another look at free markets – regulating and evaluating genetic tests lawrence silverman may 30,...
Post on 21-Dec-2015
218 views
TRANSCRIPT
Another Look at Free Markets – Regulating and Evaluating Genetic Tests
Lawrence SilvermanMay 30, 2009
•Oversight of Genetic tests – Roles of FDA, CDC, and CMS and their relationship with CLIA?
•How Are Genetic Tests Assessed? - What is Analytical Validity, Clinical Validity, Clinical Utility, and Quality Assurance
•What is Evidence-based Medicine and EGAPP
•Oversight of Genetic tests – Roles of FDA, CDC, and CMS and their relationship with CLIA?Or,“It’s Just as Good as a Sony”
•How Are Genetic Tests Assessed? - What is Analytical Validity, Clinical Validity, Clinical Utility, and Quality Assurance•Or,Just Because We Can Perform a Genetic Test, Should We?
•What is Evidence-based Medicine and EGAPPOr,Bian Hua (Things Change)
Another Look at Free Markets – Regulating and Evaluating Genetic Tests
Clinical Laboratory Improvement Amendment
•Passed in 1988 (enacted in 1992) and regulates all clinical laboratory testing aspects.•Center for Medicare and Medicaid Services (CMS) - responsible for CLIA oversight, including financial management of CLIA operations•FDA has oversight for laboratory tests under CLIA•CDC serves an advisory role on CLIA , primarily throughCLIAC (Clinical Laboratory Improvement Advisory Committee)
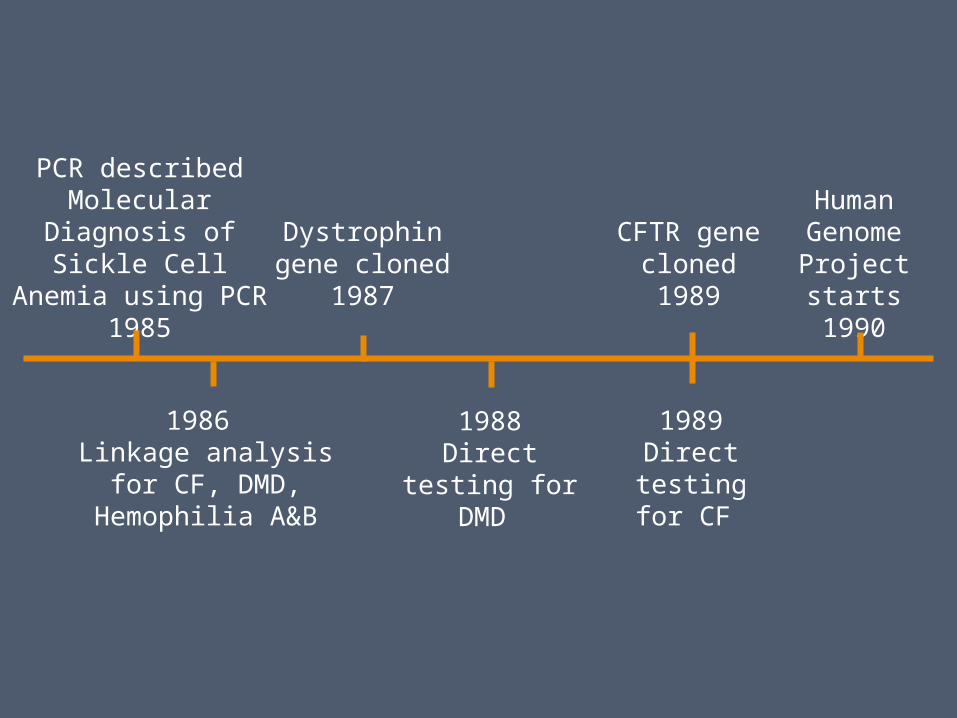
PCR describedMolecular Diagnosis of
Sickle Cell Anemia using PCR1985
1986 Linkage analysis for CF, DMD, Hemophilia A&B
Dystrophin gene cloned1987
1988Direct testing
for DMD
CFTR gene cloned1989
1989Direct testing
for CF
Human Genome Project starts
1990
Regulation of Genetics Tests
• Hot button item• IOM – 1994• Task Force on Genetics Tests – 1997• Secretary’s Advisory Committee on Genetic
Tests – 2001 – analytical validity, clinical validity, and clinical utility.
• Regulatory gaps
What are Key Issues in Assessing Genetic Tests
Analytical Validity – does the test measure the analyte in questioni.e., can the test detect both the presence and absence of mutations.
Clinical Validity – does the test result predict the presence or absenceof disease
Clinical Utility – how does the test result affect morbidity, mortality, ordisability, specifically through treatments based on the test result.
What is a genetic test and how are they used?
Genetic tests refer to the measurement of DNA, RNA, chromosomes or proteins that reflect changes in genes or gene products that are associated with specific disorders or phenotypes. These disorders may be heritable or acquired.
How genetic tests are commonly used:
Newborn screening, diagnostic testing, carrier testing,prenatal testing, preimplantation testing, predictive andpresymptomatic testing, identity and forensic testing. Predictivetesting includes pharmacogenomics.
Developing Regulatory Requirements for Genetic TestingUnder CLIA
•Recommendations were made to CLIAC on modifying CLIA to include a genetic testing specialty. Scope included definitions and requirements for pre-analytic, analytic and post-analytic phases of testing – 1997-1999•Notice of Intent (NOI) – Published in Federal Register 5/2000 notifying that a Notice of Proposed Rule Making was being prepared to revise CLIA in order to make a human genetics testing specialty.•57 responses comments were received in response to NOI•CLIAC Workgroup on Genetic Testing makes recommendations to public response - 2/2001.•CMS puts issuance of specialty area on regulatory agenda with release date of November – 4/2006•CMS decides a genetic testing specialty is unnecessary since existingCLIA regulations are sufficient (“It’s just as good as a Sony”) – 9/2006
How Are Genetic Tests Different – Let Me Count the Ways
PenetranceExpressivityModifiersEpigeneticsDe Novo versus inhertedImpriniting
Discrimination (perceived)Association v causalityPrivacy v right to knowPresymptomaticPredictiveLack of PT Surveys
Hudson K., J. Murphy, D. Kaufman, G. Javitt, S. Katsanis, and J. Scott. 2006. Oversight of US Genetic Testing Laboratories. Nature Biotechnology 24 (9): 1083-1090.
2006 Survey of Genetic Testing Laboratory Directors
• Collect data on genetic testing laboratory PT practices
• Evaluate participation in PT and laboratory quality
• Assess views of genetic testing laboratory directors
Survey Results
• 95% of molecular and biochemical testing labs reporting results to patients are CLIA certified
• 35% of laboratories do not do PT for all of the tests they perform
• 73% of genetic testing laboratory directors in this survey support CLIA specialty
FDA and the ASR Rule
However, FDA has chosen only to regulate the ingredients of LDTs (ASRs) since “CLIA regulated labs qualified to perform high complexity testing have demonstrated expertise and ability to use ASRs in test procedures and analyses.”
“It’s Just as Good as a Sony”
“Clinical laboratories that develop tests are acting as manufacturers ofmedical devices and are subject to FDA jurisdiction”.
ASR – Analyte Specific Reagent used in laboratory developed tests (LDT)
EGAPP Evaluation of Genomic Applications in Practice and Prevention
In 2004 CDC established EGAPP to evaluate a systematic, evidence-based process for assessing genetic tests and other applications of genomic technology in transition from research to clinical and public health practice. EGAPP utilizes ACCE criteria (Analytic and Clinical validity, Clinical utility and associated Ethical, legal, and social implications) developed by Foundation for BloodResearch in 2004.Published Recommendations:•Can Tumor Gene Profiling Improve Outcomes in Patients with Breast Cancer•Can UGT1A1 Genotyping Reduce Morbidity and Mortality in Patients with Metastatic Colorectal Cancer Treated with Irinotecan•Genetic Testing Strategies in Newly Diagnosed Individuals with Colorectal Cancer Aimed at Reducing Morbidity and Mortality from Lynch Syndrome in Relatives
What are Limitations of EGAPP (and ACCE)
Clinical Validity is not regulated under CLIA, which only regulatesperformance specifications, such as accuracy, precision, reportableranges and reference ranges.
Professional organizations or state agencies that have clearance toinspect and accredit laboratories can exceed CLIA specifications,thus, make requirements regarding establishment of clinical validity. However, this is not universal.
Clinical Utility is both nebulous in definition and dependent onchanging technology, clinical knowledge, and therapy.
Thus, Bian Hua, things change.
Fragile X Premutation and Ovarian Dysfunction
• Fragile X Syndrome - Most common cause of inherited mental retardation
• Affects 1:2500-1:4000 males• Affects 1:5000-1:10000 females• X-linked mental retardation
1) Mental Retardation-IQ<50 in affected males, IQ 70-90 in affected females
2) Characteristic Facies-low set ears, prominent jaw
3) Behavioural abnormalities-hyperkinetic-autistic like behaviour-learning disabilities
4) Macroorchidism
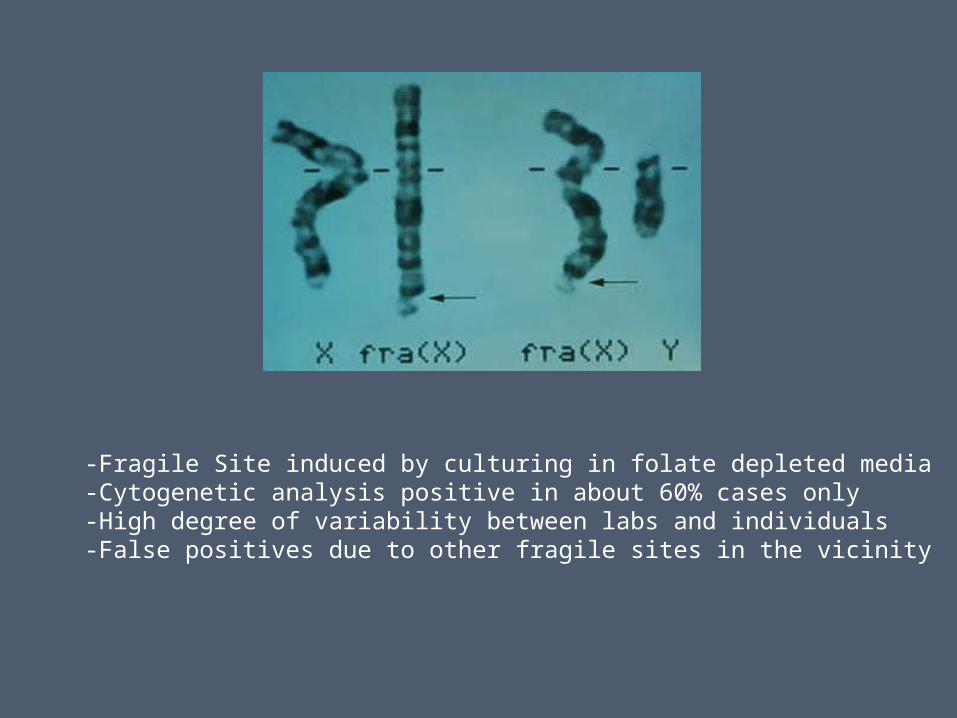
-Fragile Site induced by culturing in folate depleted media-Cytogenetic analysis positive in about 60% cases only-High degree of variability between labs and individuals-False positives due to other fragile sites in the vicinity
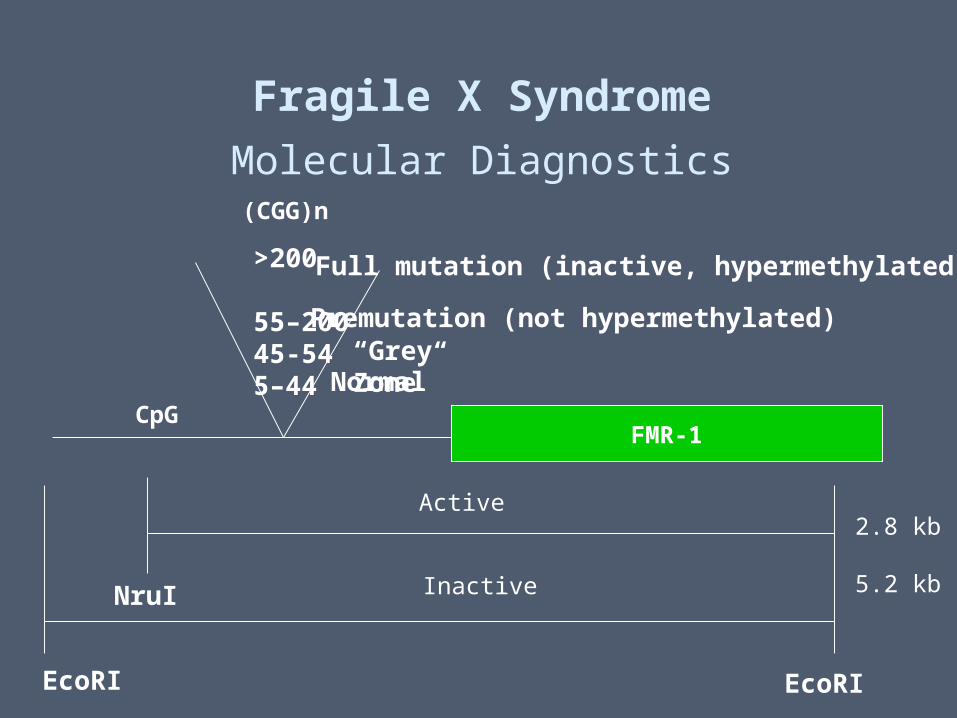
FMR-1
(CGG)n
>200
55–20045-545–44 Normal
Premutation (not hypermethylated)
Full mutation (inactive, hypermethylated)
CpG
EcoRI EcoRI
NruI
Active
Inactive
2.8 kb
5.2 kb
Fragile X Syndrome
Molecular Diagnostics
“Grey Zone”
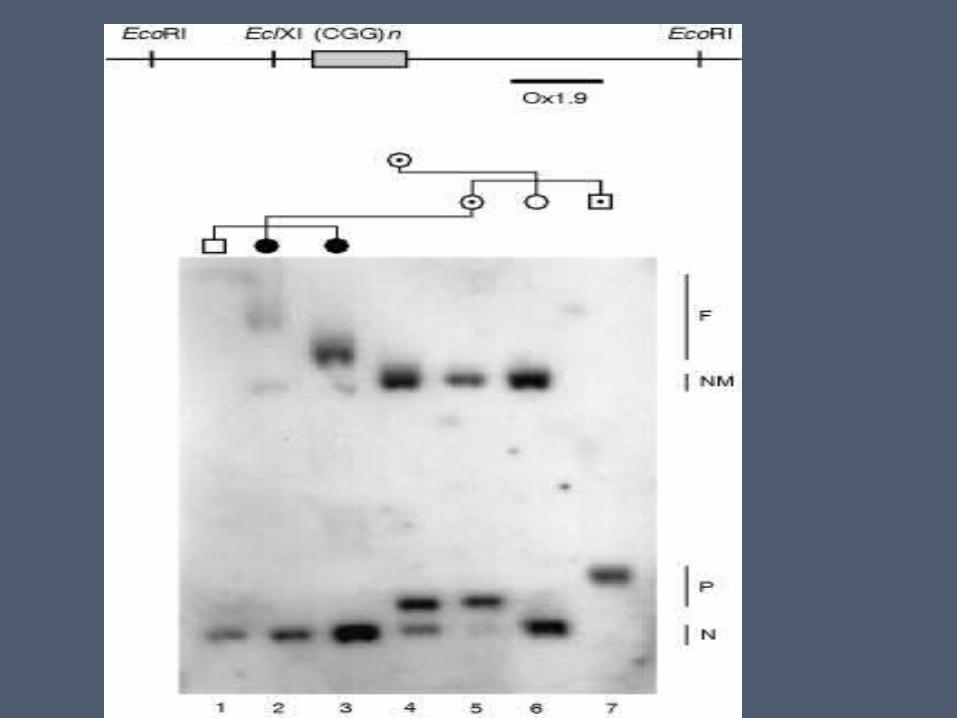
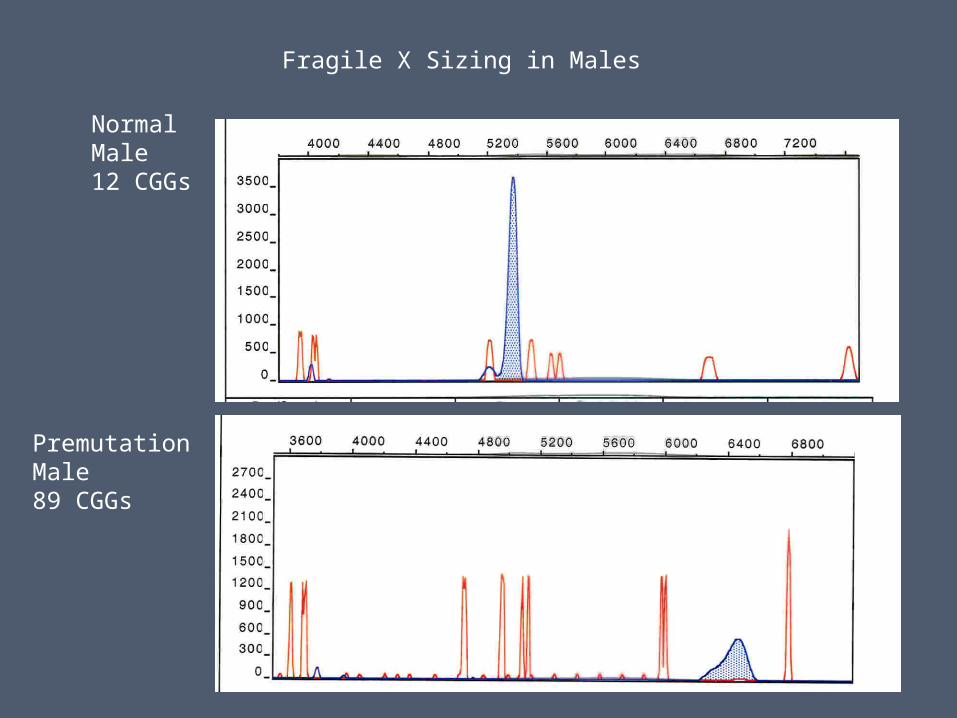
Fragile X Sizing in Males
NormalMale12 CGGs
PremutationMale89 CGGs
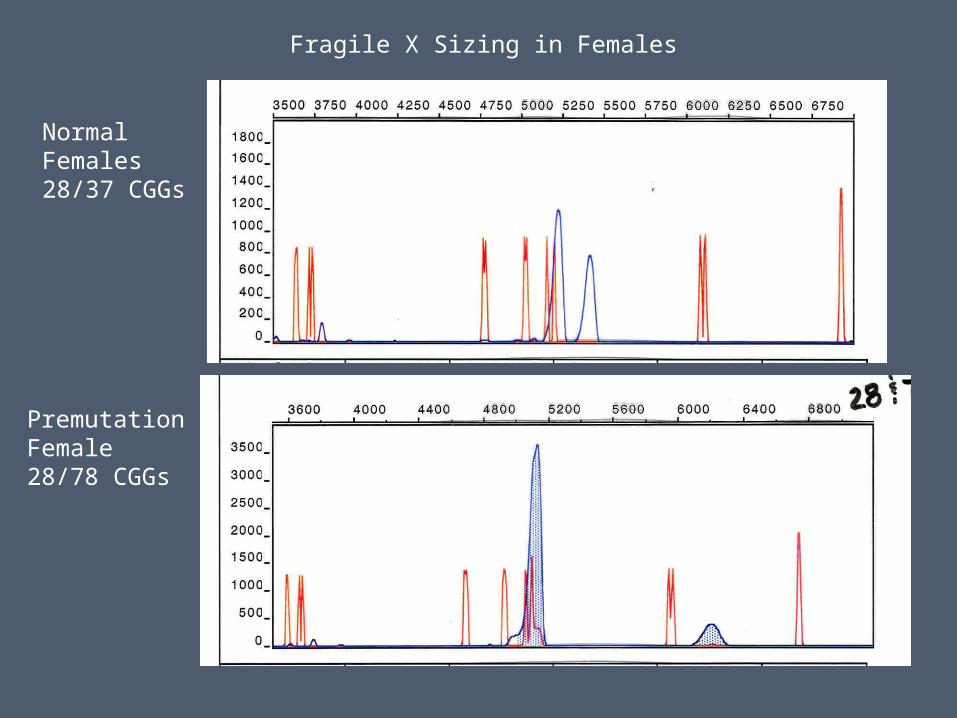
Fragile X Sizing in Females
NormalFemales28/37 CGGs
PremutationFemale28/78 CGGs
Fragile X Premutation• Defined as CGG between 55-200• Not hypermethylated; gene not shut down• Individuals do not have fragile X syndrome• Males with premutations pass on only
premutations to their daughters• Likelihood of passing full mutation from
mother to offspring increases with size of premutation; 100% likelihood by 90 CGGs
Frequency of Fragile X Premutation
• Differs from study to study• In women-1:100 to 1:250• In men-1:250 to 1:750
Premature Ovarian Failure (POF)
• Mean age of menopause is about 51• POF defined as menopause before age 40• About 1% of females have POF• Elevated FSH/LH ratios• Both genetic and environmental causes
known• However, 60% of cases have no obvious
cause
POF in Fragile X Carriers• Increased rates of POF found only in premutation
carriers • About 16-20% of premutation carriers have POF• Full mutation carriers have no higher incidence of
POF
• High FSH levels (> 15 IU/L) often found in menstruating women prior to POF
• No changes in inhibin B or 17β estradiol levels
POF in Fragile X Carriers
• Screening of all POF patients led to a pick up rate of about 1.6-8% for FRA-X premutations
• Repeat number ranged from 80-175.• No full mutations were identified
POF and Fragile X Premutation
• Pick up rate for premutation in familial POF is much higher; about 14-18%
• In sporadic POF 2-4%
What About Premutation Male Carriers?FXTAS- a new neurologic phenotype
• Several studies have now described the presence of a late-onset neurological problem in males carriers of the premutation (now termed FXTAS)
• Cerebellar ataxia and intention tremor
• Other features: short term memory loss, cognitive decline, parkinsonism, autonomous dysfunction, executive functional defects
• MRI shows approx. symmetric increases in T2 weighted signal intensity in middle cerebellar peduncle
• Eosinophilic intranuclear inclusions found in neurons and astrocytes
• Increasing penetrance of the phenotype with age; >80% by age 80
• Females also affected but severity and penetrance are less
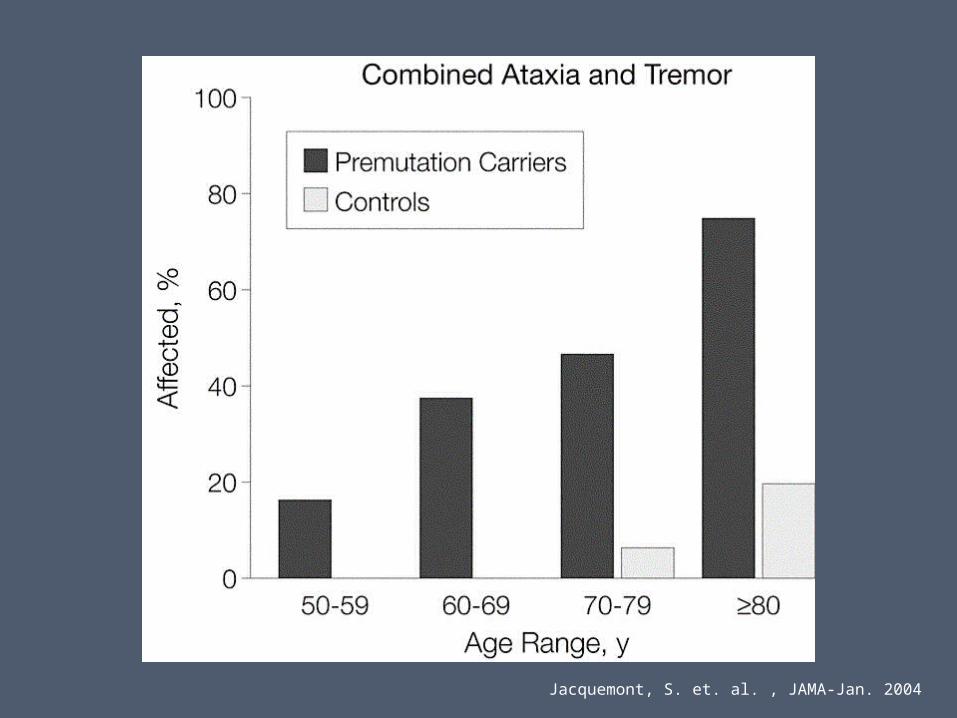
Jacquemont, S. et. al. , JAMA-Jan. 2004
Summary of Regulatory Gaps
• Lack of Genetics Specialty under CLIA• Lack of FDA oversight for LDT (except ASR)• Uncertainty regarding clinical validity and clinical
utility• Inadequacy of PT Surveys for most genetic tests• Insufficient transparency regarding laboratory
performance