acute renal replacement therapy for the infant jordan m. symons, md university of washington school...
TRANSCRIPT
Acute Renal Replacement Therapy for the Infant
Jordan M. Symons, MDUniversity of Washington School of Medicine
Children’s Hospital & Regional Medical CenterSeattle, WA

Objectives
• Indications and goals for acute renal replacement therapy
• Modalities for renal replacement therapy– Peritoneal dialysis– Intermittent hemodialysis– Continuous renal replacement therapy
(CRRT)
• Special issues related to the infant
Indications for Renal Replacement
• Volume overload
• Metabolic imbalance
• Toxins (endogenous or exogenous)
• Inability to provide needed daily fluids due to insufficient urinary excretion

Goals of Renal Replacement
• Restore fluid, electrolyte and metabolic balance
• Remove endogenous or exogenous toxins as rapidly as possible
• Permit needed therapy and nutrition
• Limit complications

Renal Replacement for the Infant: A Set of Special Challenges
• Small size of the patient
• Equipment designed for larger people
• Small blood volume will magnify effects of any errors
• Achieving access may be difficult
• Staff may have infrequent experience

Modalities for Renal Replacement
• Peritoneal dialysis
• Intermittent hemodialysis
• Continuous renal replacement therapy (CRRT)
Modalities for Renal Replacement
• Peritoneal dialysis
• Intermittent hemodialysis
• Continuous renal replacement therapy (CRRT)
PD: Considerations for Infants
ADVANTAGES• Experience in the
chronic setting• No vascular access• No extracorporeal
perfusion• Simplicity• ? Preferred modality
for cardiac patients?
DISADVANTAGES• Infectious risk• Leak• ? Respiratory
compromise?• Sodium sieving• Dead space in tubing
H2O
H2OH2O
H2O
H2O
H2O
H2O
H2O
H2O H2O
Sodium Sieving: A Problem of Short Dwell PD
Na+
Na+ Na+
Na+
H2O
Na+
Na+
Na+
Na+
Result: Hypernatremia

Dead Space: A Problem with Low Volume PD

Modalities for Renal Replacement
• Peritoneal dialysis
• Intermittent hemodialysis
• Continuous renal replacement therapy (CRRT)

IHD: Considerations for Infants
ADVANTAGES• Rapid particle and fluid
removal; most efficient modality
• Does not require anticoagulation 24h/d
DISADVANTAGES• Vascular access• Complicated• Large extracorporeal
volume• Adapted equipment• ? Poorly tolerated

Modalities for Renal Replacement
• Peritoneal dialysis
• Intermittent hemodialysis
• Continuous renal replacement therapy (CRRT)

Pediatric CRRT: Vicenza, 1984
CRRT for Infants: A Series of Challenges
• Small patient with small blood volume
• Equipment designed for bigger people
• No specific protocols
• Complications may be magnified
• No clear guidelines
• Limited outcome data

Potential Complications of Infant CRRT
• Volume related problems
• Biochemical and nutritional problems
• Hemorrhage, infection
• Thermic loss
• Technical problems
• Logistical problems
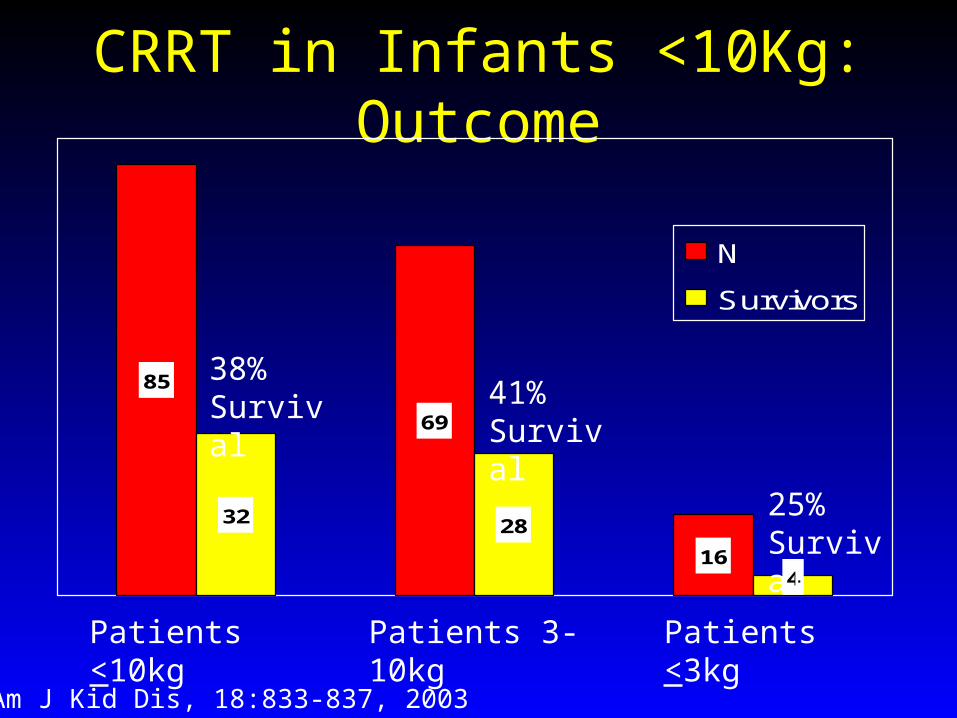
CRRT in Infants <10Kg: Outcome
85
69
16
32 28
4
N
Survivors
Patients <10kg Patients 3-10kg Patients <3kg
38% Survival 41%
Survival
25% Survival
Am J Kid Dis, 18:833-837, 2003

ppCRRT Data of Infants <10Kg: Demographic Information
Number of Subjects 84(51 boys (61%))(33 girls (39%))
Age Median 69 days(1 d - 2.9 y)
ICU Admit weight Median 4.4 kg(1.3 - 10 kg)
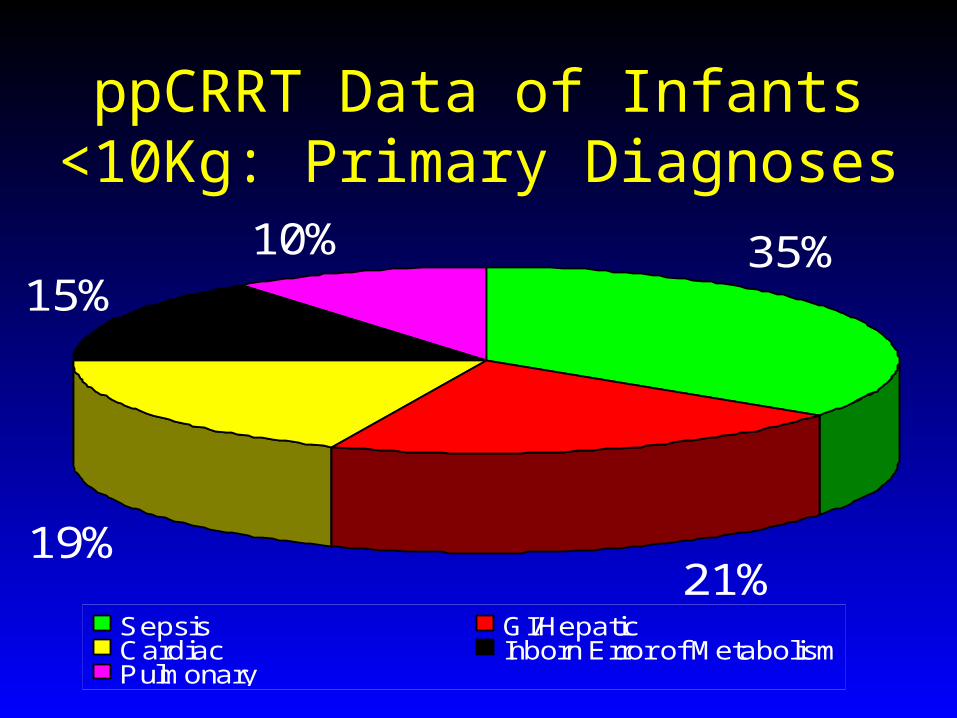
ppCRRT Data of Infants <10Kg: Primary Diagnoses
19%
10%
21%
15%35%
Sepsis GI/Hepatic Cardiac Inborn Error of MetabolismPulmonary

ppCRRT Data of Infants <10Kg: Indications for CRRT
Fluid Overload and Electrolyte Imbalance 84%
Other (Endogenous Toxin Removal) 16%
N=84

ppCRRT Data of Infants <10Kg: Clinical Data
Parameter Median Range
Days in ICU prior to CRRT 2 0 - 135
PRISM score — ICU admit 17.5 0 - 48
PRISM score — CRRT start 20 0 - 48
Inotrope number — CRRT start 1 0 - 4
Urine output — CRRT start(ml/kg/hr over prior 24hrs)
0.7 0 - 12
% Fluid overload from ICU admission to CRRT start
13.7 -28 - 220

ppCRRT Data of Infants <10Kg: Technical Characteristics of CRRT
Catheter Site Femoral 60%
Internal Jugular 28%
Subclavian 12%
Modality CVVHD 59%
CVVH 18%
CVVHDF 23%
Anticoagulation Citrate 55%
Heparin 45%
Prime Blood 87%
Saline 8%
Albumin 5%N=84
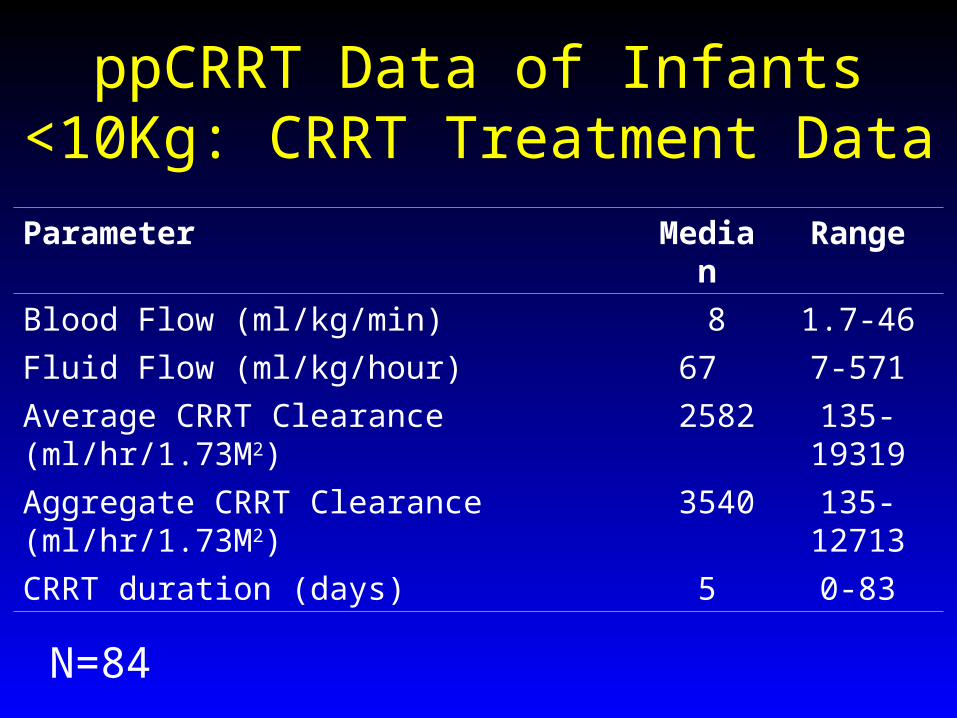
ppCRRT Data of Infants <10Kg: CRRT Treatment Data
N=84
Parameter Median Range
Blood Flow (ml/kg/min) 8 1.7-46
Fluid Flow (ml/kg/hour) 67 7-571
Average CRRT Clearance (ml/hr/1.73M2) 2582 135-19319
Aggregate CRRT Clearance (ml/hr/1.73M2) 3540 135-12713
CRRT duration (days) 5 0-83

ppCRRT Data of Infants <10Kg: Survival by Weight
0%
10%
20%
30%
40%
50%
60%
70%
<5 kg 5-10 kg <10 kg >10 kg
44% 42% 43% 64%
p=0.001
p=1.0
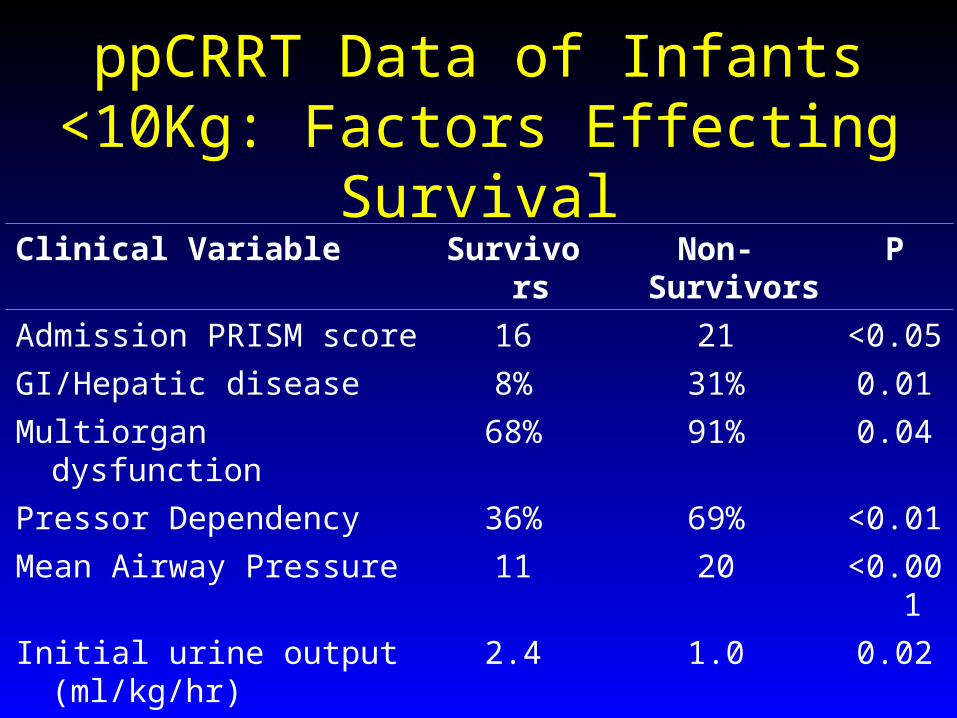
ppCRRT Data of Infants <10Kg: Factors Effecting Survival
Clinical Variable Survivors Non-Survivors P
Admission PRISM score 16 21 <0.05
GI/Hepatic disease 8% 31% 0.01
Multiorgan dysfunction 68% 91% 0.04
Pressor Dependency 36% 69% <0.01
Mean Airway Pressure 11 20 <0.001
Initial urine output (ml/kg/hr) 2.4 1.0 0.02
%Fluid Overload at Start 15% 34% 0.02
>10% Overload at Start 43% 71% 0.02

ppCRRT Data of Infants <10Kg: Survival by Return to Dry Weight
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Survivors Non-survivors
Dry Weight Achieved
Dry Weight Not Achieved
78%
35%
22%
65%

Infant CRRT at Children’s Hospital & Regional Medical Center, Seattle
Infant CRRT in Seattle: Overview
• Coordinated by nephrology
• Performed in infant/pediatric ICU
• Set up by dialysis nurses
• Run at the bedside by neonatology or critical care nurses
• Dedicated CRRT device– BM-25: 1999 – 2005– Prisma: 2005 - present

CRRT Access in the Neonate:What Works?
• Hemodialysis Line: 7 Fr double lumen
• Two single lumen lines:– 5 Fr catheters or introducers
• Umbilical lines:– 5 Fr UAC; 7 Fr UVC
• Leg position - be creative
• Tape on the skin - may need to get creative

PRISMA
• Dedicated CRRT device
• Highly automated
• Designed for ease of use at the bedside
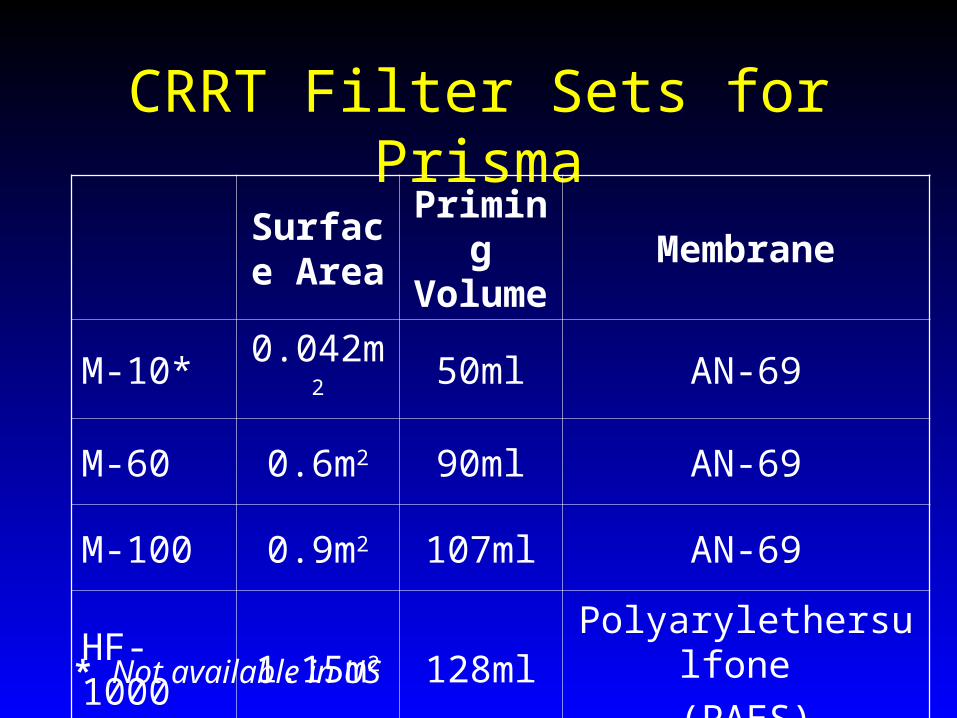
CRRT Filter Sets for PrismaSurface
AreaPriming Volume
Membrane
M-10* 0.042m2 50ml AN-69
M-60 0.6m2 90ml AN-69
M-100 0.9m2 107ml AN-69
HF-1000 1.15m2 128mlPolyarylethersulfone
(PAES)
* Not available in US

Bradykinin Release Syndrome
• Mucosal congestion, bronchospasm, hypotension at start of CRRT
• Resolves with discontinuation of CRRT
• Thought to be related to bradykinin release when patient’s blood contacts hemofilter
• Exquisitely pH sensitive
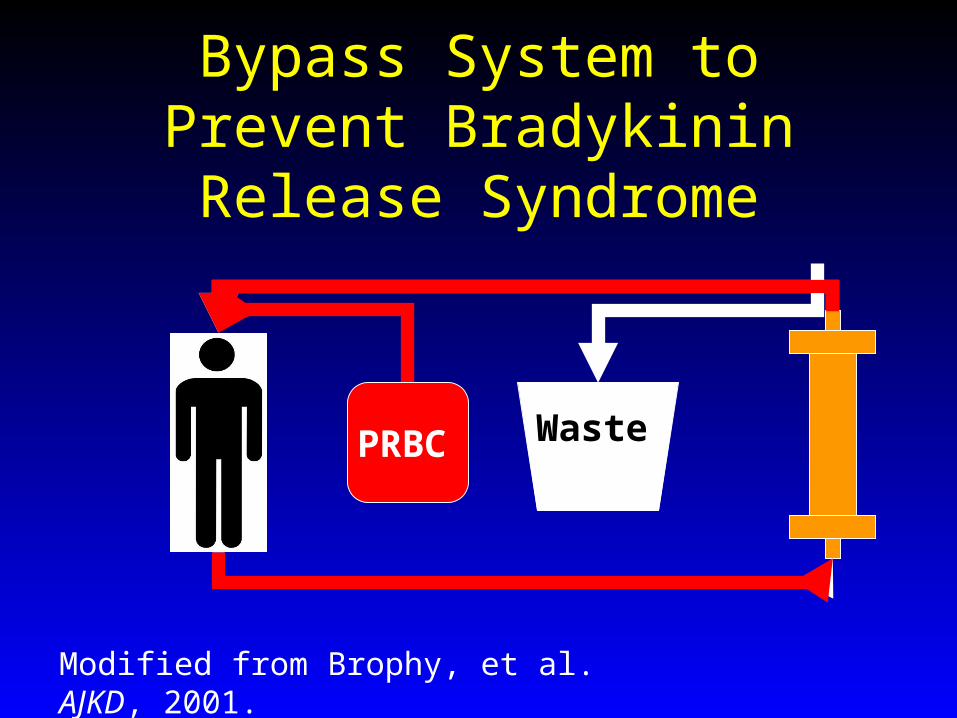
Bypass System to Prevent Bradykinin Release Syndrome
PRBC Waste
Modified from Brophy, et al. AJKD, 2001.
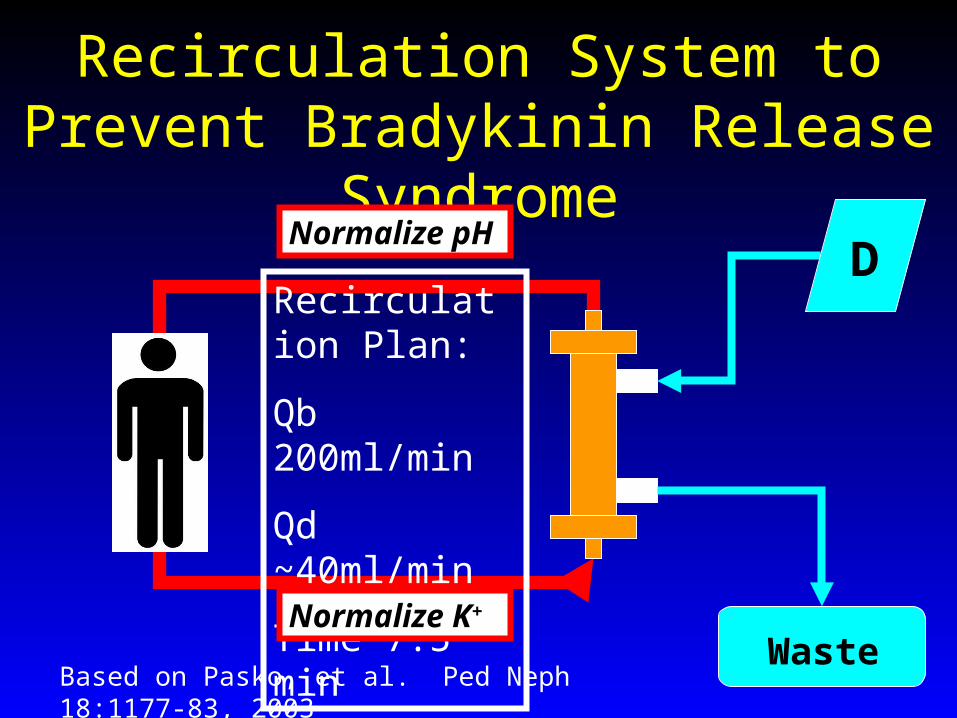
Recirculation System to Prevent Bradykinin Release Syndrome
D
Waste
Recirculation Plan:
Qb 200ml/min
Qd ~40ml/min
Time 7.5 min
Based on Pasko, et al. Ped Neph 18:1177-83, 2003
Normalize pH
Normalize K+

Simple Systems to Limit Likelihood of Bradykinin Release Syndrome
• Don’t prime on with blood
• Don’t use the AN-69 membrane
Thermal Regulation
• Hotline® blood warming tubing
• Place at venous return to patient
• Leave on at set temperature of 39 C
• Treat temp elevations if they occur
Infant CRRT in Seattle: CRRT Staffing
• Dialysis RN sets-up & initiates therapy
• PICU/IICU RN manages patient
• Nephrology/Dialysis RN on call 24/7
• Acuity assigned to pump as if a separate patient
• Staffing determined by acuity
Infant CRRT in Seattle: How to Handle a Rare Procedure
• Developed an Acute Initiation Checklist defining specific roles/actions for:– Infant ICU MD– Nephrology MD– Infant ICU RN– Dialysis RN– IV access MD
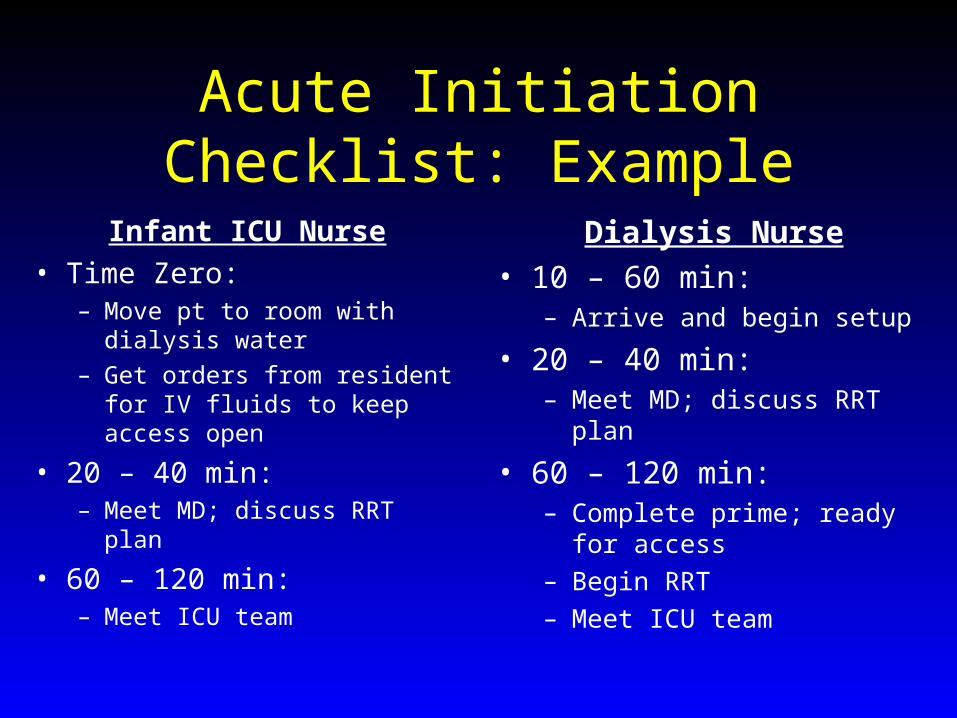
Acute Initiation Checklist: Example
Infant ICU Nurse• Time Zero:
– Move pt to room with dialysis water
– Get orders from resident for IV fluids to keep access open
• 20 – 40 min:– Meet MD; discuss RRT plan
• 60 – 120 min:– Meet ICU team
Dialysis Nurse• 10 – 60 min:
– Arrive and begin setup
• 20 – 40 min:– Meet MD; discuss RRT plan
• 60 – 120 min:– Complete prime; ready for
access– Begin RRT– Meet ICU team

Acute Initiation Checklist: Example
Nephrology MD• Time Zero:
– Contact dialysis nurse to start RRT urgently
• 10 – 20 min:– Bring catheters to ICU– Enter orders for RRT
• 20 – 40 min:– Meet ICU MDs & RNs,
discuss plan
• 60 – 120 min:– Present in ICU for initiation– Meet ICU team
IV Access MD• 10 – 30 min:
– Arrive and begin insertion of dialysis access
• 60 min (or when circuit is ready for Rx)– Complete insertion of access– Connect ports to heparin IV
solutions

Infant RRT: Summary
• All modalities of RRT possible for infants
• No modality is perfect
• Technical challenges can be met
• Careful planning with institution, program, and individuals improves care
• Cooperation, communication, and collaboration will increase our success

Thanks!