialprophylaxisshouldnotbeusedroutinelytopreventCVCcolonisationorCRBSI,either before insertion or during the use of a CVC. There are no studies demonstrating that the use of oral orintravenousantimicrobialsdecreasetheincidenceofCRBSIinadults.OftworecentCochranereviews,one concluded that there is no evidence to administer antibiotics prophylaxis to prevent CVC–related gram positive infections in oncology patients54 and the other concluded that the use of prophylactic systemic antimicrobials in neonates with CVCs reduced the rate of proven or suspected BSI but did not result in any significantdifferenceinoverallmortalityandthereforetheirusecannotberecommended.55
3.1.6 CVC Exit Site CareThe safe maintenance of a CVC and relevant care of the insertion site are essential components of a comprehensive strategy for preventing CVC-related infections. This includes good practice in caring for the patient’sCVChubandconnectionport,theuseofanappropriateexitsitedressingregimenandtheuseofflushsolutionstomaintainpatencyoftheCVC.CVCsshouldbemaintainedbyexperiencedHCWeducatedand trained in the proper procedures for maintenance and assessed as competent in using and consistently adhering to appropriate infection prevention and control practices. (Section 2.3) It is recommended that each healthcare facility has a written CVC maintenance guideline that is updated regularly/as new evidence becomes available.
3.1.6.i Hand Hygiene and Aseptic TechniqueStrict adherence to hand hygiene and aseptic technique is the cornerstone for preventing CVC-related infection. (Sections 2.1 and 2.2)
3.1.6.ii Management of IV accessories (e.g., hub/needless devices/bungs, administration sets)ContaminationoftheCVChubisanimportantcontributortointraluminalmicrobialcolonisationofCVCs,particularly long-term CVCs.10FrequentCVChubmanipulationincreasestheriskformicrobialcontamination.Duringprolongedcatherisation,CVChubsareaccessedmorefrequently,increasingthelikelihoodofaCRBSIemanatingfromacolonisedCVChubratherthantheinsertionsite.Consequently,hubsandsamplingportsmust be disinfected before they are accessed. In adults and children ≥ 2 months (assuming normal gestation atbirth),itisrecommendedthatpriortoaccessingthesystem,handhygienemustbeperformedandcatheterhub/injection port should be thoroughly decontaminated with a single patient use application of alcoholic chlorhexidinegluconatesolution(preferably2%chlorhexidinegluconatein70%isopropylalcohol),oncecompatible with the CVC and allowed to dry. (Section 3.1.2)Hub/portdecontaminationwith70%alcohol,allowing the hub/port to dry prior to further manipulation is an acceptable alternative.
Ifneedlelessdevicesareused,themanufacturer’srecommendationsforchangingtheneedlelesscomponentsshouldbefollowed.Whenneedlelessdevicesareused,HCWsshouldensurethatallcomponentsofthesystemarecompatibleandsecured,tominimiseleaksandbreaksinthesystem.
Administrationsets(IVgivingsets)includingadd-ondevices(e.g.,extensiontubing,needlessdevices,bungs) used for continuous infusions should be replaced after 72 hours.10 Infusion therapy should not bedisconnectedfromthehubunlessclinicallyindicated.Oncedisconnected,boththesolutionandadministration set must be replaced. Administration sets used for intermittent infusions should be discarded after each use.56 Blood administration sets should be changed after a maximum of 6 hours. In the event of amassivetransfusion,thebloodadministrationsetmaybechangedatthediscretionofthenurseordoctor,e.g.,intheeventofthelineblockingortheneedformultipleunits.57 Administration sets used for TPN should bechanged24hoursafterinitiatingtheinfusion.10;56
3.1.6.iii Antimicrobial OintmentsLocalapplicationofantimicrobialointmenttotheCVCinsertionsiteshasnoroleinroutineCVCsitecareandis not recommended.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-27-
3.1.6.iv Choosing the Correct DressingFollowingCVCplacement,adressingisusedtoprotecttheinsertionsite.Occlusivedressingstrapmoistureontheskin,andprovideanidealenvironmentfortherapidgrowthofmicroorganisms,thereforedressings for insertion sites must be permeable to water vapour. The two most common types of dressings used for insertion sites are:
•Sterile,transparent,semipermeablepolyurethanedressingscoatedwithalayerofanacrylicadhesive.•Steriledrygauzeandtapedressings.
Sterile,transparent,semipermeablepolyurethanedressingshavebecomeapopularmeansofdressingCVCinsertionsites.TheyreliablysecuretheCVC,permitcontinuousvisualinspectionoftheCVCsite,allowpatientstobatheandshowerwithoutsaturatingthedressing,andrequirelessfrequentchangethan that required for standard gauze and tape dressings. Transparent semipermeable dressings should be permeable to water vapour and oxygen and impermeable to microorganisms. There is no difference betweenthevarioustypesofdressingswithrespecttoprotectionagainstinfection,thereforethechoiceof dressing is a matter of preference.10 Semipermeable dressings should be changed every seven days or sooner if they are no longer intact or moisture collects under the dressing. If blood is oozing from the CVCinsertionsiteorthepatienthasprofuseperspiration,agauzedressingmightbepreferred.Gauzedressings are not waterproof and require frequent changing in order to inspect the CVC site. They are rarely useful in patients with long term CVCs. The need for a gauze dressing should be assessed daily and changedwheninspectionoftheinsertionsiteisnecessaryorwhenthedressingbecomesdamp,loosenedor soiled. A gauze dressing should be replaced by a transparent semipermeable dressing as soon as possible.
TheCommitteerecommendthatsterile,transparent,semipermeabledressingsareusedforCVCdressingand are changed every seven days or sooner if they are no longer intact or moisture collects under the dressing.Ifsterilegauzedressingisused(e.g.,ifapatienthasprofuseperspirationoriftheinsertionsiteis bleeding or oozing) it should be replaced by a transparent semipermeable dressing as soon as possible. Dressingsusedontunnelledorimplantedintravascularcatheterinsertionsitesshouldbereplacedeverysevendaysuntiltheinsertionsitehashealed,unlessthereisanindicationtochangethemsooner.
3.1.6.v Maintenance of CVC PatencyAsterile0.9%sodiumchlorideinjectionshouldbeusedtoflushandlockCVClumens.Whenrecommendedbythemanufacturer,implantedportsoropened-endedlumensshouldbeflushedandlockedwithheparinsodiumflushsolutions.Systemicanticoagulantsshouldnotbeusedroutinelytoprevent CRBSI.22
3.1.6.vi In-line FiltersAlthoughin-linefiltersreducetheincidenceofinfusion-relatedphlebitis,thereisnoevidencethattheyprevent infections associated with CVCs.10;22Filtrationofmedicationsorinfusatesinthepharmacyisamore practical and less costly way to remove the majority of particulates.
3.1.7 CVC Replacement3.1.7.i Daily ReviewDailyreviewofCVCnecessitywillpreventunnecessarydelaysinremovingCVCsthatarenolongerclearlynecessaryinthecareofthepatient.Manytimes,CVCsremaininplacesimplybecauseoftheirreliableaccessandbecauseHCWhavenotconsideredremovingtheline.However,itisclearthattheriskofinfection increases over time as the line remains in place and that the risk of infection is decreased if removed.
All CVCs should be reviewed daily and those that are no longer clearly needed should be promptly removed. The insertion site should be examined daily (or at each dressing change if gauze is used) forerythema,drainage,tenderness,pain,redness,swelling,sutureintegrityandCVCposition.Siteappearanceshouldnotbeusedastheonlyindicatorofinfectionaslocalinflammationmaynotbepresent.Thepatientshouldalsobeexaminedforfeverorothersignsofsepsis(e.g.,tachycardia,tachypnoea,hypotension). Patients should be encouraged (where possible) to report any changes in their CVC site or any new discomfort. Patients transferring from other healthcare facilities with a CVC in situ must have this device reviewed upon arrival for infectious and mechanical complications.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-28-
3.1.7.ii Replacement of Non Tunnelled CVCsAll CVCs should be replaced promptly when there is clinical evidence that the CVC is the source of infection (e.g.,purulenceattheinsertionsite)andanewCVCinserted,ideallyatadifferentsite.CVC’scanbereplacedby either removing the CVC and placing a new CVC at another site or placing a new CVC over a guidewire at theexistingsite.Becausebreachesinsteriletechniquearemorelikelyduringemergencyprocedures,CVCsinsertedduringamedicalemergencymustbereplacedassoonaspossibleandafternolongerthan48hours.AllfluidadministrationtubingandconnectorsshouldbereplacedwhentheCVCisreplaced.
Routine replacement of CVCs that are functioning and have no evidence of causing local or systemic complications (including scheduled guidewire exchanges of CVCs) as a method to reduce CRBSI has not lowered rates.10CVCsshouldbereplacedonlyonclinicalindications(i.e.,clinicalinfection/purulenceattheinsertion site). Pulmonary artery CVCs are inserted through an introducer and typically remain in place an averageofthreedays.StudieshaveshownanincreasedriskforCRBSIafterfivedays(0/442CRBSIbeforefivedaysversus5/442CSBSIafterfivedays,p<0.001)andinthoseleftinplacelongerthansevendays.AswithothernontunneledCVCs,nostudiesindicatethatpulmonaryarteryCVCreplacementatscheduledtime intervals is an effective method to reduce CRBSI.10 In patients who continue to require hemodynamic monitoring,pulmonaryarteryCVCsdonotneedtobechangedmorefrequentlythaneverysevendays.NospecificrecommendationcanbemaderegardingroutinereplacementofpulmonaryarteryCVCsthatneedtobe in place for greater than seven days.
CVC replacement over a guidewire has become an accepted technique for replacing a malfunctioning CVC or exchanging a pulmonary artery CVC for a CVC when invasive monitoring is no longer needed and is associatedwithlessdiscomfortandasignificantlylowerrateofmechanicalcomplicationsthanarethosepercutaneously inserted at a new site.10However,replacementoftemporaryCVCsoveraguidewireinthepresenceofBSI/suspectedBSIisnotanacceptablereplacementstrategy,becausethesourceofinfectionisusually colonisation of the skin tract from the insertion site to the vessel.10 Guidewire assisted CVC exchange to replace a malfunctioning CVC or to exchange an existing CVC should therefore be used only if there is no infectionattheCVCsiteornosuspicionofCRBSI.Ifafteraguidewireexchange,investigationsrevealCRBSI,the newly inserted CVC should be removed and if still required reinserted at a different site. Guidewire exchanges should not be used routinely for percutaneous CVCs to prevent infection. The exception may be early failure of the device in a situation where a new central venous puncture would be hazardous to the patient.
Forguidewireexchanges,thesamemeticulousaseptictechniqueanduseoffullsterilebarriersaremandatoryduringinsertionofthenewCVC.Afterskinasepsis,insertingtheguide-wire,removingtheoldCVC,andfurtherskinasepsis,theoperatormustre-gloveandre-drapethesite,astheoriginalglovesanddrapesarelikely to have become contaminated from manipulation of the old CVC. (Sections 3.1.2 to 3.1.3)
3.1.7.iii Replacement of Tunnelled CVCsTunnelledCVCsshouldbereplacedonlyonclinicalindications(i.e.,clinicalinfectionand/orpurulenceatthe insertion site). Guidewire-assisted CVC exchange is not advised for cuffed tunnelled CVCs when it may be technically easier and safer to insert a new CVC into a clean site. In selected patients with tunnelled haemodialysisCVCsandbacteraemia,wherevenousaccessislimited,CVCexchangeoveraguidewireincombination with antibiotic therapy might be an alternative as a salvage strategy.10
3.1.7.iv Implantable PortsFullyimplantedCVCs(implantableports)aremoresuitableforlessfrequentaccessingbutlong-termuse,whereas skin-tunnelled CVCs are recommended for intensive access. The maximum time a port can remain in placehasnotyetbeendeterminedbuthavebeenreportedtobeusedforaslongasfiveyearsorupto2000needlepunctures.Portsshouldbereplacedonlyonclinicalindications(i.e.,clinicalinfection)andallfluidadministration tubing and connectors replaced when the port is replaced.
3.1.7.v Replacement of PICCsPICC’sshouldbereplacedonlyonclinicalindications,(i.e.,clinicalinfection+/-purulenceattheinsertionsite). AllfluidadministrationtubingandconnectorsshouldbereplacedwhenthePICCisreplaced. Guidewire exchanges should not be used routinely for PICC to prevent infection. Guidewire exchanges of PICCs are not recommended in the presence of BSI.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-29-
3.1.8 CVC Care BundlesCare bundles are groupings of evidence-based best practices with respect to a disease process that individuallyimprovecare,butwhenappliedtogetherresultinsubstantiallygreaterimprovement.Thesciencesupportingthebundlecomponentsissufficientlyestablishedtobeconsideredstandardofcare.TheCVCbundleisagroupofevidence-basedinterventionsforpatientswithCVCs,thatwhenimplementedtogether result in better outcomes than when implemented individually. All the elements of the care bundle mustbeadheredtoforeverypatient,everytimetheprocedureisperformed(e.g.,CVCinsertionorCVCmaintenance). The key components of the CVC bundle are outlined in Table 3.1. Healthcare facilities may wish to monitor CVC insertion and maintenance separately. An example of a CVC insertion checklist is provided in Appendix 10 and of a CVC maintenance bundle in Appendix 11.
Use of a CVC insertion checklist should be encouraged to ensure that all processes related to CVC placement are executed for each CVC placement thereby leading to consistency in CVC insertion. This checklistincludesalistofactivitiesthatareconsideredstandardbefore,during,andaftertheprocedure,aswell as a safety checklist. The elements of the checklist and its implementation should be agreed in advance by all relevant HCW involved in inserting and caring for CVCs. CVC insertion should be observed by a HCW who has received appropriate education to ensure that aseptic technique is maintained. The observer will assistinidentifyingbreachesinaseptictechnique,whichifobservedshouldresultintheprocedurebeingaborted and restarted.
CompliancewithaCVCbundleisdefinedasthepercentageofpatientswithCVCsforwhomallelementsofthe CVC bundle are documented. This measure is an assessment of how well the unit/ward is adhering to theCVCbundle.Therefore,itisimportanttomeasurecompliancewiththeentirebundle,notjustpartsofit.Itisworthwhilenotingthatthisisan‘allornothing’indicator.Onagivenday,allpatientswithCVCsintheunit/ward being studied are selected and assessed for compliance with the CVC bundle. If one element of thebundleismissing,thecaseisnotincompliancewiththebundleandscoreszero.Ifallelementsofthebundleareperformed,thecaseisincomplianceandscoresone.Forexample,iftherearesevenpatientswithCVCsandsixhaveallfivebundleelementscompletedthenthereis86percent(sixdividedbyseven)compliancewiththeCVCbundle.Ifallsevenpatientshadallfiveelementscompleted,compliancewouldbe100percent.Ifallsevenweremissingevenasinglebundleitem,compliancewouldbe0percent.ThesampleshouldincludeallpatientswithCVCsintheunit/wardbeingstudied.Onlypatientswithallfiveelements of the CVC bundle in place are recorded as being compliant. If a bundle element is contraindicated foraparticularpatientandthisisdocumentedappropriatelyonthechecklist,thenthepatientcanstillbeconsidered compliant with regard to this measure.
Table 3.1 CVC care bundle components58
Element of CVC care bundle
Hand Hygiene 1. Include hand hygiene as part of your checklist for CVC placement.
2.Keepsoap/alcohol-basedhandwashingdispensersprominentlyplacedandmakeStandardPrecautionsequipment,suchasgloves,onlyavailablenearhandhygieneequipment.
3. Post signs at the entry and exits to the patient room as reminders.
4.InitiateacampaignusingpostersincludingphotosoflocalHCWrecommendinghandhygiene.
5. Create an environment where reminding each other about hand hygiene is encouraged.
6.Signsoftenbecome‘invisible’afterjustafewdays.Trytoalterthemweeklyormonthly(colour,shape size).
Maximal Barrier Precautions upon insertion
1. Include maximal barrier precautions as part of your checklist for CVC placement.
2.KeepequipmentreadystockedinacartforCVCplacementtoavoidthedifficultyoffindingnecessary equipment to institute maximal barrier precautions.
Chlorhexidine skin antisepsis
1. Include chlorhexidine antisepsis as part of your checklist for CVC placement.
2. Include chlorhexidine antisepsis kits in carts storing CVC equipment.
3. Ensure that solution dries completely before an attempted line insertion.
Optimal CVC site selection
Include optimal site selection as part of your checklist for CVC placement with room for appropriate contraindications(e.g.,bleedingrisks).
Daily review of CVC necessity
1. Include daily review of CVC necessity as part of your multidisciplinary rounds.
2. Include assessment for removal of CVCs part of your daily record.
3. Record time and date of line placement for record keeping purposes and evaluation by staff to aid in decision making.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-30-
3.2 SurveillanceHCAI surveillance is a key requirement under SARI and a requirement under European Commission decision2119/98/.WithoutHCAIsurveillance,thetrueburdenofHCAIisunknown.Developmentofa high quality surveillance system is essential to monitor HCAI including CRBSI and identify areas for improvement. Such an initiative will save public monies and is an essential component under the quality and safety of patient care.
ThereisalargevariationintheincidenceofCRBSIdependingonthetypeofintravascularcatheterused,thefrequencyofcathetermanipulationandthepatient’sunderlyingriskfactorsofdiseaseandseverityof illness. The incidence of infections associated with PVCs (the most frequent used device for vascular access)isusuallylow,howeverseriousinfectiouscomplicationsresultinhighmorbidityratesduetothehigh frequency of use. The majority of serious intravascular catheter-related infections are associated with CVCs,especiallyinICUpatients.Astudyinan18-bedmedicalICUofalargeteachinghealthcarefacilityin Geneva reported an incidence rate of 5.8/1000 central-line days for microbiologically documented BSIs,withdramaticdecreasesoccurringfollowingimplementationofaprogrammetargetedatvascular-access care.59 This same study reported an incidence rate of 19.8/1000 central-line days if clinical sepsis surveillancewasalsoincluded,reflectingtheimportanceofestablishingaccuratesurveillancedefinitionsatthe outset of a programme and not changing them during the programme.
3.2.1 Surveillance in Other Countries
TheUnitedStateshavebeencollectingdatausingtheCDC’sNationalNosocomialInfectionSurveillanceSystem (NNIS) on the incidence and aetiology of CRBSI in over 300 US healthcare facilities since the 1970s. Themajorityofhealthcarefacility-acquiredBSIsareassociatedwiththeuseofaCVC,withhigherBSIratesobserved in patients with CVCs compared to those without CVCs.10 Incidence rates of 5 per 1000 central-line days have been reported;60however,therateofCVC-associatedBSIvariesconsiderablydependingonhealthcarefacilitysize,patienttype,ward/unittypeandtypeofCVC.In2005,TheNationalHealthcareSafetyNetwork(NHSN)wasestablishedtointegratethreeCDCsurveillancesystems(theNNISsystem,theDialysisSurveillanceNetwork,andtheNationalSurveillanceSystemforHealthcareWorkers).61 The NHSN hasboth‘PatientSafety’and‘HealthcarePersonnelSafety’surveillancecomponents.Withinthe‘PatientSafety’component,dataarecollectedusingCDCstandardisedmethodsanddefinitionsandaregroupedintospecificmoduleprotocols
(device-associated,procedure-associatedandmedication-associated).The
modulesmaybeusedsinglyorsimultaneously,but,onceselectedtheymustbeusedforaminimumofonecalendarmonth.SimilartotheNNISsystem,participatingNHSNfacilitiesvoluntarilyreporttheirHCAIsurveillance data for aggregation into a single na tional database. The device-associated mod ule includes surveillance of CVC-associated primary BSI in both adult and paediatric settings and may also be used by facilitiesotherthanhealthcarefacilities,includingoutpatientdialysiscentres.InNICUs,dataiscollectedoncentralline-associatedandumbilicalcatheter-associatedprimaryBSI.In2006-2007,ICUratesofCVC-associated BSI ranged from 5.6 (in a burns critical care unit) to 1.0 (in a paediatric medical critical care unit)BSIsper1000CVCdays,inpatientwardratesfrom2.4(adultstep-downpostcriticalcare)to0.5(rehabilitation) BSIs per 1000 CVC days and CVC-associated BSI rates in permanent lines were 3.9 (bone marrow transplantation) and 1.7 (haematology-oncology).62
A number of European countries have established national nosocomial surveillance programmes; for example,theNosocomialInfectionNationalSurveillanceScheme(NINSS)inEngland,theKrankenhaus-Infektions-SurveillanceSystem(KISS)inGermanyandthePREventievanZIEkenhuisinfectiesdoorSurveillance(PREZIES)intheNetherlands.Thesearenotmandatorysurveillanceschemesandtargetdifferentinfections/patienttypes.NonationalCRBSIdatacollectionschemeexistsintheUnitedKingdom.Speciality-specificBSIrates/1000patient-daysareprovidedinEnglandandthereareplansthattheNational Patient Safety Agency in England will run a dedicated national patient safety initiative to tackle CVC-related BSI commencing 2009.
3.2.2 Setting up SurveillanceCRBSI can be prevented by appropriate insertion and maintenance (Section 3.1) and by monitoring CRBSI rateswithasurveillanceprogramme.IntheRepublicofIreland,healthcarefacilitiesdifferinthetypesofsurveillance resources available to them as well as in their needs for surveillance of categories of HCAI. HCAI surveillance including CRBSI surveillance must start and end with the patient in order to improve

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-31-
patientcare.LocalCRBSIsurveillanceprogrammesmustberelevanttotheneedsoftheirpatientsandlocalpriorities,thereforeaCRBSIsurveillanceprogrammeshouldbeintroducedinahealthcarefacilityasdictated by the specialities and requirements of that facility and the resources available for surveillance. ThisprogrammewilldetermineHCACRBSIrates,monitortrendsinratesandassistinidentifyinglapsesininfection control practices. Areas that may be included in a CRBSI surveillance programme are: oICU/NICU, oSpecialtycareareas(e.g.,haematology/oncology,transplant,dialysis,longtermacutecare,
interventionalradiology,TPN), o Any other inpatient location in the healthcare facility where denominator data can be collected
(e.g.,surgicalormedicalwards).
3.2.3 Surveillance InfrastructureHealthcaremanagersmustsupportsurveillanceactivities,includingsurveillanceofCRBSI.InordertoimplementaCRBSIprogrammebothlocallyandnationally,ring-fencedfundingwillneedtobeassignedtofillgapsinsurveillanceinfrastructure(ITandpersonnel).Recentguidelinesrecommendthefollowinginfrastructural requirements to prevent CRBSI:13
An adequately staffed infection prevention and control programme responsible for identifying patients •with CRBSI. Information technology to collect and calculate catheter-days as a denominator for computing rates of •CRBSI and patient-days to allow calculation of CVC utilisation. Catheter-days from information systems should be validated against a manual method.Resources to provide appropriate education and training.•Adequate laboratory support for timely processing of specimens and reporting of results.•
Inadditiontotheabove,theCommitteerecommendthefollowingforeachhealthcarefacilityinordertoestablish a CRBSI surveillance programme. Many of these resources will also support other surveillance activities:
A local multidisciplinary steering committee should be established with representatives from the relevant •area(s)inwhichsurveillanceistocommence(e.g.,ICU,haemodialysis,medicalmicrobiology,infectiousdiseases,infectionpreventionandcontrolandseniormanagement)tohelpdrivethesurveillanceproject,encouragecomplianceandadvisetherelevantarea(s)andhealthcarefacilitymanagementbased on the results of surveillance data.
Appointment of a dedicated surveillance coordinator has been demonstrated to be crucial to the •success of surveillance in Irish healthcare facilities with pre-existing surveillance programmes. This would beafull-timepositionwithresponsibilitiesincoordinatingtheprocess,trainingstaff,followinguponsurveillanceforms,liaisingwiththeanalysisteamandfeedingdatabacktotherelevantunits.Forsmallerhealthcare facilities this post might be combined with another role or shared between two smaller healthcare facilities.
Administrative support for the surveillance coordinator. •
3.2.4 Case Definitions and DenominatorsTheCommitteerecommendthatinternationallycomparablecasedefinitionsandprotocolsareemployed.ThemostcommonCRBSIdefinitionsusedinEuropeareCDCandHELICSdefinitions.IntheabsenceofagreedEuropeandefinitions,theCommitteerecommendthatCDCdefinitionsbeemployedandthatCRBSIprotocolsarestandardisedandadheretootherinternationalframeworks(e.g.,CDC)forcomparative analysis of CRBSI incidence rates. This will enable comparison of rates with other healthcare facilitiesand/orpublisheddata.AccordingtoCDCdefinitions,1primaryBSIareclassifiedaccordingtothecriteriaused,eitheraslaboratory-confirmedBSIorclinicalsepsis.Clinicalsepsismaybeusedtoreportonlya primary BSI in neonates (≤ 30 days old) and infants (≤1 year old). BSIs are recorded as CVC-associated ifaCVCorumbilicalcatheterwasinplaceatthetimeoforwithin48hoursbeforeonsetoftheevent.Incontrast,purulentphlebitisconfirmedwithapositivesemiquantitativecultureofacathetertip,butwitheithernegativeornobloodcultureisconsideredaCVS-VASC,notaBSI(seepage14forCDCsurveillancedefinitions).
TheCDCandtheJointCommissiononAccreditationofHealthcareOrganisationsrecommendthattherateof CVC-associated BSIs is expressed as the number of CVC associated BSIs per 1000 CVC days.10

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-32-
3.2.5 Data Collection Forms and ProtocolACRBSIsurveillanceprogrammerequiresactive,patient-based,prospectivesurveillanceofCVC-associatedinfectionsandtheircorrespondingdenominatordatabydatacollectorstrainedinsurveillancedefinitionsandmethodology.Thedatacollectorseeksoutinfectionsduringapatient’sstaybyscreeningavarietyofdatasources,suchaslaboratory,pharmacy,admission/discharge/transfer,radiology/imaging,pathologydatabasesandpatientcharts(includinghistoryandphysicalexaminationnotes,nurses/physiciansnotes,temperaturecharts).Laboratory-basedsurveillanceshouldnotbeusedalone,unlessallpossiblecriteriaforidentifying an infection are solely determined by laboratory evidence. Retrospective chart reviews should be used only when patients are discharged before all information can be gathered. When denominator dataareavailablefromelectronicdatabases,thesesourcesshouldbeused.
The Committee have provided some examples of forms for CRBSI surveillance. (Appendices 12-13) The forms represent a template that can be used to guide healthcare facilities in the design of their own forms. Individual healthcare facilities may wish to include additional questions to the template form so that local needs can be met. It is strongly recommended that forms are designed using form-recognition software(e.g.,Teleform,Formic)toensurehighqualitydata.Notallhealthcarefacilitieshavescanningresources,therefore,surveillancedatacouldbecollated,scanned,validatedandanalysedataregionalornationallevel(withappropriateresourcing)inordertoreduceduplicationofworkandresources(i.e.,having multiple scanners in neighbouring healthcare facilities) or if there are existing IT systems within the healthcarefacilitythatcouldbeemployedforsurveillance,thesecouldalsobeusedforCRBSIsurveillanceratherthanscanning,wherefeasible.
Form1(Appendix12)isadailycountofallCVCsintheareaundersurveillance.Datashouldbe•collectedataspecifiedtimeeachday.Thiscountwillprovidethedenominatorvaluewhendeterminingthe number of catheter related infections per line days. The hospital code on this form refers to the EARSS code as supplied by the HPSC (this can be useful if data were be returned and analysed at a national level). Healthcare facilities may wish to adapt Appendix 12 to collect more detailed denominator data such as CVC types and site of insertion.
Form2(Appendix13)isfilledoutifaCRBSIissuspected,andcontainsclinicaldatacollectedbythe•clinical staff at the area under surveillance in conjunction with the medical microbiology/infectious diseasesteam.Form2alsocollectsthelaboratoryfindingswhichareusedinconjunctionwiththeclinicaldatatoconcludeCRBSIasdefinedinthecasedefinitions.Healthcarefacilitiesmaywishtocollect additional information such as isolates associated with CRBSI. An isolate coding system may be usedsuchastheWHONETdatabase(asurveillancesystemprovidedbytheWorldHealthOrganisation),available for download at http://www.who.int/drugresistance/whonetsoftware/en/.
The NHSN Manual: Patient Safety Component Protocol is available on-line and provides information on the appropriateCDCsurveillance methodology,includinginformationaboutbloodspecimen collection and surveillancedefinitions.Anumberofprotocolsareavailableincluding‘IdentifyingHealthcareassociatedInfectionsinNHSN’‘Device-AssociatedModule:Methodology’and‘Device-AssociatedModule:CentralLine-AssociatedBloodstreamInfectionEvent’.63TheHELICSprotocolforsurveillanceofnosocomialinfectioninICUs,containsasectiononsurveillanceofCVC-relatedinfection,inadditiontosurveillanceofother nosocomial infections.64 Surveillance in outpatient units such as haemodialysis units is outlined in Section 6.2.2.i.
3.2.6 Examples - Calculation of Device-associated Infection Fig3.3outlinesaprocedurethatmaybeusefulinidentifyingpatientswithCRBSI.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-33-
Patient with CVC inunit/ward
Positive blood culture
Is it CVC related?
Signs and symptoms as perdefinitions
Patient with CRBSI in unit/ward
How many each quarter?
How many each quarter?
Denominator
Numerator
CRBSI Rate
Fig 3.3 Identifying patients with CRBSI and calculating a CRBSI rate
The following examples may provide useful for calculation of device-associated infection rate.62
Decideonthetimeperiodforyouranalysis(e.g.,amonth,aquarter,ayear).•
Selectthepatientpopulationforanalysis(e.g.,thetypeoflocationorabirth-weightcategoryina•NICU).
Selecttheinfections(i.e.,CRBSI)tobeusedinthenumerator.Theymustbesite-specificandmust•have occurred in the selected patient population. Their date of onset must be during the selected time period.
Determinethenumberofdevice-days,whichisusedasthedenominatoroftherate.Device-daysare•thetotalnumberofdaysofexposuretothedevice(e.g.,CVC,umbilicalcatheter)byallofthepatientsin the selected population during the se lected time period.
Example: FivepatientsonthefirstdayofthemonthhadoneormoreCVCsinplace;5onday2;2onday3;5onday4;3onday5;4onday6;and4onday7.AddingthenumberofpatientswithCVCsondays1through7(5+5+2+5+3+4+4)=28CVC-daysforthefirstweek.Ifcontinuedfortheentiremonth,thenumberofCVC-daysforthemonthisthesumofthedaily counts.
Calculate the device-associated infection rate (per 1000 device-days) using the following formula:•
Device-associated infection rate = Number of device-associated infections for an infection site X 1000Number of device-days
Example: CRBSI rate per 1000 CVC-days = Number of CRBSI X 1000 Number of CVC-days
3.2.7 Feedback of Surveillance ResultsCRBSIratesmustbefedbacktotherelevantarea(s)andhealthcarefacilitymanagementonaregularbasis,ideallymonthly,butatleastquarterly.Thiswillenablethesteeringgrouptoadvisetherelevantarea(s)andhealthcare facility management based on the results of surveillance data and to monitor the effectiveness of preventative programmes. It is recommended that all clusters of HCA CRBSI and all episodes of HCA CVC/PVC-related S. aureus BSIareinvestigated(e.g.,byrootcauseanalysis).Inaddition,theintroductionof new intravascular catheters that includes needleless devices should be monitored for an increase in the occurrence of intravascular catheter-associated infection.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-34-
3.3. Management of CVC-related Infection4;15;65
3.3.1 Management of CVC Exit site InfectionForpatientswithexitsiteinfection,bloodculturesshouldbetaken,theexitsiteexudate(ifpresent)sentforcultureandempirictherapywithaglycopeptideantibiotic(e.g.,vancomycin)commenced.InhealthcarefacilitieswithalowrateofMRSA,flucloxacillinisanacceptablealternative.HoweverasmanyIrishhealthcarefacilitieshavemeticillinresistanceratesof35-40%inS. aureus isolates,itisrecommendedthat glycopeptide empiric therapy is used. The CVC should be removed if treatment with systemic antibiotics fails. Exchange of the CVC over a guidewire in the presence of an exit site infection may result inbacteraemiaandsepticemboliandisnotrecommended.ForpatientswithtunnelledCVCexitsiteinfection,itisimportanttoestablishthattheinfectionhasnotspreadtothetunnelorpocketoftheportasthis is an additional indication for removal and more prolonged antibiotic therapy. If there is no associated bacteraemia,thepatientshouldbemanagedasforacellulitisorsofttissueinfection.Ifbloodculturesarepositive,thentreatmentasforCRBSIisindicated.(Section3.3.4andFigs3.5and3.6)
3.3.2 Management of Tunnel Infections/Port AbscessSuccessful treatment of tunnel infections/port abscess without CVC removal is very unlikely. In the absence ofBSI,managementinvolvesCVCremoval,incisionanddrainageifindicated(sendingappropriatespecimens for culture) and 7-10 days of antimicrobial therapy. However many of these infections are associatedwithBSIandmanagementisasforcomplicatedCRBSI(i.e.,CVCremoval,incisionanddrainageifindicatedandantimicrobialtherapycontinuedforaprolongedduration).(Section3.3.4andFig3.6)
3.3.3 Management of Positive CVC Tips CVC tips cultures should only be performed when there is clinical suspicion of a CRBSI. In patients whoseCVCtipculturesrevealsignificantgrowth(Section5.2)intheabsenceofpositivebloodcultures,antimicrobialtherapyshouldnotbegivenonthebasisofapositiveCVCtipalone.Rather,thedecisiontoconsiderantimicrobialtherapywilldependonclinicalandmicrobiologicalfindings.Forexample,ifthepatientisafebrileandalowvirulenceorganismisolated(oramixedculture),thissuggestseitherCVCcolonisation (without systemic infection) or contamination of the line during removal and antimicrobial therapywouldnotnecessarilybeindicated.Incontrast,S. aureus or Candida spp. colonisation of an intravascular catheter is more likely to be associated with CRBSI than other organisms and CRBSI due to S. aureus and Candida spp. are more likely to cause metastatic and complicated infections.66-69Recent guidelines recommend that patients whose CVC tip grows S. aureus but whose initial peripheral blood cultures are negative should receive a 5-7 day antibiotic course and close monitoring for signs & symptoms of ongoing infection with repeat blood cultures accordingly.4
3.3.4 Management of CRBSIIntheinitialmanagementofthepatientwithsuspectedCRBSI,itisimportanttoensurethatthepatienthas a true CRBSI rather than contaminated blood cultures or fever from another source. As CVCs areintravascular,infectedcathetersmaycauseintravascularinfectionssuchasendocarditis,septicthrombophlebitisorbacteraemiawhichmayresultindistantseedingoftheinfectionresultingine.g.,osteomyelitis or psoas abscess. Short course treatment will only cure infections that have not seeded and where an intravascular infection has not been established. Serial blood cultures with documentation of thedurationandultimateclearanceofbacteraemia,tranoesophagealechocardiogram(TOE)andotherinvestigationsmayberequiredtocompleteapatientassessment.EveniftheCVChasbeenremoved,persistentbacteraemia/fungaemiaoralackofclinicalimprovement,especiallyifgreaterthan72hoursafter CVC removal and initiation of appropriate antimicrobial therapy mandates an aggressive workup for a complicated infection.
•Underlyingvalvularheartdisease.•Presenceofindwellingvascularprosthesis.•Prolongeddurationofthebacteraemia/fungaemia.•Presenceofsystemiccomplications.•CRBSIduetoS. aureus or Candida spp.
Fig 3.4 Risk factors for complicated CRBSI

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-35-
The management of CRBSI therefore involves making decisions related to:
3.3.4.i Empiric Antimicrobial TherapyEmpiric therapy should begin promptly as delays are associated with increased morbidity and mortality.7 Empiric antimicrobial treatment should be initiated after appropriate cultures are obtained. The antimicrobial(s) should be given intravenously and the choice of antimicrobial(s) should take into accounttheseverityofillness,thesiteofCVCinsertion,themostlikelypathogen(s)(includinggrampositivecocci)andlocalepidemiologicalfactorsincludingantimicrobialsusceptibilitydata.Knowledgeof the local epidemiology is essential when choosing an empiric antimicrobial as the presence of a high proportionofe.g.,vancomycin-resistantenterococcimayinfluencetheinitialchoiceofempirictherapy.Itis recommended that local antimicrobial guidelines address empiric therapy of CRBSI to assist doctors in making appropriate empiric choices for that healthcare facility.
AlthoughtherearenodatathatsupporttheuseofspecificempiricalantimicrobialtherapyforCRBSI,glycopeptides(e.g.,vancomycin)areusuallyrecommendedinthosehealthcarefacilitieswithanincreasedprevalence of MRSA.Otherwisepenicillinase-resistantpenicillins(e.g.,flucloxacillin)shouldbeused.ForhealthcarefacilitieswithapreponderanceofMRSAisolateswithvancomycinMICvalues>2 µg/ml,alternativeagentssuchasdaptomycinareindicated.4 It is not recommended that linezolid be used aspreliminarydatashowedincreasedmortalityinpatientswithCVCinfectionsreceivingthisagent,however,itappearsthatthisincreaseinmortalitywasduetoinadequategram-negativecover.70 Septic and immunocompromised patients should receive additional gram negative cover with the addition of a β lactam(suchaspipericillin/tazobactamorceftazidime),anaminoglycosideorafluoroquinolone(thechoiceof second agent will be governed by local antimicrobial susceptibility data). Antifungal agents (choice depending on local epidemiology of Candida spp.)71 should be considered for empirical treatment when fungaemia is suspected. Once antimicrobial susceptibility data are available targeted treatment with potentialde-escalationshouldoccur.(Section3.3.4.ii)
Thedurationofantimicrobialtherapywillbedeterminedbytheorganismidentified,thepresenceofcomplicationsandwhethertheCVChasbeenremovedandisoutlinedbelow.Ingeneral,amoreprolongedcourseofantimicrobialtherapy(duration4–6weeks)shouldbeconsideredifthereis:
Prolongedorpersistentbacteraemia/fungaemiaafterCVCremoval(i.e.,occurring>72hoursafter•removal).Evidence of endocarditis. •Evidence of suppurative thrombophlebitis.•Clinical evidence of a metastatic focus of infection.•Osteomyelitis in paediatric patients (6-8 weeks of therapy is recommended for treatment of •osteomyelitis in adults).
3.3.4.ii Definitive Antimicrobial TherapyCVCtipandbloodculturesresultsshouldidentifytheinfectingorganism,determineifthereisanassociated BSI and give information on antimicrobial susceptibilities. This allows for targeted antimicrobial therapyandmayassistintheassessmentoftheneedforCVCremoval.Figs3.5and3.6outlinerecommendations for CRBSI management when the organism is known.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-36-
Non-tunnelled CVC CRBSI
Remove CVC and
treat with systemic antibiotic for 4-6
weeks; 6-8 weeks for osteomyelitis
Coagulase-negative staphylococci
(except S. lugdunensis)
S. aureus and
S. lugdunensis
Enterococcus spp.
Gram negative bacilli
Candida spp.
• Remove CVC* and treat with systemic antibiotic for 5-7 days
• If CVC is retained, treat with systemic antibiotic (+/- antibiotic lock) therapy for 10-14 days
Remove CVC and
treat with systemic
antibiotic for minimum 14
days
Remove CVC and
treat with systemic
antibiotic for 7-14 days
Remove CVC and
treat with systemic
antibiotic for 7-14 days
Remove CVC and
treat with antifungal therapy for 14 days after
first negative blood culture
Complicated infection Prolonged or persistent bacteraemia/fungaemia after CVC removal (i.e., occurring >72 hours after removal)Evidence of endocarditis Evidence of suppurative thrombophlebitisClinical evidence of a metastatic focus of infectionOsteomyelitis
Uncomplicated infection BSI and fever resolves within 72 hours in a patient without an active
malignancy or immunosuppresion who has no other intravascular devices and no evidence of endocarditis or suppurative thrombophlebitis
*Infections may resolve in patients without intravascular/orthopaedic prosthesis/devices with CVC removal alone (and no antibiotic therapy).BloodculturesshouldberepeatedafterCVCwithdrawaltoconfirmtheabsenceofbacteraemia.
Figure 3.5 Management of CRBSI associated with non-tunnelled CVCs

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-37-
S. aureus and
S. lugdunensis
Enterococcus spp.
Gram-negative bacilli
Candida spp.
Tunnelled CVC/port related CRBSI
Complicated infection Prolonged or persistent bacteraemia/fungaemia after CVC removal (i.e., occurring >72 hours after removal)Evidence of endocarditis Evidence of suppurative thrombophlebitisClinical evidence of a metastatic focus of infectionOsteomyelitis
Uncomplicated infection BSI and fever resolves within 72 hours in a patient without an active
malignancy or immunosuppresion who has no other intravascular devices and no evidence of endocarditis or suppurative
thrombophlebitis
Remove CVC/P and
treat with antibiotics for 7-10
days
Coagulase-negative staphylococci
(except S. lugdunensis)
Septic thrombosis, endocarditis, osteomyelitis
Tunnel infection, port abscess
Remove CVC/P and
treat with systemic antibiotics for 4-6 weeks: 6-8 weeks
for osteomyelitis in adults
May retain CVC/P & treat with
systemic antibiotic ± antibiotic lock
therapy for 10-14 days
Remove CVC/P if clinical
deterioration and/or persisting bacteraemia &
outrule complicated
infection
Remove CVC/P and
treat with systemic antibiotics for 4-6
weeks Unless suitable for
shorter (min 14 days) course
therapy*
May retain CVC/P & treat with
systemic antibiotic ± antibiotic lock therapy for 7-14
daysRemove CVC/P if
clinical deterioration,
persistent bacteraemia, insertion site/
pocket infection, suppurative
thrombophlebitis, endocarditis, or
metastatic infection, work-up for complicated
infection and treat accordingly
Remove CVC/P & treat for 7-14
daysFor CVC/P
salvage, use systemic &
antibiotic lock therapy for
10-14 days; if no response,
remove CVC/P, rule out
endocarditis or suppurative
thrombophlebitis, and if not
present treat with antibiotic for 10-14 days
Remove CVC/P & treat with antifungal
therapy for 14 days after the first negative blood culture
*Patientscanbeconsideredforashorterdurationofantimicrobialtherapy(i.e.,a minimum of 14daystherapy)iftheinfected tunnelled CVC / port is removed and
Feverandbacteraemiaresolvewithin72hoursofinitiatingappropriateantimicrobialtherapy.•Thepatienthasnoprostheticintravasculardevice(e.g.,pacemaker,recentlyplacedvasculargraft).•ThereisnoevidenceofendocarditisorsuppurativethrombophlebitisonTOEandultrasound,respectively.•There is no evidence of metastatic infection on physical exam and sign/symptom-directed diagnostic tests. •
Thepatientisnotdiabetic,notimmunosuppressed(i.e.,notreceivingsystemicsteroids,neutropaenia,orotherimmunosuppressivedrugs such as those used for transplantation).
Figure 3.6 Management of CRBSI associated with tunnelled CVCs or ports (CVC/P)
3.3.4.ii.a Coagulase-negative staphylococci Coagulase-negative staphylococci are the most common cause of CRBSI. However they are also the most common blood culture contaminants and accurate diagnosis of CRBSI is of particular importance.65 If a singlepositivebloodculturegrowscoagulase-negativestaphylococci,bloodculturesshouldberepeated(through the CVC and from a peripheral vein) before initiation of antimicrobial therapy and/or CVC removal to ensure that the patient has a true CRBSI. Microbiologic data suggestive of true CRBSI rather than contamination include the following;
Multiple positive blood cultures drawn from different sites.•Isolation of the same organism from a CVC tip and a peripheral blood culture.•CVC blood culture positive at least two hours earlier than the blood drawn from a peripheral vein.•

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-38-
Severesepsisisrare.FeverandinflammationattheCVCexit-sitearemorecommonclinicalmanifestationsof coagulase-negative staphylococcal CRBSI.15 The one exception is CRBSI due to Staphylococcus lugdunensis which is associated with endocarditis and metastatic infection and should be managed similar to S. aureus.4(Section3.3.4.ii.b)
There are no randomised trials evaluating treatment of coagulase-negative staphylococcal CRBSI. Management includes:
Consideration of CVC removal (non tunnelled CVCs). •Treatment with appropriate antibiotics; •
o CVC removed: Such infections may resolve with CVC removal alone and some recommend no antibiotic therapy in patients without intravascular or orthopaedic prosthesis/devices unless fever and/orbacteraemiapersistafterCVCremoval.However,othersrecommendantibiotictherapyfor 5-7 days if the CVC is removed.4
oCVCretained:Treatfor10-14dayswithconsiderationofantibioticlocktherapy.(Section3.3.4.iii)
Ifthereisclinicaldeteriorationorpersistingbacteraemia,theCVCshouldberemoved(ifstill• in situ) and complicated infection outruled.
The choice of antibiotics used should be based on the local antimicrobial susceptibility patterns - for meticillinresistantisolates,aglycopeptidecouldbeconsidered;formeticillinsensitiveisolatesapenicillinase-resistantpenicillin(e.g.,flucloxacillin)orfirst-generationcephalosporinisanappropriatechoice.
3.3.4.ii.b Staphylococcus aureusS. aureus isassociatedwithahighrateofdeep-seatedmetastaticinfections,includingsepticthrombosisand endocarditis. Removal of the CVC in S. aureus CRBSI (including uncomplicated cases) is associated with a more rapid response to therapy and a lower relapse rate.65 Non-tunnelled CVCs should be removed immediately for S. aureus CRBSI.4
ForS. aureus CRBSIinvolvingtunnelledCVCs/ports,theCVC/portshouldberemovedunlesstherearemajor contraindications. Relative contraindications to CVC removal include lack of alternative venous access and profound thrombocytopenia. In these cases consideration can be given to catheter salvage andantibioticlocktherapyinconjunctionwithsystemicantibiotictherapyfor4weeks.4;65ForpatientswithCRBSIinwhomCVCsalvageisattempted,repeatbloodculturesshouldbeobtainedandtheCVCremovedifbloodcultures(e.g.,twosetsofbloodculturesonagivenday)remainpositivewhendrawn72hours after initiation of appropriate therapy.4
Patients with uncomplicated S. aureusCRBSIshouldhavetheinfectedCVCremovedandreceive4to6weeksofantimicrobialtherapyunlesstheyaresuitableforashorterdurationoftherapyasoutlinedinFig3.7.4 Patients who are being considered for a shorter duration of therapy should have a TOE performed ideally 5-7 days after onset of bacteraemia and other investigations performed to outrule metastatic infection.
Identifying patients without risk factors for haematogenous complications and pursuing a full evaluation formetastaticinfectionisimportantbeforeproceedingtoshort-coursetherapy.(Fig3.7)Predictorsofhaematogenous complications include positive blood cultures 72 hours after initiation of appropriate antimicrobialtherapyandCVCremoval,community-acquiredinfection,skinchangesconsistentwithseptic emboli and failure or delay in removing the CVC. Patients with prosthetic devices and those on haemodialysis,orpatientswhoarediabeticorimmunosuppressedarealsoathigherriskofhaematogenouscomplications.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-39-
The infected CVC is removed
and
Feverandbacteraemiaresolvewithin72hoursofinitiatingappropriateantimicrobialtherapy.•
Thepatienthasnoprostheticintravasculardevice(e.g.,pacemaker,recentlyplacedvasculargraft).•
ThereisnoevidenceofendocarditisorsuppurativethrombophlebitisonTOEandultrasound,•respectively.
There is no clinical evidence of metastatic infection. •
Thepatientisnotdiabetic,notimmunosuppressed(i.e.,notreceivingsystemicsteroidsorother•immunosuppressive drugs such as those used for transplantation and is not neutropenic).
Fig 3.7 Patients with S. aureus CRBSI that can be considered for a shorter duration of antimicrobial therapy (i.e., a minimum of 14 days therapy)
A repeat TOE should be performed in patients with persistent fever or BSI 72 hours or more after CVCremovalandinitiationofappropriateantibiotics,iftheyhadanearlierTOEwithoutevidenceofendocarditisandinwhomthere’snoevidenceofanundrainedmetastaticinfection.
The choice of antibiotics used should be based on the local susceptibility patterns of S. aureus.ForMSSAasemisyntheticpenicillinase-resistantpenicillinorfirst-generationcephalosporinisthefirstchoice.ForMRSA,severaloptionscanbeconsidered,includingglycopeptidesordaptomycin(forMRSAisolateswith vancomycin MIC values >2 µg/ml; vancomycin has a lower clinical success rate in treating MRSA bacteraemia if the MIC is >2 µg/ml).
3.3.4.ii.c Enterococcus spp.In2008inIreland,CVCsrepresentedtheprimarysourceof23%(14/61)ofvancomycinresistantand14%(29/199) of vancomycin susceptible enterococcal bacteraemia.72 Removal of the infected non-tunnelled CVCisrecommendedinenterococcalCRBSI.InthecaseoftunnelledCVCs/ports,bloodculturesshouldbe repeated and the CVC retained. However CVC removal is recommended if there is insertion site or pocketinfection,suppurativethrombophlebitis,sepsis,endocarditis,persistentbacteraemiaormetastaticinfection.ForuncomplicatedenterococcalCRBSI7-14daysofantibiotictherapyisrecommended.ATOE should be performed if endocarditisisclinicallysuspected,ifthepatienthasprolongedbacteraemiaorfeverdespiteappropriateantimicrobialtherapy,ifthereisradiographicevidenceofsepticpulmonaryemboli or the patient has a prosthetic valve or other endovascular device in situ. ForpatientswithCRBSIinwhomCVCsalvageisattempted,repeatbloodculturesshouldbeobtainedandtheCVCremovedifbloodcultures(e.g.,twosetsofbloodculturesonagivenday)remainpositivewhendrawn72hoursafterinitiation of appropriate therapy.4
Ampicillin is recommended for treatment of ampicillin-sensitive enterococcal CRBSI and a glycopeptide (e.g.,vancomycin)shouldbeusediftheisolateisampicillin-resistant.Theroleofcombinationtherapy(i.e.,a cell wall-active antimicrobial and an aminoglycoside) for treating enterococcal CRBSI without endocarditis is unresolved. In cases of CRBSI due to ampicillin- and vancomycin-resistant Enterococcus spp.,linezolidor daptomycin may be used based on antibiotic susceptibility results. Antibiotic lock therapy may be considered in addition to systemic antibiotics if CVC salvage is attempted.
3.3.4.ii.d Gram negative bacilliGramnegativebacteraemiausuallyarisesfromanonCVC-relatedsource,suchasurinarytractorintra-abdominalinfection.InpatientswithgramnegativeCRBSI,failuretoremovetheCVCisassociatedwithasignificantlyhigherrateoftreatmentfailureandbacteraemiarecurrence.65 There is limited data on the use ofantibioticlocktherapy.Therefore,ifthegramnegativebacillarybacteraemiaisjudgedtobeaCRBSI,thenitisprudenttoremovetheCVCandtreatwitha7-14daycourseofappropriateantibioticsguidedbyantimicrobial susceptibility results. If the patient has a tunnelled CVC/port and CVC salvage is attempted (systemicantibioticswithorwithoutantibioticlock),bloodculturesshouldberepeatedandifthepatienthaspersistentbacteraemiadespiteappropriatetherapyorseveresepsis,theCVCshouldberemovedandcomplicated infection outruled.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-40-
3.3.4.ii.e Candida spp.CVCs are the leading source of candidaemia and antifungal therapy is recommended in all cases of CVC-related fungaemia.15 CVC removal is associated with improved outcome in non-neutropenic patients withcandidaemia.Inaretrospectivestudy,multivariateanalysisshowedthatCVCretentionformorethan72hourswasassociatedwithapooreroutcome(decreasedresponsetoantifungalagents,andincreasedmorbidity,andmortality).73 Antifungal therapy is recommended in all cases of Candida spp. CRBSI,includingpatientsinwhomclinicalmanifestationsofinfectionand/orcandidaemiaresolveafterCVCremovalpriortoinitiationofantifungaltherapy.Fluconazoleisrecommendedforazole-susceptiblestrains and echinocandins or amphotericin B for isolates with decreased susceptibility to azoles. There is limited data on the use of antifungal lock therapy. The duration of therapy for uncomplicated CVC-related candidaemiashouldbe2weeksfromthefirstnegativebloodculture.4
3.3.4.iii Antibiotic Lock Therapy Antibioticlocktherapy(ALT)involvestheinstillationofanantibioticcontainingsolutionintothelumenofaCVCinavolumesufficienttofillthelumen.Thesolutionisthenallowedtodwellforupto24hours.Thisprovides very high concentrations of antimicrobial agents at the site of infection with a low incidence of systemic toxicity of these antibiotics. WhiletheuseofALTtherapyhasbeenstudiedforpreventionofCVC-relatedinfection(Sections3.1.5.iiand3.1.5.iii),thereislimiteddatalookingattheusefulnessofALTinthetreatment of CRBSI. A recent review evaluated three comparative studies (systemic antimicrobial therapy ±ALT)and25noncomparativestudies(mainlycaseseries,ALTused±systemicantimicrobialtherapy)for treatment of CRBSI.74InonecomparativestudytherewasasignificantbenefitofadditionofALTtosystemic antimicrobial therapy in terms of longer catheter survival in haemodialysis patients.75However,nosignificantdifferencewasfoundwithrespecttotreatmentsuccessofCRBSIbetweensystemicantimicrobialtherapywithandwithoutALTinthetwoothercomparativestudies.76;77 Treatment success as high as 75% wasreportedinthenoncomparativestudies,howevertherewasconsiderablevariabilitybetweenstudieseven when they evaluated similar patient populations.74 While there appears to be a trend towards the benefitofALT,thereisaneedforwell-designedlargecomparativestudiesusingstandardiseddefinitionstoexamineiftheadditionofALTtoCRBSImanagementisindeedofbenefit.Situationsthatappeartobeassociated with lower treatment success are infection with S. aureus and Candida spp.,infectionsoftotallyimplanted devices and in patients with underlying HIV infection.74Therefore,CVCremovalisrecommendedfor S. aureus and Candida spp.CRBSIratherthanCVCsalvagewithsystemicandlockantimicrobials,unlessthereareunusualextenuatingcircumstances(e.g.,noalternativeCVCinsertionsite).ALTmaybeausefuladjuncttosystemicantibioticsinsituationswhereremovaloftheCVCisparticularlydifficultorwherevenousaccessislimited(i.e.,CVCsalvage).ALTshouldalwaysbeusedinconjunctionwithsystemicantibiotictherapy.InselectingpatientsconsiderationneedstobegiventotheCVCinfection(i.e.,tunnel/portpocketinfectionsshouldnotbeconsideredforCVCsalvage),theidentifiedorganism,selectedantibioticanddosingandtheneedforasufficientdwelltime.RecentguidelinesrecommendthatifCVCsalvageisattemptedandALTcannotbeused,administrationofsystemicantibioticsshouldbeconsideredthrough the colonised CVC.4
3.3.5 CVC Removal and Guidewire ExchangeInpatientswithBSIandanindwellingCVC,therecanbeatendencytoassumethediagnosisofaCRBSI.However,asdiscussedpreviously,itisimportanttoruleoutothersourcestoavoidunnecessaryCVCremoval.Frequently,thedevelopmentofclinicalsepsiswithoutaprimarysourceofinfectionleads to the suspicion of a CVC-related infection.10 Insuchsituations,acatheter-relatedinfectionwillbemicrobiologicallydocumentedinonly20-30%ofcases.Asdiscussedabove,onlyaminorityofCVCsassociated with a BSI can be retained and the decision to retain an infected CVC should be based on anindividualisedrisk-benefitassessment,whichshouldinclude;considerationofthetypeofCVC,theongoingneedfortheCVCandfeasibilityofplacingalternativevascularaccess.Ingeneral,thedecisionto maintain the CVC should only be considered in patients with no evidence of sepsis or in patients with potentialtechnicaldifficultiesininsertingaCVCatanewsite.ThebenefitofmaintainingaCVCneedstobebalancedwiththepotentialseriouscomplications,suchasendovascularandormetastaticinfections.ForpatientswithCRBSIinwhomCVCsalvageisattempted,repeatbloodculturesshouldbeobtainedandtheCVCremovedifbloodcultures(e.g.,twosetsofbloodculturesonagivenday)remainpositivewhendrawn 72 hours after initiation of appropriate therapy.4

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-41-
In cases without local signs of infection at the insertion site and in the absence of or pending positive bloodcultures,guidewireexchangeofthedevicehasbecomeastandardpracticeinsomehealthcarefacilities.78 Despitetheabsenceofstrongevidencesupportingthispractice,itisrecommendedbysomeexperts and guidelines.10However,aspreviouslydiscussedinthisdocument,guidewiretechniquesshouldnot be used to replace CVCs in patients suspected of having CVC-related infection. Guidewire-assisted CVC exchange to replace a malfunctioning CVC or to exchange an existing CVC should be used only if thereisnoinfectionattheCVCsiteornosuspicionofCRBSI.Ifafteraguidewireexchange,investigationsrevealCRBSI,thenewlyinsertedCVCshouldberemovedandifstillrequiredreinsertedatadifferentsite.InselectedpatientswithtunnelledhaemodialysisCVCsandbacteraemia,CVCexchangeoveraguidewire,incombinationwithantibiotictherapy,mightbeanalternativeasasalvagestrategyinpatientswithlimitedvenous access.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-42-
4. Peripheral Vascular Catheters (PVCs)
4.1 Prevention of PVC Infection 4.1.1 Hand Hygiene, Aseptic Technique and Skin AsepsisInordertopreventcontaminationofPVCsitesandsubsequentBSI,handhygieneandaseptictechniqueasoutlined in Sections 2.1 and 2.2 must be performed:
Before PVC insertion (both before and after palpating the PVC insertion site). •BeforePVCaccessormaintenance(e.g.,dressingmanipulations).•
Iftheskinisvisiblydirty,itshouldbewashedpriortoskinasepsis.Inadultsandchildren≥ 2 months (assumingnormalgestationatbirth),asinglepatientuseapplicationofalcoholicchlorhexidinegluconatesolution (preferably 2% chlorhexidine gluconate in 70% isopropyl alcohol if compatible with the PVC) should be used;
•ForskindisinfectionpriortotheinsertionofaPVC.•TodisinfectthePVCinsertionsiteduringdressingchanges.•PriortoaccessingthePVChub.
Skin should be allowed to air dry prior to further manipulation. Hub/port decontamination with 70% alcohol,allowingthehub/porttodrypriortofurthermanipulationisanacceptablealternativeto2%chlorhexidine in 70% isopropyl alcohol.
0.5-1%chlorhexidineistheoptimalrangeforneonatal(<2months)skinasepsis,however,randomisedcontrolled trials are required to clarify this range. (Section 3.1.2.i)
4.1.2 Selection of PVC TypeIngeneral,itisrecommendedthatthesmallestgaugecannulaforthetreatmentthatisrequiredshouldbeused.Forinfusionsofviscousfluidssuchasbloodandforrapidinfusions,thelargestPVC(14–16gauge)shouldbeused.Smallersizes(18–20gauge)sufficeforcrystalloids.ThesmallestPVCs(20–24gauge)areadequatefortheintermittentadministrationofdrugs,exceptthosegivenbyrapidinfusion.Steelneedlesshould not be used due to the risk of extravasation and needlestick injury. PVC and steel-winged infusion sets (if used) should be equipped with a safety device with engineered sharps injury protection.
Table 4.1 Peripheral venous cannula gauge sizes, common uses and average flow rates (using H2O)79
Gauge Sizes Flow Rate(H2O) Uses
24G yellow 24ml/min Fragileveins,Paediatrics
22G blue 35ml/min MostMedications,Bloodandfluids
20G pink 62 ml/min LargeVolumesfluids,BloodTransfusion
18G green 104ml/min LargeVolumesfluids,Stemcell,BloodTransfusion
16G grey 215ml/min LargeVolumesfluids,Resuscitation,Anaesthetics
14G orange 350ml/min LargeVolumesfluids,ResuscitationAnaesthetics
4.1.3 Selection of PVC SiteTheriskofPVCinfectionisrelatedtotheriskforphlebitisandthedensityofskinfloraatthePVCsite.Specificpatientfactorsshouldbeassessedinadvancesuchas;pre-existingPVCs,anatomicdeformity,siterestrictions(e.g.,mastectomy,arteriovenousfistulaorgraft),therelativeriskofmechanicalcomplicationsandtheriskofinfection.Fig4.1outlinesguidanceforselectingasiteforPVCinsertion. The use of a short
extension set attached to the PVC can also reduce complications and is recommended.
Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-43-
Non-dominant forearm is preferred.•Avoidareasofflexionandbonyprominences.•T he basilic or cephalic veins on the posterior forearm are the preferred site. The metacarpal •
veinsonthedorsumofthehandareeasiesttovisualisebutaremoreliabletoblock,difficulttostabilise,andpronetoinfusateormedicationinducedvesseldamage.
The antecubital fossa veins should be reserved for emergency use. • The dorsum of the hand should be used in patients with chronic renal failure. The use of the •anterior (ventral) forearm veins (particularly the cephalic veins) is not recommended in patients with impending need for dialysis in whom preservation of upper extremity veins is needed for fistulaimplantation.Whenvenipunctureofthearmveinsisnecessary,sitesshouldberotated.
PVCs inserted into the lower limbs have a greater risk of thrombophlebitis and thrombosis than •the upper limbs and should only be used for the short term or in emergencies.
Initial sites should be in the distal areas of the upper extremities; subsequent PVCs should be •proximal to the previous PVC.
Fig 4.1 Selection of PVC site
4.1.4 Procedure for PVC Insertion, PVC Fixation and Maintenance of PatencyHandhygiene,aseptictechniqueandskinasepsismustbeperformedasoutlinedinSection4.1.1forinsertion and during all manipulations of the PVC. Prophylactic antibacterial or antifungal agents are not recommended at the time of insertion or during use of a PVC to prevent infection. It is recommended that each healthcare facility has a written PVC insertion guideline that is updated regularly/as new evidence becomesavailable.AnexampleofsuchaguidelineisprovidedinAppendix14.
The PVC should be stabilised with a sterile transparent semipermeable dressing and sterile adhesive tape to prevent dislodgement. The ability to visualise the PVC site and surrounding tissues must not be obscured with adhesive tape. Non-sterile adhesive tape should not be applied under the transparent semipermeable dressing. Adhesive tape should not be placed directly on the PVC-skin junction site. Flushingisrecommendedtopromoteandmaintainpatencyandpreventthemixingofincompatiblemedicationsandsolutions.TheoptimalvolumeandfrequencyofflushingofPVCsusedforintermittentinjections or infusions is unclear. It is recommended that;
PVCsareflushedwithaminimumof2mlsolution;•
o Afterplacement,
o Priortoandafterfluidinfusionorinjection,
o Or at least every 12 hours.
Sterile0.9%sodiumchlorideforinjectionisusedtoflushaPVC.•
Onlysingle-dosesolutionsareused.A10mL(orlarger)syringeshouldbeusedtoavoidexcessive•pressure(syringessmallerthan10mLcanproducehigherpressureinthePVC).
Flushinapulsatile(push-pauseorstart-stop-start)motion.•
Theflushsolutionandflushingintervalsisdocumented.•
ManagementofIVaccessories(hub/needlessdevices/bungs,administrationsetsetc)isoutlinedinSection3.1.6.
4.1.5 PVC Removal and Replacement4.1.5.i Daily ReviewAllPVCsshouldbereviewedatleastdaily,andthosethatarenolongerneededpromptlyremoved.Theinsertionsiteshouldbevisuallyinspectedforphlebitis,tenderness,PVCpositionandinfiltration.Thisshould occur regularly with continuous infusions and at least twice daily (on every shift) if no infusion. More frequent assessments may be necessary when using high-risk solutions and medications. PVC assessment should be clearly documented. A visual infusion phlebitis score may be used to assess for signs of phlebitis and to offer guidance as to whether PVC removal should be considered.80 (Appendix 15) Patients should beencouragedtoreportanydiscomfortsuchaspain,burning,swellingorbleeding.Fig4.2outlinestheprocedure for removal of PVCs.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-44-
Fig 4.2 PVC removal
4.1.5.ii PVC ReplacementScheduled replacement of PVCs has been proposed as a method to prevent phlebitis and PVC-elated infection.10;81 Studies suggest that the incidence of both phlebitis and bacterial colonisation increases when PVCs are left in place longer than 72 hours. However rates are not considerably different in PVCs left in place for 72 or 96 hours. Some studies appear to indicate that PVCs may be safely left in place for longer periods. Phlebitis ismorelikelytooccurinthetwodaysafterPVCinsertion,82-84 therefore removing a functional PVC and re-siting it may be an unnecessary and painful intervention for patients and costly fortheorganisation.Ithadbeenreportedthattherateofcomplications(phlebitis,CRBSIormechanicalcomplications) does not vary much between regularly changed PVCs and those staying more than three days.82Inonestudy,replacementofPVCsonlywhenclinicallyindicatedhadnoeffectontheincidenceofPVCfailure,onthebasisofphlebitisandinfiltrationwhencomparedwithroutinereplacementat72hours.85Inaddition,about3%ofPVCsremainedtrouble-free for over seven days and some for as long as two weeks. The authors proposed changing PVCs according to clinical signs and symptoms rather than
usingpredeterminedtimeframes,thoughacknowledgedthatlargertrialsareneeded.However,thisstudy has attracted some criticism including being underpowered and lack of applicability to healthcare facilities without dedicated nurse IV teams (the low incidence of phlebitis may be explained by the highlyexperiencedteamthathaveinsertedandprovidedcareofthePVCs),86 poor compliance to study protocolandahighdegreeofpatientexclusion.Overall,despitethecommonuseofPVCs in healthcare facilities and the almost universal acceptance of the need for routine replacement,thepracticeofroutinelyreplacing PVCs has received little attention in the literature and the value of periodic PVC replacement remains unresolved. The Committee recommend that replacement of PVCs is considered in adults every 72-96hourstopreventphlebitis.Insituationswhereperipheralvenousaccessislimited,thedecisiontoleavethePVCdwellingbeyond96hoursshoulddependonassessmentofthePVC,skinintegrity,lengthand type of prescribed therapy and should be clearly documented. When adherence to aseptic technique cannotbeensured(i.e.,whenPVCsareinsertedduringamedicalemergency),PVCsmustbereplacedassoon as possible.
Patients transferring from other healthcare facilities with a PVC in situ should have this device reviewed upon arrival and preferably replaced unless clinically contraindicated. PVCsshouldremaininplaceinchildrenuntilIVtherapyisfinishedunlesscomplicationssuchasphlebitisoccur.
Peripheral arterial catheters are usually inserted into the radial or femoral artery and permit continuous blood pressure monitoring and blood gas measurements. The rate of CRBSI is comparable to that of temporaryCVCs(2.9versus2.3per1,000PVCdays).10 Peripheral arterial catheters demonstrated no difference in infection rates between changing at scheduled times and changing on an as-needed basis.10 AstheriskforCRBSIislikelysimilartothatofshort-termCVCs,arterialcathetersshouldbeapproachedina similar way.
4.1.6 PVC Care Bundles (Appendix 16)Asdiscussedinsection3.1.8,a‘carebundle’isacollectionofevidence-basedinterventionsthatmaybeappliedtothemanagementofaparticularcondition,inthiscasetheinsertion,careandmanagementofPVCs.AswiththeCVCbundle,compliancewiththePVCbundleisdefinedasthepercentageofpatientswith PVCs for whom all elements of the PVC bundle are documented. The components of a PVC care bundleareoutlinedinTable4.2andAppendix16outlinesanexampleofaPVCbundle.
Perform hand hygiene and don non-sterile gloves. •Clean site thoroughly with alcoholic 2% chlorhexidine and allow to dry prior to removal. •Digitalpressurewithsterilegauzeshouldbeapplieduntilhaemostasisisachieved.•Coversitewithasteriledressing;removethedressingin24hours.•PVCsitesshouldbeobservedfor48hoursafterdeviceremovaltodetectpost-infusion•phlebitis.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-45-
Table 4.2 PVC Care bundle Components
Bundle component
Check the clinical indication why the PVC is in situ – is it still required?
ALL• PVCs are clinically indicated. If there is no clinical indication then the PVC should be •removed.
Remove PVCs where there is extravasation or inflammation.
The PVC site should be assessed for evidence of •phlebitisorinfiltrationanddocumentedonthePVCassessment form.
Check the PVC dressings are intact.Anintact,dry,adherenttransparentsemipermeable•dressing should be present.
Consider removing the PVC if it is in situ longer than 72 hours.
The date of PVC insertion should be clearly •documented Remove the PVC immediately when no longer clinically •indicated. Consider re-siting every 72-96 hours when in use (not applicable in paediatrics).The decision to leave the PVC dwelling beyond 72-96 •hours should depend on clinical assessment and be clearly documented.
Perform hand hygiene before and after all PVC procedures.
Decontaminatehands(antiseptichandhygieneagentoralcohol hand rub product)
before • and after each patient contact. and
before applying and on removal of gloves.•
4.2 PVC InfectionAllPVCsshouldbeclinicallyindicated.Asrecommendedpreviously,theneedforaPVCshouldbeassesseddaily(e.g.,couldthetherapybegivenbytheoralrouteinsteadand/orisitstillrequired)andthePVCremovedpromptlyifnolongerclinicallyindicated.PVCsassociatedwithpain,induration,erythemaor exudates should be removed promptly; any exudates swabbed and blood cultures taken if the patient issystemicallyunwell.ForpatientswithPVCexitsiteinfection,bloodculturesshouldbetaken,theexitsite exudate swabbed and sent for culture (if present) and the PVC removed. If the patient is febrile or unstableandPVC-relatedinfectionissuspected,empirictherapywithaglycopeptideantibiotic(e.g.,vancomycin)shouldbecommenced.InhealthcarefacilitieswithalowrateofMRSA,flucloxacillinisanacceptablealternative.Ifthereisnoassociatedbacteraemia,antibioticsmaybegivenorallyandthepatientmanagedasforacellulitisorsofttissueinfection.Ifbloodculturesarepositive,thentreatmentasforCRBSIisindicated.(Section3.3.4)

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-46-
5. Diagnosis of Catheter associated or related Infection
5.1 Clinical Diagnosis Infectionslinkedtotheuseofintravascularcathetersinclude;exit-siteinfections,andbothcatheter-associated and catheter-related infections. Intravascular catheter-associated infections include; primary BSI andclinicalsepsis,whichareepidemiologicallyassociatedwiththeuseofcatheters.10Clinicalfindingsaloneareunreliableforestablishingadiagnosisofintravascularcatheter–relatedinfection,becauseoftheirpoorspecificityandsensitivity.Themostsensitiveclinicalfindings,suchasfeverwithorwithoutchills,havepoorspecificityandinflammationorpurulencearoundtheintravascularcatheterandBSIhavegreaterspecificitybutpoorsensitivity.15 Blood culture results that are positive for S. aureus, coagulase negativestaphylococci,orCandida spp.,intheabsenceofanyotheridentifiablesourceofinfection,shouldincreasethesuspicionforCRBSI.Intheabsenceofdeviceculture,defervescenceafterremovalofanimplicatedCVC/PVCfromapatientwithprimaryBSIisconsideredindirectevidenceofCRBSI.Ingeneral,the diagnosis of infection associated with or related to intravascular catheters relies on clinical suspicion in conjunctionwithrelevantlaboratoryfindings.
5.2 Laboratory DiagnosisMany microbiological methods have been described to diagnose intravascular catheter-related infections. Thereis,however,noconsensusonatruegoldstandardandtheaccuracyofnumerousmicrobiologicalmethodshasgenerateddebateamongexperts.Inaddition,thevariabilityinthedefinitionsusedoverthepastdecadeshasnotsimplifiedtheunderstandingoftheliterature.87Inthiscontext,thedistinctionbetweendevice-associatedanddevice-relatedinfectionsproposedintheCDCguidelinesprovidesauseful tool.10
LaboratorymethodsforthediagnosisofinfectionmaybedividedintotwocategoriesandareoutlinedinTable 5.1: these categories are methods requiring device removal and those not requiring device removal. 15;88-103
1. Methods requiring catheter removal:Quantitativecathetertipculture.•Semiquantitative catheter tip culture.•Qualitativecathetersegmentculture.•
2. Methods not requiring catheter removal:
Paired quantitative blood cultures.•Unpaired quantitative blood culture.•Differentialtimetopositivity.•Acridine-orange leukocyte cytospin on blood drawn through the device.•Unpaired qualitative blood culture.•Paired qualitative blood cultures.•Endoluminal brush.•Culture of swabs of skin insertion site and of the hub.•

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-47-
Table 5.1 Microbiological techniques for diagnosis of CRBSI78
Technique Description Criteria for positivity
Sensitivity
(%)
Specificity
(%)
Methods requiring device removal
Quantitativecathetertipculture
A distal tip segment of the removed deviceisflushedwithbrothorsonicated or vortexed in broth that is further incubated.
≥100CFU 78-88 87-91
Semi-quantitative catheter tip culture
A3–4cmdistaltipsegmentoftheremoved device is rolled across an agar plate and incubated overnight.Unable to culture intraluminal organisms.
>15CFU 81-89 85-87
QualitativeCathetersegment culture
Incubation of a segment of the removed device in broth media.
Any growth 79-96 72-78
Methods not requiring device removal
Paired quantitative blood cultures
Paired blood cultures obtained through the device and from a separate venipuncture.Labourintensive.
Positive cultures from both sites and concentration of micro-organisms from the device 5 to10-fold higher than from the peripheral venipuncture
74-84 98-100
Unpaired quantitative blood culture
Blood cultures obtained through the device.
≥100CFU 80-93 83-89
Differentialtimetopositivity
Concomitant conventional qualitative blood cultures obtained from the device and from a separate venipuncture continuously monitored until growth of microorganisms.Currently available with most automated blood culture systems. Hard to interpret when patient is taking antibiotics through the CVC.
Blood culture drawn through the device turns positive ≥120 min before those obtained from venipuncture
86–92 79–87
Acridine-orange leukocyte Cytospin on blood drawn through the device
Staining with acridine orange of a slide from 50µl blood and examined under ultraviolet light.Accuracy may be improved if performed on specimen obtained by endoluminal brushing.
Any microorganism within thecellular monolayer in a minimum of 100 high-powerfield
80–96 89–97
Unpaired qualitative blood culture
Blood cultures obtained through the device.
Any growth 84-98 83-89
Paired qualitative blood cultures
Paired blood cultures obtained through the device and from a separate venipuncture.
Any growth 51-65 78-95
Endoluminal brushing Culture of sonicated and vortexed brush passed down the internal lumen to the device distal tip. May inducebacteraemia,arrhythmias,embolisation.
≥100CFU 92-100 84-98
Culture of swabs of skin insertion site and of the hub
Semi quantitative cultures on agar plate.
Any growth 96-100 67-71

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-48-
5.2.1.i Specimen Collection104
Twosetsofbloodculturesshouldbetakenusingaseptictechnique(inthecaseofCVCs,eitherthroughthe CVC and peripherally or through different lumens of the CVC if blood cultures cannot be drawn from a peripheralvein),fromallpatientswithsuspectedCRBSI.Bloodculturesshouldbetakenpriortoinitiationofantimicrobialtherapy.Thebottlesshouldbeappropriatelymarkedtoreflectthesitetheculturesweredrawnfrom.Asufficientvolumeofbloodcollectedpersetandinoculatedintobothaerobicandanaerobicmediashouldallowtheidentificationof99%ofdetectablebacteraemia.Ifpusispresentattheintravascularcatheterexitsite,thesitemustbeswabbedpriortocleaning,theswabsentforcultureandremoval of the catheter considered as outlined previously in this document.
Routineculturingofintravascularcathetertipsisnotrecommended.However,CVCtipsshouldalwaysbe sent for culture if the CVC is removed and catheter-related infection is suspected. In these cases it isessentialthattheCVCisremovedaseptically.Whenacathetersegmentissubmittedforculture,itisadequate to culture only the catheter tip and not the subcutaneous portion of the catheter.105 On removal oftheCVC,thetip(asegmentof4cm)shouldbesentforculture.Forsuspectedpulmonaryarterycatheterinfection,cultureoftheintroducertipisrecommendedasitprovidesahigheryield,incomparisonwiththepulmonary artery catheter tip.15Forimplantableports,cultureofthematerialinsidetheportreservoirismore sensitive than culture of the catheter tip for diagnosis of CRBSI.106
5.2.2.ii Culture Techniques –Catheter Tips and Catheter Exudate Swabs78;104
Asdiscussedabove,cultureofcathetersshouldbedoneonlywhenCRBSIissuspected.Theculturemethods used after removal of a catheter can be of a quantitative or semi quantitative nature. (Table 5.1) Ifavailable,acridineorangeleukocytecytospinmaybeconsideredforrapiddiagnosisofCVCinfection.The semi-quantitative (roll plate) method where only the outside of the tip is cultured is used in many laboratories.Arecentlyinsertedcatheter(i.e.,indwelling<14days)ismostcommonlycolonisedfroma skin microorganism along the external surface of the catheter; therefore the roll-plate method has highsensitivity.Thecriterionofpositivityforthismethodis>15CFUfromasegmentofthecathetertip. Intraluminal spread of microbes from the catheter hub into the bloodstream is important for long-termcatheters(i.e.,indwelling>14days).107 There is some concern that the roll-plate method is less sensitivethanothermethodsthatalsosampletheinternalsurfaceofcatheter,67;107 though this has not beenconfirmedinotherstudies.108 The most accurate method of quantitative catheter tip culture is a distaltipsegmentoftheremoveddeviceflushedwithbrothorsonicatedorvortexedinbroththatisfurther incubated. (Tables 5.1 and 5.2) A criterion of positivity with this method is >102CFU/segment.This method gives information on both the inner and outer surface of the tip but is time-consuming. Table 5.2summarisescultureofintravascularcathetersandcatheterexudateswabsandpotentiallysignificant(target) organisms that may be cultured.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-49-
Table 5.2 Laboratory culture media / incubation / target organism
Specimen Media Incubation Read cultures
Target Organism
Intravascular catheter tip
Blood agar
35-37oC in 5-10% CO2 24-48hours
Daily Any Organism
Swabs Blood agar
35-37oC in 5-10% CO2 24-48hours
Daily Coagulase-negative staphylococciCorynebacterium spp.Enterobacteriaciae spp.Enterococci spp.Pseudomonas spp.Streptococci spp.S. aureusYeasts
The use of antimicrobial coatings on intravascular catheters may lead to false-negative culture results.109;110 It is thought that the antimicrobial effects of antiseptic-impregnated catheters wane within several days of placement109 It has been suggested that the addition of inhibitors of silver sulfadiazine-chlorhexidine to media may be prudent especially when culturing antimicrobial coated catheters removed after short indwelling times.110
AllisolatesfromCVCtipsarepotentiallysignificantandshouldbeidentifiedtogenuslevelandtospecieslevelifclinicallyindicated.Antimicrobialsusceptibilityshouldbeperformedonallclinicallysignificantisolates. Coagulase-negative staphylococci are the most frequent causes of catheter-related infections. However,theseorganismsarecommonlyisolatedascontaminantsfrombloodcultures,whichmakesinterpretationoftheirclinicalsignificancedifficult.
5.2.2.iii Comparison of Microbiological Methods A number of prospective cohort studies have evaluated laboratory methods for CRBSI diagnosis that enable the CVC to remain in situ: Whengramstainandacridine-orangeleukocytecytospin,tip-roll,tip-flush,andendoluminalbrush•methodswerecompared,gramstainandacridine-orangeleukocytecytospinhadasensitivityof96%andspecificityof92%.Bycomparison,thetip-roll,tip-flush,andendoluminal-brushmethodshadsensitivitiesof90,95,and92%,respectively,withspecificitiesof55,76,and98%,respectively.Theauthors concluded that the gram stain and acridine-orange leukocyte cytospin test are simple and rapid methodsforthediagnosisofCRBSI,whichcomparefavourablywithothermethods.99
Inanotherstudy,thesensitivitiesoftheendoluminalbrush,ofquantitativeculturebloodcultures,and•ofthedifferentialtimetopositivitywerereportedas100,89,and72%,respectively,withcorrespondingspecificitiesof89,97,and95%,respectively.Bloodcouldbedirectlyaspiratedfromonly74%ofalllumens;however,theauthorsconcludedthatthedifferentialtimetopositivitywasthesimplesttechniquetoperform.Asaresultofthehighspecificityofthemethod,theyrecommendeditsuseasafirst-lineapproach,withtheendoluminalbrushtechniquereservedforcasesinwhichbloodcannotbeobtained from the CVC.111
Athirdstudyreportedthatthesensitivityandspecificityofswabculturesfromtheinsertionsiteand•fromthehubwere78.6and92.0%,respectively;fordifferentialquantitativebloodcultures,71.4and97.7%,respectively;andforthedifferentialtimetopositivity,96.4and90.3%,respectively.Theauthorsarguedthatconvenienceindifferentmedicalcontexts,theuseofresources,andexpertiseshoulddeterminethechoiceofatechnique.Asaresultoftheeaseofperformance,lowcost,andwideavailability,theyrecommendedcombiningsemiquantitativesuperficialculturesandperipheralveinbloodculturesforthescreeningofcatheterssuspectedofcausinginfection,andtousedifferentialquantitativebloodculturesasaconfirmatorymethod.112
Thesestudiessuggestthatthechoiceofaprecisemicrobiologicalmethod,oroftheeventualcombinationsofsomeofthem,shouldbemadeaccordingtotechnicalavailabilityandafterdiscussionbetweencliniciansandmedicalmicrobiologists.Inaddition,economicconsiderations,suchascost-effectiveness,mayalsobetakenintoaccount.PCRtotargetbacterial16sribosomalDNAissensitiveandspecificfordiagnosingcatheter-related infection.113 The use of this technique has the potential to reduce the unnecessary removal of CVCs but is not routinely used at present in medical microbiology laboratories.
Expertshaveproposedalgorithmstakingintoaccountmostofthesedifficultiestohelpcliniciansinthe

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-50-
diagnosis of catheter-related infections. Some authors have suggested obtaining two sets of paired blood cultures drawn through the catheter and peripherally.114Asufficientvolumeofbloodcollectedpersetandinoculatedintobothaerobicandanaerobicmediashouldallowtheidentificationof99%ofdetectablebacteraemia.Incasesinwhichclinicaljudgementmandatestheremovalofthecatheter,catheterculturesshouldprovideinformationlikelytoconfirmthediagnosis.Iftheintravascularcatheterisnotremoved,thedifferentialtimetopositivityisthenrecommendedasthefirstlinemethod,followedbyquantitativebloodcultures.Alternatively,ifonlyqualitativebloodculturesareavailable,theauthorsstronglyrecommendperformingadditionaltests,suchascultureofthedevice,toimprovethesensitivityofthemethod.Inanycasesofpositivemicrobiologicalcultures,theauthorsrecommendapplyingmorestrictcriteriainthepresenceofcoagulase-negativestaphylococcilikelytoreflectonlycontamination.114
ThecommitteethereforerecommendthatfordiagnosisofCRBSI,thefollowingcriteriashouldbemet:Bacteraemia or fungaemia in a patient who has an intravascular device and > 1 positive blood culture obtainedfromtheperipheralvein,clinicalmanifestationsofinfection(e.g.,fever,chillsand/orhypotension)and no apparent source for BSI (with the exception of the catheter).
One of the following should be present:
Apositiveresultofsemiquantitative(>15CFU/cathetersegment)orquantitative(>10• 2CFU/cathetersegment)catheterculture,wherebythesameorganism(species)isisolatedfromacathetersegmentanda peripheral blood culture.
Simultaneousquantitativeculturesofbloodwitharatioof>3:1CFU/mlofblood(cathetervs.peripheral•blood).
Differentialtimetopositivity:Growthinabloodculturedrawnthroughcatheterhubisdetectedbyan•automatedbloodculturesystematleast2hoursearlierthanasimultaneouslydrawn,peripheralbloodculture of equal volume.
Notethisdefinitiondiffersfromthedefinitionofcentralline-associatedBSIusedforinfectioncontrolsurveillanceactivities.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-51-
6. Considerations for Specific Settings
6.1 The Emergency DepartmentCVCs,PVCsandperipheralarterialcathetersinsertedintheEmergencyDepartment(ED)havehigherratesof bacterial contamination and colonisation than those inserted in other hospital settings43;115-117 including the critical care setting.43;115 Some authors have recommended that CVC insertion is postponed until the patientistransferredfromtheEDtotheICUoroperatingtheatre.118 The committee does not necessarily supportthisapproach;howeveritsexistencedoesindicatetheproblemsassociatedwithEDinsertionofCVCs.Rather,aspreviouslyrecommended,CVCsinsertedintheEDincriticallyillpatientsshouldberemoved/replacedasearlyaspossible,oncethepatientisclinicallystable.117
Aspreviouslydiscussed,inselectinganappropriateCVCinsertionsite,therisksforinfectionshouldbeassessedagainsttherisksofmechanicalcomplications.(Section3.1.4)Recentprospectiveevidenceshowsthatsubclavian,jugularandfemoralsiteshavesimilarCRBSIratesincriticallyillpatientsthoughothershave shown that the subclavian route is associated with lower rates of catheter-related infection in the acute setting.43;119Therefore,itisrecommendedthatthesubclaviansiteshouldbetherouteofchoiceforCVCinsertionintheED,117unless the patient is likely to require long-term renal replacement when thesubclaviansiteshouldbeavoided.(Section6.2.1)Althoughtheevidencebaseisrelativelyweak,some authors suggest use of antiseptic/antibiotic coated CVCs in preference to uncoated catheters for CVCinsertioninEDpatients,duetothehigherratesofCVCbacterialcontaminationandcolonisationassociatedwithinsertionintheED.120However,recentguidelinesadviseconsideringtheiruseinspecificcircumstancesonlyandthecommitteesupportstheserecommendations.(Section3.1.4)
6.2 Haemodialysis The delivery of maintenance haemodialysis requires access to the circulation so that up to 500 mls/min of bloodcanbepurifiedthreetofourtimesaweek.Currentlytherearefourmajorformsofvascularaccess,Primaryarteriovenous(AV)fistula,polytetrafluoroethylene(PFTE)grafts,tunnelledcuffedvenousCVCsandtemporarynon-cuffedCVCs.Thechoiceofaccessdependsonmanyfactors,however,aprimaryAVfistulaif it can be created is always the most preferable access. It provides the most durable long term access with the least complications or interventions required to maintain patency. (Table 6.1)
Table 6.1 Types of vascular access and infection rates.
Type of access CRBSI rate
Temporary non-cuffed CVC 5 episodes/1000 intravascular catheter daysTunnelled cuffed CVC 3.5 episodes/1000 intravascular catheter daysPTFEgraft 0.2 episodes /patient yearPrimaryAVfistula 0.05 episodes /patient year
Approximately 30% of patients who present with chronic renal failure will not have been seen by a nephrologistpreviouslyandthereforewillnothavehadtheopportunitytohavehaddefinitivevascularaccess created prior to the initiation of haemodialysis. In these circumstances there will be no alternative buttoemployeitheracuffedtunnelledintravascularcatheteroratemporaryline.NKF-K/DOQIandother guidelines recommend that patients with progressive renal decline should have a primary AV fistulafashionedwhentheGFRislessthan15mls/minwherepossible.Suchstrategiesofpre-emptivemanagement of vascular access results in dramatic long term survival advantages for patients and dramatic reductions in bacteraemia rates.121 The Committee recommend that haemodialysis patients should have aprimaryAVfistulacreatedforvascularaccesswheneverpossibleandpractical.IfitisnotpossibletoachieveafunctioningAVfistula,aPTFEgraftisingeneralpreferabletolongtermcuffedcatheters.Renalunits will therefore need adequate access to vascular surgeons in order to ensure the timely creation of primary vascular access.
6.2.1 Choice of Access Site for Acute HaemodialysisOptionsforplacementoftemporaryhaemodialysislineswillincludethejugular,subclavianorfemoralsites.Forpatientsthatarelikelytorequirelongtermrenalreplacementthesubclaviansiteshouldbeavoidedbecause of the frequent development of subclavian stenosis which interferes with long term provision of vascular access. The opportunity for life threatening complications to develop including carotid puncture or pneumothorax is much higher for jugular line insertion when compared to femoral access. It is generally reportedthatfemoralaccessisassociatedwiththehighestratesofbacteraemia,althoughthishasrecentlybeen questioned.40Forshorttermtemporaryvascularaccess,thefemoralsitemaybeconsidered.Ifaccessisgoingtoberequiredformorethan5-7days,insertionofacuffedjugularCVCunderradiologicalguidance is recommended.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-52-
Fordialysispatients,earlyconsiderationofthelongtermvascularaccessplanisessentialpriortoCVCinsertion(includingfutureAVfistulasites).Topreserveveinsforvascularaccess,itisrecommendedtoavoidvenepunctureandinsertionofPVCsintheforearmandelbow,especiallythecephalicveinsofthenon-dominant arm.
6.2.2 Prevention of InfectionBoth haemodialysis and the presence of a CVC were important risk factors for S. aureus bacteraemia in theenhancedEARSSsurveillancescheme.From2004totheendof2008,11%(159/1428)ofpatientswithMSSAbacteraemiaand13%(143/1103)ofpatientswithMRSAbacteraemiahadhaemodialysis.Therefore,prevention of S. aureus bacteraemia and CVC infection in haemodialysis patients represents important modifiableriskfactors.MeasurestopreventinfectionsassociatedwithCVCshavebeenoutlinedinSection3.1.Specificpreventionindialysispatients requiresmeticulousexit-sitecare,bothforvascularaccess and peritonealcatheters.(Section3.1.6)DialysisunitsshoulddevelopwrittenprotocolsdescribingaseptictechniqueforCVCinsertionandmaintenance(e.g.,Appendices8-11)andalldialysisstaffshouldbeadequately trained in these techniques in addition to training in hand hygiene and aseptic technique as outlined in Sections 2.1 and 2.2. CVC care bundles are outlined in Section 3.1.8. Each unit should keep recordsofprimaryfistulaprevalence,PTFEgraftprevalenceandcuffedcatheterprevalence.Unitsshouldreview bacteraemia rates for patients with and without catheters on a regular basis. When an episode ofbacteraemiadevelopsinadialysispatient,arootcauseanalysisshouldbeundertakentoidentifythesourceofinfectionandtoidentifypotentiallymodifiableriskfactorsforfuturepreventativestrategies.
6.2.2.i SurveillanceCRBSIsurveillanceisoutlinedinSection3.2,howeverashaemodialysispatientsareoutpatientbased,itisfrequentlydifficulttoobtainaccuratedenominatordatainthissetting.TheCDCNHSNsystemconductsinfection surveillance for outpatient haemodialysis facilities (available at http://www.cdc.gov/nhsn/psc_da_de.html).Numeratordataiscollectedoneachpatientwithahospitalisation,patientscommencedonoutpatientIVantimicrobialtherapy,orpatientswithapositivebloodculture.Denominatordataisderivedfrom the number of chronic haemodialysis patients with each access type who received haemodialysis at thecentreduringthefirsttwoworkingdaysofthemonth.Thesedataareusedtoestimatethenumberof patient-months. Only chronic haemodialysis outpatients are included in the denominator. This system allows healthcare facilities to categorise haemodialysis patients by vascular access type and assess severaloutcomesincludingaccess-relatedinfections,antimicrobialstartsandhospitalisations.Usingthisinformation,healthcarefacilitiescancalculaterisk-stratifiedratesandcompareagainstnationalrisk-stratifiedratesandcanalsoassessprocessmeasuressuchascatheterandfistulaprevalence.
6.2.2.ii Antimicrobial Ointments and LocksRifampicin therapy to decrease nasal carriage of S. aureus has been reported to be associated with fewer CVC-relatedinfections,122suggesting that a large number of S. aureus infections in dialysis patients are related in part to a high rate of nasal S. aureuscarriage.However,theemergenceofresistancewithchronic antibiotic use has limited the widespread adoption of this technique and it is not recommended. Anotherapproachistheuseoftopicalantiseptics(e.g.,povidone-iodine,chlorhexidine)orantibiotics(e.g.,mupirocin) at CVC entry sites. A recent meta analysis reported that topical antibiotics compared with no antibiotictherapy,loweredthebacteraemiarate,exit-siteinfectionrate,requirementforCVCremovalandhospitalisation for infection.123However,theemergenceofresistancetotopicalantimicrobialagentsisadefiniteriskofsuchtherapies,specificallytheemergenceofmupirocinresistance,whichhasbeenreportedin Ireland.124 Although isolation of antibiotic-resistant isolates was not observed in the studies that included surveillanceofsameintherecentmetaanalysis,longerfollow-upperiodsmayberequiredtoallowforresistance to be detected in study settings. One study in patients on chronic peritoneal dialysis reported a rate of 15% mupirocin resistance in S. aureus isolates at the end of four years.125 Mupirocin is widely used fornasaldecolonisationandemergenceofresistancewouldsignificantlycompromiseMRSAdecolonisationprogrammes. Recent guidelines recommend the application of povidone-iodine or polysporin ointment to haemodialysis catheter insertion sites in patients with a history of recurrent S. aureus CRBSI. Mupirocin ointment is not recommended due to the risks of mupirocin resistance and damage to polyurethane catheters.13(Section3.1.5.i)Furtherstudiesarerequiredtoevaluatethepotentialfordevelopmentofantibiotic resistance with long term use of topical agents.
Recently,muchinteresthasfocusedontheefficacyofALTusingvancomycin,gentamicinandcitratein preventing bacteraemia in haemodialysis patients. The incidence of tunnelled CVC infection was significantly lowerinthe33patientsassignedtoALTthan in the 30 control patients. These approaches have recentlybeenthesubjectofametaanalysiswhichdemonstratedstrongbenefitfromusingCVClocksolutions.123However,itisalsopossiblethat preventativeantibiotictreatmentmayfavourresistance.ALTforprevention(Section3.1.5.iiandiii)andtreatmentof(Section3.3.4.iii)ofCVCinfectionisdiscussedelsewhere in this document.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-53-
6.2.2.iii MRSA ScreeningThe current guidelines on the control and prevention of MRSA in hospitals emphasise the importance of the early detection of patients colonised with MRSA so that they can be isolated/cohorted appropriately and decolonisation commenced as soon as possible.2 Universal screening of all hospital patients is not currentlyrecommended,buthospitalsareadvisedtoscreenthosepatientsathighrisk,e.g.,patientspreviouslyknowntobeMRSApositive,transfersfromotherhospitalsorpatientsadmittedtocriticalcareunitssuchasICU.Thereisnospecificmentionofscreeninghaemodialysispatients,noristheeffectofMRSA screening in renal patients evaluated extensively in the literature. Results from the interim report of an NHS Scotland project evaluating the feasibility of universal MRSA screening suggested that while therewasnoevidencetodatetosupportuniversalscreening,MRSAscreeningmaybeappropriateinhigh prevalence specialities which included nephrology.126 The European Renal Association recommend screeningfornasalcolonisation(anddecolonisationofthosecolonised)allhigh-riskpatients,suchasthosewith a past history of S. aureus infection and those dialysed through a CVC.127 One study evaluating the effectsofacontactisolationprogramforMRSAcolonisation/infectioninahaemodialysisunit,showedabenefitintermsofreductionofMRSAinfection.128Aspreviouslydiscussedinthisdocument,patientswithCVCsrepresentasignificantproportionofpatientswithS. aureus BSI (both MSSA and MRSA) and renal patientsrepresentasignificantproportionofpatientswithCVCs.Itcouldthereforebearguedthatrenalpatients represent high-risk patients for both MRSA cross-infection and bacteraemia and that in order to reduce the prevalence of MRSA BSI and to identify patients with MRSA earlier and break the chain of transmission,renalpatientsshouldbescreenedforMRSAcolonisationregularly(e.g.,three-monthly)anddecolonised as per national guidelines.2UnitsmayalsowishtoconsiderscreeningalsoforMSSA,however,this will have implications for the laboratory and would need resourcing.
6.2.3 Management of CVC InfectionWhenCVCinfectionissuspectedinhaemodialysispatients,peripheralbloodculturesshouldbeobtainedfromvesselsnotintendedforfutureuseincreatingadialysisfistula.However,thisisfrequentlynotfeasibleastheperipheralveinsmayhavebeenexhaustedasaresultofmultiplefaileddialysisfistulasorgrafts.Whenaperipheralbloodculturecannotbeobtained,bloodculturesshouldbedrawnduringhaemodialysisfrom bloodlines connected to the CVC.
AsignificantproportionofdialysispatientswithCRBSIaretreatedsuccessfullyintheoutpatientsetting,with hospitalisation if severe sepsis or metastatic infection. CRBSI in dialysis patients are most often due to coagulase-negative staphylococci or S. aureus.75 Empiric antibiotic therapy of CRBSI is outlined in Section 3.3.4.i.Recentlypublishedguidelinesrecommendthatempiricantibiotictherapycanbediscontinuedinpatients with suspected CRBSI if both sets of blood cultures are negative and no other source of infection isidentified.Ifabloodculturecannotbeobtained,thereisnodrainagetoculturefromtheinsertionsiteandnoclinicalevidenceforanalternatesourceofinfection,thenapositivecatheter-drawnbloodculturein a symptomatic haemodialysis patient should lead to continuation of antimicrobial therapy for possible CRBSI.4
CRBSI involving long-term catheters in haemodialysis patients is of concern as the infected CVC is the vascular access for ongoing dialysis. The prognosis of S. aureus and other gram positive bacteraemia
in dialysis patients is severe with mortality ranging from 8 to 30%. Infective endocarditis is a serious complication. In a study on dialysis patients with infective endocarditis,theoverallmortalitywas49%;morepatients who had valvular heart surgery survived than patients who did not. Metastaticinfection,discitis,osteomyelitis and myocardial abscess are less frequent but serious complications. The risk of recurrent bacteraemiaisfrequent,particularlywhenCVCs with abnormal exit sites are not removed. Administration of intravenous antibiotics alone is unsatisfactory as BSI recurs in the majority of patients once the course of antibiotics has been completed.4ForexampleinonestudytheuseoftunneledCVCsalvageandS. aureus were found to be risk factors for treatment failure of CRBSI.129 In patients whose symptoms resolveafter2-3daysofintravenousantibioticsandwhodonothaveevidenceofmetastaticinfection,guidewire exchange of the catheter is associated with comparable cure rates as immediate removal with delayed placement of a new catheter.4 Recent guidelines advise that the infected CVC should always be removed in patients with haemodialysis CRBSI due to S. aureus,Pseudomonas spp.,orCandidaspp. and a temporary (non-tunnelled catheter) inserted into another anatomical site. A long-term haemodialysis catheter can be placed once repeat blood cultures are negative. Guidewire exchange is recommended onlyifnoalternativesitesareavailableforCVCinsertion.ForCRBSIduetootherpathogens(e.g.,gramnegative bacilli other than Pseudomonas spp.,orcoagulase-negativestaphylococci),apatientcanbestarted on empiric intravenous antibiotics without immediate catheter removal. If symptoms persist or thereevidenceofametastaticinfection,thecathetershouldberemoved.Ifsymptomsresolvewithin2-3daysandthereisnometastaticinfection,thentheinfectedcathetercanbeexchangedoveraguidewireforanew,long-termhaemodialysiscatheteroralternativelythecathetercanberetainedandanantibioticlock

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-54-
usedasadjunctivetherapyaftereachdialysissessionfor10-14days.Surveillancebloodculturesshouldbeobtained one week after completing an antibiotic course for CRBSI if the catheter has been retained. If the bloodculturesarepositive,thecathetershouldberemovedandanew,long-termdialysiscathetershouldbe placed after a repeat blood cultures are negative
6.3 Critical CareSafe CVC use is essential for effective multi-organ support in critically ill patients and is associated withsurvival.CRBSIandotherHCAIs(e.g.,ventilator-associatedpneumonia,surgical-siteinfections)arenotinfrequentincriticallyillpatientsandareassociatedwithsignificantmorbidityandmortality.130 Thecausativeorganismmaybemulti-drugresistant(MDR)andMDR-HCAIsareassociatedwithfurtherincreased mortality in critically ill patients.131
Recentprospectiveevidenceshowsthatsubclavian,jugularandfemoralsiteshavesimilarCRBSIratesin critically ill patients.40-43Aspreviouslydiscussed,whenselectinganappropriateinsertionsite,therisksforinfectionshouldbeassessedagainsttherisksofmechanicalcomplications.(Section3.1.4)Ithasbeensuggestedthatinpatientswithseverehypoxiaorhaemostasisdisorders,thefemoralapproachisassociatedwithanacceptablerateofcomplications,especiallywhenthecatheterisinsertedunderstrictaseptic conditions.132
CRBSI prevention guidelines have been published.10;133TheseguidelineshavebeensimplifiedforeaseofimplementationintoaCVCbundle(www.ihi.org/IHI)offiveinterventions(handhygiene,usingfull-barrierprecautionsduringtheinsertionofCVCs,skinasepsis,avoidingthefemoralsiteifpossibleandremovingunnecessary CVCs). (Section 3.1.8) In a single centre trial the CVC bundle was associated with decreased CRBSI.134However,thiswasnotobservedinamulti-centreICUtrial.64
There is evidence that training and education increase compliance with the CRBSI prevention bundle.65 Inadditiontoaneducationprogramme,a‘tick-box’CVCinsertionproceduremaybeusedtopromoteCVCbundlecompliance,anexampleofsuchisprovidedinAppendix10.Increasedcompliancewithinfection control practices involves behavioural change in HCW. Behavioural sciences provide models of (HCW)behaviouralchangeforinfectionpreventionandcontrolpracticese.g.,handwashing.‘Successfulstrategiestoimproveinfectioncontrolpracticesresultfromtheirmultidimensionalaspect’and‘multimodalintervention strategies have more chance of success than single approaches or promotion programmes focusingononeortwoelementsalone’.135Thereisnoevidence,however,thatadirectsupervisionprogramme prevents CRBSI per se. Scheduled CVC replacement is not associated with a decreased incidenceofCRBSI.(Section3.1.7)Intheseverelycriticallyillpatient,guidewireexchangemaybesaferthannewCVCinsertionintermsofmechanicalcomplications.Forexample,amechanicalcomplicatione.g.,pneumothoraxisassociatedwithsignificantincreasedmortalityinacriticallyillpatient.130 When a criticallyillpatientispyrexicandCRBSIispartofthedifferentialdiagnosis,bloodculturesshouldbetaken,(peripherallyandthroughtheCVC),inadditiontootherappropriateculturesandeitherCVCreplacementorameticulousguidewireexchangewithcultureoftheoldCVCtipperformed.Thepatient’scriticalillnessmaybeofsuchseveritythatanunnecessarylineinsertioncomplicationmaybelethal.However,aspreviouslydiscussedinSection3.1.7,guidewireexchangeshouldbeusedonlyifthereisnoCVCexitsiteinfectionorhighsuspicionofCRBSI.Ifafteraguidewireexchange,investigationsrevealCRBSI,thenewlyinsertedCVCshouldberemovedandifstillrequiredreinsertedatadifferentsite.Forguidewireexchanges,thesamemeticulousaseptictechniqueanduseoffullsterilebarriersaremandatoryduringtheinsertionofanynewCVC.Afterskinasepsis,insertingtheguide-wire,removingtheoldCVC,andfurtherskinasepsis,theoperatormustre-gloveandre-drapethesite,astheoriginalglovesanddrapesarelikelyto have become contaminated from manipulation of the old CVC. Empiric therapy of CRBSI is as outlined inSection3.3.4.iandmanagementofCRBSIwhentheorganismisknownisasoutlinedinSection3.3.4.ii.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-55-
Section 3: Appendices and Reference List
Appendix 1: Committee Membership and Acknowledgements
Dr.FidelmaFitzpatrick,Consultant• Microbiologist,HealthProtectionSurveillanceCentre(HPSC)&BeaumontHospital,Dublin(Chair)
Prof.PeterConlon,ConsultantNephrologist,BeaumontHospital,Dublin(representingINA)•
Ms.NualaDoyle,CNM2DialysisServices,StJames’sHospital,Dublin•
Ms.MargaretFitzpatrick,MedicalScientist,MaterHospital,Dublin•
Dr.CatherineFleming,ConsultantInfectiousDiseasesPhysician,UCHG,Galway(representingIDSI)•
Ms.AnnFlynn,AssistantDirectorofNursing–InfectionPreventionandControl,St.Vincent’sHospital,•Dublin(representingIPS)
Dr.SineadKelly,ConsultantMicrobiologist,AdelaideandMeathHospital,DublinIncorporatingthe•NCH,Dublin(representingISCM)
Dr.LeoLawler,ConsultantRadiologist,MaterHospital,Dublin(representingRCPIFacultyof•Radiologists)
Dr.MaureenLynch,ConsultantMicrobiologist,MaterandCappaghHospital,Dublin(representing•ISCM)
Dr.MargaretMorris-Downes,SurveillanceScientist,BeaumontHospital,Dublin(representingSSAI)•
Mr.EddieMcCullagh,SurveillanceScientist,AdelaideandMeathHospital,DublinIncorporatingthe•NationalChildren’sHospital,Dublin(representingSSAI)
Ms.MargaretMcCann,Lecturer,SchoolofNursingandMidwifery,TrinityCollegeDublin•
Dr.DeirdreO’Brien,SpecialistRegistrarinMicrobiology,BeaumontHospital,Dublin•
Dr.NiamhO’Sullivan,ConsultantMicrobiologist,OurLadysChildren’sHospitalandCoombeHospital,•Dublin(representingISCM)
Dr.DermotPhelan,ConsultantinIntensiveCareMedicine,MaterHospital,Dublin(representingICSI)•
Dr.MichealPower,ConsultantAnaesthetist,BeaumontHospital,Dublin(representingICSI)•
MrToneyThomas,AssistantDirectorofNursing–InfectionPreventionandControl,BeaumontHospital,•Dublin(representingIPS)
Subsequent to the consultation process the following representatives were invited to join the Committee
Mr.SeanEgan,AntimicrobialPharmacist,TheAdelaideandMeathHospital,IncorporatingtheNational•Children’sHospitalDublin(representingtheIrishAntimicrobialPharmacistsGroup)
Mr.AbelWakai,LocumConsultantinEmergencyMedicine,St.James’sHospital,Dublin(representing•the Irish Association for Emergency Medicine)
Ms.SheilaDonlon,InfectionPreventionandControlManager,HPSC•
The Committee wishes to acknowledge the assistance of Ms.RebeccaRush,SurveillanceScientist,OurLadysChildren’sHospitalDublinwithdraftingthesurveillanceformsinAppendices12-13,ofMr.AjayOza,SurveillanceScientist,HPSCforenhancedEARSSdataandoftheInfectionPreventionandControlteam,GalwayUniversityHospitalsforprovidinguswiththeirpatientinformationleaflet.(Appendix7)
ThechairwishestoacknowledgeDr.KarenBurns,Ms.OrlaBannonandMr.MauriceKellyforproofreadingthe document.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-56-
Appendix 2: Consultation Process
The draft document was placed on the HSE and HPSC websites for general consultation in February 2009. In addition, a draft of this document was sent to the following groups for consultation
AcademyofMedicalLaboratoryScience
CysticFibrosisRegistryofIreland
HSE HCAI Governance Group
HSENursePracticeDevelopmentUnits
HSEDirectorsofNursing
Haematology Association of Ireland
Irish Antimicrobial Pharmacists Group
Irish Association of Critical Care Nurses
Irish Association for Emergency Medicine
Irish Association for Nurses in Oncology
Irish Association for Paediatric Nursing
Intensive Care Society of Ireland
Irish College of General Practitioners
InfectiousDiseasesSocietyofIreland
Irish Nephrology Association
Irish Nephrology Nurses Association
Irish Society of Clinical Microbiologists
Irish Society of Medical Oncology
Irish Patients Association
Infection Prevention Society
PublicHealthMedicineCommunicableDiseaseGroup
Royal College of Physicians of Ireland (RCPI)
RCPIFacultyofPathology
RCPIFacultyofPaediatrics
Royal College of Surgeons in Ireland (RCSI)
RCSIFacultyofRadiologists
SARI National Committee
SARI Regional Committees
Surveillance Scientists Association of Ireland

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-57-
Appendix 3: Abbreviations used in this documentALT AntibioticlocktherapyAV ArteriovenousBSI Bloodstream infectionCDC CentresforDiseaseControl&Prevention,USCRBSI Catheter-related bloodstream infectionCFU ColonyformingunitCIDR ComputerisedInfectiousDiseaseReportingCVC Central intravascular catheterCVC-VASC Cardiovascularsysteminfection–arterialorvenousinfection(CDCsurveillancedefinition)DoHC DepartmentofHealthandChildrenEARSS European Antimicrobial Resistance Surveillance System ED EmergencyDepartmentFV FemoralveinHCA Healthcare-associatedHCAI Healthcare-associated infectionHCF HealthcarefacilityHCW(s) Healthcare worker(s)HDU HighdependencyunitHELICS HospitalsinEuropeLinkforInfectionControlthroughSurveillanceHIS HospitalInfectionSociety,UKHPS Health Protection ScotlandHPSC Health Protection Surveillance CentreHSE Health Services ExecutiveICSI Intensive Care Society of IrelandICT Infection prevention and control teamICGP Irish College of General Practitioners ICN Infection prevention and control nurseICU Intensive care unitIDSI InfectiousDiseasesSocietyofIrelandIDSA InfectiousDiseasesSocietyofAmericaINA Irish Nephrology AssociationIPS Infection Prevention SocietyISCM Irish Society of Clinical MicrobiologistsIJ InternalJugularIV IntravascularK/DOQI KidneydiseasesoutcomesqualityinitiativeKISS Krankenhaus-Infektions-SurveillanceSystemLCBI Laboratoryconfirmedbloodstreaminfection(CDCsurveillancedefinition)MIC Minimum Inhibitory ConcentrationMDR Multi-drugresistantMRSA Meticillin-resistance S. aureus MSSA Meticillin-sensitive S. aureus NICU Neonatal intensive care unitNINSS Nosocomial Infection National Surveillance Scheme NKF-K/DOQI NationalKidneyFoundation-KidneydiseasesoutcomesqualityinitiativeNNIS National Nosocomial Infections SurveillanceNHS NationalHealthService,UKNHSN National Healthcare Safety Network (US)PICC Peripherally inserted CVCPFTE PolytetrafluoroethylenePREZIES PREventievanZIEkenhuisinfectiesdoorSurveillancePVC Peripheral intravascular catheterRCSI Royal College of Surgeons in IrelandRCPI Royal College of Physicians in Ireland SARI Strategy for the Control of Antimicrobial resistance in IrelandSC SubclavianSIGN Scottish Intercollegiate Guidelines Network SSAI Surveillance Scientists Association of IrelandSVC Superior vena cavaTOE Transoesophageal echocardiogramTPN Total parenteral nutrition

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-58-
Appendix 4: Anatomic Points of Access for Intravascular Catheters
Neck- • Internal jugular
Chest- • Subclavian
Chest-• Transatrial
Arm- • Basilic/Cephalicorunnamedsuperficialvein
Groin-• Ilio-femoral vein
Pedal-• Dorsumoffootsuperficialveinarch
Translumbar-• intravascular catheter
Transhepatic – • Hepatic Vein
Unnamed collaterals•
Additional Paediatric Access. Scalp or umbilical vein•
Line Exchange.Removal of an existing line in such a manner that the original dermatotomy and vessel point of access is preservedandnewlineinserted,usuallyoveraguidewire.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-59-
Appendix 5: Types of Intravascular Catheters D
escr
ipti
on
Cat
hete
r ty
pe
Co
mm
on
use
Cha
ract
eris
tics
Co
mm
on
site
of
acce
ssC
om
mo
n si
te o
f ti
pA
ntic
ipat
ed
dur
atio
n/Te
rmP
VC
sA
ngio
cath
Med
icat
ion
Fluids
Sho
rtP
erip
hera
lSingleLumen
ArmForearm
Han
d
Per
iphe
ral
Arm
Sho
rt 7
-10d
Vasc
ular
Sh
eath
Art
ery
Mo
nito
rin
trav
ascu
lar
cath
eter
A
cces
sM
edic
atio
nFluid
Blo
od
dra
w
SingleLumen
LargeCalibre
Po
ssib
le S
ide
arm
CommonFemoral
Vein
Bas
ilic
Cep
halic
Femoralartery
Rad
ial A
rter
y
Iliac
Vei
nSh
ort
7-1
0d
No
n tu
nnel
led
CV
C
Mo
st c
om
mo
nly
used
CV
C.
Inse
rted
per
cuta
neo
usly
via
ei
ther
the
sub
clav
ian
or
jug
ular
ve
in in
to t
he S
VC
. U
nlik
e tunnelledCVCs,theCVCenters
the
skin
at
a si
te c
lose
to
the
en
try
po
int
into
the
vei
n w
ith
no
bac
teri
ost
atic
cuf
f.
Ho
hn
cath
eter
Med
icat
ion
Fluid
Blo
od
dra
w
1or2Lumen
Mo
der
ate
Cal
ibre
Pre-defined
leng
th
Sub
clav
ian
InternalJugular
Cen
tral
SVC
Short7-14d
Trip
le lu
men
Med
icat
ion
Fluid
Blo
od
dra
wTP
N
3or4Lumen
Mo
der
ate
Cal
ibre
DefinedLength
Sub
clav
ian
InternalJugular
Cen
tral
SVC
Sho
rt 7
-10d
Swan
Gan
zP
ulm
ona
ry A
rter
y P
ress
ure
mea
sure
men
t1Lumenand
bal
loo
nSu
bcl
avia
nInternalJugular
Cen
tral
Pul
mo
nary
ar
tery
Sho
rt 7
-10d
Vasc
ath
Acu
te P
here
sis
Acu
te S
tem
Cel
l har
vest
AcuteDialysis
2Lumen
LargeCalibre
Sub
clav
ian
InternalJugular
FemoralVein
Cen
tral
SVC
Iliac
Vei
n
Sho
rt 7
-10d
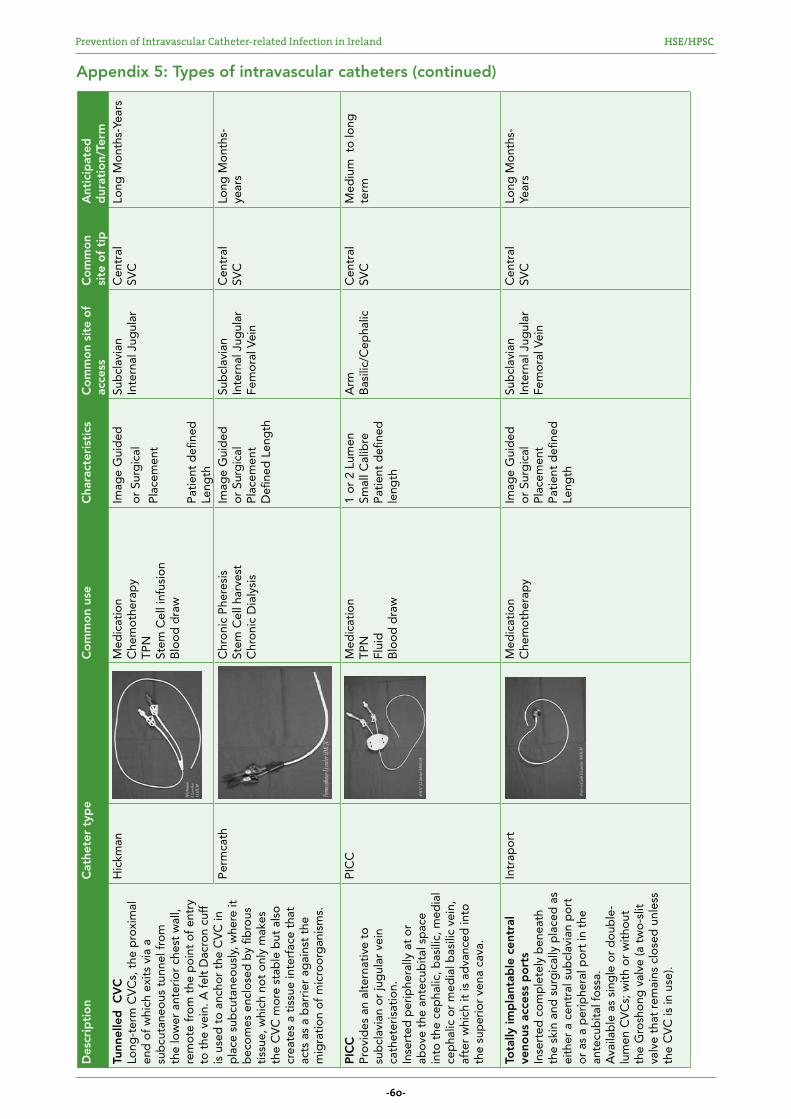
Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-60-
Des
crip
tio
nC
athe
ter
typ
eC
om
mo
n us
eC
hara
cter
isti
csC
om
mo
n si
te o
f ac
cess
Co
mm
on
site
of
tip
Ant
icip
ated
d
urat
ion/
Term
Tunn
elle
d
CV
CLong-termCVCs,theproximal
end
of
whi
ch e
xits
via
a
sub
cuta
neo
us t
unne
l fro
m
theloweranteriorchestwall,
rem
ote
fro
m t
he p
oin
t o
f en
try
tothevein.AfeltDacroncuff
is u
sed
to
anc
hor
the
CV
C in
placesubcutaneously,whereit
becomesenclosedbyfibrous
tissue,whichnotonlymakes
the
CV
C m
ore
sta
ble
but
als
o
crea
tes
a ti
ssue
inte
rfac
e th
at
acts
as
a b
arri
er a
gai
nst
the
mig
rati
on
of
mic
roo
rgan
ism
s.
Hic
kman
Med
icat
ion
Che
mo
ther
apy
TPN
Stem
Cel
l inf
usio
nB
loo
d d
raw
Imag
e G
uid
ed
or
Surg
ical
Pla
cem
ent
Patientdefined
Length
Sub
clav
ian
InternalJugular
Cen
tral
SVC
LongMonths-Years
Per
mca
thC
hro
nic
Phe
resi
sSt
em C
ell h
arve
stChronicDialysis
Imag
e G
uid
ed
or
Surg
ical
P
lace
men
tDefinedLength
Sub
clav
ian
InternalJugular
FemoralVein
Cen
tral
SVC
LongMonths-
year
s
PIC
C
Pro
vid
es a
n al
tern
ativ
e to
su
bcl
avia
n o
r ju
gul
ar v
ein
cath
eter
isat
ion.
In
sert
ed p
erip
hera
lly a
t o
r ab
ove
the
ant
ecub
ital
sp
ace
intothecephalic,basilic,medial
cephalicormedialbasilicvein,
afte
r w
hich
it is
ad
vanc
ed in
to
the
sup
erio
r ve
na c
ava.
PIC
CM
edic
atio
nTP
NFluid
Blo
od
dra
w
1or2Lumen
Smal
l Cal
ibre
Patientdefined
leng
th
Arm
Bas
ilic/
Cep
halic
Cen
tral
SVC
Med
ium
to
long
te
rm
Tota
lly im
pla
ntab
le c
entr
al
veno
us a
cces
s p
ort
sIn
sert
ed c
om
ple
tely
ben
eath
th
e sk
in a
nd s
urg
ical
ly p
lace
d a
s ei
ther
a c
entr
al s
ubcl
avia
n p
ort
o
r as
a p
erip
hera
l po
rt in
the
an
tecu
bit
al f
oss
a.
Ava
ilab
le a
s si
ngle
or
do
uble
-lu
men
CV
Cs;
wit
h o
r w
itho
ut
the
Gro
sho
ng v
alve
(a t
wo
-slit
va
lve
that
rem
ains
clo
sed
unl
ess
the
CV
C is
in u
se).
Intr
apo
rtM
edic
atio
nC
hem
oth
erap
yIm
age
Gui
ded
o
r Su
rgic
al
Pla
cem
ent
Patientdefined
Length
Sub
clav
ian
InternalJugular
FemoralVein
Cen
tral
SVC
LongMonths-
Year
s
Appendix 5: Types of intravascular catheters (continued)
Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-61-
Appendix 6: Aseptic (No touch) Technique
1. Hand hygiene Washwithanantimicrobialliquidsoapandwater, or Ifhandsarephysicallyclean,applyinganalcoholbasedhandrub. Hands that are visibly soiled or contaminated with dirt or organic material must be washed with liquid
soap and water before using an alcohol hand rub.
2. Prepare an aseptic surface Procedure trolleys/trays must be cleaned using a detergent and disinfectant.
3. Gather equipment for procedure
4. Hand hygiene and put on gloves a. Clean,non-sterilegloves:iftheprocedurecanbecompletedwithouttouchingkeyparts
(intravenousdrugadministration,bloodsamplingorconnectingordisconnectingintravenousfluidsexcept TPN).
b.Sterileglovesiftheprocedurecannotbecompletedwithouttouchingkeyparts(e.g.,linemanipulation,insertionsitedressingchanges,connectingTPNandconnectingordisconnectingcatheters used for haemodialysis).
5. Identify ‘key parts’ e.g.,cannulahub,port,infusionline,lumen
6. Prepare equipment and patient ensuring that all key parts are protected Protect key part at all time using a non-touch technique. Nonkeypartscanbetouchedwithconfidence.
7. Carry out procedure taking care to avoid contamination of sterile areas/items/key parts
8. Dispose of waste and sharps appropriately
9. Remove gloves
10. Hand hygiene
Des
crip
tio
nC
athe
ter
typ
eC
om
mo
n us
eC
hara
cter
isti
csC
om
mo
n si
te o
f ac
cess
Co
mm
on
site
of
tip
Ant
icip
ated
d
urat
ion/
Term
Tunn
elle
d
CV
CLong-termCVCs,theproximal
end
of
whi
ch e
xits
via
a
sub
cuta
neo
us t
unne
l fro
m
theloweranteriorchestwall,
rem
ote
fro
m t
he p
oin
t o
f en
try
tothevein.AfeltDacroncuff
is u
sed
to
anc
hor
the
CV
C in
placesubcutaneously,whereit
becomesenclosedbyfibrous
tissue,whichnotonlymakes
the
CV
C m
ore
sta
ble
but
als
o
crea
tes
a ti
ssue
inte
rfac
e th
at
acts
as
a b
arri
er a
gai
nst
the
mig
rati
on
of
mic
roo
rgan
ism
s.
Hic
kman
Med
icat
ion
Che
mo
ther
apy
TPN
Stem
Cel
l inf
usio
nB
loo
d d
raw
Imag
e G
uid
ed
or
Surg
ical
Pla
cem
ent
Patientdefined
Length
Sub
clav
ian
InternalJugular
Cen
tral
SVC
LongMonths-Years
Per
mca
thC
hro
nic
Phe
resi
sSt
em C
ell h
arve
stChronicDialysis
Imag
e G
uid
ed
or
Surg
ical
P
lace
men
tDefinedLength
Sub
clav
ian
InternalJugular
FemoralVein
Cen
tral
SVC
LongMonths-
year
s
PIC
C
Pro
vid
es a
n al
tern
ativ
e to
su
bcl
avia
n o
r ju
gul
ar v
ein
cath
eter
isat
ion.
In
sert
ed p
erip
hera
lly a
t o
r ab
ove
the
ant
ecub
ital
sp
ace
intothecephalic,basilic,medial
cephalicormedialbasilicvein,
afte
r w
hich
it is
ad
vanc
ed in
to
the
sup
erio
r ve
na c
ava.
PIC
CM
edic
atio
nTP
NFluid
Blo
od
dra
w
1or2Lumen
Smal
l Cal
ibre
Patientdefined
leng
th
Arm
Bas
ilic/
Cep
halic
Cen
tral
SVC
Med
ium
to
long
te
rm
Tota
lly im
pla
ntab
le c
entr
al
veno
us a
cces
s p
ort
sIn
sert
ed c
om
ple
tely
ben
eath
th
e sk
in a
nd s
urg
ical
ly p
lace
d a
s ei
ther
a c
entr
al s
ubcl
avia
n p
ort
o
r as
a p
erip
hera
l po
rt in
the
an
tecu
bit
al f
oss
a.
Ava
ilab
le a
s si
ngle
or
do
uble
-lu
men
CV
Cs;
wit
h o
r w
itho
ut
the
Gro
sho
ng v
alve
(a t
wo
-slit
va
lve
that
rem
ains
clo
sed
unl
ess
the
CV
C is
in u
se).
Intr
apo
rtM
edic
atio
nC
hem
oth
erap
yIm
age
Gui
ded
o
r Su
rgic
al
Pla
cem
ent
Patientdefined
Length
Sub
clav
ian
InternalJugular
FemoralVein
Cen
tral
SVC
LongMonths-
Year
s

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-62-
Appendix 7: Patient Information Leaflet
InformationforpatientsaboutIV(intravenous)lines
Why do I need an IV line?IVlines(sometimescalled“drips”)areoftenusedinhospitaltogivefluidsordrugsquicklyintothebloodstreamormaybeneededifyouareunabletoeatordrinknormallye.g.,ifyouarefasting for an operation.
Who puts in the IV line?An IV line is usually inserted into your arm by a doctor but sometimes a nurse or phlebotomist (staff member who takes blood specimens from you) may insert it.
How does the IV line stay in place?•Thelinewillbekeptinplacebyasterilewaterproofdressing.Ifthisgetswet,dirtyorslipsoff,
tell the nurse caring for you.•Donot remove the dressing.•Itisimportanttohandlethelinecarefullyandtrynottopullonit.•Thelinewillbecheckedeachdaybythenursingand/ormedicalstaffcaringforyoutomake
sure that the line is still working properly and not causing any problems.
How long will I have the IV line in?•ThiswilldependonwhyyouhavetheIVlineinthefirstplace.IfyounolongerneedIVfluidsordrugs,theIVlinewillberemoved.•Thelinewillusuallybechangedevery3daysandanewoneinsertedifyoustillneedanIVline.•Sometimeslinescangetinflamedorinfectedandneedtoberemovedsoonerthanthis.
Signs that may mean that the line needs to be removed:•Redness,swelling,painorhotnessatthelinesite.•Thedressingislooseorwet.•Thelinesiteissore.•Temperatures(hotorcold;shivery)
How can I help prevent infection in my IV line site?•DonottouchtheIVlinewherepossible•Ifyoumusttouchanypartoftheline,cleanyourhandsfirst.•RemindotherswhotouchyourIVlinetocleantheirhandsfirsttoo.•Keepclothingnearthelinesitecleananddry.•IfyounoticethatyourIVlinesiteis sore or red or causing you pain, please tell the nurse
and/or doctor looking after you so it can be removed.
For more information go towww.hse.ie or www.hpsc.ie

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-63-
Appendix 8: CVC Insertion Procedure Guideline
1. Before insertion•Check patient’s coagulation profile (PT, PTT, platelets) on day of procedure.
oDonotinsertCVCinpatientreceivingwarfarin,clopidogrelunlessinemergency.Ifnon-emergencyinsertion,correctcoagulopathye.g.,INR>1.4,platelets<50.
oBalanceindication(access,pressors,parenteralnutrition,antibiotics)againstcomplicationprofile(neurovascularinjury,haemorrhage,infection).
2. Site oUseinsertionsiteassociatedwithleastlikelihoodofinjury(jugular,femoral,subclavian).Consider
portableultrasoundimagingforselectedpatientsathighriskofcomplications(e.g.,knownvascularanomaly)orwherevascularaccessislikelytobedifficult(e.g.,children)
o Remove hair at the insertion site using clippers if required. Physically clean the skin if necessary.
3. Catheter typeUsesinglelumenordoublelumeninpreferencetotriple-or4-lumen.Ifsingle-lumenaccessrequired,consider PICC.
4. Preparation of sterile field•Only competent staff (or training staff supervised by competent staff) are to insert CVCs. (Section
2.3) •The CVC should be inserted in an area where asepsis can be maintained. •A trolley/cart that includes all supplies necessary for inserting a CVC including barrier precautions
should be dedicated for CVC insertion. (Appendix 9) •Thesterilefieldmustbesetupimmediatelypriortotheprocedure.
5. Hand hygiene (Section 2.1)•Handsmustbedecontaminatedbywashingwithanantimicrobialliquidsoapandwater,orifhandsarephysicallyclean,byanalcoholbasedhandrub.Handsthatarevisiblysoiledorcontaminatedwithdirtororganic material must be washed with liquid soap and water before using an alcohol hand rub.•The use of gloves does not obliviate the need for hand hygiene.•Hand hygiene must be performed
o Before and after inserting catheter CVC.
6. Maximal Barrier PrecautionsBeforeplacingaCVC(includingguidewireexchanges),theoperatorandanypersonwhoentersthesterilefieldtoassistintheprocedure,mustdonamask,sterilelong-sleevedgown,sterileglovesandprotectiveeyewear.Asurgicalcapshouldbeusedtocontainhairthatmayfallacrosstheoperator’sfaceduringthe procedure. The patient should be covered from head to toe with a sterile drape with an appropriate opening for the site of insertion.a. Donprotectivecap,eyewearandsurgicalmask-Themaskshouldcoverthenoseandmouthtightly.
b. Perform hand hygiene and dry hands with a sterile towel.
c. Aseptically don sterile gown.
d. Aseptically don sterile gloves - Ensure gloves cover cuff of gown.
e. Skin asepsis – Apply single patient use application of 2% chlorhexidine gluconate in 70% isopropyl alcohol (unless contraindicated – Section 3.1.2) in a circular motion beginning in the centre of the proposedsiteandmovingoutward,foratleast30seconds.Repeatthisstepusinganewswabforeachapplication.Allowtoairdrycompletelypriortoinsertingthecatheter,donotwipeorblot.
f.Drapetheentirebodyofthepatient(whilemaintainingasterilefield)leavingonlyasmallopeningattheinsertion site.
7. Insertion Technique•Ensureskinandsubcutaneoustissuesarenotinfectedlocally.•Considersomevolumeresuscitationtofillveinslocally.•Trendelenbergposition(orreverseTforfemoralveins)topromotevenousfilling.•Localinfiltrationoflocalanaestheticagentwherenecessary(lignocaineorbupivacaine)(ifnoallergy).•UseSeldingertechniquetoaccessinternaljugularveinatapexofthetriangleofthesternalandclavicular
heads of the sternocleidomastoid muscle.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-64-
8. Landmark technique•Palpatecarotidarteryinneck.•Insert21G‘blue’seekerneedletolocatevein.•Wherepossibleinsertcannulaintoveintoobserveforvenousflowcharacteristics.•Considerultrasoniclocatingdeviceasoutlinedabove.•Insertwireto20cm.•Inciseskinlocallytodepthof5mmtopermitpassageofintroducer.•Passintroducerwithrotatoryorswivellingactiontopreventfalsepassage.•Advancecatheteroverwirewhilemaintainingpincergriponwiretopreventwireembolus.•Confirmintravenousplacementofcatheterbyaspiratingvenousblood.•Flushcatheterlumenswithnormalsaline.
9. Catheter fixationSecure the catheter with 2/0 silk sutures to minimise to-and-fro pistoning of the catheter and subsequent catheter tract invasion by cutaneous microorganisms.Donotapplyantimicrobialointmentsorcreamstotheinsertionsite.Applyasterile,transparent,semipermeable,self-adhesive,polyurethanedressing.
10. Confirm CVC placement with Radiology (e.g., chest X-ray)
11. If accidental insertion of wide-bore CVC into subclavian artery or femoral artery above inguinal ligament,leavecatheterin situ. Consult Vascular Surgery/Interventional Radiology on-call for possible endovascular repair with closure device.
12. Documentation•Dateandtimeofinsertion.•Type of CVC and gauge.•Anatomical/insertion site.•LocationofCVCtip.•Name of operator.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-65-
Appendix 9: CVC Insertion Pack - Example of Contents
Patient safety is essential. This includes good technique to prevent complications and strict asepsis to prevent catheter-related blood stream infection (see CVC insertion procedure guideline – Appendix 8 and CVC Insertion Checklist, Appendix 10). Gloves may or may not be added to the packs below, if added a selection of packs with different glove sizes would be required. This will have cost implications so it may be preferable to add gloves at time of insertion.
Contents of CVC Insertion Pack:Pack containing (nonfenestrated) outside sterile drape with waterproof backing to cover the trolley stand completely.
Inside pack containing:• CVC+Introducer• XLdisposablesterileprotectivegownwithpoppers• Paper towel• Fenestratedadhesiveabsorbentdisposabledrapetocoverpatientfromheadtotoe. Note: If using a plastic drape, ensure that the drape conforms to the patient’s neck anatomy so that the
sterile field is maintained136
• 2%chlorhexidinegluconatein70%isopropylalcohol,plasticdisposableforceps/swabholder,four4”x4”swabs
• 2galleypots• 2/0silksuturestraightneedle,pointedscalpel• Steriletransparentsemipermeabledressing• Orange,blue,green,pinkneedle;2/5/10mlsyringes;lignocaine2%plasticampoule• 4needlefreeconnectors• 1yellowhealthcareriskwastebag60x50cm
Additional equipment for Angio-suite insertion packs-in particular for tunnelled catheters or intraports.
All tunnelled catheters• Micropuncture set- 018 wire• Peelaway sheath• Dilators• Mosquito/KellyForceps• Tunneller device
Intraport-specific• 2/0securingsutures• 3/0deepinterruptedsutures• 2/0absorbablesubcuticularsuture• Dermabond/steristrips• Port access needle

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-66-
Appendix 10: CVC Insertion Checklist
Procedure Date: Time:
Location of CVC insertion: ITU HDU Radiology ED Other: ____________
Operator: ___________________________________Grade of Operator: Consultant Specialist Registrar Registrar SHO
Operator’s specialty:EM Anaesthesia/ICU Medicine Surgery Other Please specify: ______________________
Assistant: __________________________ Supervisor: __________________________________
Procedure: Insertion Site: Position: Emergency Subclavian Right Elective Jugular Left Ultrasound guidance Femoral Other New line Guidewire exchange
Catheter Type: Lumens: Catheter Coating:Triple lumen 1 Antibiotic Vas Cath 2 Antiseptic Arterial 3 None Other 4
5 Local Anaesthetic used: Sedation used:
Number of skin punctures: 1 2 3 ≥4 Number of needle passes: 1 2 3 ≥4
Complications:Malposition Haemorrhage Pneumothorax Other____________Additional comments: __________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
This checklist is to be completed by an independent observer who should stop the procedure if a
significantbreachofaseptictechniqueisobserved.
Hand hygiene Yes No Maximal barrier precautions* Yes No Skin asepsis (Chlorhexidine 2% in alcohol (if compatible) & allowed to dry) Yes No Sterile technique maintained throughout procedure Yes No CVCsecuredanddressedwithsterile,semipermeabletransparentdressing Yes No Appropriatepositionofcatheterradiologicallyconfirmed Yes No Othermethodusedtocheckplacement(e.g.,cathetertransduced) Yes No
*The operator (and supervisor) wore hat, mask sterile gown and sterile gloves and sterile drapes were placed to create a sterile operating field
________________________________________ _______________________________________Operator signature Observer signature
MRNorPatientLabel

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-67-
Appendix 11: CVC Care Bundle This bundle has been adapted from the CVC bundle produced by Health Protection Scotland.An example of a Standard Operating Procedure to illustrate one way to use the CVC Bundle is provided below.Howeveryoumaywanttousethisinmanydifferentways,forexample,localdecisionsinclude:whenitisdone,howoftenitisdone,whodoesitandhowthedataarecollected.Thisprocedurecanbeused as a starting point but should not be considered to be prescriptive.
Central Vascular Catheter Care BundleAim: To Reduce the Incidence of Central Vascular Cannula Related Infection
Don’t put them in. Get them out.
Look after them properly.
The Bundle
1. Check the clinical indication why the CVC is in situ – is it still required?
2. Is the CVC dressing intact and changed within the last 7 days?
3. Has CVC hub decontamination been performed before each hub access?
4. Has hand hygiene been performed before and after all CVC maintenance/access procedures?
5. Has Chlorhexidine gluconate 2% in alcohol (if compatible with CVC) been used for cleaning the insertion site during dressing changes?
Example of a CVC Maintenance Bundle Standard Operating Procedure
Objectives Objectives:To optimise CVC use in • OuR ward and reduce as far as possible infection complications.To be able to demonstrate quality CVC care in • OuR ward.
Requirements Before the CVC Bundle Procedure is performed.
Qualityimprovementmustbecontinuous.Thisisnotashorttermcommitment–qualityimprovement needs to be embedded into your systems – to become part of what you do every day.Relevantclinicalteams(consultantsandNCHD’s),directorofnursingandnurseteamshouldbeinvolvedindesigning/adaptingthebundle,decidinghowfrequentlyandwhowillmonitorcomplianceandhowoftenandhowresultswillbefedbacktorelevantclinical,nursingandmanagerial staff: a multidisciplinary intravascular care team could be considered.
Prior to starting the CVC Bundle Procedure
Ensurethereisalcoholhandgelatthebedsideofallpatients(e.g.,personalstafftoggles,wallorbed mounted gels or a trolley with gel attached).
Procedure 1. Perform hand hygiene.
2.Collectabundlesheetandcompletethetopboxes:name,location,observer.
3.ProceedtothefirstpatientwithaCVC.
4.Introduceyourselftothepatient/relativeandexplainthatyouarecheckingallcatheterstoseeifany need removal.
5. Ask the nurse in charge of the patient the questions as stated on the bundle.
6.Lookfordocumentaryevidencetosupportthenurse’sstatements.
7.Ask‘buddynurse’*toconfirmhandhygieneproceduresandalcoholhubprocedureshavebeenoptimal.
8. Perform hand hygiene.
9. Record actions in the bundle.
10. If the CVC is considered not to be required refer to medical staff.
11. Repeat steps 3-10 until all patients in the ward with a CVC have been visited.
After care Complete form. Give it to:Discussanddisplaythedatawhenithasbeenreturned.(Keepbundleformsforxxtime).
*A buddy nurse can be used to verify optimal care and to act as a reminder to the nurse in charge of an individual patient.
Each buddy nurse must be prepared to observe their colleague’s care, comment on it and in turn have their own practices scrutinised

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-68-
Date:Name of person performing the bundle:______________________________________
CVC1
CVC 2
CVC3
The need for line use has been reviewed and recorded today.1.
The dressing is intact and was changed within the past 7 days.2.
Hub decontamination is performed before each hub access.3.
Handhygienebeforeandafter,isperformedonalllinemaintenance/accessprocedures.4.
Chlorhexidine gluconate 2% (or solution compatible with CVC) is used for cleaning the 5. insertion site during dressing changes.
Summary Table of CVC Bundle Findings No.Comment (if required)
Total number of CVCs in situ at start of CVC Maintenance Bundle.
Total number of CVCs with documented need to remain in situ.
Total number of CVCs with evidence of optimal dressing (intact and changed within past 7 days).
Total number of CVCs with evidence of hub decontamination prior to all line maintenance/access procedures.
Total number of CVCs with evidence of hand hygiene performed before and after all CVC procedures.
Total number of CVCs with evidence of Chlorhexidine gluconate 2% (or solution compatible with CVC) used for insertion site antisepsis at last dressing change.
All or None Table – Was CVC Care Today Optimal Tick if achieved
100% of CVCs in situ are required.
100% of CVCs had optimal dressing change.
100% of CVCs had evidence of hub decontamination prior to all access procedures.
100%ofallCVCshadevidencethatHCWsperformedaseptictechniqueincluding,handhygienebeforeandafter,forallCVCprocedures.
100% of CVCs had evidence of Chlorhexidine gluconate 2% (or solution compatible with CVC) used for insertion site antisepsis at the last dressing change.
If all the above were achieved the CVC care was optimal

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-69-
Appendix 12: Form for Collection of Denominator Data for CRBSI Surveillance

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-70-
Appendix 13: Form 2: Form for Collection of CRBSI - Clinical and Laboratory Data

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-71-
Appendix 14: PVC Insertion Procedure Guideline Asepsis, hand hygiene and appropriate technique must be adhered to. Either single use tourniquets should be used or the tourniquet cleaned and disinfected between each patient use.
A dedicated trolley/cart that includes all supplies necessary should be available.•
Confirmidentityofthepatientandexplaintothepatientorparent/guardiantheprocedureandneed•for the PVC.
Only equipment required should be taken to the bedside and set up immediately prior to the •procedure.
Performhandhygiene.(Sections2.1and4.1.1)•
Applytourniquet(tothenondominantforearmifpossible),selectandpalpateanappropriateveinfor•PVC insertion.
Release tourniquet and set up equipment on a clean trolley (sterile dressing/insertion pack).•
Iftheskinisvisiblydirty,washpriortoskinasepsis.Inadultsandchildren• ≥ 2 months (assuming normal gestationatbirth),useasinglepatientuseapplicationofalcoholicchlorhexidinegluconatesolution(preferably 2% chlorhexidine gluconate in 70% isopropyl alcohol if compatible with the PVC) for skin asepsis.(Section4.1.1).Allowthesitetodryandthenreapplythetourniquet.Donot repalpate the area after skin asepsis.
Perform hand hygiene. •
Applyclean(well-fitting)non-sterilegloves.•
Apply tourniquet. •
Insert the PVC using an aseptic (no-touch) technique. •
IfyouhavedifficultyinsertingthePVC,donotattemptrepeatedinsertionswiththesamecannulae.If•afterthreeattemptsyouareunsuccessful,requesthelpfromacolleague–donotcontinuetoattemptto insert the PVC.
The PVC should be stabilised with a sterile transparent semipermeable dressing and sterile adhesive •tapetopreventPVCdislodgement.Donotapplynon-sterileadhesivetapeunderthetransparentsemipermeabledressing.DonotobscuretheabilitytovisualisethePVCsiteandsurroundingtissueswithadhesivetape.Adhesivelabelsindicatinginsertiondetails,ondressingsarerecommended.
Secure adhesive label to dressing or record insertion date on dressing.•
Disposeallsharpscarefullyintoanapprovedsharpscontainer.•
Discardwasteanddecontaminatetrolleyinadesignatedareaawayfromthecleanutilityorwhere•intravenous medications are prepared.
Remove gloves and perform hand hygiene. •
GivethepatienttheIVinformationleafletandaskthepatienttoreportsymptomsofpainordiscomfort•at the PVC site. It is important that the patient is educated regarding hand hygiene and the importance of keeping the PVC site clean and dry.
Accuratedocumentationandrecordkeepingmustbemaintainedtoensurepatientsafety,toallowfor•audits,andtotrackanyoutbreaksofinfection.Thedocumentationshouldinclude.
o The date and time of PVC insertion (so that HCW can clearly assess the duration the PVC is in situ).
o Type of PVC and gauge.
o Anatomical site.
o Name of operator.
o When the PVC is removed/replaced.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-72-
Appendix 15: Example of a Visual Infusion Phlebitis Score.80
Condition of site Score Degree of Phlebitis.
IV Site appears healthy 0
1
2
3
4
5
No signs of Phlebitis. Observe cannula.
One of the following is evident:
Slight discomfort at IV site. •Slight Swelling at IV site.•
First signs of phlebitis. Observe cannula.
Two of the following are evident:
Pain at IV Site.•Erythema.•Swelling.•
Early stages of phlebitis. Resite cannula.
All of the following are present:
Pain along path of cannula.•Erythema.•Induration.•
Medium stages of Phlebitis.Resite cannula.Consider treatment.
All of the following signs are evident:
Pain along path of cannula.•Erythema.•Induration.•Palpable venous cord.•
Advanced stages of phlebitis, or the start of Thrombophlebitis.Resite Cannula.Consider treatment.
All of the following signs are evident and
are extensive:
Pain along path of cannula.•Erythema.•Induration.•Palpable venous cord.•Pyrexia.•
Advanced stages of Thrombophlebitis.Initiate treatment.Resite cannula.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-73-
Appendix 16: PVC Care BundleThis bundle has been adapted from the PVC bundle produced by Health Protection Scotland.An example of a Standard Operating Procedure to illustrate one way to use the PVC Bundle is provided below.Howeveryoumaywanttousethisinmanydifferentways,forexample,localdecisionsinclude:whenitisdone,howoftenitisdone,whodoesitandhowthedataarecollected.Thisprocedurecanbeused as a starting point but should not be considered to be prescriptive.
Peripheral Vascular Catheter Care Bundle
Aim: To Reduce the Incidence of Peripheral Vascular Cannula Related Infection
Don’t put them in. Get them out.
Look after them properly.
The Bundle
1. Check the clinical indication why the PVC is in situ – is it still required?
2. Remove PVCs where there is extravasation or inflammation
3. Check the PVC dressings are intact
4. Consider removing the PVC if it is in situ longer than 72 hours
5. Perform hand hygiene before and after all PVC procedures

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-74-
Example of a PVC care Bundle – Standard Operating Procedure
Objectives Objectives:
1. To optimise PVC care in OuR ward and reduce as far as possible any infectious complications.
2. To be able to demonstrate quality PVC care in OuR ward
Requirements Before the PVC Bundle Procedure can be Considered
Relevantclinicalteams(consultantsandNCHD’s),directorofnursingandnurseteamshouldbeinvolvedindesigning/adaptingthebundle,decidinghowfrequentlyandwhowillmonitorcompliance with the PVC bundle and how often and how results will be fed back to relevant clinical,nursingandmanagerialstaff:amultidisciplinaryintravascularcareteamcouldbeconsidered.
Prior to starting the PVC Bundle Procedure
Personal Protective Equipment (PPE): Gloves; plastic apron (if appropriate as per local infection prevention and control policy).
Procedure 1. Perform hand hygiene.
2.Collectabundlesheetandcompletethetopboxes:name,location,etc.
3.Proceedtothefirstpatient.
4.IntroduceyourselftothepatientandexplainthatyouarecheckingallPVCstoseeifanyneedremoved.
5.Ifitisnotobviousask‘Doyouhaveanyoftheseneedles,PVCsorcannulae?’Iftheansweris‘no’thankthepatient,moveontothenextpatientandgobacktostep4.Iftheansweris‘yes’proceed to number 6.
6.IfitisobvioustheydohaveaPVC,ortheyhavesaidtheydo,performhandhygiene.
7.Maintainingthepatient’sprivacy,asktoseethePVCinsertionsite–completethebundlequestions.
a.IsPVCinuse?(e.g.,currentIVtherapy(medicationorinfusion),PVCrequiredforplannedclinicalprocedure(radiology,transfusionetc)orvascularaccessrequiredduetounstablecondition). PVC in situ and in use select “yes” & go to question 7c. If PVC in situ but not in useandnotrequired,removePVC(ordiscusswithmedicalteamifunsure)andselect“no”tothis question
Decontaminatehandsandmovetonextpatient
b.UseVisualInfusionPhlebitisscore(Appendix15)toassessforextra-vasationorinflammation.Extra-vasation may still be detected even if there is a sterile gauze dressing over the insertion site,however,NEVER,removeadressingjusttoviewaninsertionsite.Ifthereisgauzedressing in situ – the site should be palpated through the dressing for tenderness and if patient complains of local tenderness remove dressing to view site.
c.PVCdressing–ifnotintacteitherreplacedressingorremovePVC(e.g.,ifPVChasbecomedislodged because of the non-intact dressing).
d.DurationofPVC-Determiningexactdateofinsertionfrommedicalnotes/nursingnotes.Notapplicable in paediatrics. 72 hours is not an absolute cut off – local clinical decision based on expecteddurationofPVC,conditionofPVCentrysite,vascularaccess.
e.Ask‘buddynurse’*toconfirmhandhygieneproceduresandalcoholhubprocedureshavebeen optimal. Perform hand hygiene.
8.Recordactions/findingsonthebundlesheet.Ifnecessaryrecordinthepatient’snotes.Ifdeemednecessary,removethePVCaseptically[wearingappropriatePPE]asperlocalguidelines.IfyouareunsureastowhethertoremovethePVC–confirmwithamemberofthemedical team the appropriateness of removing the PVC or it remaining in situ.
9.Gobackandrepeatsteps4-8untilallpatientsinthewardhavebeenvisited.
After care Complete form. Give it to:
Discussanddisplaythedatawhenithasbeenreturned.
*A buddy nurse can be used to verify optimal care and to act as a reminder to the nurse in charge of an individual patient.Each buddy nurse must be prepared to observe their colleague’s care, comment on it and in turn have their own practices scrutinised.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-75-
Ward: Date: Name of person performing the bundle:
Observation number
The PVC is still in use
Absence of inflammation and or extra-vasation
The PVC dressing is intact
The PVC has been inserted for <72 hrs.
Hand Hygiene before & after all PVC procedures
What was done
1(Circle correct answer)
YesContinue bundle
No Remove catheter
YesContinue bundle
No Remove catheter
YesContinue bundle
No Replace dressing or Remove catheter
YesContinue bundle
No Request removal
YesContinue bundle
No Request removal
PVC left in situ
PVC Removed
2 YesContinue bundle
No Remove catheter
YesContinue bundle
No Remove catheter
YesContinue bundle
No Replace dressing or Remove catheter
YesContinue bundle
NoRequestremoval
YesContinue bundle
No Request removal
PVC left in situ
PVC Removed
Summary Table of PVC Bundle Findings Comment (if required)
Total number of PVCs in situ at start of PVC Bundle.
Total number of PVCs removed because they were not being used or were no longer required.
Total number of PVCs removed because of extravasation or insertion siteinflammation.
Total number of PVCs removed because the dressing was not intact or was inappropriate.
Total number of PVCs in situ longer than 72 hours.
Total number of PVCs where hand hygiene has been performed before and after all PVC procedures*.
All or None Table – Was PVC Care Today Optimal Tick if achieved
100% of PVCs in situ are required.
0%(Zero)PVCshadextravasationorinsertionsiteinflammation.
100% of PVCs had appropriate and intact dressings.
0%(Zero)PVCsremovedasaconsequenceofthebundleround.
0%(Zero)ofPVCswerein situ >72 hours.
100% of PVCs were visible and well positioned.
If all the above were achieved the PVC care was optimal.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-76-
Reference List
(1) HoranT,AndrusM,DudeckM.CDC/NHSNsurveillancedefinitionofhealthcare-associatedinfectionandcriteriaforspecifictypesofinfectionsintheacutecaresetting.Am J Infect Control 2008; 36:309-332.
(2) SARI Infection Control Sub-committee. The Control and Prevention of MRSA in Hospitals and in the Community.2005.NationalDiseaseSurveillanceCentre,Ireland.
(3) HealthInformationandQualityAuthorityI.NationalStandardsforthePreventionandControlofHealthcareAssociated Infections . 2009.
(4) MermelLA,AllonM,BouzaE,CravenDE,FlynnP,O’GradyNP et al. Clinical practice guidelines for the diagnosisandmanagementofintravascularcatheter-relatedinfection:2009UpdatebytheInfectiousDiseasesSociety of America. Clin Infect Dis2009;49(1):1-45.
(5) Eggimann P. Prevention of intravascular catheter infection. Curr Opin Infect Dis 2007; 20:360-369.
(6) DimickJB,PelzRK,ConsunjiR,SwobodaSM,HendrixCW,LipsettPA.Increasedresourceuseassociatedwithcatheter-related bloodstream infection in the surgical intensive care unit. Arch Surg2001;136(2):229-234.
(7) WarrenDK,QuadirWW,HollenbeakCS,ElwardAM,CoxMJ,FraserVJ.Attributablecostofcatheter-associated bloodstream infections among intensive care patients in a nonteaching hospital. Crit Care Med 2006;34(8):2084-2089.
(8) RenaudB,Brun-BuissonC.Outcomesofprimaryandcatheter-relatedbacteremia.Acohortandcase-controlstudy in critically ill patients. Am J Respir Crit Care Med2001;163(7):1584-1590.
(9) BlotSI,DepuydtP,AnnemansL,BenoitD,HosteE,DeWaeleJJet al. Clinical and economic outcomes in critically ill patients with nosocomial catheter-related bloodstream infections. Clin Infect Dis2005;41(11):1591-1598.
(10) O’GradyNP,AlexanderM,PatchenDellingerM,GerberdingJL,StippelD,HeardSOetal.GuidelinesforthePrevention of Intravascular Catheter-Related Infections. Clin Infect Dis 2002; 35:1281-1307.
(11) RelloJ,OchagaviaA,SabanesE,RoqueM,MariscalD,ReynagaEetal.Evaluationofoutcomeofintravenouscatheter-related infections in critically ill patients. Am J Respir Crit Care Med 2000; 162(3 Pt 1):1027-1030.
(12) FraherMH,CollinsC,BourkeJ,PhelanD,LynchM.Cost-effectivenessofemployingatotalparenteralnutritionsurveillance nurse for the prevention of catheter-related bloodstream infections. J Hosp Infect 2009; 73:129-134.
(13) MarschallJ,MermelLA,ClassenD,AriasK.M,PodgornyK,AndersonDA et al. Strategies to Prevent Central Line-AssociatedBloodstreamInfectionsinAcuteCareHospitals.Infect Control Hosp Epidemiol 2008;S22-S30.
(14) SafdarN,MakiDG.InflammationattheinsertionsiteisnotpredictiveofIVC-relatedbloodstreaminfectionwithshort-term,noncuffedcentralvenouscatheters.Crit Care Med 2002; 30:2632-2635.
(15) MermelLA,FarrBM,SherertzRJ,RaadII,O’GradyNP,HarrisJS et al. Guidelines for the Management of Intravascular Catheter-Related Infections. Clin Infect Dis2001;32:1249-1272.
(16) CostaSF,MiceliMH,AnaissieEJ.Mucosaorskinassourceofcoagulase-negativestaphylococcalbacteraemia?Lancet Infect Dis2004;4(5):278-286.
(17) DepartmentofHealthandChildren.NorthSouthStudyofMRSAinIreland.ISBN07-0766-4950.2000.
(18) HealthProtectionSurveillanceCentre.EARSSReportforQuarter12009.2009.
(19) SmythET,McIlvennyG,EnstoneJE,EmmersonAM,HumphreysH,FitzpatrickF et al.Fourcountryhealthcareassociated infection prevalence survey 2006: overview of the results. J Hosp Infect2008;69(3):230-248.
(20) HumphreysH,NewcombeRG,EnstoneJ,SmythET,McIlvennyG,FitzpatrickF et al.Fourcountryhealthcareassociated infection prevalence survey 2006: risk factor analysis. J Hosp Infect2008;69(3):249-257.
(21) FitzpatrickF,McIlvennyG,OzaA,NewcombeRG,HumphreysH,CunneyR et al. Hospital Infection Society prevalence survey of Healthcare Associated Infection 2006: comparison of results between Northern Ireland and the Republic of Ireland. J Hosp Infect 2008; 69(3):265-273.
(22) PrattRJ,PelloweCM,WilsonJA,LovedatHP,HarperPJ,JonesSRLJ et al. epic2: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. J Hosp Infect 2007; 65S:S1-S64.
(23) BoyceJM,PittetD.GuidelineforHandHygieneinHealth-CareSettings:recommendationsoftheHealthcareInfectionControlPracticesAdvisoryCommitteeandtheHICPAC/SHEA/APIC/IDSAHandHygieneTaskForce.Infect Control Hosp Epidemiol2002;23(12Suppl):S3-40.
(24) SARIInfectionControlSub-committee.GuidelinesforHandHygieneinIrishHealthCareSettings.2005.
(25) Rowley S. Aseptic non-touch technique. Nursing Times 2001; 97(7):6.
(26) RowleyS,SinclairS.WorkingtowardsanNHSstandardforasepticnon-touchtechnique.Nursing Times2004;100(8):50.
(27) VanherweghemJL,DhaeneM,GoldmanM,StolearJC,SabotJP,WaterlotYet al. Infections associated with subclavian dialysis catheters: the key role of nurse training. Nephron1986;42(2):116-119.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-77-
(28) MeierPA,FredricksonM,CatneyM,NettlemanMD.Impactofadedicatedintravenoustherapyteamonnosocomial bloodstream infection rates. Am J Infect Control1998;26(4):388-392.
(29) KaplowitzLG,ComstockJA,LandwehrDM,DaltonHP,MayhallCG.Aprospectivestudyofinfectionsinhemodialysis patients: patient hygiene and other risk factors for infection. Infect Control Hosp Epidemiol 1988; 9(12):534-541.
(30) PennaTCV,MazzolaPG,SilvaMartinsAM.Theefficacyofchemicalagentsincleaninganddisinfectionprograms. BMC Infectious Diseases2001;1(1624thSeptember).
(31) HoKM,LittonE.Useofchlorhexidine-impregnateddressingtopreventvascularandepiduralcathetercolonization and infection: a meta-analysis. J Antimicrob Chemother 2006; 58(2):281-287.
(32) RuschulteH,FrankeM,GastmeierP,ZenzS,MahrKH,BuchholzS et al. Prevention of central venous catheter related infections with chlorhexidine gluconate impregnated wound dressings: a randomized controlled trial. Ann Hematol 2008.
(33) GarlandJS,AlexCP,MuellerCD,OttenD,ShivpuriC,HarrisMC et al. A randomized trial comparing povidone-iodine to a chlorhexidine gluconate-impregnated dressing for prevention of central venous catheter infections in neonates. Pediatrics2001;107(6):1431-1436.
(34) WilsonCM,GrayG,ReadJS,MwathaA,LalaS,JohnsonS et al. Tolerance and safety of different concentrations of chlorhexidine for peripartum vaginal and infant washes: HIVNET 025. J Acquir Immune Defic Syndr2004;35(2):138-143.
(35) DattaMK,ClarkeP.CurrentpracticesinskinantisepsisforcentralvenouscatheterisationinUKtertiary-levelneonatal units. Archives of Disease in Childhood - Fetal and Neonatal Edition2009;93:F328.
(36) MermelLA,McCormickRD,SpringmanSR,MakiDG.Thepathogenesisandepidemiologyofcatheter-relatedinfection with pulmonary artery Swan-Ganz catheters: a prospective study utilizing molecular subtyping. Am J Med 1991; 91(3B):197S-205S.
(37) RaadII,HohnDC,GilbreathBJ,SuleimanN,HillLA,BrusoPAetal.Preventionofcentralvenouscatheter-related infections by using maximal sterile barrier precautions during insertion. Infect Control Hosp Epidemiol 1994;15(4Pt1):231-238.
(38) KarakitsosD,LabropoulosN,DeGE,PatrianakosAP,KouraklisG,PoularasJ et al. Real-time ultrasound-guided catheterisation of the internal jugular vein: a prospective comparison with the landmark technique in critical care patients. Crit Care 2006; 10(6):R162.
(39) McCarthyMC,ShivesJK,RobisonRJ,BroadieTA.Prospectiveevaluationofsingleandtriplelumencathetersintotal parenteral nutrition. J Parenter Enteral Nutr 1987; 11(3):259-262.
(40) ParientiJJ,ThirionM,MégarbaneB,OuchikheA,PolitoA,MarquéSetal.FemoralvsJugularVenousCatheterization and Risk of Nosocomial Events in Adults Requiring Acute Renal Replacement Therapy: A Randomized Controlled Trial. JAMA2008;229(20):2413-2422.
(41) DeshpandeKS,HatemC,UlrichHL,CurrieBP,AldrichTK,Bryan-BrownCW et al. The incidence of infectious complicationsofcentralvenouscathetersatthesubclavian,internaljugular,andfemoralsitesinanintensivecare unit population. Crit Care Med 2005; 33(1):13-20.
(42) GowardmanJR,MontgomeryC,ThirlwellS,ShewanJ,IdemaA,LarsenPD et al. Central venous catheter-relatedbloodstreaminfections:ananalysisofincidenceandriskfactorsinacohortof400patients.Intensive Care Med1998;24(10):1034-1039.
(43) GowardmanJR,RobertsonIK,ParkesS,RickardCM.Influenceofinsertionsiteoncentralvenouscathetercolonization and bloodstream infection rates. Intensive Care Med2008;34(6):1038-1045.
(44) SafdarN,MakiDG.Useofvancomycin-containinglockorflushsolutionsforpreventionofbloodstreaminfectionassociatedwithcentralvenousaccessdevices:ameta-analysisofprospective,randomizedtrials.Clin Infect Dis2006;43(4):474-484.
(45) FeelyT,CopleyA,BleyerAJ.Catheterlocksolutionstopreventbloodstreaminfectionsinhigh-riskhemodialysis patients. Am J Nephrol2007;27(1):24-29.
(46) GarlandJS,AlexCP,HenricksonKJ,McAuliffeTL,MakiDG.Avancomycin-heparinlocksolutionforpreventionof nosocomial bloodstream infection in critically ill neonates with peripherally inserted central venous catheters: aprospective,randomizedtrial.Pediatrics 2005; 116(2):e198-e205.
(47) YahavD,Rozen-ZviB,Gafter-GviliA,LeiboviciL,GafterU,PaulM.Antimicrobiallocksolutionsfortheprevention of infections associated with intravascular catheters in patients undergoing hemodialysis: systematic reviewandmeta-analysisofrandomized,controlledtrials.Clin Infect Dis2008;47(1):83-93.
(48) PercivalSL,KiteP,EastwoodK,MurgaR,CarrJ,ArduinoMJ et al.TetrasodiumEDTAasanovelcentralvenouscatheterlocksolutionagainstbiofilm.Infect Control Hosp Epidemiol 2005; 26(6):515-519.
(49) SimonA,AmmannRA,WiszniewskyG,BodeU,FleischhackG,BesudenMM.Taurolidine-citratelocksolution(TauroLock)significantlyreducesCVAD-associatedgrampositiveinfectionsinpediatriccancerpatients.BMC Infect Dis 2008; 8:102.
(50) Allon M. Prophylaxis against dialysis catheter-related bacteremia with a novel antimicrobial lock solution. Clin Infect Dis2003;36(12):1539-1544.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-78-
(51) BetjesMG,vanAM.Preventionofdialysiscatheter-relatedsepsiswithacitrate-taurolidine-containinglocksolution. Nephrol Dial Transplant2004;19(6):1546-1551.
(52) OnlandW,ShinCE,FustarS,RushingT,WongWY.Ethanol-locktechniqueforpersistentbacteremiaoflong-term intravascular devices in pediatric patients. Arch Pediatr Adolesc Med2006;160(10):1049-1053.
(53) OpillaMT,KirbyDF,EdmondMB.Useofethanollocktherapytoreducetheincidenceofcatheter-relatedbloodstream infections in home parenteral nutrition patients. J Parenter Enteral Nutr2007;31(4):302-305.
(54) vandeWeteringMD,WoenselJBM.ProphylacticantibioticsforpreventingearlycentralvenouscatheterGrampositiveinfectionsinoncologypatients.Issue1.Art.No.:CD003295.DOI:10.1002/14651858.CD003295.pub2.2007.CochraneDatabaseofSystematicReviews.
(55) JardineLA,InglisGDT,DaviesMW.Prophylacticsystemicantibioticstoreducemorbidityandmortalityinneonateswithcentralvenouscatheters.Issue1.Art.No.:CD006179.DOI:10.1002/14651858.CD006179.pub2.2008.CochraneDatabaseofSystematicReviews.
(56) RoyalCollegeofNursing.StandardsforInfusiontherapy.2007.RoyalCollegeofNursing,London.
(57) IBTS-NationalBloodUsersGroup.GuidelinesfortheAdministrationofBloodandBloodComponents.2004.
(58) InstituteforHealthcareImprovement-CentralLineBundle.2009. Internet Communication
(59) HugonnetS,SaxH,EggimannP,ChevroletJC,PittetD.Nosocomialbloodstreaminfectionandclinicalsepsis.Emerg Infect Dis2004;10(1):76-81.
(60) NationalNosocomialInfectionsSurveillance(NNIS)SystemReport,datasummaryfromJanuary1992toJune2002,issuedAugust2002.Am J Infect Control2002;30(8):458-475.
(61) NationalHealthcareSafetyNetwork(NHSN).CDC.2009.
(62) EdwardsJR,PetersonKD,AndrusML,DudeckMA,PollockDA,HoranTC.NationalHealthcareSafetyNetwork(NHSN)Report,datasummaryfor2006through2007,issuedNovember2008.Am J Infect Control 2008; 36(9):609-626.
(63) NHSNManual:PatientSafetyComponentProtocol.CDC.2009.
(64) HospitalinEuropeLinkforInfectionControlthroughSurveillance.SurveillanceofNososcomialInfectionsinIntensiveCareUnits-Protocol.Version6.1.2004.
(65) RaadII,HannaH,MakiDG.Intravascularcatheter-relatedinfections:advancesindiagnosis,prevention,andmanagement. Lancet Infect Dis2007;7:645-657.
(66) PeacockSJ,EddlestonM,EmptageA,KingA,CrookDW.Positiveintravenouslinetipculturesaspredictorsofbacteraemia. J Hosp Infect1998;40(1):35-38.
(67) SherertzRJ,HeardSO,RaadII.Diagnosisoftriple-lumencatheterinfection:comparisonofrollplate,sonication,andflushingmethodologies.J Clin Microbiol1997;35(3):641-646.
(68) EkkelenkampMB,vanderBruggenT,vandeVijverDA,WolfsTF,BontenMJ.Bacteremiccomplicationsofintravascular catheters colonized with Staphylococcus aureus. Clin Infect Dis2008;46(1):114-118.
(69) RuheJJ,MenonA.ClinicalsignificanceofisolatedStaphylococcusaureuscentralvenouscathetertipcultures.Clin Microbiol Infect 2006; 12(9):933-936.
(70) USFoodandDrugAdministration.InformationforHealthcareProfessionalsLinezolid(marketedasZyvox).16-3-2007.
(71) CollinsCJ,FraherM,BourkeJ,PhelanD,LynchM.EpidemiologyofCandidaspeciesCatheterRelated-Bloodstream Infection in Patients on Total Parenteral Nurtition. Clin Infect Dis2009:49;1769-1770.
(72) Health Protection Surveillance Centre. Enhanced EARSS surveillance - report for 2008.
(73) RaadI,HannaH,BoktourM,GirgawyE,DanawiH,MardaniM et al. Management of central venous catheters in patients with cancer and candidemia. Clin Infect Dis2004;38(8):1119-1127.
(74) KorbilaIP,BliziotisI.A,LawrenceKR,FalagasME.Antibiotic-locktherapyforlong-termcatheter-relatedbacteraemia: a review of the current evidence. Expert Rev Anti Infect Ther2007;5(4):639-652.
(75) PooleCV,CarltonD,BimboL,AllonM.Treatmentofcatheter-relatedbacteraemiawithanantibioticlockprotocol: effect of bacterial pathogen. Nephrol Dial Transplant2004;19(5):1237-1244.
(76) RijndersBJ,VanWE,VandecasteeleSJ,StasM,PeetermansWE.Treatmentoflong-termintravascularcatheter-relatedbacteraemiawithantibioticlock:randomized,placebo-controlledtrial.J Antimicrob Chemother 2005; 55(1):90-94.
(77) FortunJ,GrillF,Martin-DavilaP,BlazquezJ,TatoM,Sanchez-CorralJ et al. Treatment of long-term intravascular catheter-related bacteraemia with antibiotic-lock therapy. J Antimicrob Chemother 2006; 58(4):816-821.
(78) EggimannP.Diagnosisofintravascularcatheterinfection.Curr Opin Infect Dis2007;20(4):353-359.
(79) DoughertyL,LambJ.IntravenousTherapyinNursingPractice.ChurchillLivingstone.London.;1999.
(80) JacksonA.Abattleinvein-Infusionphlebitis.Nursing Times1998;94(4):68-70.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-79-
(81) Preventing intravascular device-related bloodstream infections - Recommended practices for the insertion and management of peripheral intravenous catheters. Centre for Healthcare related Infection Surveillance and Prevention,QueenslandAustralia.2009.
(82) BregenzerT,ConenD,SakmannP,WidmerAF.Isroutinereplacementofperipheralintravenouscathetersnecessary? Arch Intern Med 1998; 158(2):151-156.
(83) HomerLD,HolmesKR.Risksassociatedwith72-and96-hourperipheralintravenouscatheterdwelltimes.J Intraven Nurs 1998; 21:301-305.
(84) CatneyMR,HillisS,WakefieldB,SimpsonL,DominoL,KellerS.Relationshipbetweenperipheralintravenouscatheterdwelltimeandthedevelopmentofphlebitisandinfiltration.J Infus Nurs2001;24:332-341.
(85) WebsterJ,ClarkeS,PatersonD,HuttonA,vanDS,GaleC et al. Routine care of peripheral intravenous catheters versus clinically indicated replacement: randomised controlled trial. BMJ 2008; 337:a339.
(86) MakiDG.Improvingthesafetyofperipheralintravenouscatheters.BMJ 2008; 337:a630.
(87) LinaresJ.Diagnosisofcatheter-relatedbloodstreaminfection:conservativetechniques.Clin Infect Dis 2007; 44(6):827-829.
(88) CleriDJ,CorradoML,SeligmanSJ.Quantitativecultureofintravenouscathetersandotherintravascularinserts.J Infect Dis1980;141(6):781-786.
(89) Brun-BuissonC,AbroukF,LegrandP,HuetY,LarabiS,RapinM.Diagnosisofcentralvenouscatheter-relatedsepsis. Critical level of quantitative tip cultures. Arch Intern Med1987;147(5):873-877.
(90) SherertzRJ,RaadII,BelaniA,KooLC,RandKH,PickettDLetal.Three-yearexperiencewithsonicatedvascularcatheter cultures in a clinical microbiology laboratory. J Clin Microbiol 1990; 28(1):76-82.
(91) MakiDG,WeiseCE,SarafinHW.Asemiquantitativeculturemethodforidentifyingintravenous-catheter-relatedinfection. N Engl J Med 1977; 296(23):1305-1309.
(92) Siegman-IgraY,AnglimAM,ShapiroDE,AdalKA,StrainBA,FarrBM.Diagnosisofvascularcatheter-relatedbloodstream infection: a meta-analysis. J Clin Microbiol1997;35(4):928-936.
(93) BlotF,NitenbergG,ChachatyE,RaynardB,GermannN,AntounS et al.Diagnosisofcatheter-relatedbacteraemia: a prospective comparison of the time to positivity of hub-blood versus peripheral-blood cultures. Lancet1999;354(9184):1071-1077.
(94) SafdarN,FineJP,MakiDG.Meta-analysis:methodsfordiagnosingintravasculardevice-relatedbloodstreaminfection. Ann Intern Med2005;142(6):451-466.
(95) DruskinMS,SiegelPD.BacterialContaminationofIndwellingIntravenousPolyethyleneCatheters.JAMA 1963; 185:966-968.
(96) CercenadoE,EnaJ,Rodriguez-CreixemsM,RomeroI,BouzaE.Aconservativeprocedureforthediagnosisofcatheter-related infections. Arch Intern Med1990;150(7):1417-1420.
(97) AtelaI,CollP,RelloJ,QuintanaE,BarrioJ,MarchF et al. Serial surveillance cultures of skin and catheter hub specimens from critically ill patients with central venous catheters: molecular epidemiology of infection and implications for clinical management and research. J Clin Microbiol1997;35(7):1784-1790.
(98) BouzaE,MunozP,BurilloA,Lopez-RodriguezJ,Fernandez-PerezC,PerezMJ et al. The challenge of anticipating catheter tip colonization in major heart surgery patients in the intensive care unit: are surface cultures useful? Crit Care Med 2005; 33(9):1953-1960.
(99) KiteP,DobbinsBM,WilcoxMH,FawleyWN,KindonAJ,ThomasDetal.Evaluationofanovelendoluminalbrush method for in situ diagnosis of catheter related sepsis. J Clin Pathol1997;50(4):278-282.
(100) KiteP,DobbinsBM,WilcoxMH,McMahonMJ.Rapiddiagnosisofcentral-venous-catheter-relatedbloodstreaminfection without catheter removal. Lancet1999;354(9189):1504-1507.
(101) TigheMJ,KiteP,FawleyWN,ThomasD,McMahonMJ.Anendoluminalbrushtodetecttheinfectedcentralvenous catheter in situ: a pilot study. BMJ 1996; 313(7071):1528-1529.
(102) RushforthJA,HoyCM,KiteP,PuntisJW.Rapiddiagnosisofcentralvenouscathetersepsis.Lancet 1993; 342(8868):402-403.
(103) MartinezJA,DesJardinJA,AronoffM,SupranS,NasrawaySA,SnydmanDR.Clinicalutilityofbloodculturesdrawn from central venous or arterial catheters in critically ill surgical patients. Crit Care Med 2002; 30(1):7-13.
(104) HealthProtectionAgency.Investigationofintravascularcannulaeandassociatedspecimens. HPA BSOP 20 . 2009.
(105) RaadII,HannaHA,DarouicheRO.Diagnosisofcatheter-relatedbloodstreaminfections:isitnecessarytoculture the subcutaneous catheter segment? Eur J Clin Microbiol Infect Dis 2001; 20(8):566-568.
(106) LonguetP,DouardMC,ArletG,MolinaJM,BenoitC,LeportC.Venousaccessport--relatedbacteremiainpatientswithacquiredimmunodeficiencysyndromeorcancer:thereservoirasadiagnosticandtherapeutictool. Clin Infect Dis 2001; 32(12):1776-1783.
(107) RaadI,CostertonW,SabharwalU,SacilowskiM,AnaissieE,BodeyGP.Ultrastructuralanalysisofindwellingvascular catheters: a quantitative relationship between luminal colonization and duration of placement. J Infect Dis1993;168(2):400-407.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-80-
(108) BouzaE,AlvaradoN,AlcalaL,Sanchez-CondeM,PerezMJ,MunozP et al.Aprospective,randomized,andcomparative study of 3 different methods for the diagnosis of intravascular catheter colonization. Clin Infect Dis 2005;40(8):1096-1100.
(109) SchmittSK,KnappC,HallGS,LongworthDL,McMahonJT,WashingtonJA.Impactofchlorhexidine-silversulfadiazine-impregnated central venous catheters on in vitro quantitation of catheter-associated bacteria. J Clin Microbiol1996;34(3):508-511.
(110) SchierholzJM,BachA,FleckC,BeuthJ,KonigD,PulvererG.Measurementofultrasonic-inducedchlorhexidineliberation: correlation of the activity of chlorhexidine-silver-sulfadiazine-impregnated catheters to agar roll technique and broth culture. J Hosp Infect2000;44(2):141-145.
(111) CattonJA,DobbinsBM,KiteP,WoodJM,EastwoodK,SugdenS et al. In situ diagnosis of intravascular catheter-relatedbloodstreaminfection:acomparisonofquantitativeculture,differentialtimetopositivity,andendoluminal brushing. Crit Care Med2005;33(4):787-791.
(112) BouzaE,AlvaradoN,AlcalaL,PerezMJ,RinconC,MunozP.Arandomizedandprospectivestudyof3procedures for the diagnosis of catheter-related bloodstream infection without catheter withdrawal. Clin Infect Dis2007;44(6):820-826.
(113) WarwickS,WilksM,HennessyE,Powell-TuckJ,SmallM,SharpJetal.Useofquantitative16SribosomalDNAdetectionfordiagnosisofcentralvascularcatheter-associatedbacterialinfection.J Clin Microbiol2004;42(4):1402-1408.
(114) WorthingtonT,ElliottTS.Diagnosisofcentralvenouscatheterrelatedinfectioninadultpatients.J Infect 2005; 51(4):267-280.
(115) KohDB,GowardmanJR,RickardCM,RobertsonIK,BrownA.Prospectivestudyofperipheralarterialcatheterinfection and comparison with concurrently sited central venous catheters. Crit Care Med2008;36(2):397-402.
(116) PujolM,HorneroA,SaballsM,ArgerichMJ,VerdaguerR,CisnalM et al. Clinical epidemiology and outcomes ofperipheralvenouscatheter-relatedbloodstreaminfectionsatauniversity-affiliatedhospital.J Hosp Infect 2007; 67(1):22-29.
(117) TrickWE,MirandaJ,EvansAT,Charles-DamteM,ReillyBM,ClarkeP.Prospectivecohortstudyofcentralvenous catheters among internal medicine ward patients. Am J Infect Control2006;34(10):636-641.
(118) EggimannP,ZanettiG.Onthewaytowardseradicationofcatheter-relatedinfections!Intensive Care Med 2008;34(6):988-990.
(119) LorenteL,HenryC,MartinMM,JimenezA,MoraML.Centralvenouscatheter-relatedinfectioninaprospectiveandobservationalstudyof2,595catheters.Crit Care 2005; 9(6):R631-R635.
(120) SmithE,ClarkeL.Antimicrobialandantibioticcoatedcentralvenouscatheters.2004.
(121) StevensonKB,AdcoxMJ,MalleaMC,NarasimhanN,WagnildJP.Standardizedsurveillanceofhemodialysisvascularaccessinfections:18-monthexperienceatanoutpatient,multifacilityhemodialysiscenter.Infect Control Hosp Epidemiol 2000; 21(3):200-203.
(122) YuVL,GoetzA,WagenerM,SmithPB,RihsJD,HanchettJetal.Staphylococcus aureus nasal carriage and infectioninpatientsonhemodialysis.Efficacyofantibioticprophylaxis.N Engl J Med 1986; 315(2):91-96.
(123) JamesMT,ConleyJ,TonelliM,MannsBJ,MacRaeJ,HemmelgamBR.Meta-analysis:AntibioticsforProphylaxisagainst Hemodialysis Catheter-Related Infections. Ann Intern Med2008;148(8):596-605.
(124) RossneyA,O’ConnellB.EmergingProblemwithHigh-levelMupirocinResistanceAmongMRSAinIreland.EpiInsight2008;9(3):4.
(125) AnnigeriR,ConlyJ,VasS,DedierH,PrakashanKP,BargmanJMetal.Emergenceofmupirocin-resistantStaphylococcus aureus in chronic peritoneal dialysis patients using mupirocin prophylaxis to prevent exit-site infection . Perit Dial Int2001;21(6):554-559.
(126) HealthProtectionScotland.NHSScotlandMRSAScreeningPathfinderProgramme-Interimreport.2009.
(127) European Renal Association. European Best Practice Guidelines for Haemodialysis (Part 1): VI.2 Prevention of infection: management of host colonization by Staphylococcus aureus. Nephrol Dial Transplant 2002; 17(Suppl 7):74-75.
(128) OsonoE,TakahashiM,KuriharaS,OhwadaK,SakuraiY,OnodaN et al. Effects of “isolating hemodialysis” on prevention of methicillin-resistant Staphylococcus aureus cross-infection in a hemodialysis unit. Clin Nephrol 2000;54(2):128-133.
(129) MokrzyckiMH,ZhangM,CohenH,GolestanehL,LautJM,RosenbergSO.Tunnelledhaemodialysiscatheterbacteraemia:riskfactorsforbacteraemiarecurrence,infectiouscomplicationsandmortality.Nephrol Dial Transplant2006;21(4):1024-1031.
(130) Garrouste-OrgeasM,TimsitJF,SoufirL,TaffletM,AdrieC,PhilippartF et al. Impact of adverse events on outcomes in intensive care unit patients. Crit Care Med2008;36(7):2041-2047.
(131) Garrouste-Org,TimsitJF,TaffletM,MissetB,ZaharJR,SoufirL et al. Excess risk of death from intensive care unit-acquired nosocomial bloodstream infections: a reappraisal. Clin Infect Dis2006;42(8):1118-1126.
(132) TimsitJF.Whatisthebestsiteforcentralvenouscatheterinsertionincriticallyillpatients?Crit Care 2003; 7(6):397-399.

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-81-
(133) Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med 2000; 132(5):391-402.
(134) Eggimann P, Harbarth S, Constantin MN, Touveneau S, Chevrolet JC, Pittet D. Impact of a prevention strategy targeted at vascular-access care on incidence of infections acquired in intensive care. Lancet 2000; 355(9218):1864-1868.
(135) Pittet D. The Lowbury lecture: behaviour in infection control. J Hosp Infect 2004; 58(1):1-13.
(136) Webster J, Alghamdi A. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database of Systematic Reviews 2007, Issue 4. Art. No.: CD006353. DOI: 10.1002/14651858.CD006353.pub2

Prevention of Intravascular Catheter-related Infection in Ireland HSE/HPSC
-82-

25-27 Middle Gardiner Street Dublin 1 IrelandTel +353 1 876 5300 Fax +353 1 856 1299 Email [email protected] www.hpsc.ie
This report is also available to download on the HPSC website at www.hpsc.ie
Antimicrobial Resistance in IrelandA Strategy for the Control of S A R I
Prevention of Intravascular Catheter-related Infection in Ireland
SARI Prevention of Intravascular Catheter-related Infection Sub-Committee