antibody-based radionuclide targeting for diagnostics and...
TRANSCRIPT

ACTAUNIVERSITATISUPSALIENSISUPPSALA2006
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 204
Antibody-Based RadionuclideTargeting for Diagnostics andTherapy
Preclinical Studies on Head and Neck Cancer
MARIKA NESTOR
ISSN 1651-6206ISBN 91-554-6729-6urn:nbn:se:uu:diva-7341

List of papers
I Ekberg T, Nestor M, Engström M, Nordgren H, Wester K, Carls-son J, Anniko M: Expression of EGFR, HER2, HER3, and HER4 in metastatic squamous cell carcinomas of the oral cavity and base of tongue. Int J Oncol 26(5), 1177-85 (2005).
II Nestor M, Ekberg T, Dring J, van Dongen GA, Wester K,
Nordgren H, Tolmachev V, Anniko M: Quantification of CD44v6 and EGFR expression in head and neck squamous cell carcinoma using a single dose radioimmunoassay. Submitted manuscript (Lab Invest).
III Nestor M, Persson M, Cheng J, Tolmachev V, van Dongen GA,
Anniko M, Kairemo, K: Biodistribution of the chimeric mono-clonal antibody U36 radioiodinated with a closo-dodecaborate-containing linker. Comparison with other radioiodination meth-ods. Bioconjug Chem 14, 805-10 (2003).
IV Nestor M, Persson M, van Dongen GA, Jensen HJ, Lundqvist H,
Anniko M, Tolmachev V: In vitro evaluation of the astatinated chimeric monoclonal antibody U36, a potential candidate for treatment of head and neck squamous cell carcinoma. Eur J Nucl Med Mol Imaging 32, 1296-304 (2005).
V Fortin MA, Nestor M, Salnikov AV, Heldin NE, Rubin K,
Lundqvist H: Immuno-PET of undifferentiated thyroid carci-noma with radioiodine-labelled antibody cMAb U36: application to antibody tumour uptake studies. Submitted manuscript (Eur J Nucl Med Mol Imaging).
Reprints were made with kind permission from International Journal of On-cology (I), American Chemical Society (III), and Springer Science and Busi-ness Media (IV).


Contents
Introduction.....................................................................................................9 Head and neck cancer.................................................................................9
Squamous cell carcinoma ......................................................................9 Thyroid cancer .......................................................................................9 Current treatments ...............................................................................10
The targeting concept ...............................................................................10 Radioimmunotherapy, RIT ..................................................................11 Radioimmunodiagnosis, RID ..............................................................11
Targets......................................................................................................12 Finding and analysing targets ..............................................................12 Targeting structures in HNSCC...........................................................13
Vectors .....................................................................................................15 cMAb U36 ...........................................................................................15 cMAb cetuximab .................................................................................16
Radiohalogens ..........................................................................................17 Radiohalogens for therapy...................................................................17 Radiohalogens for imaging..................................................................18
Labelling ..................................................................................................18 Direct labelling ....................................................................................19 Indirect labelling..................................................................................19
The complete design of the targeting conjugate.......................................20
Aim ...............................................................................................................21
The present study ..........................................................................................22 Molecular targets in HNSCC (papers I & II) ...........................................22
IHC studies ..........................................................................................22 Quantitative studies .............................................................................24 Comments............................................................................................24
Suitable radiohalogen labelling methods (paper III) ................................26 Comments............................................................................................27
Radiohalogenated cMAb U36 for therapy (paper IV)..............................28 211At-cMAb U36 and 131I-cMAb U36..................................................28 Comments............................................................................................30
Radiohalogenated cMAb U36 for imaging (paper V)..............................32 124I-cMAb U36.....................................................................................32

Comments............................................................................................33
Conclusions...................................................................................................35
Ongoing and future studies ...........................................................................37 Receptor quantification studies ................................................................37 Cocktail studies with cetuximab...............................................................37 Radiometal-labelled cMAb U36 ..............................................................38
Acknowledgements.......................................................................................39
References.....................................................................................................41

Abbreviations
18FDG [18F]-2–fluoro-2-deoxy-D-glucose CAT Chloramine T cDNA Complementary DNA CDR/s Complimentarity determining region/regions CHX-A’’-DTPA [(R)-2-Amino-3-(4-isothiocyanatophenyl)propyl]-trans-
(S,S)-cyclohexane-1,2-diamine-pentaacetic acid cMAb/s Chimeric monoclonal antibody/antibodies CPM Counts per minute DABI (4-isothiocyanato-benzylammonio)-undecahydro-closo-
dodecaborate (1-) DMEM Dulbeccos´ modified eagle medium DNA Deoxyribonucleic acid DPC Decays per cell EGFR Epidermal growth factor receptor erbB-1 Epidermal growth factor receptor erbB-2 Human epidermal growth factor receptor 2 erbB-3 Human epidermal growth factor receptor 3 erbB-4 Human epidermal growth factor receptor 4 ELISA Enzyme-linked immunosorbent assay Fab Antigen-binding fragment FDA The U.S. Food and Drug Administration Fv Variable fragment HER1 Epidermal growth factor receptor HER2 Human epidermal growth factor receptor 2 HER3 Human epidermal growth factor receptor 3 HER4 Human epidermal growth factor receptor 4 HNSCC Head and neck squamous cell carcinoma i.v. Intravenously IgG1 Immunoglobulin, class G1 IHC Immunohistochemistry KD Dissociation constant LET Linear energy transfer MP Multi point MAb Monoclonal antibody ND Not done neu Human epidermal growth factor receptor 2

NIS Sodium iodide symporter p.i. Post-injection PAB N-succinimidyl-para-astatobenzoate PET Positron emission tomography PIB N-succinimidyl-para -iodobenzoate RID Radioimmunodiagnosis RIT Radioimmunotherapy RNA Ribonucleic acid SCC Squamous cell carcinoma s.c. Subcutaneously scFv Single-chain Fv SD Single dose SPECT Single photon emission computerised tomography SPMB N-succinimidyl-para-(tri-n-methylstannyl) benzoate TAA Tumour-associated antigen TNM Tumour, Nodes, Metastasis UICC International union against cancer

9
Introduction
Head and neck cancer Cancer can occur in any of the over 30 different tissues or organs in the head and neck area. Worldwide, approximately 500,000 new cases of head and neck cancer are diagnosed each year [1, 2], and about half of these patients will eventually die of this disease [3]. Head and neck cancer is more com-mon in men than in women. It is diagnosed mostly in people over the age of 50 and is likely to be caused by lifestyles and habits (such as use of tobacco and alcohol), whereas a few are caused by genetic factors. Subclasses are carcinoma, sarcoma, lymphoma and melanoma, of which carcinoma is the most common type.
In this thesis, we have focused mainly on head and neck squamous cell carcinoma (HNSCC), and to some extent thyroid anaplastic carcinoma.
Squamous cell carcinoma About 85% of all head and neck tumours are carcinomas. This cancer type originates in the epithelium, the cells that form the lining of the mouth, nose, throat or ear, or the surface layer covering the tongue.
Squamous cell carcinoma is the predominant histological type among car-cinomas, accounting for approximately 5% of all malignant neoplasms in Europe and the USA [4]. Even though the early stages of the disease are associated with a good prognosis, there is still a high failure rate for the more advanced stages, locally as well as at distant sites [5]. An effective adjuvant systemic therapy for minimal residual disease is therefore needed to improve the survival rate for this patient category.
Thyroid cancer The thyroid, a small gland in the front of the neck just below the larynx, is one of a network of glands throughout the body that constitute the endocrine system. Thyroid carcinomas are classified according to histopathological criteria into two types: differentiated carcinoma (papillary and follicular), and undifferentiated (medullary or anaplastic) carcinoma.

10
Thyroid carcinoma accounts for roughly 1% of all new malignant disease cases, and is the most common endocrine malignancy. Differentiated tu-mours are usually curable, whereas undifferentiated tumours have a much poorer prognosis, and patient death generally occurs a few months after di-agnosis [6-9]ko. The recurrence rate of thyroid cancer is high (~30%), and thyroid carcinoma remains a diagnostic as well as a therapeutic challenge to the clinician [10-12].
Current treatments The current treatment options for HNSCC include surgery, radiotherapy, and in certain cases chemotherapy, often combined with each other. Photody-namic therapy can also be used, but is less common. However, the current treatment modalities often fail in the therapy of advanced disease, as they offer no satisfactory means to locate or treat metastases selectively without harming adjacent tissues [13].
For thyroid carcinoma, common treatments include surgery and injection of 131I, but also hormonal therapy, external radiation therapy, and in some cases chemotherapy. For anaplastic thyroid carcinoma, other strategies than intravascularly injected radioiodine need to be devised, since this cancer type has a modest expression of the sodium iodide symporter (NIS) that mediates radioactive iodine transport into the thyroid follicular cells [14].
The targeting concept Radioimmunotargeting uses radiolabelled antibodies or antibody fragments either for radioimmunotherapy (RIT) or radioimmunodiagnosis (RID). The concept is that the antibody mediates delivery of radioactivity to a targeted structure, e.g. an antigen on a tumour cell (Figure 1).
In addition to radioimmunotargeting, antibodies can be used as sole agents or in combination with other treatments, or as vectors for cytotoxic drugs [15]. Targeting therapies are a growing field, with more than 25% of all pharmacological agents currently under development being antibody based [16, 17]. In the recent years, several monoclonal antibodies (MAbs) have received FDA (The U.S. Food and Drug Administration) approval for indications in oncology, and targeting of tumour-associated antigens using MAbs, such as cetuximab and trastuzumab, is already becoming a clinical reality [18-23].

11
Figure 1. In radioimmunotargeting, an antibody (or antibody derivate) labelled with a radionuclide binds specifically to a target antigen on the cell surface. If a tumour cell overexpresses a certain antigen, this can be utilized to attain a higher concentra-tion of radionuclides in tumour tissue than in healthy tissue.
Radioimmunotherapy, RIT The objective with RIT is to cause DNA damage in the targeted cell by sub-jecting it to a maximum dose of radioactivity, but with minimum uptake in healthy organs and tissues. By using a radioactive nuclide as the cytotoxic agent, the problem of multi-drug resistance can be avoided. Also, the “cross-fire” effect reduces the need for every cancer cell to express the antigen, as the radiation emitted by some radionuclides can destroy neighbouring cancer cells [24].
RIT may be a promising way to improve the treatment of HNSCC [25]. This tumour type is particularly susceptible to RIT as it is intrinsically radio-sensitive, and expresses favourable levels of certain tumour-associated anti-gens [26].
Radioimmunodiagnosis, RID In RID, the radioactivity delivered to a tumour cell is used to visualize the tumour. Here too, the goal is to achieve the highest possible ratio of radioac-tivity concentration in the tumour to radioactivity concentration in healthy tissue. If the radionuclide emits gamma radiation, single photon emission computerized tomography (SPECT) can be used to obtain functional and physiological information. If the radionuclide instead decays by emitting positrons, positron emission tomography (PET) can be used.
In both procedures, the radiation is detected outside the body, reflecting the biodistribution of the radiolabel within the body. Generally speaking, PET is considered advantageous to SPECT due to its superior spatial and temporal resolution and greater accuracy, but is more expensive, and still not as readily available as SPECT.

12
During the last years, 18FDG-PET (18F-labelled fluoro-2-deoxy-D-glucose) has made an impact in diagnosis and staging of HNSCC [27]. This derivative measures increased glucose accumulation as an indication of ma-lignant activity. However, 18FDG-PET can show increased uptake not only in tumours but also in normal tissues with high metabolic activity (e.g. brain and heart) and at sites of infection [28]. Furthermore, a number of tumours do not incorporate 18FDG-PET, causing false negative results [29].
Immuno-PET, the combination of PET with MAbs, is an attractive option to improve tumour detection. Since it combines the high sensitivity and reso-lution of a PET camera with the specificity of a MAb, it could increase the diagnostic reliability and thus improve the local treatment of the disease [30, 31].
TargetsTargeting treatments are dependent on knowledge of suitable molecular tar-gets, and the relationships between their expression, pathogenesis and clini-cal outcome. For an effective RIT, the targeted antigen need to be accessible to the antibody, and should not be shed into circulation. The antigen must also have a high and preferably homogeneous expression in the tumour tis-sue, but a low or no expression in normal tissue, in order to obtain a high tumour to healthy tissue uptake ratio [15].
Consequently, an accurate assessment of the degree of target antigen ex-pression in the clinical setting is critical to obtain an indication of both prog-nosis and whether or not a certain patient is likely to benefit from the target treatment.
Finding and analysing targets The existence of tumour-associated target antigens (TAAs) was discovered about 40 years ago when it was demonstrated that mice injected with tumour cells developed a cellular immune response to these tumour cells, but not against other tumour cells. Since then, a variety of TAAs that can be recog-nized by human T-cells have been identified.
Several other approaches to identify TAAs rely on molecular methods rather than on identification by the immune system. For example, expressed proteins from cancer cells can be eluted from a gel and sequenced by mass spectroscopy, and then compared with those expressed by healthy cells from which the cancer arose. Using a similar strategy, microarray technologies can be used to obtain profiles of expressed RNAs. Other approaches such as preparation of recombinant complementary DNA (cDNA) expression librar-ies can also be employed [32].

13
Today, potential target antigens are analysed chiefly by immunohisto-chemistry (IHC). This is a semi-quantitative technique, whereby tissue sam-ples are stained for different antigens, and then assessed by experienced staff. IHC plays a valuable role in profiling the expression of target antigens in tumours and normal material, and can elicit important information regard-ing the distribution of the antigen within the tissue sample.
It may however be difficult to distinguish between membrane and cyto-plasmic expression when using IHC, and a degree of caution has to be exer-cised when comparing different IHC studies. Criteria for judging intensity and extent of staining may differ between studies, and different antibodies directed towards the same antigen might display different staining intensities [33-35]. In order to evaluate new targeting structures suitable for antibody-based treatments, a complement to IHC is needed to quantitate antigen ex-pression on the tumour cell surface and to facilitate comparisons between antigens [35].
Targeting structures in HNSCC CD44v6CD44v6, an isoform of the membrane-associated glycoprotein CD44, is expressed in many types of human cancer, including HNSCC [36], gastric cancer, colorectal cancer, ovarian cancer and prostate cancer [37, 38]. It has been suggested to be involved in tumour formation, tumour cell invasion and metastasis formation [39, 40]. Homogeneous expression of CD44v6 has been observed in a majority of primary and metastatic squamous cell carci-nomas, whereas expression in non-malignant tissues is essentially restricted to a subset of epithelia [26, 41]. This difference in expression between healthy and malignant cells makes the CD44v6 antigen an attractive target for antibody-based therapy.
The EGF receptor family The epidermal growth factor (EGF) receptor family consists of the epidermal growth factor receptor (EGFR/erbB-1/HER1), HER2 (neu/erbB-2), HER3 (erbB-3), and HER4 (erbB-4). These are type 1 tyrosine kinase receptors and are important for mediating signals to control proliferation and differentia-tion [42]. The signal transduction is mediated by binding of a ligand to the receptor (except for HER2, which has no known ligand [43]), which then forms a hetero- or homodimer with another receptor in the family. The re-ceptors thereafter initiate intracellular signalling via various phosphorylation steps. The HER3 receptor has no intrinsic tyrosine kinase activity, but can be transphosphorylated by both EGFR and HER2 [44]. Since there are four known members of this receptor family, and several ligands, there are nu-merous possibilities of hetero- and homodimers and signalling patterns [45].

14
EGFREGFR is a transmembrane cell surface receptor found primarily on cells of epithelial origin. Overexpression of EGFR is common in HNSCC, breast cancer, ovarian cancer, prostate cancer, bladder cancer, glioblastoma, non-small cell lung cancer, and has also been found to play a significant role in the progression of several human malignancies [46, 47].
The EGFR expression in healthy tissues is most often low, compared with that in tumour cells. One important exception is the expression of EGF re-ceptors in liver hepatocytes, which express about 105-106 EGFR per cell [48, 49].
HER2HER2 is a receptor located primarily at the cellular membrane. The HER2 receptor is overexpressed and subjected to targeting treatment in a subset of mammary malignancies, for instance breast, ovarian, and urinary bladder [50, 51]. In HNSCC, the results of studies on HER2 expression have been diverse [52, 53], but increased levels of HER2 have been suggested in sev-eral studies of HNSCC [52], with possible prognostic value in oral SCC [53-56]. Increased HER2 activity is generally associated with increased prolif-eration, reduced apoptotic activity [50, 57], and short disease-free survival [58]. Whereas HER2 is often overexpressed in a variety of cancers, it is ex-pressed only to a small extent in healthy adult tissues [59, 60].
HER3 and HER4 Although EGFR and HER2 have been extensively studied, the role of the remaining two family members, HER3 and HER4, is less evident [61].
HER3 has been shown to be overexpressed in certain HNSCC cell lines, and may have prognostic significance in oral cancer [56, 62, 63]. There are some reports on HER3 expression in HNSCC and co-expression of HER3 with other family members [56, 64, 65]. However, HER3 can also be ex-pressed in the healthy surface squamous epithelium of the tongue, orophar-ynx and oesophagus [66].
In breast cancer, the presence of HER4 has been associated with a good prognosis [67-69], whereas in colorectal cancer, HER4 expression status may identify tumours with aggressive biological behaviour and increased metastatic potential [70]. A number of human tissues and some human mammary carcinoma cell lines have HER4 transcripts [71]. Like HER3, HER4 might have prognostic significance in combination with other recep-tors but when investigated on its own it seems not to be overexpressed in HNSCC [72].

15
VectorsTargeting vectors are often antibodies or antibody derivatives. Antibodies are multichain proteins composed of two identical glycosylated heavy chains, and two identical light chains. Together they form a Y-shaped struc-ture stabilized by disulfide bonds. The antigen-binding site of an antibody consists of the complementarity determining regions (CDR’s). These are hypervariable loops that define to what and how firm the binding will be. For a schematic picture of an IgG antibody and its derivatives, see Figure 2.
Several types of antibody fragments are also used for targeting. By keep-ing the CDR’s but reducing the size (by enzymatic digestion or genetic engi-neering), a molecule targeting the same antigen, but with faster kinetics can be created. A fast clearance rate can be an advantage in RID, and the small size might improve tumour penetration. However, if a vector is smaller than 65 kDa (e.g. a diabody) it will be below the renal threshold. This instigates a shorter circulation time in the body, and may cause renal damage if residual-izing radioisotopes are used in RIT [73].
Figure 2. A schematic representation of an IgG antibody and some of its derivatives. Fab and F(ab’)2 fragments are produced by enzymatic degradation, whereas ScFv, (ScFv)2, diabodies and minibodies are produced by antibody engineering.
cMAb U36 An appropriate candidate for targeting HNSCC through CD44v6 may be the cMAb U36. This antibody specifically recognizes the CD44v6 antigen, and has been extensively studied in patients with primary HNSCC and lymph node metastases. Clinical biodistribution studies of both technetium-99m-labelled cMAb U36 and the humanized MAb BIWA 4 (bivatuzumab, also directed against CD44v6) evaluated by radioimmunoscintigraphy and by biopsy measurements in head and neck cancer patients showed abundant and selective antibody accumulation, both in primary tumours and in lymph node

16
metastases [36, 74]. Selective tumour accumulation in human HNSCC xeno-grafts in nude mice has been demonstrated for the 125I labelled cMAb U36, as well as for 131I and 186Re labelled MAb U36 [75-79]. Phase I dose escala-tion radioimmunotherapy studies with cMAb U36 and BIWA 4 using 186Reas the therapeutic radionuclide showed promising antitumour effects, with consistently stable disease at higher radioactivity dose levels [80-82]. Mye-lotoxicity (caused by circulating radioimmunoconjugate) and, in some pa-tients, mild oral mucositis was the only toxicity observed in the radioimmu-notherapy studies. In these studies, bivatuzumab seemed to have low immu-nogenicity.
In a recent study, the use of bivatuzumab mertansine was assessed in a phase I dose escalation study [83]. Bivatuzumab mertansine is a tumour-activated pro-drug conjugate, consisting of the supertoxic drug mertansine covalently linked to bivatuzumab. The main toxicity of bivatuzumab mer-tansine was directed against the skin, with most of the skin reactions being reversible. However, one fatal drug-related adverse event occurred, and it was concluded that the targeting of CD44v6 might not be selective enough for approaches in which supertoxic drugs like mertansine are used. Instead, a fundamentally different approach, such as radioimmunotherapy, would seem to be more promising, as the use of a radionuclide with a suitable half-life and energy can avoid the skin toxicity. As a matter of fact, no skin toxicity was observed in the 186Re radioimmunotherapy studies, whereas just a small proportion of patients experienced mucositis.
cMAb cetuximab The cMAb cetuximab recognizes the extracellular domain of human EGFR [84, 85]. The antibody potentially competes for receptor binding with EGF and other ligands, and inhibits tumour growth [19-23]. Cetuximab has been shown to inhibit EGFR tyrosine kinase activity and proliferation of EGFR-overexpressing squamous cell carcinoma cell lines, and synergy has been observed with doxorubicin, cisplatin and radiation in preclinical models. In phase I trials, major toxicity has been dermatological (rash and acneic skin reactions); allergic reactions have also been observed in about 3% of cases [86]. Extensive studies in head and neck cancer patients have been done, and a phase III study comparing cetuximab and cisplatin demonstrated higher response rates in the combination group, although the median survival time did not differ. In 2004, cetuximab received FDA approval for treatment of metastatic colorectal cancer [18].

17
Radiohalogens
Although the general strategies for therapy and diagnostics are alike, the choice of radionuclide depends upon what targeting concept is to be consid-ered. General factors such as decay half-life, type and energy spectrum of emitted radiation, cost and availability of the nuclide must be considered,and the nuclide must match the properties of the targeting vehicle.
Radiohalogens are attractive candidates in both RIT and RID, since they share many chemical properties, but possess a variety of half-lives and decay modes [87]. The same targeting molecule can be labelled by the same or a similar method, with a different halogen depending on the biomedical prob-lem to be solved. A -emitting halogen such as 123I can be used for initial detection of a tumour, whereas quantification of pharmacokinetics and do-simetry can be done using a positron-emitter such as 124I. For therapy, - or
-emitting halogens such as 131I or 211At can be applied.
Radiohalogens for therapy When choosing a suitable nuclide for RIT, factors such as properties of the conjugate, radiation, and size of the tumour that is to be targeted must be considered. Some radiohalogens of possible therapeutic interest are listed in Table 1.
If the conjugate is unable to penetrate the tumour completely, or if the an-tigen is heterogeneously distributed within the tumour, a -emitting nuclide is a suitable choice. The longer range of a -particle will cause radiation from one targeted cell to hit surrounding cells, so-called cross-fire irradia-tion. This way, there is no need to target every single tumour cell. On the other hand, the risk of irradiating adjacent healthy tissue will increase. A commonly used -emitting radiohalogen for therapy is 131I, due to its suitable half-life, availability and low cost. This nuclide is suitable for eradicating relatively small (104 – 106 cells) tumour clusters [24].
If the objective is to eradicate single tumour cells, or very small cell clus-ters (up to a few hundred cells), an -emitting nuclide might be preferred. Due to their short range, alpha particles deposit all their energy within a few cell diameters from the location of the decay, thus sparing surrounding healthy tissues. Moreover, the high LET (linear energy transfer) of alpha particles greatly increases the probability of double strand breaks and cell death to the targeted cell and its closest neighbours [88]. Among the alpha-emitting nuclides available, 211At has the most appropriate half-life (7.2h) for tumour targeting, and has been successfully coupled to antibodies in a num-ber of previous studies [88, 89].
Radionuclides that emit Auger electrons might be an alternative for eradi-cating single tumour cells. However, Auger electrons have a very short range

18
(in the nanometer range), and need to be located in the DNA molecule itself in order to be cytotoxic.
Table 1. Radiohalogens of interest for targeted radiotherapy
Radiohalogen Physical half-life Main therapeutic mode of decay Application
77Br 57 h Auger cascade Single tumour cells 82Br 35 h Low energy - Small cell clusters 123I 13 h Auger cascade Single tumour cells 125I 60 d Auger cascade Single tumour cells 131I 8 d Low energy - Small cell clusters 211At 7 h Single cells and small clusters
Radiohalogens for imaging When considering suitable nuclides for RID, it is important that the half-life of the nuclide is long enough to obtain an optimal tumour to background ratio. For an intact MAb, this generally takes between 2 to 4 days for a solid tumour [90]. A radiohalogen that can be used for RID is 124I, which has a suitable half-life of four days.
Besides the half-life, the mode of radionuclide decay must be considered in RID. Depending of what imaging technique is to be used, different radio-halogens can be utilized. For SPECT, a gamma emitter such as 123I can be used. For PET, positron emitters such as 18F (for small engineered antibody fragments), 76Br or 124I might be suitable choices (Table 2).
Table 2. Radiohalogens of interest for tumour imaging
Radiohalogen Physical half-life Emission Main application 18F 110 min Positron PET 76Br 16 h Positron, gamma PET 77Br 57 h Gamma SPECT 123I 13 h Gamma SPECT 124I 4 d Positron, gamma PET
Labelling When attaching the radionuclide to the antibody there are several aspects to consider. It is important that the labelling process does not harm factors such as affinity and immunocompetence of the antibody, but also that the labelled conjugate will have in vivo properties such as high tumour uptake and reten-tion of the label, and a rapid whole-body clearance of labelled catabolites. These properties can often be modified by choosing different direct or indi-rect labelling methods [87, 91-95].

19
Direct labelling A direct label creates a direct chemical bond between the amino-acid back-bone of the targeting agent (e.g. antibody) and the radionuclide. The halogen is oxidized to form a positively charged ion, using oxidants such as Chloramine T (CAT) [96] or iodogen [97]. This positively charged halogen ion then attacks the activated phenolic ring of the amino acid tyrosine in the protein, forming a stable covalent bond (Figure 1). Histidine, tryptophan and phenylalanine residues may also be halogenated, though to a lesser degree.
The direct CAT method is one of the standard halogenation methods and has many advantages; it is quick and simple, and often renders high labelling yields. However, there are disadvantages; the harsh oxidative conditions may damage the protein, and halogenated tyrosine residues in the CDR regions may destroy the immunoreactivity. It is therefore always important to inves-tigate any adverse effects from the labelling process when a new conjugate is produced.
Figure 3. Example of direct CAT radiohalogenation of an antibody. The nuclide is directly attached to the tyrosine residues of the antibody.
Indirect labelling
In indirect labelling, the radionuclide is not directly attached to the protein. Instead, it is first coupled to a linker molecule, and the linker is then con-nected to the protein (Figure 4). Generally, this provides milder labelling conditions for the protein, but is more time consuming and often generates lower yields. However, even if labelling conditions are milder, the immuno-reactivity can still be compromised if the potential conjugation sites (e.g. lysines) are in the CDR’s [98].
The use of an appropriate linker molecule is one way to influence the invivo properties of the targeting molecule towards high radioactivity retention time in the tumour, as well as a rapid whole-body clearance of labelled cata-

20
bolites. In this respect, indirect labelling methods through linker molecules that use hydrophilic anchor molecules may provide an advantage in com-parison with directly tyrosine labelled compounds [99-104].
Figure 4. Example of indirect radiohalogenation via the PIB linker. The nuclide is connected to the antibody via the linker, to the lysine residues of the antibody.
The complete design of the targeting conjugate To conclude, the complete design of a targeting conjugate is a complex task, depending on various biochemical, physical and clinical factors. The target-ing agent should have suitable transport and stability properties in vivo. Fac-tors such as tumour penetration, internalization, catabolism, cross-reactivity, and possible side effects of the targeting agent must also be considered. The radionuclide must have suitable decay, half-life and biodistribution, and it should also be cost effective and readily available. The labelling method chosen must be efficient and create a stable label in vivo with suitable degra-dation products, and it must not compromise the specificity, immunoreactiv-ity or affinity of the targeting agent.
While designing the targeting conjugate, the properties of the targeted an-tigen and tumour must also be kept in mind. The antigen should be abun-dantly expressed in the tumour, and more sparsely in healthy tissue. It should preferably be present or upregulated in corresponding metastases, and should not be shed into circulation. Moreover, tumour size, type of malignancy, tumour location, vascularization, and the tumour’s interstitial pressure are also important factors in the tumour uptake of the radioimmunoconjugate.

21
Aim
The aim of this thesis was to investigate radioimmunotargeting in head and neck cancer, particularly as regards squamous cell carcinoma. This was to be done by first identifying suitable tumour target antigens in HNSCC. A pos-sible targeting vehicle to reach these structures was then to be identified and evaluated. Finally, the possibility of labelling this vector with radiohalogens was to be assessed, and utilized for applications in RIT and RID for head and neck cancer.

22
The present study
Molecular targets in HNSCC (papers I & II) IHC studies In paper I, immunostaining of the EGFR family was performed in 19 cases of metastatic SCC of the oral cavity and tongue base. Examples of immu-nostainings are shown in Figure 5.
Generally speaking, EGFR had a similar and high expression in both pri-mary tumours and the corresponding metastases, whereas the expression in healthy epithelium was less pronounced. HER2 was not expressed to the same extent as EGFR. However, when HER2 was abundantly expressed, it was in most cases expressed to the same extent and intensity in the primary tumours, metastases, and normal epithelium. The expression of HER3 and HER4 varied, and was mainly cytoplasmic in all cases studied. No overex-pression of HER3 and HER4 was evident in tumours when compared with healthy epithelium.
Figure 5. Examples of immunostaining in tumours. A) EGFR; extent 3, intensity 3. B) HER2; extent 3, intensity 1. C) HER3; extent 3, intensity 3. D) HER4; extent 3, intensity 2.

23
In paper II, immunostaining of EGFR and CD44v6 was performed in eleven samples from HNSCC patients, and in two healthy samples from uvula and soft palate. Ten of the tumour samples were from primary tumours, and one from a lymph node metastasis from an occult primary tumour (see Table 1).
IHC scores from paper II are summarized in Table 2. CD44v6 expression was identified in all tumour samples except one, and EGFR staining was identified in all tumour samples. The uvula samples were only stained in basal cell layers. Intensity and extent of staining was similar for both recep-tors.
Table 1. Site, histological grade of differentiation, stage, and previous radiation therapy of the 11 collected patient tumour samples
Tumoursample
Site Histological grade ofdifferentiation
Stage* Previous radiation therapy
1 Tongue Moderate-poor T3N0M0 2 Gingiva Moderate T4N0M0 70 Gy 3 Lymph node Poor TxN2M0 50 Gy 4 Facial skin Moderate T2N0M0 5 Tongue High T2N0M0 6 Bucca Moderate T4N2M0 7 Tongue Moderate T2N0M0 8 Tongue High T1N0M0 9 Tongue Moderate T3N0M0 70 Gy 10 Gingiva Poor/high T4N0M0 11 Gingiva Moderate T4N2M0
*Tumour staging was T1 (n=1), T2 (n=3), T3 (n=2), T4 (n=4) and Tx (n=1) (UICC, TNM Classification of Malignant Tumours, sixth edition).
Table 2. Immunohistochemistry scores for CD44v6 and EGFR stainings CD44v6 EGFR Tissue
sampleaIntensityb Extentc Intensityb Extentc
1 2 3 2 2 2 2 2 2 2 3 3 2 3 2 4 2 1.5 2 2 5 2 3 2 2 6 0 0 2 3 7 2 3 2 3 8 1.5 2 2 1 9 3 3 2 2 10 2 3 2 3 11 2 3 2 3 U a 2 1 1 1 U b 2 1 0 0 a: Tumour samples 1-11, U=uvula samples a and b. b: Intensity was judged from 0-3 (0: nega-tive; 1: weak; 2: moderate (same as epithelia); 3: intense. c: Extent was judged from 0-3 (0: negative; 1: < ; 2: - ; 3: > ).

24
Quantitative studies
In order to obtain quantitative data of expression, a single-dose (SD) radio-immunoassay was validated and applied to the samples in paper II, using 125I-labelled cMAb U36 and cMAb cetuximab. Results from SD assays of CD44v6 and EGFR expression in patient tissue samples are shown in Figure 6. The amount of CD44v6 was generally greater than the amount of EGFR, and average antigen density was generally more pronounced in the tumour specimens than in the two uvula samples studied.
The quantity of CD44v6 binding sites was estimated to generally range between 6 and 20 nmol antigen binding sites per g cell membrane in the tumour samples, with an average of 10.8 nmol/ g cell membrane. By esti-mating a relationship between g cell membrane and number of HNSCC cells, this value was found to correspond to approximately 700,000 antigens per cell. One tumour (number six) deviated in both tissue consistency and CD44v6 expression, with an average of only 0.2 nmol/ g cell membrane. In the uvula tissue studied, the overall expression was approximately one third of the average CD44v6 expression in tumour tissue.
For EGFR, expression was even lower, ranging between 0.6 and 2.3 nmol/ g cell membrane in the tumour samples, with a mean of 1.4 nmol/ gcell membrane (corresponding to 90,000 receptors per cell). Expression in the two uvula tissues was 0.2 - 0.3 nmol/ g cell membrane.
Figure 6. Antigen quantification using the SD assay in HNSCC tumours (1 - 11) and two normal uvula samples (UA and UB) for CD44v6 using 125I-cMAb U36 (shaded bars) and EGFR using 125I-cMAb cetuximab (white bars). Error bars represent stan-dard deviation. * = not done for EGFR. N = 3.
Comments In papers I and II, the EGFR family and CD44v6 antigen expression was assessed in HNSCC in order to find suitable radioimmunotargeting struc-

25
tures. HER2 was found to be expressed to a low extent, and did therefore not seem to be a suitable target. HER3 and HER4 were on the other hand more strongly expressed, but appeared to be localized chiefly in the cytoplasm. This is in line with other studies, where IHC stainings have observed mainly cytoplasmic staining of these two receptors [61, 67, 71, 105]. Thus, HER3 and HER4 might be unsuitable targets for immunotherapy in HNSCC. How-ever, despite the cytoplasmic distribution of the immunostainings, it remains to be determined if small subsets of the receptors are localised in the cellular membrane.
The EGFR appeared to be the most promising target from the EGFR fam-ily, demonstrating mostly membrane associated expression, and with similar expression in primary tumours and corresponding lymph node metastases. However, EGF receptors are also present to a large extent in the hepatocytes of the liver [48, 49]. This limits the use of the EGF receptors as targets in systemic radioimmunotherapy. Nevertheless, for HNSCC it could be of in-terest for imaging or in local therapeutic modalities. Another application could be to use an anti-EGFR antibody like cetuximab, which has an anti-tumour effect on its own, in combination with a radiolabelled antibody to-wards a different target antigen (see ongoing and future studies).
CD44v6 expression was demonstrated by IHC to be strongly and homo-geneously expressed in HNSCC, and might therefore be a suitable target. The quantitative SD assay verified this, and revealed that the average density of CD44v6 binding sites was almost ten times higher than that of EGFR. Thus, CD44v6 seemed to be the most suitable molecular target for radioim-munotargeting of HNSCC.
The expression of different antigens in HNSCC was first assessed by means of IHC. This is a semi-quantitative technique suitable for profiling the expression of antigens in tumour and normal material, but would in some cases benefit from being complemented with other techniques. For targeted therapy, it would be useful to not only know if a target antigen is “strongly” expressed in a tissue, but also to learn a quantitative value of how many an-tigens that are generally expressed in that tissue. We therefore developed a quantitative assay, the SD assay, and applied it to the samples in paper II.
When comparing the IHC stainings in CD44v6 vs. EGFR, intensity ap-peared equally strong. However, this does not mean that the antigen density must be similar for the two antigens. Indeed, the SD analyses demonstrated that there was a tenfold difference in expression between the two antigens. The “false” impression from IHC is however not surprising, as IHC staining intensity is regulated by a number of factors other than antigen concentra-tion, and even different antibodies directed towards the same site can give different intensities in staining [33-35]. This illustrates the value of combin-ing IHC with another method when analysing antigen expression. Further-more, by combining the results from IHC stainings to SD analyses, informa-tion on antigen heterogeneity could be complemented with quantitative val-
26
ues of antigen expression, facilitating antigen profiling and comparisons between antigens. Complementing with IHC is also important as the SD assay does not distinguish between tumour and stroma cells. Therefore, the quantity of antigens may be underestimated if this is not taken into account.
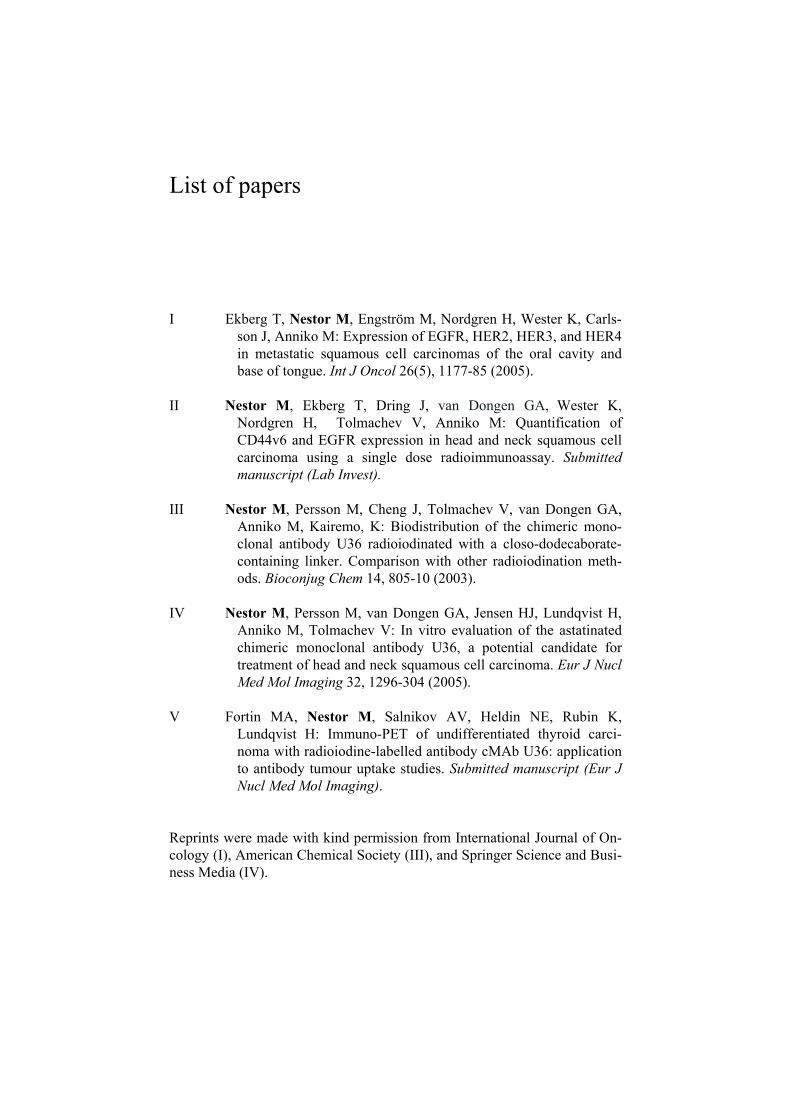
Suitable radiohalogen labelling methods (paper III) In paper III, the RIT / RID potential of the anti-CD44v6 cMAb U36 was assessed by evaluating three different radiohalogenation methods of the anti-body (Figure 7). The antibody was either iodinated directly using CAT (125I-cMAb U36), or indirectly by using the DABI or PIB linkers (125I-DABI-cMAb and 125I-PIB-cMAb U36 respectively). The three conjugates were first evaluated for their specificity and affinity in vitro, and then for their biodis-tribution patterns in normal mice.
Figure 7. Structures of the three different 125I-antibody conjugates used. In the di-rectly (CAT) labelled antibody (a), the 125I is attached directly to the tyrosine resi-dues of the antibody. In the indirectly PIB-labelled conjugate (b), the 125I is con-nected to the antibody via the PIB linker molecule to the lysine residues of the anti-body. In the case of the indirectly DABI-labelled conjugate (c), the 125I is attached via the DABI linker molecule to the lysine residues of the antibody.
All of the three differently radioiodinated cMAb U36 conjugates displayed high specific binding and similar affinities, but different biodistribution pat-terns. The 125I-DABI-cMAb conjugate demonstrated a radioactivity uptake in liver and spleen that was higher than the other two conjugates. The in vivodata also pointed out a 10 times higher radioactivity accumulation in thyroid for the directly labelled conjugate 96 h p.i. compared to the 125I-PIB-cMAb U36 and 125I-DABI-cMAb U36 conjugates, that showed a consistently sparse thyroid uptake (Figure 8).

27
Figure 8. Comparison of the radioactivity distribution of 125I-cMAb U36 (- -X- -), 125I-DABI-cMAb U36 ( ) and 125I-PIB-cMAb U36 ( ) in blood, liver, spleen and thyroid. Animals were sacrificed at 1.5, 6, 24 and 96 hours after injec-tion. The unit % ID/g refers to the activity expressed as a percentage of injected dose per gram of tissue. Significant differences (P < 0.05) could be observed at the 1½ and 96 h time points in liver and spleen, and the 96 h time point in blood, where the DABI conjugate displayed higher radioactivity values. In thyroid, the directly la-belled conjugate displayed significantly higher values than the indirectly labelled conjugates at the 24 and 96 h time points. Error bars represent standard deviations. N = 4.
Comments In this paper, a comparative investigation of three radiohalogenation meth-ods of the cMAb U36 was conducted. The data obtained in vitro showed antigen-specific binding and minor differences in affinity for all conjugates, demonstrating that all three radiohalogenation methods could be applied without damaging the antibody. This does however not mean that the conju-gates behave identically in the body. Indeed, the in vivo studies demonstrated different metabolic pathways and possibly different in vivo stability of the conjugates.
The in vivo data pointed out a tenfold greater accumulation in thyroid for the directly labelled conjugate 96 h p.i. This is consistent with a number of studies where direct radioiodination (using CAT) caused greater accumula-tion of radioactivity in thyroid than did indirect labelling using derivatives of

28
benzoic acid [99-103]. Since the thyroid is known to accumulate free ra-dioiodide, this could indicate a different catabolic pathway for the directly labelled conjugate. It has also been hypothesised that the lesser uptake of radiolabel in thyroid for the indirectly labelled compounds via benzoic de-rivatives is due to rapid urinary excretion of the intracellular catabolic prod-ucts. This quick excretion may prevent further in vivo transformation of the catabolites and the release of free halide, resulting in a lower thyroid uptake [103, 104]. The modest thyroid uptake for the indirectly labelled conjugates may favour the use of these in future studies when the tumour target is in the neck area. The uptake in thyroid will complicate diagnosis if the tumour uptake cannot be distinguished from the thyroid uptake, and dose planning for RIT may be impossible. If instead the thyroid uptake is low, medication to block radionuclide uptake can be avoided, and the RIT process simplified. Also, the risk of causing hypothyroidism in the patient can be reduced.
The in vivo data also demonstrated a greater concentration of radiolabel from 125I-DABI-cMAb U36 in liver and spleen than of the other conjugates. This increase might raise some concern about the use of this conjugate. However, this higher level could indicate residualization of the DABI linker, and future studies will have to assess if the amount of residualization ob-tained in tumours outweighs any disadvantage of increased uptake in liver and spleen.
This study demonstrates how the proper linker molecule will provide ad-ditional opportunities to further improve the properties of an antibody-radionuclide conjugate. For a fast and simple labelling method with high yield, but also accumulation in thyroid, the direct CAT method can be used. For lower thyroid uptake, the PIB linker is suitable. For possible longer tu-mour radioactivity retention time, low thyroid uptake, but higher amounts in liver and spleen, the DABI linker can be chosen. The future choice of radio-halogenation method for cMAb U36 should therefore be chosen depending on what conjugate properties are needed for the specific study.
Radiohalogenated cMAb U36 for therapy (paper IV) 211At-cMAb U36 and 131I-cMAb U36 In paper IV, the potential of cMAb U36 labelled with the therapeutically interesting radiohalogens 211At and 131I was assessed in vitro. cMAb U36 was labelled with 211At via the PAB linker, an astatine analogue to the PIB linker used in paper III. The quality of the conjugate was extensively evalu-ated for binding and internalization capacities, and compared with 125I-cMAbU36. The cellular toxicity of the astatinated conjugate was then assessed in two types of in vitro cell toxicity assays and compared with directly 131I-labelled cMAb U36.

29
Comparisons between 211At-cMAb U36 and 125I-cMAb U36 demonstrated no adverse effects of astatination of the antibody. Clonogenic survival (Fig-ure 9) and cell growth assays (Figure 10) with 211At-cMAb U36 were in ex-cellent agreement, demonstrating a dose-dependent and antigen-specific cellular toxicity for 211At-cMAb U36, with about 10% cell survival at 50 decays per cell. This toxicity was shown to be dependent on MAb-antigen interaction, rather than on free astatine in the medium, since blocking of the antigen radically improved the survival of the cells.
Figure 9. Clonogenic survival of SCC25 cells submitted to one of the following conditions. Control: no astatinated conjugate added. Unlabelled MAb: 46 µg unla-belled cMAb U36 was added in order to assess any cell inactivation effect of unla-belled antibody. 12 DPC: 92 ng 211At-cMAb U36 conjugate was added, correspond-ing to an average of 12 decays per cell (DPC). 50 DPC: 460 ng 211At-cMAb U36 conjugate was added corresponding to an average of 50 DPC. Block: 460 ng 211At-cMAb U36 conjugate was added together with a 100-fold excess (46 µg) of unla-belled antibody. 131I 55 DPC: 92 ng 131I cMAb U36 corresponding to an average of at least 55 DPC was added. Samples marked with (*) differed significantly (P < 0.05) from the control. The data has been normalized by correlating to control growth. Error bars represent standard error of mean (N = 3).
The cellular toxicity of 211At and 131I conjugates was first compared in a clonogenic survival assay (Figure 9) by exposing the cells to similar amounts of decays per cell (55 vs. 50 DPC for the iodinated and astatinated conjugate respectively) and comparing cell survival. Cells exposed to the beta-emitter 131I displayed a surviving fraction four-fold higher than the alpha-emitting astatinated conjugate (51 ± 2% vs. 13 ± 1.5%). Secondly, comparison of the two conjugates in a cell growth assay (Figure 10) demonstrated that twice the amount of decays per cell of 131I-cMAb U36 was needed to achieve a
30
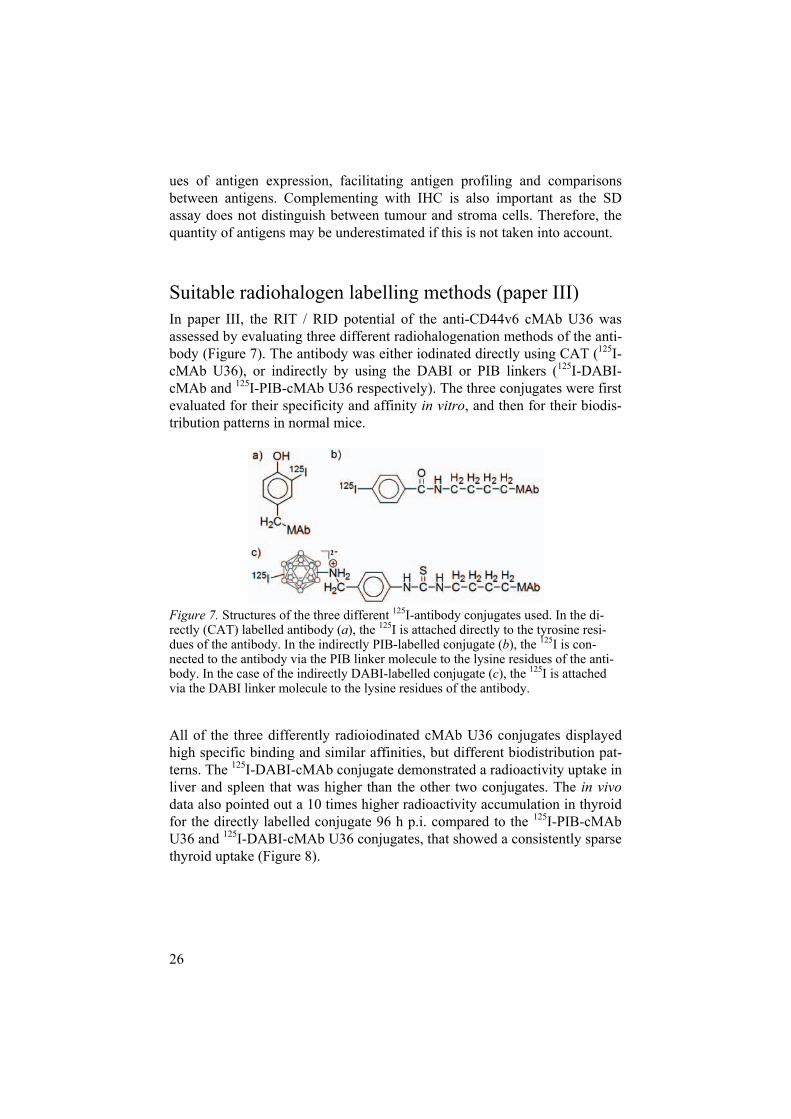
comparable anti-tumour efficacy to the astatinated conjugate (55 DPC from 131I cMAb U36 resulted in a 50 ± 7% survival, whereas 21 DPC from 211AtcMAb U36 was sufficient to achieve a survival of 55 ± 13%).
Figure 10. Cell growth assay of SCC25 cells submitted to one of the following con-ditions. No antibody added ( O ); 37 ng 211At-cMAb U36 corresponding to an average of 64 decays per cell (DPC) was added (-- --); 105 ng 211At-cMAb U36 corresponding to an average of 21 DPC was added (··· ···); 105 ng 211At-cMAb U36 was added to the cell dishes, as well as a 100-fold molar excess of non-labelled antibody ( ); 92 ng 131I cMAb U36 corresponding to an average of at least 55 DPC was added ( * ). The data has been normalized by correlating to control growth. Error bars represent standard error of mean (N = 3).
Comments In this paper, the potential of therapeutic cMAb U36 conjugates was evalu-ated in vitro, using the radiohalogens 211At and 131I as therapeutic nuclides. Even if the half-life of 211At (7.2h) is not optimal for an antibody, we chose this nuclide as alpha emitters such as 211At might be especially suitable for eradicating minimal residual disease in HNSCC [24]. Among the alpha-emitting nuclides available, 211At had the most appropriate half-life for tu-mour targeting, and has been successfully coupled to antibodies in a number of previous studies [88, 89].
The 211At-cMAb U36 appeared to be the more promising of the two RIT conjugates for eradicating single tumour cells in these studies. Since the long

31
blood clearance time of the antibody and the relatively short half-life of 211Atis not an optimal combination, an anti CD44v6 antibody fragment with faster blood clearance time could be an interesting option for future astatine stud-ies. However, the short range of the alpha particle might be a concern for possible skin toxicity [83], and this needs to be further evaluated. Eventhough the 131I-cMAb U36 conjugate seemed inferior to the astatinated con-jugate in the monolayer setting, this conjugate might be well suited for rela-tively small (104 – 106 cells) tumour clusters, thus facilitating the longer range of the beta particles. Furthermore, the longer half-life (8 days), lower cost, and greater availability of 131I might be factors furthering the choice of 131I-cMAb U36 as a therapeutic conjugate.
There are several factors that need to be taken into account when compar-ing 211At- and 131I-labelled cMAb U36. Since different labelling methods were used for the two conjugates, it is necessary to consider whether this may have contributed to the results. The two labelling methods used (indi-rect PAB labelling and direct CAT labelling) have previously been com-pared in vitro using 125I, and no major differences were identified in affinity, immunoreactivity, cellular uptake, retention or internalisation [106]. These properties are important, as they influence the number of decays received per cell, and subsequently the dose received per cell. However, since the DPC estimation is based on measurements of the conjugates specifically bound to the cells, any damaged conjugates would not influence these data.
Another factor to consider when comparing the two conjugates is the pos-sible underestimation of the average amount of decays per cell given to cells by 131I-cMAb U36, since any influence from non-specific irradiation was not taken into account. The energy of the beta particles emitted is distributed within a range of about a millimetre, and unbound 131I-cMAb U36 in the medium might contribute to the irradiation of cells. Also, the longer half-life of 131I might give an additional dose to the cell if the CD44v6 epitope (and consequently also the bound labelled conjugate) has not been completely cleaved off by the trypsinization after 24h incubation. Therefore, the average number of decays per cell given by 131I-cMAb U36 was designated as “at least” 55 DPC.

32
Radiohalogenated cMAb U36 for imaging (paper V) 124I-cMAb U36 In paper V, the potential of cMAb U36 labelled with the radiohalogen 124Ifor visualizing human anaplastic thyroid carcinoma with PET was assessed. This was done by first characterizing the thyroid carcinoma cell line KAT-4, and the effects of 124I labelling on cMAb U36 in vitro. Biodistribution and PET studies were then performed on mice bearing KAT-4 carcinoma.
The in vitro studies demonstrated that cultured human undifferenti-ated/anaplastic thyroid carcinoma KAT-4 cells expressed low levels of Na+/I-
symporter (NIS) and uptake of free iodine was insignificant. The 124I labelled cMAb U36 expressed an affinity (KD) of 11 ± 2 nM and good specificity for KAT-4 cells.
Results in selected organs from the biodistribution study of 124I-cMAb U36 (or free 124I as a comparison) can be seen in Figure 11. After injection of 124I-cMAb U36, tumour radioactivity uptake results peaked at 48 hours post-injection (~21 %I.A./g). Blood retention values were 16.0%, 13.0%, and 8.9% (%I.A./g) after 24, 48 and 72 hours respectively.
Figure 11. Radioactivity distribution of 124I and 124I-cMAb U36 in selected organs. %IA/g: Percentage injected activity per gram. N = 3 (4h), 10 (24h), 8 (48h) and 12 (72h). Tumour values are averages from arm and flank tumours at the 24 - 72h time points. Error bars represent standard deviation.

33
In the PET study, tumour-bearing animals injected with 124I-cMAb U36 were scanned with a micro-PET system (Figure 12). PET studies were consistent with the results obtained from biodistribution studies, and all of the tumours could be clearly identified in 124I-immuno-PET pictures.
Figure 12. PET images of nude mice scanned 24, 48 and 72 hours after injection of 124I-cMAb U36 (4 MBq, 100 g). Mice were injected with 124I-cMAb U36 (100 gand 4 MBq per animal). The pictures were normalized to the detected activity in the cardiac blood pool. Transaxial planes show tumours in (a) the arm and (b) the flank. Tumours are indicated by arrowheads. The animals represented at 24 and 48 hours are the same. Tumour weights: untreated 24h, 48h (a: 0.21 g ; b: 0.35 g), 72h (b: 0.09 g). H heart, T thyroid.
Comments Due to the slow kinetics of MAbs, radiolabelling for radioimmuno-PET gen-erally has to be performed with a positron emitter that allows follow-up stud-ies to more than 72 hours post-injection. This time is needed to achieve op-timal tumour to non-tumour ratios with antibodies injected in the blood. One of few radionuclide options for this purpose is 124I, which nowadays is read-ily available at reasonable costs. Furthermore, the methods by which halo-gens can be coupled to monoclonal antibodies are relatively easy and well established, and the use of 124I in radioimmuno-PET allows paired studies with other radioisotopes of iodine.
However, using iodine to label MAbs for targeting thyroid carcinoma in patients raises questions related to the presence of the NIS symporter, which is an integral plasma membrane glycoprotein that mediates active I- transport into the thyroid follicular cells. As a result, uncoupled 124I can be accumu-

34
lated in the thyroid. NIS also mediates I- transport in other tissues, including salivary glands, gastric mucosa, and lactary mammary glands [107]. Using iodine labelled MAbs would then complicate the differentiation between free radioiodine and specifically bound radioiodine-MAbs if the conjugate is not sufficiently stable in vivo.
In paper III, we demonstrated that some indirect labelling methods re-sulted in low uptake of iodine in the thyroid, possibly indicating a more sta-ble conjugate. This might be something to consider when further developing this conjugate for diagnostic use. Also, for high radionuclide concentrations (about 100 MBq/ml), which would be necessary in the establishment of clinical radioimmunodiagnostic/radioimmunotherapeutic procedures, 124I-radioiodine solutions are susceptible to radiation-induced formations of 124I-oxoiodocomplexes with anionic Lewis bases, leading to a rapid decrease in labeling yields (as low as 18% obtained with the iodogen method). There-fore, chemical restoration of the deteriorated radionuclide would also be a critical step prior to radiolabelling for clinical use [108].
In our study, we chose to use the direct CAT radiolabelling method. This was to guarantee high labelling yields in a short time span, while maintain-ing the affinity and specificity of the antibody for CD44v6 antigens [106]. Chemical restoration of the deteriorated radionuclide was not necessary in our studies, since only 4 MBq was injected per animal, and this allowed us to use radionuclide solutions containing lower radioactivity concentrations (370 MBq/ml) in the labelling procedures. Furthermore, no labelling was performed later than 6 days after the date of delivery.
Anaplastic thyroid carcinoma, the most aggressive and lethal form of thy-roid cancer, is generally associated with poor iodine uptake. Consequently, diagnosis and treatment of this form must follow other strategies than those based on the uptake of intravascularly injected radioiodine. By performing studies using 124I-cMAb U36 on mice bearing thyroid anaplastic carcinoma, we could demonstrate that CD44v6 may be a suitable target for this form of thyroid lesion. We also demonstrated that cMAb U36 could be used to suc-cessfully target this tumour model in vivo. Furthermore, by using 124I-cMAbU36 in this system, 100% of the tumours could be visualized with a micro-PET system, demonstrating the promising possibility for this conjugate in RID. Since this antibody has previously been successfully labelled with 131I,RIT using 131I-cMAb U36 in this tumour type could also be a future treat-ment possibility.

35
Conclusions
Finally, antibodies seem to be fulfilling decades of expectations as antican-cer treatments. Monoclonal antibodies now constitute the majority of recom-binant proteins currently in the clinic, and there is no doubt that this new modality may play an increasingly important role in clinical medicine and expanding patient treatment options. In HNSCC, the idea of radioimmuno-targeting is particularly appealing, as the advanced stages have a large frac-tion of spread disease that is difficult to treat with procedures available to-day.
In this work, we have investigated the possibility for radioimmunotarget-ing in head and neck cancer. This was done by first assessing possible target structures for HNSCC, and exploring the possibility of radiohalogenating the anti CD44v6 cMAb U36. The cMAb U36 labelled with 211At and 131I was then preclinically evaluated for therapeutic use. Finally, the cMAb U36 was evaluated for RID use in thyroid anaplastic carcinoma, using 124I as the diag-nostic nuclide.
Conclusions that can be drawn: CD44v6 is a suitable molecular target for radioimmunotargeting in HNSCCThe single dose assay is a valuable quantitative complement to IHC for analysis of target antigens cMAb U36 can be radiohalogenated with 125I both directly and indirectly, with no adverse effects from labelling, but resulting in different biodis-tributions for the conjugates. Directly CAT-labelling is a fast and simple method, resulting in high yield and specific activity, but radioiodine accumulates in thyroid after the use of directly radioiodinated cMAb U36. For lower thyroid uptake, the PIB linker is suitable for radioiodination of this antibody.For possible longer tumour radioactivity retention time, and low thyroid uptake, the DABI linker can be chosen to indirectly radiohalogenate cMAb U36. However, this can result in higher radioactivity accumulation in the liver and spleen. cMAb U36 can be successfully labelled with the therapeutically interest-ing radiohalogens 211At and 131I

36
Astatinated cMAb U36 demonstrates a specific and dose dependent cyto-toxicity, superior to that of the iodinated conjugate in the monolayer set-tingcMAb U36 can be successfully labelled with 124ICD44v6 may also be a suitable target antigen for radioimmunotargeting in anaplastic thyroid carcinoma 124I-cMAb U36 is a promising conjugate for RID
These results demonstrate how antibody-based targeting techniques can pro-vide more sensitive and specific methods for identifying and treating head and neck cancer, and hopefully help improve long-term survival rates for this patient group in the future.

37
Ongoing and future studies
Receptor quantification studies In paper II, we validated the quantitative SD assay, and applied it on a select number of samples. However, we refrained from carrying out any analyses of antigen expression with respect to histological grade etc, as we felt that the limited number of samples would not provide statistically reliable infor-mation.
In future studies, we aim to quantify CD44v6, EGFR, and possibly HER2 expression, in HNSCC on a larger scale. Since HNSCC is often accessible for biopsies, we aim to utilize the SD assay on biopsy samples, and evaluate antigen expression in relation to e.g. histological grade of differentiation, stage, previous radiation therapy, and in relation to healthy tissue.
Cocktail studies with cetuximab Since MAbs directed against EGFR have been shown to effectively enhance the efficacy of chemotherapy [109-111], an appealing idea is to combine radiolabelled cMAb U36 with an anti-EGFR antibody. RIT studies on HNSCC xenografts have shown that the combination of 186Re-labelled cMAb U36 with anti-EGFR MAb 425 (cetuximab) enhanced the therapeutic efficacy [78], and e.g. 211At-cMAb U36 and cetuximab might therefore be an attractive combination.
We intend to investigate if the therapeutic ratio of halogen-labelled cMAb U36 can be improved by combining it with cetuximab. So far, we have stud-ied the effects of the combination in human tumour cell culture experiments, assessing antibody processing in the cell (retention, internalization, etc), and cytotoxic effects of the combination (clonogenic survival, growth inhibition studies, etc).
In future studies, we aim to study biodistribution and therapeutic efficacy of the combination in tumour-bearing mice.

38
Radiometal-labelled cMAb U36 In this thesis, we have concentrated on radiohalogens as therapeutic and diagnostic radionuclides. An alternative to radiohalogens could be radi-ometals. Radiometals usually have a comparably longer intracellular reten-tion than halogens, probably due to the formation of charged radiocatabolites that have difficulty in penetrating the cell membrane. A radiometal com-monly used for imaging is 111In, and an 111In-cMAb U36 conjugate might be suitable for RID in HNSCC using planar gamma camera and SPECT. The low-energy beta emitter 177Lu labelled to cMAb U36, using the same chela-tor system, could be a suitable conjugate for RIT in small metastases, with a short range of emitted particles, and a suitable half-life.
So far, we have performed a pilot study in vitro, investigating the use of the linker CHX-A’’-DTPA for labelling the antibody cMAb U36 with 177Luand 111In. Properties such as labelling yield, specificity, affinity, and cellular uptake of the conjugate were investigated in a HNSCC cell line. Results showed that the antibody can be labelled with these two radiometals with a good yield, and retained specificity, cellular binding, and high affinity and immunoreactivity of the conjugate.
In future studies, biodistribution, dosimetry, imaging (111In-cMAb U36) and anti-tumour effects (177Lu-cMAb U36) of the conjugates will be assessed in vivo. Finally, we intend to test the 111In-cMAb U36 conjugate for clinical diagnosis.

39
Acknowledgements
This thesis has been the result of a collaboration between the Division of Otolaryngology and Head and Neck Surgery, and the Division of Biomedical Radiation Sciences at Uppsala University. I would like to thank all my col-leagues, and would especially like to express my sincere gratitude to the following people:
My main supervisor, Professor Matti Anniko. Thank you for your unfailing trust and support. Your knowledge, determination and drive have been a real inspiration to me!
My co-supervisors: Assistant Professor Vladimir Tolmachev. Thank you for knowing every-
thing there is to know about radiochemistry, and for trying to teach me some of it. It has been a real privilege to work with you.
Professor Hans Lundqvist. Thank you for your help with the astatine ex-periments, and for everything else revolving radiation physics.
Professor Jörgen Carlsson. Thank you for sharing your vast knowledge of radiation science and music with me! Thank you also for creating such a wonderful work atmosphere at BMS.
All my co-authors, without you there would have been no thesis! I would especially like to thank:
Professor Guus van Dongen; your help has been invaluable. You have always gone to great lengths to help out, even though I know you’ve been very busy with your own research. The articles would not have been half as good without your help and insightful advices.
Tomas Engström; thank you for great help with both practical and theo-retical tasks, and for being a great link to the clinic.
Mikael Vikström; for always lending a helping hand, whether it was for labwork, writing, HGK, computer help, or boxing.
Marc Fortin; thank you for a great cooperation, for your patience with us strange Swedish people, and for keeping track of all those protocols…
Junping Cheng; thank you for your help with the animal experiments. Kalevi Kairemo; thank you for your help in getting this project started.

40
Professor Karin Caldwell. You have been a true inspiration and role model to me. You were the one who made me realize how much fun research (and conferences!) can be in the first place.
Everyone who is or has been at BMS, for making it such a fantastic work-place! Thank you Erika and Lars, for taking me on as a thesis worker, Ve-ronika for taking care of absolutely everything, and Karin, Erika, Lina,Irina, Shirin, Amelie, Thuy, Kalle and all the rest of the past and present PhD-students for being such a great (film) crew! I would especially like to thank all the current and former members of the AmaZone, the greatest workroom ever, for countless discussions, advices, and lots of fun, particu-larly Åsa; provider of many laughs, entertaining stories, and great acting for the BMS-movies, Ann-Charlott; the BMS recruiter, event-planner, blind dog promoter, and scientific advisor who “spreads pleasure”, and Ylva (a.k.a.pluttis); the fun-loving, truth-speaking Oskar substitute!
Jag skulle också vilja tacka mina vänner som hittar på så mycket kul och visar att det finns ett liv utanför forskningen!
Sist men inte minst vill jag tacka hela min familj, framför allt: Mamma och pappa: Ni har gett mig en trygghet och ett självförtroende
som gränsar till megalomani… Bättre förutsättningar än er kärlek och tilltro till mig hade ingen kunnat få! Att ni dessutom gav mig sådana perfekta gener gjorde ju inte saken sämre… Ett extra tack till pappa som kämpade sig ige-nom avhandlingen och kom med många goda råd.
Min syster Sofia, som är världens smartaste och bästa syster, samt min blivande svåger Fredrik, vars humor och energi alltid får mig på gott humör.
Min sambo Oskar, som hänsynsfullt har stått ut med mina konstiga ar-betstider, och alltid lyckas göra mig glad!

41
References
1. Parkin, D.M., Global cancer statistics in the year 2000. Lancet On-col, 2001. 2(9): p. 533-43.
2. Parkin, D.M., et al., Estimating the world cancer burden: Globocan 2000. Int J Cancer, 2001. 94(2): p. 153-6.
3. Jemal, A., et al., Cancer statistics, 2002. CA Cancer J Clin, 2002. 52(1): p. 23-47.
4. Hoffman, H.T., et al., The National Cancer Data Base report on cancer of the head and neck. Arch Otolaryngol Head Neck Surg, 1998. 124(9): p. 951-62.
5. Alvi, A. and J.T. Johnson, Development of distant metastasis after treatment of advanced-stage head and neck cancer. Head Neck, 1997. 19(6): p. 500-5.
6. Pasieka, J.L., Anaplastic thyroid cancer. Curr Opin Oncol, 2003. 15(1): p. 78-83.
7. Khoo, M.L., et al., Thyroid calcification and its association with thyroid carcinoma. Head Neck, 2002. 24(7): p. 651-5.
8. Lo, C.Y., K.Y. Lam, and K.Y. Wan, Anaplastic carcinoma of the thyroid. Am J Surg, 1999. 177(4): p. 337-9.
9. Nilsson, O., et al., Anaplastic giant cell carcinoma of the thyroid gland: treatment and survival over a 25-year period. World J Surg, 1998. 22(7): p. 725-30.
10. Mazzaferri, E.L. and R.T. Kloos, Clinical review 128: Current ap-proaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab, 2001. 86(4): p. 1447-63.
11. Abraham, J. and C. Allegra, Bethesda handbook of clinical oncol-ogy, second edition. 2005, Philadelphia: Lippincott Williams & Wil-kins. xvii, 666 p.
12. Haisma, H., J. Hilgers, and V. Zurawski, Jr, Iodination of mono-clonal antibodies for diagnosis and radiotherapy using a convenient one vial method. J Nucl Med, 1986. 27(12): p. 1890-1895.
13. Chin, D., et al., Head and neck cancer: past, present and future.Expert Rev Anticancer Ther, 2006. 6(7): p. 1111-8.
14. Haigh, P.I., et al., Completely resected anaplastic thyroid carcinoma combined with adjuvant chemotherapy and irradiation is associated with prolonged survival. Cancer, 2001. 91(12): p. 2335-42.
15. Funaro, A., et al., Monoclonal antibodies and therapy of human cancers. Biotechnol Adv, 2000. 18(5): p. 385-401.
16. Carter, P., Improving the efficacy of antibody-based cancer thera-pies. Nat Rev Cancer, 2001. 1(2): p. 118-29.

42
17. Reff, M.E., K. Hariharan, and G. Braslawsky, Future of monoclonal antibodies in the treatment of hematologic malignancies. Cancer Control, 2002. 9(2): p. 152-66.
18. Stern, M. and R. Herrmann, Overview of monoclonal antibodies in cancer therapy: present and promise. Crit Rev Oncol Hematol, 2005. 54(1): p. 11-29.
19. Baselga, J., Targeting the epidermal growth factor receptor with tyrosine kinase inhibitors: small molecules, big hopes. J Clin Oncol, 2002. 20(9): p. 2217-9.
20. Herbst, R.S. and D.M. Shin, Monoclonal antibodies to target epi-dermal growth factor receptor-positive tumors: a new paradigm for cancer therapy. Cancer, 2002. 94(5): p. 1593-611.
21. Mendelsohn, J. and J. Baselga, The EGF receptor family as targets for cancer therapy. Oncogene, 2000. 19(56): p. 6550-65.
22. Baselga, J., Targeting the epidermal growth factor receptor: a clini-cal reality. J Clin Oncol, 2001. 19(18 Suppl): p. 41S-44S.
23. Arteaga, C.L., S.L. Moulder, and F.M. Yakes, HER (erbB) tyrosine kinase inhibitors in the treatment of breast cancer. Semin Oncol, 2002. 29(3 Suppl 11): p. 4-10.
24. Carlsson, J., et al., Tumour therapy with radionuclides: assessment of progress and problems. Radiother Oncol, 2003. 66(2): p. 107-17.
25. Potamianos, S., A.D. Varvarigou, and S.C. Archimandritis, Radio-immunoscintigraphy and radioimmunotherapy in cancer: principles and application. Anticancer Res, 2000. 20(2A): p. 925-48.
26. Heider, K.H., et al., CD44v6: a target for antibody-based cancer therapy. Cancer Immunol Immunother, 2004.
27. Brouwer, J., et al., Screening for distant metastases in patients with head and neck cancer: is there a role for (18)FDG-PET? Oral On-col, 2006. 42(3): p. 275-80.
28. Larson, S.M., Cancer or inflammation? A Holy Grail for nuclear medicine. J Nucl Med, 1994. 35(10): p. 1653-5.
29. DeGrado, T.R., et al., Synthesis and evaluation of (18)F-labeled choline analogs as oncologic PET tracers. J Nucl Med, 2001. 42(12): p. 1805-14.
30. Lee, F.T. and A.M. Scott, Immuno-PET for tumor targeting. J Nucl Med, 2003. 44(8): p. 1282-3.
31. Verel, I., G.W. Visser, and G.A. van Dongen, The promise of im-muno-PET in radioimmunotherapy. J Nucl Med, 2005. 46 Suppl 1:p. 164S-71S.
32. Tannock, I.F., et al., The Basic Science of Oncology. 4th ed, ed. M. Strauss and M. Watt. 2005, New Baskerville: Matrix Publishing Services. 592.
33. Montero, C., The antigen-antibody reaction in immunohistochemis-try. J Histochem Cytochem, 2003. 51(1): p. 1-4.
34. Moorghen, M., et al., Epidermal growth factor receptors in colorec-tal carcinoma. Anticancer Res, 1990. 10(3): p. 605-11.

43
35. Ohman, L., et al., A new antibody recognizing the vIII mutation of human epidermal growth factor receptor. Tumour Biol, 2002. 23(2): p. 61-9.
36. de Bree, R., et al., Radioimmunoscintigraphy and biodistribution of technetium-99m-labeled monoclonal antibody U36 in patients with head and neck cancer. Clin Cancer Res, 1995. 1(6): p. 591-8.
37. Dong, W.G., et al., Role of VEGF and CD44v6 in differentiating benign from malignant ascites. World J Gastroenterol, 2003. 9(11): p. 2596-600.
38. Bloor, B.K., et al., Characterization of CD44 splicing patterns in normal keratinocytes, dysplastic and squamous carcinoma cell lines.Int J Oncol, 2001. 18(5): p. 1053-9.
39. Terpe, H.J., et al., Expression of CD44 isoforms in renal cell tumors. Positive correlation to tumor differentiation. Am J Pathol, 1996. 148(2): p. 453-63.
40. Gunthert, U., et al., A new variant of glycoprotein CD44 confers metastatic potential to rat carcinoma cells. Cell, 1991. 65(1): p. 13-24.
41. Heider, K.H., et al., Characterization of a high-affinity monoclonal antibody specific for CD44v6 as candidate for immunotherapy of squamous cell carcinomas. Cancer Immunol Immunother, 1996. 43(4): p. 245-53.
42. Walker, R.A., The erbB/HER type 1 tyrosine kinase receptor family.J Pathol, 1998. 185(3): p. 234-5.
43. Peles, E., et al., Cell-type specific interaction of Neu differentiation factor (NDF/heregulin) with Neu/HER-2 suggests complex ligand-receptor relationships. Embo J, 1993. 12(3): p. 961-71.
44. Alimandi, M., et al., Cooperative signaling of ErbB3 and ErbB2 in neoplastic transformation and human mammary carcinomas. Onco-gene, 1995. 10(9): p. 1813-21.
45. Olayioye, M.A., et al., The ErbB signaling network: receptor het-erodimerization in development and cancer. Embo J, 2000. 19(13): p. 3159-67.
46. Rikimaru, K., et al., Gene amplification and overexpression of epi-dermal growth factor receptor in squamous cell carcinoma of the head and neck. Head Neck, 1992. 14(1): p. 8-13.
47. Santini, J., et al., Characterization, quantification, and potential clinical value of the epidermal growth factor receptor in head and neck squamous cell carcinomas. Head Neck, 1991. 13(2): p. 132-9.
48. Dunn, W.A., T.P. Connolly, and A.L. Hubbard, Receptor-mediatedendocytosis of epidermal growth factor by rat hepatocytes: receptor pathway. J Cell Biol, 1986. 102(1): p. 24-36.
49. Gladhaug, I.P., M. Refsnes, and T. Christoffersen, Regulation of surface expression of high-affinity receptors for epidermal growth factor (EGF) in hepatocytes by hormones, differentiating agents, and phorbol ester. Dig Dis Sci, 1992. 37(2): p. 233-9.

44
50. Yarden, Y. and M.X. Sliwkowski, Untangling the ErbB signalling network. Nat Rev Mol Cell Biol, 2001. 2(2): p. 127-37.
51. Yarden, Y., Biology of HER2 and its importance in breast cancer.Oncology, 2001. 61 Suppl 2: p. 1-13.
52. Craven, J.M., et al., Expression of c-erbB-2 gene in human head and neck carcinoma. Anticancer Res, 1992. 12(6B): p. 2273-6.
53. Xia, W., et al., Strong correlation between c-erbB-2 overexpression and overall survival of patients with oral squamous cell carcinoma.Clin Cancer Res, 1997. 3(1): p. 3-9.
54. Werkmeister, R., B. Brandt, and U. Joos, Clinical relevance of erbB-1 and -2 oncogenes in oral carcinomas. Oral Oncol, 2000. 36(1): p. 100-5.
55. Werkmeister, R., B. Brandt, and U. Joos, The erbB oncogenes as prognostic markers in oral squamous cell carcinomas. Am J Surg, 1996. 172(6): p. 681-3.
56. Xia, W., et al., Combination of EGFR, HER-2/neu, and HER-3 is a stronger predictor for the outcome of oral squamous cell carcinoma than any individual family members. Clin Cancer Res, 1999. 5(12):p. 4164-74.
57. Schiffer, I.B., et al., Switching off HER-2/neu in a tetracycline-controlled mouse tumor model leads to apoptosis and tumor-size-dependent remission. Cancer Res, 2003. 63(21): p. 7221-31.
58. Ross, J.S. and J.A. Fletcher, The HER-2/neu Oncogene in Breast Cancer: Prognostic Factor, Predictive Factor, and Target for Ther-apy. Oncologist, 1998. 3(4): p. 237-252.
59. Press, M.F., C. Cordon-Cardo, and D.J. Slamon, Expression of the HER-2/neu proto-oncogene in normal human adult and fetal tissues.Oncogene, 1990. 5(7): p. 953-62.
60. Natali, P.G., et al., Expression of the p185 encoded by HER2 onco-gene in normal and transformed human tissues. Int J Cancer, 1990. 45(3): p. 457-61.
61. Srinivasan, R., et al., Nuclear expression of the c-erbB-4/HER-4 growth factor receptor in invasive breast cancers. Cancer Res, 2000. 60(6): p. 1483-7.
62. P, O.c., et al., C-erbB receptors in squamous cell carcinomas of the head and neck: clinical significance and correlation with matrix metalloproteinases and vascular endothelial growth factors. Oral Oncol, 2002. 38(1): p. 73-80.
63. Shintani, S., et al., Prognostic significance of ERBB3 overexpression in oral squamous cell carcinoma. Cancer Lett, 1995. 95(1-2): p. 79-83.
64. Bei, R., et al., Co-localization of multiple ErbB receptors in strati-fied epithelium of oral squamous cell carcinoma. J Pathol, 2001. 195(3): p. 343-8.
65. Ibrahim, S.O., et al., Expression of c-erbB proto-oncogene family members in squamous cell carcinoma of the head and neck. Anti-cancer Res, 1997. 17(6D): p. 4539-46.
45
66. Prigent, S.A., et al., Expression of the c-erbB-3 protein in normal human adult and fetal tissues. Oncogene, 1992. 7(7): p. 1273-8.
67. Barnes, N.L., et al., Absence of HER4 expression predicts recur-rence of ductal carcinoma in situ of the breast. Clin Cancer Res, 2005. 11(6): p. 2163-8.
68. Tovey, S.M., et al., Outcome and human epidermal growth factor receptor (HER) 1-4 status in invasive breast carcinomas with prolif-eration indices evaluated by bromodeoxyuridine labelling. Breast Cancer Res, 2004. 6(3): p. R246-51.
69. Witton, C.J., et al., Expression of the HER1-4 family of receptor tyrosine kinases in breast cancer. J Pathol, 2003. 200(3): p. 290-7.
70. Kountourakis, P., et al., Prognostic significance of HER3 and HER4 protein expression in colorectal adenocarcinomas. BMC Cancer, 2006. 6: p. 46.
71. Plowman, G.D., et al., Ligand-specific activation of HER4/p180erbB4, a fourth member of the epidermal growth factor receptor family. Proc Natl Acad Sci U S A, 1993. 90(5): p. 1746-50.
72. Srinivasan, R., et al., Expression of the c-erbB-4/HER4 protein and mRNA in normal human fetal and adult tissues and in a survey of nine solid tumour types. J Pathol, 1998. 185(3): p. 236-45.
73. Adams, G.P., et al., A single treatment of yttrium-90-labeled CHX-A"-C6.5 diabody inhibits the growth of established human tumor xenografts in immunodeficient mice. Cancer Res, 2004. 64(17): p. 6200-6.
74. Stroomer, J.W., et al., Safety and biodistribution of 99mTechnetium-labeled anti-CD44v6 monoclonal antibody BIWA 1 in head and neck cancer patients. Clin Cancer Res, 2000. 6(8): p. 3046-55.
75. Vrouenraets, M.B., et al., Targeting of Aluminum (III) Phthalocya-nine Tetrasulfonate by Use of Internalizing Monoclonal Antibodies: Improved Efficacy in Photodynamic Therapy. Cancer Res, 2001. 61(5): p. 1970-1975.
76. Vrouenraets, M.B., et al., Targeting of a hydrophilic photosensitizer by use of internalizing monoclonal antibodies: A new possibility for use in photodynamic therapy. Int J Cancer, 2000. 88(1): p. 108-14.
77. Schrijvers, A.H., et al., MAb U36, a novel monoclonal antibody successful in immunotargeting of squamous cell carcinoma of the head and neck. Cancer Res, 1993. 53(18): p. 4383-90.
78. van Gog, F.B., et al., Perspectives of combined radioimmunotherapy and anti-EGFR antibody therapy for the treatment of residual head and neck cancer. Int J Cancer, 1998. 77(1): p. 13-8.
79. van Gog, F.B., et al., High dose rhenium-186-labeling of mono-clonal antibodies for clinical application: pitfalls and solutions.Cancer, 1997. 80(12 Suppl): p. 2360-70.
80. Borjesson, P.K., et al., Phase I therapy study with (186)Re-labeled humanized monoclonal antibody BIWA 4 (bivatuzumab) in patients with head and neck squamous cell carcinoma. Clin Cancer Res, 2003. 9(10 Pt 2): p. 3961S-72S.

46
81. Colnot, D.R., et al., Reinfusion of unprocessed, granulocyte colony-stimulating factor-stimulated whole blood allows dose escalation of 186Relabeled chimeric monoclonal antibody U36 radioimmuno-therapy in a phase I dose escalation study. Clin Cancer Res, 2002. 8(11): p. 3401-6.
82. Colnot, D.R., et al., Phase I therapy study of 186Re-labeled chimeric monoclonal antibody U36 in patients with squamous cell carcinoma of the head and neck. J Nucl Med, 2000. 41(12): p. 1999-2010.
83. Tijink, B.M., et al., A phase I dose escalation study with anti-CD44v6 bivatuzumab mertansine in patients with incurable squamous cell carcinoma of the head and neck or esophagus. Clin Cancer Res, 2006. 12(20 Pt 1): p. 6064-72.
84. Goldstein, N.I., et al., Biological efficacy of a chimeric antibody to the epidermal growth factor receptor in a human tumor xenograft model. Clin Cancer Res, 1995. 1(11): p. 1311-8.
85. Mendelsohn, J. and J. Baselga, Status of epidermal growth factor receptor antagonists in the biology and treatment of cancer. J Clin Oncol, 2003. 21(14): p. 2787-99.
86. Janmaat, M.L. and G. Giaccone, The epidermal growth factor recep-tor pathway and its inhibition as anticancer therapy. Drugs Today (Barc), 2003. 39 Suppl C: p. 61-80.
87. Tolmachev, V. and S. Sjöberg, Polyhedral boron compounds as potential linkers for attachment of radiohalogens to targeting pro-teins and peptides. A review. Collect Czech. Chem. Commun., 2002. 67: p. 913-935.
88. Zalutsky, M.R. and G. Vaidyanathan, Astatine-211-labeled radio-therapeutics: an emerging approach to targeted alpha-particle ra-diotherapy. Curr Pharm Des, 2000. 6(14): p. 1433-55.
89. Persson, M.I., et al., Astatinated trastuzumab, a putative agent for radionuclide immunotherapy of ErbB2-expressing tumours. Oncol Rep, 2006. 15(3): p. 673-80.
90. Borjesson, P.K., et al., Performance of immuno-positron emission tomography with zirconium-89-labeled chimeric monoclonal anti-body U36 in the detection of lymph node metastases in head and neck cancer patients. Clin Cancer Res, 2006. 12(7 Pt 1): p. 2133-40.
91. van Deurs, B., et al., The ways of endocytosis. Int Rev Cytol, 1989. 117: p. 131-77.
92. Kyriakos, R.J., et al., The fate of antibodies bound to the surface of tumor cells in vitro. Cancer Res, 1992. 52(4): p. 835-42.
93. Geissler, F., et al., Intracellular catabolism of radiolabeled anti-mu antibodies by malignant B-cells. Cancer Res, 1992. 52(10): p. 2907-15.
94. Press, O.W., et al., Comparative metabolism and retention of iodine-125, yttrium-90, and indium-111 radioimmunoconjugates by cancer cells. Cancer Res, 1996. 56(9): p. 2123-9.
47
95. Stein, R., et al., Advantage of a residualizing iodine radiolabel for radioimmunotherapy of xenografts of human non-small-cell carci-noma of the lung. J Nucl Med, 1997. 38(3): p. 391-5.
96. Bocci, V., Efficient Labelling Of Serum Proteins With I-131 Using Chloramine T. Int J Appl Radiat Isot, 1964. 15: p. 449-56.
97. Fraker, P.J. and J.C. Speck, Jr., Protein and cell membrane iodina-tions with a sparingly soluble chloroamide, 1,3,4,6-tetrachloro-3a,6a-diphrenylglycoluril. Biochem Biophys Res Commun, 1978. 80(4): p. 849-57.
98. Robinson, M.K., et al., Quantitative immuno-positron emission to-mography imaging of HER2-positive tumor xenografts with an io-dine-124 labeled anti-HER2 diabody. Cancer Res, 2005. 65(4): p. 1471-8.
99. Wilbur, D.S., et al., Development of a stable radioiodinating reagent to label monoclonal antibodies for radiotherapy of cancer. J Nucl Med, 1989. 30(2): p. 216-26.
100. Zalutsky, M.R. and A.S. Narula, A method for the radiohalogenation of proteins resulting in decreased thyroid uptake of radioiodine. Int J Rad Appl Instrum [A], 1987. 38(12): p. 1051-5.
101. Zalutsky, M.R. and A.S. Narula, Radiohalogenation of a mono-clonal antibody using an N-succinimidyl 3-(tri-n-butylstannyl)benzoate intermediate. Cancer Res, 1988. 48(6): p. 1446-50.
102. Zalutsky, M.R., et al., Enhanced tumor localization and in vivo sta-bility of a monoclonal antibody radioiodinated using N-succinimidyl 3-(tri-n-butylstannyl)benzoate. Cancer Res, 1989. 49(20): p. 5543-9.
103. Hoglund, J., On the use of 76Br-labelled Monoclonal Antibodies for PET. Preclinical Evaluation of Halogenated Antibodies for Diagno-sis and Treatment of Cancer. Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1128., in Department of Oncology, Radiology and Clinical Immunology, Section of Radiol-ogy. 2002, Acta Universitatis Upsaliensis: Uppsala. p. 64.
104. Wilbur, D.S., et al., Radioiodinated iodobenzoyl conjugates of a monoclonal antibody Fab fragment. In vivo comparisons with chloramine-T-labeled Fab. Bioconjug Chem, 1991. 2(2): p. 111-6.
105. Wiseman, S.M., et al., Coexpression of the type 1 growth factor receptor family members HER-1, HER-2, and HER-3 has a synergis-tic negative prognostic effect on breast carcinoma survival. Cancer, 2005. 103(9): p. 1770-7.
106. Nestor, M., et al., Biodistribution of the chimeric monoclonal anti-body U36 radioiodinated with a closo-dodecaborate-containing linker. Comparison with other radioiodination methods. Bioconjug Chem, 2003. 14(4): p. 805-10.
107. Dohan, O., et al., The sodium/iodide Symporter (NIS): characteriza-tion, regulation, and medical significance. Endocr Rev, 2003. 24(1): p. 48-77.

48
108. Verel, I., et al., High-quality 124I-labelled monoclonal antibodies for use as PET scouting agents prior to 131I-radioimmunotherapy.Eur J Nucl Med Mol Imaging, 2004. 31(12): p. 1645-52.
109. Baselga, J., et al., Antitumor effects of doxorubicin in combination with anti-epidermal growth factor receptor monoclonal antibodies. J Natl Cancer Inst, 1993. 85(16): p. 1327-33.
110. Fan, Z., et al., Antitumor effect of anti-epidermal growth factor re-ceptor monoclonal antibodies plus cis-diamminedichloroplatinum on well established A431 cell xenografts. Cancer Res, 1993. 53(19): p. 4637-42.
111. Aboud-Pirak, E., et al., Efficacy of antibodies to epidermal growth factor receptor against KB carcinoma in vitro and in nude mice. J Natl Cancer Inst, 1988. 80(20): p. 1605-11.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 204
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-7341
ACTAUNIVERSITATISUPSALIENSISUPPSALA2006