agency services for gestational or traditional surrogacy · 2012-11-19 · step 6: medical...
TRANSCRIPT

Agency Services for Gestational or Traditional Surrogacy
In exchange for the consideration provided by Intended Parent(s) the Agency agrees to provide the following services: Agency shall match Intended Parents with a criminally pre-screened Surrogate from our database or locate one according to your individualized search criteria. Upon agreement to match, Agency shall coordinate and arrange for Intended Parent(s) and Surrogate to be psychologically screened by a licensed mental health professional. Agency shall coordinate and arrange for selected Surrogate to be counseled regarding the IVF/IUI process and risks at the IVF/IUI clinic selected by Intended Parent(s). Agency will obtain a copy of Surrogate’s health insurance policy and will make a copy available to Intended Parent(s) for their inspection. Once matched, Agency shall coordinate and arrange for selected Surrogate to be medically screened at the IVF/IUI clinic selected by Intended Parent(s), at Intended Parent(s)’ expense. Upon completion of medical screening, Agency shall facilitate the contractual agreements between the Intended Parent(s) and the Surrogate. Agency shall provide Intended Parent(s) with a match sheet listing the standard agency contract terms and financial compensation to the Surrogate. Intended Parent(s) shall sign the match sheet and return to Agency. If Intended Parents choose the Legal Included program, Agency will oversee the drafting and review of the Surrogacy Agreement by their in-house attorneys, and refer parents to outside attorney for court filings. Included in program are costs for drafting, and review with both Intended Parent(s) and Surrogate, with standard terms and figures. If Intended Parents have not chosen Legal Included, Agency shall refer Intended Parent(s) to outside attorney to draft and review Surrogacy Agreement, and handle court filings. Outside Attorney costs will vary and will be paid directly to attorney by Intended Parent(s). No legal costs are Included in Agency Fee. Agency will ensure that the selected Surrogate has access to an independent attorney to counsel and advise her prior to signing the Surrogate Agreement so that Surrogate has “informed consent”.

Agency shall oversee all necessary legal filings and procedures (such as pre-birth orders and step parent adoptions) to establish parental rights for Intended Parents.
Agency shall coordinate travel for Surrogate and arrange for the transfer into the Surrogate of a fertilized embryo or for the IUI through a licensed IVF or IUI physician.
Agency shall work with the Surrogate and couple to make sure all doctor’s costs are correctly provided for, and all doctor’s instructions are followed.
Agency shall manage the surrogacy process by providing the following services:
Respond to messages or emails from Intended Parent(s) or Surrogate within 72 business hours or less throughout the process, unless extenuating circumstances exist,
Agency will guide and support both Intended Parent(s) and Surrogate through the entire surrogacy arrangement and will provide ongoing personal care, aid, encouragement, support and attention. Agency will be available by both phone and email to answer the Intended Parent’s questions about the surrogacy arrangement.
Agency shall oversee the payment by Intended Parent(s) of all expenses incurred by the Surrogate related to the Surrogacy Agreement,
Agency shall provide Surrogate with support from a licensed mental health professional, if necessary.
Arbitrate in the event of any disagreements.
Arrange for Surrogate to attend support group meetings or counseling or participation in an internet surrogacy support listserv.
Agency shall collect, manage and account for the monies payable to the Surrogate under the Surrogacy Agreement.
Agency shall report to Intended Parent(s) monthly regarding escrow funds according to the terms of the Fund Management Agreement.
Upon the birth of the Child, Agency shall provide the following services:
Agency shall arrange for all DNA paternity and maternity testing to be done pursuant to the provisions of the Surrogate Agreement, if requested by Intended Parent(s)
Agency shall oversee execution of legal paperwork and delivery of such to anticipated hospital or birth center
Agency shall coordinate with hospital social worker to ensure smooth process in birth certificate at hospital
Agency shall attempt to arrange, if possible at delivery hospital, a separate room for Intended Parent(s) to room with their child(ren).
Agency shall coordinate post-delivery legal process, if any.
Agency shall coordinate and pay Surrogate’s hospital bills from escrow account

PROGRAM OVERVIEW Welcome to Simple Surrogacy The information contained on the following pages is designed to give you a quick overview of our Surrogacy Program and help you understand the process. The general information here is explained in depth on our web site, should you wish for more information. We invite you to read through this overview, visit our site, and familiarize yourself with the Surrogacy and Egg Donation process. Should you have any questions, we’d be more than happy to help you find the answers. Step 1: Getting Started Congratulations! You have made the first steps toward completing your family through surrogacy and/or egg donation, by contacting our office. You must have a lot of questions about Surrogacy and Egg Donation, and we’re happy that you are considering Simple Surrogacy and/or Simple Donations as your guide to parenthood. First, please read through this information packet, and make a list of questions or concerns you have. Along with this overview, you’ll find our Schedule of Fees document and a Medical Overview so that you will have a better idea of the costs and processes of Surrogacy. Next, we will set up a phone consultation for you with Stephanie Scott, our Executive Program Director. Stephanie Scott will be able to address any questions you may have about our program or the process during the consult. If you desire an in-person consult, we can arrange that as well, at our Dallas, TX office, for a nominal consultation charge. We waive that consultation charge if you sign with our agency during that consult. Once you decide to enter our Program, we will send you paperwork to complete and return. This Paperwork is a Retainer Agreement, and an Intended Parent Profile. Once we receive your profile, and your Retainer Agreement and Retainer Fee, we submit your information to our Criminal Background Investigator. You must pass the background check and psychological evaluation before we can begin matching you. Step 2: Matching Process Surrogate Matching The next step is to match you with a Surrogate. Your Intended Parent profile will be sent

anonymously to prospective Surrogates who meet your requested search criteria. Surrogates who indicate they would be interested in working with you will also have their Surrogate profile sent to you. When you receive the profiles of the Surrogates, you will review them and let us know who you are interested in working with. Your coordinator will be available to answer any questions you may have regarding the profiles. When you find a Surrogate you are interested in working with, your coordinator will set up a phone conference for all parties to become better acquainted. If the phone conference goes well and location permits, then you would move on to meeting with your Surrogate in person. Once you have mutually agreed to work together, you are considered matched and we will begin the next step. Step 3: Escrow Before your Surrogate can be screened, you must establish escrow so that your surrogate can be compensated for her expenses at screening. For a short-distance screening at a clinic within 200 miles of your surrogate’s home, you will deposit $2,000. For a transfer greater than 200 miles from your surrogate’s home, you will deposit $4,000. This money will be used to compensate your surrogate for travel costs, meals, lost wages or childcare if any, and for invasive procedures preformed at screening. Any funds not paid out will remain in your escrow to be paid out later in your contract with your surrogate. You will receive all receipts, expense reports and statements on your escrow each month for the previous month’s expenses. Step 4: Screening Simple Surrogacy will help you select a clinic for the medical process if you do not already have a clinic in mind. We regularly refer our clients to clinics and only work with the best. You and your partner will visit the clinic to undergo screening and engage their services. You will pay your clinic directly for all medical costs of the Surrogacy. Once you have chosen your Egg Donor and/or Surrogate, we will complete her psychological evaluation. Once she passes the psychological evaluation, we will arrange for her to travel to the clinic to undergo medical screening. Once she passes screening, we will move onto the next step. Insurance As part of the screening process, we will obtain a copy of the Surrogate’s Insurance policy and provide that to you. We will check with Surrogate’s insurance company to determine if the Surrogate has medical insurance that will cover the surrogacy with no explicit surrogacy exclusion. However, final review of the policy is up to you. We can recommend an independent insurance expert to assist you with your review if you prefer. If the Surrogate does not have such coverage, then we shall assist the Surrogate

in attempting to obtain insurance that will cover the costs of pregnancy and delivery. We cannot guarantee that Surrogate’s insurance company will pay for all costs of pregnancy and delivery. As such insurance coverage is not guaranteed unless Intended Parent(s) wish to purchase the Lloyds of London policy, or similar policy, which can be costly, but does cover the surrogate’s maternity care, delivery, and its complications up to $500,000. Step 5: Legal Legal Included Program If you or your Surrogate resides in Texas and you have entered our Legal Included program, we will send you a match sheet that contains all of the terms that will be used to draft your Surrogacy Contract. After you review that document, you will return it with your signature to begin your contract drafting. Your Attorneys will contact you to sign their retainer Agreement and to pay them directly for the Validation (if you are a married couple) and/or post-birth legal work. Once you pay their fee and sign their retainer, your contract will be drafted. You will review the legal contract with your Attorneys, and your Surrogate will review with her attorney. After all parties have agreed, the contracts will be signed and notarized. Legal Process in other States If you did not enter our Legal Included Program, we will refer you to an excellent attorney in the state of expected birth to draft your legal agreement. We will send them the standard terms and amounts that all of our Surrogacy contracts contain. These terms and amounts can be found in the attached Fees document, and also on our web site. We will coordinate with them to ensure all terms and amounts are correct. Egg Donor Legal Our associate Attorney will draft your contract with your Egg Donor. He will review the contract with your Donor to insure she understands it, and can also be available to review the document with you. To save costs, may Intended Parents decide not to review the contract with the attorney themselves. All parties must sign and return the Egg Donor contract to the agency before the medical process can be begun. Escrow After the Surrogacy/Egg Donor Agreements are signed, notarized, and submitted to the Attorneys, you will fully fund the Escrow Account you already opened in accordance with your contract. Once the Escrow Account is funded, our Director of Finance will be responsible for paying the fees out in accordance with your Surrogacy Contract. You will receive monthly statements of your account, which is insured under FDIC guidelines and bonded against fraud.

Step 6: Medical Procedures Contracts are signed, and escrow is funded. You are now ready to begin necessary medical procedures for Surrogacy/Egg Donation. Your coordinator will assist you with arranging medical appointments and travel/ hotel accommodations (if needed). Please see the medical overview or our web site for descriptions of the medical process of Gestational Surrogacy, Traditional Surrogacy, and/or Egg Donation. Upon completion of IVF or IUI your coordinator will be in contact with the RE (Reproductive Endocrinologist). Your coordinator will obtain pregnancy results directly from the RE. Once pregnancy is confirmed, by either ultrasound/heart beat/beta (depending on your contract), the Surrogate’s first payment of Base Compensation is released. After pregnancy is confirmed the Surrogate will continue her medications (if any), return for frequent blood tests and an ultrasound at approximately six weeks gestation. At the appropriate time, the RE will release the surrogate to her OB/GYN, approximately at 10-12 weeks. Once released, the Surrogate will attend doctor appointments as in a typical pregnancy. We recommend Intended Parent(s) attend a few of these visits, particularly the ultrasound around 20 weeks where you can learn gender, if you desire. Step 7: Pregnancy in the Second Trimester Throughout the pregnancy, the Agency will continue to have regular contact with the Surrogate and Intended Parents, though much of the contract will occur directly between the Surrogate and IP’s. The Agency will continue to ensure that the contract is implemented, that your Surrogate is complying with her medications and prenatal care, and funds are being released properly. Our staff will be there to offer the Surrogate and Intended Parents support and encouragement every step of the way! During the second trimester of pregnancy, the process for establishing parental rights will begin. We will oversee any legal follow-up necessary to ensure this process runs smoothly. Our Executive Program Director, Stephanie Scott will make necessary arrangements with the hospital you will be delivering at, to ensure the hospital staff is aware of the impending surrogacy delivery they will receive (most hospitals will arrange for the Intended Parents to have a private room with their new baby). Our Legal Director will make sure that the Surrogate executes the necessary legal documents to insure your rights to the child, and your ability to make medical decisions on their behalf both before and after the birth. Your coordinator will assist the Intended Parent(s) and Surrogate in creating a birth plan, prior to delivery (if requested). Most Intended Parents wish to be present at the birth. Your coordinator will help you and your Surrogate discuss the expectations during the birthing process.

During the second trimester Intended Parents are preparing for their babies arrival. This includes shopping for the nursery furniture, painting the nursery, attending your baby shower, etc. This is also a very good time to take a Childcare/Newborn Care Class and Infant CPR. Simple Surrogacy is proud to offer a BABY 101 Class and Infant CPR in-office or during a private session in your home. The class instructor is a Registered Nurse who works for Cooks Children’s Hospital. In the event you are interested in obtaining more information about these classes, please email us to obtain a class schedule or call to make an appointment for a private session. Step 8: Delivery Congratulations on making it to delivery! This process can be both exciting and emotional for all parties involved. Your coordinator will be in close contact (if not present) throughout the delivery process. He or she will be there to share in your enjoyment and offer support to all parties as needed. Typically, the baby will remain in the hospital for approximately 48 hours after birth. Once the baby has received medical clearance, the couple will leave the hospital with their baby. Your attorneys will assist you in obtaining a birth certificate and passport (if needed) at this time. Your coordinator will refer all parties for post-birth counseling (if needed). Once all fees to your surrogate, medical facility, and any other expenses have been paid, the Director of Escrow will return the remainder of your funds. Step 9: Postpartum The delivery of a surrogate child can be the most amazing experience of a Surrogate’s life. It can also be very emotionally draining the first few weeks after delivery. Our staff will be there to ensure the Surrogate has support. We will be available to you 24 hours a day, 7 days a week. Most of our staff are prior surrogates and can relate to the Surrogate’s experience. Bringing home a new baby is very exciting and can be a little scary. Our staff will be here to answer any questions or concerns you may have. We are happy that you have become new parents and wish you and your family the very best! Please keep in mind what your surrogate has just done for you. Most Intended Parents choose to share photos with their Surrogate after the birth of their child. Receiving a picture of the Intended Parent(s) and their new baby, can help to reinforce the wonderful decision the surrogate has made to carry your child. The delivery of a surrogate child can be very emotional for a surrogate. It is always nice to show your surrogate she is not forgotten.

Gestational Surrogacy Medical Overview
In Gestational Surrogacy, the Surrogate Mother undergoes in vitro fertilization (IVF) and embryo
transfer to become pregnant. The eggs used under a Gestational Surrogacy are not that of the
Surrogate Mother. The sperm used is from the Intended Father or a sperm donor. The Surrogate
Mother has no genetic relationship to the child born from a Gestational Surrogacy.
In Gestational Surrogacy with an Egg Donor, the Surrogate Mother becomes pregnant through
IFF/ET using eggs from a donor other than the Intended Mother. The Surrogate has no genetic
relationship to the child born from a Gestational Surrogacy.
Medical Screening
Gestational Surrogates recruited by Simple Surrogacy, LLC are carefully screened by your clinic
of choice using the guidelines provided by The American Society for Reproductive Medicine. The
screening encompasses a review of their detailed medical history, a physical exam,
comprehensive laboratory testing, psychological assessment and medical screening.
Multidisciplinary consultations with internists and specialists, psychologists and/or counselors,
geneticists may also be required.
If there has been no previous work-up or if the testing is outdated, the Traditional Surrogate’s
work-up may include:
Gestational Surrogate Medical Screening
· Initial consultation with a Reproductive Endocrinologist
· Physical examination
· Gynecological Exam
· Blood count and chemistry
· Blood type and RH
· Drug toxicology (drugs, alcohol, and nicotine)
· Screening for rubella, cytomegalovirus, , toxoplasmosis
· HIV Antibody
· Hepatitis A, B and C Surface Antigen
· RPR for Syphilis
· Cytomegalovirus (CMV)
· Cervical Cultures for Gonorrhea, Chlamydia, Ureaplasma, and Mycoplasma.
· Genetic Testing for Cystic Fibrosis, Tay Sachs Disease, Sickle Cell Disease, and Thalassemia.

· FSH - cycle day 2 or 3
· Group B Strep
· Hysterosalpingogram or Sono-hysterosalpingogram
· Consultation with the IVF nurse coordinator regarding the treatment protocol,
medication and teaching of injections. Review and sign the consent forms.
Intended Parent(s) Screening
Your primary physician may have already performed the work-up of the Intended Parent(s)
referred for surrogacy. The philosophy at Simple Surrogacy is not to duplicate testing, thus,
Intended Parent(s) are encouraged to obtain copies of their previous testing to avoid
duplication. Testing for the Intended Parents may include but is not limited to psychological
evaluation, std testing, hysteroscopy, mock transfer, mock cycle, and blood work.
If there has been no previous work-up or if the testing is outdated, the couple’s/individual’s
work-up may include:
· Initial consultation of the couple with a staff physician of the program to review previous
medical records
· Physical examination
· Consultation with the IVF nurse coordinator regarding the treatment protocol, medication and
teaching of injections
· Review and sign the consent forms
Female Laboratory Testing
· Rubella Immunity
· Blood type and Rh
· HIV antibody
· Hepatitis B and C surface antigen
· RPR for Syphilis
· Cytomegalovirus (CMV)
· Cervical cultures for Gonorrhea, Chlamydia, Ureaplasma, and Mycoplasma (when appropriate).
· FSH - cycle day 2 or 3
Male Laboratory Testing
·Blood type and RH
· HIV antibody
· Hepatitis B and C surface antigen
· RPR for Syphilis

· CMV
· Genetic Testing for Cystic Fibrosis, Tay Sachs Disease, Sickle Cell Disease, and
Thalassemia.
· Semen analysis (within the past 6 months)
· Sperm Count
· Motility
Counseling
The role of counseling is to prepare all parties involved in the treatment and to consider all
factors which may influence the outcome. Counseling ensures that everyone is confident and
comfortable with their participation and trusts each other. Counseling also minimizes
foreseeable risks, thereby avoiding the placement of unacceptable burdens on any of the
parties, including the future child. Some clinics will require that a Minnesota Multiphasic
Personality Inventory (MMPI) be completed by a Surrogate Mother before entrance into their
medical program. The MMPI is one of the most frequently used personality tests in the mental
health fields. This assessment, or test, was designed to help identify personal, social, and
behavioral problems in psychiatric patients. The test helps provide relevant information to aid in
problem identification, diagnosis, and treatment planning for the patient.
Gestational Surrogate/Intended Parent(s) Suggestions
During the treatment cycle both the Surrogate and Intended Parent(s) should:
· Be open and honest regarding expectations and hopes throughout the process.
· Refrain from smoking, drinking, and drug use.
· Eat healthy food.
· Take vitamin supplements.
· Intended Fathers should refrain from taking hot showers or baths within the week of their
sperm donation.
· Refrain from sexual intercourse during the cycling process.
· All parties should refrain from taking any additional medication other than that prescribed by
the Reproductive Endocrinologist and/or your personal Physician.
Cycling
Once the contracts are complete and testing has finished, the Surrogate and the Egg Donor
(who can be the Intended Mother or a donor) synchronize their cycles. This is usually with birth
control pills. About 14 days into the birth control pills, both Surrogate and Egg Donor will start
Lupron. Lupron is a subcutaneous (just under the skin) injection to shut down the body's normal
hormone production used to control the cycle and ensure the Surrogate's uterus is ready to
receive the embryos at the exact time for the best chance of success.

The Surrogate is usually about a week or so ahead of the Egg Donor to ensure her uterus will be ready when the eggs are retrieved and fertilized, and because they can keep the SM in a holding pattern for up to 2 weeks once her uterine lining is at optimum. When the menstrual cycle starts while on Lupron, the Lupron dose is usually decreased by half and the Surrogate will start adding Estrogen replacement to the mix (in the form of pills, patches, or shots depending on the doctor). Some doctors have you take other medications as well (Dexamethasone to suppress male hormones to increase implantation, antibiotics to guard against any infection that might have gone undiagnosed, etc.) The Egg Donor starts on injectable fertility hormones on her cycle day 3 to stimulate her ovaries to produce several eggs as opposed to just 1 or 2. Fertility hormones continue anywhere from 7 to 12 days depending on the Egg Donor's response to the hormones. The Egg Donor is checked about 3 times a week via ultrasound and blood tests to determine her response to the drugs. Once the follicles are the right size (about 18-20mm) she is given an HCG shot which induces an LH surge which also matures the eggs. Thirty-six hours after the HCG shot the egg retrieval is performed. Up until this time, the date/time of the transfer is flexible. The eggs retrieved are fertilized with sperm from either the Intended Father or a sperm donor and incubated for 2-5 days. Lupron usually stops the day before egg retrieval in the Surrogate. Progesterone replacement (most often in the form of intramuscular injections, but sometimes with suppositories or Crinone gel) starts the day of the retrieval and continues until the 12th week of pregnancy or a negative pregnancy test. Estrogen replacement also continues until the 7th-12th week of pregnancy (when the placenta takes over hormone production). Because the Surrogate was on Lupron and had natural hormones were suppressed, The Surrogate will need to take external sources of these very important hormones in order to maintain any pregnancy that occurs. When the fertilized embryos are at the proper stage, they are loaded into a special syringe with a thin flexible catheter at the end. The catheter is inserted thru the cervix into the uterine cavity (sometimes with the assistance of abdominal ultrasound to ensure EXACT placement of the embryos) where the embryos are "injected". Most doctors will only transfer three to four 2-day old embryos or two 5-day embryos. Any unused embryos are frozen for a future attempt if a pregnancy doesn't result from the fresh cycle. Bed rest of anywhere from 2 hours to 3 days is usually required immediately following embryo transfer. A Quantitative HCG in which the amount of pregnancy hormone is measured is usually done 14 days post egg retrieval. At that time they are looking for the HCG level to be about 50 or better. Anything over 200 is usually indicative of a multiple pregnancy. The Surrogate will have a second quantitative HCG test two days later to verify that the pregnancy hormone numbers are going up (they should double about every 2 days). If the quantitative HCG is negative, all external hormones are discontinued and a menstrual cycle will usually start within 5 days. If a pregnancy has occurred (Congratulations!), an ultrasound is usually done about 6-7 weeks to check for a heartbeat and again around 12 weeks before being released to a regular OB/GYN. Usually during this time, hormone levels are checked several times to ensure that the proper levels are being maintained to ensure the pregnancy continues. Once the placenta starts taking over the hormone production, the Surrogate is weaned off the hormone replacements.

Physically, the rest of the pregnancy would be the same as any other pregnancy. **The information provided above is for general information purposes to the Clients of Simple Surrogacy and should not be construed in any way as health or medical advice or treatment recommendations.** PGD TESTING FACTS AND QUESTIONS
(Pre-implantation Genetic Diagnosis)
Does Pre-implantation Genetic Diagnosis have a role to play in Embryo Selection?
The concept of performing of PGD/ Fluorescence in-situ Hybridization (FISH) to exclude
numerical chromosome abnormalities (aneuploidy) in order to select the “best embryos” for
transfer is undoubtedly flawed and such practice should be discouraged. In contrast the
performance of PGD using comparative genomic hybridization (CGH) for the identification of
chromosomally (numerically) normal (euploid) embryos is a completely different consideration
and is emerging as a valuable tool that might significantly improve implantation potential,
reduce multiple births and , markedly reduce the risk of miscarriage and chromosomal birth
defect. The following considerations will assist in better assessing the role of PGD in the
selection of embryos for transfer:
1. Trauma to the embryo (through PGD) is always a potential problem. However this is far less
likely when PGD is done for CGH than when FISH is performed: Here is why…..PGD for FISH
requires maintaining blastomere chromosomes intact for specific analysis. This explains why 2
cells are often biopsied rather than one and why in the hands of the inexperienced, there is a
greater potential to traumatize surrounding blastomeres and compromise the embryo. While
nothing is more important than expertise (which requires a degree of experience and dexterity
that is often lacking), the level of expertise needed to perform an atraumatic single blastomere
biopsy for CGH is far less. The reason is that CGH targets DNA and unlike with FISH does not
require that the chromosomes be maintained intact. Thus the removal of a single cell for
PGD/CGH requires less dexterity and there is a lesser potential for causing trauma to the
embryo.
2. FISH does not assess all 23 chromosome pairs for numerical chromosomal abnormalities
(aneuploidy): Commercially available FISH, while capable of targeting no more than 12
chromosome pairs, usually only evaluates 8-9 pairs. Moreover, even 12-probe FISH fails to
assess several chromosome pairs commonly associated with lethal aneuploidy. CGH on the
other hand, accesses all chromosome pairs (i.e. full karyotyping).
Humans have an inordinately high incidence of egg aneuploidy which occurs primarily during
meiosis which takes place in the hours leading up to ovulation or egg retrieval. Our own studies

where CGH was performed on the first polar body (PB-1) of the mature egg (MII) have shown
that in women <35Y, about 2/3 of the eggs are aneuploid (often complex aneuploid, i.e involving
>1 chromosome pair). Preliminary data where PB-1 biopsy (with CGH) was performed on the
eggs of older women suggests that the incidence of aneuploidy increased progressively as
women age beyond 35Y such that at 40Y about 4/5 eggs are aneuploid and at 45Y the incidence
of post-meiotic egg aneuploidy might even be as high as 9/10. In addition we have observed
that the complexity of the oocyte aneuploidy increases (involving a greater number of
chromosome pairs (i.e. chaotic aneuploidy with advancing maternal age.
It has been shown that when 9-probe PGD/FISH performed on embryos derived from the eggs of
young women (<35Y) indicates no evidence of aneuploidy, there remains a 47% chance that
aneuploidy resides in the untested chromosomes. The comparable error rate in women over
40Y is greater than 55%. This serves to explain why PGD with FISH in order to diagnose embryo
aneuploidy, becomes progressively less reliable with advancing maternal age..
3. Performance of PGD when there are few Embryos available is both redundant and
unnecessary. The following facts suggest the need for discretion when it comes to PGD/CGH
performed to fully karyotype embryos so as to select the best one’s for transfer to the uterus:
· We have already shown that while achieving the blastocyst stage does not exclude embryo
aneuploidy, failure to reach blastocyst means that such embryos were almost certainly
aneuploid and unworthy of transfer or preservation. Taking embryos to the blastocyst stage
automatically culls out many severely aneuploid embryos in the process. Because of the
inevitability of an age-related increase in the incidence of egg aneuploidy, women with
advancing age beyond 39Y are far less likely to have multiple pregnancies and the likelihood of
high order multiple pregnancy (triplets or greater) is negligible beyond the age of 40Y regardless
of the number of (unselected) embryos transferred. It follows that where fewer than 6
biopsiable day 3 embryos (i.e 6-9 cells) are obtained from women over 35Y it is probably wiser
(in most cases) to allow them to develop to blastocyst and in the process cull out many
obviously aneuploid embryos… whereupon those reaching the blastocyst stage can be
transferred.
It is a fact that the full karyotyping of a single day 3 blastomere will not completely exclude the
possibility of aneuploidy in the other blastomeres of that embryo. Aneuploidy can sometimes
arise sporadically during regular cell division (i.e mitosis) as a consequence of abnormal
chromosome dispersion. Thus it is possible even in cases where full karyotyping (CGH) reveals
the tested single blastomere to be euploid that one or more of the untested blastomeres might
be aneuploid. This so called mitotic aneuploidy is referred to as mosaicism. Conversely, the
finding through CGH that a single blastomere is aneuploid, does not inevitably mean that all the
entire embryo is aneuploid since the aneuploidy affecting the randomly selected single could
(albeit rare) have resulted from mitotic (rather than meiotic) aneuploidy. So, a single mitotically
aneuploid cell might in fact be a “loner” with the remaining cells being euploid.

Mosaicism commonly arises in blastocysts and in further advanced healthy concepti. In such
cases it affects a small percentage of the total number of cells and the aneuploidy usually proves
to be harmless. Perhaps such mitotically aneuploid cells (“overwhelmed” by the majority of its
euploid neighbor cells) undergo accelerated death (apoptosis) and are so kept in check. In
contrast, when mitotic aneuploidy occurs in early embryos (e.g. by day 3) the percentage of
aneuploid cells in the later embryo is likely to be so high as to render ultimate embryo viability
unlikely.
What is true and indeed relevant is that the detection of a single euploid single cell in the 3 day
embryo provides valuable and irrefutable evidence that:
· The egg of origin was euploid
· The fertilizing sperm was euploid and,
· Fertilization took place in an orderly fashion.
Against this background, it is important to understand that the diagnosis of “embryo
competency based upon single cell (blastomere) full karyotyping (i.e. by CGH) is a presumptive
diagnosis that is likely to be accurate in about 80% of cases. Furthermore, even if the embryo is
fully euploid throughout uterine receptivity and technical prowess in performing the embryo
transfer, can preclude a successful pregnancy. That is why, based on available limited (albeit
growing) data, we currently project a 60-70% viable pregnancy rate when ≤ 2 CGH normal
embryos are transferred to a “presumably receptive” uterus. Time will undoubtedly refine and
modify these statistical projections.
In summary: PGD/FISH for gender selection and for the diagnosis of translocations is of
indisputable relevance. However, the performance of PGD/FISH for the diagnosis of embryo
aneuploidy has little if any value in selecting the” best embryos” for transfer. Full embryo
karyotyping (by CGH) is optimally suited to the selection of the most “competent” concepti for
transfer. The following indications should be considered in deciding upon PGD/CGH for embryo
selection:
1. Cases where there are >5, 6-9 cell day 3 embryos (derived from egg providers <39Y) available.
Here the decision as to which one should be transferred is pivotal.
2. In cases of unexplained repeated IVF failure where it is necessary for diagnostic purposes to
differentiate between an implantation versus an embryo factor
3. In selected cases of unexplained recurrent pregnancy loss ; to differentiate between an
implantation versus an embryo factor
4. In certain cases of male factor infertility when trying to decide whether to proceed to DS. In
such cases it is sometimes necessary to perform both PB-1 and blastomere CGH
5. To stockpile euploid, “competent” embryos over time in older women undergoing IVF

6. For egg donation at a distance where the recipient prefers to limit the time away from home.
Here St-IVF will per permit fertilization of donor eggs while she waits for the results
7. Cases where expensive treatments such as IVIG, and or surgical/medical treatments in preparation for pregnancy could be deferred until “competent euploid embryos have been safely cryo banked for subsequent dispensation

Calendar of Events and Fees
Step one: The first step to retaining Simple Surrogacy is to schedule a phone or in-office consultation
with our Executive Program Director, Stephanie Scott. During the consult we will address your personal
needs and concerns regarding the surrogacy process. If you have a significant other, they will need to
participate in the consultation. You will then fill out our Intended Parent Profile and review the Program
Information. You will need to complete the Intended Parent Profile and email it back along with a
picture of you and your spouse (if applicable). Before acceptance into our program, you will need to pass
a state/federal criminal background check. Once you have been accepted into our program and you
have chosen to retain Simple Surrogacy, you will need to sign our Retainer Agreement and pay the
program fee for the program you wish to utilize. When we receive the Retainer Agreement and the
program fee, we will begin your Surrogacy journey with the matching process.
PROGRAM FEES PAID TO SIMPLE SURROGACY
Agency Fee (gestational carrier)
Agency fee includes psychological assessment of all parties, background and criminal check of all parties by licensed private investigators, recruitment of your gestational surrogate carrier, matching of carrier and client, review of surrogate’s insurance policy, if applicable, referral to and/or coordination of medical procedures and screenings with your clinic, coordination of travel arrangements, referral to attorneys experienced in practice of reproductive law, managing escrow disbursements, coordination of birth arrangements with delivery hospital, arrange for DNA testing as needed after birth, ongoing counseling, mediation and coordination throughout arrangement, and managing your case from beginning to end.
$11,300
Legal Contracts Included Fee (in Texas)
Includes contract drafting and reviews for Intended Parent(s) and Surrogate. Intended Parent(s) and/or Surrogate must reside in Texas. Cost is additional to regular agency fee.
$2,200
Traditional Surrogacy Fee Covers all services above, but manages matching with a Traditional Surrogate. Cost is in addition to regular agency fee. Traditional surrogacy is an unsettled area of law, and your traditional surrogacy agreement may be declared void as against public policy by the courts and/or legislature, or held unenforceable, in whole or in part, by a court of law. DOES NOT INCLUDE ANY LEGAL
$4,200
International Fee
Intended Parent(s) residing outside of the United States or utilizing a Canadian Surrogate will be charged an International Program Fee. Cost is additional to regular agency fee.
$2,000

MATCHING ONLY PROGRAM FEES
Gestational Surrogate Matching Program
Agency fee includes psychological assessment of all parties, background and criminal check of all parties by licensed private investigators, recruitment of your gestational surrogate carrier, matching of carrier and client, review of surrogate’s insurance policy, if applicable, referral to attorneys experienced in practice of reproductive law. Inexperienced Surrogates are not available through this program, as they require Agency Support throughout the Surrogacy journey.
$6,500
COORDNATION ONLY PROGRAM FEES
Surrogate Coordination Program
Agency fee includes psychological assessment of surrogate, background and criminal check of surrogate by licensed private investigators, review of surrogate’s insurance policy, if applicable, referral to attorneys experienced in practice of reproductive law, coordination of the medical process of IVF or IUI, surrogate support throughout the process and escrow management. If your surrogate does not pass the background or criminal check, we will upgrade you to our regular program for only the additional program fee.
$5,750
Coordination for a Traditional Surrogate
Covers all services above, but coordinates a Traditional Surrogacy Cost is in addition to fee.
$1,000
EGG DONATION PROGRAM FEES
Egg Donation Program Agency Retainer Fee includes matching Intended Parents with an Egg Donor, psychologically and medically screening said donor (at IP’s expense for screening), arranging for the drafting and review of the donor contract, coordinating all travel arrangements, and managing the escrow account. DOES NOT INCLUDE LEGAL CONTRACTS. Legal contracts cost $850-$1,000.
$1,500 due at donor selection
$3,250 due when donor passes screening, before
contracts are signed.
International Egg Donation Program Fee
Intended Parent(s) residing outside of the United States will be charged an International Program Fee. Cost is in addition to our regular program fee.
$1,250
Step Two: Next you will begin your medical and psychological screening. We will refer the Intended Father (if applicable) to a doctor who will perform a semen analysis as well as infectious disease screening. The Intended Mother will have infectious disease screening performed, and, if using her own

eggs, be referred to a Reproductive Endocrinologist to ensure optimal egg quality. All parties will also be screened by a mental health professional. Once the medical and psychological screening is complete, we will send you profiles of surrogate mothers based on your specific search criteria. You will review the profile with your spouse (if applicable) and Simple Surrogacy will be available to answer any questions you may have. If you (and your spouse) decide you would like to pursue a match further with the surrogate, we will then send her your profile for review. The surrogate and her spouse will review your profile. If the surrogate decides she would also like to further pursue the match, we will then schedule a conference call for all parties to become better acquainted. After the conference call, if all parties agree to move forward, we will then arrange for you to meet in person. Once you have been successfully matched with a surrogate in our program, your surrogate will begin the medical and psychological screening. This process typically takes about 3 weeks to complete. All medical screening fees will be due directly to the provider utilized for the screening process.
SCREENING FEES & MEDICAL EXPENSES IN TEXAS OTHER STATES
Blood Screening Panel for Carrier & Partner
FDA Required Infectious Disease Testing of Surrogate and Surrogate's Spouse or Significant Other.
*Costs vary based on lab or clinic.*
Note: Some insurance providers will cover infectious disease screening. Simple Surrogacy gets preferential rates with many clinics in the state of Texas. For this reason, the costs for medical screening in the state of Texas are less expensive compared to other states.
$500-$1,000
$500-$2,000
Surrogate's Medical Evaluation
Consultation and examination of Surrogate Mother by a Reproductive Endocrinologist
*Costs vary by location and clinic*
Note: Some insurance providers will cover the Surrogate’s annual physical that includes pap smear, pelvic exam, and infectious disease screening. Simple Surrogacy gets preferential rates with many clinics in the state of Texas. For this reason, the costs for medical screening in the state of Texas are less expensive compared to other states.
$800 - $1,000
$1,000 - $2,000
Psychological Evaluation
Typically one session with a licensed Psychologist to determine Surrogate's suitability.
Note: Some clinics require their own psychological protocol. That cost is not included in the Program Fee.
INCLUDED IN PROGRAM FEE
INCLUDED IN PROGRAM FEE
Criminal Background Check
County, State, and Federal Criminal Background Check and Sexual Offender Registry Check. Provided by professional Investigator.
Note: Backgrounds are completed prior to matching with Intended Parents.
INCLUDED IN PROGRAM FEE
INCLUDED IN PROGRAM FEE

Fresh/Frozen IVF Cycle Fee and Medications
Simple Surrogacy gets preferential rates with many clinics in the state of Texas. For this reason, the costs for medical screening in the state of Texas are less expensive compared to other states.
**Additional costs incurred for subsequent IVF cycles** Additional costs will be incurred if using PGD Testing or Gender Selection**
$13,000-$25,000
$13,000-$38,000
Medications for Surrogate and Egg Donor
**Cost varies by pharmacy**
$800-$4,000 $800-$6,000
Step Three: Once medical/psychological screening has been completed, you will enter into the Legal Phase. We will help negotiate the contractual terms and fees associated with your agreement to ensure all parties are on the same page before the Agreements are drafted. Legal Fees are paid directly to the attorney you retain. The Legal Phase typically lasts 6 weeks. Once all parties have signed the Agreements, you will fund the escrow account. All fees due to your surrogate will come out of escrow and the Intended Parent will be sent a monthly, itemized statement detailing the escrow activity for that month. If you choose, we can also pay for medical expenses out of the escrow account. It is mandatory to keep a minimum balance of $5,000 in escrow at all times. Once your surrogate enters the second trimester, you will need to deposit the remainder of the compensation due to her under your legal agreement into the escrow account plus an additional $2,000- $4,000 to cover the medical expenses of the labor and delivery. Please understand that it is very important to us to ensure your surrogate receives all of the compensation she is due under your legal agreement, her expenses are paid, and she is not responsible for unpaid medical bills during or after the pregnancy.
LEGAL FEES IN TEXAS OTHER STATES
Egg Donor Contracts and Review
If you utilize the services of Simple Surrogacy Egg Donor attorney, we can offer preferred rates on the drafting and review of the Egg Donation contract. Other attorney’s costs might be higher than quoted preferred attorney rates.
$850-$1,200
$850-$1,200
Surrogacy Contracts and Review- Legal Included
Included in the Legal Included Gestational Surrogacy Program is the drafting and review Surrogacy Agreement with the Intended Parent(s) and Surrogate.
INCLUDED IN PROGRAM FEE
$2,500 - $5,000
Surrogacy Contracts and Review,
TRADITIONAL
We will refer you to Attorneys who specialize in Reproductive law. Legal fees vary by location and attorney and are subject to change, but through Simple Surrogacy’s referrals, many attorneys offer us preferred rates.
$2,800-$3,500 $3,800-$6,000
Surrogate Legal Representation
Review and negotiate Surrogacy Agreement with Surrogate and Surrogate’s Spouse.
INCLUDED IN PROGRAM FEE
$500 - $1,250

Surrogate Legal Representation
TRADITIONAL
We will refer the Surrogate to Attorneys who specialize in Reproductive law. Legal fees vary by location and attorney and are subject to change.
$750 - $1000 $750 - $1,250
Parental Establishment and Court Pleadings, Pre-Birth Order
Draft, review, obtain signatures, and file legal pleading papers with the Court. Arrangements for court appearances or default judgments will be made when required.
$1,900 - $3,900 $1,900 - $5,000
Traditional Program
Draft, review, obtain signatures, and file legal pleading papers with the Court. Arrangements for court appearances or default judgments will be made when required. Termination of Parental rights or step-parent adoptions as needed. Legal fees vary by location and attorney and are subject to change.
$4,800 - $10,500 $4,800 - $10,500
Surrogate Pleadings Representation
Review legal pleadings with Surrogate in connection with the establishment of the Intended Parent's parental rights. File all documents with the court. Legal fees vary by location and attorney and are subject to change.
$150 - $400
If required
$500 - $1,000
INSURANCE IN TEXAS OTHER STATES
Medical Insurance for the Surrogate
If the Surrogate's existing policy will not cover a surrogate pregnancy or if she has no health insurance. The Intended Parent(s) can purchase appropriate health insurance. The cost shown is for monthly insurance premiums for a minimum of 15 months. The insurance needs to be kept in place for 3 months post delivery. Intended Parent(s) are responsible for all co-pays, deductibles and/or uncovered expenses starting at the initial medical evaluation of the surrogate up to 3 months postpartum.
If Surrogate has health insurance coverage that does not exclude a surrogacy pregnancy, IPs are responsible for all co-pays, deductibles and/or uncovered expenses starting at the initial medical evaluation of the surrogate up to 3 months postpartum.
$400 -$600/month
if needed.
$400 -$600/month
if needed.
California Surrogates will require outside insurance, or a subsidy to their
current insurance for all
out of pocket costs.
Life Insurance Purchase of a $250,000 term policy for Surrogate in case of accidental death.
$250 - $450/year $250 - $450/year
Disability Insurance Purchasing the disability policy will help to greatly decrease the costs if your surrogate is put on bed rest or incapacitated during her pregnancy. This insurance is commonly purchased for every Gestational Carrier who is employed.
$800 -$1,200/policy
$800 -$1,200/policy
Insurance for the Intended Parents can secure health insurance coverage for Cost varies based Cost varies based

Child(ren) their child or children, if none is readily available, to take effect at birth. They also have the option of paying out-of-pocket for all of their children(s) related health/medical needs.
Note: No child will be covered under a Surrogate mother’s health insurance policy.
on number of children needing
coverage.
For international clients cost can
be $20,000+
on number of children needing
coverage.
For international clients cost can
be $20,000+
Step Four: Once you have an executed Agreement, you are ready to begin the medical process. Your surrogate will be going to the doctor quite often for monitoring of the uterine lining, progesterone and estrogen levels, etc. She will be given fertility medications to aid in becoming pregnant with your embryo(s). At this time the surrogate will be compensated for starting medications, IVF transfer fee, as well as her monthly allowance. The Reproductive Endocrinologist will typically test for pregnancy 12 days post transfer. In the event the surrogate is confirmed pregnant via ultrasound, she will begin to receive her monthly base compensation (10% of her base compensation is paid monthly until delivery).
EXPENSES AND COMPENSATION DURING PREGNANCY INEXPERIENCED
CARRIER
EXPERIENCED
CARRIER
Gestational Surrogate Base Compensation
Paid to Surrogate in 10 equal installments over the course of the pregnancy, beginning with confirmation of pregnancy via heartbeat through ultrasound. California Surrogates are now charging fees starting at $28,000 for an inexperienced surrogate, sometimes much higher.
Note: In the event the surrogate miscarries before the 32 week of pregnancy, all base compensation payments will cease. If the surrogate mother carries to 32 weeks or more, she will be entitled to all remaining compensation listed in her Surrogacy Agreement.
$24,000 (TX)
$26,000 and up in CA, other states
Traditional Carrier: $25,000
and up
$26,000 and up
CA: $28K and up, some other states
Traditional Carrier: $32,000
and up
Monthly Allowance In lieu of itemized reimbursements, this monthly fee covers mileage less than 100 miles round trip, childcare for local appointments, telephone calls, postage, co-pays, prenatal vitamins (including prescription), and pregnancy testing supplies.
Note: Begins month following contract signing & continues through one month after birth or at termination of Surrogacy Agreement.
$200/Monthly
$200-$250 Monthly
Maternity Clothing Allowance
Payment made at 13 weeks gestation.
$750 singleton
$1,000 multiples
$750 singleton
$1,000 multiples
Embryo Transfer Fee Paid after each embryo transfer procedure. Fee includes lost wages and childcare for the embryo transfer trip ($500
$500 for Fee $500 for Fee

extra is paid to cover these if the trip is long distance). Does not include meal allowance, airport parking, airport shuttles, air travel/mileage/hotel expenses. (These will be additional only for long-distance transfers. If the stay is longer than 5 days, additional lost wages will be paid to the GC.)
$200 for Expenses
$500 additional for long distance travel expenses.
$200 for Expenses
$500 additional for long distance travel expenses.
IUI Fee Paid per cycle for IUIs in Traditional Surrogates $250/Cycle $250/Cycle
Psychological Counseling
Three sessions are required, one per trimester at a cost of $90 a session.
---------------------------------------------------------------------
Monthly sessions with therapist. Not required unless requested. Determined on a case-by-case basis.
$270
-----------------
up to $1,000
$270
-----------------
up to $1,000
Birth Documents Instructs Hospital that Intended Parents are legal guardians of child and they are making the medical decisions on the child, even before birth. Drafted in the third trimester of pregnancy by an attorney.
$500 $500
FEES YOU MAY PAY, DEPENDING ON CIRCUMSTANCES
Lost Wages Lost wages are determined by actual after-tax earnings and varies based on disability insurance and actual earnings for working Surrogates only. Amount is capped at 3 months of Surrogate’s lost wages. This is for Bed Rest only.
$0 - $15,000
depends on Surrogate’s hourly
wage
$0 - $25,000
depends on Surrogate’s hourly
wage
Lost Wages for Spouse
There may be lost wages for spouse (after tax earnings as verified by recent pay stub) for medical evaluation trip, embryo transfer trip, invasive procedures, emergencies and if necessary for birth.
$0-$3,000
depends on hourly wage
$0-$3,000
depends on hourly wage
Meal Allowance If travel of more than half a day is necessary to fulfill obligations under the contract.
$50/day
$25/day companion
$50/day
$25/day companion
Travel Expenses Includes possible hotel, parking, roundtrip economy airfare for GS and companion (if required), travel to and from airport, for fulfillment of contract.
TBD TBD
Local Travel If Surrogate is required to travel by car to doctor, clinic visits, monitoring clinic, etc. Mileage is only reimbursed after the first 100 round trip miles.
$.51/mile
or current IRS guidelines
$.51/mile
or current IRS guidelines
Bed Rest If put on doctor ordered bed rest (during pregnancy, $250/week, $250/week,
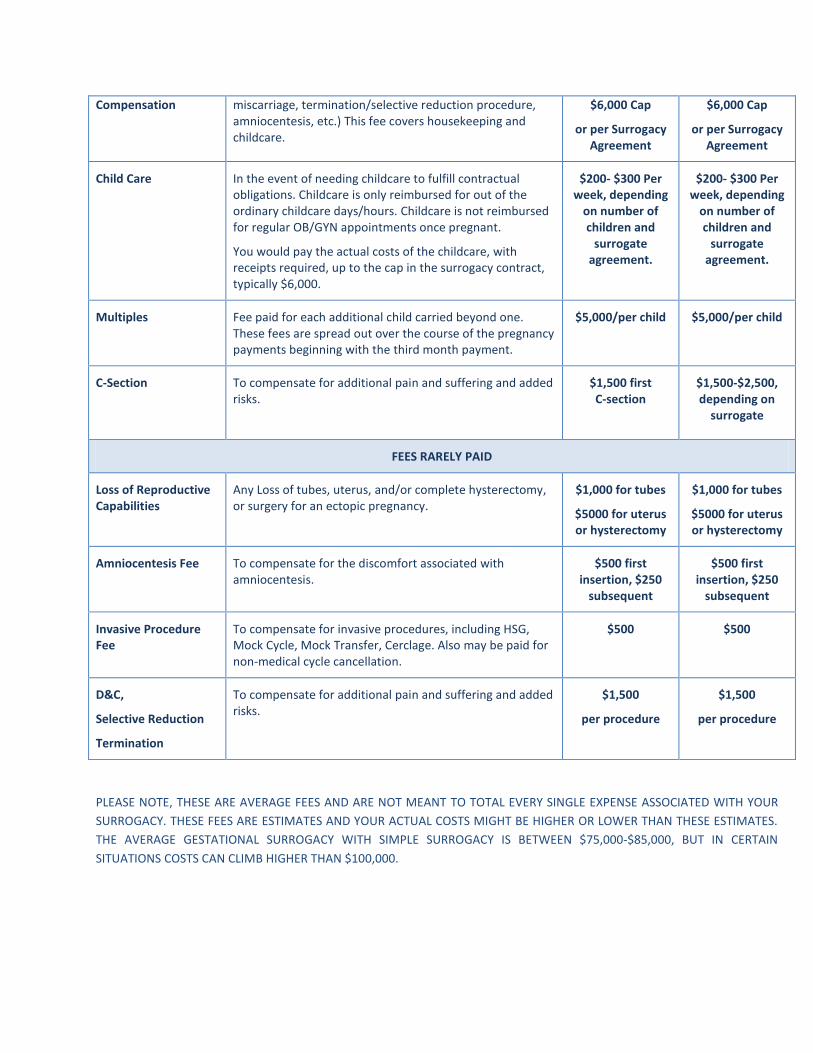
Compensation miscarriage, termination/selective reduction procedure, amniocentesis, etc.) This fee covers housekeeping and childcare.
$6,000 Cap
or per Surrogacy Agreement
$6,000 Cap
or per Surrogacy Agreement
Child Care In the event of needing childcare to fulfill contractual obligations. Childcare is only reimbursed for out of the ordinary childcare days/hours. Childcare is not reimbursed for regular OB/GYN appointments once pregnant.
You would pay the actual costs of the childcare, with receipts required, up to the cap in the surrogacy contract, typically $6,000.
$200- $300 Per week, depending
on number of children and
surrogate agreement.
$200- $300 Per week, depending
on number of children and
surrogate agreement.
Multiples Fee paid for each additional child carried beyond one. These fees are spread out over the course of the pregnancy payments beginning with the third month payment.
$5,000/per child $5,000/per child
C-Section To compensate for additional pain and suffering and added risks.
$1,500 first C-section
$1,500-$2,500, depending on
surrogate
FEES RARELY PAID
Loss of Reproductive Capabilities
Any Loss of tubes, uterus, and/or complete hysterectomy, or surgery for an ectopic pregnancy.
$1,000 for tubes
$5000 for uterus or hysterectomy
$1,000 for tubes
$5000 for uterus or hysterectomy
Amniocentesis Fee To compensate for the discomfort associated with amniocentesis.
$500 first insertion, $250
subsequent
$500 first insertion, $250
subsequent
Invasive Procedure Fee
To compensate for invasive procedures, including HSG, Mock Cycle, Mock Transfer, Cerclage. Also may be paid for non-medical cycle cancellation.
$500 $500
D&C,
Selective Reduction
Termination
To compensate for additional pain and suffering and added risks.
$1,500
per procedure
$1,500
per procedure
PLEASE NOTE, THESE ARE AVERAGE FEES AND ARE NOT MEANT TO TOTAL EVERY SINGLE EXPENSE ASSOCIATED WITH YOUR
SURROGACY. THESE FEES ARE ESTIMATES AND YOUR ACTUAL COSTS MIGHT BE HIGHER OR LOWER THAN THESE ESTIMATES.
THE AVERAGE GESTATIONAL SURROGACY WITH SIMPLE SURROGACY IS BETWEEN $75,000-$85,000, BUT IN CERTAIN
SITUATIONS COSTS CAN CLIMB HIGHER THAN $100,000.
Gestational and Traditional Surrogacy Program Fee Timeline Agency Fee The agency fee is due upfront when you sign the Agreement for Services for the program you wish to utilize. The Standard Gestational Surrogacy Program is $11,300. This program includes psychological fees but no legal fees. The Legal Included Gestational Surrogacy Program is $13,500,which includes legal fees for drafting and negotiating the Gestational Surrogacy Agreement. This program requires you to reside in or match with a surrogate residing in the state of Texas. The Traditional Surrogacy Program is $15,500. This program includes psychological fees but no legal fees. The International Program is $2,000 additional to agency fees listed above. Escrow Fees Before your Surrogate can be screened, you must establish escrow so that your surrogate can be compensated for her expenses at screening. For a short-distance screening at a clinic within 200 miles of your surrogate’s home, you will deposit $2,000. For a transfer greater than 200 miles from your surrogate’s home, you will deposit $4,000. This money will be used to compensate your surrogate for travel costs, meals, lost wages or childcare if any, and for invasive procedures preformed at screening. Any funds not paid out will remain in your escrow to be paid out later in your contract with your surrogate. You will receive all receipts, expense reports and statements on your escrow each month for the previous month’s expenses. Clinic Fees Once you are matched, you will need to pay your clinic for your Surrogate's medical consult and screening which is normally between $1,000-$2,500*. The Surrogate’s insurance will not cover any IVF medical treatments, medications, monitoring, and/or testing. It can only be used once the Surrogate has been confirmed pregnant via heartbeat and released from the Reproductive Endocrinologist to follow up with her OB/GYN for prenatal care. All fertility medications must be discontinued before the surrogate’s insurance will cover prenatal care costs. You will continue to pay your clinic directly for their medical costs throughout the medical process.

Legal Fees When screening is complete, your Surrogacy Agreement will be drafted. The drafting and negotiation of your Surrogacy Agreement will take 6-8 weeks from the time you sign the Attorney’s retainer Agreement. If you have entered the Legal Included Program, at this time you will sign the Retainer Agreement with your Attorneys and pay them for the post-birth legal work and validation directly. Post-birth legal includes a Pre-Birth order if applicable, and/or termination of parental rights. If you have entered our Traditional or Standard Gestational Surrogacy Program, we will refer you out to attorneys who specialize in Reproductive law, and you pay them directly for their fees to draft your Surrogacy Agreement. Their work on your behalf may include a Pre-birth order, or termination of parental rights or step-parent adoption. Escrow Deposits After all parties sign the Surrogacy Agreement, you will deposit additional funds into escrow. All of your surrogate’s compensation must be deposited once contracts are signed. If you need a more graduated escrow schedule, we can offer one, but there will be an additional Agency fee to administer the additional deposits. Cycling Fees Once Escrow is funded, you would begin the medical phase. From the time your contract is signed, your Surrogate would receive her monthly allowance, approximately $200 a month, to cover her expenses. You will at this time also pay her premium on a $250K life insurance. The premium is approximately $250-$350. When the medical process has begun, your Surrogate will be paid a one-time fee of $200 for starting injectable medications for the cycle (if applicable). She will also be given an IVF transfer fee or IUI fee at the time of transfer or IUI. The start of medications fee and the IVF transfer fees would also be paid for subsequent cycles. Traditional Surrogates do not always take medications during an IUI cycle. Compensation When an ultrasound confirms heartbeat, your surrogate will start to receive 10% of her base compensation once a month until delivery. Your surrogate will receive her maternity clothing allowance at 13 weeks gestation, $750 for a singleton and $1,000 for multiples. In the event your surrogate is carrying multiples, she will receive a multiple fee of $5,000 per additional child, divided by 7 and paid out over the course of the pregnancy starting in the second trimester.

Around the third trimester, the OB/GYN will ask you to pay for the obstetrical services not covered by insurance. Most insurance plans pay 80/20. This means the insurance company is responsible for paying 80% of your surrogate’s care and you are responsible for 20%. The average cost for prenatal care out of the Intended Parents pocket is $500-$700 for a normal pregnancy without complications. You will also be billed by the hospital after delivery. The out of pocket hospital costs after insurance pays their percent averages around $1,500-$3,000 depending upon whether or not the baby was delivered vaginally or by c-section. You will add the baby at birth directly to your Insurance policy and be responsible for all payments on the baby’s behalf. Below is a table showing all standard and possible fees. Standard Fees
All are payable within five (5) business days of procedure/event unless indicated otherwise.
GS is Gestational Surrogate, TS is Traditional Surrogate
Base Compensation Total Fee Special Provisions/Notes
Inexperienced Gestational Surrogate
$24,000 and up CA: $28K and up
10 equal payments through pregnancy, starts with heartbeat confirmation
Experienced Gestational Surrogate $26,000-$36,000 CA: 30K and up
10 equal payments through pregnancy, starts with heartbeat confirmation
Traditional Surrogate $28,000-$38,000 and up in CA
10 equal payments through pregnancy, starts with heartbeat confirmation
Description of Fee Total Fee Special Provisions/Notes
Monthly Non-accountable Allowance
$200/month $200-$250 exp.
Starts when contracts are signed. Includes Pre-natal Vitamins, even if prescription
IVF Transfer Compensation Fee $500/ $200 $500 long travel
$500 fee, $200 local expenses, $500 additional for long distance expenses.
IUI Fee $250 Per Cycle for Traditional Surrogates
Multiples Fee $5000 Divided into 7 payments over the pregnancy
Invasive Procedure Fee $500 Or other invasive procedure, per procedure, Need is determined by your doctor, per procedure cost.
Mock Transfer or Cycle Fee $500 Only paid once
Start of Medication Fee $200 Injectable medication only
Life Insurance $200-$450 Depends on state for costs
Disability Insurance $800-$1,200 Covers lost wages for employed surrogates
FEES UNCOMMONLY PAID
Cesarean Section Fee $1,500 First Time section only, or experienced surros
Cycle Cancellation Fee: $500 Non-medical cancellation
Amniocentesis or Cerclage $500 Subsequent draws are $250
Abortion/Termination/Selective Reduction/D&C Fee
$1,500

Loss of Reproductive organ(s) (not uterus) or Ectopic surgery
$1,000 Fee is per organ lost
Loss of Uterus $5,000 If directly related to pregnancy
Delay Fee Prior to Initial Transfer Or Initial IUI (TS)
$500 Paid after 6 months, if no transfer is attempted. Paid Monthly until start again.
Delay Fee After Initial Transfer Or Initial IUI (TS)
$250 Per month after 90 days of inactivity, in addition to expenses, until start again.
Expenses
Description of Expense Amount(s) Special Provisions/Notes
Medical Screenings $500-$2,000 Paid once matched to clinic, by the IP(s)
Maternity Clothes, single/multiple $750/$1,000
Attorney’s Fees $750-$1,200 For Surrogate’s attorney, if not included
Local Travel over 101 miles $.51/mile Or Current IRS guidelines
Counseling $125/session Max 8 sessions, 3 required ($375)
Bed Rest $200-$300 per week, actual costs
Childcare and housekeeping, Max $6,000 contract total
Travel Meals $50 day $25 for companion meals
Birth Documents $500 Once pregnant, to draft legal docs
Lost Wages Actual Net Wages of Surrogate based on paystub. Paid per hour. Capped at 3 month’s wages.
Determined by actual after-tax earnings and varies based on disability insurance and actual earnings for working Surrogates only. Potentially paid over the course of the pregnancy for: Medical Screening, Embryo Transfer, Doctor ordered bed rest, post partum recovery. Varies by Surrogate.
Lost Wages for Spouse/Partner Actual Net Wages based on paystub. Paid per hour. Capped at One week’s wages.
There may be lost wages for spouse or companion (after tax earnings as verified by recent pay stub) for medical evaluation trip, embryo transfer trip, invasive procedures (if companion is required), emergencies and for birth.

Escrow Policy Once you have an executed Agreement, you will need to fund Escrow. For domestic clients, we offer two escrow funding options. The First Option is to fund the escrow in full at contract signing with Surrogate’s compensation, allowance, transfer fee, maternity clothing and medical cushion. There is no additional agency fee for this option. The examples below use standard Inexperienced Texas Surrogate fees, but your actual fees may differ by state or Experience level of your surrogate. Regardless of fees below,
additional funds may be due to your escrow if your Surrogate goes on bed rest, or needs lost wages. All additional funds are due to Escrow by 20 weeks of pregnancy.
DOMESTIC ESCROW Option 1
Item Due at Contract Execution Due at Confirmation by Ultrasound
Due if Situation arises
Additional Agency Fee
Base Compensation $24,000
Monthly Allowance $2,400
Maternity Clothing Allowance
$750
Embryo Transfer Fee $1,000
Twins Fee $5,000 per additional
Medical Delivery Cushion‐ Singleton
$2,000
Medical Delivery Cushion‐ Twins
$2,000 per additional .
Travel Expenses All travel expenses paid to date
Legal Birth Documents $500
Lost Wages Cap In Contract
Psychological Counseling
$125 per session
Bed Rest Fee Cap in Contract
TOTAL DUE $30,150 $2,500 or $7,500 AS NEEDED

Domestic Option 2 allows a more flexible funding schedule,
but we charge an administrative Fee of $950 for that convenience.
DOMESTIC ESCROW Option 2
Item Due at Contract Execution
Due at Confirmation
by Beta
Due at Confirmation by
Ultrasound
Due at 20 Weeks
Pregnancy
Due if Situation Arises
Additional Agency Fee
$850
Base Compensation
$8,000 $8,000 $8,000 Total Remaining
Monthly Allowance
$1,000 $1,000
or total remaining
Maternity Clothing Allowance
$750
Embryo Transfer Fee
$1,000
Twins Fee $5,000
Medical Delivery Cushion‐ Singleton or twins
$2,000 or $4,000
Travel Expenses All travel expenses
paid to date
Total Remaining
Legal Birth Documents
$500
Lost Wages Cap In Contract
Psychological Counseling
$125 per session
Bed Rest Fee Cap in Contract
TOTAL DUE $10,850 $8,000 $8,000 or $13,000
TOTAL REMAINING
DUE WHEN NEEDED

For International Escrows, we require that Clients purchase the Lloyd’s of London Insurance policy for their Surrogates, or supply an additional $35,000 to escrow upon confirmation of pregnancy. In addition, International Escrows cannot be partially funded. All funds are due at
Execution of Contract, with any additional expenses incurred due at Confirmation by Ultrasound.
DOMESTIC ESCROW Option 1
Item Due at Contract Execution Due at Confirmation by Ultrasound
Due if Situation arises
Lloyd’s Policy or cushion for medical
Lloyd’s policy paid at contract signing
$35,000
Base Compensation $24,000
Monthly Allowance $2,400
Maternity Clothing Allowance
$750
Embryo Transfer Fee $1,000
Twins Fee $5,000 per additional
Medical Delivery Cushion‐ Singleton
$2,000
Medical Delivery Cushion‐ Twins
$2,000 per additional .
Travel Expenses All travel expenses paid to date
Legal Birth Documents $500
Lost Wages Cap In Contract
Psychological Counseling
$125 per session
Bed Rest Fee Cap in Contract
TOTAL DUE $30,150 $35,500 or $42,500 AS NEEDED
INTERVIEW CONSENT
As part of your health screening, you are required to submit to a psychosocial interview.
Any spouse or partner who lives with you will be interviewed separately. The purpose of
this interview is to gather your social, medical, and psychological history and identify
any needs for further evaluation such as psychological testing. You are expected to be
completely honest in this interview, and as such there may be information in your social
history that is upsetting for you to talk about or read later. Please alert the interviewer if a
topic makes you uncomfortable. Your completed assessment is forwarded directly to
Simple Surrogacy, LLC only. If you are approved to continue with Simple Surrogacy’s
Program, your assessment will then be forwarded to the clinic being utilized for IVF as
well as the party you have chosen to match with. Any further distribution will be subject
to your consent.
I certify that the information I will provide in my psychosocial interview is true, correct,
and complete. I understand that false statements reported during my interview may be
considered a breach of contract. I allow Simple Surrogacy, LLC to receive, review, retain
my completed interview, and distribute it to the clinic I will be working with for the IVF
cycle as well as the parties I am matching with.
Name (please print) _____________________________
Signature _____________________________ Date ___________
Spouse or Partner Name (please print) _____________________________
Signature _____________________________ Date ___________
You can contribute by allowing content from your interview to be used in research. All
identifying information will be removed from your responses before any use, and quotes
are not used. It will be impossible for anyone to link your responses with your personal
information. Your participation in the study is voluntary. If you do not wish to provide
consent, simply leave this section blank.
Your signature below indicates that you allow the content of your interview to be used,
without identification, for research.
Name (please print) _____________________________
Signature _____________________________ Date ___________
Spouse or Partner Name (please print) _____________________________
Signature _____________________________ Date ____________