advances in vitreoretinal surgery
DESCRIPTION
This is the first presentation i have done in my life successfully.even then suggestions are very much welcomed.TRANSCRIPT

JOURNAL REVIEW
ADVANCES IN VITREORETINAL SURGERY
DR.BHARTI AHUJA

VITRECTOMY Microsurgical procedure to remove some or
all of the vitreous humour from the eye.
TYPES OPEN SKY VITRECTOMY(KASNER,1960S)-excision of
damaged or diseased vitreous through a large limbal incision or a corneal wound.
CLOSED SYSTEM(MACHEMER,1970s)-Trans pars plana vitrectomy.-two port vitrectomy
three port vitrectomy(current technique in use)
four port vitrectomy

OCULAR ANATOMY FOR PARS PLANA

INDICATIONS OF VITRECTOMY Vitreous haemorrhage(diabetic and other causes) Vitreous inflammation-noninfectious
infectious(endophthalmitis) Vitreous floaters (significant&nonsignificant) Retinal detachment repair Macular holes repair Retinal scar tissue- removal(idiopathic,diabeticrelated,associated
with RD) Retained cataract fragments aftercataract surgery-removal Dislocated lens implants –retrieval Retinopathy of prematurity-repair Refractory diabetic macular edema-membrane peeling and
vitrectomy Severe ocular trauma-repair and removal of intraocular foreign
bodies Indeterminate diagnosis (obtain intravitreal specimen)
PRINCIPLE OF VITRECTOMY(CLOSED )
The operation is performed through water tight incisions,so that the IOP is maintained in a suitable normal range throughout the procedure and needed amount of instruments is not restricted.
Minimum levels of suction force are used throughout the operation to avoid creating retinal breaks.

PROCEDURE OF VITRECTOMY(CLOSED)
Anaesthesia –local -peribulbar(occasionally general)
Site of incision –pars plana i.e. 3-4 mm posterior to the anterior margin of limbus(optimal location)
Size of incision-3.5 mm,(1 mm with 20 guage instruments)
Three incisions-sclerotomies/ports inferotemporal,superotemporal and
superonasal( infusion,vitreous probe and endoilluminator)
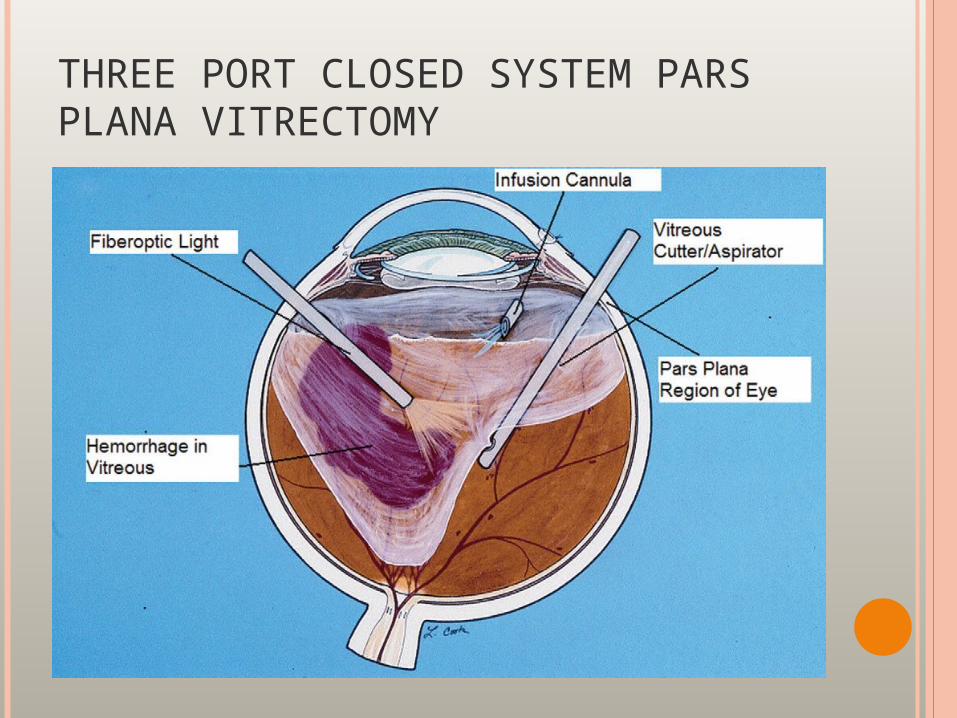
THREE PORT CLOSED SYSTEM PARS PLANA VITRECTOMY

VITREOUS PROBES(2 TYPES)
Full function(tip dia-2.2-2.5 mm )-VISC-not in use(combined infusion ,cutting and suction)-larger incision.A fiberoptic illumination-sleeve around the tip.
Divided function probes(tip dia-0.9-1.5 mm)-currently in use(smaller incision)
Modern vitreous probes-suction and cutting. pneumatic/electronic cuttersQUALITIES Higher cut rates (100-2500 cuts/min) Lower flow rate

ENDOSCOPES FOR VITREORETINAL SURGERY
CORNEAL CONTACT LENSES Plano concave Self retaining Lenses attached with infusion system Prismatic /angulated (mainster)
ILLUMINATION 19/20guage light pipe ,halogen monofilament
source

ADVANTAGES OF THREE PORT VITRECTOMY(20 GUAGE)
Reduced size of the instrument Reduced weight of the instrument Smaller incision Better visualization

DISADVANTAGES
Sutured wound Ocular surface inflammation Postoperative discomfort Postoperative retinal tears(5-10%cases)

COMPLICATIONS OF VITRECTOMY
Cataract progression Infection (endophthalmitis) Retinal tear Retinal detachment Hypotony Glaucoma Vitreous cavity hemorrhage Suprachoroidalhemorrhage

MIVS(MICROINCISIONAL VITRECTOMYSURGERY)-

EVOLUTION OF MIVS
Dr,STANLEY CHANG(1993)-23 guage system. EUGENE DE JAUN(2001)-transconjunctival 25
guage sutureless vitrectomy system CLAUS ECKHARDT ETAL(2005)-23 guage
sutureless vitrectomy system.

CURRENT THREEPORT TECNIQUE INMODERN VITERORETINAL SURGERY
Divided system of instrumentation(1st complete divided system-ocutome ,a set of 20 guage instruments-CARL WANG,mid 1970s)
Three separate sclerotomies(ports)< 1 mm incision,i.e.23 &25 guage instruments.
Xenon light source(Cold light,near normal colour to tissues)
ENDOSCOPES 19gaugewith 110° field 20gauge with 50° field

OPHTHALMIC ENDOSCOPIC SYSTEM UNIT

PHOTOGRAPH OF AN EYE DREPPED ANDUNDERGOING A 3-PORTVITRECTOMY PROCEDURE

XENON LIGHT COMPARED WITH HALOGEN LIGHT

WIDE ANGLE FUNDUS OBSERVATION SYSTEM
The BIOM noncontact system with a field of view of 70°, 90° or 110°
The EIBOS noncontact system with a field of view of 100° for 90 – diopter and 125° for 60 – diopter.
The VOLK reinverting operating lens system (ROLS); can be used to visualise upto vitreous base and ora serrata.
The AVI inverter. The iris medical contact wide-angle system

BIOM3



ADDITIONAL SURGICAL STEPS AS A PARTOF MODERN VITREORETINAL SURGERY
Membranectomy Fluid air exchange Air-gas exchange Silicon oil injection Photocoagulation Scleral buckling Lensectomy

THE JOURNAL OF RETINA AND VITREOUS,FEB2009,VOL29,ISSUE2,PG225-231
NAGPAL, MANISH MS, DO, FRCS; WARTIKAR, SHARANG MS;NAGPAL, KAMAL MS
Comparison of Clinical Outcomes and Wound Dynamics ofSclerotomy Ports of 20, 25, and 23 Gauge Vitrectomy
Purpose: To compare the benefits, the risks and the dynamics of portclosure in different gauge vitrectomy systems.
Results: Vision improved from 0.048 (3/60) to 0.206 (6/24) (p = 0.0021),from 0.069 (4/60) to 0.389 (6/18) (p < 0.0001) and from 0.055 (3/60) to0.286 (6/24) (p = 0.0010) with 20, 23, and 25-G systems, respectively.Re-bleeds occurred in 4, 1 and 4 eyes of 20, 23 and 25-G systemsrespectively and post-operative retinal detachment was seen in 2cases of 20-G system. There were no cases of post-operative hypotonyor endophthalmitis seen. With 23 and 25 gauge systems, significantamount of vitreous was seen blocking the inner lip of the sclerotomyports.

CONCLUSION
The small guage systems are equally andefective as 20 guage systems fornoncomplicated cases of vitreoushaemorrhage with faster recovery and morecomfort of the patient.

Indian journal of ophthalmology,2007(vol.55 ,issue3,page 203-206)
Vandana jain,dharmesh kar,s.natrajan,debraj shome,hitendra mehta,hijab mehta,Chaitra jaydev,nishikant borse.PHACOEMULSIFICATION AND PARS PLANAVITRECTOMY:A COMBINEDPROCEDURE
To describe the results of a combined procedure includingphacoemulsification,Insertion of PCIOL,and pars plana vitrectomyineyes with vitreoretinal pathology and coexisting cataract.

Results: In all, 65 eyes of 64 patients were included. The mean age of the patients was 50.9 years ± 17.1 (range, five to 82 years). Vitreoushemorrhage with or without retinal detachment (19 eyes, 29.2%) was the most common indication for the vitreoretinal procedure. Primaryanatomical success of retina was achieved in 59 eyes (90.7%). Visualacuity improved in 48 eyes (73.8%), was unchanged in 12 eyes (18.5%) and deteriorated in five eyes (7.7%). Postoperative inflammation was significantly more in the subgroup of previously vitrectomized eyes (42%)( P =0.014, Fisher exact test) compared to those which underwentprimary vitrectomy..
CONCLUSION
Combined surgery is a feasible option forpatients with cataract and vitreoretinaldiseases.

COMPLICATIONS WITH MIVS
HIGHER INCIDENCE OF RETINAL TEARS/DETACHMENTS
ENDOPHTHALMITIS WOUND LEAKAGE &HYPOTONY CHOROIDAL HAEMORRHAGE
&DETACHMENTS CONJUNCTIVAL BLEBS FORMATION

OPH SOURCE OPHTHALMOLOGY,VOL.116,ISSUE 7,PAGE 1360-65,JULY 2009,
ENDOOPHTHALMITIS AFTER PARS PLANAVITRECTOMY: 25 G AND 20G COMPARISON
Comparison of incidence rate of endophthalmitis after 25 guagesutureless versus 20 guage sutured vitrectomy on a large cohort ofpatients operated with a standardized perioperative anti-infectionprotocol.

Of 3372 PPV surgeries meeting inclusion and exclusion criteria, 1948and 1424 surgeries were 20- and 25-gauge PPVs, respectively. Averageage (± standard deviation) of patients was 54.6 (± 22.6) and 64.4 (± 16.5)years in the 20- and 25-gauge PPV groups, respectively (P<0.0001).Median post-PPV follow-up time was not significantly different betweenthe 2 groups (12.5 vs 13.0 months; P = 0.69). Endophthalmitis wasobserved in 1 patient (0.07%; 95% confidence interval, 0%–0.21%) fromthe 25-gauge group and none in the 20-gauge group (P = 0.42; Fisherexact test, 2-tailed). The use of air/gas endotamponade (P<0.0001) andintravitreal triamcinolone (P<0.001) was more common in 25- versus 20-gauge PPV.CONCLUSION
The incidence of endophthalmitis was low in both groups,butthe study was unable to show any significant differencebetween the incidence after 25 guage and 20 guage and thusconcluded that preioperative antiinfection control may reducethe risk associated with 25 g PPV to that of 20 g PPV.

PULSED ELECTRON AVALANCHE KNIFE IN VITREORETINALSURGERY:: precise,cold and tractionless dissection of
tissue in liquid media.
greatly facilitate both posterior surgeries like membrane dissection and sheathotomy as well as anterior segment procedures trabeculectomy and iridectomy.

ADVANTAGES OF PEAK
Sharpely defined transection &incision of epiretinal membranes.
Fine coagulation of vascularized epiretinal tissue during surgery for traction RD.
Traction free dissection of attached and elevated retina.
Mid infra red laser based cutting in vitreoretinal surgery-to minimize the collateral damage with high cutting,minimize the liquification rates.

CONTRAINDICATIONS OFVITRECTOMY
Failure to obtain appropriate informed consent
Bleeding diathesis/anticoagulation Corneal/other opacity precluding adequate
visualization Scleromalacia or otherconditions that may
prevent adequate wound healing Suspected neoplasm as
retinoblastoma[seedingorbit] Other medical contraindication to
anaesthesia/surgical procedure.
British journal of ophthalmology 2009,93 787-90
25 GUAGE FOR PAEDIATRIC VITREORETINAL CONDITIONS.
C R GONZALES,S SINGH, S D SCHWARTZ
To evaluate the feasibility and safety of 25-gauge vitrectomy for various vitreoretinal indications in the paediatric population.
intervention, choroidal detachment, endophthalmitis or sclerotomy related retinal breaks.

Results: 56 eyes in 49 children (16 girls and 33 boys) were included. Intraoperative unplanned events or complications included: conversion to 20-gauge vitrectomy (four), conversion of one port to a 20-gauge sclerotomy (two), suspected lens damage (one) and intraoperative bleeding from a vascular ridge (one). Postoperative complications included cataract (five), rhegmatogenous retinal detachment (four) and vitreous haemorrhage (three). The four retinal detachments were either recurrent or occurred in eyes with complex ocular pathology and were not felt to be related to the surgical technique. There were no cases of postoperative hypotony requiring intervention, choroidal detachment, endophthalmitis or sclerotomy-related retinal breaks.
25 guage vitreoretinal techniques can be used in various paediatric Vitreoretinal diseases.It actually facilitates access to small spaces of Paediatric eye.

SCLERAL BUCKLING - a surgical procedure in which a piece of silicone plastic or sponge is sewn onto the sclera at the site of a retinal tear to push the sclera toward the retinal tear. The buckle holds the retina against the sclera until scarring seals the tear.
PNEUMATIC RETINOPEXY VITRECTOMY- Recommended in situations like large &posterior retinal tears vitreous haemorrhage giant retinal tears advanced retinal scarring(PVR)
RETINAL DETACHMENT REPAIR

SCLERAL BUCKLING
Anaesthesia-local(peribulbar) preferred Circumcorneal conjunctival incision(peritomy)-
at the limbus /4mm posterior to it. Each of the 4 recti muscles-isolate with a
muscle hook,2-0 silk under the insertion Localization of the retinal breaks Chorioretinal adhesion-retinopexy-
cryotherapy,diathermy,photocoagulation(laser) Securing the scleral buckle Drainage of subretinal fluid closure

CRYOPEXY/CRYOTHERAPY




POSTOPERATIVE COMPLICATIONS OF SCLERAL BUCKLING SURGERY
Choroidal detachment Elevated IOP Cystoid macular edema Endophthalmitis Infection/extrusion of buckling element Diplopia Proliferative vitreoretinopathy Persistent/recurrent retinal detachment

To report the anatomic and functional results of primary vitrectomy without scleral buckling for the treatment of pseudophakic rhegmatogenous retinal detachment (PsRD)
Results Mean follow-up ± standard deviation (SD) was 12 ± 6.3 months (range, seven to 36 months). Mean final visual acuity ± SD was 0.42 ± 0.45 logarithm of the minimum angle of resolution (logMAR) compared with 0.95 ± 0.73 logMAR before surgery (P < .01). Mean number ± SD of retinal breaks found before surgery was 1.36 ± 1.12 (range, zero to five), and an additional 1.58 ± 2.26 (range, zero to 15) retinal breaks were found during surgery. The retina was reattached successfully after a single surgery in 92 eyes (92%). Recurrence of retinal detachment occurred in eight eyes (8%), caused by proliferative vitreoretinopathy in six eyes (75%) and by new breaks in two eyes (25%). Final anatomic reattachment was obtained in these cases after a mean of 1.75 subsequent operations.
Primary Vitrectomy without Scleral Buckling for Pseudophakic Rhegmatogenous Retinal Detachment
AMERICAN JOURNAL OF OPHTHALMOLOGY,JUNE 2008

Three eyes required permanent silicone oil tamponade so that final anatomic success was achieved in 97 eyes (97%). The most common postoperative complication was ocular hypertonia of more than 21 mm Hg, observed in 36 (36%) eyes, which was managed successfully.
CONCLUSION
Primary vitrectomy was successful in terms of anatomic success without scleral buckling in patients with Ps RD associated with few complications.

Primary Repair of Retinal Detachment With 25-Gauge Pars Plana Vitrectomy
To evaluate 25-gauge pars plana vitrectomy (PPV) for primary repair of rhegmatogenous retinal detachment
Results: Most patients had pseudophakic RRD (36 [85.7%] of 42 eyes). The crystalline lens was present in the remaining 6 eyes (14.3%). Of 42 eyes, 28 (66.7%) had macula-on RRD, while 14 (33.3%) had macula-off RRD. Four surgeons contributed to this study, and 25-gauge PPV instrumentation, a wide-angle viewing system, endolaser photocoagulation, and gas tamponade were used in each case. The single surgery anatomical success rate was 92.9% (39 of 42 eyes). For eyes with macula-on RRD, best-corrected visual acuity was 20/50 (0.43 logMAR [logarithm of the minimum angle of resolution]) preoperatively and 20/30 (0.23 logMAR) postoperatively (P = 0.24
Miller, Daniel ; Riemann, Christopher ; Foster, Robert E. ; Petersen, Michael R.
JOURNAL OF RETINA ,AUG 2008 VOL 28 ISSUE 7 PG 931-936

. For eyes with macula-off RRD, best-corrected visual acuity was 5/200 (1.56 logMAR) preoperatively and 20/30 (0.23 logMAR) postoperatively (P = 0.001). Three eyes required additional surgery for final reattachment. Final reattachment was achieved in 100% of patients (mean follow-up, 8 months).
25 guage PPV with laser retinopexy,plus gas tamponade is effective for primary repair of RRD.This single operation has got anatomical success rate comparable to vitrectomy with primary vitrectomy done with 20 guage instrumentation,scleral buckling and combined vitrectomy /scleral buckling.
CONCLUSION

PNEUMATIC RETINOPEXY
A gas bubble is injected into the vitreous cavity which closes the tear in the retina. Subsequently laser or cryotherapy is performed to treat the edges of the tear.

BRITISH JOURNAL OF OPHTHALMOLOGY,JULY-AUG2006,VOL.9 NO.4
PNEUMATIC RETINOPEXY:SUCCESS RATE AND COMPLICATIONS
A A ZAIDI,R ALVARADO,A IRVINE
To evaluate the success rate and complications of pneumatic retinopexy performed at a university hospital and to identify which patients are best suited for pneumatic Retinopexy
Results:33 of 61 (54%)caseswere successful with a single procedure.40 of 61(66%)Caseswere success ful with a repeat injection ofgas or laser retinopexy alone.AllCases had anatomic success at final followup.age,myopia,lens status,an dno.of breaks Were not proved to be risk factors for failure.The average duration of follow up was 15 months.
PR was less effective for repair of RRD than most published reports.however,Repair by scleral buckling or pars plana vitrectomy didn’t influence the visualAcuity at final follow up.
CONCLUSION
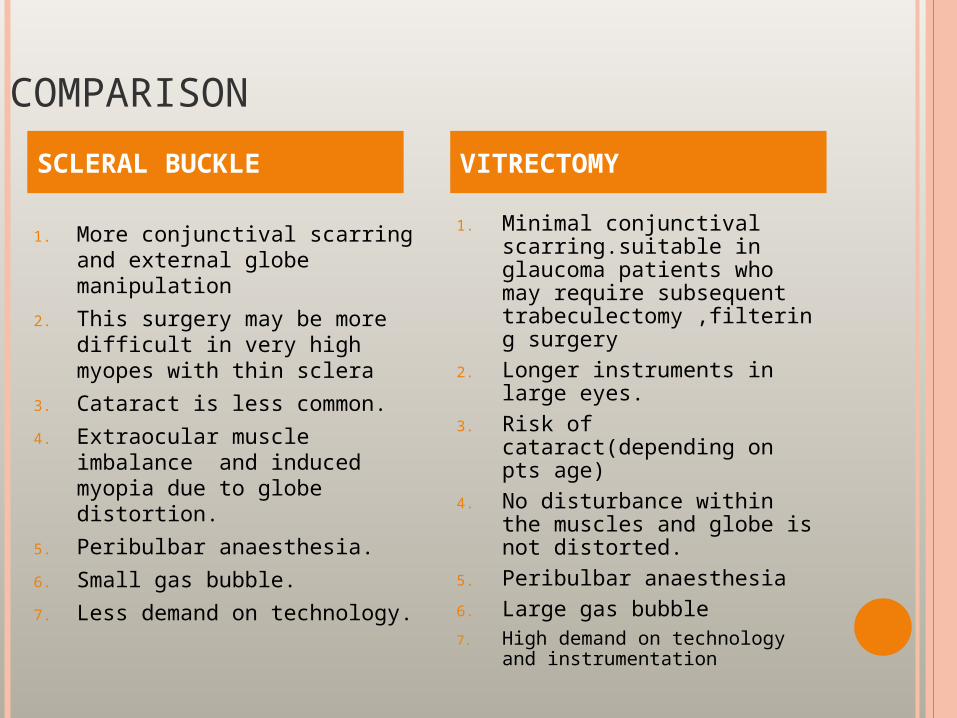
COMPARISON
SCLERAL BUCKLE
1. More conjunctival scarring and external globe manipulation
2. This surgery may be more difficult in very high myopes with thin sclera
3. Cataract is less common.
4. Extraocular muscle imbalance and induced myopia due to globe distortion.
5. Peribulbar anaesthesia.
6. Small gas bubble.
7. Less demand on technology.
VITRECTOMY
1. Minimal conjunctival scarring.suitable in glaucoma patients who may require subsequent trabeculectomy ,filtering surgery
2. Longer instruments in large eyes.
3. Risk of cataract(depending on pts age)
4. No disturbance within the muscles and globe is not distorted.
5. Peribulbar anaesthesia6. Large gas bubble7. High demand on technology
and instrumentation

BRITISH JOURNAL OFOPHTHALMOLOGY,2008,92,148387
23 GUAGE VERSUS 20 GUAGE SYSTEM FOR PARS PLANA VITRECTOMY:A SYSTEM FOR PROSPECTIVE RANDOMISED CLINICAL TRIAL.
Aim: To compare the sutureless 23-gauge system with a standard 20-gauge system in pars plana vitrectomy. .
Results: Conjunctival injection (p = 0.0003) and postoperative pain (p
= 0.01) were significantly reduced following 23-gauge vitrectomy
compared with the 20-gauge procedure. Opening (p = 0.006) and
closure times (p<0.00001) were significantly shorter, and vitrectomy time (p = 0.001) significantly longer in the 23-gauge system compared with 20-gauge vitrectomy. However, retinal manipulation and overall surgery times did not differ significantly between both groups. The same applies for eye pressure, distance and reading acuity. Regarding complications, two choroidal haemorrhages and one flat serous choroidal detachment occurred in the 23-gauge group.
CONCLUSION
23 guage system for Pars plana vitrectomy offers more postoperative comfort to the patients.

GRAEFE’S ARCHIVE FOR CLINICAL AND EXPERIMENTAL OPHTHALMOLGY,APR 2009,VOL.247,NO.4,PG495-502
WILLIAM GUALTIERI
ONE PORT PLANA VITRECTOMY(25 G MICROINCISION)
A pilot study to test a novel, minimal invasive vitrectomy, through one-port pars plana sclerotomy, by 25-G instruments, for selected vitreous, macular and vitreomacular interface disorders
Results All OPPPVs by 25 G were completed as planned. Anatomical surgical objectives were fulfilled on all eyes; functional ones on 13 out of 14 eyes. The whole OPPPV group and four of the phaco OPPPV subset of patients tolerated comfortably less than 30′ surgical time, and three phaco OPPPV ones less than 45′. Full regimen anti-inflammatory therapy for 2 weeks kept ten eyes out of 14 stable. Post-operatively, two eyes developed a transient alteration of the intraocular pressure. At the end of the follow-up, neither retinal detachment nor endophthalmitis occurred.
OPPPV by 25 G techniques promise to be an effective,comfortable, possible office-based alternative “micro-incisional, minimal invasive vitreous surgery” for selected vitreous, macula and vitreomacular interface disorders. Future research on the safety of the OPPPV by 25 G techniques compared to conventional ones is encouraged.
CONCLUSION

VITREOUS SUBSTITUTES
To restore intraocular volume after drainageof subretinal fluid or vitrectomy
To hydrokinetically manipulate retina To complement the surgical techniques
employed in membrane dissection(delamination &retinotomy)
as postoperative adjunct to vitreoretinal surgery for internal tamponade.
SUBSTANCES USED INTRAOPERATIVELY Balanced salt solution Air and other gases Viscoelastic fluids(sodium hyaluronate,chondroitin
sulfate,HPMC) SILICON LIQUID
LOW VISCOSITY PFCL(PERFLUORO N OCTANE)
INTRAOCULAR GASES xenon Air Sulfur hexafluoride Perfluoroethane perfluoropropane

To examine the effects of perfluorocarbon liquid (PFCL) and silicone oil (SO) on human retinal pigment epithelium (RPE) cells and retinal ganglion cells (RGCs) in vitro.
Results: Perfluorocarbon liquid affected the survival of ARPE-19 cells and RGCs when compared with the nontreated control group. ARPE-19 cells decreased significantly after being in contact with PFCL at the baso-lateral side for 7 days. However, PFCL contact at the apical side reduced the number of RGCs in a time-dependent manner. In case of SO, the viability of the ARPE-19 cells decreased significantly after being in contact with SO at the baso-lateral side for 7 days. However, SO did not reduce the number of RGCs after a 3-day exposure.
Effects of Perfluorocarbon Liquids and Silicone Oil on Human Retinal Pigment Epithelial Cells and Retinal Ganglion Cells
INOUE, MAIKO MD; IRIYAMA, AYA MD; KADONOSONO, KAZUAKI MD, PhD; TAMAKI, YASUHIRO MD, PhD; YANAGI, YASUO MD, PhD
JOURNAL OF RETINA,MAY 2009,VOL29 ISSUE 5 PG 677-681

Perfluorocarbon liquid is directly toxic to ARPE-19 cells when exposed to the cells for 7 days. On the contrary, it seems that RGCs are damaged in a time-dependent manner by the more mechanical rather than toxic effects of PFCL. Silicone oil seems to exert mechanical rather than toxic effects on ARPE-19 cells. When PFCL is used as a postoperative tamponade clinically, understanding the difference in the effects will lead to more effective and safer results.
CONCLUSION

The history and development of 25-gauge and 23-gauge vitrectomy are reviewed in this paper and compared with 20-gauge vitrectomy, the historical gold standard. Current advantages and disadvantages of each are delineated
. Recent findings: Transconjunctival sutureless vitrectomy continues to offer advantages of increased patient comfort decreased operative times and improved postoperative astigmatism. These advantages, however, must be weighed against the possibility of increased rates of postoperative hypotony and endopthalmitis.
CURRENT OPINION IN OPHTHLAMOLOGY 20(3):195-199, MAY 2009 Spirn, Marc J
COMPARISON OF 25,23 AND 20 GUAGE VITRECTOMY

Both 25-gauge and 23-gauge instruments continue to evolve, and have improved significantly since their introductions. Most cases can now be performed using either 25-gauge or 23-gauge techniques with success rates comparable to 20-gauge. Despite these advantages, there are still cases where 20-gauge is appropriate and preferable. Clinical experience, innovations and further studies will help dictate the future course of pars plana vitrectomy instrumention
CONCLUSION

20guage 25guage 23guage
1.15 mm incision
0.55 mm 0.72mm
Requiring suture
sutureless sutureless
Inner dia =0.91mm
Inner=0.57mmOuter=0.62mm
Inner=0.65mmOuter=0.75mm
Wt(g/4mm)130g
14gm 35gm
2500 cuts/min 1500cuts/min 2500 cuts/min
Distance(tip to port)=0.43mm
0.33mm 0.23mm
Illumination(xenon)65 lumens
30lumens 37 lumens
Increased incisional inflammation
decreased decreased
Longer visual recovery period
faster faster
Low risk of endophthalmitis
Known risk Unknown risk
5-15%cases of retinal breaks
Decreased risk of iatrogenic retinal tears
Intermediate risk

ADVANTAGES OF MIVS(23G,25G)OVER TRADITIONAL20 G VITRECTOMY
Sutureless Self sealing incisions Less conjunctival scarring Less corneal astigmatism Less operating time Less postoperative inflammation Rapid visual recovery Patient comfort Reduced incidence of vitreous
prolapse(cannula system)

LIMITATIONS OF MIVS
FLEXIBILITY LEARNING CURVE COST

RECENT DEVELOPMENTS
Macular translocation RPE Transplantation Retinal cell transplantation Retinal prosthesis Stem cell research Iris pigment epithelial cell transplantation Sustained release ganciclovir
implant(vitrasert) Intravitreal
drugs(dexamethasone,triamcinolone)

THANKYOU