all wales nutrition screening audit: nephrology inpatients.. renal nutrition audit presentation...
TRANSCRIPT

All Wales nutrition screening audit: nephrology inpatients.

StarterMalnutrition - a deficiency of energy, protein &
other nutrients that causes adverse effects on the body (shape, size & composition), the way it functions & clinical outcomes(MUST 2003).
• Major clinical problem in CKD, and in particular ESRD• Major clinical problem in CKD, and in particular ESRD- Reported prevalence in dialysis:
30-50%(Fouque at al, 2011).
- Independent predictor of poor clinical outcome-
morbidity, mortality, quality of lifelength of stay

Cost implications of Malnutrition
• The healthcare cost of managing individuals with malnutrition is more than twice that of managing non -malnourished individuals (Guest et al 2011).malnourished individuals (Guest et al 2011).
• Tackling malnutrition improves:- nutritional status, - clinical outcomes, and - reduces health care use. (Elia & Russell 2009).

Value for money
• Disease-related malnutrition costs in excess on £13 billion per annum , based on malnutrition prevalence figures & the associated costs of both health & socialcarecare (Elia et al 2009).

B.O.G.O.F
• NICE CG32 : ‘substantial cost savings can result from identifying & treating malnutrition’
• CG32 is ranked 3rd in the top clinical • CG32 is ranked 3 in the top clinical guidelines shown to produce savings(NICE 2006).
• The cost of managing malnutrition using prescribed nutrition support is low:- just 2.5% of the total expenditure on malnutrition (Stratton 2010).

Welsh Recipe -‘Blas o Gymru’
• The Welsh Government has recognised the importance of nutrition & catering as an essential part of the care patients receive in hospitals.
• 2009 All Wales Nutrition care pathway for • 2009 All Wales Nutrition care pathway for Hospitals……pathway for nutrition screening highlighted.
• 2011 All Wales Nutrition & catering standards for food & fluid provision for hospital inpatients.
• Nutritional screening is also recommended by DoH, RCN, RCP, NICE & NPSA.

Who’s role is it?
• Chief Executive & Executive Board
• Catering manager
• Dietitians
• Nursing staff (incl HCSW)
• Doctors • Pharmacists, SALT…….
• Everybody’s responsible!!!!

Underpinned by recommendations -
• Francis report (2013) and Andrews report (2014)
• “a small number of fundamental standards focusing on key areas of patient care”.
• “Whether patients are getting food and water, and help to eat and drink if they need”
All Wales Hospital Nutrition care Pathway protocol states:
• Standards(1) - “ Within 24 hours of admission to hospital all patients should be weighed & screened for malnutrition be weighed & screened for malnutrition or risk of malnutrition using a validated nutritional screening tool”
(WAASP / MUST ).

• Standards(2) - “When a Nutrition Risk Score (NRS) and weight has been established a multi-professional nutrition established a multi-professional nutrition care plan should be implemented. The care plan developed will depend on the NRS”.
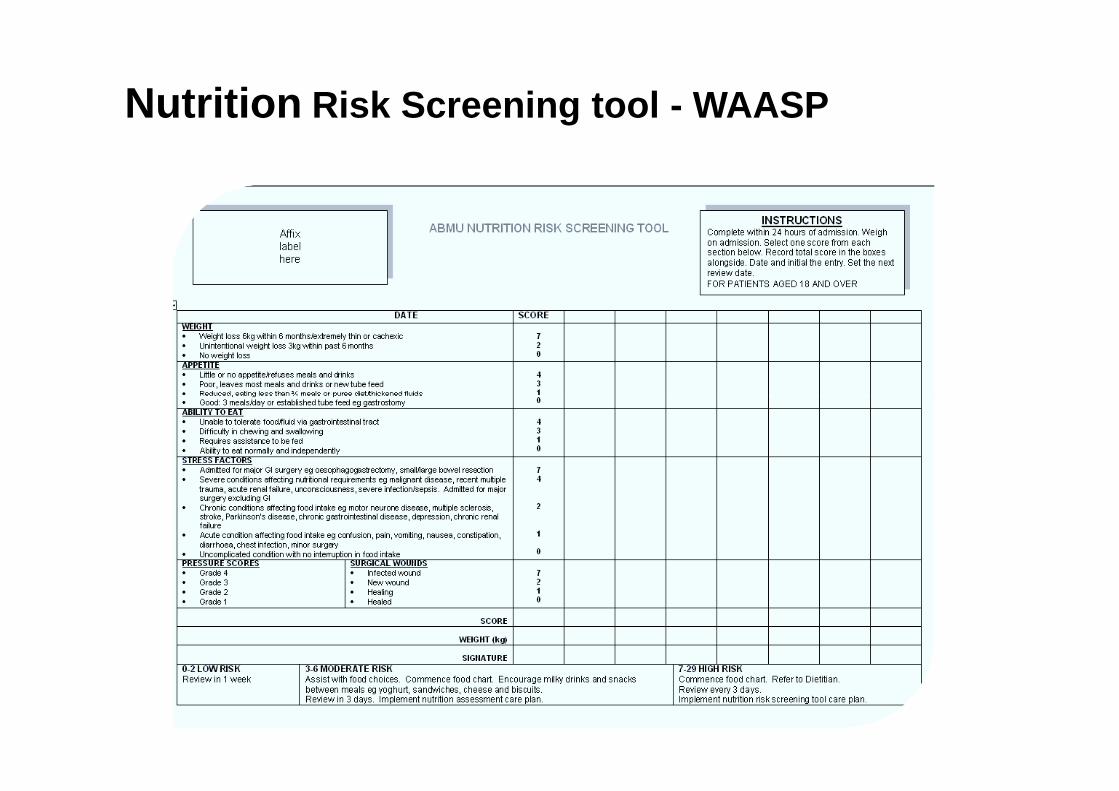
Nutrition Risk Screening tool - WAASP

MUST

All Wales Renal Nutrition Screening Audit
• Audit the nutrition screening process of inpatients in acute nephrology beds across Wales.
• Collaborative pro-forma designed to look at patients on admission , duringadmission ,their nutritional assessment & on discharge .

Methodology
1. Assessment of nutritional screening process, nutritional care and effect on outcome in all patients admitted to nephrology/transplant wards in Wales over nephrology/transplant wards in Wales over same 2 weeks, June 2014.
2. All patients admitted during this period were assessed and followed up until discharge, or following 2 weeks after audit end.

Demographics 1 – CKD vs Acute
20
1830
40
50
60
CKD Acute
No.
pat
ient
s
2821
9 13 13
18
15 819
0
10
20
30
Cardiff-neph
Swansea Wrexham maelor
Glan Clwyd
Ysbyty Gwynedd
No.
pat
ient
s

Demographics 2 - DM vs non -DM
31
40
50
60
non DM DM
No.
pat
ient
s
179 12 10
513
31
30 27
1416
19
0
10
20
30
Cardiff -neph
Cardiff -Transplant
Swansea Wrexham maelor
Glan Clwyd
Ysbyty Gwynedd
No.
pat
ient
s

Demographics 3 - malignancy vs non
malign non-malig
No.
pat
ient
s.
8 5 7 4 2
40
39 3417
1730
Cardiff-neph Cardiff-trans Swansea Wrexham maelor Glan Clwyd Ysbyty Gwynedd

83 82 7588
40
50
60
70
80
90
100
Nutritional screening completed within 24 hours
%83 82
49
75
43
88
0
10
20
30
40

WAASP & MUST Mean & Median
2
3
6
8
10WAASP score MUST score
Monitor
Interventional
0
1
0
2
4
6
Cardiff-neph Cardiff-trans Swansea Wrexham maelor
Glan Clwyd Ysbyty Gwynedd
Low risk
Monitor

Weight before & after admission: Data completeness
Number % completion
Cardiff Nephrology 36/48 75%
Cardiff Transplant 36/39 92%
Swansea 21/38 97%
WXham 8/18 75%
GC 6/21 42%
YG 2/32 6%
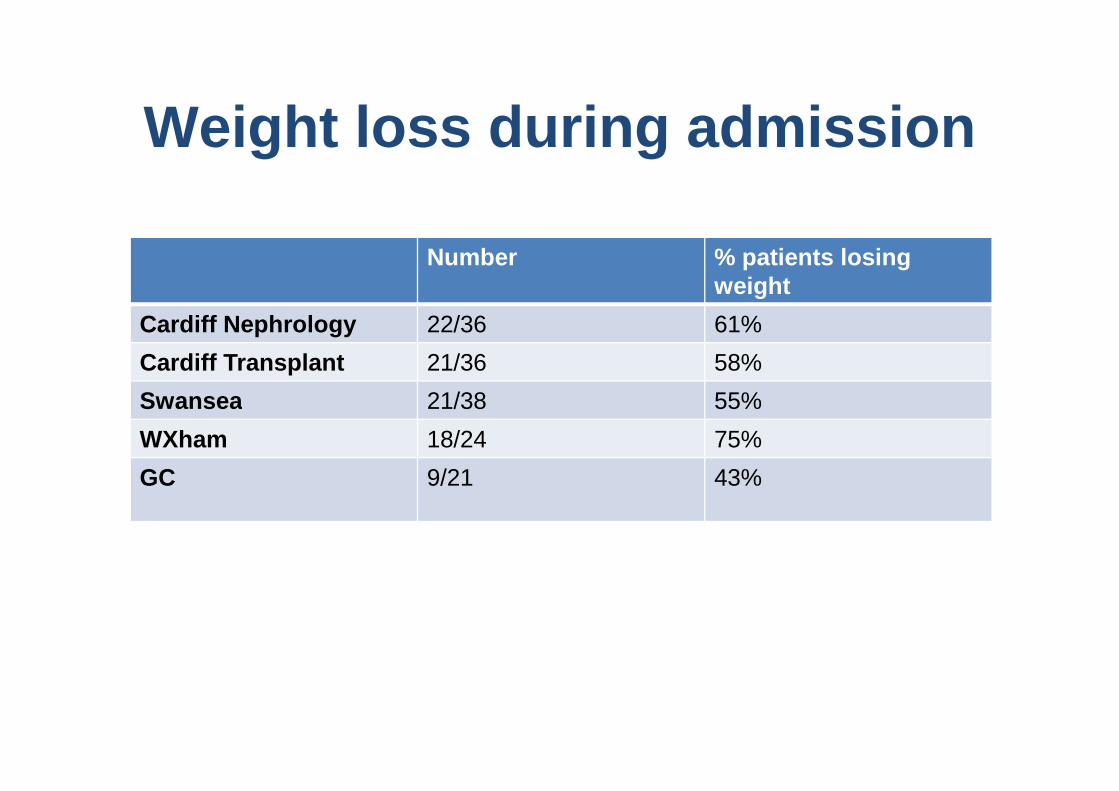
Weight loss during admission
Number % patients losing weight
Cardiff Nephrology 22/36 61%
Cardiff Transplant 21/36 58%
Swansea 21/38 55%Swansea 21/38 55%
WXham 18/24 75%
GC 9/21 43%

Weight loss during admission: mean weight before & after
90
100
110
120
Before
Wei
ght K
g
50
60
70
80
Cardiff Nephrology Cardiff Transplant Swansea Wrexham G CLBefore 88.07 79.42 80.37 91.83 79.41After 80.45 74.94 74 85.3 62.34
Before
After

8.6
10.1
6
8
10
12
Kg
Weight loss for those admitted with no oedema
2.2
0.8 0.93 0.8 1 1.2
3.22.6
0
2
4
6
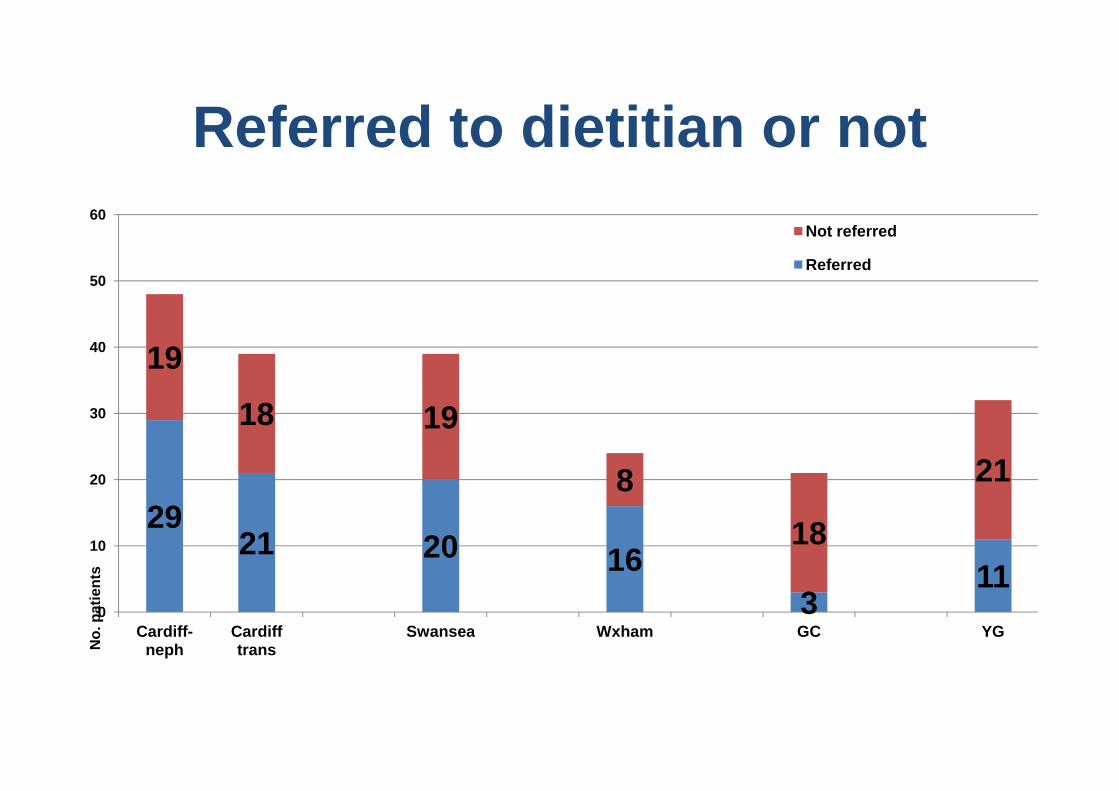
Referred to dietitian or not
19
18
40
50
60Not referred
Referred
2921 20 16
311
18 19
8
18
21
0
10
20
30
Cardiff-neph
Cardiff trans
Swansea Wxham GC YG
No.
pat
ient
s
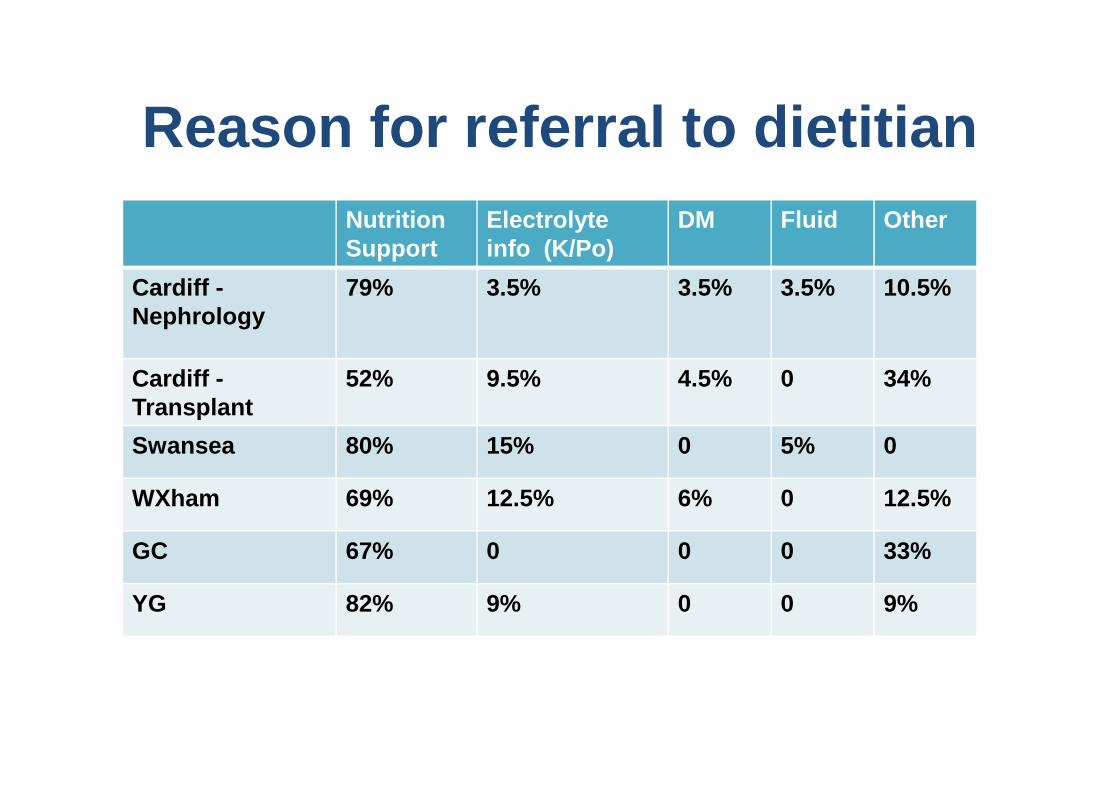
Reason for referral to dietitian
NutritionSupport
K/P/ DM Fluid Other
Cardiff Nephrology
23/29 1/29 1/29 1/29 3/29
Cardiff Transplant 11/21 2/21 1/21 7/21
NutritionSupport
Electrolyte info (K/Po)
DM Fluid Other
Cardiff -Nephrology
79% 3.5% 3.5% 3.5% 10.5%
Cardiff -Transplant
52% 9.5% 4.5% 0 34%Cardiff Transplant 11/21 2/21 1/21 7/21
Swansea 16/20 3/20 1/20
WXm 11/16 2/16 1/16 2/16
GC 2/3 1/3
Transplant
Swansea 80% 15% 0 5% 0
WXham 69% 12.5% 6% 0 12.5%
GC 67% 0 0 0 33%
YG 82% 9% 0 0 9%

• Length of stay as an outcome .• Influence of the presence of sepsis.
Biochemical markers.• Any surgery received.• Bowels .• Type of nutrition support used by
dietitians.

Problems with NRS & audit incl:
• Not ‘renal focussed’- MUST not sensitive enough in renal inpatients(Lawson et al 2010)
• Relies on accurate weight/weight history ……oedema/nephrotic patients not history ……oedema/nephrotic patients not considered.
• Renal patients referred for other things (Na/K/Po/fluid ).
• Re-screen logistics.

• Over 2 weeks audit period was data collection true reflection?
• Acutely unwell patient group, complex treatments, multi-professional input.treatments, multi-professional input.

Conclusions
• We are currently not meeting standards, for many reasons…….
• Education central to moving forwards.
• Continue audit -cycle , & look at • Continue audit -cycle , & look at auditing other CKD groups.
• Renal nutrition group (RNG) work into producing a robust , universal renal-specific NST.
• Renal Registry area to look at.

Recommendations
All Wales Renal dietitian group to look into most appropriate screening tool, referral criteria at ALL stages of CKD to ensure:
• Equity of access to service• Equity of access to service• Timely referral & review• Risk reduction• Continuous monitoring & re-auditing

Time for dessert……• We are all responsible , & have unique
roles to play to ensure adequate nutritional care is attained & maintained in our complex patient group.

• UHW Sally Finlay , Claire Farley, Rachel Long, Fiona Hillen, Helen Long, Andrea Miller, Anne Williams.
• North Wales Harriet Williams , Elizabeth Wynne, Caroline Fazakerley, Ffion Huges, Sarah Gooda.
• ABMU Sara Watkins, Jill Skinner, Eleri Wright, Emma Catling .
• Thanks/Diolch - Dr A Mikhail, Tom Hurley, Chris Brown, Fiona Willingham (RNG)

Diolch –ThanksCwestiynau?- Questions?