acute hemodynamic effects of intravenous nicardipine in patients treated chronically with...
TRANSCRIPT

Acute Hemodynamic Effects of Intravenous Nicardipine in Patients Treated Chronically with Propranolol
for Coronary Artery Disease
PAUL0 ROCHA, MD, DINA ZANNIER, MD, BERNARD BARON, MD, MICHEL PATHE, MD, DIDIER DAVID, MD, and JEAN-CLAUDE KAHN, MD
Intravenous nicardipine, 5 mg, was infused over 5 minutes in 2 comparable groups of 8 patients with chronic coronary artery disease but no clinical signs of heart failure. Eiiht pattents had received no pre- vious treatment and served as a control group; 8 other patients had received long-term treatment with large doses of proprandd. The hemodynamic responses to nifedipine were sfmilar in the 2 groups, but was greater in patients taking propranolol. At 10 minutes, systemic vascular resistance decreased by 47 % in patients taking propratxM and by 39% in the control group; mean aortk pressures decreased by 25% and 10%; heart rate increased by 23% and 19%; and cardiac index increased by 45% in both groups. At 20 minutes, left ventricular end-sys-
tolic volume index decreased by 20% in patients taking propranolol and 15% in the control patients; angiographic stroke index increased by 19% and 8 % ; left ventricular ejection fraction increased by 22 % and 11% ; and mean circumferential fiber ve- locity increased by 48 % and 32 % . Intravenous ni- cardipine infusion (5 mg) did not induce negative inotropic effects in patients with chronic coronary heart disease, and no evkknce of congestive heart failure was seen, even On patients recetving large doses of propranotot. Nicardiptne counteracted the potential deleterious effects of propranolol: in- creased peripheral vascular resistance and lefi ven- tricular stroke work and decreased cardiac output.
(Am J Cardiil 1987;59:775-781)
C alcium antagonist drug treatment causes a reduc- tion in myocardial contractility in vitro.lv2 However, this negative inotropic effect often cannot be mea- sured in intact animals or humans3s4 and can be coun- teracted by the secondary sympathetic response to the systemic hypotension often observed with these drugs.5-8 Use of calcium antagonists may be limited by negative inotropic and dromotropic effects in some patients, particularly when combined with B-blocking drug use. Cases of clinical cardiovascular disorders have been reported with nifedipine in patients receiv- ing p-blocking drugsgJO and with verapamil.1*J2 How- ever, some investigators, using a nifedipine-&blocker combination for subacute and in chronic administra- tion, found that this combination was not only well
From the Department of Cardiology, Centre Hospitalier Inter- communal de Poissy, Faculty of Medecine Paris-Ouest, Univer- sity Rene Descartes, Paris, France. Manuscript received June 12, 1986; revised manuscript received October 31, 1986, accepted November, 1986.
Address for reprints: Jean-Claude Kahn, MD, Department of Cardiology, Centre Hospitalier Intercommunal, 10, rue du Champ Gaillard, 78303 Poissy, France.
tolerated, but also therapeutically more effective.13-l5 Verapamil has also been given to patients taking pro- pranolol and has yielded further antianginal benefits and few important interactive effects.16 The same fur- ther benefits have been shown with use of a diltiazem- propranolol combination .I7 Wolfe et all* reported that this combination produces the same hemodynamic ef- fects as diltiazem alone in acute intravenous adminis- tration. Oesterle et al,lg studying the same drugs, observed 7 dangerous bradycardias in 19 patients and recommend electrocardiographic monitoring when drugs are combined acutely. Nevertheless, diltiazem may reverse some deleterious effects of propranolo120
In a broad review of the recent literature, Leon et a121 suggest the possibility of additive adverse cardiac effects with this drug combination in chronic coronary disease and recommend careful patient selection and close clinical monitoring. However, their overall im- pression is of beneficial action with few major acci- dents. For Bush et a122 these drugs together could de- crease the extent of histologic necrosis in experimental acute myocardial infarction in dogs. It would be useful to find harmless combinations of calcium-antagonist and @blocking drugs.
775

776 HEMODYNAMIC EFFECTS OF NICARDIPINE-PROPRANOLOL COMBINATION
TABLE I Control Hemodynamic Data in the Two Groups Before Nicardipine
Group N (n = 8) p Value
Group P + N (n = 8)
PR (set) HR (beats/min) RAP (mm Hg) SRVP (mm Hg) MPP (mm Hg) PWP (mm Hg) SLVP (mm Hg) LVEDP (mm Hg) DAP (mm Hg) MBP (mm Hg) LV dp/dt max (mm Hg.s-‘) Vmax (s-l) Cl (liters/mn/m*) SI (ml/beat) avD (ml OJliter VO,/m* (ml OJmin) SVR (dynes s cm-+) PVR (dynes s cm-s) LVSWI (g/beatlm2) Angiographic
EDVI (ml/m2) ESVI (ml/m*) Sla (ml/m*) HRa (beatslmin) Cla (liters/mn/m*) EF (%) Vcf (s-l)
0.17 f 0.02 NS 0.18 f 0.02 88 f 8 <0.05 80 f 8
6.3 f 2.3 NS 7.3 f 2.8 28 f 7 NS 30 f 8 18 f 4 NS 21 f 5 12 f 8 NS 13 f 4
145 f 21 NS 153 f 21 19 f 4 NS 22 f 8 78 4~ 8 NS 79 zk 12
102 f 12 NS 110 f 14 1,724 f 317 NS 1,423 f 287
1.19 f 0.14 NS 1.12 f 0.17 3.14 f 0.28 <O.Ol 2.33 f 0.30
48 f 8 NS 40 f 7 43 f 8 NS 50 f 9
135 f 22 NS 108 f 23 1,347 f 389 <O.Ol 1,990 f 394
97 f 38 -co.05 144 f 44 47 f 4 <0.05 84 f 14
89 f 13 NS 86 f 23 41 f 10 NS 44 f 20 49 f 7 <0.05 41 f 5 84 4~ 9 NS 63 h 5
3.08 f 0.40 <0.05 2.59 r!c 0.43 55 f 8 NS 50 f 9
0.85 f 0.21 NS 0.78 f 0.24
NS = not significant; other abbreviations as in Figures 1 to 4.
Few reports have been published in which the he- modynamic effects of the combined use of nicardipine and p-blocking drugs are explored. Rousseau et alz3 reported that nicardipine is a powerful arteriodilator with no detectable negative inotropic effects if used in combination with small doses of propranolol (0.1 mdkg).
We studied the hemodynamic effects of the intrave- nous injection of 5 mg of nicardipine in 2 comparable groups of patients (Table I] with proved coronary heart disease. One group had been treated chronically with large doses of propranolol.
Methods Patients: Sixteen men who underwent hemody-
namic evaluation for investigation of chest pain agreed to participate in the study. Patients with clinical signs of heart failure, bradycardia (heart rate less than 50 beats/min) or atrioventricular block were excluded. Other exclusion criteria were the inability to stop all treatment for at least 3 days or the absence of sinus rhythm.
These 16 patients were separated into 2 groups of 8 patients with similar pathologic conditions. Each group consisted of 2 patients with effort myocardial angina, 4 with inferior myocardial infarction and 2 with anterior myocardial infarction.
The mean age of patients in the first group [group N) was 51 years (range 37 to 611, mean weight was 78 f 14 kg and mean body area was 1.88 f 0.14 m2. They
had 1 to 3 stenoses (mean 1.5) (more than 70% luminal narrowing of a major coronary artery]. All previous treatment was stopped before the study for a period exceeding 5 times the half-life of the drugs.
The mean age of patients in the second group (group P + N), who had been previously treated with propranolol, was 55 years (range 41 to 74), mean weight was 74 f 13 kg and mean body area was 1.84 f 0.17 m2. They had a mean of 1.5 coronary stenoses. They re- ceived 160 to 480 mg/day of propranolol for at least 1 week before the study, with the last intake 2 hours before the examination; all other drug treatment was stopped at least 5 times the half-life of the drugs. Pro- pranolol plasma levels were a mean of 0.66 PM/liter (range 0.10 to 1.14) at the time of the measurements.
Protocol: Patients were examined in the morning, in the supine dorsal position, after fasting and without premeditation. Control measurements were made 10 minutes after the catheters had been inserted; includ- ed were right and left intracavitary pressures, cardiac output and left ventricular volumes by angiography. Ten minutes after ventriculography and during con- tinuous recording of left ventricular, aortic, pulmonary capillary wedge and right atria1 pressures, 5 mg of nicardipine was injected in 5 minutes through an in- travenous catheter. At the end of injection, all pres- sures were recorded. After 5 more minutes, i.e., 10 minutes after the beginning of the injection, pressures and cardiac output were again measured. After 5 min- utes more, pressures only were recorded. Twenty min- utes after the beginning of the infusion all measure- ments were recorded, including ventricular volumes by left ventriculography.
Materials: Right intracavitary pressures were mea- sured via a Swan-Ganz 7Fr catheter with 1 lumen in the right atrium and the other in the pulmonary artery. Cardiac output was measured by thennodilution. Left ventricular pressures were collected by a high-fidelity micromanometer (Millar 6Fr model PC 3601, inserted through an introducing sheath into the femoral artery. Mean aortic pressure was measured by the lateral ap- proach to the introducing sheath. Angiography was performed via a pigtail 7Fr catheter inserted into the other femoral artery. The left ventricular pressure tracing was recorded and also fed to a differential amplifier (Electronics for Medicine) to provide the peak positive first derivative of left ventricular pres- sure averaged over 15 cardiac cycles. The other cathe- ters were connected to a Statham 231D transducer and intracavitary pressures were transmitted via liquid columns. The signals were analyzed by an Electronics for Medicine electromanometer and recorded on a VR12 polygraph with 4 electrocardiographic leads. Left ventriculography was performed in the 30’ right anterior oblique position. Ventricular volumes were measured in end systole and end diastole according to the method of Dodgez4 and referred to body area. Cir- cumferential fiber velocity is the end-diastolic left ventricular middle diameter minus end-systolic left ventricular middle diameter divided by ejection time and by end-diastolic left ventricular middle diameter. Maximal shortening speed of myocardial fibers was
April 1. 1987 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 59 777
- c 5 10 15 20 c 5 10 15 20
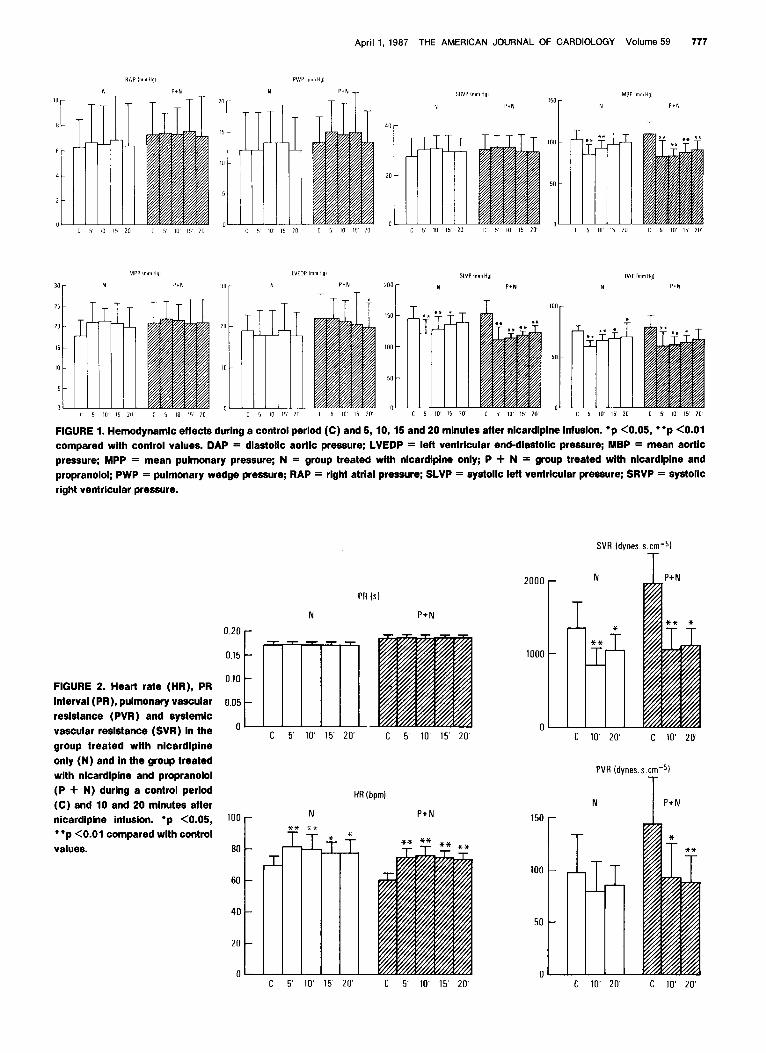
md 20 minutes after nlcardlpine infuslon. ‘p <0.05, l *p <O.Ol FIGURE 1. Hemoct .~ynamlc effects during a control period (C) and 5, 10, 15 compared with control values. DAP = dlastollc aortlc pressure; LVEDP = left ventricular end-dlastollc pressure; MBP = mean aortlc pressure; MPP = mean pulmonary pressure; N = group treated wlth nlcardlplne only; P + N = group treated with nlcardlplne and propranolol; PWP = pulmonary wedge pressure; RAP = right atria1 pressure; SLVP = systolic lefl ventricular pressure; SRVP = systolic right ventricular pressure.
SVR Idynes.s cmv5)
T
N
T P+N
PR Is)
N
II
0.20
0 15
0.10
0.05
0 ;
100
80
60
40
20
0 L
. I FIGURE 2. Heart rate (HR), PR
Interval (PR), pulmonary vascular resistance (PVR) and systemic vascular resistance (SVR) In the group treated wlth nlcardlplne only (N) and In the group treated wlth nlcardlplne and propranolol (P + N) durlng a control period (C) and 10 and 20 mlnutes after nicardlplne Infusion. l p <O.OS, “p <O.Ol compared with control values.
PVR (dynes.s cme5i
T HR (bpml
P+N N P+N

778 HEMODYNAMIC EFFECTS OF NICARDIPINE-PROPRANOLOL COMBINATION
measured using to the method of Grunk-Emeier et alz5 Other hemodynamic data were calculated using stan- dard formulas.
Statistical analysis: Values are mean f standard deviation. Comparison between the 2 groups during the control period was done by the Mann-Whitney U test. The statistical significance of the hemodynamic effects observed within each group was determined by the Friedman analysis of variance. When statistical significance appeared, the Wilcoxon matched-pairs signed-ranks test was used.
Comparison between the 2 groups of mean change between the control period and 20 minutes after nicar- dipine infusion was done by the Mann-Whitney U test.26
Results Hemodynamic control values are shown in Table I.
Results in both groups are similar to those usually found for patients with coronary artery disease.
P+N
** *-
avD (mloz/l)
N P+N
SI (ml/b)
N P+N ** T
+t -I* ,T
LVSWI 1gmlblm21
N T P+N T 60 r
Hemodynamic effects of nicardipine over 20 min- utes in both groups of patients (Fig. 1 to 4): In group N, without propranolol treatment, there was no differ- ence in PR interval, heart rate increased from 68 f 8 beats/min to 81 f 11 (p = 0.01) at 5 minutes and re- mained increased at 20 minutes (p <O.q5). Filling pres- sures remained stable. Aortic pressures decreased (p <0.001)-diastolic more than mean and systolic. Dia- stolic aortic pressure decreased from 76 f 6 to 60 f 7 mm Hg at 5 minutes (p = 0.01) and to 70 f 4 mm Hg at 20 minutes (p <0.05). Mean aortic pressure was no longer lower at the 20 minutes. Cardiac index in- creased from 3.14 f 0.26 to 4.52 f 0.57 liters/min/m2 at 10 minutes (p = 0.011 and remained increased at 20 minutes (p = 0.01). Systolic index varied in similar fashion. Systemic vascular resistance decreased from 1,347 f 369 to 826 f 219 dynes s cmm5 (p = 0.01) and was still diminished at 20 minutes. End-diastolic left ventricular volume index did not change and end- systolic left ventricular volume index decreased from
LVdp/dt Imm Hg. S-1 1
N P+N FIGURE 3. Oxygen arterial difference (avD), cardl- ac index (Cl), peak positive first derivatlve of the left ventricular pressure (LVdp/dt), left ventricular stroke work Index (LVSWI), systolic Index (SI) and maxlmal shortenlng speed of the myocardlal fiber
(Vmax) In the group treated wlth nlcardlplne only (N) and In the group treated wlth nlcardl&ne and propranolol (P + N) during a control perlod (C) and 10 and 20 mlnutes after nlcardlplne InfusIon. ‘p <0.05, l *p <O.Ql compared wlth control values.
c 5’ 10’ 15’ 20’ c 5’ 10’ 15’ 20
Vmax (S-II
N P+N
Til T

April 1, 1987 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 59 779
EDVI (ml/m’) Sla imllm’l EF%
P+N N P+N P+N
100
50
0
FIGURE 4. End-diastolic left ven- tricular volume Index (EDVI), ejection fraction (EF), end-sys- tolic left ventricular volume Index (ESVI), angiographlc cardiac ln- dex (Cla), anglographlc systolic Index (Sla) and circumferential fl- ber velocity rate (Vcf) In the group treated with nlcardlplne only (N) and In the second group treated with nlcardlplne and pro- pranolol (P -I N) during a control period (C) and 20 minutes after nicardlplne infusion. l p <0.05, l *p <O.Ol.
ESVI (ml/m’l
T, ** N
*
IIf C 20’
1 C
P+N P+N
4
2
0 ;
I
c
41 f 10 to 35 f 12 ml/m2 (p <0.05); as a result, the angiographic systolic index increased from 49 f 7 to 53 f 8 ml/beat/m2 (p <0.05) and ejection fraction in- creased from 55 f 6 to 61 f 8 % (p <0.05). The circum- ferential fiber velocity increased from 0.85 f 0.21 to 1.10 f 0.35 (p <0.05). The mean nicardipine plasma level was 48 f 17 rig/ml in group N and 83 f 36 rig/ml in group P + N.
In group P + N, previously treated with proprano- 101, there was no difference in PR interval; heart rate increased from 60 f 6 to 74 f 7 beats/min (p = 0.01) at 5 minutes and was still increased at 20 minutes (p = 0.01). Filling pressures remained stable. Aortic pres- sures decreased considerably, mean pressure from 110 f 14 to 82 f 18 mm Hg (p.= 0.01) at minute 5 and to 91 f llmmHg(p= 0.011 at minute 20. Cardiac index in- creased from 2.33 f 0.30 to 3.41 f 0.93 liters/min/m2 at 10 minutes (p <0.05) and to 3.56 f 1.14 at 20 minutes (p <O.Ol). Systolic index also increased from 40 f 7 to 49 f 15 ml/beat/m2 at 20 minutes (p <O.Ol). Systemic vascular resistance decreased dramatically, from 1,990 f 394 to 1,051 f 299 dynes s cmm5 (p = 0.01) at 10 minutes, and remained decreased, 1,105 f 262 dynes s
-5, at 20 minutes. Pulmonary vascular resistance ?&eased from 144 f 44 to 92 f 32 dynes s crnm5 at 10 minutes (p = 0.05) and remained decreased at 20 min- utes (p = 0.01). End-diastolic left ventricular volume index did not change and end-systolic left ventricular volume index decreased from 45 f 20 to 35 f 21 ml (p = 0.011; as a result, angiographic systolic index in- creased from 42 f 5 to 50 f 3.0 ml (p = 0.05) and ejection fraction increased from 50 f 9 to 61 f 16% (p
<0.05). Circumferential fiber velocity increased from 0.76 f 0.24 to 1.10 f 0.40 s-l.
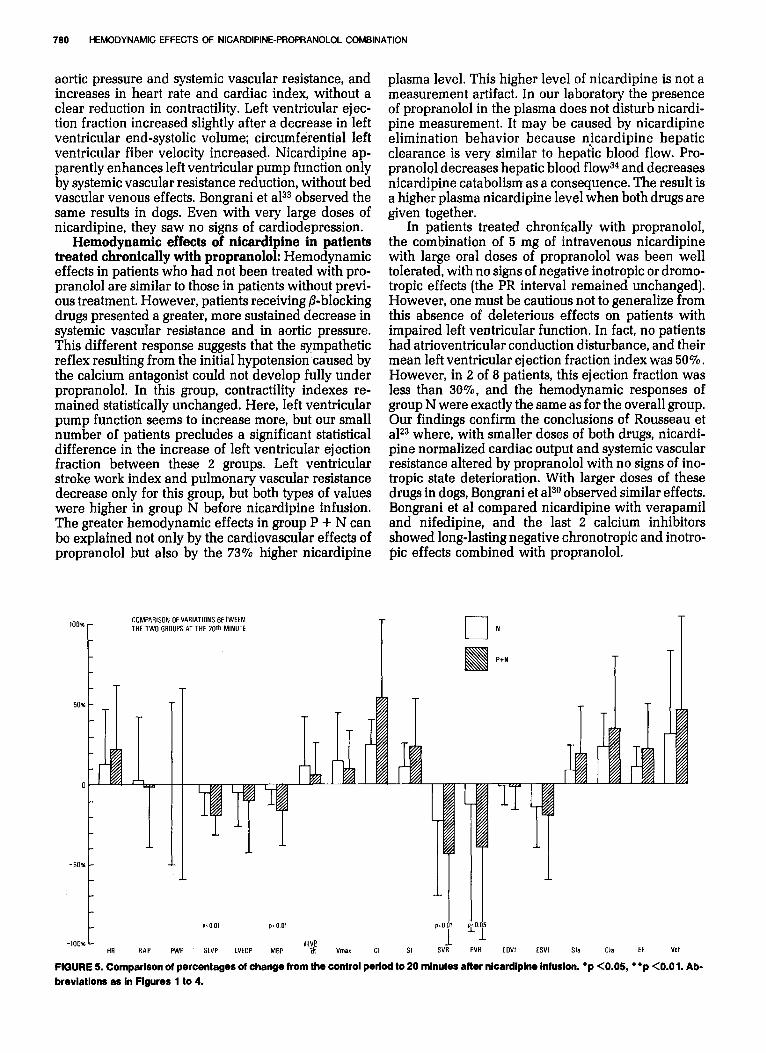
Hemodynamic changes at 20 minutes were statisti- cally identical in both groups, with 3 exceptions (Fig. 5). Mean aortic pressure decreased by 3% in group N and by 17% in group P + N (p <O.Ol). Systemic vascu- lar resistance decreased by 23% in group N and by 45% in group P + N (p < 0.01). Pulmonary vascular resistance did not decrease in group N but decreased by 40% in group P + N (p <0.05). The nicardipine plasma level was statistically higher in group P + N (p <O.Ol).
Discussion The hemodynamic effects of nicardipine in pa-
tients chronically treated with propranolol are not well known. The present study focuses on the deleterious negative inotropic effects of the combined use of ni- cardipine and propranolol in 2 groups of patients with similar pathologic conditions. Only the data influ- enced directly by propranolol differed between the 2 groups: in particular, cardiac index and heart rate were lower and arterial resistance was higher in the group treated with propranolol. These effects of pro- pranolol are well known2’ and have been confirmed by several investigators.2*-30
Hemodynamic effects of nicardipine in the nicar- dipine group: In patients not previously treated with propranolol, the effects of nicardipine administration were those usually found when the drug is adminis- tered intravenously in humans and at high therapeutic doses.23r31s32 These effects are primarily reductions in
aortic pressure and systemic vascular resistance, and increases in heart rate and cardiac index, without a clear reduction in contractility. Left ventricular ejec- tion fraction increased slightly after a decrease in left ventricular end-systolic volume; circumferential left ventricular fiber velocity increased. Nicardipine ap- parently enhances left ventricular pump function only by systemic vascular resistance reduction, without bed vascular venous effects. Bongrani et aP3 observed the same results in dogs. Even with very large doses of nicardipine, they saw no signs of cardiodepression.
Hemodynamic effects of nicardipine in patients treated chronically with propranolol: Hemodynamic effects in patients who had not been treated with pro- pranolol are similar to those in patients without previ- ous treatment. However, patients receiving /3-blocking drugs presented a greater, more sustained decrease in systemic vascular resistance and in aortic pressure. This different response suggests that the sympathetic reflex resulting from the initial hypotension caused by the calcium antagonist could not develop fully under propranolol. In this group, contractility indexes re- mained statistically unchanged. Here, left ventricular pump function seems to increase more, but our small number of patients precludes a significant statistical difference in the increase of left ventricular ejection fraction between these 2 groups. Left ventricular stroke work index and pulmonary vascular resistance decrease only for this group, but both types of values were higher in group N before nicardipine infusion. The greater hemodynamic effects in group P + N can be explained not only by the cardiovascular effects of propranolol but also by the 73% higher nicardipine
COMPARISON OFVARIATIONS BETWEEN THE TWO GAOUPSATTTHE 20th MINUTE r-l N -
P+N
T T
dlVP HA RAP PWP SLVP LVEOP MBP ai Vmax Cl SI PVR EOVI WI Sla Cla fF VCf
FIGURE 5. Comparison ot percentages of change from the control period to 20 minutes after nlcardiplne infusion. ‘p <0.05, l *p <O.Ol. Ab- breviations as in Figures 1 to 4.
plasma level. This higher level of nicardipine is not a measurement artifact. In our laboratory the presence of propranolol in the plasma does not disturb nicardi- pine measurement. It may be caused by nicardipine elimination behavior because nicardipine hepatic clearance is very similar to hepatic blood flow. Pro- pranolol decreases hepatic blood flow34 and decreases nicardipine catabolism as a consequence. The result is a higher plasma nicardipine level when both drugs are given together.
In patients treated chronically with propranolol, the combination of 5 mg of intravenous nicardipine with large oral doses of propranolol was been well tolerated, with no signs of negative inotropic or dromo- tropic effects (the PR interval remained unchanged]. However, one must be cautious not to generalize from this absence of deleterious effects on patients with impaired left ventricular function. In fact, no patients had atrioventricular conduction disturbance, and their mean left ventricular ejection fraction index was 50%. However, in 2 of 8 patients, this ejection fraction was less than 80%. and the hemodynamic responses of group N were exactly the same as for the overall group. Our findings confirm the conclusions of Rousseau et alz3 where, with smaller doses of both drugs, nicardi- pine normalized cardiac output and systemic vascular resistance altered by propranolol with no signs of ino- tropic state deterioration. With larger doses of these drugs in dogs, Bongrani et aP” observed similar effects. Bongrani et al compared nicardipine with verapamil and nifedipine, and the last 2 calcium inhibitors showed long-lasting negative chronotropic and inotro- pit effects combined with propranolol.

April 1,1987 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 59 781
Acknowledgment: We gratefully acknowledge the statistical analysis by Yolande Loria and Remy Frere and the secretarial assistance of Anne Marie Fried- mann. References 1. Fleckenstein A. Specific inhibitors and promoters of calcium action in the excitation-contraction coupling of heart muscle and their role in the preven- tion or production of myocardiol lesions. In: Harris P, Opie LH, eds. Calcium and the Heart. London, 1971: Academic Press, 135-188. 2. Lindner E. Phenyl-propyl-diphenyl-propyl-amin, eine neue Substanz mit coronar-gefaesserweiternder Wirkung. Arzneim Forsch 1960;10:569. 3. Ryden L, Saetre H. The hemodynamic effect of verapamil. Eur J CIin Pharmacol l97l;3:l53-157. 4. Atterhog JH, Ekelund LG. Hemodynamic effects of intravenous verapamil at rest and during exercise in subjectively healthy middle-aged men. Eur J CIin Pharmacol 1975;8:317-322. 5. Low RI, Takeda P, Mason DT, DeMaria AN. The effects of calcium channel blocking agents on cardiovascular function. Am J Cardiol 1982;49:547-553. 6. Sing BN, Elirodt G. Nademanee K. Calcium antagonists-cardiocirculation effects and therapeutic applications. in: Hurst JW, ed. Clinical Essays on the Heart. New York: McGraw-Hill, 1984:85-97. 7. Nakaya H, Schwartz A, Millard RW. Reflex chronotrophic and inotropic effects of calcium channel-blocking agents in conscious dogs. Circ Res 1983;52:302-311. 8. Levenson ]A, Safar ME, Bouthier JE, Benetos AM, Simon AC. Baroreflex response and vasodilating drugs in essential hypertension, Chest 1983;83:325- 327. 9. Robson RH, Wishwanath MC. Nifedipine and beta blockade as a cause of cardiac failure. Br Med J 1982;284:104. 10. Opie LH, White DA. Adverse interaction between nifedipine and beta blockade. Br Med J 1980;281:1462. 11. Denis B. Pellet J, Machecourt J, Martin-Noel P. VBrapamiI et beta-blo- quant: une association thbrapeutique dangereuse. Nouv Presse MBd 1977; 6:2075 12. Wayne VS, Harper RW. Laufer E, Federman J, Anderson ST. Adverse interaction between beta-adrenergic blocking drugs and verapamil-report of three cases. Aust NZ J Med 1982:12:285-289. 13. Ekelund LG, Oro L. Antiangina efficiency of nifedipine with and without a beta blocker studied with exercise test. A double-blind randomized subacute study. CIin Cardiol 1979;2:263-211. 14. Pfisterer M. Muller-Brand J, Burkart F. Combined acebutoIoI/nifedipine therapy in patients with chronic coronary artery disease: additional improve- ment of ischemia induced left ventricular dysfunction. Am J Cardiol 1982; 49:1259-1268. 15. Rowland E, Razis P, Sugrue D, Krikler DM. Acute and chronic haemodyn- amic and electrophysiological effects of nifedipine in patients receiving aten- 0101. Br Heart J 1983;50:383-389. 16. Leon MB, Rosing DR, Bonaw RO, Lipson LC, Epstein SE. Clinical efficacy of verapamil alone and combined with propranolol in treating patients with
chronic stable angina pectoris. Am J Cardiol 1981;48:131-139, 17. Hung I. Lamb IH, Connoly SJ. Jutzy KR, Goris ML, Schroeder JS. The effect af dihiazem and propranolol, alone and in combination, on exercise performance and left ventricular function in patients with stable effort angi- na; a double-blind, randomized and placebo-controlled study, Circulation 1983;67:560-567. lg. Wolfe CL, Tilton GD, Hillis D. El Ashram N. Winniford MD. Acute hemodynamic and electrophysiologic effects of propranolol in patients re- ceiving diltiazem. Am J Cardiol 1985;56:47-50. 19. Oesterle SN, Alderman EL, Beier-Scott L, Bairn DS, Rothman MT, Schroe- der JS. Diftiazem and propranolol combination: hemodynamic effects follow- ing acute intravenous administration. Am Heart J 1986;111:489-497. 20. Rocha P, Baron B. Delestrain A. Path6 M, Cazor JL, Kahn JC. Hemody- namic effects of intravenous diltiazem in patients treated chronically with propranolol. Am Heart J 1986;111:82-68. 21. Lean MB, Rosing DR, Bonow RO. Epstein SE. Combination therapy with calcium-channel blockers and beta blockers for chronic stable angina pecto- ris. Am J Cardiol 1985;55:69B-BOB. 22. Bush LR, Buja LM, Tilton G, Wathen M, April1 P, Ashton J, Willerson JT. Effects of propranolol and diltiazem alone and in combination on the recov- ery of left ventricular segmental function after temporary coronary occlusion and long-term reperfusion in conscious dog. Circulation 1985;72:413-430. 23. Rousseau MF, Etienne J, Van Mechelen H, Veriter C. Pauleur H. Hemo- dynamic and cardiac effects of nicardipine in patients with coronary artery disease. J Cardiovasc Pharm 1984;6:833-839. 24. Dodge HT. Determination of left ventricular volume and mass. Radio1 Clin North Am 1971;9:459-467. 25. Grunk-Emeier GL. Burg BA, Anderson RP. A simple method for calculat- ing Vmax [abstr). CIin Aes 1973;31:422. 26. Siegel S. Nonparametric Statistics for the Behavioral Sciences. New York: McGraw Hill, 1956. 27. Epstein SE, Branwald E. Beta-adrenergic receptor blocking drugs: mech- anisms of action and clinical appIications. N EngI J Med 1966;275:1106. 28. Ulrich M. Frochlich ED, Dustan AP, Page IH. Immediate hemodynamic effects of beta-adrenergic blockade with propranolol in normotensive man. Circufation 1968;37:411-416. 29. Tarazi RC. Dustan HP. Beta-adrenergic blockade in hypertension, Am J Cardiol 1972;29:633-640. 30. Tarazi RC. Dustan HP, Bravo EL. Haemodynamic effects of propranolol in hypertension: a review. Postgrad Med J 1976;52:suppl 4:92-100. 31. Lambert CR, Hill ]A, Feldman RL, Pepine CJ. Effects of nicardipine on Ieft ventricular function and energetics in man. Int J Cardial 1986;10:237-249. 32. Berland J, Savin T, Cribier A, Letac B. Effects of low dose nicardipine on systemic and coronary hemodynamics during rapid atria1 pacing in patients with ischemic heart disease (abstr). JACC 1988;7:179A. 33. Bongrani S, Razzeti R, Schiantarelli P. Cardiovascular effects of nicardi- pine in anesthetized open-chest dogs in the absence and presence of beta- adrenergic receptor blockade: a comparison with nifedipine and verapamil. J Cardiovasc Pharmacal 1985;7:899-905. 34. Parker G, Danheshmed TK, Roberts JC. Do beta blockers differ in their effects on hepatic microsomal enzymes and liver blood flow? J Clin Pharma- co1 1984;24:493-499.