an appraisal of mitral valve echocardiograms mimicking...
TRANSCRIPT
An Appraisal of Mitral Valve Echocardiograms MimickingMitral Stenosis in Conditions with Right Ventricular
Pressure OverloadBy LAMBERT P. MOLAURIN, M.D., THOMAS C. GIBSON, M.R.C.P., WiNFRuwD WAIDER, M.D.,
WILLIAM GROSSMAN, M.D., AND ERNEST CRAIGE, M.D.
SUMMARYOf seven patients with pulmonary hypertension, two had marked and one had moderate retarda-
tion of the echocardiographic anterior mitral valve leaflet closing motion, suggestive of mitralstenosis. In each patient, however, mitral stenosis was excluded by hemodynamic or anatomiccriteria. The reason for the abnormal mitral valve motion was considered to be a reduced rate ofleft ventricular diastolic filling. In the group of seven patients it was noted that the ratio of ven-
tricular filling pressures (RVedP/LVedP) was inversely correlated with the anterior mitral valveleaflet closing slope. This observation supports the hypothesis that left ventricular diastolic fillingmay be secondarily altered by right ventricular overload, and that this impairment of left ventricu-lar filling may result in alteration of the anterior mitral valve leaflet echogram mimicking mitralstenosis.
Additional Indexing Words:Pulmonary hypertension
MITRAL VALVE echocardiography has prov-en to be an exceptionally useful technique
in the evaluation of patients with suspected mitralstenosis. A reduced diastolic closing slope of theanterior leaflet of the mitral valve is the characteris-tic finding,' 2 and the slope of this motion can betaken as an approximate index of the severity ofmitral valve obstruction.'-5 Other conditions thatmay retard the diastolic downslope of mitral valveclosing motion and lead to confusion in diagnosisinclude left atrial myxoma,6-8 hypertrophic subaor-tic stenosis,9-"1 and severe left ventricular hypertro-phy due to aortic stenosis9 or nonobstructive
From the University of North Carolina, School ofMedicine, Department of Medicine, and the C. V.Richardson Cardiac Laboratory, North Carolina MemorialHospital, Chapel Hill, North Carolina.
Supported by U. S. Public Health Service Training Grant5T01-HL05727-07, Research Grant HL14883-01, and bySpecial Research Fellowship I-FO3-H155423-01 (Dr.McLaurin), and by North Carolina Heart Association Grant1-0-107-4228-ME048.
Dr. Gibson's present address is College of Medicine,University of Vermont, Burlington, Vermont.
Address for reprints: Lambert P. McLaurin, M.D.,Cardiac Laboratory, North Carolina Memorial Hospital,Chapel Hill, North Carolina 27514.
Received December 11, 1972; revision accepted forpublication May 29, 1973.
Circulation, Volume XLVII, October 1973
cardiomyopathy.'2' 13 Since it has been suggestedthat mitral valve echocardiography is a significanttool in the diagnosis of "silent" mitral stenosis,4 it isimportant that conditions which may producemitral valve echograms mimicking mitral stenosisbe brought to attention. We report seven patientswith pulmonary hypertension, two of whom hadmitral valve echograms suggesting mitral stenosis.Mitral valve disease was excluded in each case bycardiac catheterization. A theory relating theabnormal mitral valve motion to decreased leftventricular diastolic filling is proposed.
MethodsEchocardiographic examination of the aortic root,
mitral and tricuspid valves, right and left ventricles,and interventricular septum was carried out accordingto previously described techniques." 2, 14-16 A SmithKline Ekoline-20 ultrasonoscope with a 2.25 megaHertztransducer of 0.5 inch diameter was used in allexaminations. All results for mitral valve motion are themean value for five measurements. Cardiac catheteriza-tion was performed in all patients using standardretrograde techniques.
ResultsEchocardiograms from a normal patient and a
patient with documented mitral stenosis are illus-trated for reference in figure 1. Hemodynamic andechocardiographic data for the seven study patients
801
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
MMLAUURIN ET AL.
ECG-Il
MITRAL.VALVEECHO
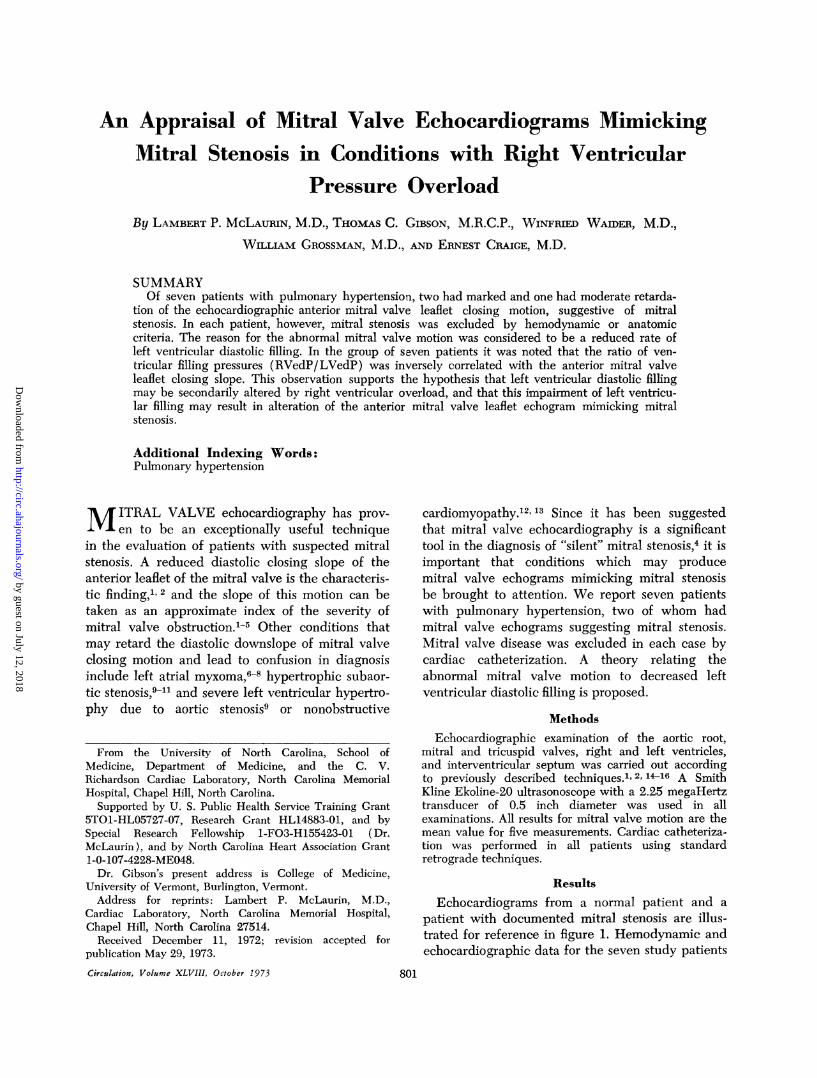
FigurXe 1
(A) The uchogram of the anterior mitral val?ve leaflet o)btained from a normal individu4al. The v}alveopenls at poingt D, reaches its maximal openz position at E, then csloses rapidly in early diastole, E to F.A represenlts the valve re-opening slightly as the result of atrial contraction. At point C the valve is closedby the onset of systole. (B) The anterior mitral valve leaflet echogram from a patient with doc.mentedrheumatic mitral stenosis. The rapid diastolic closing movement is absent and valve opening duze to atrialcontraction is minimal.
are summarized in table 1. The anterior mitral valveleaflet diastolic closing motion (E to F velocity)was markedly retarded in patients 1 and 2, andreduced in patient 3. Early diastolic openingvelocity of the anterior leaflet (D to E velocity)was decreased in patients 1, 2, and 3.
Right ventricular filling pressure exceeded leftventricular filling pressure by more than 2:1 in
patients 1, 2, and 3. Linear regression analysis of theE to F velocity against the ratio of ventricular fillingpressures (RVedP/LVedP) for the entire groupshowed a strong inverse correlation (r --.94).Case histories and echocardiograms of patients 1
and 2, in whom the anterior mitral valve leafletechogram suggested mitral stenosis, are presentedin detail below.
Table 1Hemodynamic and Echocardiographic Data
MVE D to E E to F RA(D to E) velocity velocity mean RV PA LV RVedP/
Patient mm kmm/see mm/sec mmHg mmHg mmHg mmHg LVedP
1 15 155 10 14 90/28 90/40 95/8 3.52 14 128 10 5 80/12 80/26 105/5 2.43 14 204 44 20 57/24 57/23 125/10 2.44 23 327 77 12 88/14 88/30 /13* 15 20 348 78 10 74/16 74/326 19 315 80 8 82/16 82/33 138/15 17 16 352 89 5 63/8 63/29 122/14 .6
Abbreviations: MVE = Mitral valve excursion, RA = right atrium, RV = right ventricle, PA Pulmonaryartery, LV = Left ventricle, edP = end diastolic pressure.
* = pulmonary capillary wedge pressure.
Circulation, Volume XLVIII, October 1973
802
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
ECHO AND RV PRESSURE OVERLOAD
Case ReportsPatient 1
A 40-year-old woman with a history of poissibleacute rheumatic fever in childhood was hospitalizedin late 1972 because of sharp recurrent chest pain,cough, shortness of breath, dizziness, and paroxys-mal nocturnal dyspnea. In 1965 generalized sarcoi-dosis with involvement of lung, liver, spleen, andskin had been diagnosed. In 1970 she developedpredominantly right sided congestive heart failurewith ascites, hepatomegaly, and peripheral edemawhich responded to appropriate therapy.
Physical examination revealed fine rales andexpiratory wheezes over both lungs. A normalcarotid pulse was palpated, but a prominent a-wavewas present in the jugular vein pulsations. Alongthe left sternal edge a prominent systolic heave waspresent. The first heart sound (S,) was normal. Thepulmonic component of the second heart sound(P2) was accentuated. Atrial and ventricular gallopsounds, thought to originate from the right
IV~~~~~~~~~~SEPTUMEEt --0 t
MITRA
EC.HO A.iS E( iRS ....E ina0Ea.E ia.0 t4
ventricle, were present. A grade 3/6 systolicejection murmur was maximal at the lower leftsternal edge. Hepatomegaly, moderate ascites, and2+ pitting edema of the lower extremities werepresent.The chest X-ray showed a diffuse fibronodular
infiltrate throughout both lungs. There was cardio-megaly with predominant right ventricular enlarge-ment. The left atrium did not appear significantlyenlarged. Electrocardiogram showed sinus rhythm,P waves suggesting right atrial enlargement, rightaxis deviation, and large R waves in the rightprecordial leads compatible with right ventricularhypertrophy.
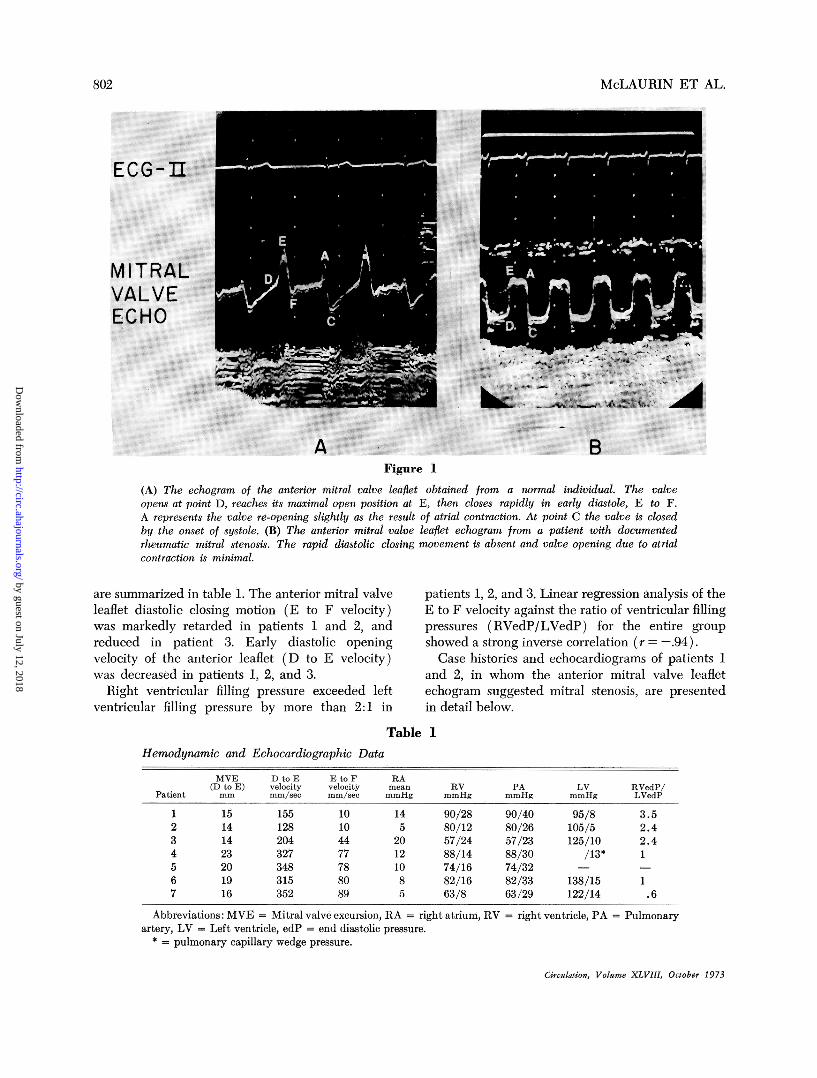
EchocardiogramFigure 2 is the mitral valve echocardiogram from
patient 1 and appears similar to that from thepatient with mitral stenosis, illustrated in figure lB.The excursion of the anterior mitral valve leaflet,measured from D to E, is 15 mm (normal 18 to 25mm), and the diastolic downslope of mitral valve
Figure 2
Mitral valve echogram from patient 1 showing absence of the rapid early diastolic closing motion, similarto figure 1B. The systolic portion of the echogram is partially obscured by the dense echo signals fromthe left atrial wall seen posteriorly. Although the septum appears to move paradoxically in this figure, otherechocardiograms obtained in a more appropriate plane for evaluation of septal motion showed it to movenormally.
Circulation, Volume XLVIIIJ, October 1973
803
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

McLAURIN ET AL.
Table 2
Hemodynamic Data
Patient Patient1 2
Systemic blood flow (liters/min)LV stroke volume (cc/beat)Pulmonary blood flow (liters/min)Right atrial pressure (mm Hg)
a wavev wavemean
Right ventricular pressure (mm Hg)Pulmonary artery pressure (mm Hg)Left atrial pressure
a wavev wavemean
Left ventricular pressure (mm Hg)Pulmonary X ascular resistance (dynes-sec-cm 5)
closing motion is only 10 mm/sec Mretarded. It was not possible to reccleaflet with sufficient diagnostic acciventricular end-diastolic internal
3.727
4.441
creased to 24 mm (normal in our laboratory is 12 to18 mm). A diagnosis of mitral stenosis wassuggested by the abnormal mitral valve echogram,and the other findings indicated an enlarged,dilated right ventricle.
3.7 4.0 Cardiac Catheterization
On the basis of the clinical picture and the216 16 echocardiogram, the patient underwent cardiac14 5 catheterization. Standard right heart, retrograde left
90/28 80/12 ventricular, and transeptal left atrial approaches90/40 80/26 were used. Hemodynamic data are presented in
table 2. Severe pulmonary hypertension was docu-12 4 mented, but no diastolic gradient across the mitral6 4 valve was found.
95/8 105/5 A left ventricular biplane angiocardiogram wasdone after left atrial injection of contrast media.
1059 848 Representative mid-diastolic films are shown infigure 3. A ventricular volume curve calculated
vhich is severely using the area-length method of Dodge'7 is)rd the posterior illustrated in figure 4. Left ventricular chamberuracy. The right volume is decreased, stroke volume is low, and adiameter is in- slow rate of diastolic filling is present.
A-P LATERAL
Figure 3
Representative anterior-posterior (A-P) and lateral films taken during the angiocardiogaphic volume study.The films correspond to the mid-diastolic volume measurements. LA = left atrium, LV = left ventricle,RV = right ventricle. Note the large area corresponding to the right ventricle in the lateral film. Thevertical interface between LV and RV corresponds to the interventricular septum which is displacedposteriorly so that it occupies a plane vertical to the film.
Circulation, Volume XLVIII, October 1973
804
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ECHO AND RV PRESSURE OVERLOAD
W
J
_i
0
-D
._
z E
LL
WJ
40
35
30
25
20
15
I0
5
EDV = 39 misESV= 12misSV 27 mIs
100 200 300 400 500TIME FROM ONSET OF QRS
(mi 11 iseconds)
600
Figure 4Left ventricular volume curve constructed from the angio-cardiographic volume study. Note the slow continuous ven-
tricular filling throughout diastole. EDV = end diastolicvolume, ESV end systolic volume, SV = stroke volume.
PathologyFour days after cardiac catheterization the
patient suffered a cardio-respiratory arrest andcould not be resuscitated. The heart weighed 370grams at post mortem examination. The leftventricle was small and had an average wallthickness of 9 mm. The right ventricle was
hypertrophied and enlarged with an average wallthickness of 11 mm. The interventricular septumwas hypertrophied, displaced leftward and poste-riorly, encroaching upon the usual area of the leftventricle. The mitral valve appeared normal to bothgross and microscopic examination, and no myocar-
dial sarcoidosis was found on histological section.The final pathologic diagnosis was generalizedsarcoidosis with severe pulmonary involvement andpulmonary hypertension.
Patient 2A 52-year-old woman with a three-year history of
progressive dyspnea and intermittent pleuritic painwas hospitalized in 1973 for evaluation of evanes-
cent pulmonary infiltrates. Detailed clinical andlaboratory evaluation failed to disclose evidence ofeither an infectious or collagen-vascular disease.
Physical exam revealed clear lung fields. Thecarotid pulse was normal to palpation. Prominent a-
waves were present in the jugular vein pulsations. Aslight left parasternal lift was present. S, was
normal. P2 was increased. A grade 2/6 systolicejection murmur was present in the pulmonic area.No diastolic murmurs were present. Hepatomegalyand slight edema of the lower extremities were
present.Chest X-ray showed several small cavitary lesions
in the right middle and left upper lobes. Moderateright ventricular enlargement was noted. Electro-Circulation, Volume XLVIII, October 1973
cardiogram showed marked right axis deviation,prominent R waves in the right precordial leads,and ST-T wave changes in leads V1-V3, allcompatible with right ventricular hypertrophy.
EchocardiogramA representative mitral valve echocardiogram is
shown in figure 5. Anterior mitral valve leafletexcursion (D to E) is 14 mm, which is significantlydecreased. The diastolic downslope (E to F),severely retarded, is 10 mm/sec. Multiple measure-ments taken on other polaroids which betterillustrated the anterior leaflet E to F slope, rangedfrom 10 to 15 mm/sec. In figure 5, the posteriormitral valve leaflet echogram can be seen to movenormally. Figure 6 shows the echocardiogram of theinterventricular septum and left ventricular poste-rior wall. The right ventricular diameter, estimatedby measuring from the right side of the septum to apoint 5 mm below the nonmoving chest wall echoesat end diastole, is increased to approximately 25mm. The left ventricular end diastolic and endsystolic diameters are decreased to 29 and 18 mmrespectively. The diagnosis of mitral stenosis,suggested by the abnormal anterior leaflet echo-gram, is not substantiated by the posterior leafletechogram which is normal. The other findingsindicate an enlarged, dilated right ventricle and asmall left ventricle.
Cardiac CatheterizationHemodynamic data are presented in table 2. The
catheter passed easily from right atrium to leftatrium and a small right to left shunt wasdemonstrated by indicator dilution curves. Severepulmonary hypertension was present. No diastolicgradient across the mitral valve could be demon-strated on multiple continuous pressure recordingsduring pull back of the catheter from left ventricleto left atrium. A pulmonary angiogram showedchanges of severe pulmonary hypertension; a leftventricular angiogram was not done. Diagnoseswere severe pulmonary hypertension, etiologyundetermined; patent foramen ovale with a smallright to left shunt at the atrial level, and rightventricular failure.
PathologyOne week after pulmonary angiography the
patient died. Autopsy showed recent and oldpulmonary emboli. The heart was grossly normalwith both left and right ventricular wall thicknessesnormal. The mitral valve was normal to both grossand microscopic examinations.
1
8(05
0
.
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

MeLAURIN ET AL.
MITRAL !
ECHO
Figure 5Mitral vazlve echogJram from patient 2. The anterior leaflet motion is decreased and the closing slope isretazrded to superficiall1y resemble mitral stenosis. The normal posterior leaflet motion (denoted by the arrow)rules our organic mitral stenosis.
DiscussionThe rate of diastolic closure of the anterior leaflet
of the mitral valve as seen on the echocardiogramdepends on multiple factors. The degree of valvethickening and rigidity, along with the extent ofshortening of the chordae tendineae, may mechan-ically retard the rate of diastolic closure in some
patients.YEHemodynamically, the rate of diastolicclosure is a function of the duration of a positivegradient across the valve and the rate of leftventricular filling during diastole.2 This latterexplanation is generally accepted as the more
important mechanism. Both of these factors,mechanical and hemodynamic, could be operativein the situation of left atrial myxoma producing a
mitral valve echogram mimicking mitral stenosis.The hemodynamic explanation, a decreased rate of
diastolic filling, has been used to account for theabnormal mitral valve echograms seen in cases ofhypertrophic subaortic stenosis9) or severe leftventricular hypertrophy.' '," It has been theorizedthat in these conditions left ventricular complianceis low, the rate of diastolic filling diminished, andthe duration of significant filling prolonged.9 13
Zaky, Nasser and Feigenbaum, in consideringmovements of the mitral valve and mitral ring, havepointed out that the two interrelate.2 A decrease indiastolic filling with a resultant decrease in mitralring movement would necessarily result in de-creased mitral valve excursion as seen in patients1, 2, and 3, although it should not specifically affectthe early diastolic descent of the leaflet.A similar hemodynamic explanation is likely in
the cases presented in this report. In the first patientCirculation, Volume XLVIII, October 1973
80)6
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ECHO AND RV PRESSURE OVERLOAD
°iar r_swz :g;\\|\\ps\iF ''\:iB
L ~~~~~
RV CAVITY
ECG-JIEIV SEPTUM
LV CAVITY
LV POSTERIOR
WALLA + X , tw wsa*S
a>8ve<\gt-t,A9Xt°Ei>~~~~~.
Figure 6
Right and left ventricular echocardiogram from patient 2. The vertical distance between the white dotsrepresents one centimeter of tissue. The RV dimension was estimated by measuring the vertical distancebetween the right side of the septum to an arbitrary point 5 mm posterior to the non-moving chest wallechoes at end diastole.
the left atrium and left ventricle can be seen to bequite small (fig. 3); the left ventricular volumecurve indicates the absence of rapid early diastolicfilling and further illustrates that significant flowacross the mitral valve continued throughoutdiastole (fig. 4). The left ventricle was small incomparison to the right ventricle and left ventricu-lar geometry was abnormal. This change inventricular geometry, resulting from the enlargedright ventricle displacing the interventricularseptum leftward and posteriorly, is illustrated infigure 3.Although left ventricular angiography was not
performed in the second case, the echocardiogramillustrates that the right ventricular internal diame-ter was significantly increased while the leftventricular internal diameter was abnormally de-creased (fig. 6). An unusually close relationshipCirculatoio, Volume XLVIII, October 1973
between the interventricular septum and anteriormitral leaflet can be seen in idiopathic hypertrophicsubaortic stenosis9-11 and in ostium primum atrialseptal defect.18 In both of these conditions the leftventricular outflow tract is narrowed. In patient 2the heart was normal at autopsy with no evidenceof septal hypertrophy or abnormality of the mitralvalve. The close relationship of the anterior mitralleaflet and the interventricular septum in patient 2can be explained by hypothesizing that during lifethe right ventricle was dilated by the severepressure overload and this process displaced theseptum posteriorly into the usual confines of the leftventricle much as was found in patient 1.The rate of diastolic opening of the anterior
leaflet (D to E velocity) was decreased in the threepatients with the lowest closing slopes (E to Fvelocity), further evidence of a decreased rate of
1- "qulp-
807
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

McLAURIN ET AL.
left ventricular diastolic filling.19 The factorscontributing to this abnormal mitral valve diastolicmotion were sought by comparing the hemodynam-ic data of these patients. A marked difference isapparent if the ratio of right and left ventricularend diastolic pressures in the patients with abnor-mally moving mitral valves are compared to thosewith normal mitral valve motion. In all threepatients with decreased mitral valve movement, theRVedP/LVedP ratio was 2.4 or greater indicating asignificant disparity between the diastolic fillingpressures in the two ventricles. These findingssuggest the hypothesis that patients with rightventricular pressure overload may develop impair-ment of early diastolic left ventricular filling, andthis impaired filling may result in alteration of themitral valve echogram mimicking mitral stenosis.
It has been demonstrated in dogs that isolatedright ventricular pressure and volume overload willalter the diastolic pressure-volume relationship ofthe left ventricle in such a fashion as to suggest adecrease in left ventricular diastolic compliance.20This change was found only when the rightventricle was overloaded and could be producedacutely by increasing the right ventricular pressureand volume in previously normal canine hearts.This suggests that left ventricular pressure-volumerelations in diastole can be altered by changes inventricular geometry independent of changes oc-curring in the myocardium. As noted above thepatients with abnormal mitral valve diastolicmotion had right ventricular diastolic filling pres-sures significantly higher than the left ventricularfilling pressures. In addition each patient had eitherangiographic or echocardiographic evidence ofright ventricular chamber enlargement exceedingany change in left ventricular chamber size. It canbe speculated that the rate of left ventriculardiastolic filling in the patients with depressed mitralvalve motion could have been decreased by theabnormal spatial and hemodynamic relationshipsbetween the right and left ventricles during diastolewhich resulted from the right ventricular overload.Whether or not the reduced left ventriculardiastolic filling resulted from a greater degree ofdistortion of left ventricular geometry or from somealteration in the actual diastolic compliance of theleft ventricular myocardium cannot be discernedfrom the available clinical data.One criticism that might be directed to the above
outlined hypothesis is that patients 1 and 2 hadrapid heart rates which could have decreased the Eto F slope of the anterior mitral valve leaflet.
Although an inverse relationship between E to Fslope and heart rate has been documented byBuyukozturk, Kingsley and Segal, marked diminu-tion of the degree seen in patients 1 and 2 was notreported.21 The rate of mitral valve opening (D toE) was not related to heart rate in their study.
Duchak, Chang and Feigenbaum noted that theechocardiogram of the posterior mitral leaflet couldbe used to discern the presence or absence of truemitral stenosis in cases where the anterior mitralleaflet had a retarded diastolic closing motion.3' Inmitral stenosis both leaflets show abnormal diastolicmovement, whereas the posterior leaflet moves
normally during diastole in circumstances whereanterior leaflet motion is retarded due to causesother than mitral stenosis. One of the cases theyused to illustrate this point had pulmonary hyper-tension and was similar to the patients of our
report.In summary, of seven patients with severe
pulmonary hypertension, two had marked and onehad moderate retardation of the anterior mitralvalve leaflet closing slope, unassociated withorganic mitral stenosis. A theory relating theabnormal mitral valve motion to decreased diastolicflow across the mitral valve is proposed. Cautionshould be exercised in making the diagnosis of"silent" mitral stenosis based on the echocardio-graphic appearance of the anterior mitral valveleaflet alone.
References1. EDLER I, GUSTAFSON A: Ultrasonic cardiogram in mitral
stenosis. Acta Med Scand 159: 85, 19572. ZAKY A, NASSER WK, FEIGENBAUM H: Study of mitral
valve action recorded by reflected ultrasound and itsapplication in the diagnosis of mitral stenosis.Circulation 37: 789, 1968
3. JOYNER CR, REID JM, BoND JP: Reflected ultrasound inthe assessment of mitral valve disease. Circulation27: 503, 1963
4. SEGAL BL, LIKOFF W, KINGSLEY B: Echocardiogra-phy: Clinical application in mitral stenosis. JAMA195: 99, 1966
5. WINTERS WL, RICCETro A, GIMENEZ J, MCDONOUGHM, SOULEN R: Reflected ultrasound as a diagnosticinstrument in study of mitral valve disease. Br HeartJ 29: 788, 1967
6. WOLFE SB, PoPP RL, FEIGENBAUm H: Diagnosis ofatrial tumors by ultrasound. Circulation 39: 615,1969
7. PoPP RL, HARRISON DC: Ultrasound for the diagnosisof atrial tumor. Ann Intern Med 71: 785, 1969
8. FINEGAN RE, HARRISON DC: Diagnosis of left atrialmyxoma by echocardiography. N EngI J Med 282:1022, 1970
Circulation, Volume XLVIII, October 1973
808
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
ECHO AND RV PRESSURE OVERLOAD
9. SHAH PM, GRAMIAK R, KRAMER DH: Ultrasoundlocalization of left ventricular oufflow obstruction inhypertrophic obstructive cardiomyopathy. Circulation40: 3, 1969
10. SHAH PM, GRAMIAK R, ADELMAN AG, WiGLE ED:Role of echocardiography in diagnostic and hemody-namic assessment of hypertrophic subaortic stenosis.Circulation 44: 891, 1971
11. Popp RL, HARRIsON DC: Ultrasound in the diagnosisand evaluation of therapy of idiopathic hypertrophicsubaortic stenosis. Circulation 40: 905, 1969
12. SHABETAI R, DAVmSON S: Asymmetrical hypertrophiccardiomyopathy simulating mitral stenosis. Circula-tion 45: 37, 1972
13. SHAH PM, GRAMIAK R, KRAMER DH, Yu PN:Determinants of atrial and ventricular gallop soundsin primary myocardial disease. N Engl J Med 278:753, 1968
14. POMBO JR, TROY BL, RUSSELL RO JR: Left ventricularvolumes and ejection fraction by echocardiography.Circulation 43: 480, 1971
15. FORTUIN NJ, HOOD WP JR, SHERMAN ME, CRAIGE E:Determination of left ventricular volumes by ultra-sound. Circulation 44: 575, 1971
16. MCDONALD IG, FEIGENBAUM H, CHANG S: Analysis ofleft ventricular wall motion by reflected ultrasound.Circulation 46: 14, 1972
17. DODGE HT, SANDLER H, BALLEW DW, LoRD JD JR:The use of biplane angiocardiography for measure-ment of left ventricular volume in man. Am Heart J60: 762, 1960
18. GRAMiAK R, NANDA NC: Echocardiographic diagnosisof ostium primum septal defect. (abstr) Circulation45 (suppl II): II-37, 1972
19. FEIGENBAUM H: Echocardiography. Philadelphia, Lea& Febiger, 1972, p 69-71
20. KELLY DT, SPOTNITZ HM, BEISER GD, PIERCE JE,EPSTEIN SE: Effects of chronic right ventricularvolume and pressure loading on left ventricularperformance. Circulation 44: 403, 1971
21. BUYUKOZTURK K, KINGSLEY B, SEGAL BL: Theinfluences of heart rate, age and sex on themovements of the mitral valve. Acta Cardiol 27: 427,1972
22. DUCHAK JM, CHANG S, FEIGENBAUM H: The posteriormitral valve echo and the echocardiographicdiagnosis of mitral stenosis. Am J Cardiol 29: 628,1972
Circulation, Volume XLVIJI, October 1973
80)9
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

GROSSMAN and ERNEST CRAIGELAMBERT P. McLAURIN, THOMAS C. GIBSON, WINFRIED WAIDER, WILLIAM
Right Ventricular Pressure OverloadAn Appraisal of Mitral Valve Echocardiograms Mimicking Mitral Stenosis in Conditions with
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1973 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.48.4.801
1973;48:801-809Circulation.
http://circ.ahajournals.org/content/48/4/801Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer in the
Permissions in the middle column of the Web page under Services. Further information about this process is availableOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from