androgen excess: investigations and management · a department of obstetrics and gynecology, ......
TRANSCRIPT

Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21
Contents lists available at ScienceDirect
Best Practice & Research ClinicalObstetrics and Gynaecology
journal homepage: www.elsevier .com/locate /bpobgyn
7
Androgen excess: Investigations andmanagement
Daria Lizneva, MD, PhD a, b, c, Larisa Gavrilova-Jordan, MD a,Walidah Walker, MS a, Ricardo Azziz, MD, MPH a, d, *
a Department of Obstetrics and Gynecology, Medical College of Georgia, Augusta State University, 1120 15thStreet, 30912 Augusta, GA, USAb Medical Company IDK, ul. Entuziastov 29, 443067 Samara, Russian Federationc Department of Reproductive Health Protection, Scientific Center of Family Health and HumanReproduction, ul. Timiryazeva 16, 664003 Irkutsk, Russian Federationd Department of Medicine, Medical College of Georgia, Augusta State University, 1120 15th Street, 30912Augusta, GA, USA
Keywords:hyperandrogenismhirsutismacnefemale pattern hair lossPCOS
* Corresponding author. Department of ObstetriGA 30912, USA. Tel.: þ1 706 721 2304.
E-mail address: [email protected] (R. Azziz).
http://dx.doi.org/10.1016/j.bpobgyn.2016.05.0031521-6934/© 2016 Published by Elsevier Ltd.
Please cite this article in press as: LiznevBest Practice & Research Clinical Obsj.bpobgyn.2016.05.003
Androgen excess (AE) is a key feature of polycystic ovary syn-drome (PCOS) and results in, or contributes to, the clinicalphenotype of these patients. Although AE will contribute to theovulatory and menstrual dysfunction of these patients, the mostrecognizable sign of AE includes hirsutism, acne, and androgenicalopecia or female pattern hair loss (FPHL). Evaluation includesnot only scoring facial and body terminal hair growth usingthe modified FerrimaneGallwey method but also recordingand possibly scoring acne and alopecia. Moreover, assessmentof biochemical hyperandrogenism is necessary, particularly inpatients with unclear or absent hirsutism, and will includeassessing total and free testosterone (T), and possibly dehydro-epiandrosterone sulfate (DHEAS) and androstenedione, althoughthese latter contribute limitedly to the diagnosis. Assessment ofT requires use of the highest quality assays available, generallyradioimmunoassays with extraction and chromatography ormass spectrometry preceded by liquid or gas chromatography.Management of clinical hyperandrogenism involves primarilyeither androgen suppression, with a hormonal combinationcontraceptive, or androgen blockade, as with an androgen re-ceptor blocker or a 5a-reductase inhibitor, or a combinationof the two. Medical treatment should be combined withcosmetic treatment including topical eflornithine hydrochloride
cs and Gynecology, Augusta University, 1120 15th Street, CB-2209, Augusta,
a D, et al., Androgen excess: Investigations and management,tetrics and Gynaecology (2016), http://dx.doi.org/10.1016/
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e212
Please cite this article in press as: LiznevBest Practice & Research Clinical Obsj.bpobgyn.2016.05.003
and short-term (shaving, chemical depilation, plucking, thread-ing, waxing, and bleaching) and long-term (electrolysis, lasertherapy, and intense pulse light therapy) cosmetic treatments.Generally, acne responds to therapy relatively rapidly, whereashirsutism is slower to respond, with improvements observed asearly as 3 months, but routinely only after 6 or 8 months oftherapy. Finally, FPHL is the slowest to respond to therapy, if itwill at all, and it may take 12 to 18 months of therapy for anobservable response.
© 2016 Published by Elsevier Ltd.
Androgen biosynthesis and metabolism in women
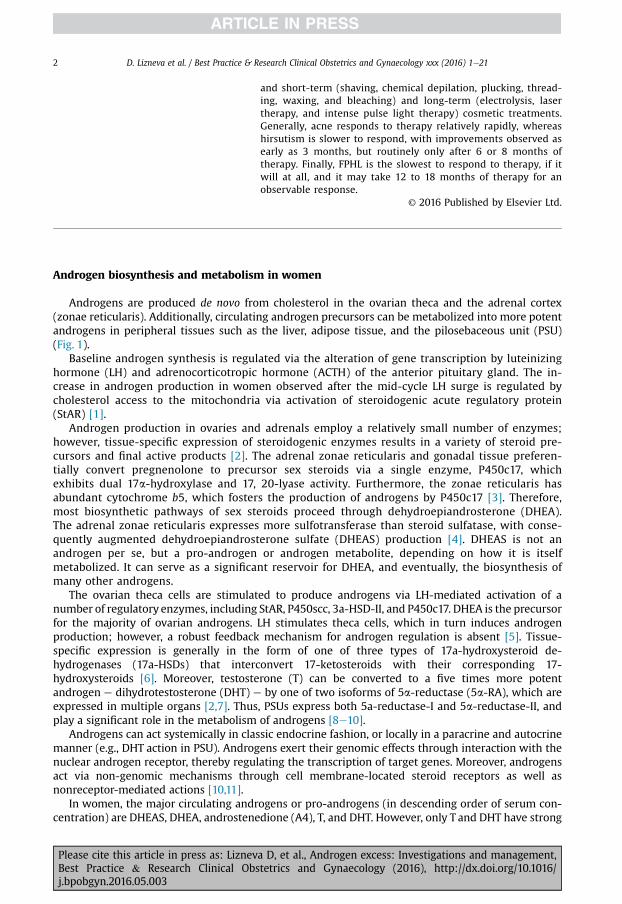
Androgens are produced de novo from cholesterol in the ovarian theca and the adrenal cortex(zonae reticularis). Additionally, circulating androgen precursors can be metabolized into more potentandrogens in peripheral tissues such as the liver, adipose tissue, and the pilosebaceous unit (PSU)(Fig. 1).
Baseline androgen synthesis is regulated via the alteration of gene transcription by luteinizinghormone (LH) and adrenocorticotropic hormone (ACTH) of the anterior pituitary gland. The in-crease in androgen production in women observed after the mid-cycle LH surge is regulated bycholesterol access to the mitochondria via activation of steroidogenic acute regulatory protein(StAR) [1].
Androgen production in ovaries and adrenals employ a relatively small number of enzymes;however, tissue-specific expression of steroidogenic enzymes results in a variety of steroid pre-cursors and final active products [2]. The adrenal zonae reticularis and gonadal tissue preferen-tially convert pregnenolone to precursor sex steroids via a single enzyme, P450c17, whichexhibits dual 17a-hydroxylase and 17, 20-lyase activity. Furthermore, the zonae reticularis hasabundant cytochrome b5, which fosters the production of androgens by P450c17 [3]. Therefore,most biosynthetic pathways of sex steroids proceed through dehydroepiandrosterone (DHEA).The adrenal zonae reticularis expresses more sulfotransferase than steroid sulfatase, with conse-quently augmented dehydroepiandrosterone sulfate (DHEAS) production [4]. DHEAS is not anandrogen per se, but a pro-androgen or androgen metabolite, depending on how it is itselfmetabolized. It can serve as a significant reservoir for DHEA, and eventually, the biosynthesis ofmany other androgens.
The ovarian theca cells are stimulated to produce androgens via LH-mediated activation of anumber of regulatory enzymes, including StAR, P450scc, 3a-HSD-II, and P450c17. DHEA is the precursorfor the majority of ovarian androgens. LH stimulates theca cells, which in turn induces androgenproduction; however, a robust feedback mechanism for androgen regulation is absent [5]. Tissue-specific expression is generally in the form of one of three types of 17a-hydroxysteroid de-hydrogenases (17a-HSDs) that interconvert 17-ketosteroids with their corresponding 17-hydroxysteroids [6]. Moreover, testosterone (T) can be converted to a five times more potentandrogen e dihydrotestosterone (DHT) e by one of two isoforms of 5a-reductase (5a-RA), which areexpressed in multiple organs [2,7]. Thus, PSUs express both 5a-reductase-I and 5a-reductase-II, andplay a significant role in the metabolism of androgens [8e10].
Androgens can act systemically in classic endocrine fashion, or locally in a paracrine and autocrinemanner (e.g., DHT action in PSU). Androgens exert their genomic effects through interaction with thenuclear androgen receptor, thereby regulating the transcription of target genes. Moreover, androgensact via non-genomic mechanisms through cell membrane-located steroid receptors as well asnonreceptor-mediated actions [10,11].
In women, the major circulating androgens or pro-androgens (in descending order of serum con-centration) are DHEAS, DHEA, androstenedione (A4), T, and DHT. However, only T and DHT have strong
a D, et al., Androgen excess: Investigations and management,tetrics and Gynaecology (2016), http://dx.doi.org/10.1016/
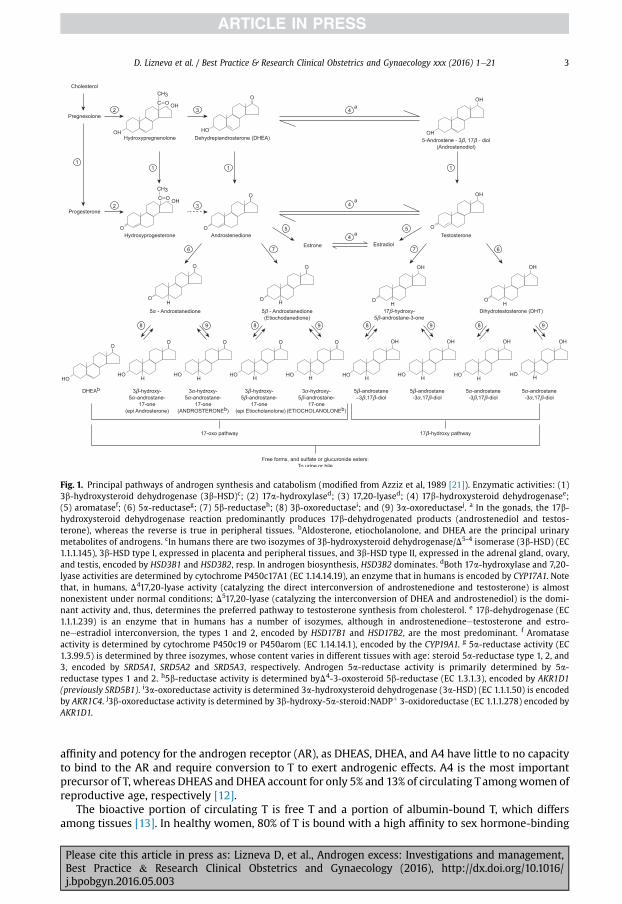
Fig. 1. Principal pathways of androgen synthesis and catabolism (modified from Azziz et al, 1989 [21]). Enzymatic activities: (1)3b-hydroxysteroid dehydrogenase (3b-HSD)c; (2) 17a-hydroxylased; (3) 17,20-lyased; (4) 17b-hydroxysteroid dehydrogenasee;(5) aromatasef; (6) 5a-reductaseg; (7) 5b-reductaseh; (8) 3b-oxoreductasei; and (9) 3a-oxoreductasej. a In the gonads, the 17b-hydroxysteroid dehydrogenase reaction predominantly produces 17b-dehydrogenated products (androstenediol and testos-terone), whereas the reverse is true in peripheral tissues. bAldosterone, etiocholanolone, and DHEA are the principal urinarymetabolites of androgens. cIn humans there are two isozymes of 3b-hydroxysteroid dehydrogenase/D5-4 isomerase (3b-HSD) (EC1.1.1.145), 3b-HSD type I, expressed in placenta and peripheral tissues, and 3b-HSD type II, expressed in the adrenal gland, ovary,and testis, encoded by HSD3B1 and HSD3B2, resp. In androgen biosynthesis, HSD3B2 dominates. dBoth 17a-hydroxylase and 7,20-lyase activities are determined by cytochrome P450c17A1 (EC 1.14.14.19), an enzyme that in humans is encoded by CYP17A1. Notethat, in humans, D417,20-lyase activity (catalyzing the direct interconversion of androstenedione and testosterone) is almostnonexistent under normal conditions; D517,20-lyase (catalyzing the interconversion of DHEA and androstenediol) is the domi-nant activity and, thus, determines the preferred pathway to testosterone synthesis from cholesterol. e 17b-dehydrogenase (EC1.1.1.239) is an enzyme that in humans has a number of isozymes, although in androstenedioneetestosterone and estro-neeestradiol interconversion, the types 1 and 2, encoded by HSD17B1 and HSD17B2, are the most predominant. f Aromataseactivity is determined by cytochrome P450c19 or P450arom (EC 1.14.14.1), encoded by the CYP19A1. g 5a-reductase activity (EC1.3.99.5) is determined by three isozymes, whose content varies in different tissues with age: steroid 5a-reductase type 1, 2, and3, encoded by SRD5A1, SRD5A2 and SRD5A3, respectively. Androgen 5a-reductase activity is primarily determined by 5a-reductase types 1 and 2. h5b-reductase activity is determined byD4-3-oxosteroid 5b-reductase (EC 1.3.1.3), encoded by AKR1D1(previously SRD5B1). i3a-oxoreductase activity is determined 3a-hydroxysteroid dehydrogenase (3a-HSD) (EC 1.1.1.50) is encodedby AKR1C4. j3b-oxoreductase activity is determined by 3b-hydroxy-5a-steroid:NADPþ 3-oxidoreductase (EC 1.1.1.278) encoded byAKR1D1.
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 3
affinity and potency for the androgen receptor (AR), as DHEAS, DHEA, and A4 have little to no capacityto bind to the AR and require conversion to T to exert androgenic effects. A4 is the most importantprecursor of T, whereas DHEAS and DHEA account for only 5% and 13% of circulating Tamongwomen ofreproductive age, respectively [12].
The bioactive portion of circulating T is free T and a portion of albumin-bound T, which differsamong tissues [13]. In healthy women, 80% of T is bound with a high affinity to sex hormone-binding
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e214
globulin (SHBG), 19% is bound to albumin, and only 1% circulates as a free fraction [12,14]. In contrast,DHEAS, DHEA, and A4 are bound to albumin with low affinity and, thus, available for peripheralconversion [15,16].
The clearance of androgens is accomplished by hepatic extraction and peripheral metabolism,which are highly dependent upon the unbound portion of circulating steroid [12]. Most of circulating Tis metabolized via hepatic conjugationwith glucuronic or sulfuric acids or voided as 17-ketosteroids inurine [17]. Only a small fraction of T and half of A4 are metabolized peripherally. Approximately 15% ofandrogen sulfates are excreted in bile, of which 80% are reabsorbed into the gut. The metabolism andclearance of circulating androgens may be altered by age, presence of obesity, medical conditions, andmedications.
Androgen excess in PCOS
The terms androgen excess (AE) and hyperandrogenismwill be used interchangeably in this article.The differential diagnosis of the hyperandrogenic patient includes idiopathic hirsutism, the hyper-androgenic insulin-resistant acanthosis nigricans (HAIRAN) syndrome, 21-hydroxylase-deficient non-classic congenital adrenal hyperplasia, classic congenital adrenal hyperplasia, and androgen-secretingneoplasms [18]. Rare causes include side effects from medication, hypothyroidism, hyper-prolactinemia, and Cushing's disease [19]. However, in women, the most common cause of AE (i.e.,hyperandrogenism) is the polycystic ovary syndrome (PCOS) and, in this disorder, gonadotropin-dependent functional ovarian AE is the major source of the hyperandrogenemia [20,21]. Ovariantheca cells increase androgen production in response to chronically elevated LH and insulin levels[22,23]. Hyperinsulinemia promotes androgen biosynthesis via the insulin receptor and, to a lesserextent, the insulin-like growth factore1 (IGF-1) receptor on theca cells, and increases levels of circu-lating free T by suppressing hepatic production of SHBG [24,25]. ACTH-dependent overproduction offunctional adrenal androgens further contributes to hyperandrogenemia [26,27].
Clinically evident hyperandrogenism results in various symptoms resulting from the impact of AEon the PSU activity in gender-specific skin areas: hirsutism, acne, and androgenic alopecia [10]. Theresponse of the PSU to androgens in regard to sebum production and the transformation of vellus toterminal hair (ie, hair terminalization) vary considerably across skin areas and between individuals[28,29]. The PSU sensitivity to androgens is, in part, determined by the local action of androgensthemselves: 5a-RA activity, which converts T to DHT; and the subsequent binding of DHT locally to PSUARs with high affinity [7,29,30]. Consequently, not all patients with hirsutism have demonstrablehyperandrogenemia, and not all patients with elevated circulating androgen levels will be hirsute[2,18,31].
Hirsutism, or the presence of male pattern terminal hair growth inwomen, is themost common andrecognizable sign of female AE. Half of the women with mild hirsutism and the majority of those withmoderate to severe hirsutism have elevated plasma total and free T levels [18,32,33]. One-third of PCOSwomen have elevated levels of adrenal androgen precursors [34]. Hirsute women commonly have lowlevels of SHBG that leads to increased concentrations of free T [14].
Androgens play significant role in the development of acne vulgaris, as AE is associated withincrease in sebum production and ameliorated shedding of hyperkeratinized epithelium, whichcauses occlusion of the hair follicle and proliferation of Propionibacterium acnes [28,30]. Bacteriametabolize sebum triglycerides to glycerol and free fatty acids that cause further inflammation ofthe PSU. Sebum production markedly increases during adrenarche, a time of maximal DHEASserum levels, and acne in PCOS women in part resembles an exaggerated form of adrenarche[10,27,28,34]. A majority of nonhirsute acneic patient, regardless of age, have variable degrees ofhyperandrogenemia [35].
Androgenic alopecia, also known as female pattern hair loss (FPHL), is characterized by thinning ofthe sagittal scalp hair growth with modest recession of the frontal and frontoparietal hair lines. It is ahighly prevalent disorder with an incidence that increases with age [36]. As a clinical sign of hyper-androgenemia, androgenic alopecia was reported in 67% of women with PCOS [37]. Elevated metab-olites of T and corticosterone, along with enhanced local 5a-RA activity, were also reported in womenwith androgenic alopecia [17].
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 5
Diagnosis of AE in women
Hyperandrogenism or AE in women can be evident clinically (by the presence of hirsutism and/orandrogenic alopecia) or biochemically, through the measurement of androgens, total, free, or in pre-cursor/metabolite forms, in the circulation or other body fluids (eg, urine, saliva, etc.).
Hirsutism
Objective and subjective methods are available for the diagnosis of hirsutism. Objective methodsof evaluation (i.e., photographic evaluations, weighing of extracted hairs) are generally time-consuming and are mainly used for research purposes [38]. More applicable to the clinical settingare the visual, albeit more subjective, scoring system widely used for the evaluation of hair growth.Several scales have been proposed; however, the modified FerrimaneGallwey scoring system (mFG)is currently considered the “gold” standard for the clinical evaluation of hirsutism [38] (Fig. 2). Inorder to improve the quality of assessment, patients should be advised to avoid use of electrolysis orlasers for at least 3 months, depilation or waxing for 4 weeks, and cautioned not to shave at least 5days prior to evaluation [38].
Establishing the cut-off score for determining an abnormal score (ie, one indicating hirsutism) hasgenerally relied on establishing the 95th percentile of a “normal,” or “control population,” with cut-offscores ranging from 3 to 8, and even as high as 10 [39e41]. However, these cut-off values do not takeinto account the type of control populations used (i.e., super-controls, who have been assessed care-fully; individuals from potentially medically biased population; or unscreened women from the gen-eral population) nor consider that the 95th percentile as a definition of “normal” has little clinical
Fig. 2. Modified FerrimaneGallwey (mFG) scoring system for facial and body terminal hair (copyright 2005 by Ricardo Azziz,reproduced with permission). Nine body areas are scored from 0 (no terminal hairs in the area observed and the score sheet is notmarked), to 1 (minimal terminal hairs are observed), 2 (more terminal hairs in the area are observed, but less than those of a normalmale), 3 (terminal hair growth in the area is similar to that seen in a lesser hirsute male), to 4 (terminal hair growth in the area issimilar to that seen in a hirsute male). Note: Terminal hairs can be recognized as those hairs that grow >5 mm in length if un-disturbed, are generally pigmented, and have a central core of compacted hairs (medulla), which may give them denser color,coarser feel, and shape.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e216
validity. Imagine that we considered only 5% of those who are overweight as being obesee the averagebody mass index (BMI) to diagnose obesity would then be 40 kg/m2 [42].
A bettermethod of defining the degree of hirsutism, and that of any other continuous parameter in apopulation that one suspects detects an “abnormal” subset, is to use cluster analysis or similar ap-proaches to identify natural breaks in the data that would suggest the presence of these distinctivepopulations. Using this approach in a large population of unselected women seeking an employmentphysical assessment, consisting of Black (African-American, n¼ 350) and White (North-AmericanCaucasians, n¼ 283) women, we found that a cut-off of 3 or more clearly detected a population thatwas abnormal or different [39].
The population with a score of >3 comprised 22.1% of all subjects. Of these subjects, 69.3% com-plained of hirsutism, compared with 15.8% of womenwith anmFG score <3, and this was similar to theproportion of womenwith an mFG score of at least 8 who considered themselves to be hirsute (70.0%).Additionally, of women with an mFG score of at least 3, 60.7% used some form of treatment for un-wanted hair, not different from the proportion of women with an mFG score of at least 8 whoconsidered themselves to be hirsute or used some form of hair treatment (36.7%). Overall, there wereno significant differences between Black and White women [39]. Using a similar analysis, Zhao andcolleagues studying 2988 women aged 20e45 years from the general population of Southern Chinaobserved that an mFG score of �5 indicates hair growth above the norm [43]. In a separate study, weobserved that more than 50% of individuals with mFG scores of between 3 and 5 had a tangible AEdisorder [44].
Overall, the cut-off mFG score value indicating “abnormal” seems to be closer to 3e5, less than thehigher values reported previously. Thus, while an mFG score of 6e8 may be used as evidence ofpathologic “hirsutism,” this definition is much more severe than how patients perceive their hairgrowth. Finally, current data suggests relatively little difference in the cut-off mFG score betweenMongoloid Asians, Caucasians, and Blacks [39,43,45,46], although further studies are needed.
Acne vulgaris
There is no universally accepted classification currently in use for evaluation of acne severity.Several global assessment scales have been developed to incorporate the clinical manifestation ofacne vulgaris into a single category. They have focused on quantity and quality of acne elements:noninflammatory lesions (NIL) e closed and/or open comedons, and inflammatory lesions (IL) e
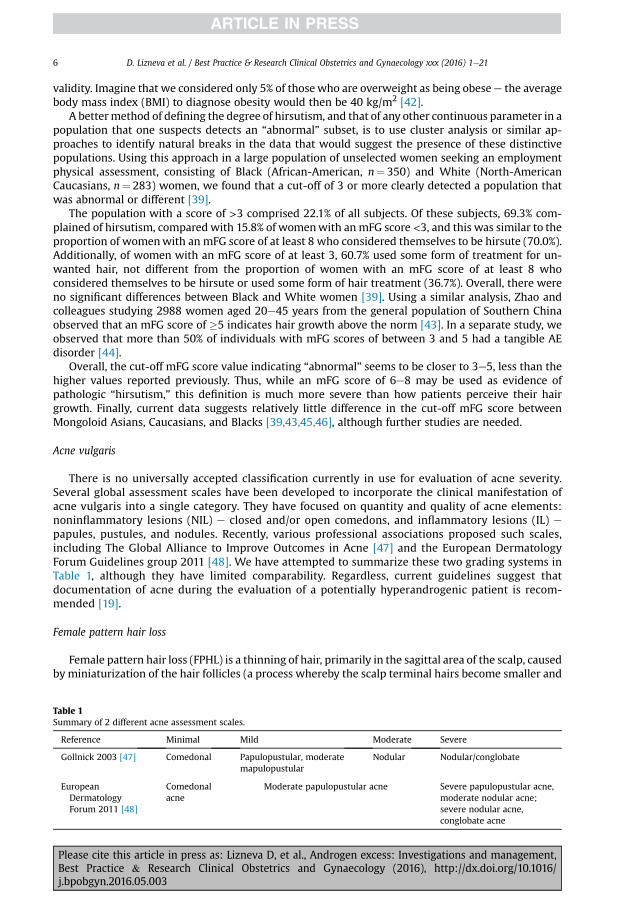
papules, pustules, and nodules. Recently, various professional associations proposed such scales,including The Global Alliance to Improve Outcomes in Acne [47] and the European DermatologyForum Guidelines group 2011 [48]. We have attempted to summarize these two grading systems inTable 1, although they have limited comparability. Regardless, current guidelines suggest thatdocumentation of acne during the evaluation of a potentially hyperandrogenic patient is recom-mended [19].
Female pattern hair loss
Female pattern hair loss (FPHL) is a thinning of hair, primarily in the sagittal area of the scalp, causedby miniaturization of the hair follicles (a process whereby the scalp terminal hairs become smaller and
Table 1Summary of 2 different acne assessment scales.
Reference Minimal Mild Moderate Severe
Gollnick 2003 [47] Comedonal Papulopustular, moderatemapulopustular
Nodular Nodular/conglobate
EuropeanDermatologyForum 2011 [48]
Comedonalacne
Moderate papulopustular acne Severe papulopustular acne,moderate nodular acne;severe nodular acne,conglobate acne
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

Fig. 3. Ludwig classification of female pattern of hair loss (androgenic alopecia) (reproduced with permission [50]).
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 7
eventually become short vellus hairs). There are two common pattern types of FPHL inwomen. Ludwigdescribed diffuse hair thinning in the centroparietal regionwith a preserved frontal line [49] (Fig. 3). Incontrast, the “Christmas tree” pattern is associated with diffuse centroparietal thinning of the hair inconjunctionwith branching of the frontal hair line [50]. FPHL is a process generally characterized by anincrease in the proportion of scalp hairs that are in telogen (i.e. lying unattached from the follicularbulb within the hair shaft ready to be extracted/shed), a finding that can be assessed by the “hair-pulltest” (Fig. 4). In the early stages of FPHL, hair-pull tests may be positive; however, in women withlongstanding, non-scarring hair shedding, a positive hair-pull test is more suggestive of telogen ef-fluvium [51].
FPHL is clinically diagnosed and represents a diagnosis of exclusion. Evaluation should include anassessment of pattern distribution, the hair-pull test (for which the patient should have beeninstructed to not brush or wash her hair for at least 48 hours prior to the exam), an mFG score,assessment for the presence of acne or acanthosis nigricans (see below), and for any defect in nailgrowth [52]. Exclusion of other causes of alopecia should be undertaken including tests to rule-out
Fig. 4. Hair pull test for the detection of hairs in telogen (photo courtesy of Dr. Daria Lizneva). The patient should not have washed orbrushed her hair for at least 24e48 hours before the test. Approximately 50 hairs are grasped and gently tugged outward by theexaminer. The easy extraction of more than six (i.e., >10% of hairs grasped) suggests the presence of excess numbers of hairs intelogen. Note: There are three phases of hair growth: Anagen, which represents the phase of active growth; catagen, which rep-resents the involution and rest phase of the hairs, as active growth ceases; and telogen, in which the hairs are now dead and liewithin the hair shaft separated from their follicle, readily extracted or shed. It is this latter population of hairs that the hair pull testassesses, and which normally comprises less than 10% of all hairs.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e218
scalp fungal infections, autoimmune disorders, hematologic or nutritional defects, and systemichyperandrogenism.
The pattern of hair on the scalp is usually assessed using the Ludwig scale (grades IeIII) orChristmas tree (grades IeIII) classification [52]. It should be noted that there is no specific definitionfor FPHL based on the grade of these scales and all measures are highly subjective. Therefore, the useof photography of the affected area should be considered a better option, at least for follow-up, ifavailable [52].
Biochemical hyperandrogenism
Most of the measurements used clinically today are measurements obtained in blood, either fromserum or plasma. Althoughmeasures can be obtained in saliva, these tend to be highly variable and lessreliable [53] Previously, the measurement of androgen metabolites in urine, such as 17-ketosteroids[54], was widely used. However, as assays for measuring androgens in blood have improved, thesehave been relegated to history. Nonetheless, we should note that androgen measurements in bloodcapture amoment in time, subject to the knownpulsatility of these hormones, whereas urinemeasurescapture a broader picture of androgen biosynthesis.
Because androgens circulate in small amounts and are small steroidal molecules that differ inonly the most minute of ways from other steroids, such as estrogens, progesterones, glucocorti-coids, or even mineralocorticoids, and their myriad metabolites, it is extremely important thatthe assays used for their detection are of the highest quality possible. This is especially true forthe measurement of T [55] and, in general, means using a high-quality radioimmunoassay (RIA)following sample extraction and chromatography, or the use of mass spectrometer with sampleseparation by liquid or gas chromatography. Currently used enzyme-linked immunosorbent orchemiluminescent assays have demonstrated poor sensitivity and specificity in females [55]Levels of serum androgens in females vary depending on age, day of menstrual cycle, and timeof sampling, and no standardization is provided based on these parameters [55]. Anotherissue related to the use of these assay kits lie in their cross-reactivity with similar steroid sub-stances [56].
Overall, total T levels are found to be elevated in 22% to 85% of PCOS patients as defined by theNational Institutes of Health (NIH) 1990 criteria, although most demonstrate that only one-third ofsamples demonstrate an abnormal value [57]. Approximately 70% of samples from PCOSwomen by theNIH 1990 criteria have elevated serum concentration levels of free T [57], which is the single mostsensitive test for hyperandrogenemia. Therefore, elevation of either total T or free T levels is a keydiagnostic feature of biochemical hyperandrogenism. Further, other androgens may be useful to thediagnosis of biochemical hyperandrogenism. The measurement of DHEAS, an androgenmetabolite andpro-androgen levels, reflects primarily adrenal androgen production. It is elevated in approximately25% of PCOS patients, although the diagnosis requires using age-related cut-off values, as DHEAS levelsdecrease with age. Furthermore, only 10% of PCOS patients demonstrate isolated DHEAS elevation [33].Androstenedione is elevated in 18% of PCOS women; however, in only 9% of cases were isolated ele-vations observed [18]. DHEAS circulates in abundance and is easily detected, because of its sulfatedgroup, by most commercial assays. Alternatively, A4 measurement has the same issues as T mea-surement. Overall, the addition of DHEAS and A4 measurement values when assessing patients withpossible hyperandrogenism increases the proportion of patients deemed “hyperandrogenic” by 10%each.
Of note, defining “abnormal” for the measurement of androgens has the same issues as whendefining the same for hirsutism (see earlier). Thus, the use of appropriate controls and the currentepidemiologic statistical testing is necessary to define a truly “normal” range and, therefore, whatis “abnormal” or excessive. Unfortunately, few laboratories do this, although we have reportedsuch an effort for the measurement of total T and free T by a high-quality RIA and a tandemmass spectrometry assay [58]. A final word on androgen measures in the circulation. Androgenmeasures are not a substitute for the clinical assessment of hyperandrogenism and, in fact,androgen measures are most useful in patients without overt or obvious clinical signs ofhyperandrogenism.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 9
Management of androgen excess
The management of AE in women generally focuses on treating the clinical consequences of theunderlying disorder. For example, patients need to be assessed and treated for anovulation andanovulatory bleeding or resultant infertility. Furthermore, patients may need to be evaluated andtreated for associated metabolic dysfunction, particularly those with PCOS. This section focuses ontreating dermatologic aspects of AE, including hirsutism, acne, and FPHL. One key fact regarding thetreatment of AE is that patients generally require combination therapy, combining not just medicationsbut mechanical approaches. Rare is the single agent that will treat a patient with clinical hyper-androgenism adequately.
Hirsutism
Our approach to managing hirsutism is based on the recommendations of the Androgen Excess andPCOS Society (AE-PCOS) [59] and the Endocrine Society [60], suitably modified by our extensiveexperience [18]. Initiation of treatment should be based on the patient's perception of the problem,rather than quantitative characteristics of hirsutism [60]. As noted earlier, approximately 70% of pa-tients with hirsutism defined by anmFG score >3 complain of being hirsute [39], and about one-half ofwomen with minimal hair growth (mFG 3e5) have PCOS [44]. The hirsutism score correlates poorlywith serum androgens [33]; therefore, monitoring of T and other androgens is generally unnecessary[61]. The choice of specific intervention depends on the patient's plan for pregnancy and the severity ofhirsutism [59].
Hirsutism is a sign, not a disease in and of itself; therefore, the underlying cause should beconsidered. PCOS is the most common etiology and is found in 72% to 82% of patients with AE [18].Treatment of clinical signs of hyperandrogenism primarily centers around the suppression of androgenproduction and/or action. The most useful medical treatment includes oral contraceptives (OCPs) andantiandrogen therapy, preferably in combination. Other useful therapies include topical and systemictreatments for acne (antibiotics, topical retinoids, isotretinoin, phototherapy, etc), topical treatmentsfor androgenic alopecia (minoxidil), and topical treatments for hirsutism (eflornithine). Finally,treatment of these hyperandrogenic signs necessities understanding and incorporating cosmeticmeans of treatment, including shaving, depilating, hair bleaching, electrolysis, laser hair removal, hairtransplantation, and others. Smoking cessation is strongly recommended for hirsute patients as many ofthe undesirable side effects of the medications prescribed to treat hirsutism are exacerbated whenpatients indulge this habit [59].
Androgen suppressionSuppression of androgen biosynthesis may be achieved by the use of hormonal contraceptives,
GnRH analogues, glucocorticoids, insulin sensitizers, and lifestyle modification.
Hormonal combination contraceptives. Progestins in hormonal combination contraceptives (HCCs) cau-ses suppression of LH levels and inhibition of LH-mediated ovarian androgen synthesis (Fig. 5) [62]. Theethinylestradiol in HCCs leads to a significant increase in SHBG, thereby contributing to a reduction offree T [63]. Moreover, HCCs modestly affect adrenal steroidogenesis by decreasing the synthesis andrelease of androgens [64]. Several progestins have antiandrogenic properties that can antagonize theAR and/or inhibit the activity of 5a-RA [64], although the amount found in HCCs alone is generallyinsufficient to mount a robust therapeutic response [60]. HCCs aremore effective than no treatment forhirsutism [65]. Therefore, approximately 60e100% of women with hirsutism demonstrate improve-ment on oral contraceptives [66]. This provides sufficient evidence to consider HCCs as monotherapyfor the treatment of hirsutism.
Several studies have demonstrated the superior efficiency of HCC monotherapy compared to fi-nasteride after 9 months of treatment [67], and this is comparable to GnRHa [68] and insulinsensitizer [69] therapy. There is some evidence that cyclical oral contraception (i.e., 21-day active/7-day placebo) provides better ovarian suppression (smaller ovarian volume and serum estrogens)
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
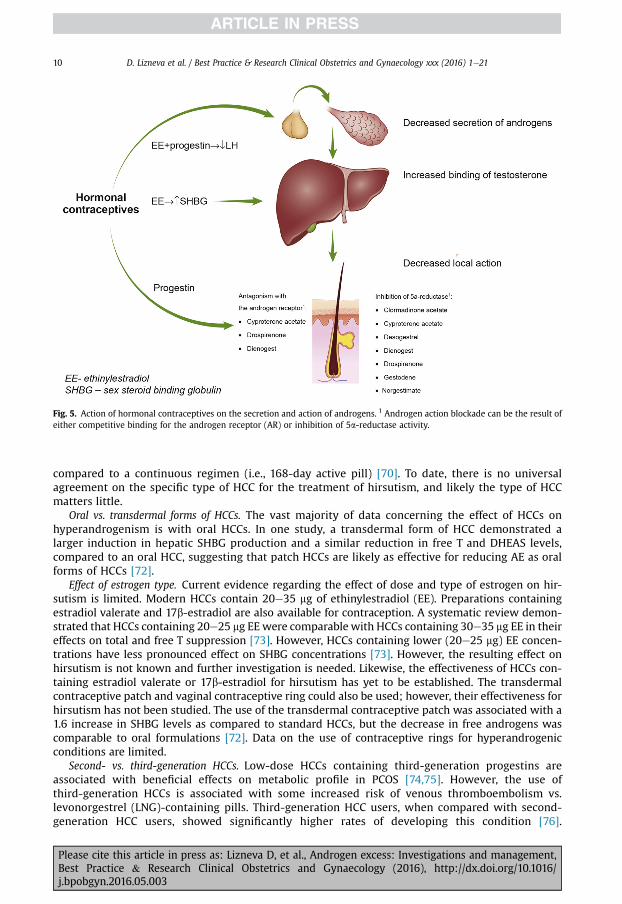
Fig. 5. Action of hormonal contraceptives on the secretion and action of androgens. 1 Androgen action blockade can be the result ofeither competitive binding for the androgen receptor (AR) or inhibition of 5a-reductase activity.
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e2110
compared to a continuous regimen (i.e., 168-day active pill) [70]. To date, there is no universalagreement on the specific type of HCC for the treatment of hirsutism, and likely the type of HCCmatters little.
Oral vs. transdermal forms of HCCs. The vast majority of data concerning the effect of HCCs onhyperandrogenism is with oral HCCs. In one study, a transdermal form of HCC demonstrated alarger induction in hepatic SHBG production and a similar reduction in free T and DHEAS levels,compared to an oral HCC, suggesting that patch HCCs are likely as effective for reducing AE as oralforms of HCCs [72].
Effect of estrogen type. Current evidence regarding the effect of dose and type of estrogen on hir-sutism is limited. Modern HCCs contain 20e35 mg of ethinylestradiol (EE). Preparations containingestradiol valerate and 17b-estradiol are also available for contraception. A systematic review demon-strated that HCCs containing 20e25 mg EE were comparable with HCCs containing 30e35 mg EE in theireffects on total and free T suppression [73]. However, HCCs containing lower (20e25 mg) EE concen-trations have less pronounced effect on SHBG concentrations [73]. However, the resulting effect onhirsutism is not known and further investigation is needed. Likewise, the effectiveness of HCCs con-taining estradiol valerate or 17b-estradiol for hirsutism has yet to be established. The transdermalcontraceptive patch and vaginal contraceptive ring could also be used; however, their effectiveness forhirsutism has not been studied. The use of the transdermal contraceptive patch was associated with a1.6 increase in SHBG levels as compared to standard HCCs, but the decrease in free androgens wascomparable to oral formulations [72]. Data on the use of contraceptive rings for hyperandrogenicconditions are limited.
Second- vs. third-generation HCCs. Low-dose HCCs containing third-generation progestins areassociated with beneficial effects on metabolic profile in PCOS [74,75]. However, the use ofthird-generation HCCs is associated with some increased risk of venous thromboembolism vs.levonorgestrel (LNG)-containing pills. Third-generation HCC users, when compared with second-generation HCC users, showed significantly higher rates of developing this condition [76].
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 11
Therefore second-generation HCCs could also be used for these purposes. A small randomizedcontrolled trial (RCT) of 47 women demonstrated that HCCs containing LNG were clinicallyeffective for the treatment of hirsutism [77]. However, there is limited data to demonstratethat second-generation HCCs are less effective in the reduction of serum androgens and the hir-sutism score [77]. Furthermore, HCCs containing LNG could worsen the metabolic profile in PCOSpatients [78].
HCCs with antiandrogenic progestins. Cyproterone acetate (CPA), chlormadinone acetate (CMA),drospirenone (DRSP), and dienogest (DNG) can be considered progestins with antiandrogenic prop-erties. HCCs containing DNG are available in combinationwith two types of estrogens, EE and estradiolvalerate. Comparative studies of HCCs containing progestins with antiandrogenic properties, however,are limited. Batukan et al. demonstrated comparable effects of HCCs containing CPA and DRSP withregard to the clinical signs of hirsutism after 12 months of therapy [79]. In contrast, another RCTdemonstrated that HCCs with DRSP were more effective in the reduction of clinical hyperandrogenismas compared to CMA-containing HCCs [80]. Yet, in a relatively recent RCT, Bhattacharya et al.demonstrated that after 12 months of treatment, use of HCCs containing CPA was associated with asignificant decrease in the mFG score as compared with HCCs containing both desogestrel (DSG) andDSP [81]. Another prospective RCT of 2 HCCs with DSG and CPA showed comparable effectiveness forhirsutism in adolescents with PCOS [82]. It is worthmentioning that these studies were relatively smallin size.
Risks and side effects of HCCs. Commonly reported side effects of HCCs include nausea, bloating,and mood changes, but these may decrease after several months of treatment [83]. Breakthroughbleeding is another significant side effect of HCCs leading to discontinuation. Data based on 1small RCT showed that third-generation progestogens demonstrate better bleeding patterns incomparison to second-generation preparations [84]. Third-generation HCCs and DRSP-containingHCCs are associated with an increased risk of thromboembolic events compared to second-generation HCCs within the general population [85,86]. These data are supported by recent asystematic review [87]. Reportedly, the use of HCCs increased the risk of developing venousthrombosis (relative risk [RR] 3.5, 95% confidence interval [CI] 2.9e4.3) [87]. The RR of venousthrombosis for low-dose third-generation HCCs containing progestins, or drospirenone, or CPAwere similar, and approximately 50% to 80% higher than for HCCs containing LNG. Higher doses ofEE in HCCs were associated with higher thrombosis risk [87]. Yet, the absolute risk of thrombo-embolism is low [86].
Gonadotropin-releasing hormone agonists (GnRH-a). Administration of GnRH-a leads to suppression ofgonadotropin secretion and, as a result, decreased ovarian androgen secretion. The use of GnRH-a isoften associated with estrogen deficiency and is usually prescribed in combination with estrogens.Data on the efficacy of GnRH-a in comparison with other methods of treatment are mixed. In twostudies, the use of GnRH-a in combination with estrogen was associated with better clinical out-comes compared to HCCs [88,89]. The use of a GnRH-a in combination with HCCs is less effectivethan in combination of antiandrogen and HCCs [90]. Given the cost of therapy and a wide range ofside effects, GnRH-a along with the necessity to combine it with estrogen therapy should bereserved for patients who cannot tolerate other treatments, or for those patients with theHyperandrogenic-insulin resistant-acanthosis nigricans (HAIRAN) syndrome [91].
Glucocorticoids. Glucocorticoids (GCs) are traditionally used for the treatment of hyperandrogenism inwomen with congenital adrenal hyperplasia. Two studies have demonstrated that GCs were moreeffective than HCCs or androgens in suppressing levels of adrenal androgens, but less effective for thetreatment of hirsutism. Therefore, routine treatment of hirsutism with GCs is not recommended [92].Even in patients with congenital adrenal hyperplasia, treatment of associated hirsutism should includethe use of an antiandrogen.
Insulin sensitizers and lifestyle modification. Insulin sensitizers and lifestyle modification may reducehair growth by indirectly reducing circulating insulin levels, which in turn will reduce ovarian theca
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e2112
stimulation. However, the overall effect is relatively modest. Overall, spironolactone and flutamide,and likely all antiandrogens, are superior to insulin sensitizers alone in the treatment of hirsutism[93].
Metformin. Metformin is an insulin sensitizer that not only has a favorable effect on insulin sensi-tivity, but also may reduce serum androgens [94e96]. However, a meta-analysis of 16 trials did notreveal a clinically significant difference in the reduction of the mFG score compared to placebo, andmetforminwas less effective compared to spironolactone and flutamide [94]. Althoughmetforminmayinfluence biochemical hyperandrogenism, it has a little effect on hirsutism and is not recommended forthe routine clinical treatment of hirsutism [59].
Troglitazone. The thiazolidinediones (TZDs) are a separate class of drugs that act to improve insulinresistance by acting on the PPARgamma receptor. Troglitazone, a TZD, was evaluated for its effect onhirsutism. Four hundred and ten PCOS women in a multicenter, double-blinded trial received placeboor troglitazone in different doses (150, 300, or 600 mg/day). There was a significant decrease in themFG score with 600 mg troglitazone as compared to placebo [97]. However, data on the use of TZDs inPCOS is limited [97,98] and, currently, these therapies are not recommended for the routine treatmentof hirsutism.
Weight loss. The prevalence and degree of hirsutism is higher among obese women with PCOS[99]. Abdominal obesity, associated with PCOS, leads to increased insulin levels, and reduced hepaticsynthesis of the SHBG [100]. This, in turn, causes an increase in free androgens concentration[99,101]. Insulin, moreover, has a direct impact on ovarian action [102,103] and functions as a co-gonadotropin [104], all of which contribute to biochemical hyperandrogenism. Some evidencesuggests that obesity itself may negatively impact the effects of pharmacologic treatments forhirsutism.
A systematic review of RCTs has shown that the effect of treatment was negatively associated withBMI in PCOS patients [105]. However, data regarding the effect of lifestyle modification on hirsutismare limited. A systematic review of six small RCTs observed that lifestyle modificationwas beneficial inthe reduction of serum androgens and increased SHBG, along with some improvement in hirsutism asevaluated by the mFG score [106].
Bariatric surgery is commonly used as a treatment modality in the advanced stages of obesity. In alongitudinal prospective non-randomized evaluation, a significant reduction in hirsutism score, serumandrogens, as well as improvement in insulin resistance (IR) and ovulatory function were observedafter surgery [107]. In some cases, obese womenwith PCOS were clinically cured after bariatric surgery[108]. However, the data regarding this approach are limited and this treatment option should bestrictly reserved for morbidly obese patients [109].
Androgen blockade
Antiandrogens in use generally include three AR blockers, spironolactone, flutamide and cyprot-erone acetate, and one 5a-RA inhibitor, finasteride. While there are other AR blockers and 5a-RA in-hibitors available, these have not been used with any regularity in women. Although the side effects ofantiandrogens vary somewhat, there are two side effects and risks that are common to all. First, allantiandrogens are teratogenic, in that they may cause feminization of the genitalia in a male fetus. Forthis reason, the use of antiandrogens alone is generally discouraged, unless they are used in a patientwith very secure contraception.
Second, they all have the potential to cause side effects related to their antiandrogenic properties,including some muscle weakness and decreased libido, although this varies greatly from patient topatient. In general, because efficacy is generally higher when using a combination of HCC and anti-androgens (see further), and because HCCs minimize the risk of teratogenicity, we generally begintherapy with a combination of HCCs and antiandrogens.
Antiandrogen monotherapyThe antiandrogens currently available for clinical use are spironolactone, CPA, finasteride, and
flutamide. RCTs using antiandrogens therapies were summarized in a systematic review [93]. In fivestudies, antiandrogen therapy (spironolactone, finasteride, and flutamide) was associated with a
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 13
reduction in mFG scores by 3.9 (95% CI, 2.3e5.4) as compared to placebo [96]. The comparative effi-ciency of antiandrogens is controversial. Some studies have not shown significant differences betweenantiandrogens on mFG scores [110e112], whereas other data demonstrated flutamide to be superior tospironolactone and CPA [90] and still other studies showed CPA and spironolactone to bemore effectivethan finasteride [67,113,114].
Combined treatment of antiandrogen with HCCsFour RCTs demonstrated that antiandrogens in combination with contraceptives were more
effective than monotherapy with HCCs [93]. These data were consistent with other publicationsdemonstrating that CPA, spironolactone, and flutamide when combined with HCCs showed a signifi-cant effect on hirsutism [105]. Of note, the addition of CPA to CPA-containing HCCs did not provideadditional benefit [93]. As indicated earlier, because efficacy is generally higher when using a com-bination of HCCs and antiandrogens, than with either HCC or antiandrogen monotherapy, and becauseHCCs minimize the risk of teratogenicity, we generally begin therapy with a combination of HCCs andantiandrogens.
Combined treatment of antiandrogen with metforminIn a relatively small RCT, flutamide in combination with metformin (4.6; CI, 1.3e7.9) appeared to be
superior to monotherapy [105].
Combined antiandrogensThe combined use of spironolactone and finasteride appears to be more clinically effective then
monotherapy with spironolactone [115], however, data on this are limited.
Cosmetic approaches
Cosmetic methods are widely used and can be categorized as short and long term [60]. Short-termmechanical methods include shaving, chemical depilation, plucking (threading), waxing, and bleach-ing; long-termmethods include electrolysis, laser therapy, and intense pulse light (IPL) therapy [60]. Inaddition, a 13.9% topical solution of eflornithine hydrochloride (HCL) can be used to reduce facial hairgrowth, although its effect is short term and requires daily use.
Eflornithine hydrochlorideDepending on accessibility and availability, in some countries, the topical use of 13.9% eflornithine
hydrochloride (HCL) is available for the treatment of facial hirsutism. This medication acts as per-manent inhibitor of enzyme ornithine decarboxylase, which is required for the growth and differ-entiation of cells in the hair follicle [116]. Topical administration of eflornithine HCL was shown toslow facial hair growth [116]. This action is reversible and hirsutism relapsed after 8 weeks ofcessation of treatment [116]. Percutaneous absorption of eflornithine is less than 1% [116]. Thegeneral use of eflornithine HCL is not approved for large surface areas of the skin due to systemiceffects; therefore, its use should be restricted to the removal of facial hair only. Treatment witheflornithine HCL has been found to significantly reduce the level of anxiety associated with hirsut-ism, as evaluated by the Bother Assessment in Skin Conditions (BASC) scale [71]. Two RCTsdemonstrated that eflornithine promotes a more rapid response to therapy when combined withlaser treatment [117,118].
Short-term cosmetic methods of hair removalDepilation is the removal of the hair shaft from the skin's surface and includes shaving and chemical
depilation. Conversely, epilation is the extraction of hair above the bulb (e.g., plucking, waxing) [60].Between these two methods, epilation provides the most long-lasting action on hair regrowth, withhair absent for 6e8 weeks [119]. If epilation is performed during the anagen phase, it could possiblydestroy the dermal papilla [120]. However, this effect is subtle and, compared with electrolysis,plucking is not as effective [121]. These methods are relatively safe and affordable. Side effects are rareand may include dermatitis with chemical epilation and bleaching; skin irritation with shaving and
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e2114
scarring; and folliculitis with epilation [60]. Despitewidespread opinion, shaving does not cause excesshair growth [60].
Long-term cosmetic methods of hair removal
Electrology. Electrolysis has been commonly used for the treatment of unwanted hair since 1875 [122].Galvanic electrolysis facilitates chemical destruction of the dermal papilla resulting in the long-termreduction of hirsutism. Thermolytic electrolysis induces heat injury of the hair follicle in the treatedarea. Currently available Blended electrolysis includes the synergetic application of both energies.
Data on the clinical effectiveness of electrolysis are limited. The blended effect of electrolysis wasshown to be more effective than plucking, and long-term hair removal was achieved in 9.9 sessions[122]. It is worth mentioning that shaving a few days before the procedure proved helpful as it allowedselective destruction of growing anagen hair [121]. Side effects associated with electrolysis includediscomfort, erythema, skin discoloration, and scarring. Application of local anesthetics has shown to beeffective in reducing the discomfort associated with this procedure [123]. However, electrolysis is lesssatisfactory as compared to intense pulsed light (IPL) [124]. A comparative study of 25 women un-dergoing hair removal at an NHS hospital showed patient satisfaction rates were 8.3 out of 10 for IPLand 5.4 out of 10 for electrolysis [124].
Laser therapy. Laser therapy is based on selective photothermolysis, wherein melanin of hairfollicles accumulate the light energy, which in turn destroys the hair bulb [125]. Several laserswith varying wavelengths are available for hair removal: ruby, alexandrite, diode, and the neo-dymium:yttriumealuminiumegarnet (Nd:YAG) [125]. Darker skin types are usually more difficultto treat using photoepilation. In this case, light energy is absorbed by the surrounding epidermis ofthe hair follicle, which makes the procedure less effective and could be associated with skindiscoloration and burns [126]. Therefore, the Nd-YAG laser, which has a longer wavelength, is thepreferred treatment for patients with darker skin [127]. A Cochrane systematic review showed analmost 50% hair reduction in a period of 6 months after treatment with alexandrite and diode lasersand limited evidence of effectiveness with other lasers [128]. However, in another systematic re-view, conducted by Haedersdal and Wulf, efficacy was shown to extend beyond 6 months aftertreatment with alexandrite, diode lasers and possibly with ruby and Nd:YAG lasers [129]. The dataon the long-term (9 months) efficacy after treatment are available only for alexandrite lasers [130].Typically, four to six treatments are required to achieve a desired effect. Use of the alexandrite lasershowed 55% hair reduction after the third treatment [130]. Maintenance therapy is recommendedevery 6 to 12 months. Lasers are associated with local complications such as scarring and skindiscoloration, and also can cause reticulate erythema and uveitis [126,127,129]. In rare cases, thistreatment has been associated with paradoxical hypertrichosis [131].
Intense pulsed light. Data regarding IPL efficacy are limited [129]. It is shown to be superior to the rubylaser, similar to the Nd:YAG laser, and less effective as compared to diode laser therapy [132e134] IPLswith radiofrequency can be used inwomenwith blond hair and light skin, when lasers are not effective.In addition, IPLs are associated with less risk of burning in patients with darker skin types. However, fordarker skin in an assessor-blinded comparison, the Nd:YAG laser was more effective than the IPL [135].Evidence of the long-term effects of IPL treatment are lacking [128,129]. Side effects of IPL are similar tothose in lasers.
Acne
As discussed earlier, acne secondary to AE will benefit from androgen suppression. The EndocrineSociety recommends the use of HCCs as the first-line intervention in the acneic hyperandrogenic pa-tient [19]. HCCs are more effective than placebo, as shown in 9 RCTs included in the Cochrane sys-tematic review [136]. In addition, HCCsmay contain antiandrogenic progestins (chlormadinone acetateor CPA), which appears to be more effective than LNG-containing HCCs for the treatment of acne [136].Alternatively, the use of progestin-only contraception: pills, devices, or injectable forms could
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 15
aggravate the development of acne and are, therefore, not recommended [137]. In acneic patients withadrenal hyperplasia, treatment of GCs also improves their acne. Alternatively, there are conflicting dataregarding the efficacy of antiandrogens on acne [138e140].
Several studies, including an RCT, demonstrated the efficiency of topical agents (i.e., topical benzoylperoxide and retinoids) in the treatment of inflammatory acne [141,142]. Oral antibiotics are alsoeffective for moderate to severe inflammatory acne, or for truncal location of lesions [143]. Oral iso-tretinoin is the only agent that has demonstrated maximum clinical effectiveness for all forms of acne[144]. It is currently reserved for severe, nodular acne, in cases of scarring, and for milder formsresistant to other treatments [48].
Female pattern hair loss
The mainstay or first-line treatment of FPHL is 2% topical minoxidil [52]. The use of 1 mL minoxidiltopically to the scalp skin and hair twice daily is recommended for FPHL. A Cochrane systematic reviewand meta-analysis observed superior efficacy for minoxidil as compared to placebo for FPHL [145].Despite some evidence of greater efficiency for a 5% solution of minoxidil, its use is associated with anincreased rate of side effects, including facial hypertrichosis [146]. Treatment efficacy should be re-evaluated after 6 months and patients should be cautioned against possible increased shedding dur-ing the first 2 months of therapy [52].
Other treatment modalities include the use of androgen suppression in combinationwith androgenblockade, laser and light treatments, the use of prostaglandin analogs, and hair transplantation. Dataon the use of systemic antiandrogens (chlormadinone acetate, drosperinone, spironolactone, andflutamide) in women with FPHL is insufficient for routine use [145]. However, in one study, the use oforal CPA was associated with improved androgenic alopecia in a subgroup of female patients withhyperandrogenism [147] and may be reserved as second-line treatment for FPHL in these women [52].In case medical therapy is not sufficiently effective, follicular unit transplantation is a possible optionfor female patients with sufficient residual hair [148].
Follow-up and prognosis
The effectiveness of therapy should be monitored at least 6 months after treatment [92]. For hir-sutism, effective treatment is associated with a reduction in the frequency of cosmetic hair removal(e.g., waxing, depilation, shaving) as well as a lowered mFG score [92]. As hirsutism scores do notcorrelate well with androgen levels [61], monitoring of serum androgens during treatment is notrecommended [60,92].
Treatment of hirsutism takes time and an absolute cure is rarely possible, whereas cessation ofmedical therapy may lead to a relapse in symptoms [149].
Therapies for most causes of androgen excess are lifelong [150]. However, we should note that themajority of studies assessing the efficacy of medical treatment for clinical hyperandrogenism havebeen of only 6 or 12 months duration; therefore, it is unclear how long treatment should or can beused [151]. The majority of experts recommend lifelong treatment [59]. However, we tend to try andtreat patients with maximum suppression for approximately 2 years and then, depending on pro-gression of hair growth and amelioration in the mFG score, we may suggest decreasing or evenstopping antiandrogen use, while continuing oral contraceptive use. In our experience, approxi-mately 50% of patients so treated are able to remainwell controlled by oral contraceptive suppressionalone.
Generally, acne responds to therapy relatively rapidly, and improvements can be observedwithin the first month of effective therapy. Hirsutism, alternatively, is slower to respond, due tothe longer growth cycle of the hair, and improvements may be observed as early as 3 months, butgenerally only after 6 or 8 months of therapy. Finally, FPHL is the slowest to respond to therapy,if it will at all, and it may take 12 to 18 months of therapy before a response is begun to beobserved.
Once medical therapy begins, a follow-up visit should be scheduled at least 1 month after the initialtreatment visit to evaluate for side effects and reinforce the treatment plan. Follow-up thereafter can be
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e2116
every 3 to 6 months until the patient's condition is stable. Once treatment responses are stable, annualvisits are appropriate. If the patient has PCOS, then monitoring and treatment for metabolic compli-cations is also necessary. Thus, the burden of care for the treating physician has increased beyond thatof solely treating the presenting complaint to include the detection and, if possible, prevention of thesemetabolic consequences [2,152].
Practice points
� Clinically evident hyperandrogenism results in hirsutism, acne, and androgenic alopecia.� The modified FerrimaneGallwey visual scoring system is currently considered the “gold”standard for the clinical evaluation of hirsutism.
� There is no universally excepted evaluation system for acne; several global assessmentscales have been offered.
� The pattern of hair loss on the scalp is usually assessed using the Ludwig scale; however,there is no universally accepted evaluation tool.
� Biochemical hyperandrogenism should be assessed by measuring total T and free T using ahigh-quality RIA or a tandem mass spectrometry assay.
� Treatment of hirsutism includes:✓ Topical eflornithine hydrochloride for mild facial hirsutism✓ Electrolysis for localized hirsutism in combination with pharmacological suppression✓ Lasers for generalized hirsutism in combination with pharmacological suppression✓ Low-dose neutral or antiandrogenic HCCs as first-line monotherapy for women with mild
hirsutism, or in combination with antiandrogens for women with moderate or severehirsutism
✓ Metformin or other insulin sensitizers, glucocorticoids, and GnRH analogues for thetreatment of clinical hyperandrogenism is not routinely recommended.
� Treatment of acne due to hyperandrogenism includes:✓ Topical astringents, or topical or oral antibiotics, as a first-line intervention✓ Topical retinoids✓ HCCs✓ Phototherapy✓ Oral isotretinoin, currently reserved for severe nodular acne, in cases of scarring, and for
milder forms proven resistant to other treatments� Treatment of FPHL includes:✓ 2% Topical minoxidil, as first-line therapy✓ 5a-reductase inhibition, as adjunct therapy✓ Other treatment modalities, including androgen suppression in combination with
androgen blockade, laser and light treatments, the use of prostaglandin analogs✓ Hair transplantation
� Therapies for most causes of androgen excess require lifelong intervention.
Research agenda
� Validated methods for acne evaluation� Validated methods for FPHL evaluation� Well-designed studies to evaluate the best medical therapy for hirsutism, acne, and alopeciain hyperandrogenic patient
� Well-designed studies to compare the effect of different HCC formulations on signs andfeatures of clinical hyperandrogenism
� Duration and prognosis of pharmacological interventions for androgen excess
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 17
Conflict of interest statement
DL, LGJ, and WW, have no conflicts of interest to declare. RA is a consultant for KinDexPharmaceuticals.
References
[1] Stocco DM, Clark BJ. Regulation of the acute production of steroids in steroidogenic cells. Endocr Rev 1996;17(3):221e44.
[2] Azziz R, Nestler JE, Dewailly D. Androgen excess disorders in women: polycystic ovary syndrome and other disorders.2nd ed. Totowa, N.J: Humana Press; 2006. xviii, 466 pp.
[3] Pandey AV, Miller WL. Regulation of 17,20 lyase activity by cytochrome b5 and by serine phosphorylation ofP450c17. J Biol Chem 2005;280(14):13265e71.
[4] Auchus RJ, Lee TC, Miller WL. Cytochrome b5 augments the 17,20-lyase activity of human P450c17 without directelectron transfer. J Biol Chem 1998;273(6):3158e65.
[5] Franchimont P. Regulation of gonadal androgen secretion. Horm Res 1983;18(1e3):7e17.[6] Wu L, Einstein M, Geissler WM, et al. Expression cloning and characterization of human 17 beta-hydroxysteroid
dehydrogenase type 2, a microsomal enzyme possessing 20 alpha-hydroxysteroid dehydrogenase activity. J BiolChem 1993;268(17):12964e9.
[7] Fassnacht M, Schlenz N, Schneider SB, et al. Beyond adrenal and ovarian androgen generation: increased peripheral 5alpha-reductase activity in women with polycystic ovary syndrome. J Clin Endocr Metab 2003;88(6):2760e6.
[8] Miller WL. Molecular biology of steroid hormone synthesis. Endocr Rev 1988;9(3):295e318.[9] Moran C, Knochenhauer E, Boots LR, et al. Adrenal androgen excess in hyperandrogenism: relation to age and body
mass. Fertil Steril 1999;71(4):671e4.[10] Deplewski D, Rosenfield RL. Role of hormones in pilosebaceous unit development. Endocr Rev 2000;21(4):363e92.[11] Roy AK, Tyagi RK, Song CS, et al. Androgen receptor: structural domains and functional dynamics after ligand-receptor
interaction. Ann N Y Acad Sci 2001;949:44e57.[12] Longcope C. Adrenal and gonadal androgen secretion in normal females. Clin Endocrinol Metab 1986;15(2):213e28.[13] Taieb J, Mathian B, Millot F, et al. Testosterone measured by 10 immunoassays and by isotope-dilution gas
chromatography-mass spectrometry in sera from 116 men, women, and children. Clin Chem 2003;49(8):1381e95.[14] Chen MJ, Yang WS, Yang JH, et al. Low sex hormone-binding globulin is associated with low high-density lipoprotein
cholesterol and metabolic syndrome in women with PCOS. Hum Reprod 2006;21(9):2266e71.[15] Parker Jr CR, Slayden SM, Azziz R, et al. Effects of aging on adrenal function in the human: responsiveness and
sensitivity of adrenal androgens and cortisol to adrenocorticotropin in premenopausal and postmenopausal women.J Clin Endocrinol Metab 2000;85(1):48e54.
[16] Moll Jr GW, Rosenfield RL. Testosterone binding and free plasma androgen concentrations under physiological con-ditons: chararacterization by flow dialysis technique. J Clin Endocrinol Metab 1979;49(5):730e6.
[17] Juricskay S, Telegdy E. Urinary steroids in women with androgenic alopecia. Clin Biochem 2000;33(2):97e101.*[18] Azziz R, Sanchez LA, Knochenhauer ES, et al. Androgen excess in women: experience with over 1000 consecutive
patients. J Clin Endocrinol Metab 2004;89(2):453e62.[19] Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine
Society clinical practice guideline. J Clin Endocrinol Metab 2013;98(12):4565e92.[20] Fruzzetti F, De Lorenzo D, Ricci C, et al. Ovarian influence on adrenal androgen secretion in polycystic ovary syndrome.
Fertil Steril 1995;63(4):734e41.[21] Azziz R. Reproductive endocrinologic alterations in female asymptomatic obesity. Fertil Steril 1989;52(5):703e25.[22] Ehrmann DA, Barnes RB, Rosenfield RL. Polycystic ovary syndrome as a form of functional ovarian hyperandrogenism
due to dysregulation of androgen secretion. Endocr Rev 1995;16(3):322e53.[23] Brennan K, Huang A, Azziz R. Dehydroepiandrosterone sulfate and insulin resistance in patients with polycystic ovary
syndrome. Fertil Steril 2009;91(5):1848e52.[24] Landay M, Huang A, Azziz R. Degree of hyperinsulinemia, independent of androgen levels, is an important deter-
minant of the severity of hirsutism in PCOS. Fertil Steril 2009;92(2):643e7.[25] Ovalle F, Azziz R. Insulin resistance, polycystic ovary syndrome, and type 2 diabetes mellitus. Fertil Steril 2002;77(6):
1095e105.[26] Kumar A, Bartolucci AA, Azziz R. Prevalence of adrenal androgen excess in patients with the polycystic ovary syn-
drome (PCOS) using age-specific DHEAS levels adjusted for body mass and ethnicity. Fertil Steril 2003;80. S46-9.[27] Kosus N, Kosus A, Kamalak Z, et al. Impact of adrenal versus ovarian androgen ratio on signs and symptoms of
polycystic ovarian syndrome. Gynecol Endocrinol 2012;28(8):611e4.[28] Rosenfield RL. Pilosebaceous physiology in relation to hirsutism and acne. Clin Endocrinol Metab 1986;15(2):341e62.[29] Randall VA. Androgens and human hair growth. Clin Endocrinol (Oxf) 1994;40(4):439e57.[30] Rosenfield RL. Hirsutism and the variable response of the pilosebaceous unit to androgen. J Investig Dermatol Symp
Proc 2005;10(3):205e8.[31] Carmina E, Rosato F, Janni A, et al. Extensive clinical experience: relative prevalence of different androgen excess
disorders in 950 women referred because of clinical hyperandrogenism. J Clin Endocrinol Metab 2006;91(1):2e6.[32] Carmina E. The spectrum of androgen excess disorders. Fertil Steril 2006;85(6):1582e5.[33] Huang A, Landay M, Azziz R. The association of androgen levels with the severity of hirsutism in the polycystic ovary
syndrome (PCOS). Fertil Steril 2006;86. S12eS.[34] Goodarzi MO, Carmina E, Azziz R. DHEA, DHEAS and PCOS. J Steroid Biochem 2015;145:213e25.[35] Slayden SM, Moran C, Sams Jr WM, et al. Hyperandrogenemia in patients presenting with acne. Fertil Steril 2001;
75(5):889e92.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e2118
[36] Venning VA, Dawber RP. Patterned androgenic alopecia in women. J Am Acad Dermatol 1988;18(5 Pt 1):1073e7.[37] Cela E, Robertson C, Rush K, et al. Prevalence of polycystic ovaries in women with androgenic alopecia. Eur J Endo-
crinol 2003;149(5):439e42.[38] Yildiz BO, Bolour S, Woods K, et al. Visually scoring hirsutism. Hum Reprod Update 2010;16(1):51e64.[39] DeUgarte CM, Woods KS, Bartolucci AA, et al. Degree of facial and body terminal hair growth in unselected black and
white women: toward a populational definition of hirsutism. J Clin Endocrinol Metab 2006;91(4):1345e50.[40] Cheewadhanaraks S, Peeyananjarassri K, Choksuchat C. Clinical diagnosis of hirsutism in Thai women. J Med Assoc
Thai 2004;87(5):459e63.[41] Moran C, Tena G, Moran S, et al. Prevalence of polycystic ovary syndrome and related disorders in Mexican women.
Gynecol Obstet Invest 2010;69(4):274e80.[42] Flegal KM, Carroll MD, Kit BK, et al. Prevalence of obesity and trends in the distribution of body mass index among US
adults, 1999e2010. JAMA 2012;307(5):491e7.[43] Zhao X, Ni R, Li L, et al. Defining hirsutism in Chinese women: a cross-sectional study. Fertil Steril 2011;96(3):792e6.[44] Souter I, Sanchez LA, Perez M, et al. The prevalence of androgen excess among patients with minimal unwanted hair
growth. Am J Obstet Gynecol 2004;191(6):1914e20.[45] Knochenhauer ES, Key TJ, Kahsar-Miller M, et al. Prevalence of the polycystic ovary syndrome in unselected black and
white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab 1998;83(9):3078e82.[46] Kim JJ, Chae SJ, Choi YM, et al. Assessment of hirsutism among Korean women: results of a randomly selected sample
of women seeking pre-employment physical check-up. Hum Reprod 2011;26(1):214e20.[47] Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from a Global Alliance to Improve Outcomes in
Acne. J Am Acad Dermatol 2003;49(1 Suppl):S1e37.[48] Nast A, Dreno B, Bettoli V, et al. European evidence-based (S3) guidelines for the treatment of acne. J Eur Acad
Dermatol Venereol 2012;26(Suppl 1):1e29.[49] Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J
Dermatol 1977;97(3):247e54.[50] Olsen EA. Current and novel methods for assessing efficacy of hair growth promoters in pattern hair loss. J Am Acad
Dermatol 2003;48(2):253e62.[51] Olsen EA, Messenger AG, Shapiro J, et al. Evaluation and treatment of male and female pattern hair loss. J Am Acad
Dermatol 2005;52(2):301e11.[52] Blumeyer A, Tosti A, Messenger A, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in
women and in men. J Dtsch Dermatol Ges 2011;9(Suppl 6):S1e57.[53] Durdiakova J, Fabryova H, Koborova I, et al. The effects of saliva collection, handling and storage on salivary testos-
terone measurement. Steroids 2013;78(14):1325e31.[54] Callow NH, Callow RK. The isolation of 17-ketosteroids from the urine of normal women. Biochem J 1939;33(6):931e4.*[55] Rosner W, Auchus RJ, Azziz R, et al. Position statement: Utility, limitations, and pitfalls in measuring testosterone: an
Endocrine Society position statement. J Clin Endocrinol Metab 2007;92(2):405e13.[56] Stanczyk FZ, Lee JS, Santen RJ. Standardization of steroid hormone assays: why, how, and when? Cancer Epidemiol
Biomarkers Prev 2007;16(9):1713e9.*[57] Azziz R, Carmina E, Dewailly D, et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syn-
drome: the complete task force report. Fertil Steril 2009;91(2):456e88.[58] Salameh WA, Redor-Goldman MM, Clarke NJ, et al. Specificity and predictive value of circulating testosterone assessed
by tandem mass spectrometry for the diagnosis of polycystic ovary syndrome by the National Institutes of Health1990 criteria. Fertil Steril 2014;101(4).
[59] Escobar-Morreale HF, Carmina E, Dewailly D, Gambineri A, Kelestimur F, Moghetti P, Pugeat M, Qiao J, Wijeyaratne CN,Witchel SF, Norman RJ. Epidemiology, diagnosis and management of hirsutism: a consensus statement by theAndrogen Excess and Polycystic Ovary Syndrome Society. Hum Reprod Update 2012;18(2):146e70.
[60] Martin KA, Chang RJ, Ehrmann DA, et al. Evaluation and treatment of hirsutism in premenopausal women: AnEndocrine Society clinical practice guideline. J Clin Endocrinol Metab 2008;93(4):1105e20.
[61] Legro RS, Schlaff WD, Diamond MP, et al. Total testosterone assays in women with polycystic ovary syndrome: pre-cision and correlation with hirsutism. J Clin Endocrinol Metab 2010;95(12):5305e13.
[62] Archer DF, Kovalevsky G, Ballagh SA, et al. Ovarian activity and safety of a novel levonorgestrel/ethinyl estradiolcontinuous oral contraceptive regimen. Contraception 2009;80(3):245e53.
[63] Vrbikova J, Cibula D. Combined oral contraceptives in the treatment of polycystic ovary syndrome. Hum ReprodUpdate 2005;11(3):277e91.
[64] Madden JD, Milewich L, Parker Jr CR, et al. The effect of oral contraceptive treatment on the serum concentration ofdehydroisoandrosterone sulfate. Am J Obstet Gynecol 1978;132(4):380e4.
[65] Porcile A, Gallardo E. Long-term treatment of hirsutism: desogestrel compared with cyproterone acetate in oralcontraceptives. Fertil Steril 1991;55(5):877e81.
[66] Burkman Jr RT. The role of oral contraceptives in the treatment of hyperandrogenic disorders. Am J Med 1995;98(1A):130Se6S.
[67] Sahin Y, Bayram F, Kelestimur F, et al. Comparison of cyproterone acetate plus ethinyl estradiol and finasteride in thetreatment of hirsutism. J Endocrinol Invest 1998;21(6):348e52.
[68] Heiner JS, Greendale GA, Kawakami AK, et al. Comparison of a gonadotropin-releasing hormone agonist and a lowdose oral contraceptive given alone or together in the treatment of hirsutism. J Clin Endocrinol Metab 1995;80(12):3412e8.
[69] Costello M, Shrestha B, Eden J, et al. Insulin-sensitising drugs versus the combined oral contraceptive pill for hirsutism,acne and risk of diabetes, cardiovascular disease, and endometrial cancer in polycystic ovary syndrome. CochraneDatabase Syst Rev 2007;(1):CD005552.
[70] Legro RS, Pauli JG, Kunselman AR, et al. Effects of continuous versus cyclical oral contraception: a randomizedcontrolled trial. J Clin Endocrinol Metab 2008;93(2):420e9.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003

D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 19
[71] Jackson J, Caro JJ, Caro G, et al. The effect of eflornithine 13.9% cream on the bother and discomfort due to hirsutism.Int J Dermatol 2007;46(9):976e81.
[72] White T, Jain JK, Stanczyk FZ. Effect of oral versus transdermal steroidal contraceptives on androgenic markers. Am JObstet Gynecol 2005;192(6):2055e9.
[73] Zimmerman Y, Eijkemans MJ, Coelingh Bennink HJ, et al. The effect of combined oral contraception on testosteronelevels in healthy women: a systematic review and meta-analysis. Hum Reprod Update 2014;20(1):76e105.
[74] Lemay A, Dodin S, Turcot L, et al. Rosiglitazone and ethinyl estradiol/cyproterone acetate as single and combinedtreatment of overweight women with polycystic ovary syndrome and insulin resistance. Hum Reprod 2006;21(1):121e8.
[75] Luque-Ramirez M, Alvarez-Blasco F, Botella-Carretero JI, et al. Comparison of ethinyl-estradiol plus cyproterone ac-etate versus metformin effects on classic metabolic cardiovascular risk factors in women with the polycystic ovarysyndrome. J Clin Endocrinol Metab 2007;92(7):2453e61.
[76] Kemmeren JM, Algra A, Grobbee DE. Third generation oral contraceptives and risk of venous thrombosis: meta-analysis. BMJ 2001;323(7305):131e4.
[77] Breitkopf DM, Rosen MP, Young SL, et al. Efficacy of second versus third generation oral contraceptives in the treat-ment of hirsutism. Contraception 2003;67(5):349e53.
[78] Bozdag G, Yildiz BO. Combined oral contraceptives in polycystic ovary syndrome e indications and cautions. FrontHorm Res 2013;40:115e27.
[79] Batukan C, Muderris II, Ozcelik B, et al. Comparison of two oral contraceptives containing either drospirenone orcyproterone acetate in the treatment of hirsutism. Gynecol Endocrinol 2007;23(1):38e44.
[80] Lello S, Primavera G, Colonna L, et al. Effects of two estroprogestins containing ethynilestradiol 30 microg and dro-spirenone 3 mg and ethynilestradiol 30 microg and chlormadinone 2 mg on skin and hormonal hyperandrogenicmanifestations. Gynecol Endocrinol 2008;24(12):718e23.
[81] Bhattacharya SM, Jha A. Comparative study of the therapeutic effects of oral contraceptive pills containing desogestrel,cyproterone acetate, and drospirenone in patients with polycystic ovary syndrome. Fertil Steril 2012;98(4):1053e9.
[82] Mastorakos G, Koliopoulos C, Creatsas G. Androgen and lipid profiles in adolescents with polycystic ovary syndromewho were treated with two forms of combined oral contraceptives. Fertil Steril 2002;77(5):919e27.
[83] Rosenberg MJ, Waugh MS, Meehan TE. Use and misuse of oral contraceptives: risk indicators for poor pill taking anddiscontinuation. Contraception 1995;51(5):283e8.
[84] Lawrie TA, Helmerhorst FM, Maitra NK, et al. Types of progestogens in combined oral contraception: effectiveness andside-effects. Cochrane Database Syst Rev 2011;(5):CD004861.
[85] Vandenbroucke JP, Rosing J, Bloemenkamp KW, et al. Oral contraceptives and the risk of venous thrombosis. N Engl JMed 2001;344(20):1527e35.
*[86] Domecq JP, Prutsky G, Mullan RJ, et al. Adverse effects of the common treatments for polycystic ovary syndrome: asystematic review and meta-analysis. J Clin Endocrinol Metab 2013;98(12):4646e54.
[87] Stegeman BH, de Bastos M, Rosendaal FR, et al. Different combined oral contraceptives and the risk of venousthrombosis: systematic review and network meta-analysis. BMJ 2013;347:f5298.
[88] Azziz R, Ochoa TM, Bradley Jr EL, et al. Leuprolide and estrogen versus oral contraceptive pills for the treatment ofhirsutism: a prospective randomized study. J Clin Endocrinol Metab 1995;80(12):3406e11.
[89] Elkind-Hirsch KE, Anania C, Mack M, et al. Combination gonadotropin-releasing hormone agonist and oral contra-ceptive therapy improves treatment of hirsute women with ovarian hyperandrogenism. Fertil Steril 1995;63(5):970e8.
[90] Pazos F, Escobar-Morreale HF, Balsa J, et al. Prospective randomized study comparing the long-acting gonadotropin-releasing hormone agonist triptorelin, flutamide, and cyproterone acetate, used in combination with an oral con-traceptive, in the treatment of hirsutism. Fertil Steril 1999;71(1):122e8.
[91] Azziz R. The hyperandrogenic-insulin-resistant acanthosis nigricans syndrome: therapeutic response. Fertil Steril1994;61(3):570e2.
*[92] Escobar-Morreale HF. Diagnosis and management of hirsutism. Ann N Y Acad Sci 2010;1205:166e74.*[93] Swiglo BA, Cosma M, Flynn DN, et al. Clinical review: antiandrogens for the treatment of hirsutism: a systematic
review and metaanalyses of randomized controlled trials. J Clin Endocrinol Metab 2008;93(4):1153e60.[94] Cosma M, Swiglo BA, Flynn DN, et al. Clinical review: insulin sensitizers for the treatment of hirsutism: a systematic
review and metaanalyses of randomized controlled trials. J Clin Endocrinol Metab 2008;93(4):1135e42.[95] Viollet B, Guigas B, Sanz Garcia N, et al. Cellular and molecular mechanisms of metformin: an overview. Clin Sci (Lond)
2012;122(6):253e70.*[96] Moghetti P, Tosi F, Tosti A, et al. Comparison of spironolactone, flutamide, and finasteride efficacy in the treatment of
hirsutism: a randomized, double blind, placebo-controlled trial. J Clin Endocrinol Metab 2000;85(1):89e94.[97] Azziz R, Ehrmann D, Legro RS, et al. Troglitazone improves ovulation and hirsutism in the polycystic ovary syndrome:
a multicenter, double blind, placebo-controlled trial. J Clin Endocrinol Metab 2001;86(4):1626e32.[98] Aroda VR, Ciaraldi TP, Burke P, et al. Metabolic and hormonal changes induced by pioglitazone in polycystic ovary
syndrome: a randomized, placebo-controlled clinical trial. J Clin Endocrinol Metab 2009;94(2):469e76.[99] Kiddy DS, Sharp PS, White DM, et al. Differences in clinical and endocrine features between obese and non-obese
subjects with polycystic ovary syndrome: an analysis of 263 consecutive cases. Clin Endocrinol (Oxf) 1990;32(2):213e20.
[100] Pasquali R. Obesity and androgens: facts and perspectives. Fertil Steril 2006;85(5):1319e40.[101] Ezeh U, Pall M, Mathur R, et al. Association of fat to lean mass ratio with metabolic dysfunction in women with
polycystic ovary syndrome. Hum Reprod 2014;29(7):1508e17.[102] Nestler JE, Jakubowicz DJ. Decreases in ovarian cytochrome P450c17 alpha activity and serum free testosterone after
reduction of insulin secretion in polycystic ovary syndrome. N Engl J Med 1996;335(9):617e23.[103] McGee E, Sawetawan C, Bird I, et al. The effects of insulin on 3 beta-hydroxysteroid dehydrogenase expression in
human luteinized granulosa cells. J Soc Gynecol Investig 1995;2(3):535e41.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e2120
[104] Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited: an update onmechanisms and implications. Endocr Rev 2012;33(6):981e1030.
[105] Koulouri O, Conway GS. A systematic review of commonly used medical treatments for hirsutism in women. ClinEndocrinol (Oxf) 2008;68(5):800e5.
[106] Moran LJ, Hutchison SK, Norman RJ, et al. Lifestyle changes in women with polycystic ovary syndrome. CochraneDatabase Syst Rev 2011;(7):CD007506.
[107] Escobar-Morreale HF, Botella-Carretero JI, Alvarez-Blasco F, et al. The polycystic ovary syndrome associated withmorbid obesity may resolve after weight loss induced by bariatric surgery. J Clin Endocrinol Metab 2005;90(12):6364e9.
[108] Eid GM, Cottam DR, Velcu LM, et al. Effective treatment of polycystic ovarian syndrome with Roux-en-Y gastric bypass.Surg Obes Relat Dis 2005;1(2):77e80.
[109] Legro RS. Obesity and PCOS: implications for diagnosis and treatment. Semin Reprod Med 2012;30(6):496e506.[110] Wong IL, Morris RS, Chang L, et al. A prospective randomized trial comparing finasteride to spironolactone in the
treatment of hirsute women. J Clin Endocrinol Metab 1995;80(1):233e8.[111] Grigoriou O, Papadias C, Konidaris S, et al. Comparison of flutamide and cyproterone acetate in the treatment of
hirsutism: a randomized controlled trial. Gynecol Endocrinol 1996;10(2):119e23.[112] Fruzzetti F, Bersi C, Parrini D, et al. Treatment of hirsutism: comparisons between different antiandrogens with central
and peripheral effects. Fertil Steril 1999;71(3):445e51.[113] Unluhizarci K, Karaca Z, Kelestimur F. Hirsutism e from diagnosis to use of antiandrogens. Front Horm Res 2013;40:
103e14.[114] Erenus M, Yucelten D, Durmusoglu F, et al. Comparison of finasteride versus spironolactone in the treatment of
idiopathic hirsutism. Fertil Steril 1997;68(6):1000e3.[115] Kelestimur F, Everest H, Unluhizarci K, et al. A comparison between spironolactone and spironolactone plus finasteride
in the treatment of hirsutism. Eur J Endocrinol 2004;150(3):351e4.[116] Wolf Jr JE, Shander D, Huber F, et al. Randomized, double-blind clinical evaluation of the efficacy and safety of topical
eflornithine HCl 13.9% cream in the treatment of women with facial hair. Int J Dermatol 2007;46(1):94e8.[117] Smith SR, Piacquadio DJ, Beger B, et al. Eflornithine cream combined with laser therapy in the management of un-
wanted facial hair growth in women: a randomized trial. Dermatol Surg 2006;32(10):1237e43.[118] Hamzavi I, Tan E, Shapiro J, et al. A randomized bilateral vehicle-controlled study of eflornithine cream combined with
laser treatment versus laser treatment alone for facial hirsutism in women. J Am Acad Dermatol 2007;57(1):54e9.[119] Ramos-e-Silva M, de Castro MC, Carneiro Jr LV. Hair removal. Clin Dermatol 2001;19(4):437e44.[120] Olsen EA. Methods of hair removal. J Am Acad Dermatol 1999;40(2 Pt 1):143e55. quiz 56e7.[121] Urushibata O, Kase K. A comparative study of axillar hair removal in women: plucking versus the blend method.
J Dermatol 1995;22(10):738e42.[122] Richards RN, Meharg GE. Electrolysis: observations from 13 years and 140,000 hours of experience. J Am Acad Der-
matol 1995;33(4):662e6.[123] Wanitphakdeedecha R, Alster TS. Physical means of treating unwanted hair. Dermatol Ther 2008;21(5):392e401.[124] Harris K, Ferguson J, Hills S. A comparative study of hair removal at an NHS hospital: Luminette intense pulsed light
versus electrolysis. J Dermatolog Treat 2014;25(2):169e73.[125] Liew SH. Laser hair removal: guidelines for management. Am J Clin Dermatol 2002;3(2):107e15.[126] Goldberg DJ. Laser- and light-based hair removal: an update. Expert Rev Med Devices 2007;4(2):253e60.[127] Tanzi EL, Lupton JR, Alster TS. Lasers in dermatology: four decades of progress. J Am Acad Dermatol 2003;49(1):1e31.
quiz-4.*[128] Haedersdal M, Gotzsche PC. Laser and photoepilation for unwanted hair growth. Cochrane Database Syst Rev 2006;
(4):CD004684.[129] Haedersdal M, Wulf HC. Evidence-based review of hair removal using lasers and light sources. J Eur Acad Dermatol
Venereol 2006;20(1):9e20.[130] Hussain M, Polnikorn N, Goldberg DJ. Laser-assisted hair removal in Asian skin: efficacy, complications, and the effect
of single versus multiple treatments. Dermatol Surg 2003;29(3):249e54.[131] Kontoes P, Vlachos S, Konstantinos M, et al. Hair induction after laser-assisted hair removal and its treatment. J Am
Acad Dermatol 2006;54(1):64e7.[132] Bjerring P, Cramers M, Egekvist H, et al. Hair reduction using a new intense pulsed light irradiator and a normal mode
ruby laser. J Cutan Laser Ther 2000;2(2):63e71.[133] Goh CL. Comparative study on a single treatment response to long pulse Nd:YAG lasers and intense pulse light therapy
for hair removal on skin type IV to VIeis longer wavelengths lasers preferred over shorter wavelengths lights forassisted hair removal. J Dermatolog Treat 2003;14(4):243e7.
[134] Klein A, Steinert S, Baeumler W, et al. Photoepilation with a diode laser vs. intense pulsed light: a randomized,intrapatient left-to-right trial. Br J Dermatol 2013;168(6):1287e93.
[135] Ismail SA. Long-pulsed Nd:YAG laser vs. intense pulsed light for hair removal in dark skin: a randomized controlledtrial. Br J Dermatol 2012;166(2):317e21.
*[136] Arowojolu AO, Gallo MF, Lopez LM, et al. Combined oral contraceptive pills for treatment of acne. Cochrane DatabaseSyst Rev 2012;7:CD004425.
[137] Cohen EB, Rossen NN. [Acne vulgaris in connection with the use of progestagens in a hormonal IUD or a subcutaneousimplant]. Ned Tijdschr Geneeskd 2003;147(43):2137e9.
[138] Brown J, Farquhar C, Lee O, et al. Spironolactone versus placebo or in combination with steroids for hirsutism and/oracne. Cochrane Database Syst Rev 2009;(2):CD000194.
[139] Muhlemann MF, Carter GD, Cream JJ, et al. Oral spironolactone: an effective treatment for acne vulgaris in women. Br JDermatol 1986;115(2):227e32.
[140] Goodfellow A, Alaghband-Zadeh J, Carter G, et al. Oral spironolactone improves acne vulgaris and reduces sebumexcretion. Br J Dermatol 1984;111(2):209e14.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003
D. Lizneva et al. / Best Practice & Research Clinical Obstetrics and Gynaecology xxx (2016) 1e21 21
[141] Thiboutot D, Zaenglein A, Weiss J, et al. An aqueous gel fixed combination of clindamycin phosphate 1.2% and benzoylperoxide 2.5% for the once-daily treatment of moderate to severe acne vulgaris: assessment of efficacy and safety in2813 patients. J Am Acad Dermatol 2008;59(5):792e800.
[142] Wolf Jr JE, Kaplan D, Kraus SJ, et al. Efficacy and tolerability of combined topical treatment of acne vulgaris withadapalene and clindamycin: a multicenter, randomized, investigator-blinded study. J Am Acad Dermatol 2003;49(3Suppl):S211e7.
[143] Hayashi N, Kawashima M. Efficacy of oral antibiotics on acne vulgaris and their effects on quality of life: a multicenterrandomized controlled trial using minocycline, roxithromycin and faropenem. J Dermatol 2011;38(2):111e9.
[144] Strauss JS, Rapini RP, Shalita AR, et al. Isotretinoin therapy for acne: results of a multicenter dose-response study. J AmAcad Dermatol 1984;10(3):490e6.
*[145] van Zuuren EJ, Fedorowicz Z, Carter B, et al. Interventions for female pattern hair loss. Cochrane Database Syst Rev2012;5:CD007628.
[146] Blume-Peytavi U, Hillmann K, Dietz E, et al. A randomized, single-blind trial of 5% minoxidil foam once daily versus 2%minoxidil solution twice daily in the treatment of androgenetic alopecia in women. J Am Acad Dermatol 2011;65(6):1126e34. e2.
[147] Vexiau P, Chaspoux C, Boudou P, et al. Effects of minoxidil 2% vs. cyproterone acetate treatment on female andro-genetic alopecia: a controlled, 12-month randomized trial. Br J Dermatol 2002;146(6):992e9.
[148] Rousso DE, Kim SW. A review of medical and surgical treatment options for androgenetic alopecia. JAMA Facial PlastSurg 2014;16(6):444e50.
[149] Kokaly W, McKenna TJ. Relapse of hirsutism following long-term successful treatment with oestrogen-progestogencombination. Clin Endocrinol (Oxf) 2000;52(3):379e82.
[150] Wild S, Pierpoint T, Jacobs H, et al. Long-term consequences of polycystic ovary syndrome: results of a 31 year follow-up study. Hum Fertil (Camb) 2000;3(2):101e5.
[151] Pasquali R, Gambineri A. Therapy in endocrine disease: treatment of hirsutism in the polycystic ovary syndrome. Eur JEndocrinol 2014;170(2):R75e90.
[152] Cussons AJ, Stuckey BG, Watts GF. Metabolic syndrome and cardiometabolic risk in PCOS. Curr Diab Rep 2007;7(1):66e73.
Please cite this article in press as: Lizneva D, et al., Androgen excess: Investigations and management,Best Practice & Research Clinical Obstetrics and Gynaecology (2016), http://dx.doi.org/10.1016/j.bpobgyn.2016.05.003