addressing mental health problems in youth on the spectrum ... · spectrum: individual and...
TRANSCRIPT
1
Addressing Mental Health Problems in Youth on the Spectrum: Individual and Contextual Solutions Jonathan A. Weiss, Ph.D., C.Psych.
Oklahoma Statewide Autism Conference, November 2018

2
Overview• Individual-contextual approach to mental health
• The individual as the target
• The family as target
• The community as target
3
Mental health problems in youth with autism
• 4-5x greater than youth in the general population (Totsika et al. 2011)
• 70% will meet criteria for at least one psychiatric disorder, and many meet criteria for multiple conditions (Simonoff et al., 2008)
• Overall rates may be inflated due to miscoding autism symptoms, but the same pattern emerges (Mazefsky et al, 2012)

4
It’s not just about autism
19 22 18
84
6474
63
46 42
87
6571
0102030405060708090
100
Hyperactivity Conductproblems
Emotionalproblems
%ComparisonASDIDASD/ID
• Population based study of 5 to 16 year olds in the UK; M age = 10 years (SD = 3.0) (Totsika et al., 2011)
5
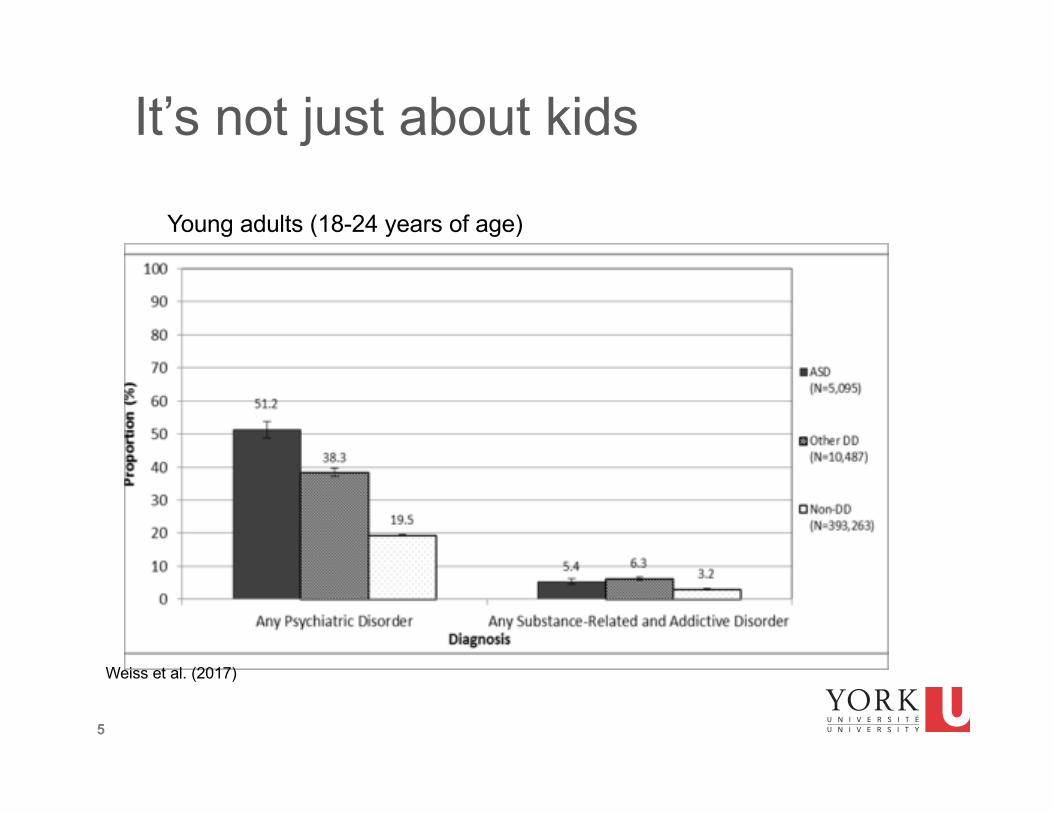
It’s not just about kids
Weiss et al. (2017)
Young adults (18-24 years of age)
6
It’s not just about anxiety
• Transdiagnostic processes
• Anxiety can be the tip of the iceberg
• Depression and anxiety are correlated with externalizing issues (noncompliance, aggressive behaviour, and irritability)
• Many psychiatric diagnoses at the same time
7
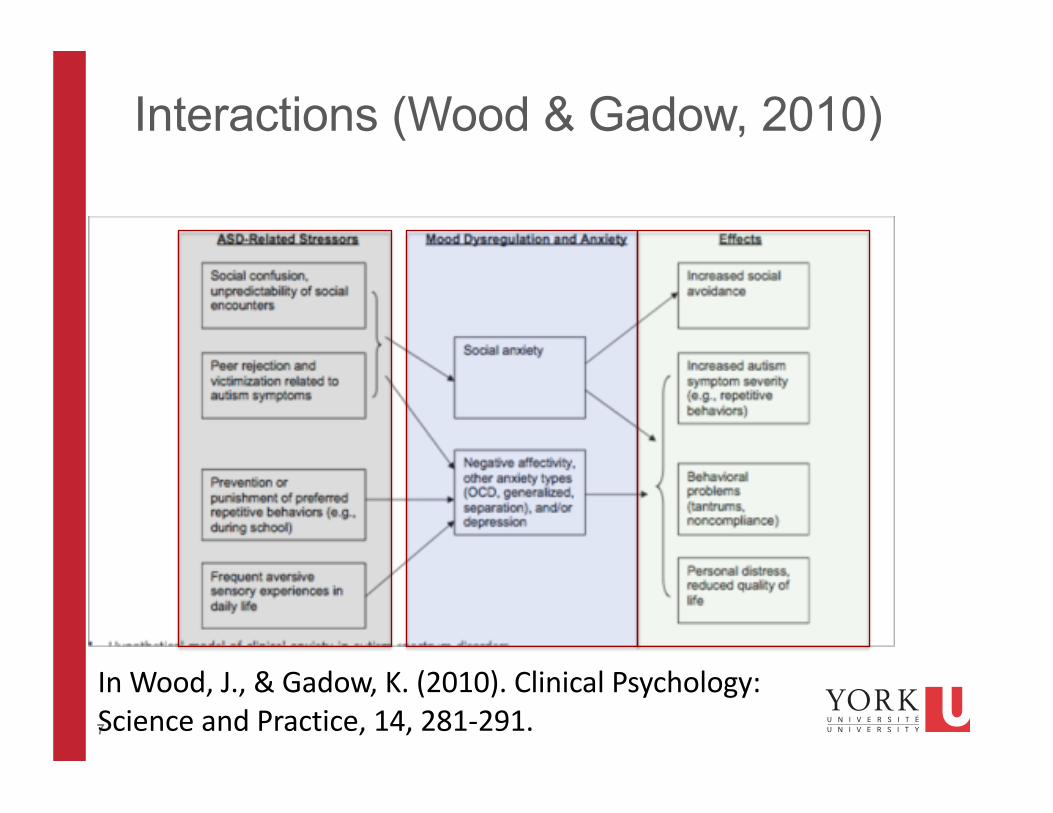
Interactions (Wood & Gadow, 2010)
In Wood, J., & Gadow, K. (2010). Clinical Psychology: Science and Practice, 14, 281-291.
8
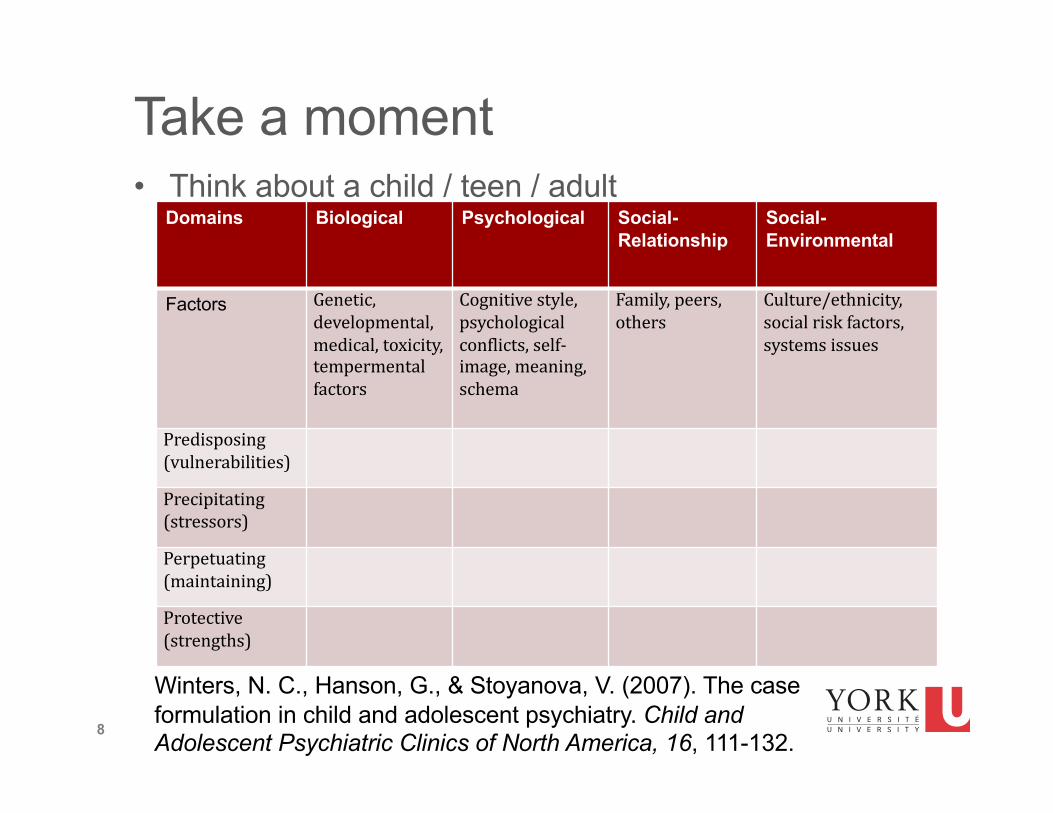
Take a moment• Think about a child / teen / adult
Domains Biological Psychological Social-Relationship
Social-Environmental
Factors Genetic,developmental,medical,toxicity,tempermentalfactors
Cognitivestyle,psychologicalconflicts,self-image,meaning,schema
Family,peers,others
Culture/ethnicity,socialriskfactors,systemsissues
Predisposing(vulnerabilities)Precipitating(stressors)Perpetuating(maintaining)Protective(strengths)
Winters, N. C., Hanson, G., & Stoyanova, V. (2007). The case formulation in child and adolescent psychiatry. Child and Adolescent Psychiatric Clinics of North America, 16, 111-132.
9
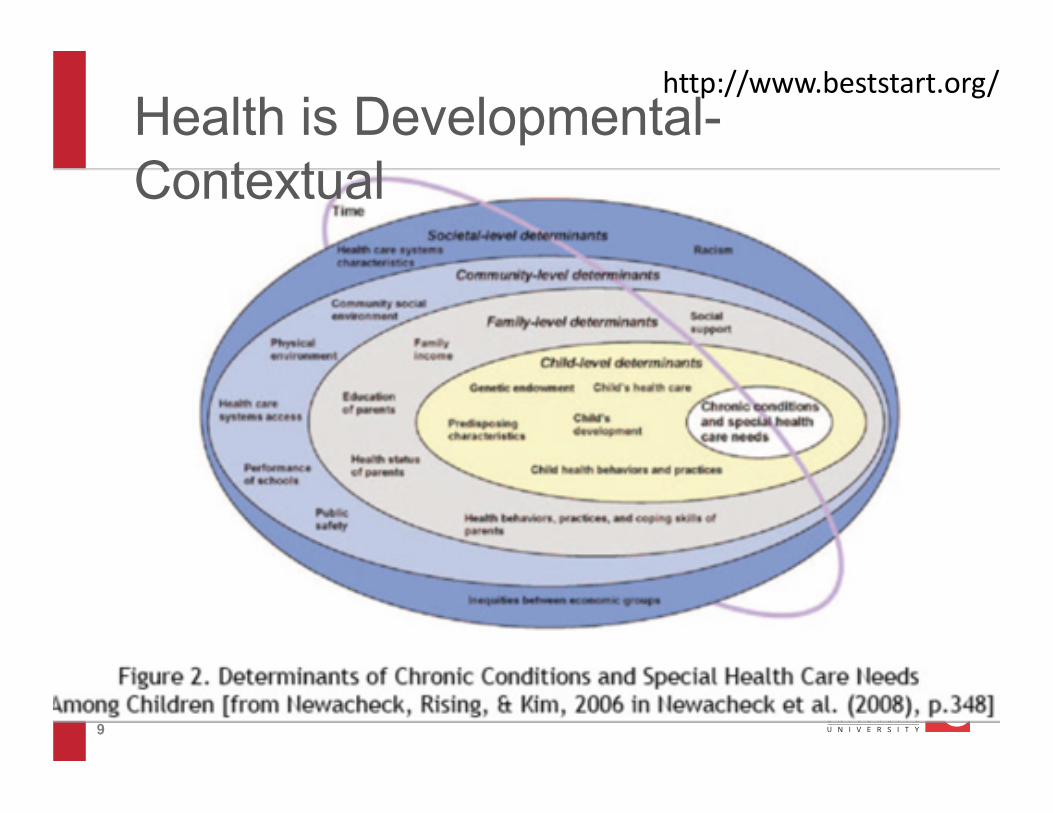
Health is Developmental-Contextual
http://www.beststart.org/

10
Move beyond a deficit focused approach• The absence of mental health problems is not exactly
the same thing as good mental health
• If I were to ask you to describe how mentally healthy you are, what words would you use?
• Positive outcomes need to be defined by positive constructs
• If I were to ask you to describe what successful living means to you, what words would you use?
11
A role for positive psychology• Most of the field of developmental disabilities has been
a deficit and pathology model (Dykens, 2006)
• Understanding what’s wrong with people only tells us so much about what contributes to people doing well (Seligman, 2002)• Happiness, flow, thriving beyond simply reducing
psychological suffering• In the general population, it is related to improved problem
solving, learning, health and longevity (Fredrickson, 2001)
• More work is needed• To inform operationalization and measurement, and
ultimately to treatment planning

12
Mental health as an individual-contextual developmental process
Key ecological assets in school, family, and community:• Positive people• Physical and institutional
resources• Collective activity• Positive opportunities
Key individual strengths (including intentional self-regulation):• Academic• Cognitive• Social• Physical• Emotional
Positive Development:CompetenceConfidenceConnectionsCharacterCaring
Contribution to:SelfFamilyCommunityCivic society
Internalizing and externalizing problems (mental health problems)
+
-
Mueller… Lerner et al., 2011
13
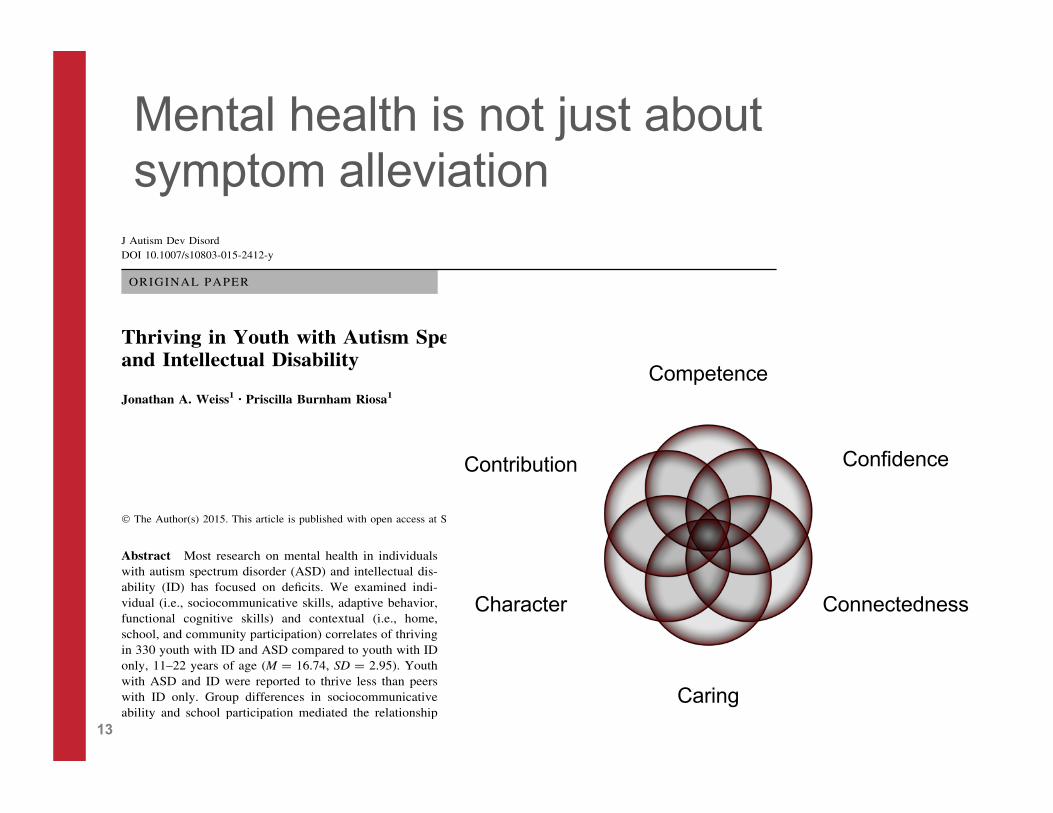
ORIGINAL PAPER
Thriving in Youth with Autism Spectrum Disorderand Intellectual Disability
Jonathan A. Weiss1• Priscilla Burnham Riosa1
! The Author(s) 2015. This article is published with open access at Springerlink.com
Abstract Most research on mental health in individualswith autism spectrum disorder (ASD) and intellectual dis-
ability (ID) has focused on deficits. We examined indi-
vidual (i.e., sociocommunicative skills, adaptive behavior,functional cognitive skills) and contextual (i.e., home,
school, and community participation) correlates of thriving
in 330 youth with ID and ASD compared to youth with IDonly, 11–22 years of age (M = 16.74, SD = 2.95). Youth
with ASD and ID were reported to thrive less than peers
with ID only. Group differences in sociocommunicativeability and school participation mediated the relationship
between ASD and less thriving. Research is needed to
further elucidate a developmental-contextual frameworkthat can inform interventions to promote mental health and
wellness in individuals with ASD and ID.
Keywords Autism spectrum disorder ! Intellectualdisability ! Special Olympics ! Thriving ! Mental health !Positive psychology ! Positive outcomes
Introduction
Individuals with autism spectrum disorder (ASD) and in-
tellectual disability (ID) have significant and pervasivesupport needs across many life domains, including educa-
tional, health, and community areas, and many struggle
with emotional and behavior problems (Mannion et al.
2014; Simonoff et al. 2008; White et al. 2009). In the mostrecent CDC (2014) report, 31 % of youth with ASD had
intellectual skills in the ID range (with another 23 % in the
borderline range), although estimates across studies rangewidely, from 26 to 68 % (CDC 2012; Fombonne 2005;
Yeargin-Allsopp et al. 2003). We also know a great deal
about the correlates of these pervasive needs, at individual(e.g., age, sex, diagnosis: Anagnostou et al. 2014), family
(e.g., parent stress: Witwer and Lecavalier 2008), and more
distal social levels (e.g., socio-economic status: Emersonand Hatton 2007). Understandably, research has largely
focused on these problem behaviors and the remediation of
negative outcomes, and we know far less about theseyouths’ strengths or how to promote positive outcomes,
such as happiness, satisfaction, or resilience (Dykens
2006).There is a role for positive psychology in identifying the
characteristics of wellbeing and the situations that promote
thriving, in a way that is more balanced than focusing solely onwhat is deficient (Gillham and Seligman 1999; Schalock
2004). Studies of positive or optimal outcomes of individualswith ASD are limited (Fein et al. 2013; Magiati et al. 2014).
Indeed, thriving is an important but almost altogether unused
term in the ASD research literature. Benson and Scales (2009)define thriving as ‘‘an individual’s pursuing a life path on
which individual or functionally-valued behaviors grow (e.g.,
character, confidence, caring) and move the person towardattainment of an ‘idealized personhood’ characterized by so-
cially or structurally-valued behaviors such as contribution to
self, family, community, and civil society (Lerner 2006)’’(p. 90). Thriving reflects both wellbeing and an upward de-
velopmental trajectory, the demonstration of continued growth
of knowledge and skills, and success in relationships withothers (Carver 1998), and ultimately, contributions in a
meaningful way to oneself and one’s environments according
& Jonathan A. [email protected]
1 Department of Psychology, York University, BehaviouralScience Building, 4700 Keele Street, Toronto, ON M3J 1P3,Canada
123
J Autism Dev Disord
DOI 10.1007/s10803-015-2412-y
Mental health is not just about symptom alleviation
Competence
Confidence
Connectedness
Caring
Character
Contribution
14
Components of thriving• Competence: My child has the skills to succeed in school, in
social situations with friends and adults, in play, and at home. My child knows how to behave and does what is needed to do well.
• Confidence: My child believes that he/she can succeed and do what is needed to do well in the family, in school, in social situations with friends and adults, in play and in other areas that are important to him/her (for example, sports, music, religious activities).
• Connectedness: My child has positive relationships with his/her parents, siblings, and other family members, and with friends, teachers, coaches, or mentors
Adapted with permission from the 4-H Study of Positive Youth Development. PI: Richard M. Lerner, Tufts University
15
Components of thriving• Caring: My child cares about other people. He or she is concerned
about whether others have what they need (shows sympathy) and shows a sense of compassion (empathy). My child is both sympathetic and empathetic to others.
• Character: My child knows what is right and wrong; and does the right thing; My child is open to others’ perspectives and believes in social justice for all. My child is honest.
• Contribution to self/others/community: My child tries to do things to help the family, to help neighbors, and to help the community. My child tries to also help himself/herself by staying healthy (eating right, exercising, getting enough sleep).
Adapted with permission from the 4-H Study of Positive Youth Development. PI: Richard M. Lerner, Tufts University

16
ASD status Thrivingc’
Cognitive ability
Sociocommunicative
Home participation
School participation
Community participation
a (p < .001)
a (p < .01)
b (p < .001)
b (p < .001)
b (p < .01)
b (p < .001)
Adaptive behaviour
a (p < .001)
Age
Gender

17
We can work with the individual• In any one domain, or in many, we can struggle• It may also be our relative strength
Self-regulation
Cognitive
Academic Social
Physical
Emotional
Spiritual
18
Lots of manuals• Facing Your Fears (Reaven, et
al., 2011). Paul Brookes.• Child anxiety disorders: A
family-based treatment manual for practitioners (Wood, et al., 2008). WW Norton & Co.
• Exploring Feelings (anger / anxiety) Attwood, 2004). Future Horizons.
• Coping Cat (Kendall & Hedtke, 2006). Workbook Pub.
19
Where’s the evidence?
• Overall effectiveness of CBT• Recent systematic review and meta analysis (Weston,
Hodgekins & Langdon, 2016)• 48 studies met inclusion criteria• High risk of bias• 24 studies addressed affective problems
• 17 were < 18 years• 15 group based• 19 targeted anxiety• 14 were RCTs• Small to medium effect sizes, when using informant report or
clinician ratings
19

20
Where’s the evidence?
• CBT reduces symptoms of anxiety• Most between 8 – 15 years of age
• Usually 14-16 sessions, but can go as high as 32
• 50% to 70% show considerable improvement
• We know little in terms of long term maintenance
• Participants without ID
• Perhaps anger (Sofronoff, Attwood, Hinton, & Levin, 2007)
• Maybe emotion regulation (
• ABA to shape behaviour, including reducing maladaptive behaviour, evidence base throughout development (Wong et al. 2013)
• Focus on shaping individual behaviour, but also address contingencies with environment and antecedent strategies can involve altering the environment
21
Categories of issues and challenges reported by therapists
• Rigidity or B&W thinking• Pacing (needing to go slower)• Communication issues (e.g., literal
use of language)• Problems with therapeutic
relationship• Adaptive or including written
materials
• Difficulty recognizing and understanding emotions
• Co-occurring problems and problem identification
• Difficulties generalizing• Systemic factors• Not completing
homework• Sensory issues
Cooper, K., Loades, M., Russell, A. Adapting psychological therapies for autism. Research in Autism Spectrum Disorders, 45, 43-50.
22
CBT to focus on emotion regulation

23
An RCT to evaluate CBT targeting emotion regulation: SAS:OR
The Secret Agent Society: Operation Regulation was developed by Dr. Renae Beaumont (University of Queensland, Australia), based on the evidence-based Secret Agent Society
Support from the CIHR Chair in ASD Treatment and Care Research
24
Review of Materials• Handbooks
• Cadet Handbook• Parent Handbook• Teacher Handouts• Facilitator Manual• Weekly therapist forms • Weekly parent/child feedback forms
• SAS-OR Session Materials:• Challenge Card • Manipulatives: Codecards, holder,
stress ball• Emotionometer and Stickers• Computer game

25
Parent report of ER
• Overall emotion regulation in social situations (ERSSQ)• F (1, 57) = 12.94, p = .001, d = .96
• Pairwise• TI change, p < .001 vs WLC change, p =.59

26
• Overall psychiatric symptom severity (ADIS Severity Score)
• F (1, 57) = 4.56, p = .04, d = .56
• Pairwise• TI change, p < .001 vs WLC change, p =.54
Clinician ratings
27
Where’s the evidence?• Recent attention to mindfulness-based therapy (Cachia
et al. 2016)• 6 studies identified: 3 pre-post design, 2 multiple baseline
design, 1 employed an RCT
• Anxiety and thought problems in children• Aggression, well-being and social responsiveness in
teens • Reduced anxiety, depression and rumination in adults
28
But
• CBT (ERP) vs. anxiety management therapy to address OCD in teens and adults with autism (Russell et al. 2013)
• CBT vs. non-directive person-centered counselling to address anxiety in teens with autism (Murphy et al. 2017)
• CBT vs. MBSR to address anxiety and depression in adults with autism (Sizoo & Kuiper, 2017)
• Group CBT vs. group recreational activities for adults with autism to improve quality of life, self-esteem and psychiatric symptoms (Hesselmark, Plenty & Beejerot, 2014)
• CBT vs. a social recreation program in adolescents with autism to address anxiety (Sung et al. 2011)
• CBT vs. treatment as usual to address anxiety disorders in adults with autism (Langdon et al. 2016)
29
MYMind: Parent-youth concurrent treatmentYouth• awareness, self-control,
distress tolerance
Parents• impact of reactivity, attend
to youth non-judgmentally, acceptance of youth and their own feelings about parenting
Funded by Kids Brain Health Network (formerly NeuroDevNet)
30
Where’s the evidence?• Psychotropic medication use (Jobski, Hofer, Hoffman &
Bachmann, 2016)• 47 studies• Some evidence for “ASD related irritability” children and
teens, ADHD medication for ADHD symptoms in ASD• Evidence for anti-depressants is very limited
• Many reviews seems to suggest the need for far more work and some form of caution in use of medication to address mental health problems (Dove et al., 2012; McPheeters et al., 2011)

31
We can work with broader contexts• Context matters greatly
Social inclusion
Personal resources
Positive people
Collective activity
Positive opportunities
Positive places
Institutional resources

32
Parental positive affect is a resiliency factor
33
Positive peers
• Peer relationships or supports• The challenge of inclusive education (Rotheram-Fuller, Kasari,
Chamberlain & Locke, 2010)• Less likely to be accepted and fewer reciprocal friendships• More likely to be isolated or peripheral to social
relationships, with increasing isolation with grade
• “Promoting children with ASD’s skills in popular activities to share with peers in early childhood may be a key preventive intervention...”
• Social inclusion is the experience of belonging while participating in meaningful social activities

34
Positive peers
Theme 1: ConnectednessTheme 2: Training in Sport
35
Positive people• Mentorship
programs• SFU’s Autism
Mentorship Program
• York U’s Asperger Mentorship Program
Supporting students on the autism spectrum student mentor guidelines
By Catriona Mowat, Anna Cooper and Lee Gilson
36
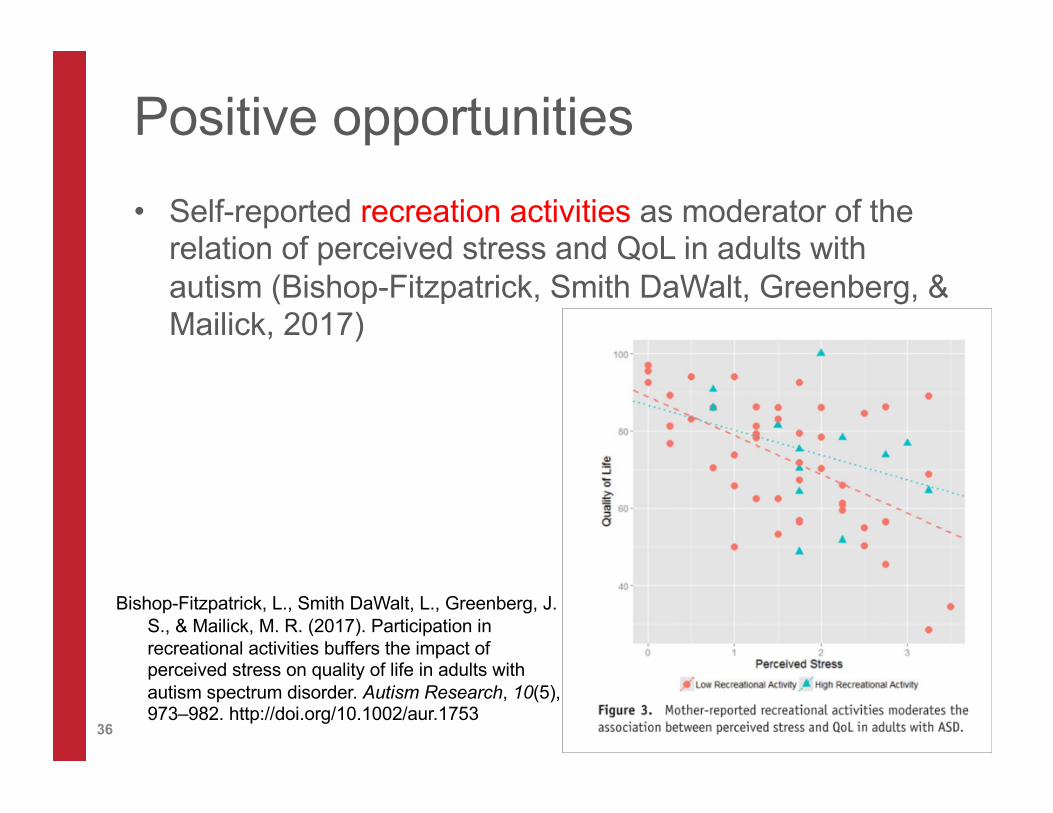
Positive opportunities
• Self-reported recreation activities as moderator of the relation of perceived stress and QoL in adults with autism (Bishop-Fitzpatrick, Smith DaWalt, Greenberg, & Mailick, 2017)
Bishop-Fitzpatrick, L., Smith DaWalt, L., Greenberg, J. S., & Mailick, M. R. (2017). Participation in recreational activities buffers the impact of perceived stress on quality of life in adults with autism spectrum disorder. Autism Research, 10(5), 973–982. http://doi.org/10.1002/aur.1753

37
Working with communities

38

40
Final thoughts
n Skills to manage stress
n Good physical health and physical activity
n Sense of control over one’s life
n Reciprocal, non-stressful relationships
n Caregivers who are nurtured and supported to promote mental health in those they care for
n A safe place to live and learn
n An environment with limited stresses
n Meaningful activities in community
Individual Family
Environment Society
41
• Identify at least two things you learned during this presentation to apply in your personal or professional life.
• Identify three steps you will take in the next month to implement what you learned in your personal or professional life

42
Thank you! Questions?
Jonathan Weiss, PhD,CPsych
Associate Professor
Dept. of Psychology
York University
Tel: 416-736-5891
http://www.tedxyorkusalon.orghttp://asdmentalhealth.blog.yorku.ca/

43
References• Cachia, R. L., Anderson, A., & Moore, D. W. (2016). Mindfulness in Individuals with Autism
Spectrum Disorder: a Systematic Review and Narrative Analysis. Review Journal of Autism and Developmental Disorders, 3(2), 165–178.
• Dykens, E. M. (2006). Toward a positive psychology of mental retardation. American Journal of Orthopsychiatry, 76(2), 185–193.
• Mazefsky, C. A., Oswald, D. P., Day, T. N., Eack, S. M., & Minshew, N. J. (2012). ASD, a psychiatric disorder, or both? Psychiatric diagnoses in adolescents with high-functioning ASD. … Child & Adolescent …, 41(4), 516–523.
• Mueller, M. K., Phelps, E., Bowers, E. P., Agans, J. P., Urban, J. B., & Lerner, R. M. (2011). Youth development program participation and intentional self-regulation skills: Contextual and individual bases of pathways to positive youth development. Journal of Adolescence, 34(6), 1115–1125.
• Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric Disorders in Children With Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47(8), 921–929.

44
References• Sofronoff, K., Attwood, T., Hinton, S., & Levin, I. (2007). A randomized controlled trial of a
cognitive behavioural intervention for anger management in children diagnosed with Asperger syndrome. Journal of Autism and Developmental Disorders, 37(7), 1203–1214.
• Taylor, J. L., & Seltzer, M. M. (2012). Developing a Vocational Index for Adults with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders, 42(12), 2669–2679.
• Tint, A., Thomson, K., & Weiss, J. A. (2017). A systematic literature review of the physical and psychosocial correlates of Special Olympics participation among individuals with intellectual disability. Journal of Intellectual Disability Research, 61(4), 301–324.
• Totsika, V., Hastings, R. P., Emerson, E., Berridge, D. M., & Lancaster, G. A. (2011). Behavior Problems at 5 Years of Age and Maternal Mental Health in Autism and Intellectual Disability. Journal of Abnormal Child Psychology, 39(8), 1137–1147.
• Rotheram-Fuller, E., Kasari, C., Chamberlain, B., & Locke, J. (2010). Social involvement of children with autism spectrum disorders in elementary school classrooms. Journal of Child Psychology and Psychiatry, 51(11), 1227–1234.

45
References• Sung, M., Ooi, Y. P., Goh, T. J., Pathy, P., Fung, D. S. S., Ang, R. P., … Lam, C. M. (2011). Effects of
Cognitive-Behavioral Therapy on Anxiety in Children with Autism Spectrum Disorders: A Randomized Controlled Trial. Child Psychiatry & Human Development, 42(6), 634–649.
• Weiss, J. A. (2014). Transdiagnostic Case Conceptualization of Emotional Problems in Youth with ASD: An Emotion Regulation Approach. Clinical Psychology: Science and Practice, 21(4), 331–350.
• Weiss, J. A., & Burnham Riosa, P. (2015). Thriving in Youth with Autism Spectrum Disorder and Intellectual Disability. Journal of Autism and Developmental Disorders, 45(8), 2474–2486.
• Weiss, J. A., Cappadocia, M. C., Tint, A., & Pepler, D. (2015). Bullying Victimization, Parenting Stress, and Anxiety among Adolescents and Young Adults with Autism Spectrum Disorder. Autism Research, 8(6), 727–737.
• Weiss, J. A., Thomson, K., Burnham Riosa, P., Albaum, C., Chan, V., Maughan, A., … Black, K. (2018). A randomized waitlist-controlled trial of cognitive behavior therapy to improve emotion regulation in children with autism. Journal of Child Psychology and Psychiatry.
46
References• Weiss, J. A., Isaacs, B., Diepstra, H., Wilton, A. S., Brown, H. K., McGarry, C., & Lunsky, Y.
(2017). Health Concerns and Health Service Utilization in a Population Cohort of Young Adults with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders.
• Weston, L., Hodgekins, J., & Langdon, P. E. (2016). Effectiveness of cognitive behavioural therapy with people who have autistic spectrum disorders: A systematic review and meta-analysis. Clinical Psychology Review.
• Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., … Schultz, T. R. (n.d.). Evidence-Based Practices for Children, Youth, and Young Adults with Autism Spectrum Disorder: A Comprehensive Review. Journal of Autism and Developmental Disorders.
• Winters, N. C. (2007). The case formulation in child and adolescent psychiatry., 16(1), 111– 132.
• Wood, J. J., & Gadow, K. D. (2010). Exploring the Nature and Function of Anxiety in Youth with Autism Spectrum Disorders. Clinical Psychology: Science and Practice, 17(4), 281-292.